- You are here:
-
Home

-
Part XVII. Services and Trade
-
Transport Industry and Warehousing
- Water Transport
Pesticides
Adapted from 3rd edition, Encyclopaedia of Occupational Health and Safety. Revision includes information from A. Baiinova, J.F. Copplestone, L.A. Dobrobolskij,
F. Kaloyanova-Simeonova, Y.I. Kundiev and A.M. Shenker.
The word pesticide generally denotes a chemical substance (which may be mixed with other substances) that is used for the destruction of an organism deemed to be detrimental to humans. The word clearly has a very wide meaning and includes a number of other terms, such as insecticides, fungicides, herbicides, rodenticides, bactericides, miticides, nematocides and molluscicides, which individually indicate the organisms or pests that the chemical or class of chemicals is designed to kill. As different types of chemical agents are used for these general classes, it is usually advisable to indicate the particular category of pesticide.
General Principles
Acute toxicity is measured by the LD50 value; this is a statistical estimate of the number of mg of the chemical per kg of body weight required to kill 50% of a large population of test animals. The dose may be administered by a number of routes, usually orally or dermally, and the rat is the standard test animal. Oral or dermal LD50 values are used according to which route has the lower value for a specific chemical. Other effects, either as a result of short-term exposure (such as neurotoxicity or mutagenicity) or of long-term exposure (such as carcinogenicity), have to be taken into account, but pesticides with such known properties are not registered for use. The WHO Recommended Classification of Pesticides by Hazard and Guidelines to Classification 1996-1997 issued by the World Health Organization (WHO) classifies technical products according to the acute risk to human health as follows:
- Class IA—extremely hazardous
- Class IB—highly hazardous
- Class II—moderately hazardous
- Class III—slightly hazardous.
The guidelines based on the WHO Classification list pesticides according to toxicity and physical state; these are presented in a separate article in this chapter.
Poisons enter the body through the mouth (ingestion), the lungs (inhalation), the intact skin (percutaneous absorption) or wounds in the skin (inoculation). The inhalation hazard is determined by the physical form and solubility of the chemical. The possibility and degree of percutaneous absorption varies with the chemical. Some chemicals also exert a direct action on the skin, causing dermatitis. Pesticides are applied in many different forms—as solids, by spraying in dilute or concentrated form, as dusts (fine or granulated), and as fogs and gases. The method of use has a bearing on the likelihood of absorption.
The chemical may be mixed with solids (often with food used as bait), water, kerosene, oils or organic solvents. Some of these diluents have some degree of toxicity of their own and may influence the rate of absorption of the pesticide chemical. Many formulations contain other chemicals which are not themselves pesticides but which enhance the effectiveness of the pesticide. Added surface-active agents are a case in point. When two or more pesticides are mixed in the same formulation, the action of one or both may be enhanced by the presence of the other. In many cases, the combined effects of mixtures have not been fully worked out, and it is a good rule that mixtures should always be treated as more toxic than any of the constituents on their own.
By their very nature and purpose, pesticides have adverse biological effects on at least some species, human beings included. The following discussion provides a broad overview of the mechanisms by which pesticides can act, and some of their toxic effects. Carcinogenicity, biological monitoring and safeguards in the use of pesticides are discussed in more detail elsewhere in this Encyclopaedia.
Organochlorine Pesticides
The organochlorine pesticides (OCPs) have caused intoxication following skin contact, ingestion or inhalation. Examples are endrin, aldrin and dieldrin. The rate of absorption and toxicity differ depending on the chemical structure and the solvents, surfactants and emulsifiers used in the formulation.
The elimination of OCPs from the body takes place slowly through the kidneys. Metabolism in the cells involves various mechanisms—oxidation, hydrolysis and others. OCPs have a strong tendency to penetrate cell membranes and to be stored in the body fat. Because of their attraction to fatty tissues (lipotropic properties) OCPs tend to be stored in the central nervous system (CNS), liver, kidneys and the myocardium. In these organs they cause damage to the function of important enzyme systems and disrupt the biochemical activity of the cells.
OCPs are highly lipophilic and tend to accumulate in fatty tissue as long as exposure persists. When exposure ceases, they are released slowly into the bloodstream, often over a period of many years, from whence they can be transported to other organs where genotoxic effects, including cancer, may be initiated. The great majority of US residents, for example, have detectable levels of organochlorine pesticides, including breakdown products of DDT, in their adipose (fatty) tissue, and the concentrations increase with age, reflecting lifetime accumulations.
A number of OCPs that have been used throughout the world as insecticides and herbicides are also proven or suspected carcinogens to humans. These are discussed in more detail in the Toxicology and Cancer chapters of this Encyclopaedia.
Acute intoxications
Aldrin, endrin, dieldrin and toxaphene are most frequently implicated in acute poisoning. Delay in the onset of symptoms in severely acute intoxications is about 30 minutes. With lower toxicity OCPs it is several hours but not more than twelve.
Intoxication is demonstrated by gastrointestinal symptoms: nausea, vomiting, diarrhoea and stomach pains. The basic syndrome is cerebral: headache, dizziness, ataxia and paraesthesia. Gradually tremors set in, starting from the eyelids and the face muscles, descending towards the whole body and the limbs; in severe cases this leads to fits of tonic-clonic convulsions, which gradually extend to the different muscle groups. Convulsions may be connected with elevated body temperature and unconsciousness and may result in death. In addition to the cerebral signs, acute intoxications may lead to bulbar paralysis of the respiratory and/or vasomotor centres, which causes acute respiratory deficiency or apnoea, and to severe collapse.
Many patients develop signs of toxic hepatitis and toxic nephropathy. After these symptoms have disappeared some patients develop signs of prolonged toxic polyneuritis, anaemia and haemorrhagic diathesis connected with the impaired thrombocytopoiesis. Typical of toxaphene is an allergic bronchopneumonia.
Acute intoxications with OCPs last up to 72 hours. When organ function has been seriously impaired, the illness may continue up to several weeks. Complications in cases of liver and kidney damage can be long-lasting.
Chronic poisoning
During the application of OCPs in agriculture as well as in their production, poisoning is most commonly chronic—that is, low doses of exposure over time. Acute intoxication (or high-level exposures at a particular instant) are less common and are usually the result of misuse or accidents, both in the home and in industry. Chronic intoxication is characterized by damage to the nervous, digestive and cardiovascular systems and the blood-formation process. All OCPs are CNS stimulants and are capable of producing convulsions, which frequently appear to be epileptic in character. Abnormal electroencephalographic (EEG) data have been recorded, such as irregular alpha rhythms and other abnormalities. In some cases bitemporal sharp-peaked waves with shifting localization, low voltage and diffuse theta activity have been observed. In other cases paroxysmal emissions have been registered, composed of slow sharp-peaked waves, sharp-peaked complexes and rhythmic peaks with low voltage.
Polyneuritis, encephalopolyneuritis and other nervous system effects have been described following occupational exposure to OCPs. Tremor of the limbs and alterations in the electromyograms (EMGs) have also been observed in workers. In workers handling OCPs such as BHC, polychloropinene, hexachlorobutadiene and dichloroethane, non-specific signs (e.g., diencephalic signs) have been observed and very often develop together with other signs of chronic intoxication. The most common signs of intoxication are headache, dizziness, numbness and tingling in the limbs, rapid changes in blood pressure and other signs of circulatory disturbances. Less frequently, colic pains below the right ribs and in the region of the umbilicus, and dyskinesia of the bile ducts, are observed. Behavioural changes, such as disturbances of sensory and equilibrium functions, are found. These symptoms are often reversible after cessation of the exposure.
OCPs cause liver and kidney damage. Microsomal enzyme induction has been observed, and increased ALF and aldolase activity have also been reported. Protein synthesis, lipoid synthesis, detoxification, excretion and liver functions are all affected. Reduction of creatinine clearance and phosphorus reabsorption are reported in workers exposed to pentachlorophenol, for example. Pentachlorophenol, along with the family of chlorophenols, are also considered possible human carcinogens (group 2B as classified by the International Agency for Research on Cancer (IARC)). Toxaphene is also considered to be a group 2B carcinogen.
Cardiovascular disturbances have been observed in exposed persons, most frequently demonstrated as dyspnoea, high heart rate, heaviness and pain in the heart region, increased heart volume and hollow heart tones.
Blood and capillary disturbances have also been reported following contact with OCPs. Thrombopenia, anaemia, pancytopenia, agranulocytosis, haemolysis and capillary disorders have all been reported. Medullar aplasia can be complete. The capillary damage (purpura) can develop following long- or short-term but intensive exposures. Eosinopenia, neutropenia with lymphocytosis, and hypochromic anaemia have been observed in workers subjected to prolonged exposures.
Skin irritation is reported to follow from skin contact with some OCPs, particularly chlorinated terpenes. Often chronic intoxications are clinically demonstrated by signs of allergic damage.
Organophosphate Pesticides
The organophosphorus pesticides are chemically related esters of phosphoric acid or certain of its derivatives. The organic phosphates are also identified by a common pharmacological property—the ability to inhibit the action of the cholinesterase enzymes.
Parathion is among the most dangerous of the organophosphates and is discussed in some detail here. In addition to parathion’s pharmacological effects, no insect is immune to its lethal action. Its physical and chemical properties have rendered it useful as an insecticide and acaricide for agricultural purposes. The description of parathion’s toxicity applies to other organophosphates, although their effects may be less rapid and extensive.
The toxic action of all organic phosphates is on the CNS through inhibition of the cholinesterase enzymes. Inhibiting these cholinesterases produces excessive and continuous stimulation of those muscle and gland structures which are activated by acetylcholine, to a point where life can no longer be sustained. Parathion is an indirect inhibitor because it must be converted in the environment or in vivo before it can effectively inhibit cholinesterase.
Organophosphates can generally enter the body by any route. Serious and even fatal poisoning may occur by ingesting a small amount of parathion while eating or smoking, for example. Organophosphates may be inhaled when dusts or volatile compounds are even briefly handled. Parathion is easily absorbed through the skin or the eye. The ability to penetrate the skin in fatal quantities without the warning of irritation makes parathion especially difficult to handle.
Signs and symptoms of organophosphate poisoning can be explained on the basis of cholinesterase inhibition. Early or mild poisoning may be hard to distinguish because of a number of other conditions; heat exhaustion, food poisoning, encephalitis, asthma and respiratory infections share some of the manifestations and confuse the diagnosis. Symptoms can be delayed for several hours after the last exposure but rarely longer than 12 hours. Symptoms most often appear in this order: headaches, fatigue, giddiness, nausea, sweating, blurred vision, tightness in the chest, abdominal cramps, vomiting and diarrhoea. In more advanced poisoning, difficult breathing, tremors, convulsions, collapse, coma, pulmonary oedema and respiratory failure follow. The more advanced the poisoning, the more obvious are the typical signs of cholinesterase inhibition, which are: pinpoint pupils; rapid, asthmatic type breathing; marked weakness; excessive sweating; excessive salivation; and pulmonary oedema.
