A cold environment is defined by conditions that cause greater than normal body heat losses. In this context “normal” refers to what people experience in everyday life under comfortable, often indoor conditions, but this may vary due to social, economic or natural climatic conditions. For the purpose of this article environments with an air temperature below 18 to 20ºC would be considered cold.
Cold work comprises a variety of industrial and occupational activities under different climatic conditions (see table 1). In most countries the food industry requires work under cold conditions—normally 2 to 8ºC for fresh food and below –25ºC for frozen food. In such artificial cold environments, conditions are relatively well defined and the exposure is about the same from day to day.
Table 1. Air temperatures of various cold occupational environments
|
–120 ºC |
Climatic chamber for human cryotherapy |
|
–90 ºC |
Lowest temperature at south polar base Vostock |
|
–55 ºC |
Cold store for fish meat and production of frozen, dried products |
|
–40 ºC |
“Normal” temperature at polar base |
|
–28 ºC |
Cold store for deep-frozen products |
|
+2 to +12 ºC |
Storage, preparation and transportation of fresh, alimentary products |
|
–50 to –20 ºC |
Average January temperature of northern Canada and Siberia |
|
–20 to –10 ºC |
Average January temperature of southern Canada, northern Scandinavia, central Russia |
|
–10 to 0 ºC |
Average January temperature of northern USA, southern Scandinavia, central Europe, parts of middle and far East, central and northern Japan |
Source: Modified from Holmér 1993.
In many countries the seasonal climatic changes imply that outdoor work and work in unheated buildings for shorter or longer periods has to be carried out under cold conditions. The cold exposure may vary considerably between different locations on the earth and type of work (see table 1). Cold water presents another hazard, encountered by people engaged in, for example, offshore work. This article deals with responses to cold stress, and preventive measures. Methods for assessment of cold stress and acceptable temperature limits according to recently adopted international standards are dealt with elsewhere in this chapter.
Cold Stress and Work in the Cold
Cold stress may be present in many different forms, affecting the whole-body heat balance as well as the local heat balance of extremities, skin and lungs. The type and nature of cold stress is extensively described elsewhere in this chapter. The natural means of dealing with cold stress is by behavioural action—in particular, change and adjustment of clothing. Sufficient protection prevents cooling. However, protection itself may cause unwanted, adverse effects. The problem is illustrated in figure 1.
Figure 1. Examples of cold effects.
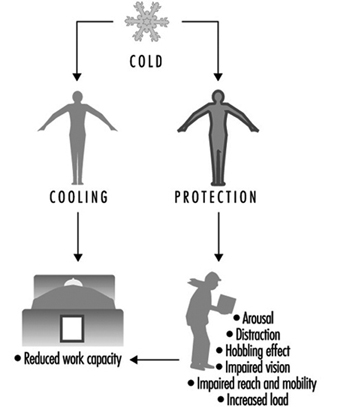
Cooling of the whole body or parts of the body results in discomfort, impaired sensory and neuro-muscular function and, ultimately, cold injury. Cold discomfort tends to be a strong stimulus to behavioural action, reducing or eliminating the effect. Prevention of cooling by means of donning cold-protective clothing, footwear, gloves and headgear interferes with the mobility and dexterity of the worker. There is a “cost of protection” in the sense that movements and motions become restricted and more exhausting. The continuous need for adjustment of the equipment to maintain a high level of protection requires attention and judgement, and may compromise factors such as vigilance and reaction time. One of the most important objectives of ergonomics research is the improvement of the functionality of clothing while maintaining cold protection.
Accordingly, effects of work in the cold must be divided into:
- effects of tissue cooling
- effects of protective measures (“cost of protection”).
On exposure to cold, behavioural measures reduce the cooling effect and, eventually, allow the maintenance of normal thermal balance and comfort. Insufficient measures evoke thermoregulatory, physiologically compensatory reactions (vasoconstriction and shivering). The combined action of behavioural and physiological adjustments determines the resulting effect of a given cold stress.
In the following sections these effects will be described. They are divided into acute effects (occurring within minutes or hours), long-term effects (days or even years) and other effects (not directly related to cooling reactions per se). Table 2 presents examples of reactions associated with the duration of cold exposure. Naturally, types of responses and their magnitude depend largely upon the stress level. However, long exposures (days and longer) hardly involve the extreme levels that can be attained for a short time.
Table 2. Duration of uncompensated cold stress and associated reactions
|
Time |
Physiological effects |
Psychological effect |
|
Seconds |
Inspiratory gasp |
Skin sensation, discomfort |
|
Minutes |
Tissue cooling |
Performance decrement |
|
Hours |
Impaired physical work capacity |
Impaired mental function |
|
Days/months |
Non-freezing cold injury |
Habituation |
|
Years |
Chronic tissue effects (?) |
Acute effects of cooling
The most obvious and direct effect of cold stress is the immediate cooling of the skin and the upper airways. Thermal receptors respond and a sequence of thermoregulatory reactions is initiated. The type and magnitude of reaction is determined primarily by the type and severity of cooling. As previously mentioned, peripheral vasoconstriction and shivering are the main defence mechanisms. Both contribute to preserving body heat and core temperature, but compromise cardiovascular and neuro-muscular functions.
However, the psychological effects of cold exposure also modify the physiological reactions in a complex and partly unknown way. The cold environment causes distraction in the sense that it requires increased mental effort to handle the new stress factors (avoid cooling, take protective measures, etc.). On the other hand, the cold also causes arousal, in the sense that the increased stress level increases sympathetic nervous activity and, thereby, preparedness for action. In normal conditions people use only minor portions of their capacity, thereby preserving a large buffer capacity for unexpected or demanding conditions.
Cold perception and thermal comfort
Most humans experience a sensation of thermal neutrality at an operative temperature between 20 and 26ºC when engaged in very light, sedentary work (office work at 70 W/m2) in appropriate clothing (insulation values between 0.6 and 1.0 clo). In this state and in the absence of any local thermal imbalances, like draught, people are in thermal comfort. These conditions are well documented and specified in standards such as ISO 7730 (see the chapter Controlling the indoor environment in this Encyclopaedia).
Human perception of cooling is closely related to whole-body heat balance as well as local tissue heat balance. Cold thermal discomfort arises when body heat balance cannot be maintained due to inappropriate matching of activity (metabolic heat production) and clothing. For temperatures between +10 and +30ºC, the magnitude of “cold discomfort” in a population can be predicted by Fanger’s comfort equation, described in ISO 7730.
A simplified and reasonably accurate formula for computation of the thermoneutral temperature (t) for the average person is:
t = 33.5 – 3·Icl – (0.08 + 0.05·Icl)·M
where M is the metabolic heat measured in W/m2 and Icl the insulation value of clothing measured in clo.
The required clothing insulation (clo value) is higher at +10ºC than that calculated with the IREQ method (calculated required insulation value) (ISO TR 11079, 1993). The reason for this discrepancy is the application of different “comfort” criteria in the two methods. ISO 7730 focuses heavily on thermal comfort and allows for considerable sweating, whereas ISO TR 11079 allows only “control” sweating at minimal levels—a necessity in the cold. Figure 2 depicts the relationship between clothing insulation, activity level (heat production) and air temperature according to the equation above and the IREQ method. The filled areas should represent the expected variation in required clothing insulation due to different levels of “comfort”.
Figure 2. Optimal temperature for thermal "comfort" as function of clothing and activity level (![]() ).
).

The information in figure 2 is only a guide for establishing optimal indoor thermal conditions. There is considerable individual variation in perception of thermal comfort and discomfort from cold. This variation originates from differences in clothing and activity patterns, but subjective preferences and habituation also contribute.
In particular, people engaged in very light, sedentary activity become increasingly susceptible to local cooling when air temperature drops below 20 to 22ºC. In such conditions air velocity must be kept low (below 0.2 m/s), and additional insulative clothing must be selected to cover sensitive body parts (e.g., head, neck, back and ankles). Seated work at temperatures below 20ºC requires insulated seat and backrest to reduce local cooling due to compression of clothing.
When ambient temperature falls below 10ºC, the comfort concept becomes more difficult to apply. Thermal asymmetries become “normal” (e.g., cold face and cold air inhalation). Despite an optimal body heat balance, such asymmetries may be felt to be uncomfortable and require extra heat to eliminate. Thermal comfort in the cold, unlike under normal indoor conditions, is likely to coincide with a slight feeling of warmth. This should be remembered when cold stress is assessed using the IREQ index.
Performance
Cold exposure and the associated behavioural and physiological reactions have an impact on human performance at various levels of complexity. Table 3 presents a schematic overview of different types of performance effects that may be anticipated with mild and extreme cold exposure.
Table 3. Indication of anticipated effects of mild and severe cold exposure
|
Performance |
Mild cold exposure |
Severe cold exposure |
|
Manual performance |
0 – |
– – |
|
Muscular performance |
0 |
– |
|
Aerobic performance |
0 |
– |
|
Simple reaction time |
0 |
– |
|
Choice reaction time |
– |
– – |
|
Tracking, vigilance |
0 – |
– |
|
Cognitive, mental tasks |
0 – |
– – |
0 indicates no effect; – indicates impairment; – – indicates strong impairment; 0 – indicates contradictory finding.
Mild exposure in this context implies no or negligible body core cooling and moderate cooling of the skin and extremities. Severe exposure results in negative heat balance, a drop in core temperature and concomitant pronounced lowering of temperature of the extremities.
The physical characteristics of mild and severe cold exposure are very much dependent on the balance between internal body heat production (as a result of physical work) and heat losses. Protective clothing and ambient climatic conditions determine the amount of heat loss.
As previously mentioned, cold exposure causes distraction and cooling (figure 1). Both have an impact on performance, although the magnitude of impact varies with the type of task.
Behaviour and mental function are more susceptible to the distraction effect, whereas physical performance is more affected by cooling. The complex interaction of physiological and psychological responses (distraction, arousal) to cold exposure is not fully understood and requires further research work.
