- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Chemicals in the Health Care Environment
Livestock Confinement
Global economic forces have contributed to the industrialization of agriculture (Donham and Thu 1995). In the developed countries, there are trends toward increased specialization, intensity and mechanization. Increased confinement production of livestock has been a result of these trends. Many developing countries have recognized the need to adopt confinement production in an attempt to transform their agriculture from a subsistence to a globally competitive enterprise. As more corporate organizations obtain ownership and control of the industry, fewer, but larger, farms with many employees replace the family farm.
Conceptually, the confinement system applies principles of industrial mass production to livestock production. The concept of confinement production includes raising animals in high densities in structures that are isolated from the outside environment and equipped with mechanical or automated systems for ventilation, waste handling, feeding and watering (Donham, Rubino et al. 1977).
Several European countries have been using confinement systems since the early 1950s. Livestock confinement started to appear in the United States in the late 1950s. Poultry producers were first to use the system. By the early 1960s, the swine industry had also started to adopt this technique, followed more recently by dairy and beef producers.
Accompanying this industrialization, several worker health and social concerns have developed. In most Western countries, farms are getting fewer in number but larger in size. There are fewer family farms (combined labour and management) and more corporate structures (particularly in North America). The result is that there are more hired workers and relatively fewer family members working. Additionally, in North America, more workers are coming from minority and immigrant groups. Therefore, there is a risk of producing a new underclass of workers in some segments of the industry.
A whole new set of occupational hazardous exposures has arisen for the agricultural worker. These can be categorized under four main headings:
- toxic and asphyxiating gases
- bioactive aerosols of particulates
- infectious diseases
- noise.
Respiratory hazards are also a concern.
Toxic and Asphyxiating Gases
Several toxic and asphyxiating gases resulting from microbial degradation of animal wastes (urine and faeces) may be associated with livestock confinement. Wastes are most commonly stored in liquid form under the building, over a slatted floor or in a tank or lagoon outside the building. This manure storage system is usually anaerobic, leading to the formation of a number of toxic gases (see table 1) (Donham, Yeggy and Dauge 1988). See also the article “Manure and waste handling" in this chapter.
Table 1. Compounds identified in swine confinement building atmospheres
|
2-Propanol |
Ethanol |
Isopropyl propionate |
|
3-Pentanone |
Ethyl formate |
Isovaleric acid |
|
Acetaldehyde |
Ethylamine |
Methane |
|
Acetic acid |
Formaldehyde |
Methyl acetate |
|
Acetone |
Heptaldehyde |
Methylamine |
|
Ammonia |
Heterocylic nitrogen compound |
Methylmercaptan |
|
n-Butanol |
Hexanal |
Octaldehyde |
|
n-Butyl |
Hydrogen sulphide |
n-Propanol |
|
Butyric acid |
Indole |
Propionic acid |
|
Carbon dioxide |
Isobutanol |
Proponaldehyde |
|
Carbon monoxide |
Isobutyl acetate |
Propyl propionate |
|
Decaldehyde |
Isobutyraldehyde |
Skatole |
|
Diethyl sulphide |
Isobutyric acid |
Triethylamine |
|
Dimethyl sulphide |
Isopentanol |
Trimethylamine |
|
Disulphide |
Isopropyl acetate |
There are four common toxic or asphyxiating gases present in almost every operation where anaerobic digestion of wastes occurs: carbon dioxide (CO2), ammonia (NH3), hydrogen sulphide (H2S) and methane (CH4). A small amount of carbon monoxide (CO) may also be produced by the decomposing animal wastes, but its main source is heaters used to burn fossil fuels. Typical ambient levels of these gases (as well as particulates) in swine confinement buildings are shown in table 2. Also listed are maximum recommended exposures in swine buildings based on recent research (Donham and Reynolds 1995; Reynolds et al. 1996) and threshold limit values (TLVs) set by the American Conference of Governmental Industrial Hygienists (ACGIH 1994). These TLVs have been adopted as legal limits in many countries.
Table 2. Ambient levels of various gases in swine confinement buildings
|
Gas |
Range (ppm) |
Typical ambient concentrations (ppm) |
Recommended maximum exposure concentrations (ppm) |
Threshold limit values (ppm) |
|
CO |
0 to 200 |
42 |
50 |
50 |
|
CO2 |
1,000 to 10,000 |
8,000 |
1,500 |
5,000 |
|
NH3 |
5 to 200 |
81 |
7 |
25 |
|
H2S |
0 to 1,500 |
4 |
5 |
10 |
|
Total dust |
2 to 15 mg/m3 |
4 mg/m3 |
2.5 mg/m3 |
10 mg/m3 |
|
Respirable dust |
0.10 to 1.0 mg/m3 |
0.4 mg/m3 |
0.23 mg/m3 |
3 mg/m3 |
|
Endotoxin |
50 to 500 ng/m3 |
200 ng/m3 |
100 ng/m3 |
(none established) |
It can be seen that in many of the buildings, at least one gas, and often several, exceeds the exposure limits. It should be noted that simultaneous exposure to these toxic substances may be additive or synergistic—the TLV for the mixture may be exceeded even when individual TLVs are not exceeded. Concentrations are often higher in the winter than in the summer, because ventilation is reduced to conserve heat.
These gases have been implicated in several acute conditions in workers. H2S has been implicated in many sudden animal deaths and several human deaths (Donham and Knapp 1982). Most acute cases have occurred shortly after the manure pit has been agitated or emptied, which may result in a sudden release of a large volume of the acutely toxic H2S. In other fatal cases, manure pits had recently been emptied, and workers who entered the pit for inspection, repairs or to retrieve a dropped object collapsed without any forewarning. The available post-mortem results of these cases of acute poisoning revealed massive pulmonary oedema as the only notable finding. This lesion, combined with the history, is compatible with hydrogen sulphide intoxication. Rescue attempts by bystanders have often resulted in multiple fatalities. Confinement workers should therefore be informed of the risks involved and advised never to enter a manure storage facility without testing for the presence of toxic gases, being equipped with a respirator with its own oxygen supply, ensuring adequate ventilation and having at least two other workers stand by, attached by a rope to the worker who enters, so they can effect a rescue without endangering themselves. There should be a written confined-space programme.
CO may also be present at acute toxic levels. Abortion problems in swine at an atmospheric concentration of 200 to 400 ppm and subacute symptoms in humans, such as chronic headache and nausea, have been documented in swine confinement systems. The possible effects on the human foetus should also be of concern. The primary source of CO is from improperly functioning hydrocarbon-burning heating units. Heavy accumulation of dust in swine confinement buildings makes it difficult to keep heaters in correct working order. Propane-fuelled radiant heaters are also a common source of lower levels of CO (e.g., 100 to 300 ppm). High-pressure washers powered by an internal combustion engine that may be run inside the building are another source; CO alarms should be installed.
Another acutely dangerous situation occurs when the ventilation system fails. Gas levels may then rapidly build up to critical levels. In this case the major problem is replacement of oxygen by other gases, primarily CO2 produced from the pit as well as from the respiratory activity of the animals in the building. Lethal conditions could be reached in as few as 7 hours. Regarding the health of the pigs, ventilation failure in warm weather may allow temperature and humidity to increase to lethal levels in 3 hours. Ventilation systems should be monitored.
A fourth potentially acute hazard arises from build-up of CH4, which is lighter than air and, when emitted from the manure pit, tends to accumulate in the upper portions of the building. There have been several instances of explosions occurring when the CH4 accumulation was ignited by a pilot light or a worker’s welding torch.
Bioactive Aerosols of Particulates
The sources of dust in confinement buildings are a combination of feed, dander and hair from the swine and dried faecal material (Donham and Scallon 1985). The particulates are about 24% protein and therefore have the potential not only for initiating an inflammatory response to foreign protein but also for initiating an adverse allergic reaction. The majority of particles are smaller than 5 microns, allowing them to be respired into the deep portions of the lungs, where they may produce a greater danger to health. The particulates are laden with microbes (104 to 107/m3 air). These microbes contribute several toxic/inflammatory substances including, among others, endotoxin (the most documented hazard), glucans, histamine and proteases. The recommended maximum concentrations for dusts are listed in table 2. Gases present within the building and bacteria in the atmosphere are adsorbed on the surface of the dust particles. Thus, the inhaled particles have the increased potentially hazardous effect of carrying irritating or toxic gases as well as potentially infectious bacteria into the lungs.
Infectious Diseases
Some 25 zoonotic diseases have been recognized as having occupational significance for agricultural workers. Many of these may be transmitted directly or indirectly from livestock. The crowded conditions prevailing in confinement systems offer a high potential for transmission of zoonotic diseases from livestock to humans. Swine confinement environment may offer a risk for transmission to workers of swine influenza, leptospirosis, Streptococcus suis and salmonella, for example. The poultry confinement environment may offer a risk for ornithosis, histoplasmosis, New Castle disease virus and salmonella. Bovine confinement could offer a risk for Q fever, Trichophyton verrucosum (animal ringworm) and leptospirosis.
Biologicals and antibiotics have also been recognized as potential health hazards. Injectable vaccines and various biologicals are commonly used in veterinary preventive medical programmes in animal confinement. Accidental inoculation of Brucella vaccines and Escherichia coli bacteria has been observed to cause illness in humans.
Antibiotics are commonly used both parenterally and incorporated in animal feed. Since it is recognized that feed is a common component of the dust present in animal confinement buildings, it is assumed that antibiotics are also present in the air. Thus, antibiotic hypersensitivity and antibiotic-resistant infections are potential hazards for the workers.
Noise
Noise levels of 103 dBA have been measured within animal confinement buildings; this is above the TLV, and offers a potential for noise-induced hearing loss (Donham, Yeggy and Dauge 1988).
Respiratory Symptoms of Livestock Confinement Workers
The general respiratory hazards within livestock confinement buildings are similar regardless of the species of livestock. However, swine confinements are associated with adverse health effects in a larger percentage of workers (25 to 70% of active workers), with more severe symptoms than those in poultry or cattle confinements (Rylander et al. 1989). The waste in poultry facilities is usually handled in solid form, and in this instance ammonia seems to be the primary gaseous problem; hydrogen sulphide is not present.
Subacute or chronic respiratory symptoms reported by confinement workers have been observed to be most frequently associated with swine confinement. Surveys of swine confinement workers have revealed that about 75% suffer from adverse acute upper respiratory symptoms. These symptoms can be broken down into three groups:
- acute or chronic inflammation of the respiratory airways (manifested as bronchitis)
- acquired occupational (non-allergic) constriction of the airways (asthma)
- delayed self-limited febrile illness with generalized symptoms (organic dust toxic syndrome (ODTS)).
Symptoms suggestive of chronic inflammation of the upper respiratory system are common; they are seen in about 70% of swine confinement workers. Most commonly, they include tightness of the chest, coughing, wheezing and excess sputum production.
In approximately 5% of workers, symptoms develop after working in the buildings for only a few weeks. The symptoms include chest tightness, wheezing and difficult breathing. Usually these workers are affected so severely that they are forced to seek employment elsewhere. Not enough is known to indicate whether this reaction is an allergic hypersensitivity or a non-allergic hypersensitivity to dust and gas. More typically, symptoms of bronchitis and asthma develop after 5 years of exposure.
Approximately 30% of workers occasionally experience episodes of delayed symptoms. Approximately 4 to 6 hours after working in the building they develop a flu-like illness manifested by fever, headache, malaise, general muscle aches and chest pain. They usually recover from these symptoms in 24 to 72 hours. This syndrome has been recognized as ODTS.
The potential for chronic lung damage certainly seems to be real for these workers. However, this has not been documented so far. It is recommended that certain procedures be followed to prevent chronic exposure as well as acute exposure to the hazardous materials in swine confinement buildings. Table 3 summarizes the medical conditions seen in swine confinement workers.
Table 3. Respiratory diseases associated with swine production
|
Upper airway disease |
Sinusitis |
|
Lower airway disease |
Occupational asthma |
|
Interstitial disease |
Alveolitis |
|
Generalized illness |
Organic dust toxic syndrome (ODTS) |
Sources: Donham, Zavala and Merchant 1984; Dosman et al. 1988; Haglind and Rylander 1987; Harries and Cromwell 1982; Heedrick et al. 1991; Holness et al. 1987; Iverson et al. 1988; Jones et al. 1984; Leistikow et al. 1989; Lenhart 1984; Rylander and Essle 1990; Rylander, Peterson and Donham 1990; Turner and Nichols 1995.
Worker Protection
Acute exposure to hydrogen sulphide. Care should always be taken to avoid exposure to H2S that may be given off when agitating an anaerobic liquid manure storage tank. If the storage is under the building, it is best to stay out of the building when the emptying procedure is going on and for several hours afterwards, until air sampling indicates it is safe. Ventilation should be at the maximum level during this time. A liquid manure storage facility should never be entered without the safety measures mentioned above being followed.
Particulate exposure. Simple management procedures, such as the use of automated feeding equipment designed to eliminate as much feed dust as possible should be used to control particulate exposure. Adding extra fat to feed, frequent power-washing of the building and installing slatted flooring that cleans well are all proven control measures. An oil-misting dust-control system is presently under study and may be available in the future. In addition to good engineering control, a good-quality dust mask should be worn.
Noise. Ear protectors should be provided and worn, particularly when working in the building in order to vaccinate the animals or for other management procedures. A hearing conservation programme should be instituted.
Forage Crops
As populations tended to concentrate and the need for winter feeding in northern climates grew, the need to harvest, cure and feed hay to domestic animals emerged. Although pasture dates to the earliest domestication of animals, the first cultivated forage plant may have been alfalfa, with its recorded use dating back to 490 BC in Persia and Greece.
Livestock forage is a crucial input for livestock rearing. Forages are grown for their vegetation and not their grains or seeds. Stems, leaves and inflorescences (flower clusters) of some legumes (e.g., alfalfa and clover) and a variety of non-legume grasses are used for grazing or harvested and fed to livestock. When grain crops such as corn, sorghum or straw are harvested for their vegetation, they are considered forage crops.