In very severe parathion poisoning, in which the victim has been unconscious for some time, brain damage from anoxia may occur. Fatigue, ocular symptoms, electroencephalogram abnormalities, gastrointestinal complaints, excessive dreams and exposure intolerance to parathion have been reported to persist for days to months following acute poisoning. There is no evidence that permanent impairment occurs.
Chronic exposure to parathion may be cumulative in the sense that repeated exposures closely following each other can reduce cholinesterase faster than it can be regenerated, to the point where a very small exposure can precipitate acute poisoning. If the person is removed from exposure, clinical recovery is usually rapid and complete within a few days. The red blood cells and plasma should be tested for cholinesterase inhibition when phosphate ester poisoning is suspected. Red cell cholinesterase activity is most often reduced and close to zero in severe poisoning. Plasma cholinesterase is also severely reduced and is a more sensitive and more rapid indicator of exposure. There is no advantage in chemical determinations of parathion in the blood because metabolism of the pesticide is too rapid. However, p-nitrophenol, an end-product of the metabolism of parathion, can be determined in the urine. Chemical examination to identify the pesticide can be made on contaminated clothing or other material where contact is suspected.
Carbamates and Thiocarbamates
The biological activity of carbamates was discovered in 1923 when the structure of the alkaloid eserine (or physostigmine) contained in the seeds of Calabar beans was first described. In 1929 physostigmine analogues were synthesized, and soon such derivatives of dithiocarbamic acid as thiram and ziram were available. The study of carbamic compounds began in the same year, and now more than 1,000 carbamic acid derivatives are known. More than 50 of them are used as pesticides, herbicides, fungicides and nematocides. In 1947 the first carbamic acid derivatives having insecticide properties were synthesized. Some thiocarbamates have proved effective as vulcanization accelerators, and derivatives of dithiocarbamic acid have been obtained for the treatment of malignant tumours, hypoxia, neuropathies, radiation injuries and other diseases. Aryl esters of alkylcarbamic acid and alkyl esters of arylcarbamic acid are also used as pesticides.
Some carbamates can produce sensitization in exposed individuals, and a variety of foetotoxic, embryotoxic and mutagenic effects have also been observed for members of this family.
Chronic effects
The specific effects produced by acute poisoning have been described for each substance listed. A review of the specific effects gained from an analysis of published data makes it possible to distinguish similar features in the chronic action of the different carbamates. Some authors believe that the main toxic effect of carbamic acid esters is the involvement of the endocrine system. One of the peculiarities of carbamate poisoning is the possible allergic reaction of exposed subjects. The toxic effects of carbamates may not be immediate, which can present a potential hazard because of lack of warning. Results from animal experiments are indicative of embryotoxic, teratogenic, mutagenic and carcinogenic effects of some carbamates.
Baygon (isopropoxyphenyl-N-methylcarbamate) is produced by reaction of alkyl isocyanate with phenols, and is used as an insecticide. Baygon is a systemic poison. It causes inhibition of the serum cholinesterase activity up to 60% after oral administration of 0.75 to 1 mg/kg. This highly toxic substance exerts a weak effect on the skin.
Carbaryl is a systemic poison which produces moderately severe acute effects when ingested, inhaled or absorbed through the skin. It may cause local skin irritation. Being a cholinesterase inhibitor, it is much more active in insects than in mammals. Medical examinations of workers exposed to concentrations of 0.2 to 0.3 mg/m3 seldom reveal a fall in cholinesterase activity.
Betanal (3-(methoxycarbonyl)aminophenyl-N-(3-methylphenyl) carbamate; N-methylcarbanilate) belongs to the arylcarbamic acid alkyl esters and is used as a herbicide. Betanal is slightly toxic for the gastrointestinal and respiratory tracts. Its dermal toxicity and local irritation are insignificant.
Isoplan is a highly toxic member of the group, its action, like that of Sevin and others, being characterized by the inhibition of acetylcholinesterase activity. Isoplan is used as an insecticide. Pyrimor (5,6-dimethyl-2-dimethylamino-4-pyrimidinyl methylcarbamate) is a derivative of arylcarbamic acid alkyl esters. It is highly toxic for the gastrointestinal tract. Its general absorption and local irritative effect are not very pronounced.
Thiocarbamic Acid Esters
Ronite (sym-ethylcyclohexylethyl thiocarbamate; Eurex); Eptam (sym-ethyl-N,N-dipropyl thiocarbamate); and Tillam (sym-propyl-N-ethyl-N-butylthiocarbamate) are esters which are synthesized by reaction of alkylthiocarbamates with amines and of alkaline mercaptides with carbamoyl chlorides. They are effective herbicides of selective action.
The compounds of this group are slightly to moderately toxic, and the toxicity is reduced when they are absorbed through the skin. They can affect the oxidative processes as well as the nervous and endocrine systems.
Dithiocarbamates and bisdithiocarbamates include the following products, which have much in common as regards their use and their biological effects. Ziram is used as a vulcanization accelerator for synthetic rubbers and, in agriculture, as a fungicide and seed fumigant. This compound is very irritant to the conjunctiva and upper airway mucous membranes. It can cause extreme pain in the eyes, skin irritation and liver function disorders. It has embryotoxic and teratogenic effects. TTD is used as a seed fumigant, irritates the skin, causes dermatitis and affects the conjunctiva. It increases sensitivity to alcohol. Nabam is a plant fungicide and serves as an intermediate in the production of other pesticides. It is irritating to the skin and mucous membranes, and it is a narcotic in high concentrations. In the presence of alcohol it can cause violent vomiting. Ferbam is a fungicide of relatively low toxicity, but may cause renal function disorders. It irritates the conjunctiva, the mucous membranes of the nose and upper airways, and the skin.
Zineb is an insecticide and fungicide that can cause irritation of the eyes, nose and larynx, and is harmful if inhaled or swallowed. Maneb is a fungicide that can cause irritation of the eyes, nose and larynx, and is harmful if inhaled or swallowed. Vapam (sodium methyldithiocarbamate; carbation) is white crystalline powder of unpleasant smell similar to that of carbon disulphide. It is an effective soil fumigant which destroys weed seeds, fungi and insects. It irritates the skin and mucous membranes.
Rodenticides
Rodenticides are toxic chemicals used for the control of rats, mice and other pest species of rodents. An effective rodenticide must conform to stringent criteria, a fact that is borne out by the small number of compounds that are currently in satisfactory use.
Poisoned baits are the most generally effective and widely used means of formulating rodenticides, but some are used as “contact” poisons (i.e., dusts, foams and gels), where the toxicant adheres to the fur of the animal and is ingested during subsequent grooming, while a few are applied as fumigants to burrows or infested premises. Rodenticides may conveniently be divided into two categories, depending on their mode of action: acute (single dose) poisons and chronic (multiple dose) poisons.
Acute poisons, such as zinc phosphide, norbormide, fluoracetamide, alpha-chloralose, are highly toxic compounds, with LD50s that are usually less than 100 mg/kg, and can cause death after a single dose consumed during a period not longer than a few hours.
Most acute rodenticides have the disadvantages of producing symptoms of poisoning rather quickly, of being generally rather non-specific, and lacking satisfactory antidotes. They are used at relatively high concentrations (0.1 to 10%) in bait.
Chronic poisons, which may act, for example, as anticoagulants (e.g., calciferol), are compounds that, having a cumulative mode of action, may need to be eaten by the prey over a succession of days to cause death. Anticoagulants have the advantage of producing symptoms of poisoning very late, usually well after the target species has eaten a lethal dose. An effective antidote to anticoagulants is available for those accidentally exposed. Chronic poisons are used at relatively low concentrations (0.002 to 0.1%).
Application
Rodenticides intended for use in baits are available in one or more of the following forms: technical grade material, concentrate (“master-mix”) or ready-to-use bait. Acute poisons are usually acquired as the technical material and mixed with the bait-base shortly before use. Chronic poisons, because they are used at low concentrations, are normally sold as concentrates, where the active ingredient is incorporated into a finely powdered flour (or talc) base.
When the final bait is prepared, the concentrate is added to the bait-base at the relevant rate. If the bait-base is of a coarse consistency, it may be necessary to add a vegetable or mineral oil at a prescribed rate to act as a “sticker”, thus ensuring that the poison adheres to the bait-base. It is commonly compulsory for a warning dye to be added to concentrates or ready-to-use baits.
In control treatments against rats and mice, poisoned baits are laid at frequent intervals throughout the infested area. When acute rodenticides are used, better results are obtained when unpoisoned bait (“prebait”) is laid for a few days before the poison is given. In “acute” treatments, poisoned bait is presented for a few days only. When anticoagulants are used, prebaiting is unnecessary, but the poison should remain in position for 3 to 6 weeks to achieve complete control.
Contact formulations of rodenticides are especially useful in situations where baiting is difficult for any reason, or where the rodents are not being drawn satisfactorily off their normal diet. The poison is usually incorporated in a finely divided powder (e.g., talc), which is laid on runways or around bait points, or is blown into burrows, wall cavities and so on. The compound may also be formulated in gels or foams, which are inserted into burrows.
The use of contact rodenticides relies on the target animal ingesting the poison while grooming itself. Because the amount of dust (or foam, etc.) adhering to the fur may be small, the concentration of the active ingredient in the formulation is usually relatively high, making it safe to use only where the contamination of food and so on cannot occur. Other specialized formulations of rodenticides include water baits and wax-impregnated blocks. The former, which are aqueous solutions of soluble compounds, are especially useful in dry environments. The latter are made by impregnating the toxicant and bait-base in molten paraffin wax (of low melting point) and casting the mixture into blocks. Wax-impregnated baits are designed to withstand wet climates and insect attack.
Hazards of rodenticides
Although toxicity levels of rodenticides may vary between target and non-target species, all poisons must be presumed to be potentially lethal to humans. Acute poisons are potentially more dangerous than chronic ones because they are rapid in action, non-specific and generally lack effective antidotes. Anticoagulants, on the other hand, are slow and cumulative, allowing adequate time for the administration of a reliable antidote, such as vitamin K.
As stated above, the concentrations of active ingredients in contact formulations of a given poison are higher than those in bait preparations, thus making operator hazard considerably greater. Fumigants present a special danger when used to treat infested premises, holds of ships and so on, and should be used only by trained technicians. The gassing of rodent burrows, although less hazardous, must also be carried out with extreme caution.
Herbicides
Grassy and broad-leaved weeds compete with crop plants for light, space, water and nutrients. They are hosts to bacteria, fungi and viruses, and hamper mechanical harvesting operations. Losses in crop yields as a result of weed infestation can be very heavy, commonly reaching 20 to 40%. Weed-control measures such as hand weeding and hoeing are ineffective in intensive farming. Chemical weedkillers or herbicides have successfully replaced mechanical methods of weed control.
