- You are here:
-
Home

-
Part XII. Chemical Industries
-
Chemical Processing
- Examples of Chemical Processing Operations
Role of the Employee Health Service in Preventive Programmes
The primary functions of the employee health service are treatment of acute injuries and illnesses occurring in the workplace, conducting fitness-to-work examinations (Cowell 1986) and the prevention, detection and treatment of work-related injuries and illnesses. However, it may also play a significant role in preventive and health maintenance programs. In this article, particular attention will be paid to the “hands on” services that this corporate unit may provide in this connection.
Since its inception, the employee health unit has served as a focal point for prevention of non-occupational health problems. Traditional activities have included distribution of health education materials; the production of health promotion articles by staff members for publication in company periodicals; and, perhaps most important, seeing to it that occupational physicians and nurses remain alert to the advisability of preventive health counseling in the course of encounters with employees with incidentally observed potential or emerging health problems. Periodic health surveillance examinations for potential effects of occupational hazards have frequently demonstrated an incipient or early non-occupational health problem.
The medical director is strategically situated to play a central role in the organization’s preventive programs. Significant advantages attaching to this position include the opportunity to build preventive components into work-related services, the generally high regard of employees, and already established relationships with high-level managers through which desirable changes in work structure and environment can be implemented and the resources for an effective prevention program obtained.
In some instances, non-occupational preventive programs are placed elsewhere in the organization, for example, in the personnel or human resources departments. This is generally unwise but may be necessary when, for example, these programs are provided by different outside contractors. Where such separation does exist, there should at least be coordination and close collaboration with the employee health service.
Depending upon the nature and location of the worksite and the organization’s commitment to prevention, these services may be very comprehensive, covering virtually all aspects of health care, or they may be quite minimal, providing only limited health information materials. Comprehensive programs are desirable when the worksite is located in an isolated area where community-based services are lacking; in such situations, the employer must provide extensive health care services, often to employees’ dependants as well, to attract and retain a loyal, healthy and productive workforce. The other end of the spectrum is usually found in situations where there is a strong community-based health care system or where the organization is small, poorly resourced or, regardless of size, indifferent to the health and welfare of the workforce.
In what follows, neither of these extremes will be the subject of consideration; instead, attention will be focused on the more common and desirable situation where the activities and programs provided by the employee health unit complement and supplement services provided in the community.
Organization of Preventive Services
Typically, worksite preventive services include health education and training, periodic health assessments and examinations, screening programs for particular health problems, and health counseling.
Participation in any of these activities should be viewed as voluntary, and any individual findings and recommendations must be held confidential between the employee health staff and the employee, although, with the consent of the employee, reports may be forwarded to his or her personal physician. To operate otherwise is to preclude any program from ever being truly effective. Hard lessons have been learned and are continuing to be learned about the importance of such considerations. Programs which do not enjoy employees’ credibility and trust will have no or only half-hearted participation. And if the programs are perceived as being offered by management in some self-serving or manipulative way, they have little chance of achieving any good.
Worksite preventive health services ideally are provided by staff attached to the employee health unit, often in collaboration with an in-house employee education department (where one exists). When the staff lacks time or the necessary expertise or when special equipment is required (e.g., with mammography), the services may be obtained by contracting with an outside provider. Reflecting the peculiarities of some organizations, such contracts are sometimes arranged by a manager outside the employee health unit—this is often the case in decentralized organizations when such service contracts are negotiated with community-based providers by the local plant managers. However, it is desirable that the medical director be responsible for setting out the framework of the contract, verifying the capabilities of potential providers and monitoring their performance. In such instances, while aggregate reports may be provided to management, individual results should be forwarded to and retained by the employee health service or maintained in sequestered confidential files by the contractor. At no time should such health information be allowed to form part of the employee’s human resources file. One of the great advantages of having an occupational health unit is not only being able to keep health records separate from other company records under the supervision of an occupational health professional but, also, the opportunity to use this information as the basis of a discreet follow-up to be sure that important medical recommendations are not ignored. Ideally, the employee health unit, where possible in concert with the employee’s personal physician, will provide or oversee the provision of recommended diagnostic or therapeutic services. Other members of the employee health service staff, such as physical therapists, massage therapists, exercise specialists, nutritionists, psychologists and health counselors will also lend their special expertise as required.
The health promotion and protection activities of the employee health unit must complement its primary role of preventing and handling work-related injury and illness. When properly introduced and managed, they will greatly enhance the basic occupational health and safety program but at no time should they displace or dominate it. Placing responsibility for the preventive health services in the employee health unit will facilitate the seamless integration of both programs and make for optimal utilization of critical resources.
Program Elements
Education and training
The goal here is informing and motivating employees—and their dependants—to select and maintain a healthier lifestyle. The intent is to empower the employees to change their own health behavior so they will live longer, healthier, more productive and enjoyable lives.
A variety of communication techniques and presentation styles may be used. A series of attractive, easy-to-read pamphlets can be very useful where there are budget constraints. They may be offered in waiting-room racks, distributed by company mail, or mailed to employees’ homes. They are perhaps most useful when handed to the employee as a particular health issue is being discussed. The medical director or the person directing the preventive program must take pains to be sure that their content is accurate, relevant and presented in language and terms understood by the employees (separate editions may be required for different cohorts of a diverse workforce).
In-plant meetings may be arranged for presentations by employee health staff or invited speakers on health topics of interest. “Brown bag” lunch hour meetings (i.e., employees bring picnic lunches to the meeting and eat while they listen) are a popular mechanism for holding such meetings without interfering with work schedules. Small interactive focus groups led by a well-informed health professional are especially beneficial for workers sharing a particular health problem; peer pressure often constitutes a powerful motivation for compliance with health recommendations. One-on-one counseling, of course, is excellent but very labor-intensive and should be reserved for special situations only. However, access to a source of reliable information should always be available to employees who may have questions.
Topics may include smoking cessation, stress management, alcohol and drug consumption, nutrition and weight control, immunizations, travel advice and sexually-transmitted diseases. Special emphasis is often given to controlling such risk factors for cardiovascular and heart disease as hypertension and abnormal blood lipid patterns. Other topics often covered include cancer, diabetes, allergies, self-care for common minor ailments, and safety in the home and on the road.
Certain topics lend themselves to active demonstration and participation. These include training in cardiopulmonary resuscitation, first aid training, exercises to prevent repetitive strain and back pain, relaxation exercises, and self-defense instruction, especially popular among women.
Finally, periodic health fairs with exhibits by local voluntary health agencies and booths offering mass screening procedures are a popular way of generating excitement and interest.
Periodic medical examinations
In addition to the required or recommended periodic health surveillance examinations for employees exposed to particular work or environmental hazards, many employee health units offer more or less comprehensive periodic medical check-ups. Where personnel and equipment resources are limited, arrangements may be made to have them performed, often at the employer’s expense, by local facilities or in private physicians’ offices (i.e., by contractors). For worksites in communities where such services are not available, arrangements may be made for a vendor to bring a mobile examination unit into the plant or set up examination vans in the parking area.
Originally, in most organizations, these examinations were made available only to executives and senior managers. In some, they were extended down into the ranks to employees who had rendered a required number of years of service or who had a known medical problem. They frequently included a complete medical history and physical examination supplemented by an extensive battery of laboratory tests, x-ray examinations, electrocardiograms and stress tests, and exploration of all available body orifices. As long as the company was willing to pay their fees, examination facilities with an entrepreneurial bent were quick to add tests as new technology became available. In organizations prepared to offer even more elaborate service, the examinations were provided as part of a short stay at a popular health resort. While they often turned up important and useful findings, false positives were also frequent and, to say the least, examinations conducted in these surroundings were expensive.
In recent decades, reflecting growing economic pressures, a trend toward egalitarianism and, particularly, the marshalling of evidence regarding the advisability and utility of the different elements in these examinations, have led to their being simultaneously made more widely available in the workforce and less comprehensive.
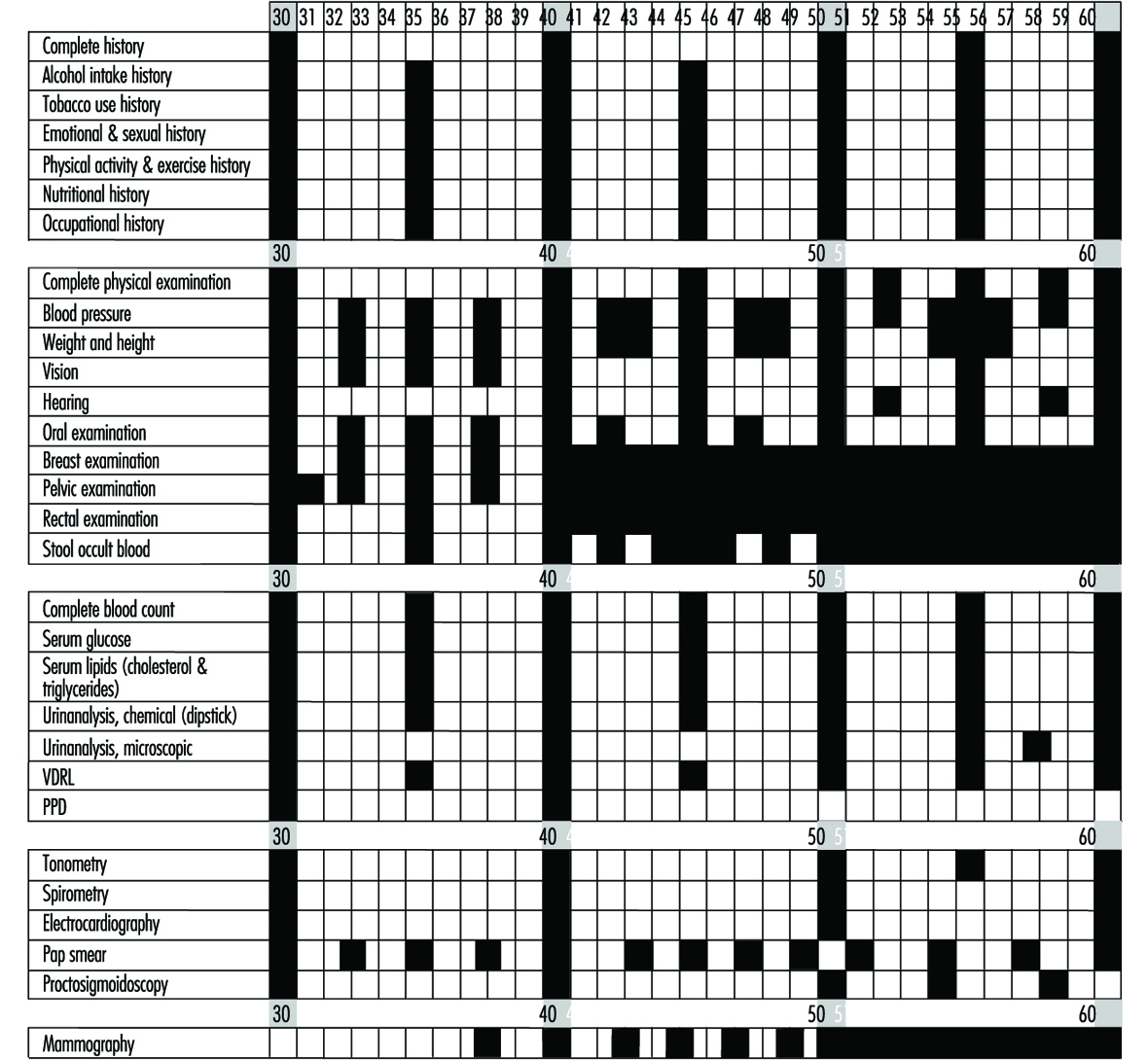
The US Preventive Services Task Force published an assessment of the effectiveness of 169 preventive interventions (1989). Figure 1 presents a useful lifetime schedule of preventive examinations and tests for healthy adults in low-risk managerial positions (Guidotti, Cowell and Jamieson 1989) Thanks to such efforts, periodic medical examinations are becoming less costly and more efficient.
Figure 1. Lifetime health monitoring programme.
Periodic health screening
These programs are designed to detect as early as possible health conditions or actual disease processes which are amenable to early intervention for cure or control and to detect early signs and symptoms associated with poor lifestyle habits, which if changed will prevent or delay the occurrence of disease or premature aging.
The focus is usually towards cardiorespiratory, metabolic (diabetes) and musculoskeletal conditions (back, repetitive strain), and early cancer detection (colorectal, lung, uterus and breast).
Some organizations offer a periodic health risk appraisal (HRA) in the form of a questionnaire probing health habits and potentially significant symptoms often supplemented by such physical measurements as height and weight, skin-fold thickness, blood pressure, “stick test” urinalysis and “finger-stick” blood cholesterol. Others conduct mass screening programs aimed at individual health problems; those aimed at examining subjects for hypertension, diabetes, blood cholesterol level and cancer are most common. It is beyond the scope of this article to discuss which screening tests are most useful. However, the medical director may play a critical role in selecting the procedures most appropriate for the population and in evaluating the sensitivity, specificity and predictive values of the particular tests being considered. Particularly when temporary staff or outside providers are employed for such procedures, it is important that the medical director verify their qualifications and training in order to assure the quality of their performance. Equally important are prompt communication of the results to those being screened, the ready availability of confirmatory tests and further diagnostic procedures for those with positive or equivocal results, access to reliable information for those who may have questions, and an organized follow-up system to encourage compliance with the recommendations. Where there is no employee health service or its involvement in the screening program is precluded, these considerations are often neglected, with the result that the value of the program is threatened.
Physical conditioning
In many larger organizations, physical fitness programs constitute the core of the health promotion and maintenance program. These include aerobic activities to condition the heart and lungs, and strength and stretching exercises to condition the musculoskeletal system.
In organizations with an in-plant exercise facility, it is often placed under the direction of the employee health service. With such a linkage, it becomes available not only for fitness programs but also for preventive and remedial exercises for back pain, hand and shoulder syndromes, and other injuries. It also facilitates medical monitoring of special exercise programs for employees who have returned to work following pregnancy, surgery or myocardial infarction.
Physical conditioning programs can be effective, but they must be structured and guided by trained personnel who know how to guide the physically unfit and impaired to a state of proper physical fitness. To avoid potentially adverse effects, each individual entering a fitness program should have an appropriate medical evaluation, which may be performed by the employee health service.
Program Evaluation
The medical director is in a uniquely advantageous position to evaluate the organization’s health education and promotion program. Cumulative data from periodic health risk appraisals, medical examinations and screenings, visits to the employee health service, absences due to illness and injury, and so on, aggregated for a particular cohort of employees or the workforce as a whole, can be collated with productivity assessments, worker’s compensation and health insurance costs and other management information to provide, over time, an estimate of the effectiveness of the program. Such analyses may also identify gaps and deficiencies suggesting the need for modification of the program and, at the same time, may demonstrate to management the wisdom of continuing allocation of the required resources. Formulas for calculating the cost/benefit of these programs have been published (Guidotti, Cowell and Jamieson 1989).
Conclusion
There is ample evidence in the world literature supporting worksite preventive health programs (Pelletier 1991 and 1993). The employee health service is a uniquely advantageous venue for conducting these programs or, at the very least, participating in their design and monitoring their implementation and results. The medical director is strategically placed to integrate these programs with activities directed at occupational health and safety in ways that will promote both aims for the benefit of both individual employees (and their families, when included in the program) and the organization.
Health Promotion in Small Organizations: The US Experience
The rationale for worksite health promotion and protection programs and approaches to their implementation have been discussed in other articles in this chapter. The greatest activity in these initiatives has taken place in large organizations that have the resources to implement comprehensive programs. However, the majority of the workforce is employed in small organizations where the health and well-being of individual workers is likely to have a greater impact on productive capacity and, ultimately, the success of the enterprise. Recognizing this, small firms have begun to pay more attention to the relationship between preventive health practices and productive, vital employees. Increasing numbers of small firms are finding that, with the help of business coalitions, community resources, public and voluntary health agencies, and creative, modest strategies designed to meet their specific needs, they can implement successful yet low-cost programs that yield significant benefits.
Over the last decade, the number of health promotion programs in small organizations has increased significantly. This trend is important as regards both the progress it represents in worksite health promotion and its implication for the nation’s future health care agenda. This article will explore some of the varied challenges faced by small organizations in implementing these programs and describe some of the strategies adopted by those who have overcome them. It is derived in part from a 1992 paper generated by a symposium on small business and health promotion sponsored by the Washington Business Group on Health, the Office of Disease Prevention of the US Public Health Service and the US Small Business Administration (Muchnick-Baku and Orrick 1992). By way of example, it will highlight some organizations that are succeeding through ingenuity and determination in implementing effective programs with limited resources.
Perceived Barriers to Small Business Programs
While many owners of small firms are supportive of the concept of worksite health promotion, they may hesitate to implement a program in the face of the following perceived barriers (Muchnick-Baku and Orrick 1992):
- “It’s too costly.” A common misconception is that worksite health promotion is too costly for a small business. However, some firms provide programmes by making creative use of free or low-cost community resources. For example, the New York Business Group on Health, a health-action coalition with over 250 member organizations in the New York City Metropolitan Area regularly offered a workshop entitled Wellness On a Shoe String that was aimed primarily at small businesses and highlighted materials available at little or no cost from local health agencies.
- “It’s too complicated.” Another fallacy is that health promotion programmes are too elaborate to fit into the structure of the average small business. However, small firms can begin their efforts very modestly and gradually make them more comprehensive as additional needs are recognized. This is illustrated by Sani-Dairy, a small business in Johnstown, Pennsylvania, that began with a home-grown monthly health promotion publication for employees and their families produced by four employees as an “ extracurricular” activity in addition to their regular duties. Then, they began to plan various health promotion events throughout the year. Unlike many small businesses of this size, Sani-Dairy emphasizes disease prevention in its medical programme. Small companies can also reduce the complexity of health promotion programmes by offering health promotion services less frequently than larger companies. Newsletters and health education materials can be distributed quarterly instead of monthly; a more limited number of health seminars can be held at appropriate seasons of the year or linked to annual national campaigns such as Heart Month, the Great American Smoke Out or Cancer Prevention Week in the United States.
- “It hasn’t been proven that the programmes work.” Small businesses simply do not have the time or the resources to do formal cost-benefit analyses of their health promotion programmes. They are forced to rely on anecdotal experience (which may often be misleading) or on inference from the research done in large-firm settings. “What we try to do is learn from the bigger companies,” says Shawn Connors, President of The International Health Awareness Center, “and we extrapolate their information. When they show that they’re saving money, we believe the same thing is happening to us.” While much of the published research attempting to validate the effectiveness of health promotion is flawed, Pelletier has found ample evidence in the literature to confirm impressions of its value (Pelletier 1991 and 1993).