Production Processes
The major categories of forage crops are pastures and open ranges, hay and silage. Forage crops can be harvested by livestock (in pastures) or by humans, either by hand or machinery. The crop can be used for farm feeding or for sale. In forage production, tractors are a source of traction and processing power, and, in dry areas, irrigation may be required.
Pasture is fed by allowing the livestock to graze or browse. The type of pasture crop, typically grass, varies in its production with the season of the year, and pastures are managed for spring, summer and fall grazing. Range management focuses on not overgrazing an area, which involves rotating livestock from one area to another. Crop residues may be part of the pasture diet for livestock.
Alfalfa, a popular hay crop, is not a good pasture crop because it causes bloating in ruminants, a condition of a gas build-up in the rumen (the first part of the cow’s stomach) that can kill a cow. In temperate climates, pastures are ineffective as a feed source in the winter, so stored feed is needed. Moreover, in large operations, harvested forage—hay and silage—is used because pasture is impractical for large concentrations of animals.
Hay is forage that is grown and dry-cured before storage and feeding. After the hay crop has grown, it is cut with a mowing machine or swather (a machine that combines the mowing and raking operations) and raked by a machine into a long row for drying (a windrow). During these two processes it is field cured for baling. Historically harvesting was done by pitchforking loose hay, which may still be used to feed the animals. Once cured, the hay is baled. The baling machine picks up the hay from the windrow, and compresses and wraps it into either a small square bale for manual handling, or large square or round bales for mechanical handling. The small bale may be kicked mechanically from the baler back into a trailer, or it may be picked up by hand and placed—a task called bucking—onto a trailer for transport to the storage area. The bales are stored in stacks, usually under a cover (barn, shed or plastic) to protect them from rain. Wet hay can easily spoil or spontaneously combust from the heat of the decaying process. Hay may be processed for commercial use into compressed pellets or cubes. A crop can be cut several times in a season, three times being typical. When it is fed, a bale is moved to the feeding trough, opened and placed into the trough where the animal can reach it. This part of the operation is typically manual.
Other forage that is harvested for livestock feeding is corn or sorghum for silage. The economic advantage is that corn has as much as 50% more energy when harvested as silage than grain. A machine is used to harvest most of the green plant. The crop is cut, crushed, chopped and ejected into a trailer. The material is then fed as green chop or stored in a silo, where it undergoes fermentation in the first 2 weeks. The fermentation establishes an environment that prevents spoilage. Over a year, the silo is emptied as the silage is fed to livestock. This feeding process is primarily mechanical.
Hazards and Their Prevention
The storage of animal feed presents health hazards for workers. Early in the storage process, nitrogen dioxide is produced and can cause serious respiratory damage and death (“silo filler’s disease”). Storage in enclosed environments, such as silos, can create this hazard, which can be avoided by not entering silos or enclosed storage spaces in the first few weeks after feed has been stored. Further problems can occur later if the alfalfa, hay, straw or other forage crop was wet when it was stored and there is a build-up of fungi and other microbial contaminants. This can result in acute respiratory illness (“silo unloader’s disease”, organic dust toxicity) and/or chronic respiratory diseases (“farmer’s lung”). The risk of acute and chronic respiratory diseases can be reduced through the use of appropriate respirators. There should also be appropriate confined space entry procedures.
The straw and hay used for bedding is usually dry and old, but may contain moulds and spores which can cause respiratory symptoms when dust is made airborne. Dust respirators can reduce exposure to this hazard.
Harvesting and baling equipment and bedding choppers are designed to chop, cut and mangle. They have been associated with traumatic injuries to farm workers. Many of these injuries occur when workers try to clear clogged parts while the equipment is still operating. The equipment should be turned off before clearing jams. If more than one person is working, then a lockout/tagout programme should be in effect. Another major source of injuries and fatalities is tractor overturns without proper roll-over protection for the driver (Deere & Co. 1994). More information on farm machinery hazards is also discussed elsewhere in this Encyclopaedia.
Where animals are used to plant, harvest and store feed, there is a possibility of animal-related injuries from kicks, bites, strains, sprains, crush injuries and lacerations. Correct animal handling techniques are the most likely means to reduce these injuries.
Manual handling of bales of hay and straw can result in ergonomic problems. Workers should be trained in correct lifting procedures, and mechanical equipment should be used where possible.
Forage and bedding are fire hazards. Wet hay, as mentioned previously, is a spontaneous combustion hazard. Dry hay, straw and so forth will burn easily, especially when loose. Even bailed forage is a major fuel source in a fire. Basic fire precautions should be instituted, such as no-smoking rules, elimination of spark sources and fire suppression measures.
Case Study: Arthropod-Related Occupational Health Problems
Arthropods comprise more than 1 million species of insects and thousands of species of ticks, mites, spiders, scorpions and centipedes. Bees, ants, wasps and scorpions sting and inject venom; mosquitoes and ticks suck blood and transmit diseases; and the scales and hairs from insect bodies can irritate the eyes and skin, as well as tissues in the nose, mouth and respiratory system. Most stings in humans are from social bees (bumble bees, honey bees). Other stings are from paper wasps, yellow jackets, hornets and ants.
Arthropods can be a health hazard in the workplace (see table 1), but in most cases, potential arthropod hazards are not unique to specific occupations. Rather, exposure to arthropods in the workplace depends on geographic location, local conditions and the time of year. Table 2 lists some of these hazards and their corresponding arthropod agents. For all arthropod hazards, the first line of defence is avoidance or exclusion of the offending agent. Venom immunotherapy may increase a person’s tolerance to arthropod venom and is accomplished by injecting increasing doses of venom over time. It is effective in 90 to 100% of venom hypersensitive individuals but involves an indefinite course of expensive injections. Table 3 lists normal and allergic reactions to insect stings.
Table 1. Different occupations and their potential for contact with arthropods that may adversely affect health and safety.
|
Occupation |
Arthropods |
|
Construction personnel, environmentalists, farmers, fishers, foresters, fish and wildlife workers, naturalists, transportation workers, park rangers, utility workers |
Ants, bees, biting flies, caterpillars, chiggers, centipedes, caddisflies, fly maggots, mayflies, scorpions, spiders, ticks, wasps |
|
Cosmetics manufacturers, dock workers, dye makers, factory workers, food processors, grainery workers, homemakers, millers, restaurant workers |
Ants; beetles; bean, grain and pea weevils; mites; scale insects; spiders |
|
Beekeepers |
Ants, bumble bees, honey bees, wasps |
|
Insect production workers, laboratory and field biologists, museum curators |
Over 500 species of arthropods are reared in the laboratory. Ants, beetles, mites, moths, spiders and ticks are especially important. |
|
Hospital and other health care workers, school administrators, teachers |
Ants, beetles, biting flies, caterpillars, cockroaches, mites |
|
Silk producers |
Silk worms |
Table 2. Potential arthropod hazards in the workplace and their causative agent(s)
|
Hazard |
Arthropod agents |
|
Bites, envenomation1 |
Ants, biting flies, centipedes, mites, spiders |
|
Sting envenomation, venom hypersensitivity2 |
Ants, bees, wasps, scorpions |
|
Tick toxicosis/paralysis |
Ticks |
|
Asthma |
Beetles, caddisflies, caterpillars, cockroaches, crickets, dust mites, fly maggots, grain mites, grain weevils, grasshoppers, honeybees, mayflies, moths, silk worms |
|
Contact dermatitis3 |
Blister beetles, caterpillars, cockroaches, dried fruit mites, dust mites, grain mites, straw itch mites, moths, silk worms, spiders |
1 Envenomation with poison from glands associated with mouthparts.
2 Envenomation with poison from glands not associated with mouthparts.
3 Includes primary irritant and allergic dermatitis.
Table 3. Normal and allergic reactions to insect sting
|
Type of response |
Reaction |
| I. Normal, non-allergic reactions at the time of the sting |
Pain, burning, itching, redness at the sting site, white area surrounding the sting site, swelling, tenderness |
| II. Normal, non-allergic reactions hours or days after sting |
Itching, residual redness, small brown or red damage spot at sting site, swelling at the sting site |
|
III. Large local reactions |
Massive swelling around the sting site extending over an area 10 cm or more and increasing in size for 24 to 72 hours, sometimes lasting up to a week or more |
|
IV. Cutaneous allergic reactions |
Hives anywhere on the skin, massive swelling remote from the sting site, generalized itching of the skin, generalized redness of the skin remote from the sting site |
|
V. Non life-threatening systemic |
Allergic rhinitis, minor respiratory symptoms, abdominal cramps |
|
VI. Life-threatening systemic allergic reactions |
Shock, unconsciousness, hypotension or fainting, difficulty in breathing, massive swelling in the throat. |
Source: Schmidt 1992.
Health Problems and Disease Patterns
The domestication of animals occurred independently in a number of areas of the Old and New World over 10,000 years ago. Until domestication, hunting and gathering was the predominant subsistence pattern. The transformation to human control over animal and plant production and reproduction processes resulted in revolutionary changes in the structure of human societies and their relationships to the environment. The change to agriculture marked an increase in labour intensity and work time spent in food procurement-related activities. Small nuclear families, adapted to nomadic hunting and gathering groups, were transformed into large, extended, sedentary social units suited to labour-intensive domesticated food production.
The domestication of animals increased human susceptibility to animal-related injuries and diseases. Larger non-nomadic populations quartered in close proximity to animals provided greater opportunity for transmission of disease between animals and humans. The development of larger herds of more intensely handled livestock also increased the likelihood of injuries. Throughout the world, differing forms of animal agriculture are associated with varying risks for injury and disease. For example, the 50 million inhabitants who practice swidden (cut and burn) agriculture in equatorial regions face different problems from the 35 million pastoral nomads across Scandinavia and through central Asia or the 48 million food producers who practise an industrialized form of agriculture.
In this article, we provide an overview of selected injury patterns, infectious diseases, respiratory diseases and skin diseases associated with livestock production. The treatment is topically and geographically uneven because most research has been conducted in industrialized countries, where intensive forms of livestock production are common.
Overview
Types of human health problems and disease patterns associated with livestock production can be grouped according to the type of contact between animals and people (see table 1). Contact can occur via direct physical interaction, or contact with an organic or inorganic agent. Health problems associated with all types of livestock production can be grouped into each of these areas.
Table 1. Types of human health problems associated with livestock production
Health problems from direct physical contact
Allergic contact dermatitis
Allergic rhinitis
Bites, kicks, crushing
Envenomation and possible hypersensitivity
Asthma
Scratches
Traumatic injury
Health problems from organic agents
Agrochemical poisoning
Antibiotic resistance
Chronic bronchitis
Contact dermatitis
Allergies from drug residue food exposures
Food-borne illnesses
“Farmer’s lung”
Hypersensitivity pneumonitis
Mucous membrane irritation
Occupational asthma
Organic dust toxic syndrome (ODTS)
Allergies from pharmaceutical exposures
Zoonotic diseases
Health problems from physical agents
Hearing loss
Machinery-related trauma
Methane emission and greenhouse effect
Musculoskeletal disorders
Stress
Direct human contact with livestock ranges from the brute force of large animals such as the Chinese buffalo to the undetected skin contact by microscopic hairs of the Japanese oriental tussock moth. A corresponding range of health problems can result, from the temporary irritant to the debilitating physical blow. Notable problems include traumatic injuries from handling large livestock, venom hypersensitivity or toxicosis from venomous arthropod bites and stings, and contact and allergic contact skin dermatitis.
A number of organic agents utilize various pathways from livestock to humans, resulting in a range of health problems. Among the most globally important are zoonotic diseases. Over 150 zoonotic diseases have been identified worldwide, with approximately 40 significant for human health (Donham 1985). The importance of zoonotic diseases depends on regional factors such as agricultural practices, environment and a region’s social and economic status. The health consequences of zoonotic diseases range from the relatively benign flu-like symptoms of brucellosis to debilitating tuberculosis or potentially lethal strains of Escherichia coli or rabies.
Other organic agents include those associated with respiratory disease. Intensive livestock production systems in confined buildings create enclosed environments where dust, including microbes and their by-products, becomes concentrated and aerosolized along with gases that are in turned breathed by people. Approximately 33% of swine confinement workers in the United States suffer from organic dust toxic syndrome (ODTS) (Thorne et al. 1996).
Comparable problems exist in dairy barns, where dust containing endotoxin and/or other biologically active agents in the environment contributes to bronchitis, occupational asthma and inflammation of the mucous membrane. While these problems are most notable in developed countries where industrialized agriculture is widespread, the increasing export of confined livestock production technologies to developing areas such as Southeast Asia and Central America increases the risks for workers there.
Health problems from physical agents typically involve tools or machinery either directly or indirectly involved with livestock production in the agricultural work environment. Tractors are the leading cause of farm fatalities in developed countries. In addition, elevated rates of hearing loss associated with machinery and confined livestock production noises, and musculoskeletal disorders from repetitive motions, are also consequences of industrialized forms of animal agriculture. Agricultural industrialization, characterized by the use of capital-intensive technologies which interface between humans and the physical environment to produce food, is behind the growth of physical agents as significant livestock-related health factors.
Injuries
Direct contact with livestock is a leading cause of injuries in many industrialized regions of the world. In the United States, the national Traumatic Injury Surveillance of Farmers (NIOSH 1993) indicates that livestock is the primary source of injury, with cattle, swine and sheep constituting 18% of all agricultural injuries and accounting for the highest rate of lost workdays. This is consistent with a 1980-81 survey conducted by the US National Safety Council (National Safety Council 1982).