In addition to their use in agriculture in cereals, meadows, open fields, pastures, fruit growing, greenhouses and forestry, herbicides are applied on industrial sites, railway tracks and power lines to remove vegetation. They are used for destroying weeds in canals, drainage channels and natural or artificial pools.
Herbicides are sprayed or dusted on weeds or on the soil they infest. They remain on the leaves (contact herbicides) or penetrate into the plant and so disturb its physiology (systemic herbicides). They are classified as non-selective (total—used to kill all vegetation) and selective (used to suppress the growth of or kill weeds without damaging the crop). Both non-selective and selective can be contact or systemic.
Selectivity is true when the herbicide applied in the correct dose and, at the right time, is active against certain species of weed only. An example of true selective herbicides are the chlorophenoxy compounds, which affect broad-leaved but not grassy plants. Selectivity can also be achieved by placement (i.e., by using the herbicide in such a way that it comes into contact with the weeds only). For example, paraquat is applied to orchard crops, where it is easy to avoid the foliage. Three types of selectivity are distinguished:
1. physiological selectivity, which relies upon the plant’s ability to degrade the herbicide into non-phytotoxic components
2. physical selectivity, which exploits the particular habit of the cultivated plant (e.g., the upright in cereals) and/or a specially fashioned surface (e.g., wax-coating, resistant cuticule) protecting the plant against herbicide penetration
3. positional selectivity, in which the herbicide remains fixed in the upper soil layers adsorbed on colloidal soil particles and does not reach the root zone of the cultivated plant, or at least not in harmful quantities. Positional selectivity depends on the soil, precipitation and temperature as well as the water solubility and soil adsorption of the herbicide.
Some commonly used herbicides
Following are brief descriptions of acute and chronic effects associated with some commonly used herbicides.
Atrazine gives rise to decreased body weight, anaemia, disturbed protein and glucose metabolism in rats. It causes occupational contact dermatitis due to skin sensitization. It is considered a possible human carcinogen (IARC group 2B).
Barban, in repeated contact with 5% water emulsion, causes severe skin irritation in rabbits. It provokes skin sensitization in both experimental animals and agricultural workers, and causes anaemia, methaemoglobinaemia and changes in lipid and protein metabolism. Ataxia, tremor, cramps, bradycardia and ECG deviations are found in experimental animals.
Chlorpropharm can produce slight dermal irritation and penetration. In rats, exposure to atrazine causes anaemia, methaemoglobinaemia and reticulocytosis. Chronic application causes skin carcinoma in rats.
Cycloate causes polyneuropathia and liver damage in experimental animals. No clinical symptoms have been described after occupational exposure of workers for three consecutive days.
2,4-D poses moderate dermal toxicity and skin irritancy risks to exposed persons. It is highly irritating to the eyes. Acute exposures in workers provoke headache, dizziness, nausea, vomiting, raised temperature, low blood pressure, leucocytosis, and heart and liver injury. Chronic occupational exposure without protection may cause nausea, liver functional changes, contact toxic dermatitis, irritation of airways and eyes, as well as neurological changes. Some of the derivatives of 2,4-D are embryotoxic and teratogenic for experimental animals in high doses only.
2,4-D and the related phenoxy herbicide 2,4,5-T are rated as group 2B carcinogens (possible human carcinogens) by the IARC. Lymphatic cancers, particularly non-Hodgkin lymphoma (NHL), have been associated in Swedish agricultural workers with exposure to a commercial mixture of 2,4-D and 2,4,5-T (similar to the herbicide Agent Orange used by the US military in Viet Nam during the years 1965 to 1971). Possible carcinogenicity is often ascribed to contamination of 2,4,5-T with 2,3,7,8-tetrachloro-dibenzo-p-dioxin. However, a US National Cancer Institute research group reported a risk of 2.6 for adult NHL among Kansas residents exposed to 2,4-D alone, which is not thought to be dioxin-contaminated.
Dalapon-Na can cause depression, an unbalanced gait, decreased body weight, kidney and liver changes, thyroid and pituitary dysfunctions, and contact dermatitis in workers who are exposed. Diallate has dermal toxicity and causes irritation to the skin, eyes and mucous membranes. Diquat is an irritant to the skin, eyes and upper respiratory tract. It can cause a delay in the healing of cuts and wounds, gastrointestinal and respiratory disturbances, bilateral cataract and functional liver and kidney changes.
Dinoseb presents dangers because of its toxicity through dermal contact. It can cause moderate skin and pronounced eye irritation. The fatal dose for humans is about 1 to 3 g. After an acute exposure, Dinoseb causes central nervous system disturbances, vomiting, reddening (erythema) of the skin, sweating and high temperature. Chronic exposure without protection results in decreased weight, contact (toxic or allergic) dermatitis and gastrointestinal, liver and kidney disturbances. Dinoseb is not used in many countries because of its serious adverse effects.
Fluometuron is a moderate skin sensitizer in guinea-pigs and humans. It has been observed to cause decreased body weight, anaemia, and liver, spleen and thyroid gland disturbances. The biological action of diuron is similar.
Linuron causes mild irritation to the skin and eyes, and has low cumulative toxicity (threshold value after single inhalation 29 mg/m3). It causes CNS, liver, lung and kidney changes in experimental animals, as well as thyroid dysfunction.
MCPA is highly irritant to skin and mucous membranes, has low cumulative toxicity and is embryotoxic and teratogenic in high doses in rabbits and rats. Acute poisoning in humans (an estimated dose of 300 mg/kg) results in vomiting, diarrhoea, cyanosis, mucus burns, clonic spasms, and myocardium and liver injury. It provokes severe contact toxic dermatitis in workers. Chronic exposure without protection results in dizziness, nausea, vomiting, stomach aches, hypotonia, enlarged liver, myocardium dysfunction and contact dermatitis.
Molinate can reach a toxic concentration after single inhalation of 200 mg/m3 in rats. It causes liver, kidney and thyroid disturbances, and is gonadotoxic and teratogenic in rats. It is a moderate skin sensitizer in humans.
Monuron in high doses can result in liver, myocardium and kidney disturbances. It causes skin irritation and sensitization. Similar effects are shown by monolinuron, chloroxuron, chlortoluron and dodine.
Nitrofen is a strong skin and eye irritant. Chronic occupational exposure without protection results in CNS disturbances, anaemia, raised temperature, decreased body weight, fatigue and contact dermatitis. It is considered a possible human carcinogen (group 2B) by the IARC.
Paraquat has dermal toxicity and irritant effects on skin or mucous membranes. It causes nail damage and nose bleeding in occupational conditions without protection. Accidental oral poisoning with paraquat has resulted when it was left within reach of children or transferred from the original container into a bottle used for a beverage. Early manifestations of such intoxication are corrosive gastrointestinal effects, renal tubular damage and liver dysfunction. Death is due to circulatory collapse and progressive pulmonary damage (pulmonary oedema and haemorrhage, intra-alveolar and interstitial fibrosis with alveolitis and hyaline membranes), clinically revealed by dyspnoea, hypoxaemia, basal rales and roentgenographic evidence of infiltration and athelectasis. The renal failure is followed by lung damage, and accompanied in some cases by liver or myocardium disturbances. Mortality is higher with poisoning from liquid concentrate formulations (87.8%), and lower from granular forms (18.5%). The fatal dose is 6 g paraquat ion (equivalent to 30 ml Gramoxone or 4 packets of Weedol), and no survivors are reported at greater doses, irrespective of the time or vigour of treatment. Most survivors had ingested less than 1 g paraquat ion.
Potassium cyanate is associated with high inhalation and dermal toxicity in experimental animals and humans due to the metabolic conversion to cyanide, which is discussed elsewhere in this Encyclopaedia.
Prometryn exhibits moderate dermal toxicity and skin and eye irritation. It provokes decreased clotting and enzyme abnormalities in animals and has been found to be embryotoxic in rats. Exposed workers may complain of nausea and sore throat. Analogous effects are shown by propazine and desmetryne.
Propachlor’s toxicity is doubled at high environmental temperatures. Skin and mucous membrane irritation and mild skin allergy are associated with exposure. The toxic concentration after single inhalation is 18 mg/m3 in rats, and it is thought to exhibit moderate cumulative toxicity. Propachlor causes polyneuropathies; liver, myocardium and kidney disturbances; anaemia; and damage to testes in rats. During spraying from the air, the concentration in the spray cabin has been found to be about 0.2 to 0.6 mg/m3. Similar toxic properties are shown by propanil.
Propham exhibits moderate cumulative toxicity. It causes haemodynamic disturbances, and liver, lung and kidney changes are found in experimental animals.
Simazine causes slight irritation of the skin and mucous membranes. It is a moderate skin sensitizer in guinea-pigs. It also causes CNS, liver and kidney disturbances and has mutagenic effect in experimental animals. Workers may complain of weariness, dizziness, nausea and olfactory deviations after application without protective equipment.
2,4,5-T causes pronounced irritation and embryotoxic, teratogenic and carcinogenic effects in animals; there are also data on its gonadotoxic action in women. Because the extremely toxic chemical dioxin can be a contaminant of the trichlorophenoxy acids, use of 2,4,5-T is prohibited in many countries. Agricultural, forestry and industrial workers exposed to mixtures of 2,4-D and 2,4,5-T have been reported at increased risk for both soft-tissue sarcomas and non-Hodgkin lymphomas.
Trifluralin causes slight irritation of skin and mucous membranes. An increased incidence of liver carcinoma has been found in hybrid female mice, probably due to contamination with N-nitroso compounds. Trifluralin causes anaemia and liver, myocardium and kidney changes in experimental animals. Extensively exposed workers have developed contact dermatitis and photodermatitis.
Fungicides
Some fungi, such as rusts, mildews, moulds, smuts, storage rots and seedling blights, are able to infect and cause diseases in plants, animals and humans. Others can attack and destroy non-living materials such as wood and fibre products. Fungicides are used to prevent these diseases and are applied by spraying, dusting, seed dressing, seedling and soil sterilization, and fumigation of warehouses and greenhouses.
Fungi causing plant diseases can be arranged into four sub-groups, which differ by the microscopic characters of the mycelium, the spores and the organs on which the spores were developed:
1. phycomycetes—soil-borne organisms causing club rot of brassicae, wart diseases of potatoes and so on
2. ascomycetes—perithecia-forming powdery mildews and fungi causing apple scab, black currant leaf spot and rose black spot
3. basidiomycetes, including loose smut of wheat and barley, and several rusts species
4. fungi imperfecti, which includes the genera Aspergillus, Fusarium, Penicillium and so on, that are of great economic importance because they cause significant losses during plant growth, at harvest, and after harvest. (e.g., Fusarium species infect barley, oats and wheat; Penicillium species cause brown rot of pomaceous fruit).
Fungicides have been used for centuries. Copper and sulphur compounds were the first to be used, and Bordeaux mixture was applied in 1885 to vineyards. A great number of widely differing chemical compounds with fungicidal action are used in many countries.