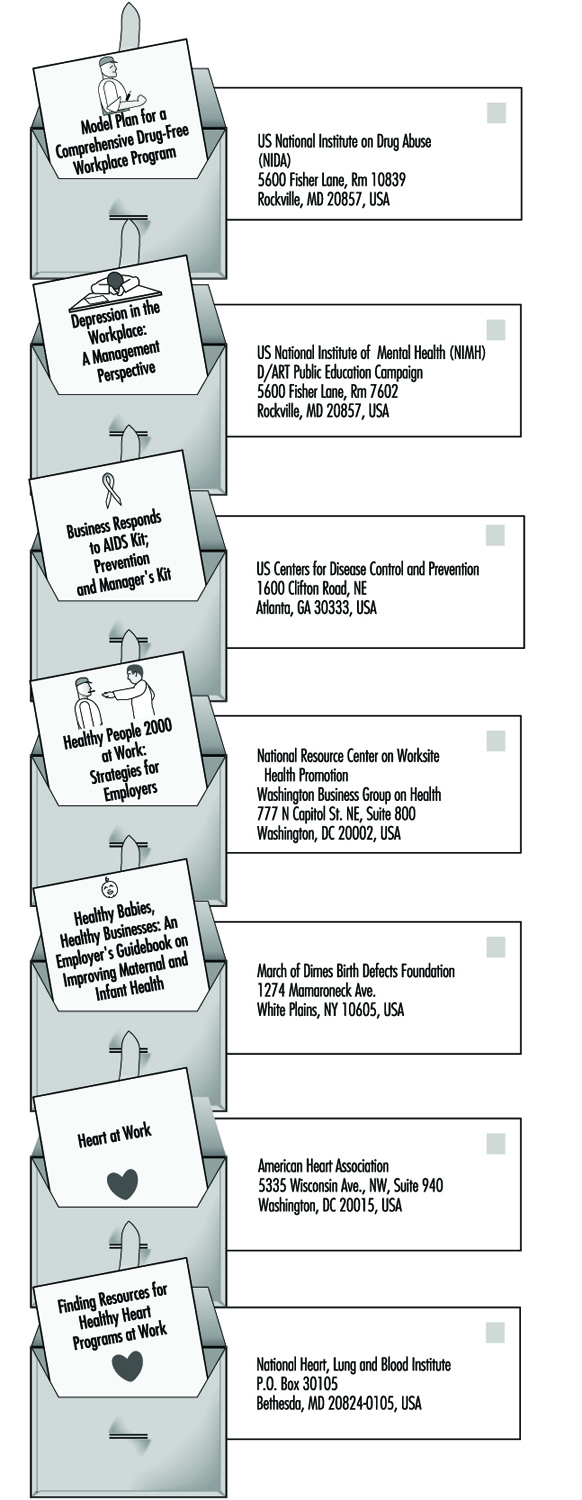
- “We don’t have the expertise to design a programme.” While this is true for most managers of small businesses, it need not present a barrier. Many of the governmental and voluntary health agencies provide free or low-cost kits with detailed instructions and sample materials (see figure 1) for presenting a health promotion programme. In addition, many offer expert advice and consulting services. Finally, in most larger communities and many universities, there are qualified consultants with whom one may negotiate short-term contracts for relatively modest fees covering onsite help in tailoring a particular health promotion programme to the needs and circumstances of a small business and guiding its implementation.
- “We’re not big enough-we don’t have the space.” This is true for most small organizations but it need not stop a good programme. The employer can “buy into” programmes offered in the neighborhood by local hospitals, voluntary health agencies, medical groups and community organizations by subsidizing all or part of any fees that are not covered by the group health insurance plan. Many of these activities are available outside of working hours in the evening or on weekends, obviating the necessity of releasing participating employees from the workplace.
Figure 1. Examples of "do-it-yourself" kits for worksite health promotion programmes in the United States.
Advantages of the Small Worksite
While small businesses do face significant challenges related to financial and administrative resources, they also have advantages. These include (Muchnick-Baku and Orrick 1992):
- Family orientation. The smaller the organization, the more likely it is that employers know their employees and their families. This can facilitate health promotion becoming a corporate-family affair building bonds while promoting health.
- Common work cultures. Small organizations have less diversity among employees than do larger organizations, making it easier to develop more cohesive programmes.
- Interdependency of employees. Members of small units are more dependent on each other. An employee absent because of illness, particularly if prolonged, means a significant loss of productivity and imposes a burden on co-workers. At the same time, the closeness of members of the unit makes peer pressure a more effective stimulant to participation in health promotion activities.
- Approachability of top management. In a smaller organization, management is more accessible, more familiar with the employees and more likely to be aware of their personal problems and needs. Furthermore, the smaller the organization, the more promptly the owner/chief operating officer is likely to become directly involved in making decisions about new programme activities, without the often stultifying effects of the bureaucracy found in most large organizations. In a small firm, that key person is more apt to provide the top-level support so vital to the success of worksite health promotion programmes.
- Effective use of resources. Because they are usually so limited, small businesses tend to be more efficient in the use of their resources. They are more likely to turn to community resources such as voluntary, government and entrepreneurial health and social agencies, hospitals and schools for inexpensive means of providing information and education to employees and their families (see figure 1).
Health Insurance and Health Promotionin Small Businesses
The smaller the firm, the less likely it is to provide group health insurance to employees and their dependants. It is difficult for an employer to claim concern for employees’ health as a basis for offering health promotion activities when basic health insurance is not made available. Even when it is made accessible, exigencies of cost restrict many small businesses to “bare bones” health insurance programs with very limited coverage.
On the other hand, many group plans do cover periodic medical examinations, mammography, Pap smears, immunizations and well baby/child care. Unfortunately, the out-of-pocket cost of covering the deductible fees and co-payments required before insured benefits are payable often acts as a deterrent to using these preventive services. To overcome this, some employers have arranged to reimburse employees for all or part of these expenditures; others find it less troublesome and costly simply to pay for them as an operating expense.
In addition to including preventive services in their coverage, some health insurance carriers offer health promotion programs to group policy holders usually for a fee but sometimes without extra charges. These programs generally focus on printed and audio-visual materials, but some are more comprehensive. Some are particularly suitable for small businesses.
In a growing number of areas, businesses and other types of organizations have formed “health-action” coalitions to develop information and understanding as well as responses to the health-related problems besetting them and their communities. Many of these coalitions provide their members with assistance in designing and implementing worksite health promotion programs. In addition, wellness councils have been appearing in a growing number of communities where they encourage the implementation of worksite as well as community-wide health promotion activities.
Suggestions for Small Businesses
The following suggestions will help to ensure the successful initiation and operation of a health promotion program in a small business:
- Integrate the programme with other company activities. The programme will be more effective and less expensive when it is integrated with the employee group health insurance and benefit plans, the labour relations policies and the corporate environment, and the company’s business strategy. Most important, it must be coordinated with the company’s occupational and environmental health and safety policies and practices.
- Analyze cost data for both employees and the company. What employees want, what they need, and what the company can afford can be vastly different. The company must be able to allocate the resources required for the programme in terms of both the financial outlays and the time and effort of employees involved. It would be futile to launch a programme that could not be continued for lack of resources. At the same time, budget projections should include increases in resource allocations to cover expansion of the programme as it takes hold and grows.
- Involve employees and their representatives. A cross-section of the workforce-i.e., top management, supervisors and rank-and-file workers-should be involved in designing, implementing and evaluating the programme. Where there is a labour union, its leadership and shop stewards should be similarly involved. Often an invitation to co-sponsor the programme will defuse a union’s latent opposition to company programmes intended to enhance employee welfare if that exists; it may also serve to stimulate the union to work for replication of the programme by other companies in the same industry or area.
- Involve employees’ spouses and dependants. Health habits usually are characteristics of the family. Educational materials should be addressed to the home and, to the extent possible, employees’ spouses and other family members should be encouraged to participate in the activities.
- Obtain top management’s endorsement and participation. The company’s top executives should publicly endorse the programme and confirm its value by actually participating in some of the activities.
- Collaborate with other organizations. Wherever possible, achieve economies of scale by joining forces with other local organizations, using community facilities, etc.
- Keep personal information confidential. Make a point of keeping personal information about health problems, test results and even participation in particular activities out of personnel files and obviate potential stigmatization by keeping it confidential.
- Give the programme a positive theme and keep changing it. Give the programme a high profile and publicize its objectives widely. Without dropping any useful activities, change the programme’s emphasis to generate new interest and to avoid appearing stagnant. One way to accomplish this is to “piggy back” on national and community programmes such as National Heart Month and Diabetes Week in the United States.
- Make it easy to be involved. Activities that cannot be accommodated at the worksite should be located at convenient locations nearby in the community. When it is not feasible to schedule them during working hours, they may be held during the lunch hour or at the end of a work shift; for some activities, evenings or weekends may be more convenient.
- Consider offering incentives and awards. Commonly used incentives to encourage programme participation and recognize achievements include released time, partial or 100% rebates of any fees, reduction in employee’s contribution to group health insurance plan premiums (“risk-rated” health insurance), gift certificates from local merchants, modest prizes such as T-shirts, inexpensive watches or jewelry, use of a preferred parking space, and recognition in company newsletters or on worksite bulletin boards.
- Evaluate the programme. The numbers of participants and their drop-out rates will demonstrate the acceptability of particular activities. Measurable changes such as smoking cessation, loss or gain of weight, lower levels of blood pressure or cholesterol, indices of physical fitness, etc., can be used to appraise their effectiveness. Periodic employee surveys can be used to assess attitudes toward the programme and elicit suggestions for improvement. And review of such data as absenteeism, turnover, appraisal of changes in quantity and quality of production, and utilization of health care benefits may demonstrate the value of the programme to the organization.
Conclusion
Although there are significant challenges to be overcome, they are not insurmountable. Health promotion programs may be no less, and sometimes even more, valuable in small organizations than in larger ones. Although valid data are difficult to come by, it may be expected that they will yield similar returns of improvement with regard to employee health, well-being, morale and productivity. To achieve these with resources that are often limited requires careful planning and implementation, the endorsement and support of top executives, the involvement of employees and their representatives, the integration of the health promotion program with the organization’s health and safety policies and practices, a health care insurance plan and appropriate labor-management policies and agreements, and utilization of free or low-cost materials and services available in the community.
Health Promotion in the Workplace: England
In its Health of the Nation policy declaration, the government of the United Kingdom subscribed to the twin strategy (to paraphrase their statement of aims) of (1) “adding years to life” by seeking an increase in life expectancy and a reduction in premature death, and (2) “adding life to years” by increasing the number of years lived free from ill-health, by reducing or minimizing the adverse effects of illness and disability, by promoting healthy lifestyles and by improving physical and social environments—in short, by improving the quality of life.
It was felt that efforts to achieve these aims would be more successful if they were exerted in already existent “settings”, namely schools, homes, hospitals and workplaces.
While it was known that there was considerable health promotion activity at the workplace (European Foundation 1991), no comprehensive baseline information existed on the level and nature of workplace health promotion. Various small-scale surveys had been conducted, but these had all been limited in one way or another, either by being concentrated on a single activity such as smoking, or restricted to a small geographical area or based on a small number of workplaces.
A comprehensive survey of workplace health promotion in England was undertaken on behalf of the Health Education Authority. Two models were used to develop the survey: the 1985 US National Survey of Worksite Health Promotion (Fielding and Piserchia 1989) and a 1984 survey carried out by the Policy Studies Institute of Workplaces in Britain (Daniel 1987).
The survey
There are over 2,000,000 workplaces in England (the workplace is defined as a geographically contiguous setting). The distribution is enormously skewed: 88% of workplaces employ fewer than 25 people onsite and cover about 30% of the workforce; only 0.3% of workplaces employ more than 500 people, yet these few very large sites account for some 20% of total employees.
The survey was originally structured to reflect this distribution by over-sampling the larger worksites in a random sample of all workplaces, including both the public and private sectors and all sizes of workplace; however, those who were self-employed and were working from home were excepted from the survey. The only other exclusions were various public bodies such as defense establishments, police and prison services.
In total 1,344 workplaces were surveyed in March and April of 1992. Interviewing was carried out by telephone, with the average completed interview taking 28 minutes. Interviews were held with whatever person was responsible for health-related activities. At smaller workplaces, this was seldom someone with a health specialization.
Findings of the survey
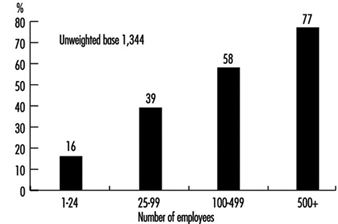
Figure 1 shows the spontaneous response to the inquiry as to whether any health-related activities had been undertaken in the past year and the marked size relationship to type of respondent.
Figure 1. Whether any health-related activities were undertaken in last 12 months.
A succession of spontaneous questions, and questions that were prompted in the course of interviewing, elicited from respondents considerably more information as to the extent and nature of health-related activities. The range of activities and incidence of such activity is shown in table 1. Some of the activities, such as job satisfaction (understood in England as a catch-all term covering such aspects as responsibility for both the pace and content of the work, self-esteem, management-worker relationships and skills and training) are normally regarded as outside the scope of health promotion, but there are commentators who believe that such structural factors are of great importance in improving health.
Table 1. Range of health-related activities by size of workforce.
|
Size of workforce (activity in %) |
|||||
|
All |
1-24 |
25-99 |
100-499 |
500+ |
|
|
Smoking and tobacco |
31 |
29 |
42 |
61 |
81 |
|
Alcohol and sensible drinking |
14 |
13 |
21 |
30 |
46 |
|
Diet |
6 |
5 |
13 |
26 |
47 |
|
Healthy catering |
5 |
4 |
13 |
30 |
45 |
|
Stress management |
9 |
7 |
14 |
111 |
32 |
|
HIV/AIDS and sexual health practices |
9 |
7 |
16 |
26 |
42 |
|
Weight control |
3 |
2 |
4 |
12 |
30 |
|
Exercise and fitness |
6 |
5 |
10 |
20 |
37 |
|
Heart health and heart disease-related activities |
4 |
2 |
9 |
18 |
43 |
|
Breast screening |
3 |
2 |
4 |
15 |
29 |
|
Cervical screening |
3 |
2 |
5 |
12 |
23 |
|
Health screening |
5 |
4 |
10 |
29 |
54 |
|
Lifestyle assessment |
3 |
2 |
2 |
5 |
21 |
|
Cholesterol testing |
4 |
3 |
5 |
11 |
24 |
|
Blood pressure control |
4 |
3 |
9 |
16 |
44 |
|
Drugs and alcohol abuse-related activities |
5 |
4 |
13 |
14 |
28 |
|
Women’s health-related activities |
4 |
4 |
6 |
14 |
30 |
|
Men’s health-related activities |
2 |
2 |
5 |
9 |
32 |
|
Repetitive strain injury avoidance |
4 |
3 |
10 |
23 |
47 |
|
Back care |
9 |
8 |
17 |
25 |
46 |
|
Eyesight |
5 |
4 |
12 |
27 |
56 |
|
Hearing |
4 |
3 |
8 |
18 |
44 |
|
Desk and office layout design |
9 |
8 |
16 |
23 |
45 |
|
Interior ventilation and lighting |
16 |
14 |
26 |
38 |
46 |
|
Job satisfaction |
18 |
14 |
25 |
25 |
32 |
|
Noise |
8 |
6 |
17 |
33 |
48 |
Unweighted base = 1,344.
Other matters that were investigated included the decision-making process, budgets, workforce consultation, awareness of information and advice, benefits of health promotion activity to employer and employee, difficulties in implementation, and perception of the importance of health promotion. There are several general points to make:
- Overall, 40% of all workplaces undertook at least one major health related activity in the previous year. Apart from activity on smoking in workplaces with more than 100 employees, no single health promotion activity occurs in a majority of workplaces ranked by size.
- In small workplaces the only direct health promoting activities of any significance are for smoking and alcohol. Even then, both are of minority incidence (29% and 13%).
- The immediate physical environment, reflected in such factors as ventilation and lighting, are considered to be substantively health related, as is job satisfaction. However, these are mentioned by less than 25% of workplaces with under 100 employees.
- As the workplace increases in size, it is not just that a higher percentage of workplaces undertake any activity, there is also a wider range of activity in any one workplace. This is shown in figure 15.5, which illustrates the likelihood of one or more of the major programmes. Only 9% of the largest workplaces have no programme at all and over 50% have at least three. In the smallest workplaces, only 19% have two or more programmes. In between, 35% of 25-99 workplaces have two or more programmes, while 56% of 100-499 workplaces have two or more programmes and 33% have three or more. However, it would be too much to read into these figures any semblance of what might be called a “healthy workplace”. Even if such a workplace were defined as one with 5+ programmes in place, there needs to a be an evaluation of the nature and intensity of the programme. In-depth interviewing suggests that in very few instances is the health activity integrated into a planned health promotion function and in even fewer cases, if any, is there modification of either the practices or objectives of the workplace to increase the emphasis on health enhancement.
- After smoking programmes, which get an 81% incidence in the largest workplaces, and alcohol, the next highest incidences are for eyesight testing, health screening and back care.
- Breast and cervical screening have a low incidence, even in workplaces with 60%+ of female employees (see table 2).
- Public sector workplaces show double the level of incidence for activities of those in the private sector. This holds across all the activities
- In regard to smoking and alcohol, foreign-owned companies have a higher incidence of workplace activity than British ones. However, the differential is relatively minor in most activities apart from health screening (15% against 5%) and the concomitant activities such as cholesterol and blood pressure.
- Only in the public sector is there a significant involvement in HIV/AIDS activity. In most of the activities the public sector outperforms the other industry sectors with the notable exception of alcohol.
- Workplaces which have no health promotion activity are virtually all small or medium-size in the private sector, British-owned and predominantly in the distribution and catering industries.
Figure 2. Likelihood of number of major health promotion programmes, by size of workforce.
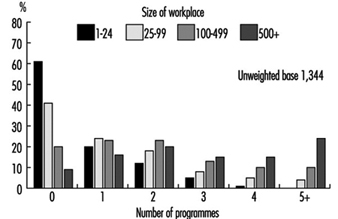
Table 2. Participation rates in breast and cervical cancer screening (spontaneous and prompted) by percentage of female workforce.
|
Percentage of the workforce that is female |
||
|
More than 60% |
Less than 60% |
|
|
Breast screening |
4% |
2% |
|
Cervical screening |
4% |
2% |
Unweighted base = 1,344.
Discussion
The quantitative telephone survey and the parallel face-to-face interviewing revealed a considerable amount of information as to the level of health promotion activity at the workplace in England.
In a study of this nature, it is not possible to untangle all the confounding variables. However, it would seem that size of workplace, in terms of number of employees, public as opposed to private ownership, levels of unionization, and the nature of the work itself are important factors.
Communication of health promotion messages is largely through group methods such as posters, leaflets or videos. In larger workplaces there is a far greater likelihood of individual counseling being available, particularly for things like smoking cessation, alcohol problems and stress management. It is clear from the research methods used that health promotion activities are not “embedded” in the workplace and are highly contingent activities which, in the large majority of cases, are dependent for effectiveness on individuals. To date, health promotion has not made out the necessary cost/benefit base for its implementation. Such a cost/benefit calculation need not be a detailed and sophisticated analysis but simply an indication that it is of value. Such an indication may be of great benefit in persuading more private sector workplaces to increase their activity levels. There are very few of what might be termed “healthy workplaces”. In very few instances is the health promotion activity integrated into a planned health promotion function and in even fewer cases, if any, is there modification of either the practice or objectives of the workplace to increase emphasis on health enhancement.
Conclusion
Health promotion activities seem to be increasing, with 37% of respondents claiming that such activity had increased in the previous year. Health promotion is considered to be an important issue, with even 41% of small workplaces saying it was very important. Considerable benefits to employee health and fitness were ascribed to health promotion activities, as was reduced absenteeism and sickness.
However, there is little formal evaluation, and while written policies have been introduced, they are by no means universal. While there is support for the aims of health promotion and positive advantages are perceived, there is yet too little evidence of institutionalization of the activities into the culture of the workplace. Workplace health promotion in England seems to be contingent and vulnerable.
Worksite Health Promotion
Rationale
Occupational settings are appropriate sites for the furtherance of such health-related aims as assessment, education, counseling and health promotion in general. From a public policy perspective, worksites provide an efficient locus for activities such as these, involving as they often do a far-ranging aggregation of individuals. Moreover, most workers are in a predictable work location for a significant portion of time almost every week. The worksite is usually a controlled environment, where individuals or groups can be exposed to educational programming or receive counseling without the distractions of a home setting or the often hurried atmosphere of a medical setting.
Health is an enabling function, that is to say, one that permits individuals to pursue other goals, including successful performance in their work roles. Employers have a vested interest in maximizing health because of its tight linkage with productivity at work, as to both quantity and quality. Thus, reducing the occurrence and burden of diseases that lead to absences, disability or sub-par job performance is a goal that warrants a high priority and considerable investment. Worker organizations, established to improve the welfare of members, also have an inherent interest in sponsoring programs that can improve health status and quality of life.