Regional US studies consistently show livestock as a leading cause of injury in agricultural work. Early work on hospital visits by farmers in New York from 1929 to 1948 revealed livestock accounting for 17% of farm-related injuries, second only to machinery (Calandruccio and Powers 1949). Such trends continue, as research indicates livestock account for at least one-third of agricultural injuries among Vermont dairy farmers (Waller 1992), 19% of injuries among a random sample of Alabama farmers (Zhou and Roseman 1995), and 24% of injuries among Iowa farmers (Iowa Department of Public Health 1995). One of the few studies to analyse risk factors for livestock-specific injuries indicates such injuries may be related to the organization of production and specific features of the livestock rearing environment (Layde et al. 1996).
Evidence from other industrialized agricultural areas of the world reveals similar patterns. Research from Australia indicates that livestock workers have the second-highest occupational fatal injury rates in the country (Erlich et al. 1993). A study of accident records and emergency department visits of British farmers in West Wales (Cameron and Bishop 1992) reveals livestock were the leading source of injuries, accounting for 35% of farm-related accidents. In Denmark, a study of 257 hospital-treated agricultural injuries revealed livestock as the second-leading cause of injuries, accounting for 36% of injuries treated (Carstensen, Lauritsen and Rasmussen 1995). Surveillance research is necessary to address the lack of systematic data on livestock-related injury rates in developing areas of the world.
Prevention of livestock-related injuries involves understanding animal behaviour and respecting dangers by acting appropriately and using appropriate control technologies. Understanding animal habits related to feeding behaviours and environmental fluctuations, social relationships such as animals isolated from their herd, nurturing and protective instincts of female animals and the variable territorial nature and feeding patterns of livestock are critical in reducing the risk of injury. Prevention of injury also depends on using and maintaining livestock control equipment such as fences, pens, stalls and cages. Children are at particular risk and should be supervised in designated play areas well away from livestock holding areas.
Infectious Diseases
Zoonotic diseases can be classified according to their modes of transmission, which are in turn linked to forms of agriculture, human social organization and the ecosystem. The four general routes of transmission are:
- direct single vertebrate host
- cyclical multiple vertebrate host
- combination vertebrate-invertebrate host
- inanimate intermediary host.
Zoonotic diseases can be generally characterized as follows: they are non-fatal, infrequently diagnosed and sporadic rather than epidemic; they mimic other diseases; and humans are typically the dead-end hosts. Primary zoonotic diseases by region are listed in table 2.
Table 2. Primary zoonoses by world region
|
Common name |
Principal source |
Region |
|
Anthrax |
Mammals |
Eastern Mediterranean, West and Southeast Asia, Latin America |
|
Brucellosis |
Goats, sheep, cattle, swine |
Europe, Mediterranean area, United States |
|
Encephalitis, arthropod-borne |
Birds, sheep, rodents |
Africa, Australia, Central Europe, Far East, Latin America, Russia, United States |
|
Hydatidosis |
Dogs, ruminants, swine, wild carnivores |
Eastern Mediterranean, southern South America, South and East Africa, New Zealand, southern Australia, Siberia |
|
Leptospirosis |
Rodents, cattle, swine, wild carnivores, horses |
Worldwide, more prevalent in Caribbean |
|
Q fever |
Cattle, goats, sheep |
Worldwide |
|
Rabies |
Dogs, cats, wild carnivores, bats |
Worldwide |
|
Salmonellosis |
Birds, mammals |
Worldwide, most prevalent in regions with industrial agriculture and higher use of antibiotics |
|
Trichinosis |
Swine, wild carnivores, Arctic animals |
Argentina, Brazil, Central Europe, Chile North America, Spain |
|
Tuberculosis |
Cattle, dogs, goats |
Worldwide, most prevalent in developing countries |
Rates of zoonotic diseases among human populations are largely unknown owing to the lack of epidemiological data and to misdiagnoses. Even in industrialized countries such as the United States, zoonotic diseases such as leptospirosis are frequently mistaken for influenza. Symptoms are non-specific, making diagnosis difficult, a characteristic of many zoonoses.
Prevention of zoonotic diseases consists of a combination of disease eradication, animal vaccinations, human vaccinations, work environment sanitation, cleaning and protecting open wounds, appropriate food handling and preparation techniques (such as pasteurization of milk and thorough cooking of meat), use of personal protection equipment (such as boots in rice fields) and prudent use of antibiotics to reduce the growth of resistant strains. Control technologies and preventive behaviours should be conceptualized in terms of pathways, agents and hosts and specifically targeted to the four routes of transmission.
Respiratory Diseases
Given the variety and extent of exposures related to livestock production, respiratory diseases may be the major health problem. Studies in some sectors of livestock production in developed areas of the world reveal that 25% of livestock workers suffer from some form of respiratory disease (Thorne et al. 1996). The kinds of work most commonly associated with respiratory problems include grain production and handling and working in animal confinement units and dairy farming.
Agricultural respiratory diseases may result from exposures to a variety of dusts, gases, agricultural chemicals and infectious agents. Dust exposures may be divided into those primarily consisting of organic components and those consisting mainly of inorganic components. Field dust is the primary source of inorganic dust exposures. Organic dust is the major respiratory exposure to agricultural production workers. Disease results from periodic short-term exposures to agricultural organic dust containing large numbers of microbes.
ODTS is the acute flu-like illness seen following periodic short-term exposure to high concentrations of dust (Donham 1986). This syndrome has features very similar to those of acute farmer’s lung, but does not carry the risk of pulmonary impairment associated with farmer’s lung. Bronchitis affecting agricultural workers has both an acute and chronic form (Rylander 1994). Asthma, as defined by reversible airway obstruction associated with airway inflammation, can also be caused by agricultural exposures. In most cases this type of asthma is related to chronic inflammation of the airways rather than a specific allergy.
A second common exposure pattern is daily exposure to a lower level of organic dust. Typically, total dust levels are 2 to 9 mg/m3, microbe counts are at 103 to 105 organisms/m3 and endotoxin concentration is 50 to 900 EU/m3. Examples of such exposures include work in a swine confinement unit, a dairy barn or a poultry-growing facility. Usual symptoms seen with these exposures include those of acute and chronic bronchitis, an asthma-like syndrome and symptoms of mucous membrane irritation.
Gases play an important role in causing lung disorders in the agricultural setting. In swine confinement buildings and in poultry facilities, ammonia levels often contribute to respiratory problems. Exposure to the fertilizer anhydrous ammonia has both acute and long-term effects on the respiratory tract. Acute poisoning from hydrogen sulphide gas released from manure storage facilities in dairy barns and swine confinement units can cause fatalities. Inhalation of insecticidal fumigants can also lead to death.
Prevention of respiratory illnesses may be aided by controlling the source of dusts and other agents. In livestock buildings, this includes managing a correctly designed ventilation system and frequent cleaning to prevent build-up of dust. However, engineering controls alone are likely insufficient. Correct selection and use of a dust respirator is also needed. Alternatives to confinement operations can also be considered, including pasture-based and partially enclosed production arrangements, which can be as profitable as confined operations, particularly when occupational health costs are considered.
Skin Problems
Skin problems can be categorized as contact dermatitis, sun-related, infectious or insect-induced. Estimates indicate that agricultural workers are at highest occupational risk for certain dermatoses (Mathias 1989). While prevalence rates are lacking, particularly in developing regions, studies in the United States indicate that occupational skin disease may account for up to 70% of all occupational diseases among agricultural workers in certain regions (Hogan and Lane 1986).
There are three types of contact dermatoses: irritant dermatitis, allergic dermatitis and photocontact dermatitis. The most common form is irritant contact dermatitis, while allergic contact dermatitis is less common and photocontact reactions are rare (Zuehlke, Mutel and Donham 1980). Common sources of contact dermatitis on the farm include fertilizers, plants and pesticides. Of particular note is dermatitis from contact with livestock feed. Feeds containing additives such as antibiotics may result in allergic dermatitis.
Light-complexioned farmers in developing areas of the world are at particular risk for chronic sun-induced skin problems, including wrinkling, actinic keratoses (scaly non-cancerous lesions) and skin cancer. The two most common types of skin cancer are squamous and basal cell carcinomas. Epidemiological work in Canada indicates that farmers are at higher risk for squamous cell carcinoma than non-farmers (Hogan and Lane 1986). Squamous cell carcinomas often arise from actinic keratoses. Approximately 2 out of 100 squamous cell carcinomas metastasize, and they are most common on the lips. Basal cell carcinomas are more common and occur on the face and ears. While locally destructive, basal cell carcinomas rarely metastasize.
Infectious dermatoses most relevant for livestock workers are ringworm (dermatophytic fungi), orf (contagious ecthyma) and milker’s nodule. Ringworm infections are superficial skin infections that appear as red scaling lesions that result from contact with infected livestock, particularly dairy cattle. A study from India, where cattle generally roam free, revealed over 5% of rural inhabitants suffering from ringworm infections (Chaterjee et al. 1980). Orf, by contrast, is a pox virus usually contracted from infected sheep or goats. The result is typically lesions on the backs of hands or fingers which usually disappear with some scarring in about 6 weeks. Milker’s nodules result from infection with the pseudocowpox poxvirus, typically from contact with infected udders or teats of milk cows. These lesions appear similar to those of orf, though they are more often multiple.
Insect-induced dermatoses result primarily from bites and stings. Infections from mites that parasitize livestock or contaminate grains is particularly notable among livestock handlers. Chigger bites and scabies are typical skin problems from mites that result in various forms of reddened irritations that usually heal spontaneously. More serious are bites and stings from various insects such as bees, wasps, hornets or ants that result in anaphylactic reactions. Anaphylactic shock is a rare hypersensitivity reaction that occurs with an overproduction of chemicals emitted from white blood cells that result in constriction of the airways and can lead to cardiac arrest.
All of these skin problems are largely preventable. Contact dermatitis can be prevented by reducing exposures through use of protective clothing, gloves and appropriate personal hygiene. Additionally, insect-related problems can be prevented by wearing light-coloured and nonflowery clothing and by avoiding scented skin applications. The risk of skin cancer can be dramatically reduced by using appropriate clothing to minimize exposure, such as a wide-brimmed hat. Use of appropriate sunscreen lotions can also be helpful, but should not be relied upon.
Conclusion
The number of livestock worldwide has grown apace with the increase in human population. There are approximately 4 billion cattle, pigs, sheep, goats, horses, buffalo and camels in the world (Durning and Brough 1992). However, there is a notable lack of data on livestock-related human health problems in developing areas of the world such as China and India, where much of the livestock currently reside and where future growth is likely to occur. However, given the emergence of industrialized agriculture worldwide, it can be anticipated that many of the health problems documented in North American and European livestock production will likely accompany the emergence of industrialized livestock production elsewhere. It is also anticipated that health services in these areas will be inadequate to deal with the health and safety consequences of industrialized livestock production generally described here.
The worldwide emergence of industrialized livestock production with its attendant human health consequences will accompany fundamental changes in the social, economic and political order comparable to those that followed from the domestication of animals over 10,000 years ago. Preventing human health problems will require broad understanding and appropriate engagement of these new forms of human adaptation and the place of livestock production within them.
Livestock Rearing: Its Extent and Health Effects
Overview
Humans depend upon animals for food and related by-products, work and a variety of other uses (see table 1). To meet these demands, they have domesticated or held in captivity species of mammals, birds, reptiles, fish and arthropods. These animals have become known as livestock, and rearing them has implications for occupational safety and health. This general profile of the industry includes its evolution and structure, the economic importance of different commodities of livestock, and regional characteristics of the industry and workforce. The articles in this chapter are organized by occupational processes, livestock sectors and consequences of livestock rearing.
Table 1. Livestock uses
|
Commodity |
Food |
By-products and other uses |
|
Dairy |
Fluid and dried milk, butter, cheese and curd, casein, evaporated milk, cream, yoghurt and other fermented milk, ice cream, whey |
Male calves and old cows sold into the cattle commodity market; milk as an industrial feedstock of carbohydrates (lactose as a diluent for drugs), proteins (used as a surfactant to stabilize food emulsions) and fats (lipids have potential uses as emulsifiers, surfactants and gels), offal |
|
Cattle, buffalo, sheep |
Meat (beef, mutton), edible tallow |
Hides and skins (leather, collagens for sausage casings, cosmetics, wound dressing, human tissue repair), offal, work (traction), wool, hair, dung (as fuel and fertilizer), bone meal, religious objects, pet food, tallow and grease (fatty acids, varnish, rubber goods, soaps, lamp oil, plastics, lubricants) fat, blood meal |
|
Poultry |
Meat, eggs, duck eggs (in India) |
Feathers and down, manure (as fertilizer), leather, fat, offal, flightless bird oil (carrier for dermal path pharmaceuticals), weed control (geese in mint fields) |
|
Pig |
Meat |
Hides and skins, hair, lard, manure, offal |
|
Fish (aquaculture) |
Meat |
Fishmeal, oil, shell, aquarium pets |
|
Horse, other equines |
Meat, blood, milk |
Recreation (riding, racing), work (riding, traction), glue, dog feed, hair |
|
Micro-livestock (rabbit, guinea pig), dog, cat |
Meat |
Pets, furs and skins, guard dogs, seeing-eye dogs, hunting dogs, experimentation, sheep herding (by the dog), rodent control (by the cat) |
|
Bulls |
Recreation (bull-fighting, rodeo riding), semen |
|
|
Insects and other invertebrates (e.g., |
Honey, 500 species (grubs, grasshoppers, ants, crickets, termites, locusts, beetle larvae, wasps and bees, moth caterpillars) are a regular diet among many non-western societies |
Beeswax, silk, predatory insects (>5,000 species are possible and 400 are known as controls for crop pests; the carnivorous “tox” mosquito |
Sources: DeFoliart 1992; Gillespie 1997; FAO 1995; O’Toole 1995; Tannahil 1973; USDA 1996a, 1996b.