Fungicides can be classified into two groups according to their mode of action: protective fungicides (applied at a time prior to the arrival of the fungal spores—e.g., sulphur and copper compounds) or eradicant fungicides (applied after the plant has become infected—e.g., mercury compounds and nitroderivatives of the phenols). The fungicides either act on the surface of the leaves and seeds or penetrate into the plant and exert their toxic action directly on the fungi (systemic fungicides). They can also alter the physiological and biochemical processes in the plant and thus produce artificial chemical immunization. Examples of this group are the antibiotics and the rodananilides.
Fungicides applied to seed act primarily against surface-borne spores. However, in some cases they are required to persist on the seed coat long enough to be effective against the dormant mycelium contained within the seed. When applied to the seed before sowing, the fungicide is called seed disinfectant or seed dressing, though the latter term may include treatment not intended to counter seed-borne fungi or soil pests. To protect wood, paper, leather and other materials, fungicides are used by impregnation or staining. Special drugs with fungicidal action are also used to control fungal diseases in humans and animals.
Specific field applications include:
- Seed dressing. This is a simple and economically efficient method for the control of plant diseases. The pests are destroyed on the seeds and in the soil during the development of the seed. Despite the availability of efficient alternative compounds, the mercury fungicides are still used to a considerable extent for this purpose. Dithiocarbamates, and particularly thiuram, are widely used. Chloranil and dichlone of the quinone group, hexachlorobenzene, formaldehyde and some antibiotics are also used for seed dressing. The seeds can be treated by either the dry or the wet method.
- Soil disinfection. This is a more general action, with fungicides incorporated into the soil as solid or liquid formulations that liberate volatile or easily soluble components (e.g., chloropicrin, methyl bromide, dibromomethane, formaldehyde, vapam, dazomet, allyl alcohol, pentachloronitrobenzene and chloroneb). These fungicides are used most intensively on greenhouse soil. Several of them are known or suspected carcinogens.
- Application on plants. To control airborne diseases, fungicides are used on annual field crops, fruit trees and berry crops. Almost all fungicide groups are used for this purpose. Copper compounds, dithiocarbamates, aromatic nitro derivatives, quinones, phthalamides, guanidines and chlorinated hydrocarbons are the most frequently used; some heterocyclics, nickel compounds and some antibiotics are also used.
Hazards of fungicides
The fungicides cover a great variety of chemical compounds differing widely in their toxicity. Highly toxic compounds are used as fumigants of foods and warehouses, for seed dressing and for soil disinfection, and cases of poisoning have been described with organomercurials, hexachlorobenzene and pentachlorobenzene, as well as with the slightly toxic dithiocarbamates. These and several other chemicals are discussed in more detail elsewhere in this article, chapter and Encyclopaedia. Some are briefly reviewed here.
Chinomethionate has a high cumulative toxicity and inhibits thiol groups and some enzymes containing them; it lowers phagocytic activity and has antispermatogenic effects. It is irritant to the skin and the respiratory system. It can damage the CNS, the liver and the gastrointestinal tract. Glutathione and cysteine provide protection against the acute effects of chinomethionate.
Chloranil is irritating to the skin and the upper respiratory tract; it can also cause depression of the CNS and dystrophic changes in the liver and kidney. The biological monitoring of exposed persons has shown an increased level of the urinary phenols, both free and bound.
Dazomet is used also as a nematocide and a slimicide. This compound and its decomposition products are sensitizers and mild irritants of the eye, nose, mouth and skin. Poisoning is characterized by a variety of symptoms, including anxiety, tachycardia and quick breathing, hypersalivation, clonic cramps, impaired movement coordination, sometimes hyperglycaemia and cholinesterase inhibition. The main pathomorphological findings are enlargement of the liver and degenerative changes of the kidney and other internal organs.
Dichlofluanid inhibits thiol groups. In experimental animals it caused histological changes in liver, proximal tubules of the kidney and adrenal cortex, with the reduction of the lymphatic tissue in the spleen. It is a moderate irritant of the skin and mucous membranes.
Diclone, in addition to sharing the irritant and blood depressant properties common to quinones, is an experimental animal carcinogen.
Dinobuton, like dinitro-o-cresol (DNOC), disturbs cell metabolism by inhibiting oxidative phosphorylation, with the loss of energy-rich compounds such as adenosintriphosphoric acid (ATP). It can cause severe liver dystrophy and necrosis of the convoluted tubules of the kidneys. The clinical manifestations of the intoxication are high temperature, methaemoglobinaemia and haemolysis, nervous disturbances and irritation of the skin and mucous membranes.
Dinocap can increase the blood level of alkaline phosphatase and is a moderate irritant of the skin and mucous membranes. It produces distrophic changes in the liver and kidney, and hypertrophy of the myocardium. In acute poisoning, disturbances in thermoregulation, clonic cramps and breathing difficulties have been observed.
Hexachlorobenzene (HCB) is stored in the body fat. It interferes with porphyrin metabolism, increasing the urinary excretion of coproporphyrins and uroporphyrins; it increases also the levels of transaminases and dehydrogenases in the blood. It can produce liver injury (hepatomegaly and cirrhosis), photosensitization of the skin, a porphyria similar to porphyria cutanea tarda, arthritis and hirsutism (monkey disease). It is a skin irritant. Chronic poisoning needs long-term treatment, mainly symptomatic, and it is not always reversible on cessation of exposure. It is classified as a possible human carcinogen (group 2B) by the IARC.
Milneb can cause gastrointestinal disturbances, weakness, decrease of the body temperature and leukopoenia.
Nirit has haemotoxic properties and causes anaemia and leucocytosis with toxic granulation of the leucocytes, in addition to degenerative changes in the liver, spleen and kidneys.
Quinones, in general, cause blood disturbances (methaemoglobinaemia, anaemia), affect the liver, disturb vitamin metabolism, particularly that of ascorbic acid, and are irritant to the respiratory ways and the eye. Chloranil and dichlone are the quinone derivatives most widely used as fungicides.
Thiabendazole has caused thymus involution, colloid depletion in the thyroid and increase in liver and kidney size. It is also used as an anthelmintic in cattle.
Safety and Health Measures
Labelling and storage
The requirements regarding the labelling of pesticides laid down in national and international legislation should be strictly applied to both imported and locally produced chemicals. The label should give the following essential information: both the approved name and the trade name of the chemical; the name of the manufacturer, packager or supplier; the directions for use; the precautions to be taken during use, including details of protective equipment to be worn; the symptoms of poisoning; and the first-aid treatment for suspected poisoning.
The greater the degree of toxicity or hazard of the chemical, the more precise should be the wording on the label. It is sound practice for the different classes to be clearly distinguished by background colours on the label and, in the case of compounds of high or extreme hazard, for the appropriate danger symbol to be incorporated. It often occurs that an adequately labelled quantity of pesticide in bulk is locally repacked into smaller containers. Each such small package should bear a similar label, and repacking in containers which have held, or are easily identifiable with, containers used for food should be absolutely forbidden. If small packages are to be transported, the same rules apply as for the carriage of larger packages. (See the chapter Using, storing and transporting chemicals.)
Pesticides of moderate or higher hazard should be so stored that only authorized persons can have access to them. It is particularly important that children should be excluded from any contact with pesticide concentrates or residues. Spillages often occur in storage and repacking rooms, and they must be cleaned up with care. Rooms used only for storage should be soundly constructed and fitted with secure locks. Floors should be kept clear and the pesticides clearly identified. If repacking is carried out in storage rooms, adequate ventilation and light should be available; floors should be impervious and sound; washing facilities should be available; and eating, drinking and smoking should be prohibited in the area.
A few compounds react with other chemicals or with air, and this has to be taken into account when planning storage facilities. Examples are cyanide salts (which react with acid to produce hydrogen cyanide gas) and dichlorvos (which vaporizes in contact with air). (Dichlorvos is classified as a group 2B possible human carcinogen by the IARC.).
Mixing and application
Mixing and application may comprise the most hazardous phase of the use of pesticides, since the worker is exposed to the concentrate. In any particular situation, only selected persons should be responsible for mixing; they should be thoroughly conversant with the hazards and provided with the proper facilities for dealing with accidental contamination. Even when the mixed formulation is of such a toxicity that it can be used with a minimum of personal protective equipment (PPE), more elaborate equipment may need to be provided for and used by the mixer.
For pesticides of moderate or higher hazard, some type of PPE is almost always necessary. The choice of particular items of equipment will depend on the hazard of the pesticide and the physical form in which it is being handled. Any consideration of PPE must also include not only provision but also adequate cleaning, maintenance and replacement.
Where climatic conditions preclude the use of some types of PPE, three other principles of protection can be applied—protection by distance, protection by time and protection by change of working method. Protection by distance involves modification of the equipment used for application, so that the person is as far away as possible from the pesticide itself, bearing in mind the likely routes of absorption of a specific compound.
Protection by time involves limitation of hours of work. The suitability of this method depends on whether the pesticide is readily excreted or whether it is cumulative. Accumulation of some compounds occurs in the body when the rate of excretion is slower than the rate of absorption. With some other compounds, a cumulative effect may occur when the person is exposed to repeated small doses which, taken individually, may not give rise to symptoms.
Protection by change of working method involves a reconsideration of the whole operation. Pesticides differ from other industrial processes in that they can be applied from the ground or the air. Changes of method on the ground depend largely on the choice of equipment and the physical nature of the pesticide to be applied.
Pesticides that are applied from the air can be in the form of liquids, dusts or granules. Liquids may be sprayed from very low altitudes, frequently as fine droplets of concentrated formulations, known as ultra-low volume (ULV) applications. Drift is a problem particularly with liquids and dusts. Aerial application is an economical way of treating large tracts of land but entails special hazards to pilots and to workers on the ground. Pilots can be affected by leakage from hoppers, by pesticides carried into the cockpit on clothes and boots, and by flying back through the swathe just released or through the drift from the swathe. Even minor degrees of absorption of some pesticides or their local effects (such as may be caused, for instance, by an organophosphorus compound in the eye) can affect a pilot to the extent that he or she cannot maintain the high degree of vigilance necessary for low flying. Pilots should not be allowed to engage in pesticide operations unless they have been specially trained in the items listed above, in addition to any special aviation and agricultural operational requirements.
On the ground, loaders and flaggers may be affected. The same principles apply to loaders as to others dealing with pesticides in bulk. Flaggers mark the swathe to be flown and can be severely contaminated if the pilot misjudges the moment of release. Balloons or flags can be placed in position before or ahead of the operation, and workers should never be used as flaggers within the flight pattern.
Other restrictions
The hazards associated with pesticides do not end with their application; with the more toxic compounds it has been shown that there is a danger to workers entering a sprayed crop too soon after application. It is therefore important that all workers and members of the general public should be informed concerning the areas where a toxic pesticide has been applied and the earliest date on which it is safe to enter and work in these areas. Where a food crop has been sprayed, it is also important that the crop not be harvested until a sufficient period has elapsed for degradation of the pesticide to take place, in order to avoid excessive residues on food.
