The History of Occupational Exposure Limits
Over the past 40 years, many organizations in numerous countries have proposed occupational exposure limits (OELs) for airborne contaminants. The limits or guidelines that have gradually become the most widely accepted both in the United States and in most other countries are those issued annually by the American Conference of Governmental Industrial Hygienists (ACGIH), which are termed threshold limit values (TLVs) (LaNier 1984; Cook 1986; ACGIH 1994).
The usefulness of establishing OELs for potentially harmful agents in the working environment has been demonstrated repeatedly since their inception (Stokinger 1970; Cook 1986; Doull 1994). The contribution of OELs to the prevention or minimization of disease is now widely accepted, but for many years such limits did not exist, and even when they did, they were often not observed (Cook 1945; Smyth 1956; Stokinger 1981; LaNier 1984; Cook 1986).
It was well understood as long ago as the fifteenth century, that airborne dusts and chemicals could bring about illness and injury, but the concentrations and lengths of exposure at which this might be expected to occur were unclear (Ramazinni 1700).
As reported by Baetjer (1980), “early in this century when Dr. Alice Hamilton began her distinguished career in occupational disease, no air samples and no standards were available to her, nor indeed were they necessary. Simple observation of the working conditions and the illness and deaths of the workers readily proved that harmful exposures existed. Soon however, the need for determining standards for safe exposure became obvious.”
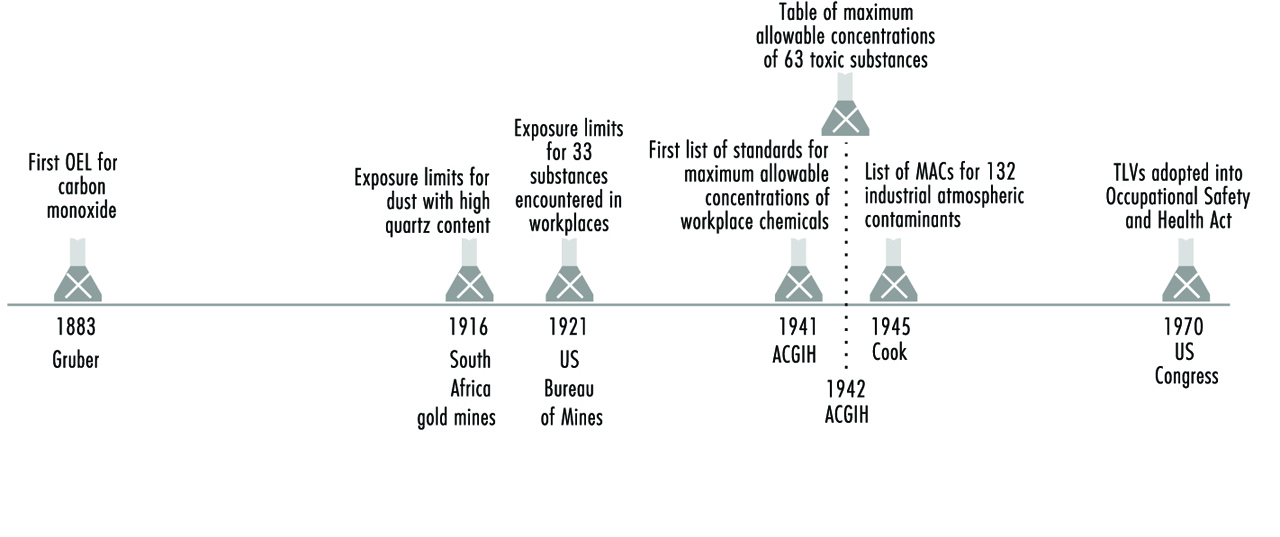
The earliest efforts to set an OEL were directed to carbon monoxide, the toxic gas to which more persons are occupationally exposed than to any other (for a chronology of the development of OELs, see figure 1. The work of Max Gruber at the Hygienic Institute at Munich was published in 1883. The paper described exposing two hens and twelve rabbits to known concentrations of carbon monoxide for up to 47 hours over three days; he stated that “the boundary of injurious action of carbon monoxide lies at a concentration in all probability of 500 parts per million, but certainly (not less than) 200 parts per million”. In arriving at this conclusion, Gruber had also inhaled carbon monoxide himself. He reported no symptoms or uncomfortable sensations after three hours on each of two consecutive days at concentrations of 210 parts per million and 240 parts per million (Cook 1986).
