- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Chemicals in the Health Care Environment
Water Transportation and the Maritime Industries
The very definition of the maritime setting is work and life that takes place in or around a watery world (e.g., ships and barges, docks and terminals). Work and life activities must first accommodate the macro-environmental conditions of the oceans, lakes or waterways in which they take place. Vessels serve as both workplace and home, so most habitat and work exposures are coexistent and inseparable.
The maritime industry comprises a number of sub-industries, including freight transportation, passenger and ferry service, commercial fishing, tankships and barge shipping. Individual maritime sub-industries consist of a set of merchant or commercial activities that are characterized by the type of vessel, targeted goods and services, typical practices and area of operations, and community of owners, operators and workers. In turn, these activities and the context in which they take place define the occupational and environmental hazards and exposures experienced by maritime workers.
Organized merchant maritime activities date back to the earliest days of civilized history. The ancient Greek, Egyptian and Japanese societies are examples of great civilizations where the development of power and influence was closely associated with having an extensive maritime presence. The importance of maritime industries to development of national power and prosperity has continued into the modern era.
The dominant maritime industry is water transportation, which remains the primary mode of international trade. The economies of most countries with ocean borders are heavily influenced by the receipt and export of goods and services by water. However, national and regional economies heavily dependent on the transport of goods by water are not limited to those which border oceans. Many countries removed from the sea have extensive networks of inland waterways.
Modern merchant vessels may process materials or produce goods as well as transport them. Globalized economies, restrictive land use, favourable tax laws and technology are among the factors which have spurred the growth of vessels that serve as both factory and means of transportation. Catcher-processor fishing vessels are a good example of this trend. These factory ships are capable of catching, processing, packaging and delivering finished sea food products to regional markets, as discussed in the chapter Fishing industry.
Merchant Transport Vessels
Similar to other transport vehicles, the structure, form and function of vessels closely parallel the vessel’s purpose and major environmental circumstances. For example, craft that transport liquids short distances on inland waterways will differ substantially in form and crew from those that carry dry bulk on trans-oceanic voyages. Vessels can be free moving, semi-mobile or permanently fixed structures (e.g., offshore oil-drilling rigs) and be self-propelled or towed. At any given time, existing fleets are comprised of a spectrum of vessels with a wide range of original construction dates, materials and degrees of sophistication.
Crew size will depend on the typical duration of trip, vessel purpose and technology, expected environmental conditions and sophistication of shore facilities. Larger crew size entails more extensive needs and elaborate planning for berthing, dining, sanitation, health care and personnel support. The international trend is toward vessels of increasing size and complexity, smaller crews and expanding reliance on automation, mechanization and containerization. Table 1 provides a categorization and descriptive summary of merchant vessel types.
Table 1. Merchant vessel types.
|
Vessel types |
Description |
Crew size |
|
Freight ships |
||
|
Bulk carrier
Break bulk
Container
Ore, bulk, oil (OBO)
Vehicle
Roll-on roll- off (RORO) |
Large vessel (200-600 feet (61-183 m)) typified by large open cargo holds and many voids; carry bulk cargoes such as grain and ore; cargo is loaded by chute, conveyor or shovel
Large vessel (200-600 feet (61-183 m)); cargo carried in bales, pallets, bags or boxes; expansive holds with between decks; may have tunnels
Large vessel (200-600 (61-183 m)) with open holds; may or may not have booms or cranes to handle cargo; containers are 20-40 feet (6.1-12.2 m) and stackable
Large vessel (200-600 feet (61-183 m)); holds are expansive and shaped to hold bulk ore or oil; holds are water tight, may have pumps and piping; many voids
Large vessel (200-600 feet (61-183 m)) with big sail area; many levels; vehicles can be self loading or boomed aboard
Large vessel (200-600 feet (61-183 m)) with big sail area; many levels; can carry other cargo in addition to vehicles |
25-50
25-60
25-45
25-55
25-40
25-40 |
|
Tank ships |
||
|
Oil
Chemical
Pressurized |
Large vessel (200-1000 feet (61-305 m)) typified by stern house piping on deck; may have hose handling booms and large ullages with many tanks; can carry crude or processed oil, solvents and other petroleum products
Large vessel (200-1000 feet (61-305 m)) similar to oil tankship, but may have additional piping and pumps to handle multiple cargoes simultaneously; cargoes can be liquid, gas, powders or compressed solids
Usually smaller (200-700 feet (61-213.4 m)) than typical tankship, having fewer tanks, and tanks which are pressurized or cooled; can be chemical or petroleum products such as liquid natural gas; tanks are usually covered and insulated; many voids, pipes and pumps |
25-50
25-50
15-30
|
|
Tug boats |
Small to mid-size vessel (80-200 feet (24.4-61 m)); harbour, push boats, ocean going |
3-15 |
|
Barge |
Mid-size vessel (100-350 feet (30.5-106.7 m)); can be tank, deck, freight or vehicle; usually not manned or self-propelled; many voids |
|
|
Drillships and rigs |
Large, similar profile to bulk carrier; typified by large derrick; many voids, machinery, hazardous cargo and large crew; some are towed, others self propelled |
40-120 |
|
Passenger |
All sizes (50-700 feet (15.2-213.4 m)); typified by large number of crew and passengers (up to 1000+) |
20-200 |
Morbidity and Mortality in the Maritime Industries
Health care providers and epidemiologists are often challenged to distinguish adverse health states due to work-related exposures from those due to exposures outside the workplace. This difficulty is compounded in the maritime industries because vessels serve as both workplace and home, and both exist in the greater environment of the maritime milieu itself. The physical boundaries found on most vessels result in close confinement and sharing of workspaces, engine-room, storage areas, passageways and other compartments with living spaces. Vessels often have a single water, ventilation or sanitation system that serves both work and living quarters.
The social structure aboard vessels is typically stratified into vessel officers or operators (ship’s master, first mate and so on) and remaining crew. Ship officers or operators are generally relatively more educated, affluent and occupationally stable. It is not uncommon to find vessels with crew members of an entirely different national or ethnic background from that of the officers or operators. Historically, maritime communities are more transient, heterogeneous and somewhat more independent than non-maritime communities. Work schedules aboard ship are often more fragmented and intermingled with non-work time than are land-based employment situations.
These are some reasons why it is difficult to describe or quantify health problems in the maritime industries, or to correctly associate problems with exposures. Data on maritime worker morbidity and mortality suffer from being incomplete and not representative of entire crews or sub-industries. Another shortfall of many data sets or information systems that report on the maritime industries is the inability to distinguish among health problems due to work, vessel or macro-environmental exposures. As with other occupations, difficulties in capturing morbidity and mortality information is most obvious with chronic disease conditions (e.g., cardiovascular disease), particularly those with a long latency (e.g., cancer).
Review of 11 years (1983 to 1993) of US maritime data demonstrated that half of all fatalities due to maritime injuries, but only 12% of non-fatal injuries, are attributed to the vessel (i.e., collision or capsizing). The remaining fatalities and non-fatal injuries are attributed to personnel (e.g., mishaps to an individual while aboard ship). Reported causes of such mortality and morbidity are described in figure 1 and figure 2 respectively. Comparable information on non-injury-related mortality and morbidity is not available.
Figure 1. Causes of leading fatal unintentional injuries attributed to personal reasons (US maritime industries 1983-1993).
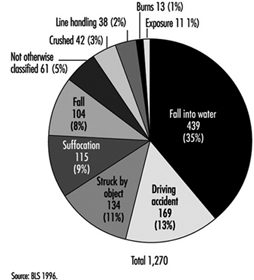
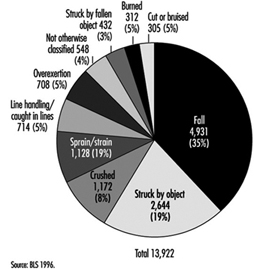
Figure 2. Causes of leading non-fatal unintentional injuries attributed to personal reasons (US maritime industries 1983-1993).
Combined vessel and personal US maritime casualty data reveal that the highest proportion (42%) of all maritime fatalities (N = 2,559), occurred among commercial fishing vessels. The next highest were among towboats/barges (11%), freight ships (10%) and passenger vessels (10%).
Analysis of reported work-related injuries for the maritime industries shows similarities to patterns reported for the manufacturing and construction industries. Commonalities are that most injuries are due to falls, being struck, cuts and bruises or muscular strains and overuse. Caution is needed when interpreting these data, however, as there is reporting bias: acute injuries are likely to be over-represented and chronic/latent injuries, which are less obviously connected to work, under-reported.
Occupational and Environmental Hazards
Most health hazards found in the maritime setting have land-based analogs in the manufacturing, construction and agricultural industries. The difference is that the maritime environment constricts and compresses available space, forcing close proximity of potential hazards and the intermingling of living quarters and workspaces with fuel tanks, engine and propulsion areas, cargo and storage spaces.
Table 2 summaries health hazards common across different vessel types. Health hazards of particular concern with specific vessel types are highlighted in table 3. The following paragraphs of this section expand discussion of selected environmental, physical and chemical, and sanitation health hazards.
Table 2. Health hazards common across vessel types.
|
Hazards |
Description |
Examples |
|
Mechanical |
Unguarded or exposed moving objects or their parts, which strike, pinch, crush or entangle. Objects can be mechanized (e.g., fork-lift) or simple (hinged door). |
Winches, pumps, fans, drive shafts, compressors, propellers, hatches, doors, booms, cranes, mooring lines, moving cargo |
|
Electrical |
Static (e.g., batteries) or active (e.g., generators) sources of electricity, their distribution system (e.g., wiring) and powered devices (e.g., motors), all of which can cause direct electrical-induced physical injury |
Batteries, vessel generators, dockside electrical sources, unprotected or ungrounded electric motors (pumps, fans, etc.), exposed wiring, navigation and communication electronics |
|
Thermal |
Heat- or cold-induced injury |
Steam pipes, cold storage spaces, power plant exhaust, cold- or warm-weather exposure above deck |
|
Noise |
Adverse auditory and other physiological problems due to excessive and prolonged sound energy |
Vessel propulsion system, pumps, ventilation fans, winches, steam-powered devices, conveyor belts |
|
Fall |
Slips, trips and falls resulting in kinetic-energy-induced injuries |
Steep ladders, deep vessel holds, missing railings, narrow gangways, elevated platforms |
|
Chemical |
Acute and chronic disease or injury resulting from exposure to organic or inorganic chemicals and heavy metals |
Cleaning solvents, cargo, detergents, welding, rusting/corrosion processes, refrigerants, pesticides, fumigants |
|
Sanitation |
Disease related to unsafe water, poor food practices or improper waste disposal |
Contaminated potable water, food spoilage, deteriorated vessel waste system |
|
Biologic |
Disease or illness causes by exposure to living organisms or their products |
Grain dust, raw wood products, cotton bales, bulk fruit or meat, seafood products, communicable disease agents |
|
Radiation |
Injury due to non-ionizing radiation |
Intense sunlight, arc welding, radar, microwave communications |
|
Violence |
Interpersonal violence |
Assault, homicide, violent conflict among crew |
|
Confined space |
Toxic or anoxic injury resulting from entering an enclosed space with limited entry |
Cargo holds, ballast tanks, crawl spaces, fuel tanks, boilers, storage rooms, refrigerated holds |
|
Physical work |
Health problems due to overuse, disuse or unsuitable work practices |
Shovelling ice in fish tanks, moving awkward cargo in restricted spaces, handling heavy mooring lines, prolonged stationary watch standing |
Table 3. Notable physical and chemical hazards for specific vessel types.
|
Vessel Types |
Hazards |
|
Tank vessels |
Benzene and various hydrocarbon vapours, hydrogen sulphide off-gassing from crude oil, inert gases used in tanks to create oxygen-deficient atmosphere for explosion control, fire and explosion due to combustion of hydrocarbon products |
|
Bulk cargo vessels |
Pocketing of fumigants used on agricultural products, personnel entrapment/suffocation in loose or shifting cargo, confined space risks in conveyor or man tunnels deep in vessel, oxygen deficiency due to oxidation or fermentation of cargo |
|
Chemical carriers |
Venting of toxic gases or dusts, pressurized air or gas release, leakage of hazardous substances from cargo holds or transfer pipes, fire and explosion due to combustion of chemical cargoes |
|
Container ships |
Exposure to spills or leakage due to failed or improperly stored hazardous substances; release of agricultural inerting gases; venting from chemical or gas containers; exposure to mislabeled substances that are hazardous; explosions, fire or toxic exposures due to mixing of separate substances to form a dangerous agent (e.g., acid and sodium cyanide) |
|
Break bulk vessels |
Unsafe conditions due to shifting of cargo or improper storage; fire, explosion or toxic exposures due to mixing of incompatible cargoes; oxygen deficiency due to oxidation or fermentation of cargoes; release of refrigerant gases |
|
Passenger ships |
Contaminated potable water, unsafe food preparation and storage practices, mass evacuation concerns, acute health problems of individual passengers |
|
Fishing vessels |
Thermal hazards from refrigerated holds, oxygen deficiency due to decomposition of seafood products or use of antioxidant preservatives, release of refrigerant gases, entanglement in netting or lines, contact with dangerous or toxic fish or sea animals |
Environmentalhazards
Arguably the most characteristic exposure defining the maritime industries is the pervasive presence of the water itself. The most variable and challenging of water environments is the open ocean. Oceans present constantly undulating surfaces, extremes of weather and hostile travel conditions, which combine to cause constant motion, turbulence and shifting surfaces and can result in vestibular disturbances (motion sickness), object instability (e.g., swinging latches and sliding gear) and the propensity to fall.
Humans have limited capability to survive unaided in open water; drowning and hypothermia are immediate threats upon immersion. Vessels serve as platforms that permit the human presence at sea. Ships and other water craft generally operate at some distance from other resources. For these reasons, vessels must dedicate a large proportion of total space to life support, fuel, structural integrity and propulsion, often at the expense of habitability, personnel safety and human factor considerations. Modern supertankers, which provide more generous human space and liveability, are an exception.
Excessive noise exposure is a prevalent problem because sound energy is readily transmitted through a vessel’s metallic structure to nearly all spaces, and limited noise attenuation materials are used. Excessive noise can be nearly continuous, with no available quiet areas. Sources of noise include the engine, propulsion system, machinery, fans, pumps and the pounding of waves on the vessel hull.
Mariners are an identified risk group for developing skin cancers, including malignant melanoma, squamous cell carcinoma and basal cell carcinoma. The increased risk is due to excess exposure to direct and water-surface-reflected ultraviolet solar radiation. Body areas of particular risk are exposed parts of the face, neck, ears and forearms.
Limited insulation, inadequate ventilation, internal sources of heat or cold (e.g., engine rooms or refrigerated spaces) and metallic surfaces all account for potential thermal stress. Thermal stress compounds physiological stress from other sources, resulting in reduced physical and cognitive performance. Thermal stress that is not adequately controlled or protected against can result in heat- or cold-induced injury.
Physical and chemical hazards
Table 3 highlights hazards unique or of particular concern to specific vessel types. Physical hazards are the most common and pervasive hazard aboard vessels of any type. Space limitations result in narrow passageways, limited clearance, steep ladders and low overheads. Confined vessel spaces means that machinery, piping, vents, conduits, tanks and so forth are squeezed in, with limited physical separation. Vessels commonly have openings that allow direct vertical access to all levels. Inner spaces below the surface deck are characterized by a combination of large holds, compact spaces and hidden compartments. Such physical structure places crew members at risk for slips, trips and falls, cuts and bruises, and being struck by moving or falling objects.
Constricted conditions result in being in close proximity to machinery, electrical lines, high-pressure tanks and hoses, and dangerously hot or cold surfaces. If unguarded or energized, contact can result in burns, abrasions, lacerations, eye damage, crushing or more serious injury.
Since vessels are basically a composite of spaces housed within a water-tight envelope, ventilation can be marginal or deficient in some spaces, creating a hazardous confined space situation. If oxygen levels are depleted or air is displaced, or if toxic gases enter these confined spaces, entry can be life threatening.
Refrigerants, fuels, solvents, cleaning agents, paints, inert gases and other chemical substances are likely to be found on any vessel. Normal ship activities, such as welding, painting and trash burning can have toxic effects. Transport vessels (e.g., freight ships, container ships and tank ships) can carry a host of biological or chemical products, many of which are toxic if inhaled, ingested or touched with the bare skin. Others can become toxic if allowed to degrade, become contaminated or mix with other agents.
Toxicity can be acute, as evidenced by dermal rashes and ocular burns, or chronic, as evidenced by neurobehavioural disorders and fertility problems or even carcinogenic. Some exposures can be immediately life-threatening. Examples of toxic chemicals carried by vessels are benzene-containing petrochemicals, acrylonitrile, butadiene, liquefied natural gas, carbon tetrachloride, chloroform, ethylene dibromide, ethylene oxide, formaldehyde solutions, nitropropane, o-toluidine and vinyl chloride.
Asbestos remains a hazard on some vessels, principally those constructed prior to the early 1970s. The thermal insulation, fire protection, durability and low cost of asbestos made this a preferred material in ship building. The primary hazard of asbestos occurs when the material becomes airborne when it is disturbed during renovations, construction or repair activities.
Sanitation and communicable disease hazards
One of the realities aboard ship is that the crew is often in close contact. In the work, recreation and living environments, crowding is often a fact of life that heightens the requirement for maintaining an effective sanitation programme. Critical areas include: berthing spaces, including toilet and shower facilities; food service and storage areas; laundry; recreation areas; and, if present, the barbershop. Pest and vermin control is also of critical importance; many of these animals can transmit disease. There are many opportunities for insects and rodents to infest a vessel, and once entrenched they are very difficult to control or eradicate, especially while underway. All vessels must have a safe and effective pest control programme. This requires training of individuals for this task, including annual refresher training.
Berthing areas must be kept free of debris, soiled laundry and perishable food. Bedding should be changed at least weekly (more often if soiled), and adequate laundry facilities for the size of the crew should be available. Food service areas must be rigorously maintained in a sanitary manner. The food service staff must receive training in proper techniques of food preparation, storage and galley sanitation, and adequate storage facilities must be provided aboard ship. The staff must adhere to recommended standards to ensure that food is prepared in a wholesome manner and is free of chemical and biological contamination. The occurrence of a food-borne disease outbreak aboard a vessel can be serious. A debilitated crew cannot carry out its duties. There may be insufficient medication to treat the crew, especially underway, and there may not be competent medical staff to care for the ill. In addition, if the ship is forced to change its destination, there may be significant economic loss to the shipping company.