Table 4 indicates reported relationships between physical performance and temperatures of the body. It is assumed that physical performance is highly dependent on tissue temperature and deteriorates when temperature of vital tissue and organ parts drops. Typically, manual dexterity is critically dependent upon finger and hand temperature, as well as muscle temperature of the forehand. Gross muscular activity is little affected by local surface temperature, but very sensitive to muscle temperature. Since some of these temperatures are related to each other (e.g., core and muscle temperature) it is difficult to determine direct relationships.
Table 4. Importance of body tissue temperature for human physical performance
|
Performance |
Hand/finger skin temperature |
Mean skin temperature |
Muscle temperature |
Core temperature |
|
Simple manual |
– |
0 |
– |
0 |
|
Complex manual |
– – |
(–) |
– – |
– |
|
Muscular |
0 |
0 – |
– – |
0 – |
|
Aerobic |
0 |
0 |
– |
– – |
0 indicates no effect; – indicates impairment with lowered temperature; – – indicates strong impairment; 0 – indicates contradictory findings; (–) indicates possible minor effect.
The overview of performance effects in table 3 and 4 is by necessity very schematic. The information should serve as a signal for action, where action means a detailed assessment of conditions or undertaking of preventive measures.
An important factor contributing to performance decrements is exposure time. The longer the cold exposure, the greater the effect upon the deeper tissues and neuro-muscular function. On the other hand, factors such as habituation and experience modify the detrimental effects and restore some of the performance capacity.
Manual performance
Hand function is very susceptible to cold exposure. Due to their small mass and large surface area, hands and fingers lose much heat while maintaining high tissue temperatures (30 to 35ºC). Accordingly, such high temperatures can be maintained only with a high level of internal heat production, allowing for sustained high blood flow to the extremities.
Hand heat loss can be reduced in the cold by wearing appropriate handwear. However, good handwear for cold weather means thickness and volume, and, consequently, impaired dexterity and manual function. Hence, manual performance in the cold cannot be preserved by passive measures. At best, the reduction in performance may be limited as the result of a balanced compromise between the choice of functional handwear, work behaviour and exposure scheme.
Hand and finger function is much dependent on local tissue temperatures (figure 3). Fine, delicate and fast finger movements deteriorate when tissue temperature drops by a few degrees. With more profound cooling and temperature drop, gross hand functions are also impaired. Significant impairment in hand function is found at hand skin temperatures around 15ºC, and severe impairments occur at skin temperatures about 6 to 8ºC due to blocking of function of sensory and thermal skin receptors. Depending on task requirements, it may be necessary to measure skin temperature at several sites on the hand and fingers. Temperature of the fingertip may be more than ten degrees lower than on the back of the hand under certain exposure conditions.
Figure 3. Relation between finger dexterity and finger skin temperature.
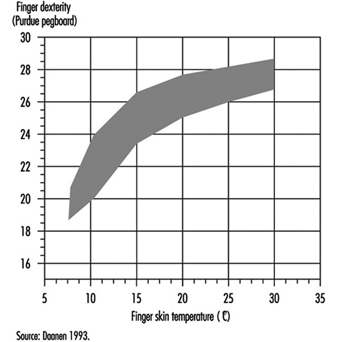
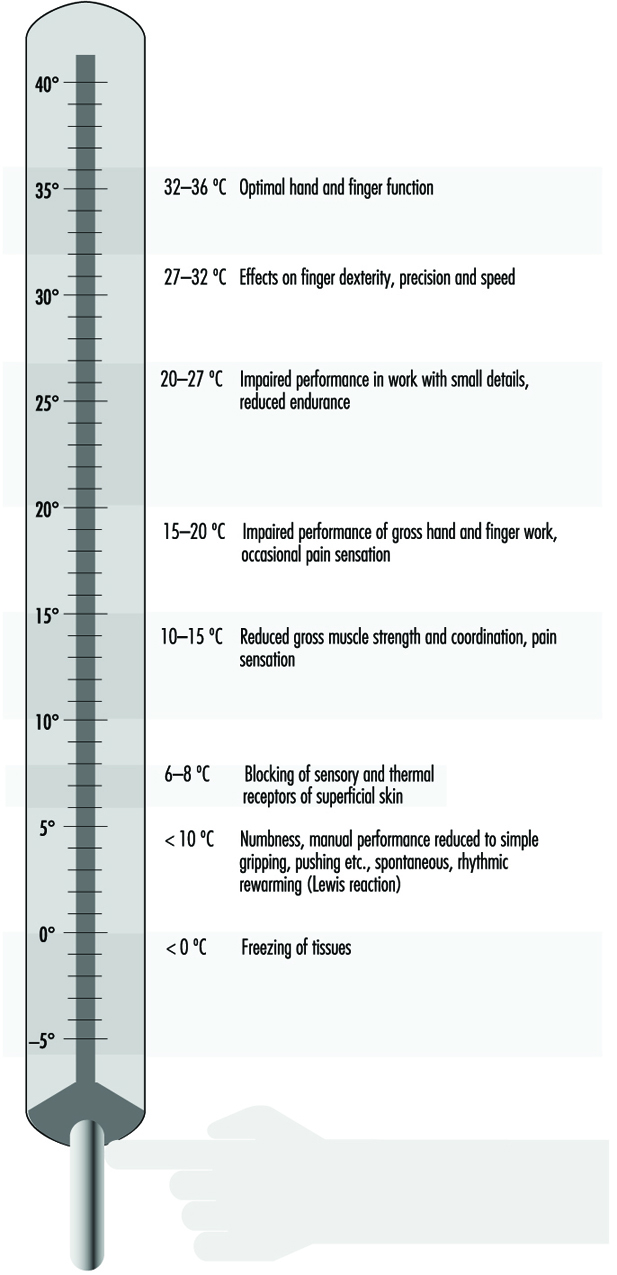
Figure 4 indicates critical temperatures for different types of effects on manual function.
Figure 4. Estimated gross effects on manual performance at different levels of hand/finger temperature.
Neuro-muscular performance
It is evident from figures 3 and 4 that there is a pronounced effect of cold on muscular function and performance. Cooling of muscle tissue reduces blood flow and slows down neural processes like transmission of nerve signals and synaptic function. In addition, viscosity of tissues increases, resulting in higher internal friction during motion.
Isometric force output is reduced by 2% per ºC of lowered muscle temperature. Dynamic force output is reduced by 2 to 4% per ºC of lowered muscle temperature. In other words, cooling reduces the force output of muscles and has an even greater effect on dynamic contractions.
Physical work capacity
As previously mentioned, muscular performance deteriorates in the cold. With impaired muscle function there is a general impairment of physical work capacity. A contributing factor to the reduction in aerobic work capacity is the increased peripheral resistance of the systemic circulation. Pronounced vasoconstriction increases central circulation, eventually leading to cold diuresis and elevated blood pressure. Cooling of the core may also have a direct effect on the contractility of the heart muscle.
Work capacity, as measured by maximal aerobic capacity, decreases by 5 to 6% per ºC lowered core temperature. Thus endurance may deteriorate rapidly as the practical consequence of the lowered maximal capacity and with an increased energy requirement of muscular work.
Other cold effects
Body temperatures
As the temperature drops, the surface of the body is most affected (and also most tolerant). Skin temperature may fall below 0ºC in a few seconds when the skin is in contact with very cold metal surfaces. Likewise hand and finger temperatures may decrease by several degrees per minute under conditions of vasoconstriction and poor protection. At normal skin temperature the arms and hands are superperfused due to peripheral arterio-venous shunts. This creates warmth and enhances dexterity. Cooling of the skin shuts these shunts and decreases perfusion in hands and feet to one tenth. The extremities constitute 50% of the body surface and 30% of its volume. The return of blood passes via deep veins concomitant to the arteries, thereby reducing heat loss according to the counter-current principle.
Adrenergic vasoconstriction does not occur in the head-neck region, which must be borne in mind in emergency situations to prevent hypothermia. A bareheaded individual may lose 50% or more of his or her resting heat production at subzero temperatures.
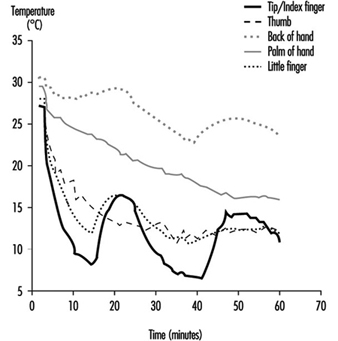
A high and sustained rate of whole-body heat loss is required for the development of hypothermia (drop in core temperature) (Maclean and Emslie-Smith 1977). The balance between heat production and heat loss determines the resultant cooling rate, be it a whole-body cooling or a local cooling of a part of the body. The conditions for heat balance can be analysed and assessed on the basis of the IREQ index. A remarkable response to local cooling of protruding parts of the human body (e.g., fingers, toes and ears) is the hunting phenomenon (Lewis reaction). After an initial drop to a low value, finger temperature increases by several degrees (figure 5). This reaction is repeated in a cyclic manner. The response is very local—more pronounced at the tip of the finger than at the base. It is absent in the hand. The response on the palm of the hand most likely reflects the variation in temperature of the blood flow supplying the fingers. The response can be modified by repeated exposures (amplified), but is more or less abolished in association with whole-body cooling.
Figure 5. Cold-induced vasodilatation of finger vessels causing cyclic rises in tissue temperature.
Progressive cooling of the body results in a number of physio-logical and mental effects. Table 16 indicates some typical responses associated with different levels of core temperature.
Table 5. Human responses to cooling: Indicative reactions to different levels of hypothermia
|
Phase |
Core |
Physiological |
Psychological |
|
Normal |
37 36 |
Normal body temperature Vasoconstriction, cold hands and feet |
Thermoneutral sensation Discomfort |
|
Mild hypothermia |
35 34 33 |
Intense shivering, reduced work capacity Fatigue Fumbling and stumbling |
Impaired judgment, disorientation, apathy Conscious and |
|
Moderate |
32 31 30 29 |
Muscle rigidity Faint breathing No nerve reflexes, heart rate slow and almost unnoticeable |
Progressive Consciousness clouds Stuporous |
|
Severe |
28 27 25 |
Heart dysrhythmias (atrial Pupils non reactive to Death due to ventricular fibrillation or asystole |
Heart and circulation
Cooling of the forehead and head elicit acute elevation of systolic blood pressure and, eventually, elevated heart rate. A similar reaction may be seen when putting bare hands in very cold water. The reaction is of short duration, and normal or slightly elevated values are attained after seconds or minutes.