Sponsorship
Sponsorship by employers usually includes full or partial financial support of the program. However, some employers may support only planning or arranging for the actual health promotion activities for which individual workers must pay. Employer-sponsored programs sometimes provide employee incentives for participation, program completion, or successfully changing health habits. Incentives may include time off from work, financial rewards for participation or results, or recognition of achievement in reaching health-related goals. In unionized industries, particularly where workers are scattered among smaller workplaces too small to mount a program, health promotion programs may be designed and delivered by the labor organization. Although sponsorship of health education and counseling programs by employers or worker organizations commonly involves programs delivered at the worksite, they may take place in whole or in part at facilities in the community, whether run by government, non-profit-making or for-profit organizations.
Financial sponsorship needs to be complemented by employer commitment, on the part of top management and of middle management as well. Every employer organization has many priorities. If health promotion is to be viewed as one of these, it must be actively and visibly supported by senior management, both financially and by means of continuing to pay attention to the program, including the emphasizing of its importance in addressing employees, stockholders, senior managers and even the outside investment community.
Confidentiality and Privacy
While employee health is an important determinant of productivity and of the vitality of work organizations, health in itself is a personal matter. An employer or worker organization that wishes to provide health education and counseling must build into the programs procedures to ensure confidentiality and privacy. The willingness of employees to volunteer for work-related health education and counseling programs requires that employees feel that private health information will not be revealed to others without their permission. Of particular concern to workers and their representatives is that information obtained from health improvement programs not be utilized in any way in assessment of job performance or in managerial decisions about hiring, firing or advancement.
Needs Assessment
Program planning usually begins with a needs assessment. An employee survey is often performed to obtain information on such matters as: (a) self-reported frequency of health habits (e.g., smoking, physical activity, nutrition), (b) other health risks such as stress, hypertension, hypercholesterolemia, and diabetes, (c) personal priorities for risk reduction and health improvement, (d) attitude toward alternative program configurations, (e) preferred sites for health promotion programming, (f) willingness to participate in programmatic activities, and sometimes, (g) willingness to pay a portion of the cost. Surveys may also cover attitudes toward existing or potential employer policies, such as smoking bans or offering more nutritionally healthful fare in workplace vending machines or cafeterias.
The needs assessment sometimes includes analysis of the health problems of the employed group through examination of medical department clinical files, health care records, disability and worker’s compensation claims, and absenteeism records. Such analyses provide general epidemiological information on the prevalence and cost of different health problems, both somatic and psychological, allowing assessment of prevention opportunities from both the programmatic and financial point of view.
Program Structure
Results of needs assessments are considered in light of available monetary and human resources, past program experience, regulatory requirements and the nature of the workforce. Some of the key elements of a program plan that need to be clearly defined during a planning process are listed in figure 1. One of the key decisions is identifying effective modalities to reach the target population(s). For example, for a widely dispersed workforce, community-based programming or programming via telephone and mail may be the most feasible and cost-effective choice. Another important decision is whether to include, as some programmers do, retirees and spouses and children of employees in addition to the employees themselves.
Figure 1. Elements of a health promotion programme plan.

Responsibility for a worksite health promotion program can fall to any of a number of pre-existing departments, including the following: the medical or employee health unit; human resources and personnel; training; administration; fitness; employee assistance and others; or a separate health promotion department may be established. This choice is often very important to program success. A department with strong interest in doing its best for its clients, an appropriate knowledge base, good working relationships with other parts of the organization and the confidence of senior and line management has a very high likelihood of success in organizational terms. Employees’ attitudes toward the department in which the program is placed and their confidence in its integrity with particular reference to confidentiality of personal information may influence their acceptance of the program.
Topics
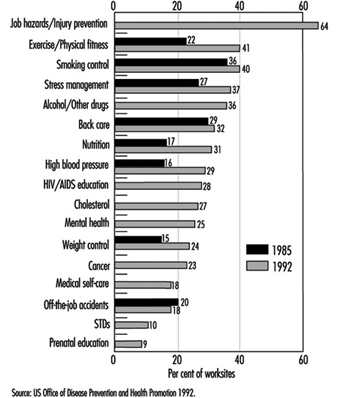
The frequency with which diverse health promotion topics is addressed based on surveys of private employers with 50 or more employees is shown in Figure 2. A review of results from comparable surveys in 1985 and 1992 reveals substantial increases in most areas. Overall in 1985, 66% of the worksites had at least one activity, whereas in 1992, 81% had one or more. Areas with the largest increases were those to do with exercise and physical fitness, nutrition, high blood pressure and weight control. Several topic areas queried for the first time in 1992 showed relatively high frequencies, including AIDS education, cholesterol, mental health and job hazards and injury prevention. Symptomatic of the expansion of areas of interest, the 1992 survey found that 36% of worksites provided education or other programs for abuse of alcohol and other drugs, 28% for AIDS, 10% for prevention of sexually-transmitted diseases, and 9% for prenatal education.
Figure 2. Health promotion information or activities offered by subject, 1985 and 1992.
A broad topic category increasingly included within worksite health promotion programming (16% of worksites in 1992) is health care mediated by self-help programs. Common to these programs are materials that address ways in which to treat minor health problems and to apply simple rules for judging the seriousness of various signs and symptoms in order to decide whether it may be advisable to seek professional help and with what degree of urgency.
Creating better-informed consumers of health care services is an allied program objective, and includes educating them such as how to choose a physician, what questions to ask the doctor, the pros and cons of alternative treatment strategies, how to decide whether and where to have a recommended diagnostic or therapeutic procedure, non-traditional therapies and patients’ rights.
Health Assessments
Regardless of mission, size and target population, multidimensional assessments of health are commonly administered to participating employees during the initial stages of the program and at periodic intervals thereafter. Data systematically collected usually cover health habits, health status, simple physiological measures, such as blood pressure and lipid profile, and (less commonly) health attitudes, the social dimensions of health, the use of preventive services, safety practices and family history. Computerized outputs, fed back to individual employees and aggregated for program planning, monitoring and evaluation, usually provide some absolute or relative risk estimates, which range from the absolute risk of having a heart attack during the ensuing ten-year period (or how an individual’s quantifiable risk of having a heart attack compares to the average risk for individuals of the same age and sex) to qualitative ratings of health and risks on a scale from poor to excellent. Individual recommendations are also commonly provided. For example, regular physical activity would be recommended for sedentary individuals, and more social contacts for an individual without frequent contact with family or friends.
Health assessments may be systematically offered at the time of hire or in association with specific programs, and thereafter at fixed intervals or with periodicity defined by age, sex and health risk status.
Counseling
Another common element of most programs is counseling to effect changes in such deleterious health habits as smoking, poor nutritional practices or high-risk sexual behavior. Effective methods exist to assist individuals to increase their motivation and readiness to make changes in their health habits, to help them along in the actual process of making changes, and to minimize backsliding, often termed recidivism. Group sessions led by a health professional or lay person with special training are often used to help individuals make changes, while the peer support to be found in the workplace can enhance results in areas such as smoking cessation or physical activity.
Health education for workers may include topics that can positively influence the health of other family members. For example, education might include programming on healthy pregnancy, the importance of breast feeding, parenting skills, and how to effectively cope with the health care and related needs of older relatives. Effective counseling avoids stigmatizing program participants who have difficulty making changes or who decide against making recommended lifestyle changes.
Workers with Special Needs
A significant proportion of a working population, particularly if it includes many older workers, will have one or more chronic conditions, such as diabetes, arthritis, depression, asthma or low back pain. In addition, a substantial subpopulation will be considered at high risk for a serious future health problem, for example cardiovascular disease due to elevation of risk factors such as total serum cholesterol, high blood pressure, smoking, significant obesity or high levels of stress.
These populations may account for a disproportionate amount of health services utilization, health benefits costs and lost productivity, but these effects can be attenuated through prevention efforts. Therefore, education and counseling programs targeted at these conditions and risks have become increasingly common. Such programs often utilize a specially trained nurse (or less commonly, a health educator or nutritionist) to help these individuals make and maintain necessary behavioral changes and work more closely with their primary care physician to utilize appropriate medical measures, especially as regards the use of pharmaceutical agents.
Program Providers
Providers of employer-sponsored or worker-sponsored health promotion programming are varied. In larger organizations, particularly with significant geographic concentrations of employees, existing full- or part-time personnel may be the principal program staff—nurses, health educators, psychologists, exercise physiologists and others. Staffing can also come from outside providers, individual consultants or organizations providing personnel in a wide range of disciplines. Organizations offering these services include hospitals, voluntary organizations (e.g., the American Heart Association); for-profit health promotion companies offering health screening, fitness, stress management, nutrition and other programs; and managed care organizations. Program materials may also come from any of these sources or they may be developed internally. Worker organizations sometimes develop their own programs for their members, or may provide some health promotion services in partnership with the employer.
Many education and training programs have been established to prepare both students and health professionals to plan, implement and evaluate worksite health promotion programs. Many universities offer courses in these subjects and some have a special “worksite health promotion” major or area of specialization. A large number of continuing education courses on how to work in a corporate setting, program management and advances in techniques are offered by public and private educational institutions as well as professional organizations. To be effective, providers must understand the specific context, constraints and attitudes associated with employment settings. In planning and implementing programs they should take into account policies specific to the type of employment and worksite, as well as the relevant labor relations issues, work schedules, formal and informal organizational structures, not to mention the corporate culture, norms and expectations.
Technology
Applicable technologies range from self-help materials that include traditional books, pamphlets, audiotapes or videotapes to programmed learning software and interactive videodiscs. Most programs involve interpersonal contact through groups such as classes, conferences and seminars or through individual education and counseling with an onsite provider, by telephone or even via computer link. Self-help groups may also be utilized.
Computer-based data collection systems are essential for program efficiency, serving a variety of management functions—budgeting and use of resources, scheduling, individual tracking, and both process and outcome evaluation. Other technologies could include such sophisticated modalities as a direct bio-computer linkage to record physiological measures—blood pressure or visual acuity for instance—or even the subject’s participation in the program itself (e.g., attendance at a fitness facility). Hand-held computer-based learning aids are being tested to assess their ability to enhance behavioral change.
Evaluation
Evaluation efforts run the gamut from anecdotal comments from employees to complex methodologies that justify publication in peer-reviewed journals. Evaluations may be directed towards a wide variety of processes and outcomes. For example, a process evaluation could assess how the program was implemented, how many employees participated and what they thought of it. Outcome evaluations may target changes in health status, such as the frequency or level of a health risk factor, whether self-reported (e.g., level of exercise) or objectively evaluated (e.g., hypertension). An evaluation may focus upon economic changes such as the use and cost of health care services or upon absenteeism or disability, whether this may be related to the job or not.
Evaluations may cover only program participants or they may cover all at-risk employees. The former sort of evaluation can answer questions relating to the efficacy of a given intervention but the latter answers the more important question as to the effectiveness with which risk factors in an entire population may have been reduced. While many evaluations focus on efforts to change a single risk factor, others address the simultaneous effects of multicomponent interventions. A review of 48 published studies assessing outcomes of comprehensive health promotion and disease prevention in the worksite found that 47 reported one or more positive health outcomes (Pelletier 1991). Many of these studies have significant weaknesses in design, methodology or analysis. Nonetheless, their near-unanimity with respect to positive findings, and the optimistic results of the best designed studies, suggest that real effects are in the desired direction. What is less clear is the reproducibility of effects in replicated programs, how long the initially observed effects endure, and whether their statistical significance translates into clinical significance. In addition, evidence of effectiveness is much stronger for some risk factors, such as smoking and hypertension, than for physical activity, nutritional practices and mental health factors, including stress.
Trends
Worksite health promotion programs are expanding beyond the traditional topics of controlling alcohol and drug abuse, nutrition, weight control, smoking cessation, exercise and stress management. Today, activities generally cover a wider variety of health topics, ranging from healthy pregnancy or the menopause to living with chronic health conditions such as arthritis, depression or diabetes. Increased emphasis is being placed on aspects of good mental health. For example, under the rubric of employer-sponsored programs may appear courses or other activities such as “improving interpersonal communications”, “building self-esteem”, “improving personal productivity at work and home”, or “overcoming depression”.
Another trend is to provide a wider range of health information and counseling opportunities. Individual and group counseling may be supplemented with peer counseling, computer-based learning, and use of interactive videodiscs. Recognition of multiple learning styles has led to a broader array of delivery modes to increase efficiency with a better match between individual learning styles and preferences and instructional approaches. Offering this diversity of approaches allows individuals to choose the setting, intensity and educational form that best fits their learning habits.
Today, health education and counseling are being increasingly offered to employees of larger organizations, including those who may work at distant locations with few co-workers and those that work at home. Delivery via mail and phone, when possible, can facilitate this broader reach. The advantage of these modes of program delivery is greater equity, with field staff employees not disadvantaged compared to their home office counterparts. One cost of greater equity is sometimes reduced interpersonal contact with health professionals on health promotion issues.
Healthy Policies
Recognition is increasing that organizational policy and social norms are important determinants of health and of the effectiveness of health improvement efforts. For example, limiting or banning smoking at the workplace can yield substantial declines in per capita cigarette consumption among smoking workers. A policy that alcoholic beverages will not be served at company functions lays out behavioral expectations for employees. Providing food that is low in fat and high in complex carbohydrates in the company cafeteria is another opportunity to help employees improve their health.
However, there is also concern that healthful organizational policies or expressed social normative beliefs about what constitutes good health may stigmatize individuals who wish to engage in certain unhealthy habits, such as smoking, or those who have a strong genetic predisposition to an unhealthy state, such as obesity. It is not surprising that most programs have higher participation rates by employees with “healthy” habits and lower risks.
Integration with Other Programs
The promotion of health has many facets. It appears that growing efforts are being made to seek a closer integration among health education and counseling, ergonomics, employee assistance programs, and particular health-oriented benefits like screening and fitness plans. In countries where employers can design their own health benefit plans or can supplement a government plan with defined benefits, many are offering clinical preventive services benefits, particularly screening and health-enhancing benefits such as membership in community health and fitness facilities. Tax policies that permit employers to deduct these employee benefits from taxes provide strong financial incentives for their adoption.
Ergonomic design is an important determinant of worker health and involves more than just the physical fit of the employee to the tools employed on the job. Attention should be directed to the overall fit of the individual to his or her tasks and to the overall working environment. For example, a healthful job environment requires a good match between job autonomy and responsibility and effective adaptations among individual work style, family needs and the flexibility of work requirements. Nor should the relationship between work stresses and individual coping capacities be left out of this account. In addition, health can be promoted by having workers, individually and in groups, help mould job content in ways that contribute to feelings of self-efficacy and achievement.
Employee assistance programs, which generically speaking include employer-sponsored professionally directed activities that provide assessment, counseling and referral to any employee for personal problems, should have close ties with other health promoting programs, functioning as a referral source for the depressed, the overstressed and the preoccupied. In return, employee assistance programs can refer appropriate workers to employer-sponsored stress management programs, to physical fitness programs that help relieve depression, to nutritional programs for those overweight, underweight, or simply with bad nutrition, and to self-help groups for those who lack social support.
Conclusion
Worksite health promotion has come of age owing largely to incentives for employer investment, positive reported results for most programs, and increasing acceptance of worksite health promotion as an essential part of a comprehensive benefit plan. Its scope has broadened considerably, reflecting a more encompassing definition of health and an understanding of the determinants of individual and family health.
Well-developed approaches to program planning and implementation exist, as does a cadre of well-trained health professionals to staff programs and a wide variety of materials and delivery vehicles. Program success depends on individualizing any program to the corporate culture and to the health promotion opportunities and organizational constraints of a particular worksite. Results of most evaluations have supported movement toward stated program objectives, but more evaluations using scientifically valid designs and methods are needed.
Health Protection and Promotion in the Workplace: An Overview
It has often been said that the workforce is the most critical element in the productive apparatus of the organization. Even in highly automated plants with their smaller number of workers, decrements in their health and well-being will sooner or later be reflected in impaired productivity or, sometimes, even in disasters.
Through governmental legislation and regulation, employers have been made responsible for maintaining the safety of the work environment and work practices, and for the treatment, rehabilitation and compensation of workers with occupational injuries and disease. In recent decades, however, employers have begun to recognize that disabilities and absences are costly even when they originate outside the workplace. Consequently, they have begun to provide more and more comprehensive health promotion and protection programs not only for employees but for their families as well. In opening a 1987 meeting of a World Health Organization (WHO) Expert Committee on Health Promotion in the Worksetting, Dr. Lu Rushan, Assistant Director-General of WHO, reiterated that WHO viewed workers’ health promotion as an essential component of occupational health services (WHO 1988).
Why the Workplace?
The rationale for employer sponsorship of health promotion programs includes preventing loss of worker productivity due to avoidable illnesses and disability and their associated absenteeism, improving employee well-being and morale, and controlling the costs of employer-paid health insurance by reducing the amount of health care services required. Similar considerations have stimulated union interest in sponsoring programs, particularly when their members are scattered among many organizations too small to mount effective programs on their own.
The workplace is uniquely advantageous as an arena for health protection and promotion. It is the place where workers congregate and spend a major portion of their waking hours, a fact that makes it convenient to reach them. In addition to this propinquity, their camaraderie and sharing of similar interests and concerns facilitate the development of peer pressures that can be a powerful motivator for participation and persistence in a health promotion activity. The relative stability of the workforce—most workers remain in the same organization for long periods of time—makes for the continuing participation in healthful behaviors necessary to achieve their benefit.
The workplace affords unique opportunities to promote the improved health and well-being of the workers by:
- integrating the health protection and promotion programme into the organization’s efforts to control occupational diseases and injuries
- modifying the structure of the job and its environment in ways that will make it less hazardous and less stressful
- providing employer- or union-sponsored programmes designed to enable employees to cope more effectively with personal or family burdens that may impinge on their well-being and work performance (i.e., modified work schedules and financial assistance benefits and programmes that address alcohol and drug abuse, pregnancy, child care, caring for elderly or disabled family members, marital difficulties or planning for retirement).
Does Health Promotion Work?
There is no doubt of the efficacy of immunizations in preventing infectious diseases or of the value of good occupational health and safety programs in reducing the frequency and severity of work-related diseases and injuries. There is general agreement that early detection and appropriate treatment of incipient diseases will reduce mortality and lower the frequency and extent of residual disability from many diseases. There is growing evidence that elimination or control of risk factors will prevent or, at least, substantially delay the onset of life-threatening diseases such as stroke, coronary artery disease and cancer. There is little doubt that maintaining a healthy lifestyle and coping successfully with psychosocial burdens will improve well-being and functional capacity so as to achieve the goal of wellness defined by the World Health Organization as a state beyond the mere absence of disease. Yet some remain skeptical; even some physicians, at least to judge by their actions.
There is perhaps a higher level of skepticism about the value of worksite health promotion programs. In large part, this reflects the lack of adequately designed and controlled studies, the confounding effect of secular events such as the declining incidence of mortality from heart disease and stroke and, most important, the length of time required for most preventive measures to have their effect. However, in the Health Project report, Freis et al. (1993) summarize the growing literature confirming the effectiveness of worksite health promotion programs in reducing health care costs. In its initial review of over 200 workplace programs, the Health Project, a voluntary consortium of business leaders, health insurers, policy scholars and members of government agencies which advocate health promotion to reduce the demand and the need for health services, found eight with convincing documentation of savings in health care costs.
Pelletier (1991) assembled 24 studies of comprehensive worksite programs published in peer-review journals between 1980 and 1990. (Reports of single-focus programs, such as those dealing with hypertension screening and smoking cessation, even though demonstrated to have been successful, were not included in this review.) He defined “comprehensive programs” as those which “provide an ongoing, integrated program of health promotion and disease prevention that knits the particular components (smoking cessation, stress management, coronary risk reduction, etc.) into a coherent, ongoing program that is consistent with corporate objectives and includes program evaluation.” All of the 24 programs summarized in this review achieved improvement in employees’ health practices, reductions in absenteeism and disability, and/or increases in productivity, while each of these studies that analyzed for impact on health care and disability costs, cost-effectiveness or cost/benefit changes demonstrated a positive effect.
