- You are here:
-
Home

-
Part XVII. Services and Trade
-
Transport Industry and Warehousing
- Storage
Rehabilitation and Prevention Programmes
Most individuals with recognized CVD are able to work effectively and productively in most of the jobs found in the modern workplace. Just a few decades ago, individuals surviving an acute myocardial infarction were cosseted and pampered for weeks and months with close supervision and enforced inactivity. Laboratory confirmation of the diagnosis was enough to justify labelling the individual as “permanently and totally disabled”. New diagnostic technology that provides more accurate evaluation of cardiac status and the favourable experiences of those who could not or would not accept such a label, soon demonstrated that an early return to work and an optimal level of activity was not only possible but desirable (Edwards, McCallum and Taylor 1988; Theorell et al. 1991; Theorell 1993). Today, patients commence supervised physical activity as soon as the acute effects of the infarction subside, are often out of the hospital in a few days instead of the mandatory 6 to 8 weeks of yore, and are often back on the job within a few weeks. When desirable and feasible, surgical procedures such as angioplasty, by-pass operations and even cardiac transplantation can improve the coronary blood flow, while a regimen featuring diet, exercise and control of the risk factors for CHD can minimize (or even reverse) the progression of coronary atherosclerosis.
Once the acute, often life-threatening phases of the CVD have been overcome, passive movement followed by active exercise should be initiated early during the stay in the hospital or clinic. With heart attacks, this phase is completed when the individual can climb stairs without great difficulty. At the same time, the individual is schooled in a risk-prevention regimen that includes proper diet, cardiovascular conditioning exercises, adequate rest and relaxation, and stress management. During these phases of rehabilitation, support from family members, friends and co-workers can be particularly helpful (Brusis and Weber-Falkensammer 1986). The programme can be carried out in rehabilitation facilities or in ambulatory “heart groups” under the supervision of a trained physician (Halhubar and Traencker 1986). The focus on controlling lifestyle and behavioural risk factors and controlling stress has been shown to result in a measurable reduction in the risk of re-infarction and other cardiovascular problems.
Throughout the programme the attending physician should maintain contact with the employer (and particularly with the company doctor, if there is one) to discuss the prospects for recovery and the probable duration of the period of disability, and to explore the feasibility of any special arrangements that may be needed to permit an early return to the job. The worker’s knowledge that the job is waiting and that he or she is expected to be able to return to it is a potent motivating factor for the enhancement of recovery. Experience has amply demonstrated that the success of the rehabilitation effort diminishes as the absence from work lengthens.
In instances where desirable adjustments in the job and/or the workplace are not possible or feasible, retraining and appropriate job placement can obviate unnecessary invalidism. Specially protected workshops are often helpful in reintegrating into the workplace people who have been absent from the job for long periods while receiving treatment for the serious effects of stroke, congestive heart failure or disabling angina pectoris.
Following the return to work, continued surveillance by both the attending physician and the occupational physician is eminently desirable. Periodic medical evaluations, at intervals that are frequent initially but lengthen as recovery is assured, are helpful in assessing the worker’s cardiovascular status, adjusting medications and other elements in the maintenance regimen and monitoring the adherence to the lifestyle and behavioural recommendations. Satisfactory findings in these examinations may allow the gradual easing of any work limitations or restrictions until the worker is fully integrated into the workplace.
Workplace Health Promotion and Prevention Programmes
The prevention of occupational diseases and injuries is a prime responsibility of the organization’s occupational health and safety programme. This includes primary prevention (i.e., the identifica- tion and elimination or control of potential hazards and strains by changing the work environment or the job). It is supplemented by secondary prevention measures which protect the workers from the effects of existing hazards and strains that cannot be elim- inated (i.e., personal protective equipment and periodic medical surveillance examinations). Workplace health promotion and pre- vention (HPP) programmes go beyond these goals. They place their emphasis on health-conscious behaviour as it relates to life- style, behavioural risk factors, eliminating or coping with stress and so on. They are of great significance, particularly in pre- venting CVD. The goals of HPP, as formulated by the WHO Committee on Environmental and Health Monitoring in Occupational Health, extend beyond the mere absence of disease and injury to include well-being and functional capacity (WHO 1973).
The design and operation of HPP programmes are discussed in more detail elsewhere in the chapter. In most countries, they have a particular focus on the prevention of CVDs. For example, in Germany, the “Have a heart for your heart” programme supplements the heart health circles organized by the health insurance companies (Murza and Laaser 1990, 1992), while the “Take Heart” movement in Britain and Australia has similar goals (Glasgow et al. 1995).
That such programmes are effective was verified in the 1980s by the WHO Collaborative Trial in Prevention of Heart Disease, which was carried out in 40 pairs of factories in four European countries and involved approximately 61,000 men aged 40 to 59. The preventive measures largely comprised health education activities, carried out primarily by the organization’s employee health service, focused on cholesterol-lowering diets, giving up cigarette smoking, weight control, increased physical activity and controlling hypertension. A randomized screening of 10% of the eligible workers in the factories designated as controls demonstrated that during the 4 to 7 years of the study, overall risk of CVDs could be reduced by 11.1% (19.4% among those initially at high risk). In the study factories, mortality from CHDs fell by 7.4%, while overall mortality fell by 2.7%. The best results were achieved in Belgium, where the intervention was carried out continuously during the entire study period, while the poorest results were seen in Britain, where the prevention activities were sharply curtailed prior to the last follow-up examination. This disparity emphasizes the relationship of success to the duration of the health education effort; it takes time to inculcate the desired lifestyle changes. The intensity of the educational effort was also a factor: in Italy, where six full-time health educators were involved, a 28% reduction in overall risk-factor profile was achieved, whereas in Britain, where only two full-time educators served three times the number of workers, a risk factor reduction of only 4% was achieved.
While the time required to detect reductions in CHD mortality and morbidity is a formidable limiting factor in epidemiological studies aimed at evaluating the results of company health programmes (Mannebach 1989), reductions in risk factors have been demonstrated (Janssen 1991; Gomel et al. 1993; Glasgow et al. 1995). Temporary decreases in the number of lost workdays and a decline in hospitalization rates have been reported (Harris 1994). There seems to be general agreement that HPP activities in the community and particularly in the workplace have significantly contributed to the reduction in cardiovascular mortality in the United States and other western industrialized countries.
Conclusion
CVDs loom large in the workplace, not so much because the cardiovascular system is particularly vulnerable to environmental and job hazards, but because they are so common in the popu- lation of working age. The workplace offers a singularly advant- ageous arena for the detection of unrecognized, asymptomatic CVDs, for the circumvention of workplace factors that might accelerate or aggravate them and for the identification of factors that increase the risk of CVDs and the mounting of programmes to eliminate or control them. When CVDs do occur, prompt attention to control of job-related circumstances that may prolong or increase their severity can minimize the extent and duration of disability, while early, professionally supervised rehabilitation efforts will facilitate the restoration of working capacity and reduce the risk of recurrences.
Physical, Chemcial and Biological Hazards
The intact cardiovascular system is remarkably resistant to the harmful effects of physical, chemical and biological hazards encountered on the job or in the workplace. With a very few exceptions, such hazards are rarely a direct cause of CVDs. On the other hand, once the integrity of the cardiovascular system is compromised—and this may be entirely silent and unrecognized—exposure to these hazards may contribute to the ongoing development of a disease process or precipitate symptoms reflecting functional impairment. This dictates early identification of workers with incipient CVD and modification of their jobs and/or the work environment to reduce the risk of harmful effects. The following segments will include brief discussions of some of the more commonly encountered occupational hazards that may affect the cardiovascular system. Each of the hazards presented below is discussed more fully elsewhere in the Encyclopaedia.
The Risk Factor Concept in Cardiovascular Disease
Risk factors are genetic, physiological, behavioural and socioeconomic characteristics of individuals that place them in a cohort of the population that is more likely to develop a particular health problem or disease than the rest of the population. Usually applied to multifactorial diseases for which there is no single precise cause, they have been particularly useful in identifying candidates for primary preventive measures and in assessing the effectiveness of the prevention programme in controlling the risk factors being targeted. They owe their development to large-scale prospective population studies, such as the Framingham study of coronary artery disease and stroke conducted in Framingham, Massachusetts, in the United States, other epidemiological studies, intervention studies and experimental research.
It should be emphasized that risk factors are merely expressions of probability—that is, they are not absolute nor are they diagnostic. Having one or more risk factors for a particular disease does not necessarily mean that an individual will develop the disease, nor does it mean that an individual without any risk factors will escape the disease. Risk factors are individual characteristics which affect that person’s chances of developing a particular disease or group of diseases within a defined future time period. Categories of risk factors include:
- somatic factors, such as high blood pressure, lipid metabolism disorders, overweight and diabetes mellitus
- behavioural factors, such as smoking, poor nutrition, lack of physical movement, type-A personality, high alcohol consumption and drug abuse
- strains, including exposures in the occupational, social and private spheres.
Naturally, genetic and dispositional factors also play a role in high blood pressure, diabetes mellitus and lipid metabolism disorders. Many of the risk factors promote the development of arteriosclerosis, which is a significant precondition for the onset of coronary heart disease.
Some risk factors may put the individual at risk for the development of more than one disease; for example, cigarette smoking is associated with coronary artery disease, stroke and lung cancer. At the same time, an individual may have multiple risk factors for a particular disease; these may be additive but, more often, the combinations of risk factors may be multiplicative. Somatic and lifestyle factors have been identified as the main risk factors for coronary heart disease and stroke.
Hypertension
Hypertension (increased blood pressure), a disease in its own right, is one of the major risk factors for coronary heart disease (CHD) and stroke. As defined by the WHO, blood pressure is normal when the diastolic is below 90 mm Hg and the systolic is below 140 mm Hg. In threshold or borderline hypertension, the diastolic ranges from 90 to 94 mm Hg and the systolic from 140 to 159 mm Hg. Individuals with diastolic pressures equal to or greater than 95 mm Hg and systolic pressures equal to or greater than 160 mm Hg are designated as being hypertensive. Studies have shown, however, that such sharp criteria are not entirely correct. Some individuals have a “labile” blood pressure—the pressure fluctuates between normal and hypertensive levels depending on the circumstances of the moment. Further, without regard to the specific categories, there is a linear progression of relative risk as the pressure rises above the normal level.
In the United States, for example, the incidence rate of CHD and stroke among men aged 55 to 61 was 1.61% per year for those whose blood pressure was normal compared to 4.6% per year for those with hypertension (National Heart, Lung and Blood Institute 1981).
Diastolic pressures over 94 mm Hg were found in 2 to 36% of the population aged 35 to 64 years, according to the WHO-MONICA study. In many countries of Central, Northern and Eastern Europe (e.g., Russia, the Czech Republic, Finland, Scotland, Romania, France and parts of Germany, as well as Malta), hypertension was found in over 30% of the population aged 35 to 54, while in countries including Spain, Denmark, Belgium, Luxembourg, Canada and the United States, the corresponding figure was less than 20% (WHO-MONICA 1988). The rates tend to increase with age, and there are racial differences. (In the United States, at least, hypertension is more frequent among African-Americans than in the White population.)
Risks for developing hypertension
The important risk factors for developing hypertension are excess body weight, high salt intake, a series of other nutritional factors, high alcohol consumption, physical inactivity, and psychosocial factors, including stress (Levi 1983). Furthermore, there is a certain genetic component whose relative significance is not yet fully understood (WHO 1985). Frequent familial high blood pressure should be considered a danger and special attention paid to controlling lifestyle factors.
There is evidence that psychosocial and psychophysical factors, in conjunction with the job, can have an influence on developing hypertension, especially for short-term blood pressure increases. Increases have been found in the concentration of certain hormones (adrenalin and noradrenalin) as well as cortisol (Levi 1972), which, alone and in combination with high salt consumption, can lead to increased blood pressure. Work stress also appears to be related to hypertension. A dose-effect relationship with intensity of air traffic was shown (Levi 1972; WHO 1985) in comparing groups of air traffic controllers with different high psychic strain.
Treatment of hypertension
Hypertension can and should be treated, even in the absence of any symptoms. Lifestyle changes such as weight control, reduction of sodium intake and regular physical exercise, coupled when necessary with anti-hypertensive medications, regularly evoke re- ductions in blood pressure, often to normal levels. Unfortunately, many individuals found to be hypertensive are not receiving adequate treatment. According to the WHO-MONICA study (1988), less than 20% of hypertensive women in Russia, Malta, eastern Germany, Scotland, Finland and Italy were receiving adequate treatment during the mid-1980s, while the comparable figure for men in Ireland, Germany, China, Russia, Malta, Finland, Poland, France and Italy was under 15%.
Prevention of hypertension
The essence of preventing hypertension is identifying individuals with blood pressure elevation through periodic screening or medical examination programmes, repeated checks to verify the extent and duration of the elevation, and the institution of an appropriate treatment regimen that will be maintained indefinitely. Those with a family history of hypertension should have their pressures checked more frequently and should be guided to elimination or control of any risk factors they may present. Control of alcohol abuse, physical training and physical fitness, normal weight maintenance and efforts to reduce psychological stress are all important elements of prevention programmes. Improvement in workplace conditions, such as reducing noise and excess heat, are other preventive measures.
The workplace is a uniquely advantageous arena for programmes aimed at the detection, monitoring and control of hypertension in the workforce. Convenience and low or no cost make them attractive to the participants and the positive effects of peer pressure from co-workers tend to enhance their compliance and the success of the programme.
Hyperlipidemia
Many long-term international studies have demonstrated a convincing relationship between abnormalities in lipid metabolism and an increased risk of CHD and stroke. This is particularly true for elevated total cholesterol and LDL (low density lipoproteins) and/or low levels of HDL (high density lipoproteins). Recent research provides further evidence linking the excess risk with different lipoprotein fractions (WHO 1994a).
The frequency of elevated total cholesterol levels >>6.5 mmol/l) was shown to vary considerably in population groups by the worldwide WHO-MONICA studies in the mid-1980s (WHO- MONICA 1988). The rate of hypercholesterolemia for popu- lations of working age (35 to 64 years of age) ranged from 1.3 to 46.5% for men and 1.7 to 48.7% for women. Although the ranges were generally similar, the mean cholesterol levels for the study groups in different countries varied significantly: in Finland, Scot- land, East Germany, the Benelux countries and Malta, a mean of over 6 mmol/l was found, while the means were lower in east Asian countries like China (4.1 mmol/l) and Japan (5.0 mmol/l). In both regions, the means were below 6.5 mmol/l (250 mg/dl), the level designated as the threshold of normal; however, as noted above for blood pressure, there is a progressive increase of risk as the level rises, rather than a sharp demarcation between normal and abnormal. Indeed, some authorities have pegged a total chol- esterol level of 180 mg/dl as the optimal level that should not be exceeded.
It should be noted that gender is a factor, with women averaging lower levels of HDL. This may be one reason why women of working age have a lower mortality rate from CHD.
Except for the relatively few individuals with hereditary hyper- cholesterolemia, cholesterol levels generally reflect the dietary intake of foods rich in cholesterol and saturated fats. Diets based on fruit, plant products and fish, with reduced total fat intake and substitution of poly-unsaturated fats, are generally associated with low cholesterol levels. Although their role is not yet entirely clear, intake of anti-oxidants (vitamin E, carotene, selenium and so on) is also thought to influence cholesterol levels.
Factors associated with higher levels of HDL cholesterol, the “protective” form of lipoprotein, include race (Black), gender (female), normal weight, physical exercise and moderate alcohol intake.
Socio-economic level also appears to play a role, at least in industrialized countries, as in West Germany, where higher cholesterol levels were found in population groups of both men and women with lower education levels (under ten years of schooling) compared to those completing 12 years of education (Heinemann 1993).
Cigarette Smoking
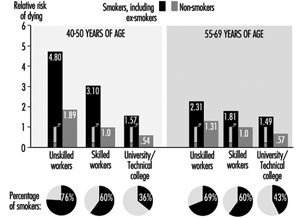
Cigarette smoking is among the most important risk factors for CVD. The risk from cigarette smoking is directly related to the number of cigarettes one smokes, the length of time one has been smoking, the age at which one began to smoke, the amount one inhales and the tar, nicotine and carbon monoxide content of the inspired smoke. Figure 1 illustrates the striking increase in CHD mortality among cigarette smokers compared to non-smokers. This increased risk is demonstrated among both men and women and in all socio-economic classes.
The relative risk of cigarette smoking declines after tobacco use is discontinued. This is progressive; after about ten years of non-smoking, the risk is down almost to the level of those who never smoked.
Recent evidence has demonstrated that those inhaling “second-hand smoke” (i.e., passive inhalation of smoke from cigarettes smoked by others) are also at significant risk (Wells 1994; Glantz and Parmley 1995).
Rates of cigarette smoking vary among countries, as demonstrated by the international WHO-MONICA study (1988). The highest rates for men aged 35 to 64 were found in Russia, Poland, Scotland, Hungary, Italy, Malta, Japan and China. More women smokers were found in Scotland, Denmark, Ireland, the United States, Hungary and Poland (the recent Polish data are limited to large cities).
Social status and occupational level are factors in the level of smoking among workers. Figure 1, for example, demonstrates that the proportions of smokers among men in East Germany increased in the lower social classes. The reverse is found in countries with relatively low numbers of smokers, where there is more smoking among those at higher social levels. In East Germany, smoking is also more frequent among shift-workers when compared with those on a “normal” work schedule.
Figure 1. Relative mortality risk from cardiovascular diseases for smokers (including ex-smokers) and social classes compared to non-smoking, normal weight, skilled workers (male) based on occupational medical care examinations in East Germany, mortality 1985-89, N= 2.7 million person years.
Unbalanced Nutrition, Salt Consumption
In most industrialized countries traditional low-fat nutrition has been replaced by high-calorie, high-fat, low carbohydrate, too sweet or too salty eating habits. This contributes to the development of overweight, high blood pressure, and high cholesterol level as elements of high cardiovascular risk. The heavy consumption of animal fats, with their high proportion of saturated fatty acids, leads to an increase in LDL cholesterol and increased risk. Fats derived from vegetables are much lower in these substances (WHO 1994a). Eating habits are also strongly associated with both socio-economic level and occupation.
Overweight
Overweight (excess fat or obesity rather than increased muscle mass) is a cardiovascular risk factor of lesser direct significance. There is evidence that the male pattern of excess fat distribution (abdominal obesity) is associated with a greater risk of cardiovascular and metabolic problems than the female (pelvic) type of fat distribution.
