- You are here:
-
Home

-
Part XVI. Construction
-
Construction
- Major Sectors and Their Hazards
Shifting Paradigms and Policies
Although this article focuses to a large extent on women, it is actually about humans, and humans as workers. All humans need challenge and security; healthy workplaces provide both. When we cannot succeed despite best efforts (impossible goals without adequate means) or when there are no challenges (routine, monotonous work), the conditions are met for “learned helplessness”. While exceptional persons may triumph over adversity and hostile environments, most humans need nurturant, enabling and empowering environments in order to develop and exercise their capabilities. The case for stimulation, not only in childhood, but lifelong, is supported by neuroscience research, which suggests that increasing stimulation and input can promote brain growth and increase brain power. These suggestive findings have implications for an enriched psychosocial environment at work, for the prevention of certain brain disorders and for the restorative benefits of rehabilitation after trauma or disease.
The dazzling intellectual feats of Stephen Hawking, or the equally dazzling performance of paralympic athletes with severe physical or mental disabilities, bear witness to the importance of personal drive, buttressed by supportive environments with favourable opportunity structures, aided by the application of appropriate modern technologies.
The workplace is made up of workers with diverse characteristics. ILO Convention No. 111 (1958) which deals with discrimination, employment and occupation states in Article 5 (2):
Any member may ... determine that other special measures ... to meet the particular requirement of persons who, for such reasons as sex, age, disablement, family responsibilities or social or cultural status, are generally recognized to require special protection or assistance shall not be deemed to be discrimination.
The Organization for Economic Cooperation and Development has stated that European legislative instruments pertaining to safety and health in the work environment require adaptations of workplace design, choice of equipment, and production methods (e.g., eliminating monotonous work and machine pacing) to meet the individual needs of workers and that reduce adverse health effects (OECD 1993). Some statutes call for prevention of policies addressing technology, the introduction of work organization and conditions, social relations and other aspects of the working environment. The reduction of absences, of turnover and of costs for treatment, rehabilitation, re-education and training are viewed as benefits to employers accruing from the introduction and maintenance of healthy work environments and conditions.
North American employers, generally in response to advancing legal requirements for workplace human rights, are developing positive policies and strategies for management of a diverse workforce. The United States has developed probably the most comprehensive legislation for disabled Americans, including legislation regarding their entitlements in education, employment and all other spheres of living. Reasonable accommodations are changes made to the work environment, job responsibilities or conditions of work that provide opportunities for workers with special needs to perform essential job functions. Reasonable accommodation can cover the special needs of, for example: persons with disabilities; women; workers with chronic or recurrent disease, including persons with AIDS; persons with language training needs; those who need to harmonize work and family responsibilities; pregnant or breast-feeding mothers; or religious or ethnic minorities. Accommodation may include technical assistance devices; customization, including personal protective equipment and clothing; and changes to processes, location or timing for essential job functions. For equity and justice to all workers, these accommodations are best developed through joint management and worker committees and through collective agreements.
Cost-effective appropriate technologies and policies need to be developed for the benefits of reasonable accommodation to be enjoyed by workers throughout the world, not only by some in economically advanced societies. Globalization could achieve this, through existing multilateral agencies and the World Trade Organization.
Women Workers
Why are women included among the workers with special needs? When we look at the needs, risks and tasks of women we must consider the following factors:
- gender discrimination
- poverty or the threat thereof. (Most of the world’s poor are women and their children, especially sole-support mothers, who comprise 20 to 30% of households worldwide; and 75% of the world’s 18 million refugees are women and children.)
- reproductive functions of pregnancy, childbirth and breast-feeding
- gender-based violence, now internationally accepted as a human rights violation
- sexual harassment
- gender-support gap, with women providing most of the caring functions. (A Canadian social survey showed that 10% of men in dual-earner families share equally in household tasks.)
- longevity, a factor affecting their long-term social security and health needs.
All of these risks and needs can be addressed to some extent or taken into consideration at the workplace. Additionally, we must bear in mind that women constitute half of other categories of workers with special needs, a fact that places them in potential double jeopardy and makes gender a central factor in assessing their capabilities and entitlements.
Sexism is the belief that women need less, deserve less and are worth less than men. The UN International Woman’s Decade, 1975–1985, with its themes of equality, development and peace, revealed that throughout the world women are overworked and undervalued. From a reanalysis of past studies and new research the realization slowly emerged that women’s work was undervalued because women themselves were devalued, not because of inherent deficiencies.
During the 1960s there were many studies of why women worked and which women worked, as though work was an aberration for women. Indeed, women were routinely fired when they married or when they became pregnant. In the late 1960s European countries with strong labour demands preferred the recruitment of foreign workers to the mobilization of their own female workforce. While work conferred dignity on male family breadwinners, the paid work of married women was considered demeaning; but the unpaid community work of married women was considered ennobling, especially as it enhanced the social status of their husbands.
Beginning in the 1970s and established by the mid-1980s was women’s permanent presence in the workplace over the work-life cycle. Having children no longer impacts negatively on women’s participation rates; indeed the necessity to provide for children acts as a natural impetus for pursuit of work. According to the ILO, women now constitute 41% of the world’s documented workforce (ILO 1993a). In Nordic countries their participation rate is almost equal to men’s, although in Sweden, part-time work for women, while declining, is still high. In OECD industrialized countries, as the general female life expectancy is now 79, the importance of secure work as a source of income security over the adult lifespan is underscored.
The OECD acknowledges that the marked increase in female participation in employment has not produced any major convergence in the overall distribution of female and male employment. The sex-segregated workforce persists vertically and horizontally. Compared with men, women work in different sectors and occupations, work for smaller industries or organizations, have different tasks within occupations, are more often in irregular and unregulated work, have less opportunity for work control, and face the psychological demands of people-oriented or machine-paced work.
Much literature still blames women for choosing less competitive jobs that complement family responsibilities. However, a generation of studies has shown that workers not only choose, but are chosen into, occupations. The higher the rewards and status, the more restrictive the selection process and, in the absence of equity-oriented public policy and structures, the more likely that selectors choose candidates with characteristics matching their own regarding gender, race, socio-economic status or physical attributes. Stereotyped prejudices extend to a whole range of capabilities, including the ability to think abstractly.
Not only are women concentrated in few occupations with low pay and status and with restricted physical and occupational mobility, the OECD notes also that women’s occupations are often classified in broad categories comprising very different tasks, while a more precise job categorization has been developed for men’s occupations with implications for job evaluation, pay, mobility, and for the identification of safety and health risks in the work environment.
The health sector is probably the greatest example of persistent gender discrimination, where capabilities and performance are secondary to gender. Women everywhere are the major stakeholders in the health care system, as providers, guardians, brokers and, because of their reproductive needs and their longevity, users of the health care. But they do not run the system. In the former Soviet Union, where women predominated as physicians, that profession had relatively low status. In Canada, where 80% of health care workers are women, they earn 58 cents of every dollar earned by men in the same sector, less than the two-thirds of male pay earned by women in other sectors. Pay equity measures in both federal and provincial jurisdictions are attempting to close this gender gap. In many countries females and males performing comparable work are given different job titles and, in the absence of legislation and enforcement of pay equity or equal pay for work of equal value, inequities persist, with female health care workers, particularly nurses, bearing major responsibilities without commensurate authority, status and pay. It is of interest that only recently did the ILO include health in the category of heavy work.
Despite the presence of a “glass ceiling”, which confined women to middle management and the lower professional echelons, the growth of employment opportunities in the public sectors of both industrialized and developing countries was very beneficial to women, especially those with high educational attainment. The stagnation and downsizing of this sector has had serious adverse effects on women’s initial opening prospects. These positions offered greater social security, more opportunities for mobility, quality working conditions and fairer employment practices. Cutbacks have also resulted in heavier workloads, lack of security, and deterioration of working conditions, particularly in the health sector, but also in blue-collar and machine-paced pink-collar work.
“Poisoning” the Workplace
Backlash is defined by Faludi (1991) as a pre-emptive strike that stops women long before they reach the finish line. Backlash takes many forms, one of the most insidious being the derision of “political correctness” to discredit social acceptance of employment equity for disadvantaged groups. Used by persons in authority, intellectual elites or media personalities, it has an intimidating, brainwashing effect.
To understand backlash we must understand the nature of the perceived threat. Although the aspirations and efforts of the women’s movement for gender equality are nowhere realized, those who lead the backlash realize that what has been happening for the past two decades is not just incremental change, but the beginning of a cultural transformation affecting all spheres of society. The inroads to power-sharing are still minor and fragile when women occupy barely 10% of all legislative seats throughout the world. But backlash is aimed at arresting, reversing and de-legitimizing any progress achieved through employment equity or affirmative or positive action as measures to control discrimination. Combined with weak enforcement and shrinking job opportunities, backlash can have a toxic effect on the workplace, fostering confusion about wrongs and rights.
Moghadam (1994) of the United Nations Educational, Scientific and Cultural Organization (UNESCO) writes of cultural backlash, employed by fundamentalist groups, playing on emotions of fear and shame to restrict women’s visibility and their control over their lives and confine them to the private domestic sphere.
Systematic implementation of the United Nations Convention on the Elimination of Discrimination Against Women in All Its Forms (CEDAW), which has been ratified by nearly all Member States of the United Nations, would both demonstrate and promote political will to end gender discrimination, particularly in employment, health and education, along with discrimination against other “non-charter” groups.
Harassment, which can seriously interfere with the exercise of one’s capabilities, has only recently become an occupational health and human rights issue. Ethnic slurs, graffiti, name calling of persons with disabilities or of visible minorities have often been trivialized as “part of the job”. Employment insecurity, fear of reprisal, denial and lack of acknowledgement by one’s social milieu or the authorities, and lack of awareness of its systemic nature, together with lack of recourse, have contributed to complicity and tolerance.
Sexual harassment, while experienced at all occupational levels, is most pervasive at the lower levels where women are concentrated and most vulnerable. (A very small percentage of males are victims.) It became an employment and public policy issue only when large numbers of professional and executive women during the 1970s were confronted by this unwelcome interference and as women were entering trades, making them feel like intruders in their new workplaces. The effects on the health of the worker are widespread, leading in extreme cases to suicide attempts. It also contributes to family breakdown. Unions, not at the forefront of combating sexual harassment, now regard it as a grievable employment and human rights issue and have developed policies and mechanisms of redress. Services to promote healing and coping of survivors are still underdeveloped.
In a 1989 case, the Supreme Court of Canada defined sexual harassment as “unwelcome conduct of a sexual nature which detrimentally affects the work environment ... ”. The Supreme Court determined that the Canadian Human Rights legislation confers a statutory duty on employers to provide a safe and healthy working environment, free of sexual harassment, and that employers could be held liable for the actions of their employees, especially supervisors (Human Resources Development Canada 1994).
Violence is a workplace risk. Evidence of this comes from a US Justice Department survey which revealed that one-sixth of violent crimes, affecting nearly 1 million victims annually, occur at work: 16% of assaults, 8% of rapes and 7% of robberies, with a loss of 1.8 million workdays. Fewer than half are reported to the police.
Assault or abuse constitutes a major threat to the mental and physical health of girls and women of all ages and cultures, but mostly of the young and the old. The Pan-American Health Organization (PAHO) has found that in the Americas, violent deaths (i.e., accidents, suicides and homicides) represent more than 25% of all deaths in girls aged 10 to 14 and 30% in the 15- to 19-year age group (PAHO 1993).
Gender-based violence includes physical, sexual and psychological abuse and financial misappropriation, as well as sexual harassment, pornography, sexual assault and incest. In a global context we could add sex selection, abortion of female foetuses, wilful malnutrition, ritual gender mutilation, dowry deaths, and sale of daughters for prostitution or marriage. It is acknowledged that violence against women disrupts their lives, limits their options and intentionally blocks their aspirations. Both intent and consequences signify it as criminal behaviour. However, the violence from known assailants against women at home, at work or on the street, has generally been considered a private matter. The 1989 massacre of 27 Montreal women students at a Polytechnic, precisely because they were women engineering students at a Polytechnic, is brutal evidence of gender-based violence aimed at thwarting occupational aspirations.
The prevention and control of violence are workplace issues which can be addressed through employee assistance programmes and health and safety committees, working in partnership with law enforcement agencies and other agencies of society including grass-roots women’s organizations throughout the world, which placed the matter on public agendas and have been attempting, bare-knuckled, to achieve zero tolerance and to aid the survivors.
Changing World of Work
From 1970 to 1990, the economically predominant G-7 countries (excepting Japan and Germany) experienced de-industrialization, with a decline in manufacturing employment and the emergence of a post-industrial service economy. This period also coincided with the rise of the welfare state. At the end of the period, services in general (including manufacture-related services) accounted for two-thirds to three-quarters of employment. Excepting Japan and Italy, social services accounted for one-quarter to one-third of employment. These two trends created unprecedented demands for female employees who had benefited from improved educational opportunities. A zeitgeist of growing demands for human rights and equal opportunities also favoured the beginning integration of other “non-preferred” workers (e.g., persons with disabilities, minorities) (Castells and Oayama 1994).
Today, the world of work is undergoing a radical transformation characterized by globalization, take-overs and mergers, joint ventures, relocation, deregulation, privatization, computerization, proliferating technologies, structural adjustments, downsizing, outsourcing and the change from command to market economies. These changes and comprehensive re-engineering have altered the scale, the nature, the location, and the means and processes of production and communications, as well as the organization of and social relations in places of work. By the early 1990s, the technological revolution of information processing and communications, biotechnology and automated materials-processing was widespread, modifying, extending or reducing human effort and producing “efficient” jobless growth. In 1990, there were at least 35,000 transnational corporations with 150,000 foreign affiliates. About 7 million of the 22 million persons they employ, work in developing countries. Transnational corporations now account for 60% of world trade (much of it internal to its subsidiaries.)
A World Health Organization Issues Paper prepared for the Global Commission on Women’s Health (1994) states:
The struggle for access to markets brings with it increased threats to the health of millions of producers. In a highly competitive climate with an emphasis on the production of cheap, tradeable goods, companies seek to produce at the lowest costs by cutting wages, increasing working hours and sacrificing costly safety standards. In many cases companies may relocate their production units to developing countries where the controls in these areas may be less strict. Women often fill the ranks of these low-paid workers. The most extreme health consequences can be seen in tragedies where scores of workers lose their lives in factory fires due to inadequate safety standards and poor working conditions.