The integrity and maintenance of a vessel’s potable water system is also of vital importance. Historically, water-borne outbreaks aboard ship have been the most common cause of acute disability and death among crews. Therefore, the potable water supply must come from an approved source (wherever possible) and be free from chemical and biological contamination. Where this is not possible, the vessel must have the means to effectively decontaminate the water and render it potable. A potable water system must be protected against contamination by every known source, including cross-contaminations with any non-potable liquids. The system also must be protected from chemical contamination. It must be cleaned and disinfected periodically. Filling the system with clean water containing at least 100 parts per million (ppm) of chlorine for several hours and then flushing the entire system with water containing 100 ppm chlorine is effective disinfection. The system should then be flushed with fresh potable water. A potable water supply must have at least 2 ppm residual of chlorine at all times, as documented by periodic testing.
Communicable disease transmission aboard ship is a serious potential problem. Lost work time, the cost of medical treatment and the possibility of having to evacuate crew members make this an important consideration. Besides the more common disease agents (e.g., those that cause gastroenteritis, such as Salmonella, and those that cause upper respiratory disease, such as the influenza virus), there has been a re-emergence of disease agents that were thought to be under control or eliminated from the general population. Tuberculosis, highly pathogenic strains of Escherichia coli and Streptococcus, and syphilis and gonorrhoea have reappeared in increasing incidence and/or virulence.
In addition, previously unknown or uncommon disease agents such as the HIV virus and the Ebola virus, which are not only highly resistant to treatment, but highly lethal, have appeared. It is therefore important that assessment be made of appropriate crew immunization for such diseases as polio, diphtheria, tetanus, measles, and hepatitis A and B. Additional immunizations may be required for specific potential or unique exposures, since crew members may have occasion to visit a wide variety of ports around the world and at the same time come in contact with a number of disease agents.
It is vital that crew members receive periodic training in the avoidance of contact with disease agents. The topic should include blood-borne pathogens, sexually transmitted diseases (STDs), food- and water-borne diseases, personal hygiene, symptoms of the more common communicable diseases and appropriate action by the individual on discovering these symptoms. Communicable disease outbreaks aboard ship can have a devastating effect on the vessel’s operation; they can result in a high level of illness among the crew, with the possibility of serious debilitating disease and in some cases death. In some instances, vessel diversion has been required with resultant heavy economic losses. It is in the best interest of the vessel owner to have an effective and efficient communicable disease programme.
Hazard Control and Risk Reduction
Conceptually, the principles of hazard control and risk reduction are similar to other occupational settings, and include:
- hazard identification and characterization
- inventory and analysis of exposures and at-risk populations
- hazard elimination or control
- personnel monitoring and surveillance
- disease/injury prevention and intervention
- programme evaluation and adjustment (see table 4).
Table 4. Vessel hazard control & risk-reduction.
|
Topics |
Activities |
|
Programme development and evaluation |
Identify hazards, shipboard and dockside. |
|
Hazard identification |
Inventory shipboard chemical, physical, biological, and environmental hazards, in both work and living spaces (e.g., broken railings, use and storage of cleaning agents, presence of asbestos). |
|
Assessment of exposure |
Understand work practices and job tasks (prescribed as well as those actually done). |
|
Personnel at risk |
Review work logs, employment records and monitoring data of entire ship’s complement, both seasonal and permanent. |
|
Hazard control and |
Know established and recommended exposure standards (e.g., NIOSH, ILO, EU). |
|
Health surveillance |
Develop health information gathering and reporting system for all injuries and illnesses (e.g., maintain a ship’s daily binnacle). |
|
Monitor crew health |
Establish occupational medical monitoring, determine performance standards, and establish fitness-for-work criteria (e.g., pre-placement and periodic pulmonary testing of crew handling grain). |
|
Hazard control and risk reduction effectiveness |
Devise and set priorities for goals (e.g., reduce shipboard falls). |
|
Programme evolution |
Modify prevention and control activities based on changing circumstances and prioritization. |
To be effective, however, the means and methods to implement these principles must be tailored to the specific maritime arena of interest. Occupational activities are complex and take place in integrated systems (e.g., vessel operations, employee/employer associations, commerce and trade determinants). The key to prevention is to understand these systems and the context in which they take place, which requires close cooperation and interaction between all organizational levels of the maritime community, from general deck hand through vessel operators and company upper management. There are many government and regulatory interests that impact the maritime industries. Partnerships between government, regulators, management and workers are essential for meaningful programmes for improving the health and safety status of the maritime industries.
The ILO has established a number of Conventions and Recommendations relating to shipboard work, such as the Prevention of Accidents (Seafarers) Convention, 1970 (No. 134), and Recommendation, 1970 (No. 142), the Merchant Shipping (Minimum Standards) Convention, 1976 (No. 147), the Merchant Shipping (Improvement of Standards) Recommendation, 1976 (No. 155), and the Health Protection and Medical Care (Seafarers) Convention, 1987 (No. 164). The ILO has also published a Code of Practice regarding the prevention of accidents at sea (ILO 1996).
Approximately 80% of vessel casualties are attributed to human factors. Similarly, the majority of reported injury-related morbidity and mortality have human factor causes. Reduction in maritime injury and death requires successful application of principles of human factors to work and life activities aboard vessels. Successful application of human factors principles means that vessel operations, vessel engineering and design, work activities, systems and management policies are developed that integrate human anthropometrics, performance, cognition and behaviours. For example, cargo loading/unloading presents potential hazards. Human factor considerations would highlight the need for clear communication and visibility, ergonomic matching of worker to task, safe separation of workers from moving machinery and cargo and a trained workforce, well acquainted with work processes.
Prevention of chronic diseases and adverse health states with long latency periods is more problematic than injury prevention and control. Acute injury events generally have readily recognized cause-effect relationships. Also, the association of injury cause and effect with work practices and conditions is usually less complicated than for chronic diseases. Hazards, exposures and health data specific to the maritime industries are limited. In general, health surveillance systems, reporting and analyses for the maritime industries are less developed than those for many of their land-based counterparts. The limited availability of chronic or latent disease health data specific to maritime industries hinders development and application of targeted prevention and control programmes.
Subways
While railroad safety comes under the jurisdiction of national governments, which issue rules and policies for safety governance and enforcement, subways are usually governed by local public authorities, which in essence govern themselves.
Subway fares usually do not cover operating cost and, through subsidies, are kept at certain levels to maintain an affordable public transportation service. Subway and other city mass transit systems make city roads more accessible and reduce the pollution associated with urban automobile traffic.
Budget cuts that have become so common in many countries in recent years also affect mass transit systems. Preventive maintenance personnel and the upgrade of tracks, signals and rolling stock are the first to be affected. The controlling authorities are often unwilling or unable to enforce their own regulatory procedures on a rapid transit system abandoned by government subsidies. Inevitably in such circumstances, a transportation accident with catastrophic loss of life during the budget cuts results in a public outcry demanding improvements in safety.
While it is recognized that great variation exists in the design, construction and age of the physical facilities of the rapid transit properties in Canada, the United States and other countries, certain standard maintenance functions must be carried out to keep operating track, aerial and underground structures, passenger stations and related facilities in the safest possible condition.
Subway Operation and Maintenance
Subways differ from railroads in several basic ways:
- most subways run underground in tunnels
- subways run on electricity rather than diesel or steam (although there are also some electrical trains)
- subways run much more frequently than railroad trains
- graffiti removal is a major problem.
These factors influence the degree of risk for subway train operators and maintenance crews.
Collisions between subway trains on the same track and with maintenance crews on the track are a serious problem. These collisions are controlled by proper scheduling, central communications systems to alert subway train operators of problems and signal light systems indicating when operators can proceed safely. Breakdowns in these control procedures resulting in collisions can occur due to radio communication problems, broken or improperly placed signal lights that do not give operators adequate time to stop and fatigue problems from shift work and excessive overtime, resulting in inattention.
Maintenance crews patrol the subway tracks doing repairs to tracks, signal lights and other equipment, picking up rubbish and performing other duties. They face electrical hazards from the third rail carrying the electricity to operate the subways, fire and smoke hazards from burning rubbish and possible electrical fires, inhalation hazards from steel dust and other particulates in the air from the subway wheels and rails and the hazard of being hit by subway cars. Floods in subways can also create electrical shock and fire hazards. Because of the nature of subway tunnels, many of these hazardous situations are confined-space hazards.
Adequate ventilation to remove air contaminants, proper confined-space and other emergency procedures (e.g., evacuation procedures) for fires and floods and adequate communication procedures including radios and signal lights to notify subway train operators of the presence of maintenance crews on the tracks are essential to protect these crews. There should be frequent emergency spaces along subway walls or adequate space between tracks to allow maintenance crew members to avoid passing subway cars.
Graffiti removal from both the inside and outside of subway cars is a hazard in addition to regular painting and cleaning of cars. Graffiti removers often contained strong alkalis and hazardous solvents and can be a hazard both by skin contact and inhalation. Exterior graffiti removal is done by driving the cars through a car wash where the chemicals are sprayed on the exterior of the car. The chemicals are also applied by brushing and spraying inside subway cars. Applying hazardous graffiti removers inside cars could be a confined-space hazard.
Precautions include using the least toxic chemicals possible, proper respirator protection and other personal protective equipment and proper procedures to ensure that car operators know what chemicals are being used.
Rail Operations
Railroads provide a major mode of transportation around the world. Today, even with competition from road and airborne transport, rail remains an important means of land-based movement of bulk quantities of goods and materials. Railroad operations are carried out in an enormously wide variety of terrains and climates, from Arctic permafrost to equatorial jungle, from rainforest to desert. The roadbed of partly crushed stone (ballast) and track consisting of steel rails and ties of wood, concrete or steel are common to all railroads. Ties and ballast maintain the position of the rails.
The source of power used in railroad operations worldwide (steam, diesel-electric and current electricity) spans the history of development of this mode of transportation.
Administration and Train Operations
Administration and train operations create the public profile of the railroad industry. They ensure that goods move from origin to destination. Administration includes office personnel involved in business and technical functions and management. Train operations include dispatchers, rail traffic control, signal maintainers, train crews and yard workers.
Dispatchers ensure that a crew is available at the appropriate point and time. Railroads operate 24 hours per day, 7 days per week throughout the year. Rail traffic control personnel coordinate train movements. Rail traffic control is responsible for assigning track to trains in the appropriate sequence and time. This function is complicated by single sets of track that must be shared by trains moving in both directions. Since only one train can occupy a particular section of track at any time, rail traffic control must assign occupancy of the main line and sidings, in a manner that assures safety and minimizes delay.
Signals provide visual cues to train operators, as well as to drivers of road vehicles at level train crossings. For train operators, signals must provide unambiguous messages about the status of the track ahead. Signals today are used as an adjunct to rail traffic control, the latter being conducted by radio on channels received by all operating units. Signal maintainers must ensure operation of these units at all times, which can sometimes involve working alone in remote areas in all weather at any time, day or night.
Yard workers’ duties include ensuring that the rolling stock is prepared to receive cargo, which is an increasingly important function in this era of quality management. Tri-level automobile transporter cars, for example, must be cleaned prior to use and readied to accept vehicles by moving chocks to appropriate positions. The distance between levels in these cars is too short for the average male to stand upright, so that work is done in a hunched over position. Similarly, the handholds on some cars force yard workers to assume an awkward posture during shunting operations.
For long runs, a train crew operates the train between designated transfer points. A replacement crew takes over at the transfer point and continues the journey. The first crew must wait at the transfer point for another train to make the return trip. The combined trips and the wait for the return train can consume many hours.
A train trip on single track can be very fragmented, in part because of problems in scheduling, track work and the breakdown of equipment. Occasionally a crew returns home in the cab of a trailing locomotive, in the caboose (where still in use) or even by taxi or bus.
The train crew’s duties may include dropping off some cars or picking up additional ones en route. This could occur at any hour of the day or night under any imaginable weather conditions. The assembly and disassembly of trains are the sole duties of some train crews in yards.
On occasion there is a failure of one of the knuckles that couple cars together or a break in a hose that carries braking system air between cars. This necessitates investigative work by one of the train crew and repair or replacement of the defective part. The spare knuckle (about 30 kg) must be carried along the roadbed to the repair point, and the original removed and replaced. Work between cars must reflect careful planning and preparation to ensure that the train does not move during the procedure.
In mountainous areas, breakdown may occur in a tunnel. The locomotive must maintain power above idle under these conditions in order to keep the braking functional and to prevent train runaway. Running the engine in a tunnel could cause the tunnel to fill with exhaust gases (nitrogen dioxide, nitric oxide, carbon monoxide and sulphur dioxide).
Table 1 summarizes potential hazardous conditions associated with administration and train operations.
Table 1. Hazardous conditions associated with administration and train operations.
|
Conditions |
Affected groups |
Comments |
|
Exhaust emissions |
Train crew, supervisors, technical advisors |
Emissions primarily include nitrogen dioxide, nitric oxide, carbon monoxide, sulphur dioxide and particulates containing polycyclic aromatic hydrocarbons (PAHs). Potential for exposure is most likely in unventilated tunnels. |
|
Noise |
Train crew, supervisors, technical advisors |
In-cab noise could exceed regulated limits. |
|
Whole-body vibration |
Train crew |
Structure-borne vibration transmitted through the floor and seats in the cab originates from the engine and motion along the track and over gaps between rails. |
|
Electromagnetic fields |
Train crew, signal maintainers |
AC and DC fields are possible, depending on design of power unit and traction motors. |
|
Radio-frequency fields |
Users of two-way radios |
Effects on humans are not fully established. |
|
Weather |
Train crew, yard workers, signal maintainers |
Ultraviolet energy can cause sunburn, skin cancer and cataracts. Cold can cause cold stress and frostbite. Heat can cause heat stress. |
|
Shiftwork |
Dispatchers, rail traffic control, train crews, signal maintainers |
Train crews can work irregular hours; remuneration is often based on travelling a fixed distance within a time period. |
|
Musculoskeletal injury |
Train crew, yard workers |
Ankle injury can occur during disembarkment from moving equipment. Shoulder injury can occur during embarkment onto moving equipment. Injury can occur at various sites while carrying knuckles on rough terrain. Work is performed in awkward postures. |
|
Video displays units |
Management, administrative and technical staff, dispatchers, rail traffic control |
Effective use of computerized workstations depends on application of visual and office ergonomic principles. |
|
Rundown accidents |
All workers |
Rundown can occur when the individual stands on an active track and fails to hear approach of trains, track equipment and moving cars. |
Maintenance of Rolling Stock and Track Equipment
Rolling stock includes locomotives and railcars. Track equipment is specialized equipment used for track patrol and maintenance, construction and rehabilitation. Depending on the size of the railroad, maintenance can range from onsite (small-scale repairs) to complete stripdown and rebuilding. Rolling stock must not fail in operation, since failure carries serious adverse safety, environmental and business consequences. If a car carries a hazardous commodity, the consequences that can arise from failure to find and repair a mechanical defect can be enormous.
Larger rail operations have running shops and centralized stripdown and rebuild facilities. Rolling stock is inspected and prepared for the trip at running shops. Minor repair is performed on both cars and locomotives.
Railcars are rigid structures that have pivot points near each end. The pivot point accepts a vertical pin located in the truck (the wheels and their support structure). The body of the car is lifted from the truck for repairs. Minor repair can involve the body of the car or attachments or brakes or other parts of the truck. Wheels may require machining on a lathe to remove flat spots.
Major repair could include removal and replacement of damaged or corroded metal sheeting or frame and abrasive blasting and repainting. It could also include removal and replacement of wooden flooring. Trucks, including wheel-axle sets and bearings, may require disassembly and rebuilding. Rehabilitation of truck castings involves build-up welding and grinding. Rebuilt wheel-axle sets require machining to true the assembly.
Locomotives are cleaned and inspected prior to each trip. The locomotive may also require mechanical service. Minor repairs include oil changes, work on brakes and servicing of the diesel engine. Removal of a truck for wheel truing or evening may also be needed. Operation of the engine may be required in order to position the locomotive inside the service building or to remove it from the building. Prior to re-entry into service the locomotive could require a load test, during which the engine is operated at full throttle. Mechanics work in close proximity to the engine during this procedure.
Major servicing could involve complete stripdown of the locomotive. The diesel engine and engine compartment, compressor, generator and traction motors require thorough degreasing and cleaning owing to heavy service and contact of fuel and lubricants with hot surfaces. Individual components may then be stripped and rebuilt.
Traction motor casings may require build-up welding. Armatures and rotors may need machining in order to remove old insulation, then be repaired and impregnated with a solution of varnish.
Track maintenance equipment includes trucks and other equipment that can operate on road and rail, as well as specialized equipment that operates only on rail. The work may include highly specialized units, such as track inspection units or rail-grinding machines, which may be “one of a kind”, even in large railroad companies. Track maintenance equipment may be serviced in garage settings or in field locations. The engines in this equipment may produce considerable exhaust emissions due to long periods between service and lack of familiarity of mechanics. This can have major pollution consequences during operation in confined spaces, such as tunnels and sheds and enclosing formations.
Table 2 summarizes potential hazardous conditions associated with maintenance of rolling stock and track equipment as well as transportation accidents.
Table 2. Hazardous conditions associated with maintenance and transportation accidents.
|
Conditions |
Affected groups |
Comments |
|
Skin contamination with waste oils and lubricants |
Diesel mechanics, traction motor mechanics |
Decomposition of hydrocarbons in contact with hot surfaces can produce polycyclic aromatic hydrocarbons (PAHs). |
|
Exhaust emissions |
All workers in diesel shop, wash facility, refuelling area, load test area |
Emissions primarily include nitrogen dioxide, nitric oxide, carbon monoxide, sulphur dioxide and particulates containing (PAHs). Potential for exposure most likely where exhaust emissions are confined by structures. |
|
Welding emissions |
Welders, tackers, fitters, operators of overhead cranes |
Work primarily involves carbon steel; aluminium and stainless steel are possible. Emissions include shield gases and fluxes, metal fumes, ozone, nitrogen dioxide, visible and ultraviolet energy. |
|
Brazing emissions |
Electricians working on traction motors |
Emission include cadmium end lead in solder. |
|
Thermal decomposition products from coatings |
Welders, tackers, fitters, grinders, operators of overhead cranes |
Emissions can include carbon monoxide, inorganic pigments containing lead and other chromates, decomposition products from paint resins. PCBs may have been used prior to 1971. PCBs can form furans and dioxins when heated. |
|
Cargo residues |
Welders, fitters, tackers, grinders, mechanics, strippers |
Residues reflect service in which car was used; cargoes could include heavy metal concentrates, coal, sulphur, lead ingots, etc. |
|
Abrasive blasting dust |
Abrasive blaster, bystanders |
Dust can contain cargo residues, blast material, paint dust. Paint applied prior to 1971 may contain PCBs. |
|
Solvent vapours |
Painter, bystanders |
Solvent vapours can be present in paint storage and mixing areas and paint booth; flammable mixtures may develop inside confined spaces, such as hoppers and tanks, during spraying. |
|
Paint aerosols |
Painter, bystanders |
Paint aerosols contain sprayed paint plus diluent; solvent in droplets and vapour can form flammable mixtures; resin system can include isocyanates, epoxys, amines, peroxides and other reactive intermediates. |
|
Confined spaces |
All shop workers |
Interior of some railcars, tanks and hoppers, nose of locomotive, ovens, degreasers, varnish impregnator, pits, sumps and other enclosed and partially enclosed structures |
|
Noise |
All shop workers |
Noise generated by many sources and tasks can exceed regulated limits. |
|
Hand-arm vibration |
Users of powered hand tools and hand-held equipment |
Vibration is transmitted through hand grips. |
|
Electromagnetic fields |
Users of electrical welding equipment |
AC and DC fields are possible, depending on design of the unit. |
|
Weather |
Outside workers |
Ultraviolet energy can cause sunburn, skin cancer and cataracts. Cold can cause cold stress and frostbite. Heat can cause heat stress. |
|
Shiftwork |
All workers |
Crews can work irregular hours. |
|
Musculoskeletal injury |
All workers |
Ankle injury can occur during disembarkment from moving equipment. Shoulder injury can occur during embarkment onto moving equipment or climbing onto cars. Work is performed in awkward posture especially when welding, burning, cutting and operating powered hand tools. |
|
Rundown accidents |
All workers |
Rundown can occur when the individual stands on active track and fails to hear approach of track equipment and moving cars. |
Maintenance of Track and Right of Way
Maintenance of track and right of way primarily involves work in the outdoor environment in conditions associated with the outdoors: sun, rain, snow, wind, cold air, hot air, blowing sand, biting and stinging insects, aggressive animals, snakes and poisonous plants.
