- You are here:
-
Home

-
Part III. Management & Policy
- Disability and Work

17. Disability and Work
Chapter Editors: Willi Momm and Robert Ransom
Table of Contents
Figures
Disability: Concepts and Definitions
Willi Momm and Otto Geiecker
Case Study: Legal Classification of Disabled People in France
Marie-Louise Cros-Courtial and Marc Vericel
Social Policy and Human Rights: Concepts of Disability
Carl Raskin
International Labour Standards and National Employment Legislation in Favour of Disabled Persons
Willi Momm and Masaaki Iuchi
Vocational Rehabilitation and Employment Support Services
Erwin Seyfried
Disability Management at the Workplace: Overview and Future Trends
Donald E. Shrey
Rehabilitation and Noise-induced Hearing Loss
Raymond Hétu
Rights and Duties: An Employer’s Perspective
Susan Scott-Parker
Case Study: Best Practices Examples
Rights and Duties: Workers’ Perspective
Angela Traiforos and Debra A. Perry
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.







Disability: Concepts and Definitions
Preliminary Considerations
Most people seem to know what a disabled person is and are certain that they would be able to identify an individual as disabled, either because the disability is visible or because they are aware of a specific medical condition that lends itself to be called disability. However, what precisely the term disability means is less easy to determine. A common view is that having a disability makes an individual less capable of performing a variety of activities. In fact, the term disability is as a rule used to indicate a reduction or deviation from the norm, a shortcoming of an individual that society has to reckon with. In most languages, terms equivalent to that of disability contain the notions of less value, less ability, a state of being restricted, deprived, deviant. It is in line with such concepts that disability is exclusively viewed as a problem of the affected individual and that the problems indicated by the presence of a disability are considered to be more or less common to all situations.
It is true that a disabling condition may affect to varying degrees the personal life of an individual and his or her relations with family and community. The individual who has a disability may, in fact, experience the disability as something that sets him or her apart from others and that has a negative impact on the way life is organized.
However, meaning and impact of disability change substantially depending on whether the environment and the attitudes of the public accommodate a disability or whether they do not. For example, in one context, the person who uses a wheelchair is in a state of complete dependency, in another he or she is as independent and working as any other person.
Consequently, the impact of an alleged dysfunction is relative to the environment, and disability is thus a social concept and not solely the attribute of an individual. It is also a highly heterogeneous concept, making the search for a homogeneous definition a virtually impossible task.
Despite many attempts to define disability in general terms, the problem remains concerning what renders an individual disabled and who should belong to this group. For example, if disability is defined as dysfunction of an individual, how to classify a person who despite a serious impairment is fully functional? Is the blind computer specialist who is gainfully employed and has managed to solve his or her transport problems, secure adequate housing and have a family still a disabled person? Is the baker who can no longer exercise his profession because of a flour allergy to be counted among disabled job-seekers? If so, what is the real meaning of disability?
To understand this term better, one has first to distinguish it from other related concepts that are often confused with disability. The most common misunderstanding is to equate disability with disease. Disabled people are often described as the opposite of healthy people and, consequently, as needing the help of the health profession. However, disabled people, as anyone else, need medical help only in situations of acute sickness or illness. Even in cases where the disability results from a protracted or chronic illness, such as diabetes or a cardiac disease, it is not the sickness as such, but its social consequences that are involved here.
The other most common confusion is to equate disability with the medical condition that is one of its causes. For example, lists have been drawn up that classify disabled people by types of “disability”, such as blindness, physical malformations, deafness, paraplegia. Such lists are important for determining who should be counted as a disabled person, except that the use of the term disability is inaccurate, because it is confounded with impairment.
More recently, efforts have been made to describe disability as difficulty in performing certain types of function. Accordingly, a disabled person would be someone whose ability to perform in one or several key areas—such as communication, mobility, dexterity and speed—is affected. Again, the problem is that a direct link is made between the impairment and the resulting loss of function without taking into account the environment, including the availability of technology that could compensate for the loss of function and thus render it insignificant. To look at disability as the functional impact of impairment without acknowledging the environmental dimension means to put the blame for the problem entirely on the disabled individual. This definition of disability still stays within the tradition of regarding disability as a deviation from the norm and ignores all other individual and societal factors that together constitute the phenomenon of disability.
Can disabled people be counted? This may be possible within a system that applies precise criteria as to who is sufficiently impaired to be counted as disabled. The difficulty is to make comparisons between systems or countries that apply different criteria. However, who will be counted? Strictly speaking, censuses and surveys that undertake to produce disability data can count only people who themselves indicate that they have an impairment or a functional restriction on account of an impairment, or who believe that they are in a situation of disadvantage because of an impairment. Unlike gender and age, disability is not a clearly definable statistical variable, but a contextual term that is open to interpretation. Therefore, disability data can offer only approximations and should be treated with utmost care.
For the reasons outlined above, this article does not constitute yet another attempt to present a universal definition of disability, or to treat disability as an attribute of an individual or a group. Its intention is to create an awareness about the relativity and heterogeneity of the term and an understanding about the historical and cultural forces that have shaped legislation as well as positive action in favour of people identified as disabled. Such an awareness is the prerequisite for the successful integration of disabled people in the workplace. It will permit a better understanding of the circumstances that need to be in place to make the disabled worker a valuable member of the workforce instead of being barred employment or pensioned off. Disability is presented here as being manageable. This requires that individual needs such as skill upgrading or the provision with technical aids, be addressed, and accommodated by adjusting the workplace.
There is currently a vivid international debate, spearheaded by disability organizations, regarding a non-discriminatory definition of disability. Here, the view is gaining ground that disability should be identified where a particular social or functional disadvantage occurs or is anticipated, linked to an impairment. The issue is how to prove that the disadvantage is not the natural, but rather the preventable result of the impairment, caused by a failure of society to make adequate provision for the removal of physical barriers. Leaving aside that this debate reflects primarily the view of disabled people with a mobility impairment, the possible unwelcome consequence of this position is that the state may shift expenditures, such as for disability benefits or special measures, based on disability, to those that improve the environment.
Nevertheless, this debate, which is continuing, has highlighted the need to find a definition of disability that reflects the social dimension without sacrificing the specificity of the disadvantage based on an impairment, and without losing its quality as an operational definition. The following definition tries to reflect this need. Accordingly, disability can be described as the environmentally determined effect of an impairment that, in interaction with other factors and within a specific social context, is likely to cause an individual to experience an undue disadvantage in his or her personal, social or professional life. Environmentally determined means that the impact of the impairment is influenced by a variety of factors, including preventive, corrective and compensatory measures as well as technological and accommodative solutions.
This definition recognizes that in a different environment that erects fewer barriers, the same impairment could be without any significant consequences, hence without leading to a disability. It stresses the corrective dimension over a concept that takes disability as an unavoidable fact and that simply seeks to ameliorate the living conditions of the afflicted persons. At the same time, it maintains the grounds for compensatory measures, such as cash benefits, because the disadvantage is, despite the recognition of other factors, still specifically linked to the impairment, irrespective of whether this is the result of a dysfunction of the individual or of negative attitudes of the community.
However, many disabled people would experience substantial limitations even in an ideal and understanding environment. In such cases the disability is primarily based in the impairment and not in the environment. Improvements in environmental conditions can substantially reduce dependency and restrictions, but they will not alter the fundamental truth that for many of these severely disabled people (which is different from severely impaired) participation in social and professional life will continue to be restricted. It is for these groups, in particular, that social protection and ameliorative provisions will continue to play a more significant role than the aim of full integration into the workplace which, if it takes place, is often done for social rather than for economic reasons.
But this is not to suggest that persons thus defined as severely disabled should live a life apart and that their limitations should be grounds for segregation and exclusion from the life of the community. One of the major reasons for exercising utmost caution as regards the use of disability definitions is the widespread practice of making a person thus identified and labelled the object of discriminatory administrative measures.
Nevertheless, this points to an ambiguity in the concept of disability that gives rise to so much confusion and that could be a main reason for the social exclusion of disabled people. For, on the one hand, many campaign with the slogan that disability does not mean inability; on the other, all existing protective systems are based on the grounds that disability means inability to make a living on one’s own. The reluctance of many employers to hire disabled people may be founded in this basic contradiction. The answer to this is a reminder that disabled people are not a homogeneous group, and that each case should be judged individually and without bias. But it is true that disability may mean both: an inability to perform according to the norm or an ability to perform as well as or even better than others, if given the opportunity and the right kind of support.
It is obvious that a concept of disability as outlined above calls for a new foundation for disability policies: sources of inspiration for how to modernize policies and programmes in favour of disabled persons can be found among others in the Vocational Rehabilitation and Employment (Disabled Persons) Convention, 1983 (No. 159) (ILO 1983) and the United Nations Standard Rules on the Equalization of Opportunities for Persons with Disabilities (United Nations 1993).
In the following paragraphs, the various dimensions of the disability concept as it affects present law and practice will be explored and described in an empirical manner. Evidence will be provided that various disability definitions are in use, mirroring the world’s different cultural and political legacies rather than giving cause for the hope that a single universal definition can be found which is understood by everyone in the same manner.
Disability and normality
As mentioned above, most past regulatory attempts at defining disability have fallen prey, in one form or another, to the temptation of describing disability as primarily negative or deviatory. The human being afflicted with disability is seen as a problem and becomes a “social case”. A disabled person is assumed to be unable to pursue normal activities. He or she is a person with whom all is not quite in order. There is an abundance of scientific literature that depicts disabled people as having a behavioural problem, and in many countries “defectology” was and still is a recognized science that sets out to measure the degree of deviation.
Individuals who have a disability generally defend themselves against such a characterization. Others resign themselves to the role of a disabled person. Classifying persons as disabled disregards the fact that what disabled individuals have in common with the non-disabled usually far outweighs that which makes them different. Further, the underlying concept that disability is a deviation from the norm is a questionable value statement. These considerations have incited many people to prefer the term persons with disabilities to that of disabled persons, as the latter term could be understood as making disability the primary characteristic of an individual.
It is thoroughly conceivable that human and social reality be defined in such a way that disability be regarded as consistent with normalcy and not as a deviation from it. In fact, the Declaration that was adopted in 1995 by the heads of state and government at the UN World Summit for Social Development in Copenhagen describes disability as a form of social diversity. This definition demands a conception of society which is a society “for all”. Thereby previous attempts at defining disability negatively, as deviation from the norm or as deficiency, are no longer valid. A society which adapts itself to disability in an inclusive manner could substantially overcome those effects of disability which were previously experienced as overly restrictive.
Disability as identity
Despite the danger that the label will invite segregation and discrimination, there are valid reasons to adhere to the usage of the term disability and to group individuals in this category. It cannot be denied, from an empirical standpoint, that many individuals with disability share similar, mostly negative, experiences of discrimination, exclusion and economic or social dependency. There exists a factual categorization of human beings as disabled, because specific negative or censorious social behaviour patterns appear to be based upon disability. Conversely, where there are efforts made to fight discrimination on the basis of disability, it also becomes necessary to stipulate who should have the right to enjoy protection under such measures.
It is in reaction to the way society treats people with disabilities that many individuals who have experienced discrimination in one form or another because of their disability join together in groups. They do so partly because they feel more at ease among individuals who share their experience, partly because they wish to advocate common interests. They accordingly accept the disabled role, if indeed for very different motives: some, because they want to induce society to view disability, not as an attribute of isolated individuals, but rather as the result of action and neglect on the part of the community which unduly curtails their rights and opportunities; the others, because they acknowledge their disability and demand their right to be accepted and respected in their difference, which includes their right to struggle for equality of treatment.
However, most individuals who, on account of an impairment, have a functional limitation of one form or another appear not to see themselves as disabled. This creates a problem not to be underestimated for those engaged with the politics of disability. For example, should those who do not self-identify as disabled be counted among the numbers of disabled persons, or only those who register as disabled?
Legal recognition as disabled
In many constituencies definitions of disability are identical with an administrative act of recognizing a disability. This recognition as disabled becomes a prerequisite for the claiming of support on the basis of a physical or mental limitation or for litigation under an anti-discrimination law. Such support can comprise provisions for rehabilitation, special education, retraining, privileges in the securing and preserving of a place of employment, guarantee of subsistence through income, compensation payments and assistance with mobility, etc.
In all cases in which legal regulations are in force in order to compensate for or to prevent disadvantages, there arises the need to clarify who has a claim on such legal provisions, be these benefits, services or protective measures. It follows thereupon, that the definition of disability is conditioned by the type of service or regulation which is offered. Virtually every existing definition of disability thus mirrors a legal system and draws its meaning from this system. Being recognized as disabled means to fulfil the conditions for benefiting from the possibilities presented by this system. These conditions, however, may vary among constituencies and programmes and, consequently, many different definitions may coexist side by side within a country.
Further evidence that the legal realities of the respective nations determine the definition of disability is offered by those countries, such as Germany and France, which have introduced a regulation including quotas or the levying of fines in order to assure disabled people access to employment opportunities. It can be demonstrated that with the introduction of such legislation, the number of “disabled” workers has risen drastically. This rise is to be explained only by the fact that employees—often on the recommendation of employers—who in the absence of such a law would never have designated themselves as disabled, register themselves as such. These same individuals were also never previously registered statistically as disabled.
Another legal difference among countries is the treatment of a disability as a temporary or permanent condition. In some countries, which offer disabled persons specific advantages or privileges, these privileges are limited to the duration of a recognized disadvantage. If this state of disadvantage is overcome through corrective actions, the disabled person loses his or her privileges—independently of whether medical facts (e.g., the loss of an eye or a limb) remain. For example, an individual who has successfully completed rehabilitation that has re-established lost functional abilities may lose entitlements to disability benefits or may not even enter a benefit scheme.
In other countries, lasting privileges are offered to offset real or hypothetical handicaps. This practice has resulted in the development of a legally recognized disability status bearing elements of “positive discrimination”. These privileges often apply even to those who are no longer actually in need of them because they are socially and economically well integrated.
The problem with statistical registration
A definition of disability that can be applied universally is impossible, since every country, and practically every administrative body, works with different concepts of disability. Every attempt to measure disability statistically must take into account the fact that disability is a system-dependent, and therefore a relative, concept.
Consequently, most regular statistics contain information only about the beneficiaries of specific state or public provisions who have accepted disability status in accordance with the operative definitions of the law. People who do not view themselves as disabled and manage alone with a disability usually do not come within the purview of official statistics. In fact, in many countries, such as the United Kingdom, many disabled people avoid statistical registration. The right not to be registered as disabled is in keeping with the principles of human dignity.
Therefore, occasionally, efforts are made to determine the total number of disabled persons through surveys and censuses. As already argued above, these come up against objective conceptual limits which render the comparability of such data between countries practically impossible. Above all, it is controversial what precisely such surveys are meant to prove, in particular as the notion of disability, as an objective set of findings that is equally applied and understood in all countries, cannot be sustained. Thus, a low number of statistically registered persons with disability in some countries does not necessarily reflect an objective reality, but most likely the fact that the countries in question offer fewer services and legal regulations in favour of disabled persons. Conversely, those countries which have an extensive social protection and rehabilitation system are likely to show a high percentage of disabled individuals.
Contradictions in the use of the concept of disabled persons
Objective results are, therefore, not to be expected on the level of quantitative comparison. But there is also no uniformity of interpretation from a qualitative point of view. Here again, the respective context and the intention of lawmakers determine the definition of disability. For example, the effort to guarantee disabled persons social protection requires disability to be defined as the inability to earn one’s own living. In contrast, a social policy whose goal is vocational integration endeavours to describe disability as a condition that, with the help of appropriate measures, need not have any detrimental effects on the level of performance.
International Definitions of Disability
The concept of disability in Convention No. 159 of the International Labour Organization
The above considerations also underlie the framework definition used in the Vocational Rehabilitation and Employment (Disabled Persons) Convention, 1983 (No. 159) (ILO 1983). Article 1.1 contains the following formulation: “For the purposes of this Convention, the term ‘disabled person’ means an individual whose prospects of securing, retaining and advancing in suitable employment are substantially reduced as a result of a duly recognized physical or mental impairment”.
This definition contains the following constituent elements: the reference to mental or physical impairment as the original cause of the disability; the necessity of a state recognition procedure that—in accordance with the respective national realities—determines who should be considered disabled; the determination that disability is not constituted by the impairment itself but by the possible and real social consequences of an impairment (in this case a more difficult situation on the labour market); and the established entitlement to measures which help to secure equality of treatment on the labour market (see Article 1.2). This definition consciously avoids an association with concepts such as inability and leaves room for an interpretation which holds that disability can also be conditioned by misconceived opinions held by an employer which may result in conscious or unconscious discrimination. On the other hand, this definition does not rule out the possibility that, in the case of a disability, objective limitations with respect to performance can occur, and leaves open whether or not the equal treatment principle of the Convention would apply in this case.
The definition in the ILO Convention does not make a claim to be a comprehensive, universally applicable definition of disability. Its sole intention is to provide for a clarification of what disability could mean in the context of employment and labour measures.
The concept of disability in light of the definition of the World Health Organization
The International Classification of Impairments, Disabilities and Handicaps (ICIDH) of the World Health Organization (WHO 1980) offers a definition of disability, in the area of health policy, which differentiates between impairment, disability and handicaps:
- “In the context of health experience, an impairment is any loss or abnormality of psychological, physiological, or anatomical structure or function.”
- “In the context of health experience, a disability is any restriction or lack (resulting from an impairment) of ability to perform an activity in the manner or within the range considered normal for a human being.”
- “In the context of health experience, a handicap is a disadvantage for a given individual, resulting from an impairment or a disability, that limits or prevents the fulfilment of a role that is normal (depending on age, sex, and social and cultural factors) for that individual.”
The new and distinctive aspects of this conceptual differentiation do not lie in its traditional epidemiological approach and its classificatory apparatus, but rather in its introduction of the concept of handicap, which calls on those concerned with public health policy to reflect on the social consequences of specific impairments on a person affected and to regard the treatment process as part of a holistic concept of life.
The WHO clarification was especially necessary because the words impairment and disability were previously often equated with concepts such as crippled, mentally retarded and the like, which convey an exclusively negative image of disability to the public. A categorization of this kind is, in fact, not suited to a precise definition of the concrete situation of a disabled individual within society. The WHO terminology has since become a reference for the discussion on the concept of disability at the national and international levels. It will, therefore, be necessary to dwell on these concepts a little more.
Impairment. With this concept, health professionals customarily designate an existing or developing injury to bodily functions or to vital life processes in a particular person that affects one or more parts of the organism or that indicates a defect in the psychic, mental or emotional functioning as the result of an illness, accident or congenital or hereditary condition. An impairment can be temporary or permanent. The influences of professional or social contexts or of the environment as a whole are not taken into consideration in this category. Here, the physician’s assessment of a person’s medical condition or an impairment is exclusively at issue, without consideration of the consequences that this impairment may have upon that person.
Disability. Such impairment or loss can result in substantial limitation to the active lives of persons afflicted. This consequence of impairment is termed disability. Functional disorders of the organism, such as, for example, psychic disorders and mental breakdowns, can lead to more or less severe disabilities and/or negative effects in the execution of specific activities and duties of daily living. These effects can be temporary or permanent, reversible or irreversible, constant, progressive or subject to successful treatment. The medical concept of disability designates, therefore, functional limitations which arise in the lives of specific individuals as the direct or indirect result of a physical, psychosocial or mental impairment. Above all, disability reflects the personal situation of the individual who has an impairment. However, as the personal consequences of a disability depend upon age, sex, social position and profession, and so on, the same or similar functional disorders can have thoroughly different personal consequences for different individuals.
Handicap. As soon as persons with physical or mental impairments enter their social, professional or private context, difficulties may arise which bring them into a situation of disadvantage, or handicap, in relation to others.
In the original version of the ICIDH, the definition of handicap signifies a disadvantage which emerges as the result of an impairment or a disability, and which limits an individual in the performance of what is regarded as a “normal” role. This definition of handicap, which bases the problem exclusively upon the personal situation of the person afflicted, has since come under criticism, for the reason that it does not sufficiently take into account the role of the environment and the attitude of society in bringing about the situation of disadvantage. A definition which takes these objections into account should reflect upon the relationship between the disabled individual and the manifold environmental, cultural, physical or social barriers that a society reflecting the attitudes of non-disabled members tends to erect. In light of this, every disadvantage in the life of a specific person that is not so much the result of an impairment or a disability, but of negative or unaccommodating attitudes in the largest sense, should be termed “handicap”. Further, any measures taken towards the improvement of the situation of disabled individuals, including those that help them to fully participate in life and in society, would contribute to preventing the “handicap”. A handicap thus is not the direct result of an existing impairment or disability, but the result of the interaction between an individual with a disability, the social context and the immediate surroundings.
It may not be assumed at the outset, therefore, that a person with an impairment or disability must automatically also have a handicap. Many disabled individuals succeed, despite the limitations caused by their disability, in the full pursuit of a profession. On the other hand, not every handicap can be attributed to a disability. It can also be caused by a lack of education that may or may not be linked with disability.
This hierarchical system of classification—impairment, disability, handicap—can be compared with the various phases of rehabilitation; for example, when the purely curative treatment is followed by rehabilitation of functional and psycho-social limitations and is completed with vocational rehabilitation or training for an independent pursuit of life.
The objective assessment of the degree of a disability in the sense of its social consequences (handicap) cannot, for this reason, rely solely upon medical criteria, but must take into account the vocational, social and personal contexts—especially the attitude of the non-disabled population. This state of affairs makes it quite difficult to measure and unequivocally establish a “state of disability”.
Definitions in Use in Various Countries
Disability as a legal category for the establishment of claims
Disability status is determined, as a rule, by a competent national authority on the basis of findings after an examination of individual cases. Therefore, the purpose for which disability status should be recognized plays an essential role—for example, where the determination of the presence of a disability serves the purpose of laying claim to specific personal rights and legal benefits. The primary interest in having a legally sound definition of disability is thus motivated not by medical, rehabilitative or statistical reasons, but rather by juridical reasons.
In many countries, persons whose disability is recognized can lay claim to the right to various services and regulatory measures in specific areas of health and social policies. As a rule, such regulations or benefits are designed to improve their personal situation and to support them in overcoming difficulties. The basis for the guarantee of such benefits thus is an act of official recognition of an individual’s disability on the strength of the respective statutory provisions.
Examples of definition from legislative practice
These definitions vary widely between different states. Only a few examples that are currently in use can be cited here. They serve to illustrate the variety as well as the questionable character of many definitions. As it cannot be the purpose here to discuss specific legal models, the sources of the quotations are not given, nor is an evaluation of which definitions appear more adequate than others. Examples of national definitions of disabled persons:
- Those who are afflicted with a not only temporary functional impairment which is due to an irregular physical, mental or psychological condition or any who are threatened with such a disability. If the degree of disability amounts to at least 50%, it is considered a severe disability.
- All those whose working capacity is diminished by at least 30% (for physical disability) or at least 20% (for mental disability).
- All those whose opportunities to obtain and hold (secure and retain) employment are restricted by either a lack or limitation in their physical or mental capabilities.
- All those who because of an impairment or invalidity are hindered or prevented from the accomplishment of normal activities. The impairment may concern both mental and bodily functions.
- All those whose ability to work is permanently restricted because of a physical, psychical or sensory defect.
- All those who need care or special treatment to assure the support, development and restoration of their vocational capabilities. This includes physical, mental, psychical and social disabilities.
- All those who because of a permanent limitation to their physical, mental or sensory capabilities—independent of whether hereditary or acquired—enjoy only restricted opportunities to pursue an education and participate in vocational and social life.
- Victims of industrial accidents, war disabled and individuals who suffer from a physical, mental or psychical impairment. The reduction of working capacity must amount to at least 30%.
- All those who because of an impairment, illness or hereditary disease experience substantially reduced opportunities in securing and retaining employment appropriate to their age, experience and qualifications.
- Persons with a physical or mental impairment which, to a significant extent, restricts an important part of their life activity or those who are assumed to suffer from such an impairment or for whom earlier records about such impairments exist.
- Persons who are afflicted with a functional disorder or disease that leads to: (a) a total or partial loss of physical or mental functions; (b) illnesses caused or which will forseeably be caused by the presence of organisms in the body; (c) a loss of normal function due to deformation of body parts; (d) the appearance of learning difficulties not present in individuals without functional disorders or restrictions; (e) an impairment to behaviour, thought process, judgement and emotional life.
- Persons who, due to physical or mental impairment as a result of a birth defect, illness or accident, are presumed incapable of earning their living, either permanently or for an extended period of time.
- Persons who, as a result of an illness, injury, a mental or physical weakness, are not in the position for a period of at least six months to earn, from work that corresponds to their potential abilities and cultural level, a specific fraction (1/3, 1/2, 2/3) of that income, which an individual in good condition in the same profession and at the same cultural level would receive.