Excessive body heat loss causes peripheral vasoconstriction. In particular, during the transient phase the increased peripheral resistance results in an elevation of systolic blood pressure and increased heart rate. Cardiac work is greater than it would be for similar activities at normal temperatures, a phenomenon painfully experienced by persons with angina pectoris.
As previously mentioned, deeper tissue cooling generally slows down the physiological processes of cells and organs. Cooling weakens the innervation process and suppresses heart contractions. Contraction power is reduced and, in addition to the increase in peripheral resistance of the blood vessels, cardiac output is reduced. However, with moderate and severe hypothermia, cardiovascular function declines in relation to the general reduction in metabolism.
Lungs and airways
Inhalation of moderate volumes of cold, dry air presents limited problems in healthy persons. Very cold air may cause discomfort, in particular, with nasal breathing. High ventilation volumes of very cold air may also cause micro-inflammation of the mucosal membrane of the upper airways.
With progression of hypothermia, lung function is depressed contemporaneously with the general reduction in body meta-bolism.
Functional aspects (work capacity)
A fundamental requirement for function in cold environments is the provision of sufficient protection against cooling. However, protection itself may seriously interfere with conditions for performance. The hobbling effect of clothing is well-known. Headgear and helmets interfere with speech and vision, and handwear impairs manual function. Whereas protection is necessary for preservation of healthy and comfortable working conditions, the consequences in terms of impaired performance must be fully recognized. Tasks take longer to complete and require greater effort.
Protective clothing against cold may easily weigh 3 to 6 kg including boots and headwear. This weight adds to workload, in particular during ambulatory work. Also, friction between layers in multi-layer clothing yields resistance to motion. The weight of boots should be kept low, since added weight on the legs contributes relatively more to workload.
Work organization, workplace and equipment should be adapted to the specific requirements of a cold work task. More time must be allowed for tasks, and frequent breaks for recovery and warming are needed. The workplace must allow for easy movements, despite bulky clothing. Similarly, equipment must be designed so that it can be operated by a gloved hand or insulated in the case of bare hands.
Cold Injuries
Serious injuries by cold air are in most cases preventable and occur only sporadically in civilian life. On the other hand, these injuries are often of major significance in war and in cataclysms. However, many workers run the risk of getting cold injuries in their routine activities. Outdoor work in harsh climate (as in arctic and subarctic areas—for example, fishing, agriculture, construction, gas and oil exploration and reindeer herding) as well as indoor work carried out in cold environments (as in food or warehousing industries) can all involve danger of cold injury.
Cold injuries may be either systemic or localized. The local injuries, which most often precede systemic hypothermia, constitute two clinically different entities: freezing cold injuries (FCI) and non-freezing cold injuries (NFCI).
Freezing cold injuries
Pathophysiology
This type of local injury occurs when heat loss is sufficient to allow a true freezing of the tissue. Besides a direct cryogenic insult to the cells, vascular damage with decreased perfusion and tissue hypoxia are contributing pathogenic mechanisms.
The vasoconstriction of cutaneous vessels is of great importance in the origin of a frostbite. Due to wide arteriovenous shunts, peripheral structures such as hands, feet, nose and ears are superperfused in a warm environment. Only about one-tenth of the blood flow in the hands, for example, is needed for tissue oxygenation. The rest creates warmth, thereby facilitating dexterity. Even in the absence of any decrease in core temperature, local cooling of the skin occludes these shunts.
In order to protect the viability of the peripheral parts of the extremities during cold exposure, an intermittent cold-induced vasodilatation (CIVD) takes place. This vasodilatation is a result of opening of the arteriovenous anastomoses and occurs every 5 to 10 minutes. The phenomenon is a compromise in the human physiological plan to conserve heat and yet intermittently preserve function of hands and feet. The vasodilatation is perceived by the person as periods of prickling heat. CIVD becomes less pronounced as body temperature decreases. Individual variations in the degree of CIVD might explain different susceptibility to local cold injury. People indigenous to a cold climate present a more pronounced CIVD.
In contrast to cryopreservation of living tissue, where ice crystallization occurs both intra- and extracellularly, the clinical FCI, with a much slower rate of freezing, produces only extra- cellular ice crystals. The process is an exothermic one, liberating heat, and therefore tissue temperature remains at the freezing point until freezing is complete.
As the extracellular ice crystals grow, extracellular solutions are condensed, causing this space to become a hyperosmolar milieu, which leads to passive diffusion of water from the intracellular compartment; that water in turn freezes. This process progresses until all “available” water (not otherwise bound to protein, sugar and other molecules) has been crystallized. Cell dehydration alters protein structures, membrane lipids and cellular pH, leading to destruction incompatible with cell survival. Resistance to FCI varies in different tissues. Skin is more resistant than muscles and nerves, for example, which might be the result of a smaller water content both intra- and intercellularly in the epidermis.
The role of indirect haemorheological factors was earlier interpreted as similar to that found in non-freezing cold injuries. Recent studies in animals have, however, shown that freezing causes lesions in the intima of arterioles, venules and capillaries prior to any evidence of damage to other skin elements. Thus, it is obvious that the rheological part of the pathogenesis of FCI is also a cryobiological effect.
When a frostbite is rewarmed, water begins to rediffuse to the dehydrated cells, leading to intracellular swelling. Thawing induces maximal vascular dilation, creating oedema and blister formation due to the endothelial (internal layer of the skin) cell injury. Disruption of the endothelial cells exposes the basement membrane, which initiates platelet adhesions and starts the coagulation cascade. The following blood stagnation and thrombosis induce anoxia.
As it is the heat loss from the exposed area that determines the risk of getting a frostbite, wind-chill is an important factor in this respect, and this means not only the wind which is blowing but also any movement of air past the body. Running, skiing, skijoring and riding in open vehicles must be considered in this context. However, the exposed flesh will not freeze as long as the ambient temperature is above the freezing point, even at high wind velocities.
Use of alcohol and tobacco products as well as under-nourishment and fatigue are predisposing factors to FCI. A previous cold injury increases the risk of subsequent FCI, due to an abnormal post-traumatic sympathetic response.
Cold metal can rapidly cause a frostbite when grasped with the bare hand. Most people are aware of this, but often don’t realize the risk of handling super-cooled liquids. Petrol cooled down to –30ºC will freeze exposed flesh almost instantly as evaporative heat loss is combined with conductive loss. Such rapid freezing causes extra- as well as intracellular crystallization with destruction of cell membranes primarily on a mechanical basis. A similar type of FCI occurs when liquid propane is spilled directly onto the skin.
Clinical picture
Freezing cold injuries are subdivided into superficial and deep frostbites. The superficial injury is limited to the skin and the immediate underlying subcutaneous tissues. In most cases the injury is localized to nose, earlobes, fingers and toes. Stinging, pricking pain is often the first sign. The affected part of the skin turns pale or wax-white. It is numb, and will indent upon pressure, as the underlying tissues are viable and pliable. When the FCI extends into a deep injury, the skin becomes white and marble-like, feels hard, and adheres when touched.
Treatment
A frostbite should be taken care of immediately in order to prevent a superficial injury from turning into a deep one. Try to take the victim indoors; otherwise protect him or her from the wind by shelter of comrades, a wind sack or other similar means. The frost-bitten area should be thawed by passive transmission of heat from a warmer part of the body. Put the warm hand against the face and the cold hand into the armpit or into the groin. As the frostbitten individual is under cold stress with peripheral vaso-constriction, a warm companion is a much better therapist. Massage and rubbing the frostbitten part with snow or woollen muffler is contraindicated. Such mechanical treatment would only aggravate the injury, as the tissue is filled with ice crystals. Nor should thawing in front of a campfire or a camp stove be considered. Such heat does not penetrate to any depth, and as the area is partly anaesthetized the treatment may even result in a burn injury.
The signals of pain in a frostbitten foot disappear before actual freezing takes place, as nerve conductivity is abolished at around +8ºC. The paradox is that the last sensation one feels is that one does not feel anything at all! Under extreme conditions when evacuation requires travel on foot, thawing should be avoided. Walking on frostbitten feet does not seem to increase the risk of tissue loss, whereas refreezing of a frostbite does so in the highest degree.
The best treatment for a frostbite is thawing in warm water at 40 to 42ºC. The thawing procedure should continue at that water temperature until sensation, colour and tissue softness return. This form of thawing often ends up in not a pink, but rather a burgundy hue due to venous stasis.
Under field conditions one must be aware that treatment requires more than local thawing. The whole individual has to be taken care of, as a frostbite is often the first sign of a creeping hypothermia. Put on more clothes and give warm, nourishing beverages. The victim is most often apathetic and has to be forced to cooperate. Urge the victim to do muscular activity such as buffeting arms against sides. Such manoeuvres open peripheral arteriovenous shunts in the extremities.
A deep frostbite is present when thawing with passive warmth transfer for 20 to 30 minutes is without success. If so, the victim should be sent to the nearest hospital. However, if such transportation can take hours, it is preferable to get the person into the nearest housing and thaw his or her injuries in warm water. After complete thawing, the patient should be put to bed with the injured area elevated, and prompt transportation to the nearest hospital should be arranged.
Rapid rewarming gives moderate to severe pain, and the patient will often need an analgesic. The capillary damage causes leakage of serum with local swelling and blister formation during the first 6 to 18 hours. Blisters should be kept intact in order to prevent infection.