Track and right-of-way maintenance can include track patrol, as well as the maintenance, rehabilitation and replacement of buildings and structures, track and bridges, or service functions, such as snowplowing and herbicide application, and may involve local operating units or large, specialized work gangs that deal with replacement of rails, ballast or ties. Equipment is available to almost completely mechanize each of these activities. Small-scale work, however, could involve small, powered equipment units or even be a completely manual activity.
In order to carry out maintenance of operating lines, a block of time must be available during which the work can occur. The block could become available at any time of day or night, depending on train scheduling, especially on a single-track main line. Thus, time pressure is a main consideration during this work, since the line must be returned to service at the end of the assigned block of time. Equipment must proceed to the site, the work must be completed, and the track vacated within the set period.
Ballast replacement and tie and rail replacement are complex tasks. Ballast replacement first involves removal of contaminated or deteriorated material in order to expose the track. A sled, a plow-like unit that is pulled by a locomotive, or an undercutter performs this task. The undercutter uses a continuous toothed chain to pull ballast to the side. Other equipment is used to remove and replace rail spikes or tie clips, tie plates (the metal plate on which the rail sits on the tie) and ties. Continuous rail is akin to a noodle of wet spaghetti that can flex and whip and that is easily moved vertically and laterally. Ballast is used to stabilize the rail. The ballast train delivers new ballast and pushes it into position. Labourers walk along with the train and systematically open chutes located at the bottom of the cars in order to enable ballast to flow.
After the ballast is dropped, a tamper uses hydraulic fingers to pack the ballast around and under the ties and lifts the track. A spud liner drives a metal spike into the roadbed as an anchor and moves the track into the desired position. The ballast regulator grades the ballast to establish the final contours of the roadbed and sweeps clean the surface of the ties and rails. Considerable dust is generated during ballast dumping, regulating and sweeping.
There are a variety of settings in which track work can take place—open areas, semi-enclosed areas such as cuts, and hill and cliff faces and confined spaces, such as tunnels and sheds. These have a profound influence on working conditions. Enclosed spaces, for example, will confine and concentrate exhaust emissions, ballast dust, dust from grinding, fumes from thermite welding, noise and other hazardous agents and conditions. (Thermite welding uses powdered aluminium and iron oxide. Upon ignition the aluminium burns intensely and converts the iron oxide to molten iron. The molten iron flows into the gap between the rails, welding them together end to end.)
Switching structures are associated with track. The switch contains moveable, tapered rails (points) and a wheel guide (frog). Both are manufactured from specially hardened steel containing a high level of manganese and chromium. The frog is an assembled structure containing several pieces of specially bent rail. The self-locking nuts which are used to bolt together these and other track structures may be cadmium-plated. Frogs are built up by welding and are ground during refurbishing, which can occur onsite or in shop facilities.
Bridge repainting is also an important part of right-of-way maintenance. Bridges often are situated in remote locations; this can considerably complicate provision of personal hygiene facilities which are needed to prevent contamination of individuals and the environment.
Table 3 summarizes the hazards of track and right-of-way maintenance.
Transportation Accidents
Possibly the greatest single concern in rail operations is the transportation accident. The large quantities of material that could be involved could cause serious problems of exposure of personnel and the environment. No amount of preparation for a worst-case accident is ever enough. Therefore, minimizing risk and the consequences of an accident are imperative. Transportation accidents occur for a variety of reasons: collisions at level crossings, obstruction of the track, failure of equipment and operator error.
The potential for such accidents can be minimized through conscientious and ongoing inspection and maintenance of track and right-of-way and equipment. The impact of a transportation accident involving a train carrying mixed cargo can be minimized through strategic positioning of cars that carry incompatible freight. Such strategic positioning, however, is not possible for a train hauling a single commodity. Commodities of particular concern include: pulverized coal, sulphur, liquefied petroleum (fuel) gases, heavy metal concentrates, solvents and process chemicals.
All of the groups in a rail organization are involved in transportation accidents. Rehabilitation activities can literally involve all groups working simultaneously at the same location on the site. Thus, coordination of these activities is extremely important, so that the actions of one group do not interfere with those of another.
Hazardous commodities generally remain contained during such accidents because of the attention given to crashproofing in the design of shipping containers and bulk rail cars. During an accident, the contents are removed from the damaged car by emergency response crews that represent the shipper. Equipment maintainers repair the damage to the extent possible and put the car back on the track, if possible. However, the track under the derailed car may have been destroyed. If so, repair or replacement of track occurs next, using prefabricated sections and techniques similar to those described above.
In some situations, loss of containment occurs and the contents of the car or shipping container spill onto the ground. If substances are shipped in quantities sufficient to require placarding because of transportation laws, they are readily identifiable on shipping manifests. However, highly hazardous substances that are shipped in smaller quantities than mandated for listing in a shipping manifest can escape identification and characterization for a considerable period. Containment at the site and collection of the spilled material are the responsibility of the shipper.
Railway personnel can be exposed to materials that remain in snow, soil or vegetation during rehabilitation efforts. The severity of exposure depends on the properties and quantity of the substance, the geometry of the site and weather conditions. The situation could also pose fire, explosion, reactivity and toxic hazards to humans, animals and the surrounding environment.
At some point following the accident, the site must be cleared so that the track can be put back into service. Transfer of cargo and repair of equipment and track may still be required. These activities could be dramatically complicated by the loss of containment and the presence of spilled material. Any action taken to address this type of situation requires considerable prior planning that includes input from specialized knowledgeable professionals.
Hazards and Precautions
Table 1, table 2 and table 3 summarize the hazardous conditions associated with the various groups of workers involved in railroad operations. Table 4 summarizes the types of precautions used to control these hazardous conditions.
Table 3. Hazardous conditions associated with maintenance on track and right of way.
|
Condition |
Affected group(s) |
Comments |
|
Exhaust emissions |
All workers |
Emissions include nitrogen dioxide, nitric oxide, carbon monoxide, sulphur dioxide and particulates containing polycyclic aromatic hydrocarbons (PAHs). Potential for exposure is most likely in unventilated tunnels and other circumstances where exhaust is confined by structures. |
|
Ballast dust/spilled cargo |
Track equipment operators, labourers |
Depending on the source, ballast dust can contain silica (quartz), heavy metals or asbestos. Track work around operations that produce and handle bulk commodities can cause exposure to these products: coal, sulphur, heavy metal concentrates, etc. |
|
Welding, cutting and grinding emissions |
Field and shop welders |
Welding primarily involves hardened steel; emissions can include shield gases and fluxes, metal fumes, ozone, nitrogen dioxide, carbon monoxide, ultraviolet and visible energy. Exposure to manganese and chromium can occur during work involving rail; cadmium may occur in plated nuts and bolts. |
|
Abrasive blasting dust |
Abrasive blaster, bystanders |
Dust contains blast material and paint dust; paint likely contains lead and other chromates. |
|
Solvent vapours |
Painter, bystanders |
Solvent vapours can be present in paint storage and mixing areas; flammable mixtures could develop inside enclosed spray structure during spraying. |
|
Paint aerosols |
Painter, bystanders |
Paint aerosols contain sprayed paint plus diluent; solvent in droplets and vapour can form flammable mixture; resin system can include isocyanates, epoxys, amines, peroxides and other reactive intermediates. |
|
Confined spaces |
All workers |
Interior of tunnels, culverts, tanks, hoppers, pits, sumps and other enclosed and partially enclosed structures |
|
Noise |
All workers |
Noise generated by many sources and tasks can exceed regulated limits. |
|
Whole-body vibration |
Truck drivers, track equipment operators |
Structure-borne vibration transmitted through the floor and seat in the cab originates from the engine and motion along roads and track and over gaps between rails. |
|
Hand-arm vibration |
Users of powered hand tools and hand-held equipment |
Vibration transmitted through hand grips |
|
Electromagnetic fields |
Users of electrical welding equipment |
AC and DC fields are possible, depending on design of the unit. |
|
Radio-frequency fields |
Users of two-way radios |
Effects on humans not fully established |
|
Weather-related |
Outside workers |
Ultraviolet energy can cause sunburn, skin cancer and cataracts; cold can cause cold stress and frostbite; heat can cause heat stress. |
|
Shiftwork |
All workers |
Gangs work irregular hours due to problems in scheduling blocks of track time. |
|
Musculoskeletal injury |
All workers |
Ankle injury during disembark from moving equipment; shoulder injury during embark onto moving equipment; work in awkward posture, especially when welding and operating powered hand tools |
|
Rundown accident |
All workers |
Rundown can occur when the individual stands on active track and fails to hear approach of track equipment, trains and moving cars. |
Table 4. Railway industry approached to controlling hazardous conditions.
|
Hazardous conditions |
Comments/control measures |
|
Exhaust emissions |
Locomotives have no exhaust stack. Exhaust discharges vertically from the top surface. Cooling fans also located on the top of the locomotive can direct exhaust-contaminated air into the airspace of tunnels and buildings. In-cab exposure during normal transit through a tunnel does not exceed exposure limits. Exposure during stationary operations in tunnels, such as investigation of mechanical problems, rerailing of derailed cars or track repair, can considerably exceed exposure limits. Stationary operation in shops also can create significant overexposure.Track maintenance and construction equipment and heavy vehicles usually have vertical exhaust stacks. Low-level discharge or discharge through horizontal deflectors can cause overexposure. Small vehicles and portable gasoline-powered equipment discharge exhaust downward or have no stack. Proximity to these sources can cause overexposure. Control measures include:
|
|
Noise |
Control measures include:
|
|
Whole-body vibration |
Control measures include:
|
|
Electromagnetic fields |
Hazard not established below present limits. |
|
Radio-frequency fields |
Hazard not established below present limits. |
|
Weather |
Control measures include:
|
|
Shiftwork |
Arrange work schedules to reflect current knowledge about circadian rhythms. |
|
Musculoskeletal injury |
Control measures include:
|
|
Video display units |
Apply office ergonomic principles to selection and utilization of video display units. |
|
Rundown accidents |
Rail equipment is confined to the track. Unpowered rail equipment creates little noise when in motion. Natural features can block noise from powered rail equipment. Equipment noise can mask warning sound from the horn of an approaching train. During operations in rail yards, switching can occur under remote control with the result that all tracks could be live. Control measures include:
|
|
Ballast operations/ spilled cargo |
Wetting ballast prior to track work eliminates dust from ballast and cargo residues. Personal and respiratory protective equipment should be provided. |
|
Skin contamination by waste oils and lubricants |
Equipment should be cleaned prior to dismantling to remove contamination. Protective clothing, gloves and/or barrier creams should be used. |
|
Welding, cutting and brazing emissions, grinding dust |
Control measures include:
|
|
Thermal decomposition products from coatings |
Control measures include:
|
|
Cargo residues |
Control measures include:
|
|
Abrasive blasting dust |
Control measures include:
|
|
Solvent vapours, paint aerosols |
Control measures include:
|
|
Confined spaces |
Control measures include:
|
|
Hand-arm vibration |
Control measures include:
|
Violence in Gasoline Stations
Gasoline station workers rank fourth among US occupations with the highest rates of occupational homicides, with almost all occurring during attempted armed robberies or other crimes (NIOSH 1993b). The recent trend to replace repair shops with convenience stores has made them even more of a target. Study of the circumstances involved has led to the delineation of the following risk factors for such criminal violence:
- exchange of money with the public
- working alone or in small numbers
- working late night or early morning hours
- working in high-crime areas
- guarding valuable property or possessions
- working in community settings.
An additional risk factor is being in locations that are readily accessible and particularly suited to quick getaways.
To defend themselves against attempted robberies, some gasoline station workers have provided themselves with baseball bats or other cudgels and even acquired firearms. Most police authorities oppose such measures, arguing that they are likely to provoke violent reactions on the part of the criminals. The following preventive measures are suggested as more effective deterrents of robbery attempts:
- bright lighting of the gasoline pump and parking areas and of the interiors of stores and cashier’s areas
- large, unobstructed, bullet-resistant windows to enhance the visibility of the interior of the store and enclosures of bullet-resistant glass for the cashier
- separate outside entrances to any public rest rooms so that persons using them do not have to enter the store. (A separate, indoor, employee-only rest room would provide privacy for employees and obviate the need for them to go outside to use the public restroom.)
- provision of drop-boxes and time-release safes to hold all but a very limited amount of cash, as well as highly visible signs indicating their use
- establishing a policy of not making change for cash purchases during night and early morning hours
- hiring an additional worker or a security guard so that the worker is never alone (operators of gasoline stations and convenience stores object to the additional cost)
- installing an electrical or electronic alarm system (triggered by easily accessed “panic” buttons) that will provide audible and visual distress signals to attract police or other assistance—this can be combined with an alarm wired directly to a local police station
- installing high-fidelity television monitors to assist in identifying and, ultimately, apprehending the perpetrator(s).
Consultation with local police authorities and crime-prevention experts will assist in the selection of the most appropriate and cost-effective deterrents. It must be remembered that the equipment should be properly installed and periodically tested and maintained, and that the workers must be trained in its use.
Motor Vehicle Fueling and Servicing Operations
Petroleum-based fuels and lubricants are sold directly to consumers at full-service and self-service (with or without repair bays) service stations, car washes, automotive service centres, motor vehicle agencies, truck stops, repair garages, automotive parts stores and convenience stores. Service station attendants, mechanics and other employees who fuel, lubricate and service motor vehicles should be aware of the physical and chemical hazards of the petroleum fuels, lubricants, additives and waste products they come into contact with and follow appropriate safe work procedures and personal protection measures. The same physical and chemical hazards and exposures are present at commercial facilities, such as those operated by motor truck fleets, automobile rental agencies and bus companies for fuelling and servicing their own vehicles.
Because they are the facilities where motor fuels are delivered direct to the user’s vehicle, service stations, particularly those where drivers fuel their own vehicles, are where employees and the general public are most likely to come into direct contact with hazardous petroleum products. Other than those drivers who change their own oil and lubricate their own vehicles, the likelihood of contact with lubricants or used oil by motorists, except for incidental contact when checking fluid levels, is very small.
Service Station Operations
Fuel island area and dispensing system
Employees should be aware of the potential fire, safety and health hazards of gasoline, kerosene, diesel and other fuels dispensed at service stations. They should also be aware of suitable precautions. These include: safe dispensing of fuels into vehicles and containers, clean-up and disposal of spills, fighting incipient fires and draining fuels safely. Service stations should provide fuel-dispenser pumps which operate only when the fuel-hose nozzles are removed from the dispensers’ brackets and the switches are manually or automatically activated. Fuel-dispensing devices should be mounted on islands or protected against collision damage by barriers or curbs. Dispensing equipment, hoses and nozzles should be inspected regularly for leaks, damage and malfunctions. Safety features may be installed on fuel dispensers such as emergency breakaway devices on hoses, which retain liquid on each side of the break point, and impact valves with fusible links at the base of dispensers, which close automatically in event of severe impact or fire.
Government regulations and company policies may require that signs be posted in dispensing areas similar to the following signs, which are required in the United States:
- “No Smoking—Shut off engine”
- “WARNING: It is unlawful and dangerous to dispense gasoline into unapproved containers”
- “Federal Law prohibits the introduction of any gasoline containing lead or phosphorus into any motor vehicle labelled UNLEADED GASOLINE ONLY”
- “UNLEADED GASOLINE”, posted at unleaded gasoline dispensers and “CONTAINS LEAD ANTIKNOCK COMPOUNDS”, posted at leaded gasoline dispensers.
Fuelling vehicles
Service station employees should know where the fuel dispenser pump emergency shut-off switches are located and how to activate them, and should be aware of potential hazards and procedures for safely dispensing fuel into vehicles, such as the following:
- Vehicle engines should be shut off and smoking prohibited while fuelling to reduce the hazards of accidental vehicle movement, spills and fuel vapour ignition.
- When fuel is dispensed, the nozzle should be inserted into the vehicle’s fill pipe and contact between the nozzle and the fill pipe maintained to provide for an electric bond until the delivery has been completed. Nozzles should not be blocked open with fuel caps or other objects. Where allowed, approved latches should be used to hold open automatic nozzles.
- Vehicles such as cement mixers and recreation vehicles with auxiliary internal combustion engines should not be fuelled until both the vehicle’s engines and auxiliary engines are shut off. Care should be taken when fuelling recreational or other vehicles equipped with gas-fired stoves, refrigerators and water heaters to ensure that fuel vapours are not ignited by pilot lights. Employees should not fuel trucks while standing on the side rail, truck bed or fuel tank.
- Fuel tanks on motorcycles, motor bicycles, fork-lift trucks and similar vehicles should not be filled while the engine is running or when anyone is seated on the vehicle. The tanks should be filled at a slow rate to prevent fuel spills that could run onto hot engines and start fires.
- After fuelling, hose nozzles should be promptly replaced on the dispensers, pumps turned off and caps replaced on fill pipes or containers.
Filling portable fuel containers
Service stations should establish procedures such as the following for safely dispensing fuel into portable containers:
- Where required by government regulation or company policies, fuel should be dispensed only into approved, properly identified and labelled portable containers, with or without dispensing spouts, nozzles or hoses and equipped with vents and screw tops or self-closing gravity, spring action or combination fusible link covers designed to provide pressure relief.