Disposal of pesticides and containers. Spillage of pesticides at any stage of their storage or handling should be treated with great care. Liquid formulations may be reduced to solid phase by evaporation. Dry sweeping of solids is always hazardous; in the factory environment, these should be removed by vacuum cleaning or by dissolving them in water or other solvent. In the field they may be washed away with water into a suitable soak-hole. Contaminated topsoil should be removed and buried if any domestic animals or fowls are in the area. Soak-holes should be used for disposing of washing waters from cleaning application equipment, clothing or hands. These should be at least 30 cm deep and sited well away from wells or watercourses.
Empty pesticide containers should be collected with care, or disposed of safely. Plastic liners, and paper or card containers should be crushed and buried well below the topsoil or burned, preferably in an incinerator. Metal containers of some pesticides can be decontaminated according to the instructions of the pesticide manufacturers. Such drums should be clearly marked “Not to be used for food or for water for drinking or domestic use”. Other metal containers should be punctured, crushed or buried.
Hygiene and first aid
Where a pesticide is of moderate or higher hazard and can be readily absorbed through the skin, special precautions are necessary. In some situations where workers may become accidentally contaminated with large quantities of concentrate, such as in factory situations and mixing, it is necessary to provide a shower bath in addition to the usual washing facilities. Special arrangements for cleaning clothing and overalls may be necessary; in any case, these should not be left for the worker to wash at home.
Since pesticides are often applied outside the factory environment, depending on the chemical used, special care may have to be taken to provide washing facilities at the workplace, even though this may be in remote fields. Workers must never bathe themselves in canals and rivers, the water from which may be subsequently used for other purposes; the washing water provided should be disposed of with care as outlined above. Smoking, eating and drinking before washing should be absolutely prohibited when any pesticide of moderate or higher toxicity is being handled or used.
Where an antidote exists which can be readily used as a first-aid measure for a specific pesticide (e.g., atropine for organophosphorus poisoning), it should be readily available to workers, who should be instructed in the method of its use. When any pesticide is being used on a substantial scale, medical personnel in the area should be informed by the persons responsible for distribution. The nature of the chemical used should be well defined so that medical facilities can be equipped and will know the specific antidotes, where these are applicable and how to recognize cases of poisoning. Facilities should also be available in order to make proper differential diagnosis, even if these are of the simplest type, such as test papers for determining cholinesterase levels. Strict routine medical supervision of workers heavily exposed to concentrates, as in the manufacture and packing of pesticides, is essential and should include laboratory tests and routine surveillance and record keeping.
Training
While all workers using pesticide formulations of moderate or higher hazard should be thoroughly trained in their use, such training is particularly important if the pesticide is extremely toxic. Training programmes must cover: toxicity of compounds used and routes of absorption; handling of concentrates and formulations; methods of use; cleaning of equipment; precautions to be taken and PPE to be worn; maintenance of PPE; avoidance of contamination of other crops, foods and water supplies; early symptoms of poisoning; and first-aid measures to be taken. All training should be strictly relevant to the pesticide actually being used, and, in the case of extremely hazardous compounds, it is wise to license operators following an examination to show that they have, in fact, a good understanding of the hazards and the procedures to be followed.
Public health measures
When pesticides are used, every effort must be made to avoid contamination of water supplies, whether these are officially recognized supplies or not. This not only concerns the actual application (when there may be immediate contamination) but must also include consideration of remote contamination by run-off through rainfall on recently treated areas. While pesticides in natural watercourses may be diluted to such a degree that the contaminated water may not be hazardous in itself, the effect on fish, on water vegetables used as food and grown in the watercourses, and on wild life as a whole must not be overlooked. Such hazards may be economic rather than directly related to health, but are no less important.
Agricultural Chemicals
Agricultural chemicals are usually defined as pesticides, fertilizers and health products. The US Environmental Protection Agency (EPA) defines pesticides as any materials manufactured or formulated to kill a pest. This means that herbicides, fungicides, insecticides and miticides are pesticides. Fertilizers are nutrient chemicals that enhance the growth of the plant. The important elements in the fertilizers are nitrogen, phosphorus and potassium. Nitrogen is usually in the form of ammonia, ammonium nitrate, ammonium sulphate, ammonium phosphate or solutions of these materials. Other nitrogen-containing chemicals are used for some special nutrient needs. Ammonium phosphate is the normal source of phosphorous. Potash (potassium oxide) is the potassium nutrient. Animal health products are any chemicals that are used to promote the health or growth of an animal. This includes products that are used topically by drenching or pouring-on, orally as a tablet or gel, and injectibles.
Pesticides
The most significant development in the pesticide manufacturing industry has been the introduction of the environmentally friendly pesticides. The imidazolinone family of herbicides has been a benefit to soybean and other field crops, as the herbicides are much more effective pound for pound; are less toxic to humans, animals and fish; have less persistence in the soil; and are formulated using water instead of flammable solvents, as compared to the old generation nitroaromatics. Concurrent with these innovations is the development of imidazolinones-resistant seeds that can be protected from weed growth. Corn is in the forefront in this area and has been successfully grown, protected by the imidazolinones. This also makes carry-over from year to year of the herbicide an insignificant problem, as in many areas soybeans and corn are rotated.
A newer development is the production of the synthetic pyrethroids, which are broad-range pesticides. These products are effective pesticides and are less toxic to animals and humans than the old organophosphates and carbamates. They are activated by the insect’s biological system and therefore not a danger to vertebrates. They are also less persistent in the environment, as they are biodegradable.
There have also been developments in the use of the old generation pesticides and herbicides. Herbicide formulations have been developed that utilize water dispersion technology that eliminates the use of volatile solvents. This not only reduces the amount of volatile organic chemicals that go to the atmosphere, but also makes handling, storage, formulation and transportation much safer. In the area of pesticides, a superior method of handling the toxic pesticides has been developed that uses closed container transfer of the material from the package to the spreader, called “Lock-N-Load”. This reduces the chances of exposure to these toxic materials. Organophosphates are still being used successfully to help eradicate health problems such as malaria and river blindness. Some of the less toxic organophosphates are effective in the treatment of animals for insects, worms and mites by direct application to the skin using pour-on or aerosol formulations.
The pesticide industry is regulated by many countries, and labelling, application to plants and soil, training in pesticide use, and transportation are controlled. Many pesticides can only be spread by licensed applicators. Precautions during pesticide application are discussed elsewhere in this Encyclopaedia. Bulk transportation vehicles can only be operated by qualified drivers. The producers of pesticide have a legal obligation to provide safe handling and application methods. This is usually accomplished by providing comprehensive labelling, training and material safety data sheets (MSDSs) (see the chapter Using, storing and transporting chemicals).
Another problem is the disposal of empty containers. It is not advisable, and in many places it is illegal, to reuse pesticide containers. Many advances have been made to mitigate this problem. Plastic containers have been collected by the distributors and reprocessed into plastic pipe. Bulk, refillable containers have been used. With the advent of the wettable powders and water-based dispersions, triple rinsing the container into the solutions tank gives the applicator a method to decontaminate the container before landfilling or recycling. Hand lances with spray nozzles that can pierce the container are used to assure proper cleaning and the destruction of the container so that it can not be reused.
Pesticides are made to kill; therefore, care is necessary to handle them safely. Some of the problems have been lessened by the product advances. In most cases, copious quantities of water are the best first-aid treatment for superficial exposures to skin and eyes. For ingestion, it is best to have a specific antidote available. It is important that the nearest health facility know what is being used and have a supply of the appropriate antidote on hand. For instance, organophosphates and carbamates cause cholinesterase inhibition. Atropine, the specific antidote for the treatment of this reaction, should be available wherever these pesticides are used.
For further discussion of pesticides, see the eponymous article in this chapter.
Fertilizers
Ammonia is the base of most important fertilizers. The major fertilizers are ammonia itself, ammonium nitrate, urea, ammonium sulphate and ammonium phosphate. There appears to be an environmental problem associated with nitrogen use, as the ground water in many farming areas is contaminated with nitrates, which causes health problems when the water is consumed as drinking water. There are pressures for farmers to use less fertilizer and to rotate crops of nitrogen-using legumes such as soy beans and rye grass. Ammonium nitrate, an oxidizer, is explosive if heated. The dangers of ammonium nitrate as a blasting agent were demonstrated by the destruction of a US federal building in Oklahoma City, Oklahoma, in 1995. There is some movement to add inert ingredients to make fertilizer-grade ammonium nitrate detonation-resistant. An industrial explosion resulting in multiple fatalities which occurred in an ammonium nitrate solutions plant that was thought to be safe from detonation because the ammonium nitrate was handled as an 85% solution is anonther example. Investigation results indicated that an intricate condition of temperature and contamination caused the incident. These conditions would not exist in the retail or farming sector. Anhydrous ammonia is a moderately toxic gas at room temperature and must be kept under pressure or refrigeration during storage and use. It is a skin, eye and respiratory irritant, can cause burns, and is flammable. It is directly applied to the soil or used as an aqueous solution. There is significant anhydrous ammonia storage in many farming areas. A hazardous condition is created if the storage is not managed correctly. This should include monitoring for leaks and emergency leak procedures.
Animal Health Products
The development and marketing of bovine somatotropin (BST) has caused controversy. BST, a fermentation product, raises the productivity of milk cows by 10 to 20%. Many people are opposed to the product because it introduces a chemical into the production of milk. However, the BST milk is indistinguishable from ordinary milk since BST is produced naturally by the milk cow. A problem seems to be an increase in infections of the cow’s udder. Antibiotics for these infections are available, but the use of these antibiotics is also controversial. The important benefits of BST are the increased production of milk with a reduction in food consumption and a similar reduction in cow manure, a material that is a solid-waste problem in many areas. A similar product, porcine somatotropin (PST), is still in the testing stage. It produces bigger hogs quickly, utilizing less feed, and results in pork containing less fat.
Antibiotic use in the beef-raising industry is also causing controversy. There is fear that consumption of large amounts of beef will result in hormonal problems in humans. There has been little in the way of confirmed problems, but the concern persists. Animal health products have been developed that control worms in animals. The previous generation was a synthetic chemical product, but the new generation products are the result of biological fermentation technology. These products are effective in many types of animals at very low use levels, and include domestic pets in their protection arena. These products are very toxic to aquatic life, though, so much care must be taken to avoid contamination of creeks and streams. These materials do biodegrade, so there appear to be no long-term or residual aquatic problems.