Overweight is associated with hypertension, hypercholesterolemia and diabetes mellitus, and, to a much greater extent in women than men, tends to increase with age (Heuchert and Enderlein 1994) (Figure 2). It is also a risk factor for musculoskeletal problems and osteoarthritis, and makes physical exercise more difficult. The frequency of significant overweight varies considerably among countries. Random population surveys conducted by the WHO-MONICA project found it in more than 20% of females aged 35 to 64 in the Czech Republic, East Germany, Finland, France, Hungary, Poland, Russia, Spain and Yugoslavia, and in both sexes in Lithuania, Malta and Romania. In China, Japan, New Zealand and Sweden, fewer than 10% of both men and women in this age group were significantly overweight.
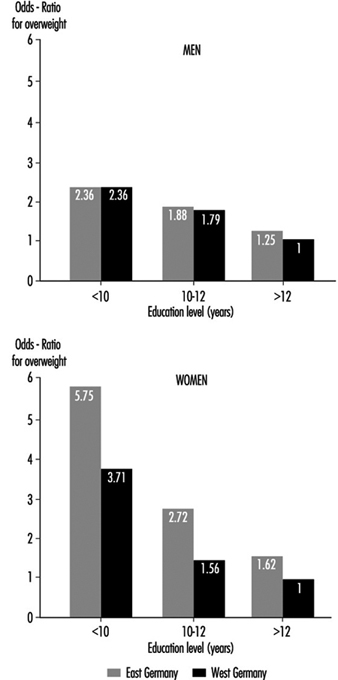
Common causes of overweight include familial factors (these may in part be genetic but more often reflect common dietary habits), overeating, high-fat and high-carbohydrate diets and lack of physical exercise. Overweight tends to be more common among the lower socio-economic strata, particularly among women, where, among other factors, financial constraints limit the availability of a more balanced diet. Population studies in Germany demonstrated that the proportion of significant overweight among those with lower education levels is 3 to 5 times greater than that among people with more education, and that some occupations, notably food preparation, agriculture and to some extent shift work, have a high percentage of overweight people (Figure 3) (Heinemann 1993).
Figure 2. Prevalence of hypertension by age, sex and six levels of relative body weight according tot he body-mass index (BMI) in occupational medical care examinations in East Germany (normal BMI values are underlined).
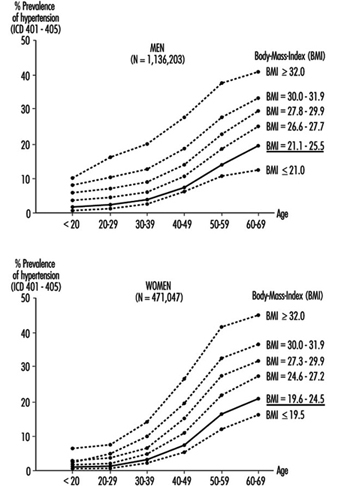
Figure 3. Relative risk from overweight by length of education(years of schooling) in Germay (population 25-64 years).
Physical Inactivity
The close association of hypertension, overweight and diabetes mellitus with lack of exercise at work and/or off the job has made physical inactivity a significant risk factor for CHD and stroke (Briazgounov 1988; WHO 1994a). A number of studies have demonstrated that, holding all other risk factors constant, there was a lower mortality rate among persons engaging regularly in high-intensity exercises than among those with a sedentary lifestyle.
The amount of exercise is readily measured by noting its duration and either the amount of physical work accomplished or the extent of the exercise-induced increase in heart rate and the time required for that rate to return to its resting level. The latter is also useful as an indicator of the level of cardiovascular fitness: with regular physical training, there will be less of an increase in heart rate and a more rapid return to the resting rate for a given intensity of exercise.
Workplace physical fitness programmes have been shown to be effective in enhancing cardiovascular fitness. Participants in these tend also to give up cigarette smoking and to pay greater attention to proper diets, thus significantly reducing their risk of CHD and stroke.
Alcohol
High alcohol consumption, especially the drinking of high-proof spirits, has been associated with a greater risk of hypertension, stroke and myocardiopathy, while moderate alcohol use, particularly of wine, has been found to reduce the risk of CHD (WHO 1994a). This has been associated with the lower CHD mortality among the upper social strata in industrialized countries, who generally prefer wine to “hard” liquors. It should also be noted that while their alcohol intake may be similar to that of wine drinkers, beer drinkers tend to accumulate excess weight, which, as noted above, may increase their risk.
Socio-economic Factors
A strong correlation between socio-economic status and the risk of CVD has been demonstrated by analyses of the death register mortality studies in Britain, Scandinavia, Western Europe, the United States and Japan. For example, in eastern Germany, the cardiovascular death rate is considerably lower for the upper social classes than for the lower classes (see Figure 1) (Marmot and Theorell 1991). In England and Wales, where general mortality rates are declining, the relative gap between the upper and lower classes is widening.
Socio-economic status is typically defined by such indicators as occupation, occupational qualifications and position, level of education and, in some instances, income level. These are readily translated into standard of living, nutritional patterns, free-time activities, family size and access to medical care. As noted above, behavioural risk factors (such as smoking and diet) and the somatic risk factors (such as overweight, hypertension and hyperlipidemia) vary considerably among social classes and occupational groups (Mielck 1994; Helmert, Shea and Maschewsky Schneider 1995).
Occupational Psychosocial Factors and Stress
Occupational stress
Psychosocial factors at the workplace primarily refer to the combined effect of working environment, work content, work demands and technological-organizational conditions, and also to personal factors like capability, psychological sensitivity, and finally also to health indicators (Karasek and Theorell 1990; Siegrist 1995).
The role of acute stress on people who already suffer from cardiovascular disease is uncontested. Stress leads to episodes of angina pectoris, rhythm disorders and heart failure; it can also precipitate a stroke and/or a heart attack. In this context stress is generally understood to mean acute physical stress. But evidence has been mounting that acute psychosocial stress can also have these effects. Studies from the 1950s showed that people who work two jobs at a time, or who work overtime for long periods, have a relatively higher risk of heart attack, even at a young age. Other studies showed that in the same job, the person with the greater work and time pressure and frequent problems on the job is at significantly greater risk (Mielck 1994).
In the last 15 years, job stress research suggests a causal relationship between work stress and the incidence of cardiovascular disease. This is true for cardiovascular mortality as well as frequency of coronary disease and hypertension (Schnall, Landsbergis and Baker 1994). Karasek’s job strain model defined two factors that could lead to an increased incidence of cardiovascular disease:
- extent of job demands
- extent of decision-making latitude.
Later Johnson added as a third factor the extent of social support (Kristensen 1995) which is discussed more fully elsewhere in this Encyclopaedia. The chapter Psychosocial and Organizational Factors includes discussions on individual factors, such as Type A personality, as well as social support and other mechan- isms for overcoming the effects of stress.
The effects of factors, whether individual or situational, that lead to increased risk of cardiovascular disease can be reduced by “coping mechanisms”, that is, by recognizing the problem and overcoming it by attempting to make the best of the situation.
Until now, measures aimed at the individual have predominated in the prevention of the negative health effects of work stress. Increasingly, improvements in organizing the work and expanding employee decision-making latitude have been used (e.g., action research and collective bargaining; in Germany, occupational quality and health circles) to achieve an improvement in productivity as well as to humanize the work by decreasing the stress load (Landsbergis et al. 1993).
Night and Shift Work
Numerous publications in the international literature cover the health risks posed by night and shift work. It is generally accepted that shift work is one risk factor which, together with other relev- ant (including indirect) work-related demands and expectation factors, leads to adverse effects.
In the last decade research on shift work has increasingly dealt with the long-term effects of night and shift work on the frequency of cardiovascular disease, especially ischaemic heart disease and myocardial infarction, as well as cardiovascular risk factors. The results of epidemiological studies, especially from Scandinavia, permit a higher risk of ischemic heart disease and myocardial infarction to be presumed for shift workers (Alfredsson, Karasek and Theorell 1982; Alfredsson, Spetz and Theorell 1985; Knutsson et al. 1986; Tüchsen 1993). In Denmark it was even estimated that 7% of cardiovascular disease in men as well as women can be traced to shift work (Olsen and Kristensen 1991).
The hypothesis that night and shift workers have a higher risk (estimated relative risk approximately 1.4) for cardiovascular disease is supported by other studies that consider cardiovascular risk factors like hypertension or fatty acid levels for shift workers as compared to day workers. Various studies have shown that night and shift work may induce increased blood pressure and hypertension as well as increased triglyceride and/or serum cholesterol (as well as normal range fluctuations for HDL-cholesterol in increased total cholesterol). These changes, together with other risk factors (like heavy cigarette smoking and overweight among shift workers), can cause increased morbidity and mortality due to atherosclerotic disease (DeBacker et al. 1984; DeBacker et al. 1987; Härenstam et al. 1987; Knutsson 1989; Lavie et al. 1989; Lennernäs, Åkerstedt and Hambraeus 1994; Orth-Gomer 1983; Romon et al. 1992).
In all, the question of possible causal links between shift work and atherosclerosis cannot be definitively answered at present, as the pathomechanism is not sufficiently clear. Possible mechanisms discussed in the literature include changes in nutrition and smoking habits, poor sleep quality, increases in lipid level, chronic stress from social and psychological demands and disrupted circadian rhythms. Knutsson (1989) has proposed an interesting pathogenesis for the long-term effects of shift work on chronic morbidity.
The effects of various associated attributes on risk estimation have hardly been studied, since in the occupational field other stress-inducing working conditions (noise, chemical hazardous materials, psychosocial stress, monotony and so on) are connected with shift work. From the observation that unhealthy nutritional and smoking habits are often connected with shift work, it is often concluded that an increased risk of cardiovascular disease among shift workers is more the indirect result of unhealthy behaviour (smoking, poor nutrition and so on) than directly the result of night or shift work (Rutenfranz, Knauth and Angersbach 1981). Furthermore, the obvious hypothesis of whether shift work promotes this conduct or whether the difference comes primarily from the choice of workplace and occupation must be tested. But regardless of the unanswered questions, special attention must be paid in cardiovascular prevention programmes to night and shift workers as a risk group.
Summary
In summary, risk factors represent a broad variety of genetic, somatic, physiological, behavioural and psychosocial characteristics which can be assessed individually for individuals and for groups of individuals. In the aggregate, they reflect the probability that CVD, or more precisely in the context of this article, CHD or stroke will develop. In addition to elucidating the causes and pathogenesis of multifactorial diseases, their chief importance is that they delineate individuals who should be targets for risk factor elimination or control, an exercise admirably suited to the workplace, while repeated risk assessments over time demonstrate the success of that preventive effort.
Cardiovascular Morbidity and Mortality in the Workforce
In the following article, the term cardiovascular diseases (CVDs) refers to organic and functional disorders of the heart and circu- latory system, including the resultant damage to other organ systems, which are classified under numbers 390 to 459 in the 9th revision of the International Classification of Diseases (ICD) (World Health Organization (WHO) 1975). Based essentially on international statistics assembled by the WHO and data collected in Germany, the article discusses the prevalence of CVDs, new disease rates, and frequency of deaths, morbidity and disability.
Definition and Prevalence in the Working-Age Population
Coronary artery disease (ICD 410-414) resulting in ischaemia of the myocardium is probably the most significant CVD in the working population, particularly in industrialized countries. This condition results from a constriction in the vascular system that supplies the heart muscle, a problem caused primarily by arteriosclerosis. It affects 0.9 to 1.5% of working-age men and 0.5 to 1.0% of women.
Inflammatory diseases (ICD 420-423) may involve the endo- cardium, the heart valves, the pericardium and/or the heart muscle (myocardium) itself. They are less common in industrialized countries, where their frequency is well below 0.01% of the adult population, but are seen more frequently in developing countries, perhaps reflecting the greater prevalence of nutritional disorders and infectious diseases.
Heart rhythm disorders (ICD 427) are relatively rare, although much media attention has been given to recent instances of disability and sudden death among prominent professional athletes. Although they can have a significant impact on the ability to work, they are often asymptomatic and transitory.
The myocardiopathies (ICD 424) are conditions which involve enlargement or thickening of the heart musculation, effectively narrowing the vessels and weakening the heart. They have attracted more attention in recent years, largely because of improved methods of diagnosis, although their pathogenesis is often obscure. They have been attributed to infections, metabolic diseases, immunologic disorders, inflammatory diseases involving the capillaries and, of particular importance in this volume, to toxic exposures in the workplace. They are divided into three types:
- dilative—the most common form (5 to 15 cases per 100,000 people), which is associated with the functional weakening of the heart
- hypertrophic—thickening and enlargement of the myocardium resulting in relative insufficiency of the coronary arteries
- restrictive—a rare type in which myocardial contractions are limited.
Hypertension (ICD 401-405) (increased systolic and/or diastolic blood pressure) is the most common circulatory disease, being found among 15 to 20% of working people in industrialized countries. It is discussed in greater detail below.
Atherosclerotic changes in the major blood vessels (ICD 440), often associated with hypertension, cause disease in the organs they serve. Foremost among these is cerebrovascular disease (ICD 430-438), which may result in a stroke due to infarction and/or haemorrhage. This occurs in 0.3 to 1.0% of working people, most commonly among those aged 40 and older.
Atherosclerotic diseases, including coronary artery disease, stroke and hypertension, by far the most common cardiovascular diseases in the working population, are multifactorial in origin and have their onset early in life. They are of importance in the workplace because:
- so large a proportion of the workforce has an asymptomatic or unrecognized form of cardiovascular disease
- the development of that disease may be aggravated or acute symptomatic events precipitated by working conditions and job demands
- the acute onset of a symptomatic phase of the cardiovascular disease is often attributed to the job and/or the workplace environment
- most individuals with an established cardiovascular disease are capable of working productively, albeit, sometimes, only after effective rehabilitation and job retraining
- the workplace is a uniquely propitious arena for primary and secondary preventive programmes.
Functional circulatory disorders in the extremities (ICD 443) include Raynaud’s disease, short-term pallor of the fingers, and are relatively rare. Some occupational conditions, such as frostbite, long-term exposure to vinyl chloride and hand-arm exposure to vibration can induce these disorders.
Varicosities in the leg veins (ICD 454), often improperly dismissed as a cosmetic problem, are frequent among women, especially during pregnancy. While a hereditary tendency to weakness of the vein walls may be a factor, they are usually associated with long periods of standing in one position without movement, during which the static pressure within the veins is increased. The result- ant discomfort and leg oedema often dictate change or modifi- cation of the job.
Annual incidence rates
Among the CVDs, hypertension has the highest annual new case rate among working people aged 35 to 64. New cases develop in approximately 1% of that population every year. Next in frequency are coronary heart disease (8 to 92 new cases of acute heart attack per 10,000 men per year, and 3 to 16 new cases per 10,000 women per year) and stroke (12 to 30 cases per 10,000 men per year, and 6 to 30 cases per 10,000 women per year). As demonstrated by global data collected by the WHO-Monica project (WHO-MONICA 1994; WHO-MONICA 1988), the lowest new incidence rates for heart attack were found among men in China and women in Spain, while the highest rates were found among both men and women in Scotland. The significance of these data is that in the population of working age, 40 to 60% of heart attack victims and 30 to 40% of stroke victims do not survive their initial episodes.
Mortality
Within the primary working ages of 15 to 64, only 8 to 18% of deaths from CVDs occur prior to age 45. Most occur after age 45, with the annual rate increasing with age. The rates, which have been changing, vary considerably from country to country (WHO 1994b).
Table 1 shows the death rates for men and for women aged 45 to 54 and 55 to 64 for some countries. Note that the death rates for men are consistently higher than those for women of corresponding ages. Table 2 compares the death rates for various CVDs among people aged 55 to 64 in five countries.
Table 1. Mortality from cardiovascular diseases in 1991 and 1990 in the age groups 45-54 and 55-64 for selected countries.
|
Country |
Men |
Women |
||||||
|
45-54 Years |
55-64 Years |
45-54 Years |
55-64 Years |
|||||
|
Rate |
% |
Rate |
% |
Rate |
% |
Rate |
% |
|
|
Russia** |
528 |
36 |
1,290 |
44 |
162 |
33 |
559 |
49 |
|
Poland** |
480 |
38 |
1,193 |
45 |
134 |
31 |
430 |
42 |
|
Argentina* |
317 |
40 |
847 |
44 |
131 |
33 |
339 |
39 |
|
Britain** |
198 |
42 |
665 |
47 |
59 |
20 |
267 |
32 |
|
USA* |
212 |
35 |
623 |
40 |
83 |
24 |
273 |
31 |
|
Germany** |
181 |
29 |
597 |
38 |
55 |
18 |
213 |
30 |
|
Italy* |
123 |
27 |
404 |
30 |
41 |
18 |
148 |
25 |
|
Mexico** |
128 |
17 |
346 |
23 |
82 |
19 |
230 |
24 |
|
France** |
102 |
17 |
311 |
22 |
30 |
12 |
94 |
18 |
|
Japan** |
111 |
27 |
281 |
26 |
48 |
22 |
119 |
26 |
*1990. **1991. Rate=Deaths per 100,000 inhabitants. % is from all causes of death in the age group.
Table 2. Mortality rates from special cardiovascular diagnosis groups in the years 1991 and 1990 in the age group 55-64 for selected countries
|
Diagnosis group |
Russia (1991) |
USA (1990) |
Germany (1991) |
France (1991) |
Japan (1991) |
|||||
|
|
M |
F |
M |
F |
M |
F |
M |
F |
M |
F |
|
393–398 |
16.8 |
21.9 |
3.3 |
4.6 |
3.6 |
4.4 |
2.2 |
2.3 |
1.2 |
1.9 |
|
401–405 |
22.2 |
18.5 |
23.0 |
14.6 |
16.9 |
9.7 |
9.4 |
4.4 |
4.0 |
1.6 |
|
410 |
160.2 |
48.9 |
216.4 |
79.9 |
245.2 |
61.3 |
100.7 |
20.5 |
45.9 |
13.7 |
|
411–414 |
586.3 |
189.9 |
159.0 |
59.5 |
99.2 |
31.8 |
35.8 |
6.8 |
15.2 |
4.2 |
|
415–429 |
60.9 |
24.0 |
140.4 |
64.7 |
112.8 |
49.2 |
73.2 |
27.0 |
98.7 |
40.9 |
|
430–438 |
385.0 |
228.5 |
54.4 |
42.2 |
84.1 |
43.8 |
59.1 |
26.7 |
107.3 |
53.6 |
|
440 |
|
|
4.4 |
2.1 |
11.8 |
3.8 |
1.5 |
0.3 |
0.3 |
0.1 |
|
Total 390–459 |
1,290 |
559 |
623 |
273 |
597 |
213 |
311 |
94 |
281 |
119 |
Deaths per 100,000 inhabitants; M=male; F=female.