- The term disability means, with respect to an individual: (a) a physical or mental impairment that substantially limits one or more of the major life activities of such individual; (b) a record of such an impairment; or (c) being regarded as having such impairment.
The multitude of legal definitions which partially supplement and partially exclude one another suggest that definitions serve, above all, bureaucratic and administrative goals. Among all the listed definitions not one can be considered satisfactory, and all raise more questions than they answer. Beyond a few exceptions, most definitions are oriented towards the representation of an individual deficiency and do not address the correlation between an individual and his or her environment. What in reality is the reflection of a complex relativity is reduced in an administrative context to an apparently clear-cut and stable quantity. Such oversimplified definitions then tend to take on a life of their own and frequently force individuals into accepting a status that is commensurate with the law, but not necessarily with their own potential and aspirations.
Disability as an issue for sociopolitical action
Individuals who are recognized as disabled are, as a rule, entitled to measures such as medical and/or vocational rehabilitation or to draw on specific financial benefits. In some countries, the range of sociopolitical measures also includes the granting of certain privileges and support as well as special protective measures. Examples include: a legally embodied principle of equality of opportunity in vocational and social integration; a legally established right to needed assistance in the realization of equal opportunity, a constitutional right to education and vocational integration; the furtherance of vocational training and placement in employment; and a constitutional assurance of increased support in case of need of special help from the state. Several states proceed from the absolute equality of all citizens in all areas of life and have set the realization of this equality as their goal, without seeing a reason for treating the special problems of disabled persons in laws enacted expressly for that purpose. These states usually refrain from defining disability altogether.
Disability in the context of vocational rehabilitation
In contrast to the establishment of pension claims or privileges, the definition of disability in the area of vocational integration emphasizes the avoidable and correctable effects of disability. It is the purpose of such definitions to eliminate, through rehabilitative provisions and active labour market policies, the vocational disadvantages connected with disability. The vocational integration of disabled persons is supported by the allocation of financial assistance, by accompanying provisions in the area of vocational training and by the accommodation of the workplace to the special needs of the disabled worker. Here again, the practices vary greatly between different countries. The range of benefits runs from relatively slight and short-term financial allocations to large-scale, longer-term vocational rehabilitation measures.
Most states set a relatively high value on the furtherance of vocational training for disabled individuals. This can be provided in ordinary or special centres run by public or private agencies, as well as in an ordinary enterprise. Preference given to each differs from country to country. Sometimes the vocational training is conducted in a sheltered workshop or provided as on-the-job training that is reserved for a disabled worker.
As the financial implications of these measures can be considerable for the taxpayer, the act of recognizing a disability is a far-reaching measure. Often, however, the registration is done by a different authority than that which administers the vocational rehabilitation programme and which meets its costs.
Disability as a permanent disadvantage
While the goal of vocational rehabilitation is to overcome the possible negative effects of disability, there exists wide agreement in disability legislation that further protective social measures are sometimes necessary to assure the vocational and social integration of rehabilitated individuals. It is also generally recognized that disability presents the continuing risk of social exclusion independent of the existence of an actual functional disorder. In recognition of this permanent threat, legislators provide a series of protective and supportive measures.
In many countries, for example, employers who are prepared to employ disabled persons in their companies can expect subsidies towards the wages and social security contributions of the disabled workers, the amount and duration of which will vary. Generally, an effort is made to assure that disabled employees receive the same income as non-disabled employees. This can result in situations wherein disabled individuals who receive a lower wage from their employers are refunded up to the full difference through arrangements made by the social protection system.
Even the establishment of small businesses by disabled individuals may be supported through various measures such as loans and loan guarantees, interest subsidies and rent allowances.
In many countries, the protection of disabled individuals from dismissal and the protection of their right to re-employment is handled in different ways. Many states have no special legal regulation for the dismissal of disabled persons; in some, a special commission or institution decides on the justification and legitimacy of a dismissal; in others, special regulations for victims of industrial accidents, for severely disabled workers and for workers on extended periods of sick-leave are still in effect. The legal situation with regard to the re-employment of disabled individuals is similar. Here too, there are countries which recognize a general obligation of the enterprise to keep a worker employed after injury or to re-employ him or her after completion of rehabilitation measures. In other countries, businesses are not under any obligation to re-employ disabled employees. Furthermore, there exist in some countries recommendations and conventions as to how to proceed in such cases, as well as countries in which the employee who has suffered a specific occupational disability is guaranteed either redeployment or return to the previous job after his or her medical recovery is complete.
Differences in treatment by cause of disability
The above overview helps to illustrate that laws provide different types of legal claim which bear clear consequences for the respective national concept of disability. Also the reverse is true: in those countries which provide no such legal entitlements, there exists no need to define disability in legally clear and binding terms. In such cases, the predominant inclination is to recognize as disabled only those who are visibly and markedly disabled in a medical sense—that is, persons with physical impairments, blindness, deafness or mental handicap.
In modern disability legislation—though less in the realm of social security provision—the principle of finality is becoming more grounded. This principle means that not the cause of a disability, but exclusively the needs associated with the disability and the final outcome of measures should be the concern of legislators. Nevertheless, the social status and the legal claims of disabled individuals are often dependent on the cause of their disability.
In consideration of the cause of disability, definitions differ not only in meaning but also in the implications they have in terms of potential benefits and assistance. The most important distinctions are made between disabilities that result from hereditary or birth-related physical, mental or psychological deficiencies or impairments; disabilities brought on by diseases; disabilities caused by home, work, sport or traffic accidents; disabilities brought on by occupational or environmental influences; and disabilities as a result of civil strife and armed conflict.
The relative preference shown to some disabled groups is often the consequence of their respectively better coverage under the social security system. Preference can also reflect the attitude of a community—for instance in the case of war veterans or accident victims—that feels a co-responsibility for the incident that led to the disability, while hereditary disability is often regarded as a problem of the family only. Such societal attitudes towards disability often have more significant consequences than official policy and can sometimes exert a decisive influence—negative or positive—on the process of social reintegration.
Summary and outlook
The diversity of historical, legal and cultural situations renders the discovery of a unitary concept of disability, equally applicable to all countries and situations, virtually impossible. For lack of a common and objective definition of disability, statistics are frequently provided by authorities as a means of keeping client records and interpreting the outcome of measures—a fact that makes an international comparison very difficult, as systems and conditions vary greatly among countries. Even where reliable statistics exist, the problem remains that individuals may be included in statistics who are no longer disabled or who, after successful rehabilitation, are no longer inclined to consider themselves disabled.
In most industrialized countries, the definition of disability is, above all, connected with legal entitlements to medical, social and vocational measures, to protection against discrimination or to cash benefits. As such, most definitions in use reflect legal practice and requirements that differ from country to country. In many cases, the definition is linked to an act of official recognition of disability status.
Owing to developments as different as the emergence of human rights legislation and technological advancements, traditional concepts of disability that led to situations of protected exclusion and segregation are losing ground. A modern concept of disability puts the issue at the intersection between social and employment policies. Disability is thus a term of social and vocational, rather than of medical, relevance. It demands corrective and positive measures to ensure equal access and participation, rather than passive measures of income support.
A certain paradox arises out of the understanding of disability as, on the one hand, something which can be overcome through positive measures, and, on the other, as something lasting which necessitates permanent protective or ameliorative measures. A similar frequently encountered contradiction is that between the idea of disability as fundamentally an issue of individual performance or function restriction, and the idea of disability as the unjustified cause for social exclusion and discrimination.
Opting for one all-encompassing definition can have grave social consequences for particular individuals. Were it declared that all disabled persons are able to work, many would be deprived of their pension claims and social protection. Were all disabled persons judged to show a reduced productivity/performance, hardly a disabled individual would obtain employment. This means that a pragmatic approach must be sought that accepts the heterogeneity of the reality that an ambiguous term such as disability tends to conceal. The new view of disability takes into account the specific situation and needs of disabled individuals as well as the economic and social feasibility of removing barriers to integration.
The goal of preventing undue disadvantage that may be linked with a disability will best be achieved where a flexible definition of disability is applied that takes into account the specific personal and social circumstances of an individual and that avoids stereotyped assumptions. This calls for a case-by-case approach to recognizing disability, which still is needed where different statutory rights and entitlements, notably those to achieve equal training and employment opportunities, are granted under various national laws and regulations.
Nonetheless, definitions of disability are still in use that evoke negative connotations and that contradict integrative concepts by overemphasizing the limiting effects of an impairment. A new view of the matter is called for. The focus should be on recognizing disabled individuals as citizens endowed with rights and abilities, and on empowering them to take charge of their destiny as adults who want to take part in the mainstream of social and economic life.
Likewise, efforts must continue to instill in the community a sense of solidarity that no longer uses a flawed concept of disability as grounds for the careless exclusion of fellow citizens. Between excessive care and neglect there should exist a sober conception of disability which neither mystifies nor underestimates its consequences. Disability can, but need not always, provide the grounds for specific measures. It should in no case provide a justification for discrimination and social exclusion.
International Labour Standards and National Employment Legislation in Favour of Disabled Persons
The Vocational Rehabilitation and Employment (Disabled Persons) Convention, 1983 (No. 159) and Vocational Rehabilitation and Employment (Disabled Persons) Recommendation, 1983 (No.168), which supplement and update the Vocational Rehabilitation (Disabled) Recommendation, 1955 (No. 99), are the principal reference documents for a social policy on the issue of disability. However, there are a number of other ILO instruments which explicitly or implicitly make reference to disability. There are notably the Discrimination (Employment and Occupation) Convention, 1958 (No. 111), the Discrimination (Employment and Occupation) Recommendation, 1958 (No. 111), the Human Resources Development Convention, 1975 (No. 142) and the Human Resources Development Recommendation, 1975 (No.150)
In addition, important references to disability issues are included in a number of other key ILO instruments, such as: Employment Service Convention, 1948 (No. 88); Social Security (Minimum Standards) Convention, 1952 (No. 102); Employment Injury Benefits Convention, 1964 (No. 121); Employment Promotion and Protection against Unemployment Convention, 1988 (No. 168); Employment Service Recommendation, 1948 (No. 83); Labour Administration Recommendation, 1978 (No. 158) and Employment Policy (Supplementary Provisions) Recommendation, 1984 (No. 169).
International labour standards treat disability basically under two different headings: as passive measures of income transfer and social protection, and as active measures of training and employment promotion.
One early objective of the ILO was to ensure that workers receive adequate financial compensation for disability, in particular if it was caused in relation to work or war activities. The underlying concern has been to ensure that a damage is adequately compensated, that the employer is liable for accidents and unsafe working conditions, and that in the interest of good labour relations, there should be fair treatment of workers. Adequate compensation is a fundamental element of social justice.
Quite distinct from the compensation objective is the social protection objective. ILO standards which deal with issues of social security look at disability largely as a “contingency” which needs to be covered under social security legislation, the idea being that disability can be a cause of loss of earning capacity and therefore be a legitimate reason to secure income through transfer payments. The principal objective is to provide insurance against loss of income and thus guarantee decent living conditions for people deprived of the means of gaining their own income due to impairment.
In a similar way, policies which pursue a social protection objective tend to provide public assistance to people with disabilities not covered by social insurance. Also in this case the tacit assumption is that disability means incapacity to find adequate income from work, and that a disabled person has therefore to be the responsibility of the public. As a result, disability policy is in many countries predominantly a concern of the social welfare authorities, and the primary policy is that of providing passive measures of financial assistance.
However, those ILO standards which deal explicitly with disabled persons (such as Conventions Nos. 142 and 159, and Recommendations Nos. 99, 150 and 168) treat them as workers and put disability—quite in contrast to the compensation and social protection concepts—in the context of labour market policies, which have as their objective to ensure equality of treatment and opportunity in training and employment, and which look at disabled people as being part of the economically active population. Disability is understood here basically as a condition of occupational disadvantage which can be and should be overcome through a variety of policy measures, regulations, programmes and services.
ILO Recommendation No. 99 (1955), which for the first time invited member States to shift their disability policies from a social welfare or social protection objective towards a labour integration objective, had a profound impact on law in the 1950s and 1960s. But the real breakthrough occurred in 1983 when the International Labour Conference adopted two new instruments, ILO Convention No. 159 and Recommendation No. 168. As of March 1996, 57 out of 169 member States had ratified this Convention.
Many others have readjusted their legislation so as to comply with this Convention even if they have not, or not yet, ratified this international treaty. What distinguishes these new instruments from the former ones is the recognition by the international community and by employers’ and workers’ organizations of the right of disabled persons to equal treatment and opportunity in training and employment.
These three instruments now form a unity. They aim to ensure active labour market participation of disabled people and thus to challenge the sole validity of passive measures or of policies which treat disability as a health problem.
The purposes of the international labour standards which have been adopted with this objective in mind can be described as follows: to remove the barriers which stand in the way of full social participation and integration of disabled people in the mainstream, and to provide the means to promote effectively their economic self-reliance and social independence. These standards oppose a practice that treats disabled people as being outside the norm and excludes them from the mainstream. They object to the tendency of taking disability as a justification for social marginalization and for denying people, on account of their disability, civil and workers’ rights which non-disabled people enjoy as a matter of course.
For the purpose of clarity we may group the provisions of international labour standards which promote the concept of the right of disabled people to active participation in training and employment into two groups: those which address the principle of equal opportunity and those which address the principal of equal treatment.
Equal opportunity: the policy goal which lies behind this formula is to ensure that a disadvantaged population group has access to the same employment and income-earning possibilities and opportunities as the mainstream population.
In order to achieve equal opportunity for disabled people, the pertinent international labour standards have established rules and recommended measures for three types of action:
- Action to empower the disabled individual to achieve the level of competencies and abilities required to take advantage of employment opportunity and to provide the technical means and the required assistance which would enable that individual to cope with the demands of a job. This type of action is what essentially constitutes the process of vocational rehabilitation.
- Action which helps to adjust the environment to the special needs of disabled persons, such as worksite, job, machine or tool adaptations as well as legal and promotional action which helps to overcome negative and discriminatory attitudes that cause exclusion.
- Action which ensures disabled people real employment opportunities. This includes legislation and policies which favour remunerative work over passive income support measures, as well as those which entice employers to employ, or to maintain in employment, workers with a disability.
- Action which sets employment targets or establishes quotas or levies (fines) under affirmative action programmes. It also includes services by which labour administrations and other bodies may assist disabled people to find jobs and to advance in their careers.
Therefore, these standards, which have been developed to guarantee equality of opportunity, imply the promotion of special positive measures to help disabled people make the transition into active life or to prevent unnecessary, unwarranted transition into a life reliant upon passive income support. Policies geared to establish equality of opportunity are, therefore, usually concerned with the development of support systems and special measures to bring about effective equality of opportunities, which are justified by the need to compensate for the real or presumed disadvantages of disability. In ILO legal parlance: “Special positive measures aimed at effective equality of opportunity … between disabled workers and other workers shall not be regarded as discriminating against other workers” (Convention No. 159, Article 4).
Equal treatment: The precept of equal treatment has a related but distinct objective. Here the issue is that of human rights, and the regulations which ILO member States have agreed to observe have precise legal implications and are subject to monitoring and—in case of violation—to legal recourse and/or arbitration.
ILO Convention No. 159 established equal treatment as a guaranteed right. It furthermore specified that equality has to be “effective”. This means that conditions should be such as to ensure that the equality is not only formal but real and that the situation resulting from such treatment puts the disabled person into an “equitable” position, that is one which corresponds by its results and not by its measures to that of non-disabled persons. For example, to assign a disabled worker the same job as a non-disabled worker is not equitable treatment if the worksite is not fully accessible or if the job is not suited to the disability.
Present Legislation on Vocational Rehabilitation and Employment of Disabled Persons
Each country has a different history of vocational rehabilitation and employment of disabled persons. The legislation of member States varies due to their different stages of industrial development, social and economic situations, and so on. For example, some countries already had legislation on disabled persons before the Second World War, deriving from disability measures for disabled veterans or poor people at the beginning of this century. Other countries started to take concrete measures to support disabled persons after the Second World War, and established legislation in the field of vocational rehabilitation. This was often expanded following the adoption of the Vocational Rehabilitation of the Disabled Recommendation, 1955 (No. 99) (ILO 1955). Other countries only recently started taking measures for disabled persons due to the awareness created by the International Year of Disabled Persons in 1981, the adoption of ILO Convention No.159 and Recommendation No. 168 in 1983 and the United Nations Decade of Disabled Persons (1983–1992).
The current legislation on vocational rehabilitation and employment of disabled persons is divided into four types according to different historical backgrounds and policies (figure 1).
Figure 1. Four types of legislation on rights of persons with disabilities.
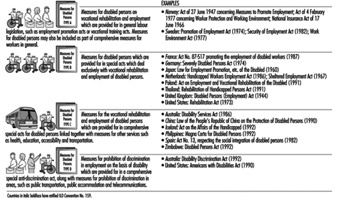
We must realize that there are no clear divisions between these four groups and that they may overlap. Legislation in a country may correspond not only to one type, but to several. For example, the legislation of many countries is a combination of two types or more. It seems that the legislation of Type A is formulated in the early stage of measures for disabled persons, whereas the legislation of Type B is from a later stage. The legislation of Type D, namely the prohibition of discrimination because of disabilities, has been growing in recent years, supplementing the prohibition of discrimination on the basis of race, sex, religion, political opinion and so on. The comprehensive nature of legislation of Types C and D may be used as models for those developing countries which have not yet formulated any concrete legislation on disability.
Sample Measures of each Type
In the following paragraphs, the structure of legislation and measures stipulated are outlined by some examples of each type. As measures for vocational rehabilitation and employment of disabled persons in each country are often more or less the same, regardless of the type of legislation in which they are provided for, some overlaps occur.
Type A: Measures for disabled persons on vocational rehabilitation and employment which are provided for in general labour legislation such as employment promotion acts or vocational training acts. Measures for disabled persons may also be included as part of comprehensive measures for workers in general.
The characteristic of this type of legislation is that measures for disabled people are provided for in the acts which apply to all workers, including disabled workers, and to all enterprises employing workers. As measures on employment promotion and employment security for disabled persons are basically incorporated as part of comprehensive measures for workers in general, the national policy gives priority to internal rehabilitation efforts of enterprises and to preventive activities and early intervention in working environments. To this end, working environment committees, which consist of employers, workers and safety and health personnel are often set up in enterprises. The details of the measures tend to be provided for in regulations or rules under the acts.
For example, the Working Environment Act of Norway applies to all workers employed by most enterprises in the country. Some special measures for handicapped persons are incorporated: (1) Passageways, sanitary facilities, technical installations and equipment shall be designed and arranged so that handicapped persons can work in the enterprise, as far as possible. (2) If a worker has become handicapped in the workplace as a result of accident or sickness the employer shall, as far as possible, take the necessary measures to enable the worker to obtain or retain suitable employment. The worker shall preferably be given an opportunity to continue his or her former work, possibly after special adaptation of the work activity, alteration of technical installations, rehabilitation or retraining and so on. The following are examples of action that must be taken by the employer:
- procurement of or changes to technical equipment used by the worker—for instance, tools, machinery, and so on
- alterations to the workplace—this could refer to alterations to furniture and equipment, or to alterations to doorways, thresholds, installation of lifts, procurement of wheelchair ramps, repositioning of door handles and light switches, and so on
- organization of the work—this could involve alteration of routines, changes in working hours, active participation by other workers; for instance, recording on and transcribing from a dictaphone cassette
- measures in connection with training and retraining.
In addition to these measures, there is a system which provides employers of handicapped persons with subsidies concerning the additional cost to adapt the workplace to the worker, or vice versa.
Type B: Measures for disabled persons which are provided for in special acts which deal exclusively with vocational rehabilitation and employment of disabled persons.
This type of legislation usually has specific provisions on vocational rehabilitation and employment dealing with various measures, while other measures for disabled people are stipulated in other acts.
For example, the Severely Disabled Persons Act of Germany provides for the following special assistance for disabled persons to improve their employment opportunities, as well as vocational guidance and placement services:
- vocational training in enterprises and training centres or in special vocational rehabilitation institutions
- special benefits for disabled persons or employers—payment of application and removal costs, transitional allowances, technical adaptation of workplaces, payment of housing costs, assistance in acquiring a special vehicle or additional special equipment or in obtaining a driving licence
- the obligation for public and private employers to reserve 6% of their workplaces for severely disabled persons; compensation payments must be paid in respect of the places not filled in this manner
- special protection against dismissal for all severely disabled persons after a period of six months
- representation of the interests of severely disabled persons in the enterprise by means of a staff counsellor
- supplementary benefits for severely disabled persons to ensure their integration into occupation and employment
- special workshops for disabled persons who are unable to work on the general labour market because of the nature or severity of their impediment
- grants for employers of up to 80% of the wage paid to disabled persons for a period of two years, as well as payments in respect of the adaptation of workplaces and the establishment of specified probationary periods of employment.
Type C: Measures for the vocational rehabilitation and employment of disabled persons which are provided for in comprehensive special acts for disabled persons linked together with measures for other services such as health, education, accessibility and transportation.
This type of legislation usually has general provisions concerning the purpose, declaration of policy, coverage, definition of terms in the first chapter, and after that several chapters which deal with services in the fields of employment or vocational rehabilitation as well as health, education, accessibility, transportation, telecommunications, auxiliary social services and so on.
For example, the Magna Carta for Disabled Persons of the Philippines provides for the principle of equal opportunity for employment. The following are several measures from chapter on employment:
- 5% of reserved employment for disabled persons in departments or agencies of the government
- incentives for employers such as a deduction from their taxable income equivalent to a certain part of the wages of disabled persons or of the costs of improvements or modifications of facilities
- vocational rehabilitation measures that serve to develop the skills and potentials of disabled persons and enable them to compete favourably for available productive and remunerative employment opportunities, consistent with the principle of equal opportunity for disabled workers and workers in general
- vocational rehabilitation and livelihood services for disabled people in the rural areas
- vocational guidance, counselling and training to enable disabled persons to secure, retain and advance in employment, and the availability and training of counsellors and other suitably qualified staff responsible for these services
- government-owned vocational and technical schools in every province for a special vocational and technical training programme for disabled persons
- sheltered workshops for disabled individuals who cannot find suitable employment in the open labour market
- apprenticeship.
Furthermore, this act has provisions concerning prohibition of discrimination against disabled persons in employment.
Type D: Measures for prohibition of discrimination in employment on the basis of disability which are provided for in a comprehensive special anti-discrimination act along with measures for prohibition of discrimination in areas such as public transportation, public accommodation and telecommunications.
The feature of this type of legislation is that there are provisions which deal with discrimination on the ground of disability in employment, public transportation, accommodation, telecommunications and so on. Measures for vocational rehabilitation services and the employment of disabled people are provided for in other acts or regulations.
For example, the Americans with Disabilities Act prohibits discrimination in such important areas as employment, access to public accommodations, telecommunications, transportation, voting, public services, education, housing and recreation. As for employment in particular, the Act prohibits employment discrimination against “qualified individuals with a disability” who, with or without “reasonable accommodation”, can perform the essential functions of the job, unless such accommodation would impose “undue hardship” on the operation of the business. The Act prohibits discrimination in all employment practices, including job application procedures, hiring, firing, advancement, compensation, training and other terms, conditions and privileges of employment. It applies to recruitment, advertising, tenure, layoff, leave, fringe benefits and all other employment-related activities.
In Australia, the purpose of the Disability Discrimination Act is to provide improved opportunities for people with a disability and to assist in breaking down barriers to their participation in the labour market and other areas of life. The Act bans discrimination against people on the grounds of disability in employment, accommodation, recreation and leisure activities. This complements existing anti-discrimination legislation that outlaws discrimination on the grounds of race or gender.
Quota/Levy Legislation or Anti-discrimination Legislation?
The structure of national legislation on vocational rehabilitation and employment of disabled persons varies somewhat from country to country, and it is therefore difficult to determine which type of legislation is best. However, two types of legislation, namely quota or levy legislation and anti-discrimination legislation, seem to emerge as the two main legislative modes.
Although some European countries, among others, have quota systems which are usually provided in the legislation of Type B, they are quite different in some points, such as the category of disabled persons to whom the system is applied, the category of employers on whom the employment obligation is imposed (for example, size of the enterprise or public sector only) and the employment rate (3%, 6%, etc.). In most countries the quota system is accompanied by a levy or grant system. Quota provisions are also included in the legislation of non-industrialized countries as varied as Angola, Mauritius, the Philippines, Tanzania and Poland. China is also examining the possibility of introducing a quota system.
There is no doubt that a quota system that is enforceable could contribute considerably to raising the employment levels of disabled persons in the open labour market. Also, the system of levies and grants helps to rectify the financial inequality between the employers who try to employ disabled workers and the ones who do not, while levies contribute to accumulating valuable resources that are needed to finance vocational rehabilitation and incentives for employers.