Moreover, an estimated 70 million persons, mostly from developing countries, are migrant workers cut off from family support. The value of cash remittances from migrant workers in 1989 was US$66 billion—much more than international development assistance of $46 billion, and exceeded only by oil in international trade value. In China’s booming coastal provinces, the province of Guangdong alone has an estimated 10 million migrants. Throughout Asia, women are over-represented among workers in unregulated and un-unionized workplaces. In India (which has reputedly received over $40 billion of loans for development from international financing institutions) 94% of the female labour force is in the unorganized sector.
Behind the miracle of exponential economic growth in Southeast Asia is the labour in the export sector of young female, capable and docile workers who earn from US$1.50 to US$2.50 a day, about one-third the basic wage. In one country, college-educated key-punch operators earn US$150 per month. In Asia as in Latin America, the pull to urban centres has created major slums and shanty towns, with millions of unschooled children living and working in precarious conditions. Over 90 developing countries are now attempting to stem the pace of this urban drift. Thailand, in an attempt to stem or reverse the process, has established a rural development initiative to retain or return young persons to their communities, some for work in cooperative factories where their work benefits them and their communities.
The United Nations Fund for Population Activities (UNFPA) has noted that modernization strategies have often destroyed women’s economic bases as traders, craftswomen or farmers, without altering the socio-cultural context (e.g., access to credit) which prevents them from pursuing other economic opportunities (UNFPA 1993). In Latin America and the Caribbean, the economic crisis and structural adjustments policies of the 1980s engendered major cuts in the social services and health sector which both served and employed women, cut subsidies on basic food items and introduced user charges for many services formerly provided by governments as part of the development and fulfilment of basic human needs. By the end of the 1980s, 31% of all non-agricultural employment was in the precarious informal sector.
In Africa, the 1980s have been characterized as the lost decade. Per capita income dropped by an annual average of 2.4% in Sub-Saharan Africa. Almost 50% of the urban population and 80% of the rural population live in poverty. The informal sector acts as a sponge, absorbing the “excess” urban labour force. In Sub-Saharan Africa, where women produce up to 80% of the food for local consumption, only 8% own the land they work (ILO 1991).
Economic restructuring, privatization and democratization have severely affected the employment of female workers in Eastern Europe. Previously burdened by heavy work, with fewer rewards than men, household responsibilities not shared by spouses and curtailment of political freedom, they nevertheless had secure employment with state-supported benefits of social security, maternity leave and child-care provisions. Currently entrenched gender discrimination, combined with market arguments against social expenditure, have rendered women expendable and less desirable workers. As the female-predominant health and social domains of work are reduced, capable professional workers become redundant.
Unemployment is a severely disorganizing experience in the life of workers, threatening not only their livelihood, but also their social relations, their self-esteem and their mental health. Recent studies have shown that not only mental but also physical health can be compromised as unemployment may have immuno-suppressive effects, increasing the risk of disease.
We are entering the twenty-first century with a crisis of values, of weighing self-interest against the public interest. Are we building a world based on unfettered, winner-takes-all competition, whose sole criterion is the “bottom line”, a world where ethnic cleansing triumphs? Or are we building a world of interdependence, where growth is pursued together with distributive justice and respect for human dignity? At United Nations global conferences in the 1990s, the world has made a number of landmark commitments to environmental protection and renewal, to ethical and equitable population policies, to the protection and developmental nurturing of all children, to an allocation of 20% of international development funds and 20% of budgets of developing countries to social development, to an expansion and enforcement of human rights, to gender equality, and to the removal of the threat of nuclear annihilation. Such Conventions have established the moral compass. The question that looms before us is whether we have the political will to meet these goals.
Work and Workers
The World Health Organization concept of “Health for All” envisions a state of health which enables persons to lead economically and socially productive lives. This is contrary to the guiding individualistic precept of “economic man”, who seeks only to satisfy or improve his economic well-being. Moreover, as we re-contemplate the world of work, it is time to rethink the notion of “human resources” or “human capital”, a concept which views humans as expendable economic instruments, diminishing their essential and transcendental humanity. And how valid is the “dependency ratio” concept, which views all younger and older persons as non-productive dependants? Thus our precepts and current practices subordinate or subvert the idea of the society to that of the economy. Advocates of human development emphasize the need for robust economies as engines for the satisfaction of societal needs, through the equitable production, distribution and enjoyment of goods and services.
When the emphasis is unduly placed on the economy, the family is viewed merely as the unit which produces, maintains and restores workers; from this viewpoint, the family must accommodate to work demands, and the workplace is absolved of accommodation to harmonize work and family life. The ILO Workers with Family Responsibilities Convention, 1981 (No. 156), has been ratified by only 19 states, in contrast with the United Nations’ Convention on the Elimination of Discrimination Against Women in All Its Forms, which has been ratified by nearly all its members. The ILO found that very few countries reported the adoption and implementation of explicit national policies covering men and women workers with family responsibilities, in accordance with the Convention.
The World Bank Human Development projects currently account for only 17% of loans. The World Bank in recent reports has recognized the importance of investments in health and education, and has acknowledged that a significant number of development mega-projects have failed because they lacked the participation of intended beneficiaries. In a vision statement for the future, the Bank’s president has indicated that there would be greater emphasis on environmental effects and on human development to support education, nutrition, family planning and improvement in the status of women.
But there is still a conceptual lag. We are entering the twenty-first century anachronistically saddled with the philosophies and theories of the nineteenth. Sigmund Freud (despite conferring his mantle on his daughter) believed that women with their unstable superegos were morally as well as biologically deficient; Adam Smith taught us that the servant girl, unlike the factory worker, was not economically productive, while Charles Darwin believed in the “survival of the fittest”.
In this chapter we present essays on the transformation of work, on the new technologies and their implications for worker well-being, and on various forms of exploitation of workers. We consider the needs of women workers and the challenges we face in maximizing human potential.
The world has arrived at a crossroads. It can continue on the path of neoclassical economics and “Social Darwinism”, with unequal and inequitable development, with waste and disparagement of human capabilities. Or, it can opt for healthy public policy, nationally and internationally. Healthy public policy is aimed at reducing inequities, building supportive and sustainable environments and enhancing human coping and control. To accomplish this we require democratic institutions that are transparent, responsive, accountable, responsible and truly representative.
The Aerospace Industry
General Profile
History and future trends
When Wilbur and Orville Wright made their first successful flight in 1903, aircraft manufacturing was a craft practised in the small shops of experimenters and adventurers. The small but dramatic contributions made by military aircraft during the First World War helped to take manufacturing out of the workshop and into mass production. Second-generation aircraft helped post-war operators to make inroads into the commercial sphere, particularly as carriers of mail and express cargo. Airliners, however, remained unpressurized, poorly heated and unable to fly above the weather. Despite these drawbacks, passenger travel increased by 600% from 1936 to 1941, but was still a luxury that relatively few experienced. The dramatic advances in aeronautical technology and the concomitant use of air power during the Second World War fostered the explosive growth of aircraft manufacturing capacity that survived the war in the United States, the United Kingdom and the Soviet Union. Since the Second World War, tactical and strategic missiles, reconnaissance and navigational satellites and piloted aircraft have taken on ever greater military significance. Satellite communication, geo-monitoring and weather-tracking technology have become of increasing commercial importance. The introduction of turbojet-powered civilian aircraft in the late 1950s made air travel faster and more comfortable and began a dramatic growth in commercial air travel. By 1993 over 1.25 trillion passenger miles were flown worldwide annually. This figure is projected to nearly triple by 2013.
Employment patterns
Employment in aerospace industries is highly cyclical. Direct aerospace employment in the European Union, North America and Japan peaked at 1,770,000 in 1989 before decreasing to 1,300,000 in 1995, with much of the employment loss occurring in the United States and the United Kingdom. The large aerospace industry in the Confederation of Independent States has been significantly disrupted subsequent to the break-up of the Soviet Union. Small but rapidly growing manufacturing capability exists in India and China. Manufacture of intercontinental and space missiles and long-range bombers has been largely restricted to the United States and the former Soviet Union, with France having developed commercial space launch capabilities. Shorter-range strategic missiles, tactical missiles and bombers, commercial rockets and fighter aircraft are more widely manufactured. Large commercial aircraft (those with 100 or greater seat capacity) are built by, or in cooperation with, manufacturers based in the United States and Europe. The manufacture of regional aircraft (less than 100 seat capacity) and business jets is more dispersed. The manufacture of aircraft for private pilots, based primarily in the United States, decreased from nearly 18,000 aircraft in 1978 to fewer than 1,000 in 1992 before rebounding.
Employment is divided in roughly equal measures among the manufacture of military aircraft, commercial aircraft, missiles and space vehicles and related equipment. Within individual enterprises, engineering, manufacturing and administrative positions each account for approximately one-third of the employed population. Males account for about 80% of the aerospace engineering and production workforce, with the overwhelming majority of highly skilled craftspeople, engineers and production managers being male.
Industry divisions
The markedly different needs and practices of governmental and civilian customers typically result in the segmentation of aerospace manufacturers into defense and commercial companies, or divisions of larger corporations. Airframes, engines (also called powerplants) and avionics (electronic navigational, communication and flight control equipment) are generally supplied by separate manufacturers. Engines and avionics each may account for one-quarter of the final cost of an airliner. Aerospace manufacturing requires the design, fabrication and assembly, inspection and testing of a vast array of components. Manufacturers have formed interconnected arrays of subcontractors and external and internal suppliers of components to meet their needs. Economic, technological, marketing and political demands have led to an increasing globalization of the manufacture of aircraft components and sub-assemblies.
Manufacturing Materials, Facilities and Processes
Materials
Airframes were originally made from wood and fabric, and then evolved to metal structural components. Aluminium alloys have been widely used due to their strength and light weight. Alloys of beryllium, titanium and magnesium are also used, particularly in high-performance aircraft. Advanced composite materials (arrays of fibre embedded in plastic matrices) are a family of strong and durable replacements for metallic components. Composite materials offer equal or greater strength, lower weight and greater heat resistance than currently used metals and have the additional advantage in military aircraft of significantly reducing the radar profile of the airframe. Epoxy resin systems are the most commonly used composites in aerospace, representing about 65% of materials used. Polyimide resin systems are used where high temperature resistance is required. Other resin systems used include phenolics, polyesters and silicones. Aliphatic amines are often used as curing agents. Supporting fibres include graphite, Kevlar and fibreglass. Stabilizers, catalysts, accelerators, antioxidants and plasticizers act as accessories to produce a desired consistency. Additional resin systems include saturated and unsaturated polyesters, polyurethanes and vinyl, acrylic, urea and fluorine-containing polymers.
Primer, lacquer and enamel paints protect vulnerable surfaces from extreme temperatures and corrosive conditions. The most common primer paint is composed of synthetic resins pigmented with zinc chromate and extended pigment. It dries very rapidly, improves adhesion of top coats and prevents corrosion of aluminium, steel and their alloys. Enamels and lacquers are applied to primed surfaces as exterior protective coatings and finishes and for colour purposes. Aircraft enamels are made of drying oils, natural and synthetic resins, pigments and appropriate solvents. Depending on their application, lacquers may contain resins, plasticizers, cellulose esters, zinc chromate, pigments, extenders and appropriate solvents. Rubber mixtures find common use in paints, fuel cell lining materials, lubricants and preservatives, engine mountings, protective clothing, hoses, gaskets and seals. Natural and synthetic oils are used to cool, lubricate and reduce friction in engines, hydraulic systems and machine tools. Aviation gasoline and jet fuel are derived from petroleum-based hydrocarbons. High-energy liquid and solid fuels have space flight applications and contain materials with inherently hazardous physical and chemical properties; such materials include liquid oxygen, hydrazine, peroxides and fluorine.
Many materials are used in the manufacturing process which do not become part of the final airframe. Manufacturers may have tens of thousands of individual products approved for use, although far fewer are in use at any time. A large quantity and variety of solvents are used, with environmentally damaging variants such as methyl ethyl ketone and freon being replaced with more environmentally friendly solvents. Chromium- and nickel-containing steel alloys are used in tooling, and cobalt- and tungsten carbide-containing hard-metal bits are used in cutting tools. Lead, formerly used in metal-forming processes, is now rarely used, having been replaced with kirksite.
In total, the aerospace industry uses more than 5,000 chemicals and mixtures of chemical compounds, most with multiple suppliers, and with many compounds containing between five and ten ingredients. The exact composition of some products is proprietary, or a trade secret, adding to the complexity of this heterogeneous group.
Facilities and manufacturing processes
Airframe manufacturing typically is done in large, integrated plants. Newer plants often have high-volume exhaust ventilation systems with controlled make-up air. Local exhaust systems may be added for specific functions. Chemical milling and large component painting are now routinely performed in closed, automated ranks or booths that contain fugitive vapour or mist. Older manufacturing facilities may provide much poorer control of environmental hazards.
A large cadre of highly trained engineers develop and refine the structural characteristics of the aircraft or space vehicle. Additional engineers characterize the strength and durability of component materials and develop effective manufacturing processes. Computers have taken on much of the calculating and drafting work that was previously performed by engineers, drafters and technicians. Integrated computer systems can now be used to design aircraft without the aid of paper drawings or structural mock-ups.
Manufacturing begins with fabrication: the making of parts from stock materials. Fabrication includes tool and jig making, sheet-metal working, machining, plastic and composite working and support activities. Tools are built as templates and work surfaces on which to construct metal or composite parts. Jigs guide cutting, drilling and assembly. Fuselage sub-sections, door panels and wing and tail skins (outer surfaces) are typically formed from aluminium sheets that are precisely shaped, cut and chemically treated. Machine operations are often computer controlled. Huge rail-mounted mills machine wing spars from single aluminium forgings. Smaller parts are precisely cut and shaped on mills, lathes and grinders. Ducting is formed from sheet metal or composites. Interior components, including flooring, are typically formed from composites or laminates of thin but rigid outer layers over a honeycomb interior. Composite materials are laid up (put into carefully arranged and shaped overlapping layers) by hand or machine and then cured in an oven or autoclave.