Figure 1. Chronology of occupational exposure levels (OELS).
The earliest and most extensive series of animal experiments on exposure limits were those conducted by K.B. Lehmann and others under his direction. In a series of publications spanning 50 years they reported on studies on ammonia and hydrogen chloride gas, chlorinated hydrocarbons and a large number of other chemical substances (Lehmann 1886; Lehmann and Schmidt-Kehl 1936).
Kobert (1912) published one of the earlier tables of acute exposure limits. Concentrations for 20 substances were listed under the headings: (1) rapidly fatal to man and animals, (2) dangerous in 0.5 to one hour, (3) 0.5 to one hour without serious disturbances and (4) only minimal symptoms observed. In his paper “Interpretations of permissible limits”, Schrenk (1947) notes that the “values for hydrochloric acid, hydrogen cyanide, ammonia, chlorine and bromine as given under the heading ‘only minimal symptoms after several hours’ in the foregoing Kobert paper agree with values as usually accepted in present-day tables of MACs for reported exposures”. However, values for some of the more toxic organic solvents, such as benzene, carbon tetrachloride and carbon disulphide, far exceeded those currently in use (Cook 1986).
One of the first tables of exposure limits to originate in the United States was that published by the US Bureau of Mines (Fieldner, Katz and Kenney 1921). Although its title does not so indicate, the 33 substances listed are those encountered in workplaces. Cook (1986) also noted that most of the exposure limits through the 1930s, except for dusts, were based on rather short animal experiments. A notable exception was the study of chronic benzene exposure by Leonard Greenburg of the US Public Health Service, conducted under the direction of a committee of the National Safety Council (NSC 1926). An acceptable exposure for human beings based on long-term animal experiments was derived from this work.
According to Cook (1986), for dust exposures, permissible limits established before 1920 were based on exposures of workers in the South African gold mines, where the dust from drilling operations was high in crystalline free silica. In 1916, an exposure limit of 8.5 million particles per cubic foot of air (mppcf) for the dust with an 80 to 90% quartz content was set (Phthisis Prevention Committee 1916). Later, the level was lowered to 5 mppcf. Cook also reported that, in the United States, standards for dust, also based on exposure of workers, were recommended by Higgins and co-workers following a study at the south-western Missouri zinc and lead mines in 1917. The initial level established for high quartz dusts was ten mppcf, appreciably higher than was established by later dust studies conducted by the US Public Health Service. In 1930, the USSR Ministry of Labour issued a decree that included maximum allowable concentrations for 12 industrial toxic substances.
The most comprehensive list of occupational exposure limits up to 1926 was for 27 substances (Sayers 1927). In 1935 Sayers and Dalle Valle published physiological responses to five concentrations of 37 substances, the fifth being the maximum allowable concentration for prolonged exposure. Lehmann and Flury (1938) and Bowditch et al. (1940) published papers that presented tables with a single value for repeated exposures to each substance.
Many of the exposure limits developed by Lehmann were included in a monograph initially published in 1927 by Henderson and Haggard (1943), and a little later in Flury and Zernik’s Schadliche Gase (1931). According to Cook (1986), this book was considered the authoritative reference on effects of injurious gases, vapours and dusts in the workplace until Volume II of Patty’s Industrial Hygiene and Toxicology (1949) was published.
The first lists of standards for chemical exposures in industry, called maximum allowable concentrations (MACs), were prepared in 1939 and 1940 (Baetjer 1980). They represented a consensus of opinion of the American Standard Association and a number of industrial hygienists who had formed the ACGIH in 1938. These “suggested standards” were published in 1943 by James Sterner. A committee of the ACGIH met in early 1940 to begin the task of identifying safe levels of exposure to workplace chemicals, by assembling all the data which would relate the degree of exposure to a toxicant to the likelihood of producing an adverse effect (Stokinger 1981; LaNier 1984). The first set of values were released in 1941 by this committee, which was composed of Warren Cook, Manfred Boditch (reportedly the first hygienist employed by industry in the United States), William Fredrick, Philip Drinker, Lawrence Fairhall and Alan Dooley (Stokinger 1981).