Work Disability and Early Retirement
Diagnosis-related statistics on time lost from work represent an important perspective on the impact of morbidity on the working population, even though the diagnostic designations are usually less precise than in cases of early retirement because of disability. The case rates, usually expressed in cases per 10,000 employees, provide an index of the frequency of the disease categories, while the average number of days lost per case indicates the relative seriousness of particular diseases. Thus, according to statistics on 10 million workers in western Germany compiled by the Allgemeinen Ortskrankenkasse, CVDs accounted for 7.7% of the total disability in 1991-92, although the number of cases for that period was only 4.6% of the total (Table 3). In some countries, where early retirement is provided when work ability is reduced due to illness, the pattern of disability mirrors the rates for different categories of CVD.
Table 3. Rate of cardiovascular disease among early pensioners* due to reduced ability to work (N = 576,079) and diagnosis-related work disability in the western part of Germany, 1990-92
|
Diagnosis group |
Main cause of illness |
Access to early retirement; number per 100,000 early retirees |
Average annual work disability 1990–92 |
||||
|
Cases per 100,000 employed |
Duration (days) per case |
||||||
|
Men |
Women |
Men |
Women |
Men |
Women |
||
|
390–392 |
Acute rheumatic fever |
16 |
24 |
49 |
60 |
28.1 |
32.8 |
|
393–398 |
Chronic rheumatic heart disease |
604 |
605 |
24 |
20 |
67.5 |
64.5 |
|
401–405 |
Hypertension, high blood pressure diseases |
4,158 |
4,709 |
982 |
1,166 |
24.5 |
21.6 |
|
410–414 |
Ischaemic heart diseases |
9,635 |
2,981 |
1,176 |
529 |
51.2 |
35.4 |
|
410, 412 |
Acute and existing myocardial infarction |
2,293 |
621 |
276 |
73 |
85.8 |
68.4 |
|
414 |
Coronary heart disease |
6,932 |
2,183 |
337 |
135 |
50.8 |
37.4 |
|
415–417 |
Pulmonary circulatory diseases |
248 |
124 |
23 |
26 |
58.5 |
44.8 |
|
420–429 |
Other non-rheumatic heart diseases |
3,434 |
1,947 |
645 |
544 |
36.3 |
25.7 |
|
420–423 |
Inflammatory heart diseases |
141 |
118 |
20 |
12 |
49.4 |
48.5 |
|
424 |
Heart valve disorders |
108 |
119 |
22 |
18 |
45.6 |
38.5 |
|
425 |
Myocardiopathy |
1,257 |
402 |
38 |
14 |
66.8 |
49.2 |
|
426 |
Stimulus performance disorder |
86 |
55 |
12 |
7 |
39.6 |
45.0 |
|
427 |
Cardiac rhythm disorder |
734 |
470 |
291 |
274 |
29.3 |
21.8 |
|
428 |
Cardiac insufficiency |
981 |
722 |
82 |
61 |
62.4 |
42.5 |
|
430–438 |
Cerebrovascular diseases |
4,415 |
2,592 |
172 |
120 |
75.6 |
58.9 |
|
440–448 |
Diseases of the arteries, arterioles and capillaries |
3,785 |
1,540 |
238 |
90 |
59.9 |
44.5 |
|
440 |
Arteriosclerosis |
2,453 |
1,090 |
27 |
10 |
71.7 |
47.6 |
|
443 |
Raynaud’s disease and other vascular diseases |
107 |
53 |
63 |
25 |
50.6 |
33.5 |
|
444 |
Arterial embolism and thrombosis |
219 |
72 |
113 |
34 |
63.3 |
49.5 |
|
451–456 |
Diseases of the veins |
464 |
679 |
1,020 |
1,427 |
22.9 |
20.3 |
|
457 |
Noninfectious diseases of the lymph nodes |
16 |
122 |
142 |
132 |
10.4 |
14.2 |
|
458 |
Hypotension |
29 |
62 |
616 |
1,501 |
9.4 |
9.5 |
|
459 |
Other circulatory diseases |
37 |
41 |
1,056 |
2,094 |
11.5 |
10.2 |
|
390–459 |
Total cardiovascular diseases |
26,843 |
15,426 |
6,143 |
7,761 |
29.6 |
18.9 |
*Early pensioned: Statutory pensions insurance for former Federal Republic of Germany, work disability AOK-West.
Introduction
Cardiovascular diseases (CVDs) are among the most common causes of illness and death in the working population, particularly in industrialized countries. They are also increasing in developing countries (Wielgosz 1993). In the industrialized countries, 15 to 20% of all working people will suffer from a cardiovascular dis- order sometime during their working lives and the frequency climbs sharply with age. Among those between 45 to 64 years of age, more than a third of the deaths among men and more than a quarter of deaths among women are caused by this group of diseases (see table 1). In recent years, CVDs have become the most frequent cause of death among post-menopausal women.
Table 1. Mortality from cardiovascular diseases in 1991 and 1990 in the age groups 45-54 and 55-64 for selected countries.
|
Country |
Men |
Women |
||||||
|
45-54 Years |
55-64 Years |
45-54 Years |
55-64 Years |
|||||
|
Rate |
% |
Rate |
% |
Rate |
% |
Rate |
% |
|
|
Russia** |
528 |
36 |
1,290 |
44 |
162 |
33 |
559 |
49 |
|
Poland** |
480 |
38 |
1,193 |
45 |
134 |
31 |
430 |
42 |
|
Argentina* |
317 |
40 |
847 |
44 |
131 |
33 |
339 |
39 |
|
Britain** |
198 |
42 |
665 |
47 |
59 |
20 |
267 |
32 |
|
USA* |
212 |
35 |
623 |
40 |
83 |
24 |
273 |
31 |
|
Germany** |
181 |
29 |
597 |
38 |
55 |
18 |
213 |
30 |
|
Italy* |
123 |
27 |
404 |
30 |
41 |
18 |
148 |
25 |
|
Mexico** |
128 |
17 |
346 |
23 |
82 |
19 |
230 |
24 |
|
France** |
102 |
17 |
311 |
22 |
30 |
12 |
94 |
18 |
|
Japan** |
111 |
27 |
281 |
26 |
48 |
22 |
119 |
26 |
*1990. **1991. Rate=Deaths per 100,000 inhabitants. % is from all causes of death in the age group.
Because of their complex aetiology, only a very small pro- portion of the cases of cardiovascular disease are recognized as occupational. Many countries, however, recognize that occu- pational exposures contribute to CVDs (sometimes referred to as work-related diseases). Working conditions and job demands play an important role in the multifactorial process that leads to these diseases, but ascertaining the role of the individual causal com- ponents is very difficult. The components interact in close, shifting relationships and often the disease is triggered by a combination or accumulation of different causal factors, including those that are work related.
The reader is referred to the standard cardiology texts for details of the epidemiology, pathophysiology, diagnosis and treatment of cardiovascular diseases. This chapter will focus on those aspects of cardiovascular disease that are particularly relevant in the workplace and are likely to be influenced by factors in the job and work environment.
Workplace Biohazards
The assessment of biohazards in the workplace has been concentrated on agricultural workers, health-care workers and laboratory personnel, who are at considerable risk of adverse health effects. A detailed compilation of biohazards by Dutkiewicz et al. (1988) shows how widespread the risks can be to workers in many other occupations as well (table 1).
Dutkiewicz et al. (1988) further taxonomically classified the micro-organisms and plants (table 2), as well as animals (table 3), which might possibly present biohazards in work settings.
Table 1. Occupational settings with potential exposure of workers to biological agents
|
Sector |
Examples |
|
Agriculture |
Cultivating and harvesting |
|
Agricultural products |
Abattoirs, food packaging plants |
|
Laboratory animal care |
|
|
Health care |
Patient care: medical, dental |
|
Pharmaceutical and herbal products |
|
|
Personal care |
Hairdressing, chiropody |
|
Clinical and research laboratories |
|
|
Biotechnology |
Production facilities |
|
Day-care centres |
|
|
Building maintenance |
“Sick” buildings |
|
Sewage and compost facilities |
|
|
Industrial waste disposal systems |
Source: Dutkiewicz et al. 1988.
Micro-organisms
Micro-organisms are a large and diverse group of organisms that exist as single cells or cell clusters (Brock and Madigan 1988). Microbial cells are thus distinct from the cells of animals and plants, which are unable to live alone in nature but can exist only as parts of multicellular organisms.
Very few areas on the surface of this planet do not support microbial life, because micro-organisms have an astounding range of metabolic and energy-yielding abilities and many can exist under conditions that are lethal to other life forms.
Four broad classes of micro-organisms that can interact with humans are bacteria, fungi, viruses and protozoa. They are hazardous to workers due to their wide distribution in the working environment. The most important micro-organisms of occupational hazard are listed in tables 2 and 3.
There are three major sources of such microbes:
- those arising from microbial decomposition of various substrates associated with particular occupations (e.g., mouldy hay leading to hypersensitivity pneumonitis)
- those associated with certain types of environments (e.g., bacteria in water supplies)
- those stemming from infective individuals harbouring a particular pathogen (e.g., tuberculosis).
Ambient air may be contaminated with or carry significant levels of a variety of potentially harmful micro-organisms (Burrell 1991). Modern buildings, especially those designed for commercial and administrative purposes, constitute a unique ecological niche with their own biochemical environment, fauna and flora (Sterling et al. 1991). The potential adverse effects on workers are described elsewhere in this Encyclopaedia.
Water has been recognized as an important vehicle for extra-intestinal infection. A variety of pathogens are acquired through occupational, recreational and even therapeutic contact with water (Pitlik et al. 1987). The nature of non-enteric water-borne disease is often determined by the ecology of aquatic pathogens. Such infections are of basically two types: superficial, involving damaged or previously intact mucosae and skin; and systemic, often serious infections that may occur in the setting of depressed immunity. A broad spectrum of aquatic organisms, including viruses, bacteria, fungi, algae and parasites may invade the host through such extra-intestinal routes as the conjunctivae, respiratory mucosae, skin and genitalia.
Although zoonotic spread of infectious disease continues to occur in laboratory animals used in biomedical research, reported outbreaks have been minimized with the advent of rigorous veterinary and husbandry procedures, the use of commercially reared animals and the institution of appropriate personnel health programmes (Fox and Lipman 1991). Maintaining animals in modern facilities with appropriate safeguards against the introduction of vermin and biological vectors is also important in preventing zoonotic disease in personnel. Nevertheless, established zoonotic agents, newly discovered micro-organisms or new animal species not previously recognized as carriers of zoonotic micro-organisms are encountered, and the potential for spread of infectious disease from animals to humans still exists.
Active dialogue between veterinarians and physicians regarding the potential of zoonotic disease, the species of animals that are involved, and the methods of diagnosis, is an indispensable component of a successful preventive health programme.
Table 2. Viruses, bacteria, fungi and plants: Known biohazards in the workplace
|
Infec- |
Infection zoo- |
Allergic |
Respir- |
Toxin |
Carcino- |
|
|
Viruses |
x |
x |
||||
|
Bacteria |
||||||
|
Rickettsiae |
x |
|||||
|
Chlamydiae |
x |
|||||
|
Spiral bacteria |
x |
|||||
|
Gram-negative |
|
|
|
|
||
|
Gram-positive |
|
|
||||
|
Spore-forming |
|
|
|
|||
|
Non-sporing gram- |
|
|
||||
|
Mycobacteria |
x |
x |
||||
|
Actinomycetes |
x |
|||||
|
Fungi |
||||||
|
Moulds |
x |
x |
x(m)3 |
x |
||
|
Dermatophytes |
x |
x |
x |
|||
|
Yeast-like geophilic |
|
|
||||
|
Endogenous yeasts |
x |
|||||
|
Parasites of wheat |
x |
|||||
|
Mushrooms |
x |
|||||
|
Other lower plants |
||||||
|
Lichens |
x |
|||||
|
Liverworts |
x |
|||||
|
Ferns |
x |
|||||
|
Higher plants |
||||||
|
Pollen |
x |
|||||
|
Volatile oils |
x |
x |
||||
|
Dusts-processing |
x |
x |
x |
1 Infection-zoonosis: Causes infection or invasion usually contracted from vertebrate animals (zoonosis).
2 (e) Endotoxin.
3 (m) Mycotoxin.
Source: Dutkiewicz et al. 1988.
Some Occupational Settings with Biohazards
Medical and laboratory staff and other health-care workers, including related professions, are exposed to infection by micro-organisms if the appropriate preventive measures are not taken. Hospital workers are exposed to many biological hazards, including human immunodeficiency virus (HIV), hepatitis B, herpes viruses, rubella and tuberculosis (Hewitt 1993).
Work in the agricultural sector is associated with a wide variety of occupational hazards. Exposure to organic dust, and to airborne micro-organisms and their toxins, may lead to respiratory disorders (Zejda et al. 1993). These include chronic bronchitis, asthma, hypersensitivity pneumonitis, organic dust toxic syndrome and chronic obstructive pulmonary disease. Dutkiewicz and his colleagues (1988) studied samples of silage for the identification of potential agents causing symptoms of organic and toxic syndrome. Very high levels of total aerobic bacteria and fungi were found. Aspergillus fumigatus predominated among the fungi, whereas bacillus and gram-negative organisms (Pseudomonas, Alcaligenes, Citrobacter and Klebsiella species) and actinomycetes prevailed among the bacteria. These results show that contact with aerosolized silage carries the risk of exposure to high concentrations of micro-organisms, of which A. fumigatus and endotoxin-producing bacteria are the most probable disease agents.
Short-term exposures to certain wood dusts may result in asthma, conjunctivitis, rhinitis or allergic dermatitis. Some thermophilic micro-organisms found in wood are human pathogens, and inhalation of ascomycete spores from stored wood chips has been implicated in human illnesses (Jacjels 1985).
Examples illustrative of specific working conditions follow:
- The fungus Penicillium camemberti var. candidum is used in the production of some types of cheese. The high frequency of precipitating antibodies of this fungus in the workers’ blood samples, together with the clinical causes of the airway symptoms, indicate an aetiological relationship between airway symptoms and heavy exposure to this fungus (Dahl et al. 1994).
- Micro-organisms (bacteria and fungi) and endotoxins are potential agents of occupational hazard in a potato processing plant (Dutkiewicz 1994). The presence of precipitins to microbial antigens was significantly correlated with the occurrence of the work-related respiratory and general symptoms that were found in 45.9% of the examined workers.
- Museum and library personnel are exposed to moulds (e.g., Aspergillus, Pencillium) which, under certain conditions, contaminate books (Kolmodin-Hedman et al. 1986). Symptoms experienced are attacks of fever, chill, nausea and cough.
- Ocular infections can result from the use of industrial microscope eyepieces on multiple shifts. Staphylococcus aureus has been identified among the micro-organism cultures (Olcerst 1987).
Prevention
An understanding of the principles of epidemiology and the spread of infectious disease is essential in the methods used in the control of the causing organism.
Preliminary and periodic medical examinations of workers should be carried out in order to detect biological occupational diseases. There are general principles for conducting medical examinations in order to detect adverse health effects of workplace exposure, including biological hazards. Specific procedures are to be found elsewhere in this Encyclopaedia. For example, in Sweden the Farmers’ Federation initiated a programme of preventive occupational health services for farmers (Hoglund 1990). The main goal of the Farmers’ Preventive Health Service (FPHS) is to prevent work-related injuries and illnesses and to provide clinical services to farmers for occupational medical problems.
For some infectious disease outbreaks, appropriate preventive measures may be difficult to put in place until the disease is identified. Outbreaks of the viral Crimean-Congo haemorrhagic fever (CCHF) which demonstrated this problem were reported among hospital staff in the United Arab Emirates (Dubai), Pakistan and South Africa (Van Eeden et al. 1985).
Table 3. Animals as a source of occupational hazards
|
Infection |
Infection1 |
Allergic |
Toxin |
Vector2 |
|
|
Invertebrates other than arthropods |
|||||
|
Protozoa |
x |
x |
|||
|
Sponges |
x |
||||
|
Coelenterates |
x |
||||
|
Flatworms |
x |
x |
|||
|
Roundworms |
x |
x |
x |
||
|
Bryozoa |
x |
||||
|
Sea-squirts |
x |
||||
|
Arthropods |
|||||
|
Crustaceans |
x |
||||
|
Arachnids |
|||||
|
Spiders |
x(B)3 |
||||
|
Mites |
x |
x |
x(B) |
x |
|
|
Ticks |
x(B) |
x |
|||
|
Insects |
|||||
|
Cockroaches |
x |
||||
|
Beetles |
x |
||||
|
Moths |
x |
x |
|||
|
Flies |
x(B) |
x |
|||
|
Bees |
x |
x(B) |
|||
|
Vertebrates |
|||||
|
Fish |
x |
x(B) |
|||
|
Amphibians |
x |
||||
|
Reptiles |
x(B) |
||||
|
Birds |
x |
||||
|
Mammals |
x |
||||
1 Infection-zoonosis: Causes infection or invasion contracted from vertebrate animals.
2 Vector of pathogenic viruses, bacteria or parasites.
3 Toxic B produces toxin or venom transmitted by bite or sting.
Vertebrates: Snakes and Lizards
In hot and temperate zones, snakebites may constitute a definite hazard for certain categories of workers: agricultural workers, woodcutters, building and civil engineering workers, fishermen, mushroom gatherers, snake charmers, zoo attendants and laboratory workers employed in the preparation of antivenom serums. The vast majority of snakes are harmless to humans, although a number are capable of inflicting serious injury with their venomous bites; dangerous species are found among both the terrestrial snakes (Colubridae and Viperidae) and aquatic snakes (Hydrophiidae) (Rioux and Juminer 1983).
According to the World Health Organization (WHO 1995), snakebites are estimated to cause 30,000 deaths per year in Asia and about 1,000 deaths each in Africa and South America. More detailed statistics are available from certain countries. Over 63,000 snakebites and scorpion stings with over 300 deaths are reported yearly in Mexico. In Brazil, about 20,000 snakebites and 7,000 to 8,000 scorpion stings occur annually, with a case-fatality rate of 1.5% for snake bites and between 0.3% and 1% for scorpion stings. A study in Ouagadougou, Burkina Faso, showed 7.5 snakebites per 100,000 population in peri-urban areas and up to over 69 per 100,000 in more remote areas, where case-fatality rates reached 3%.
Snakebites are a problem also in developed parts of the world. Each year about 45,000 snakebites are reported in the United States, where the availability of health care has reduced the number of deaths to 9–15 per year. In Australia, where some of the world’s most venomous snakes exist, the annual number of snakebites is estimated at between 300 and 500, with an average of two deaths.
Environmental changes, particularly deforestation, may have caused the disappearance of many snake species in Brazil. However, the number of reported cases of snakebites did not decrease as other and sometimes more dangerous species proliferated in some of the deforested areas (WHO 1995).
Sauria (lizards)
There are only two species of venomous lizards, both members of the genus Heloderma: H. suspectum (Gila monster) and H. horridum (beaded lizard). Venom similar to that of the Viperidae penetrates wounds inflicted by the anterior curved teeth, but bites in humans are uncommon and recovery is generally rapid (Rioux and Juminer 1983).