Assembly begins with the build-up of component parts into sub-assemblies. Major sub-assemblies include wings, stabilizers, fuselage sections, landing gear, doors and interior components. Wing assembly is particularly intensive, requiring a large number of holes to be precisely drilled and counter-sunk in the skins, through which rivets are later driven. The finished wing is cleaned and sealed from the inside to ensure a leak-proof fuel compartment. Final assembly takes place in huge assembly halls, some of which are among the world’s largest manufacturing buildings. The assembly line comprises several sequential positions where the airframe remains for several days to more than a week while predetermined functions are performed. Numerous assembly operations take place simultaneously at each position, creating the potential for cross exposures to chemicals. Parts and sub-assemblies are moved on dollies, custom-built carriers and by overhead crane to the appropriate position. The airframe is moved between positions by overhead crane until the landing and nose gear are installed. Subsequent movements are made by towing.
During final assembly, the fuselage sections are riveted together around a supporting structure. Floor beams and stringers are installed and the interior coated with a corrosion-inhibiting compound. Fore and aft fuselage sections are joined to the wings and wing stub (a box-like structure that serves as a main fuel tank and the structural center of the aircraft). The fuselage interior is covered with blankets of fibreglass insulation, electrical wiring and air ducts are installed and interior surfaces are covered with decorative panelling. Storage bins, typically with integrated passenger lights and emergency oxygen supplies, are then installed. Pre-assembled seating, galleys and lavatories are moved by hand and secured to floor tracks, permitting the rapid reconfiguration of the passenger cabin to conform to air carrier needs. Powerplants and landing and nose gear are mounted, and avionic components are installed. The functioning of all components is thoroughly tested prior to towing the completed aircraft to a separate, well-ventilated paint hanger, where a protective primer coat (normally zinc-chromate based) is applied, followed by a decorative top-coat of urethane or epoxy paint. Prior to delivery the aircraft is put through a rigorous series of ground and flight tests.
In addition to workers engaged in the actual engineering and manufacturing processes, many employees are engaged in planning, tracking and inspecting work and expediting the movement of parts and tools. Craftspeople maintain power tools and reface cutting bits. Large staffs are needed for building maintenance, janitorial services and ground vehicle operation.
Case Study: Industrialization and Occupational Health Problems in China
The Chinese farmer’s achievements in rural industrialization and in developing township enterprises (table 1) have been remarkable. This development has indeed been the most important opportunity for rural people to escape poverty quickly. Since about the seventies, more than 100 million farmers have moved to township enterprises, a number of workers exceeding the total number of employees then in state-owned and city/collectively owned enterprises. At present, one out of every five rural labourers works in various township enterprises. A total of 30% to 60% of the total average personal net income of rural people comes from the value created by township enterprises. The output value from township industries accounted for 30.8% of the total value of national industrial production in 1992. It is predicted that by the year 2000, more than 140 million surplus farm labourers, or some 30% of the estimated rural labour force, will be absorbed by township industries (Chen 1993; China Daily, 5 Jan. 1993).
Table 1. Development of China’s township enterprises
|
1978 |
1991 |
|
|
Number of enterprises (million) |
1.52 |
19 |
|
Number of employees (million) |
28 |
96 |
|
Fixed assets (billion yuan RMB) |
22.96 |
338.56 |
|
Total output value (billion yuan RMB) |
49.5 |
1,162.1 |
This quick transfer of the labour force from agriculture to non-agricultural work in rural areas has imposed heavy pressure on the resources of occupational health services. The Survey on Occupational Health Service Needs and Countermeasures in Township Industries (SOHSNCTI) in 30 sample counties of 13 provinces and 2 municipalities, organized by the Ministry of Public Health (MOPH) and the Ministry of Agriculture (MOA) jointly in 1990, showed that most township enterprises had not provided basic occupational health service (MOPH 1992). The coverage of five routine occupational health service activities provided for township enterprises by local occupational health institutions (OHIs) or health and epidemic prevention stations (HEPSs) was very low, only 1.37% to 35.64% (table 2). Those services which need complicated techniques or well-trained occupational health professionals are particularly limited. For example, preventive occupational health inspection, physical examination for workers exposed to hazards, and workplace monitoring were evidently insufficient.
Table 2. The coverages of OHS provided to township industries by county HEPS
|
Items |
Enterprises |
Enterprises covered by OHS |
% |
|
Preventive OH inspection |
7,716 |
106 |
1.37 |
|
General industrial hygiene walk-through |
55,461 |
19,767 |
35.64 |
|
Workplace hazard monitoring |
55,461 |
2,164 |
3.90 |
|
Worker’s physical examination |
55,461 |
1,494 |
2.69 |
|
Help to set up OH record keeping |
55,461 |
16,050 |
28.94 |
Meanwhile, there is a trend that occupational health problems in rural enterprises are worsening. First, the survey showed that 82.7% of rural industrial enterprises had at least one type of occupational hazard in the workplace. Workers exposed to at least one kind of hazard accounted for 33.91% of the blue-collar workers. The air samples of lead, benzene analogues, chromium, silica dust, coal dust and asbestos dust at 2,597 worksites in 1,438 enterprises indicated that the total compliance rate was 40.82% (table 3); the compliance rates with respect to dusts were very low: 7.31% for silica, 28.57% for coal dust, and 0.00% for asbestos. The total compliance rate for noise in 1,155 enterprises was 32.96%. Physical examinations for workers exposed to more than seven hazards were conducted (table 4). The total prevalence of occupational diseases caused only by exposures to these seven types of hazard was 4.36%, much higher than the prevalence of total compensable occupational diseases in state-owned enterprises. There were another 11.42% of exposed workers suspected of having occupational diseases. Next, hazardous industries continue transferring from urban to rural areas, and from state-owned enterprises to township enterprises. Most of the workers in these industries used to be farmers before employment and lacked education. Even the employers and the managers still have very little education. A survey covering 29,000 township enterprises indicated that 78% of the employers and managers had only junior middle school or primary school education and that some of them were simply illiterate (table 5). A total of 60% of employers and managers were not aware of governmental occupational health requirements. It predicted that the prevalence of occupational diseases in rural industries will increase and reach a peak by the year 2000.
Table 3. The compliance rates of six hazards in worksites
|
Hazards1 |
Enterprises |
Worksites monitored |
Worksites complying |
Compliance rate (%)2 |
|
Lead |
177 |
250 |
184 |
73.60 |
|
Benzene analogues |
542 |
793 |
677 |
85.37 |
|
Chromium |
56 |
64 |
61 |
95.31 |
|
Silica dust |
589 |
1,338 |
98 |
7.31 |
|
Coal dust |
68 |
140 |
40 |
28.57 |
|
Asbestos dust |
6 |
12 |
0 |
0.00 |
|
Total |
1,438 |
2,597 |
1,060 |
40.82 |
1 Mercury was not found in sample areas.
2 The compliance rate for noise was 32.96%; see text for details.
Table 4. The detectable rates of occupational diseases
|
Occupational diseases |
Persons checked |
No illness |
With illness |
Suspected illness |
|||
|
No. |
No. |
% |
No. |
% |
No. |
% |
|
|
Silicosis |
6,268 |
6,010 |
95.88 |
75 |
1.20 |
183 |
2.92 |
|
Coal workers pneumoconiosis |
1,653 |
1,582 |
95.70 |
18 |
1.09 |
53 |
3.21 |
|
Asbestosis |
87 |
66 |
75.86 |
3 |
3.45 |
18 |
20.69 |
|
Chronic lead poisoning |
1,085 |
800 |
73.73 |
45 |
4.15 |
240 |
22.12 |
|
Benzene analogues poisoning1 |
3,071 |
2,916 |
94.95 |
16 |
0.52 |
139 |
4.53 |
|
Chronic chromium poisoning |
330 |
293 |
88.79 |
37 |
11.21 |
- |
- |
|
Noise-induced hearing loss |
6,453 |
4,289 |
66.47 |
6332 |
9.81 |
1,5313 |
23.73 |
|
Total |
18,947 |
15,956 |
84.21 |
827 |
4.36 |
2,164 |
11.42 |
1 Benzene, toluene and xylene, measured separately.
2 Hearing impairment in sound frequency.
3 Hearing impairment in high frequency.
Table 5. Distribution of hazardous working and the education of employers
|
Education of employers |
Total no. of enterprises (1) |
Enterprises with hazardous working (2) |
Blue-collar workers (3) |
Workers exposed (4) |
Hazardous enterprises (%) (2)/(1) |
Exposed workers (%) (4)/(3) |
|
Illiteracy |
239 |
214 |
8,660 |
3,626 |
89.54 |
41.87 |
|
Primary school |
6,211 |
5,159 |
266,814 |
106,076 |
83.06 |
39.76 |
|
Junior middle school |
16,392 |
13,456 |
978,638 |
338,450 |
82.09 |
34.58 |
|
Middle technical school |
582 |
486 |
58,849 |
18,107 |
83.51 |
30.77 |
|
Senior middle school |
5,180 |
4,324 |
405,194 |
119,823 |
83.47 |
29.57 |
|
Universities |
642 |
544 |
74,750 |
21,840 |
84.74 |
29.22 |
|
Total |
29,246 |
24,183 |
1,792,905 |
607,922 |
82.69 |
33.91 |
The Challenge of the Mass Migration of the Labour Force
The social labour force in China in 1992 was 594.32 million, of which 73.7% were classified as rural (National Statistics Bureau 1993). It is reported that one-third of the country’s 440 million rural labourers are actually unemployed (China Daily, 7 Dec. 1993). The vast surplus of labourers who have far exceeded the pool of employability in rural industries are migrating towards urban areas. The mass movement of farmers to the urban areas over the last few years, especially heavy since the beginning of the 1990s, has been the big challenge to the central and local governments. For example, in the first half of 1991, only 200,000 farmers left their hometowns in Jiangxi province, but in 1993, more than three million followed the tide, which accounted for one-fifth of the province’s rural labourers (China Daily, 21 May 1994). On the basis of state statistics, it has been predicted that 250 million rural workers would hit the urban labour market by the end of the century (China Daily, 25 Nov. 1993). In addition, there are about 20 million young people every year entering legal employment age in the entire country (National Statistics Bureau 1993). Thanks to widespread urbanization and the extensive opening to the outside world, which is attracting foreign investment, more job opportunities for migrant rural labourers have been created. The migrants are engaged in a greater variety of business in the cities, including industry, civil engineering, transport, commerce and service trades and most high-risk or hazardous work which urban people do not like to do. These workers have the same personal background as those in the rural township enterprises and are facing similar occupational health problems. In addition, because of their mobility, it is difficult to trace them and employers could easily escape from their responsibilities for the workers’ health. Furthermore, these workers are often involved in various occupations in which the health risk from hazardous exposures might be complicated and it is hard to provide them access to occupational health services. These conditions make the situation more serious.
The Occupational Health Problems Faced in Foreign-Funded Industries
There are currently more than 10 million domestic labourers nationwide employed in over 70,000 foreign-funded enterprises. Preferential policies for encouraging investment of foreign capital, the existence of vast natural resources and a cheap labour force are attracting more and more investors. The State Planning Commission of the State Council has decided to impose fewer administrative examinations on applicants. Local governments were given more power to approve the investment projects. Those involving funding under US$30 million can be decided by local authorities, with registration at the State Planning Commission, and foreign enterprises are encouraged to bid for them (China Daily, 18 May 1994). Of course, foreign-funded enterprises are also very attractive to many Chinese labourers, mainly because of the higher wages to be earned.
During the course of encouraging foreign investment, hazardous industries have also been transferred to this country. The MOPH and other related agencies have long been concerned for the occupational health of the workers in these sectors. Some local surveys have indicated the magnitude of the problem, which involves high exposure to occupational hazards, long working hours, poor working arrangements, special problems for female workers, no proper personal protection, no health examination and education, no medical insurance and discharge of workers who are affected by occupational diseases, among other problems.
The incidence of chemical poisoning accidents has been increasing in recent years. Information from the Guangdong Provincial Institute of Occupational Disease Prevention and Treatment in 1992 reported that two accidents of solvent poisoning happened simultaneously in two overseas-funded toy factories in the Zhuhai special economic zone, resulting in a total of 23 cases of worker toxicity. Of these, 4 persons were afflicted by 1,2-dichloroethane poisoning and three of them died; another 19 cases had benzene analogues (benzene, xylene and toluene) poisoning. These workers had worked in the factories for just less than one year, a few of them for only 20 days (Guangdong Provincial Occupational Disease Prevention and Treatment Hospital 1992). In the same year, two poisoning accidents were reported from Dalian City, Liaoning Province; one had involved 42 workers and another involved 1,053 workers (Dalian City Occupational Disease Prevention and Treatment Institute 1992b). Table 6 shows some basic occupational health–related conditions in three special economic zones (SEZs) in Guangdong and the Dalian Economic and Technological Development Area, surveyed by local OHIs or HEPSs (Dalian City Occupational Disease Prevention and Treatment Institute 1992b).
Table 6. Occupational health-related background in foreign-funded enterprises
|
Area |
No. of enterprises |
No. of employees |
Enterprises with occupational hazards (%) |
Exposed workers (%) |
Enterprises having OHSO1 (%) |
Enterprises providing health examinations (%) |
||
|
Periodic |
Pre-employment |
|||||||
|
Guangdong2 |
657 |
69,996 |
86.9 |
17.9 |
29.3 |
19.6 |
31.2 |
|
|
Dalian3 |
72 |
16,895 |
84.7 |
26.9 |
19.4 |
0.0 |
0.0 |
|
1 Any form of occupational health and safety organization in plan, e.g. clinics, OHS committee, etc.
2 The survey in 1992, in three special economic zones (SEZs): Shenzhen, Zhuhai and Shantou.
3 The survey in 1991 in Dalian Economic and Technological Development Area.
The employers of foreign-funded enterprises, especially small manufacturing factories, ignore governmental regulations and rules in protecting workers’ rights and their health and safety. Only 19.6% or 31.2% of workers in three Guongdong SEZs could get any kind of health examination (see table 6). Those enterprises making no provision for personal protective equipment for exposed workers accounted for 49.2% and only 45.4% of the enterprises provided hazard exposure subsidies (China Daily, 26 Nov. 1993). In Dalian, the situation was even worse. Another survey conducted by the Guangdong Provincial Trade Union in 1993 indicated that more than 61% of employees worked over six days a week (China Daily, 26 Nov. 1993).