Manufacture of Agricultural Chemicals
The manufacturing of agricultural chemicals entails many processes and raw materials. Some agricultural chemicals are batch chemical syntheses that involve exothermic reactions where temperature control and emergency relief sizing are an issue. Hazard evaluations are necessary to assure that all the hazards are discovered and addressed. Hazard and operability studies (HAZOP) are recommended for conducting reviews. Relief sizing must be conducted using Design Institute for Emergency Relief Systems (DIERS) technology and data from calorimetric equipment. Usually, because of the complexity of the molecules, the production of agricultural chemicals involves many steps. Sometimes there is considerable aqueous and organic liquid waste. Some of the organics may be recyclable, but most of the aqueous waste must be biologically treated or incinerated. Both methods are difficult because of the presence of organic and inorganic salts. The previous generation herbicides, because they involved nitrations, were produced using continuous reactors to minimize the quantities of the nitrated materials at reaction temperatures. Severe runaway reactions, resulting in property damage and injuries, have occurred when batch reactors of nitrated organics have been subjected to a temperature excursion or contamination.
Many modern pesticide products are dry powders. If the concentration, particle size, oxygen concentration and a source of ignition are present at the same time, a dust explosion can occur. The use of inerting, the exclusion of oxygen, and utilization of nitrogen or carbon dioxide minimizes the oxygen source and can make the processes safer. These dusts may also be an industrial hygiene issue. Ventilation, both general and local, is a solutions to these problems.
The major fertilizers are made continuously rather than by the batch process. Ammonia is made by reforming methane at high temperatures utilizing a specific catalyst. Carbon dioxide and hydrogen are also formed and must be separated from the ammonia. Ammonium nitrate is made from ammonia and nitric acid in a continuous reactor. The nitric acid is formed by the continuous oxidation of ammonia on a catalytic surface. Ammonium phosphate is a reaction of ammonia and phosphoric acid. Phosphoric acid is made by reacting sulphuric acid with phosphate -containing ores. Sulphuric acid is formed by burning sulphur to sulphur dioxide, and catalytically converting the sulphur dioxide continuously to sulphur trioxide, and then adding water to form the sulphuric acid. Urea is a continuous high-pressure reaction of carbon dioxide and ammonia, the carbon dioxide usually coming from the ammonia continuous reaction by-product.
Many of these raw materials are toxic and volatile. Release of the raw materials or finished products, through an equipment failure or operator error, can expose employees and others in the community. A detailed emergency response plan is a necessary tool to minimize the effects of a release. This plan should be developed by determining a credible worst-case event through hazard evaluations and then forecasting consequences using dispersion modelling. This plan should include a method to notify employees and the community, an evacuation plan, emergency services and a recovery plan.
Transportation of agricultural chemicals should be thoroughly investigated to choose the safest route—one that minimizes the exposures if an incident occurs. A transportation emergency response plan should be implemented to address transportation incidents. This plan should include a published emergency response telephone number, company personnel to respond to calls and, in some cases, an accident site emergency response team.
Fermentation is the method of producing some of the animal health products. Fermentation is usually not a hazardous process, as it involves growing a culture using a nutritional medium such as lard oil, glucose, or starch. Sometimes anhydrous ammonia is used for pH (acidity) control or as a nutrient, so the process can involve hazards. Solvents may be used to extract the active cells, but the quantities and the methodology are such that is can be done safely. Recycling these solvents is often part of the process.
Minerals
Adapted from 3rd edition, Encyclopaedia of Occupational Health and Safety. Revision includes information from A. Bruusgaard, L.L. Cash, Jr., G. Donatello, V. D’Onofrio, G. Fararone, M. Kleinfeld, M. Landwehr, A. Meiklejohn, J.A. Pendergrass, S.A. Roach, T.A. Roscina, N.I. Sadkovskaja and R. Stahl.
Minerals are used in ceramics, glass, jewellery, insulation, stone carving, abrasives, plastics and numerous other industries in which they present primarily an inhalation hazard. The amount and type of impurities within the minerals may also determine the potential hazard associated with inhalation of the dust. The major concern during mining and production is the presence of silica and asbestos. The silica content in different rock formations, such as sandstone, feldspars, granite and slate, may vary from 20% to nearly 100%. It is therefore imperative that worker exposure to dust concentrations be kept to a minimum by the implementation of strict dust-control measures.
Improved engineering controls, wet drilling, exhaust ventilation and remote handling are recommended to prevent the development of lung disease in mineral workers. Where effective engineering controls are not possible, workers should wear approved respiratory protection, including the proper selection of respirators. Where possible, industrial substitution of less hazardous agents can reduce occupational exposure. Finally, the education of workers and employers regarding the hazards and proper control measures is an essential component of any prevention programme.
Regular medical examinations of mineral-dust-exposed workers should include evaluations for respiratory symptoms, lung function abnormalities and neoplastic disease. Workers showing the first signs of lung changes should be assigned to other jobs entailing no dust hazards. In addition to individual reports of illness, data from groups of workers should be collected for prevention programmes. The chapter Respiratory system provides more detail on the health effects of several of the minerals described here.
Apatite (Calcium Phosphate)
Occurrence and uses. Apatite is a natural calcium phosphate, usually containing fluorine. It occurs in the earth’s crust as phosphate rock, and it is also the chief component of the bony structure of teeth. Deposits of apatite are located in Canada, Europe, the Russian Federation and the United States.
Apatite is used in laser crystals and as a source of phosphorus and phosphoric acid. It is also employed in the manufacture of fertilizers.
Health hazards. Skin contact, inhalation or ingestion may cause irritation of skin, eyes, nose, throat or gastric system. Fluorine may be present in the dust and may cause toxic effects.
Asbestos
Occurrence and uses. Asbestos is a term used to describe a group of naturally occurring fibrous minerals which are widely distributed throughout the world. The asbestos minerals fall into two groups—the serpentine group, which includes chrysotile, and the amphiboles, which include crocidolite, tremolite, amosite and anthophyllite. Chrysotile and the various amphibole asbestos minerals differ in crystalline structure, in chemical and surface characteristics, and in the physical characteristics of their fibres.
The industrial features which have made asbestos so useful in the past are the high tensile strength and flexibility of the fibres, and their resistance to heat and abrasion and to many chemicals. There are many manufactured products which contain asbestos, including construction products, friction materials, felts, packings and gaskets, floor tiles, paper, insulation and textiles.
Health hazards. Asbestosis, asbestos-related pleural disease, malignant mesothelioma and lung cancer are specific diseases associated with exposure to asbestos dust. The fibrotic changes which characterize the pneumoconiosis, asbestosis, are the consequence of an inflammatory process set up by fibres retained in the lung. Asbestos is discussed in the chapter Respiratory system.
Bauxite
Occurrence and uses. Bauxite is the principal source of aluminium. It consists of a mixture of minerals formed by the weathering of aluminium-bearing rocks. Bauxites are the richest form of these weathered ores, containing up to 55% alumina. Some lateritic ores (containing higher percentages of iron) contain up to 35% Al2O3. The commercial deposits of bauxite are mainly gibbsite (Al2O3 3H2O) and boehmite (Al2O3 H2O), and are found in Australia, Brazil, France, Ghana, Guinea, Guyana, Hungary, Jamaica and Surinam. Gibbsite is more readily soluble in sodium hydroxide solutions than boehmite, and is therefore preferred for alumina production.
Bauxite is extracted by open-cast mining. The richer ores are used as mined. The lower-grade ores may be upgraded by crushing and washing to remove clay and silica waste.
Health hazards. Severe pulmonary disability has been reported in workers employed on smelting bauxite that is combined with coke, iron and very small amounts of silica. The affliction is known as “Shaver’s disease”. Because silica contamination of aluminium-containing ores is common, the health hazards associated with the presence of free crystalline silica in bauxite ores must be considered an important causal factor.
Clays (Hydrated Aluminium Silicates)
Occurrence and uses. Clay is a malleable plastic material formed by the weathered disintegration residues of argillaceous silicate rock; it usually contains 15 to 20% water and is hygroscopic. It occurs as a sediment in many geological formations in all parts of the world and contains in varying amounts feldspars, mica and admixtures of quartz, calcspar and iron oxide.
The quality of clay depends on the amount of alumina in it—for example, a good porcelain clay contains about 40% alumina, and the silica content is as low as 3 to 6%. On average the quartz content of clay deposits is between 10 and 20%, but at worst, where there is less alumina than usual, the quartz content may be as high as 50%. Content may vary in a deposit, and separation of grades may take place in the pit. In its plastic state, clay can be moulded or pressed, but when fired it becomes hard and retains the shape into which it has been formed.
Clay is often extracted in open-cast pits but sometimes in underground mines. In open-cast pits the method of extraction depends on the quality of the material and the depth of the deposit; sometimes the conditions require the use of hand-operated pneumatic tools, but, wherever possible, mining is mechanized, using excavators, power shovels, clay cutters, deep digging machines and so on. The clay is taken to the surface by truck or cable transport. The clay brought to the surface may be subjected to preliminary processing before dispatch (drying, crushing, pugging, mixing and so on) or it may be sold whole (see the chapter Mining and quarrying). Sometimes, as in many brickyards, the clay pit may be adjacent to the factory where the finished articles are made.
Different types of clay form the basic material in the manufacture of pottery, bricks and tiles, and refractories. Clay may be used without any processing in dam construction; in situ, it sometimes serves as a cover for gas stored in lower stratum. Appropriate ventilation and engineering controls are required.
Health hazards. Clays usually contain large amounts of free silica, and chronic inhalation can cause silicosis. Skin contact with wet clay may cause skin drying and irritation. There is a silicosis risk to underground workers where there is mechanized mining of clay with a high quartz content and little natural moisture. Here the decisive factor is not merely the quartz content but also the natural dampness: if the moisture level is less than 12%, much fine dust must be expected in mechanical extraction.
Coal
Occurrence and uses. Coal is a natural, solid, combustible material formed from prehistoric plant life. It occurs in layers or veins in sedimentary rocks. Conditions suitable for the natural formation of coal occurred between 40 and 60 million years ago in the Tertiary Age (brown-coal formation) and over 250 million years ago in the Carboniferous Age (bituminous-coal formation), when swampland forests thrived in a hot climate and then gradually subsided during ensuing geological movements. The main deposits of brown coal are found in Australia, eastern Europe, Germany, the Russian Federation and the United States. Major reserves of bituminous coal are located in Australia, China, India, Japan, the Russian Federation and the United States.
Coal is an important source of chemical raw materials. Pyrolysis or destructive distillation yields coal tar and hydrocarbon gases, which can be upgraded by hydrogenation or methanation to synthetic crude oil and fuel gas. Catalytic hydrogenation yields hydrocarbon oils and gasoline. Gasification produces carbon monoxide and hydrogen (synthetic gas), from which ammonia and other products can be made. While in 1900, 94% of the world’s energy requirements were met by coal and only 5% by petroleum and natural gas, coal has been increasingly replaced by liquid and gaseous fuels throughout the world.
Health hazards. Hazards of mining and of coal dust are discussed in the chapters Mining and quarrying and Respiratory system.