In 1941, a committee (designated as Z-37) of the American Standards Association, which later became the American National Standards Institute, developed its first standard of 100 ppm for carbon monoxide. By 1974 the committee had issued separate bulletins for 33 exposure standards for toxic dusts and gases.
At the annual meeting of the ACGIH in 1942, the newly appointed Subcommittee on Threshold Limits presented in its report a table of 63 toxic substances with the “maximum allowable concentrations of atmospheric contaminants” from lists furnished by the various state industrial hygiene units. The report contains the statement, “The table is not to be construed as recommended safe concentrations. The material is presented without comment” (Cook 1986).
In 1945 a list of 132 industrial atmospheric contaminants with maximum allowable concentrations was published by Cook, including the then current values for six states, as well as values presented as a guide for occupational disease control by federal agencies and maximum allowable concentrations that appeared best supported by the references on original investigations (Cook 1986).
At the 1946 annual meeting of ACGIH, the Subcommittee on Threshold Limits presented their second report with the values of 131 gases, vapours, dusts, fumes and mists, and 13 mineral dusts. The values were compiled from the list reported by the subcommittee in 1942, from the list published by Warren Cook in Industrial Medicine (1945) and from published values of the Z-37 Committee of the American Standards Association. The committee emphasized that the “list of M.A.C. values is presented … with the definite understanding that it be subject to annual revision.”
Intended use of OELs
The ACGIH TLVs and most other OELs used in the United States and some other countries are limits which refer to airborne concentrations of substances and represent conditions under which “it is believed that nearly all workers may be repeatedly exposed day after day without adverse health effects” (ACGIH 1994). (See table 1). In some countries the OEL is set at a concentration which will protect virtually everyone. It is important to recognize that unlike some exposure limits for ambient air pollutants, contaminated water, or food additives set by other professional groups or regulatory agencies, exposure to the TLV will not necessarily prevent discomfort or injury for everyone who is exposed (Adkins et al. 1990). The ACGIH recognized long ago that because of the wide range in individual susceptibility, a small percentage of workers may experience discomfort from some substances at concentrations at or below the threshold limit and that a smaller percentage may be affected more seriously by aggravation of a pre-existing condition or by development of an occupational illness (Cooper 1973; ACGIH 1994). This is clearly stated in the introduction to the ACGIH’s annual booklet Threshold Limit Values for Chemical Substances and Physical Agents and Biological Exposure Indices (ACGIH 1994).
Table 1. Occupational exposure limits (OELs) in various countries (as of 1986)
|
Country/Province |
Type of standard |
|
Argentina |
OELs are essentially the same as those of the 1978 ACGIH TLVs. The principal difference from the ACGIH list is that, for the 144 substances (of the total of 630) for which no STELs are listed by ACGIH, the values used for the Argentina TWAs are entered also under this heading. |
|
Australia |
The National Health and Medical Research Council (NHMRC) adopted a revised edition of the Occupational Health Guide Threshold Limit Values (1990-91) in 1992. The OELs have no legal status in Australia, except where specifically incorporated into law by reference. The ACGIHTLVs are published in Australia as an appendix to the occupational health guides, revised with the ACGIH revisions in odd-numbered years. |
|
Austria |
The values recommended by the Expert Committee of the Worker Protection Commission for Appraisal of MAC (maximal acceptable concentration) Values in cooperation with the General Accident Prevention Institute of the Chemical Workers Trade Union, is considered obligatory by the Federal Ministry for Social Administration. They are applied by the Labour Inspectorate under the Labour Protection Law. |
|
Belgium |
The Administration of Hygiene and Occupational Medicine of the Ministry of Employment and of Labour uses the TLVs of the ACGIH as a guideline. |
|
Brazil |
The TLVs of the ACGIH have been used as the basis for the occupational health legislation of Brazil since 1978. As the Brazilian work week is usually 48 hours, the values of the ACGIH were adjusted in conformity with a formula developed for this purpose. The ACGIH list was adopted only for those air contaminants which at the time had nationwide application. The Ministry of Labour has brought the limits up to date with establishment of values for additional contaminants in accordance with recommendations from the Fundacentro Foundation of Occupational Safety and Medicine. |