Non-freezing cold injuries
Pathophysiology
Prolonged exposure to cold and wet conditions above the freezing point combined with immobilization causing venous stagnation are the prerequisites for NFCI. Dehydration, inadequate food, stress, inter-current illness or injury, and fatigue are contributory factors. NFCI almost exclusively affects legs and feet. Severe injuries of this type occur with great rarity in civilian life, but in wartime and catastrophes it has been and will always be a serious problem, most often caused by an unawareness of the condition due to the slow and indistinct first appearance of symptoms.
NFCI can occur under any conditions where the environmental temperature is lower than body temperature. As in FCI, sympathetic constrictor fibres, together with the cold itself, induce prolonged vasoconstriction. The initial event is rheological in nature and resembles that observed in ischaemic reperfusion injury. In addition to the duration of the low temperature, the susceptibility of the victim seems to be of importance.
The pathological change due to the ischaemic injury affects many tissues. Muscles degenerate, undergoing necrosis, fibrosis and atrophy; bones show early osteoporosis. Of special interest are the effects on the nerves, as nerve damage accounts for the pain, prolonged dysaesthesia and hyperhidrosis often found as a sequel in these injuries.
Clinical picture
In a non-freezing cold injury the victim realizes too late the threatening danger because the initial symptoms are so vague. The feet become cold and swollen. They feel heavy, woody and numb. The feet are presented as cool, painful, tender, often with wrinkled soles. The first ischaemic phase last for hours up to a few days. It is followed by a hyperaemic phase of 2 to 6 weeks, during which the feet are warm, with bounding pulses and increased oedema. Blistering and ulcerations are not uncommon, and in severe cases gangrene can arise.
Treatment
The treatment is above all supportive. On the worksite, the feet should be dried carefully but kept cool. On the other hand, the whole body should be warmed. Plenty of warm beverages should be given. Contrary to the freezing cold injuries, NFCI should never be actively warmed. Warm water treatment in local cold injuries is only allowed when ice-crystals are present in the tissue. The further treatment should as a rule be conservative. However, fever, signs of disseminated intravascular coagulation, and liquefaction of affected tissues requires surgical intervention, occasionally ending in an amputation.
Non-freezing cold injuries can be prevented. Exposure time should be minimized. Adequate foot care with time to dry the feet is of importance, as well as facilities to change into dry socks. Rest with feet elevated as well as administering hot beverages whenever possible may seem ridiculous but often is of crucial importance.
Hypothermia
Hypothermia means subnormal body temperature. However, from a thermal point of view the body consists of two zones—the shell and the core. The former is superficial and its temperature varies considerably according to the external environment. The core consists of deeper tissues (e.g., brain, heart and lungs, and upper abdomen), and the body strives to maintain a core temperature of 37 ± 2ºC. When thermoregulation is impaired and core temperature starts to decline, the individual suffers cold stress, but not until the central temperature reaches 35ºC is the victim considered to be in a hypothermic state. Between 35 and 32ºC, the hypothermia is classified as mild; between 32 and 28ºC it is moderate and below 28ºC, severe (Table 16).
Physiological effects of lowered core temperature
When core temperature starts to decline, an intense vasoconstriction redirects blood from the shell to the core, thereby preventing heat conduction from the core to the skin. In order to maintain temperature, shivering is induced, often preceded by increased muscular tone. Maximal shivering can increase the metabolic rate four- to sixfold, but as the involuntary contractions oscillate, the net result is often not more than doubled. Heart rate, blood pressure, cardiac output and respiratory rate increase. The centralization of blood volume causes an osmolal diuresis with sodium and chloride as the main constituents.
Atrial irritability in early hypothermia often induces atrial fibrillation. At lower temperatures, ventricular extra systoles are common. Death occurs at or below 28ºC, most often resulting from ventricular fibrillation; asystole may also supervene.
Hypothermia depresses the central nervous system. Lassitude and apathy are early signs of decreasing core temperature. Such effects impair judgement, cause bizarre behaviour and ataxia, and end in lethargy and coma between 30 and 28ºC.
Nerve conduction velocity decreases with lowered temperature. Dysarthria, fumbling and stumbling are clinical manifestations of this phenomena. Cold also affects muscles and joints, impairing manual performance. It slows reaction time and coordination, and increases frequency of mistakes. Muscle rigidity is observed in even mild hypothermia. At a core temperature lower than 30ºC, physical activity is impossible.
Exposure to an abnormally cold environment is the basic prerequisite for hypothermia to occur. Extremes of age are risk factors. Elderly persons with impaired thermoregulatory function, or persons whose muscle mass and insulating fat layer are reduced, run a greater risk of suffering hypothermia.
Classification
From a practical point of view the following subdivision of hypo-thermia is useful (see also Table 16):
- accidental hypothermia
- acute immersion hypothermia
- sub-acute exhaustion hypothermia
- hypothermia in trauma
- sub-clinical chronic hypothermia.
Acute immersion hypothermia occurs when a person falls into cold water. Water has a thermal conductivity approximately 25 times that of air. The cold stress becomes so great that the core temperature is forced down despite a maximal heat production of the body. Hypothermia sets in before the victim becomes exhausted.
Sub-acute exhaustion hypothermia may happen to any worker in a cold environment as well as to skiers, climbers and walkers in the mountains. In this form of hypothermia, muscular activity maintains the body temperature as long as energy sources are available. However, then hypoglycaemia ensures the victim is at risk. Even a relatively mild degree of cold exposure may be sufficient to continue cooling and cause a hazardous situation.
Hypothermia with major trauma is an ominous sign. The injured person is often unable to maintain body temperature, and heat loss may be exacerbated by infusion of cold fluids and by removal of clothing. Patients in shock who become hypothermic have a much higher mortality than normothermic victims.
Sub-clinical chronic hypothermia is often encountered in elderly persons, often in association with malnutrition, inadequate clothing and restricted mobility. Alcoholism, drug abuse and chronic metabolic diseases as well as psychiatric disorders are contributory causes in this type of hypothermia.
Pre-hospital management
The main principle of primary care of a worker suffering from hypothermia is to prevent further heat loss. A conscious victim should be moved indoors, or at least into a shelter. Remove wet clothing and try to insulate the person as much as possible. Keeping the victim in a lying position with the head covered is mandatory.
Patients with acute immersion hypothermia require quite different treatment from that required by those with sub-acute exhaustion hypothermia. The immersion victim is often in a more favourable situation. The decreased core temperature occurs long before the body becomes exhausted, and heat-generating capacity remains unimpaired. Water and electrolyte balance is not deranged. Therefore such an individual may be treated with rapid immersion in a bath. If a tub is not available, put the patient’s feet and hands into warm water. The local heat opens the arterio- venous shunts, rapidly increases the blood circulation in the extremities and enhances the warming process.
In exhaustion hypothermia, on the other hand, the victim is in a much more serious situation. The caloric reserves are consumed, the electrolyte balance is deranged and, above all, the person is dehydrated. The cold diuresis starts immediately after cold exposure; the fight against the cold and wind exaggerates sweating, but this is not perceived in the cold and dry environment; and lastly, the victim does not feel thirsty. A patient suffering from exhaustion hypothermia should never be rapidly rewarmed out in the field due to the risk of inducing hypovolemic shock. As a rule it is better not to actively rewarm the patient out in the field or during transportation to hospital. A prolonged state of not progressing hypothermia is far better than enthusiastic efforts to warm the patient under circumstances where supervening complications cannot be managed. It is mandatory to handle the patient gently to minimize the risk of possible ventricular fibrillation.
Even for trained medical personnel it is often difficult to determine whether a hypothermic individual is alive or not. Apparent cardiovascular collapse may actually be only depressed cardiac output. Palpation or auscultation for at least a minute to detect spontaneous pulses is often necessary.
The decision as to whether or not to administer cardiopulmonary resuscitation (CPR) is difficult out in the field. If there is any sign of life at all, CPR is contra-indicated. Prematurely performed chest compressions may induce ventricular fibrillation. CPR should, however, immediately be initiated following a witnessed cardiac arrest and when the situation allows the procedures to be performed reasonably and continuously.
Health and cold
A healthy person with appropriate clothing and equipment and working in an organization suitable for the task is not in a health risk situation, even if it is very cold. Whether or not long-term cold exposure while living in cold climate areas means health risks is controversial. For individuals with health problems the situation is quite different, and cold exposure could be a problem. In a certain situation cold exposure or exposure to cold-related factors or combinations of cold with other risks can produce health risks, especially in an emergency or accident situation. In remote areas, when communication with a supervisor is difficult or does not exist, the employees themselves must be allowed to decide whether a health risk situation is at hand or not. In these situations they must take necessary precautions to make the situation safe or stop work.
In arctic regions, climate and other factors can be so harsh that other considerations must be taken.
Infectious diseases. Infectious diseases are not related to cold. Endemic diseases occur in arctic and subarctic regions. Acute or chronic infectious disease in an individual dictates cessation of exposure to cold and hard work.
The common cold, without fever or general symptoms, does not make work in the cold harmful. However, for individuals with complicating diseases like asthma, bronchitis or cardiovascular problems, the situation is different and indoor work in warm conditions during the cold season is recommended. This is also valid with a cold with fever, deep cough, muscle pain and impaired general condition.
Asthma and bronchitis are more common in cold regions. Exposure to cold air often worsens the symptoms. Change of medication sometimes reduces the symptoms during the cold season. Some individuals can also be helped by using medicinal inhalers.
People with asthmatic or cardiovascular diseases may respond to cold air inhalation with bronchoconstriction and vasospasm. Athletes training several hours at high intensities in cold climates have been shown to develop asthmatic symptoms. Whether or not extensive cooling of the pulmonary tract is the primary explanation is not yet clear. Special, light masks are now on the market that do provide some kind of heat exchanger function, thereby conserving energy and moisture.
An endemic type of chronic disease is “Eskimo lung”, typical for Eskimo hunters and trappers exposed to extreme cold and hard work for long periods. A progressive pulmonary hyper- tension often ends in a right-sided heart failure.
Cardiovascular disorders. Exposure to cold affects the cardio- vascular system to a higher degree. The noradrenalin released from the sympathetic nerve terminals raises the cardiac output and heart rate. Chest pain due to angina pectoris often worsens in a cold environment. The risk of getting an infarct increases during cold exposure, especially in combination with hard work. Cold raises blood pressure with an increased risk of cerebral haemorrhage. Individuals at risk should therefore be warned and reduce their exposure to hard work in the cold.