- Containers should be placed on the ground and filled slowly to avoid splash filling and overfills and to provide for grounding (earthing). Containers should not be filled while in a vehicle or in the bed of a truck, particularly one with a plastic liner, as proper grounding cannot be achieved. Bonding wires and clamps should be provided and used, or contact should be maintained between dispenser nozzles and containers to provide a bond while filling, and between container spouts or funnels and tanks during refuelling from containers.
- When pouring fuel from containers which do not have built-in spouts, funnels should be used to minimize spillage and avoid splash filling.
- Portable containers which contain fuel or vapours should be properly stored in approved storage cabinets or rooms away from sources of heat and ignition.
Storage tanks, fill pipes, fill caps and vents
Service station underground and aboveground storage-tank gauge and fill-caps should be kept closed except when filling and gauging to minimize release of fuel vapours. When tank-gauge openings are located inside buildings, spring-loaded check valves or similar devices should be provided to protect each of the openings against fluid overflow and possible vapour release. Storage-tank vents should be located in accordance with government regulations and company policy. Where venting to open air is permitted, vent-pipe openings from both underground and aboveground storage tanks should be located at a high level so that flammable vapours are directed away from potential sources of ignition and will not enter windows or air intakes or doors or become trapped under eaves or overhangs.
Improper mixing of different products during deliveries may be caused by lack of identification or improper colour coding or markings on storage tanks. Storage-tank covers, fill pipes, caps and fill-box rims or pads should be properly identified as to products and grades so as to reduce the potential of a delivery into the wrong tank. Identification symbols and colour coding should conform to government regulations, company policies or industry standards, such as the American Petroleum Institute’s (API) Recommended Practice 1637, Using the API Color Symbol System to Mark Equipment and Vehicles for Product Identification at Service Stations and Distribution Terminals. A chart indicating the symbols or colour codes in use should be available at the service station during deliveries.
Delivery of fuel to service stations
Service stations should establish and implement procedures such as the following, for the safe delivery of fuel into aboveground and underground service station storage tanks:
Prior to delivery
- Vehicles and other objects should be moved from the area where the delivery tank truck and delivery hoses will be located.
- Delivery tank trucks should be positioned away from traffic areas, and vehicles should be restricted from driving near the unloading area or over hoses by the use of traffic cones or barriers.
- Receiving storage tanks should be gauged prior to delivery to determine if there is sufficient capacity, and checked to see if any water is in the tank.
- Drivers should assure that fuel is delivered into the correct tanks, that gauge caps are replaced before starting delivery and that all tank openings not being used for delivery are covered.
- Where required by company policies or government regulation, the tank truck vapour recovery system should be connected to the receiving storage tank prior to starting delivery.
During delivery
- Drivers should monitor the area near the receiving tank’s vents for potential ignition sources and check that the vents operate properly during delivery.
- Drivers should remain where they can observe the delivery and be able to stop delivery or take other appropriate action in event of an emergency, such as ejection of liquid from vents or if an overfill device or tank vent alarm activates.
After delivery
- Storage tanks may be gauged after delivery to verify that specific tanks have received the correct products and the proper amount of products as indicated on the delivery ticket or record. Samples may be taken from the tanks after delivery for quality-control purposes.
- After delivery, spill containment devices should be drained if necessary and the correct fill and gauge caps and storage tank covers replaced on the proper tanks.
Other Service Station Functions
Storage of flammable and combustible liquids
Government regulations and company policies may control the storage, handling and dispensing of flammable and combustible liquids and automotive chemicals such as paints, starter fluids, antifreeze, battery acids, window washer fluids, solvents and lubricants in service stations. Service stations should store aerosols and flammable liquids in closed containers in approved, well-ventilated areas, away from sources of heat or ignition, in appropriate flammable liquid rooms, lockers or cabinets, or in separate, outside buildings.
Electrical safety and lighting
Service station employees should be familiar with electrical safety fundamentals applicable to service stations, such as the following:
- Lighting and electrical installations, equipment and fixtures of the proper electrical classification should be provided and maintained in accordance with codes and regulations and should not be replaced by equipment of lesser classification.
- Electric tools, water coolers, ice machines, refrigerators and similar electrical equipment should be properly grounded (earthed). Portable lights should be protected against breakage to minimize the chance that a spark might ignite flammable vapours in case bulbs break.
Adequate illumination should be provided at appropriate locations in service stations to reduce the potential for accidents and injuries. Government regulations, company policies or voluntary standards may be used to determine appropriate illumination levels. See table 1.
Table 1. Illumination levels for service station areas.
|
Service station area |
Suggested foot candles |
|
Active traffic areas |
20 |
|
Storage areas and stockrooms |
10–20 |
|
Washrooms and waiting areas |
30 |
|
Dispenser islands, work benches and cashier areas |
50 |
|
Service, repair, lubrication and washing areas |
100 |
|
Offices |
100–150 |
Source: ANSI 1967.
Lockout/tagout
Service stations should establish and implement lockout/tagout procedures to prevent the release of potentially hazardous energy while performing maintenance, repair and service work on electrical, mechanical, hydraulic and pneumatic powered tools, equipment, machinery and systems such as lifts, hoists and jacks, lubrication equipment, fuel-dispenser pumps and compressors. Safe work procedures to prevent the accidental start-up of vehicle engines during servicing or repair should include disconnecting the battery or removing the key from the ignition.
Service station fluids
Fluid and coolant levels
Before working under a hood (bonnet), employees should assure that it will stay open by testing the tension or using a rod or brace. Employees should exercise caution when checking vehicle engine fluids to avoid burns from exhaust manifolds and to prevent contact between dipsticks and electrical terminals or wires; care is also necessary when checking transmission fluid levels (since the engine must be running). Employees should follow safe work procedures when opening radiators, such as allowing pressurized radiators to cool and covering radiator caps with a heavy cloth when opening, using PPE and standing with face turned away from radiators so as to not inhale any escaping steam or vapours.
Antifreeze and window washer fluids
Employees servicing vehicles should be aware of the hazards of both glycol and alcohol antifreezes and window washer fluid concentrates and how to safely handle them. This includes precautions such as storing alcohol-based products in tightly closed drums or packaged containers, in separate rooms or lockers, away from all heating equipment, and providing containment to prevent contamination of drains and ground in the event of a spill or leak of glycol-type antifreeze. Antifreeze or washer fluid should be dispensed from upright drums by using tightly connected hand pumps equipped with drip returns, rather than by using faucets or valves on horizontal drums, which may leak or be knocked open or broken off, causing spills. Air pressure should not be used to pump antifreeze or washer fluid concentrates from drums. Empty portable antifreeze and washer fluid concentrate containers should be completely drained prior to disposal, and applicable regulations governing the disposal of glycol antifreeze solutions should be followed.
Lubrication
Service stations should ensure that employees are aware of the characteristics and uses of the different fuels, oils, lubricants, greases, automotive fluids and chemicals available in the facility and their correct selection and application. The proper tools should be used to remove crankcase, transmission and differential drains, test plugs and oil filters so as to not damage vehicles or equipment. Pipe wrenches, extenders and chisels should be used only by employees who know how to safely remove frozen or rusted plugs. Because of the potential hazards involved, high-pressure lubricating equipment should not be started until the nozzles are set firmly against grease fittings. If testing is to be done prior to use, the nozzle should be aimed into an empty drum or similar receptacle, and not into a hand-held rag or cloth.
Lift operations
Employees working in and around vehicle service areas should be aware of unsafe conditions and follow safe work practices such as not standing in front of vehicles while they are being driven into service bays, over lubrification pits or onto lifts, or when vehicles are being lifted.
- Vehicles should be properly aligned on two-rail, free-wheel or frame-contact lifts, since an off-centre position may cause a vehicle to fall.
- Lifts should not be raised until occupants have left the vehicles and a check of overhead clearance has been made.
- Once the vehicle is in position, the emergency stop device should be set so the lift will not fall in the event of a pressure drop. If a lift is in a position where the emergency stop device cannot be engaged, blocks or safety stands should be placed under the lift or vehicle.
- A hydraulic lift may be equipped with a low-oil control valve, which prevents operation if the oil in the supply tank falls below a minimum level, since the lift can drop accidentally under those conditions.
When wheel-bearing lubrication, brake repair, tyre changing or other services are performed on free-wheel or frame-contact lifts, vehicles should be raised slightly above the floor to allow employees to work from a squatting position, to reduce the possibility of back strain. After vehicles are raised, the wheels should be blocked to prevent rolling, and safety stands should be placed underneath for support in case of jack or lift failure. When removing wheels from vehicles on drive-on lifts, the vehicles should be blocked securely to prevent rolling. If jacks or stands are used to lift and support vehicles, they should be of the proper capacity, placed at appropriate lift points on the vehicles and checked for stability.
Servicing tyres
Employees should be aware of how to safely check pressures and inflate tyres; tyres should be inspected for excessive wear, maximum tyre pressures should not be exceeded, and the worker should stand or kneel to the side and turn the face when inflating tyres. Employees should be aware of hazards and follow safe work practices when servicing wheels with multi-piece and single-piece rims and lock-ring-rim wheels on trucks and trailers. When repairing tyres with flammable or toxic patching compounds or liquids, precautions such as controlling ignition sources, using PPE and providing adequate ventilation, should be observed.
Parts cleaning
Service station employees should be aware of the fire and health hazards of using gasoline or low-flashpoint solvents to clean parts and should follow safe practices such as using approved solvents with a flashpoint above 60ºC. Parts washers should have a protective cover that is kept closed when the washer is not in use; when the washer is open, there should be a hold-open device such as fusible links, which allows the cover to close automatically in case of fire.
Employees should take precautions so that gasoline or other flammable liquids do not contaminate the cleaning solvent and lower its flashpoint to create a fire hazard. Contaminated cleaning solvent should be removed and placed in approved containers for proper disposal or recycling. Employees who clean parts and equipment using cleaning solvents should avoid skin and eye contact and use appropriate PPE. Solvents should not be used for hand-washing and other personal hygiene.
Compressed air
Safe work practices should be established by service stations for the operation of air compressors and the use of compressed air. The air hoses should be used only for inflating tyres and for lubrication, maintenance and auxiliary services. Employees should be aware of the hazards of pressurizing fuel tanks, air horns, water tanks and other non-air pressure containers. Compressed air should not be used for cleaning or to blow residue from vehicle brake systems, since many brake linings, especially on older model vehicles, contain asbestos. Safer methods such as cleaning with vacuums or liquid solutions should be used.
Storage battery service and handling
Service stations should establish procedures to ensure that storage, handling and disposal of batteries and battery electrolyte fluids follow government regulations and company policies. Employees should be aware of the hazards of electrical short circuits when charging, removing, installing or handling batteries; disconnect the ground (negative) cable first before removing batteries; and reconnect the ground (negative) cable last when installing batteries. When removing and replacing batteries, a carrier may be used to facilitate lifting and to avoid touching the battery.
Employees should be aware of safe practices such as the following for handling battery solution:
- Containers of electrolyte solution should be stored at temperature ranges between 16 and
32ºC in safe areas where they cannot overturn. Any electrolyte solution spilled on the batteries or in the filling area should be flushed with water. Baking soda (sodium bicarbonate) may be used on spills, since it is an effective neutralizer for battery electrolyte solution.
- New batteries should be placed on the floor or work table when being filled with electrolyte solution, and the caps should be replaced prior to installation. New batteries should not be filled when they are inside vehicles.
- Face shields and chemical goggles, aprons and gloves may be used to minimize exposure to battery solution. Battery solution should be handled and dispensed where a supply of potable water or eye wash fluid is available, in case the battery solution spills or contacts an employee’s skin or eyes. Do not use neutralizing solutions on skin or eyes.
- When servicing batteries, corrosive particles which accumulate around the terminals should be brushed away, washed with clean water, neutralized with baking soda or other similar agents and prevented from contacting eyes or clothing.
Employees should check fluid levels in batteries prior to charging and periodically check them during charging to determine whether batteries are overheating. Chargers should be turned off before disconnecting cables from batteries, to avoid creating sparks which may ignite hydrogen gas generated during the charge. When “quick charging” batteries are installed in vehicles, the vehicles should be moved away from the fuel-dispensing islands, and the battery ground (negative) cables should be disconnected before connecting the charger units. If the batteries are located within passenger compartments or under vehicle floorboards, they should be removed before charging.
Employees should be familiar with the hazards and safe procedures to “jump start” vehicles that have dead batteries, in order to avoid electrical system damage or injury from exploding batteries if the jumper cables are hooked up incorrectly. Employees should never jump start or charge frozen batteries.
Driving vehicles and towing
Employees should be trained, qualified and have proper motor vehicle operator’s licences to drive customer or company vehicles, service trucks or towing equipment either on or off the premises. All vehicles should be operated in compliance with government regulations and company policies. Operators should check the vehicle’s brakes immediately, and vehicles with faulty brakes should not be driven. Employees operating tow trucks should be familiar with safe operating procedures, such as operating the hoist, checking the transmission and frame of the vehicle to be towed and not exceeding the tow truck’s maximum lifting capacity.
Confined spaces in service stations
Service station employees should be aware of the hazards associated with entry into confined spaces such as aboveground and underground tanks, sumps, pump pits, waste containment tanks, septic tanks and environmental collection wells. Unauthorized entry should not be allowed, and confined-space entry permit procedures should be established that apply to both employee and contractor entrants.
Emergency procedures
Service stations should develop emergency procedures, and employees should know how to sound the alarms, how to notify authorities of emergencies when and how to evacuate and what appropriate response actions should be taken (such as shutting off emergency switches in the event of spills or fires in the dispensing pump areas). Service stations may establish security programmes to familiarize employees with robbery and violence prevention, depending on the service station’s location, hours of operation and potential threats.
Service Station Health and Safety
Fire protection
Gasoline vapours are heavier than air and may travel long distances to reach sources of ignition when released during fuel filling, spills, overflows or repairs. Proper ventilation should be provided in enclosed areas to allow for dissipation of gasoline vapours. Fires may occur from spills and overflows when fuelling or servicing vehicles or delivering product into service station tanks, particularly if smoking is not restricted or if vehicle engines remain running during fuelling. To avoid fires, vehicles should be pushed away from spill areas or the spilled gasoline should be cleaned from under or around vehicles before starting their engines. Vehicles should not be permitted to enter or drive through spills.
Employees should be aware of other causes of fires in service stations, such as improper handling, transfer and storage of flammable and combustible liquids, accidental releases during fuel system repairs, electrostatic discharge when changing filters on gasoline dispensers and the use of improper or unprotected work lights. Draining gasoline from vehicle fuel tanks could be very hazardous due to the potential for release of fuel and vapours, especially in enclosed service areas when sources of ignition may be present.
Hot-work permits should be issued when work other than vehicle repair and servicing is performed which introduces sources of ignition in areas where flammable vapours may be present. Employees should be aware that carburettor priming should not be attempted while vehicle engines are running or being turned over with their starters, since flashbacks could ignite the fuel vapours. Employees should follow safe procedures, such as using starter fluid and not gasoline for priming carburettors and using clamps to hold the chokes open while attempting to start the engine.
Although government regulations or company policies may require the installation of fixed fire-protection systems, fire extinguishers are usually the primary means of fire protection in service stations. Service stations should provide fire extinguishers of the proper classification for the expected hazards. Fire extinguishers and fixed fire protection systems should be regularly inspected, maintained and serviced, and employees should know when, where and how to use the fire extinguishers and how to activate the fixed systems.
Service stations should install fuel-dispenser emergency shut-down controls at clearly identified and accessible locations and ensure that employees know the purpose, location and operation of these controls. To prevent spontaneous combustion, oily rags should be kept in covered metal containers until they are recycled or discarded.
Safety
Employee injuries at service stations may result from improper use of tools, equipment and ladders; not wearing PPE; falling or tripping; working in awkward positions; and lifting or carrying cases of materials incorrectly. Injuries and accidents may also occur from not following safe practices when working on hot radiators, transmissions, engines and exhaust systems, servicing tyres and batteries, and working with lifts, jacks, electrical equipment and machinery; from robbery and assault; and from improper use of or exposure to automotive cleaners, solvents and chemicals.
Service stations should develop and implement programmes to prevent accidents and incidents which can be attributed to problems associated with service station physical conditions, such as poor maintenance, storage and housekeeping practices. Other factors contributing toward accidents in service stations include employees’ lack of attention, training or skills, which may result in the improper use of equipment, tools, automotive parts, supplies and maintenance materials. Figure 1 provides a safety checklist.
Figure 1. Service station safety and health checklist.

Robberies are a major safety hazard in service stations. Appropriate precautions and training are discussed in the accompanying box and elsewhere in this Encyclopaedia.
Health
Employees should be aware of health hazards associated with working in service stations, such as the following:
Carbon monoxide. Internal combustion engine exhaust gases contain carbon monoxide, a highly toxic, odourless and colourless gas. Employees should be aware of the dangers of exposure to carbon monoxide, particularly when vehicles are inside service bays, garages or car washes with their engines running. Vehicle exhaust gases should be piped outside through flexible hoses, and ventilation should be provided to assure an adequate supply of fresh air. Fuel oil appliances and heaters should be checked to assure that carbon monoxide is not vented to inside areas.
Toxicity of petroleum fuels. Employees who come in contact with gasoline, diesel fuel, heating oil or kerosene should be aware of the potential hazards of exposure and know how to handle these fuels safely. Inhaling sufficient concentrations of petroleum fuel vapours for extended periods of time may result in mild intoxication, anaesthesia or more serious conditions. Short exposure to high concentrations will cause dizziness, headaches and nausea, and irritate the eyes, nose and throat. Gasoline, solvents or fuel oils should never be siphoned from containers or tanks by mouth, since the toxicity of low viscosity liquid hydrocarbons aspired directly into the lungs is 200 times greater than if they are ingested. Aspiration into the lungs may cause pneumonia with extensive pulmonary oedema and haemorrhage, leading to serious injury or death. Vomiting should not be induced. Immediate medical assistance should be sought.
Benzene. Service station employees should be aware of the potential hazards of benzene, which is found in gasoline, and avoid inhaling gasoline vapours. Although gasoline contains benzene, low-level exposure to gasoline vapours is unlikely to cause cancer. Numerous scientific studies have shown that service station employees are not exposed to excessive levels of benzene during the course of their normal work activities; however, there is always the possibility that overexposure could occur.
Dermatitis hazards. Employees who handle and come into contact with petroleum products as part of their jobs should be aware of the hazards of dermatitis and other skin disorders and the personal hygiene and personal protective measures needed to control exposure. If eye contact with gasoline, lubricants or antifreeze occurs, the eyes should be flushed with clean, lukewarm potable water, and medical assistance should be provided.