|
Canada (and Provinces) |
Each province has its own regulations: |
|
Alberta |
OELs are under the Occupational Health and Safety Act, Chemical Hazard Regulation, which requires the employer to ensure that workers are not exposed above the limits. |
|
British Columbia |
The Industrial Health and Safety Regulations set legal requirements for most of British Columbia industry, which refer to the current schedule of TLVs for atmospheric contaminants published by the ACGIH. |
|
Manitoba |
The Department of Environment and Workplace Safety and Health is responsible for legislation and its administration concerning the OELs. The guidelines currently used to interpret risk to health are the ACGIH TLVs with the exception that carcinogens are given a zero exposure level “so far as is reasonably practicable”. |
|
New Brunswick |
The applicable standards are those published in the latest ACGIH issue and, in case of an infraction, it is the issue in publication at the time of infraction that dictates compliance. |
|
Northwest Territories |
The Northwest Territories Safety Division of the Justice and Service Department regulates workplace safety for non-federal employees under the latest edition of the ACGIH TLVs. |
|
Nova Scotia |
The list of OELs is the same as that of the ACGIH as published in 1976 and its subsequent amendments and revisions. |
|
Ontario |
Regulations for a number of hazardous substances are enforced under the Occupational Health and Safety Act, published each in a separate booklet that includes the permissible exposure level and codes for respiratory equipment, techniques for measuring airborne concentrations and medical surveillance approaches. |
|
Quebec |
Permissible exposure levels are similar to the ACGIH TLVs and compliance with the permissible exposure levels for workplace air contaminants is required. |
|
Chile |
The maximum concentration of eleven substances having the capacity of causing acute, severe or fatal effects cannot be exceeded for even a moment. The values in the Chile standard are those of the ACGIH TLVs to which a factor of 0.8 is applied in view of the 48-hour week. |
|
Denmark |
OELs include values for 542 chemical substances and 20 particulates. It is legally required that these not be exceeded as time-weighted averages. Data from the ACGIH are used in the preparation of the Danish standards. About 25 per cent of the values are different from those of ACGIH with nearly all of these being somewhat more stringent. |
|
Ecuador |
Ecuador does not have a list of permissible exposure levels incorporated in its legislation. The TLVs of the ACGIH are used as a guide for good industrial hygiene practice. |
|
Finland |
OELs are defined as concentrations that are deemed to be hazardous to at least some workers on long-term exposure. Whereas the ACGIH has as their philosophy that nearly all workers may be exposed to substances below the TLV without adverse effect, the viewpoint in Finland is that where exposures are above the limiting value, deleterious effects on health may occur. |
|
Germany |
The MAC value is “the maximum permissible concentration of a chemical compound present in the air within a working area (as gas, vapour, particulate matter) which, according to current knowledge, generally does not impair the health of the employee nor cause undue annoyance. Under these conditions, exposure can be repeated and of long duration over a daily period of eight hours, constituting an average work week of 40 hours (42 hours per week as averaged over four successive weeks for firms having four work shifts).- Scientifically based criteria for health protection, rather than their technical or economical feasibility, are employed.” |
|
Ireland |
The latest TLVs of the ACGIH are normally used. However, the ACGIH list is not incorporated in the national laws or regulations. |
|
Netherlands |
MAC values are taken largely from the list of the ACGIH, as well as from the Federal Republic of Germany and NIOSH. The MAC is defined as “that concentration in the workplace air which, according to present knowledge, after repeated long-term exposure even up to a whole working life, in general does not harm the health of workers or their offspring.” |
|
Philippines |
The 1970 TLVs of the ACGIH are used, except 50 ppm for vinyl chloride and 0.15 mg/m(3) for lead, inorganic compounds, fume and dust. |
|
Russian Federation |
The former USSR established many of its limits with the goal of eliminating any possibility for even reversible effects. Such subclinical and fully reversible responses to workplace exposures have, thus far, been considered too restrictive to be useful in the United States and in most other countries. In fact, due to the economic and engineering difficulties in achieving such low levels of air contaminants in the workplace, there is little indication that these limits have actually been achieved in countries which have adopted them. Instead, the limits appear to serve more as idealized goals rather than limits which manufacturers are legally bound or morally committed to achieve. |