Female workers suffer even more from appalling work conditions, according to a report released in June by the All-China Confederation of Trade Unions (ACFTU). A poll conducted by the ACFTU in 1991 and 1992 among 914 foreign-funded enterprises showed that women accounted for 50.4% of the total 160 thousand employees. The proportion of women is higher in some areas in recent years. Many foreign firms did not sign labour contracts with their employees and some factories hired and fired woman workers at will. Some overseas investors employed only unmarried girls between the ages of 18 and 25 years, whom they dismissed once they got married or became pregnant. Meanwhile, many women were often forced to work overtime without extra pay. In a toy factory in Guangzhou, capital of Guangdong Province, workers, most of them women, had to work 15 hours a day. Even then, they were not allowed to take Sundays off or enjoy any annual holiday (China Daily, 6 July 1994). This is not a very rare phenomenon. Details of workers’ occupational health status in foreign-funded enterprises have not yet been made known. From the information above, however, one can imagine the gravity of the problem.
New Problems in State-Owned Enterprises
In order to meet the requirements of a market economy, the state-owned enterprises, especially the large and medium ones, have to transform the traditional operational mechanism and establish a modern enterprise system which would clearly outline property rights and enterprise rights and responsibilities and at the same time push the state-owned enterprises into the market to increase their vitality and efficiency. Some small state-owned enterprises may be leased or sold to collectives or individuals. The reforms have to affect every aspect of business, including occupational health programmes.
At present, losing money is a serious problem faced by many state-owned enterprises. It is reported that about one-third of the enterprises are in deficit. The reasons for this are diverse. First, there is a heavy tax and financial burden intended to take care of a large contingent of retired employees and to provide a host of social welfare benefits to current workers. Second, a huge surplus labour force, about 20 to 30% on average, in an enterprise cannot be released into the existing fragile social security system. Third, the outdated management system was adapted to the traditional planned economy. Fourth, the state-owned enterprises have no competitive policy advantages over foreign-funded firms (China Daily, 7 April 1994).
Under these circumstances, occupational health in the state-owned enterprises tends to become inevitably weakened. First, financial support for health programmes has been reduced in the case of some enterprises and the medical/health institutions in enterprises which used to offer health care only to their own employees before are opening them now to communities. Second, some in-plant health facilities are being divorced from affiliation with enterprises as part of an effort to shift the burden of costs from state-owned enterprises. Before the new social security system was set up, there was concern, too, that funding for occupational health in-plant programmes might also be affected. Third, much outdated technology and equipment has been operating for decades, usually with high levels of hazardous emissions, and cannot be improved or replaced in a short period of time. More than 30% of the worksites of state-owned and city-collective enterprises are not in compliance with national hygienic standards (MAC or MAI). Fourth, the implementation of occupational health regulations or rules has been weakened in recent years; of course, one of the reasons for this is the incompatibility between the old management system of occupational health in the days of central planning with the new situation of enterprise reform. Fifth, to decrease the cost of labour and to offer more widespread employment opportunities, the hiring of temporary or seasonal workers, most of whom are migrants from rural areas, to engage in hazardous work in state-owned enterprises has become a common phenomenon. Many of them cannot get even the simplest personal protective equipment or any safety training from their employers. This has continued to be a potential health threat affecting the working population of China.
Problems in the Occupational Health Service System
The coverage of occupational health services is not extensive enough. As mentioned above, only 20% of the workers exposed to hazards can be covered by periodic health examination, most of whom are working in state-owned enterprises. The reasons why the coverage is so low are as follows:
First, the shortage of occupational health service resources is one of the main factors. This is especially the case for rural industries, which have no capacity to provide such services themselves. The data from the SOHSNCTI has shown that there were 235 occupational health professionals in county HEPSs in 30 sampled counties. They have to deliver occupational health service to 170,613 enterprises with 3,204,576 employees in those areas (MOPH 1992). Thus, each full-time occupational health worker covered an average of 1,115 enterprises and 20,945 employees. Also emerging from the 1989 survey was the fact that the health expenditures of 30 county governments accounted for 3.06% of the total county government expenditures. The total expenditures for both disease prevention and health inspection accounted for only 8.36% of the total county governmental health expenditures. The fraction expended purely on occupational health services was even smaller. Lack of basic equipment for occupational health service is a big problem in the surveyed counties. The average availability of thirteen categories of equipment in 28 of the 30 counties was only 24% of the requirement defined in the national standard (table 7).
Table 7. Routine instruments for occupational health in HEPS of 28 countries in 1990, China
|
Items |
Number of instruments |
Number of instruments required by standard |
Per cent (%) |
|
Air sampler |
80 |
140 |
57.14 |
|
Personal sampler |
45 |
1,120 |
4.02 |
|
Dust sampler |
87 |
224 |
38.84 |
|
Detector for noise |
38 |
28 |
135.71 |
|
Detector for vibration |
2 |
56 |
3.57 |
|
Detector for heat radiation |
31 |
28 |
110.71 |
|
Spectrophotometer (Type 721) |
38 |
28 |
135.71 |
|
Spectrophotometer (Type 751) |
10 |
28 |
35.71 |
|
Mercury determination meter |
20 |
28 |
71.43 |
|
Gas chromatograph |
22 |
28 |
78.57 |
|
Weighing balance (1/10,000g) |
31 |
28 |
110.71 |
|
Electrocardiograph |
25 |
28 |
89.29 |
|
Lung function test |
7 |
28 |
25.00 |
|
Total |
436 |
1,820 |
23.96 |
Second, low utilization of existing occupational health facilities is another factor. The shortage of resources on the one hand and insufficient utilization on the other is the case with occupational health service in China right now. Even at higher levels, for example, with the provincial OHIs, the equipment is still not being fully put to use. The reasons for this are complicated. Traditionally, occupational health and various preventive medical services were all financed and maintained by government, including the wages of health workers, the equipment and buildings, routine outlays and so forth. All occupational health services provided by governmental OHIs were free of charge. With the rapid industrialization and economic reform since 1979, the needs of society for occupational health service have been increasing, and the cost for providing services at the same time increased rapidly, reflecting an increasing price index. The budgets of the OHIs from government, however, have not increased to keep pace with their needs. The more services an OHI provides, the more funding it needs. To promote the development of public health service and meet growing social needs, the central government has instituted the policy of allowing the public health sector to subsidize payments for services, and stipulations have been made to control the price of health services. Because of weak compulsory legislation in providing occupational health service for enterprises in the past, OHIs are finding it difficult to maintain themselves by collecting payment for services.
Further Policy Considerations and Trends in Occupational Health Services
Without doubt, occupational health service is one of the most important issues in a developing country like China, which is undergoing rapid modernization and possesses such huge numbers of workers. While facing the great challenges, the country is also, at the same time, welcoming the great opportunities arising from present social reforms. Many successful experiences exemplified across the international scene can be taken as references. In opening up so widely to the world today, China is willing actively to absorb the advanced occupational health managerial ideas and technologies of the broader world.
Economic Aspects of Occupational Health and Safety
The losses to society from work-related accidents and illnesses are very large, but no society can afford to prevent all these losses. Because of the scarcity of resources, limited investments have to be targeted carefully to give the “biggest bang for the buck”. The mere costing of occupational ill-health does not facilitate the targeting of investment. Proper economic evaluation can be helpful if it is well designed and executed. The results of such evaluation can be used, with appropriate critical appraisal of the practice of evaluations, to inform investment choices. Economic evaluation will not and should not determine investment decisions. Such decisions will be the product of economic, political and social values. As Fuchs (1974) argued:
At the root of most of our major health problems are value choices. What kind of people are we? What kind of life do we want to lead? What kind of society do we want to build for our children and grandchildren? How much weight do we want to put on individual freedom? How much to equality? How much to material progress? How much to the realm of the spirit? How important is our own health to us? How important is our neighbour’s health to us? The answers we give to these questions, as well as the guidance we get from economics, will and should shape health care policy.
A decision to regulate the mining industry so that fewer workers are killed and maimed will, if successful, bring health benefits to the workforce. These benefits, however, have associated costs. In real-life situations, the increased costs of improving safety will drive up prices and reduce sales in competitive world markets and may induce in employers deviance from regulations. Such deviation may be condoned by labour unions and their members, who may prefer imperfect implementation of health and safety laws if it improves incomes and employment prospects.
The purpose of economic analysis in occupational health is to facilitate the identification of that level of safety investment which is efficient. Efficiency means that the costs of doing a little more (the marginal cost) to enhance safety equal the benefits (the marginal returns in terms of health and welfare enhancements result from risk reduction). The economic aspects of occupational health and safety are central to decision making at all levels: the shop floor, the firm, the industry and the society. To behave as if all workplace risks to workers’ health can be eradicated may be inefficient. Risks should be eradicated where it is cost effective. But some risks are rare and too costly to eradicate: they have to be tolerated and when these rare events damage workers’ welfare, they have to be accepted as unfortunate but efficient. There is an optimal level of occupational risk beyond which the costs of risk reduction exceed the benefits. Investment in safety beyond this point will generate safety benefits which should be bought only if society is prepared to act inefficiently. This is a social policy decision.
Types of Economic Analysis
Cost analysis
Cost analysis involves the identification, measurement and valuation of the resource consequences of occupational accidents and ill health. Such descriptions illuminate the size of the problem but do not inform decision makers about which of many competing interventions by all who govern and regulate the workplace environment is the most efficient.
A nice example of this is a British study of the costs to economy of work accidents and work related illness (Davies and Teasdale 1994). In the year 1990 there were 1.6 million accidents reported at work, and 2.2 million people suffered ill health which was caused or exacerbated by the working environment. As a result of the events, 20,000 people were obliged to give up work and 30 million working days were lost. The loss of income and welfare to the victims and their families was estimated to be £5.2 billion. The loss to employers was between £4.4 and £9.4 billion. The loss to society as a whole was £10.9 to £16.3 billion (see table 1). The authors of the British report noted that whilst the numbers of reported accidents and industrial diseases had fallen, the estimated costs were higher.
Table 1. The costs to the British economy of work accidents and work-related health (1990 £m)
|
Costs to individual victims and their families |
Costs to their employers |
Costs to society as a whole |
|||
|
Loss of income |
(£m) |
Extra production costs |
(£m) |
Lost output |
(£m) |
|
Injury Illness |
376 579 |
Injury Illness |
336 230 |
Injury Illness |
1,365 1,908 |
|
Damage and loss in accidents |
Resource costs: Damage in accidents |
||||
|
Injury Non-injury Insurance |
15-140 2,152-6,499 505 |
Injury Non-injury Insured |
15-140 2,152-6,499 430 |
||
|
Medical treatment |
|||||
|
Injury Illness |
58-244 58-219 |
||||
|
Administration/recruitment |
Administration, etc. |
||||
|
Injury Illness Non-injury |
58-69 79-212 307-712 |
Injury Illness Non-injury |
132-143 163-296 382-787 |
||
|
Loss of welfare |
Loss of welfare |
||||
|
Injury Illness |
1,907 2,398 |
Employer liability Insurance |
750 |
Injury Illness |
1,907 2,398 |
|
Total |
5,260 |
Total |
4,432-9,453 |
Total |
10,968-16,336 |
|
Less: compensation from employers’ liability insurance |
650 |
||||
|
Net total |
4,610 |
||||
Source: Davies and Teasdale 1994.
The costs were higher than those reported in previous studies because of revised techniques of welfare loss estimation and better sources of information. The central information ingredient in this sort of costing exercise is the epidemiology of work-related accidents and diseases. As in all other areas of social cost analysis (e.g., alcohol—see McDonnell and Maynard 1985) the measurement of the volume of events tends to be poor. Some (how many?) accidents are not reported. The link between disease and the workplace may be obvious in some cases (e.g., asbestos-related diseases) but uncertain in other cases (e.g., heart disease and occupational risk factors). Thus it is difficult to identify the volume of work-related events.
The costing of those events which are identified is also problematic. If work stress leads to alcoholism and dismissal from employment, how are the effects of these events on the family to be valued? If an accident at work causes pain for life, how is that to be valued? Many costs can be identified, some can be measured, but often a considerable proportion of costs which are measured and even quantified, cannot be valued.
Before too much effort is expended on the costing of work-related health events, it is essential to be certain about the purpose of such work and the value of great accuracy. The costing of accidents and work-related illness does not inform the decision-making about investments in prevention of such events because it tells managers nothing about the costs and benefits of doing a little bit more or a little bit less of that prevention activity. The cost of events related to occupational ill health can identify section losses (to the individual, the family and the employer) and the costs to society. Such work does not inform prevention activity. The relevant information for such choices can be derived only from economic evaluation.
The principles of economic evaluation
There are four types of economic evaluation: cost minimization analysis, cost benefit analysis, cost effectiveness analysis and cost utility analysis. The characteristics of these approaches are outlined in table 2.
Table 2. Types of economic evaluation
|
Cost measurement |
Outcome measurement: What? |
Outcome measurement: How valued? |
|
|
Cost minimization analysis |
£ |
Assumed identical |
None |
|
Cost benefit analysis |
£ |
All effects producedby the alternative |
Pounds |
|
Cost effectiveness analysis |
£ |
Single common specific variable achieved to varying extents |
Common units (e.g., life years) |
|
Cost utility analysis |
£ |
Effects of the competing therapies and achieved to differing levels |
QALYs or DALYs |
In cost minimization analysis (CMA) it is assumed that the outcome effect is identical in each of the alternatives being compared. Thus we may have two interventions to reduce the carcinogenic effects of a production process, and engineering and other data shows that the effects are identical in terms of exposure and cancer reductions. CMA can be used to cost the alternative strategies in order to identify the cheapest alternative.
Obviously the assumption of identical effects is strong and not likely to be met in most investment cases; for example, the effects of alternative safety strategies on the length and quality of workers’ lives will be unequal. In this case alternative evaluation methods have to be used.
The most ambitious of these methods is cost benefit analysis (CBA). This requires the analyst to identify, measure and value both the costs and the benefits of the alternative prevention strategies in terms of a common monetary measure. Valuing the costs of such investments can be difficult. However these problems tend to be slight compared to the monetary valuation of the benefits of such investments: how much is an injury avoided or life saved worth? As a consequence of such difficulties CBA has not been used extensively in the accident and health areas.