Prevention
Snakes do not usually attack humans unless they feel menaced, are disturbed or are trodden on. In regions infested with venomous snakes, workers should wear foot and leg protection and be provided with monovalent or polyvalent antivenom serum. It is recommended that persons working in a danger area at a distance of over half-an-hour’s travel from the nearest first-aid post should carry an antivenom kit containing a sterilized syringe. However, it should be explained to workers that bites even from the most venomous snakes are seldom fatal, since the amount of venom injected is usually small. Certain snake charmers achieve immunization by repeated injections of venom, but no scientific method of human immunization has yet been developed (Rioux and Juminer 1983).
International Standards and Biological Hazards
Many national occupational standards include biological hazards in their definition of harmful or toxic substances. However, in most regulatory frameworks, biological hazards are chiefly restricted to micro-organisms or infectious agents. Several US Occupational Safety and Health Administration (OSHA) regulations include provisions on biological hazards. The most specific are those concerning hepatitis B vaccine vaccination and blood-borne pathogens; biological hazards are also covered in regulations with a broader scope (e.g., those on hazard communication, the specifications for accident prevention signs and tags, and the regulation on training curriculum guidelines).
Although not the subject of specific regulations, the recognition and avoidance of hazards relating to animal, insect or plant life is addressed in other OSHA regulations concerning specific work settings—for example, the regulation on telecommunications, the one on temporary labour camps and the one on pulpwood logging (the latter including guidelines concerning snake-bite first-aid kits).One of the most comprehensive standards regulating biological hazards in the workplace is European Directive No. 90/679. It defines biological agents as “micro-organisms, including those which have been genetically modified, cell cultures and human endoparasites, which may be able to provoke any infection, allergy or toxicity,” and classifies biological agents into four groups according to their level of risk of infection. The Directive covers the determination and assessment of risks and employers’ obligations in terms of the replacement or reduction of risks (through engineering control measures, industrial hygiene, collective and personal protection measures and so on), information (for workers, workers’ representatives and the competent authorities), health surveillance, vaccination and record-keeping. The Annexes provide detailed information on containment measures for different “containment levels” according to the nature of the activities, the assessment of risk to workers and the nature of the biological agent concerned.
Prevention of Occupational Hazards at High Altitudes
Working at high altitudes induces a variety of biological responses, as described elsewhere in this chapter. The hyperventilatory response to altitude should cause a marked increase in the total dose of hazardous substances which may be inhaled by persons occupationally exposed, as compared to people working under similar conditions at sea level. This implies that 8-hour exposure limits used as the basis of exposure standards should be reduced. In Chile, for example, the observation that silicosis progresses faster in mines at high altitudes, led to the reduction of the permitted exposure level proportional to the barometric pressure at the workplace, when expressed in terms of mg/m3. While this may be overcorrecting at intermediate altitudes, the error will be in the favour the exposed worker. The threshold limit values (TLVs), expressed in terms of parts per million (ppm), require no adjustment, however, because both the proportion of millimoles of contaminant per mole of oxygen in air and the number of moles of oxygen required by a worker remain approximately constant at different altitudes, even though the air volume containing one mole of oxygen will vary.
In order to assure that this is true, however, the method of measurement used to determine the concentration in ppm must be truly volumetric, as is the case with Orsat’s apparatus or the Bacharach Fyrite instruments. Colourimetric tubes that are calibrated to read in ppm are not true volumetric measurements because the markings on the tube are actually caused by a chemical reaction between the air contaminant and some reagent. In all chemical reactions, substances combine in proportion to the number of moles present, not in proportion to volumes. The hand-operated air pump draws a constant volume of air through the tube at any altitude. This volume at a higher altitude will contain a smaller mass of contaminant, giving a reading lower than the actual volumetric concentration in ppm (Leichnitz 1977). Readings should be corrected by multiplying the reading by the barometric pressure at sea level and dividing the result by the barometric pressure at the sampling site, using the same units (such as torr or mbar) for both pressures.
Diffusional samplers: The laws of gas diffusion indicate that the collection efficiency of diffusional samplers is independent of barometric pressure changes. Experimental work by Lindenboom and Palmes (1983) shows that other, as yet undetermined factors influence the collection of NO2 at reduced pressures. The error is approximately 3.3% at 3,300 m and 8.5% at 5,400 m equivalent altitude. More research is needed on the causes of this variation and the effect of altitude on other gases and vapours.
No information is available on the effect of altitude on portable gas detectors calibrated in ppm, which are equipped with electrochemical diffusion sensors, but it could reasonably be expected that the same correction mentioned under colourimetric tubes would apply. Obviously the best procedure would be to calibrate them at altitude with a test gas of known concentration.
The principles of operation and measurement of electronic instruments should be examined carefully to determine whether they need recalibration when employed at high altitudes.
Sampling pumps: These pumps usually are volumetric—that is, they displace a fixed volume per revolution—but they usually are the last component of the sampling train, and the actual volume of air aspirated is affected by the resistance to flow opposed by the filters, hose, flow meters and orifices that are part of the sampling train. Rotameters will indicate a lower flow rate than that actually flowing through the sampling train.
The best solution of the problem of sampling at high altitudes is to calibrate the sampling system at the sampling site, obviating the problem of corrections. A briefcase sized bubble film calibration laboratory is available from sampling pump manufacturers. This is easily carried to location and permits rapid calibration under actual working conditions. It even includes a printer which provides a permanent record of calibrations made.
TLVs and Work Schedules
TLVs have been specified for a normal 8-hour workday and a 40-hour workweek. The present tendency in work at high altitudes is to work longer hours for a number of days and then commute to the nearest town for an extended rest period, keeping the average time at work within the legal limit, which in Chile is 48 hours per week.
Departures from the normal 8-hour working schedules make it necessary to examine the possible accumulation in the body of toxic substances due to the increase in exposure and reduction of detoxification times.
Chilean occupational health regulations have recently adopted the “Brief and Scala model’’ described by Paustenbach (1985) for reducing TLVs in the case of extended working hours. At altitude, the correction for barometric pressure should also be used. This usually results in very substantial reductions of permissible exposure limits.
In the case of cumulative hazards not subject to detoxifying mechanisms, such as silica, correction for extended working hours should be directly proportional to the actual hours worked in excess of the usual 2,000 hours per year.
Physical Hazards
Noise: The sound pressure level produced by noise of a given amplitude is in direct relation to air density, as is the amount of energy transmitted. This means that the reading obtained by a sound level meter and the effect on the inner ear are reduced in the same way, so no corrections would be required.
Accidents: Hypoxia has a pronounced influence on the central nervous system, reducing response time and disrupting vision. An increase in the incidence of accidents should be expected. Above 3,000 m, the performance of persons engaged in critical tasks will benefit from supplementary oxygen.
Precautionary Note: Air Sampling
Kenneth I. Berger and William N. Rom
The monitoring and maintenance of the occupational safety of workers requires special consideration for high altitude environments. High-altitude conditions can be expected to influence the accuracy of sampling and measuring instruments that have been calibrated for use at sea level. For example, active sampling devices rely on pumps to pull a volume of air onto a collection medium. Accurate measurement of the pump flow rate is essential in order to determine the exact volume of air drawn through the sampler and, therefore, the concentration of the contaminant. Flow calibrations are often performed at sea level. However, changes in air density with increasing altitude may alter the calibration, thereby invalidating subsequent measurements made in high altitude environments. Other factors that may influence the accuracy of sampling and measurement instruments at high altitude include changing temperature and relative humidity. An additional factor that should be considered when evaluating worker exposure to inhaled substances is the increased respiratory ventilation that occurs with acclimatization. Since ventilation is markedly increased after ascent to high altitude, workers may be exposed to excessive total doses of inhaled occupational contaminants, even though measured concentrations of the contaminant are below the threshold limit value.
Health Considerations for Managing Work at High Altitudes
Large numbers of people work at high altitudes, particularly in the cities and villages of the South American Andes and the Tibetan plateau. The majority of these people are highlanders who have lived in the area for many years and perhaps several generations. Much of the work is agricultural in nature—for example, tending domesticated animals.
However, the focus of this article is different. Recently there has been a large increase in commercial activities at altitudes of 3,500 to 6,000 m. Examples include mines in Chile and Peru at altitudes of around 4,500 m. Some of these mines are very large, employing over 1,000 workers. Another example is the telescope facility at Mauna Kea, Hawaii, at an altitude of 4,200 m.
Traditionally, the high mines in the South American Andes, some of which date back to the Spanish colonial period, have been worked by indigenous people who have been at high altitude for generations. Recently however, increasing use is being made of workers from sea level. There are several reasons for this change. One is that there are not enough people in these remote areas to operate the mines. An equally important reason is that as the mines become increasingly automated, skilled people are required to operate large digging machines, loaders and trucks, and local people may not have the necessary skills. A third reason is the economics of developing these mines. Whereas previously whole towns were set up in the vicinity of the mine to accommodate the workers’ families, and necessary ancillary facilities such as schools and hospitals, it is now seen to be preferable to have the families live at sea level, and have the workers commute to the mines. This is not purely an economic issue. The quality of life at an altitude of 4,500 m is less than at lower altitudes (e.g., children grow more slowly). Therefore the decision to have the families remain at sea level while the workers commute to high altitude has a sound socio-economic basis.
The situation where a workforce moves from sea level to altitudes of approximately 4,500 m raises many medical issues, many of which are poorly understood at the present time. Certainly most people who travel from sea level to an altitude of 4,500 m develop some symptoms of acute mountain sickness initially. Tolerance to the altitude often improves after the first two or three days. However, the severe hypoxia of these altitudes has a number of deleterious effects on the body. Maximal work capacity is decreased, and people fatigue more rapidly. Mental efficiency is reduced and many people find it is much more difficult to concentrate. Sleep quality is often poor, with frequent arousals and periodic breathing (the breathing waxes and wanes three or four times every minute) with the result that that the arterial PO2 falls to low levels following the periods of apnoea or reduced breathing.
Tolerance to high altitude varies greatly between individuals, and it is often very difficult to predict who is going to be intolerant of high altitude. A substantial number of people who would like to work at an altitude of 4,500 m find that they are unable to do so, or that the quality life is so poor that they refuse to remain at that altitude. Topics such as the selection of workers who are likely to tolerate high altitude, and the scheduling of their work between high altitude and the period with their families at sea level, are relatively new and not well understood.
Pre-employment Examination
In addition to the usual type of pre-employment examination, special attention should be given to the cardio-pulmonary system, because working at high altitude makes great demands on the respiratory and cardiovascular systems. Medical conditions such as early chronic obstructive pulmonary disease and asthma will be much more disabling at high altitude because of the high levels of ventilation, and should be specifically looked for. A heavy cigarette smoker with symptoms of early bronchitis is likely to have difficulty tolerating high altitude. Forced spirometry should be measured in addition to the usual chest examination including chest radiograph. If possible, an exercise test should be carried out because any exercise intolerance will be exaggerated at high altitude.
The cardiovascular system should be carefully examined, including an exercise electrocardiogram if that is feasible. Blood counts should be made to exclude workers with unusual degrees of anaemia or polycythaemia.
Living at high altitude increases the psychological stress in many people, and a careful history should be taken to exclude prospective workers with previous behavioural problems. Many modern mines at high altitude are dry (no alcohol permitted). Gastro-intestinal symptoms are common in some people at high altitude, and workers who have a history of dyspepsia may do poorly.
Selection of Workers to Tolerate High Altitude
In addition to excluding workers with lung or heart disease who are likely to do poorly at high altitude, it would be very valuable if tests could be carried out to determine who is likely to tolerate altitude well. Unfortunately little is known at the present time about predictors of tolerance to high altitude, though considerable work is being done on this at the present time.
The best predictor of tolerance to high altitude is probably previous experience at high altitude. If someone has been able to work at an altitude of 4,500 m for several weeks without appreciable problems, it is very likely that he or she will be able to do this again. By the same token, somebody who tried to work at high altitude and found that he or she could not tolerate it, is very likely to have the same problem next time. Therefore in selecting workers, a great deal of emphasis should be placed on successful previous employment at high altitude. However, clearly this criterion cannot be used for all workers because otherwise no new people would enter the high-altitude working pool.
Another possible predictor is the magnitude of the ventilatory response to hypoxia. This can be measured at sea level by giving the prospective worker a low concentration of oxygen to breathe and measuring the increase in ventilation. There is some evidence that people who have a relatively weak hypoxic ventilatory response tolerate high altitude poorly. For example, Schoene (1982) showed that 14 high-altitude climbers had significantly higher hypoxic ventilatory responses than ten controls. Further measurements were made on the 1981 American Medical Research Expedition to Everest, where it was shown that the hypoxic ventilatory response measured before and on the Expedition correlated well with performance high on the mountain (Schoene, Lahiri and Hackett 1984). Masuyama, Kimura and Sugita (1986) reported that five climbers who reached 8,000 m in Kanchenjunga had a higher hypoxic ventilatory response than five climbers who did not.
However, this correlation is by no means universal. In a prospective study of 128 climbers going to high altitudes, a measure of hypoxic ventilatory response did not correlate with the height reached, whereas a measurement of maximal oxygen uptake at sea level did correlate (Richalet, Kerome and Bersch 1988). This study also suggested that the heart rate response to acute hypoxia might be a useful predictor of performance at high altitude. There have been other studies showing a poor correlation between hypoxic ventilatory response and performance at extreme altitude (Ward, Milledge and West 1995).
The problem with many of these studies is that the results are chiefly applicable to much higher altitudes than of interest here. Also there are many examples of climbers with moderate values of hypoxic ventilatory response who do well at high altitude. Nevertheless, an abnormally low hypoxic ventilatory response is probably a risk factor for tolerating even medium altitudes such as 4,500 m.
One way of measuring the hypoxic ventilatory response at sea level is to have the subject rebreathe into a bag which is initially filled with 24% oxygen, 7% carbon dioxide, and the balance nitrogen. During rebreathing the PCO2 is monitored and held constant by means of a variable bypass and carbon dioxide absorber. Rebreathing can be continued until the inspired PO2 falls to about 40 mmHg (5.3 kPa). The arterial oxygen saturation is measured continually with a pulse oximeter, and the ventilation plotted against the saturation (Rebuck and Campbell 1974). Another way of measuring the hypoxic ventilatory response is to determine the inspiratory pressure during a brief period of airway occlusion while the subject is breathing a low-oxygen mixture (Whitelaw, Derenne and Milic-Emili 1975).
Another possible predictor of tolerance to high altitude is work capacity during acute hypoxia at sea level. The rationale here is that someone who is not able to tolerate acute hypoxia is more likely to be intolerant of chronic hypoxia. There is little evidence for or against this hypothesis. Soviet physiologists used tolerance to acute hypoxia as one of the criteria for selection of climbers for their successful 1982 Everest expedition (Gazenko 1987). On the other hand, the changes that occur with acclimatization are so profound that it would not be surprising if exercise performance during acute hypoxia were poorly correlated with the ability to work during chronic hypoxia.
Another possible predictor is the increase in pulmonary artery pressure during acute hypoxia at sea level. This can be measured non-invasively in many people by Doppler ultrasound. The main rationale for this test is the known correlation between the development of high-altitude pulmonary oedema and the degree of hypoxic pulmonary vasoconstriction (Ward, Milledge and West 1995). However, since high-altitude pulmonary oedema is uncommon in people working at an altitude of 4,500 m, the practical value of this test is questionable.
The only way to determine whether these tests for the selection of workers have practical value is a prospective study where the results of the tests done at sea level are correlated with subsequent assessment of tolerance to high altitude. This raises the question of how high-altitude tolerance will be measured. The usual way of doing this is by questionnaires such as the Lake Louise questionnaire (Hackett and Oelz 1992). However, questionnaires may be unreliable in this population because workers perceive that if they admit to altitude intolerance, they might lose their jobs. It is true that there are objective measures of altitude intolerance such as quitting work, rales in the lungs as indications of subclinical pulmonary oedema, and mild ataxia as an indication of subclinical high-altitude cerebral oedema. However, these features will be seen only in people with severe altitude intolerance, and a prospective study based solely on such measurements would be very insensitive.
It should be emphasized that the value of these possible tests for determining tolerance to working at high altitude has not been established. However, the economic implications of taking on a substantial number of workers who are unable to perform satisfactorily at high altitude are such that it would be very valuable to have useful predictors. Studies are presently underway to determine whether some of these predictors are valuable and feasible. Measurements such as the hypoxic ventilatory response to hypoxia, and work capacity during acute hypoxia at sea level, are not particularly difficult. However, they need to be done by a professional laboratory, and the cost of these investigations can be justified only if the predictive value of the measurements is substantial.
Scheduling between High Altitude and Sea Level
Again, this article is addressed to the specific problems which occur when commercial activities such as mines at altitudes of about 4,500 m employ workers who commute from sea level where their families live. Scheduling is obviously not an issue where people live permanently at high altitude.
Designing the optimal schedule for moving between high altitude and sea level is a challenging problem, and as yet there is little scientific basis for the schedules that have been employed so far. These have been based mainly on social factors such as how long the workers are willing to spend at high altitude before seeing their families again.
The main medical rationale for spending several days at a time at high altitude is the advantage gained from acclimatization. Many people who develop symptoms of acute mountain sickness after going to high altitude feel much better after two to four days. Therefore rapid acclimatization is occurring over this period. In addition it is known that the ventilatory response to hypoxia takes seven to ten days to reach a steady state (Lahiri 1972; Dempsey and Forster 1982). This increase in ventilation is one of the most important features of the acclimatization process, and therefore it is reasonable to recommend that the working period at high altitude be at least ten days.
Other features of high-altitude acclimatization probably take much longer to develop. One example is polycythaemia, which takes several weeks to reach a steady state. However, it should be added that the physiological value of polycythaemia is much less certain than was thought at one time. Indeed, Winslow and Monge (1987) have shown that the severe degrees of polycythaemia which are sometimes seen in permanent dwellers at altitudes of about 4,500 m are counterproductive in that work capacity can sometimes be increased if the haematocrit is lowered by removing blood over several weeks.
Another important issue is the rate of deacclimatization. Ideally the workers should not lose all the acclimatization that they have developed at high altitude during their period with their families at sea level. Unfortunately, there has been little work on the rate of deacclimatization, although some measurements suggest that the rate of change of the ventilatory response during deacclimatization is slower than during acclimatization (Lahiri 1972).
Another practical issue is the time required to move workers from sea level to high altitude and back again. In a new mine at Collahuasi in north Chile, it takes only a few hours to reach the mine by bus from the coastal town of Iquique, where most of the families are expected to live. However, if the worker resides in Santiago, the trip could take over a day. Under these circumstances, a short working period of three or four days at high altitude would clearly be inefficient because of the time wasted in travelling.