On the other hand, one of the problems of the system is the fact that it requires a clear definition of disability for recognizing qualification, and strict rules and procedures for registration, and therefore it may raise the problem of stigma. There may also be the potential discomfort of a disabled person being at a place of employment where he or she is not wanted by the employer but is merely tolerated to avoid legal sanctions. In addition, credible enforcement mechanisms and their effective application are required for quota legislation to achieve results.
Anti-discrimination legislation (Type D) seems to be more appropriate for the principle of normalization, ensuring disabled persons equal opportunities in society, because it promotes employers’ initiatives and social consciousness by means of environmental improvement, not employment obligation.
On the other hand, some countries have difficulties in enforcing anti-discrimination legislation. For example, remedial action usually requires a victim to play the role of complainant, and in some cases it is difficult to prove discrimination. Also the process of remedial action commonly takes a long time because a lot of complaints of discrimination on the basis of disability are sent to courts or equal rights commissions. It is generally admitted that anti-discrimination legislation has still to prove its effectiveness in placing and maintaining large numbers of disabled workers in employment.
Future Trends
Although it is difficult to forecast future trends in legislation, it appears that anti-discrimination acts (Type D) are one stream which both developed countries and developing countries will consider.
It seems that industrialized countries with a history of quota or quota/levy legislation will watch the experience of countries such as the United States and Australia before taking action to adjust their own legislative systems. In particular in Europe, with its concepts of redistributive justice, it is likely that the prevailing legislative systems will be maintained, while, however, introducing or strengthening anti-discrimination provisions as an additional legislative feature.
In a few countries like the United States, Australia and Canada, it could be politically difficult to legislate a quota system for disabled people without having quota provisions also in relation to other population groups that experience disadvantages in the labour market, such as women and ethnic and racial minority groups currently covered by human rights or employment equity legislation. Although a quota system would have some advantages for disabled people, the administrative apparatus required for such a multicategory quota system would be enormous.
It appears that developing countries which have no disability legislation may choose legislation of Type C, including a few provisions concerning prohibition of discrimination, because it is the more comprehensive approach. The risk of this approach, however, is that comprehensive legislation which cuts across the responsibility of many ministries becomes the affair of a single ministry, mostly that responsible for social welfare. This may be counterproductive, reinforce segregation and weaken the government’s ability to implement the law. Experience shows that comprehensive legislation looks good on paper, but is rarely applied.
Case Study: Legal Classification of Disabled People in France
The heterogeneity of disability is mirrored in the diversity of legal provisions and benefits that most countries have introduced and codified over the last hundred years. The example of France is chosen because it has perhaps one of the most elaborate regulatory frameworks regarding the classification of disability. While the French system may not be typical compared with those of many other countries, it has—with respect to the topic of this chapter—all the typical elements of an historically grown classification system. Therefore, this case study reveals the fundamental issues that have to be tackled in any system that grants to disabled persons rights and entitlements which are subject to legal recourse.
The twentieth anniversary of the law of 30 June 1975 regarding disabled persons has triggered a renewed interest in the lot of the disabled in France. Estimates of the number of disabled French nationals range from 1.5 to 6 million (equivalent to 10% of the population), although these estimates suffer from a lack of precision in the definition of disability. This population is all too often relegated to the margins of society, and despite progress over the last two decades, their condition remains a serious societal problem with painful human, moral and emotional ramifications that transcend collective considerations of national solidarity.
Under French law, disabled persons enjoy the same rights and freedoms as other citizens, and are guaranteed equality of opportunity and treatment. Unless specific support mechanisms are implemented, this equality is, however, purely theoretical: disabled individuals may, for example, require specialized transportation and city planning to allow them to come and go as freely as other citizens. Measures such as these, which allow disabled persons to enjoy equal treatment in fact, are designed not to confer privilege, but to remove disadvantages associated with disability. These include legislation and other state-initiated measures that guarantee equitable treatment in education, training, employment and housing. Equality of treatment and palliation of the disability constitute the prime objectives of social policy concerning disabled persons.
In most cases, however, the various measures (usually termed political discriminatory measures) prescribed by French law are not available to all persons suffering from a given disability, but rather to selected subgroups: for example, a specific allowance or programme designed to favour occupational reintegration is available only to a specific category of disabled persons. The variety of disabilities and the multiple contexts in which disability may occur have necessitated the development of classification systems that take into account an individual’s official status as well as his or her level of disability.
Variety of Disabilities and Determination of Official Status
In France, the context in which disabilities arise constitutes the fundamental basis for classification. Classifications based on the nature (physical, mental or sensory) and degree of disability are also relevant to the treatment of disabled persons, of course, and are taken into account. These other classification systems are particularly important in determining whether health care or occupational therapy is the best approach, and whether guardianship is appropriate (persons suffering from mental disabilities may become wards of the state). Nevertheless, classification on the basis of the nature of the disability is the primary determinant of a disabled person’s official status, rights and eligibility for benefits.
A review of the body of French law applicable to disabled persons reveals the multiplicity and complexity of support systems. This organizational redundancy has historical origins, but persists to this day and remains problematic.
Development of “official status”
Until the end of the nineteenth century, care of the disabled was essentially a form of “good works” and usually took place in hospices. It was not until the beginning of the twentieth century that the ideas of rehabilitation and income replacement developed against the backdrop of a new cultural and social view of disability. In this view, the disabled were seen as damaged persons who needed to be rehabilitated—if not to the status quo ante, at least to an equivalent situation. This change in mentality was an outgrowth of the development of mechanization and its corollary, occupational accidents, and of the impressive number of First World War veterans suffering permanent disability.
The law of 8 April 1898 improved the occupational-accident compensation system by no longer requiring proof of employer liability and establishing a flat-fee compensation payment system. In 1946, management of the risk associated with occupational accidents and diseases was transferred to the social security system.
Several laws were passed in an attempt to correct prejudices suffered by injured or disabled First World War veterans. These include:
- a 1915 law establishing an occupational retraining system
- a 1916 law (complemented by a 1923 law) giving war invalids first call on public-sector jobs
- the law of 31 March 1918 instituting the right to a fixed pension based on the degree of disability
- the law of 26 April 1924 requiring private-sector companies to employ a specific percentage of war invalids
The interwar period saw the development of the first large-scale associations of civilian disabled persons. The most noteworthy of these are: the Fédération des mutilés du travail (1921), the Ligue pour l’adaptation des diminués physiques au travail (LADAPT) (1929) and the Association des Paralysés de France (APF) (1933). Under pressure from these associations and from unions, victims of work accidents, and eventually all the civilian disabled, progressively benefited from support systems based on those established for war invalids.
A disability insurance system was established for workers in 1930 and reinforced by the 1945 Decree creating the social security system. Under this system, workers receive a pension if their ability to work or earn a livelihood is significantly reduced by disease or accident. The right of victims of occupational accidents to retraining was recognized by a 1930 law. A training and retraining system for the blind was established in 1945 and extended to all seriously disabled persons in 1949. In 1955, the obligation to hire a minimum percentage of war invalids was extended to other disabled persons.
The development of the concept of occupational integration led to the promulgation of three laws which improved and reinforced existing support systems: the law of 27 November 1957 concerning occupational reclassification of disabled workers, the law of 30 June 1975 concerning disabled persons (the first to adopt a global approach to the problems faced by disabled persons, especially that of social reintegration), and the law of 10July 1987 favouring the employment of disabled workers. However, these laws in no way eliminated the specific dispositions of the systems responsible for war invalids and the victims of occupational accidents.
Multiplicity and diversity of regimes supporting disabled persons
Today, there are three quite distinct regimes providing support to disabled persons: one for war invalids, one for victims of occupational accidents, and the common-law system, which deals with all other disabled persons.
A priori, the coexistence of multiple regimes that select their clientele on the basis of the origin of disability does not appear to be a satisfactory arrangement, especially since each regime provides the same type of support, namely integration-support programmes, particularly those aimed at occupational reintegration, and one or more allowances. Accordingly, there has been a concerted effort to harmonize employment-support systems. For example, the vocational training and medical rehabilitation programmes of all the systems aim as much at distributing costs through society as at providing financial compensation for disability; the specialized training and medical rehabilitation centres, including the centres operated by the Office des anciens combattants (ONAC), are open to all disabled persons, and the reservation of positions in the public sector for war invalids was extended to disabled civilians by the Decree of 16 December 1965.
Finally, the law of 10 July 1987 united the private- and public-sector minimum-employment programmes. Not only were the conditions of these programmes extremely complex to apply, but they also differed depending on whether the individual was a disabled civilian (in which case the common law system applied) or a war invalid. With the coming into force of this law, however, the following groups are entitled to consideration for minimum-employment programmes: disabled workers recognized by the Commission technique d’orientation et de réinsertion professionnelle (COTOREP), victims of occupational accidents and diseases receiving a pension and suffering from a permanent disability of at least 10%, recipients of civilian disability allowances, former members of the armed forces and other recipients of military disability allowances. COTOREP is responsible, under the common law system, for the recognition of disabled status.
On the other hand, the actual allowances provided by the three regimes differ widely. Disabled persons benefiting from the common-law system receive what is essentially a disability pension from the social security system and a complementary allowance to bring their total benefit up to the adult disabled pension level (as of 1July 1995) of FF 3,322 per month. The amount of the state pension received by war invalids depends on the degree of disability. Finally, the monthly amount (or a lump-sum payment if the permanent disability is below 10%) received by victims of occupational accidents and diseases from the social security system depends on the recipient’s degree of disability and previous salary.
The eligibility criteria and amounts of these allowances are entirely different in each system. This leads to significant differences in the way individuals with disabilities of different organs are treated, and to anxiety that may interfere with rehabilitation and social integration (Bing and Levy 1978).
Following numerous calls for the harmonization, if not unification, of the various disability allowances (Bing and Levy 1978), the Government established a task force in 1985 to study solutions to this problem. To date, however, no solution has been forthcoming, in part because the different goals of the allowances constitute a serious obstacle to their unification. Common-law allowances are subsistence allowances—they are intended to allow recipients to maintain a decent standard of living. In contrast, the war disability pensions are intended to compensate for disabilities acquired while in national service, and allowances paid to victims of occupational accidents and diseases are intended to compensate for disabilities acquired while earning a living. These last two allowances are therefore generally significantly higher, for a given level of disability, than those received by individuals with disabilities that are either congenital or resulting from non-military, non-occupational accidents or illnesses.
Effect of Official Status on Assessments of the Degree of Disability
Different disability-compensation regimes have evolved over time. This diversity is reflected not only in the different allowances each pays to disabled persons but also in each system’s eligibility criteria and system for evaluating the degree of disability.
In all cases, eligibility for compensation and evaluation of the extent of disability is established by an ad hoc committee. Recognition of disability requires more than a simple declaration by the applicant—applicants are required to testify before the commission if they desire to be granted official status as a disabled person and receive eligible benefits. Some people may find this procedure dehumanizing and counter to the goal of integration, since individuals who do not wish to have their differences “officialized” and refuse, for example, to appear before the COTOREP, will not be granted official disabled-person status and will thus be ineligible for occupational reintegration programmes.
Disability eligibility criteria
Each of the three regimes relies on a different set of criteria to determine whether an individual is entitled to receive disability benefits.
Common-law regime
The common-law regime pays disabled persons subsistence allowances (including the adult disability allowance, a compensatory allowance, and the educational allowance for disabled children), to allow them to remain independent. Applicants must suffer from a serious permanent disability—an 80% disability is required in the majority of cases—to receive these allowances, although a lower level of disability (of the order of 50 to 80%) is required in the case of a child attending a specialized institute or receiving special education or home care. In all cases, the degree of disability is evaluated by reference to an official disability scale contained in Appendix 4 of the Decree of 4 November 1993 concerning the payment of various allowances to disabled persons.
Different eligibility criteria apply to applicants for disability insurance, which, like the common-law allowances, includes a subsistence component. To qualify for this pension, applicants must be receiving social security and must suffer from a disability that reduces their earning capacity by at least two thirds, that is, that prevents them from earning, in any occupation, a salary greater than one third of their pre-disability salary. The pre-disability salary is calculated on the basis of the salary of comparable workers in the same region.
There are no official criteria for the determination of eligibility, which instead is based on the individual’s overall situation. “The degree of disability is evaluated on the basis of residual fitness for work, overall condition, age, physical and mental faculties, aptitudes, and occupational training”, according to the social security law.
As this definition makes clear, disability is considered to include the inability to earn a living in general, rather than being limited to physical disability or the inability to exercise a given occupation, and is evaluated on the basis of factors likely to affect the occupational reclassification of the individual. These factors include:
- the nature and severity of the disability, and the applicant’s age, physical and mental faculties, aptitudes, occupational training and previous occupation
- the applicant’s residual fitness for work relative to the workforce in his or her region of residence.
To be eligible for specific occupational reintegration programmes, disabled adults must satisfy the following legal criterion: “a disabled worker is any person whose ability to obtain or maintain a job is reduced in fact as a result of inadequate or reduced physical or mental capacities”.
This definition was greatly influenced by the Vocational Rehabilitation of the Disabled Recommendation, 1955 (No. 99) (ILO 1955), which defines a disabled person as “an individual whose prospects of securing and retaining suitable employment are substantially reduced as a result of physical or mental impairment”.
This pragmatic approach nevertheless leaves room for interpretation: what does “in fact” mean? What is the standard to be used in determining whether fitness for work is “inadequate” or “reduced”? The absence of clear guidelines in these matters has resulted in widely divergent evaluations of occupational disability by different commissions.
Specific regimes
To accomplish their primary goal of reparation and compensation, these regimes pay the following allowances and pensions:
- War disability pensions are based on the degree of purely physical disability, as evaluated by experts. Permanent disabilities of at least 10 and 30% are generally required for injuries and diseases, respectively. The degree of disability is evaluated using the official disability scale (Decree of 29 May 1919).
- In the occupational accident system, victims of occupational accidents and diseases suffering from a permanent disability receive either a lump-sum payment or an allowance.
The degree of permanent disability is established using an official disability scale that takes into account the nature of the disability, and the applicant’s general condition, physical and mental faculties, aptitudes and occupational qualifications.
Disability evaluation scales
While eligibility for each regime’s benefits depends on administrative decisions, the medical evaluation of disability, established through examination or consultation, remains critically important.
There are two approaches to the medical evaluation of the degree of disability, one involving the calculation of compensation on the basis of the degree of permanent partial disability, the other based on the reduction in fitness for work.
The first system is used by the war disability system, while the occupational accident and common-law systems require the examination of the applicant by the COTOREP.
The degree of permanent partial disability in war invalids is established using standards contained in the official disability scale applicable to cases covered by the Code des pensions militaires d’invalidité et victimes de guerre (updated 1 August 1977 and including the scales of 1915 and 1919). For the victims of occupational accidents, a scale of occupational accidents and diseases established in 1939 and revised in 1995 is used.
The classification systems used in these two regimes are organ- and function-specific (such as blindness, renal failure, cardiac failure) and establish a level of permanent partial disability for each type of disability. Several possible classification systems for mental disability are suggested, but all of them are imprecise for these purposes. It should be noted that these systems, apart from their other weaknesses, may assess different levels of permanent partial disability for a given disability. Thus, a 30% reduction of bilateral visual acuity is equivalent to a permanent partial disability rating of 3% in the occupational-accident system and 19.5% in the war- disability system, while a 50% loss is equivalent to permanent partial disabilities of 10 and 32.5%, respectively.
Until recently, the COTOREP used the disability scale established in the Code des pensions militaires d’invalidité et victimes de guerre to determine compensation and benefits such as disability cards, adult disability allowances, and third-party compensatory allowances. This scale, developed to ensure fair compensation for war injuries, is not well suited to other uses, especially to birth rate. The absence of a common reference has meant that different sittings of the COTOREP have arrived at significantly different conclusions concerning the degree of disability, which has created serious inequities in the treatment of disabled persons.
To remedy this situation, a new scale of deficiencies and disabilities, which reflects a new approach to disability, came into force on 1 December 1993 (Appendix to Decree No.93-1216 of 4 November 1993, Journal Officiel of 6 November 1993). The methodological guide is based on concepts proposed by the WHO, namely impairment, disability and handicap, and is used primarily to measure disability in family, school and occupational life, regardless of the specific medical diagnosis. While the medical diagnosis is a critical predictor of the condition’s evolution and the most effective case management strategy, it nevertheless is of limited usefulness for the purposes of establishing the degree of disability.
With one exception, these scales are meant to be only indicative: their use is mandatory for the evaluation of permanent partial disability in recipients of military pensions who have suffered amputation or organ resection. Several other factors affect the evaluation of the degree of disability. In occupational accident victims; for example, the establishment of the degree of permanent partial disability must also take into account medical factors (general condition, nature of the disability, age, mental and physical faculties) and social factors (aptitudes and occupational qualifications). The inclusion of other factors allows physicians to fine-tune their evaluation of the degree of permanent partial disability to take into account therapeutic advances and the potential for rehabilitation, and to counteract the rigidity of the scales, which are rarely updated or revised.
The second system, based on the loss of working capacity, raises other questions. The reduction in working capacity may need to be evaluated for different purposes: evaluation of the reduction in working capacity for the purposes of disability insurance, recognition of the loss of working capacity by COTOREP, evaluation of an occupational deficit for the purposes of recognizing a worker as disabled or placing such a worker in a special workshop.
No standards can exist for the evaluation of the loss of working capacity, since the “average worker” is a theoretical construct. In fact, the whole field of working capacity is poorly defined, as it relies not only on an individual’s inherent aptitudes but also on the needs and adequacy of the occupational environment. This dichotomy illustrates the distinction between the capacity at work and the capacity for work. Schematically, two situations are possible.
In the first case, the degree of the loss of working capacity relative to the applicant’s recent and specific occupational situation must be objectively established.
In the second case, the loss of working capacity must be evaluated in disabled persons who are either not currently in the workforce (e.g., individuals with chronic illnesses who have not worked for a long time) or who have never been in the workforce. This last case is frequently encountered when establishing adult disability pensions, and eloquently illustrates the difficulties that physicians responsible for quantifying the loss of working capacity are faced with. Under these circumstances, physicians often refer, either consciously or unconsciously, to degrees of permanent partial disability for establishing working capacity.
Despite the obvious imperfections of this disability-evaluation system and the occasional medico-administrative contortions it imposes, it nevertheless allows the level of disability compensation to be established in most cases.
It is clear that the French system, involving official classification of disabled persons on the basis of the origin of their disability, is problematic on several levels under the best of circumstances. The case of individuals suffering from disabilities of different origins and who are therefore ascribed multiple official statuses is even more complex. Consider for example the case of a person suffering from a congenital motor disability who suffers an occupational accident: the problems associated with the resolution of this situation can easily be imagined.
Because of the historical origins of the various official statuses, it is unlikely that the regimes can ever be made completely uniform. On the other hand, continued harmonization of the regimes, especially their systems for the evaluation of disability for the purpose of the awarding of financial compensation, is highly desirable.
Social Policy and Human Rights: Concepts of Disability
Most persons with disabilities who are of working age can and want to work, yet they often encounter major obstacles in their quest for access to and equality in the workplace. This article highlights the principal issues concerning the inclusion of persons with disabilities in the world of work, with reference to social policy and human rights concepts.
First, the overall extent and consequences of disability, as well as the extent to which disabled persons have traditionally been excluded from full participation in both social and economic life, will be described. Human rights concepts will then be presented in terms of a process to overcome the obstacles to equitable employment faced by persons with disabilities. Such obstacles to full participation in the workplace and national life are often due to attitudinal and discriminatory barriers, rather than to causes relating to one’s disability. The end result is that persons with disabilities often experience discrimination, which is either deliberate or is a result of inherent or structural barriers in the environment.
Finally, a discussion of discrimination leads to a description of ways in which such treatment may be overcome through equitable treatment, workplace accommodation and accessibility.
Extent and Consequences of Disability
Any discussion of social policy and human rights concepts about disability must begin with an overview of the global situation persons with disabilities face.
The exact extent of disability is subject to wide interpretation, depending upon the definition used. The United Nations Disability Statistics Compendium (1990) (also referred to as the DISTAT Compendium) reports results of 63 surveys of disability in 55 countries. It notes that the percentage of disabled persons is between 0.2% (Peru) and 20.9% (Austria). During the 1980s, approximately 80% of disabled persons lived in the developing world; due to malnutrition, and disease, disabled persons form approximately 20% of the population of these nations. It is not possible to compare the percentage of the population that is disabled as reflected in various national surveys, due to the use of different definitions. From the overall but limited perspective provided by the DISTAT Compendium, it may be noted that disability is largely a function of age; that it is more prevalent in rural areas; and that it is associated with a higher incidence of poverty and lower economic status and educational attainment. Moreover, statistics consistently show lower labour-force participation rates for persons with disabilities than for the population in general.
With respect to employment. a graphic description of the situation faced by persons with disabilities was given by Shirley Carr, a member of the Governing Body of the ILO and a past president of the Canadian Labour Congress, who noted during a parliamentary forum on disability held in Canada in 1992 that disabled persons experience a “cement ceiling” and that “Disabled persons suffer from the three ‘U’s: under-employment, unemployment and under-utilization”. Unfortunately, the situation persons with disabilities face in most places in the world is at best like what exists in Canada; in many cases, their circumstances are far worse.
Disability and Social Exclusion
For a variety of reasons, many persons with disabilities have historically experienced social and economic isolation. However, since the end of the Second World War, there has been a slow but steady movement away from segregating disabled persons from the general population, and away from the view that “the disabled” need care, philanthropy and charity. Persons with disabilities are increasingly insisting on their right not to be excluded from the workplace but rather to be treated in an inclusive manner, equitable to other, non-disabled members of society, including the right to participate as active members of the economic life of the nation.
Disabled persons should participate fully in the labour force because it makes economic sense for them to have the opportunity to engage in remunerative employment to the fullest extent of their capacities, instead of drawing social assistance. However, disabled persons should first and foremost participate in the mainstream of the labour force and thus national life because it is ethically and morally the correct thing to do. In this regard, one is mindful of the remarks of the UN Special Rapporteur Leandro Despouy, who stated in his report to the Economic and Social Council of the United Nations (1991) that “the treatment given to disabled persons defines the innermost characteristics of a society and highlights the cultural values that sustain it”. He goes on to state what is, unfortunately, not obvious to all, that:
persons with disabilities are human beings—as human as, and usually even more human than, the rest. The daily effort to overcome impediments and discriminatory treatment they regularly receive usually provides them with special personality features, the most obvious and common are integrity, perseverance, and a deep spirit of comprehension in the face of a lack of understanding and intolerance. However, this last feature should not lead us to overlook the fact that as subjects of law they enjoy all the legal attributes inherent in human beings and hold specific rights in addition. In a word, persons with disabilities, as persons like ourselves, have the right to live with us and as we do.
Disability and Societal Attitudes
The issues raised by the UN Special Rapporteur point to the existence of negative societal attitudes and stereotypes as a significant barrier to equitable workplace opportunities for persons with disabilities. Such attitudes include the fear that the cost of accommodating persons with disabilities in the workplace will be too high; that persons with disabilities are not productive; or that other vocational trainees or employees and customers will be uncomfortable in the presence of persons with disabilities. Still other attitudes relate to the assumed weakness or sickness of persons with disabilities and the impact this has on “their” ability to complete a vocational training programme or to succeed in a job. The common element is that they are all founded on assumptions based on one characteristic of a person, the presence of a disability. As noted by the Province of Ontario (Canada) Advisory Council for Disabled Persons (1990):
Assumptions about the needs of persons with disabilities are often premised on notions about what the person cannot do. The disability becomes the characterization of the whole person rather than one aspect of the person.… Incapacity is seen as a generalized condition and tends to incorporate notions of incompetence.
Disability and Empowerment: The Right of Choice
Inherent in the principle that persons with disabilities have the right to participate fully in the mainstream of the social and economic life of the nation is the notion that such individuals should be empowered to exercise free choice as to their vocational training and choice of occupation.
This basic right is set forth in the Human Resources Development Convention, 1975 (No. 142) (ILO 1975), which states that vocational training policies and programmes shall “encourage and enable all persons, on an equal basis and without discrimination whatsoever, to develop and use their capabilities for work in their own best interests and in accordance with their own aspirations”.
Learning to make choices is an intrinsic part of personal development. However, many individuals with disabilities have not been given the opportunity to make meaningful selections concerning their choice of occupational training and placement. Persons with severe disabilities may lack experience in skills needed to identify personal preferences and to make effective choices from a series of options. However, the lack of self-direction and power is not related to impairments or limitations. Rather, as noted above, it is often due to negative attitudes and practices. Often, disabled persons are presented with options that are artificially preselected or restricted. For example, they may be pressured to participate in a vocational training course that happens to be available, without other options being seriously considered. Or the “choices” may merely be the avoidance of undesirable alternatives, such as agreeing to live in a group setting or with roommates not of one’s choice, to avoid even more unpleasant situations, such as having to live in an institution. Unfortunately for many disabled persons, the chance to express a vocational interest, to choose vocational training options or to seek a job is often determined by a person’s disability label and other people’s assumptions about the capabilities of the individual. This lack of choice also frequently stems from a historical attitude that as involuntary users of the social welfare system, “beggars can’t be choosers”.