Increased mortality during winter season is a frequent observation. One reason could be the previously mentioned increase in heart work, promoting arrhythmia in sensitive persons. Another observation is that the haematocrit is increased during the cold season, causing increased viscosity of blood and increased resistance to flow. A plausible explanation is that cold weather may expose people to sudden, very heavy work loads, such as snow cleaning, walking in deep snow, slipping and so on.
Metabolic disorders. Diabetes mellitus is also found with a higher frequency in the colder areas of the world. Even an uncomplicated diabetes, especially when treated with insulin, can make cold outdoor work impossible in more remote areas. Early peripheral arteriosclerosis makes these individuals more sensitive to cold and increases the risk of local frostbite.
Individuals with impaired thyroid function can easily develop hypothermia due to lack of the thermogenic hormone, while hyperthyroid persons tolerate cold even when lightly dressed.
Patients with these diagnoses should be given extra attention from health professionals and be informed of their problem.
Musculoskeletal problems. Cold itself is not supposed to cause diseases in the musculoskeletal system, not even rheumatism. On the other hand, work in cold conditions is often very demanding for muscles, tendons, joints and spine because of the high load often involved in these kinds of work. The temperature in the joints decreases faster than the temperature of the muscles. Cold joints are stiff joints, because of increasing resistance to movement due to augmented viscosity of the synovial fluid. Cold decreases the power and duration of muscle contraction. In combination with heavy work or local overload, the risk of injury increases. Furthermore, protective clothing may impair the ability to control movement of body parts, hence contributing to the risk.
Arthritis in the hand is a special problem. It is suspected that frequent cold exposure may cause arthritis, but so far the scientific evidence is poor. An existing arthritis of the hand reduces hand function in the cold and causes pain and discomfort.
Cryopathies. Cryopathies are disorders where the individual is hypersensitive to cold. The symptoms vary, including those involving the vascular system, blood, connective tissue, “allergy” and others.
Some individuals suffer from white fingers. White spots on the skin, a sensation of cold, reduced function and pain are symptoms when fingers are exposed to cold. The problems are more common among women, but above all are found in smokers and workers using vibrating tools or driving snowmobiles. Symptoms can be so troublesome that work during even slight cold exposure is impossible. Certain types of medication can also worsen the symptoms.
Cold urticaria, due to sensitized mast cells, appears as an itching erythema of cold-exposed parts of the skin. If exposure is stopped, the symptoms usually disappear within one hour. Rarely the disease is complicated with general and more threatening symptoms. If so, or if the urticaria itself is very troublesome, the individual should avoid exposure to any kind of cold.
Acrocyanosis is manifested by changes in skin colour towards cyanosis after exposure to cold. Other symptoms could be dysfunction of hand and fingers in the acrocyanotic area. The symptoms are very common, and can often be acceptably reduced by reduced cold exposure (e.g., proper clothing) or reduced nicotine use.
Psychological stress. Cold exposure, especially in combination with cold-related factors and remoteness, stresses the individual, not only physiologically but also psychologically. During work in cold climate conditions, in bad weather, over long distances and perhaps in potentially dangerous situations, the psychological stress can disturb or even deteriorate the individual’s psychological function so much that work cannot be safely done.
Smoking and snuffing. The unhealthy long-term effects of smoking and, to some extent, snuffing are well known. Nicotine increases peripheral vasoconstriction, reduces dexterity and raises the risk of cold injury.
Alcohol. Drinking alcohol gives a pleasant feeling of warmth, and it is generally thought that the alcohol inhibits cold-induced vasoconstriction. However, experimental studies on humans during relatively short exposures to cold have shown that alcohol does not interfere with heat balance to any greater extent. However, shivering becomes impaired and, combined with strenuous exercise, the heat loss will become obvious. Alcohol is known to be a dominant cause of death in urban hypothermia. It gives a feeling of bravado and influences judgement, leading to ignoring prophylactic measures.
Pregnancy. During pregnancy women are not more sensitive to cold. To the contrary, they can be less sensitive, due to raised metabolism. Risk factors during pregnancy are combined with the cold-related factors such as accident risks, clumsiness due to clothing, heavy lifting, slipping and extreme working positions. The health care system, the society and the employer should therefore pay extra attention to the pregnant woman in cold work.
Pharmacology and cold
Negative side effects of drugs during cold exposure could be thermoregulatory (general or local), or the effect of the drug can be altered. As long as the worker retains normal body temperature, most prescribed drugs don’t interfere with performance. However, tranquilizers (e.g., barbiturates, benzodiazepines, phentothiazides as well as cyclic antidepressants) may disturb vigilance. In a threatening situation the defence mechanisms against hypothermia may be impaired and the awareness of the hazardous situation is reduced.
Beta-blockers induce peripheral vasoconstriction and decrease the tolerance to cold. If an individual needs medication and has cold exposure in his or her working situation, attention should be paid to negative side effects of these drugs.
On the other hand, no drug or anything else drunk, eaten or otherwise administered to the body has been shown to be able to raise normal heat production, for example in an emergency situation when hypothermia or a cold injury threatens.
Health control programme
Health risks connected to cold stress, cold-related factors and accidents or trauma are known only to a limited extent. There is a large individual variation in capacities and health status, and this requires careful consideration. As previously mentioned, special diseases, medication and some other factors may render a person more susceptible to the effects of cold exposure. A health control programme should be part of the employment procedure, as well as a repeated activity for the staff. Table 6 specifies factors to control for in different types of cold work.
Table 6. Recommended components of health control programs for personnel exposed to cold stress and cold-related factors
|
Factor |
Outdoor work |
Cold store work |
Arctic and subarctic work |
|
Infectious diseases |
** |
** |
*** |
|
Cardio-vascular diseases |
*** |
** |
*** |
|
Metabolic diseases |
** |
* |
*** |
|
Musculoskeletal problems |
*** |
* |
*** |
|
Cryopathies |
** |
** |
** |
|
Psychological stress |
*** |
** |
*** |
|
Smoking and snuffing |
** |
** |
** |
|
Alcohol |
*** |
** |
*** |
|
Pregnancy |
** |
** |
*** |
|
Medication |
** |
* |
*** |
*= routine control, **= important factor to consider, ***= very important factor to consider.
Prevention of Cold Stress
Human adaptation
With repeated exposures to cold conditions, people perceive less discomfort and learn to adjust to and cope with conditions in an individual and more efficient way, than at the onset of exposure. This habituation reduces some of the arousal and distraction effect, and improves judgement and precaution.
Behaviour
The most apparent and natural strategy for prevention and control of cold stress is that of precaution and intentional behaviour. Physiological responses are not very powerful in preventing heat losses. Humans are, therefore, extremely dependent on external measures such as clothing, shelter and external heat supply. The continuous improvement and refinement of clothing and equipment provides one basis for successful and safe exposures to cold. However, it is essential that products be adequately tested in accordance with international standards.
Measures for prevention and control of cold exposure are often the responsibility of the employer or the supervisor. However, the efficiency of protective measures relies to a significant degree upon knowledge, experience, motivation and ability of the individual worker to make the necessary adjustments to his or her requirements, needs and preferences. Hence, education, information and training are important elements in health control programmes.
Acclimatization
There is evidence for different types of acclimatization to long-term cold exposure. Improved hand and finger circulation allows for the maintenance of a higher tissue temperature and produces a stronger cold-induced vasodilatation (see Figure 18). Manual performance is better maintained after repeated cold exposures of the hand.
Repeated whole-body cooling appears to enhance peripheral vasoconstriction, thereby increasing surface tissue insulation. Korean pearl-diving women showed marked increases in skin insulation during the winter season. Recent investigations have revealed that the introduction and use of wet suits reduces the cold stress so much that tissue insulation does not change.
Three types of possible adaptations have been proposed:
- increased tissue insulation (as previously mentioned)
- hypothermic reaction (“controlled” drop in core temperature)
- metabolic reaction (increased metabolism).
The most pronounced adaptations should be found with native people in cold regions. However, modern technology and living habits have reduced most extreme types of cold exposure. Clothing, heated shelters and conscious behaviour allow most people to maintain an almost tropical climate at the skin surface (micro- climate), thereby reducing cold stress. The stimuli to physiological adaptation become weaker.
Probably the most cold-exposed groups today belong to polar expeditions and industrial operations in arctic and subarctic regions. There are several indications that any eventual adaptation found with severe cold exposure (air or cold water) is of the insulative type. In other words, higher core temperatures can be kept with a reduced or unchanged heat loss.
Diet and water balance
In many cases cold work is associated with energy-demanding activities. In addition, protection against cold requires clothing and equipment weighing several kilograms. The hobbling effect of clothing increases muscular effort. Hence, given work tasks require more energy (and more time) under cold conditions. The caloric intake through food must compensate for this. An increase of the percentage of calories provided by fat should be recommended to outdoor workers.
Meals provided during cold operations must provide sufficient energy. Enough carbohydrates must be included to ensure stable and safe blood sugar levels for workers engaged in hard work. Recently, food products have been launched on the market with claims that they stimulate and increase body heat production in the cold. Normally, such products consist merely of carbohydrates, and they have so far failed in tests to perform better than similar products (chocolate), or better than expected from their energy content.
Water loss may be significant during cold exposure. First, tissue cooling causes a redistribution of blood volume, inducing “cold diuresis”. Tasks and clothing must allow for this, since it may develop rapidly and requires urgent execution. The almost dry air at subzero conditions allows a continuous evaporation from skin and respiratory tract that is not readily perceived. Sweating contributes to water loss, and should be carefully controlled and preferably avoided, due to its detrimental effect on insulation when absorbed by clothing. Water is not always readily available at subzero conditions. Outdoors it must be supplied or produced by melting snow or ice. As there is a depression of thirst it is mandatory that workers in the cold drink water frequently to eliminate the gradual development of dehydration. Water deficit may lead to reduced working capacity and increased risk of getting cold injuries.