Social factors also play a critical role in any scheduling that involves time away from the family. Even if there are medical and physiological reasons why an acclimatization period of 14 days is optimal, the fact that the workers are unwilling to leave their families for more than seven or ten days may be an overriding factor. Experience so far shows that a schedule of seven days at high altitude followed by seven days at sea level, or ten days at high altitude followed by the same period at sea level are probably the most acceptable schedules.
Note that with this type of schedule, the worker never fully acclimatizes to high altitude, nor fully deacclimatizes while at sea level. He therefore spends his time oscillating between the two extremes, never receiving the full benefit of either state. In addition, some workers complain of extreme tiredness when they return to sea level, and spend the first two or three days recovering. Possibly this is related to the poor quality of sleep which is often a feature of living at high altitude. These problems highlight our ignorance of the factors that determine the best schedules, and more work is clearly needed in this area.
Whatever schedule is used, it is highly advantageous if the workers can sleep at a lower altitude than the workplace. Naturally whether this is feasible depends on the topography of the region. A lower altitude for sleeping is not feasible if it takes several hours to reach it because this cuts too much off the working day. However, if there is a location several hundred metres lower which can be reached within, say, one hour, setting up sleeping quarters at this lower altitude will improve sleep quality, workers’ comfort and sense of well-being, and productivity.
Oxygen Enrichment of Room Air to Reduce the Hypoxia of High Altitude
The deleterious effects of high altitude are caused by the low partial pressure of oxygen in the air. In turn, this results from the fact that while the oxygen concentration is the same as at sea level, the barometric pressure is low. Unfortunately there is little that can be done at high altitude to counter this “climatic aggression”, as it was dubbed by Carlos Monge, the father of high-altitude medicine in Peru (Monge 1948).
One possibility is to increase the barometric pressure in a small area, and this is the principle of the Gamow bag, which is sometimes used for the emergency treatment of mountain sickness. However, pressurizing large spaces such as rooms is difficult from a technical point of view, and there are also medical problems associated with entering and leaving a room with increased pressure. An example is middle ear discomfort if the Eustachian tube is blocked.
The alternative is to raise the oxygen concentration in some parts of the work facility, and this is a relatively new development that shows great promise (West 1995). As pointed out earlier, even after a period of acclimatization of seven to ten days at an altitude of 4,500 m, severe hypoxia continues to reduce work capacity, mental efficiency and sleep quality. It would therefore be highly advantageous to reduce the degree of hypoxia in some parts of the work facility if that were feasible.
This can be done by adding oxygen to the normal air ventilation of some rooms. The value of relatively minor degrees of oxygen enrichment of the room air is remarkable. It has been shown that every 1% increase in oxygen concentration (for example from 21 to 22%) reduces the equivalent altitude by 300 m. The equivalent altitude is that which has the same inspired PO2 during air breathing as in the oxygen-enriched room. Thus at an altitude of 4,500 m, raising the oxygen concentration of a room from 21 to 26% would reduce the equivalent altitude by 1,500 m. The result would be an equivalent altitude of 3,000 m, which is easily tolerated. The oxygen would be added to the normal room ventilation and therefore would be part of the air conditioning. We all expect that a room will provide a comfortable temperature and humidity. Control of the oxygen concentration can be regarded as a further logical step in humanity’s control of our environment.
Oxygen enrichment has become feasible because of the introduction of relatively inexpensive equipment for providing large quantities of nearly pure oxygen. The most promising is the oxygen concentrator that uses a molecular sieve. Such a device preferentially adsorbs nitrogen and thus produces an oxygen-enriched gas from air. It is difficult to produce pure oxygen with this type of concentrator, but large amounts of 90% oxygen in nitrogen are readily available, and these are just as useful for this application. These devices can work continuously. In practice, two molecular sieves are used in an alternating fashion, and one is purged while the other is actively adsorbing nitrogen. The only requirement is electrical power, which is normally in abundant supply at a modern mine. As a rough indication of the cost of oxygen enrichment, a small commercial device can be bought off the shelf, and this produces 300 litres per hour of 90% oxygen. It was developed to produce oxygen for treating patients with lung disease in their homes. The device has a power requirement of 350 watts and the initial cost is about US$2,000. Such a machine is sufficient to raise the oxygen concentration in a room by 3% for one person at a minimal though acceptable level of room ventilation. Very large oxygen concentrators are also available, and they are used in the paper pulp industry. It is also possible that liquid oxygen might be economical under some circumstances.
There are several areas in a mine, for example, where oxygen enrichment might be considered. One would be the director’s office or conference room, where important decisions are being made. For example, if there is a crisis in the mine such as a serious accident, such a facility would probably result in clearer thinking than the normal hypoxic environment. There is good evidence that an altitude of 4,500 m impairs brain function (Ward, Milledge and West 1995). Another place where oxygen enrichment would be beneficial is a laboratory where quality control measurements are being carried out. A further possibility is oxygen enrichment of sleeping quarters to improve sleep quality. Double blind trials of the effectiveness of oxygen enrichment at altitudes of about 4,500 m would be easy to design and should be carried out as soon as possible.
Possible complications of oxygen enrichment should be considered. Increased fire hazard is one issue that has been raised. However, increasing the oxygen concentration by 5% at an altitude of 4,500 m produces an atmosphere which has a lower flammability than air at sea level (West 1996). It should be borne in mind that although oxygen enrichment increases the PO2, this is still much lower than the sea-level value. Flammability of an atmosphere depends on two variables (Roth 1964):
- the partial pressure of oxygen, which is much lower in the enriched air at high altitude than at sea level
- the quenching effect of the inert components (i.e., nitrogen) of the atmosphere.
This quenching is slightly reduced at high altitude, but the net effect is still a lower flammability. Pure or nearly pure oxygen is dangerous, of course, and the normal precautions should be taken in piping the oxygen from the oxygen concentrator to the ventilation ducting.
Loss of acclimatization to high altitude is sometimes cited as a disadvantage of oxygen enrichment. However, there is no basic difference between entering a room with an oxygen-enriched atmosphere, and descending to a lower altitude. Everybody would sleep at a lower altitude if they could, and therefore this is hardly an argument against using oxygen enrichment. It is true that frequent exposure to a lower altitude will result in less acclimatization to the higher altitude, other things being equal. However, the ultimate objective is effective working at the high altitude of the mine, and this can presumably be enhanced using oxygen enrichment.
It is sometimes suggested that altering the atmosphere in this way might increase the legal liability of the facility if some kind of hypoxia-related illness developed. Actually, the opposite view seems more reasonable. It is possible that a worker who develops, say, a myocardial infarction while working at high altitude could claim that the altitude was a contributing factor. Any procedure which reduces the hypoxic stress makes altitude-induced illnesses less likely.
Emergency Treatment
The various types of high-altitude sickness, including acute mountain sickness, high-altitude pulmonary oedema and high-altitude cerebral oedema, were discussed earlier in this chapter. Little needs to be added in the context of work at high altitude.
Anyone who develops a high-altitude illness should be allowed to rest. This may be sufficient for conditions such as acute mountain sickness. Oxygen should be given by mask if this is available. However, if the patient does not improve, or deteriorates, descent is by far the best treatment. Usually this is easily done in a large commercial facility, because transportation is always available. All the high-altitude-related illnesses usually respond rapidly to removal to lower altitude.
There may be a place in a commercial facility for a small pressurized container in which the patient can be placed, and the equivalent altitude reduced by pumping in air. In the field, this is commonly done using a strong bag. One design is known as the Gamow bag, after its inventor. However, the main advantage of the bag is its portability, and since this feature is not really essential in a commercial facility, it would probably be better to use a larger, rigid tank. This should be big enough for an attendant to be inside the facility with the patient. Of course adequate ventilation of such a container is essential. Interestingly, there is anecdotal evidence that raising the atmospheric pressure in this way is sometimes more efficacious in the treatment of high-altitude illness than giving the patient a high concentration of oxygen. It is not clear why this should be so.
Acute mountain sickness
This is usually self-limiting and the patient feels much better after a day or two. The incidence of acute mountain sickness can be reduced by taking acetazolamide (Diamox), one or two 250 mg tablets per day. These can be started before reaching high altitude or can be taken when symptoms develop. Even people with mild symptoms find that half a tablet at night often improves the quality of sleep. Aspirin or paracetamol is useful for headache. Severe acute mountain sickness can be treated with dexamethasone, 8 mg initially, followed by 4 mg every six hours. However, descent is by far the best treatment if the condition is severe.
High-altitude pulmonary oedema
This is a potentially serious complication of mountain sickness and must be treated. Again the best therapy is descent. While awaiting evacuation, or if evacuation is not possible, give oxygen or place in a high-pressure chamber. Nifedipine (a calcium channel blocker) should be given. The dose is 10 mg sublingually followed by 20 mg slow release. This results in a fall in pulmonary artery pressure and is often very effective. However, the patient should be taken down to a lower altitude.
High-altitude cerebral oedema
This is potentially a very serious complication and is an indication for immediate descent. While awaiting evacuation, or if evacuation is not possible, give oxygen or place in an increased pressure environment. Dexamethasone should be given, 8 mg initially, followed by 4 mg every six hours.
As indicated earlier, people who develop severe acute mountain sickness, high-altitude pulmonary oedema or high-altitude cerebral oedema are likely to have a recurrence if they return to high altitude. Therefore if a worker develops any of these conditions, attempts should be made to find employment at a lower altitude.
Physiological Effects of Reduced Barometric Pressure
The major effects of high altitude on humans relate to the changes in barometric pressure (PB) and its consequential changes in the ambient pressure of oxygen (O2). Barometric pressure decreases with increasing altitude in a logarithmic fashion and can be estimated by the following equation:
![]()
where a = altitude, expressed in metres. In addition, the relationship of barometric pressure to altitude is influenced by other factors such as distance from the equator and season. West and Lahiri (1984) found that direct measurements of barometric pressure near the equator and at the summit of Mt. Everest (8,848 m) were greater than predictions based on the International Civil Aviation Organization Standard Atmosphere. Weather and temperature also affect the relationship between barometric pressure and altitude to the extent that a low-pressure weather system can reduce pressure, making sojourners to high altitude “physiologically higher”. Since the inspired partial pressure of oxygen (PO2) remains constant at approximately 20.93% of barometric pressure, the most important determinant of inspired PO2 at any altitude is the barometric pressure. Thus, inspired oxygen decreases with increasing altitude due to decreased barometric pressure, as shown in figure 1.
Figure 1. Effects of altitude on barometric pressure and inspired PO2
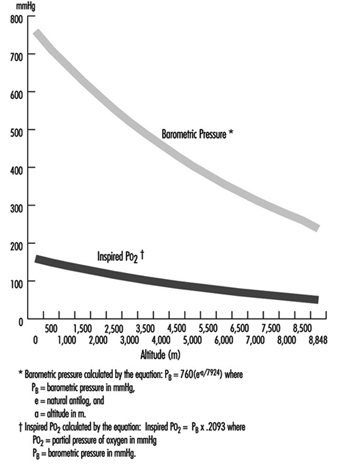
Temperature and ultraviolet radiation also change at high altitudes. Temperature decreases with increasing altitude at a rate of approximately 6.5 °C per 1,000 m. Ultraviolet radiation increases approximately 4% per 300 m due to decreased cloudiness, dust, and water vapour. In addition, as much as 75% of ultraviolet radiation can be reflected back by snow, further increasing exposure at high altitude. Survival in high altitude environments is dependent on adaptation to and/or protection from each of these elements.
Acclimatization
While rapid ascent to high altitudes often results in death, slow ascent by mountaineers can be successful when accompanied by compensatory physiological adaptation measures. Acclimatization to high altitudes is geared towards maintaining an adequate supply of oxygen to meet metabolic demands despite the decreasing inspired PO2. In order to achieve this goal, changes occur in all organ systems involved with oxygen uptake into the body, distribution of O2 to the necessary organs, and O2 unloading to the tissues.
Discussion of oxygen uptake and distribution requires understanding the determinants of oxygen content in the blood. As air enters the alveolus, the inspired PO2 decreases to a new level (called the alveolar PO2) because of two factors: increased partial pressure of water vapour from humidification of inspired air, and increased partial pressure of carbon dioxide (PCO2) from CO2 excretion. From the alveolus, oxygen diffuses across the alveolar capillary membrane into the blood as a result of a gradient between alveolar PO2 and blood PO2. The majority of oxygen found in blood is bound to haemoglobin (oxyhaemoglobin). Thus, oxygen content is directly related to both the haemoglobin concentration in the blood and the percentage of O2 binding sites on haemoglobin that are saturated with oxygen (oxyhaemoglobin saturation). Therefore, understanding the relationship between arterial PO2 and oxyhaemoglobin saturation is essential for understanding the determinants of oxygen content in the blood. Figure 2 illustrates the oxyhaemoglobin dissociation curve. With increasing altitude, inspired PO2 decreases and, therefore, arterial PO2 and oxyhaemoglobin saturation decreases. In normal subjects, altitudes greater than 3,000 m are associated with sufficiently decreased arterial PO2 that oxyhaemoglobin saturation falls below 90%, on the steep portion of the oxyhaemoglobin dissociation curve. Further increases in altitude will predictably result in significant desaturation in the absence of compensatory mechanisms.
Figure 2. Oxyhaemoglobin dissociation curve

The ventilatory adaptations that occur in high-altitude environments protect the arterial partial pressure of oxygen against the effects of decreasing ambient oxygen levels, and can be divided into acute, subacute and chronic changes. Acute ascent to high altitude results in a fall in the inspired PO2 which in turn leads to a decrease in the arterial PO2 (hypoxia). In order to minimize the effects of decreased inspired PO2 on arterial oxyhaemoglobin saturation, the hypoxia that occurs at high altitude triggers an increase in ventilation, mediated through the carotid body (hypoxic ventilatory response–HVR). Hyperventilation increases carbon dioxide excretion and subsequently the arterial and then the alveolar partial pressure of carbon dioxide (PCO2) falls. The fall in alveolar PCO2 allows alveolar PO2 to rise, and consequently, arterial PO2 and arterial O2 content increases. However, the increased carbon dioxide excretion also causes a decrease in blood hydrogen ion concentration ([H+]) leading to the development of alkalosis. The ensuing alkalosis inhibits the hypoxic ventilatory response. Thus, on acute ascent to high altitude there is an abrupt increase in ventilation that is modulated by the development of an alkalosis in the blood.
Over the next several days at high altitude, further changes in ventilation occur, commonly referred to as ventilatory acclimatization. Ventilation continues to increase over the next several weeks. This further increase in ventilation occurs as the kidney compensates for the acute alkalosis by excretion of bicarbonate ions, with a resultant rise in blood [H+]. It was initially believed that renal compensation for the alkalosis removed the inhibitory influence of alkalosis on the hypoxic ventilatory response, thereby allowing the full potential of the HVR to be reached. However, measurements of blood pH revealed that the alkalosis persists despite the increase in ventilation. Other postulated mechanisms include: (1) cerebrospinal fluid (CSF) pH surrounding the respiratory control centre in the medulla may have returned to normal despite the persistent serum alkalosis; (2) increased sensitivity of the carotid body to hypoxia; (3) increased response of the respiratory controller to CO2. Once ventilatory acclimatization has occurred, both hyperventilation and the increased HVR persist for several days after return to lower altitudes, despite resolution of hypoxia.
Further ventilatory changes occur after several years of living at high altitude. Measurements in high-altitude natives have shown a decreased HVR when compared to values obtained in acclimatized individuals, although not to levels seen in subjects at sea level. The mechanism for the decreased HVR is unknown, but may be related to hypertrophy of the carotid body and/or development of other adaptive mechanisms for preserving tissue oxygenation such as: increased capillary density; increased gas exchange capacity of the tissues; increased number and density of mitochondria; or increased vital capacity.
In addition to its effect on ventilation, hypoxia also induces constriction of the vascular smooth muscle in the pulmonary arteries (hypoxic vasoconstriction). The ensuing increase in pulmonary vascular resistance and pulmonary artery pressure redirects blood flow away from poorly ventilated alveoli with low alveolar PO2 and towards better ventilated alveoli. In this manner, pulmonary arterial perfusion is matched to lung units that are well ventilated, providing another mechanism for preserving arterial PO2.
Oxygen delivery to the tissues is further enhanced by adaptations in the cardiovascular and haematological systems. On initial ascent to high altitude, heart rate increases, resulting in an increase in cardiac output. Over several days, cardiac output falls due to decreased plasma volume, caused by an increased water loss that occurs at high altitudes. With more time, increased erythropoietin production leads to increased haemoglobin concentration, providing the blood with increased oxygen-carrying capacity. In addition to increasing levels of haemoglobin, changes in the avidity of oxygen binding to haemoglobin may also help maintain tissue oxygenation. A shift of the oxyhaemoglobin dissociation curve to the right may be expected because it would favour release of oxygen to the tissues. However, data obtained from the summit of Mt. Everest and from hypobaric chamber experiments simulating the summit suggest that the curve is shifted to the left (West and Lahiri 1984; West and Wagner 1980; West et al. 1983). Although a left shift would make oxygen unloading to the tissues more difficult, it may be advantageous at extreme altitudes because it would facilitate oxygen uptake in the lungs despite markedly reduced inspired PO2 (43 mmHg on the summit of Mt. Everest versus 149 mmHg at sea level).
The last link in the chain of oxygen supply to the tissues is cellular uptake and utilization of O2. Theoretically, there are two potential adaptations that can occur. First, minimization of the distance that oxygen has to travel on diffusion out of the blood vessel and into the intracellular site responsible for oxidative metabolism, the mitochondria. Second, biochemical alterations can occur that improve mitochondrial function. Minimization of diffusion distance has been suggested by studies that show either increased capillary density or increased mitochondrial density in muscle tissue. It is unclear whether these changes reflect either recruitment or development of capillaries and mitochondria, or are an artefact due to muscle atrophy. In either case, the distance between the capillaries and the mitochondria would be decreased, thereby facilitating oxygen diffusion. Biochemical alterations that may improve mitochondrial function include increased myoglobin levels. Myoglobin is an intracellular protein that binds oxygen at low tissue PO2 levels and facilitates oxygen diffusion into the mitochondria. Myoglobin concentration increases with training and correlates with muscle cell aerobic capacity. Although these adaptations are theoretically beneficial, conclusive evidence is lacking.
Early accounts of high altitude explorers describe changes in cerebral function. Decreased motor, sensory and cognitive abilities, including decreased ability to learn new tasks and difficulty expressing information verbally, have all been described. These deficits may lead to poor judgement and to irritability, further compounding the problems encountered in high-altitude environments. On return to sea level, these deficits improve with a variable time course; reports have indicated impaired memory and concentration lasting from days to months, and decreased finger-tapping speed for one year (Hornbein et al. 1989). Individuals with greater HVR are more susceptible to long-lasting deficits, possibly because the benefit of hyperventilation on arterial oxyhaemoglobin saturation may be offset by hypocapnia (decreased PCO2 in the blood), which causes constriction of the cerebral blood vessels leading to decreased cerebral blood flow.