This issue is of great concern. Research has shown that the degree of influence which individuals have on decisions that affect their working lives has a significant impact on job satisfaction, and hence on the success of integration strategies. Every person, notwithstanding the severity of his or her disabilities, has the right and ability to communicate with others, express everyday preferences, and exercise at least some control over his or her daily life. Inherent in liberty is the right to have freedom of vocational choice, the necessary training based on available technology, and respect for and encouragement to work. For disabled persons at all levels of severity and ability, including those who have intellectual and psychosocial disabilities, making choices is key to establishing one’s identity and individuality. It must also be recalled that it is part of the human experience to make mistakes and to learn from them.
It must be stressed again that disabled persons are human beings. It is a matter of basic respect of human dignity to provide disabled persons with opportunities to make those decisions in life that non-disabled persons routinely make.
Disability and Social Justice: The Issue of Discrimination
Why have negative stereotypes developed and how do they relate to discrimination? Hahn (1984) notes the apparent contradiction between the vast sympathy displayed toward individuals with disabilities and the fact that, as a group, they are subjected to patterns of discrimination more severe than any other recognized minority. This can be explained by the fact that persons with disabilities often display physical and behavioural characteristics that set them apart from the non-disabled population.
Without these identifiable physical differences, disabled persons could not be subjected to the same processes of stereotyping, stigmatizing, bias, prejudice, discrimination, and segregation that plague every minority group. Moreover, when such traits are coupled with adverse social labelling, the effects of discrimination are compounded.
Hahn also suggests that there is a positive correlation between the amount of discrimination experienced by persons with disabilities and the visibility of their disability.
The key, then, for persons with disabilities to attain equitable treatment in society and the workplace is the reduction and elimination of negative attitudes and stereotypes which result in discriminatory behaviour, coupled with the institution of practices and programmes that accommodate the special needs of disabled persons as individuals. The remainder of this article explores these concepts.
What Is Meant by Discrimination?
In the course of our lives, we “discriminate” on a daily basis. Choices are made concerning whether to go to the cinema or the ballet, or whether to buy the more expensive article of clothing. To discriminate in this sense is not problematic. However, discrimination does become troublesome when negative differentiations are made on the basis of immutable characteristics of persons, or groups of persons, such as on the basis of disability.
The International Labour Conference adopted a definition of the discrimination which is contained in the Discrimination (Employment and Occupation) Convention, 1958 (No. 111):
For the purpose of this Convention, the term “discrimination” includes—
(a) any distinction, exclusion or preference made on the basis of race, colour, sex, religion, political opinion, national extraction or social origin, which has the effect of nullifying or impairing equality of opportunity or treatment in employment or occupation;
(b) such other distinction, exclusion or preference which has the effect of nullifying or impairing equality of opportunity or treatment in employment or occupation as may be determined by the Member concerned after consultation with representative employers’ and workers’ organisations, where such exist, and with other appropriate bodies.
Three Forms of Discrimination
The above-noted definition is best understood in light of the three forms of discrimination that have arisen since the end of the Second World War. The following three approaches, first conceptualized in the United States, have now received widespread acceptance in many countries.
Evil motive or animus
Initially, discrimination was seen strictly in terms of prejudicial treatment, that is, harmful acts motivated by personal antipathy towards the group of which the target person was a member. These acts consisted of deliberate denials of employment opportunities. It was necessary to prove not only the act of denial, but also a motive based on prejudice. In other words the definition was based upon the evil-motive, mens rea, or state-of-mind test. An example of such discrimination would be an employer indicating to a disabled person that he or she would not be hired because of fear of negative customer reaction.
Differential treatment
During the 1950s and in the mid-1960s after the passage of the Civil Rights Act, agencies in the United States came to apply what is called the “equal protection” concept of discrimination. In this approach discrimination was seen to cause economic harm “by treating members of a minority group in a different and less favourable manner than similarly situated members of the majority group” (Pentney 1990). Under the differential treatment approach, the same standards are seen to apply to all employees and applicants without the need to demonstrate discriminatory intent. Discrimination in this context would include requiring disabled employees to undergo a medical examination to receive group health insurance benefits when such examinations are not required for non-disabled employees.
Indirect or adverse effect discrimination
Although the differential treatment model of discrimination mandates that employment policies and practices be equally applied to all, many superficially neutral requirements, such as education and testing, had unequal effects on various groups. In 1971, the United States Supreme Court dealt with this issue by articulating a third definition of employment discrimination in the famous case Griggs vs. Duke Power. Prior to the passage of the Civil Rights Act, Duke Power discriminated against Blacks by restricting them to the low-paying labour department. After passage of the legislation, completion of high school and successful completion of aptitude tests were made prerequisites to transfer out of the labour department. In the candidate catchment area, 34% of Whites but only 12% of Blacks had the necessary education. In addition, while 58% of Whites passed the tests, only 6% of Blacks were successful. These requirements were imposed despite evidence that showed that employees without these qualifications, hired before the policy change, continued to perform satisfactorily. The Supreme Court struck down the educational and test requirements that screened out a greater percentage of blacks, on the grounds that such practices had the consequence of excluding Blacks and because they bore no relationship to job requirements. The intent of the employer was not at issue. Rather, what was important was the effect of the policy or practice. An example of this form of discrimination would be the requirement to pass an oral examination. Such a criterion might have an adverse impact on deaf or orally impaired candidates.
Equal versus Equitable Treatment
The model of adverse impact or indirect discrimination is the most problematic for persons with disabilities. For if disabled persons are treated the same as everyone else, “how can it be discrimination?” Central to an appreciation of this concept is the notion that to treat all people the same is, sometimes, a form of discrimination. This principle was most eloquently put forth by Abella in her report (Canada Royal Commission 1984), when she noted:
Formerly, we thought that equality only meant sameness and that treating persons as equals meant treating everyone the same. We now know that to treat everyone the same may be to offend the notion of equality. Ignoring differences may mean ignoring legitimate needs. It is not fair to use the differences between people as an excuse to exclude them arbitrarily from equitable participation. Equality means nothing if it does not mean that we are of equal worth regardless of the differences in gender, race, ethnicity, or disability. The projected, mythical, and attributed meaning of these differences cannot be permitted to exclude full participation.
To underscore this notion, the term equitable is used increasingly, as opposed to equal treatment.
Disability and the Environment: Accessibility and Workplace Accommodation
Flowing from concepts of adverse impact discrimination and equitable treatment is the idea that in order to treat persons with disabilities in a non-discriminatory manner, it is necessary to ensure that the environment and workplace are accessible, and that efforts have been made to reasonably accommodate the individual workplace requirements of the disabled person. Both concepts are discussed below.
Accessibility
Accessibility does not just mean that a building entrance has been ramped for use by wheelchair users. Rather it requires that persons with disabilities are provided with accessible or alternative transportation systems to allow them to get to work or school; that sidewalk curbs have been lowered; that Braille indications have been added to elevators and buildings; that washrooms are accessible to persons who use wheelchairs; that carpets whose pile density provides an obstacle to wheelchair mobility have been removed; that visually impaired persons are provided with technical aids such as large-print manuals and audiocassettes, and hearing-impaired persons are provided with optical signals, among other measures.
Reasonable workplace accommodation
Equitable treatment also means that attempts should be made to reasonably accommodate the individual needs of disabled persons at the workplace. Reasonable accommodation can be understood as the removal of barriers which prevent persons with disabilities from enjoying equity of opportunity in vocational training and employment. Lepofsky (1992) notes that accommodation is:
tailoring of a work rule, practice, condition or requirement to the specific needs of an individual or group.… An accommodation can include such steps as an exemption of the worker from an existing work requirement or condition applicable to others.… The litmus test of the accommodation’s necessity is whether such a measure is needed to ensure that the worker can fully and equally participate in the workplace.
Actually, the list of possible accommodations is theoretically endless, since each disabled person has specific needs. Moreover, two persons who experience the same or similar disabilities may have quite different accommodation needs. The important thing to recall is that accommodation is based on the needs of an individual, and the person requiring the adjustments should be consulted.
However, it must be recognized that there are circumstances in which, despite the best of intentions, it is not possible to reasonably accommodate persons with disabilities. Accommodation becomes unreasonable or an undue hardship:
- when an individual cannot perform the essential elements of a job, or cannot complete the essential or core elements of the training curriculum
- when to accommodate the individual would result in a risk to health and safety either to the person concerned, or to others, which outweighs the enhancing of equality for disabled persons.
In ascertaining the risks to safety and health, consideration must be given to the willingness of a disabled person to accept the risk that providing the accommodation would engender. For example, it may not be possible for a person who must wear an orthopaedic prosthesis to use safety boots as part of a training programme. If no other safety footwear can be found, the requirement to use the boots should be waived, if the individual is prepared to accept the risk, based on an informed decision. This is known as the doctrine of dignity of risk.
Determination must be made as to whether accommodation poses a serious risk to persons other than the disabled individual, based on the accepted levels of risk tolerated within society.
Assessments of the degree of risk must be made on the basis of objective criteria. Such objective criteria would include existing data, expert opinions and detailed information about the employment or training activity to be undertaken. Impressions or subjective judgements are not acceptable.
Accommodation also is an undue hardship when the costs would substantially adversely affect the financial viability of the employer or training facility. However, many jurisdictions provide funds and grants in order to facilitate modifications that promote the integration of disabled persons.
Disability and Social Policy: Obtaining the Viewpoint of Disabled Persons’ Organizations
As already observed, persons with disabilities should have the inherent right of choice in all aspects of life, including vocational training and occupational placement. This implies, at the level of the individual, consulting with the person concerned as to his or her wishes. Similarly, when policy decisions are made by the social partners (employers’ and workers’ organizations and government), voice must be given to organizations that represent the views of persons with disabilities. Simply put, when considering vocational training and employment policies, persons with disabilities individually and collectively know their needs and how best to meet them.
In addition, it should be recognized that while the terms disability and persons with disabilities are often used generically, individuals who have physical or motor impairments have accommodation and vocational training needs that are different from those of people with intellectual or sensory impairments. For example, while ramped sidewalks are of great benefit to wheelchair users, they may present formidable obstacles to blind people who may not be able to ascertain when they have placed themselves in danger by leaving the sidewalk. Hence, the views of organizations that represent persons with various types of disabilities should be consulted whenever contemplating policy and programme changes.
Additional Guidance Concerning Social Policy and Disability
Several important international documents provide useful guidance on concepts and measures concerning equalization of opportunities for persons with disabilities. These include the following: the United Nations World Programme of Action Concerning Disabled Persons (United Nations 1982), the Vocational Rehabilitation and Employment (Disabled Persons) Convention, 1983 (No.159) (ILO 1983) and the United Nations Standard Rules on the Equalization of Opportunities for Persons with Disabilities (United Nations 1993).
Vocational Rehabilitation and Employment Support Services
As a rule disabled people have far fewer opportunities for occupational integration open to them than does the general population, a situation confirmed by all available data. However, in many countries political initiatives have been developed to improve this situation. Thus we find, for example, legal regulations requiring business enterprises to employ a specific percentage of disabled people, as well as—often in addition to this—financial incentives for employers to hire disabled people. Moreover, recent years have also seen the creation of services in many countries providing support and assistance to disabled people making their way into working life. The following contribution aims to describe these services and their specific tasks in the context of vocational rehabilitation and the integration of disabled people into employment.
We are concerned with services which become active, providing advice and support, during the rehabilitation phase—the preparatory phase prior to the disabled person’s entry into working life. Whereas support services used to limit themselves almost exclusively to this area, modern services have, in view of the continued existence on a global scale of employment problems of the disabled, turned their attention increasingly towards the stages dealing with placement and integration in an enterprise.
The increase in importance achieved by these services for the promotion of occupational integration has come about not least by growing community-based rehabilitation activities and, from a practical viewpoint, ever more numerous and successful approaches to the social integration of the disabled into the community. The continuing tendency towards the opening and overcoming of care institutions as mere places of confinement for disabled individuals has made the occupational and employment requirements for this group of people really visible for the first time. We are thus confronted with a growing variety of these support services because the growing demand for the integration of all disabled people into the community brings with it an increase in the associated tasks.
Rehabilitation and Integration
Only when disabled people are integrated into the community is the real aim and purpose of rehabilitation actually achieved. The objective of vocational rehabilitation programmes thus ultimately remains the finding of a job and hence participation in the local labour market.
As a rule, measures for medical and vocational rehabilitation lay the foundations for the (re)integration of disabled persons into working life. They aim to put the disabled individual in a position to be able to develop his or her own abilities in such a way that a life with no, or with a minimum of limitations in society at large becomes possible. The services which are active in this phase and which accompany the disabled person during this process are termed rehabilitation support services. Whereas one used to be able to assume that a completed course of medical rehabilitation and a well-founded vocational rehabilitation were, if not guarantees, then at least key factors for occupational integration, these elementary conditions are no longer adequate in view of the changing situation on the labour market and the complex requirements of the workplace. Of course solid vocational qualifications still form the basis of occupational integration, yet under today’s conditions many disabled people require additional assistance in looking for work and in integration into the workplace. The services active during this phase can be summarized under the name employment support services.
Whereas medical and vocational rehabilitation measures take as their primary point of departure the disabled persons themselves, and attempt to develop their functional capacities and vocational skills, the main emphasis of the employment support services lies on the side of the working environment and hence on the adaptation of the environment to the requirements of the disabled individual.
General Perspectives for Vocational Integration
In spite of the importance of the support services it should never be forgotten that rehabilitation should never, in any phase, be a merely passive form of treatment, but a process actively directed by the disabled person. Diagnosis, counselling, therapy and other forms of support can at best be an aid in the pursuit of self-defined objectives. Ideally the task of these services is still to outline the various options for action available, options which disabled people should ultimately decide for themselves, as far as possible.
Another no less significant parameter for occupational integration is to be seen in the holistic character which should be a hallmark of this process. That means that rehabilitation should be comprehensive and not just deal with the overcoming of impairment. It should involve the whole person and provide him or her with support in finding a new identity or in coping with the social consequences of disability. The rehabilitation of disabled people is in many cases far more than a process of physical stabilization and the extension of skills; if the course of rehabilitation is to run successfully and satisfactorily it must also be a process of psychosocial stabilization, identity formation and integration into everyday social relationships.
An important area of work for support services, and one which is unfortunately all too often ignored, is the field of the prevention of serious disabilities. For working life in particular it is crucial that rehabilitation and employment services are open not just to people who are already disabled but also to those who are threatened by disability. The earlier the reaction to a commencing disability, the sooner that steps towards occupational reorientation can be taken, and the earlier that serious disabilities can be avoided.
These general perspectives for vocational rehabilitation also provide an outline of the essential tasks and parameters for the work of the support services. Furthermore, it should also be clear that the complex tasks described here can best be fulfilled by the interdisciplinary collaboration of experts from various professions. Modern rehabilitation can thus be seen as cooperation between the disabled person and a team of professional trainers as well as qualified medical, technical, psychological and educational personnel.
Medical Rehabilitation
Medical rehabilitation measures usually take place in hospitals or in special rehabilitation clinics. The task of the support services in this phase consists of initiating first steps towards coping psychologically with a disability which has been suffered. However, occupational (re)orientation should also take place as soon as possible, practically at the patient’s bedside, since the construction of a new vocational perspective often helps to lay decisive motivational foundations which can also facilitate the medical rehabilitation process. Other measures such as motor and sensory training programmes, physiotherapy, movement and occupational or speech therapy can also contribute during this phase towards accelerating the natural regenerative process and reducing or avoiding the creation of dependencies.
The decision concerning the vocational perspectives of a disabled person should under no circumstances be taken from a purely medical point of view by a doctor, as is unfortunately still often the case in practice. The basis of any decision on the vocational future of a disabled person should be formed not just by deficits which can be medically diagnosed but rather by existing abilities and skills. The rehabilitation support services should therefore undertake together with the disabled person an extensive review of the client’s vocational background and an inventory of potential abilities and existing interests. Building on this an individual rehabilitation plan should then be drawn up which takes into account the potentialities, interests and requirements of the disabled person as well as the potential resources in his or her social environment.
A further area of work for the rehabilitation support services in this phase lies in the counselling of the disabled person with regard to any technical assistance, equipment, wheelchairs, artificial limbs, and so on which may be required. Use of this kind of technical assistance may at first be accompanied by rejection and refusal. Should a disabled person fail to receive the proper support and instruction during this initial phase, he or she may run the risk of the initial rejection escalating into a phobia which may later make it difficult to obtain the full benefit of the apparatus in question. In view of the wide variety of technical assistance nowadays available, the choice of such equipment must be made with the greatest care, tailored as far as possible to the individual needs of the disabled person. Ideally the selection of technical equipment required should also take into account both the disabled person’s vocational perspective and—as far as possible—the demands of the future workplace, given that the latter will also determine the purpose which the technical assistance must fulfil.
Vocational Rehabilitation
In the ILO “Convention (159) concerning vocational rehabilitation and employment (disabled persons)” adopted in 1983, the purpose of vocational rehabilitation is considered “as being to enable a disabled person to secure, retain and advance in suitable employment and thereby to further such person’s integration or reintegration into society”.
The past 30 years have seen rapid developments in vocational rehabilitation services for disabled persons. They include vocational assessment, which aims to get a clear picture of the person’s potential abilities; orientation courses to help the person to restore lost confidence in his or her abilities; vocational guidance, to develop a (new) vocational perspective and to choose a certain occupation; vocational training and retraining opportunities in the chosen field of activity; and placement services, designed to assist the disabled person in finding employment adapted to his or her disability.
A disabled person’s (re)entry into employment usually takes place via individual or combined vocational rehabilitation programmes, which can be carried out in different locations. It is the task of the rehabilitation support services to discuss with the disabled person whether the vocational qualification measure should be carried out in a mainstream institution for vocational training, in a specialized institution for vocational rehabilitation, by making use of community-based facilities or even directly in a normal workplace. The latter option is especially suitable when the previous job is still available and the workplace management have demonstrated their readiness in principle to rehire their former employee. However, in other cases cooperation with a regular workplace may already be a recommended option during the course of the vocational training, given that experience has shown that such cooperation also improves the chances of the participant subsequently being taken on by the firm. Thus in the case of vocational training in a vocational rehabilitation centre, it goes without saying that the support services should undertake the task of assisting disabled people in the search for possibilities of on-the-job practical training.
Of course these options for carrying out vocational rehabilitation measures cannot be seen separately from certain parameters and conditions which vary from country to country. Furthermore, the actual decision on the location of the vocational rehabilitation activity also depends on the kind of work envisaged and the type of disability, as well as on the disabled person’s social environment and the natural support potential available within it.
Wherever vocational rehabilitation takes place, it remains the task of the rehabilitation support services to accompany this process, to discuss together with the disabled person the experiences gained and to further extend the individual rehabilitation plan, adapting it to new developments as necessary.
Employment Support Services
Whereas medical and vocational rehabilitation in many countries can count on the support of a more or less extensive system of institutional settings, a comparable infrastructure for the promotion of the integration of disabled people into employment does not as yet exist even in some highly industrialized countries. And although various countries do have a number of quite successful models, some of which have been in existence for a number of years, employment services in most countries, with the exception of certain approaches in Australia, the United States, New Zealand and Germany, still do not form an integral part of national policy for disabled persons.
While the placement of disabled people into employment is an obligatory part of general labour administration in many countries, in view of the growing number of unemployed these institutions are less and less in a position to fulfil their obligations to place disabled people in work. This is exacerbated in many cases by a lack of appropriately qualified staff capable of doing justice to the abilities and wishes of the disabled person as well as to the requirements of the world of work. The creation of employment support services is also a reaction to the increasing lack of success of the traditional “train and place” approach implicit in institutionalized vocational rehabilitation. In spite of elaborate and often successful medical and vocational rehabilitation measures, integration into employment without additional assistance is becoming increasingly difficult.
It is at this point that the requirement for specific employment support services expresses itself. Wherever such services have been installed, they have been met by enormous demand from disabled persons and their families. This kind of service is particularly necessary and successful at the institutional interfaces between schools, rehabilitation institutions, sheltered workshops and other facilities for disabled persons on the one hand and the workplace on the other. However, the existence of employment support services also reflects the experience that many disabled people also require support and accompaniment not just in the phase of placement in employment, but also during the adjustment phase in the workplace. A number of larger firms have their own, internal employee assistance service, responsible for the integration of newly employed disabled people and for maintaining the jobs of disabled workers already employed.
Tasks of Employment Support Services
The primary intervention focus of the employment support services is on the critical threshold of entry into working life. Generally speaking, their task consists of creating links between the disabled person and the firm in question, that is, with the direct superior and future colleagues in the workplace.
Employment support services must on the one hand provide support for the disabled person in finding work. This takes place by means of self-confidence and (video supported) job interview training and assistance in the writing of letters of application, but also and primarily in placement in on-the-job practical training. All experiences have shown that such practical on-the-job training forms the most important bridge into the firm. Where necessary the services accompany the disabled person to job interviews, providing assistance with official paperwork and in the initial adjustment phase in the workplace. Lack of capacity means that most employment support services are unable to provide support beyond the confines of the workplace. However, in theory such support is also undesirable. To the extent that further assistance in the private sphere, whether psychological, medical or life-skills related in nature, is also required, it is usually provided by referral to the appropriately qualified facilities and institutions.
On the other hand, with regard to firms, the most important tasks of the support services consist initially of motivating an employer to take on a disabled person. Although many firms do have broad reservations about employing disabled people, it is still possible to find firms prepared to enter into continual cooperation with vocational rehabilitation facilities and employment support services. Once such a general readiness for cooperation has been identified or established, it is then a case of locating suitable jobs within the firm. Before any placement in the firm, there should of course be a comparison of the requirements of the job with the abilities of the disabled person. However, the time and energy occasionally spent in model projects which use supposedly “objective” procedures to compare differentiated ability and requirement profiles in order to work out the “optimal” job for a specific disabled person, usually bears no relation to the chances of success and the practical efforts involved in actually finding the job. It is more important to turn disabled persons into the agents of their own vocational development, since in terms of psychological significance we cannot place too high a value on the involvement of the persons concerned in the shaping of their own vocational future.
Placement approaches already elaborated attempt to build on detailed analyses of organizational structure and working procedure by making suggestions to the firm regarding the reorganization of certain working areas and hence to create work opportunities for disabled people. Such suggestions can include a reduction in certain working requirements, the creation of part-time work and flexible work times as well as the reduction of noise and stress in the workplace.
Employment support services also offer to assist firms in applying for public subsidies, such as wage subsidies, or in overcoming bureaucratic hurdles when applying for state grants for technical compensation for disability-related limitations. However, support for the disabled person in the workplace must not necessarily be only of a technical nature: people with visual impairment may under certain circumstances require not only a Braille keyboard for their computer and an appropriate printer, but also someone to read aloud for them; and persons with hearing impairment could be assisted through a sign-language interpreter. Sometimes support in acquiring the qualifications required for the job or in social integration into the firm will be necessary. These and other similar tasks are often undertaken by an employment support services worker designated as a “job coach”. The individualized support provided by the job coach decreases over time.
People with mental or psychiatric disabilities usually require a step-by-step integration with a gradual increase in work requirements, working hours and social contact, which has to be organized by the support services in cooperation with the firm and the disabled person.
For every form of support the maxim applies that it must be tailored to the individual requirements of the disabled person as well as harmonized with the firm’s own resources.
The Example of Supported Employment
Supported employment for persons with disabilities is a concept in which wage subsidies for the firms involved and individualized support services for disabled persons are connected with each other in order to achieve full integration into working life. This concept is particularly widespread in Australia and New Zealand, in various European countries and in the United States. It has so far primarily been used for the workplace integration of mentally and psychiatrically disabled people.
Employment support services undertake the placement of disabled people in a firm, organize the financial, technical and organizational support required by the firm and provide a job coach who accompanies the job-related and social integration of the disabled person into the firm.
The employer is thus relieved of all normally anticipated problems related to the hiring of disabled persons. As far as possible and necessary, the employment support services also undertake the required adaptations in the workplace and the disabled person’s immediate working environment. Occasionally it will be necessary for the applicant to receive additional training outside the firm, although instruction usually takes the form of on-the-job training by the job coach. It is also the job coach’s task to orient the colleagues and superiors in the technical and social support of the disabled person, since the aim in principle is to gradually reduce the professional assistance of the employment support service. It is, however, absolutely necessary that in the case of acute problems the employment support service should be present to provide continual assistance to the extent required. This means that support both for the disabled person and for the employer, the superior and colleagues, must be individualized and correspond to specific needs.
Cost-benefit analyses of this approach carried out in the United States have shown that although the initial integration phase is very intensive in terms of support provided and hence costs, the longer employment lasts, the more this investment is also justified from a financial point of view, not just for the disabled person, but also for the employer and the public budget.