Corundum (Aluminium Oxide)
Occurrence and uses. Corundum is one of the principal natural abrasives. Natural corundum and artificial corundum (alundum or artificial emery) are usually relatively pure. The artificial material is produced from bauxite by smelting in an electric furnace. Because of its hardness, corundum is used to shape metals, wood, glass and ceramics, by a process of grinding or polishing. Health hazards are discussed elsewhere in this Encyclopaedia.
Diatomaceous Earth (Diatomite, Kieselguhr, Infusorial Earth)
Occurrence and uses. Diatomaceous earth is a soft, bulky material composed of skeletons of small, prehistoric aquatic plants related to algae (diatoms). Certain deposits comprise up to 90% free amorphous silica. They have intricate geometric forms and are available as light-coloured blocks, bricks, powder and so on. Diatomaceous earth absorbs 1.5 to 4 times its weight of water and has a high oil absorption capacity. Deposits occur in Algeria, Europe, the Russian Federation and the western United States. Diatomaceous earth may be used in foundries, in paper coating, in ceramics and in the maintenance of filters, abrasives, lubricants and explosives. It is used as a filtering medium in the chemical industry. Diatomaceous earth also finds use as a drilling-mud thickener; an extender in paints, rubber and plastic products; and as an anti-caking agent in fertilizers.
Health hazards. Diatomaceous earth is highly respirable. For many industrial purposes diatomaceous earth is calcined at 800 to 1,000 ºC to produce a greyish-white powder called kieselguhr, which may contain 60% or more crystobalite. During mining and processing of diatomaceous earth, the risk of death from both respiratory diseases and lung cancer has been related to the inhalation of dust as well as to cumulative crystalline silica exposures, as discussed in the chapter Respiratory system.
Erionite
Occurrence and uses. Erionite is a crystalline, fibrous zeolite. Zeolites, a group of alumino-silicates found in the cavities of volcanic rocks, are used in the filtration of hard water and in the refining of oil. Erionite occurs in California, Nevada and Oregon in the United States, and in Ireland, Iceland, New Zealand and Japan.
Health hazards. Erionite is a known human carcinogen. Chronic inhalation may cause mesothelioma.
Feldspar
Occurrence and uses. Feldspar is a general name for a group of sodium, potassium, calcium and barium aluminium silicates. Commercially, feldspar usually refers to the potassium feldspars with the formula KAlSi3O8, usually with a little sodium. Feldspar occurs in the United States. It is used in pottery, enamel and ceramic ware, glass, soaps, abrasives, cements and concretes. Feldspar serves as a bond for abrasive wheels, and it finds use in insulating compositions, tarred roofing materials and fertilizers.
Health hazards. Chronic inhalation may cause silicosis due to the presence of substantial amounts of free silica. Feldspars may also contain irritating sodium oxide (soda spars), potassium oxide (potash spars), and calcium oxide (lime spars) in insoluble form. See the section “Silica” below.
Flint
Occurrence and uses. Flint is a crystalline form of native silica or quartz. It occurs in Europe and the United States. Flint is used as an abrasive, a paint extender and a filler for fertilizer. In addition, it finds use in insecticides, rubber, plastics, road asphalt, ceramics and chemical tower packing. Historically, flint has been an important mineral because it was used to make some of the first known tools and weapons.
Health hazards are related to the toxic properties of silica.
Fluorspar (Calcium Fluoride)
Occurrence and uses. Fluorspar is a mineral that contains 90 to 95% calcium fluoride and 3.5 to 8% silica. It is extracted by drilling and blasting. Fluorspar is a principal source of fluorine and its compounds. It is used as a flux in open hearth steel furnaces and in metal smelting. In addition, it finds use in the ceramics, paint and optical industries.
Health hazards. The hazards of fluorspar are due primarily to the harmful effects of the fluorine content and its silica content. Acute inhalation may cause gastric, intestinal, circulatory and nervous system problems. Chronic inhalation or ingestion may cause loss of weight and appetite, anaemia, and bone and teeth defects. Pulmonary lesions have been reported among persons inhaling dust containing 92 to 96% calcium fluoride and 3.5% silica. It appears that calcium fluoride intensifies the fibrogenic action of silica in the lungs. Cases of bronchitis and silicosis have been reported among fluorspar miners.
In the mining of fluorspar, dust control should be carefully enforced, including wet drilling, watering of loose rock, and exhaust and general ventilation. When heating fluorspar, there is also the hazard of hydrofluoric acid being formed, and the relevant safety measures should be applied.
Granite
Occurrence and uses. The coarse-grained igneous rock granite consists of quartz, feldspar and mica in shapeless interlocking grains. It finds use as crushed granite and as dimension granite. After it is crushed to the required size, granite may be used for concrete aggregate, road metal, railroad ballast, in filter beds, and for riprap (large chunks) in piers and breakwaters. The colors—pink, grey, salmon, red and white—are desirable for dimension granite. The hardness, uniform texture and other physical properties make dimension granite ideal for monuments, memorials, foundation blocks, steps and columns.
Large production of crushed granite comes mainly from California, with substantial amounts from the other US States of Georgia, North Carolina, South Carolina and Virginia. Major production areas of dimension granite in the United States include Georgia, Maine, Massachusetts, Minnesota, North Carolina, South Dakota, Vermont, and Wisconsin.
Health hazards. Granite is heavily contaminated with silica. Therefore, silicosis is a major health hazard in granite mining.
Graphite
Occurrence and uses. Graphite is found in almost every country of the world, but the majority of production of the natural ore is limited to Austria, Germany, Madagascar, Mexico, Norway, the Russian Federation and Sri Lanka. Most, if not all, natural graphite ores contain crystalline silica and silicates.
Lump graphite is found in veins which cross different types of igneous and metamorphic rock containing mineral impurities of feldspar, quartz, mica, pyroxine, zircon, rutile, apatite and iron sulphides. The impurities are often in isolated pockets in the veins of ore. Mining is commonly underground, with hand drills for selective mining of narrow veins.
Deposits of amorphous graphite are also underground, but usually in much thicker beds than the veins of lumps. Amorphous graphite is commonly associated with sandstone, slate, shale, limestone and adjunct minerals of quartz and iron sulphides. The ore is drilled, blasted and hand-loaded into wagons and brought to the surface for grinding and impurity separation.
Flake graphite is usually associated with metamorphosed sedimentary rock such as gneiss, schists and marbles. The deposits are often on or near the surface. Consequently, normal excavating equipment such as shovels, bulldozers and scarifiers are used in open-cast mining, and a minimum of drilling and blasting is necessary.
Artificial graphite is produced by the heating of coal or petroleum coke, and generally contains no free silica. Natural graphite is used in the manufacture of foundry linings, lubricants, paints, electrodes, dry batteries and crucibles for metallurgical purposes. The “lead” in pencils is also graphite.
Health hazards. Inhalation of carbon, as well as associated dusts, may occur during the mining and milling of natural graphite, and during the manufacture of artificial graphite. X-ray examinations of natural and artificial graphite workers have shown varying classifications of pneumoconioses. Microscopic histopathology has revealed pigment aggregates, focal emphysema, collagenous fibrosis, small fibrous nodules, cysts and cavities. The cavities have been found to contain an inky fluid in which graphite crystals were identified. Recent reports note that the materials implicated in exposures leading to severe cases with massive pulmonary fibrosis are likely to be mixed dusts.
Graphite pneumoconiosis is progressive even after the worker has been removed from the contaminated environment. Workers may remain asymptomatic during many years of exposure, and disability often comes suddenly. It is essential that periodic analyses are made of the raw ore and airborne dust for crystalline silica and silicates, with special attention to feldspar, talc and mica. Acceptable dust levels must be adjusted to accommodate the effect these disease-potentiating dusts may have on workers’ health.
In addition to being exposed to the physical hazards of mining, graphite workers may also face chemical hazards, such as hydrofluoric acid and sodium hydroxide used in graphite purification. Protection against the risks associated with these chemicals should be part of any health programme.
Gypsum (Hydrated Calcium Sulphate)
Occurrence and uses. Though it occurs throughout the world, gypsum is rarely found pure. Gypsum deposits may contain quartz, pyrites, carbonates and clayey and bituminous materials. It occurs in nature in five varieties: gypsum rock, gypsite (an impure, earthy form), alabaster (a massive, fine-grained translucent variety), satin spar (a fibrous silky form) and selenite (transparent crystals).
Gypsum rock may be crushed and ground for use in the dihydrate form, calcined at 190 to 200 ºC (thus removing part of the water of crystallization) to produce calcium sulphate hemihydrate or plaster of Paris, or completely dehydrated by calcining at over 600 ºC to produce anhydrous or dead-burned gypsum.
Ground dihydrate gypsum is used in the manufacture of Portland cement and artificial marble products; as a soil conditioner in agriculture; as a white pigment, filler or glaze in paints, enamels, pharmaceuticals, paper and so on; and as a filtration agent.
Health hazards. Workers employed in the processing of gypsum rock may be exposed to high atmospheric concentrations of gypsum dust, furnace gases and smoke. In gypsum calcining, workers are exposed to high environmental temperatures, and there is also the hazard of burns. Crushing, grinding, conveying and packaging equipment presents a danger of machinery accidents. The pneumoconiosis observed in gypsum miners has been attributed to silica contamination.
Dust formation in gypsum processing should be controlled by mechanization of dusty operations (crushing, loading, conveying and so on), addition of up to 2% by volume of water to gypsum prior to crushing, use of pneumatic conveyors with covers and dust traps, enclosure of dust sources and provision of exhaust systems for kiln openings and for conveyor transfer points. In the workshops containing the calcining kilns, it is advisable to face the walls and floors with smooth materials to facilitate cleaning. Hot piping, kiln walls and drier enclosures should be lagged to reduce the danger of burns and to limit heat radiation to the work environment.
Limestone
Occurrence and uses. Limestone is a sedimentary rock composed mainly of calcium carbonate in the form of mineral calcite. Limestones may be classified either according to the impurities they contain (dolomitic limestone, which contains substantial amounts of magnesium carbonate; argillaceous limestone, with a high clay content; siliceous limestone, which contains sand or quartz; and so on) or according to the formation in which they occur (e.g., marble, which is a crystalline limestone). Limestone deposits are widely distributed throughout the earth’s crust and are extracted by quarrying.
Since early times, limestone has been used as a building stone. It is also crushed for use as a flux in smelting, in refining, and for the manufacture of lime. Limestone is used as hardcore and ballast in road and railway construction, and it is mixed with clay for the manufacture of cement.
Health hazards. During extraction, the appropriate quarrying safety measures should be taken, and machinery-guarding principles should be observed on crushers. The main health hazard in limestone quarries is the possible presence, in the airborne limestone dust, of free silica, which normally accounts for 1 to 10% of limestone rock. In studies of limestone quarry and processing workers, x-ray examinations revealed pulmonary changes, and clinical examination showed pharyngitis, bronchitis and emphysema. Workers dressing stone for construction work should observe the safety measures appropriate to the stone industry.