The preceding discussion has been limited to resting conditions; exercise provides an additional stress as oxygen demand and consumption increases. The fall in ambient oxygen at high altitude causes a fall in maximal oxygen uptake and, therefore, maximal exercise. In addition, the decreased inspired PO2 at high altitudes severely impairs oxygen diffusion into the blood. This is illustrated in figure 3, which plots the time course of oxygen diffusion into the alveolar capillaries. At sea level, there is excess time for equilibration of end-capillary PO2 to alveolar PO2, whereas at the summit of Mt. Everest, full equilibration is not realized. This difference is due to the decreased ambient oxygen level at high altitudes leading to a decreased diffusion gradient between alveolar and venous PO2. With exercise, cardiac output and blood flow increase, thereby reducing transit time of blood cells across the alveolar capillary, further exacerbating the problem. From this discussion, it becomes apparent that the left shift in the O2 and haemoglobin dissociation curve with altitude is necessary as compensation for the decreased diffusion gradient for oxygen in the alveolus.
Figure 3. The calculated time course of oxygen tension in the alveolar capillary
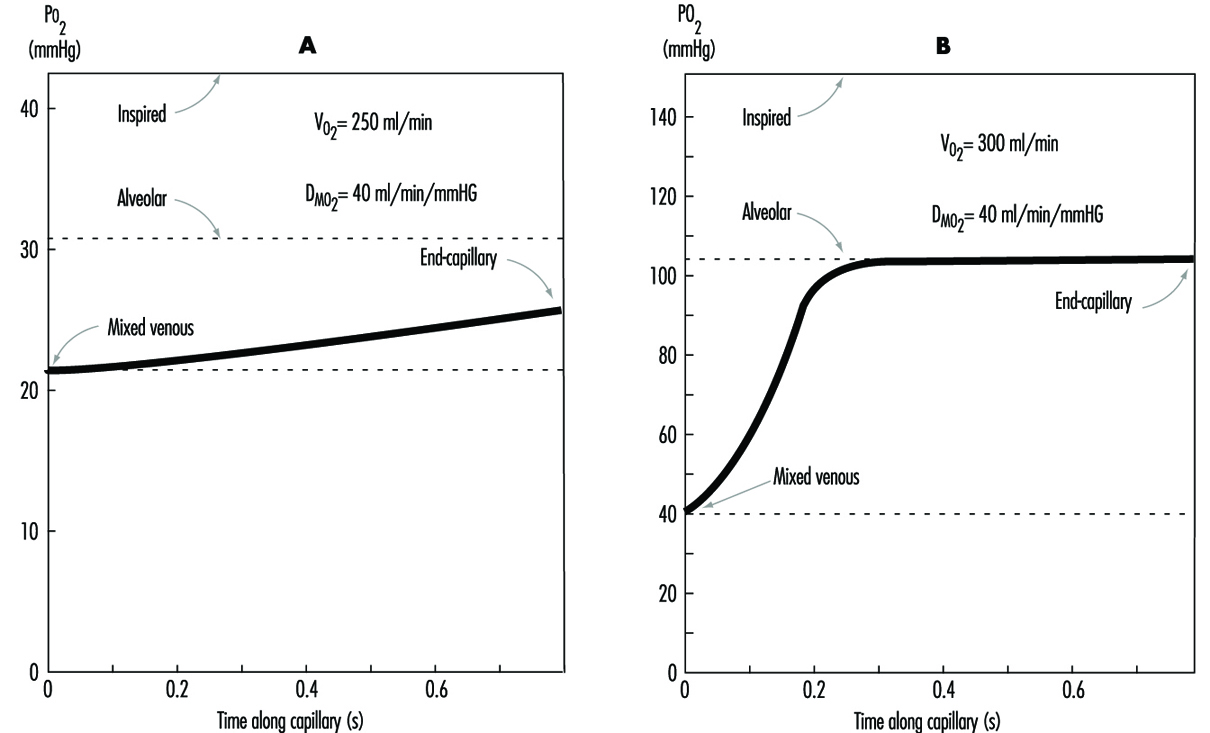
Disturbed sleep is common among sojourners at high altitude. Periodic (Cheyne-Stokes) breathing is universal and characterized by periods of rapid respiratory rate (hyperpnoea) alternating with periods of absent respirations (apnoea) leading to hypoxia. Periodic breathing tends to be more pronounced in individuals with the greatest hypoxic ventilatory sensitivity. Accordingly, sojourners with lower HVR have less severe periodic breathing. However, sustained periods of hypoventilation are then seen, corresponding with sustained decreases in oxyhaemoglobin saturation. The mechanism for periodic breathing probably relates to increased HVR causing increased ventilation in response to hypoxia. The increased ventilation leads to increased blood pH (alkalosis), which in turn suppresses ventilation. As acclimatization progresses, periodic breathing improves. Treatment with acetazolamide reduces periodic breathing and improves arterial oxyhaemoglobin saturation during sleep. Caution should be used with medications and alcohol that suppress ventilation, as they may exacerbate the hypoxia seen during sleep.
Pathophysiological Effects of Reduced Barometric Pressure
The complexity of human physiological adaptation to high altitude provides numerous potential maladaptive responses. Although each syndrome will be described separately, there is considerable overlap between them. Illnesses such as acute hypoxia, acute mountain sickness, high-altitude pulmonary oedema, and high-altitude cerebral oedema most likely represent a spectrum of abnormalities that share a similar pathophysiology.
Hypoxia
Hypoxia occurs with ascent to high altitudes because of the decreased barometric pressure and the resultant decrease in ambient oxygen. With rapid ascent, hypoxia occurs acutely, and the body does not have time to adjust. Mountaineers have generally been protected from the effects of acute hypoxia because of the time that elapses, and hence the acclimatization that occurs, during the climb. Acute hypoxia is problematic for both aviators and rescue personnel in high-altitude environments. Acute oxyhaemoglobin desaturation to values less than 40 to 60% leads to loss of consciousness. With less severe desaturation, individuals note headache, confusion, drowsiness and loss of coordination. Hypoxia also induces a state of euphoria which Tissandier, during his balloon flight in 1875, described as experiencing “inner joy”. With more severe desaturation, death occurs. Acute hypoxia responds rapidly and completely to either administration of oxygen or descent.
Acute mountain sickness
Acute mountain sickness (AMS) is the most common disorder in high-altitude environments and afflicts up to two-thirds of sojourners. The incidence of acute mountain sickness is dependent on multiple factors, including rate of ascent, length of exposure, degree of activity, and individual susceptibility. Identification of affected individuals is important in order to prevent progression to pulmonary or cerebral oedema. Identification of acute mountain sickness is made through recognition of characteristic signs and symptoms occurring in the appropriate setting. Most often, acute mountain sickness occurs within a few hours of a rapid ascent to altitudes greater than 2,500 m. The most common symptoms include headache that is more pronounced at night, loss of appetite that may be accompanied by nausea and vomiting, disturbed sleep, and fatigue. Individuals with AMS often complain of shortness of breath, cough and neurological symptoms such as memory deficits and auditory or visual disturbances. Findings on physical exam may be lacking, although fluid retention may be an early sign. The pathogenesis of acute mountain illness may relate to relative hypoventilation that would increase cerebral blood flow and intracranial pressure by increasing arterial PCO2 and decreasing arterial PO2. This mechanism may explain why persons with greater HVR are less likely to develop acute mountain sickness. The mechanism for fluid retention is not well understood, but may be related to abnormal plasma levels for proteins and/or hormones that regulate renal excretion of water; these regulators may respond to the increased activity of the sympathetic nervous system noted in patients with acute mountain sickness. The accumulation of water may in turn lead to the development of oedema or swelling of the interstitial spaces in the lungs. More severe cases may go on to develop pulmonary or cerebral oedema.
Prevention of acute mountain sickness can be accomplished through slow, graded ascent, allowing adequate time for acclimatization. This may be especially important for those individuals with greater susceptibility or a prior history of acute mountain sickness. In addition, administration of acetazolamide before or during ascent may help prevent and ameliorate symptoms of acute mountain sickness. Acetazolamide inhibits the action of carbonic anhydrase in the kidneys and leads to increased excretion of bicarbonate ions and water, producing an acidosis in the blood. The acidosis stimulates respiration, leading to increased arterial oxyhaemoglobin saturation and decreased periodic breathing during sleep. Through this mechanism, acetazolamide speeds the natural process of acclimatization.
Treatment of acute mountain sickness can be accomplished most effectively by descent. Further ascent to high altitudes is contra-indicated, as the disease may progress. When descent is not possible, oxygen may be administered. Alternatively, portable lightweight fabric hyperbaric chambers may be brought on expeditions to high-altitude environments. Hyperbaric bags are particularly valuable when oxygen is not available and descent is not possible. Several drugs are available that improve symptoms of acute mountain sickness, including acetazolamide and dexamethasone. The mechanism of action of dexamethasone is unclear, although it may act by decreasing oedema formation.
High-altitude pulmonary oedema
High-altitude pulmonary oedema affects approximately 0.5 to 2.0% of individuals who ascend to altitudes greater than 2,700 m and is the most common cause of death due to illnesses encountered at high altitudes. High-altitude pulmonary oedema develops from 6 to 96 hours after ascent. Risk factors for the development of high-altitude pulmonary oedema are similar to those for acute mountain sickness. Common early signs include symptoms of acute mountain sickness accompanied by decreased exercise tolerance, increased recovery time after exercise, shortness of breath on exertion, and persistent dry cough. As the condition worsens, the patient develops shortness of breath at rest, findings of audible congestion in the lungs, and cyanosis of the nail beds and lips. The pathogenesis of this disorder is uncertain but probably relates to increased microvascular pressure or increased permeability of the microvasculature leading to the development of pulmonary oedema. Although pulmonary hypertension may help explain the pathogenesis, elevation in the pulmonary artery pressure due to hypoxia has been observed in all individuals who ascend to high altitude, including those who do not develop pulmonary oedema. Nevertheless, susceptible individuals may possess uneven hypoxic constriction of the pul-monary arteries, leading to over-perfusion of the microvasculature in localized areas where hypoxic vasoconstriction was absent or diminished. The resulting increase in pressure and shear forces may damage the capillary membrane, leading to oedema formation. This mechanism explains the patchy nature of this disease and its appearance on x-ray examination of the lungs. As with acute mountain sickness, individuals with a lower HVR are more likely to develop high-altitude pulmonary oedema as they have lower oxyhaemoglobin saturations and, therefore, greater hypoxic pulmonary vasoconstriction.
Prevention of high-altitude pulmonary oedema is similar to prevention of acute mountain sickness and includes gradual ascent and use of acetazolamide. Recently, use of the smooth-muscle relaxing agent nifedipine has been shown to be of benefit in preventing disease in individuals with a prior history of high-altitude pulmonary oedema. Additionally, avoidance of exercise may have a preventive role, although it is probably limited to those individuals who already posses a subclinical degree of this disease.
Treatment of high-altitude pulmonary oedema is best accomplished by assisted evacuation to a lower altitude, keeping in mind that the victim needs to limit his or her exertion. After descent, improvement is rapid and additional treatment other than bed rest and oxygen are usually not necessary. When descent is not possible, oxygen therapy may be beneficial. Drug treatment has been attempted with multiple agents, most successfully with the diuretic furosemide and with morphine. Caution must be used with these drugs, as they can lead to dehydration, decreased blood pressure, and respiratory depression. Despite the effectiveness of descent as therapy, mortality remains at approximately 11%. This high mortality rate may reflect failure to diagnose the disease early in its course, or inability to descend coupled with lack of availability of other treatments.
High-altitude cerebral oedema
High-altitude cerebral oedema represents an extreme form of acute mountain sickness that has progressed to include generalized cerebral dysfunction. The incidence of cerebral oedema is unclear because it is difficult to differentiate a severe case of acute mountain sickness from a mild case of cerebral oedema. The pathogenesis of high-altitude cerebral oedema is an extension of the pathogenesis of acute mountain sickness; hypoventilation increases cerebral blood flow and intracranial pressure progressing to cerebral oedema. Early symptoms of cerebral oedema are identical to symptoms of acute mountain sickness. As the disease progresses, additional neurological symptoms are noted, including severe irritability and insomnia, ataxia, hallucinations, paralysis, seizures and eventually coma. Examination of the eyes commonly reveals swelling of the optic disc or papilloedema. Retinal haemorrhages are frequently noted. In addition, many cases of cerebral oedema have concurrent pulmonary oedema.
Treatment of high-altitude cerebral oedema is similar to treatment of other high-altitude disorders, with descent being the preferred therapy. Oxygen should be administered to maintain oxyhaemoglobin saturation greater that 90%. Oedema formation may be decreased with use of corticosteroids such as dexamethasone. Diuretic agents have also been utilized to decrease oedema, with uncertain efficacy. Comatose patients may require additional support with airway management. The response to treatment is variable, with neurological deficits and coma persisting for days to weeks after evacuation to lower altitudes. Preventative measures for cerebral oedema are identical to measures for other high-altitude syndromes.
Retinal haemorrhages
Retinal haemorrhages are extremely common, affecting up to 40% of individuals at 3,700 m and 56% at 5,350 m. Retinal haemorrhages are usually asymptomatic. They are most likely caused by increased retinal blood flow and vascular dilatation due to arterial hypoxia. Retinal haemorrhages are more common in individuals with headaches and can be precipitated by strenuous exercise. Unlike other high-altitude syndromes, retinal haemorrhages are not preventable by acetazolamide or furosemide therapy. Spontaneous resolution is usually seen within two weeks.
Chronic mountain sickness
Chronic mountain sickness (CMS) afflicts residents and long-term inhabitants of high altitude. The first description of chronic mountain sickness reflected Monge’s observations of Andean natives living at altitudes above 4,000 m. Chronic mountain sickness, or Monge’s disease, has since been described in most high-altitude dwellers except Sherpas. Males are more commonly affected than females. Chronic mountain sickness is characterized by plethora, cyanosis and elevated red blood cell mass leading to neurological symptoms that include headache, dizziness, lethargy and impaired memory. Victims of chronic mountain sickness may develop right heart failure, also called cor pulmonale, due to pulmonary hypertension and markedly reduced oxyhaemoglobin saturation. The pathogenesis of chronic mountain sickness is unclear. Measurements from affected individuals have revealed a decreased hypoxic ventilatory response, severe hypoxemia that is exacerbated during sleep, increased haemoglobin concentration and increased pulmonary artery pressure. Although a cause-and-effect relationship seems likely, evidence is lacking and often confusing.
Many symptoms of chronic mountain sickness can be ameliorated by descent to sea level. Relocation to sea level removes the hypoxic stimulus for red blood cell production and pulmonary vasoconstriction. Alternate treatments include: phlebotomy to reduce red blood cell mass, and low-flow oxygen during sleep to improve hypoxia. Therapy with medroxyprogesterone, a respiratory stimulant, has also been found to be effective. In one study, ten weeks of medroxyprogesterone therapy was followed by improved ventilation and hypoxia, and decreased red blood cell counts.
Other conditions
Patients with sickle cell disease are more likely to suffer from painful vaso-occlusive crisis at high altitude. Even moderate altitudes of 1,500 m have been known to precipitate crises, and altitudes of 1,925 m are associated with a 60% risk of crises. Patients with sickle cell disease residing at 3,050 m in Saudi Arabia have twice as many crises as patients residing at sea level. In addition, patients with sickle cell trait may develop splenic infarct syndrome on ascent to high altitude. Likely aetiologies for the increased risk of vaso-occlusive crisis include: dehydration, increased red blood cell count, and immobility. Treatment of vaso-occlusive crisis includes descent to sea level, oxygen and intravenous hydration.
Essentially no data exist describing the risk to pregnant patients on ascent to high altitudes. Although patients residing at high altitude have an increased risk of pregnancy-induced hypertension, no reports of increased foetal demise exist. Severe hypoxia may cause abnormalities in foetal heart rate; however, this occurs only at extreme altitudes or in the presence of high-altitude pulmonary oedema. Therefore, the greatest risk to the pregnant patient may relate to the remoteness of the area rather than to altitude-induced complications.
Ventilatory Acclimatization to High Altitude
People are increasingly working at high altitudes. Mining operations, recreational facilities, modes of transportation, agricultural pursuits and military campaigns are often at high altitude, and all of these require human physical and mental activity. All such activity involves increased requirements for oxygen. A problem is that as one ascends higher and higher above sea level, both the total air pressure (the barometric pressure, PB) and the amount of oxygen in the ambient air (that portion of total pressure due to oxygen, PO2) progressively fall. As a result, the amount of work we can accomplish progressively decreases. These principles affect the workplace. For example, a tunnel in Colorado was found to require 25% more time to complete at an altitude of 11,000 ft than comparable work at sea level, and altitude effects were implicated in the delay. Not only is there increased muscular fatigue, but also, deterioration of mental function. Memory, computation, decision making and judgement all become impaired. Scientists doing calculations at the Mona Loa Observatory at an altitude above 4,000 m on the island of Hawaii have found they require more time to perform their calculations and they make more mistakes than at sea level. Because of the increasing scope, magnitude, variety and distribution of human activities on this planet, more people are working at high altitude, and effects of altitude become an occupational issue.
Fundamentally important to occupational performance at altitude is maintaining the oxygen supply to the tissues. We (and other animals) have defences against low oxygen states (hypoxia). Chief among these is an increase in breathing (ventilation), which begins when the oxygen pressure in the arterial blood (PaO2) decreases (hypoxemia), is present for all altitudes above sea level, is progressive with altitude and is our most effective defence against low oxygen in the environment. The process whereby breathing increases at high altitude is called ventilatory acclimatization. The importance of the process can be seen in figure 1, which shows that the oxygen pressure in the arterial blood is higher in acclimatized subjects than in unacclimatized subjects. Further, the importance of acclimatization in maintaining the arterial oxygen pressure increases progressively with increasing altitude. Indeed, the unacclimatized person is unlikely to survive above an altitude of 20,000 ft, whereas acclimatized persons have been able to climb to the summit of Mount Everest (29,029 ft, 8,848 m) without artificial sources of oxygen.