Placement of disabled people by supported employment approaches is most common in relatively undemanding jobs, which tend to run the risk of being eliminated. The future of the supported employment approach will be decided not just by developments in the labour market but also by the further development of the concept.
Challenges for the Future of Employment Support Services
The following sections contain descriptions of a number of critical points whose significance for the further development of the concepts and for the practical work of employment support services should not be underestimated.
Networking with Vocational Rehabilitation Facilities and Firms
If employment support services are not to miss the mark in terms of what is actually required, a central task everywhere will be to create organic links with the existing vocational rehabilitation facilities. Integration services with no links to rehabilitation facilities run the risk—as experience has shown—of functioning primarily as instruments of selection and less as services for the vocational integration of disabled persons.
However, support services require not only networking and cooperation with vocational rehabilitation facilities, but also and more importantly, a clear positioning with regard to cooperation with firms. Under no circumstances should employment support services function merely as counselling services for disabled persons and their families; they must also be active in work-finding and placement services. Proximity to the labour market is the key to access to firms and ultimately to the possibilities of finding employment for disabled individuals. If these services’ access threshold to the firm is to be maximized, they must be situated as close as possible to actual economic activity.
Connections Between Qualification, Placement and Employment
An important part of all vocational integration efforts, and hence a central challenge for employment support services, is the coordination of vocational preparation and qualification with the requirements of the workplace—an aspect often still neglected. As justified as a criticism of the traditional “train and place” model may be, in practice just to first place and then provide training in the required skills is not enough either. Working under today’s conditions means not only having the so-called secondary working virtues at one’s disposal—punctuality, concentration and speed—but also a number of technical qualifications which are always required and which must already be present before employment can be started. Anything else would be asking too much, both of the persons to be placed and of the firms prepared to take them on.
Mobilizing Natural Support
The chances of the successful vocational integration of disabled people into the labour market increase with the possibility of organizing help and support, either in parallel to the work process or directly in the workplace. Especially in the initial adjustment phase it is important both to assist the disabled person in coping with the demands of work and also to provide support for those who make up the working environment. This form of accompanying assistance is usually provided by the employment support services. The integration of a disabled person will be all the more successful in the long term, the more this kind of professional help can be replaced by a mobilization of natural support in the firm, whether by colleagues or superiors. In a project recently carried out in Germany for the mobilization of natural support by so-called foster workers in the workplace, 42 disabled people were successfully integrated in the course of 24 months; over 100 firms were asked to participate. The project showed that few employees had the required level of knowledge and experience in dealing with disabled people. It thus appeared to be of strategic importance for the employment services to develop a conceptual framework in order to organize the replacement of professional support and the mobilization of natural support in the workplace. In the UK for example, employees prepared to act as foster workers for a certain time receive recognition in the form of a small financial reward.
Success Orientation and User Control
Finally, employment support services should also offer their own employees incentives to go into firms and bring about the placement of disabled people, for it is on these placement efforts within the firms that the central focus of the services must lie. Yet the placement of disabled people can be secured in the long term only when the funding of the employment support services and their employees is to a certain extent related to their success. How can service employees be motivated in a continual way to leave their institution, only to undergo the frustration of rejection in the firms? The placement of disabled people in employment is a difficult business. Where is the impetus to come from to battle doggedly and constantly against prejudice? All organizations develop their own interests, which are not necessarily in accord with those of their clients; all publicly funded institutions run the risk of becoming divorced from the needs of their clients. For this reason a corrective is required which creates general incentives—not just for employment support services but also for other social facilities—in the direction of the desired result.
A further necessary modification of the work of publicly funded social facilities consists of the users and their organizations having a say in matters relating to them. This culture of participation should also find an echo in the concepts behind the support services. In this context the services, like all other publicly funded institutions, should be subjected to regular control and evaluation by their clients—their users and their families—and last but not least by the firms cooperating with the services.
Concluding Remarks
Which and how many disabled persons can ultimately be integrated into the labour market by the activities of vocational rehabilitation and employment support services cannot be answered in the abstract. Experience shows that neither the degree of disability nor the situation on the labour market can be regarded as absolute limitations. The factors determining development in practice include not just the support services’ way of working and the situation on the job market, but also the dynamics arising within institutions and facilities for disabled persons, when this kind of employment option becomes a concrete possibility. In any case, experiences from various countries have shown that collaboration between employment support services and sheltered facilities tends to have considerable effect on the internal practices within these facilities.
People need perspectives, and motivation and development arise to the extent that perspectives exist or are created by new options. Important as the absolute number of placements realized by the employment support services is, of equal importance is the opening up of options for the personal development of disabled people made possible by the very existence of such services.
Disability Management at the Workplace: Overview and Future Trends
* Portions of this article have been adapted from Shrey and Lacerte (1995) and Shrey (1995).
Employers are faced with increasing societal and legislative pressure to integrate and accommodate people with disabilities. Increasing workers’ compensation and health care costs are threatening the survival of business and draining resources otherwise allocated to future economic development. Trends suggest that employers can be successful in the effective management of injury and disability problems. Impressive disability management programme models are prominent among employers that assume control and responsibility for injury prevention, early intervention, injured worker reintegration and worksite accommodation. Current disability management practice in industry reflects a paradigm shift from services provided in the community to interventions occurring at the worksite.
This article offers an operational definition of disability management. A model is presented to illustrate the structural components of an optimal worksite-based disability management programme. Effective disability management strategies and interventions are outlined, including key organizational concepts that strengthen service delivery and successful outcome. This article also includes a focus on joint labour-management collaboration and the use of interdisciplinary services, which are considered by many to be essential to the implementation of optimal disability management programmes in industry. Promoting respect and dignity between workers with disabilities and the professionals who serve them is emphasized.
Definition of Disability Management
Disability management is operationally defined as an active process of minimizing the impact of an impairment (resulting from injury, illness or disease) on the individual’s capacity to participate competitively in the work environment (Shrey and Lacerte 1995). The basic principles of disability management are as follows:
- It is a proactive (not passive or reactive) process.
- It is a process that enables labour and management to assume joint responsibility as proactive decision-makers, planners and coordinators of workplace-based interventions and services.
- It promotes disability prevention strategies, rehabilitation treatment concepts, and safe work return programmes designed to control the personal and economic costs of workplace injury and disability.
Successfully managing the consequences of illness, injury and chronic disease in the workforce requires:
- an accurate understanding of the types of injury and illness that occur
- the employer’s timely response to the injury or illness
- clear administrative policies and procedures
- the effective utilization of health care and rehabilitation services.
Disability management practices are based on a comprehensive, cohesive and progressive employer-based approach to managing the complex needs of people with disabilities within a given work and socio-economic environment. Despite rapidly escalating costs of injury and disability, rehabilitation technologies and disability management resources are available to facilitate immediate and recurrent savings among business and industry. Disability management policies, procedures and strategies, when properly integrated within the employer’s organization, provide the infrastructure which enables employers to effectively manage disability and continue to compete in a global environment.
Controlling the cost of disability in business and industry and its ultimate impact on employee productivity is not a simple task. Complex and conflicting relationships exist between employer goals, resources and expectations; the needs and self-interests of workers, health care providers, labour unions and attorneys; and the services available in the community. The ability of the employer to participate actively and effectively in this relationship will contribute to the control of costs, as well as to the protection of the worker’s sustained and productive employment.
Disability Management Objectives
Employer policy and procedure, as well as disability management strategies and interventions, should be designed to accomplish realistic and attainable objectives. Disability management programmes at the worksite should enable the employer to:
- facilitate control of disability issues
- improve corporate competitiveness
- reduce work disruptions and unacceptable lost time
- decrease incidence of accidents and magnitude of disability
- reduce illness and disability duration (and costs)
- promote early involvement and preventive interventions
- maximize use of internal (employer) resources
- improve coordination and accountability, with respect to external service providers
- reduce human cost of disability
- enhance morale by valuing employee physical and cultural diversity
- protect the employability of the worker
- ensure compliance with reintegration and employer equity legislation (e.g., Americans with Disabilities Act of 1990)
- reduce adversarial nature of disability and litigation
- improve labour relations
- promote joint labour-management collaboration
- facilitate direct worker involvement in planning
Essential Disability Management Conceptsand Strategies
Both labour and management have vested interests in protecting the employability of workers while controlling industry’s injury and disability costs. Labour unions want to protect the employability of the workers they represent. Management wants to avoid costly worker turnover, while retaining productive, reliable and experienced employees. Research suggests that the following concepts and strategies are important when developing and implementing effective worksite-based disability management programmes:
Joint labour-management involvement
Disability management requires employer and union involvement, support and accountability. Both are key contributors in the disability management process, participating actively as decision-makers, planners and coordinators of interventions and services. It is important for both labour and management to assess their joint capacities for responding to injury and disability. This often requires an initial analysis of joint strengths and weaknesses, as well as an assessment of the resources available to properly manage accommodation and return-to-work activities among workers with disabilities. Many unionized employers have successfully developed and implemented on-site disability management programmes under the guidance and support of joint labour- management committees (Bruyere and Shrey 1991).
Corporate culture
Organizational structures, worker attitudes, management intentions and historical precedents contribute to the corporate culture. Prior to developing a disability management programme in industry, it is important to understand the corporate culture, including the motivations and self-interests of labour and management regarding injury prevention, worksite accommodation and injured worker rehabilitation.
Injury and disability patterns
Disability management programmes in industry must be customized to address the unique patterns of injury and disability in the employer’s workforce, including types of impairments, ages of workers, lost-time statistics, accident data and costs associated with disability claims.
Interdisciplinary disability management team
Disability management requires an interdisciplinary disability management team. Members of this team often include employer representatives (e.g., safety managers, occupational health nurses, risk managers, human resources personnel, operations managers), labour union representatives, the worker’s treating physician, a rehabilitation case manager, an onsite physical or occupational therapist and the worker with a disability.
Early intervention
Perhaps the most important principle of disability management is early intervention. Rehabilitation policy and practice among most disability benefit systems recognizes the value of early intervention, in light of compelling empirical evidence resulting from disability management research over the past decade. Employers have substantially reduced disability costs by promoting early intervention concepts, including the systematic monitoring of workers with work restrictions. Early intervention strategies and programmes for an early return to work result in decreased lost time, increased employer productivity and decreased workers’ compensation and disability costs. Whether the disability is work related or not, early intervention is considered to be the primary factor upon which the foundation of medical, psychosocial and vocational rehabilitation is established (Lucas 1987; Pati 1985; Scheer 1990; Wright 1980). However, the successful management of disability also requires early return to work opportunities, accommodations and supports (Shrey and Olshesky 1992; Habeck et al. 1991). Typical early-return-to-work programmes in industry include a combination of disability management interventions, facilitated by an employer-based multidisciplinary team and coordinated by a skilled case manager.
Proactive interventions at individual and work environment levels
Disability management interventions must be directed at both the individual and the work environment. The traditional approach to rehabilitation often ignores the fact that occupational disability may originate as much from environmental barriers as from the worker’s personal traits. Workers dissatisfied with their jobs, supervisor-worker conflicts and poorly designed workstations rank high among the many environmental barriers to disability management. In short, to maximize rehabilitation outcomes among injured workers, an equally balanced focus on the individual and the work environment is needed. Job accommodations, as required under the Americans with Disabilities Act and other employment equity legislation, often expand the range of transitional work options for an injured worker. Redesigned tools, ergonomically correct workstations, adaptive devices, and work-schedule modifications are all effective disability management methods that enable the worker to perform essential job tasks (Gross 1988). These same interventions can be utilized in a preventive manner to identify and redesign jobs which are likely to cause future injuries.
Benefit plan design
Employee benefit plans often reward workers for remaining disabled. One of the strongest negative forces impacting on unacceptable lost time and associated costs is economic disincentives. Benefit plans should not create an economic disincentive to work, but should reward workers who have disabilities for returning to work and remaining healthy and productive.
Return-to-work programmes
There are two basic ways to reduce disability costs in industry: (1)prevent accidents and injuries; and (2) reduce unnecessary lost time. Traditional light duty programmes in industry have been less than fully effective in returning injured workers to their jobs. Employers are increasingly using flexible and creative work return transition options and reasonable accommodations for workers with restrictions. The transitional work approach enables employees with disabilities to return to work before they fully recover from their injuries. Transitional work typically includes a combination of temporary assignment to modified work, physical conditioning, safe work practices education and work adjustment. Reduced lost time through transitional work translates into lower costs. The injured worker is enabled to perform temporary alternative productive work while gradually transitioning back to the original job.
Promotion of positive labour relations
Relationships between workers and work environments are dynamic and complex. Compatible relationships often lead to job satisfaction, enhanced productivity and positive labour relations, all of which are mutually rewarding for the worker and the employer. However, relationships characterized by unresolved conflicts can lead to mutually destructive consequences for workers and employers. Understanding the dynamics of person-environmental interactions in the workplace is an important first step in resolving injury and disability claims. The responsible employer is one that supports positive labour relations and promotes job satisfaction and worker involvement in decision making.
Psychological and social aspects of disability
Employers need to be sensitive to the psychological and social consequences of injury and disability and the overall impact of work disruption on the worker’s family. Psychosocial problems that are secondary to the initial physical injury typically emerge as lost work time increases. Relationships with family members often deteriorate rapidly, under the strain of excessive drinking and learned helplessness. Maladaptive behaviours resulting from work disruption are common. However, when other family members become adversely affected by the consequences of a worker’s injuries, pathological relationships within the family emerge. The disabled worker undergoes role changes. Family members experience “role change reactions”. The once independent, self-supporting worker now takes on a role of passive dependency. Resentment abounds when the family is disrupted by the presence of an ever-demanding, sometimes angry and often depressed individual. This is the typical outcome of unresolved labour relations problems, fuelled by stress and ignited by litigation activity and intense adversarial proceedings. Although the relationship among these forces is not always understood, the damage is usually profound.
Accident prevention and occupational ergonomics programmes
Many employers have experienced significant reductions in accidents by establishing formal safety and ergonomics committees. Such committees are typically responsible for safety surveillance and monitoring risk factors such as exposures to dangerous chemicals and fumes, and establishing controls to reduce the incidence and magnitude of accidents. More frequently, joint labour-management safety and ergonomics committees are addressing problems such as repetitive motion injuries and cumulative trauma disorders (e.g., carpal tunnel syndrome). Ergonomics is the application of technology to assist the human element in manual work. The overall objective of ergonomics is to fit the task to humans in order to enhance their effectiveness in the workplace. This means that ergonomics aims at:
- eliminating or minimizing injuries, strains and sprains
- minimizing fatigue and overexertion
- minimizing absenteeism and labour turnover
- improving quality and quantity of output
- minimizing lost time and costs associated with injuries and accidents
- maximizing safety, efficiency, comfort and productivity.
Ergonomic interventions can be considered preventive as well as rehabilitative. As a preventive approach, it is important to analyse ergonomically jobs that cause injuries and to develop effective ergonomic modifications that prevent future work disabilities. From a rehabilitation viewpoint, ergonomic principles can be applied to the jobsite accommodation process for workers with restrictions. This may involve exerting ergonomic administrative controls (e.g., rest periods, job task rotation, reduced work hours) or by ergonomically engineering the job tasks to eliminate re-injury risk factors (e.g., changing the table height, increasing illumination, repackaging to reduce lift loads).
Employer responsibility, accountability and empowerment
Employer empowerment is a basic principle of disability management. Except for the worker with a disability, the employer is the central figure in the disability management process. It is the employer who takes the first step in initiating early intervention strategies subsequent to an industrial accident and injury. The employer, being intimately familiar with work processes, is in the best position to implement effective safety and injury prevention programmes. Likewise, the employer is best positioned to create work return options for persons with lost-time injuries. Unfortunately, history has revealed that many employers have relinquished control and responsibility for disability management to parties external to the work environment. Decision making and problem solving, as relates to the resolution of work disability, have been assumed by insurance carriers, claims managers, workers’ compensation boards, physicians, therapists, case managers, rehabilitation professionals and even attorneys. It is only when employers become empowered in disability management that the lost-time trends and associated costs of workplace injury are reversed. However, employer empowerment over disability costs does not occur by chance. Not unlike persons with disabilities, employers often become empowered upon recognition of their internal resources and potentials. It is only with a new awareness, confidence and guidance that many employers are able to escape the relentless forces and consequences of workplace disability.
Case management and return-to-work coordination
Case management services are necessary to facilitate the development and implementation of disability management strategies and return-to-work plans for workers with disabilities. The case manager serves as a central disability management team member by functioning as a liaison between employers, labour representatives, injured workers, community health care providers and others. The case manager may facilitate the development, implementation and evaluation of an on-site transitional work or worker retention programme. It may be desirable for an employer to develop and implement such programmes, in order to: (1)prevent work disruptions among employees with medical impairments that effect work performance; and (2) promote a safe and timely return to work among impaired workers on medical leave, workers’ compensation or long-term disability. In the administration of an on-site transitional work programme, the case manager may take on direct rehabilitative responsibilities, such as: (1)objective worker evaluations; (2) classification of the physical job demands; (3) medical surveillance and follow-up; and (4) planning for placement in an acceptable permanent modified-duty option.
Disability management policy and procedure: creating expec-tations among supervisors, labour representatives and workers
It is important for employers to maintain a balance between worker and union expectations and the intentions of managers and supervisors. This requires joint labour-management involvement in the development of formal disability management policies and procedures. Mature disability management programmes have written policy and procedure manuals that include mission statements reflecting the interests and commitments of labour and management. Written procedures often delineate the roles and functions of internal disability management committee members, as well as the step-by-step activities from the point of injury to the safe and timely return to work. Disability management policies often define the relationships between the employer, health care providers and rehabilitation services in the community. A written policy and procedures manual serves as an effective communication vehicle among the various stakeholders, including physicians, insurance carriers, unions, managers, employees and service providers.
Enhancement of physician awareness of jobs and work environments
A universal problem in work injury management involves the lack of employer influence over the physician’s return-to-work determination. Treating physicians are often reluctant to release an injured employee to work with no restrictions prior to a full recovery. Physicians are often asked to make return-to-work judgements without adequate knowledge of the worker’s physical job demands. Disability management programmes have been successful in communicating with doctors regarding the employer’s willingness to accommodate workers with restrictions through transitional work programmes and the availability of temporary alternate duty assignments. It is essential for employers to develop functional job descriptions that quantify the exertional demands of job tasks. These tasks can then be reviewed by the treating physician to make a determination of the compatibility of the worker’s physical abilities and the functional demands of the job. Many employers have adopted the practice of inviting doctors to visit production sites and work areas to increase their familiarity with job demands and work environments.
Selection, utilization and evaluation of community services
Employers have realized substantial savings and improved work return outcomes by identifying, utilizing and evaluating effective medical and rehabilitation services in the community. Workers who become ill or injured are influenced by someone to make treatment provider choices. Poor advice often leads to extended or unnecessary treatment, higher medical costs and inferior results. In effective disability management systems, the employer takes an active role in identifying quality services that are responsive to the needs of workers with disabilities. When the employer “internalizes” these external resources, they become a vital partner in the overall disability management infrastructure. Workers with disabilities can then be guided to responsible service providers that share mutual return-to-work goals.
Utilization of independent medical evaluators
Occasionally an injured worker’s medical report fails to substantiate objectively the worker’s alleged impairments and medical restrictions. Employers often feel that they are held hostage to the treating physician’s opinions, particularly when the doctor’s rationale for determining the employee’s work restrictions are unsubstantiated by objective medical tests and measurable assessments. Employers need to exercise their right to independent medical and/or physical capacity evaluations when evaluating questionable disability claims. This approach requires that the employer take the initiative to explore objective and qualified medical and rehabilitation evaluators in the community.
Essential Components of an Optimal Disability Management System
An employer’s foundation for an optimal disability management system has three major components (Shrey 1995, 1996). First, a worksite-based disability management programme requires a human resource component. A major part of this component is the development of the employer’s internal disability management team. Joint worker-management teams are preferred, and they often include members representing the interests of labour unions, risk management, occupational health and safety, employer operations and financial management. Important criteria for the selection of disability management-team membership may include:
- resourcefulness—familiar with employer’s operations, labour relations, internal/external resources and corporate culture
- influence—able to initiate change within management decision-making process
- leadership—earns respect among workers, supervisors and senior management
- creativity—ability to design proactive interventions that work, despite obstacles
- commitment—professional views that are consistent with disability management mission and principles
- motivation—both self-motivated and able to motivate others towards programme goals and objectives
Gaps often exist with respect to the assignment and delegation of responsibilities for resolving disability problems. New tasks must be assigned to ensure that the steps from injury to work return are properly orchestrated. The human resource component includes knowledge and skill supports or training which enable managers and supervisors to perform their designated roles and functions. Accountability is essential, and it must be built into the organizational structure of the employer’s disability management programme.
The second component of an optimal disability management system is the operations component. This component includes activities, services and interventions which are implemented at the pre-injury, during injury and post-injury levels. Pre-injury operations components include effective safety programmes, ergonomic services, pre-placement screening mechanisms, loss prevention programmes and the development of joint labour-management committees. A strong pre-injury operations component is oriented towards injury prevention, and it may include health promotion and wellness services such as weight loss programmes, smoking cessation groups and aerobic conditioning classes.
The during-injury level of an optimal disability management system includes early intervention strategies, case management services, formalized transitional work programmes, worksite accommodations, employee assistance programmes and other health services. These activities are designed to resolve the disabilities that are not prevented at the pre-injury level.
The post-injury level of an optimal disability management system includes worker retention services. Worker retention services and interventions are designed to facilitate the worker’s adjustment to work performance within the context of the worker’s physical or mental restrictions and environmental demands. The post-injury level of a disability management system should also include programme evaluation, financial management for cost-effectiveness, and programme enhancements.
The third component of an optimal disability management system is the communications component. This includes internal and external communications. Internally, the operational aspects of the employer’s disability management programme must be consistently and accurately communicated among employees, managers, supervisors and labour representatives. The policies, procedures and protocols for return-to-work activities should be communicated through labour and management orientations.
External communications enhance the employer’s relationship with treating physicians, claims managers, rehabilitation service providers and workers’ compensation administrators. The employer can influence an earlier return to work by providing treating physicians with functional job descriptions, job safety procedures and transitional work options for injured workers.
Conclusions
Workplace disability management and transitional work programmes represent a new paradigm in the rehabilitation of workers with illnesses and injuries. Trends reflect a shift in rehabilitative interventions from medical institutions to the worksite. Joint labour-management initiatives in disability management are commonplace, creating new challenges and opportunities for employers, unions and rehabilitation professionals in the community.
The interdisciplinary members of the worksite-based disability management team are learning to harness existing technologies and resources within the work environment. The demands on employers are essentially limited to their creativity, imagination and flexibility to adapt disability management interventions to the work environment. Job accommodations and temporary non-traditional job options expand the range of transitional work alternatives for workers with restrictions. Redesigned tools, ergonomically correct workstations, adaptive devices and work schedule modifications are all effective disability management methods that enable the worker to perform essential job tasks. These same interventions can be utilized in a preventive manner to identify and redesign jobs which are likely to cause future injuries.
Protecting the rights of injured workers is an important component of disability management. Every year thousands of workers become disabled through industrial accidents and occupational diseases. Without transitional work options and accommodations, workers with disabilities risk discrimination similar to that faced by other individuals with disabilities. Thus, disability management is an effective advocate tool, whether advocating for the employer or the person with a disability. Disability management interventions protect the employability of the worker as well as the economic interests of the employer.
The profound impact of rapidly escalating workers’ compensation costs will be experienced worldwide by business and industry throughout the next decade. Just as this crisis offers a challenge to industry, disability management interventions and transitional work programmes create an opportunity. With a decreasing labour pool, an ageing workforce and increased worldwide competition, employers in industrialized societies must seize the opportunities to control the personal and economic costs of injury and disability. An employer’s success will be determined by the extent to which he is able to shape positive attitudes among labour and management representatives, while creating an infrastructure supportive of disability management systems.
Rehabilitation and Noise - Induced Hearing Loss
Raymond Hétu
* This article was written by Dr. Hétu shortly before his untimely death. His colleagues and friends consider it one memoriam to him.
Although this article deals with disability due to noise-exposure and hearing loss, it is included here because it also contains fundamental principles applicable to rehabilitation from disabilities arising from other hazardous exposures.
Psychosocial Aspects of Occupationally Induced Hearing Loss
Like all human experience, hearing loss caused by exposure to workplace noise is given meaning—it is qualitatively experienced and evaluated—by those whom it affects and by their social group. This meaning can, however, be a powerful obstacle to the rehabilitation of individuals suffering from occupationally induced hearing loss (Hétu and Getty 1991b). The chief reasons, as discussed below, are that the victims of hearing loss experience perceptual barriers related to the signs and effects of their deficiency and that the manifestation of overt signs of hearing loss is highly stigmatizing.