Evolution and structure of the industry
Livestock evolved over the past 12,000 years through selection by human communities and adaptation to new environments. Historians believe that goat and sheep were the first species of animals domesticated for human use. Then, about 9,000 years ago, humans domesticated the pig. The cow was the last major food animal that humans domesticated, about 8,000 years ago in Turkey or Macedonia. It was probably only after cattle were domesticated that milk was discovered as a useful foodstuff. Goat, sheep, reindeer and camel milk were also used. People of the Indus valley domesticated the Indian jungle fowl primarily for its egg production, which became the world’s chicken, with its source of eggs and meat. People of Mexico had domesticated the turkey (Tannahill 1973).
Humans used several other mammalian and avian species for food, as well as amphibian and fish species and various arthropods. Insects have always provided an important source of protein, and today they are part of the human diet principally in the world’s non-western cultures (DeFoliart 1992). Honey from the honey bee was an early food; smoking bees from their nest to collect honey was known in Egypt as early as 5,000 years ago. Fishing is also an ancient occupation used to produce food, but because fishers are depleting wild fisheries, aquaculture has been the fastest growing contributor to fish production since the early 1980s, contributing about 14% to the total current production of fish (Platt 1995).
Humans also domesticated many mammals for use for draught, including the horse, donkey, elephant, dog, buffalo, camel and reindeer. The first animal used for draught, perhaps with the exception of the dog, was likely the goat, which could defoliate scrub for land cultivation through its browsing. Historians believe that Asians domesticated the Asian wolf, which was to become the dog, 13,000 years ago. The dog proved to be useful to the hunter for its speed, hearing and sense of smell, and the sheepdog aided in the early domestication of sheep (Tannahill 1973). The people of the steppe lands of Eurasia domesticated the horse about 4,000 years ago. Its use for work (traction) was stimulated by the invention of the horseshoe, collar harness and feeding of oats. Although draught is still important in much of the world, farmers displace draught animals with machines as farming and transportation becomes more mechanized. Some mammals, such as the cat, are used to control rodents (Caras 1996).
The structure of the current livestock industry can be defined by commodities, the animal products that enter the market. Table 2 shows a number of these commodities and the worldwide production or consumption of these products.
Table 2. International livestock production (1,000 tonnes)
|
Commodity |
1991 |
1992 |
1993 |
1994 |
1995 |
1996 |
|
Beef and veal carcasses |
46,344 |
45,396 |
44,361 |
45,572 |
46,772 |
47,404 |
|
Pork carcasses |
63,114 |
64,738 |
66,567 |
70,115 |
74,704 |
76,836 |
|
Lamb, mutton, goat carcasses |
6,385 |
6,245 |
6,238 |
6,281 |
6,490 |
6,956 |
|
Bovine hides and skins |
4,076 |
3,983 |
3,892 |
3,751 |
3,778 |
3,811 |
|
Tallow and grease |
6,538 |
6,677 |
7,511 |
7,572 |
7,723 |
7,995 |
|
Poultry meat |
35,639 |
37,527 |
39,710 |
43,207 |
44,450 |
47,149 |
|
Cow’s milk |
385,197 |
379,379 |
379,732 |
382,051 |
382,747 |
385,110 |
|
Shrimps |
815 |
884 |
N/A |
N/A |
N/A |
N/A |
|
Molluscs |
3,075 |
3,500 |
N/A |
N/A |
N/A |
N/A |
|
Salmonoids |
615 |
628 |
N/A |
N/A |
N/A |
N/A |
|
Freshwater fish |
7,271 |
7,981 |
N/A |
N/A |
N/A |
N/A |
|
Egg consumption (million pieces) |
529,080 |
541,369 |
567,469 |
617,591 |
616,998 |
622,655 |
Sources: FAO 1995; USDA 1996a, 1996b.
Economic importance
The world’s growing population and increased per capita consumption both increased the global demand for meat and fish, the results of which are shown in figure 1. Global meat production nearly trebled between 1960 and 1994. Over this period, per capita consumption increased from 21 to 33 kilograms per annum. Because of the limitations of available rangeland, beef production levelled off in 1990. As a result, animals that are more efficient in converting feed grain into meat, such as pigs and chickens, have gained a competitive advantage. Both pork and poultry have been increasing in dramatic contrast to beef production. Pork overtook beef in worldwide production in the late 1970s. Poultry may soon exceed beef production. Mutton production remains low and stagnant (USDA 1996a). Milk cows worldwide have been slowly decreasing while milk production has been increasing because of increasing production per cow (USDA 1996b).
Figure 1. World production of meat and fish
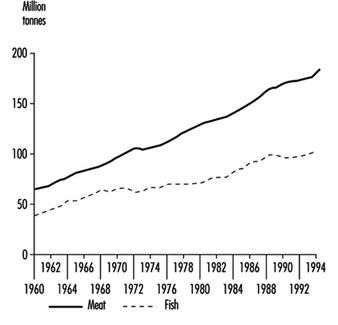
Aquaculture production increased at an annual rate of 9.1% from 1984 to 1992. Aquaculture animal production increased from 14 million tonnes worldwide in 1991 to 16 million tonnes in 1992, with Asia providing 84% of world production (Platt 1995). Insects are rich in vitamins, minerals and energy, and provide between 5% and 10% of the animal protein for many people. They also become a vital source of protein during times of famine (DeFoliart 1992).
Regional Characteristics of the Industry and Workforce
Separating the workforce engaged in livestock rearing from other agricultural activities is difficult. Pastoral activities, such as those in much of Africa, and heavy commodity-based operations, such as those in the United States, have differentiated more between livestock and crop raising. However, many agro-pastoral and agronomic enterprises integrate the two. In much of the world, draught animals are still used extensively in crop production. Moreover, livestock and poultry depend upon feed and forage generated from crop operations, and these operations are commonly integrated. The principal aquaculture species in the world is the plant-eating carp. Insect production is also tied directly to crop production. The silkworm feeds exclusively on mulberry leaves; honeybees depend upon flower nectar; plants depend upon them for pollination work; and humans harvest edible grubs from various crops. The 1994 world population totalled 5,623,500,000, and 2,735,021,000 people (49% of the population) were engaged in agriculture (see figure 2). The largest contribution to this workforce is in Asia, where 85% of the agricultural population rear draught animals. Regional characteristics related to livestock rearing follow.
Figure 2. Human population engaged in agriculture by world region, 1994.

Sub-Saharan Africa
Animal husbandry has been practised in sub-Saharan Africa for more than 5,000 years. Nomadic husbandry of the early livestock has evolved species that tolerate poor nutrition, infectious diseases and long migrations. About 65% of this region, much of it around desert areas, is suitable only for producing livestock. In 1994, 65% of the approximately 539 million people in sub-Saharan Africa depended upon agricultural income, down from 76% in 1975. Although its importance has grown since the mid-1980s, aquaculture has contributed little to the food supply for this region. Aquaculture in this region is based upon pond farming of tilapias, and export enterprises have attempted to culture marine shrimps. An export aquaculture industry in this region is expected to grow because Asian demand for fish is expected to increase, which will be fuelled by Asian investment and technology drawn to the region by a favourable climate and by African labour.
Asia and the Pacific
In Asia and the Pacific region, nearly 76% of the world’s agricultural population exists on 30% of the world’s arable land. About 85% of the farmers use cattle (bullocks) and buffaloes to cultivate and thresh crops.
Livestock rearing operations are mainly small-scale units in this region, but large commercial farms are establishing operations near urban centres. In rural areas, millions of people depend on livestock for meat, milk, eggs, hides and skins, draught power and wool. China exceeds the rest of the world with 400 million pigs; the remainder of the world has a total of 340 million pigs. India accounts for over one-fourth of the number of cattle and buffaloes worldwide, but because of religious policies that restrict cattle slaughter, India contributes less than 1% to the world’s beef supply. Milk production is a part of traditional agriculture in many countries of this region. Fish is a frequent ingredient in most people’s diet in this region. Asia contributes 84% of the world’s aquaculture production. At 6,856,000 tonnes, China alone produces nearly half of the world production,. Demand for fish is expected to increase rapidly, and aquaculture is expected to meet this demand.
Europe
In this region of 802 million people, 10.8% were engaged in agriculture in 1994, which has decreased significantly from 16.8% in 1975. Increased urbanization and mechanization have led to this decrease. Much of this arable land is in the moist, cool northern climates and is conducive to growing pastures for livestock. As a result, much of the livestock raising is located in the northern part of this region. Europe contributed 8.5% to the world’s production of aquaculture in 1992. Aquaculture has concentrated on relatively high-value species of finfish (288,500 tonnes) and shellfish (685,500 tonnes).
Latin America and the Caribbean
The Latin American and Caribbean region differs from other regions in many ways. Large tracts of land remain to be exploited, the region has large populations of domestic animals and much of the agriculture is operated as large operations. Livestock represents about one-third of the agricultural production, which makes up a significant part of the gross domestic product. Meat from beef cattle accounts for the largest share and makes up 20% of the world’s production. Most livestock species have been imported. Among those indigenous species that have been domesticated are guinea pigs, dogs, llamas, alpacas, Muscovy ducks, turkeys and black chickens. This region contributed only 2.3% to world aquaculture production in 1992.
Near East
Currently, 31% of the population of the Near East is engaged in agriculture. Because of the shortage of rainfall in this region, the only agricultural use for 62% of this land area is animal grazing. Most of the major livestock species were domesticated in this region (goats, sheep, pigs and cattle) at the confluence of the Tigris and Euphrates rivers. Later, in North Africa, water buffaloes, dromedary camels and asses were domesticated. Some livestock raising systems that existed in ancient times still exist today. These are subsistence systems in Arab tribal society, in which herds and flocks are moved seasonally over great distances in search of feed and water. Intensive farming systems are used in the more developed countries.
North America
Although agriculture is a major economic activity in Canada and the United States, the proportion of the population engaged in agriculture is less than 2.5%. Since the 1950s, agriculture has become more intensive, leading to fewer but larger farms. Livestock and livestock products make up a major proportion of the population’s diet, contributing 40% to the total food energy. The livestock industry in this region has been very dynamic. Introduced animals have been bred with indigenous animals to form new breeds. Consumer demand for leaner meats and eggs with less cholesterol is having an impact on breeding policy. Horses were used extensively at the turn of the nineteenth century, but they have declined in numbers because of mechanization. They are currently used in the race horse industry or for recreation. The United States has imported about 700 insect species to control more than 50 pests. Aquaculture in this region is growing, and accounted for 3.7% of the world’s aquaculture production in 1992 (FAO 1995; Scherf 1995).
Environmental and Public Health Issues
Occupational hazards of livestock rearing may lead to injuries, asthma or zoonotic infections. In addition, livestock rearing poses several environmental and public health issues. One issue is the effect of animal waste upon the environment. Other issues include the loss of biological diversity, risks associated with animal and product importation and food safety.
Water and air pollution
Animal wastes pose potential environmental consequences of water and air pollution. Based upon US annual discharge factors shown in table 3, major livestock breeds discharged a total of 14.3 billion tonnes of faeces and urine worldwide in 1994. Of this total, cattle (milk and beef) discharged 87%; pigs, 9%; and chickens and turkeys, 3% (Meadows 1995). Because of their high annual discharge factor of 9.76 tonnes of faeces and urine per animal, cattle contributed the most waste among these livestock types for all six United Nations Food and Agricultural Organization (FAO) regions of the world, ranging from 82% in both Europe and Asia to 96% in sub-Saharan Africa.
Table 3. Annual US livestock faeces and urine production
|
Livestock type |
Population |
Waste (tonnes) |
Tonnes per animal |
|
Cattle (milk and beef) |
46,500,000 |
450,000,000 |
9.76 |
|
Pig |
60,000,000 |
91,000,000 |
1.51 |
|
Chicken and turkey |
7,500,000,000 |
270,000,000 |
0.04 |
Source: Meadows 1995.
In the United States, farmers who specialize in livestock rearing do not engage in crop farming, as had been the historical practice. As a result, livestock waste is no longer systematically applied to crop land as a fertilizer. Another problem with modern livestock raising is the high concentration of animals into small areas such as confinement buildings or feedlots. Large operations may confine 50,000 to 100,000 cattle, 10,000 pigs or 400,000 chickens to an area. In addition, these operations tend to cluster near the processing plants to shorten the transportation distance of the animals to the plants.
Several environmental problems result from concentrated operations. These problems include lagoon spills, chronic seepage and runoff and airborne health effects. Nitrate peculation into the groundwater and runoff from fields and feedlots are major contributors to water contamination. A greater use of feedlots leads to concentration of animal manure and a greater risk for contamination of groundwater. Waste from cattle and pig operations is typically collected in lagoons, which are large, shallow pits dug into the ground. Lagoon design depends upon the settling of solids to the bottom, where they anaerobically digest, and the excess liquids are controlled by spraying them onto nearby fields before they overflow (Meadows 1995).
Biodegrading livestock waste also emits odorous gases that contain as many as 60 compounds. These compounds include ammonia and amines, sulphides, volatile fatty acids, alcohols, aldehydes, mercaptans, esters and carbonyls (Sweeten 1995). When humans sense odours from concentrated livestock operations, they can experience nausea, headaches, breathing problems, sleep interruption, appetite loss and irritation of the eyes, ears and throat.
Less understood are the adverse effects of livestock waste upon global warming and atmospheric deposition. Its contribution to global warming is through the generation of the greenhouse gases, carbon dioxide and methane. Livestock manure may contribute to nitrogen depositions because of ammonia release from waste lagoons into the atmosphere. Atmospheric nitrogen re-enters the hydrologic cycle through rain and flows into streams, rivers, lakes and coastal waters. Nitrogen in water contributes to increased algae blooms that reduce the oxygen available to fish.
Two modifications in livestock production offer solutions to some of the problems of pollution. These are less animal confinement and improved waste treatment systems.