Lubricants, used motor oil and automotive chemicals. Employees who change oil and other motor vehicle fluids, including antifreeze, should be aware of the hazards and know how to minimize exposure to products such as gasoline in used motor oil, glycol in antifreeze and other contaminants in transmission fluids and gear lubricants by the use of PPE and good hygiene practices. If high-pressure lubricating guns are discharged against an employee’s body, the affected area should be examined immediately to see if petroleum products have penetrated the skin. These injuries cause little pain or bleeding, but involve almost instant separation of the skin tissues and possible deeper damage, which should receive immediate medical attention. The attending physician should be informed of the cause and the product involved in the injury.
Welding. Welding, besides being a fire hazard, can involve exposure to lead pigments from welding on car exteriors, as well as metal fumes and welding gases. Local exhaust ventilation or respiratory protection is needed.
Spray painting and auto body fillers. Spray painting can involve exposure to solvent vapours and pigment particulates (e.g., lead chromate). Auto body fillers often are epoxy or polyester resins and can involve skin and respiratory hazards. Drive-in spray booths for spray painting, local exhaust ventilation and skin and eye protection are recommended while using auto body fillers.
Storage batteries. Batteries contain corrosive electrolyte solutions of sulphuric acid that can cause burns and other injuries to the eyes or skin. Exposure to battery solution should be minimized by the use of PPE, including rubber gloves and eye protection. Employees should immediately flush electrolyte solution from the eyes or skin with clean potable water or eye wash fluid for at least 15 minutes and seek immediate medical attention. Employees should thoroughly wash their hands after servicing batteries and keep their hands away from the face and eyes. Employees should be aware that overcharging batteries can create explosive and toxic quantities of hydrogen gas. Because of the potential harmful effects of exposure to lead, used storage batteries should be properly disposed of or recycled in accordance with government regulations or company policies.
Asbestos. Employees who check and service brakes should be aware of the hazards of asbestos, know how to recognize whether brake shoes contain asbestos and take appropriate protective measures to reduce exposure and contain waste for proper disposal (see figure 2).
Figure 2. Portable enclosure for preventing exposure to asbestos dust from brake drums It is equipped with an enclosed compressed-air gun with a cotton sleeve and is connected to a HEPA vacuum cleaner.

Courtesy of Nilfisk of America, Inc.
Personal protective equipment (PPE)
Injuries to employees may occur from contact with automotive fuels, solvents and chemicals or from chemical burns caused by exposure to battery acids or caustic solutions. Service station employees should be familiar with the need to use and wear PPE such as the following:
- Work shoes with oil- and slip-resistant soles should be worn for general work in service stations, and approved protective-toe safety shoes with oil/slip-resistant soles should be worn where there is a danger of foot injuries due to rolling or falling objects or equipment.
- Safety goggles and respiratory protection should be used for protection against exposures to chemicals, dust or steam, such as when painting or working around batteries and radiators. Industrial safety glasses or face shields with goggles should be worn when the potential exists for exposure to impact materials, such as working with grinders or wire buffers, repairing or mounting tyres, or replacing exhaust systems. Welding glasses should be worn when cutting or welding to prevent flash burns and injuries from particles.
- Impervious gloves, aprons, footwear, face shields and chemical goggles should be worn when handling automotive chemicals and solvents, battery acid and caustic solutions and when cleaning up chemical or fuel spills. Leather work gloves should be worn when handling sharp objects such as broken glass, motor vehicle parts or tyre rims and while emptying trash cans.
- Head protection may be needed when working beneath vehicles in pits or changing overhead signage or lights and in other areas where a potential exists for injury to the head.
- Employees working on vehicles should not wear rings, wristwatches, bracelets or long chains, since the jewellery may contact the vehicle’s moving parts or electrical system and cause injury.
To prevent fires, dermatitis or chemical burns to the skin, clothing that is soaked with gasoline, antifreeze or oil should be immediately removed in an area or room with good ventilation and where no sources of ignition, such as electric heaters, engines, cigarettes, lighters or electric hand dryers, are present. The affected areas of the skin should then be thoroughly washed with soap and warm water to remove all traces of contamination. Clothing should be air dried outside or in well-ventilated areas away from sources of ignition before laundering to minimize contamination of wastewater systems.
Service Station Environmental Issues
Storage tank inventory control
Service stations should maintain and reconcile accurate inventory records on all gasoline and fuel oil storage tanks on a regular basis to control losses. Manual stick gauging may be used to provide a check of the integrity of underground storage tanks and connecting pipes. Where automatic gauging or leak detection equipment is installed, its accuracy should be verified regularly by manual stick gauging. Any storage tank or system suspected of leaking should be investigated, and if leakage is detected, the tank should be made safe or emptied and repaired, removed or replaced. Service station employees should be aware that leaking gasoline can travel long distances underground, contaminate water supplies, enter sewer and drainage systems and cause fires and explosions.
Handling and disposal of waste materials
Waste lubricants and automotive chemicals, used motor oil and solvents, spilled gasoline and fuel oil and glycol-type antifreeze solutions should be drained into approved, properly labelled tanks or containers and stored until disposed of or recycled in accordance with government regulations and company policies.
Because engines with worn cylinders or other defects may allow small amounts of gasoline to enter their crankcases, precautions are needed to prevent vapours which could be released from tanks and containers with crankcase drainings from reaching sources of ignition.
Used oil filters and transmission fluid filters should be drained of oil prior to disposal. Used fuel filters which have been removed from vehicles or fuel dispenser pumps should be drained into approved containers and stored in well-ventilated locations away from sources of ignition until dry before disposal.
Used battery-electrolyte containers should be thoroughly rinsed with water before discarding or recycling. Used batteries contain lead and should be properly disposed of or recycled.
Cleaning large spills may require special training and PPE. Recovered spilled fuel may be returned to the terminal or bulk plant or otherwise disposed of according to government regulations or company policy. Lubricants, used oil, grease, antifreeze, spilled fuel and other materials should not be swept, washed or flushed into floor drains, sinks, toilets, sewers, sumps or other drains or the street. Accumulated grease and oil should be removed from floor drains and sumps to prevent these materials from flowing into sewers. Asbestos dust and used asbestos brake linings should be handled and disposed of according to government regulations and company policies. Employees should be aware of the environmental impact and potential health, safety and fire hazards of these wastes.
Ergonomics of Bus Driving
Bus driving is characterized by psychological and physical stresses. Most severe are the stresses of traffic in big cities, because of the heavy traffic and frequent stops. In most transit companies, the drivers must, in addition to driving responsibilities, handle tasks such as selling tickets, observing passenger loading and unloading and providing information to passengers.
Psychological stresses result from the responsibility for the safe transport of passengers, scant opportunity to communicate with colleagues and the time pressure of holding to a fixed schedule. Rotating shift work is also psychologically and physically stressful. Ergonomic shortcomings in the driver’s workstation increase physical stresses.
Numerous studies of the activity of bus drivers have shown that the individual stresses are not great enough to cause an immediate health hazard. But the sum of the stresses and the resulting strain leads to bus drivers having more frequent health problems than other workers. Especially significant are diseases of the stomach and digestive tract, of the motor system (especially the spine) and of the cardiovascular system. This results in drivers often not reaching retirement age, but rather having to quit driving early for health reasons (Beiler and Tränkle 1993; Giesser-Weigt and Schmidt 1989; Haas, Petry and Schühlein 1989; Meifort, Reiners and Schuh 1983; Reimann 1981).
In order to achieve more effective occupational safety in the field of commercial driving, technical as well as organizational measures are necessary. An important work practice is the arranging of shift schedules so that the stress on the drivers is minimized and their personal desires are also taken into account to the extent possible. Informing the personnel of and motivating them to health-conscious conduct (e.g., proper diet, adequate movement within and outside of the workstation) can play an important role in promoting health. An especially necessary technical measure is the ergonomically optimal design of the driver’s workstation. In the past, the requirements of the driver’s workstation were considered only after other requirements, such as design of the passenger area. Ergonomic design of the driver’s workstation is a necessary component of driver safety and health protection. In recent years, research projects on, among other things, the ergonomically optimal driver’s workstation were conducted in Canada, Sweden, Germany and the Netherlands (Canadian Urban Transit Association 1992; Peters et al. 1992; Wallentowitz et al. 1996; Streekvervoer Nederland 1991). The results of the interdisciplinary project in Germany resulted in a new, standardized driver’s workstation (Verband Deutscher Verkehrsunternehmen 1996).
The driver’s workstation in buses is normally designed in the form of a half-open cabin. The measurements of the driver’s cabin and the adjustments that can be made to the seat and steering wheel must fall within a range that is applicable to all drivers. For central Europe, this means a body-size range of 1.58 to 2.00 m. Special proportions, such as being overweight and having long or short limbs, should also be taken into account in the design.
The adjustability and the ways of adjusting the driver’s seat and steering wheel should be coordinated so that all drivers within the design range can find positions for their arms and legs that are comfortable and ergonomically healthy. For this purpose, the optimal seat placement has a back incline about 20°, which is further from the vertical than has previously been the norm in commercial vehicles. Furthermore, the instrument panel should also be adjustable for optimal access to adjustment levers and for good visibility of the instruments. This can be coordinated with the steering wheel adjustment. Using a smaller steering wheel also improves spatial relations. The steering wheel diameter now in general use apparently comes from a time when power steering was not common in buses. See figure 1.
Figure 1. Ergonomically optimized and unified driver's workstation for busses in Germany.

Courtesy of Erobus GmbH, Mannheim, Germany
The instrument panel with the controls can be adjusted in coordination with the steering wheel.
Since stumbling and falling are the most common causes of workplace accidents among drivers, particular attention should be paid to the design of the entrance to the driver’s workstation. Anything that can be stumbled on should be avoided. Steps in the entrance area must be of equal height and have adequate step depth.
The driver’s seat should have a total of five adjustments: seat length and height settings, seat back angle, seat bottom angle and seat depth. Adjustable lumbar support is strongly advised. To the extent that it is not already legally required, equipping the driver’s seat with a three-point seat-belt and head rest are recommended. Since experience shows that manually adjusting to the ergonomically right position is time-consuming, in the future some way of electronically storing the adjustment functions listed in table 1 should be used, allowing for quickly and easily refinding the individual seating adjustment (e.g., by entering it onto an electronic card).
Table 1. Bus driver seat measurements and seat adjustment ranges.
|
Component |
Measurement/ |
Standard value |
Adjustment range |
Memorized |
|
Entire seat |
Horizontal |
— |
≥ 200 |
Yes |
|
Vertical |
— |
≥ 100 |
Yes |
|
|
Seat surface |
Seat surface depth |
— |
390–450 |
Yes |
|
Seat surface width (total) |
Min. 495 |
— |
— |
|
|
Seat surface width (flat part, in pelvic area) |
430 |
— |
— |
|
|
Side upholstering in pelvic area (crosswise) |
40–70 |
— |
— |
|
|
Depth of seat recess |
10–20 |
— |
— |
|
|
Seat surface slope |
— |
0–10° (rising toward front) |
Yes |
|
|
Seatback |
Seatback height |
|||
|
Min. height |
495 |
— |
— |
|
|
Max. height |
640 |
— |
— |
|
|
Seatback width (total)* |
Min. 475 |
— |
— |
|
|
Seatback width (flat part) |
||||
|
—lumbar area (lower) |
340 |
— |
— |
|
|
—shoulder area (upper) |
385 |
— |
— |
|
|
Seatback |
Side upholstering* (side depth) |
|||
|
—lumbar area (lower) |
50 |
— |
— |
|
|
—shoulder area (upper) |
25 |
— |
— |
|
|
Seatback slope (to vertical) |
— |
0°–25° |
Yes |
|
|
Headrest |
Height of headrest upper edge above seat surface |
— |
Min. 840 |
— |
|
Height of headrest itself |
Min. 120 |
— |
— |
|
|
Width of headrest |
Min. 250 |
— |
— |
|
|
Lumbar pad |
Forward arch of lumbar support from lumbar surface |
— |
10–50 |
— |
|
Height of lumbar support lower edge over seat surface |
— |
180–250 |
— |
– Not applicable
* The width of the lower part of the backrest should correspond approximately to the width of the seat surface and grow narrower as it goes up.
** The side upholstering of the seat surface applies only to the recess area.
Stress through whole-body vibrations in the driver’s workstation is low in modern buses compared to other commercial vehicles, and it falls well below the international standards. Experience shows that driver’s seats in buses are often not optimally adjusted to the vehicle’s actual vibration. An optimal adaptation is advised to avoid certain frequency ranges causing an increase in whole-body vibration on the driver, which can interfere with productivity.
Noise levels that are a hazard to hearing are not anticipated in the bus driver’s workstation. High-frequency noise can be irritating and should be eliminated because it could interfere with the drivers’ concentration.
All adjustment and service components in the driver’s workstation should be arranged for comfortable access. A large number of adjustment components are often required due to the amount of equipment added to the vehicle. For this reason, switches should be grouped and consolidated according to use. Frequently used service components such as door openers, bus stop brakes and windshield wipers should be placed in the main access area. Less frequently used switches can be located outside the main access area (e.g., on a side console).
Analyses of visual movements have shown that driving the vehicle in traffic and observing the loading and unloading of passengers at the stops is a serious burden on the driver’s attention. Thus, the information conveyed by instruments and indicator lights in the vehicle should be limited to those absolutely necessary. Vehicle computerized electronics offer the possibility of eliminating numerous instruments and indicator lights, and instead installing a liquid crystal display (LCD) in a central location to convey information, as shown in the instrument panel in figure 2 and figure 3.
Figure 2. View of an instrument panel.

Courtesy of Erobus GmbH, Mannheim, Germany
With the exception of the speedometer and a few legally required indicator lights, the functions of the instrument and indicator displays have been assumed by a central LCD display.
Figure 3. Illustration of an instrument panel with legend.
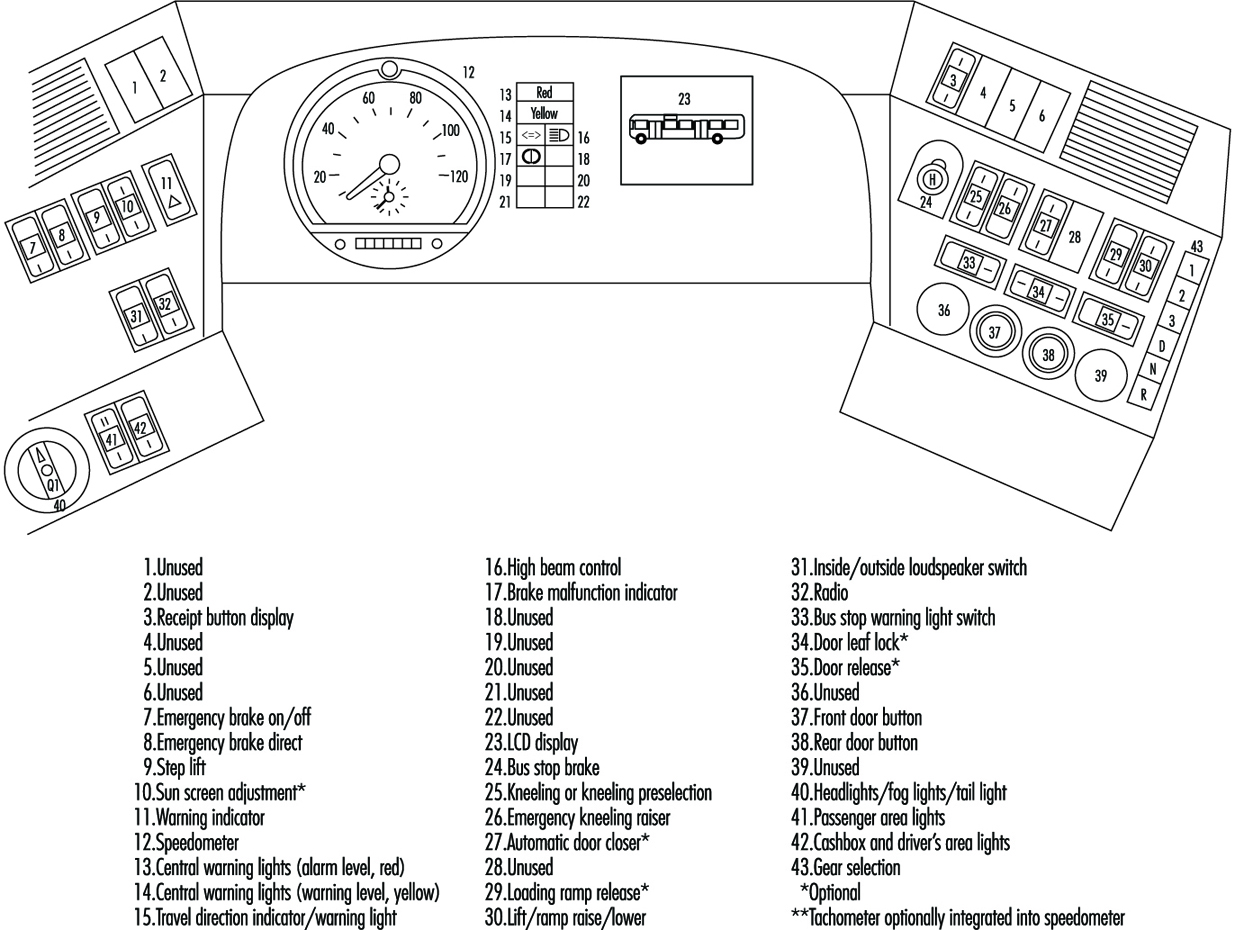
With the proper computer software, the display will show only a selection of information that is needed for the particular situation. In the case of malfunction, a description of the problem and brief instructions in clear text, rather than in difficult-to- understand pictograms, can provide the driver with important assistance. A hierarchy of malfunction notifications can also be established (e.g., “advisory” for less significant malfunctions, “alarm” when the vehicle must be stopped immediately).
Heating systems in buses often heat the interior with warm air only. For real comfort, however, a higher proportion of radiant heat is desirable (e.g., by heating the side walls, whose surface temperature often lies significantly below the interior air temperature). This, for example, can be achieved by circulating warm air through perforated wall surfaces, which thereby will also have the right temperature. Large window surfaces are used in the driver’s area in buses to improve visibility and also for appearance. These can lead to a significant warming of the inside by sun rays. The use of air conditioning is thus advisable.
The air quality of the driver’s cabin depends heavily on the quality of the outside air. Depending on the traffic, high concentrations of harmful substances, such as carbon monoxide and diesel motor emissions, can briefly occur. Providing fresh air from less-used areas, such as the roof instead of the vehicle front, lessens the problem significantly. Fine-particle filters should also be used.