A more restricted form of economic evaluation, cost effectiveness analysis (CEA), has been used extensively in the health field. (CEA) was developed by the US military, whose analysts adopted the notorious measure of effect, “body count”, and sought then to identify which was the cheapest way of achieving a given enemy body count (i.e., what were the relative costs of artillery barrages, napalm bombing, infantry charges, tank advances and other “investments” in achieving a target mortality effect on the enemy).
Thus in CEA there is usually a simple, sector-specific effect measure, and the costs of achieving differing levels of reduction in, for instance, workplace events or workplace mortality can thus be computed.
The limitation of the CEA approach is that the effect measures may not be generalizable—that is, a measure used in one sector (e.g., reducing exposure to asbestos) may not be usable in another area (e.g., reducing electrical accident rates in the power distribution industry). Thus CEA may inform the decision making in a particular area but will not generate evaluative information to elucidate the costs and effects of investment choices across a wide range of prevention strategies.
Cost utility analysis (CUA) was devised to overcome this problem by using a generic effect measure, such as a quality adjusted life year (QALY) or disability adjusted life year (DALY) (see Williams 1974 and World Bank Report on Health 1993, for example). CUA techniques can be used to identify the cost/QALY effects of alternative strategies and such information can inform prevention investment strategies in a more comprehensive manner.
The use of techniques of economic evaluation in health care is well established, although their use in occupational medicine is more limited. Such techniques, given the difficulties of measuring and valuing both costs and benefits (e.g., QALYs), are useful, if not essential, in informing choices about prevention investment. It is extraordinary that they are used all too rarely and that, as a consequence, investment is determined “by guess and by God” rather than by careful measurement within an agreed analytical framework.
The Practice of Economic Evaluation
As in all other areas of scientific endeavour, there is variance between the principles of economic evaluation and its practice. Thus when using studies about the economic aspects of occupational accidents and diseases, it is essential to evaluate the evaluations with care! The criteria to judge the merit of economic evaluations have long been established (e.g., Drummond, Stoddart and Torrance 1987 and Maynard 1990). A pioneer in this work, Alan Williams, set out the following list of relevant issues over two decades ago (Williams 1974):
- What precisely is the question which the study was trying to answer?
- What is the question that it has actually answered?
- What are the assumed objectives of the activity studied?
- By what measures are these represented?
- How are they weighted?
- Do they enable us to tell whether the objectives are being attained?
- What range of options was considered?
- What other options might there have been?
- Were they rejected, or not considered, for good reasons?
- Would their inclusion have been likely to change the results?
- Is anyone who has not been considered in the analysis likely to be affected?
- If so why are they excluded?
- Does the notion of cost go wider or deeper than the expenditure of the agency concerned?
- If not, is it clear that these expenditures cover all the resources used and accurately represent their value if released for other uses?
- If so, is the line drawn so as to include all potential beneficiaries and losers, and are resources costed at their value in their best alternative use?
- Is the differential timing of the items in the streams of benefits and costs suitably taken care of (e.g., by discounting) and, if so, at what rate?
- Where there is uncertainty, or there are known margins of error, is it made clear how sensitive the outcome is to these elements?
- Are the results, on balance, good enough for the job at hand?
- Has anyone else done better?
There are several areas in economic evaluation where practice tends to be defective. For instance in the area of back pain, which causes major work-related illness losses to society, there is dispute about the competing treatments and their effects. The “old-fashioned” treatment for back pain was bed rest, but the preferred modern treatment is activity and exercise to dissipate the muscle strain which generates the pain (Klaber Moffett et al. 1995). Any economic evaluation has to build on clinical knowledge, and this is often uncertain. Thus without careful appraisal of the effectiveness knowledge base, modelling of the economic effects of alternative interventions may be biased and confusing for decision makers, as happens in the health care field (Freemantle and Maynard 1994).
High quality economic evaluations of prevention investments to reduce work-related illness and accidents are few in number. As in health care in general, the studies that are available are often of poor quality (Mason and Drummond 1995). Thus, buyer beware! Economic evaluations are essential but deficiencies in current practice are such that users of this science must be able to appraise critically the available knowledge base before committing society’s scarce resources.
Product Stewardship and the MIgration of Industrial Hazards
Multinational corporations are dominant in the manufacturing and marketing of chemicals and other products where occupational health and safety hazards are known to exist. These corporations have long but variable experience in managing to control such hazards and some have developed large staffs and procedures for this purpose. With the trend towards ever more free-trade agreements, the dominance of multinational corporations (MNCs) is expected to expand, with a corresponding decline in the scale of state-owned industries and privately owned industries within nations. It is thus appropriate to consider the proper role of MNCs as industries are expanded all over the world, particularly in countries that have to date had minimal resources made available for worker and environmental protection.
The European Chemical Industry Council (CEFIC), in its CEFIC Guidelines on Transfer of Technology (Safety, Health and Environment Aspects), says that transferred technology should achieve a degree of safety, health protection and protection of the environment equal to that of the technology supplier from which it is derived and “equivalent to that achieved in the home facilities of the technology supplier” (CEFIC 1991). This would seem especially applicable to the worldwide subsidiary operations of MNCs.
Double Standards
There have been many examples where MNCs have not been as thorough in controlling industrial hazards in developing countries as they were in their home countries. The most numerous reports of this double standard have arisen in connection with asbestos and other ultra-hazardous materials, where substantial control of the hazards would represent a major share of overall costs of production and reduce sales in other ways. The cases described in the 1970s and early 1980s involved firms based in West Germany, the United States, the United Kingdom, Switzerland, Italy, Austria and Japan (Castleman and Navarro 1987).
The best-examined case of this double standard involves the pesticide manufacturing plant which caused thousands of deaths and permanent health impairment to many thousands of people in Bhopal, India, in 1984. Comparison of the Bhopal plant with a similar plant operated in the United States showed numerous double standards in plant design and operation, safety auditing, worker training, staffing of hazardous jobs, plant maintenance and management accountability. Additional relevant factors were the relative lack of government regulation and civil liability in India, compared with the United States (Castleman and Purkayastha 1985).
The Bhopal disaster focused world attention on the policies and practices of MNCs for safeguarding worker health and safety and the environment. Many giant manufacturing companies suddenly realized that they were running excessive, reducible risks and moved to reduce the amounts of highly toxic compressed gases they were storing and transporting. Transport of large cylinders of phosgene gas, for example, went from being a common practice in the United States to being completely avoided. Such changes were in no small part due to the fact that insurance for the consequences of chemical releases into communities became virtually unavailable. But above and beyond purely economic considerations, the ethics and morality of the conduct of the multinational companies were subjected to unprecedented scrutiny.
Obviously, lower standards of worker and environmental protection can confer at least short-term savings on factory owners. The temptation to increase profits by cutting costs is especially great where there is virtually no governmental regulation, public awareness, trade union pressure or liability for damages when something does go wrong. The Bhopal case showed that when profit levels are low, there is an added pressure on management to reduce operating costs by methods whose immediate costs are slight but whose long-term risks may be catastrophic. The structure of MNCs seemed ideal, moreover, for insulating top management from bearing any personal responsibility for the consequences of complying with local standards around the world.
The ILO investigation, Safety and Health Practices of Multinational Enterprises, found that “in comparing the health and safety performance of home-based (MNCs) with that of the subsidiaries, it could generally be said that the home country operations were better than those of the subsidiaries in the developing countries” (ILO 1984). A United Nations Centre on Transnational Corporations (UNCTC) report urged examination of MNC policies with regard to “occupational health and safety in their global operations.” The report concluded that there were “numerous examples of a ‘double standard’ in which worker and community health protection measures by transnational corporations are far weaker in the developing countries than in the transnational corporations’ home nations”. Examples of this were in vinyl chloride, pesticides, chromates, steel, chlorine and asbestos industries (UNCTC 1985).
The response of the very largest chemical MNCs based in the United States and the United Kingdom was to deny that it was company policy to have different standards in different countries for protecting people from the same industrial hazards. However, these sentiments have been expressed in different ways, some of which entail greater commitment than others. Moreover, many remain sceptical that a wide gulf remains between corporate policy statements and the reality of double standards in corporate conduct.
Product Stewardship
Product stewardship refers to a seller’s responsibility for preventing harm arising from products marketed, throughout the life cycle of product use and disposal. It includes the responsibility of assuring that a company buying the seller’s chemical product does not use it in a hazardous manner; at least one US firm, Dow Chemical, has long expressed a policy of refusing to sell chemicals to such customers. In 1992, the Chemical Manufacturers Association member companies in the United States adopted a code that contemplates termination of sales to customers who do not correct “improper practices” in the use of the chemicals they sell.
Examples of the need for product stewardship by pesticide producers abound. Repackaging of pesticides in food containers and the use of pesticide drums to store drinking water are causes of widespread death and disease. Small farmers’ use and storage of pesticides and pesticide containers reflect a general lack of training that manufacturers could provide.
In the Dominican Republic’s Costanza Valley, defoliation from overuse of pesticides has caused the area to be called the “Valley of Death”. As the area gained media attention in 1991, Ciba-Geigy, a major chemical MNC, introduced a programme to teach small farmers something about agronomy, integrated pest management and safety. It was recognized that pesticide use in the valley had to be reduced. Community response to Ciba’s effort to “prove the economic and social benefits of a sustainable market” was reported to be encouraging in the trade press. Ciba operates similar small farmer programmes in Colombia, the Philippines, Indonesia, Pakistan, Mali, Mozambique and Nigeria. The Pesticide Action Network is sceptical of corporate versions of “integrated pest management” that stress the “best mix” of pesticides instead of training people in techniques whereby pesticide use is seen as a last resort.
An important aspect of product stewardship is educational outreach to workers and the public using the product, through warning labels, brochures and customer training programmes. For certain hazardous products and containers in which they are sold, product stewardship entails retrieving materials that customers would otherwise use improperly or dispose of as hazardous wastes.
In US courts, product stewardship is strongly encouraged by the existence of liability for damages caused by hazardous products and pollution. Individuals harmed by products whose dangers were not always expressed in warnings by manufacturers have been awarded substantial compensation for economic loss, pain and suffering and in some cases punitive damages in addition. Manufacturers have withdrawn from the US market products shown in animal experiments to cause reproductive abnormalities—rather than risk multimillion dollar lawsuits from children of workers using the agent who have been born with birth defects. These same products have sometimes continued to be marketed by the same companies in other countries, where product liability is not a factor.
Liability and regulation have thus imposed a duty on manufacturers in some countries to develop less toxic processes and products. But in the absence of public awareness, liability and regulation, there is the possibility that the discredited, more hazardous technologies will remain economically competitive, and there may even be a market for the older technology that can be exploited in many countries. Thus, despite the advances being made by MNCs in the development of “clean technology”, there is no reason to expect that these improvements will be promptly transmitted to Africa, Asia, Latin America and Central and Eastern Europe. It is very possible that some of the newly built industry in these regions will be made with used, imported equipment. This poses an ethical challenge to the MNCs who own equipment that is being replaced in Europe and North America.
Public Health Advances
A number of advances have occurred in recent years, which would unquestionably contribute to the protection of public health and the environment wherever they take root. Industrial research chemists, whose goal has traditionally been the maximization of product yield with little concern about toxicity of products and by-products, now discuss developments in less toxic technology at symposia on “green chemistry”, or “industrial ecology” (Illman 1994). Examples include:
- the replacement of glycol ethers, chlorinated solvents and chlorofluorocarbon solvents as cleaning agents in microelectronics processing
- replacement of organic solvents by water-based solvents in adhesives and sealants
- reduction of volatile, organic solvents in many paints, in favour of water-based paints, spray-painting technology using supercritical carbon dioxide, and powder coatings
- replacement of cadmium and lead in pigments
- elimination of nitrous oxide air pollution in making adipic acid (used to make nylon, polyester and polyurethane)
- replacement of acrylamide in grouting compounds
- replacement of chlorine bleaching in making paper
- conversion of phosgene, arsine and other toxic gases to less toxic intermediates which can be handled instead in industrial processes, thus avoiding the need to store and transport large quantities of highly toxic, compressed gases
- replacement of the phosgene process for making polycarbonates with a dimethyl carbonate process
- synthesis of aliphatic isocyanates from amines and carbon dioxide instead of processes using phosgene
- replacement of hydrofluoric acid with sulphuric acid or, better still, with solid catalysts, in oil refinery gasoline alkylation units
- use of zeolite catalysts in cumene production, replacing phosphoric acid or aluminium chloride catalysts and eliminating problems of acid waste disposal and the handling of corrosive materials.
The worldwide promotion of less toxic technologies can be carried on both by individual MNCs and through collective bodies. The Industry Cooperative for Ozone Layer Protection is one vehicle major firms have used to promote environmentally superior technology. Through this organization, with additional support by the World Bank, IBM has tried to help companies in Asia and Latin America to switch to water-based cleaning and drying of circuit boards and disk components.
Roles of Government
Industrial expansion is taking place in many countries, and in considering applications for new industrial projects, governments have the opportunity and responsibility to evaluate health and safety hazards of the imported technology. The host country should seek to ensure that new operations will achieve high standards of performance. The project applicant should make the commitment to achieve specific levels of pollutant release that will not be exceeded during plant operations, and limits of worker exposure to toxic substances that will be attained. The applicant should be willing to pay for the government to obtain the necessary monitoring equipment to assure that these limits are observed in practice and to allow immediate access to government inspectors at any time.
Special attention should be directed towards having project applicants describe their past experience with the technology involved and its hazards. The host government has every reason and right to know what workplace hazards and pollution levels exist at similar factories operated by the project applicants. Similarly, it is important to know what laws, regulations and standards for public health protection are honoured by the applicants at similar facilities in other countries.
The host government application process should include critical evaluation from the standpoint, “Do we really need this?” And if the answer is yes, follow-up analysis should proceed along the lines of trying to ensure that the technology is designed to produce the least hazardous processes and products to provide whatever needs are served. This procedure comports with the stated policies of leading MNCs. The fulfilment of ethical duties by governments and corporations can best assure that public health related advances in technology are transmitted rapidly around the world.
Major new projects in developing countries usually involve participation of foreign investor MNCs. The accompanying guidelines (table 1) have been published by Greenpeace and Third World Network (Malaysia), detailing information that governments can request from foreign investors (Bruno 1994). To the extent that information on the technology and its hazards is not submitted by the prospective foreign investors, governments can and should take steps to obtain information on it independently.