Animal diversity
The potential for rapid loss of genes, species and habitats threatens the adaptability and traits of a variety of animals that are or could be useful. International efforts have stressed the need to preserve biological diversity at three levels: genetic, species and habitat. An example of declining genetic diversity is the limited number of sires used to breed artificially females of many livestock species (Scherf 1995).
With the decline of many livestock breeds, and thus the reduction of species diversity, dominant breeds have been increasing, with an emphasis on uniformity in higher production breeds. The problem of a lack of dairy cattle-breed diversity is particularly acute; with the exception of the high-producing Holstein, dairy populations are declining. Aquaculture has not reduced pressure on wild fish populations. For example, the use of fine nets for biomass fishing for shrimp food results in the collection of juveniles of valuable wild species, which adds to their depletion. Some species, such as groupers, milkfish and eels, cannot be bred in captivity, so their juveniles are caught in the wild and raised on fish farms, further reducing the stock of wild populations.
An example of a loss of habitat diversity is the impact of feed for fish farms on wild populations. Fish feed used in coastal areas affects wild populations of shrimp and fish by destroying their natural habitat such as mangroves. In addition, fish faeces and feed can accumulate on the bottom and kill the benthic communities that filter the water (Safina 1995).
Animal species that survive in abundance are those used as a means to human ends, but a social dilemma emerges from an animal rights movement that espouses that animals, especially warm-blooded animals, are not to be used as a means to human ends. Preceding the animal rights movement, an animal welfare movement started before the mid-1970s. Animal welfare proponents advocate the humane treatment of animals that are used for research, food, clothing, sport or companionship. Since the mid-1970s, the animal rights advocates assert that sentient animals have a right not to be used for research. It appears highly unlikely that the human use of animals will be abolished. It is also likely that animal welfare will continue as a popular movement (NIH 1988).
Animal and animal product importation
The history of livestock rearing is closely linked to the history of livestock importation into new areas of the world. Diseases spread with the spread of imported livestock and their products. Animals may carry disease that can infect other animals or humans, and countries have established quarantine services to control the spread of these zoonotic diseases. Among these diseases are scrapie, brucellosis, Q-fever and anthrax. Livestock and food inspection and quarantines have emerged as methods to control disease importation (MacDiarmid 1993).
Public concern about the potential infection of humans with the rare Creutzfeldt-Jakob disease (CJD) emerged among beef-importing nations in 1996. Eating beef infected with bovine spongiform encephalopathy (BSE), popularly known as mad cow disease, is suspected of leading to CJD infection. Although unproven, public perceptions include the proposition that the disease may have entered cattle from feed containing bone meal and offal from sheep afflicted with the similar disease, scrapie. All three diseases, in humans, cattle and sheep, exhibit common symptoms of sponge-like brain lesions. The diseases are fatal, their causes are unknown, and there are no tests to detect them. Britons launched a pre-emptive slaughter of one-third of their cattle population in 1996 to control BSE and restore consumer confidence in the safety of their beef exports (Aldhous 1996).
The importation of African bees into Brazil has also emerged into a public health issue. In the United States, subspecies of European bees produce honey and beeswax and pollinate crops. They rarely swarm aggressively, which aids safe beekeeping. The African subspecies has migrated from Brazil into Central America, Mexico and the Southeastern United States. This bee is aggressive and will swarm in defence of its colony. It has interbred with the European subspecies, which results in an Africanized bee that is more aggressive. The public health threat is multiple stings when the Africanized bee swarms and severe toxic reactions in humans.
Two controls currently exist for the Africanized bee. One is that they are not hardy in northern climates and may be restricted to warmer temperate climates like the Southern United States. The other control is routinely to replace the queen bee in hives with queen bees of the European subspecies, although this does not control wild colonies (Schumacher and Egen 1995).
Food safety
Many human food-borne illnesses result from pathogenic bacteria of animal origin. Examples include listeria and salmonellae found in dairy products and salmonellae and campylobacter found in meat and poultry. The Centers for Disease Control and Prevention estimates that 53% of all food-borne illness outbreaks in the United States were caused by bacterial contamination of animal products. They estimate that 33 million food-borne illnesses occur each year, from which 9,000 deaths result.
The subtherapeutic feeding of antibiotics and antibiotic treatment of diseased animals are current animal health practices. The potential diminished effectiveness of antibiotics for disease therapy is a rising concern because of the frequent development of antibiotic resistance of zoonotic pathogens. Many antibiotics added to animal feed are also used in human medicine, and antibiotic-resistant bacteria could develop and cause infections in animals and humans.
Drug residues in food that result from medication of livestock also present risks. Residues of antibiotics used in livestock or added to feed have been found in food-producing animals including dairy cows. Among these drugs are chloramphenicol and sulphamethazine. Alternatives to the prophylactic feeding use of antibiotics to maintain animal health include the modification of production systems. These modifications include reduced animal confinement, improved ventilation and improved waste treatment systems.
Diet has been associated with chronic diseases. Evidence of an association between fat consumption and heart disease has stimulated efforts to produce animal products with less fat content. These efforts include animal breeding, feeding intact rather than castrated males and genetic engineering. Hormones are also seen as a method for decreasing fat content in meat. Porcine growth hormones increase growth rate, feed efficiency and the ratio of muscle to fat. The growing popularity of low-fat, low-cholesterol species such as ostriches is another solution (NRC 1989).
Environmental and Public Health Issues
Use and Disposal of Wood Waste
By-products of the lumber industry which can cause environmental problems may include air emissions, liquid effluent and solid wastes. Most of these problems arise from waste wood, which may include wood chips or sawdust from milling operations, bark from debarking operations and log debris in waterways where logs are stored.
Sawdust and other process dust presents a fire and explosion hazard in mills. To minimize this hazard, dust may be removed by manual means or, preferably, gathered by local exhaust ventilation systems and collected in bag houses or cyclones. Larger wood waste is chipped. Most of the sawdust and chips produced in the lumber industry can be used in other wood products (e.g., particleboard, pulp and paper). Efficient use of this type of wood waste is becoming more common as the expense of waste disposal rises, and as forest companies become more vertically integrated. Some types of wood waste, especially fine dust and bark, are not as easily used in other wood products, so other means of disposal must be sought.
Bark can represent a high proportion of tree volume, especially in regions where the logs harvested are of small diameter. Bark and fine sawdust, and, in some operations, all wood waste including chips, may be burned (see figure 1). Older style operations have used inefficient burning techniques (e.g., beehive burners, teepee burners) which produce a range of incomplete organic combustion products. Particulate air pollution, which can produce “fog”, is a common complaint in the vicinity of these burners. In sawmills where chlorophenols are used, there is also concern about dioxin and furan production in these burners. Some modern sawmills use enclosed temperature-controlled power boilers to produce steam for kilns or power for the mill or other electricity users. Others sell their wood waste to pulp and paper mills, where it is burned to meet their high power requirements (see the chapter Paper and pulp industry). Boilers and other burners usually must meet particulate emission control standards using systems such as electrostatic precipitators and wet scrubbers. To minimize burning of wood waste, other uses can be found for bark and fine sawdust, including as compost or mulch in landscaping, agriculture, surface mine revegetation and forest renewal, or as extenders in commercial products. In addition, use of thin-kerf saws in the mill can result in dramatic reductions in sawdust production.
Figure 1. Conveyor belts transport waste to a beehive burner

Leanne Van Zwieten
Bark, logs and other wood debris may sink in water-based log storage areas, blanketing the bottom and killing benthic organisms. To minimize this problem, logs in booms can be bundled together and the bundles broken apart on land, where the debris can be easily collected. Even with this modification, sunken debris needs to be dredged from time to time. Recovered logs are available for lumber, but other waste requires disposal. Land-based disposal and deep-water dumping have both been used in the industry. Hydraulic debarking effluent can cause similar problems - thus the trend to mechanical systems.
Chip piles can create storm-water run-off problems since the leachate from wood includes resin and fatty acids and phenolics which are acutely toxic to fish. Landfill disposal of wood waste also produces leachate, requiring mitigation measures to protect ground and surface waters.
Antisapstain and Wood Preservation Fungicides
Wood treatment with fungicides to prevent the growth of sapstain organisms has led to contamination of nearby waterways (sometimes with large fish kills), as well as contamination of the soil on site. Treatment systems which involve driving bundled lumber through large, uncovered dip tanks and drainage in the sawmill yard allow rainfall overflows and widespread travel of runoff. Covered dip tanks with automated dipping elevators, spray booths in the production line, and containment berms around both the treatment system and the lumber drying area greatly reduce the potential for and impact of spills. However, although antisapstain spray booths minimize environmental exposure potential, they may entail more downstream worker exposure than dip tanks that treat finished bundled lumber.
Environmental impacts appear to have been reduced by the new generation of fungicides that have replaced chlorophenols. Although toxicity to aquatic organisms may be the same, certain substitute fungicides bind more strongly to wood, making them less bioavailable, and they are more easily degraded in the environment. In addition, the greater expense of many of the substitutes and the cost of disposal has encouraged recycling of liquid waste and other waste minimization procedures.
Thermal and pressure treatment of wood for long-term resistance to fungi and insects has traditionally been done in more enclosed facilities than antisapstain treatment, and therefore tends not to produce the same liquid waste problems. Disposal of solid wastes including sludge from treatment and storage tanks presents similar problems for both processes. Options may include contained storage in leak-proof containers in a bermed impermeable area, burial in a secure, hydrogeologically isolated hazardous-waste landfill or incineration at high temperatures (e.g., 1,000°C) with specified residence times (e.g., 2 seconds).
Special Issues in Plywood and Particleboard Operations
Veneer dryers in plywood mills can produce a characteristic blue haze made up of volatile wood extractives such as terpenes and resin acids. This tends to be more of a problem inside plants, but can also be present in the dryer water-vapour plumes. Particleboard and plywood mills often burn wood waste to produce heat for the presses. Vapour and particulate control methods, respectively, can be used for these airborne emissions.
Wash water and other liquid effluents from plywood and particleboard mills can contain the formaldehyde resins used as glues; however, it is now common practice for waste water to be recycled for making up the glue mixtures.
Disease and Injury Patterns
Injuries
Sawmills and other lumber mills are extremely hazardous work environments due to the nature of the process, which involves the movement and cutting of large, very heavy pieces of wood at relatively high speeds. Even when good engineering controls are in place, strict adherence to safety rules and procedures is necessary. There are a number of general factors which may contribute to the risk of injury. Poor housekeeping can increase the risk of slips, trips and falls, and wood dust may pose a fire or explosion hazard. The high noise levels have been a cause of injuries due to the reduced ability of workers to communicate and hear audible warning signals. Many large mills operate on multiple shifts, and the hours of work, particularly changes in shift, can increase the probability of accidents.
Some common causes of fatal or very serious injuries are being struck by mobile equipment; falls from elevated walkways and platforms; failure to de-energize or lockout equipment during maintenance or attempts to remove jams; kick-backs from saws, edgers and planers; and drowning in log ponds or waterways. Newly hired workers are at increased risk. For example, in an analysis of the causes of 37 sawmill fatalities between 1985 and 1994 in British Columbia, Canada, 13 (35%) of the fatalities occurred within the first year of employment, and 5 of these occurred within the first week of employment (4 on the first day) (Howard 1995).
There is also a high risk of injuries which are not life threatening. Eye injuries may result from particles and small pieces of wood or debris ejected from machinery. Splinters, cuts and puncture wounds can result from contact between lumber and unprotected skin. Strains, sprains and other musculoskeletal injuries can result from attempts to push, pull or lift heavy materials during sorting, grading and other operations.
Non-Malignant Diseases
Workers in sawmills and related industries are exposed to a variety of respiratory hazards, including wood dust, the volatile components of wood, airborne moulds and bacteria, and formaldehyde. A number of studies have examined respiratory health among sawmill, plywood, particleboard and strandboard workers. The focus of the sawmill studies has generally been on wood dust, while the focus of the plywood and particleboard studies has primarily been on formaldehyde exposure.
Occupational exposure to wood dust has been associated with a broad range of upper- and lower-respiratory effects. Because of the particle sizes generated by operations in the lumber industries, the nose is a natural site for the effects of wood dust exposure. A wide variety of sino-nasal effects have been reported, including rhinitis, sinusitis, nasal obstruction, nasal hypersecretion and impaired mucociliary clearance. Lower-respiratory effects, including asthma, chronic bronchitis and chronic airflow obstruction, have also been associated with exposure to wood dust. Both upper- and lower-respiratory effects have been associated with both softwood and hardwood tree species from both temperate and tropical climates. For example, occupational asthma has been found to be associated with exposure to dust from African maple, African zebra, ash, California redwood, cedar of Lebanon, Central American walnut, Eastern white cedar, ebony, iroko, mahogany, oak, ramin and Western red cedar as well as other tree species.
Wood is primarily composed of cellulose, polyoses and lignin, but also contains a variety of biologically active organic compounds such as monoterpenes, tropolones, resin acids (diterpenes), fatty acids, phenols, tannins, flavinoids, quinones, lignanes and stilbenes. Because health effects have been found to vary by species of tree, it is suspected they may be due to these naturally occurring chemicals, referred to as extractives, which also vary by species. In some cases specific extractives have been identified as the cause of the health effects associated with exposure to wood. For example, plicatic acid, which occurs naturally in Western red cedar and Eastern white cedar, is responsible for asthma and other allergenic effects in humans. While higher-molecular-weight extractives remain with the dust during woodworking operations, other, lighter-weight extractives, such as the monoterpenes, are easily volatilized during kiln drying, sawing and trimming operations. The monoterpenes (such as α-pinene, β-pinene, d3-carene and limonene) are major components of the resin from many common softwoods and are associated with mouth and throat irritation, shortness of breath, and impaired lung function.