In most transit companies, an important part of the driving personnel’s activity consists of selling tickets, operating devices to provide information to passengers and communicating with the company. Until now, separate devices, located in the available work space and often hard for the driver to reach, have been used for these activities. An integrated design should be sought from the start that arranges the devices in an ergonomically convenient manner in the driver’s area, especially the input keys and display panels.
Finally, the assessment of the driver’s area by the drivers, whose personal interests should be taken into account, is of great importance. Supposedly minor details, such as placement of the driver’s bag or storage lockers for personal effects, are important for driver satisfaction.
Truck and Bus Driving
Transport by road includes the movement of people, livestock and freight of all kinds. Freight and livestock generally move in some form of truck, although buses often carry packages and passenger baggage and may transport fowl and small animals. People generally move by bus on the road, although in many areas trucks of various kinds serve this function.
Truck (lorry) drivers may operate several different types of vehicles, including, for example, semi-trailers, tanker trucks, dump trucks, double and triple trailer combinations, mobile cranes, delivery trucks and panel or pickup vehicles. Legal gross vehicle weights (which vary by jurisdiction) range from 2,000 kg to over 80,000 kg. Truck cargo may include any imaginable item—for example, small and large packages, machinery, rock and sand, steel, lumber, flammable liquids, compressed gases, explosives, radioactive materials, corrosive or reactive chemicals, cryogenic liquids, food products, frozen foods, bulk grain, sheep and cattle.
In addition to driving the vehicle, truck drivers are responsible for inspecting the vehicle prior to use, checking shipping papers, verifying that proper placards and markings are in place and maintaining a log book. Drivers may also be responsible for servicing and repairing the vehicle, loading and unloading cargo (either by hand or using a fork truck, crane or other equipment) and collecting money received for goods delivered. In the event of an accident, the driver is responsible for securing the cargo and summoning assistance. If the incident involves hazardous materials, the driver may attempt, even without proper training or necessary equipment, to control spills, stop leaks or put out a fire.
Bus drivers may carry a few people in a small van or operate medium and large buses carrying 100 or more passengers. They are responsible for boarding and discharging passengers safely, providing information and possibly collecting fares and maintaining order. Bus drivers may also be responsible for servicing and repairing the bus and loading and unloading cargo and baggage.
Motor vehicle accidents are one of the most serious hazards facing both truck and bus drivers. This hazard is aggravated if the vehicle is not properly maintained, especially if the tyres are worn or the brake system is faulty. Driver fatigue caused by a long or irregular schedules, or by other stress, increases the likelihood of accidents. Excessive speed and hauling excessive weight add to the risk, as do heavy traffic and adverse weather conditions which impair traction or visibility. An accident involving hazardous materials may cause additional injury (toxic exposure, burns and so on) to the driver or passengers and may affect a wide area surrounding the accident.
Drivers face a variety of ergonomic hazards. The most obvious are back and other injuries caused by lifting excessive weight or using improper lifting technique. The use of back belts is quite common, although their efficacy has been questioned, and their use may create a false sense of security. The necessity of loading and unloading cargo at locations where fork-lift trucks, cranes or even dollies are not available and the great variety of package weights and configurations add to the risk of lifting injuries.
Driver’s seats are often poorly designed and cannot be adjusted to provide proper support and long-term comfort, resulting in back problems or other musculoskeletal damage. Drivers may experience damage to the shoulder caused by vibration as the arm may rest for long periods in a somewhat raised position on the window opening. Whole-body vibration can cause damage to the kidneys and back. Ergonomic injury may also result from repetitive use of poorly placed vehicle controls or fare box keypads.
Drivers are at risk of industrial hearing loss caused by long-term exposure to loud engine noises. Poor maintenance, faulty mufflers and inadequate cab insulation aggravate this hazard. Hearing loss may be more pronounced in the ear adjacent to the driver’s window.
Drivers, especially long-haul truck drivers, often work excessive hours without adequate rest. The International Labour Organization (ILO) Hours of Work and Rest Periods (Road Transport) Convention, 1979 (No. 153), requires a break after 4 hours of driving, limits total driving time to 9 hours per day and 48 hours per week and requires at least 10 hours of rest in each 24-hour period. Most nations also have laws which govern driving times and rest periods and require drivers to maintain logbooks indicating hours worked and rest periods taken. However, management expectations and economic necessity, as well as certain terms of remuneration, such as pay per load or the lack of pay for an empty return trip, put strong pressure on the driver to operate for excessive hours and to make bogus log entries. Long hours cause psychological stress, aggravate ergonomic problems, contribute to accidents (including accidents caused by falling asleep at the wheel) and may cause the driver to use artificial, addictive stimulants.
In addition to ergonomic conditions, long work hours, noise and economic anxiety, drivers experience psychological and physiological stress and fatigue caused by adverse traffic conditions, poor road surfaces, bad weather, night driving, the fear of assault and robbery, concern about faulty equipment and continuous intense concentration.
Truck drivers are potentially exposed to any chemical, radioactive or biological hazard associated with their load. Leaking containers, faulty valves on tanks and emissions during loading or unloading may cause worker exposures to toxic chemicals. Improper packaging, inadequate shielding or improper placement of radioactive cargo may allow radiation exposure. Workers transporting livestock may be infected with animal-borne infections such as brucellosis. Bus drivers are exposed to infectious diseases of their passengers. Drivers are also exposed to fuel vapours and engine exhaust, especially if there are fuel-line or exhaust system leaks or if the driver makes repairs or handles freight while the engine is running.
In the event of an accident involving hazardous materials, the driver may experience acute chemical or radiation exposures or may be injured by a fire, explosion or chemical reaction. Drivers generally lack the training or equipment to deal with hazardous materials incidents. Their responsibility should be limited to protecting themselves and summoning emergency responders. The driver faces additional risks in attempting emergency response actions for which he or she is not properly trained and adequately equipped.
The driver may be injured in the course of making mechanical repairs to the vehicle. A driver could be struck by another vehicle while working on a truck or bus alongside the road. Wheels with split rims pose a special injury hazard. Improvised or inadequate jacks may cause a crushing injury.
Truck drivers face the risk of assault and robbery, especially if the vehicle carries a valuable cargo or if the driver is responsible for collecting money for goods delivered. Bus drivers are at risk of fare box robberies and abuse or assault by impatient or inebriated passengers.
Many aspects of a driver’s life may contribute to poor health. Because they work long hours and need to eat on the road, drivers often suffer from poor nutrition. Stress and peer pressure may lead to drug and alcohol use. Using the services of prostitutes increases the risk of AIDS and other sexually transmitted diseases. The drivers appear to be one of the main vectors for carrying AIDS in some countries.
The risks described above are all preventable, or at least controllable. As with most safety and health issues, what is needed is a combination of adequate remuneration, worker training, a strong union contract and strict adherence to applicable standards on the part of management. If drivers receive adequate pay for their work, based on proper work schedules, there is less incentive to speed, work excessive hours, drive unsafe vehicles, carry overweight loads, take drugs or make bogus log entries. Management must require drivers to comply with all safety laws, including keeping an honest logbook.
If management invests in well-made vehicles and assures their regular inspection, maintenance and servicing, breakdowns and accidents can be greatly reduced. Ergonomic injury can be reduced if management is willing to pay for the well-designed cabs, fully adjustable driver’s seats and good vehicle control arrangements that are now available. Proper maintenance, especially of exhaust systems, will reduce noise exposure.
Toxic exposures can be reduced if management assures compliance with packaging, labelling, loading and placarding standards for hazardous materials. Measures which reduce vehicular accidents also reduce the risk of a hazardous materials incident.
Drivers must be given time to thoroughly inspect the vehicle prior to use and must not face any penalty or disincentive for refusing to operate a vehicle that is not functioning properly. Drivers must also receive adequate driver training, vehicle inspection training, hazard recognition training and first-responder training.
If drivers are responsible for loading and unloading, they must receive training in proper lifting technique and be provided with hand-trucks, fork-lifts, cranes or other equipment necessary to handle goods without excessive strain. If drivers are expected to make repairs to vehicles, they must be provided with the correct tools and proper training. Adequate security measures must be taken to protect drivers who transport valuables or handle passenger fares or money received for goods delivered. Bus drivers should have proper supplies for dealing with body fluids from sick or injured passengers.
Drivers must receive medical services both to assure their fitness for work and to maintain their health. Medical surveillance must be provided for drivers who handle hazardous materials or are involved in an incident with exposure to blood-borne pathogens or hazardous materials . Both management and drivers must comply with standards governing the evaluation of medical fitness.
Health Effects and Disease Patterns
The health and safety problems in the forestry and lumber industries are covered elsewhere in this Encyclopaedia. This article will deal with wood as it arrives from the mill and is used in carpentry and the making of furniture and other articles. These activities are predominantly performed in small enterprises. Many workers in these industries are individual contractors and, therefore, not listed as employees, and large numbers of individuals are exposed in do-it-yourself projects and in-home workshops. This means that many of the workers involved are inadequately trained and are supervised poorly or not at all, while proper safeguards and protective equipment are often lacking.
Ahman and colleagues (1995a, 1995b, 1996) call attention to the exposure of teachers of industrial arts and woodworking in Sweden. In contrast to unexposed controls, these teachers had notable (but mainly reversible) nasal effects and complaints that increased with the number of classes from the beginning of the week and receded over the weekends, even though the dust concentrations were below the Swedish threshold limit of 2 mg/m3. In several establishments in the Netherlands, dust levels regularly exceeded that limit, and during sanding operations in a furniture factory, almost all exposures were over the local threshold limit of 5 mg/m3 (Scheeper, Kromhout and Boleij 1995).
Accidental Injuries
The most common health problem in the wood and woodworking industries is accidental injuries. These are more frequent among younger, inexperienced workers, and, for the most part, they are relatively minor. On occasion, however, they may involve long-term impairment or loss of an extremity. They include: splinters, which may become infected, and lacerations, gouges and amputations resulting from improperly used or inadequately guarded woodworking machinery (Ma, Wang and Chou 1991); sprains and strains from injudicious lifting or working in an awkward position (Nestor, Bobick and Pizatella 1990); repetitive motion injuries involving the hand or shoulder; and eye injuries. Many if not most of these can be prevented by proper training, the judicious application of machine guards and restraints and the use of personal protective equipment such as gloves and safety glasses. When they occur, prompt removal of splinters and prevention of infection by expeditious cleansing and first aid treatment of wounds will minimize disability.
Wood Dust
Wood dust exposure occurs whenever wood is sawed, chipped, planed, routed or sanded. The effects vary with the intensity and duration of the exposure and the size of the particles. Particles in the eyes may cause irritation, and wood dust gathering in skin folds may be aggravated by perspiration and chemicals and lead to irritation and infection. These effects may be reduced by vacuum removal of the dust, protective masks and clothing and good personal hygiene practices.
Nasopharyngeal and respiratory passages
Wood dust in the nasal passages may diminish mucociliary clearance and impair olfactory sensitivity (Andersen, Solgaard and Andersen 1976; Ahman et al. 1996). These may lead to irritation, frequent sneezing, nosebleeds and infection of the sinuses (Imbus 1994).
Exposures in a furniture factory (Whitehead, Ashikaga and Vacek 1981) and in sawmill workers (Hessel et al. 1995) were shown to be accompanied by decreases in both 1-second forced expiratory volume (FEV1) and forced vital capacity (FVC), adjusted for age, height and smoking. These were accompanied by significant increases in shortness of breath and wheeze with chest tightness and the occurrence of bronchitis and asthma. There is, however, no convincing evidence of other lung disease due to wood dust exposures (Imbus 1994). In a 6-year prospective follow-up study of approximately 350,000 males in the United States, the 11,541 individuals who reported having been employed in wood-related occupations had a lower relative risk of mortality due to non-malignant respiratory disease than those who did not report exposure to wood dust (Demers et al. 1996).
Allergy and Asthma
Some woods, notably teak, mansonia and radiata pine, contain chemicals that are irritants (see table 1 for an extended list of wood species, their geographic origins, and their health effects). Some species may cause allergic contact dermatitis (e.g., Douglas fir, western red cedar, poplar, rosewood, teak, African mahogany and other “exotic” woods). Western red cedar, rosewood, mahogany and other exotic woods have been shown to cause asthma (Imbus 1994).
Cancer
An unusually high incidence of nasal cancer has been described among woodworkers in Australia, Canada, Denmark, Finland, France, Italy, the Netherlands, the United Kingdom and the United States (Imbus 1994). A recent pooled re-analysis of 12 case-control cohort studies conducted in seven countries confirmed a high risk of nasopharyngeal cancer among woodworkers (Demers et al. 1995). The cause of these excesses of nasal cancer is not known, but, according to recent reports from the United Kingdom and the United States, the risk of nasal cancer among furniture workers has declined since the Second World War, presumably reflecting changes in the manufacturing process (Imbus 1994). No excess risk of sino-nasal cancer was found among the 45,399 men exposed to wood dust included among the 362,823 men enrolled in the American Cancer Society’s 6-year Cancer Prevention Study, but, the researchers note, the number of cases was small. They did, however, find an especially high increase in lung cancer mortality among woodworkers who also reported exposure to asbestos or formaldehyde, and suggested that exposure to these known carcinogens was responsible for the observed increased risk (Stellman et al., in press).
Chemical Exposures
Wood may contain biological contaminants. Moulds and fungi, which often grow on the bark of trees, may cause allergic reactions. Inhalation of fungal spores found on maple, redwood and cork trees has been shown to cause maple bark disease, sequoiosis and suberosis (Imbus 1994).
Wood often contains exogenous chemicals applied in the course of its processing. These include adhesives, solvents, resin binders, insecticides and fungicides, waterproofing compounds, paints and pigments, lacquers and varnishes. Many of these are volatile and may be emitted when the wood is treated, heated or incinerated; they are also conveyed as elements in wood dust. The most important of these include: toluene, methanol, xylene, methyl ethyl ketone, n-butyl alcohol, 1, 1,1-trichlorethane and dichloromethane (EPA 1995).
Conclusion
Health hazards of the wood and woodworking industries may be controlled by installation of engineering controls (e.g., proper placement and guarding of power machinery, ventilation systems to control wood dust and chemical emissions) and personal protective equipment (e.g., gloves, safety glasses, respirators), coupled with periodic inspections to ensure that these are properly maintained and used. Perhaps most important is appropriate education and training of the workers and their supervisors.