Figure 1. Ventilatory acclimatization
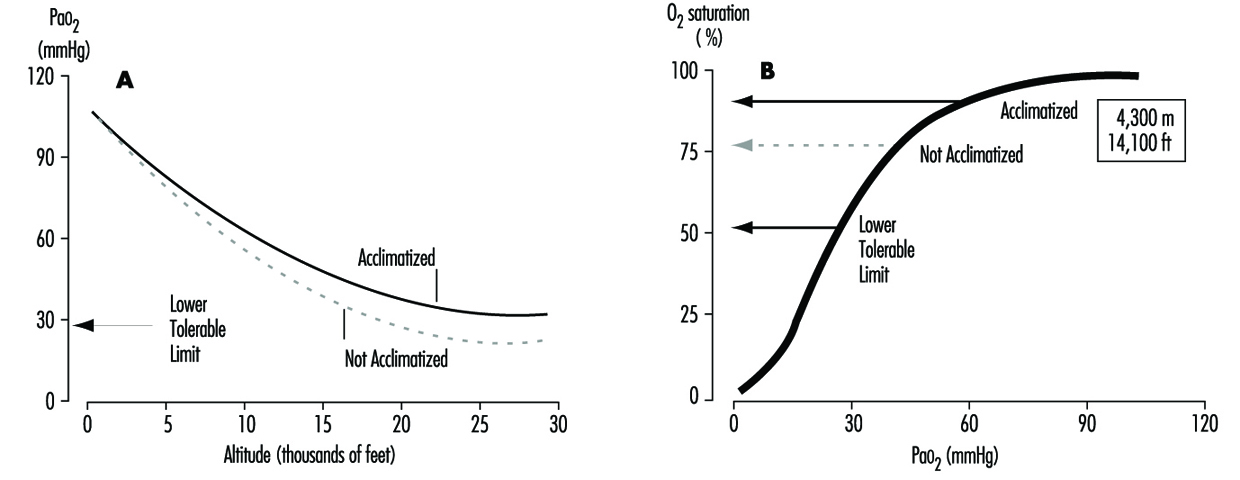
Mechanism
The stimulus for the increase in ventilation at high altitude largely and almost exclusively arises in a tissue which monitors the oxygen pressure in the arterial blood and is contained within an organ called the carotid body, about the size of a pinhead, located at a branch point in each of the two carotid arteries, at the level of the angle of the jaw. When the arterial oxygen pressure falls, nerve-like cells (chemoreceptor cells) in the carotid body sense this decrease and increase their firing rate along the 9th cranial nerve, which carries the impulses directly to the respiratory control centre in the brain stem. When the respiratory centre receives increased numbers of impulses, it stimulates an increase in the frequency and depth of breathing via complex nerve pathways, which activate the diaphragm and the muscles of the chest wall. The result is an increased amount of air ventilated by the lungs, figure 2, which in turn acts to restore the arterial oxygen pressure. If a subject breathes oxygen or air enriched with oxygen, the reverse happens. That is, the chemoreceptor cells decrease their firing rate, which decreases the nerve traffic to the respiratory centre, and breathing decreases. These small organs on each side of the neck are very sensitive to small changes in oxygen pressure in the blood. Also, they are almost entirely responsible for maintaining the body’s oxygen level, for when both of them are damaged or removed, ventilation no longer increases when blood oxygen levels fall. Thus an important factor controlling breathing is the arterial oxygen pressure; a decrease in oxygen level leads to an increase in breathing, and an increase in oxygen level leads to a decrease in breathing. In each case the result is, in effect, the body’s effort to maintain blood oxygen levels constant.
Figure 2. Sequence of events in acclimatization
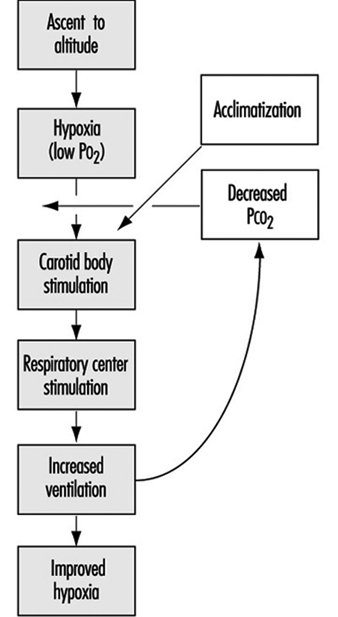
Time course (factors opposing the increase in ventilation at altitude)
Oxygen is required for the sustained production of energy, and when oxygen supply to tissues is reduced (hypoxia), tissue function may become depressed. Of all organs, the brain is most sensitive to lack of oxygen, and, as noted above, centres within the central nervous system are important in the control of breathing. When we breathe a low-oxygen mixture, the initial response is an increase in ventilation, but after 10 minutes or so the increase is blunted to some extent. While the cause for this blunting is not known, its suggested cause is depression of some central neural function related to the ventilation pathway, and has been called hypoxic ventilatory depression. Such depression has been observed shortly after ascent to high altitude. The depression is transient, lasting only a few hours, possibly because there is some tissue adaptation within the central nervous system.
Nevertheless, some increase in ventilation usually begins immediately on going to high altitude, although time is required before maximum ventilation is achieved. On arrival at altitude, increased carotid body activity attempts to increase ventilation, and thereby to raise the arterial oxygen pressure back to the sea level value. However, this presents the body with a dilemma. An increase in breathing causes an increased excretion of carbon dioxide (CO2) in the exhaled air. When CO2 is in body tissues, it creates an acid aqueous solution, and when it is lost in exhaled air, the body fluids, including blood, become more alkaline, thus altering the acid-base balance in the body. The dilemma is that ventilation is regulated not only to keep oxygen pressure constant, but also for acid-base balance. CO2 regulates breathing in the opposite direction from oxygen. Thus when the CO2 pressure (i.e., the degree of acidity somewhere within the respiratory centre) rises, ventilation rises, and when it falls, ventilation falls. On arrival at high altitude, any increase in ventilation caused by the low oxygen environment will lead to a fall in CO2 pressure, which causes alkalosis and acts to oppose the increased ventilation (figure 2). Therefore, the dilemma on arrival is that the body cannot maintain constancy in both oxygen pressure and acid-base balance. Human beings require many hours and even days to regain proper balance.
One method for rebalancing is for the kidneys to increase alkaline bicarbonate excretion in the urine, which compensates for the respiratory loss of acidity, thus helping to restore the body’s acid-base balance toward the sea-level values. The renal excretion of bicarbonate is a relatively slow process. For example, on going from sea level to 4,300 m (14,110 ft), acclimatization requires from seven to ten days (figure 3). This action of the kidneys, which reduces the alkaline inhibition of ventilation, was once thought to be the major reason for the slow increase in ventilation following ascent, but more recent research assigns a dominant role to a progressive increase in the sensitivity of the hypoxic sensing ability of the carotid bodies during the early hours to days following ascent to altitude. This is the interval of ventilatory acclimatization. The acclimatization process allows, in effect, ventilation to rise in response to low arterial oxygen pressure even though the CO2 pressure is falling. As the ventilation rises and CO2 pressure falls with acclimatization at altitude, there is a resultant and concomitant rise in oxygen pressure within the lung alveoli and the arterial blood.
Figure 3. Time course of ventilatory acclimatization for sea level subjects taken to 4,300 m altitude
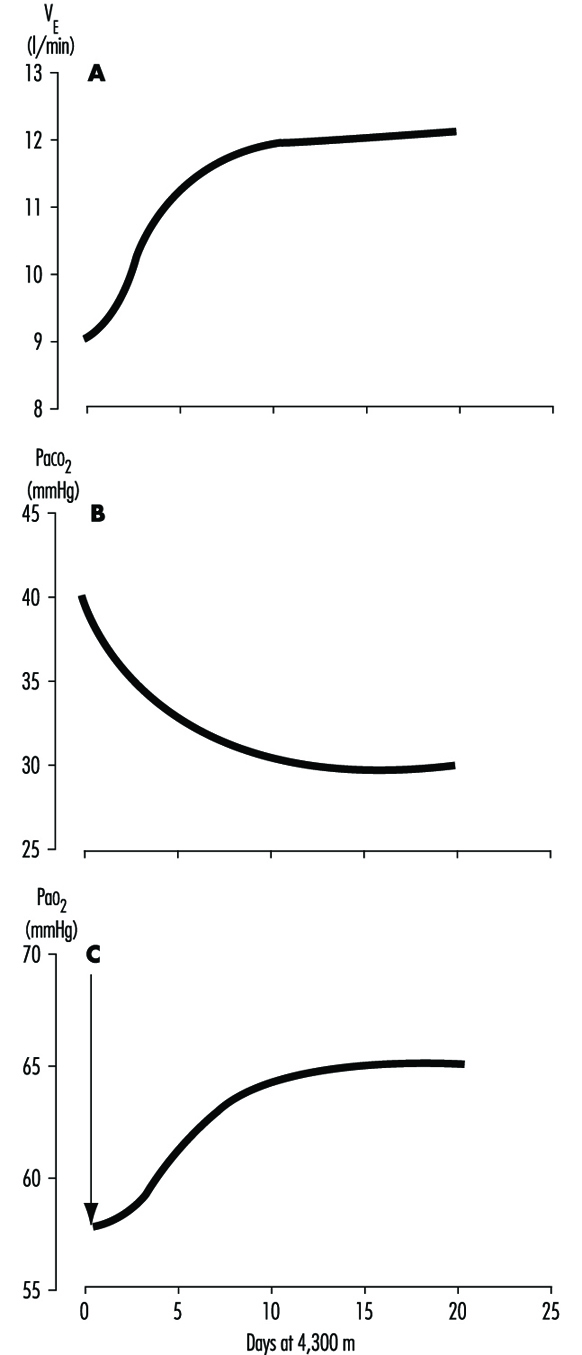
Because of the possibility of transient hypoxic ventilatory depression at altitude, and because acclimatization is a process which begins only upon entering a low oxygen environment, the minimal arterial oxygen pressure occurs upon arrival at altitude. Thereafter, the arterial oxygen pressure rises relatively rapidly for the initial days and thereafter increases more slowly, as in figure 3. Because the hypoxia is worse soon after arrival, the lethargy and symptoms which accompany altitude exposure are also worse during the first hours and days. With acclimatization, a restored sense of well-being usually develops.
The time required for acclimatization increases with increasing altitude, consistent with the concept that greater increase in ventilation and acid-base adjustments require longer intervals for renal compensation to occur. Thus while acclimatization may require three to five days for a sea-level native to acclimatize at 3,000 m, for altitudes above 6,000 to 8,000 m, complete acclimatization, even if it is possible, may require six weeks or more (figure 4). When the altitude-acclimatized person returns to sea level, the process reverses. That is, the arterial oxygen pressure now rises to the sea-level value and ventilation falls. Now there is less CO2 exhaled, and CO2 pressure rises in the blood and in the respiratory centre. The acid-base balance is altered toward the acid side, and the kidneys must retain bicarbonate to restore balance. Although the time required for the loss of acclimatization is not as well understood, it seems to require approximately as long an interval as the acclimatization process itself. If so, then return from altitude, hypothetically, gives a mirror image of altitude ascent, with one important exception: arterial oxygen pressures immediately become normal on descent.
Figure 4. Effects of altitude on barometric pressure and inspired PO2
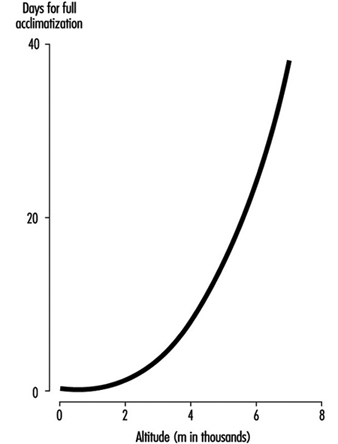
Variability among individuals
As might be expected, individuals vary with regard to time required for, and magnitude of, ventilatory acclimatization to a given altitude. One very important reason is the large variation between individuals in the ventilatory response to hypoxia. For example, at sea level, if one holds the CO2 pressure constant, so that it does not confound the ventilatory response to low oxygen, some normal persons show little or no increase in ventilation, while others show a very large (up to fivefold) increase. The ventilatory response to breathing low-oxygen mixtures seems to be an inherent characteristic of an individual, because family members behave more alike than do persons who are not related. Those persons who have poor ventilatory responses to low oxygen at sea level, as expected, also seem to have smaller ventilatory responses over time at high altitude. There may be other factors causing inter-individual variability in acclimatization, such as variability in the magnitude of ventilatory depression, in the function of the respiratory centre, in sensitivity to acid-base changes, and in renal handling of bicarbonate, but these have not been evaluated.
Sleep
Poor sleep quality, particularly before there is ventilatory acclimatization, is not only a common complaint, but also a factor that will impair occupational efficiency. Many things interfere with the act of breathing., including emotions, physical activity, eating and the degree of wakefulness. Ventilation decreases during sleep, and the capacity for breathing to be stimulated by low oxygen or high CO2 also decreases. Respiratory rate and depth of breathing both decrease. Further, at high altitude, where there are fewer oxygen molecules in the air, the amount of oxygen stored in the lung alveoli between breaths is less. Thus if breathing ceases for a few seconds (called apnoea, which is a common event at high altitude), the arterial oxygen pressure falls more rapidly than at sea level, where, in essence, the reservoir for oxygen is greater.
Periodic cessation of breathing is almost universal during the first few nights following ascent to high altitude. This is a reflection of the respiratory dilemma of altitude, described earlier, working in cyclic fashion: hypoxic stimulation increases ventilation, which in turn lowers carbon dioxide levels, inhibits breathing, and increases hypoxic stimulation, which again stimulates ventilation. Usually there is an apnoeic period of 15 to 30 seconds, followed by several very large breaths, which often briefly awakens the subject, after which there is another apnoea. The arterial oxygen pressure sometimes falls to alarming levels as a result of the apnoeic periods. There may be frequent awakenings, and even when total sleep time is normal its fragmentation impairs sleep quality such that there is the impression of having had a restless or sleepless night. Giving oxygen eliminates the cycling of hypoxic stimulation, and alkalotic inhibition abolishes the periodic breathing and restores normal sleep.
Middle-aged males in particular also are at risk for another cause of apnoea, namely intermittent obstruction of the upper airway, the common cause of snoring. While intermittent obstruction at the back of the nasal passages usually causes only annoying noise at sea level, at high altitude, where there is a smaller reservoir of oxygen in the lungs, such obstruction may lead to severely low levels of arterial oxygen pressure and poor sleep quality.
Intermittent Exposure
There are work situations, particularly in the Andes of South America, that require a worker to spend several days at altitudes above 3,000 to 4,000 m, and then to spend several days at home, at sea level. The particular work schedules (how many days are to be spent at altitude, say four to 14, and how many days, say three to seven, at sea level) are usually determined by the economics of the workplace more than by health considerations. However, a factor to be considered in the economics is the interval required both for acclimatization and loss of acclimatization to the altitude in question. Particular attention should be placed on the worker’s sense of well-being and performance on the job on arrival and the first day or two thereafter, regarding fatigue, time required to perform routine and non-routine functions, and errors made. Also strategies should be considered to minimize the time required for acclimatization at altitude, and to improve function during the waking hours.
Decompression Disorders
A wide range of workers are subject to decompression (a reduction in ambient pressure) as part of their working routine. These include divers who themselves are drawn from a wide range of occupations, caisson workers, tunnellers, hyperbaric chamber workers (usually nurses), aviators and astronauts. Decompression of these individuals can and does precipitate a variety of decompression disorders. While most of the disorders are well understood, others are not and in some instances, and despite treatment, injured workers can become disabled. The decompression disorders are the subject of active research.
Mechanism of Decompression Injury
Principles of gas uptake and release
Decompression may injure the hyperbaric worker via one of two primary mechanisms. The first is the consequence of inert gas uptake during the hyperbaric exposure and bubble formation in tissues during and after the subsequent decompression. It is generally assumed that the metabolic gases, oxygen and carbon dioxide, do not contribute to bubble formation. This is almost certainly a false assumption, but the consequent error is small and such an assumption will be made here.
During the compression (increase in ambient pressure) of the worker and throughout their time under pressure, inspired and arterial inert gas tensions will be increased relative to those experienced at normal atmospheric pressure—the inert gas(es) will then be taken up into tissues until an equilibrium of inspired, arterial and tissue inert gas tensions is established. Equilibrium times will vary from less than 30 minutes to more than a day depending upon the type of tissue and gas involved, and, in particular, will vary according to:
- the blood supply to the tissue
- the solubility of the inert gas in blood and in the tissue
- the diffusion of the inert gas through blood and into the tissue
- the temperature of the tissue
- the local tissue work-loads
- the local tissue carbon dioxide tension.
The subsequent decompression of the hyperbaric worker to normal atmospheric pressure will clearly reverse this process, gas will be released from tissues and will eventually be expired. The rate of this release is determined by the factors listed above, except, for as yet poorly understood reasons, it appears to be slower than the uptake. Gas elimination will be slower still if bubbles form. The factors that influence the formation of bubbles are well established qualitatively, but not quantitatively. For a bubble to form the bubble energy must be sufficient to overcome ambient pressure, surface tension pressure and elastic tissue pressures. The disparity between theoretical predictions (of surface tension and critical bubble volumes for bubble growth) and actual observation of bubble formation is explained variously by arguing that bubbles form in tissue (blood vessel) surface defects and/or on the basis of small short-lived bubbles (nuclei) that are continually formed in the body (e.g., between tissue planes or in areas of cavitation). The conditions that must exist before gas comes out of solution are also poorly defined—although it is likely that bubbles form whenever tissue gas tensions exceed ambient pressure. Once formed, bubbles provoke injury (see below) and become increasingly stable as a consequence of coalescence and recruitment of surfactants to the bubble surface. It may be possible for bubbles to form without decompression by changing the inert gas that the hyperbaric worker is breathing. This effect is probably small and those workers that have had a sudden onset of a decompression illness after a change in inspired inert gas almost certainly already had “stable” bubbles in their tissues.
It follows that to introduce a safe working practice a decompression programme (schedule) should be employed to avoid bubble formation. This will require modelling of the following:
- the uptake of the inert gas(es) during the compression and the hyperbaric exposure
- the elimination of the inert gas(es) during and after the decompression
- the conditions for bubble formation.
It is reasonable to state that to date no completely satisfactory model of decompression kinetics and dynamics has been produced and that hyperbaric workers now rely on programmes that have been established essentially by trial and error.
Effect of Boyle’s Law on barotrauma
The second primary mechanism by which decompression can cause injury is the process of barotrauma. The barotraumata can arise from compression or decompression. In compression barotrauma, the air spaces in the body that are surrounded by soft tissue, and hence are subject to increasing ambient pressure (Pascal’s principle), will be reduced in volume (as reasonably predicted by Boyles’ law: doubling of ambient pressure will cause gas volumes to be halved). The compressed gas is displaced by fluid in a predictable sequence:
- The elastic tissues move (tympanic membrane, round and oval windows, mask material, clothing, rib cage, diaphragm).
- Blood is pooled in the high compliance vessels (essentially veins).