Two years later, Pelletier reviewed an additional 24 studies published between 1991 and the early part of 1993 and found that 23 reported positive health gains and, again, all of those studies which analyzed cost-effectiveness or cost/benefit effects indicated a positive return (Pelletier 1993). Factors common to the successful programs, he noted, included specific program goals and objectives, easy access to the program and facilities, incentives for participation, respect and confidentiality, support of top management and a corporate culture that encourages health promotion efforts (Pelletier 1991).
While it is desirable to have evidence confirming the effectiveness and value of worksite health promotion programs, the fact is that such proof has rarely been required for the decision to initiate a program. Most programs have been based on the persuasive power of the conviction that prevention does work. In some instances, programs have been stimulated by interest articulated by employees and, occasionally, by the unexpected death of a top executive or a key employee from cancer or heart disease and the fond hope that a preventive program will keep “lightning from striking twice”.
Structure of a Comprehensive Program
In many organizations, particularly smaller ones, the health promotion and disease prevention program consists merely of one or more largely ad hoc activities that are informally related to each other, if at all, that have little or no continuity, and that often are triggered by a particular event and abandoned as it fades into memory. A truly comprehensive program should have a formal structure comprising a number of integrated elements, including the following:
- a clear statement of goals and objectives that are approved by management and acceptable to the employees
- explicit endorsement by top management and, where they exist, the labour organizations involved, with the continuing allocation of resources adequate to achieve desired goals and objectives
- appropriate placement in the organization, effective coordination with other health-related activities, and communication of programme plans across divisions and departments to mid-level managers and employees. Some organizations have found it expedient to create a labour-management committee comprising representatives from all levels and segments of the workforce for “political” reasons as well as to provide input on programme design
- designation of a “programme director,” a person with the requisite administrative skills who also has had training and experience in health promotion or has access to a consultant who might supply the necessary expertise
- a mechanism for feedback from participants and, if possible, non-participants as well, in order to confirm the validity of the programme design and to test the popularity and utility of particular programme activities
- procedures for maintaining the confidentiality of personal information
- systematic record-keeping to keep track of activities, participation and outcomes as a basis for monitoring and potential evaluation
- compilation and analysis of available relevant data, ideally for a scientific evaluation of the programme or, when that is not feasible, to generate a periodic report to management to justify continuation of the resource allocation and to form a basis for possible changes in the programme.
Program Objectives and Ideology
The basic objectives of the program are to enhance and maintain the health and well-being of employees on all levels, to prevent disease and disability, and to ease the burden on individuals and the organization when disease and disability cannot be prevented.
The occupational health and safety program is directed to those factors on the job and in the workplace that may affect employees’ health. The wellness program recognizes that their health concerns cannot be confined within the boundaries of the plant or office, that problems arising in the workplace inevitably affect the health and well-being of workers (and, by extension, also their families) in the home and in the community and that, just as inevitably, problems arising outside of work affect attendance and work performance. (The term wellness can be considered the equivalent of the expression health promotion and protection, and has been used increasingly in the field during the last two decades; it epitomizes the World Health Organization’s positive definition of health.) Accordingly, it is quite appropriate for the health promotion program to address problems that some argue are not proper concerns for the organization.
The need to achieve wellness assumes greater urgency when it is recognized that workers with diminished capacities, however acquired, may be potentially hazardous to their co-workers and, in certain jobs, to the public as well.
There are those who hold that, since health is fundamentally a personal responsibility of the individual, it is inappropriate, and even intrusive, for employers or labor unions (or both) to undertake involvement with it. They are correct insofar as overly paternalistic and coercive approaches are employed. However, health-promoting adjustments of the job and the workplace along with enhanced access to health-promoting activities provide the awareness, knowledge and tools that enable employees to address that personal responsibility more effectively.
Program Components
Needs assessment
While the alert program director will take advantage of a particular event that will create interest in a special activity (e.g., the unexpected illness of a popular person in the organization, reports of cases of an infectious disease that raise fears of contagion, warnings of a potential epidemic), the comprehensive program will be based on a more formal needs assessment. This may simply consist of a comparison of the demographic characteristics of the workforce with morbidity and mortality data reported by public health authorities for such population cohorts in the area, or it may comprise the aggregate analyses of company-specific health-related data, such as health care insurance claims and the recorded causes of absenteeism and of disability retirement. Determination of the health status of the workforce through compilation of the results of health screenings, periodic medical examinations and health risk appraisal programs can be supplemented by surveys of employees’ health-related interests and concerns to identify optimal targets for the program. (It should be borne in mind that health problems affecting particular cohorts of employees that warrant attention may be obscured by relying only on data aggregated for the entire workforce.) Such needs assessments are not only useful in selecting and prioritizing program activities but also in planning to “market” them to the employees most likely to find them beneficial. They also provide a benchmark for measuring the effectiveness of the program.
Program elements
A comprehensive health promotion and disease prevention program includes a number of elements, such as the following.
Promoting the program
A constant stream of promotional devices, such as handbills, memoranda, posters, brochures, articles in company periodicals, etc., will serve to call attention to the availability and desirability of participating in the program. With their permission, stories of the accomplishments of individual employees and any awards for achieving health promotion goals they may have earned may be highlighted.
Health assessment
Where possible, each employee’s health status should be assessed on entering the program to provide a basis for a “prescription” of personal objectives to be achieved and of the specific activities that are indicated, and periodically to assess progress and interim changes in health status. The health risk appraisal may be used with or without a medical examination as comprehensive as circumstances permit, and supplemented by laboratory and diagnostic studies. Health screening programs can serve to identify those for whom specific activities are indicated.
Activities
There is a long list of activities that may be pursued as part of the program. Some are continuing, others are addressed only periodically. Some are targeted to individuals or to particular cohorts of the workforce, others to the entire employee population. Prevention of illness and disability is a common thread that runs through each activity. These activities may be divided into the following overlapping categories:
- Clinical services. These require health professionals and include: medical examinations; screening programmes; diagnostic procedures such as mammography; Pap smears and tests for cholesterol level; immunizations and so forth. They also include counseling and behaviour modification in relation to weight control, fitness, smoking cessation and other lifestyle factors.
- Health education. Education to promote awareness of potential diseases, the importance of controlling risk factors, and the value of maintaining healthy lifestyles, for instance, through weight control, fitness training and smoking cessation. Such education should also point the way to appropriate interventions.
- Guidance in managing medical care. Advice should be given with regard to the following concerns: dealing with the health care system and procuring prompt and high-quality medical care; managing chronic or recurrent health problems; rehabilitation and return to work after disease or injury; treatment for alcohol and drug abuse; prenatal care and so on.
- Coping with personal problems. Coping skills to be developed include, for example, stress management, pre-retirement planning and outplacement. Help can also be provided for workers who need to deal with work and family problems such as family planning, prenatal care, dependant care, parenting, and so forth.
- Workplace amenities and policies. Workplace features and policies supplementary to those addressing occupational health and safety activities would include personal washing-up and locker facilities, laundry service where needed, catering facilities offering nutrition advice and helpful food choices, and the establishment of a smoke-free and drug-free workplace, among others.
In general, as programs have developed and expanded and awareness of their effectiveness has spread, the number and variety of activities have grown. Some, however, have been de-emphasized as resources have either been reduced because of financial pressures or shifted to new or more popular areas.
Tools
The tools employed in pursuing health promotion activities are determined by the size and location of the organization, the degree of centralization of the workforce with respect to geography and work schedules; the available resources in terms of money, technology and skills; the characteristics of the workforce (as regards educational and social levels); and the ingenuity of the program director. They include:
- Information gathering: employee surveys; focus groups
- Print materials: books; pamphlets (these may be distributed or displayed in take-away racks); pay envelope stuffers; articles in company publications; posters
- Audiovisual materials: audiotapes; recorded messages accessible by telephone; films; videos for both individual and group viewing. Some organizations maintain libraries of audiotapes and videos which employees may borrow for home use
- Professional health services: medical examinations; diagnostic and laboratory procedures; immunizations; individual counselling
- Training: first aid; cardiopulmonary resuscitation; healthy shopping and cooking
- Meetings: lectures; courses; workshops
- Special events: health fairs; contests
- Self-help and support groups: alcohol and drug abuse; breast cancer; parenting; eldercare
- Committees: an intramural task force or committee to coordinate health-related programmes among different departments and divisions and a labour-management committee for overall programme guidance are often useful. There may also be special committees centred on particular activities
- Sports programmes: intramural sports; the sponsoring of individual participation in community programmes; company teams
- Computer software: available for individual personal computers or accessed through the organization’s network; health-promotion-oriented computer or video games
- Screening programmes: general (e.g., health risk appraisal) or disease specific (e.g., hypertension; vision and hearing; cancer; diabetes; cholesterol)
- Information and referral: employee assistance programmes; telephone resource for personal questioning and advice
- Ongoing activities: physical fitness; healthful food selection in worksite catering facilities and vending machines
- Special benefits: released time for health promotion activities; tuition reimbursement; modified work schedules; leaves of absence for particular personal or family needs
- Incentives: awards for participation or goals achievement; recognition in company publications and on bulletin boards; contests and prizes.
Implementing the Program
In many organizations, particularly smaller ones, health promotion activities are pursued on an ad hoc, haphazard basis, often in response to actual or threatened health “crises” in the workforce or in the community. After a time, however, in larger organizations, they are often pulled together into a more or less coherent framework, labelled “a program,” and made the responsibility of an individual designated as program director, coordinator or given some other title.
Selection of activities for the program may be dictated by the responses to employee interest surveys, secular events, the calendar or the suitability of the available resources. Many programs schedule activities to take advantage of the publicity generated by the categorical voluntary health agencies in connection with their annual fund-raising campaigns, for example, Heart Month, or National Fitness and Sports Week. (Each September in the United States, the National Health Information Center in the Office of Disease Prevention and Health Protection publishes National Health Observances, a list of the designated months, weeks and days devoted to the promotion of particular health issues; it is now also available via electronic mail.)
It is generally agreed that it is prudent to install the program incrementally, adding activities and topics as it gains credibility and support among the employees and to vary the topics to which special emphasis is given so that the program does not become stale. J.P. Morgan & Co., Inc., the large financial organization based in New York City, has instituted an innovative “scheduled cyclical format” in its health promotion program that emphasizes selected topics sequentially over a four-year period (Schneider, Stewart and Haughey 1989). The first year (the Year of the Heart) focuses on cardiovascular disease prevention; the second (the Year of the Body) addresses AIDS and early cancer detection and prevention; the third (the Year of the Mind) deals with psychological and social issues; and the fourth (the Year of Good Health) covers such significant topics as adult immunization, arthritis and osteoporosis, accident prevention, diabetes and healthy pregnancy. At this point, the sequence is repeated. This approach, Schneider and his co-authors state, maximizes involvement of available corporate and community resources, encourages employee participation by sequential attention to different issues, and affords the opportunity for directing attention to program revisions and additions based on medical and scientific advances.
Evaluating the Program
It is always desirable to evaluate the program both to justify continuation of its resource allocations and to identify any need for improvement and to support recommendations for expansion. The evaluation may range from simple tabulations of participation (including drop-outs) coupled with expressions of employee satisfaction (solicited and unsolicited) to more formal surveys. The data obtained by all these means will demonstrate the degree of utilization and the popularity of the program as a whole entity and of its individual components, and are usually readily available soon after the end of the evaluation period.
Even more valuable, however, are data reflecting the outcomes of the program. In an article pointing the way to improving evaluations of health promotion programs, Anderson and O’Donnell (1994) offer a classification of areas in which health promotion programs may have significant results (see figure 1).
Figure 1. Categories of health promotion outcomes.
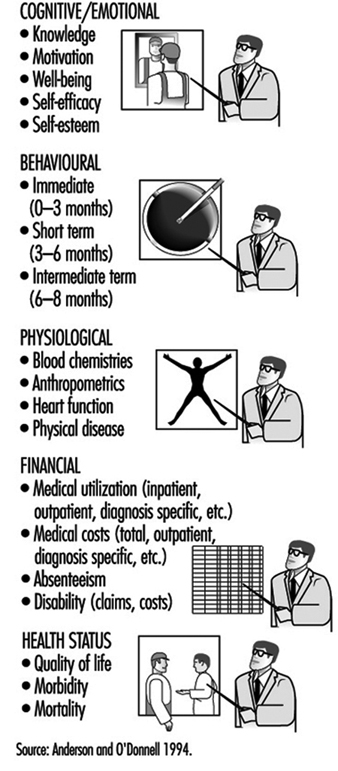
Outcome data, however, require an effort planned prior to the outset of the program, and they have to be collected over a time sufficient to allow the outcome to develop and be measured. For example, one can count the number of individuals who receive an influenza immunization and then follow the total population for a year to demonstrate that those inoculated had a lower incidence of influenza-like respiratory infections than those who refused the inoculation. The study can be enlarged to correlate rates of absenteeism of the two cohorts and compare the program costs with the direct and indirect savings accrued by the organization.
Furthermore, it is not too difficult to demonstrate individuals’ achievement of more desirable profiles of risk factors for cardiovascular disease. However, it will take at least one and probably several decades to demonstrate a reduction in morbidity and mortality from coronary heart disease in an employee population cohort. Even then, the size of that cohort may not be large enough to make such data significant.
The review articles cited above demonstrate that good evaluation research can be done and that it is increasingly being undertaken and reported. There is no question of its desirability. However, as Freis and his co-authors (1993) said, “There are already model programs that improve health and decrease costs. It is not knowledge that is lacking, but penetration of these programs into a greater number of settings.”
Comments and Caveats
Organizations contemplating the launching of a health promotion program should be cognizant of a number of potentially sensitive ethical issues to be considered and a number of pitfalls to avoid, some of which have already been alluded to. They are comprised under the following headings:
Elitism versus egalitarianism
A number of programs exhibit elitism in that some of the activities are limited to individuals above a certain rank. Thus, an in-plant physical fitness facility may be restricted to executives on the grounds that they are more important to the organization, they work longer hours, and they find it difficult to free up the time to go to an outside “health club”. To some, however, this seems to be a “perk” (i.e., a special privilege), like the key to the private washroom, admission to the free executive dining room, and use of a preferred parking space. It is sometimes resented by rank-and-file workers who find visiting a community facility too expensive and are not allowed the liberty of taking time during the working day for exercise.
A more subtle form of elitism is seen in some in-plant fitness facilities when the quota of available memberships is taken up by “jocks” (i.e., exercise enthusiasts) who would probably find ways to exercise anyway. Meanwhile, those who are sedentary and might derive much greater benefit from regular supervised exercise are denied entry. Even when they make it into the fitness program, their continued participation is often discouraged by embarrassment at being outperformed by lower-ranking workers. This is particularly true of the manager whose male self-image is tarnished when he finds that he cannot perform at the level of his female secretary.
Some organizations are more egalitarian. Their fitness facilities are open to all on a first-come, first-served basis, with continuing membership available only to those who use it frequently enough to be of value to them. Others go part of the way by reserving some of the memberships for employees who are being rehabilitated following an illness or injury, or for older workers who may require a greater inducement to participate than their younger colleagues.
Discrimination
In some areas, anti-discrimination laws and regulations may leave the organization open to complaints, or even litigation, if the health promotion program can be shown to have discriminated against certain individuals on the basis of age, sex or membership in minority or ethnic groups. This is not likely to happen unless there is a more pervasive pattern of bias in the workplace culture but discrimination in the health promotion program might trigger a complaint.
Even if formal charges are not made, however, resentment and dissatisfaction, which may be magnified as they are communicated informally among employees, are not conducive to good employee relations and morale.
Concern about allegations of sex discrimination may be exaggerated. For example, even though it is not recommended for routine use in asymptomatic men (Preventive Services Task Force 1989), some organizations offer screening for prostatic cancer to compensate for making Pap tests and mammography available to female employees.
Complaints of discrimination have come from individuals who are denied the opportunity of winning incentive awards because of congenital health problems or acquired diseases that preclude participation in health promotion activities or achieving the ideal personal health goals. At the same time, there is the equity issue of rewarding individuals for correcting a potential health problem (e.g., giving up smoking or losing excess weight) while denying such rewards to individuals who do not have such problems.
“Blaming the victim”
Growing out of the valid concept that health status is a matter of personal responsibility is the notion that individuals are culpable when health defects are found and are to be held guilty for failing to correct them on their own. This sort of thinking fails to take notice of the fact that genetic research is increasingly demonstrating that some defects are hereditary and, therefore, although they may sometimes be modified, are beyond the individual’s capacity to correct.
Examples of “blaming the victim” are (a) the too-prevalent attitude that HIV/AIDS is a fitting retribution for sexual “indiscretions” or intravenous drug use and, therefore, its victims do not deserve compassion and care, and (b) the imposition of financial and bureaucratic barriers that make it difficult for unmarried young women to get adequate prenatal care when they become pregnant.
Most important, focusing in the workplace on individuals’ responsibility for their own health problems tends to obscure the employer’s accountability for factors in job structure and work environment that may be hazardous to health and well-being. Perhaps the classic example is the organization that offers stress management courses to teach employees to cope more effectively but that does not examine and correct features of the workplace that are needlessly stressful.
It must be recognized that hazards present in the workplace may not only affect the workers, and by extension their families as well, but they may also precipitate and aggravate personal health problems generated away from the job. While retaining the concept of individual responsibility for health, it must be balanced by the understanding that factors in the workplace for which the employer is responsible may also have a health-related influence. This consideration highlights the importance of communication and coordination between the health promotion program and the employer’s occupational safety and health and other health-related programs, especially when they are not in the same box on the organization chart.
Persuasion, not coercion
A cardinal tenet of worksite health promotion programs is that participation should be voluntary. Employees should be educated about the desirability of suggested interventions, provided with access to them, and persuaded to participate in them. There often is, however, a narrow margin between enthusiastic persuasion and compulsion, between well-meaning paternalism and coercion. In many instances, the coercion may be more or less subtle: e.g., some health promotion professionals tend to be overly authoritarian; employees may be fearful of embarrassment, being ostracized or even penalized if they reject the advice given them; a worker’s choices as to recommended health promotion activities may be overly limited; and executives may make it unpleasant for their subordinates not to join them in a favorite activity, such as jogging in the very early morning.
While many organizations offer rewards for healthy behavior, for instance, certificates of achievement, prizes, and “risk-rated” health insurance (involving, in the United States, for example, a reduction in the employee’s share of the premiums), a few impose penalties on those who do not meet their arbitrary standards of health behavior. The penalties may range from refusing employment, withholding advancement, or even dismissal or denying benefits that might otherwise be forthcoming. An example of an American firm levying such penalties is E.A. Miller, a meat-packing plant located in Hyrum, Utah, a town of 4,000 inhabitants located some 40 miles north of Salt Lake City (Mandelker 1994). E.A. Miller is the largest employer in this small community and provides group health insurance for its 900 employees and their 2,300 dependants. Its health promotion activities are typical in many ways except that there are penalties for not participating:
- Employees and spouses who do not attend prenatal seminars are not reimbursed for the cost of obstetrical care or of the baby’s care in the hospital. Also, to qualify for the insurance benefits, the pregnant woman must visit a doctor during the first trimester.
- If employees or their dependants smoke, they must contribute over twice as much to their share of group health insurance premiums: $66 per month instead of $30. The plant has had a smoke-free policy since 1991 and the company offers smoking cessation courses onsite or pays employees’ tuition if they take the course in the community.
- The company will not cover any of the medical costs if a covered employee or dependant was injured in an automobile accident while driving under the influence of drugs or alcohol or was not wearing a seat belt, nor will it cover injuries sustained while riding a motorcycle without a helmet.