The moulds which grow on timber are another natural, wood-related exposure with potentially harmful effects. Exposure to moulds among sawmill workers appears to be common in regions where the climate is sufficiently damp and warm for moulds to grow. Cases of extrinsic allergic alveolitis, also referred to as hypersensitivity pneumonitis, have been observed among sawmill workers in Scandinavia, Great Britain and North America (Halpin et al. 1994). A much more common, although less serious, effect of exposure to moulds is inhalation fever, also referred to as organic dust toxic syndrome, consisting of acute attacks of fever, malaise, muscular pain and cough. The prevalence of inhalation fever among Swedish wood trimmers has been estimated to be between 5 and 20% in the past, although rates are likely to be much lower now due to the introduction of preventive measures.
Respiratory effects are also possible from exposure to chemicals used as adhesives in the lumber industry. Formaldehyde is an irritant and can cause inflammation of the nose and throat. Acute effects on lung function have been observed and chronic effects are suspected. Exposure has also been reported to cause asthma and chronic bronchitis.
The irritant or allergenic effects of wood dust, formaldehyde and other exposures are not limited to the respiratory system. For example, studies reporting nasal symptoms have often reported an increased prevalence of eye irritation. Dermatitis has been found to be associated with dust from over 100 different species of trees including some common hardwoods, softwoods and tropical species. Formaldehyde is also a skin irritant and can cause allergic contact dermatitis. In addition, a number of the anti-sapstain fungicides used on softwoods have also been found to cause eye and skin irritation.
Workers in sawmills and other lumber industries have a high risk for noise-related hearing loss. For example, in a recent survey in a United States sawmill, 72.5% of workers exhibited some degree of hearing impairment at one or more audiometric test frequencies (Tharr 1991). Workers in the vicinity of saws and other wood processing machinery are typically exposed to levels above 90 or 95 dBA. Despite this well recognized hazard, attempts to reduce noise levels are relatively rare (with the exception of planer mill enclosures), and new cases of noise-induced hearing loss continue to occur.
Cancer
Work in the lumber industries may entail exposure to both known and suspected carcinogens. Wood dust, the most common exposure in the lumber industries, has been classified as a human carcinogen (International Agency for Research on Cancer (IARC) - Group 1). Very high relative risks of sino-nasal cancer, particularly sino-nasal adenocarcinoma, have been observed among workers exposed to high levels of dust from hardwoods, such as beech, oak and mahogany, in the furniture industry. The evidence for softwood dust is less conclusive, and smaller excess risks have been observed. There is evidence of an excess risk among workers in sawmills and related industries based on a pooled re-analysis of the raw data from 12 sino-nasal cancer case-control studies (IARC 1995). Sino-nasal cancer is a relatively rare cancer in almost all regions of the world, with a crude annual incidence rate of approximately 1 per 100,000 population. Ten per cent of all sino-nasal cancers are thought to be adenocarcinomas. Although associations between wood dust and other, more common, cancers have been observed in some studies, the results have been much less consistent than for sino-nasal cancer.
Formaldehyde, a common exposure among workers in the plywood, particleboard and related industries, has been classified as a probable human carcinogen (IARC - Group 2A). Formaldehyde has been found to cause cancer in animals, and excesses of both nasopharyngeal and sino-nasal cancer have been observed in some studies of humans, but the results have been inconsistent. Pentachlorophenol and tetrachlorophenol pesticides, until recently commonly used in the wood industries, are known to be contaminated with furans and dioxins. Pentachlorophenol and 2,3,7,8-tetrachlorodibenzo-para-dioxin have been classified as possible human carcinogens (IARC - Group 2B). Some studies have found an association between chlorophenols and the risk of non-Hodgkin lymphoma and soft-tissue sarcoma. The results for non-Hodgkin lymphoma have been more consistent than for soft-tissue sarcoma. Other potential carcinogenic exposures which may affect some workers in the lumber industries include asbestos (IARC - Group 1), which is used for insulation of steam pipes and kilns, diesel exhaust (IARC - Group 2A) from mobile equipment, and creosote (IARC - Group 2A), which is used as a wood preservative for railroad ties and telephone poles.
Relatively few studies of cancer among workers specifically employed in sawmills, plywood mills or related board manufacturing industries have been performed. The largest was a cohort study of over 26,000 Canadian sawmill workers conducted by Hertzman and colleagues (1997) in order to examine the risk of cancer associated with exposure to chlorophenol pesticides. A twofold excess of sino-nasal cancer and a smaller excess of non-Hodgkin lymphoma were observed. The excess of non-Hodgkin lymphoma appeared to be associated with exposure to chlorophenates. The remaining studies have been much smaller. Jäppinen, Pukkala and Tola (1989) studied 1,223 Finnish sawmill workers and observed excesses of skin, mouth and pharyngeal cancers, and lymphomas and leukaemias.
Blair, Stewart and Hoover (1990) and Robinson and colleagues (1986) conducted studies of 2,309 and 2,283 US plywood mill workers, respectively. In an analysis of pooled data from the two plywood cohorts, excesses were observed for nasopharyngeal cancer, multiple myeloma, Hodgkin’s disease and non-Hodgkin’s lymphoma. It is unclear from the results of these studies which, if any, occupational exposures may have been responsible for the excesses observed. The smaller studies have lacked the power to examine the risk of rare cancers, and many of the excesses were based on very small numbers. For example, no sino-nasal cancers were observed, but only 0.3 were expected in the smaller sawmill study, and 0.3 and 0.1 were expected in the plywood mill studies.
Major Sectors and Processes: Occupational Hazards and Controls
Sawmill Process
Sawmills can vary greatly in size. The smallest are either stationary or portable units consisting of a circular saw headrig, a simple log carriage and a two-saw edger (see descriptions below) powered by a diesel or gasoline engine and operated by as few as one or two workers. The largest mills are permanent structures, have much more elaborate and specialized equipment, and can employ over 1,000 workers. Depending on the size of the mill and the climate of the region, operations may be performed outdoors or indoors. While the type and size of logs determine to a large degree what types of equipment are needed, the equipment in sawmills can also vary considerably based on the age and size of the mill as well as the type and quality of boards produced. Below is a description of some of the processes conducted in a typical sawmill.
After transport to a sawmill, logs are stored on land, in water bodies adjacent to the mill or in ponds constructed for storage purposes (see figure 1 and figure 2). The logs are sorted according to quality, species or other characteristics. Fungicides and insecticides may be used in land-based log storage areas if the logs will be stored for a long time until further processing. A cut-off saw is used to even up the ends of the logs either before or after debarking and prior to further processing in the sawmill. The removal of bark from a log may be accomplished by a number of methods. Mechanical methods include peripheral milling by rotating logs against knives; ring debarking, in which tool points are pressed against the log; wood-to-wood abrasion, which pounds the logs against themselves in a rotating drum; and using chains to tear away the bark. Bark may also be removed hydraulically by using high-pressure water jets. After debarking and between all operations within the sawmill, logs and boards are moved from one operation to the next using a system of conveyors, belts and rollers. In large sawmills these systems can become quite complex (see figure 3).
Figure 1. Chip loading with water storage of logs in background

Source: Canadian Forest Products Ltd.
Figure 2. Longs entering a sawmill; storage and kilns in background

Source: Canadian Forest Products Ltd.
Figure 3. Mill interior; conveyor belts and rollers transport wood
British Columbia Ministry of Forests
The first phase of sawmilling, sometimes referred to as primary breakdown, is performed at a headrig. The headrig is a large, stationary circular saw or band-saw used to cut the log longitudinally. The log is transported back and forth through the headrig using a travelling carriage which can rotate the log for the optimum cut. Multiple band-saw headrigs may also be used, especially for smaller logs. The products of the headrig are a cant (the square centre of the log), a series of slabs (the rounded outer edges of the log) and, in some cases, large boards. Lasers and x rays are becoming common in sawmills for use as viewing and cutting guides in order to optimize wood use and the size and types of boards produced.
In secondary breakdown, the cant and large boards or slabs are further processed into functional lumber sizes. Multiple parallel saw blades are usually used for these operations - for example, quad saws with four linked circular saws, or gang saws which may be of the sash or circular saw type. Boards are cut to the proper width using edgers, consisting of at least two parallel saws, and to the proper length using trim saws. Edging and trimming are usually performed using circular saws, though edgers sometimes are band-saws. Manual chain-saws are usually available in sawmills for freeing lumber caught in the system because it is bent or flared. In modern sawmills, each operation (i.e., headrig, edger) will generally have a single operator, often stationed within an enclosed booth. In addition, workers may be stationed between operations in later stages of secondary breakdown in order to manually ensure that the boards are properly positioned for subsequent operations.
After processing in the sawmill, the boards are graded, sorted according to dimensions and quality, then stacked by hand or machine (see figure 4). When lumber is manually handled, this area is referred to as a “green chain”. Automated sorting bins have been installed in many modern mills to replace labour-intensive manual sorting. In order to increase airflow to assist in drying, small pieces of wood may be placed between the boards as they are being stacked.
Figure 4. Fork-lift with load

Canadian Forest Productions Ltd.
Construction grades of lumber may be seasoned in the open air outdoors or dried in kilns, depending on local weather conditions and the wetness of the green lumber; but finishing grades are more commonly kiln dried. There are many kinds of kilns. Compartment kilns and high-temperature kilns are serial kilns. In continuous kilns, stacked bundles can move through the kiln in a perpendicular or parallel position, and the direction of air movement can be perpendicular or parallel to the boards. Asbestos has been used as an insulating material for steam pipes in kilns.
Prior to storage of green lumber, especially in wet or humid locales, fungicides may be applied to prevent growth of fungi which stain wood blue or black (sapstain). Fungicides may be applied in the production line (usually by spraying) or after bundling lumber (usually in dip tanks). The sodium salt of pentachlorophenol was introduced in the 1940s for the control of sapstain, and was replaced in the 1960s by the more water soluble tetrachlorophenate. Chlorophenate use has largely been discontinued because of concern regarding health effects and contamination with polychlorinated dibenzo-p-dioxins. Substitutes include didecyldimethyl ammonium chloride, 3-iodo-2-propynyl butyl carbamate, azaconazole, borax and 2-(thiocyanomethylthio)benzthiazole, most of which have been little studied among user workforces. Often lumber, especially that which has been kiln dried, does not need to be treated. In addition, wood of some tree species, such as Western red cedar, is not susceptible to sapstain fungi.
Either before or after drying, the wood is marketable as green or rough lumber; however, the lumber must be further processed for most industrial uses. Lumber is cut to final size and surfaced in a planing mill. Planers are used to reduce the wood to standard marketable sizes and to smooth the surface. The planer head is a series of cutting blades mounted on a cylinder which revolves at high speed. The operation is generally power fed and performed parallel to the wood grain. Often planing is performed simultaneously on two sides of the board. Planers which operate on four sides are called matchers. Moulders are sometimes used to round the edges of the wood.
After final processing, the wood must be sorted, stacked and bundled in preparation for shipping. Increasingly, these operations are being automated. In some specialized mills, wood may be further treated with chemical agents used as wood preservatives or fire retardants, or for protection of the surface from mechanical wear or weathering. For example, railroad ties, pilings, fence posts, telephone poles or other wood expected to be in contact with soil or water may be pressure treated with chromated or ammoniacal copper arsenate, pentachlorophenol or creosote in petroleum oil. Stains and colourants may also be used for marketability, and paints may be used to seal the ends of boards or to add company marks.
Large amounts of dust and debris are generated by saws and other wood-processing operations in sawmills. In many sawmills the slabs and other large pieces of wood are chipped. Chippers are generally large rotating discs with straight blades imbedded in the face, and slots for the chips to pass through. The chips are produced when logs or mill wastes are introduced to the blades using inclined gravity feed, horizontal self-feed or controlled power feeding. Generally the cutting action of the chipper is perpendicular to the blades. Different designs are used for whole logs than for slabs, edgings and other pieces of waste wood. It is common for a chipper to be integrated into the headrig to chip unusable slabs. Separate chippers to handle waste from the rest of the mill are also used. Wood chips and sawdust may be sold for pulp, reconstituted board manufacturing, landscaping, fuel or other uses. Bark, wood chips, sawdust and other material may also be burned either as fuel or as waste.
Large, modern sawmills will typically have a sizeable maintenance staff which includes clean-up workers, millwrights (industrial mechanics), carpenters, electricians and other skilled workers. Waste material may collect on machinery, conveyors and floors if sawmill operations are not equipped with local exhaust ventilation or the equipment is not operating properly. Clean-up operations are often performed using compressed air to remove wood dust and dirt from machinery, floors and other surfaces. Saws must be regularly inspected for broken teeth, cracks or other defects, and must be properly balanced to prevent vibration. This is done by a trade that is unique to the wood industries - saw filers, who are responsible for the re-toothing, sharpening and other maintenance of circular saws and band-saws.
Sawmill Health and Safety Hazards
Table 1 indicates the major types of occupational health and safety hazards found in the major process areas of a typical sawmill. There are many serious safety hazards within sawmills. Machine guarding is necessary at the point of operation for saws and other cutting devices as well as for gears, belts, chains, sprockets and nip points on conveyors, belts and rollers. Anti-kickback devices are necessary on many operations, such as circular saws, to prevent jammed lumber from being ejected from machines. Guard rails are necessary on walkways adjacent to operations or crossing over conveyors and other production lines. Proper housekeeping is necessary to prevent dangerous accumulation of wood dust and debris, which could result in falls as well as presenting a fire and explosion hazard. Many areas which require clean-up and routine maintenance are located in hazardous areas which would normally be inaccessible during times when the sawmill is in operation. Proper adherence to machinery lock-out procedures is extremely important during maintenance, repair and clean-up operations. Mobile equipment should be equipped with audible warning signals and lights. Traffic lanes and pedestrian walkways should be clearly marked. Reflective vests are also necessary to increase the visibility of pedestrians.