- Once the limits of compliance of blood vessels are reached, there is an extravasation of fluid (oedema) and then blood (haemorrhage) into the surrounding soft tissues.
- Once the limits of compliance of the surrounding soft tissues are reached, there is a shift of fluid and then blood into the air space itself.
This sequence can be interrupted at any time by an ingress of additional gas into the space (e.g., into the middle ear on performing a valsalva manoeuvre) and will stop when gas volume and tissue pressure are in equilibrium.
The process is reversed during decompression and gas volumes will increase, and if not vented to atmosphere will cause local trauma. In the lung this trauma may arise from either over-distension or from shearing between adjacent areas of lung that have significantly different compliance and hence expand at different rates.
Pathogenesis of Decompression Disorders
The decompression illnesses can be divided into the barotraumata, tissue bubble and intravascular bubble categories.
Barotraumata
During compression, any gas space may become involved in barotrauma and this is especially common in the ears. While damage to the external ear requires occlusion of the external ear canal (by plugs, a hood, or impacted wax), the tympanic membrane and middle ear is frequently damaged. This injury is more likely if the worker has upper respiratory tract pathology that causes eustachian tube dysfunction. The possible consequences are middle ear congestion (as described above) and/or tympanic membrane rupture. Ear pain and a conductive deafness are likely. Vertigo may result from an ingress of cold water into the middle ear through a ruptured tympanic membrane. Such vertigo is transient. More commonly, vertigo (and possibly also a sensorineural deafness) will result from inner ear barotrauma. During compression, inner ear damage often results from a forceful valsalva manoeuvre (that will cause a fluid wave to be transmitted to the inner ear via the cochlea duct). The inner ear damage is usually within the inner ear—round and oval window rupture is less common.
The paranasal sinuses often are similarly involved and usually because of a blocked ostium. In addition to local and referred pain, epistaxis is common and cranial nerves may be “compressed”. It is noteworthy that the facial nerve may be likewise affected by middle ear barotrauma in individuals with a perforate auditory nerve canal. Other areas that may be affected by compressive barotrauma, but less commonly, are the lungs, teeth, gut, diving mask, dry-suits and other equipment such as buoyancy compensating devices.
Decompressive barotraumata are less common than compressive barotraumata, but tend to have a more adverse outcome. The two areas primarily affected are the lungs and inner ear. The typical pathological lesion of pulmonary barotrauma has yet to be described. The mechanism has been variously ascribed to the over-inflation of alveoli either to “open up pores” or mechanically to disrupt the alveolus, or as the consequence of shearing of lung tissue due to local differential lung expansion. Maximum stress is likely at the base of alveoli and, given that many underwater workers often breathe with small tidal excursions at or near total lung capacity, the risk of barotrauma is increased in this group as lung compliance is lowest at these volumes. Gas release from damaged lung may track through the interstitium to the hilum of the lungs, mediastinum and perhaps into the subcutaneous tissues of the head and neck. This interstitial gas may cause dyspnoea, substernal pain and coughing which may be productive of a little bloodstained sputum. Gas in the head and neck is self-evident and may occasionally impair phonation. Cardiac compression is extremely rare. Gas from a barotraumatised lung may also escape into the pleural space (to cause a pneumothorax) or into the pulmonary veins (to eventually become arterial gas emboli). In general, such gas most commonly either escapes into the interstitium and pleural space or into the pulmonary veins. Concurrent obvious damage to the lung and arterial gas embolism are (fortunately) uncommon.
Autochthonous tissue bubbles
If, during decompression, a gas phase forms, this is usually, initially, in tissues. These tissue bubbles may induce tissue dysfunction via a variety of mechanisms—some of these are mechanical and others are biochemical.
In poorly compliant tissues, such as long bones, the spinal cord and tendons, bubbles may compress arteries, veins, lymphatics and sensory cells. Elsewhere, tissue bubbles may cause mechanical disruption of cells or, at a microscopic level, of myelin sheaths. The solubility of nitrogen in myelin may explain the frequent involvement of the nervous system in decompression illness amongst workers who have been breathing either air or an oxygen-nitrogen gas mixture. Bubbles in tissues may also induce a biochemical “foreign-body” response. This provokes an inflammatory response and may explain the observation that a common presentation of decompression illness is an influenza-like illness. The significance of the inflammatory response is demonstrated in animals such as rabbits, where inhibition of the response prevents the onset of decompression illness. The major features of the inflammatory response include a coagulopathy (this is particularly important in animals, but less so in humans) and the release of kinins. These chemicals cause pain and also an extravasation of fluid. Haemoconcentration also results from the direct effect of bubbles on blood vessels. The end result is a significant compromise of the microcirculation and, in general, measurement of the haematocrit correlates well with the severity of the illness. Correction of this haemoconcentration has a predictably significant benefit on outcome.
Intravascular bubbles
Venous bubbles may either form de-novo as gas comes out of solution or they may be released from tissues. These venous bubbles travel with blood flow to the lungs to be trapped in the pulmonary vasculature. The pulmonary circulation is a highly effective filter of bubbles because of the relatively low pulmonary artery pressure. In contrast, few bubbles are trapped for long periods in the systemic circulation because of the significantly greater systemic arterial pressure. The gas in bubbles trapped in the lung diffuses into the pulmonary air spaces from where it is exhaled. While these bubbles are trapped, however, they may cause adverse effects by either provoking an imbalance of lung perfusion and ventilation or by increasing pulmonary artery pressure and consequently right heart and central venous pressure. The increased right heart pressure can cause “right to left” shunting of blood through pulmonary shunts or intra-cardiac “anatomical defects” such that bubbles bypass the lung “filter” to become arterial gas emboli. Increases in venous pressure will impair venous return from tissues, thereby impairing the clearance of inert gas from the spinal cord; venous haemorrhagic infarction may result. Venous bubbles also react with blood vessels and blood constituents. An effect on blood vessels is to strip the surfactant lining from endothelial cells and hence to increase vascular permeability, which may be further compromised by the physical dislocation of endothelial cells. However, even in the absence of such damage, endothelial cells increase the concentration of glycoprotein receptors for polymorphonuclear leukocytes on their cell surface. This, together with a direct stimulation of white blood cells by bubbles, causes leucocyte binding to endothelial cells (reducing flow) and subsequent infiltration into and through the blood vessels (diapedesis). The infiltrating polymorphonuclear leukocytes cause future tissue injury by release of cytotoxins, oxygen free radicals and phospholipases. In blood, bubbles will not only cause the activation and accumulation of polymorphonuclear leukocytes, but also the activation of platelets, coagulation and complement, and the formation of fat emboli. While these effects have relatively minor importance in the highly compliant venous circulation, similar effects in the arteries can reduce blood flow to ischaemic levels.
Arterial bubbles (gas emboli) can arise from:
- pulmonary barotrauma causing the release of bubbles into the pulmonary veins
- bubbles being “forced” through the pulmonary arterioles (this process is enhanced by oxygen toxicity and by those bronchodilators that are also vasodilators such as aminophylline)
- bubbles bypassing the lung filter through a right to left vascular channel (e.g., patent foramen ovale).
Once in the pulmonary veins, bubbles return to the left atrium, left ventricle, and then are pumped into the aorta. Bubbles in the arterial circulation will distribute according to buoyancy and blood flow in large vessels, but elsewhere with blood flow alone. This explains the predominant embolism of the brain and, in particular, the middle cerebral artery. The majority of bubbles that enter the arterial circulation will pass through into the systemic capillaries and into the veins to return to the right side of the heart (usually to be trapped in the lungs). During this transit these bubbles may cause a temporary interruption of function. If the bubbles remain trapped in the systemic circulation or are not redistributed within five to ten minutes, then this loss of function may persist. If bubbles embolise the brain stem circulation, then the event may be lethal. Fortunately, the majority of bubbles will be redistributed within minutes of first arrival in the brain and a recovery of function is usual. However, during this transit the bubbles will cause the same vascular (blood vessels and blood) reactions as described above in venous blood and veins. Consequently, a significant and progressive decline in cerebral blood flow may occur, which may reach the levels at which normal function cannot be sustained. The hyperbaric worker will, at this time, suffer a relapse or deterioration in function. In general, about two-thirds of hyperbaric workers who suffer cerebral arterial gas embolism will spontaneously recover and about one-third of these will subsequently relapse.
Clinical Presentation of Decompression Disorders
Time of onset
Occasionally, the onset of decompression illness is during the decompression. This is most commonly seen in the barotraumata of ascent, particularly involving the lungs. However, the onset of the majority of decompression illnesses occurs after decompression is complete. Decompression illnesses due to the formation of bubbles in tissues and in blood vessels usually become evident within minutes or hours after decompression. The natural history of many of these decompression illnesses is for the spontaneous resolution of symptoms. However, some will only resolve spontaneously incompletely and there is a need for treatment. There is substantial evidence that the earlier the treatment the better the outcome. The natural history of treated decompression illnesses is variable. In some cases, residual problems are seen to resolve over the following 6-12 months, while in others symptoms appear not to resolve.
Clinical manifestations
A common presentation of decompression illness is an influenza-like condition. Other frequent complaints are various sensory disorders, local pain, particularly in the limbs; and other neurologic manifestations, which may involve higher functions, special senses and motor weariness (less commonly the skin and lymphatic systems may be involved). In some groups of hyperbaric workers, the most common presentation of decompression illness is pain. This may be a discrete pain about a specific joint or joints, back pain or referred pain (when the pain is often located in the same limb as are overt neurologic deficits), or less commonly, in an acute decompression illness, vague migratory aches and pains may be noticed. Indeed, it is reasonable to state that the manifestations of the decompression illnesses are protean. Any illness in a hyperbaric worker that occurs up to 24-48 hours after a decompression should be assumed to be related to that decompression until proven otherwise.
Classification
Until recently, the decompression illnesses were classified into:
- the barotraumata
- cerebral arterial gas embolism
- decompression sickness.
Decompression sickness was further subdivided into Type 1 (pain, itch, swelling and skin rashes), Type 2 (all other manifestations) and Type 3 (manifestations of both cerebral arterial gas embolism and decompression sickness) categories. This classification system arose from an analysis of the outcome of caisson workers using new decompression schedules. However, this system has had to be replaced both because it is neither discriminatory nor prognostic and because there is a low concordance in diagnosis between experienced physicians. The new classification of the decompression illnesses recognises the difficulty in distinguishing between cerebral arterial gas embolism and cerebral decompression sickness and similarly the difficulty in distinguishing Type 1 from Type 2 and Type 3 decompression sickness. All decompression illnesses are now classified as such—decompression illness, as described in table 1. This term is prefaced with a description of the nature of the illness, the progression of symptoms and a list of the organ systems in which the symptoms are manifest (no assumptions are made about the underlying pathology). For example, a diver may have acute progressive neurological decompression illness. The complete classification of the decompression illness includes a comment on the presence or absence of barotrauma and the likely inert gas loading. These latter terms are relevant to both treatment and likely fitness to return to work.
Table 1. Revised classification system of the decompression illnesses
|
Duration |
Evolution |
Symptoms |
|
|
Acute |
Progressive |
Musculoskeletal |
|
|
Chronic |
Spontaneously resolving |
Cutaneous |
Decompression illness + or - |
|
|
Static |
Lymphatic |
Evidence of barotrauma |
|
|
Relapsing |
Neurological |
|
|
|
|
Vestibular |
|
|
|
|
Cardiorespiratory |
|
First Aid Management
Rescue and resuscitation
Some hyperbaric workers develop a decompression illness and require to be rescued. This is particularly true for divers. This rescue may require their recovery to a stage or diving bell, or a rescue from underwater. Specific rescue techniques must be established and practised if they are to be successful. In general, divers should be rescued from the ocean in a horizontal posture (to avoid possibly lethal falls in cardiac output as the diver is re-subjected to gravity—during any dive there is a progressive loss of blood volume consequent to displacement of blood from the peripheries into the chest) and consequent diuresis and this posture should be maintained until the diver is, if necessary, in a recompression chamber.
The resuscitation of an injured diver should follow the same regimen as used in resuscitations elsewhere. Of specific note is that the resuscitation of a hypothermic individual should continue at least until the individual is rewarmed. There is no convincing evidence that resuscitation of an injured diver in the water is effective. In general, the divers’ best interests are usually served by early rescue ashore, or to a diving bell/platform.
Oxygen and fluid resuscitation
A hyperbaric worker with a decompression illness should be laid flat, to minimize the chances of bubbles distributing to the brain, but not placed in a head-down posture which probably adversely affects the outcome. The diver should be given 100% oxygen to breathe; this will require either a demand valve in a conscious diver or a sealing mask, high flow rates of oxygen and a reservoir system. If oxygen administration is to be prolonged, then airbreaks should be given to ameliorate or retard the development of pulmonary oxygen toxicity. Any diver with decompression illness should be re-hydrated. There is probably no place for oral fluids in the acute resuscitation of a severely injured worker. In general, it is difficult to administer oral fluids to someone lying flat. Oral fluids will require the administration of oxygen to be interrupted and then usually have negligible immediate effect on the blood volume. Finally, since subsequent hyperbaric oxygen treatment may cause a convulsion, it is not desirable to have any stomach contents. Ideally then, fluid resuscitation should be by the intravenous route. There is no evidence of any advantage of colloid over crystalloid solutions and the fluid of choice is probably normal saline. Solutions containing lactate should not be given to a cold diver and dextrose solutions should not be given to anyone with a brain injury (as aggravation of the injury is possible). It is essential that an accurate fluid balance be maintained as this is probably the best guide to the successful resuscitation of a hyperbaric worker with decompression illness. Bladder involvement is sufficiently common that early recourse to bladder catheterization is warranted in the absence of urinary output.
There are no drugs that are of proven benefit in the treatment of the decompression illnesses. However, there is growing support for lignocaine and this is under clinical trial. The role of lignocaine is thought to be both as a membrane stabiliser and as an inhibitor of the polymorphonuclear leukocyte accumulation and blood vessel adherence that is provoked by bubbles. It is noteworthy that one of the probable roles of hyperbaric oxygen is also to inhibit the accumulation of and adherence to blood vessels of leucocytes. Finally, there is no evidence that any benefit is derived from the use of platelet inhibitors such as aspirin or other anticoagulants. Indeed, as haemorrhage into the central nervous system is associated with severe neurological decompression illness, such medication may be contra-indicated.
Retrieval
Retrieval of a hyperbaric worker with decompression illness to a therapeutic recompression facility should occur as soon as is possible, but must not involve any further decompression. The maximum altitude to which such a worker should be decompressed during aeromedical evacuation is 300 m above sea level. During this retrieval, the first aid and adjuvant care described above should be provided.
Recompression Treatment
Applications
The definitive treatment of most of the decompression illnesses is recompression in a chamber. The exception to this statement are the barotraumata that do not cause arterial gas embolism. The majority of aural barotrauma victims require serial audiology, nasal decongestants, analgesics and, if inner ear barotrauma is suspected, strict bed rest. It is possible however that hyperbaric oxygen (plus stellate ganglion blockade) may be an effective treatment of this latter group of patients. The other barotraumata that often require treatment are those of the lung—most of those respond well to 100% oxygen at atmospheric pressure. Occasionally, chest cannulation may be needed for a pneumothorax. For other patients, early recompression is indicated.
Mechanisms
An increase in ambient pressure will make bubbles smaller and hence less stable (by increasing surface tension pressure). These smaller bubbles will also have a greater surface area to volume for resolution by diffusion and their mechanical disruptive and compressive effects on tissue will be reduced. It is also possible that there is a threshold bubble volume that will stimulate a “foreign-body” reaction. By reducing bubble size, this effect may be reduced. Finally, reducing the volume (length) of columns of gas that are trapped in the systemic circulation will promote their redistribution to the veins. The other outcome of most recompressions is an increase in the inspired (PiO2) and arterial oxygen tension (PaO2). This will relieve hypoxia, lower interstitial fluid pressure, inhibit the activation and accumulation of polymorphonuclear leukocytes that is usually provoked by bubbles, and lower the haematocrit and hence blood viscosity.
Pressure
The ideal pressure at which to treat decompression illness is not established, although the conventional first choice is 2.8 bar absolute (60 fsw; 282 kPa), with further compression to 4 and 6 bar absolute pressure if the response of symptoms and signs is poor. Experiments in animals suggest that 2 bars absolute pressure is as effective a treatment pressure as greater compressions.
Gas(es)
Similarly, the ideal gas to be breathed during the therapeutic recompression of these injured workers is not established. Oxygen-helium mixtures may be more effective in the shrinkage of air bubbles than either air or 100% oxygen and are the subject of ongoing research. The ideal PiO2 is thought, from in vivo research, to be about 2 bar absolute pressure although it is well established, in head injured patients, that the ideal tension is lower at 1.5 bars absolute. The dose relationship with regard to oxygen and inhibition of bubble-provoked polymorphonuclear leukocyte accumulation has not yet been established.
Adjuvant care
The treatment of an injured hyperbaric worker in a recompression chamber must not be allowed to compromise his/her need for adjuvant care such as ventilation, rehydration and monitoring. To be a definitive treatment facility, a recompression chamber must have a working interface with the equipment routinely used in critical care medical units.
Follow-up treatment and investigations
Persistent and relapsing symptoms and signs of decompression illness are common and most injured workers will require repeated recompressions. These should continue until the injury is and remains corrected or at least until two successive treatments have failed to produce any sustained benefit. The basis of ongoing investigation is careful clinical neurological examination (including mental status), as available imaging or provocative investigative techniques have either an associated excessive false positive rate (EEG, bone radio-isotope scans, SPECT scans) or an associated excessive false negative rate (CT, MRI, PET, evoked response studies). One year after an episode of decompression illness, the worker should be x-rayed to determine if there is any dysbaric osteonecrosis (aseptic necrosis) of their long bones.
Outcome
The outcome after recompression therapy of decompression illness depends entirely upon the group being studied. Most hyperbaric workers (e.g., military and oil-field divers) respond well to treatment and significant residual deficits are uncommon. In contrast, many recreational divers treated for decompression illness have a subsequent poor outcome. The reasons for this difference in outcome are not established. Common sequelae of decompression illness are in order of decreasing frequency: depressed mood; problems in short-term memory; sensory symptoms such as numbness; difficulties with micturition and sexual dysfunction; and vague aches and pains.
Return to hyperbaric work
Fortunately, most hyperbaric workers are able to return to hyperbaric work after an episode of decompression illness. This should be delayed for at least a month (to allow a return to normal of the disordered physiology) and must be discouraged if the worker suffered pulmonary barotrauma or has a history of recurrent or severe inner ear barotrauma. A return to work should also be contingent upon:
- the severity of the decompression illness being commensurate with the extent of the hyperbaric exposure/decompression stress
- a good response to treatment
- no evidence of sequelae.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."