|
United States |
At least six groups recommend exposure limits for the workplace: the TLVs of the ACGIH, the Recommended Exposure Limits (RELs) suggested by the National Institute for Occupational Safety and Health (NIOSH), the Workplace Environment Exposure Limits (WEEL) developed by the American Industrial Hygiene Association (AIHA), standards for workplace air contaminants suggested by the Z-37 Committee of the American National Standards Institute (EAL), the proposed workplace guides of the American Public Health Association (APHA 1991), and recommendations by local, state or regional governments. In addition, permissible exposure limits (PELs), which are regulations that must be met in the workplace because they are law, have been promulgated by the Department of Labor and are enforced by the Occupational Safety and Health Administration (OSHA). |
Source: Cook 1986.
This limitation, although perhaps less than ideal, has been considered a practical one since airborne concentrations so low as to protect hypersusceptibles have traditionally been judged infeasible due to either engineering or economic limitations. Until about 1990, this shortcoming in the TLVs was not considered a serious one. In light of the dramatic improvements since the mid-1980s in our analytical capabilities, personal monitoring/sampling devices, biological monitoring techniques and the use of robots as a plausible engineering control, we are now technologically able to consider more stringent occupational exposure limits.
The background information and rationale for each TLV are published periodically in the Documentation of the Threshold Limit Values (ACGIH 1995). Some type of documentation is occasionally available for OELs set in other countries. The rationale or documentation for a particular OEL should always be consulted before interpreting or adjusting an exposure limit, as well as the specific data that were considered in establishing it (ACGIH 1994).
TLVs are based on the best available information from industrial experience and human and animal experimental studies—when possible, from a combination of these sources (Smith and Olishifski 1988; ACGIH 1994). The rationale for choosing limiting values differs from substance to substance. For example, protection against impairment of health may be a guiding factor for some, whereas reasonable freedom from irritation, narcosis, nuisance or other forms of stress may form the basis for others. The age and completeness of the information available for establishing occupational exposure limits also varies from substance to substance; consequently, the precision of each TLV is different. The most recent TLV and its documentation (or its equivalent) should always be consulted in order to evaluate the quality of the data upon which that value was set.
Even though all of the publications which contain OELs emphasize that they were intended for use only in establishing safe levels of exposure for persons in the workplace, they have been used at times in other situations. It is for this reason that all exposure limits should be interpreted and applied only by someone knowledgeable of industrial hygiene and toxicology. The TLV Committee (ACGIH 1994) did not intend that they be used, or modified for use:
- as a relative index of hazard or toxicity
- in the evaluation of community air pollution
- for estimating the hazards of continuous, uninterrupted exposures or other extended work periods
- as proof or disproof of an existing disease or physical condition
- for adoption by countries whose working conditions differ from those of the United States.
The TLV Committee and other groups which set OELs warn that these values should not be “directly used” or extrapolated to predict safe levels of exposure for other exposure settings. However, if one understands the scientific rationale for the guideline and the appropriate approaches for extrapolating data, they can be used to predict acceptable levels of exposure for many different kinds of exposure scenarios and work schedules (ACGIH 1994; Hickey and Reist 1979).
Philosophy and approaches in setting exposure limits
TLVs were originally prepared to serve only for the use of industrial hygienists, who could exercise their own judgement in applying these values. They were not to be used for legal purposes (Baetjer 1980). However, in 1968 the United States Walsh-Healey Public Contract Act incorporated the 1968 TLV list, which covered about 400 chemicals. In the United States, when the Occupational Safety and Health Act (OSHA) was passed it required all standards to be national consensus standards or established federal standards.