Table 1. Occupational health and safety hazards by lumber industry process area
|
Process area |
Safety hazards |
Physical hazards |
Dust/chemical hazards |
Biological hazards |
|
Yard and pond |
Mobile equipment;* unsecure logs/lumber;* conveyor belts |
Noise; temperate |
Road dust, other |
Mould and bacteria* |
|
Debarking |
Elevated walk-ways; machine kick-back; unsecure logs/lumber;* |
Noise |
Wood dust; road dust; |
Mould and bacteria* |
|
Sawing, trimming, |
Elevated walk-ways; machine kick-back;* unsecure logs/lumber; |
Noise;* repetitive strain |
Wood dust;* volatile |
Mould and bacteria |
|
Kiln drying |
Mobile equipment |
Temperature extremes |
Volatile wood |
Mould and bacteria |
|
Planing |
Elevated walk-ways; machine kick-back;* unsecure logs/lumber; |
Noise;* repetitive |
Wood dust;* volatile |
|
|
Sorting and grading |
Elevated walk-ways; unsecure logs/lumber; conveyor belts;* |
Noise; repetitive strain |
Wood dust; pesticides |
|
|
Chipping and related operations |
Elevated walk-ways; machine kick-back; conveyor belts; saws/ |
Noise* |
Wood dust;* volatile |
Mould and bacteria* |
|
Veneer cutting |
Elevated walk-ways; mobile equipment; conveyor belts; |
Noise* |
Wood dust; volatile wood |
Mould and bacteria* |
|
Veneer drying |
Mobile equipment; slivers |
Temperature extremes; |
Volatile wood components; |
Mould and bacteria |
|
Glue mixing and |
Repetitive strain injuries |
Formaldehyde;* other resin |
||
|
Hot press |
Mobile equipment; slivers; failure to lock-out machinery* |
Noise; repetitive strain |
Volatile wood components; |
|
|
Panel sanding |
Mobile equipment; saws/cutting equipment; flying debris; |
Noise;* repetitive strain |
Wood dust; formaldehyde; |
|
|
Clean-up operations |
Elevated walk-ways; conveyor belts;* flying debris;* slivers; |
Noise |
Wood dust;* formaldehyde; |
Mould and bacteria* |
|
Saw filing |
Elevated walk-ways; saws/cutting equipment; flying debris; |
Noise |
Metal fumes* |
|
|
Other maintenance |
Elevated walk-ways; mobile equipment;* failure to lock-out |
Wood dust; asbestos; |
||
|
Packing and shipping |
Elevated walk-ways; mobile equipment;* unsecure logs/lumber; |
Noise; temperature |
Road dust, other |
* Signifies high degree of hazard.
Sorting, grading and some other operations may involve the manual handling of boards and other heavy pieces of wood. Ergonomic design of the conveyors and receiving bins, and proper material-handling techniques should be used to help prevent back and upper extremity injuries. Gloves are necessary to prevent splinters, puncture wounds and contact with preservatives. Panels of safety glass or similar material should be placed between operators and points of operation because of the risk of eye and other injuries from wood dust, chips and other debris ejected from saws. Laser beams are also potential ocular hazards, and areas using Class II, III or IV lasers should be identified and warning signs posted. Safety glasses, hardhats and steel-toed boots are standard personal protective gear that should be worn during most sawmill operations.
Noise is a hazard in most areas of sawmills from debarking, sawing, edging, trimming, planing and chipping operations, as well as from logs striking each other on conveyors, rollers and drop-sorters. Feasible engineering controls to reduce noise levels include sound-proof booths for operators, enclosure of cutting machines with sound-absorbent material at the in- and out-feeds, and construction of sound barriers of acoustical materials. Other engineering controls are also possible. For example, idle running noise from circular saws may be reduced by purchasing saws with a suitable tooth shape or adjusting the speed of rotation. The installation of absorbing material on walls and ceilings may aid in reducing reflected noise throughout the mill, though source control would be necessary where noise exposure is direct.
Workers in almost all areas of the sawmill have the potential for exposure to particulate matter. Debarking operations involve little or no exposure to wood dust, since the goal is to leave the wood intact, but exposure to airborne soil, bark and biological agents, such as bacteria and fungi, is possible. Workers in almost all sawing, chipping and planing areas have the potential for exposure to wood dust. The heat generated by these operations may cause exposure to the volatile elements of the wood, such as monoterpenes, aldehydes, ketones and others, which will vary by tree species and temperature. Some of the highest wood dust exposures may occur among workers using compressed air for clean-up. Workers near kiln drying operations are likely to be exposed to wood volatiles. In addition, there is a potential for exposure to pathogenic fungi and bacteria, which grow at temperatures below 70°C. Exposure to bacteria and fungi is also possible during the handling of wood chips and waste, and the transport of logs in the yard.
Feasible engineering controls, such as local exhaust ventilation, exist to control the levels of airborne contaminants, and it may be possible to combine noise- and dust-control measures. For example, enclosed booths may reduce both noise and dust exposures (as well as preventing eye and other injuries). However, booths provide protection only to the operator, and controlling exposures at the source through enclosure of operations is preferable. Enclosure of planing operations has become increasingly common and has had the effect of reducing exposure to both noise and dust among persons who do not have to enter the enclosed areas. Vacuum and wet clean-up methods have been used in some mills, usually by clean-up contractors, but are not in general use. Exposure to fungi and bacteria may be controlled by reducing or increasing kiln temperatures and taking other steps to eliminate the conditions which promote the growth of these micro-organisms.
Other potentially hazardous exposures exist within sawmills. Exposure to cold and hot temperature extremes is possible near points where materials enter or leave the building, and heat is also a potential hazard in kiln areas. High humidity may be a problem when sawing wet logs. Exposure to fungicides is primarily via the dermal route and may occur if the boards are handled while still wet during grading, sorting and other operations. Appropriate gloves and aprons are necessary when handling boards that are wet with fungicides. Local exhaust ventilation with spray curtains and mist eliminators should be used in spraying operations. Exposure to carbon monoxide and other combustion products is possible from mobile equipment used to move logs and lumber within storage areas and to load semi-trailers or railroad cars. Saw filers may be exposed to hazardous levels of metal fumes including cobalt, chromium and lead from grinding, welding and soldering operations. Local exhaust ventilation as well as machine guarding are necessary.
Veneer and Plywood Mill Processes
The term plywood is used for panels consisting of three or more veneers which have been glued together. The term is also used to refer to panels with a core of solid wood strips or particleboard with top and bottom veneer surfaces. Plywood can be made from a variety of trees, including both conifers and non-conifers.
Veneers are usually created directly from debarked whole logs using rotary peeling. A rotary peeler is a lathe-like machine used to cut veneers, thin sheets of wood, from whole logs using a shearing action. The log is rotated against a pressure bar as it hits a cutting knife to produce a thin sheet between 0.25 and 5 mm in thickness. The logs used in this process may be soaked in hot water or steamed to soften them prior to peeling. The edges of the sheet are usually trimmed by knives attached to the pressure bar. Decorative veneers may be created by slicing a cant (the square centre of the log) using a pressure arm and blade in a manner similar to peeling. After either peeling or slicing, the veneers are collected on long, flat trays or rolled onto reels. The veneer is clipped into functional lengths using a guillotine-like machine, and dried using artificial heating or natural ventilation. The dried panels are inspected and, if necessary, patched using small pieces or strips of wood and formaldehyde-based resins. If the dried veneers are smaller than a standard-size panel, they may be spliced together. This is done by applying a liquid formaldehyde-based adhesive to the edges, pressing the edges together, and applying heat to cure the resin.
To produce the panels, veneers are roller- or spray-coated with formaldehyde-based resins, then placed between two unglued veneers with their grains in the perpendicular direction. The veneers are transferred to a hot press, where they are subjected to both pressure and heat to cure the resin. Phenol-resin adhesives are widely used to produce softwood plywood for severe service conditions, such as for construction and boat building. Urea-resin adhesives are used extensively in producing hardwood plywood for furniture and interior panelling; these can be fortified with melamine resin to increase their strength. The plywood industry has used formaldehyde-based glues in assembling of plywood for over 30 years. Prior to the introduction of formaldehyde-based resins in the 1940s, soybean and blood-albumen adhesives were used, and cold pressing of panels was common. These methods may still be used, but are increasingly rare.
The panels are cut to the proper dimensions using circular saws and are surfaced using large drum or belt sanders. Additional machining may also be performed in order to give the plywood special characteristics. In some cases, pesticides such as chlorophenols, lindane, aldrin, heptachlor, chloronaphthalenes and tributyltin oxide may be added to glues or used to treat the surface of panels. Other surface treatments may include the application of light petroleum oils (for concrete-form panels), paints, stains, lacquers and varnishes. These surface treatments may be performed at separate locations. Veneers and panels are often transported between operations using mobile equipment.
Veneer and Plywood Mill Hazards
Table 1 indicates the major types of occupational health and safety hazards found in the major process areas of a typical plywood mill. Many of the safety hazards in plywood mills are similar to those in sawmills, and the control measures are also similar. This section deals with only those issues which differ from sawmill operations.
Both dermal and respiratory exposure to formaldehyde and other components of glues, resins and adhesives is possible among workers in glue preparation, splicing, patching, sanding and hot pressing operations, and among workers nearby. Urea-based resins more readily release formaldehyde during curing than phenol-based ones; however, improvements in resin formulation have reduced exposures. Proper local exhaust ventilation and the use of appropriate gloves and other protective equipment are necessary to reduce respiratory and dermal exposure to formaldehyde and other resin components.
The wood used to produce veneers is wet, and the peeling and clipping operations do not generally produce much dust. The highest wood dust exposures during the production of plywood occur during the sanding, machining and sawing necessary to finish the plywood. Sanding, in particular, can produce large amounts of fine dust because as much as 10 to 15% of the board may be removed during surfacing. These processes should be enclosed and have local exhaust ventilation; hand sanders should have integral exhaust to a vacuum bag. If local exhaust is not present or it is not functioning properly, significant exposure to wood dust may occur. Vacuum and wet clean-up methods are more commonly found in plywood mills because the fine size of the dust makes other methods less effective. Unless noise control measures are in place, noise levels from sanding, sawing and machining operations are likely to exceed 90 dBA.
When veneers are dried, a number of chemical constituents of the wood may be released, including monoterpenes, resin acids, aldehydes and ketones. The types and amounts of chemical released depend on the species of tree and veneer dryer temperature. Proper exhaust ventilation and the prompt repair of veneer dryer leaks are necessary. Exposure to engine exhaust from fork-lifts may occur throughout plywood mills, and mobile equipment also presents a safety hazard. Pesticides mixed in glues are only slightly volatile and should not be detectable in workroom air, with the exception of chloronaphthalenes, which evaporate substantially. Exposure to pesticides may occur through the skin.
Other Manufactured Board Industries
This group of industries, including the manufacture of particleboard, waferboard, strandboard, insulation board, fibreboard and hardboard, produces boards consisting of wood elements of varying sizes, ranging from large flakes or wafers to fibres, held together by resinous glues or, in the case of wet process fibreboard, “natural” bonding between fibres. In the simplest sense, boards are created using a two-step process. The first step is the generation of the elements either directly from whole logs or as a waste by-product of other wood industries, such as sawmills. The second step is their recombination into sheet or panel form using chemical adhesives.
Particleboard, flakeboard, strandboard and waferboard are made from chips of wood of varying sizes and shapes using similar processes. Particleboard and flakeboard are made from small wood elements and are often used to make wood-veneered or plastic-laminated panels for the manufacture of furniture, cabinets and other wood products. Most elements may be made directly from wood waste. Waferboard and strandboard are made from very large particles - wood shavings and strands, respectively - and are primarily used for structural applications. The elements are generally made directly from logs using a machine containing a series of rotating knives which peel thin wafers. The design can be similar to a chipper, except the wood must be fed to the flaker with the grain oriented parallel to the knives. Peripheral milling designs can also be used. Water-saturated wood works best for these processes and, because the wood must be oriented, short logs are often used.
Before making sheets or panels, the elements must be sorted by size and grade, and then dried using artificial means, to a closely controlled moisture content. The dried elements are mixed with an adhesive and laid out in mats. Both phenol-formaldehyde and urea-formaldehyde resins are used. As is the case with plywood, phenolic resins are likely to be used for panels destined for applications requiring durability under adverse conditions, while the urea-formaldehyde resins are used for less demanding, interior applications. Melamine formaldehyde resins may also be used to increase durability, but rarely are because they are more expensive. In recent decades a new industry has emerged to produce reconstituted lumber for various structural uses as beams, supports and other weight-bearing elements. While the manufacturing processes used may be similar to particleboard, isocyanate-based resins are used because of the added strength needed.
The mats are divided into panel-sized sections, generally using an automated compressed air source or a straight blade. This operation is done in an enclosure so that the excess mat material can be recycled. The panels are formed into sheets by curing the thermosetting resin using a hot press in a manner similar to plywood. Afterwards the panels are cooled and trimmed to size. If necessary, sanders may be used to finish the surface. For example, reconstituted boards which are to be covered with a wood veneer or plastic laminate must be sanded to produce a relatively smooth, even surface. While drum sanders were used early in the industry, wide belt sanders are now generally used. Surface coatings may also be applied.
Fibreboards (including insulation board, medium-density fibreboard (MDF) and hardboard) are panels consisting of bonded wood fibres. Their production varies somewhat from particle- and other manufactured boards (see figure 5). To create the fibres, short logs or wood chips are reduced (pulped) in a manner similar to that used for producing pulp for the paper industry (see the chapter Paper and pulp industry). In general, a mechanical pulping process is used in which chips are soaked in hot water and then mechanically ground. Fibreboards can vary greatly in density, from low-density insulation boards to hardboards, and can be made from either conifers or non-conifers. Non-conifers generally make better hardboards, while conifers make better insulation boards. The processes involved in pulping have a minor chemical effect on the ground wood, removing a small amount of the lignin and extractive materials.