One form of coercion that has wide acceptance is “job jeopardy” for employees whose alcohol or drug abuse has had an impact on their attendance and work performance. Here, the employee is confronted with the problem and told that disciplinary actions will be stayed as long as he or she continues with the prescribed treatment and remains abstinent. With allowance for an occasional relapse (in some organizations, this is limited to a specific number), failure to comply results in dismissal. Experience has amply shown that the threat of job loss, regarded by some as the most potent stressor encountered in the workplace, is an effective motivator for many individuals with such problems to agree to take part in a program for their correction.
Confidentiality and privacy
Another hallmark of the successful health promotion program is that personal information about participating employees —and non-participants as well—must be kept confidential and, particularly, out of personnel files. To preserve the privacy of such information when it is needed for evaluative tabulations and research, some organizations have set up data bases in which individual employees are identified by code numbers or by some similar device. This is particularly relevant to mass screening and laboratory procedures where clerical errors are not unknown.
Who participates
Health promotion programs are criticized by some on the basis of evidence that participants tend to be younger, healthier and more health conscious than those who do not (the “coals to Newcastle” phenomenon). This presents to those designing and operating programs the challenge of involving those who have more to gain through their participation.
Who pays
Health promotion programs involve some costs to the organization. These may be expressed in terms of financial outlays for services and materials, time taken from work hours, distraction of participating employees, and the burden of management and administration. As noted above, there is increasing evidence that these are more than offset by reduced personnel costs and by improvements in productivity. There are also the less tangible benefits of embellishing the public relations image of the organization and of enhancing its reputation as a good place to work, thereby facilitating recruitment efforts.
Most of the time, the organization will cover the entire cost of the program. Sometimes, particularly when an activity is conducted off the premises in a community-based facility, the participants are required to share its cost. In some organizations, however, all or part of the employee’s portion is refunded on successful completion of the program or course.
Many group health insurance programs cover preventive services provided by health professionals including, for example, immunizations, medical examinations, tests, and screening procedures. Such health insurance coverage, however, presents problems: it may increase the cost of the insurance and the out-of-pocket costs of the deductible fees and co-payments usually required may constitute an effective obstacle to their use by low-salaried workers. In the last analysis, it may be less costly for employers to pay for preventive services directly, saving themselves the administrative costs of processing insurance claims and of reimbursement.
Conflicts of interest
While most health professionals exhibit exemplary integrity, vigilance must be exercised to identify and deal with those who do not. Examples include those who falsify records to make their efforts look good and those who have a relationship with an outside provider of services who provides kickbacks or other rewards for referrals. The performance of outside vendors should be monitored to identify those who underbid to win the contract and then, to save money, use poorly qualified personnel to deliver the services.
A more subtle conflict of interest exists when staff members and vendors subvert the needs and interests of employees in favor of the organization’s goals or the agenda of its managers. This sort of reprehensible action may not be explicit. An example is steering troubled employees into a stress management program without making a strenuous effort to persuade the organization to reduce inordinately high levels of stress in the workplace. Experienced professionals will have no difficulty in properly serving both the employees and the organization, but should be ready to move to a situation in which ethical values are more conscientiously observed whenever improper pressures on the part of management become too great.
Another subtle conflict that may affect employees adversely arises when a relationship of competition, rather than coordination and collaboration, develops between the health promotion program and other health-related activities in the organization. This state of affairs is found not infrequently when they are placed in different areas of the organization chart and report to different lines of management authority. As has been said before, it is critical that, even when part of the same entity, the health promotion program should not operate at the expense of the occupational safety and health program.
Stress
Stress is probably the most pervasive health hazard encountered both in the workplace and away from it. In a landmark survey sponsored by the St. Paul Fire and Marine Insurance Company and involving nearly 28,000 workers in 215 diverse American organizations, Kohler and Kamp (1992) found that work stress was strongly related to employee health and performance problems. They also found that among personal life problems, those created by the job are most potent, showing more impact than purely off-the-job issues such as family, legal or financial problems. This suggests, they said, that “some workers become caught in a downward spiral of work and home life problems—problems on the job create problems at home, which in turn are taken back to work, and so on.” Accordingly, while primary attention should be directed to the control of psychosocial risk factors intrinsic to the job, this should be complemented by health promotion activities aimed at personal stress factors most likely to affect work performance.
Access to health care
A subject worthy of attention in its own right, education in navigating the health care delivery system should be made part of the program with an eye to future needs for health services. This begins with self-care—knowing what to do when signs and symptoms appear and when professional services are needed—and goes on to selecting a qualified health professional or a hospital. It also includes inculcating both the ability to distinguish good from poor health care and an awareness of patients’ rights.
To save employees time and money, some in-plant medical units offer more or less extensive in-plant health services, (often including x rays, laboratory tests and other diagnostic procedures), reporting the results to the employees’ personal physicians. Others maintain a roster of qualified physicians, dentists and other health professionals to whom employees themselves and sometimes also their dependants may be referred. Time off from work to keep medical appointments is an important adjunct where health professional services are not available outside of working hours.
In the United States, even where there is a good group health insurance program, low-salaried workers and their families may find the deductible and coinsurance portions of covered charges to be barriers to procuring recommended health services in all but dire circumstances. Some employers are helping to overcome such obstacles by exempting these employees from such payments or by making special fee arrangements with their health care providers.
Worksite “climate”
Worksite health promotion programs are presented, often explicitly, as an expression of the employer’s concern for the health and well-being of the workforce. That message is contradicted when the employer is deaf to employees’ complaints about working conditions and does nothing to improve them. Employees are not likely to accept or participate in programs offered under such circumstances or at times of labor-management conflict.
Workforce diversity
The health promotion program should be designed to accommodate to the diversity increasingly characteristic of today’s workforce. Differences in ethnic and cultural background, educational levels, age and sex should be recognized in the content and presentation of health promotion activities.
Conclusion
It is clear from all of the above that the worksite health promotion program represents an extension of the occupational safety and health program which, when properly designed and implemented, can benefit individual employees, the workforce as a whole and the organization. In addition, it may also be a force for positive social change in the community.
Over the past few decades, worksite health promotion programs have increased in number and comprehensiveness, in small and medium-sized organizations as well as in larger ones, and in the private, voluntary and public sectors. As demonstrated by the array of articles contained in this chapter, they have also increased in scope, expanding from direct clinical services dealing, for example, with medical examinations and immunizations, to involvement with personal and family problems whose relationship to the workplace may seem more tenuous. One should allow one’s selection of program elements and activities to be guided by the particular characteristics of the workforce, the organization and the community, keeping in mind that some will be needed only by specific cohorts of employees rather than by the population as a whole.
In considering the creation of a worksite health promotion program, readers are advised to plan carefully, to implement incrementally, allowing room for growth and expansion, to monitor performance and program quality and, to the extent possible, evaluate outcomes. The articles in this chapter should prove to be uniquely helpful in such an endeavor.
A New Approach to Learning and Training: A Case Study by the ILO-FINNIDA African Safety and Health Project
Abuya: What’s the matter? You look worn out.
Mwangi: I am worn out—and disgusted. I was up half the night getting ready for this lecture I just gave and I don’t think it went very well. I couldn’t get anything out of them—no questions, no enthusiasm. For all I know, they didn’t understand a word I said.
Kariuki: I know what you mean. Last week I was having a terrible time trying to explain chemical safety in Swahili.
Abuya: I don’t think it’s the language. You were probably just talking over their heads. How much technical information do these workers really need to know anyway?
Kariuki: Enough to protect themselves. If we can’t get the point across, we’re just wasting our time. Mwangi, why didn’t you try asking them something or tell a story?
Mwangi: I couldn’t figure out what to do. I know there has to be a better way, but I was never trained in how to do these lectures right.
Abuya: Why all the fuss? Just forget about it! With all the inspections we have to do, who’s got time to worry about training?
The above discussion in an African factory inspectorate, which could take place anywhere, highlights a real problem: how to get the message through in a training session. Using a real problem as a discussion starter (or trigger) is an excellent training technique to identify potential obstacles to training, their causes and potential solutions. We have used this discussion as a role play in our Training of Trainers’ workshops in Kenya and Ethiopia.
The ILO-FINNIDA African Safety and Health Project is part of the ILO’s technical cooperation activities aimed to improve occupational safety and health training and information services in 21 African countries where English is commonly spoken. It is sponsored by FINNIDA, the Finnish International Development Agency. The Project took place from 1991 to 1994 with a budget of US$5 million. One of the main concerns in the implementation of the Project was to determine the most appropriate training approach by which to facilitate high quality learning. In the following case study we will describe the practical implementation of the training approach, the Training the Trainers’ (TOT) course (Weinger 1993).
Development of a New Training Approach
In the past, the training approach in most African factory inspectorates, and also in many technical cooperation projects of the ILO, has been based on randomly selected, isolated topics of occupational safety and health (OSH) which were presented mainly by using lecturing methods. The African Safety and Health Project conducted the first pilot course in TOT in 1992 for 16 participating countries. This course was implemented in two parts, the first part dealing with basic principles of adult education (how people learn, how to establish learning objectives and select teaching contents, how to design the curriculum and select instructional methods and learning activities and how to improve personal teaching skills) and the second part with practical training in OSH based on individual assignments which each participant completed during a four month’s time period following the first part of the course.
The main characteristics of this new approach are participation and action orientation. Our training does not reflect the traditional model of classroom learning where participants are passive recipients of information and the lecture is the dominant instructional method. In addition to its action orientation and participatory training methods, this approach is based on the latest research in modern adult education and takes a cognitive and activity-theoretical view of learning and teaching (Engeström 1994).
On the basis of the experience gained during the pilot course, which was extremely successful, a set of detailed course material was prepared, call the Training of Trainers Package, which consists of two parts, a trainer’s manual and a supply of participants’ handout matter. This package was used as a guideline during planning sessions, attended by from 20 to 25 factory inspectors over a period of ten days, and concerned with establishing national TOT courses in Africa. By the spring of 1994, national TOT courses had been implemented in two African countries, Kenya and Ethiopia.
High Quality Learning
There are four key components of high quality learning.
Motivation for learning. Motivation occurs when participants see the “use-value” of what they are learning. It is stimulated when they can perceive the gap that separates what they know and what they need to know to solve a problem.
Organization of subject matter. The content of learning is too commonly thought of as separate facts stored in the brain like items in boxes on a shelf. In reality, people construct models, or mental pictures, of the world while learning. In promoting cognitive learning, teachers try to organize facts into models for better learning and include explanatory principles or concepts (the “but whys” behind a fact or skill).
Advancing through steps in the learning process. In the learning process, the participant is like an investigator looking for a model by which to understand the subject matter. With the help of the teacher, the participant forms this model, practices using it and evaluates its usefulness. This process can be divided into the following six steps:
- motivation
- orientation
- integrating new knowledge (internalization)
- application
- programme critique
- participant evaluation.
Social interaction. The social interaction between participants in a training session is an essential component of learning. In group activities, participants learn from one another.
Planning training for high quality learning
The kind of education aimed at particular skills and competencies is called training. The goal of training is to facilitate high quality learning and it is a process that takes place in a series of steps. It requires careful planning at each stage and each step is equally important. There are many ways of breaking the training into components but from the point of view of the cognitive conception of learning, the task of planning a training course can be analysed into six steps.
Step 1: Conduct a needs assessment (know your audience).
Step 2: Formulate learning objectives.
Step 3: Develop an orientation basis or “road map” for the course.
Step 4: Develop the curriculum, establishing its contents and associated training methods and using a chart to outline your curriculum.
Step 5: Teach the course.
Step 6: Evaluate the course and follow up on the evaluation.
Practical Implementation of National TOT Courses
Based on the above-mentioned training approach and experience from the first pilot course, two national TOT courses were implemented in Africa, the one in Kenya in 1993 and the other in Ethiopia in 1994.
Training needs were based on the work activity of factory inspectors and were determined by means of a pre-workshop questionnaire and a discussion with the course participants about their everyday work and about the kinds of skills and competencies necessary to carry it out (see figure 1). The course has thus been designed primarily for factory inspectors (in our national TOT courses, usually 20 to 25 inspectors participated), but it could be extended to other personnel who may need to carry out safety and health training, such as shop stewards, foremen, and safety and health officers.
Figure 1. Orientation basis for the factory inspector's work activity.

A compilation of course objectives for the national TOT course was assembled step by step in cooperation with the participants, and is given immediately below.
Objectives of the national TOT course
The aims of the training of trainers (TOT) course are as follows:
- Increase participants’ understanding of the changing role and tasks of factory inspectors from immediate enforcement to long-term advisory service, including training and consultation.
- Increase participants’ understanding of the basic principles of high quality learning and instruction.
- Increase participants’ understanding of the variety of skills involved in planning training programmes: identification of training needs, formulation of learning objectives, development of training curricula and materials, selection of appropriate teaching methods, effective presentation and programme evaluation.
- Enhance participants’ skills in effective communication for application during inspections and consultation, as well as in formal training sessions.
- Facilitate the development of short and long-term training plans in which new instructional practices will be implemented.
Course contents
The key subject areas or curriculum units that guided the implementation of the TOT course in Ethiopia are outlined in figure 2. This outline may also serve as an orientation basis for the whole TOT course.
Figure 2. The key subject areas of the TOT course.
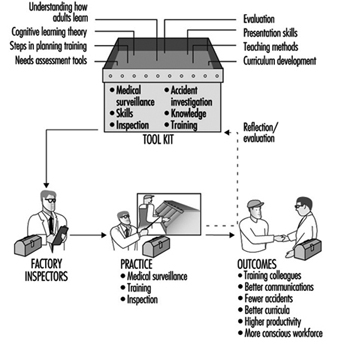
Determining training methods
The external aspect of the teaching method is immediately observable when you step into a classroom. You might observe a lecture, a discussion, group or individual work. However, what you do not see is the most essential aspect of teaching: the kind of mental work being accomplished by the student at any given moment. This is called the internal aspect of the teaching method.
Teaching methods can be divided into three main groups:
- Instructional presentation: participant presentations, lectures, demonstrations, audio-visual presentations
- Independent assignment: tests or exams, small group activities, assigned reading, use of self-guided learning materials, role plays
- Cooperative instruction
Most of the above methods were used in our TOT courses. However, the method one selects depends on the learning objectives one wants to achieve. Each method or learning activity should have a function. These instructional functions, which are the activities of a teacher, correspond with the steps in the learning process described above and can help guide your selection of methods. There follows a list of the nine instructional functions:
- preparation
- motivation
- orientation
- transmitting new knowledge
- consolidating what has been taught
- practising (development of knowledge into skills)
- application (solving new problems with the help of new knowledge)
- programme critique
- participant evaluation.
Planning the curriculum: Charting your course
One of the functions of curriculum or course plan is to assist in guiding and monitoring the teaching and learning process. The curriculum can be divided into two parts, the general and the specific.
The general curriculum gives an overall picture of the course: its goals, objectives, contents, participants and guidelines for their selection, the teaching approach (how the course will be conducted) and the organizational arrangements, such as pre-course tasks. This general curriculum would usually be your course description and a draft programme or list of topics.
A specific curriculum provides detailed information on what one will teach and how one plans to teach it. A written curriculum prepared in chart form will serve as a good outline for designing a curriculum specific enough to serve as a guide in the implementation of the training. Such a chart includes the following categories:
Time: the estimated time needed for each learning activity
Curriculum Units: primary subject areas
Topics: themes within each curriculum unit
Instructional function: the function of each learning activity in helping to achieve your learning objectives
Activities: the steps for conducting each learning activity
Materials: the resources and materials needed for each activity
Instructor: the trainer responsible for each activity (when there are several trainers)
To design the curriculum with the aid of the chart format, follow the steps outlined below. Completed charts are illustrated in connection with a completed curriculum in Weinger 1993.
- Specify the primary subject areas of the course (curriculum units) which are based on your objectives and general orientation basis.
- List the topics you will cover in each of those areas.
- Plan to include as many instructional functions as possible in each subject area in order to advance through all the steps of the learning process.
- Choose methods which fulfil each function and estimate the amount of time required. Record the time, topic and function on the chart.
- In the activities column, provide guidelines for the instructor on how to conduct the activity. Entries can also include main points to be covered in this session. This column should offer a clear picture of exactly what will occur in the course during this time period.
- List the materials, such as worksheets, handouts or equipment required for each activity.
- Make sure to include appropriate breaks when designing a cycle of activities.
Evaluating the course and follow-up
The last step in the training process is evaluation and follow-up. Unfortunately, it is a step that is often forgotten, ignored and, sometimes, avoided. Evaluation, or the determination of the degree to which course objectives were met, is an essential component of training. This should include both programme critique (by the course administrators) and participant evaluation.
Participants should have an opportunity to evaluate the external factors of teaching: the instructor’s presentation skills, techniques used, facilities and course organization. The most common evaluation tools are post-course questionnaires and pre- and post-tests.
Follow-up is a necessary support activity in the training process. Follow-up activities should be designed to help the participants apply and transfer what they have learned to their jobs. Examples of follow-up activities for our TOT courses include:
- action plans and projects
- formal follow-up sessions or workshops
Selection of trainers
Trainers were selected who were familiar with the cognitive learning approach and had good communication skills. During the pilot course in 1992 we used international experts who had been involved in development of this learning approach during the 1980s in Finland. In the national courses we have had a mixture of experts: one international expert, one or two regional experts who had participated in the first pilot course and two to three national resource persons who either had responsibility for training in their own countries or who had participated earlier in this training approach. Whenever it was possible, project personnel also participated.
Discussion and Summary
Factory training needs assessment
The factory visit and subsequent practice teaching are a highlight of the workshop. This training activity was used for workplace training needs assessment (curriculum unit VI A, figure 1). The recommendation here would be to complete the background on theory and methods prior to the visit. In Ethiopia, we scheduled the visit prior to addressing ourselves to the question of teaching methods. While two factories were looked at, we could have extended the time for needs assessment by eliminating one of the factory visits. Thus, visiting groups will visit and focus on only that factory where they will be actually training.
The risk mapping component of the workshop (this is also part of curriculum unit VI A) was even more successful in Ethiopia than in Kenya. The risk maps were incorporated in the practice teaching in the factories and were highly motivating for the workers. In future workshops, we would stress that specific hazards be highlighted wherever they occur, rather than, for example, using a single green symbol to represent any of a variety of physical hazards. In this way, the extent of a particular type of hazard is more clearly reflected.
Training methods
The instructional methods focused on audio-visual techniques and the use of discussion starters. Both were quite successful. In a useful addition to the session on transparencies, the participants were asked to work in groups to develop a transparency of their own on the contents of an assigned article.
Flip charts and brainstorming were new teaching methods for participants. In fact, a flip chart was developed especially for the workshop. In addition to being an excellent training aid, the use of flip charts and “magic markers” is a very inexpensive and practical substitute for the overhead projector, which is unavailable to most inspectors in the developing countries.
Videotaped microteaching
“Microteaching”, or instruction in the classroom focusing on particular local problems, made use of videotape and subsequent critique by fellow participants and resource people, and was very successful. In addition to enhancing the working of external teaching methods, the taping was a good opportunity for comment on areas for improvement in content prior to the factory teaching.
A common error, however, was the failure to link discussion starters and brainstorm activities with the content or message of an activity. The method was perfunctorily executed, and its effect ignored. Other common errors were the use of excessively technical terminology and the failure to make the training relevant to the audience’s needs by using specific workplace examples. But the later presentations in the factory were designed to clearly reflect the criticisms that participants had received the day before.
Practice teaching in the factory
In their evaluation of the practice teaching sessions in the factory, participants were extremely impressed with the use of a variety of teaching methods, including audiovisuals, posters that they developed, flip charts, brainstorming, role plays, “buzz groups” and so on. Most groups also made use of an evaluation questionnaire, a new experience for them. Of particular note was their success in engaging their audiences, after having relied solely on the lecture method in the past. Common areas for improvement were time management and the use of overly technical terms and explanations. In the future, the resource persons should also try to ensure that all groups include the application and evaluation steps in the learning process.
Course planning as a training experience
During these two courses it was possible to observe significant changes in the participants’ understanding of the six steps in high quality learning.