Conditioning workers for work in the cold
By far the most effective and appropriate measures for adapting humans to cold work, are by conditioning—education, training and practice. As previously mentioned, much of the success of adjustments to cold exposure depends on behavioural action. Experience and knowledge are important elements of this behavioural process.
Persons engaged in cold work should be given a basic introduction to the specific problems of cold. They must receive information about physiological and subjective reactions, health aspects, risk of accidents, and protective measures, including clothing and first aid. They should be gradually trained for the required tasks. Only after a given time (days to weeks) should they work full hours under the extreme conditions. Table 7 provides recommendations as to the contents of conditioning programmes for various types of cold work.
Table 7. Components of conditioning programs for workers exposed to cold
|
Element |
Outdoor work |
Cold store work |
Arctic and subarctic work |
|
Health control |
*** |
** |
*** |
|
Basic introduction |
*** |
** |
*** |
|
Accident prevention |
*** |
** |
*** |
|
Basic first aid |
*** |
*** |
*** |
|
Extended first aid |
** |
* |
*** |
|
Protective measures |
*** |
** |
*** |
|
Survival training |
see text |
* |
*** |
*= routine level, **= important factor to consider, ***= very important factor to consider.
Basic introduction means education and information about the specific cold problems. Registration and analysis of accidents/injuries is the best base for preventive measures. Training in first aid should be given as a basic course for all personnel, and specific groups should get an extended course. Protective measures are natural components of a conditioning programme and are dealt with in the following section. Survival training is important for arctic and subarctic areas, and also for outdoor work in other remote areas.
Technical control
General principles
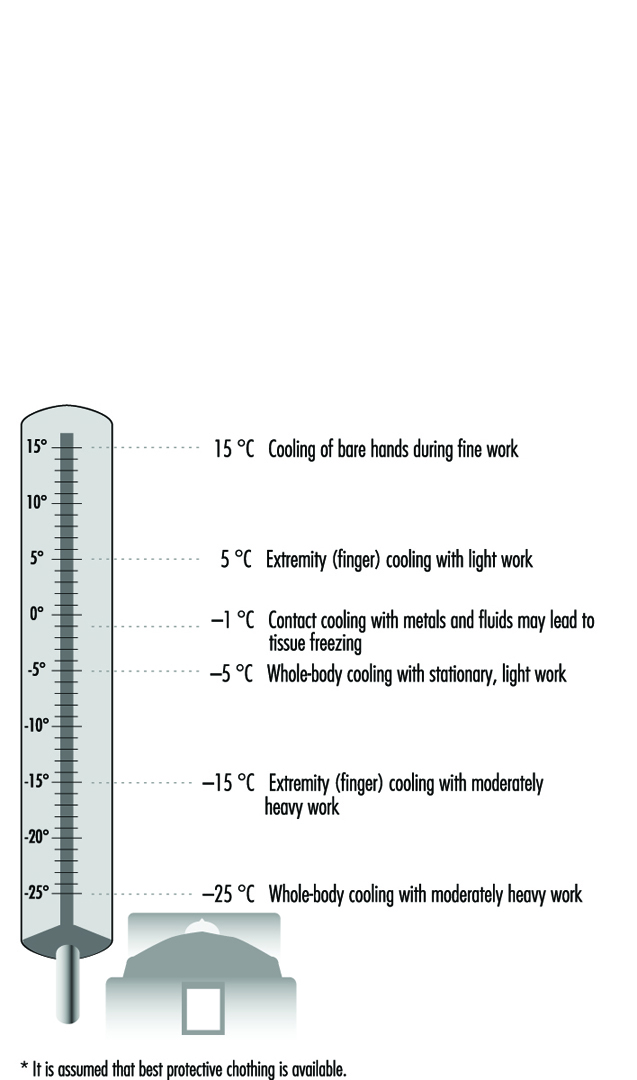
Due to the many complex factors that influence human heat balance, and the considerable individual variations, it is difficult to define critical temperatures for sustained work. The temperatures given in Figure 6 must be regarded as action levels for improvement of conditions by various measures. At temperatures below those given in figure 6, exposures should be controlled and evaluated. Techniques for assessment of cold stress and recommendations for time-limited exposures are dealt with elsewhere in this chapter. It is assumed that best protection of hands, feet and body (clothing) is available. With inappropriate protection, cooling will be expected at considerably higher temperatures.
Figure 6. Estimated temperatures at which certain thermal imbalances of the body may develop.*
Tables 8 and 9 list different preventive and protective measures that can be applied to most types of cold work. Much effort is saved with careful planning and foresight. Examples given are recommendations. It must be emphasized that the final adjustment of clothing, equipment and work behaviour must be left to the individual. Only with a cautious and intelligent integration of behaviour with the requirements of the real environmental conditions can a safe and efficient exposure be created.
Table 8. Strategies and measures during various phases of work for prevention and alleviation of cold stress
|
Phase/factor |
What to do |
|
Planning phase |
Schedule work for a warmer season (for outdoor work). Check if work can be done indoors (for outdoor work). Allow more time per task with cold work and protective clothing. Analyse suitability of tools and equipment for work. Organize work in suitable work-rest regimens, considering task, load and protection level. Provide heated space or heated shelter for recovery. Provide training for complex work tasks under normal conditions. Check medical records of staff. Ascertain appropriate knowledge and competence of staff. Provide information about risks, problems, symptoms and preventive actions. Separate goods and worker line and keep different temperature zones. Care for low velocity, low humidity and low noise level of the air- Provide extra personnel to shorten exposure. Select adequate protective clothing and other protective equipment. |
|
Before work shift |
Check climatic conditions at onset of work. Schedule adequate work-rest regimens. Allow for individual control of work intensity and clothing. Select adequate clothing and other personal equipment. Check weather and forecast (outdoors). Prepare schedule and control stations (outdoors). Organize communication system (outdoors). |
|
During work shift |
Provide for break and rest periods in heated shelter. Provide for frequent breaks for hot drinks and food. Care for flexibility in terms of intensity and duration of work. Provide for replacement of clothing items (socks, gloves, etc.). Protect from heat loss to cold surfaces. Minimize air velocity in work zones. Keep workplace clear from water, ice and snow. Insulate ground for stationary standing work places. Provide access to extra clothing for warmth. Monitor subjective reactions (buddy system) (outdoors). Report regularly to foreman or base (outdoors). Provide for sufficient recovery time after severe exposures (outdoors). Protect against wind effects and precipitation (outdoors). Monitor climatic conditions and anticipate weather change (outdoors). |
Source: Modified from Holmér 1994.
Table 9. Strategies and measures related to specific factors and equipment
|
Behaviour |
Allow for time to adjust clothing. Prevent sweating and chilling effects by making adjustments of clothing in due time before change in work rate and/or exposure. Adjust work rate (keep sweating minimal). Avoid rapid shifts in work intensity. Allow for adequate intake of hot fluid and hot meals. Allow for time to return to protected areas (shelter, warm room) (outdoors). Prevent wetting of clothing from water or snow. Allow for sufficient recovery in protected area (outdoors). Report on progress of work to foreman or base (outdoors). Report major deviations from plan and schedule (outdoors). |
|
Clothing |
Select clothing you have previous experience with. With new clothing, select tested garments. Select insulation level on the basis of anticipated climate and activity. Care for flexibility in clothing system to allow for great adjustment of insulation. Clothing must be easy to put on and take off. Reduce internal friction between layers by proper selection of fabrics. Select size of outer layers to make room for inner layers. Use multi-layer system: —inner layer for micro climate control —middle layer for insulation control —outer layer for environmental protection. Inner layer should be non-absorbent to water, if sweating cannot be sufficiently controlled. Inner layer may be absorbent, if sweating is anticipated to be none or low. Inner layer may consist of dual-function fabrics, in the sense that fibre in contact with skin is non absorbing and fibres next to the middle layer is absorbing water or moisture. Middle layer should provide loft to allow stagnant air layers. Middle layer should be form-stable and resilient. Middle layer may be protected by vapour barrier layers. Garments should provide sufficient overlap in the waist and back region. Outer layer must be selected according to additional protection requirements, such as wind, water, oil, fire, tear or abrasion. Design of outer garment must allow easy and extensive control of openings at neck, sleeves, wrists etc., to regulate ventilation of interior space. Zippers and other fasteners must function also with snow and windy conditions. Buttons should be avoided. Clothing shall allow operation even with cold, clumsy fingers. Design must allow for bent postures without compression of layers and loss of insulation. Avoid unnecessary constrictions. Carry extra wind proof blankets (NOTE! The aluminized “astronaut blanket” does not protect more than expected from being wind proof. A large polyethylene garbage bag has the same effect). |
|
Education Training |
Provide education and information on the special problems of cold. Provide information and training in first-aid and treatment of cold injuries. Test machinery, tools and equipment in controlled cold conditions. Select tested goods, if available. Train complex operations under controlled cold conditions. Inform about accidents and accident prevention. |
|
Handwear |
Mittens provide the best overall insulation. Mittens should allow fine gloves to be worn underneath. Prolonged exposures requiring fine hand work, must be intercepted by frequent warm-up breaks. Pocket heaters or other external heat sources may prevent or delay hand cooling. Sleeve of clothing must easily accommodate parts of gloves or mittens —underneath or on top. Outer garment must provide easy storage or fixing of handwear when taken off. |
|
Footwear |
Boots shall provide high insulation to the ground (sole). Sole shall be made of a flexible material and have an anti-slippery pattern. Select size of boot so it can accommodate several layers of socks and an insole. Ventilation of most footwear is poor, so moisture should be controlled by frequent replacement of socks and insole. Control moisture by vapour barrier between inner and outer layer. Allow boots to dry completely between shifts. Legs of clothing must easily accommodate parts of boots —underneath or on top. |
|
Headgear |
Flexible headgear comprises an important instrument for control of heat and whole-body heat losses. Headgear should be windproof. Design should allow sufficient protection of ears and neck. Design must accommodate other types of protective equipment (e.g., ear muffs, safety goggles). |
|
Face |
Face mask should be windproof and insulative. No metallic details should contact skin. Significant heating and humidification of inspired air can be achieved by special breathing masks or mouth pieces. Use safety goggles outdoors, especially in sleet and snow. Use eye protection against ultra-violet radiation and glare. |
|
Equipment Tools |
Select tools and equipment intended and tested for cold conditions. Choose design that allows operation by gloved hands. Prewarm tools and equipment. Store tools and equipment in heated space. Insulate handles of tools and equipment. |
|
Machinery |
Select machinery intended for operation in cold environments. Store machinery in protected space. Prewarm machinery before use. Insulate handles and controls. Design handles and controls for operation by gloved hands. Prepare for easy repair and maintenance under adverse conditions. |
|
Workplace |
Keep air velocity as low as possible. Use wind-breaking shields or windproof clothing. Provide insulation to ground with prolonged standing, kneeling or lying work. Provide auxiliary heating with light, stationary work. |
Source: Modified from Holmér 1994.