Table 1. Poisonous, allergenic and biologically active wood varieties
| Scientific names | Selected commercial names | Family | Health Impairment |
| Abies alba Mill (A. pectinata D.C.) | Silver fir | Pinaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Acacia spp. A. harpophylla F. Muell. A. melanoxylon R. Br. A. seyal Del. A. shirley Maiden |
Australian blackwood | Mimosaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Acer spp. A. platanoides L. |
Maple | Aceraceae | Dermatitis |
| Afrormosia elata Harms. (Pericopsis elata Van Meeuwen) |
Afrormosia, kokrodua, asamala, obang, oleo pardo, bohele, mohole | Papilionaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Afzelia africana Smith A. bijuga A. Chev. (Intsia bijuga A. Cunn.) A. palembanica Bak. (Intsia palembanica Bak.) |
Doussié, afzelia, aligua, apa, chanfuta, lingue merbau, intsia, hintsy | Caesalpinaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Agonandra brasiliensis Miers | Pao, marfim, granadillo | Olacaceae | Dermatitis |
| Ailanthus altissima Mill | Chinese sumac | Simaroubaceae | Dermatitis |
| Albizzia falcata Backer A. ferruginea Benth. A. lebbek Benth A. toona F.M. Bail |
Iatandza Kokko, siris |
Mimosaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Alnus spp. A. glutinosa Gaertn. |
Common alder Black alder |
Betulaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Amyris spp. A. balsamifera L. A. toxifera Willd. |
Venezuelan or West Indian sandalwood | Rutaceae | Dermatitis; toxic effects |
| Anacardium occidentale L. A. excelsum Skels. |
Cashew | Anacardiaceae | Dermatitis |
| Andira araroba Aguiar. (Vataireopsis araroba Ducke) A. coriacea Pulle A. inermis H.B.K. |
Red cabbage tree Partridge wood | Papilionaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Aningeria spp. A. robusta Aubr. and Pell. A. altissima Aubr. and Pell. Antiaris africana Engl. A. welwitschi Engl. |
Aningeria Antiaris, ako, chen chen | Sapotaceae Moraceae | Conjunctivitis-rhinitis; asthma Toxic effects |
| Apuleia molaris spruce (A. leiocarpa MacBride) (A. ferrea Mart.) |
Redwood | Caesalpinaceae | Dermatitis; toxic effects |
| Araucaria angustifolia O. Ktze A. brasiliana A. Rich. |
Parana pine, araucaria | Araucariaceae | Toxic effects |
| Aspidosperma spp. A. peroba Fr. All. A. vargasii A. DC. |
Red peroba Pau marfim, pau amarello, pequia marfim, guatambu, amarilla, pequia | Apocynaceae | Dermatitis; conjunctivitis- rhinitis; asthma; toxic effects |
| Astrocaryum spp. | Palm | Palmaceae | Dermatitis; toxic effects |
| Aucoumea klaineana Pierre | Gabon mahogany | Burseraceae | Dermatitis; conjunctivitis-rhinitis; asthma; allergic extrinsic alveolitis |
| Autranella congolensis A. Chev. (Mimusops congolensis De Wild.) |
Mukulungu, autracon, elang, bouanga, kulungu | Sapotaceae | Dermatitis |
| Bactris spp. (Astrocaryum spp.) | Palm | Palmaceae | Dermatitis; toxic effects |
| Balfourodendron riedelianum Engl. | Guatambu, gutambu blanco | Rutaceae | Dermatitis |
| Batesia floribunda Benth. | Acapu rana | Caesalpinaceae | Toxic effects |
| Berberis vulgaris L. | Barberry | Berberidaceae | Toxic effects |
| Betula spp. B. alba L. (B. pendula Roth.) |
Birch | Betulaceae | Dermatitis |
| Blepharocarva involucrigera F. Muell. | Rosebutternut | Anacardiaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Bombax brevicuspe Sprague B. chevalieri Pell |
Kondroti, alone | Bombacaceae | Dermatitis |
| Bowdichia spp. B. nitida Benth. B. guianensis Ducke (Diplotropis guianensis Benth.) (Diplotropis purpurea Amsh.) |
Black sucupira | Papilionaceae | Dermatitis |
| Brachylaena hutchinsii Hutch. | Muhuhu | Compositae | Dermatitis |
| Breonia spp. | Molompangady | Rubiaceae | Dermatitis |
| Brosimum spp. B. guianense Hub. (Piratinera guianensis Aubl.) |
Snakewood, letterwood, tigerwood | Moraceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Brya ebenus DC. (Amerimnum ebenus Sw.) Brya buxifolia Urb. |
Brown ebony, green ebony, Jamaican ebony, tropical American ebony | Papilionaceae | Dermatitis |
| Buxus sempervirens L. B. macowani Oliv. |
European boxwood, East London b., Cape b. | Buxaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Caesalpinia echinata Lam. (Guilandina echinata Spreng.) | Brasilwood | Caesalpinaceae | Dermatitis; toxic effects |
| Callitris columellaris F. Muell. | White cypress pine | Cupressaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Calophyllum spp. C. brasiliense Camb. |
Santa maria, jacareuba, kurahura, galba | Guttiferae | Dermatitis; toxic effects |
| Campsiandra laurifolia Benth. | Acapu rana | Caesalpinaceae | Toxic effects |
| Carpinus betulus | Hornbeam | Betulaceae | Dermatitis |
| Cassia siamea Lamk. | Tagayasan, muong ten, djohar | Caesalpinaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Castanea dentata Borkh C. sativa Mill. C. pumila Mill. |
Chestnut, sweet chestnut | Fagaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Castanospermum australe A. Cunn. | Black bean, Australian or Moreton Bay chestnut | Papilionaceae | Dermatitis |
| Cedrela spp. (Toona spp.) | Red cedar, Australian cedar | Meliaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Cedrus deodara (Roxb. ex. Lamb.) G. Don (C. libani Barrel. lc) |
Deodar | Pinaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Celtis brieyi De Wild. C. cinnamomea Ldl. |
Diania Gurenda |
Ulmaceae | Dermatitis |
| Chlorophora excelsa Benth. and Hook I. C. regia A. Chev. C. tinctoria (L.) Daub. |
Iroko, gelbholz, yellowood, kambala, mvule, odum, moule, African teak, abang, tatajuba, fustic, mora | Moraceae | Dermatitis; conjunctivitis-rhinitis; asthma; allergic extrinsic alveolitis |
| Chloroxylon spp. C. swietenia A.DC. |
Ceylon satinwood | Rutaceae | Dermatitis; toxic effects |
| Chrysophyllum spp. | Najara | Sapotaceae | Dermatitis |
| Cinnamomum camphora Nees and Ebeim | Asian camphorwood, cinnamon | Lauraceae | Toxic effects |
| Cryptocarya pleurosperma White and Francis | Poison walnut | Lauraceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Dacrycarpus dacryoides (A. Rich.) de Laub. | New Zealand white pine | Podocarpaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Dacrydium cupressinum Soland | Sempilor, rimu | Podocarpaceae | conjunctivitis-rhinitis; asthma |
| Dactylocladus stenostachys Oliv. | Jong kong, merebong, medang tabak | Melastomaceae | Toxic effects |
| Dalbergia spp. D. amerimnon Benth. D. granadillo Pitt. D. hypoleuca Standl. D. latifolia Roxb. D. melanoxylon Guill. and Perr. D. nigra Fr. All. D. oliveri Gamble D. retusa Hemsl. D. sissoo Roxb. D. stevensonii Standl. |
Ebony Red foxwood Indian rosewood, Bombay blackwood, African blackwood, pallisander, riopalissandro, Brasilian rosewood, jacaranda Burma rosewood Red foxwood Nagaed wood, Honduras rosewood |
Papilionaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Dialium spp. D. dinklangeri Harms. |
Eyoum, eyum | Caesalpinaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Diospyros spp. D. celebica Bakh. D. crassiflora Hiern D. ebenum Koenig |
Ebony, African ebony Macassar ebony, African ebony, Ceylon ebony | Ebenaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Dipterocarpus spp. D. alatus Roxb. |
Keruing, gurjum, yang, keruing | Dipterocarpaceae | Dermatitis |
| Distemonanthus benthamianus Baill. | Movingui, ayan, anyaran, Nigerian satinwood | Caesalpinaceae | Dermatitis |
| Dysoxylum spp. D. fraseranum Benth. |
Mahogany, stavewood, red bean | Meliaceae | dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| D. muelleri Benth. | Rose mahogany | ||
| Echirospermum balthazarii Fr. All. (Plathymenia reticulataBenth.) | Vinhatico | Mimosaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Entandophragma spp. E. angolense C.D.C. E. candollei Harms. E. cylindricum Sprague E. utile Sprague |
Tiama Kosipo, omo Sapelli, sapele, aboudikro Sipo, utile, assié, kalungi, mufumbi |
Meliaceae | Dermatitis; allergic extrinsic alveolitis |
| Erythrophloeum guineense G. Don E. ivorense A. Chev. |
Tali, missanda, eloun, massanda, sasswood, erun, redwater tree | Caesalpinaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Esenbeckia leiocarpa Engl. | Guaranta | Rutaceae | Dermatitis |
| Eucalyptus spp. E. delegatensis R.T. Back E. hemiphloia F. Muell. E. leucoxylon Maiden E. maculata Hook. E. marginata Donn ex Sm. E. microtheca F. Muell. E. obliqua L. Herit. E. regnans F. Muell. E. saligna Sm. |
Alpine ash Grey box Yellow gum Spotted gum Mountain ash |
Myrtaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Euxylophora paraensis Hub. | Boxwood | Rutaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Excoecaria africana M. Arg. (Spirostachys africana Sand) E. agallocha L. |
African sandalwood, tabootie, geor, aloewood, blind-your-eye | Euphorbiaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Fagara spp. F. flava Krug and Urb. (Zanthoxylum flavum Vahl.) F. heitzii Aubr. and Pell. F. macrophylla Engl. |
Yellow sanders, West Indian satinwood, atlaswood, olon, bongo, mbanza | Rutaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Fagus spp. (Nothofagus spp.) F. sylvatica L. |
Beech | Fagaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Fitzroya cupressoides (Molina) Johnston (F. patagonica Hook. f.) |
Alerce | Cupressaceae | Dermatitis |
| Flindersia australis R. Br. F. brayleyana F. Muell. F. pimenteliana F. Muell. |
Australian teak, Queensland maple, maple Silkwood, Australian maple |
Rutaceae | Dermatitis |
| Fraxinus spp. F. excelsior L. |
Ash | Oleaceae | Dermatitis |
| Gluta spp. G. rhengas L. (Melanorrhoea spp.) M. curtisii Pierre M. laccifera wallichii Hook. |
Rengas, gluta Renga wood Rhengas |
Anacardiaceae | Dermatitis; toxic effects |
| Gonioma kamassi E. Mey. | Knysna boxwood, kamassi | Apocynaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Gonystylus bancanus Baill. | Ramin, melawis, akenia | Gonystylaceae | Dermatitis; conjunctivitis-rhinitis; asthma; allergic extrinsic alveolitis |
| Gossweilerodendron balsamiferum (Verm.) Harms. | Nigerian cedar | Caesalpinaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Grevillea robusta A. Cunn. | Silky oak | Proteaceae | Dermatitis |
| Guaiacum officinale L. | Gaiac, lignum vitae | Zygophyllaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Guarea spp. G. cedrata Pell. G. laurentii De Wild. G. thompsonii Sprague |
Bossé Nigerian pearwood Cedar mahogany Scented guarea Black guarea |
Meliaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Halfordia scleroxyla F. Muell. H. papuana Lauterb. |
Saffron-heart | Polygonaceae | Dermatitis; allergic extrinsic alveolitis |
| Hernandia spp. H. sonora L. (H. guianensis Aubl.) |
Mirobolan, topolite | Hernandiaceae | Dermatitis |
| Hippomane mancinella L. | Beach apple | Euphorbiaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Illipe latifolia F. Muell. I. longifolia F. Muell. (Bassia latifolia Roxb.) (B. longifoliaRoxb.) |
Moak, edel teak | Sapotaceae | Dermatitis |
| Jacaranda spp. J. brasiliana Pers. Syn. (Bignonia brasiliana Lam.) J. coerulea (I.) Gris. |
Jacaranda Caroba, boxwood | Bignoniaceae | Dermatitis |
| Juglans spp. J. nigra L. J. regia L. |
Walnut | Juglandaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Juniperus sabina L. J. phoenicea L. J. virginiana L. |
Virginian pencil cedar, Eastern red cedar | Cupressaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Khaya antotheca C. DC. K. ivorensis A. Chev. K. senegalensis A. Juss. |
Ogwango, African mahogany, krala Dry-zone mahogany | Meliaceae | Dermatitis; allergic extrinsic alveolitis |
| Laburnum anagyroides Medic. (Cytisus laburnum L.) L. vulgare Gris |
Laburnum | Papilionaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Larix spp. L. decidua Mill. L. europea D.C. |
Larch European larch |
Pinaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Liquidambar styracifolia L. | Amberbaum, satin-nussbaum | Hamamelidaceae | Dermatitis |
| Liriodendron tulipifera L. | American whitewood, tulip tree | Magnoliaceae | Dermatitis |
| Lovoa trichilioides Harms. (L. klaineana Pierre) | Dibetou, African walnut, apopo, tigerwood, side | Meliaceae | dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Lucuma spp. (Pouteria spp.) L. procera |
Guapeva, abiurana Massaranduba |
Sapotaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Maba ebenus Wight. | Makassar-ebenholz | Ebenaceae | Dermatitis |
| Machaerium pedicellatum Vog. M. scleroxylon Tul. M. violaceum Vog. |
Kingswood | Papilionaceae | Dermatitis |
| Mansonia altissima A. Chev. | Nigerian walnut | Sterculiaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Melanoxylon brauna Schott | Brauna, grauna | Caesalpinaceae | Dermatitis |
| Microberlinia brazzavillensis A. Chev. M. bisulcata A. Chev. |
African zebrawood | Caesalpinaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Millettia laurentii De Wild. M. stuhlmannii Taub. |
Wenge Panga-panga |
Papilionaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Mimusops spp. (Manilkara spp.) Mimusops spp. (Dumoria spp.) (Tieghemella spp.) M. congolensis De Wild. (Autranella congolensis A. Chev.) M. djave Engl. (Baillonella toxisperma Pierre) M. heckelii Hutch. et Dalz. (Tieghemella heckelii Pierre) (Dumoria heckelii A. Chev.) |
Muirapiranga Makoré Mukulungu, autracon Moabi Cherry mahogany |
Sapotaceae | Dermatitis; conjunctivitis-rhinitis; asthma; allergic extrinsic alveolitis; toxic effects |
| Mitragyna ciliata Aubr. and Pell. M. stipulosa O. Ktze |
Vuku, African poplar Abura |
Rubiaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Nauclea diderrichii Merrill (Sarcocephalus diderrichii De Wild.) Nauclea trillessi Merrill |
Bilinga, opepe, kussia, badi, West African boxwood | Rubiaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Nesogordonia papaverifera R. Capuron | Kotibé, danta, epro, otutu, ovové, aborbora | Tiliaceae | Toxic effects |
| Ocotea spp. O. bullata E. Mey O. porosa L. Barr. (Phoebe porosa Mez.) O. rodiaei Mez. (Nectandra rodiaei Schomb.) O. rubra Mez. O. usambarensis Engl. |
Stinkwood Laurel Brazilian walnut Greenheart Louro vermelho East African camphorwood |
Lauraceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Paratecoma spp. P. alba P. peroba Kuhlm. |
Brazilian white peroba Peroba white. p. |
Bignoniaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Parinarium spp. P. guianense (Parinari spp.) (Brosimum spp.) P. variegatum |
Guyana-satinholz Antillen-satinholz |
Rosaceae | Dermatitis |
| Peltogyne spp. P. densiflora Spruce |
Blue wood, purpleheart | Caesalpinaceae | Toxic effects |
| Phyllanthus ferdinandi F.v.M. | Lignum vitae, chow way, tow war | Euphorbiaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Picea spp. P. abies Karst. P. excelsa Link. P. mariana B.S.P. P. polita Carr. |
European spruce, whitewood Black spruce |
Pinaceae | Dermatitis; conjunctivitis-rhinitis; asthma; allergic extrinsic alveolitis |
| Pinus spp. P. radiata D. Don |
Pine | Pinaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Piptadenia africana Hook f. Piptadeniastrum africanum Brenan |
Dabema, dahoma, ekhimi agobin, mpewere, bukundu |
Mimosaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Platanus spp. | Plane | Platanaceae | Dermatitis |
| Pometia spp. P. pinnata Forst. |
Taun Kasai |
Sapindaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Populus spp. | Poplar | Salicaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Prosopis juliflora D.C. | Cashaw | Mimosaceae | Dermatitis |
| Prunus spp. P. serotina Ehrl. |
Cherry Blackcherry |
Rosaceae | dermatitis; conjunctivitis-rhinitis; asthma |
| Pseudomorus brunoniana Bureau | White handlewood | Moraceae | Dermatitis; toxic effects |
| Pseudotsuga douglasii Carr. (P. menziesii Franco) | Douglas fir, red fir, Douglas spruce | Pinaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Pterocarpus spp. P. angolensis D.C. P. indicus Willd. P. santalinus L.f. (Vatairea guianensis Aubl.) |
African padauk, New Guinea rosewood, red sandalwood, red sanders, quassia wood | Papilionaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Pycnanthus angolensis Warb. (P. kombo Warb.) | Ilomba | Myristicaceae | Toxic effects |
| Quercus spp. | Oak | Fagaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Raputia alba Engl. R. magnifica Engl. |
Arapoca branca, arapoca | Rutaceae | Dermatitis |
| Rauwolfia pentaphylla Stapf. O. | Peroba | Apocynaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Sandoricum spp. S. indicum Cav. |
Sentul, katon, kra-ton, ketjapi, thitto | Meliaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Schinopsis lorentzii Engl. S. balansae Engl. |
Quebracho colorado, red q., San Juan, pau mulato | Anacardiaceae | Dermatitis; toxic effects |
| Semercarpus australiensis Engl. S. anacardium L. |
Marking nut | Anacardiaceae | Dermatitis; toxic effects |
| Sequoia sempervirens Endl. | Sequoia, California redwood |
Taxodiaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Shorea spp. | Alan, almon, red balau White heavy, red lauan, white L., yellow L., mayapis, meranti bakau, dark red M., light red M., red M., white M., yellow M., red seraya, white seraya |
Dipterocarpaceae | Dermatitis |
| S. assamica Dyer | Yellow lauan, white meranti | ||
| Staudtia stipitata Warb. (S. gabonensis Warb.) | Niové | Myristicaceae | Dermatitis |
| Swietenia spp. S. macrophylla King S. mahogany Jacq. |
Mahogany, Honduras mahogany, Tabasco m., baywood, American mahogany, Cuban mahogany |
Meliaceae | Dermatitis; conjunctivitis-rhinitis; asthma; allergic extrinsic alveolitis; toxic effects |
| Swintonia spicifera Hook. S. floribunda Griff. |
Merpauh | Anacardiaceae | Dermatitis |
| Tabebuia spp. T. ipe Standl. (T. avellanedae Lor. ex Gris.) T. guayacan Hensl. (T. lapacho K. Schum) |
Araguan, ipé preto, lapacho | Bignoniaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Taxus baccata L. | Yew | Taxaceae | Dermatitis; conjunctivitis-rhinitis; asthma; allergic extrinsic alveolitis; toxic effects |
| Tecoma spp. T. araliacea D.C. T. lapacho |
Green heart Lapacho |
Bignoniaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Tectona grandis L. | Teak, djati, kyun, teck | Verbenaceae | Dermatitis; conjunctivitis-rhinitis; asthma; allergic extrinsic alveolitis |
| Terminalia alata Roth. T. superba Engl. and Diels. |
Indian laurel limba, afara, ofram, fraké, korina, akom |
Combretaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Thuja occidentalis L. T. plicata D. Don T. standishii Carr. |
White cedar Western red cedar |
Cupressaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Tieghemella africana A. Chev. (Dumoria spp.) T. heckelii Pierre |
Makoré, douka, okola, ukola, makoré, abacu, baku, African cherry | Sapotaceae | Dermatitis; conjunctivitis-rhinitis; asthma; toxic effects |
| Triplochiton scleroxylon K. Schum | Obeche, samba, wawa, abachi, African whitewood, arere | Sterculiaceae | Dermatitis; conjunctivitis-rhinitis; asthma |
| Tsuga heterophylla Sarg. | Tsuga, Western hemlock | Pinaceae | Dermatitis |
| Turraeanthus africana Pell. | Avodiré Lusamba |
Meliaceae | Dermatitis; allergic extrinsic alveolitis |
| Ulmus spp. | Elm | Ulmaceae | Dermatitis |
| Vitex ciliata Pell. | Verbenaceae | Dermatitis | |
| V. congolensis De Wild. and Th. Dur | Difundu | ||
| V. pachyphylla Bak. | Evino | ||
| Xylia dolabriformis Benth. | Mimosaceae | Conjunctivitis-rhinitis; | |
| X. xylocarpa Taub. | Pyinkado | asthma | |
| Zollernia paraensis Huber | Santo wood | Caesalpinaceae | Dermatitis; toxic effects |
Source: Istituto del Legno, Florence, Italy.
Wood Planning Machines
The development of stationary planing machines can be traced back to the beginning of the 19th century. On the first machines of this type, the workpiece was clamped to a carriage and fed below a horizontal shaft fitted with blades extending over the full working width. In 1850 a planing machine was built in Germany on which the workpiece was fed over a cutterblock located between two tables used to position and to support the workpiece. Apart from technical improvements this basic design has been maintained to this day. Such a machine is called a surface planing machine or a jointer (see figure 1).
Figure 1. Jointer
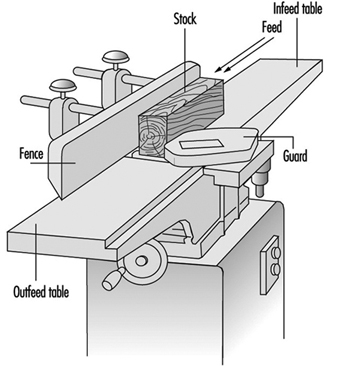
More recently, machines were designed to plane the upper surface of a workpiece to a predetermined thickness by means of a horizontally rotating cutterblock. The distance between the cutting circle diameter and the surface of the table supporting the workpiece is adjustable. Such machines are called one-side-thickness planing machines.
These two basic machine types were eventually combined into a machine which could be used for both surface and thickness planing. This development ended in planing machines for two-, three- and four-sided working in one pass.
From the point of view of occupational safety and health, it is strongly recommended that measures be taken for the extraction of wood dust and chips from the planing machine (e.g., by connecting the planing machine to a dust extraction system). Dust originating from hardwood (oak, beech) and tropical wood is considered a particular health hazard and must be extracted. Measures to reduce the noise level of planing machines should also be taken. An automatic brake for the cutterblock is compulsory in many countries.
Surface Planing Machines
A surface planing machine has rigid main frame that supports the infeed and the outfeed table. The cutterblock is located between the two tables and mounted on ball bearings. The main frame should be ergonomically designed (i.e., it should enable the operator to work comfortably).