In the last course a section on writing objectives, where each participant writes a series of instructional objectives, was added into the programme. Most participants had never written training objectives and this activity was extremely useful.
As for the use of the curriculum chart in planning, we have seen definite progress among all participants and mastery by some. This area could definitely benefit from more time. In future workshops, we would add an activity where participants use the chart to follow one topic through the learning process, using all of the instructional functions. There is still a tendency to pack the training with content material (topics) and to intersperse, without due consideration of their relevance, the various instructional functions throughout a series of topics. It is also necessary that trainers emphasize those activities that are chosen to accomplish the application step in the learning process, and that they acquire more practice in developing learners’ tasks. Application is a new concept for most and difficult to incorporate in the instructional process.
Finally the use of the term curriculum unit was difficult and sometimes confusing. The simple identification and ordering of relevant topic areas is an adequate beginning. It was also obvious that many other concepts of the cognitive learning approach were difficult, such as the concepts of orientation basis, external and internal factors in learning and teaching, instructional functions and some others.
In summary, we would add more time to the theory and curriculum development sections, as outlined above, and to the planning of future curriculum, which affords the opportunity of observing individual ability to apply the theory.
Conclusion
The ILO-FINNIDA African Safety and Health Project has undertaken a particularly challenging and demanding task: to change our ideas and old practices about learning and training. The problem with talking about learning is that learning has lost its central meaning in contemporary usage. Learning has come to be synonymous with taking in information. However, taking in information is only distantly related to real learning. Through real learning we re-create ourselves. Through real learning we become able to do something we were never able to do before (Senge 1990). This is the message in our Project’s new approach on learning and training.
Training of Health and Safety Professionals
Categories of Occupational Safety and Health Professionals Requiring Training and Education
The delivery of occupational safety and health services requires a highly-trained and multidisciplinary team. In a few less-developed countries, such a team may not exist, but in the vast majority of countries in the world, experts in different aspects of OSH are usually at least available though not necessarily in sufficient numbers.
The question of who belong to the categories of OSH professionals is fraught with controversy. Usually there is no dispute that occupational physicians, occupational nurses, occupational hygienists and safety professionals (sometimes referred to as safety practitioners) are OSH professionals. However, there are also members of many other disciplines who can make a plausible claim to belonging to the OSH professions. They include those ergonomists, toxicologists, psychologists and others who specialize in the occupational aspects of their subjects. For the purpose of this article, nevertheless, the training of these latter types of personnel will not be discussed, as the main focus of their training is often not on OSH.
Historical Perspective
In most countries, specific OSH training is of fairly recent origin. Until the Second World War, most OSH professionals received little or no formal training in their chosen calling. Few schools of public health or universities provided formal OSH courses, though some such institutions offered OSH as a subject in the context of a wider degree course, usually in public health. Segments of OSH were taught at the postgraduate level for physicians training in disciplines such as dermatology or respiratory medicine. Some engineering aspects of safety, such as machine guarding, were taught in technological and engineering schools. In most countries, even training in individual components of occupational hygiene courses were hard to find before the Second World War. The development of occupational nursing training is even more recent.
In the developed countries, OSH training received a boost during the Second World War, just as OSH services did. The mass mobilization of whole nations for the war effort led to greater emphasis on protecting the health of workers (and therefore their fighting capability or productivity with respect to the manufacturing of more munitions, warplanes, tanks and warships). At the same time, however, wartime conditions and the drafting of both university teachers and students into the armed forces made it extremely difficult to set up formal courses of OSH training. After the Second World War, however, many such courses were established, some with the help of the generous study grants for demobilized servicemen awarded by grateful governments.
After the Second World War, most colonies of European empires achieved independence and embarked upon the path of industrialization to a greater or lesser extent as a means to national development. Before long, such developing countries found themselves confronting the ills of the industrial revolution of nineteenth-century Europe, but within a much telescoped time span and on an unprecedented scale. Occupational accidents and diseases and environmental pollution became rampant. This led to the development of OSH training, although even today there are large variations in the availability of such training in these countries.
Review of Current International Initiatives
International Labour Organization (ILO)
There have been several initiatives of the ILO in recent years which relate to OSH training. Many of them relate to practical training for interventive measures at the worksite. Some other initiatives are carried out in collaboration with national governments (Rantanen and Lehtinen 1991).
Other ILO activities since the 1970s have been carried on largely in developing countries throughout the world. Several such activities relate to the upgrading of training of factory inspectors in countries such as Indonesia, Kenya, the Philippines, Tanzania, Thailand, and Zimbabwe.
The ILO, together with other United Nations agencies such as the United Nations Development Programme, has also assisted in the establishment or upgrading of national institutes of OSH, the training functions of which are usually among their top priorities.
The ILO has also produced several practical monographs which are very useful as training materials for OSH courses (Kogi, Phoon and Thurman 1989).
World Health Organization (WHO)
The WHO has held in recent years a number of important international and regional conferences and workshops on OSH training. In 1981, a conference entitled “Training of Occupational Health Personnel” was held under the auspices of the Regional Office for Europe of the WHO. In the same year, the WHO convoked with the ILO a Joint ILO/WHO Committee on Occupational Health which focused on “educational and training in occupational health, safety and ergonomics” (WHO 1981). That meeting assessed the needs for education and training at different levels, developed policies in education and training and advised on methodology and programmes for education and training (WHO 1988).
In 1988 a WHO Study Group published a report entitled Training and Education in Occupational Health to address particularly the new policies on primary health care strategies adopted by the WHO member states, new needs resulting from technological developments and new approaches to health promotion at work (WHO 1988).
International Commission on Occupational Health (ICOH)
In 1985, the ICOH established a Scientific Committee on Education and Training in Occupational Health. This Committee has organized four international conferences as well as mini-symposia on the subject in the International Congresses on Occupational Health (ICOH 1987). Among the conclusions of the second conference, the need to develop training strategies and training methodologies received prominent mention in the list of priority issues (ICOH 1989).
A main feature of the third conference was the methodology of OSH training, including such functions as learning by participation, problem-based learning and evaluation of courses, teaching and students (ICOH 1991).
Regional initiatives
In different parts of the world, regional bodies have organized training activities in OSH. For example, the Asian Association of Occupational Health, established in 1954, has a Technical Committee in Occupational Health Education which conducts surveys on training of medical students and related subjects.
Types of Professional Programmes
Degree-granting and similar programmes
Probably the prototype of degree-granting and similar programmes is the sort which was developed in schools of public health or equivalent establishments. Higher education for public health is a relatively recent development. In the United States, the first school dedicated to this purpose was established in 1916 as the Institute of Hygiene at Johns Hopkins University. At that time, the overriding public health concerns centred around the communicable diseases. As time went on, education about the prevention and control of man-made hazards and about occupational health drew increasing emphasis in the training programmes of schools of public health (Sheps 1976).
Schools of public health offer OSH courses for a postgraduate diploma or for the degree of Master of Public Health, allowing students to concentrate in occupational health. Usually entry requirements include the possession of a tertiary educational qualification. Some schools insist upon relevant prior experience in OSH as well. The duration of training on a full-time basis is usually one year for the diploma and two years for the Master’s course.
Some of the schools train the different OSH personnel together in core courses, with training in the specific OSH disciplines (e.g., occupational medicine, hygiene or nursing) being offered to students specializing in these areas. This common training is probably a great advantage, as trainees of the different OSH disciplines could develop a greater understanding of each other’s functions and a better experience of team work.
Especially in recent years, schools of medicine, nursing and engineering have offered courses similar to those in schools of public health.
A few universities are offering OSH courses at the basic or undergraduate level. Unlike the traditional OSH tertiary courses, admission to which is usually dependent upon the acquisition of a previous degree, these newer courses admit students who have just graduated from high school. Much controversy still surrounds the merits of this development. Proponents of such courses argue that they produce more OSH professionals in less time and at lower cost. Their opponents argue that OSH practitioners are more effective if they build their OSH training on a basic discipline into which they integrate their special OSH practice, such as occupational medicine or nursing. Knowledge of basic sciences may be acquired at the specialization level if they have not been taught as part of undergraduate training.
Training courses in OSH for physicians vary in their clinical component. The conference, mentioned above, on the training of occupational health personnel organized by the WHO/Regional Office for Europe emphasized that “occupational medicine is fundamentally a clinical skill and its practitioners must be fully competent in clinical medicine”. It must also be stressed that the diagnosis of chemical intoxication among workers is largely clinical, as is the differentiation between “occupational disease” and other diseases and their management (Phoon 1986). It has become, therefore, a worldwide trend to insist upon postings to different clinics as part of the training of the occupational physician. In the United States and Canada, for example, trainees undergo a four-year residency programme which includes a substantial clinical component in such subjects as dermatology and respiratory medicine in addition to the curriculum required for the degree of Master of Public Health or its equivalent.
Formal training for occupational nurses probably varies even more in different parts of the world than that for occupational physicians. These differences hinge on the variations of responsibilities and functions of occupational nurses. Some countries define occupational health nursing as “the application of nursing principles in conserving the health of workers in all occupations. It involves prevention, recognition, and treatment of illness and injury and requires special skills and knowledge in the fields of health education and counselling, environmental health, rehabilitation and human relations” (Kono and Nishida 1991).On the other hand, other countries understand occupational nursing as the role of the nurse in an interdisciplinary occupational health team, who is expected to participate in all the fields of general health management, delivery of health services, environmental control, healthy and safe working procedures and OSH education. A survey in Japan showed, however, that not all the graduates from an occupational nursing staff took part in all these activities. This was probably due to a lack of understanding of the nurse’s role in OSH and to inadequate training in some of the fields (Kono and Nishida 1991).
The discipline of occupational hygiene has been defined by the American Industrial Hygiene Association as the science and art devoted to the recognition, evaluation and control of those environmental factors and stresses, arising in or from the workplace, which may cause sickness, impaired health and well-being, or significant discomfort and inefficiency among workers or among the citizens of the community. Speciality training has also emerged within the general field of occupational hygiene, including that in chemistry, engineering, noise, radiation, air pollution and toxicology.
Curricula for Occupational Safety and Health Personnel
The detailed contents of the curricula for the training of occupational physicians, nurses, hygienists and safety personnel, as recommended by the 1981 Joint ILO/WHO Committee an Occupational Health mentioned above will be represented in the pages to follow. As regards the main subject areas to be taught, the Committee recommends:
- organization of occupational safety and health services, their activities, legislation and regulations
- occupational medicine
- occupational hygiene
- occupational safety
- work physiology and ergonomics, dealing particularly with the adaptation of work to man, but also with the readjustment of the handicapped to work
- occupational psychology, sociology and health education.
According to the profile of the personnel, the educational programmes will go more or less deeply into different subjects to meet the demands of the respective professions, as discussed below for several categories.
It is difficult to comment in detail what should go into the curricula of OSH courses. It is generally agreed that such courses should have a greater input of behavioural sciences than is now the case, but such input should be relevant to the sociocultural milieu of a particular country or region for which a course is designed. Moreover, OSH should not be taught in isolation from the general health services and the community health situation in a given country or region. The fundamentals of management science should be included in OSH curricula to improve the understanding of organizational structures and practices in enterprises as well as to enhance administrative skills of OSH professionals. The art of communication and the ability to conduct an investigation of OSH problems scientifically and to formulate solutions were also recommended for inclusion in all OSH curricula (Phoon 1985b).
Physicians and nurses
All medical students should be taught some occupational health. In some countries, there are separate courses; in others, occupational health is dealt with in such courses as physiology, pharmacology and toxicology, public health, social medicine and internal medicine. Nevertheless, medical students do not, as a rule, acquire sufficient knowledge and skill to allow them to practice occupational health independently, and some postgraduate training in occupational health and safety is necessary. For further specialization in occupational health (e.g., occupational diseases, or even more narrow fields, like occupational neurology or dermatology), postgraduate training programmes should be available. For nurses active in occupational health services, both long-term and short-term courses need to be organized, depending on their range of activities.
Figure 1 lists subjects to be included in specialized postgraduate training for physicians and nurses.
Figure 1. Postgraduate training syllabus for physicians and nurses.
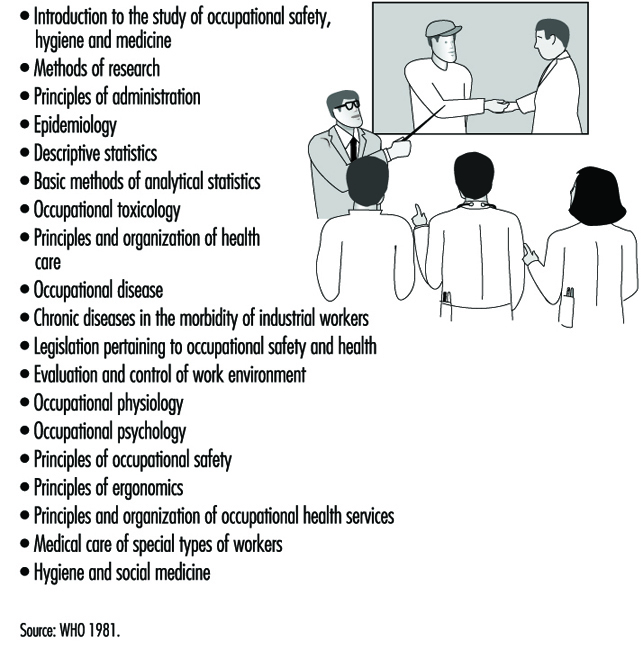
Safety and health engineers and safety officers
The practice of occupational safety is concerned with such failures of materials, machines, processes and structures as may give rise to dangerous situations, including the release of harmful agents. The aim of education in this field is to enable students to foresee danger, both at the planning stage of projects and in existing situations, to quantify the danger and to design measures to combat it. Training in occupational safety involves the student in a substantial study of selected topics from engineering and materials science, particularly those related to mechanical, civil, chemical, electrical and structural engineering.
Separate curricular units would be concerned, for example, with the structure and strength of materials, in mechanical engineering; with forces in structures, in civil engineering; with handling and transportation of chemicals, in chemical engineering; with design standards, protective equipment and the theory of preventive maintenance, in electrical engineering; and with the behaviour of strata, in mining engineering.
Safety engineers, in addition to acquiring a basic knowledge, should also undergo a course of specialization. The 1981 Joint ILO/WHO Committee recommendations for a specialized safety engineering course of study are listed in figure 2.
Figure 2. A syllabus for specialization in safety engineering.
Courses can be either full-time, part-time or “sandwich courses”—in the lattermost case, periods of studying are interspersed with periods of practice. The selection of which courses to take is very much a matter of individual circumstances or preference. This is especially true since many safety practitioners have extensive knowledge gained through on-the-job experience in particular industries. However, within a large community or a country, there should preferably be a large range of choices to cater for all these different needs.
The recent enormous advances in communications technology should enable the greater usage of distance-learning courses which can be delivered both to remote areas of a country or even across national frontiers. Unfortunately, such technology is still quite expensive, and countries or areas which need such distance-learning capabilities most may be the very ones least able to afford them.
Primary health care practitioners
There is a severe shortage of OSH professionals in developing countries. In addition, among primary health care practitioners and health professionals as a whole, there is a tendency to direct their main activities to curative services. This should be counterbalanced with the help of appropriate training to emphasize the great value of instituting preventive measures at the workplace in collaboration with other responsible parties such as workers and managers. This would help, to a certain extent, to alleviate the problems caused by the present shortage of OSH personnel in developing countries (Pupo-Nogueira and Radford 1989).
A number of developing countries have recently embarked on short courses of OSH training for primary health care and public health personnel. There is a wide spectrum of organizations which have undertaken such training. They include national productivity boards (Phoon 1985a), farmers’ associations, national safety councils, national institutes of health, and professional bodies such as medical and nurses’ associations (Cordes and Rea 1989).
A scarcity of OSH professionals affects not only developing countries, but many developed ones as well. In the United States, one response to this problem took the form of a joint report by a preventive medicine and internal medicine study group that recommended that training programmes in internal medicine emphasize controls of hazards in the workplace and in the environment, since most patients seen by internists are members of the workforce. Furthermore, the American Academy of Family Physicians and the American Medical Association have published several monographs on occupational health for the family physician. A study by the American Institute of Medicine reaffirmed the role of the primary care physician in occupational health, outlined the basic skills required and emphasized the need to enhance occupational health activity in basic training and continuing education (Ellington and Lowis 1991). In both developed and developing countries, however, there is still an inadequate number of OSH training programmes for primary health care personnel and an insufficient number of trained personnel.
Multidisciplinary training
Training in the multidisciplinary nature of OSH can be enhanced by making sure that everyone who trains is fully familiar with the roles, activities and areas of concern of the other OSH personnel. In an OSH course in Scotland, for example, members of the different OSH professions participate in the teaching programme. The students are also provided with self-instruction packages designed to give them detailed knowledge of and insight into the different OSH professional areas. Extensive use is also made of experiential learning techniques such as role-playing simulations and participative case studies. For example, students are asked to complete personal checklists on how each particular area of occupational health activity is likely to affect them in their own work situations, and on how they can cooperate effectively with other occupational health professionals.
In the running of a multidisciplinary OSH course, a key element is the mix of learners of different professional backgrounds in the same class. The course material, such as group exercises and essays, must be carefully selected without any bias to a particular discipline. Lecturers must also receive training in the setting of multidisciplinary questions and problems (D’Auria, Hawkins and Kenny 1991).
Continuing Education
In professional education as a whole, there is an increasing awareness of the need for continuing education. In the field of OSH, new knowledge concerning old hazards and new problems arising from changes in technology are developing so rapidly that no OSH practitioner could hope to keep up to date without making a systematic and constant effort to do so.
Continuing education in OSH can be formal or informal, voluntary or obligatory in order to maintain certification. It is essential for every OSH practitioner to keep up with reading the key professional journals, at least in his or her own disciplines. When a new hazard is encountered, it would be very useful to mount a literature search on that subject through a library. If such a library is unavailable, the CIS service of the ILO could be asked to undertake that service instead. Moreover, having continual and direct access to at least a few up-to-date texts on OSH is essential to any kind of OSH practice.
More formal kinds of continuing education could take the form of conferences, workshops, lectures, journal clubs or seminars. Usually tertiary institutions of learning or professional organizations can provide the means of delivery of such programmes. Whenever possible, there should be annual events in which a broader range of views or expertise could be canvassed than is usually available within the framework of a small community or town. Regional or international conferences or seminars can provide extremely useful opportunities for participants, not only to take advantage of the formal programme but also to exchange information with other practitioners or researchers outside the formal sessions.
Nowadays, more and more OSH professional organizations require members to attend a minimum number of continuing education activities as a condition for extension of certification or membership. Usually only the fact of attendance at approved functions is required. Attendance by itself is, of course, no guarantee that the participant has benefited from being present. Alternatives such as subjecting OSH professionals to regular examinations are also fraught with problems. Within a single OSH discipline, there is such a wide diversity of practice even within the same country that it is extremely difficult to devise an examination equitable to all the OSH practitioners concerned.
Self-learning
In every OSH training course there should be emphasis on the need for self-learning and its continuing practice. To this end, training in information retrieval and critical analysis of published literature is imperative. Training on the use of computers to facilitate obtaining of information from the many excellent OSH resources around the world would be also beneficial. Several courses have been developed in recent years to promote self-learning and information management through microcomputers (Koh, Aw and Lun 1992).
Curriculum Development
There is an increasing demand on the part of trainees and the community to ensure that curricula are constantly evaluated and improved. Many modern curricula are competency-based. A series of professional competencies required is first compiled. Since competence may be defined by different groups in different ways, extensive consultations on this matter should be held with faculty members and OSH practitioners (Pochyly 1973). In addition, there is a need for consultations with “consumers” (e.g., students, workers and employers), an inbuilt evaluation programme and well-defined but flexible educational objectives (Phoon 1988). Sometimes the establishment of advisory committees on curriculum or teaching programmes, which normally include faculty and student representatives, but sometimes also involve members of the general community, can provide a useful forum for such consultations.