Some recommendations as to the climatic conditions under which certain measures should be taken have been given by the American Conference of Governmental Industrial Hygienists (ACGIH 1992). The fundamental requirements are that:
- workers be provided with sufficient and appropriate protective clothing
- special precautions should be taken for older workers or workers with circulatory problems.
Further recommendations related to the provision of hand protection, to workplace design and to work practices are presented below.
Hand protection
Fine barehanded operations below 16ºC require provision for heating the hands. Metal handles of tools and bars should be covered by insulating materials at temperatures below –1ºC. Anticontact gloves should be worn when surfaces at –7ºC or lower are within reach. At –17ºC insulative mittens must be used. Evaporative liquids at temperatures below 4 °C should be handled so as to avoid splashes to bare or poorly protected skin areas.
Work practices
Below –12ºC Equivalent Chill Temperature, workers should be under constant supervision (buddy system). Many of the measures given in Table 18 apply. With lowered temperatures it is increasingly important that workers are instructed in safety and health procedures.
Workplace design
Workplaces must be shielded from wind, and air velocities kept below 1 m/s. Wind-protective clothing should be used when appropriate. Eye protection must be supplied for special outdoor conditions with sunshine and snow-covered ground. Medical screening is recommended for persons working routinely in cold below –18ºC. Recommendations as to workplace monitoring include the following:
- Suitable thermometry should be arranged when the temperature is below 16ºC.
- Indoor wind speeds should be monitored at least every 4 hours.
- Outdoor work requires measurement of wind speed and air temperatures below –1ºC.
- The Equivalent Chill Temperature should be determined for combinations of wind and air temperature.
Most of the recommendations in Tables 8 and 9 are pragmatic and straightforward.
Clothing is the most important measure for individual control. The multi-layer approach allows for more flexible solutions than single garments incorporating the function of several layers. In the end, however, the specific needs of the worker should be the ultimate determinant of what would be the most functional system. Clothing protects against cooling. On the other hand overdressing in the cold is a common problem, also reported from the extreme exposures of arctic expeditions. Overdressing may rapidly result in large amounts of sweat, which accumulates in clothing layers. During periods of low activity, the drying of moist clothing increases body heat loss. The obvious preventive measure is to control and reduce sweating by appropriate selection of clothing and early adjustments to changes in work rate and climate conditions. There is no clothing fabric that can absorb large amounts of sweat and also preserve good comfort and insulative properties. Wool remains lofty and apparently dry despite absorption of some water (moisture regain), but large amounts of sweat will condense and cause problems similar to those of other fabrics. The moisture yields some heat liberation and may contribute to the preservation of warmth. However, when the wool garment dries on the body, the process reverses as discussed above, and the person is inevitably cooled.
Modern fibre technology has produced many new materials and fabrics for clothing manufacturing. Garments are now available that combine waterproofness with good water vapour permeability, or high insulation with reduced weight and thickness. It is essential, however, to select garments with guaranteed tested properties and functions. Many products are available that try to mimic the more expensive original products. Some of them represent such poor quality that they may even be hazardous to use.
Protection against cold is determined primarily by the thermal insulation value of the complete clothing ensemble (clo value). However, properties such as air permeability, vapour permeability and waterproofness of the outer layer in particular are essential for cold protection. International standards and test methods are available for measuring and classifying these properties. Similarly, handgear and footwear may be tested for their cold-protective properties using international standards such as European standards EN 511 and EN 344 (CEN 1992, 1993).
Outdoor cold work
Specific problems of outdoor cold work are the aggregate of climatic factors that may result in cold stress. The combination of wind and low air temperature significantly increases the cooling power of the environment, which has to be considered in terms of work organization, workplace shielding and clothing. Precipitation, either in the air as snow or rain, or on the ground, requires adjustments. The variation in weather conditions requires workers to plan for, bring and use additional clothing and equipment.
Much of the problem in outdoor work relates to the sometimes great variations in activity and climate during a work shift. No clothing system is available that can accommodate such large variations. Consequently, clothing must be frequently changed and adjusted. Failure to do so may result in cooling due to insufficient protection, or sweating and overheating caused by too much clothing. In the latter case, most of the sweat condenses or is absorbed by clothing. During periods of rest and low activity, wet clothing represents a potential hazard, since its drying drains the body of heat.
Protective measures for outdoor work include appropriate work-rest regimens with rest pauses taken in heated shelters or cabins. Stationary work tasks can be protected from wind and precipitation by tents with or without additional heating. Spot heating by infrared or gas heaters may be used for certain work tasks. Prefabrication of parts or components may be carried out indoors. Under subzero conditions, workplace conditions including weather should be regularly monitored. Clear rules must exist regarding what procedures to apply when conditions get worse. Temperature levels, eventually corrected for wind (wind chill index), should be agreed upon and linked to an action programme.
Cold storage work
Frozen food requires storage and transportation at low ambient temperatures (–20ºC). Work in cold stores can be found in most parts of the world. This kind of artificial cold exposure is characterized by a constant, controlled climate. Workers may perform continuous work or, most common, intermittent work, shifting between cold and temperate or warm climates outside the storehouse.
As long as work requires some physical effort, heat balance can be achieved by selecting appropriate protective clothing. The special problems of hand and feet often require regular breaks every 1.5 to 2 hours. The break must be long enough to allow rewarming (20 minutes).
Manual handling of frozen goods requires protective gloves with sufficient insulation (in particular, of the palm of the hand). Requirements and test methods for cold-protective gloves are given in the European standard EN 511, which is described in more detail in the article “Cold indices and standards” in this chapter. Local heaters (e.g., infrared radiator), placed in workplaces with stationary work, improve heat balance.
Much work in cold stores is carried out with fork-lifts. Most of these vehicles are open. Driving creates a relative wind speed, which in combination with the low temperature increases body cooling. In addition, the work itself is rather light and the associated metabolic heat production low. Accordingly, the required clothing insulation is quite high (around 4 clo) and cannot be met with most types of overalls in use. The driver gets cold, starting with feet and hands, and exposure has to be time limited. Depending on available protective clothing, appropriate work schedules should be organized in terms of work in cold and work or rest in normal environments. A simple measure to improve heat balance is to install a heated seat in the truck. This may prolong work time in the cold and prevent local cooling of the seat and back. More sophisticated and expensive solutions include the use of heated cabs.
Special problems arise in hot countries, where the cold store worker, usually the truck driver, is intermittently exposed to cold (–30ºC) and heat (30ºC). Brief exposures (1 to 5 min) to each condition make it difficult to adopt suitable clothing—it may be too warm for the outdoor period and too cold for the cold store work. Truck cabs may be one solution, once the problem of condensation upon windows is solved. Appropriate work-rest regimens must be elaborated and based on work tasks and available protection.
Cool workplaces, found for example in the fresh food industry, comprise climatic conditions with air temperatures of +2 to +16ºC, depending on type. Conditions are sometimes characterized by high relative humidities, inducing condensation of water at cold spots and moist or water-covered floors. The risk of slipping is increased in such workplaces. Problems can be solved by good workplace hygiene and cleaning routines, which contribute to reducing the relative humidity.
The local air velocity of work stations is often too high, resulting in complaints of draught. The problems can often be solved by changing or adjusting the inlets for cold air or by rearranging work stations. Buffers of frozen or cold goods close to work stations may contribute to draught sensation due to the increased radiation heat exchange. Clothing must be selected on the basis of an assessment of the requirements. The IREQ method should be used. In addition clothing should be designed to protect from local draught, moisture and water. Special hygienic requirements for food handling put some restrictions on design and type of clothing (i.e., the outer layer). An appropriate clothing system must integrate underwear, insulating middle layers and the outer layer to form a functional and sufficient protective system. Headgear is often required due to hygienic demands. However, existing headgear for this purpose is often a paper cap, which does not offer any protection against cold. Similarly, footwear often comprises clogs or light shoes, with poor insulation properties. Selection of more suitable headgear and footwear should better preserve warmth of these body parts and contribute to an improved general heat balance.
A special problem in many cool workplaces is the preservation of manual dexterity. Hands and fingers cool rapidly when muscular activity is low or moderate. Gloves improve protection but impair dexterity. A delicate balance between the two demands has to be found. Cutting meat often requires a metal glove. A thin textile glove worn underneath may reduce the cooling effect and improve comfort. Thin gloves may be sufficient for many purposes. Additional measures to prevent hand cooling include the provision of insulated handles of tools and equipment or spot heating using, for example, infrared radiators. Electrically heated gloves are on the market, but often suffer from poor ergonomics and insufficient heating or battery capacity.
Cold-water exposure
During immersion of the body in water the potential for large losses of heat in a short time is great and presents an apparent hazard. The heat conductivity of water is more than 25 times higher than that of air, and in many exposure situations the capacity of surrounding water to absorb heat is effectively infinite.
Thermoneutral water temperature is around 32 to 33ºC, and at lower temperatures the body responds by cold vasoconstriction and shivering. Long exposures in water at temperatures between 25 and 30ºC provoke body cooling and progressive development of hypothermia. Naturally, this response becomes stronger and more serious with the lowering of the water temperature.