Communication problems due to the distorted perception of hearing
Difficulties in hearing and communication resulting from occupationally induced hearing loss are usually attributed to other causes, for example unfavourable conditions for hearing or communication or a lack of attention or interest. This erroneous attribution is observed in both the affected individual and among his or her associates and has multiple, although converging, causes.
- Internal ear injuries are invisible, and victims of this type of injury do not see themselves as physically injured by noise.
- Hearing loss per se progresses very insidiously. The virtually daily auditory fatigue due to workplace noise suffered by exposed workers makes the timely detection of irreversible alterations in hearing function a matter of the greatest difficulty. Individuals exposed to noise are never aware of tangible deteriorations of hearing capacity. In fact, in most workers exposed daily to harmful levels of noise, the increase in the auditory threshold is of the order of one decibel per year of exposure (Hétu, Tran Quoc and Duguay 1990). When hearing loss is symmetric and progressive, the victim has no internal reference against which to judge the induced hearing deficit. As a result of this insidious evolution of hearing loss, individuals undergo a very progressive change of habits, avoiding situations which place them at a disadvantage—without however explicitly associating this change with their hearing problems.
- The signs of hearing loss are very ambiguous and usually take the form of a loss of frequency discrimination, that is, a diminished ability to discriminate between two or more simultaneous acoustic signals, with the more intense signal masking the other(s). Concretely, this takes the form of varying degrees of difficulty in following conversations where reverberation is high or where background noise due to other conversations, televisions, fans, vehicle motors, and so forth, is present. In other words, the hearing capacity of individuals suffering from impaired frequency discrimination is a direct function of the ambient conditions at any given moment. Those with whom the victim comes into daily contact experience this variation in hearing capacity as inconsistent behaviour on the part of the affected individual and reproach him or her in terms like, “You can understand well enough when it suits your purpose”. The affected individual, on the other hand, considers his or her hearing and communication problems to be the result of background noise, inadequate articulation by those addressing him or her, or a lack of attention on their part. In this way, the most characteristic sign of noise-induced hearing loss fails to be recognized for what it is.
- The effects of hearing loss are usually experienced outside of the workplace, within the confines of family life. Consequently, problems are not associated with occupational exposure to noise and are not discussed with work colleagues suffering similar difficulties.
- Acknowledgement of hearing problems is usually triggered by reproaches from the victim’s family and social circles (Hétu, Jones and Getty 1993). Affected individuals violate certain implicit social norms, for example by speaking too loudly, frequently asking others to repeat themselves and turning the volume of televisions or radios up too high. These behaviours elicit the spontaneous—and usually derogatory—question, “Are you deaf?” from those around. The defensive behaviours that this triggers do not favour the acknowledgement of partial deafness.
As a result of the convergence of these five factors, individuals suffering from occupationally induced hearing loss do not recognize the effects of their affliction on their daily lives until the loss is well advanced. Typically, this occurs when they find themselves frequently asking people to repeat themselves (Hétu, Lalonde and Getty 1987). Even at this point, however, victims of occupationally induced hearing loss are very unwilling to acknowledge their hearing loss on account of the stigma associated with deafness.
Stigmatization of the signs of deafness
The reproaches elicited by the signs of hearing loss are a reflection of the extremely negative value construct typically associated with deafness. Workers exhibiting signs of deafness risk being perceived as abnormal, incapable, prematurely old, or handicapped—in short, they risk becoming socially marginalized in the workplace (Hétu, Getty and Waridel 1994). These workers’ negative self-image thus intensifies as their hearing loss progresses. They are obviously reluctant to embrace this image, and by extension, to acknowledge the signs of hearing loss. This leads them to attribute their hearing and communication problems to other factors and to become passive in the face of these factors.
The combined effect of the stigma of deafness and the distorted perception of the signs and effects of hearing loss on rehabilitation is illustrated in figure 1.
Figure 1. Conceptual framework for incapacity from handicap

When hearing problems progress to the point that it is no longer possible to deny or minimize them, individuals attempt to hide the problem. This invariably leads to social withdrawal on the part of the worker and exclusion on the part of the worker’s social group, which ascribes the withdrawal to a lack of interest in communicating rather than to hearing loss. The result of these two reactions is that the affected individual is not offered help or informed of coping strategies. Workers’ dissimulation of their problems may be so successful that family members and colleagues may not even realize the offensive nature of their jokes elicited by the signs of deafness. This situation only exacerbates the stigmatization and its resultant negative effects. As Figure 1 illustrates, the distorted perceptions of the signs and effects of hearing loss and the stigmatization which results from these perceptions are barriers to the resolution of hearing problems. Because affected individuals are already stigmatized, they initially refuse to use hearing aids, which unmistakably advertise deafness and so promote further stigmatization.
The model presented in Figure 1 accounts for the fact that most people suffering occupationally induced hearing loss do not consult audiology clinics, do not request modification of their workstations and do not negotiate enabling strategies with their families and social groups. In other words, they endure their problems passively and avoid situations which advertise their auditory deficit.
Conceptual Framework of Rehabilitation
For rehabilitation to be effective, it is necessary to overcome the obstacles outlined above. Rehabilitative interventions should therefore not be limited to attempts to restore hearing capacity, but should also address issues related to the way hearing problems are perceived by affected individuals and their associates. Because stigmatization of deafness is the greatest obstacle to rehabilitation (Hétu and Getty 1991b; Hétu, Getty and Waridel 1994), it should be the primary focus of any intervention. Effective interventions should therefore include both stigmatized workers and their circles of family, friends, colleagues and others with whom they come into contact, since it is they who stigmatize them and who, out of ignorance, impose impossible expectations on them. Concretely, it is necessary to create an environment which allows affected individuals to break out of their cycle of passivity and isolation and actively seek out solutions to their hearing problems. This must be accompanied by a sensitization of the entourage to the specific needs of affected individuals. This process is grounded in the ecological approach to incapacity and handicap illustrated in figure 2.
Figure 2. Model of restrictions due to hearing loss
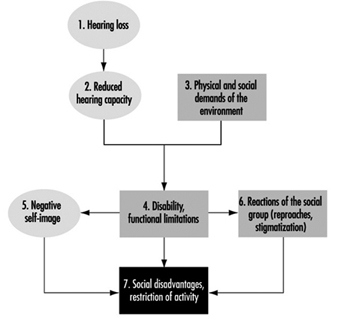
In the ecological model, hearing loss is experienced as an incompatibility between an individual’s residual capacity and the physical and social demands of his or her environment. For example, workers suffering from a loss of frequency discrimination associated with noise-induced hearing loss will have difficulty detecting acoustic alarms in noisy workplaces. If the alarms required at workstations cannot be adjusted to levels significantly louder than those appropriate for people with normal hearing, the workers will be placed in a handicapped position (Hétu 1994b). As a result of this handicap, workers may be at the obvious disadvantage of being deprived of a means to protect themselves. Yet, simply acknowledging hearing loss puts the worker at risk of being considered “abnormal” by his or her colleagues, and when labelled disabled he or she will fear being seen as incompetent by colleagues or superiors. In either case, workers will attempt to hide their handicap or deny the existence of any problems, placing themselves at a functional disadvantage at work.
As figure 2 illustrates, disability is a complex state of affairs with several interrelated restrictions. In such a network of relationships, prevention or minimization of disadvantages or restrictions of activity require simultaneous interventions on many fronts. For example, hearing aids, while partially restoring hearing capacity (component 2), do not prevent either the development of a negative self-image or stigmatization by the worker’s entourage (components 5 and 6), both of which are responsible for isolation and avoidance of communication (component 7). Further, auditory supplementation is incapable of completely restoring hearing capacity; this is particularly true with regard to frequency discrimination. Amplification may improve the perception of acoustic alarms and of conversations but is incapable of improving the resolution of competing signals required for the detection of warning signals in the presence of significant background noise. The prevention of disability-related restrictions therefore necessitates the modification of the social and physical demands of the workplace (component 3). It should be superfluous to note that although interventions designed to modify perceptions (components 5 and 6) are essential and do prevent disability from arising, they do not palliate the immediate consequences of these situations.
Situation-specific Approaches to Rehabilitation
The application of the model presented in Figure 2 will vary depending on the specific circumstances encountered. According to surveys and qualitative studies (Hétu and Getty 1991b; Hétu, Jones and Getty 1993; Hétu, Lalonde and Getty 1987; Hétu, Getty and Waridel 1994; Hétu 1994b), the effects of disability suffered by victims of occupationally induced hearing loss are particularly felt: (1) at the workplace; (2) at the level of social activities; and (3) at the family level. Specific intervention approaches have been proposed for each of these situations.
The workplace
In industrial workplaces, it is possible to identify the following four restrictions or disadvantages requiring specific interventions:
- accident hazards related to the failure to detect warning signals
- efforts, stress and anxiety resulting from hearing and com-munication problems
- obstacles to social integration
- obstacles to professional advancement.
Accident hazards
Acoustic warning alarms are frequently used in industrial workplaces. Occupationally induced hearing loss may considerably diminish workers’ ability to detect, recognize or locate such alarms, particularly in noisy workplaces with high levels of reverberation. The loss of frequency discrimination which inevitably accompanies hearing loss may in fact be so pronounced as to require warning alarms to be 30 to 40db louder than background levels to be heard and recognized by affected individuals (Hétu 1994b); for individuals with normal hearing, the corresponding value is approximately 12 to 15db. Currently, it is rare that warning alarms are adjusted to compensate for background noise levels, workers’ hearing capacity or the use of hearing protection equipment. This puts affected workers at a serious disadvantage, especially as far as their safety is concerned.
Given these constraints, rehabilitation must be based on a rigorous analysis of the compatibility of auditory perception requirements with residual auditory capacities of affected workers. A clinical examination capable of characterizing an individual’s ability to detect acoustic signals in the presence of background noise, such as the DetectsoundTM software package (Tran Quoc, Hétu and Laroche 1992), has been developed, and is available to determine the characteristics of acoustic signals compatible with workers’ hearing capacity. These devices simulate normal or impaired auditory detection and take into account the characteristics of the noise at the workstation and the effect of hearing protection equipment. Of course, any intervention aimed at reducing the noise level will facilitate the detection of acoustic alarms. It is nevertheless necessary to adjust the alarms’ level as a function of the residual hearing capacity of affected workers.
In some cases of relatively severe hearing loss, it may be necessary to resort to other types of warning, or to supplement hearing capacity. For example, it is possible to transmit warning alarms over FM bandwidths and receive them with a portable unit connected directly to a hearing aid. This arrangement is very effective as long as: (1) the tip of the hearing aid fits perfectly (in order to attenuate background noise); and (2) the response curve of the hearing aid is adjusted to compensate for the masking effect of background noise attenuated by the hearing aid tip and the worker’s hearing capacity (Hétu, Tran Quoc and Tougas 1993). The hearing aid may be adjusted to integrate the effects of the full spectrum of background noise, the attenuation produced by the hearing aid’s tip, and the worker’s hearing threshold. Optimal results will be obtained if the frequency discrimination of the worker is also measured. The hearing aid-FM receptor may also be used to facilitate verbal communication with work colleagues when this is essential for worker safety.
In some cases, the workstation itself must be redesigned in order to ensure worker safety.
Hearing and communication problems
Acoustic warning alarms are usually used to inform workers of the state of a production process and as a means of inter operator communication. In workplaces where such alarms are used, individuals with hearing loss must rely upon other sources of information to perform their work. These may involve intense visual surveillance and discreet help offered by work colleagues. Verbal communication, whether over the telephone, in committee meetings or with superiors in noisy workshops, requires great effort on the part of affected individuals and is also highly problematic for affected individuals in industrial workplaces. Because these individuals feel the need to hide their hearing problems, they are also plagued by the fear of being unable to cope with a situation or of committing costly errors. Often, this may cause extremely high anxiety (Hétu and Getty 1993).
Under these circumstances, rehabilitation must first focus on eliciting explicit acknowledgement by the company and its representatives of the fact that some of their workers suffer from hearing difficulties caused by noise exposure. The legitimization of these difficulties helps affected individuals to communicate about them and to avail themselves of appropriate palliative means. However, these means must in fact be available. In this regard, it is astonishing to note that telephone receivers in the workplace are rarely equipped with amplifiers designed for individuals suffering from hearing loss and that conference rooms are not equipped with appropriate systems (FM or infrared transmitters and receptors, for example). Finally, a campaign to increase awareness of the needs of individuals suffering from hearing loss should be undertaken. By publicizing strategies which facilitate communication with affected individuals, communication-related stress will be greatly reduced. These strategies consist of the following phases:
- approaching the affected individual and facing him or her
- articulating without exaggeration
- repeating misunderstood phrases, using different words
- keeping as far away from sources of noise as possible
Clearly, any control measures that lead to lower noise and reverberation levels in the workplace also facilitate communication with individuals suffering from hearing loss.
Obstacles to social integration
Noise and reverberation in the workplace render communication so difficult that it is often limited to the strict minimum required by the tasks to be accomplished. Informal communication, a very important determinant of the quality of working life, is thus greatly impaired (Hétu 1994a). For individuals suffering from hearing loss, the situation is extremely difficult. Workers suffering from occupationally induced hearing loss are isolated from their work colleagues, not only at their workstation but even during breaks and meals. This is a clear example of the convergence of excessive work requirements and the fear of ridicule suffered by affected individuals.
The solutions to this problem lie in the implementation of the measures already described, such as the lowering of overall noise levels, particularly in rest areas, and the sensitization of work colleagues to the needs of affected individuals. Again, recognition by the employer of affected individuals’ specific needs itself constitutes a form of psychosocial support capable of limiting the stigma associated with hearing problems.
Obstacles to professional advancement
One of the reasons individuals suffering from occupationally induced hearing loss take such pains to hide their problem is the explicit fear of being disadvantaged professionally (Hétu and Getty 1993): some workers even fear losing their jobs should they reveal their hearing loss. The immediate consequence of this is a self-restriction with regard to professional advancement, for example, failure to apply for a promotion to shift supervisor, supervisor or foreman. This is also true of professional mobility outside the company, with experienced workers failing to take advantage of their accumulated skills since they feel that pre-employment audiometric examinations would block their access to better jobs. Self-restriction is not the only obstacle to professional advancement caused by hearing loss. Workers suffering from occupationally induced hearing loss have in fact reported instances of employer bias when positions requiring frequent verbal communication have become available.
As with the other aspects of disability already described, explicit acknowledgement of affected workers’ specific needs by employers greatly eliminates obstacles to professional advancement. From the standpoint of human rights (Hétu and Getty 1993), affected individuals have the same right to be considered for advancement as do other workers, and appropriate workplace modifications can facilitate their access to higher-level jobs.
In summary, the prevention of disability in the workplace requires sensitization of employers and work colleagues to the specific needs of individuals suffering from occupationally induced hearing loss. This can be accomplished by information campaigns on the signs and effects of noise-induced hearing loss aimed at dissipating the view of hearing loss as an improbable abnormality of little import. The use of technological aids is possible only if the need to use them has been legitimized in the workplace by colleagues, superiors and affected individuals themselves.
Social activities
Individuals suffering from occupationally induced hearing loss are at a disadvantage in any non-ideal hearing situation, for instance, in the presence of background noise, in situations requiring communication at a distance, in environments where reverberation is high and on the telephone. In practice, this greatly curtails their social life by limiting their access to cultural activities and public services, thus hindering their social integration (Hétu and Getty 1991b).
Access to cultural activities and public services
In accordance with the model in Figure 2, restrictions related to cultural activities involve four components (components 2, 3, 5 and 6) and their elimination relies on multiple interventions. Thus concert halls, auditoriums and places of worship can be made accessible to persons suffering from hearing loss by equipping them with appropriate listening systems, such as FM or infrared transmission systems (component 3) and by informing those responsible for these institutions of the needs of affected individuals (component 6). However, affected individuals will request hearing equipment only if they are aware of its availability, know how to use it (component 2) and have received the necessary psychosocial support to recognize and communicate their need for such equipment (component 5).
Effective communication, training and psychosocial support channels for hearing-impaired workers have been developed in an experimental rehabilitation programme (Getty and Hétu 1991, Hétu and Getty 1991a), discussed in “Family life”, below.
As regards the hearing-impaired, access to public services such as banks, stores, government services and health services is hindered primarily by a lack of knowledge on the part of the institutions. In banks, for example, glass screens may separate clients from tellers, who may be occupied in entering data or filling out forms while talking to clients. The resulting lack of face-to-face visual contact, coupled with unfavourable acoustic conditions and a context in which misunderstanding can have very serious consequences, render this an extremely difficult situation for affected individuals. In health service facilities, patients wait in relatively noisy rooms where their names are called by an employee located at a distance or via a public address system that may be difficult to comprehend. While individuals with hearing loss worry a great deal about being unable to react at the correct time, they generally neglect to inform staff of their hearing problems. There are numerous examples of this type of behaviour.
In most cases, it is possible to prevent these handicap situations by informing staff of the signs and effects of partial deafness and of ways to facilitate communication with affected individuals. A number of public services have already undertaken initiatives aimed at facilitating communication with individuals suffering from occupationally induced hearing loss (Hétu, Getty and Bédard 1994) with results as follows. The use of appropriate graphical or audio visual material allowed the necessary information to be communicated in less than 30 minutes and the effects of such initiatives were still apparent six months after the information sessions. These strategies greatly facilitated communication with the personnel of the services involved. Very tangible benefits were reported not only by clients with hearing loss but also by the staff, who saw their tasks simplified and difficult situations with this type of client prevented.
Social integration
Avoidance of group encounters is one of the most severe consequences of occupationally induced hearing loss (Hétu and Getty 1991b). Group discussions are extremely demanding situations for affected individuals, In this case, the burden of accommodation rests with the affected individual, as he or she can rarely expect the entire group to adopt a favourable rhythm of conversation and mode of expression. Affected individuals have three strategies available to them in these situations:
- reading facial expressions
- using specific communication strategies
- using a hearing aid.
The reading of facial expressions (and lip-reading) can certainly facilitate comprehension of conversations, but requires considerable attention and concentration and cannot be sustained over long periods. This strategy can, however, be usefully combined with requests for repetition, reformulation and summary. Nevertheless, group discussions occur at such a rapid rhythm that it is often difficult to rely upon these strategies. Finally, the use of a hearing aid may improve the ability to follow conversation. However, current amplification techniques do not allow the restoration of frequency discrimination. In other words, both signal and noise are amplified. This often worsens rather than improves the situation for individuals with serious frequency discrimination deficits.
The use of a hearing aid as well as the request for accommodation by the group presupposes that the affected individual feels comfortable revealing his or her condition. As discussed below, interventions aimed at strengthening self-esteem are therefore prerequisites for attempts to supplement auditory capacity.
Family life
The family is the prime locus of the expression of hearing problems caused by occupational hearing loss (Hétu, Jones and Getty 1993). A negative self-image is the essence of the experience of hearing loss, and affected individuals attempt to hide their hearing loss in social interactions by listening more intently or by avoiding overly demanding situations. These efforts, and the anxiety which accompanies them, create a need for release in the family setting, where the need to hide the condition is less strongly felt. Consequently, affected individuals tend to impose their problems on their families and coerce them to adapt to their hearing problems. This takes a toll on spouses and others and causes irritation at having to repeat oneself frequently, tolerate high television volumes and “always be the one to answer the telephone”. Spouses must also deal with serious restrictions in the couples’ social life and with other major changes in family life. Hearing loss limits companionship and intimacy, creates tension, misunderstandings and arguments and disturbs relations with children.
Not only does hearing and communication impairment affect intimacy, but its perception by affected individuals and their family (components 5 and 6 of figure 2) tends to feed frustration, anger and resentment (Hétu, Jones and Getty 1993). Affected individuals frequently do not recognize their impairment and do not attribute their communications problems to a hearing deficit. As a result, they may impose their problems on their families rather than negotiate mutually satisfactory adaptations. Spouses, on the other hand, tend to interpret the problems as a refusal to communicate and as a change in the affected individual’s temperament. This state of affairs may lead to mutual reproaches and accusations, and ultimately to isolation, loneliness and sadness, particularly on the part of the unaffected spouse.
The solution of this interpersonal dilemma requires the participation of both partners. In fact, both require:
- information on the auditory basis of their problems.
- psychosocial support
- training in the use of appropriate supplemental means of communication.
With this in mind, a rehabilitation programme for affected individuals and their spouses has been developed (Getty and Hétu 1991, Hétu and Getty 1991a). The goal of the programme is to stimulate research on the resolution of problems caused by hearing loss, taking into account the passivity and social withdrawal that characterize occupationally induced hearing loss.
Since the stigma associated with deafness is the principal source of these behaviours, it was essential to create a setting in which self-esteem could be restored so as to induce affected individuals to seek out actively solutions to their hearing-related problems. The effects of stigmatization can be overcome only when one is perceived by others as normal regardless of any hearing deficit. The most effective way to achieve this consists of meeting other people in the same situation, as was suggested by workers asked about the most appropriate aid to offer their hearing-impaired colleagues. However, it is essential that these meetings take place outside the workplace, precisely to avoid the risk of further stigmatization (Hétu, Getty and Waridel 1994).
The rehabilitation programme mentioned above was developed with this in mind, the group encounters taking place in a community health department (Getty and Hétu 1991). Recruitment of participants was an essential component of the programme, given the withdrawal and passivity of the target population. Accordingly, occupational health nurses first met with 48 workers suffering from hearing loss and their spouses at their homes. Following an interview on hearing problems and their effects, every couple was invited to a series of four weekly meetings lasting two hours each, held in the evening. These meetings followed a precise schedule aimed at meeting the objectives of information, support and training defined in the programme. Individual follow-up was provided to participants in order to facilitate their access to audio-logical and audioprosthetic services. Individuals suffering from tinnitus were referred to the appropriate services. A further group meeting was held three months after the last weekly meeting.
The results of the programme, collected at the end of the experimental phase, demonstrated that participants and their spouses were more aware of their hearing problems, and were also more confident of resolving them. Workers had undertaken various steps, including technical aids, revealing their impairment to their social group, and expressing their needs in an attempt to improve communication.
A follow-up study, performed with this same group five years after their participation in the programme, demonstrated that the programme was effective in stimulating participants to seek solutions. It also showed that rehabilitation is a complex process requiring several years of work before affected individuals are able to avail themselves of all the means at their disposal to regain their social integration. In most cases, this type of rehabilitation process requires periodic follow-up.
Conclusion
As figure 2 indicates, the meaning that individuals suffering from occupationally induced hearing loss and their associates give to their condition is a key factor in handicap situations. The approaches to rehabilitation proposed in this article explicitly take this factor into account. However, the manner in which these approaches are applied concretely will depend on the specific sociocultural context, since the perception of these phenomena may vary from one context to another. Even within the sociocultural context in which the intervention strategies described above were developed, significant modifications may be necessary. For example, the programme developed for individuals suffering from occupationally induced hearing loss and their spouses (Getty and Hétu 1991) was tested in a population of affected males. Different strategies would probably be necessary in a population of affected females, especially when one considers the different social roles men and women occupy in conjugal and parental relations (Hétu, Jones and Getty 1993). Modifications would be necessary a fortiori when dealing with cultures which differ from that of North America from which the approaches emerged. The conceptual framework proposed (figure 2) can nevertheless be used effectively to orient any intervention aimed at rehabilitating individuals suffering from occupationally induced hearing loss.
Furthermore, this type of intervention, if applied on a large scale, will have important preventive effects on hearing loss itself. The psychosocial aspects of occupationally induced hearing loss hinder both rehabilitation (figure 1) and prevention. The distorted perception of hearing problems delays their recognition, and their dissimulation by severely affected individuals fosters the general perception that these problem are rare and relatively innocuous, even in noisy workplaces. This being so, noise-induced hearing loss is not perceived by workers at risk or by their employers as an important health problem, and the need for prevention is thus not strongly felt in noisy workplaces. On the other hand, individuals already suffering from hearing loss who reveal their problems are eloquent examples of the severity of the problem. Rehabilitation can thus be seen as the first step of a prevention strategy.
Rights and Duties: An Employer's Perspective
The traditional approach to helping disabled people into work has had little success, and it is evident that something fundamental needs to be changed. For example, the official unemployment rates for disabled people are always at least twice that of their non-disabled peers—often higher. The numbers of disabled people not working often approach 70% (in the United States, United Kingdom, Canada). Disabled people are more likely than their non-disabled peers to live in poverty; for example, in the United Kingdom two-thirds of the 6.2 million disabled citizens have only state benefits as income.
These problems are compounded by the fact that rehabilitation services are often unable to meet employer demand for qualified applicants.
In many countries, disability is not generally defined as an equal opportunities or rights issue. It is thus difficult to encourage corporate best practice which positions disability firmly alongside race and gender as an equal opportunities or diversity priority. Proliferation of quotas or the complete absence of relevant legislation reinforces employer assumptions that disability is primarily a medical or charity issue.