Infrastructure Development
Infrastructure is often ignored in discussions on OSH training and education. Yet supporting facilities and human resources such as computers, libraries, efficient administrative staff and procedures and safe and convenient access are among the host of infrastructure considerations which could be crucial to the success of training courses. Proper monitoring of students’ progress, counselling and assistance of students with problems, health care of students and their families (where indicated), minding of students’ children, canteen and recreational facilities and provision of lockers or cupboards for the storage of personal possessions of trainees are all important details which should receive careful attention.
Faculty Recruitment and Development
The quality and popularity of a training programme are often vital factors in determining the quality of staff applying for a vacant position. Obviously, other factors such as satisfactory service conditions and opportunities for career and intellectual development are also important.
Careful consideration should be given to job specifications and job requirements. Faculty should have the necessary OSH qualifications, though flexibility should be exercised to allow the recruitment of staff from non-OSH disciplines who may be able to make special contributions to teaching or especially promising applicants who may have the capability but not all the qualifications or experience normally required for the job. Whenever possible, faculty should have practical OSH experience.
After recruitment, it is the responsibility of the leadership and senior members of the school or department to make sure that new staff are given as much encouragement and opportunity to develop as possible. New staff should be inducted into the culture of the organization but also encouraged to express themselves and to participate in decision-making processes related to teaching and research programmes. Feedback should be given to them concerning their teaching performance in a sensitive and constructive manner. Whenever necessary, offers of help to remedy identified limitations should be given. Many departments have found the regular holding of teaching or evaluation workshops for staff to be extremely useful. Cross-postings to industries and sabbatical leave are other important measures for staff development. Some extent of consultancy work, which could be either clinical, worksite or laboratory (depending on the discipline and areas of activity of the faculty member) helps to make academic teaching more practical.
Teaching Venues
Classrooms should be designed and furnished according to appropriate ergonomic principles and equipped with audio-visual aid equipment and video projection facilities. The lighting and acoustics should be satisfactory. Access to an exit should be located in such a way as to minimize the disturbance of an ongoing class.
Proper principles of OSH should be applied to the design and construction of laboratories. Such safety equipment as showers, eye washing facilities, first aid supplies and resuscitation equipment and fume cupboards should be installed or made available where indicated, and laboratories should be bright, airy and odourless.
Venues for field visits should be chosen to provide a wide range of OSH experiences for the trainees. If possible, worksites with different levels of OSH standards should be chosen. However, on no account should the safety or health of trainees be compromised.
Locations for clinical work would very much depend on the nature and level of the training course. In some circumstances, bedside teaching may be indicated to demonstrate the appropriate clinical approach to skills in history taking. In some other circumstances, presentation of cases with or without patients could serve the same purpose.
Examinations and Assessment
The recent trend has been to seek alternatives to administering an all-important and single final examination at the end of a course. Some courses have abolished formal examinations altogether and replaced them with assignments or periodic assessments. Some other courses have a combination of such assignments and assessments, open book examinations and closed book examinations as well. It is nowadays increasingly understood that examinations or assessments are as much measures of the quality of courses and teachers as of the trainees.
A feedback of trainees’ opinions concerning the entire course or components thereof through questionnaires or discussions is invaluable in the evaluation or revision of a course. As far as possible, all courses should be constantly evaluated, at least on an annual basis, and revised if necessary.
Insofar as modes of examination are concerned, essay questions can test organization, integrating ability and writing skills. The precision and validity of essay examinations, however, have been found to be weak. Multiple-choice questions (MCQs) are less subjective, but good ones are difficult to formulate and do not allow a display of practical knowledge. Modified essay questions (MEQs) differ from essays or MCQs in that the candidate is presented with a progressive amount of information about a problem. It avoids cueing by requesting short-answer responses rather than presenting candidates with alternatives from which to choose the appropriate answer. Oral examinations can measure problem-solving skills, professional judgement, communication skills and ability to retain composure under stress. The main difficulty with the oral examination is the potential for so-called “lack of objectivity”. The oral examination can be made more reliable by imposing some structure on it (Verma, Sass-Kortsak and Gaylor 1991). Perhaps the best alternative is to use a battery of these different types of examination rather than to rely on one or two of them only.
Certification and Accreditation
The word certification usually refers to the conferment upon a professional of authorization to practise. Such certification could be conferred by a national board or a college or an institution of practitioners of an OSH discipline. Usually, the OSH professional is given certification only after fulfilling a stipulated period of training in connection with an approved course or positions and also upon passing an examination. In general, such “global certification” is valid for life, unless there is proven professional negligence or misconduct. However, there are other forms of accreditation which require periodic renewal. They include such accreditation as that required in some countries to either conduct special statutory medical examinations or to report on radiographs of asbestos-exposed persons.
Accreditation, on the other hand, refers to the recognition of OSH courses by a national board or professional organization or a scholarship-granting body. Such accreditation should be subject to periodic reappraisal to ensure that courses keep to an appropriate level of currency and effectiveness.
Safety and Health Training of Managers
Following a brief review of the development of educational contributions to worker health and safety and of the first attempts to establish the foundations of management education, this article will address curriculum development. The two career paths along which future senior managers develop will be considered as an issue relevant to the educational needs of managers. The curriculum content for managerial issues will be set forth first, to be followed by that pertinent to an understanding of injury causation.
Education for occupational safety and health has been directed, in the main, to people such as safety managers and occupational physicians, and more recently, to occupational health nurses, ergonomists and hygienists—people who have been appointed to specialist staff positions in organizations.
The advisory roles of these specialists have incorporated tasks such as the administration of pre-employment medical examinations, health surveillance, monitoring employee exposures to a range of hazards and environmental examination. Their activities moreover include contributing to job and task design in order to adjust engineering or administrative controls by way of minimizing if not eliminating (for example) the harmful effects of postural demands or of exposure to toxic hazards.
This specialist-oriented educational approach has tended to ignore the central fact that the provision of safe and healthy workplaces requires an extraordinarily broad scope of operational knowledge necessary to make them a reality. It must be borne in mind that managers carry the responsibility for planning, organizing and controlling work activities in public and private enterprises across all industry sectors.
Background
During the decade of the 1970s many initiatives were taken to offer study programmes at the tertiary level to provide a professional education with practical training for the range of specialist engineers, scientists and health care workers entering the field of occupational safety and health.
In the 1980s it was recognized that the people most directly concerned with occupational safety and health, the managers, the workers themselves and their associations, were the most significant entities in the move to reduce workplace injury and ill health. Legislation in many jurisdictions was introduced to provide education for workers serving on safety committees or as elected safety and health representatives. These changes highlighted for the first time the very limited education and training facilities then available to managers.
An early initiative to address management education
Several steps were taken to overcome this problem. The most widely known is Project Minerva, an initiative of the US National Institute for Occupational Safety and Health (NIOSH), which represented an early effort to inculcate that body of specific managerial skills which is necessary to ensure workplace safety and which “generally exceeds that which is offered through courses in the traditional business curriculum” (NIOSH 1985). Teaching materials intended to address the more urgent safety and health concerns were provided for business schools. The resource guide comprised instructional modules, case studies and a book of readings. Module topics are listed in figure 1.
Figure 1. Modular curriculum content, Project Minerva resource guide.
The Canadian Society of Safety Engineers has recommended this structure to business schools seeking to incorporate occupational safety and health materials into their curricula.
Fundamentals of Managing: General Rather Than Specific Needs
Any job responsibility entails the acquisition of relevant knowledge and appropriate skills in order to discharge it. Responsibility for managing occupational safety and health within any organization will be placed increasingly upon line managers at each level in the job hierarchy. Associated with that responsibility ought to be commensurate accountability and the authority to command the necessary resources. The knowledge and skills needed to discharge this responsibility form the curriculum for occupational safety and health management education.
At first sight, it would seem necessary that a curriculum of this sort be developed with the aim of meeting all the special demands of the whole range of management functions as they relate to such a diversity of positions as office administrator, nurse manager, operations director, supplies and purchasing superintendent, fleet coordinator and even ship’s captain. The curricula need also, perhaps, address the whole range of industries and the occupations found within them. However, experience strongly suggests that this is not so. The necessary skills and knowledge are, in fact, common to all management functions and are more fundamental than those of the specialists. They are operative at the level of basic management expertise. However, not all managers arrive at their position of responsibility by taking similar paths.
Managerial Career Paths
The usual path to a managerial career is through either supervisory or specialist functions. In the former case, career development is dependent on work experience and job knowledge and in the latter it ordinarily presupposes off-the-job college education and postgraduate study, for example as an engineer or nurse manager. Both streams need to develop occupational safety and health (OSH) skills. For the latter this may be done in graduate school.
It is usual today for successful managers to acquire the degree of Master of Business Administration (MBA). For this reason the Minerva Project directed its attention to the 600 or more graduate management schools in the United States. By incorporating into MBA curricula such aspects of occupational safety and health as were determined to be critical for successful management of the field, it was believed that this material would be integrated into the formal studies of middle management.
Given the extremely high rate of technological invention and scientific discovery, undergraduate courses, particularly in engineering and scientific disciplines, have only limited opportunities to integrate broadly-based safety theory and practice into design, process and operation studies.
Since managerial roles begin fairly soon after graduation for those with specialist education, there is a need to provide the knowledge and skills that will support the safety and health responsibility of both specialist and generalist managers.
It is important that an awareness of the content of any curriculum devoted to occupational safety and health objectives among management be promoted among other personnel having related responsibilities. Thus, the training of such key employees as safety and health representatives should be designed to keep them current with such curricular developments.
Curriculum for Managing Occupational Safety and Health
There are two broad classes of knowledge into which the discipline of occupational safety and health falls. One is that relating to the functions and principles of management and the other deals with the nature and proactive control of hazards. The model of curriculum development set forth below will follow this division. Both the supervisory path to management and the specialist path will require their own particular coverage of each of these classes.
The question of what level of complexity and technological detail needs to be provided to students may be determined by the purpose of the course, its length and the intention of the providers regarding subsequent education and skills development. These issues will be addressed in a later section.
Specifically, curricula should address machinery and plant safety, noise, radiation, dust, toxic materials, fire, emergency procedures, medical and first aid arrangements, workplace and employee monitoring, ergonomics, environmental hygiene, workplace design and maintenance and, most importantly, the development of standard operating procedures and training. This last is an essential component of managerial understanding. Not only must tasks and processes be the subject of operator training but the requirement for continuous improvement of people and processes makes training and retraining the most critical step in improving the quality of both. Adult learning theory and practice needs to be applied in the development of the curricular materials that guide this continuing training process.
The functions and principles of management
The fundamental purposes of management embrace the planning, organizing and control of workplace activities. They also embrace the incorporation of practices which maximize opportunities for workforce participation in goal setting, team operation and quality improvement. Furthermore, successful management requires the integration of occupational safety and health into all the organization’s activities.
It is rare for undergraduate programmes, outside those of colleges of business, to cover any of this knowledge. However, it is a most essential component for the specialist practitioners to have incorporated into their undergraduate study.
Organizational framework
The mission statement, strategic plan and structure set up to guide and facilitate the attainment of the organization’s objectives must be understood by the managers to be the basis for their individual activities. Each division of the organization whether it is a hospital, trucking business or coal mine, will in turn have its own goals and structure. Each will reflect the need to achieve organizational goals, and, taken together, will drive the organization towards them.
Policies and procedures
The primary embodiment of an organization’s goals are comprised by policy documents, the guides for individual employees on specific topics. (In some jurisdictions, the publication of an organization’s overall policy is required by law.) These documents ought to include reference to the range of occupational safety and health programmes designed with regard to the activities and processes which occupy the working time of employees. A sample of some general policy statements might include documents on emergency evacuation, fire fighting, purchasing procedures, injury reporting and accident and incident investigation. On the other hand, specific hazards will require their own process-specific policy materials concerning, for example, hazardous substances management, ergonomic interventions or entry into confined spaces.
After establishing policy, an activity preferably carried out with worker representative participation and union involvement, detailed procedures would then be put in place to give effect to them. Again, participative practices will contribute to the wholehearted acceptance of them by the workforce as a valuable contribution to their safety and health.
A safety and health management system is schematically illustrated in figure 2.
Figure 2. A health and safety management system.
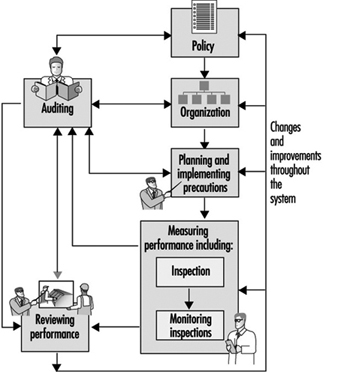
Organizational structures defining key roles
The next stage in the management process is to define an organizational structure which characterizes the roles of key people—for example, the chief executive—and professional advisors such as safety advisors, occupational hygienists, the occupational health nurse, the physician and the ergonomist. In order to facilitate their roles, the relationships of these people and elected safety and health representatives (required in some jurisdictions) and worker members of safety committees to the organizational structure need to be explicit.
The planning and organizing functions of management will integrate structures, policies and procedures into the operational activities of the enterprise.
Control
Control activities—establishing processes and goals, determining standards of acceptable achievement and measuring performance against those standards—are the operational steps which bring to realization the intentions of the strategic plan. They also need to be established through co-determination. The tools for control are workplace audits, which may be continuous, frequent, random or formal.
An understanding of these activities is an important component of a management education syllabus, and skills should be developed in carrying them out. Such skills are as essential to the success of an integrated safety and health plan as they are to the discharge of any other management function, whether purchasing or fleet operation.
Organizational development and curriculum
Since the introduction of new organizational structures, new equipment and new materials is occurring at a rapid pace, special attention must be given to the processes of change. The employees who will be affected by these changes can have a deciding influence on their effectiveness and on the efficiency of the work group. An understanding of the psychosocial factors influencing the activities of the organization must be acquired and skills must be developed in using this knowledge to reach organizational objectives. Of particular importance is the delegation of the authority and the accountability of the manager to work groups formed into autonomous or semi-autonomous work teams. The management education curriculum must place at the disposal of its students the tools necessary to carry out their obligation to ensure not only process improvement and quality but the development of the multiple skills and quality awareness of personnel with which the issue of safety is so closely involved.
There are two further components of the management curriculum requiring examination. One of these is the activity of incident investigation and the other, on which the whole of this activity rests, is an understanding of the accident phenomenon.
The accident phenomenon
The work of Derek Viner (1991) in clearly expounding the significance of energy sources as the potential hazards in all workplaces has defined half of the accident equation. In conjunction with Viner’s work, the contribution of Dr. Eric Wigglesworth (1972) in identifying human error, the crucial element in managing workplace safety activities, completes its definition. An emphasis on the process of each damaging occurrence has been shown by Benner (1985) when considering accident investigation methods to be the most productive approach to managing worker safety and health.
Wigglesworth’s visualization of the sequence of events which results in injury, damage and loss appears in figure 3. It highlights the role of nonculpable human error, as well as the essential element of loss of energy containment and the potential for the injury outcome where this occurs.
Figure 3. The error/injury process.
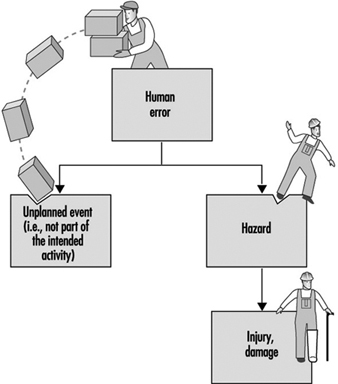
The implications of the model for management become clear when planning for work processes takes account of the behavioural inputs which affect those processes. This is so in particular when the role of design is given its rightful place as the initiating mechanism for both equipment and process development. When planning takes account both of the design of plant and equipment and of the human factors influencing work activity, coordination and control mechanisms can then be implemented to assure containment of the identified hazards.
A model may be used to illustrate the significance of the interaction between the worker, the equipment, tools and machines employed to further the task objectives and the environment within which the activity takes place. The model highlights the need to address factors within all three elements which may contribute to damaging events. Within the workstation environment, which encompasses the thermal, aural and lighting components, among others, the worker interacts with the tools and equipment necessary to get the work done (see figure 4).
Figure 4. Representation of workstation elements relevant to injury causation and control.

Accident investigation and analysis
Accident investigation serves a number of important functions. First, it can be a proactive process, being used in situations where an incident occurs which results in no damage or injury but where there is a potential for harm. Studying the sequence of events can uncover features of the work process which could lead to more serious consequences. Second, one may gain an understanding of the process by which the events unfolded and thus can identify the absence of, or weakness in, process or task design, training, supervision or controls over energy sources. Third, many jurisdictions legally require investigations of certain types of incidents, for example, scaffolding and trench collapses, electrocutions and failures of hoisting equipment. The work of Benner (1985) illustrates well the importance of having a clear understanding of the accident phenomenon and an effective protocol for investigating injury and damage events.
The nature and control of hazards
All injury results from some form of energy exchange. The uncontrolled release of physical, chemical, biological, thermal, or other forms of energy is a source of potential harm to a variety of workers. Containment by suitable engineering and administrative mechanisms is one essential aspect of suitable control. Identifying and evaluating these energy sources is a prerequisite for control.
A management education curriculum would thus contain topics covering a range of activities which includes establishing objectives, planning the work, developing policy and procedures, undertaking organizational change and installing controls over work processes (and specifically the energy sources utilized in carrying out that work), all aimed at injury prevention. While curricula designed for the technical areas of operations need address only fundamental principles, organizations that make use of very hazardous materials or processes must have in their employ a senior member of management with sufficient training in the specific modes of handling, storage and transport of such technology to ensure the safety and health of workers and members of the community.
Larger enterprises and small business
Managers who work in larger organizations employing, say, a hundred or more people usually have one or only a few functional responsibilities and report to a senior manager or a board of directors. They have occupational safety and health responsibility for their own subordinates and act within established policy guidelines. Their educational needs may be addressed by the formal programmes offered in business schools at the undergraduate or graduate level.
On the other hand, the sole managers or partners in small enterprises are less likely to have had graduate education, and, if they have, it is more likely to be of a technological than managerial sort, and it is more difficult to address their needs for the management of occupational health and safety.
Small business needs
Providing training programmes for these managers, who often work very long hours, has represented a difficulty of long standing. Although a number of large legislative jurisdictions have produced guidance booklets setting out minimum performance stands, the more promising approaches are being made available through industry associations, such as the Ontario Industrial Accident Prevention Associations funded by levies placed by the Workers’ Compensation Board upon all businesses in the given industrial sector.
Syllabus Content
A body of knowledge and skills which addresses the needs of managers at the first-line supervisory level, middle management and senior executives is outlined in figure 5 by topic. Individual short-form syllabuses follow in figure 6. These have been collated from the syllabuses of a number of university graduate study programmes.
Figure 5. Syllabus for an OSH study programme.
Figure 6. Short form syllabuses for an OSH study programme.

The needs of first-line supervisors will be met through the acquisition of knowledge and skills covered by those topics that relate to operational demands. The training of senior executives will concentrate on such topics as strategic planning, risk management and compliance matters as well as initiating policy proposals. The allocation of hours for each course of study should reflect student needs.
Summary
Management education for occupational safety and health demands an eclectic approach to the broadest range of issues. It shares with quality the imperative of being integrated into every management and worker activity, into every employee’s job description and should be a part of the performance appraisal of all.
Worker Education and Environmental Improvement
The articles in this chapter have thus far concentrated on training and education regarding workplace hazards. Environmental education serves multiple purposes and is a useful complement to occupational safety and health training. Worker education is a critical and often overlooked aspect of a broad and effective environmental protection strategy. Environmental issues are frequently viewed as purely technological or scientific matters that stand outside the purview of workers. Yet worker knowledge is critical to any effective environmental solutions. Workers are concerned as citizens and as employees about environmental matters because the environment shapes their lives and affects their communities and families. Even when technological solutions are required that use new hardware, software or process approaches, worker commitment and competence are necessary for their effective implementation. This is true for workers whether involved directly in environmental industries and occupations or in other kinds of jobs and industrial sectors.