Table 1. Information from foreign investors for environmental review
A. The foreign investor shall provide an Environmental Impact Analysis of the proposed project, including:
1. list of all raw materials, intermediates, products and wastes (with flow diagram)
2. list of all occupational health and safety standards and environment standards (wastewater effluent releases, atmospheric emission rates for all air pollutants, detailed description and rate of generation of solid wastes or other wastes to be disposed of on land or by incineration)
3. plan for control of all occupational health and safety hazards in plant operation, storage, and transport of potentially hazardous raw materials, products and wastes
4. copy of corporation guidelines of the foreign investor for conducting environmental and occupational health and safety impact analyses for new projects
5. manufacturer’s safety data sheets on all substances involved.
B. The foreign investor shall provide complete information on locations, ages and performance of existing plants and plants closed within the past five years in which the foreign investor has partial or full ownership, where similar processes and products are used, including:
1. list of all applicable occupational health and safety standards and environmental standards, including both legal requirements (standards, laws, regulations) and corporate voluntary standards and practices for the control of occupational and environmental hazards of all kinds
2. description of all cases of permanent and/or total disability sustained or allegedly sustained by workers, including workers’ compensation claims
3. explanation of all fines, penalties, citations, violations, regulatory agreements, and civil damage claims involving environmental and occupational health and safety matters as well as hazards from or harm attributed to the marketing and transport of the products of such enterprises
4. description of the foreign investor’s percentage of ownership and technology involvement in each plant location and similar information for other equity partners and providers of technology
5. names and addresses of governmental authorities who regulate or oversee environmental and occupational health and safety for each plant location
6. explanation of cases where any plant’s environmental impact has been the subject of controversy within the local community or with regulatory authorities, including description of the practices criticized and how criticism was resolved in each case
7. copies, with summary, of all corporate occupational health and safety and environmental audits and inspection reports for each location, including such audits and reports by consultants
8. copies of safety reports, reports of hazard assessment, and risk analysis reports carried out with similar technology by the foreign investor and its consultants
9. copies of toxic release forms that have been submitted to governmental bodies (e.g., the US Environmental Protection Agency or similar agencies in other countries) within the past five years, for all plant locations
10.any information considered relevant by the foreign investor.
C. The foreign investor shall submit a statement of corporate policy on health, safety, and environmental performance of worldwide operations. This must include the corporate policy on laws, regulations, standards, guidelines, and practices for new industrial projects and production facilities. The foreign investor shall explain how its global policy is implemented by: describing the staff responsible for carrying out this policy, its authority and responsibilities, and its position in the foreign investor corporate structure. Such descriptions will also include the name, address, and telephone number of senior corporate management officials in charge of this staff function. The foreign investor shall state whether it follows the same standards worldwide for worker and environmental protection in all new projects; and if not, explain why not.
D. The foreign investor shall agree to provide the developing country immediate access to the proposed industrial facility at any time during its operation to conduct inspections, monitor exposure of workers to hazards, and sample for pollution releases.
E. The foreign investor shall agree to fully train all employees exposed to potential occupational hazards, including training on potential health effects of all exposures and the most effective control measures.
F. The foreign investor shall agree to provide the developing country with equipment to analyze workplace exposures and pollutant generation, including but not limited to all limits specified in A(2) above, for the lifetime of the proposed project. The foreign investor shall agree that the proposed project will pay the cost to the developing country government for all medical and exposure monitoring during the lifetime of the proposed project.
G. The foreign investor shall agree that the proposed project will fully compensate any person whose health, earning capacity, or property is harmed as a result of the project’s occupational hazards and environmental impacts, as determined by the government of the developing country.
H. The foreign investor shall follow marketing safeguards as restrictive as those it applies anywhere in the world, to assure that workers and members of the public are not harmed as a result of the use of its products.
I. If the foreign investor becomes aware of a substantial risk of injury to health or the environment from a substance it manufactures or sells in the developing country, a risk not known and disclosed at the time of this application, the foreign investor agrees to notify the environmental protection agency of the government of the developing country immediately of such risk. (This is similar to requirements under section 8e of the Toxic Substances Control Act of the USA.)
J. The foreign investor shall provide the names, titles, addresses, phone, and fax numbers of its senior corporate officials charged with implementing environmental and occupational and safety and health policies including plant design and operations, corporate inspections and reviews of plant performance, and product stewardship.
Source: Bruno 1994.
Industrial hazards are not the only reason countries have for wanting to do environmental impact reviews, and industrial projects are not the only ones warranting such scrutiny. The importation and widespread use of energy-inefficient technology for manufacture of refrigerators, electric motors and lighting has caused significant problems. In many countries, electrical power generation could hardly keep up with demand even if energy efficiency were a criterion in the evaluation of new technology and the design of commercial buildings. Energy inefficiency poses major problems in development, including the cost of building and operating excessive power generation capacity, pollution and the disincentives to expansion caused by unreliable power supplies and breakdowns. Energy efficiency could free tremendous resources for meeting basic needs instead of building and operating unneeded power plants.
Conclusion
Multinational corporations are in the most powerful position to determine what types of technology will be transferred to countries in Asia, Africa, Latin America and Eastern and Central Europe. The big companies have an ethical and moral obligation to promptly implement global policies to eliminate double standards with respect to public health and the environment. The lives of present and future generations will be vitally affected by the rate of transfer of improved, less hazardous technologies throughout the world.
Governments, further, have the ethical duty to independently and critically screen industrial and commercial projects. This role is best fulfilled by conducting searching analyses of the technologies and companies involved. The credibility and effectiveness of the screening process will depend greatly upon the transparency of the process and public participation in it.
Quotations from corporate sources are based on reports published in chemical trade journals and communications to the author
Free-Trade Agreements
Economists have long viewed free trade as an ideal. In 1821 economist David Ricardo argued that each country should export those commodities it could produce with comparative advantage. Although Ricardo considered only a single factor of production, labour, later theorists of relative factor proportions extended this framework to capital, natural resources and other factors. Most modern economists believe that restrictions on trade—protective tariffs, export subsidies and import quotas—create economic inefficiencies, distorting the incentives of both producers and consumers and costing nations money. They argue that in restricted national markets small firms proliferate to serve small markets, violating economies of scale, and that incentives for producers to innovate and compete are blunted. Free-trade advocates believe that arguments for trade restrictions, while often based on “the national interest”, are usually disguised claims on behalf of special interests.
However, there are several economic arguments against free trade. One is based on domestic market failures. If a domestic market such as the labour market does not function properly, then deviation from free trade may help to restore that market or may yield compensatory gains in other parts of the domestic economy. A second argument is that a fundamental assumption of free-trade theory, immobility of capital, is no longer correct, so free trade may disadvantage some countries. Daly and Cobb (1994) write:
The free flow of capital and goods (instead of goods only) means that investment is governed by absolute profitability and not by comparative advantage. The absence of a free flow of labour means that opportunities for employment decline for workers in the country in which investments are not being made. This represents a more nearly accurate account of the world in which we live than does the principle of comparative advantage, however applicable that may have been in Ricardo’s day.
Within a free-trade area, the prices of goods that are traded tend to equalize. According to the factor price equalization theorem, this is also true of factors of production, including wages, costs of regulatory compliance, and perhaps externalized factors such as air pollution. That leads to a third argument against free trade: it may exert downward pressure on wages, on health, safety, and environmental practices, and on other factors of production, towards the lowest levels of any of the trading countries. This raises serious occupational health and safety concerns.
Since the Second World War, industry has become increasingly international. Communications and transportation have advanced rapidly. Information and capital are increasingly mobile. Multinational firms have become an ever more prominent part of the world economy. In the process, production patterns change, plants relocate, and employment is destabilized. Unlike capital, labour is relatively immobile, both geographically and in terms of skills. Industrial relocation has therefore placed considerable strains on workers.
Against this background free trade has steadily increased. Eight rounds of multilateral trade negotiations have taken place since 1947 under the General Agreement on Tariffs and Trade (GATT). The most recent, the Uruguay Round, concluded in 1994 with the formation of the World Trade Organization (WTO). GATT (and now WTO) member nations agree to three general principles: they refrain from export subsidies (except in agriculture); they refrain from unilateral import quotas (except when imports threaten “market disruption”); and any new or increased tariffs must be offset by reductions in other tariffs to compensate trading partners. The WTO does not eliminate tariffs but it limits and regulates them. Over 130 nations, many of them developing or “transition” nations, are WTO members. Total membership is expected to exceed 150.
Since the 1980s further moves towards free trade have occurred on a regional level, through preferential trading agreements. Under these agreements, countries agree to eliminate tariffs on trade with each other while continuing to maintain tariff barriers against the rest of the world. These agreements are known as customs unions, common markets or free-trade areas; examples include the European Union and the three nations of North America. More loosely knit economic alliances, such as the Asian Pacific Economic Cooperation (APEC), the Association of South-East Asian Nations (ASEAN) and the Mercado Común del Sur (MERCOSUR), also promote trade among their members.
Job Health and Safety in Free-Trade Agreements
Free-trade agreements are designed to promote trade and economic development and most address social issues such as worker health and safety only indirectly, if at all. However, a wide range of issues affecting job health and safety may arise in the context of free-trade agreements.
Worker dislocation, unemployment and migration
Free-trade agreements occur in the context of larger economic and social trends, and may in turn influence these trends. Consider free trade between two countries with different levels of development, different wage scales and different employment opportunities. In this situation industries may relocate, displacing workers from their jobs and creating unemployment in the country of origin. The newly unemployed workers may then migrate to areas of greater employment opportunity, especially if, as in Europe, barriers to emigration have also been lifted.
Unemployment, fear of unemployment, migration and the accompanying stress and social disruption have a profound impact on the health of workers and their families. Some governments have attempted to mitigate these effects with social programmes, including job retraining, relocation assistance and similar supports, with mixed success.
Job health and safety standards
The member countries of a free-trade agreement may differ in their job health and safety standards. This implies lower production costs for the countries with less stringent standards, an important trade advantage. One likely result is political pressure within more protective countries to lower their standards, and within less protective countries not to advance their standards, in order to preserve trade advantages. Advocates of occupational health and safety cite this scenario as one of the major adverse consequences of free trade.
Another likely result is also worrisome. A country may decide to block the importation of certain hazardous materials or equipment to advance its occupational health agenda. Its trading partners may charge it with unfair trade practices, viewing this policy as a disguised trade barrier. In 1989, under the US-Canada Free Trade Agreement, Canada accused the United States of unfair trading when the United States moved to phase out asbestos imports. Such disputes can undermine the health and safety standards of a country with more stringent standards.
On the other hand, free trade may also provide an opportunity to improve standards through collaborative standard-setting, sharing of the technical information on which standards are based and harmonization of disparate standards up to high levels. This is true of both occupational health and safety standards and related labour standards such as child labour laws, minimum-wage requirements and collective-bargaining regulations. A major obstacle to harmonization has been the issue of national sovereignty; some countries have been reluctant to negotiate away any control over their labour standards.
Enforcement practices
Identical concerns arise with regard to enforcement of regulations that are on the books. Even if two trading partners have comparable occupational health and safety standards, one may enforce them less scrupulously than the other, lowering production costs and gaining a competitive advantage. Remedies include a dispute resolution process to allow countries to appeal an alleged unfair trade practice, and collaborative efforts to harmonize enforcement practices.
Hazard communication
Hazard communication refers to a wide range of practices: worker training, provision of written materials on hazards and protective measures, container labelling and worker access to medical and exposure records. These practices are widely recognized as key components of successful occupational health and safety programmes. Free trade and international commerce more generally have an impact on hazard communication in at least two ways.
First, if hazardous chemicals or processes are transported across national borders, workers in the receiving country may be placed at risk. The receiving country may lack the capacity for appropriate hazard communication. Information sheets, training materials and warning labels need to be provided in the language of the receiving country, at a reading level appropriate for the exposed workers, as part of the import-export process.
Second, inconsistent requirements for hazard communication place a burden on companies that operate in more than one country. Uniform requirements, such as a single format for chemical information sheets, help address this problem, and may be encouraged in the context of free trade.
Training and human resource development
When trading partners differ in their levels of economic development, they are likely also to differ in their human resources. Less affluent nations face shortages of industrial hygienists, safety engineers, occupational physicians and nurses, trained labour educators and other key professionals. Even when two nations have comparable levels of development, they may differ in their technical approaches to occupational health and safety. Free-trade agreements provide an opportunity to reconcile these disparities. Through parallel structures the occupational health and safety professionals from trading nations can meet, compare their practices, and agree on common procedures when appropriate. Similarly, when a country has a shortage of certain professionals relative to one or more of its trading partners, they can cooperate in offering formal training, short courses and other means of human resource development. Such efforts are a necessary part of harmonizing occupational health practice effectively.
Data collection
An important aspect of coordinated efforts to protect worker health and safety is data collection. Under a free-trade agreement several kinds of data collection may bear on worker health and safety. First, information on each country’s occupational health practices, particularly its means of implementing workplace standards, is necessary. Such information helps monitor progress towards harmonization and can disclose violations that may constitute unfair trade practices. Data on workplace exposures must be collected, not only for these reasons but also as part of routine occupational health practice. Exposure data must be collected according to good industrial hygiene practice; if member countries use consistent measurement procedures then comparisons among them are possible. Similarly, morbidity and mortality data are essential as part of good occupational health and safety programmes. If the countries of a free-trade agreement use consistent methods of collecting this information, then they can compare their health effects, identify problem areas and target interventions. This may be difficult to achieve since many countries collect their health and safety data from workers’ compensation statistics, and compensation schemes vary widely.
Prevention
Finally, free trade provides an opportunity for harmonization of preventive approaches, technical assistance among member nations and sharing of solutions. This may occur in the private sector when a company operates in several countries and can implement a preventive practice or technology across borders. Companies that specialize in occupational health services may themselves function internationally, spurred by a free-trade agreement, and function to diffuse preventive practices among member countries. National labour unions in a free-trade agreement may also collaborate. For example, the European Trade Union Technical Bureau for Health and Safety in Brussels was created by the European Parliament with the support of key unions. Such efforts can push member countries towards upward harmonization of preventive activities. Harmonization of preventive approaches may also occur at the governmental level, through collaboration in technology development, training and other activities. Ultimately, the most positive effect of free trade on occupational health and safety is improved prevention in each of the member countries.