Evidence of the frustrations created by inadequacies inherent in the present system can be seen in growing pressure from disabled people themselves for legislation based on civil rights and/or employment rights, such as exists in the United States, Australia, and, from 1996, in the United Kingdom. It was the failure of the rehabilitation system to meet the needs and expectations of enlightened employers which prompted the UK business community to establish the Employers Forum on Disability.
Employers’ attitudes unfortunately reflect those of the wider society—although this fact is often overlooked by rehabilitation practitioners. Employers share with many others widespread confusion regarding such issues as:
- What is a disability? Who is and who is not disabled?
- Where do I get advice and services to help me recruit and retain disabled people?
- How do I change my organization’s culture and working practices?
- What benefit will best practice on disability bring my business—and the economy in general?
The failure to meet the information and service needs of the employer community constitutes a major hurdle for disabled people wanting work, yet it is rarely addressed adequately by government policy makers or rehabilitation practitioners.
Deep-Rooted Myths that Disadvantage Disabled People in the Labour Market
Non-governmental organizations (NGOs), governments, indeed all those involved in the medical and employment rehabilitation of persons with disabilities, tend to share a set of deep-rooted, often unspoken assumptions which only further disadvantage the disabled individuals these organizations seek to help:
- “The employer is the problem—indeed, often the adversary.” It is employer attitudes which are often blamed for the failure of disabled people to find jobs, despite the evidence that numerous other factors may well have been highly significant.
- “The employer is not treated either as a client or a customer.” Rehabilitation services do not measure their success by the extent to which they make it easier for the employer to recruit and retain disabled employees. As a result, the unreasonable difficulties created by suppliers of rehabilitation services make it difficult for the well-intentioned and enlightened employer to justify the time, cost and effort required to effect change. The not-so-enlightened employer has his or her reluctance to effect change more than justified by the lack of cooperation from rehabilitation services..
- “Disabled people really cannot compete on merit.” Many service providers have low expectations of disabled people and their potential to work. They find it difficult to promote the “business case” to employers because they themselves doubt that employing people with disability brings genuine mutual benefit. Instead the tone and underlying ethos of their communication with employers stresses the moral and perhaps (occasional) legal obligation in a way which only further stigmatizes disabled people.
- “Disability is not a mainstream economic or business issue. It is best left in the hands of the experts, doctors, rehabilitation providers and charities.” The fact that disability is portrayed in the media and through fund-raising activities as a charity issue, and that disabled people are portrayed as the natural and passive recipients of charity, is a fundamental barrier to the employment of disabled people. It also creates tension in organizations that are trying to find jobs for people, while on the other hand using images which tug at the heartstrings.
The consequence of these assumptions is that:
- Employers and disabled people remain separated by a maze of well-meaning but often uncoordinated and fragmented services which only rarely define success in terms of employer satisfaction.
- Employers and disabled people alike remain excluded from real influence over policy development; only rarely is either party asked to evaluate services from its own perspective and to propose improvements.
We are beginning to see an international trend, typified by the development of “job coach” services, towards acknowledging that successful rehabilitation of disabled people depends upon the quality of service and support available to the employer.
The statement “Better services for employers equals better services for disabled people” must surely come to be much more widely accepted as economic pressures build on rehabilitation agencies everywhere in the light of governments’ retrenchment and restructuring. It is nonetheless very revealing that a recent report by Helios (1994), which summarizes the competencies required by vocational or rehabilitation specialists, fail to make any reference to the need for skills which relate to the employers as customer.
While there is a growing awareness of the need to work with employers as partners, our experience shows that it is difficult to develop and sustain a partnership until the rehabilitation practitioners first meet the needs of the employer as customer and begin to value that “employer as customer” relationship.
Employers’ Roles
At various times and in various situations the system and services position the employer in one or more of the following roles—though only rarely is it articulated. Thus we have the employer as:
- the Problem—“you require enlightenment”
- the Target—“you need education, information, or consciousness raising”
- the Customer—“the employer is encouraged to use us in order to recruit and retain disabled employees”
- the Partner—the employer is encouraged to “enter into a long term, mutually beneficial relationship”.
And at any time during the relationship the employer may be called upon—indeed is typically called upon—to be a funder or philanthropist.
The key to successful practice lies in approaching the employer as “The Customer”. Systems which regard the employer as only “The Problem”, or “The Target”, find themselves in a self-perpetuating dysfunctional cycle.
Factors outside the Employer’s Control
Reliance on perceived employer negative attitudes as the key insight into why disabled people experience high unemployment rates, consistently reinforces the failure to address other highly significant issues which must also be tackled before real change can be brought about.
For example:
- In the United Kingdom, in a recent survey 80% of employers were not aware they had ever had a disabled applicant.
- Benefits and social welfare systems often create financial disincentives for disabled people moving into work.
- Transport and housing systems are notoriously inaccessible; people can look for work successfully only when basic housing, transport and subsistence needs have been met.
- In a recent UK survey, 59% of disabled job seekers were unskilled compared to 23% of their peers. Disabled people, in general, are simply not able to compete in the labour market unless their skill levels are competitive.
- Medical professionals frequently underestimate the extent to which a disabled person can perform in work and are often unable to advise on adaptations and adjustments which might make that person employable.
- Disabled people often find it difficult to obtain high quality career guidance and throughout their lives are subject to the lower expectations of teachers and advisers.
- Quotas and other inappropriate legislation actively undermine the message that disability is an equal opportunities issue.
A legislative system that creates an adversarial or litigious environment can further undermine the job prospects of disabled people because bringing a disabled person into the company could expose the employer to risk.
Rehabilitation practitioners often find it difficult to access expert training and accreditation and are themselves rarely funded to deliver relevant services and products to employers.
Policy Implications
It is vital for service providers to understand that before the employer can effect organizational and cultural change, similar changes are required on the part of the rehabilitation provider. Providers approaching employers as customers need to recognize that actively listening to the employers will almost inevitably trigger the need to change the design and delivery of services.
For example, service providers will find themselves asked to make it easier for the employer to:
- find qualified applicants
- obtain high quality employer-oriented services and advice
- meet disabled people as applicants and colleagues
- understand not just the need for policy change but how to make such change come about
- promote attitude change across their organizations
- understand the business as well as the social case for employing disabled people
Attempts at significant social policy reforms related to disability are undermined by the failure to take into account the needs, expectations and legitimate requirements of the people who will largely determine success—that is, the employers. Thus, for example, the move to ensure that people currently in sheltered workshops obtain mainstream work frequently fails to acknowledge that it is only employers who are able to offer that employment. Success therefore is limited, not only because it is unnecessarily difficult for the employers to make opportunities available but also because of the missed added value resulting from active collaboration between employers and policy makers.
Potential for Employer Involvement
Employers can be encouraged to contribute in numerous ways to making a systematic shift from sheltered employment to supported or competitive employment. Employers can:
- advise on policy—that is, on what needs to be done which would make it easier for employers to offer work to disabled candidates.
- offer advice on the competencies required by disabled individ-uals if they are to be successful in obtaining work.
- advise on the competencies required by service providers if they are to meet employer expectations of quality provision.
- evaluate sheltered workshops and offer practical advice on how to manage a service that is most likely to enable people to move into mainstream work.
- offer work experience to rehabilitation practitioners, who thus gain an understanding of a particular industry or sector and are better able to prepare their disabled clients.
- offer on-the-job assessments and training to disabled individuals.
- offer mock interviews and be mentors to disabled job seekers.
- loan their own staff to work inside the system and/or its institutions.
- help to market rehabilitation agencies and promote policies, organizations and disabled job seekers to other employers.
- offer customized training whereby they become directly involved in helping disabled individuals to acquire specific job-related skills.
- participate on management boards of rehabilitation agencies or set themselves up in an informal advisory capacity to national policy makers or suppliers.
- lobby alongside rehabilitation providers and disabled people for better government policies and programmes.
- advise on the services and products they require in order to deliver best practice.
Employer as Customer
It is impossible for rehabilitation practitioners to build partnerships with employers without first acknowledging the need to deliver efficient services.
Services should emphasize the theme of mutual benefit. Those who do not passionately believe that their disabled clients have something of real benefit to contribute to the employer are unlikely to be able to influence the employer community.
Improving the quality of service to employers will quickly—and inevitably—improve services for disabled job-seekers. The following represents a useful audit for services wishing to improve the quality of service to the employer.
Does the service offer employers:
1. information and consultancy regarding:
- business benefits which result from employing disabled persons
- possible applicants
- access to the services and the nature of services offered
- models of policy and procedures proven successful by other employers
- legal obligations
2. recruitment services, including access to:
- suitable applicants
- job coaches
3. pre-screening of applicants as per employer expectations
4. professional job analysis and job modification services, able to advise on job restructuring and the use of technical aids and adaptations in the workplace, both for existing and potential employees
5. financial support programmes which are well marketed, appropriate to employer requirements, easy to access, efficiently delivered
6. information and practical help so that employers can make the worksite more physically accessible
7. training for employers and employees regarding the benefits of employing people with disabilities generally, and when specific individuals have been employed
8. work-experience services which provide the employer with relevant support
9. work habituation or employee-orientation services to include job coaches and job-sharing schemes
10. post–job offer support for employers to include advice on best practice in the management of absenteeism and presentation of work-related impairments
11. advice for employers on career development of disabled employees and on meeting the needs of underemployed disabled employees.
Practical Steps: Making it Easier for the Employer
Any system of services which aims to help disabled people into training and work will inevitably be more successful if the needs and expectations of the employer are adequately addressed. (Note: It is difficult to find a term which adequately encompasses all those agencies and organizations—governmental, NGOs, not for profit—which are involved in policy making and service delivery to disabled people seeking work. For the sake of brevity, the term service or service provider is used to encompass all those involved in this entire complex system.)
Close consultation over time with employers will in all likelihood produce recommendations similar to the following.
Codes of practice are needed which describe the high quality of service employers should receive from employment-related agencies. Such codes should, in consultation with employers, set standards which relate both to the efficiency of the existing services and to the nature of services offered—This code should be monitored via regular surveys of employer satisfaction.
Specific training and accreditation for rehabilitation practition-ers in how to meet the needs of employers is required and should be a high priority.
Services should recruit people who have direct experience of the world of industry and commerce and who are skilled in bridging the communication gap between the not-for-profit and profit-making sectors.
Services themselves should employ significantly more disabled people, thus minimizing the numbers of non-disabled intermediaries dealing with employers. They should ensure that disabled people in various capacities have a high profile in the employer community.
Services should minimize the fragmentation of education, marketing and campaigning activities. It is particularly counterproductive to create a milieu characterized by messages, posters and advertising which reinforces the medical model of disability and the stigma attached to particular impairments, rather than focusing on the employability of individuals and the need for employers to respond with appropriate policy and practice.
Services should collaborate to simplify access, to services and support, for both the employer and for the disabled person. Considerable attention should be given to analysing the client journey (with both employer and disabled person as client) in a way that minimizes assessments and moves the individual speedily, step by step, into employment. Services should build on mainstream business initiatives to ensure that disabled people are given priority.
Services should bring employers together routinely and ask their expert advice regarding what has to be done to make services and job candidates more successful.
Conclusion
In many countries, the services designed to help disabled people into work are complex, cumbersome and resistant to change, despite the evidence decade after decade that change is required.
A fresh approach to employers offers enormous potential to transform this situation significantly by radically altering the position of one key protagonist—the employer.
We see business and government engaged in a wide-ranging debate regarding the way in which relationships between stakeholders or social partners must inevitably change over the next 20 years. Thus employers launch the European Business against Social Exclusion Initiative in Europe, major companies join together to re-think their relationship with society in the UK in “Tomorrow’s Company”, and the Employers Forum on Disability becomes only one of various UK employer initiatives aimed at addressing issues of equality and diversity.
Employers have much to do if the issue of disability is to take its rightful place as a business and ethical imperative; the rehabilitation community in turn needs to take a fresh approach which redefines working relationships between all stakeholders in a way that makes it easier for employers to make equal opportunities a reality.
Rights and Duties: Workers' Perspective
Historically, people with disabilities have had tremendous barriers to entering the workforce, and those who became injured and disabled on the job have often faced job loss and its negative psychological, social and financial ramifications. Today, people with disabilities are still underrepresented in the workforce, even in countries with the most progressive civil rights and employment promotion legislation, and in spite of international efforts to address their situation.
Awareness has increased of the rights and needs of workers with disabilities and the concept of managing disability in the workplace. Workers’ compensation and social insurance programmes that protect income are common in industrialized countries. The increased costs related to operating such programmes have provided an economic basis for promoting the employment of people with disabilities and the rehabilitation of injured workers. At the same time, people with disabilities have become organized to demand their rights and integration into all aspects of community life, including the workforce.
Labour unions in many countries have been among those who have supported such efforts. Enlightened companies are recognizing the need to treat workers with disabilities equitably and are learning the importance of maintaining a healthy workplace. The concept of managing disability or dealing with disability issues in the workplace has emerged. Organized labour has been partly responsible for this emergence and continues to play an active role.
According to ILO Recommendation No. 168 concerning the vocational rehabilitation and employment of disabled persons, “workers’ organizations should adopt a policy for the promotion of training and suitable employment of disabled persons on an equal footing with other workers”. The recommendation further suggests that workers’ organizations become involved in formulating national policies, cooperate with rehabilitation specialists and organizations, and foster the integration and vocational rehabilitation of disabled workers.
The purpose of this article is to explore the issue of disability in the workplace from the perspective of the rights and duties of workers and to describe the specific role that labour unions play in facilitating the on-the-job integration of people with disabilities.
In a healthy work environment, both the employer and the worker care about the quality of work, health and safety, and the fair treatment of all workers. Workers are hired on the basis of their abilities. Both workers and employers contribute to maintaining health and safety and, when an injury or disability does occur, they have the rights and duties to minimize the impact of the disability on the individual and the workplace. Although workers and employers may have different perspectives, by working in partnership they can effectively achieve goals related to maintaining a healthy, safe and fair workplace.
The term rights is often associated with legal rights determined by legislation. Many European countries, Japan and others have enacted quota systems requiring that a certain percentage of employees be persons with disabilities. Fines may be levied on employers who fail to meet the prescribed quota. In the United States, the Americans with Disabilities Act (ADA) prohibits discrimination against people with disabilities in work and community life. Health and safety laws exist in most countries to protect workers from unsafe working conditions and practices. Workers’ compensation and social insurance programmes have been legislated to provide a variety of medical, social, and, in some instances, vocational rehabilitation services. Specific workers’ rights may also become part of negotiated labour agreements and therefore legally mandated.
A worker’s legal rights (and duties) related to disability and work will depend on the complexity of this legislative mix, which varies from country to country. For purposes of this article, workers’ rights are simply those legal or moral entitlements considered to be in the workers’ interest as they relate to productive activity in a safe and non-discriminating work environment. Duties refer to those obligations that workers have to themselves, other workers and their employers to contribute effectively to the productivity and safety of the workplace.
This article organizes worker rights and duties within the context of four key disability issues: (1) recruitment and hiring; (2) health, safety and the prevention of disability; (3) what happens when a worker becomes disabled, including rehabilitation and the return to work after injury; and (4) the total integration of the worker into the workplace and the community. Labour union activities related to these issues include: organizing and advocating for the rights of workers with disabilities through national legislation and other vehicles; ensuring and protecting rights by including them in negotiated labour agreements; educating union members and employers on disability issues and rights and responsibilities related to disability management; collaborating with management to further the rights and duties related to disability management; providing services to workers with disabilities to assist them in becoming integrated or more integrated into the workforce; and, when all else fails, engaging in resolving or litigating disputes, or fighting for legislative changes to protect rights.
Issue 1: Recruitment, Hiring and Employment Practices
While the legal obligations of labour unions may relate specifically to their members, unions traditionally helped to improve the working lives of all workers, including those with disabilities. This is a tradition that is as old as the labour movement itself. However, fair and equitable practices related to recruitment, hiring and employment practices take on special significance when the worker has a disability. Because of negative stereotypes as well as architectural, communication and other barriers related to disability, disabled job seekers and workers are often denied their rights or face discriminatory practices.
The following basic lists of rights (figure 1 to 4), although simply stated, have profound implications for equal access to employment opportunities by disabled workers. Disabled workers also have certain duties, as do all workers, to present themselves, including their interests, abilities, skills and workplace requirements, in an open and forthright manner.
Figure 1. Rights and duties: recruitment, hiring and employment practices

In the hiring process, applicants should be judged on their abilities and qualifications (figure 1). They need to have a full understanding of the job to evaluate their interest and ability to do the job. Further, once hired, all workers should be judged and evaluated according to their job performance, without bias based on factors not related to the job. They should have equal access to employment benefits and opportunities for advancement. When necessary, reasonable accommodations should be made so that an individual with a disability can perform the requisite job tasks. Job accommodations can be as simple as raising a workstation, making a chair available or adding a foot pedal.
In the United States, the Americans with Disabilities Act not only prohibits discrimination against qualified workers (a qualified worker is one who has the qualifications and abilities to perform the essential functions of the job) based on disability, but also requires that employers make reasonable accommodation—that is, the employer provides a piece of equipment, changes non-essential job functions or makes some other adjustment that does not cause the employer undue hardship, so that the person with a disability can perform the essential functions of the job. This approach is designed to protect workers’ rights and make it “safe” to request accommodations. According to the US experience, most accommodations are relatively low in cost (less than US$50).
Rights and duties go hand in hand. Workers have a responsibility to notify their employer of a condition that may affect their ability to do the job, or that may affect their safety or that of others. Workers have a duty to represent themselves and their abilities in an honest manner. They should request a reasonable accommodation, if necessary, and accept that which is most appropriate for the situation, cost-effective and least intrusive to the workplace while still meeting their needs.
ILO Convention No. 159 concerning the vocational rehabilitation and employment of disabled persons, and Recommendation No. 168 address these very rights and duties and their implications for workers’ organizations. Convention No.159 suggests that special positive measures may sometimes be necessary to ensure “effective equality of opportunity and treatment between disabled workers and other workers”. It adds that such measures “shall not be regarded as discriminating against other workers”. Recommendation No. 168 encourages the implementation of specific measures to create job opportunities, such as providing financial support to employers to make reasonable accommodations, and encourages labour organizations to promote such measures and provide advice about making such accommodations.
What labour unions can do
Union leaders typically have deep roots within the communities in which they operate and can be valuable allies in promoting the recruitment, hiring and continued employment of persons with disabilities. One of the first things they can do is to develop a policy statement on the employment rights of people with disabilities. Education of members and a plan of action to support the policy should follow. Labour unions can advocate rights for workers with disabilities on a broad scale by promoting, monitoring and supporting relevant legislative initiatives. In the workplace they should encourage management to develop policies and actions that remove barriers to employment for disabled workers. They can assist in developing appropriate job accommodations and, through negotiated labour agreements, protect and further the rights of disabled workers in all employment practices.
Organized labour can initiate programmes or cooperative efforts with employers, government ministries, non-governmental organizations, and companies to develop programmes that will result in increased recruitment and hiring of, and fair practices towards, people with disabilities. Representatives can sit on boards and lend their expertise to community-based organizations that work with people with disabilities. They can promote awareness among union members, and, in their role as employers, labour unions can set an example of fair and equitable hiring practices.
Examples of what labour unions are doing
In England, the Trades Union Congress (TUC) has taken an active role in promoting equal rights in employment for persons with disabilities, through published policy statements and active advocacy. It regards the employment of disabled people as an equal opportunities issue, and the experiences of disabled persons as not unlike those of other groups that have been discriminated against or excluded. The TUC supports existing quota legislation and advocates for levies (fines) on employers who fail to comply with the law.
It has published several related guides to support its activities and educate its members, including TUC Guidance: Trade Unions and Disabled Members, Employment of Disabled People, Disability Leave and Deaf People and Their Rights. Trade Unions and Disabled Members includes guidance about basic points that unions should consider when negotiating for disabled members. The Irish Congress of Trade Unions has produced a guide with similar intent, Disability and Discrimination in the Workplace: Guidelines for Negotiators. It provides practical steps to tackle workplace discrimination and to promote equality and access through negotiated labour agreements.
The Federation of German Trade Unions also has developed a comprehensive position paper stating its policy for integrative employment, its stance against discrimination and its commitment to use its influence to further its positions. It supports broad employment training and access to apprenticeships for disabled persons, addresses the double discrimination faced by disabled women, and advocates for union activities that support access to public transportation and integration into all aspects of society.
The Screen Actors Guild in the United States has approximately 500 members with disabilities. A statement on non-discrimination and affirmative action appears in its collective bargaining agreements. In a cooperative venture with the American Federation of Television and Radio Artists, the Guild has met with national advocacy groups to develop strategies to increase the representation of people with disabilities in their respective industries. The International Union of United Automobile, Aerospace and Agricultural Implement Workers of America is another labour union that includes language in its collective bargaining agreements prohibiting discrimination based on disability. It also fights for reasonable accommodations for its members and provides regular training on disability and work issues. The United Steel Workers of America has included for years non-discrimination clauses in its collective bargaining agreements, and resolves disability discrimination complaints through a grievance process and other procedures.
In the United States, the passage and implementation of the Americans with Disabilities Act (ADA) was, and continues to be, promoted by US-based labour unions. Even before passage of the ADA, many AFL-CIO member unions were actively involved in training their memberships on disability rights and awareness (AFL-CIO 1994). The AFL-CIO and other labour union representatives are carefully monitoring the implementation of the law, including litigation and alternative dispute resolution processes, to support the rights of workers with disabilities under the ADA and to ensure that their interests and the rights of all workers are fairly considered.
With passage of the ADA, labour unions have produced scores of publications and videos and organized training programmes and workshops to further educate their members. The Civil Rights Department of the AFL-CIO produced brochures and held workshops for their affiliated unions. The International Association of Machinists and Aerospace Workers Center for Administering Rehabilitation and Education Services (IAM CARES), with support from the federal government, produced two videos and ten booklets for employers, people with disabilities and union personnel to inform them of their rights and responsibilities under the ADA. The American Federation of State, County and Municipal Employees (AFSCME) has a long-standing history of protecting the rights of workers with disabilities. With passage of the ADA, AFSCME updated its publications and other efforts and trained thousands of members and AFSCME staff on the ADA and workers with disabilities.
Although Japan has a quota and levy system in place, one Japanese labour union recognized that individuals who are mentally disabled are the most likely to be underrepresented in the labour force, especially among larger employers. It has been taking action. The Kanagawa Regional Council of the Japanese Electrical, Electronic and Information Union is working with the city of Yokohama to develop an employment support center. Its purpose will include training individuals who are mentally disabled and providing services to facilitate their placement and that of other disabled persons. Further, the union plans to establish a training centre that will provide disability awareness and sign-language training to union members, personnel managers, production supervisors and others. It will capitalize on good labour-employer relationships and engage business people in the management and activities of the centre. Initiated by the labour union, the project promises to be a model of collaboration between business, labour and government.
In the United States and Canada, labour unions have been working cooperatively and creatively with government and employers to facilitate the employment of people with disabilities through a programme called Projects with Industry (PWI). By matching labour union resources with government funding, IAM CARES and the Human Resources Development Institute (HRDI) of the AFL-CIO have been operating training and job placement programmes for individuals with disabilities regardless of their union affiliation. In 1968, HRDI began to function as the AFL-CIO’s employment and training arm by providing assistance to diverse ethnic groups, women and people with disabilities. In 1972, it began a programme with a specific focus on people with disabilities, to place them with employers who had labour agreements with national and international labour unions. As of 1995, more than 5,000 people with disabilities have been employed as a result of this activity. Since 1981, the IAM CARES programme, which operates in the Canadian and US labour markets, has enabled more than 14,000 individuals, most of whom are severely disabled, to find jobs. Both programmes provide professional assessment, counselling and job placement assistance through linkages with businesses and with government and labour union support.
In addition to providing direct services to workers with disabilities, these PWI programmes engage in activities that enhance public awareness of people with disabilities, promote cooperative labour-management action to foster employment and job retention, and provide training and consulting services to local unions and employers.
These are only some examples from around the world of activities that labour unions have taken to facilitate fairness in employment for workers with disabilities. It is fully in line with their broad goal to facilitate worker solidarity and to end all forms of discrimination.
Issue 2: Disability Prevention, Health and Safety
While securing safe working conditions is a hallmark of labour union activity in many countries, maintaining health and safety in the workplace has traditionally been an employer function. Typically, management has control over job design, tool selection, and decisions about processes and the work environment that affect safety and prevention. Yet, only someone who performs the tasks and procedures on a regular basis, under specific work conditions and demands, can fully appreciate the implications of procedures, conditions and hazards on safety and productivity.
Fortunately, enlightened employers recognize the importance of worker feedback, and as the organizational structure of the workplace is changing to increase worker autonomy, such feedback is more readily invited. Safety and prevention research also supports the need to involve the worker in job design, policy formulation and the implementation of programmes on health, safety and disability prevention.