Worker education can also provide a conceptual foundation to enhance workers’ participation in environmental improvement, health and safety protection, and organizational improvement. The UNEP Industry and Environment Programme notes that “many companies have found that worker involvement in environmental improvement can yield important benefits” (UNEP 1993). The Cornell Work and Environment Initiative (WEI) in a study of US enterprises found that intense worker participation yielded triple the source reduction of technical or external solutions alone and boosted yields of some technological approaches even higher (Bunge et al. 1995).
Worker environmental education comes in a variety of forms. These include trade union awareness and education, occupational training and orientation, connecting environment to workplace health and safety concerns and broad awareness as citizens. Such education occurs in a range of venues including worksites, trade union halls, classrooms and study circles, using both traditional and newer computer-based delivery systems. It is fair to say that workers’ environmental education is an underdeveloped field, especially in comparison with managerial and technical training and school-based environmental education. At the international level, education of front-line workers is often mentioned in passing and is overlooked when it comes to implementation. The European Foundation for the Improvement of Living and Working Conditions has commissioned a series of studies on the educational dimension of environmental protection, and in its next programme of work will directly look at the shop-floor workers and their environmental educational needs.
What follows are several examples gathered through the WEI at Cornell University that illustrate both practice and possibility in worker environmental education.The WEI is a network of managers, trade unionists, environmentalists and government policy officials from 48 countries in all parts of the world, committed to finding ways that workers and the workplace can contribute to environmental solutions. It addresses a wide range of industries from primary extraction to production, service and public-sector enterprises. It provides a means for education and action on environmental matters that seeks to build knowledge at the workplace and in academic institutions that can lead to cleaner and more productive workplaces and better connection between internal and external environments.
Australia: Eco-Skills Modules
The Australian Council of Trade Unions (ACTU) has developed new approaches to workers’ education for the environment that provides both broad social awareness and specific competencies for employment, especially among young workers.
The ACTU has organized an Environment Training Company with a broad mandate to address a variety of sectors but with an initial focus on land management issues. This focus includes teaching ways to handle reclamation work safely and effectively but also ways to assure compatibility with indigenous peoples and natural environments. With input from trade unionists, environmentalists and employers, the training company developed a set of “Eco-Skills” modules to establish basic environmental literacy among workers from an array of industries. These are integrated with a set of skill competencies that are technical, social and safety oriented.
Eco-Skills modules 1 and 2 contain a broad base of environmental information. They are taught alongside other entry-level training programmes. Levels 3 and higher are taught to people who specialize in work focused on reduction of environmental impacts. The first two Eco-Skills modules are composed of two forty-hour sessions. Trainees attain skills through lectures, group problem-solving sessions and practical hands-on techniques. Workers are assessed through written and oral presentations, group work and role plays.
Concepts covered in the sessions include an introduction to the principles of ecologically sustainable development, efficient resource use and cleaner production and environmental management systems. Once Module 1 is completed workers should be able to:
- identify the implications of a given lifestyle for long-term sustainability with specific emphasis placed on the learner’s present and future lifestyle
- identify ways to reduce the environmental impact of human activities
- describe strategies to reduce environmental impacts in a given industry (agriculture, forestry, manufacturing, tourism, leisure, mining)
- describe the main features of an Environmental Management System
- identify the role of stakeholders in reducing environmental pollution and resource depletion.
Module 2 expands upon these initial objectives and prepares workers to begin applying pollution prevention and resource conservation methods.
Some industries are interested in connecting environmental impact skills and knowledge to their industry standards at every level. Awareness of environmental issues would be reflected in the day-to-day work of all industry workers at all skill levels. An incentive for workers lies in the fact that pay rates are linked to industry standards. The Australian experiment is in its infancy, but it is a clear attempt to work with all parties to develop competency-based activities that lead to increased and safer employment while enhancing environmental performance and awareness.
Linking Occupational Health and Safety and Environmental Training
One of the most active unions in the United States in environmental training is the Laborers International Union of North American (LIUNA). US government regulations require that hazardous-waste abatement workers receive 40 hours of training. The union along with participating contractors have developed an intensive 80-hour course designed to provide potential hazardous-waste workers with greater awareness of safety and the industry. In 1995, over 15,000 workers were trained in lead, asbestos and other hazardous-waste abatement and other environmental remediation work. The Laborers–Associated General Contractors programme has developed 14 environmental remediation courses and associated train-the-trainer programmes to assist nationwide efforts at safe and quality remediation. These are conducted at 32 training sites and four mobile units.
In addition to providing safety and technical training, the programme encourages participants to think about larger environmental issues. As part of their classwork, trainees gather materials from local papers on environmental issues and use this local connection as an opening to discuss broader environmental challenges. This joint environmental training fund employs a full-time equivalent staff of 19 at its central office and spends over US$10 million. The materials and training methods meet high quality standards with extensive use of audio-visual and other training aids, specific competency focus, and quality commitment and assessment built in throughout the curricula. A “learn-at-home” video is used to help meet literacy concerns and environmental and basic literacy training are connected. For those who desire it, six of the courses are transferable into college credit. The programme is active in serving minority communities, and over half of the participants come from minority population groups. Additional programmes are developed in partnership with minority consortiums, public housing projects and other training providers.
The union understands that a great deal of its future membership will come in environmentally related businesses and sees the development of worker education programmes as building the foundation for that growth. While both safety and productivity are better on jobs using trained workers, the union also sees the broader impact:
The most interesting impact environmental training has had on members is their increased respect for chemicals and harmful substances in the workplace and at home. … Awareness is also increasing with respect to the consequences of continued pollution and the cost involved with cleaning up the environment. … The true impact is much greater than just preparing people for work (LIUNA 1995).
In the United States, such hazardous-materials training is also conducted by the Operating Engineers; Painters; Carpenters; Oil, Chemical and Atomic Workers; Chemical Workers Union; Machinists; Teamsters; Ironworkers and Steelworkers.
LIUNA is also working internationally with the Mexican Confederation of Workers (CTM), federal and private training groups and employers to develop training methodologies. The focus is on training Mexican workers in environmental remediation work and construction skills. The Inter-American Partnership for Environmental Education and Training (IPEET) held its first training course for Mexican workers during the summer of 1994 in Mexico City. A number of labour leaders and workers from local industries, including paint manufacturing and metal plating, attended the one-week course on environmental safety and health. Other LIUNA partnerships are being developed in Canada with French editions of the materials and “Canadianization” of the content. The European Institute for Environmental Education and Training is also a partner for similar training in Eastern European and CIS countries.
Zambia: Educational Manual on Occupational Health and Safety
In Zambia, too often occupational health and safety is taken seriously only when there is an incident involving injury or damage to company property. Environmental issues are also ignored by industry. The Manual on Occupational Health and Safety was written in an effort to educate employees and employers on the importance of occupational health and safety issues.
The first chapter of this manual outlines the importance of education at all levels in a company. Supervisors are expected to understand their role in creating safe, healthy working conditions. Workers are taught how maintaining a positive, cooperative attitude relates to their own safety and work environment.
The manual specifically addresses environmental issues, noting that all major towns in Zambia face
threats of increasing environmental damage. In specific, the Zambia Congress of Trade Unions (ZCTU) identified environmental hazards in the mining industry through strip mining and air and water pollution that results from poor practices. Many factories are responsible for air and water pollution because they discharge their waste directly into nearby streams and rivers and allow smoke and fumes to escape unchecked into the atmosphere (ZCTU 1994).
Though many African trade unions are interested in further education on the environment, lack of adequate funding for worker education and the need for materials that link environmental, community and workplace hazards are major barriers.
Employer-Based Worker Environmental Education and Training
Employers, especially larger ones, have extensive environmental education activities. In many cases, these are mandated training linked to occupational or environmental safety requirements. However, an increasing number of companies recognize the power of broad worker education that goes well beyond compliance training. The Royal Dutch/Shell Group of companies have made health, safety and environment (HSE) part of their overall approach to training, and environment is an integral part of all management decisions (Bright and van Lamsweerde 1995). This is a global practice and mandate. One of the company’s goals is to define HSE competencies for appropriate jobs. Worker competence is developed through improved awareness, knowledge and skill. Appropriate training will increase worker awareness and knowledge, and skills will develop as new knowledge is applied. A wide range of delivery techniques helps share and reinforce the environmental message and learning.
At Duquesne Light in the United States, all 3,900 employees were successfully trained “on how the company and its employees actually affect the environment.” William DeLeo, Vice-President of Environmental Affairs said:
To develop a training programme that enabled us to meet out strategic objectives we determined that our employees needed a general awareness of the importance of environmental protection as well as specific technical training relative to their job responsibilities. These two points became the guiding strategy for our environmental education program (Cavanaugh 1994).
Worker and Union-Based Environmental Education Programmes
The Workers’ Education Branch of the ILO has developed a six-booklet set of background materials to spark discussion among trade unionists and others. The booklets address workers and the environment, the workplace and the environment, the community and the environment, world environmental issues, the new bargaining agenda, and provide a guide to resources and a glossary of terms. They provide a broad, insightful and easy-to-read approach that can be used in both developing and industrial countries to discuss topics relevant to workers. The materials are based on specific projects in Asia, the Caribbean and Southern Africa, and can be used as a whole text or can be separated in a study circle format to promote general dialogue.
The ILO in a review of training needs pointed out:
Trade unionists must increase their awareness about environmental concerns in general and the impact their employing firms are having on the environment, including the safety and health of their workers, in particular. Trade unions and their members need to understand environmental issues, the consequences that environmental hazards have on their members and the community at large, and be able to develop sustainable solutions in their negotiations with company management and employers’ organizations. (ILO 1991.)
The European Foundation for the Improvement of Living and Working Conditions has observed:
Local trade unions and other employee representatives are in a particularly difficult situation. They will have the relevant knowledge of the local situation and the workplace but will, in most cases, not be sufficiently specialised in complex environmental and strategic issues.
They will, therefore, be unable to exercise their functions unless they received additional and specialised training. (European Foundation for the Improvement of Living and Working Conditions 1993.)
A number of national unions have urged increased workers’ education on the environment. Included among them is the LO in Sweden, whose 1991 Environmental Programme called both for more education and action at the workplace and for additional study circle material on the environment to promote awareness and learning. The Manufacturing Workers Union in Australia has developed a training course and set of materials to assist the union in providing environmental leadership, including how to address environmental issues through collective bargaining.
Summary
Good worker-based environmental education provides both conceptual and technical information to workers that assists them in increasing environmental awareness and in learning concrete ways to change work practices that are damaging to the environment. These programmes also learn from workers at the same time to build on their awareness, reflection and insight about workplace environmental practice.
Workplace environmental education is best done when it is connected to community and global environmental challenges so that workers have a clear idea of how the ways they work are connected to the overall environment and how they can contribute to a cleaner workplace and global ecosystem.
Environmental Education and Training: The State of Hazardous Materials Worker Education in the United States
The term environmental education covers a potentially wide range of issues and activities when applied to employees, managers and workplaces. These encompass:
- education for general awareness of environmental concerns
- education and training toward modifying work practices, processes and materials to reduce the environmental impact of industrial processes on local communities
- professional education for engineers and others seeking expertise and careers in environmental fields
- education and training of workers in the growing field of environmental abatement, including hazardous waste cleanup, emergency response to spills, releases and other accidents, and asbestos and lead paint remediation.
This article focuses on the state of worker training and education in the United States in the growing environmental remediation field. It is not an exhaustive treatment of environmental education, but rather an illustration of the link between occupational safety and health and the environment and of the changing nature of work in which technical and scientific knowledge has become increasingly important in such traditional “manual” trades as construction. “Training” refers in this context to shorter-term programmes organized and taught by both academic and non-academic institutions. “Education” refers to programmes of formal study at accredited two-year and four-year institutions. Currently a clear career path does not exist for individuals with interest in this field. The development of more defined career paths is one goal of the National Environmental Education and Training Center, Inc. (NEETC) at Indiana University of Pennsylvania. Meanwhile, a wide range of education and training programmes exist at different levels, offered by a variety of academic and non-academic institutions. A survey of the institutions involved in this type of training and education formed the source material for the original report from which this article was adapted (Madelien and Paulson 1995).
Training Programmes
A 1990 study conducted by Wayne State University (Powitz et al. 1990) identified 675 separate and distinct noncredit short courses for hazardous waste worker training at colleges and universities, offering over 2,000 courses nationwide each year. However, this study did not cover some of the primary providers of training, namely community college programmes, US Occupational Safety and Health Administration training programmes and independent firms or contractors. Thus, the Wayne State number could probably be doubled or tripled to estimate the number of noncredit, noncertification course offerings available in the United States today.
The major government-funded training programme in environmental remediation is that of the National Institute for Environmental Health Sciences (NIEHS). This program, established under the Superfund legislation in 1987, provides grants to non-profit organizations with access to appropriate worker populations. Recipients include labour unions; university programmes in labour education/labour studies and public health, health sciences and engineering; community colleges; and non-profit-making safety and health coalitions, known as COSH groups (Committees on Occupational Safety and Health). Many of these organizations operate in regional consortia. The target audiences include:
- construction trades workers involved in cleanup of hazardous waste sites
- emergency response personnel working for fire and emergency services agencies and industrial plants
- transportation workers involved in transporting hazardous materials
- hazardous waste treatment, storage and disposal facility workers
- wastewater treatment workers.
The NIEHS program has resulted in extensive curriculum and materials development and innovation, which has been characterized by considerable sharing and synergy among grantees. The programme funds a national clearinghouse which maintains a library and curriculum centre and publishes a monthly newsletter.
Other government funded programmes offer short courses targeting hazardous waste industry professionals as opposed to front-line remedial workers. Many of these programmes are housed in university Educational Resource Centers funded by the National Institute for Occupational Safety and Health (NIOSH).
Education Programmes
Community colleges
The broadest change on the hazardous waste education and training landscape in the past few years is the dramatic development of community college programmes and consortia to improve vocational education at the associate’s degree level. Since the 1980s, community colleges have been doing the most organized and extensive curriculum development work in secondary education.
The Department of Energy (DOE) has funded programmes nationwide to provide for a trained workforce at sites where the need has changed from nuclear technicians to hazardous waste clean-up workers. This training is taking place most rigorously at community colleges, many of which have historically provided for personnel needs at specific DOE sites. DOE-funded programmes at community colleges have also given rise to major efforts in curriculum development and consortia for sharing information. Their goals are to establish more consistent and higher standards of training and to provide mobility for the workforce, enabling an individual trained to work at a site in one part of the country to move to another site with minimal retraining requirements.
Several consortia of community colleges are advancing curricula in this area. The Partnership for Environmental Technology Education (PETE) operates in six regions. PETE is working with the University of Northern Iowa to create a world-class network of community college environmental programmes, linked with high schools, that inform and prepare students for entry into these two-year degree programmes. The goals include the development of (1) nationally validated curriculum models, (2) comprehensive professional development programmes and (3) a national clearinghouse for environmental education.
The Hazardous Materials Training and Research Institute (HMTRI) serves the curriculum development, professional development, print and electronic communications needs of 350 colleges with two-year environmental technologies credit programmes. The Institute develops and distributes curricula and materials and implements educational programmes at its own Environmental Training Center at Kirkwood Community College in Iowa, which has extensive classroom, laboratory and simulated field site facilities.
The Center for Occupational Research and Development (CORD) provides national leadership in the US Department of Education’s Tech Prep/Associate Degree initiative. The Tech Prep program requires coordination between secondary and post-secondary institutions to give students a solid foundation for a career pathway and the world of work. This activity has led to the development of several contextual, experiential student texts in basic science and mathematics, which are designed for students to learn new concepts in relationship to existing knowledge and experience.
CORD has also played a significant role in the Clinton administration’s national educational initiative, “Goals 2000: Educate America”. In recognition of the need for qualified entry-level personnel, the initiative provides for the development of occupational skills standards. (“Skills standards” define the knowledge, skills, attitudes and level of ability necessary to successfully function in specific occupations.) Among the 22 skills standards development projects funded under the programme is one for hazardous materials management technology technicians.
Articulation between vocational and baccalaureate programmes
A continuing problem has been the poor linkage between two-year and four-year institutions, which hampers students who wish to enter engineering programmes after completing associate’s (two-year) degrees in hazardous/radioactive waste management. However, a number of community college consortia have begun to address this problem.
The Environmental Technology (ET) consortium is a California community college network that has completed articulation agreements with four four-year colleges. The establishment of a new job classification, “environmental technician”, by the California Environmental Protection Agency provides added incentive for graduates of the ET program to continue their education. An ET certificate represents the entry level requirement for the environmental technician position. Completion of an associate’s degree makes the employee eligible for promotion to the next job level. Further education and work experience allows the worker to progress up the career ladder.
The Waste-management Education and Research Consortium (WERC), a consortium of New Mexico schools, is perhaps the most advanced model which attempts to bridge gaps between vocational and traditional four-year education. Consortium members are the University of New Mexico, the New Mexico Institute of Mining and Technology, New Mexico State University, Navajo Community College, Sandia Laboratory and Los Alamos Laboratories. The approach to curriculum transfer has been an interactive television (ITV) program in distance learning, which takes advantage of the varied strengths of the institutions.
Students enrolled in the environmental programme are required to take 6 hours of courses from the other institutions through distance learning or an offsite semester of coursework. The programme is decidedly inter-disciplinary, combining a minor in hazardous materials/waste management with a major from another department (political science, economics, pre-law, engineering or any of the sciences). The programme is “both broad and narrow” in focus, in that it recognizes a need to develop students with both a broad knowledge base in their field and some specific training in hazardous materials and hazardous waste management. This unique programme couples student participation in realistic applied research and industry-led curriculum development. The courses for the minor are very specific and take advantage of the particularized specialties at each school, but each program, including the associate degree, has a large core requirement in humanities and social sciences.
Another unique feature is the fact that the four-year schools offer two-year associate’s degrees in radioactive and hazardous materials technology. The two-year associate’s degree in environmental science offered at the Navajo Community College includes courses in Navajo history and substantial courses in communications and business, as well as technical courses. A hands-on laboratory has also been developed on the Navajo Community College campus, an unusual feature for a community college and part of the consortium’s commitment to hands-on laboratory learning and technology development/applied research. The WERC member institutions also offer a “non-degree” certificate programme in waste management studies, which seems to be above and beyond the 24-hour and 40-hour courses offered at other colleges. It is for individuals who already have a bachelor’s or graduate degree and who further wish to take advantage of seminars and specialty courses at the universities.
Conclusions
Several significant changes have taken place in the focus of education and training related to the hazardous waste industry in the past few years, in addition to the proliferation of short-course training programmes and traditional engineering programmes. Overall, the Department of Energy seems to have focused education at the community college level on workforce retraining, primarily through the Partnership for Environmental Technology Education (PETE), the Waste-management Education and Research Consortium (WERC) and other consortia like them.
There is a major gap between vocational training and traditional education in the environmental field. Because of this gap, there is not a clear, routine career path for hazardous waste workers, and it is difficult for these workers to advance in industry or government without classic technical degrees. Although inter-departmental options for education at a management level are being established within economics, law and medicine departments which recognize the breadth of the environmental industry, these are still academic-based professional degrees which miss a large part of the available and experienced workforce.
As the environmental clean-up industry matures, the long-term needs of the workforce for more balanced training and education and a well-developed career path become more clear. The large numbers of displaced workers from closed military sites means more people are entering the environmental workforce from other fields, making the demand on union training and placement of displaced workers (both discharged military personnel and displaced civilian personnel) even greater than before. Educational programmes are needed which meet both the needs of personnel entering the industry and of industry itself for a more balanced and better-educated workforce.
Since labour union members are one of the main groups poised to enter the hazardous waste clean-up and environmental remediation field, it would seem that labour studies and industrial relations departments might be logical entities to develop degree programmes that incorporate a hazardous waste/environmental curriculum with development of labour/management skills.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."