Exposure limits for workplace air contaminants are based on the premise that, although all chemical substances are toxic at some concentration when experienced for a period of time, a concentration (e.g., dose) does exist for all substances at which no injurious effect should result no matter how often the exposure is repeated. A similar premise applies to substances whose effects are limited to irritation, narcosis, nuisance or other forms of stress (Stokinger 1981; ACGIH 1994).
This philosophy thus differs from that applied to physical agents such as ionizing radiation, and for some chemical carcinogens, since it is possible that there may be no threshold or no dose at which zero risk would be expected (Stokinger 1981). The issue of threshold effects is controversial, with reputable scientists arguing both for and against threshold theories (Seiler 1977; Watanabe et al. 1980, Stott et al. 1981; Butterworth and Slaga 1987; Bailer et al. 1988; Wilkinson 1988; Bus and Gibson 1994). With this in mind, some occupational exposure limits proposed by regulatory agencies in the early 1980s were set at levels which, although not completely without risk, posed risks that were no greater than classic occupational hazards such as electrocution, falls, and so on. Even in those settings which do not use industrial chemicals, the overall workplace risks of fatal injury are about one in one thousand. This is the rationale that has been used to justify selecting this theoretical cancer risk criterion for setting TLVs for chemical carcinogens (Rodricks, Brett and Wrenn 1987; Travis et al. 1987).
Occupational exposure limits established both in the United States and elsewhere are derived from a wide variety of sources. The 1968 TLVs (those adopted by OSHA in 1970 as federal regulations) were based largely on human experience. This may come as a surprise to many hygienists who have recently entered the profession, since it indicates that, in most cases, the setting of an exposure limit has come after a substance has been found to have toxic, irritational or otherwise undesirable effects on humans. As might be anticipated, many of the more recent exposure limits for systemic toxins, especially those internal limits set by manufacturers, have been based primarily on toxicology tests conducted on animals, in contrast to waiting for observations of adverse effects in exposed workers (Paustenbach and Langner 1986). However, even as far back as 1945, animal tests were acknowledged by the TLV Committee to be very valuable and they do, in fact, constitute the second most common source of information upon which these guidelines have been based (Stokinger 1970).
Several approaches for deriving OELs from animal data have been proposed and put into use over the past 40 years. The approach used by the TLV Committee and others is not markedly different from that which has been used by the US Food and Drug Administration (FDA) in establishing acceptable daily intakes (ADI) for food additives. An understanding of the FDA approach to setting exposure limits for food additives and contaminants can provide good insight to industrial hygienists who are involved in interpreting OELs (Dourson and Stara 1983).
Discussions of methodological approaches which can be used to establish workplace exposure limits based exclusively on animal data have also been presented (Weil 1972; WHO 1977; Zielhuis and van der Kreek 1979a, 1979b; Calabrese 1983; Dourson and Stara 1983; Leung and Paustenbach 1988a; Finley et al. 1992; Paustenbach 1995). Although these approaches have some degree of uncertainty, they seem to be much better than a qualitative extrapolation of animal test results to humans.
Approximately 50% of the 1968 TLVs were derived from human data, and approximately 30% were derived from animal data. By 1992, almost 50% were derived primarily from animal data. The criteria used to develop the TLVs may be classified into four groups: morphological, functional, biochemical and miscellaneous (nuisance, cosmetic). Of those TLVs based on human data, most are derived from effects observed in workers who were exposed to the substance for many years. Consequently, most of the existing TLVs have been based on the results of workplace monitoring, compiled with qualitative and quantitative observations of the human response (Stokinger 1970; Park and Snee 1983). In recent times, TLVs for new chemicals have been based primarily on the results of animal studies rather than human experience (Leung and Paustenbach 1988b; Leung et al. 1988).