Figure 5. Classification of manufactured boards by particle size, density and process type

Two different processes, wet and dry, may be used to bond the fibres and create the panels. Hardboard (high density fibreboard) and MDF can be produced by “wet” or “dry” processes, while insulation board (low density fibreboard) can be produced only by the wet process. The wet process was developed first, and extends from paper production, while the dry process was developed later and stems from particleboard techniques. In the wet process, a slurry of pulp and water is distributed on a screen to form a mat. Afterwards, the mat is pressed, dried, cut and surfaced. The boards created by wet processes are held together by adhesive-like wood components and the formation of hydrogen bonds. The dry process is similar, except that the fibres are distributed on the mat after addition of a binder (either a thermosetting resin, thermoplastic resin or a drying oil) to form a bond between the fibres. Generally, either phenol-formaldehyde or urea-formaldehyde resins are used during the manufacture of dry-process fibreboard. A number of other chemicals may be used as additives, including inorganic salts as fire retardants and fungicides as preservatives.
In general, the health and safety hazards in the particleboard and related manufactured board industries are quite similar to those in the plywood industry, with the exception of pulping operations for fibreboard production (see table 1). Exposure to wood dust is possible during the processing to create the elements and may vary greatly depending on the moisture content of the wood and the nature of the processes. The highest wood dust exposures would be expected during the cutting and finishing of panels, especially during sanding operations if engineering controls are not in place or not functioning properly. Most sanders are enclosed systems, and large capacity air systems are needed to remove the dust generated. Exposure to wood dust, as well as fungi and bacteria, is also possible during the chipping and grinding of dried wood and among workers involved in the transport of chips from storage to processing areas. Very high noise exposures are possible near all sanding, chipping, grinding and related wood-processing operations. Exposure to formaldehyde and other resin constituents is possible during the mixing of glues, laying of the mat and the hot pressing operations. The control measures for limiting exposure to safety hazards, wood dust, noise and formaldehyde in the manufactured board industries are similar to those for the plywood and sawmill industries.
Environmental Protection and Public Health Issues
Visual Arts
The visual arts produce a wide range of potential environmental problems and raise a number of public health issues. The visual arts use a broad range of chemicals and techniques which can create air and water pollution problems similar to that of the comparable industrial processes, only on a much smaller scale.
Hazardous waste produced by artists can include: (1) toxic and extremely toxic wastes, including solvents, lead compounds, chromates and cyanide solutions; (2) flammable waste, including flammable and combustible liquids (e.g., rags soaked with oil and turpentine), oxidizing substances such as potassium chlorate and dichromates, and ignitable compressed gases; (3) corrosive waste, including acids with a pH less than 2 and alkalis with a pH greater than 12; and (4) reactive wastes, such as organic peroxides, cyanide solutions and sulphide solutions. Artists and artisans are less likely, however, to know how to dispose of this waste or even to know what is hazardous. The most common method of waste disposal for artists is pouring down the sink or onto the ground, tossing in the garbage or evaporation. Although the individual amounts of pollutants are small, cumulatively they can result in significant pollution.
In the United States and Canada and many other countries, artists working in their homes are usually exempted from industrial hazardous waste regulations under a household hazardous waste exemption. Many localities, however, do provide special household hazardous waste days when households can bring their hazardous waste to a central site for collection. However, even in countries which do regulate artists as small businesses, there is little enforcement of hazardous waste regulations for these cottage industries.
Types of waste management methods available include many of the same ones used by industry, including source reduction, waste separation and concentration, recycling, energy and material recovery, incineration or treatment, and secure land disposal. Some of these methods are more available to artists than others.
The best way of managing hazardous waste is to actually eliminate or minimize its production by substituting materials which are less toxic—for example, using lead-free glazes instead of leaded glazes in pottery and enamelling, and using water-based screen printing inks and other coating materials instead of solvent-based ones.
Separating hazardous materials from non-hazardous materials—for example, separating solvent-based paints and water-based paints—can be a simple method to reduce the amount of hazardous waste and prevent it from contaminating regular garbage.
Traditional industrial methods of concentration, such as evaporation of large volumes of photographic wastes, are usually not feasible for artists.
Recycling can involve the reusing of materials (such as solvents used for oil painting cleanup) by the individual, or the passing of unwanted materials to someone else who can use them. Large printmaking facilities, which generate many solvent- or oil-soaked rags, can contract for laundering and reuse them.
Treatment can involve several processes. The most common one used by artists is neutralization of acids or alkaline solutions. Incineration is usually restricted to burning wood dust. Evaporation of solvents is also commonly done. This reduces the amount of hazardous waste potentially contaminating water supplies, although it does contaminate the atmosphere to some degree.
The least favourable option is secure land disposal in a proper hazardous waste disposal site. This is usually not a viable option for artists, especially in developing countries.
A public health issue that is common to many of the visual arts is the problem of the exposure of children to toxic chemicals found in many art materials, including those intended for use by children. Examples include solvents in permanent felt-tip markers and lead in ceramic glazes. Children and other family members can be exposed to hazardous substances and conditions in the home.
A widespread problem in many countries is lead poisoning, including fatalities from cooking and storing food in containers that have been made with lead-containing pottery glazes. In the commercial industry, the problem of lead leaching from glazed pottery has been mostly eliminated through government regulations and good quality control. The World Health Organization has standards for lead and cadmium leaching from pottery intended for food and drink use. The cost of the testing required, however, is not feasible for craft potters, and therefore craft potters should use only lead-free glazes for food and drink containers.
Performing and Media Arts
Theatres, scenery shops and motion picture and television production areas also can produce hazardous waste, since they use many of the same chemicals as are used in the visual arts. The same solutions apply. In particular, the widespread shift from solvent-based paints to water-based paints has greatly decreased the amount of solvent pollution.
One of the main public health issues for theatres (and other places of public assembly) is fire safety. Many theatres and other performance spaces, especially small, non-commercial ones, do not meet applicable fire codes and are dangerously overcrowded. There have been many disastrous fires with numerous fatalities in the performing arts. The use of fogs and smokes for special effects in theatre and opera can also pose the risk of asthma attacks in asthmatic audience members in the front of the theatre if the building does not have adequate exhaust ventilation to prevent the fog or smoke from affecting the audience.
Entertainment Industry
Entertainment industries such as amusement and theme parks can face all the solid waste and other pollution problems of a small town. Zoos, circuses and other types of entertainment involving animals can have many of the same pollution problems as livestock raising, but on a smaller scale.
A public health concern at all entertainment events where food is sold is the possibility of developing salmonella poisoning, hepatitis or other diseases if there are not adequate public health controls.
Crowd control is another major public health concern in many large entertainment events, such as certain types of popular concerts and sports events. Widespread use of drugs and alcohol, overcrowding, allowing extensive standing room (festival seating) and lack of adequate preplanning have led to many incidents involving riots and panic, with resulting multiple injuries and fatalities. In addition, lack of adequate construction standards has caused fires and collapses of seating areas in several countries. There is a need for better regulations and provision of proper crowd control measures in these situations.
Visitors to parks and zoos can also present hazards to themselves. There have been many incidents where zoo visitors have been maimed or killed after entering animal enclosures. Visitors who get too close to wild animals in the parks have also experienced attacks, many of which have been fatal. The problems of inexperienced parks visitors getting lost, caught in storms, or falling from mountains is also a constant public health risk which can use up extensive resources for rescue.
The sex industry, especially prostitution, is particularly infamous for the possibility of patrons being robbed and possibly contracting sexually transmitted diseases. This is particularly true in countries where prostitution is not legally controlled. Criminal activities are often associated with prostitution.
Nightlife Entertainment
This grouping of extremely varied and miscellaneous entertainment occupations includes work locations such as bars, nightclubs, discotheques, dancehalls, topless bars, go-go clubs, casinos, bingo and gambling parlours, and pool halls, as well as cinema theatres. Occupations include bartenders, waiters, hostess/host, card dealers, bouncers (security personnel), musicians, dancers, strippers and movie projectionists. Hotels and restaurants often have night entertainment venues within them. There are several categories of hazards common to almost all nightlife entertainment workers.
Shiftwork. Entertainment workers such as bartenders may have routine nightshifts, while musicians working in a club may have irregular shifts. Various physiological, psychological and social effects are associated with nightshift or irregular shiftwork. Often bartenders and cocktail waitresses work shifts that are 10 to 14 hours long.
Violence. Workplace violence is a major problem in establishments that serve alcohol, as well as in gambling enterprises. The United States National Institute for Occupational Safety and Health studied homicide rates among workers in the United States during 1980–1989. They found bartenders to be ranked the eighth highest occupational group, with a homicide rate of 2.1 per 100,000, compared to the average homicide rate of 0.7 homicides per 100,000 for all workers. The exchange of money with the public, often working alone or in small numbers and working late at night or early in the morning, as well as working in high-crime areas, were all found to be factors related to the high rate. Preventive measures for lowering the violence rate include increasing the visibility of the workplace, such as by installing better lighting. The amounts of cash on hand should be minimized and signs posted which clearly indicate that little or no cash in on hand. Silent alarms and hidden cameras can be installed and workers can be trained in non-violent response techniques for emergencies, such as robberies. Arrangements can be made for having routine police checks on workers’ safety, and workers may even be provided bullet-proof barriers and vests if needed.
Fire Safety. Many smaller nightclubs, dancehalls, movie theatres and bars may not meet with local assembly, building or fire code requirements. There have been several high-profile fatal fires in urban clubs, which are often more crowded than permissible by law. Adherence to fire and assembly codes, a fire safety and emergency programme and availability of fire extinguishers and training in their use, as well as other emergency procedures, can reduce risks (Malhotra 1984).
Second-hand smoke. In many locations where there is nightlife entertainment, second-hand cigarette smoke is a significant hazard. The risk of lung cancer and heart disease is increased with exposure to cigarette smoke in the workplace (NIOSH 1991). The risk of laryngeal cancer, also associated with tobacco use, is elevated in bartenders and food servers. Often, smaller bars and night entertainment clubs do not have adequate ventilation for cigarette smoke. In many countries, efforts are being made to regulate exposure to second-hand smoke; but such governmental restriction are not universal. Ventilation and air cleaning devices, such as electrostatic precipitators, as well as the restriction of smoking will decrease exposure.
Alcohol and drug abuse. Working in certain occupations has been found to be correlated to increased alcohol consumption, and one suggestive study has found that death from liver cirrhosis, a disease associated with alcohol consumption, is elevated among waiters, bartenders and musicians (Olkinuora 1984). In nightlife entertainment work there is easy access to alcohol and a social pressure to drink. Often there is isolation from a usual homelife because of working during the night shift or because of touring through different locations. Poor management and lack of supervision can contribute to the problem. Performance anxiety (in the case of musicians), or the need to stay awake during night shift, as well as the fact that patrons may be apt to abuse drugs, can also increase the risks for drug abuse among workers in the nightlife environment. The risks for alcohol and drug abuse intervention programmes can be decreased by well-designed training programmes which assist workers dealing with these problems.
Noise. Excessive noise exposure can be a problem in bars and restaurants. While the problem of noise is obvious in discotheques and music clubs which feature excessively high sound levels, noise overexposure can also be a problem in bars and other locations in which there is only pre-recorded or jukebox music, which can also be played very loudly. Sound levels of over 100 decibels (dB) are common in discos (Tan, Tsang and Wong 1990). One survey of 55 nightclubs in New Jersey in the United States revealed noise levels from 90 to 107 dB. Placement of speakers and jukeboxes away from work stations can reduce worker exposure, and acoustic baffling and barriers can also help. In some cases a general reduction in volume may be possible. If possible, wearing ear plugs can reduce worker exposure.
Dermatitis. Nightlife workers share many skin problems with food handlers. Skin infections, such as candidiasis of the hands, can arise from extensive contact with soiled glassware, washing and cleaning fluids and water. Automatic dish- and glass-washing equipment can address this problem. Food sensitivities are also known, such as contact dermatitis in a bartender with a sensitivity to lemon and lime peels (Cardullo, Ruszkowski and Deleo 1989). Bartenders have developed eczema from handling mint. Other specific sensitivities leading to dermatitis have been reported, such as dermatitis in a professional blackjack dealer who developed a sensitivity to chromate salts used in the green dye for the felt on gaming tables (Fisher 1976).
Musculoskeletal problems. Repetitive motion injuries and other problems associated with workplace design can be found among nightlife workers. For example, musicians and dancers are prone to specific musculoskeletal problems, as discussed elsewhere in this chapter. Bartenders who continually wash glassware and card dealers who must shuffle and deal cards for games in casinos have been found to suffer from carpal tunnel syndrome. More frequent breaks during shifts, in addition to job and task redesign, may reduce these hazards. Bartenders, cocktail waitresses, casino dealers and food servers often must stand for their entire workshift, which may be 10 to 12 hours long. Excessive standing can result in back strain and other circulatory and musculoskeletal problems. Corrugated rubber floor mats and comfortable, supportive shoes can lessen the strain.
Film projection booths. Projection booths are small and problems of excessive heat can arise. Older film projection booths use a carbon arc light source to project images, while more modern booths employ xenon lamps. In either case, ultraviolet (UV) radiation and ozone gas exposure can occur. Levels of ozone that ranged from 0.01 to 0.7 parts per million have been reported. The ozone is generated by the UV radiation, which ionizes oxygen found in the air. (Maloy 1978). In addition, use of carbon arc light sources is associated with rare earth metal fumes, carbon dioxide, carbon monoxide, ozone, electromagnetic radiation (EMF) and heat exposures. Local exhaust ventilation is required.
Special effects. Many different special effects can be used in clubs and discotheques, including, various smokes and fogs, laser light shows and even pyrotechnics. Adequate training in laser operation and safety and other special effects is necessary. UV light emitted from “black” lights may pose additional hazards, especially to strippers and go-go dancers (Schall et al. 1969). It has been suggested that a glass barrier between the black light and the performers would help decrease the hazards. These effects are described in more detail in other articles in this chapter.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."