Conclusion
Free-trade agreements are primarily designed to lower trade barriers and most do not directly address social issues such as worker health and safety (see also "Case Study: World Trade Organization"). In Europe, free trade developed over several decades in a process that embraced social concerns to an unusual extent. The organizations in Europe responsible for occupational health and safety are well funded, include representation from all sectors, and can pass directives that are binding on member countries; this is clearly the most advanced of the world’s free-trade agreements with respect to worker health. In North America, NAFTA includes a detailed dispute resolution process that extends to occupational health and safety, but few other initiatives to improve working conditions in the three member countries. Other regional trade pacts have not incorporated occupational health and safety initiatives.
Economic integration of the world’s nations is moving forward, due to rapid advances in communications, transportation and capital investment strategies. Free-trade agreements govern some but not all of this increased trade among nations. The changes in commercial patterns and the expansion of international trade have major implications for worker health and safety. It is essential to link trade issues with occupational health and safety issues, using free-trade agreements and other means, to ensure that advances in commerce are accompanied by advances in worker protection.
Transfer of Technology and Technological Choice
The Recent Period of Rapid Transition
The migration of industry from developed to developing countries is usually explained by the lower cost of labour. Companies also establish operations abroad to reduce transportation costs by producing within foreign markets, to overcome trade barriers and to avoid fluctuations in currency markets. But some companies migrate to developing nations to escape occupational and environmental regulations and enforcement at home. For many nations such investment is the primary source of new jobs.
Foreign companies and investors have been responsible for more than 60% of all industrial investment in developing countries over the past decade. During the 1980s, a global financial market began to emerge. In a span of ten years, international bank lending by the major developed countries rose from 4% of GDP to 44%. Between 1986 and 1990, foreign investment by the United States, Japan, West Germany, France and Britain grew at an annual rate of 27%. Global cross-border investment is now estimated to be $1,700 billion (LaDou and Levy 1995). There are about 35,000 transnational corporations, with 147,000 foreign affiliates. Much of the investment in the developing world comes from these corporations. The total annual sales of the 350 biggest transnational corporations are equal to one-third of the combined gross domestic products of the industrial world and exceed by far that of the developing world.
Most investment in developing countries goes to Asia. Between 1986 and 1990, East and Southeast Asia received $14 billion, Latin America $9 billion and Africa $3 billion. Central Europe is now openly competing for a share of global investment. India, Vietnam, Egypt, Nicaragua and Uzbekistan have recently liberalized their ownership rules to increase their attractiveness to investors.
Japanese companies and investments are found in almost every country in the world. With limited land and great population density, Japan has a pressing need to export its waste-producing industries. European nations have exported hazardous and environmentally outmoded industries to Africa and the Middle East and are now beginning to export them to Central Europe. Western European corporations are the largest investors in Bangladesh, India, Pakistan, Singapore and Sri Lanka.
China and India, with the world’s largest populations, have had dramatic policy reversals in recent years and as a result have welcomed industries from many countries. United States corporations are dominant in China, Indonesia, the Philippines, Thailand and Hong Kong and Taiwan (China). US companies were expected to commit $l billion of investment to Singapore in 1995, up 31% from 1994.
The Industrialized Countries’ Motivation
In the developed countries, industry provides jobs, pays taxes that support community services and is subject to environmental and occupational health laws. As industrialized nations enact laws to limit the environmental hazards associated with many industrial operations, production costs rise and undermine competitive advantages. To offset this problem, manufacturers move many of their hazardous operations to the newly industrialized countries. They are welcomed because the creation of an infrastructure in many developing nations relies on industrial expansion by foreigners.
When industry migrates to developing nations, companies not only take advantage of lower wages, but also benefit from the low tax rates in communities that are not spending much on such things as sewage systems, water treatment plants, schools and public transportation. When companies establish plants in developing countries, their tax burden is a small fraction of what it would be in most developed countries.
Anecdotal evidence in support of the transition
The University of California, the Johns Hopkins University and the University of Massachusetts have all recently studied the health of American semiconductor workers. The studies demonstrate that women have a major increase in the risk of miscarriage when they work in semiconductor plants. Researchers participating in these studies remark that the companies are laying off the workers and shutting down the plants so rapidly that these studies will probably be the last of sufficient size to give reliability to the findings to be conducted with US workers.
Predictions for a reduction in studies on occupational health
The migration of American and Japanese semiconductor companies to Southeast Asia is dramatically demonstrated in the newly industrialized country of Malaysia. Since the mid-1970s, Malaysia has become the world’s third largest semiconductor manufacturer and the world’s largest exporter of semiconductors. It is very unlikely that foreign companies will continue to fund research on occupational and environmental health in a distant country with foreign workers. The savings realized by the foreign manufacture of semiconductors will be enhanced by the ability of these companies to neglect health and safety as do their international rivals. The miscarriage rate of semiconductor workers will be ignored by governments and by industry in newly industrialized countries. Workers, for the most part, will not recognize the association between work and miscarriage.
The Developing Countries’ Environmental and Occupational Health Decline
Developing countries seldom have enforceable occupational and environmental regulations. They are concerned with overwhelming problems of unemployment, malnutrition and infectious diseases, often to the exclusion of environmental hazards. Newly industrialized countries are eager for the financial benefits that foreign companies and foreign investors bring them. But with those benefits come social and ecological problems.
The positive economic and social results of industrial activity in developing nations are accompanied by serious environmental degradation. The major cities of developing nations are now reeling with the impact of air pollution, the absence of sewage treatment and water purification, the growing quantities of hazardous waste buried in or left on the soil or dumped into rivers or the oceans. In many of the world’s countries, there are no environmental regulations or, if they exist at all, there is little or no enforcement.
The workforce of developing nations is accustomed to working in small industry settings. Generally, the smaller the industry, the higher the rate of workplace injury and illness. These workplaces are characterized by unsafe buildings and other structures, old machinery, poor ventilation, and noise, as well as with workers of limited education, skill and training and employers with limited financial resources. Protective clothing, respirators, gloves, hearing protectors and safety glasses are seldom available. The companies are often inaccessible to inspections by government health and safety enforcement agencies. In many instances, they operate as an “underground industry” of companies not even registered with the government for tax purposes.
The common public perception of off-shore industries is that of the major multinationals. Far more common than these industrial giants are the many thousands of small companies owned by foreign interests and operated or supervised by local managers. The ability of most foreign governments to regulate industry or even to monitor the passage of goods and materials is extremely limited. Migrating industries generally conform to the environmental and occupational health and safety standards of the host country. Consequently, worker fatality rates are much higher in newly industrialized countries than in the developed nations, and workplace injuries occur with rates common to the developed nations during the early years of the Industrial Revolution. In this regard, the Industrial Revolution is taking place all over again, but with much larger populations of workers and in many more countries.
Virtually all of the world’s population growth is occurring in the developing world. At present, the labour force in developing countries totals around 1.76 billion, but it will rise to more than 3.1 billion in 2025— implying a need for 38 to 40 million new jobs every year (Kennedy 1993). This being the case, worker demands for better working conditions are not likely to occur.
Migration of Occupational Illness and Injury to the Developing World
The incidence of occupational diseases has never been greater than it is today. The United Nations estimates that 6 million occupational disease cases occur each year worldwide. Occupational diseases occur with greater frequency per exposed worker in the developing countries, and, of even greater significance, they occur with greater severity. Among miners, construction and asbestos workers in some developing countries, asbestos is the major cause of disability and ill health and, by some counts, the major cause of deaths. The occupational and environmental hazards posed by asbestos products do not discourage the asbestos industry from promoting asbestos in the developing world, where demand for low-cost building materials outweighs health concerns.
Lead smelting and refining is migrating from developed countries to developing countries. Recycling of lead products also passes from developed countries to poorer nations that are often ill-prepared to deal with the occupational and environmental hazards created by lead. Developed nations have few lead smelters today, this industrial activity having been passed to the newly industrialized countries. Many lead-smelting activities in the developing world operate with technologies that are unchanged from a century ago. When developed countries boast of accomplishments in the area of lead recycling, almost invariably the lead is recycled in developing countries and returned to the developed countries as finished products.
In developing countries, governments and industries accept the hazardous materials knowing that reasonable exposure levels are not likely to be legislated or enforced. Leaded gasoline, paints, inks and dyes, batteries and many other lead-containing products are produced in developing countries by companies that are usually foreign-owned and the products are then sold internationally by the controlling interests.
In developing countries, where the majority of workers are in agriculture, pesticides are often applied by hand. Three million pesticide poisonings occur each year in Southeast Asia (Jeyaratnam 1992). Most pesticide manufacture in developing countries is done by foreign-owned companies or local companies with capital invested by foreigners. The use of pesticides in the developing countries is growing rapidly as they learn the advantages that such chemicals offer to the agricultural industry and as they gain the capability to produce the pesticides in their own countries. Pesticides such as DDT and dibromochloropropane (DBCP), which are banned in most developed nations, are widely sold and used without restrictions in the developing world. When health hazards cause removal of a pesticide from a developed country’s market, it often finds its way to the unregulated markets in developing countries.
The chemical industry is one of the most rapidly growing industrial sectors in the emerging global economy. The chemical companies of the developed countries are found throughout the world. Many smaller chemical companies migrate to the developing countries, making the chemical industry a major contributor to environmental contamination. As population growth and industrialization continue throughout the poorer regions of the world, demand for pesticides, chemical fertilizers and industrial chemicals grows as well. To compound this problem, chemicals that are banned in developed countries are often manufactured in increased quantities in the newly industrialized countries. DDT is a compelling example. Its worldwide production is at record levels, yet it has been illegal to produce or use DDT in most developed countries since the 1970s.
Costs Shifting to Developing World
The experience of industrialized countries with the costs of occupational safety and environmental programmes is that a very substantial financial burden is being shifted to newly-industrialized nations. The cost of future accidents such as Bhopal, mitigation of environmental damage and effects on the public health are not often discussed with candour in the developing world. The consequences of global industry may become the roots of widespread international conflicts when the long-term economic realities of industrial migration become more apparent.
The Developing Nation Conundrum
Developing nations seldom support the adoption of the environmental standards of the developed world. In some instances, opponents argue that it is a matter of national sovereignty that allows each nation to develop its own standards. In other cases, there is long-standing resentment of any foreign influence, especially from the nations that have already increased their standard of living from the industrial activities that are now being regulated. Developing nations take the position that after they have the standard of living of the developed nations, they will then adopt stricter regulatory policies. When developed nations are asked to provide developing nations with industries whose technology is environmentally benign, interest in industrial migration lessens dramatically.
The Need for International Intervention
International organizations must take a stronger lead in approving and coordinating technology transfer. The shameful practice of exporting obsolete and hazardous technologies to developing countries when these processes can no longer satisfy the environmental standards of the developed countries must be stopped. International agreements must replace the perverse incentives that threaten the world’s environment.
There have been many efforts to control the behaviour of industry. The Organization for Economic Cooperation and Development (OECD) Guidelines for Multinational Enterprises, the United Nations (UN) Code of Conduct on Transnational Corporations and the International Labour Organization (ILO) Tripartite Declaration of Principles Concerning Multinational Enterprises and Social Policy attempt to provide a framework of ethical behaviour. The Basel Convention on the Control of Transboundary Movements of Hazardous Wastes and Their Disposal was adopted in March 1994. Although it halts most hazardous wastes from crossing borders, it also serves to institutionalize a trade in recyclable wastes that reflected the need for political compromise.
Some international lending institutions are now producing environmental impact assessments (EIAs) when the host country is unable to perform this task. Assessment of the local impact potential of at least certain hazardous industry sitings ought to be mandatory and occupational health and safety standards could be added to plant siting assessments.
The International Organization for Standardization (ISO) has undertaken the development of voluntary standards, the ISO 14000 series that are likely to become the international standard for environmental management. These encompass environmental management systems, environmental audits, eco-labelling, environmental performance evaluations, life-cycle assessment and environmental aspects in product standards (Casto and Ellison, 1996).
Many developed nations have established recommended exposure levels for workers that cannot be exceeded without regulatory or legal action. But in developing countries, exposure standards are often non-existent, not enforced, or too lax to be of use. International standards can and should be developed. Developing countries, and particularly the foreign companies that manufacture there, can be given a reasonable period of time to comply with the standards that are enforced throughout most of the developed world. If this is not done, some workers in these countries will pay an inordinate part of the cost of industrialization.
Conclusions
The most logical international standard of occupational health and safety is the development of an international workers’ compensation insurance system. Workers in all countries are entitled to the basic benefits of workers’ compensation law. The incentive for employers to provide a healthy and safe work setting that workers’ compensation insurance provides for should be such as to benefit workers in all countries, regardless of the ownership of the company.
There must be an international legal system to deal with the environment and there must be an enforcement capability strong enough to discourage even the most criminal of polluters. In 1972, the member countries of OECD agreed to base their environmental policies on a “polluter pays” principle (OECD 1987). The intent was to encourage industries to internalize environmental costs and reflect them in the prices of products. Expanding on the principle, strict liability provision in the laws of all countries could be developed for both property and third-party damage. Thus, the waste generator would be responsible through an international system of strict liability for management of waste from its production to its disposal.
Developing countries do not have large, well-funded environmental groups such as those that exist in developed countries. Enforcement will require the training of personnel and the support of governments which, until recently, placed so much emphasis on industrial expansion that the issue of environmental protection was not even a consideration.
Small Enterprises and Occupational Health and Safety
Small workplaces have been a characteristic mode of production since earliest times. Cottage industries where members of a family work on the basis of a division of labour still exist in both urban and rural situations to this day. In fact, it is true of all countries that the majority of workers, paid or unpaid, work in enterprises which can be classified as small.
Before defining their health problems, it is necessary to define a small enterprise. It is generally recognized that a small enterprise is one employing 50 or fewer workers. It may be located in the home, a farm, a small office, a factory, mine or quarry, a forestry operation, a garden or a fishing boat. The definition is based on the number of workers, not what they do or whether they are paid or unpaid. The home is clearly a small enterprise.
Common Features of Small Enterprises
Common features of small enterprises include (see table 1):
- They are likely to be undercapitalized.