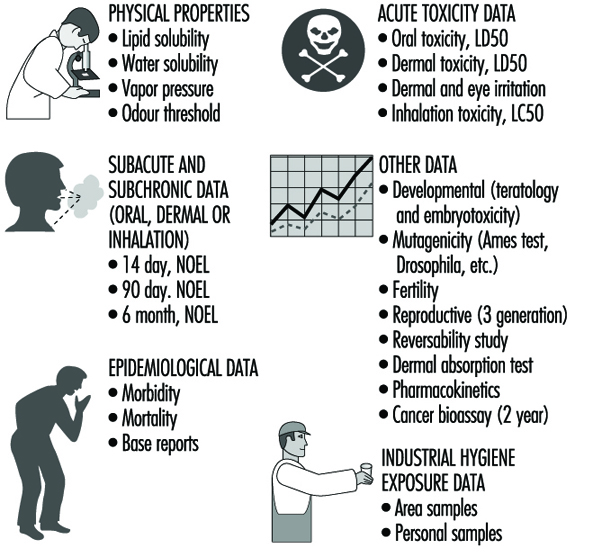
It is noteworthy that in 1968 only about 50% of the TLVs were intended primarily to prevent systemic toxic effects. Roughly 40% were based on irritation and about two per cent were intended to prevent cancer. By 1993, about 50% were meant to prevent systemic effects, 35% to prevent irritation, and five per cent to prevent cancer. Figure 2 provides a summary of the data often used in developing OELs.
Figure 2. Data often used in developing an occupational exposure.
Limits for irritants
Prior to 1975, OELs designed to prevent irritation were largely based on human experiments. Since then, several experimental animal models have been developed (Kane and Alarie 1977; Alarie 1981; Abraham et al. 1990; Nielsen 1991). Another model based on chemical properties has been used to set preliminary OELs for organic acids and bases (Leung and Paustenbach 1988).
Limits for carcinogens
In 1972, the ACGIH Committee began to distinguish between human and animal carcinogens in its TLV list. According to Stokinger (1977), one reason for this distinction was to assist the stakeholders in discussions (union representatives, workers and the public) in focusing on those chemicals with more probable workplace exposures.
Do the TLVs Protect Enough Workers?
Beginning in 1988, concerns were raised by numerous persons regarding the adequacy or health protectiveness of TLVs. The key question raised was, what percentage of the working population is truly protected from adverse health effects when exposed to the TLV?
Castleman and Ziem (1988) and Ziem and Castleman (1989) argued both that the scientific basis of the standards was inadequate and that they were formulated by hygienists with vested interests in the industries being regulated.
These papers engendered an enormous amount of discussion, both supportive of and opposed to the work of the ACGIH (Finklea 1988; Paustenbach 1990a, 1990b, 1990c; Tarlau 1990).
A follow-up study by Roach and Rappaport (1990) attempted to quantify the safety margin and scientific validity of the TLVs. They concluded that there were serious inconsistencies between the scientific data available and the interpretation given in the 1976 Documentation by the TLV Committee. They also note that the TLVs were probably reflective of what the Committee perceived to be realistic and attainable at the time. Both the Roach and Rappaport and the Castleman and Ziem analyses have been responded to by the ACGIH, who have insisted on the inaccuracy of the criticisms.
Although the merit of the Roach and Rappaport analysis, or for that matter, that of Ziem and Castleman, will be debated for a number of years, it is clear that the process by which TLVs and other OELs will be set will probably never be as it was between 1945 and 1990. It is likely that in coming years, the rationale, as well as the degree of risk inherent in a TLV, will be more explicitly described in the documentation for each TLV. Also, it is certain that the definition of “virtually safe” or “insignificant risk” with respect to workplace exposure will change as the values of society change (Paustenbach 1995, 1997).
The degree of reduction in TLVs or other OELs that will undoubtedly occur in the coming years will vary depending on the type of adverse health effect to be prevented (central nervous system depression, acute toxicity, odour, irritation, developmental effects, or others). It is unclear to what degree the TLV committee will rely on various predictive toxicity models, or what risk criteria they will adopt, as we enter the next century.