Another trend, the sharp increase in workers’ compensation and other costs of job-related injury and disability, has led employers to examine prevention as a key component of the disability management effort. Prevention programmes should focus on the full range of stressors, including those of a psychological, sensory, chemical or physical nature, as well as on trauma, accidents and exposure to obvious hazards. Disability can result from repeated exposure to mild stressors or agents, rather than from a single incident. For example, some agents can cause or activate asthma; repeated or loud noises can lead to hearing loss; production pressure, such as piece-rate demands, can cause symptoms of psychological stress; and repetitive motions can lead to cumulative stress disorders (e.g., carpal tunnel syndrome). Exposure to such stressors can exacerbate disabilities that already exist and make them more debilitating.
From a worker’s perspective, the benefits of prevention can never be overshadowed by compensation. Figure 2 lists some of the rights and responsibilities that workers have in relation to disability prevention in the workplace.
Figure 2. Rights and duties - health and safety
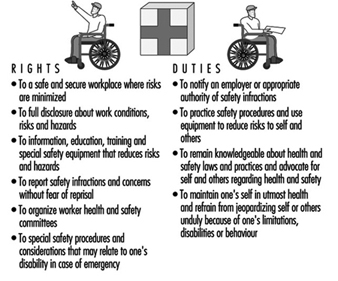
Workers have a right to the safest work environment possible and to the complete disclosure about risks and working conditions. Such knowledge is especially important to workers with disabilities who may need knowledge of certain conditions to determine whether they can perform the job functions without jeopardizing their health and safety or that of others.
Many jobs involve risks or dangers that cannot be fully removed. For example, construction jobs or those that deal with exposure to toxic substances have obvious, inherent risks. Other jobs, like data entry or sewing machine operation, seem relatively safe; however, repetitive motions or improper body mechanics can lead to disabilities. These risks can also be reduced.
All workers should be provided with necessary safety equipment and information on practices and procedures that reduce risk of injury or illness due to exposure to hazardous conditions, repetitive motions or other stressors. Workers must feel free to report/complain about safety practices, or to make suggestions to improve working conditions, without fear of losing their jobs. Workers should be encouraged to report an illness or disability, especially one that is caused or could be exacerbated by the work task or environment.
With regard to duties, workers have a responsibility to practice safety procedures that reduce risks to themselves and others. They must report unsafe conditions, advocate for health and safety issues, and be responsible regarding their health. For example, if a disability or illness places a worker or others at risk, the worker should remove him- or herself from the situation.
The field of ergonomics is emerging, with effective approaches to reducing disabilities incurred as a result of the manner in which the work is organized or performed. Ergonomics is basically the study of work. It involves fitting the job or task to the worker rather than vice versa (AFL-CIO 1992). Ergonomic applications have been used successfully to prevent disability in fields as diverse as agriculture and computers. Some ergonomic applications include flexible workstations that can be adapted to an individual’s height or other physical characteristics (e.g., adjustable office chairs), tools with handles to fit hand differences and simple changes in work routines to reduce repetitive motions or stress to certain parts of the body.
Increasingly, labour unions and employers recognize the need to extend health and safety programmes beyond the workplace. Even when disability or illness is not work-related, employers incur the costs of absenteeism, health insurance and perhaps rehiring and retraining. Further, some illnesses, such as alcoholism, drug addiction and psychological problems, can result in decreased worker productivity or increased vulnerability to on-the-job accidents and stress. For these and other reasons, many enlightened employers are engaging in education about health, safety and disability prevention on and off the job. Wellness programmes that address issues such as stress reduction, good nutrition, smoking cessation and AIDS prevention are being provided in the workplace by unions, management and through joint partnership efforts that may include the government as well.
Some employers provide wellness and employee assistance (counselling and referral) programmes to address these concerns. All of these prevention and health programmes are in the worker’s and employer’s best interests. For example, figures typically show savings-to-investment ratios between 3:1 and 15:1 for some health promotion and employee assistance programmes.
What can labour unions do?
Labour unions are in a unique position to use their leverage as representatives of workers to facilitate health, safety, disability prevention or ergonomics programmes in the workplace. Most prevention and ergonomics experts agree that worker participation and involvement in prevention policies and prescriptions increases the likelihood of their implementation and effectiveness (LaBar 1995; Westlander et al. 1995; AFL-CIO 1992). Labour unions can play a key role in establishing labour-management health and safety councils and ergonomics committees. They can lobby to promote legislation on workplace safety and work with management to establish joint safety committees, which can result in a substantial reduction in job-related accidents (Fletcher et al. 1992).
Labour unions need to educate their members about their rights, regulations and safe practices related to workplace safety and disability prevention on and off the job. Such programmes can become part of the negotiated labour agreement or union-based health and safety committees.
Further, in policy statements and labour agreements and through other mechanisms, labour unions can negotiate disability prevention measures and special conditions for those with disabilities. When a worker becomes disabled, especially if the disability is work-related, the union should support that worker’s right to accommodations, tools or reassignment to prevent exposure to stress or hazardous conditions that can increase the limitation. For example, those with occupationally induced hearing loss must be prevented from continued exposure to certain types of noise.
Examples of what labour unions are doing
The policy statement of the Federation of German Trade Unions concerning employees with disabilities specifically identifies the need to avoid health risks for workers with disabilities and to take measures to prevent them from incurring additional injury.
Under a negotiated labour agreement between the Boeing Aircraft Corporation and the International Association of Machinists and Aerospace Workers (IAMAW), the IAM/Boeing Health and Safety Institute authorizes funding, develops pilot programmes and makes recommendations for improvements related to worker health and safety issues, and manages the return to work of industrially impaired workers. The Institute was established in 1989 and funded by a four cent per hour health and safety trust fund. It is operated by a Board of Directors that is composed of 50% management and 50% union representation.
The Disabled Forestry Workers Foundation of Canada is another example of a joint labour-management project. It evolved from a group of 26 employers, unions and other organizations that collaborated to produce a video (Every Twelve Seconds) to draw attention to the high accident rate among forestry workers in Canada. Now the Foundation focuses on health, safety, accident prevention and workplace models for reintegrating injured workers.
IAM CARES is engaged in an active programme of educating its members on safety issues, particularly in high-risk and hazardous jobs in the chemical industries, the construction trades and the steel industry. It conducts training for shop stewards and line workers, and encourages the formation of safety and health committees that are union-operated and independent of management.
The George Meany Center of the AFL-CIO, with a grant from the US Department of Labor, is developing educational materials on substance abuse to help union members and their families deal with alcohol and drug addictions.
The Association of Flight Attendants (AFA) has done some remarkable work in the area of AIDS and AIDS prevention. Volunteer members have developed the AIDS, Critical and Terminal Illness Awareness Project, which is educating members on AIDS and other life-threatening illnesses. Thirty-three of its locals have educated a total of 10,000 members about AIDS. It has established a foundation to administer funds to members who are also coping with a life-threatening disease.
Issue 3: When a Worker Becomes Disabled—Support, Rehabilitation, Compensation
In many countries, labour unions have fought for workers’ compensation, disability and other benefits related to on-the-job injury. Since one purpose of disability management programmes is to decrease the costs related to these benefits, it may be assumed that labour unions are not in favour of such programmes. In fact, this is not the case. Labour unions support rights related to job protection, early intervention in the provision of rehabilitation services and aspects of sound disability management practice. Disability management programmes that focus on reducing the worker’s suffering, address concerns about work loss, including its financial implications, and try to prevent short- and long-term disability are welcomed. Such programmes should return the worker to his or her job, if feasible, and provide accommodations when necessary. When it is not feasible, alternatives such as reassignment and retraining should be provided. As a last resort, long-term compensation and wage replacement should be guaranteed.
Fortunately, data suggest that disability management programmes can be structured to meet the needs and rights of the workers and still be cost effective for employers. As workers’ compensation costs have skyrocketed in industrialized countries, effective models that incorporate rehabilitation services have been developed and are being evaluated. Unions have a definitive role to play in developing such programmes. They need to promote and protect the rights listed in Figure 3 and educate workers about their duties.
Figure 3. Rights and duties: support, rehabilitation and compensation.

Most of the workers’ rights listed are part of standard return-to-work services for injured workers according to state-of-the-art rehabilitation techniques (Perlman and Hanson 1993). Workers have a right to prompt medical attention and to the assurance that their wages and jobs will be protected. Swift attention and early intervention are found to reduce the time away from work. Withholding benefits can result in refocusing efforts away from rehabilitation and returning to work, and into litigation and animosity towards the employer and the system. Workers need to understand what will happen if they become injured or disabled, and should have a clear understanding of company policy and legal protections. Unfortunately, some systems related to prevention, workers’ compensation and rehabilitation have been fragmented, open to abuse and confusing for those who depend on these systems at a vulnerable time.
Most trade unionists would agree that workers who become disabled gain little if they lose their jobs and their ability to work. Rehabilitation is a desired response to injury or disability and should include early intervention, comprehensive assessment and individualized planning with worker involvement and choice. Return-to-work plans may include returning to work gradually, with accommodation, at reduced hours or in reassigned positions until the worker is ready to return to optimal functioning.
Such accommodations, however, can interfere with the protected rights of workers in general, including those related to seniority. While trade unionists support and protect the rights of disabled workers to return to work, they seek solutions that do not interfere with negotiated seniority clauses or require restructuring of jobs in such a way that other workers are expected to assume new tasks or responsibilities for which they are not responsible or compensated. Collaboration and union involvement are necessary to resolve these issues when they arise, and such circumstances further illustrate the need for labour union involvement in the design and implementation of legislation, disability management and rehabilitation policies and programmes.
What labour unions can do
Labour unions need to be involved in national legislative planning committees related to disability, and in task forces which deal with such issues. Within corporate structures and the workplace, labour unions should help organize joint labour-management committees engaged in developing company-level disability management programmes, and should monitor individual outcomes. Unions can assist with return to work by suggesting accommodations, engaging the assistance of co-workers, and providing assurance to the injured worker.
Labour unions can work cooperatively with employers to develop model disability management programmes that assist workers and meet cost-containment goals. They can engage in research of worker needs, best practices and other activities to determine and protect worker interests. Worker education rights and responsibilities and needed actions are also critical to ensuring the best responses to injury and disability.
Examples of what labour unions have done
Some unions have been active in helping governments address the inadequacies of their systems related to on-the-job injuries and workers’ compensation. In 1988, responding to cost concerns related to injury compensation and to labour union concern over a lack of effective rehabilitation programmes, Australia passed the Commonwealth Employees Rehabilitation and Compensation Act, which provided a new coordination system for managing and preventing workplace illness and injuries of federal workers. The revised system is based on the premise that effective rehabilitation and return to work, if possible, is the most beneficial outcome for the worker and the employer. It incorporates prevention, rehabilitation and compensation into the system. Benefits and jobs are protected while the individual undergoes rehabilitation. Compensation includes wage replacement, medical and related expenses, and in certain instances limited lump sum payments. When individuals are unable to return to work they are adequately remunerated. Early results are demonstrating an 87% return-to-work rate. Success is attributed to many factors, including the collaborative involvement of all stakeholders, including labour unions, in the process.
The IAM/Boeing Health and Safety Institute, already mentioned, provides an example of a labour-management programme that was developed in one corporate setting. The model return-to-work programme was one of the first initiatives taken by the Institute because the needs of industrially injured workers were being neglected by fragmented service-delivery systems administered by federal, state, local and private rehabilitation agencies and programmes. After analysing data and conducting interviews, the union and the corporation set up a model programme that is felt to be in the best interests of both. The programme involves many of the rights already listed: early intervention; quick response with services and compensation requirements; intensive case management focused on return to work with accommodation, if needed; and regular evaluation of the programme’s outcomes and workers’ satisfaction.
Current satisfaction surveys indicate that management and injured workers have found the joint labour-management Return-to-Work Programme an improvement over existing services. The previous programme has been replicated at four additional Boeing plants and the joint programme is expected to become standard practice throughout the company. To date, more than 100,000 injured workers have received rehabilitation services through the programme.
The AFL-CIO’s HRDI programme also offers return-to-work rehabilitation services for workers injured on the job at companies with affiliated union representation. In partnership with Columbia University’s Workplace Center, it administered a demonstration programme called the Early Intervention Program, which sought to determine if early intervention can speed the process of getting workers, who are out of work because of short-term disability, back to the job. The programme returned 65% of participants to work and isolated several factors critical to success. Two findings are of particular significance to this discussion: (1)workers almost universally experience distress related to financial concerns; and (2) the programme’s union affiliation reduced suspicion and hostility.
The Disabled Forestry Workers Foundation of Canada developed a programme it calls the Case Management Model for Workplace Integration. Also using the joint union-management initiative, the programme rehabilitates and reintegrates disabled workers. It has published Industrial Disability Management: An Effective Economic and Human Resource Strategy to assist in the implementation of the model, built on partnership between employers, unions, government and consumers. Further, it has developed the National Institute of Occupational Disability and Research, involving labour, management, educators and rehabilitation professionals. The Institute is developing training programmes for human resource and union representatives that will lead to further implementation of its model.
Issue 4: Inclusion and Integration in the Community and the Workplace
In order for people with disabilities to become fully integrated in the workplace, they must first have equal access to all community resources that predispose and assist people to work (education and training opportunities, social services, etc.) and that give them access to the work environment (accessible housing, transportation, information, etc.). Many labour unions have recognized that people with disabilities are not able to participate in the workplace if they are excluded from full participation in community life. Further, once employed, people with disabilities may need special services and accommodations to be fully integrated or to maintain job performance. Equality in community life is a precursor to employment equity, and to fully address the issue of disability and work, the broader issue of human or civil rights must be considered.
Labour unions have also recognized that to ensure employment equity, sometimes special services or accommodations may be required for job maintenance, and in the spirit of solidarity, may provide such services to their members or promote the provision of such accommodations and services. Figure 4 lists the rights and duties that recognize the need for full access to community life.
Figure 4. Rights and duties: inclusion and integration in the community and the workplace.
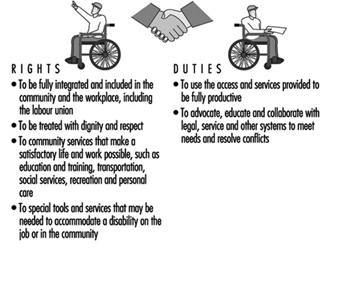
What unions can do
Labour unions can be direct agents of change in their communities by encouraging the total integration of people with disabilities in the workplace and community. Labour unions can reach out to workers with disabilities and the organizations that represent them, and collaborate to take positive action. The opportunities to exert political leverage and affect legislative change have been noted throughout this article, and they are fully in keeping with ILO Recommendation No. 168 and ILO Convention No. 159. Both stress the role of employers’ and workers’ organizations in the formulation of policies related to vocational rehabilitation, and their involvement in the implementation of policy and services.
Labour unions have a responsibility to represent the needs of all their workers. They should provide model services, programmes and representation within the labour union structure to include, accommodate and engage members with disabilities in all aspects of the organization. As some of the following examples will demonstrate, labour unions have used their members as a resource for raising funds, to serve as volunteers or to engage in direct services on the job and in the community to ensure that people with disabilities are fully included in community life and the workplace.
What unions have done
In Germany, a type of advocacy is legally mandated. According to the Severely Disabled Persons Act, any enterprise, including labour unions, that has five or more permanent employees, must have a person who is elected to the staff council as a representative of disabled employees. This representative ensures that the rights and concerns of disabled employees are addressed. Management is required to consult this representative in matters related to general recruitment as well as policy. As a result of this law, labour unions have become actively involved in disability issues.
The Irish Congress of Trade Unions (ICTU) has published and disseminated a Charter of Rights of People with Disabilities (1990), which is a list of 18 fundamental rights considered essential to the full equality of people with disabilities in the workplace and the community at large. It includes the rights to a barrier-free environment, housing, quality health care, education, training, employment and accessible transportation.
In 1946, the IAMAW began to help people with disabilities by establishing the International Guiding Eyes. This programme provides guide dogs and training in how to use them to blind and visually impaired individuals so that they can lead more independent and satisfying lives. Approximately 3,000 individuals from many countries have been helped. Part of the costs to operate the programme are borne by the contributions of union members.
The work of one Japanese labour union has been previously described. Its work was a natural evolution from the work of the Assembly of Trade Unions begun in the 1970s when a union member who had an autistic child requested labour union support to focus on the needs of children with disabilities. The Assembly established a foundation that was supported by the sale of matches and, later, boxes of tissues, by union members. The foundation started a counselling service and a telephone hotline to help parents cope with the challenges of raising a disabled child in a segregated society. As a result, parents became organized and lobbied the government to address accessibility (railways were pressured to improve accessibility, a process that continues today) and to provide educational training and upgrade other services. Summer activities and festivals were sponsored, as well as national and international tours, to foster understanding of disability issues.
After twenty years, when the children grew up, their needs for recreation and education became needs for vocational skills and employment. A vocational experience programme for youth with disabilities was developed and has been in effect for several years. The unions requested companies to provide work experiences for second-year high school students with disabilities. It was out of this programme that the need for the Employment Support Center, noted under Issue 1, became apparent.
Many unions provide extra support services to people with disabilities on the job to assist them in maintaining employment. The Japanese labour unions use on-the-job volunteers to support young people in work-experience programmes with companies that have union representation. IAM CARES in the United States and Canada uses a buddy system to match new employees who have disabilities with a union member who serves as a mentor. IAM CARES also has sponsored supported employment programmes with Boeing and other companies. Supported employment programmes provide job coaches to assist those with the most severe disabilities in learning their jobs and maintaining their performance at productive levels.
Some labour unions have established subcommittees or task forces composed of disabled workers, to ensure that the rights and needs of disabled members are fully represented within the union structure. The American Postal Workers Union is an excellent example of such a task force and the wide implications it can have. In the 1970s, the first deaf shop steward was appointed. Since 1985, several conferences have been held just for hearing-impaired members. These members also serve on negotiating teams to resolve job accommodation and disability management issues. In 1990, the task force worked with the postal service to develop an official stamp depicting the words “I love you” in a hand sign.
Conclusions
Unions, at their most basic level, are about people and their needs. Since the earliest days of labour union activity, unions have done more than fight for fair wages and optimal working conditions. They have sought to improve the quality of life and to maximize opportunities for all workers, including those with disabilities. Although the union perspective emanates from the workplace, the union influence is not limited to enterprises where negotiated labour agreements exist. As many examples in this article demonstrate, labour unions can also affect the larger social environment through a variety of activities and initiatives that are aimed at eliminating discrimination and inequities towards people with disabilities.
While unions, employers, government entities, vocational rehabilitation representatives and men and women with disabilities may have different perspectives, they should share the desire for a healthy and productive workplace. Unions are in a unique position to bring these groups together on common ground, and thereby play a key role in improving the lives of people with disabilities.
Case Study: Best Practices Examples
SABRE Employment (UK)
Mission Statement:To communicate overall objectives/business goals which not only embrace the provision of quality service to applicants, but clearly reflect the desire to provide an efficient recruitment service to employers and which assist employers to improve their capacity to employ people with disabilities. Emphasis should be placed on the primary aim to achieve customer satisfaction. “All of Sabre’s activities begin with our customers. Our goals are to provide recruitment solutions through effective job matching, reliable training and support and to offer expertise in the recruitment and employment of people with disabilities.”
A job fair was recently held to give people a chance to meet employers and learn about different jobs. McDonald’s Restaurants Ltd. ran a workshop on interview skills and also sponsored the job fair event along with Shell and Pizza Hut. There were employer displays which provided an opportunity for employers and prospective employees with learning difficulties to meet in an informal way.
The Coverdale Bursary Programme (UK)
For five years, Coverdale, a small (70 people) management consultancy has offered bursaries to the value of £10,000 per person to disabled individuals seeking high quality management training. These individuals then go into companies like Barclays Bank, the Post Office and Midland Bank for additional training, in a process which promotes long-term attitude change across participating companies. This programme is now being expanded. It has been adapted by The Canadian Council for Rehabilitation and Work.
Brook Street and FYD (UK)
A commercial recruitment agency, Brook Street, and a charity for young deaf people, Friends for the Young Deaf (FYD), have worked in partnership for some years. Brook Street offers work experience and assessment to the young deaf graduates completing the FYD leadership training programme; Brook Street then places appropriate candidates into jobs, charging the same commercial fee they would charge for any candidate.
Employers’ Forum on Disability (UK)
Companies involved in the Employers’ Forum on Disability, an employer-funded association that promotes the integration of disabled persons in the labour market and provides advisory services for interested enterprises, helped disabled entrepreneur Stephen Duckworth to establish his business, Disability Matters, which now offers high quality consultancy and awareness-raising on disability to companies across the UK. Its philosophy encompasses the following:
- to understand and define the business case for employing disabled people
- an authoritative employers’ voice on disability
- employment- and training-related services which are more market led
- to develop new ways to attract qualified disabled applicants and to retain disabled employees
- The key to influencing employers and mobilizing their involvement is to network in a way that:
- promotes the business case through business-to-business communication
- promotes personal contact between employers and disabled individuals
- promotes employer ownership of the issue and an awareness on the part of rehabilitation providers that the employer should be valued as stakeholder, customer and potential partner
- positions disability as part of the wider debate regarding economic and social regeneration, long-term unemployment, poverty and micro and macroeconomic policies
Other examples in the UK: The Employer Forum on Disabilities
Leading UK companies drafted a highly influential policy framework called the “Employers Agenda on Disability, a Ten Point Plan”. This was launched by the Prime Minister and is now publicly supported by more than 100 major firms. It has proven a powerful force for change because it was drafted by the employers themselves in consultation with disability experts. It is now a key tool in helping employers to comply with discrimination legislation.
Supporters of the Agenda are publicly committed to structuring their corporate policy on disability using a 10-point framework addressing the following issues: Equal Opportunities Policy and Procedures Statement; Staff Training and Disability Awareness; The Working Environment; Recruitment; Career Development; Retention, Retraining and Redeployment; Training and Work Experience; People with Disabilities in the Wider Community; Involvement of Disabled People; Monitoring Performance.
The Action File on Disability, a unique manual which provides practical information on how to implement the Agenda, has been produced by the Employers’ Forum on Disability.
Graduate Recruitment:
More than 20 companies are involved in a consortium working with “Workable”, which brokers work-experience opportunities to disabled students in a planned and structured manner.
Twenty-five companies jointly fund an initiative making annual Career Fairs for students accessible for disabled students. The Career Fairs are now wheelchair accessible, and interpreters for the deaf are available, as well as large-print brochures and other support. Employers had experienced such difficulty attracting disabled graduates to apply for jobs using traditional intermediaries that they are now pioneering recruitment methods which speak directly to the disabled students.
HIRED (US)
The project HIRED in San Francisco embodies this new employer orientation. The acronym stands for Helping Industry Recruit Employees with Disabilities. Their literature highlights the services they offer employers:
“Project HIRED is a private, not for profit organization serving the San Francisco Bay area. Our purpose is to assist individuals with disabilities to secure jobs appropriate to their qualifications and career goals. Our services to employers include:
- free referrals, pre-screened, qualified candidates matched to a company’s job openings
- quality temporary employment services at competitive rates
- customized, on site seminars on the technical, legal and interpersonal aspects of disability in the workplace, and
- consultation on all topics related to disabilities in the workplace.
In addition to less formal corporate partnerships, Project HIRED has a corporate membership programme involving approximately 50 Bay Area companies. As corporate members, these companies are entitled to free consulting and a discount on seminars. We are currently exploring additional services, such as library of video resources, to further assist corporate members successfully incorporate people with disabilities in their workforce.”
ASPHI (Italy)
The origins of ASPHI (Associazione per lo Sviluppo di Progetti Informatici per gli Handicappati) go back to the late 1970s when IBM Italy organized courses in computer programming for the visually impaired. A number of companies which had subsequently employed the trainees, together with specialist partner agencies from the non-profit sector, created ASPHI for the physically disabled and the hearing and mentally impaired. The Association involves more than 40 companies which provide financial support, staff and volunteer helpers, advice as well as employment opportunities for ASPHI’s graduates. ASPHI’s objective is to harness information technologies for the social and vocational integration of disadvantaged groups. Its activities include: job training, research and development of new products (mainly software) which facilitate alternative methods of communication, personal autonomy and rehabilitation, and community education, thus breaking down prejudices and discrimination against disabled people. Each year, some 60 young people are qualified by ASPHI. With about 85% of its graduates finding a permanent job, ASPHI’s success has brought it national and international recognition.
Swedish Employers’ Federation Initiative
The Swedish Employers’ Federation Initiative, “Persons with Disabilities in Companies”, positions disability firmly in the labour market debate in the country and conveys the message that disability is an issue of importance to the Swedish Employers Confederation and its members. The Federation states: “The path to employment for persons with disabilities must be made smoother. Requirements for this include:
- clear signals to employers concerning responsibility and costs
- financial compensation for extra costs, if any, incurred by employers who appoint persons with disabilities
- more knowledge of disabilities and the scope of persons with disabilities for changing attitudes and values
- improved cooperation between companies, authorities and individuals to create a dynamic and flexible labour market.”
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."