- They are usually non-unionized (the home and the farm in particular) or under-unionized (office, factory, food shop, etc.).
- They are less likely to be inspected by government agencies. In fact, a study carried out some years ago indicated that the existence of many small enterprises was not even known to the government department responsible for them (Department of Community Health 1980).
Table 1. Features of small-scale enterprises and their consequences
Lack of capital
- poor environmental conditions
- cheaper raw materials
- inferior equipment maintenance
- inadequate personal protection
Non- or under-unionization
- inferior pay rates
- longer working hours
- non-compliance with award conditions
- exploitation of child labour
Inferior inspection services
- poor environmental conditions
- greater hazard level
- higher injury/illness rates
As a result, workplace environmental conditions, which generally reflect available capital, are inevitably inferior to those in larger enterprises: cheaper raw materials will be purchased, maintenance of machinery will be reduced and personal protective equipment will be less available.
Under- or non-unionization will lead to inferior pay rates, longer working hours and non-compliance with award conditions. Work will often be more intensive and children and old people are more likely to be exploited.
Inferior inspection services will result in poorer working environments, more workplace hazards and higher injury and illness rates.
These characteristics of small enterprises place them at the edge of economic survival. They come into and go out of existence on a regular basis.
To balance these significant disadvantages, small enterprises are flexible in their productive systems. They can respond quickly to change and often develop imaginative and flexible solutions to the requirements of technical challenge. At a social level, the owner is usually a working manager and interacts with the workers on a more personal level.
There is evidence to support these beliefs. For example, one US study found that the workers in neighbourhood panel beating shops were regularly exposed to solvents, metal pigments, paints, polyester plastic fumes and dust, noise and vibration (Jaycock and Levin 1984). Another US survey showed that multiple short-term exposures to chemical substances were characteristic of small industries (Kendrick, Discher and Holaday 1968).
A Finnish study investigating this occurrence in 100 workplaces found that short-duration exposures to chemicals were typical in small industry and that the duration of exposure increased as the firm grew (Vihina and Nurminen 1983). Associated with this pattern were multiple exposures to different chemicals and frequent exposures to peak levels. This study concluded that chemical exposure in small enterprises is complex in character.
Perhaps the most dramatic illustration of the impact of size on occupational health risk was presented at the Second International Workshop on Benzene in Vienna, 1980. For most of the delegates from the petroleum industry, benzene posed little health risk in the workplace; their workplaces employed sophisticated medical, hygiene and engineering techniques to monitor and eliminate any potential exposure. In contrast, a delegate from Turkey when commenting on the boot-making industry, which to a large extent was a cottage industry carried out in the home, reported that men, women and children were exposed to high concentrations of “an unlabelled solvent”, benzene, which resulted in the occurrence of anaemias and leukaemias (Aksoy et al. 1974). The difference in exposure in the two situations was a direct consequence of workplace size and the more intimate contact of the workers in the cottage-style, boot-making industry, compared with the large-scale petroleum enterprises.
Two Canadian researchers have identified the main difficulties faced by small businesses as: a lack of awareness of health hazards by managers; the higher cost per worker to reduce these hazards; and an unstable competitive climate which makes it unlikely that such businesses can afford to implement the safety standards and regulations (Lees and Zajac 1981).
Thus, much of the experience and recorded evidence indicate that the workers in small enterprises constitute an under-served population from the standpoint of their health and safety. Rantanan (1993) attempted a critical review of available sources for the WHO Interregional Task Group on Health Protection and Health Promotion of Workers in Small Scale Industries, and found that reliable quantitative data on illnesses and injuries to workers in small-scale industries are unfortunately sparse.
In spite of the lack of reliable quantitative data, experience has demonstrated that the characteristics of small-scale industries result in a greater likelihood of musculoskeletal injuries, lacerations, burns, puncture wounds, amputations and fractures, poisonings from inhalation of solvents and other chemicals and, in the rural sector, pesticide poisonings.
Serving the Health Needs of Workers in Small-Scale Enterprises
The difficulty in serving the health and safety needs of workers in small enterprises stems from a number of features:
- Rural enterprises are often isolated as a result of being located at a distance from main centres with bad roads and poor communications.
- Workers on small fishing vessels or in forestry operations also have limited access to health and safety services.
- The home, where most cottage industry and unpaid “housework” is located, is frequently ignored in health and safety legislation.
- Educational levels of workers in small-scale industries are likely to be lower as a result of leaving school earlier or the lack of access to schools. This is accentuated by the employment of children and migrant workers (legal and illegal) who have cultural and language difficulties.
- Although it is clear that small-scale enterprises contribute significantly to the gross domestic product, the fragility of the economies in developing countries makes it difficult to provide funds to serve the health and safety needs of their workers.
- The great number and variability of small-scale enterprises make it difficult to effectively organize health and safety services for them.
In summary, workers in small-scale enterprises have certain characteristics which make them vulnerable to health problems and make it difficult to provide them with health care. These include:
- Inaccessibility to available health services for geographic or economic reasons and a willingness to tolerate unsafe and unhealthy conditions of work, primarily because of poverty or ignorance.
- Deprivation because of poor education, housing, transport and recreation.
- An inability to influence policy making.
What are the Solutions?
These exist at several levels: international, national, regional, local and workplace. They involve policy, education, practice and funding.
A conceptual approach was developed at the Colombo meeting (Colombo Statement 1986), although this looked particularly at developing countries. A restatement of these principles as applicable to small-scale industry, wherever it is located, follows:
- National policies need to be formulated to improve health and safety of all workers in small-scale industries with special emphasis on education and training of managers, supervisors and workers and the means of ensuring that they receive adequate information to protect the health and safety of all workers.
- Occupational health services for small-scale industries need to be integrated with the existing health systems providing primary health care.
- Adequate training for occupational health personnel is needed. This should be tailored to the type of work carried out, and would include training for primary health care workers and specialists as well as the public health inspectors and nurses mentioned above.
- Adequate communication systems are needed to ensure the free flow of occupational health and safety information among workers, management and occupational health personnel at all levels.
- Occupational health care for small isolated groups through primary health care workers (PHCWs) or their equivalent should be provided. In rural areas, such a person is likely to be providing general health care on a part-time basis and an occupational health content can be added. In small urban workplaces, such a situation is less likely. Persons from the workforce selected by their fellow workers will be needed.
- These rural and urban PHCWs, who will require initial and ongoing training and supervision, need to be linked to the existing health services. The “link health worker” should be an appropriate full-time health professional with at least three years of training. This health professional is the crucial link in the effective functioning of the service. (See figure 1.)
- Occupational hygiene which measures, evaluates and controls environmental hazards, is an essential part of occupational health care. Appropriate occupational hygiene services and skills should be introduced into the service both centrally and peripherally.
Figure 1. Patterns of health care for workers in small plants
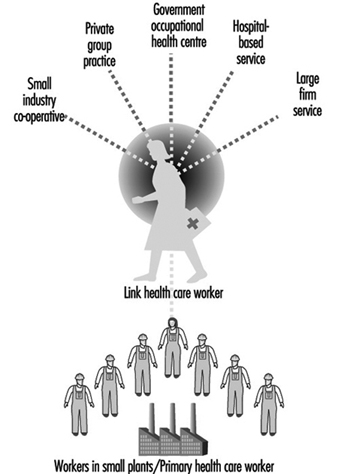
Despite the establishment of these principles, very little progress has been made, almost certainly because small workplaces and the workers who work in them are given a low priority in the health service planning of most countries. Reasons for this include:
- lack of political pressure by such workers
- difficulty in servicing the health needs because of such features as isolation, educational levels and innate traditionalism, already mentioned
- the lack of an effective primary health care system.
Approaches to the solution of this problem are international, national and local.
International
A troublesome feature of the global economy is the negative aspects associated with the transfer of technology and the hazardous processes associated with it from developed to developing countries. A second concern is “social dumping”, in which, in order to compete in the global marketplace, wages are lowered, safety standards ignored, hours of work extended, age of employment is lowered and a form of modern-day slavery is instituted. It is urgent that new ILO and WHO instruments (Conventions and Recommendations) banning these practices be developed.
National
All-embracing occupational safety and health legislation is needed, backed up by a will to implement and enforce it. This legislation needs to be supported by positive and widespread health promotion.
Local
There are a number of organizational models for occupational health and safety services which have been successful and which, with appropriate modifications, can accommodate most local situations. They include:
- An occupational health centre can be established in localities where there is a dense population of small workplaces, to provide both accident and emergency treatment as well as education and intervention functions. Such centres are usually supported by government funding, but they may also be funded through a sharing of costs by a number of local small industries, usually on a per-employee basis.
- A big company’s occupational health service may be extended to surrounding small industries.
- A hospital-based occupational health service which already covers accident and emergency services can supplement this with a visiting primary health care service concentrating on education and intervention.
- A service can be provided where a general practitioner provides treatment services in a clinic but uses a visiting occupational health nurse to offer education and intervention in the workplace.
- A specialist occupational health service staffed by a multidisciplinary team comprising occupational physicians, general practitioners, occupational health nurses, physiotherapists and specialists in radiography, pathology and so on, may be established.
- Whatever the model employed, the service must be linked to the workplace by a “link health care worker”, a trained health professional multiskilled in both the clinical and hygiene aspects of the workplace. (See figure 1)
Regardless of the organizational form utilized, the essential functions should include (Glass 1982):
- a centre for training first-aiders among the workers in surrounding small industries
- a centre for the treatment of minor injuries and other work-related health problems
- a centre for the provision of basic biological monitoring including screening examinations of hearing, lung function, vision, blood pressure and so on, as well as the earliest signs of the toxic effects of exposure to occupational hazards
- a centre for the provision of basic environmental investigations to be integrated with the biological monitoring
- a centre for the provision of health and safety education that is directed by or at least coordinated by safety consultants familiar with the kinds of workplaces being served
- a centre from which rehabilitation programmes could be planned, provided and coordinated with return to work.
Conclusion
Small enterprises are a widespread, fundamental and essential form of production. Yet, the workers who work in them frequently lack coverage by health and safety legislation and regulation, and lack adequate occupational health and safety services. Consequently, reflecting the unique characteristics of small enterprises, workers in them have greater exposures to work hazards.
Current trends in the global economy are increasing the extent and the degree of exploitation of workers in small workplaces and, thereby, increasing the risk of exposure to hazardous chemicals. Appropriate international, national and local measures have been designed to diminish such risks and enhance the health and well-being of those working in small-scale enterprises.
Case Studies in Technological Change
Changes in plant technologies production pressures and the need for continually training workers are essential to the safe and healthful environment. The following three examples occurred in the United States. Technological change affects all workers around the world.
Production versus Safety
Production pressures can severely compromise safety and health unless management is careful to analyse the potential consequences of decisions designed to increase productivity. One example comes from a 1994 accident in a small steel plant in the United States.
At about 4:00 a.m. several workers were preparing to tap molten steel from an electric arc furnace. The steel market was good and the enterprise was selling all the steel it could produce. Workers were on heavy overtime schedules and the plant was working at full capacity. The furnace had been scheduled for a shutdown in order to replace its refractory lining, which had worn dangerously thin. Hot spots had already developed in the furnace shell, but the company wanted a couple of final batches of steel.
As the tap began, the lining of the vessel burned through. Steel and slag poured from the break and quickly melted through a water line supplying the cooling system for the furnace. The water exploded into steam with tremendous force. Two workers were in the path. Both were severely burned. One of them died three days later.
One obvious cause of the accident was operating the furnace beyond the safe life of its refractory lining. In addition, electric furnaces are generally designed to keep the main cooling water lines above the height of the molten steel and slag at all times, in order to prevent exactly this kind of accident. However, this furnace had been modified in the recent past to increase its capacity by raising the level of the molten material, and the engineers overlooked the water line. A simple breakout of molten metal and slag would have been serious, but without the water line it would not have caused a steam explosion, and the injuries would not have been as severe. Both factors resulted from the demand for productivity without sufficient concern for safety.
Training
Worker training should include more than a set of specific safety rules. The best safety training conveys a comprehensive understanding of the process, equipment and potential hazards. It is important that workers understand the reason for each safety rule and can respond to unforeseen situations not covered by the rules.
The importance of comprehensive training is illustrated by a 1986 accident in a North American steel plant. Two workers entered a furnace vessel in order to remove scaffolding that had been used to reline the vessel with new refractory brick. The workers followed a detailed “job safety analysis”, which outlined each step in the operation. However, the job safety analysis was defective. The vessel had been refitted two years previously with a system for blowing argon gas through the molten metal, in order to stir it more effectively, and the job safety analysis had never been updated to account for the new argon system.
Another work crew reconnected the argon system shortly before the two workers entered the vessel. The valves were leaking, and the lines had not been blanked out. The atmospheric test required for confined space entry was not properly done and the workers who entered the vessel were not present to observe the test.
Both workers died from oxygen deficiency. A third worker entered the vessel in a rescue effort, but was himself overcome. His life was saved by a fourth worker, who cut the end from a compressed air hose and threw the hose in the vessel, thus providing oxygen to the unconscious victim.
One obvious cause of the accident was the failure of the enterprise to update the job safety analysis. However, comprehensive training in the process, equipment and hazards might have enabled the workers to identify the deficiencies in the job analysis and take steps to ensure that they could enter the vessel safely.
Technological Change
The importance of analysing new or changed technology is illustrated by a 1978 accident in a North American chemical plant. The enterprise was reacting toluene and other organic chemicals in a closed vessel. The reaction was driven by heat, which was supplied to the vessel through a heating coil with circulating hot water. The plant engineering department decided to replace the water with molten sodium nitrate, in order to speed the reaction. However, the coil had been repaired with braising compounds which melted at a temperature lower than the temperature of the sodium nitrate. As a result, sodium nitrate began to leak into the vessel, where it reacted with the organic compounds to form unstable organic nitrates.
The subsequent explosion injured several workers, destroyed the reactor vessel, and damaged the building. However, the consequences could have been much worse. The accident happened late at night, when no workers were near the vessel. In addition, hot shrapnel entered a nearby process unit containing large amounts of diethyl ether. Fortunately, none of those vessels or lines were hit. An explosion on the day shift, or one which released a vapour cloud of diethyl ether, could have caused multiple deaths.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."