Standards and Nontraditional Work Schedules
The degree to which shift work affects a worker’s capabilities, longevity, mortality, and overall well-being is still not well understood. So-called nontraditional work shifts and work schedules have been implemented in a number of industries in an attempt to eliminate, or at least reduce, some of the problems caused by normal shift work, which consists of three eight-hour work shifts per day. One kind of work schedule which is classified as nontraditional is the type involving work periods longer than eight hours and varying (compressing) the number of days worked per week (e.g., a 12-hours-per-day, three-day workweek). Another type of nontraditional work schedule involves a series of brief exposures to a chemical or physical agent during a given work schedule (e.g., a schedule where a person is exposed to a chemical for 30 minutes, five times per day with one hour between exposures). The last category of nontraditional schedule is that involving the “critical case” wherein persons are continuously exposed to an air contaminant (e.g., spacecraft, submarine).
Compressed workweeks are a type of nontraditional work schedule that has been used primarily in non-manufacturing settings. It refers to full-time employment (virtually 40 hours per week) which is accomplished in less than five days per week. Many compressed schedules are currently in use, but the most common are: (a) four-day workweeks with ten-hour days; (b) three-day workweeks with 12-hour days; (c) 4-1/2–day workweeks with four nine-hour days and one four-hour day (usually Friday); and (d) the five/four, nine plan of alternating five-day and four-day workweeks of nine-hour days (Nollen and Martin 1978; Nollen 1981).
Of all workers, those on nontraditional schedules represent only about 5% of the working population. Of this number, only about 50,000 to 200,000 Americans who work nontraditional schedules are employed in industries where there is routine exposure to significant levels of airborne chemicals. In Canada, the percentage of chemical workers on nontraditional schedules is thought to be greater (Paustenbach 1994).
One Approach to Setting International OELs
As noted by Lundberg (1994), a challenge facing all national committees is to identify a common scientific approach to setting OELs. Joint international ventures are advantageous to the parties involved since writing criteria documents is both a time- and cost-consuming process (Paustenbach 1995).
This was the idea when the Nordic Council of Ministers in 1977 decided to establish the Nordic Expert Group (NEG). The task of the NEG was to develop scientifically-based criteria documents to be used as a common scientific basis of OELs by the regulatory authorities in the five Nordic countries (Denmark, Finland, Iceland, Norway and Sweden). The criteria documents from the NEG lead to the definition of a critical effect and dose-response/dose-effect relationships. The critical effect is the adverse effect that occurs at the lowest exposure. There is no discussion of safety factors and a numerical OEL is not proposed. Since 1987, criteria documents are published by the NEG concurrently in English on a yearly basis.
Lundberg (1994) has suggested a standardized approach that each county would use. He suggested building a document with the following characteristics:
- A standardized criteria document should reflect the up-to-date knowledge as presented in the scientific literature.
- The literature used should preferably be peer-reviewed scientific papers but at least be available publicly. Personal communications should be avoided. An openness toward the general public, particularly workers, decreases the kind of suspiciousness that recently has been addressed toward documentation from the ACGIH.
- The scientific committee should consist of independent scientists from academia and government. If the committee should include scientific representatives from the labour market, both employers and employees should be represented.
- All relevant epidemiological and experimental studies should be thoroughly scrutinized by the scientific committee, especially “key studies” that present data on the critical effect. All observed effects should be described.
- Environmental and biological monitoring possibilities should be pointed out. It is also necessary to thoroughly scrutinize these data, including toxicokinetic data.
- Data permitting, the establishment of dose-response and dose-effect relationships should be stated. A no observable effect level (NOEL) or lowest observable effect level (LOEL) for each observed effect should be stated in the conclusion. If necessary, reasons should be given as to why a certain effect is the critical one. The toxicological significance of an effect is thereby considered.
- Specifically, mutagenic, carcinogenic and teratogenic properties should be pointed out as well as allergic and immunological effects.
- A reference list for all studies described should be given. If it is stated in the document that only relevant studies have been used, there is no need to give a list of references not used or why. On the other hand, it could be of interest to list those databases that have been used in the literature search.
There are in practice only minor differences in the way OELs are set in the various countries that develop them. It should, therefore, be relatively easy to agree upon the format of a standardized criteria document containing the key information. From this point, the decision as to the size of the margin of safety that is incorporated in the limit would then be a matter of national policy.