Exposure to cold water is common in accidents at sea and in conjunction with water sports of various kinds. However, even in occupational activities, workers run the risk of immersion hypo-thermia (e.g., diving, fishing, shipping and other offshore operations).
Victims of shipwrecks may have to enter cold water. Their protection varies from pieces of thin clothing to immersion suits. Lifejackets are mandatory equipment aboard ships. They should be equipped with a collar to reduce heat loss from the head of unconscious victims. The equipment of the ship, the efficiency of the emergency procedures and the behaviour of crew and passengers are important determinants for the success of the operation and the subsequent exposure conditions.
Divers regularly enter cold waters. The temperature of most waters with commercial diving, in particular at some depth, is low—often lower than 10ºC. Any prolonged exposure in such cold water requires thermally insulated diving suits.
Heat loss. Heat exchange in the water may be seen as simply a flow of heat down two temperature gradients—one internal, from core to skin, and one external, from the skin surface to the surrounding water. Body surface heat loss can be simply described by:
Cw = hc·(Tsk–Tw)·AD
where Cw is the rate of convective heat loss (W), hc is the convective heat transfer coefficient (W/°Cm2), Tsk is the average skin temperature (°C), Tw is the water temperature (°C) and AD is the body surface area. The small components of heat loss from respiration and from non-immersed parts (e.g., head) can be neglected (see the section on diving below).
The value of hc is in the range of 100 to 600 W/°Cm2. The lowest value applies to still water. Turbulence, be it caused by swimming movements or flowing water, doubles or triples the convection coefficient. It is easily understood that the unprotected body may suffer a considerable heat loss to the cold water—eventually exceeding what can be produced even with heavy exercise. In fact, a person (dressed or undressed) who falls into cold water in most cases saves more heat by lying still in the water than by swimming.
Heat loss to the water can be significantly reduced by wearing special protective suits.
Diving. Diving operations several hundreds of metres below sea level must protect the diver from the effects of pressure (one ATA or 0.1 MPa/10 m) and cold. Breathing cold air (or a cold gas mixture of helium and oxygen) drains the lung tissues of body heat. This direct heat loss from the body core is large at high pressures and can easily achieve values higher than the resting metabolic heat production of the body. It is poorly sensed by the human organism. Dangerously low internal temperatures may develop without a shivering response if the body surface is warm. Modern offshore work requires the diver to be supplied with extra heat to the suit as well as to the breathing apparatus, to compensate for large convective heat losses. In deep-sea diving, the comfort zone is narrow and warmer than at sea level: 30 to 32ºC at 20 to 30 ATA (2 to 3 MPa) and increasing to 32 to 34ºC up to 50 ATA (5 MPa).
Physiological factors: Cold immersion elicits a strong, acute respiratory drive. The initial responses include an “inspiratory gasp”, hyperventilation, tachycardia, peripheral vasoconstriction and hypertension. An inspiratory apnoea for several seconds is followed by an increased ventilation. The response is almost impossible to control voluntarily. Hence, a person may easily inhale water if the sea is rough and the body becomes submersed. The first seconds of exposure to very cold water, accordingly, are dangerous, and sudden drowning may occur. Slow immersion and proper protection of the body reduce the reaction and allow for better control of respiration. The reaction gradually fades and normal breathing is usually achieved within a few minutes.
The rapid rate of heat loss at the skin surface emphasizes the importance of internal (physiological or constitutional) mechanisms for reducing the core-to-skin heat flow. Vasoconstriction reduces extremity blood flow and preserves central heat. Exercise increases extremity blood flow, and, in conjunction with the increased external convection, it may in fact accelerate heat loss despite the elevated heat production.
After 5 to 10 min in very cold water, extremity temperature drops quickly. Neuromuscular function deteriorates and the ability to coordinate and control muscular performance degrades. Swimming performance may be severely reduced and quickly put the person at risk in open waters.
Body size is another important factor. A tall person has a larger body surface area and loses more heat than a small person at given ambient conditions. However, the relatively larger body mass compensates for this in two ways. Metabolic heat production rate increases in relation to the larger surface area, and the heat content at a given body temperature is greater. The latter factor comprises a larger buffer to heat losses and a slower rate of core temperature decrease. Children are at a greater risk than adults.
By far the most important factor is body fat content—in parti-cular, subcutaneous fat thickness. Adipose tissue is more insulating than other tissues and is bypassed by much of the peripheral circulation. Once vasoconstriction has occurred, the layer of subcutaneous fat acts as an extra layer. The insulative effect is almost linearly related to the layer thickness. Accordingly, women in general have more cutaneous fat than men and lose less heat under the same conditions. In the same way, fat persons are better off than lean persons.
Personal protection. As previously mentioned, prolonged stay in cold and temperate waters requires additional external insulation in the form of diving suits, immersion suits or similar equipment. The wet suit of foamed neoprene provides insulation by the thickness of the material (closed foam cells) and by the relatively controlled “leakage” of water to the skin microclimate. The latter phenomenon results in the warming of this water and the establishment of a higher skin temperature. Suits are available in various thickness, providing more or less insulation. A wet suit compresses at depth and loses thereby much of its insulation.
The dry suit has become standard at temperatures below 10ºC. It allows the maintenance of a higher skin temperature, depending on the amount of extra insulation worn under the suit. It is a fundamental requirement that the suit not leak, as small amounts of water (0.5 to 1 l) seriously reduce the insulative power. Although the dry suit also compresses at depth, dry air is automatically or manually added from the scuba tank to compensate for the reduced volume. Hence, a microclimate air layer of some thickness can be maintained, providing good insulation.
As previously mentioned, deep-sea diving requires auxiliary heating. Breathing gas is prewarmed and the suit is heated by the flushing of warm water from the surface or the diving bell. More recent warming techniques rely upon electrically heated underwear or closed-circuit tubules filled with warm fluid.
Hands are particularly susceptible to cooling and may require extra protection in the form of insulative or heated gloves.
Safe exposures. The rapid development of hypothermia and the imminent danger of death from cold-water exposure necessitates some sort of prediction of safe and unsafe exposure conditions.
Figure 7 depicts predicted survival times for typical North Sea offshore conditions. The applied criterion is a drop in core temperature to 34ºC for the tenth percentile of the population. This level is assumed to be associated with a conscious and manageable person. The proper wearing, use and functioning of a dry suit doubles the predicted survival time. The lower curve refers to the unprotected person immersed in normal clothing. As clothing gets completely soaked with water the effective insulation is very small, resulting in short survival times (modified from Wissler 1988).
Figure 7. Predicted survival times for typical North Sea offshore scenarios.

Work in arctic and subarctic regions
Arctic and subarctic regions of the world comprise additional problems to those of normal cold work. The cold season coincides with darkness. Days with sunlight are short. These regions cover vast, unpopulated or sparsely populated areas, such as Northern Canada, Siberia and Northern Scandinavia. In addition nature is harsh. Transportation takes place over large distances and takes a long time. The combination of cold, darkness and remoteness require special consideration in terms of work organization, preparation and equipment. In particular, training in survival and first aid must be provided and the appropriate equipment supplied and made easily available at work.
For the working population in the arctic regions there are many health-threatening hazards, as mentioned elsewhere. The risks of accident and injury are high, drug abuse is common, cultural patterns produce problems, as does the confrontation between local/native culture and modern western industrial demands. Snowmobile driving is an example of multiple-risk exposure in typical arctic conditions (see below). Cold stress is thought to be one of the risk factors that produces higher frequencies of certain diseases. Geographical isolation is another factor producing different types of genetic defects in some native areas. Endemic diseases—for example, certain infectious diseases—are also of local or regional importance. Settlers and guest workers also run a higher risk for different kinds of psychological stress reactions secondary to new environment, remoteness, harsh climate conditions, isolation and awareness.
Specific measures for this kind of work must be considered. Work must be carried out in groups of three, so that in case of emergency, one person may go for help while one is left taking care of the victim of, for example, an accident. The seasonal variation in daylight and climate must be considered and work tasks planned accordingly. Workers must be checked for health problems. If required, extra equipment for emergency or survival situations must be available. Vehicles such as cars, trucks or snowmobiles must carry special equipment for repair and emergency situations.
A specific work problem in these regions is the snowmobile. Since the sixties the snowmobile has developed from a primitive, low-technology vehicle to one that is fast and technically highly developed. It is most frequently used for leisure activities, but also for work (10 to 20%). Typical professions using the snowmobile are police, military personnel, reindeer herders, lumberjacks, farmers, tourist industry, trappers and search and rescue teams.
The vibration exposure from a snowmobile means a highly increased risk for vibration-induced injuries to the driver. The driver and the passengers are exposed to unpurified exhaust gas. The noise produced by the engine may induce hearing loss. Due to high speed, terrain irregularities and poor protection for the driver and the passengers, the risk of accidents is high.
The musculoskeletal system is exposed to vibrations and extreme working positions and loads, especially when driving in harsh terrain areas or slopes. If you get stuck, handling the heavy engine induces perspiration and often musculoskeletal problems (e.g., lumbago).
Cold injuries are common among snowmobile workers. The speed of the vehicle aggravates the cold exposure. Typical injured parts of the body are especially the face (could in extreme cases include cornea), ears, hands and feet.
Snowmobiles are usually used in remote areas where climate, terrain and other conditions contribute to the risks.
The snowmobile helmet must be developed for the working situation on the snowmobile with attention to the specific exposure risks produced by the vehicle itself, terrain conditions and climate. Clothing must be warm, windproof and flexible. The activity transients experienced during snowmobile riding are difficult to accommodate in one clothing system and require special consideration.
Snowmobile traffic in remote areas also presents a communication problem. Work organization and equipment should ensure safe communication with the home base. Extra equipment must be carried to handle emergency situations and allow protection for a time long enough for the rescue team to function. Such equipment includes, for example, wind sack, extra clothing, first-aid equipment, snow shovel, repair kit and cooking gear.