Hand-operated control devices should be installed in such a way that the operator is not placed in a hazardous situation when operating them, and the possibility of inadvertent operation should be minimized.
The side of the main frame facing the operator’s position must be free of projecting parts such as handwheels, levers and so on. The table to the left of the cutterblock (outfeed table) is normally set at the same height as the cutting circle of the cutterblock. The table to the right of the cutterblock (infeed table) is set lower than the outfeed table to obtain the desired depth of cut. Contact between the table lips and the cutterblock should not be possible over the full setting range of the tables. However, the clearance between the table lips and the cutting circle of the cutterblock shall be as small as possible to provide for good support of the workpiece to be planed.
The major operations on a surface planing machine are flatting and edging. The position of the hands on the workpiece is important from an operational and safety viewpoint. When flatting, the workpiece should be fed with one hand, with the other hand holding it down initially on the infeed table. As soon as there is a sufficient portion of timber on the outfeed table, the latter hand can pass safely over the bridge-guard to apply pressure on the outfeed table and will be followed by the feeding hand to complete the feeding operation. When edging, the hands should not pass over the cutterblock while in contact with the timber. Their prime function is to exert horizontal pressure on the workpiece to maintain it square to the fence.
The noise produced by the rotating cutterblock often may exceed the level considered harmful to the ear. Measures to reduce the noise level are therefore necessary. Some of the noise reduction measures which have proved successful on surface planers are the following:
- use of a “quiet” cutterblock (e.g., a round form with minimum blade projection, helical blade instead of straight blade, segmental rotating tools with offset cutting)
- slotted or drilled table lips (the configuration and the dimensions of the apertures in the table lips must be selected so that no accident hazards arise; e.g., slots shall be no more than 6 mm wide and the diameter of the holes shall not exceed 6 mm)
- aerodynamic design of the chip deflectors below the table lips
- reduction of the cutterblock speed to below 1,000 rpm, provided the surface quality of the workpiece is still satisfactory.
Noise reduction up to 12 dBA when idling and 10 dBA under load can be achieved.
Cutterblocks should have a circular cross-section, and the chip clearance grooves and slots should be as small as possible. The blades and inserts shall be properly secured, preferably by form lock fixing.
The cutterblock rotates generally at speeds between 4,500 and 6,000 rpm. The diameters of conventional cutterblocks vary from 56 to 160 mm, and their lengths (working widths) from 200 to 900 mm. By analogy with the kinematics of conventional milling, the surface of the workpiece planed with a cutterblock is composed of cycloid arcs. The surface quality of the work therefore depends on the speed and diameter of the cutterblock, the number of cutting blades and the feed rate of the workpiece.
Equipping surface planing machines with an automatic brake for the cutterblock is recommended. The brake should be activated when the machine is stopped, and the braking time should not exceed 10 seconds.
Access to the cutterblock at the rear of the fence should be prevented by a guard attached either to the fence or the fence support. The cutterblock in front of the fence should be guarded by an adjustable bridge-type guard fixed to the machine (e.g., to the main frame on the outfeed table side) (see figure 2). Access to the transmission elements should be prevented by a fixed guard.
Figure 2. Fence & rear cutterblock guard
Hazards
As the cutterblock rotates opposite to the direction in which the workpiece is fed, the hazard of kickback exists. If the workpiece is ejected, the operator’s hand or fingers may come in contact with the rotating cutterblock unless adequate guarding has been provided. It also frequently happens that the hand comes in contact with the cutterblock while feeding the workpiece with stretched fingers instead of pushing it forward with closed fist. Cutting blades not properly secured may be ejected by centrifugal force and may cause severe injury and/or material damage.
Guarding systems for surface planing machines
In many countries legislation covering the use of surface planing machines requires that the cutterblock be covered by an adjustable guarding system in order to prevent accidental contact of the operator’s hand with the rotating cutterblock.
In 1938, the SUVA introduced a planer guard which efficiently met all practical requirements. Over the years this guard has proved useful not only as a guarding system but also as an aid for most operations. It is well accepted by the woodworking trade in Switzerland, and almost all industrial surface planing machines are equipped with it. The design features of this guard have been introduced into the draft European standard for surface planing machines. The main features of this guard are the following:
- strong and rigid
- not easily deflected to expose cutterblock
- always stays parallel to the cutterblock axis regardless of its horizontal or vertical adjustment
- easily adjustable horizontally and vertically without the use of a tool.
However, accidents still happen. These accidents are mainly caused by failure to adjust the guard properly. Therefore, SUVA engineers have developed a bridge-type guard which covers the cutterblock in front of the fence automatically, and constantly exerts a defined pressure against the workpiece or the fence. This guard has been available since 1992.
The main design features of this new guard, called “Suvamatic”, are the following:
- complete guarding of the cutterblock. The full planing width is safeguarded by one single bridge-type guard. It can be folded down using a hinged locking system. This prevents the guard from projecting too far over the face of the machine.
- practical workpiece guiding system. The workpiece guiding system consists of a pressure pad and a guide for the workpiece. Both are fitted to the tip of the guard. The latter can be tilted to guide the workpiece both for flatting and edging.
- pressure application to assist work. For edging, the guard exerts pressure in direction of the fence. After edging, it automatically covers the full length of the cutterblock in front of the fence.
- automatic lifting and lowering of the guard. For flatting, the guard is lifted by the workpiece guide. After flatting, it lowers itself automatically to cover the cutterblock.
- guard can be locked in position for batch jobs. For batch jobs, the guard can be locked in vertical position to just accommodate the thickness of the workpiece. The guard will return automatically to this preset position after being pressed down.
- will fit all machines. The guard can be fitted to all surface planing machines and combined surface and thickness planing machines.
One-Side Thickness Planing Machines
The main frame of a one-side thickness planing machine houses the cutterblock, thickness planing table and feed elements.
Once the workpiece has been flattened and edged on a surface planing machine, it is planed to the desired thickness on the thickness planing machine. Unlike that of a surface planing machine, the cutterblock of a thickness planing machine is located above the planing table and the workpiece is no longer fed by hand but mechanically by feed rollers. The feed rollers are driven either by a separate motor (approximately 1 kW) or via a speed-reduction gearbox receiving its power from the cutterblock motor. With a separate drive the feed rate remains constant, but if the power is transmitted from the cutterblock motor the feed rate varies according to the cutterblock speed. Feed rates between 4 and 35 m/min are common.
Two spring-mounted feed rollers rest on the upper surface of the workpiece. The feed roller in front of the cutterblock is grooved for better grip on the workpiece; the feed roller at the outfeed end of the cutterblock is smooth. An infeed and an outfeed pressure bar located next to the cutterblock press the workpiece down onto the table, thereby ensuring a clean and even cut. The design and arrangement of the feed rollers and pressure bars should be such that contact with the rotating cutterblock is impossible.
Sectional feed rollers and pressure bars allow for the simultaneous working of two or more workpieces of slightly different thickness. From the point of view of accident prevention, sectional feed rollers and pressure bars are essential. The width of the individual feed roller or pressure bar section should not exceed 50 mm.
Two idle rollers are arranged in the table. They are designed to facilitate the passage of the workpiece over the table.
The surface of the table must be a plane free from slots or holes. Accidents involving an operator’s fingers being squeezed between openings and the workpiece have occurred. Vertical adjustment of the table may be manual or power assisted. A mechanical end-stop should prevent any contact of the table with the cutterblock or feed rollers. It must be ensured that the vertical adjustment mechanism hold the table in a stable position.
In order to prevent the feeding of oversize workpieces, a device (e.g., a fixed rod or fixed bar) is located on the infeed side of the machine, thereby limiting the maximum workpiece height. A maximum height of 250 mm between the surface of the table in its lowest position and the above-mentioned safety device is rarely exceeded. The usual working width varies between 315 and 800 mm (for special machines this width might go up to 1,300 mm).
The cutterblock diameter generally varies from 80 to 160 mm. Normally four blades are fitted to the cutterblock. The cutterblock rotates at speeds between 4,000 and 6,000 rpm, and its input power varies from 4 to 20 kW. The maximum depth of cut is 10 to 12 mm.
To minimize the danger of kickback, one-side thickness planing machines should be fitted with an anti-kickback device covering the full working width of the machine. This anti-kickback device generally consists of several grooved elements arranged on a rod. The individual element is between 8 and 15 mm wide, and it falls under its own weight to the rest position. The lowest point of the individual grooved element in its rest position should be 3 mm below the cutting circle of the cutterblock. The grooved elements should be made of a material (preferably steel) with a resilience strength of 15 J/cm2 and a surface hardness of 100 HB.
The following noise-reduction measures have proved to be successful on one-side thickness planing machines:
- use of a “quiet” cutterblock (like that suggested for surface planing machines)
- aerodynamic design of the pressure bars and the chip extraction hood
- reduction of the cutterblock speed
- partial or complete enclosure of the machine (tunnel-like design of the infeed and outfeed opening with sound-absorbing material on the surface facing the source of noise)
Noise reduction of up to 20 dBA may be achieved by a well designed complete enclosure.
Hazards
The major cause of accidents on one-side thickness planing machines is kickback of the workpiece. Kickback may happen because of:
- poor maintenance of the anti-kickback device (the individual elements may not fall free under their own weight but stick together because of dust accumulation; the grooves in the elements may be covered with resin, be blunt or be incorrectly reground)
- poor maintenance of the sectional feed rollers and pressure bars (e.g., resin-covered or rusty sections)
- insufficient spring load on feed rollers and pressure bars when several pieces of non-uniform thickness are fed at the same time.
Typical causes of other accidents are:
- contact of the hand with the rotating cutterblock when removing chips and dust from the table by hand rather than with a wooden stick or rake
- ejection of cutterblock blades due to incorrect fixing.
Combined Surface Planing and Thicknessing Machines
The design and operation of combined machines (see figure 3) are similar to those of the individual machines described above. The same can be said in regards to the feed rates, motor power, table and roller adjustments. For thickness planing the surface planing tables are either pulled away, folded down or lifted up sideways, exposing the cutterblock, which is covered by a chip extraction hood to prevent access Combined machines are mainly used in small workshops with few workers, or where space is limited (i.e., in cases where the installation of two individual machines is impossible or unprofitable).
Figure 3. Combined surface & thickness planer
The changeover from one operation to the other is often time-consuming and may be annoying if only a few pieces have to be machined. Moreover, usually only one person at a time can use the machine. However, since 1992 machines have been introduced to the market where simultaneous operation (surface and thickness planing at the same time) is possible.
The hazards of combined machines are to a large extent identical to the hazards listed for the individual machines.
Routing Machines
Stationary routing machines are used in general for the manufacture of wood articles and furniture elements, but sometimes also for machining plastics and light alloys. Important types of routing machines are copy routers, pattern millers, machines with mobile router heads and automatic copying machines. The automatic copying machines are generally used for machining several workpieces simultaneously.
A common feature of all routing machines is that the tool is located above the workpiece support, which is normally a table. The tool-spindle axis is nearly always vertical, but on some machines the router head, and thus also the tool-spindle axis, may be tilted. The machining head is lowered for machining and returns automatically to its initial (rest) position. On older machines the machining head is lowered manually by operating a mechanical foot-pedal or hand lever. On modern machines the head is generally lowered by a pneumatic or hydraulic system. Figure 1 shows various accessories (hold-down shoes, guides and so on) and the Swiss National Accident Insurance Organization (SUVA) safety guard.
Figure 1. SUVA safety device with routing tool in working position

The tool-spindle is driven either by a belt drive or directly by a high-frequency motor, which is often of the two-speed type. The tool-spindle speeds generally range from 6,000 to 24,000 rpm. They are lower in pattern millers, where the lowest speed may be 250 rpm. Pattern millers are often equipped with a gearbox for the selection of different speeds.
The cutting diameter of the routing tool varies from 3 to 50 mm. However, on special pattern millers the cutting diameter of the tool may be as large as 300 mm.
Tooling
On routing machines single-edged spoon bits, double-edged panel cutters or solid-shaped cutters mainly are used. Like any tool they must be designed and made of such materials that will withstand the forces and loads to be expected during operation. Machines should be used and maintained in compliance with the manufacturer’s instructions.
The routing tools should be:
- clearly and permanently marked with the permissible speed, e.g., less than 20,000 rpm
- of a type tested by an approved body
- of round form design with a minimal radial cutting edge projection to reduce the danger of kickback.
Guarding of the tool
On routing machines where the tool is moving and the workpiece remains fixed, access to the rotating tool should be prevented by an adjustable guard (hand protector). It should be supplemented by a movable guard which can be lowered on to the workpiece surface. The lower end of this movable guard may be a brush.
On routing machines where the workpiece is held and/or fed by hand, it is highly recommended to use a safety device exerting vertical pressure on the workpiece. The SUVA has designed such a guard. This safety device has been successfully used since the end of the 1940s and is still the most complete guard of its kind. Its main features are:
- prevention of unintentional contact with the rotating tool both in its rest position and in its working position
- fast and easy changeover from one size of hold-down shoe to another. Several sizes of hold-down shoes are available to fit tools with different cutting diameters
- manually adjustable amount of pressure exerted on the workpiece by the hold-down shoe
- automatic return of the hold-down shoe to its upper position when the router head rises to its rest position. The guarding device can be adjusted so that the hold-down shoe may be lifted only when the lower edge of the tool is above the level of the lower edge of the hold-down shoe; this is to prevent any unintentional contact with the tool from below (see figure 2. Serious injuries to the back of the hand, where the tendons are protected only by the skin, are thus avoided.
Figure 2. Safety device with routing tool in initial position
- possibility of connection of a chip extraction system to the guarding device.
This guarding device also enables workpieces to be routed along a guide with the aid of a horizontal pressure pad.
Hazards
Routing machines have been found to be less dangerous than vertical spindle moulding machines. One reason for this is the smaller diameter of most routing tools. However, the tools on routing machines are easily accessible and thus present a constant hazard for the hands and arms of the operator. Therefore, copy routers, where the workpiece is generally fed by hand, are by far the most dangerous routing machines.
Causes of accidents
The main causes of router accidents are:
- unintentional contact of the hand or arm with the rotating tool in its rest position (1) when removing chips and dust from the table by hand rather than using a wooden stick, (2) when the workpiece or the jig is not correctly handled or (3) when the sleeve of the operator’s clothing becomes entangled in the rotating tool
- unintentional contact of the hand with the routing tool as a result of kickback of the workpiece held by hand.
Kickback may happen because of:
- an unsafe working practice
- faults in the workpiece (knots, etc.)
- workpieces being fed into the tool too abruptly or from the wrong direction
- blunt cutter edges
- inadequate cutting speed
- incorrect fixing of the workpiece to the jig
- workpiece breakage
- ejection of the tool or parts of the tool due to bad tool design, excessive hardness of the tool material, faults in the material of the tool, overspeed of the tool or poor clamping of the tool in the tool holder.
In the event of ejection of a tool or workpiece, not only the operator but also other persons working in the area may be injured by ejected parts.
Measures to prevent accidents
Measures to prevent accidents should be directed at:
- the design and construction of the machine
- the tooling
- guarding the tool in its rest position (figure 15) and as far as possible in the working position (figure 14), in particular when the workpiece is held and fed by hand.
Design and Construction of the Machine
Routing machines must be designed to be safe to operate. It should be ensured that:
- the machine is sufficiently rigid
- the electrical equipment conforms to safety regulations
- actuators used to initiate a start function or movement of a machine element are constructed and mounted so as to minimize inadvertent operation
- access to moving machine parts, such as belt drives, hydraulic or pneumatically moved router heads or travelling tables on machines with automatic feeds, are prevented by adequate guarding
- the actual revolutions per minute of the tool are clearly visible to the operator
- the safety devices and chip extraction systems are easy to install
- the noise level of the machine is reduced as far as possible.
Furthermore, it is advisable to equip the tool drive of the routing machine with an automatic brake that activates when the machine is stopped. The braking time should not exceed 10 seconds.
Sample checklist
Housekeeping
1. A daily housekeeping programme is essential.
2. Dust accumulations of 1/8” depth in any area indicate a need for cleaning. It should be noted that any accumulation of dust may lead to a fire. The finer the dust, the greater the hazards.
3. Clean wood dust frequently.
a. Wipe down daily around hot surfaces.
b. Major blow down or vacuum when possible of all areas, including rafters, at least twice per year.
c. When concentrations are high, work small areas at a time.
d. Low humidity increases the potential for hazards and should be taken in consideration during blow downs.
4. Schedule blow downs or clean ups while equipment is down, such as Friday afternoons and weekends.
Electrical maintenance
1. Inspect/clean all motors regularly to avoid dust build-up.
2. Ensure all electrical boxes and panels meet the National Electrical Code requirements for their classified location.
3. Listen for unusual sounds, note unusual smells and watch for visual dust accumulations on machines and motors. Check motors and other electricals often to detect overheating.
4. Ensure that maintenance or operating personnel are lubricating bearings to motors, conveyors, chains and sprockets on a timely basis.
5. Ensure that electrical panels and boxes are kept closed and maintained to prevent dust accumulations, including keeping all knockout holes plugged.
Fire prevention
1. Actively prohibit smoking in unauthorized locations.
2. Adopt procedures for hot-work permits and ensure that procedures are followed.
3. Do not allow operator-controlled machines to operate unattended.
4. Install a device at the mouth of the dust collecting system to prevent sanding belts and other spark producing items from entering the system and causing a fire.
5. Trap metal in wood hogs by installing magnets in the conveyor system and metal detectors in the hog. Policies and procedures should be implemented to prevent metal and other foreign objects from reaching the hogs.
6. Conduct weekly and monthly inspections of fire protective systems including fire extinguishers, fire hoses, alarms and sprinkler control valves.
7. Ensure that boiler rooms and heating equipment are free of dust accumulations, that written boiler start-up procedures are being followed and that properly classified equipment is used.
8. Recognize the correct procedure in fighting dust fires.
9. Request a detailed inspection by the local fire marshal or insurance carrier.
10. Encourage mock drills/visits by the local fire department.
11. Install spark detection and extinguishing systems in dust collection systems and check periodically to ensure that they are working.
12. Review evacuation plans, emergency lighting, fire drills periodically for each work shift.
Miscellaneous
1. Contact insurance carrier for assistance in hazard identifications associated with safety, health and fire prevention.
2. Contact appropriate government safety agencies for additional assistance.
3. Employees should enter dust silos only when confined space procedures are followed.
4. All operators should ensure that dust collecting systems are working properly and report any malfunctions to management immediately.
5. Check for objects obstructing the ducts to the dust system.
6. It is recommended that all supervisors, safety committee members and other employees be made aware of the contents of this voluntary checklist to achieve maximum implementation.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."