Marble (Calcium Carbonate)
Occurrence and uses. Marble is geologically defined as a metamorphosed (re-crystallized) limestone composed primarily of crystalline grains of calcite, dolomite, or both, having a visible crystalline texture. Long usage of the term marble by the quarry and finishing industry has led to the development of the term commercial marble, which includes all crystalline rock capable of taking a polish and composed primarily of one or more of the following minerals: calcite, dolomite or serpentine.
Marble has been utilized throughout historic time as an important construction material because of its strength, durability, ease of workability, architectural adaptability and aesthetic satisfaction. The marble industry comprises two major branches—dimension marble and crushed and broken marble. The term dimension marble is applied to deposits of marble quarried for the purpose of obtaining blocks or slabs that meet specifications as to size and shape. The uses of dimension marble include building stone, monumental stone, ashlar, veneer panelling, wainscotting, tiling, statuary and so on. Crushed and broken marble ranges in size from large boulders to finely ground products, and products include aggregates, ballast, roofing granules, terrazzo chips, extenders, pigments, agricultural lime and so on.
Health hazards. Occupational diseases specifically connected with the mining, quarrying and processing of marble itself have not been described. In underground mining there may be exposure to toxic gases produced by blasting and some types of motor-driven equipment; adequate ventilation and respiratory protection are necessary. In abrasive blasting there will be exposure to silica if sand is used, but silicon carbide or aluminium oxide are equally effective, carry no silicosis risk, and should be substituted. The large quantities of dust generated in processing marble should be subject to dust control, either by the use of moist methods or by exhaust ventilation.
Mica
Occurrence and uses. Mica (from the Latin micare, to gleam or sparkle) is a mineral silicate which occurs as a primary constituent of igneous rocks, particularly granites. It is also a common component of such silicate materials as kaolin, which are produced by the weathering of these rocks. In the rock bodies, particularly in the pegmatite veins, mica occurs as lenticular masses of cleavable sheets (known as books) of up to 1 m in diameter, or as particles. There are many varieties, of which the most useful are muscovite (common, clear or white mica), phlogopite (amber mica), vermiculite, lepidolite and sericite. Muscovite is generally found in siliceous rocks; there are substantial deposits in India, South Africa and the United States. Sericite is the small plate variety of muscovite. It results from the weathering of schists and gneisses. Phlogopite, which occurs in calcareous rocks, is concentrated in Madagascar. Vermiculite has the outstanding characteristic of expanding considerably when quickly heated to around 300 ºC. There are large deposits in the United States. The main value of lepidolite lies in its high content of lithium and rubidium.
Mica is still used for slow-combustion stoves, lanterns or peep-holes of furnaces. The supreme quality of mica is that it is dielectric, which makes it a top-priority material in aircraft construction. Mica powder is used in the manufacture of electric cables, pneumatic tyres, welding electrodes, bituminized cardboard, paints and plastics, dry lubricants, dielectric dressings and flameproof insulators. It is often compacted with alkyd resins. Vermiculite is widely used as an insulating material in the building industry. Lepidolite is used in the glass and ceramic industries.
Health hazards. When working with mica, the generation of static electricity is possible. Straightforward engineering techniques can harmlessly discharge it. Mica miners are exposed to the inhalation of a wide variety of dusts, including quartz, feldspar and silicates. Chronic inhalation may cause silicosis. Exposure of workers to mica powder may cause irritation of the respiratory tract, and, after several years, nodular fibrotic pneumoconiosis can occur. It was long considered to be a form of silicosis, but it is now believed not to be, because pure mica dust contains no free silica. The radiological appearance is often close to that of asbestosis. Experimentally, mica has proved to possess a low cytotoxicity on macrophages and to induce only a poor fibrogenic response limited to the formation of thick reticulin fibres.
Chronic inhalation of vermiculite, which often contains asbestos, may cause asbestosis, lung cancer and mesothelioma. Ingestion of vermiculite is also suspected in stomach and intestinal cancer.
Pumice
Occurrence and uses. Pumice is a porous rock, grey or white, fragile and of low specific gravity, coming from recent volcanic magma; it is composed of quartz and silicates (mainly feldspar). It is found either pure or mixed with various substances, chief among them obsidian, which differs by its shiny black colour and its specific gravity, which is four times greater. It occurs principally in Ethiopia, Germany, Hungary, Italy (Sicily, Lipari), Madagascar, Spain and the United States. Some varieties, such as Lipari pumice, have a high content of total silica (71.2 to 73.7%) and a fair amount of free silica (1.2 to 5%).
In commerce and for practical uses, a distinction is made between pumice in blocks and in powder. When it is in block form the designation differs according to the size of block, colour, porosity and so on. The powder form is classified by numbers according to grain size. Industrial processing comprises a number of operations: sorting to separate the obsidian, crushing and pulverizing in machines with stone or metal grinding wheels, drying in open kilns, sifting and screening using hand-operated flat and open sieves and reciprocating or rotating screens, the waste matter generally being recovered.
Pumice is used as an abrasive (block or powder), as a lightweight building material, and in the manufacture of stoneware, explosives and so on.
Health hazards. The most dangerous operations involving exposure to pumice are kiln drying and sifting, because of the large amount of dust produced. Apart from the characteristic signs of silicosis observed in the lungs and sclerosis of the hilar lymphatic glands, the study of some fatal cases has revealed damage to various sections of the pulmonary arterial tree. Clinical examination has revealed respiratory disorders (emphysema and sometimes pleural damage), cardiovascular disorders (cor pulmonale) and renal disorders (albuminuria, haematuria, cylindruria), as well as signs of adrenal deficiency. Radiological evidence of aortitis is more common and serious than in the case of silicosis. A typical radiological appearance of lungs in liparitosis is the presence of linear thickening due to lamellar atelactasis.
Sandstone
Occurrence and uses. Sandstone is a siliciclastic sedimentary rock consisting primarily of sand, usually sand that is predominantly quartz. Sandstones often are poorly cemented and can be easily crumbled into sand. Yet, strong, durable sandstone, with tan and grey colours, is used as dimension sandstone for exterior facing and trim for buildings, in houses, as curbstones, in bridge abutments and in various retaining walls. Firm sandstones are crushed for use as concrete aggregate, railroad ballast and riprap. However, many commercial sandstones are weakly cemented and therefore are crumbled and used for moulding sand and glass sand. Glass sand is the main ingredient in glass. In the metalworking industry, sand with good cohesiveness and refractoriness is used for making special shaped moulds into which molten metal is poured.
Sandstone is found throughout the United States, in Illinois, Iowa, Minnesota, Missouri, New York, Ohio, Virginia and Wisconsin.
Health hazards. The primary risks are from the silica exposure, which is discussed in the chapter Respiratory system.
Silica
Occurrence and uses. Silica occurs naturally in crystalline (quartz, cristobalite and tridymite), cryptocrystalline (e.g., chalcedony) and amorphous (e.g., opal) forms, and the specific gravity and melting point depend on the crystalline form.
Crystalline silica is the most widely occurring of all minerals, and it is found in most rocks. The most commonly occurring form of silica is the sand found on beaches throughout the world. The sedimentary rock sandstone consists of grains of quartz cemented together with clays.
Silica is a constituent of common glass and most refractory bricks. It is also used extensively in the ceramic industry. Rocks containing silica are used as common building materials.
Free and combined silica. Free silica is silica which is not combined with any other element or compound. The term free is used to distinguish it from combined silica. Quartz is an example of free silica. The term combined silica originates from the chemical analysis of naturally occurring rocks, clays and soils. The inorganic constituents are found to consist almost always of oxides bound chemically, commonly including silicon dioxide. Silica so combined with one or more other oxides is known as combined silica. The silica in mica, for example, is present in the combined state.
In crystalline silica, the silicon and oxygen atoms are arranged in a definite, regular pattern throughout the crystal. The characteristic crystal faces of a crystalline form of silica are the outward expression of this regular arrangement of atoms. The crystalline forms of free silica are quartz, cristobalite and tridymite. Quartz is crystallized in the hexagonal system, cristobalite in the cubic or tetragonal system and tridymite in the ortho-rhombic system. Quartz is colourless and transparent in the pure form. The colours in naturally occurring quartz are due to contamination.
In amorphous silica the different molecules are in a dissimilar spatial relationship one to another, with the result that there is no definite regular pattern between molecules some distance apart. This absence of long-range order is characteristic of amorphous materials. Cryptocrystalline silica is intermediate between crystalline and amorphous silica in that it consists of minute crystals or crystallites of silica which are themselves arranged in no regular orientation one to another.
Opal is an amorphous variety of silica with a varying amount of combined water. A commercially important form of amorphous silica is diatomaceous earth, and calcinated diatomaceous earth (kieselguhr). Chalcedony is a cryptocrystalline form of silica which occurs filling cavities in lavas or associated with flint. It is also found in the annealing of ceramics when, under certain temperature conditions, the quartz in silicates may crystallize out in minute crystals in the body of the ware.
Health hazards. The inhalation of airborne dust of silica gives rise to silicosis, a serious and potentially fatal fibrotic disease of the lungs. The chronic, accelerated, and acute forms of silicosis reflect differing exposure intensities, latency periods and natural histories. Chronic silicosis may progress to progressive massive fibrosis, even after exposure to silica-containing dust has ceased. Hazards of silica are discussed in more detail in the chapter Respiratory system.
Slate
Occurrence and uses. Slate is very fine-grained, sedimentary argillaceous or schisto-argillaceous rock, easily split, of a leaden-grey, reddish or greenish colour. The principal deposits are in France (Ardennes), Belgium, the United Kingdom (Wales, Cornwall), the United States (Pennsylvania, Maryland) and Italy (Liguria). With a high calcium carbonate content, they contain silicates (mica, chlorite, hydrosilicates), iron oxides and free silica, amorphous or crystalline (quartz). The quartz content of hard slates is in the region of 15%, and that of soft slates, less than 10%. In North Wales quarries, respirable slate dust contains between 13 and 32% of respirable quartz.
Slate slabs are used for roofing; stair treads; door, window and porch casements; flooring; fireplaces; billiard tables; electricity switch panels; and school blackboards. Powdered slate has been used as a filler or pigment in rustproofing or insulating paints, in mastics, and in paints and bituminous products for road surfacing.
Health hazards. Disease in slate workers has attracted attention since the early nineteenth century, and cases of “miner’s phthisis” uncomplicated by tubercle bacilli were described at an early date. Pneumoconiosis has been found in a third of workers studied in the slate industry in North Wales, and in 54% of slate pencil makers in India. Slateworkers’ pneumoconiosis may have features of silicosis due to the high quartz content of some slates. Chronic bronchitis and emphysema are frequently observed, especially in extraction workers.
The replacement of the hand pick by low-velocity mechanical equipment considerably reduces dust generation in slate quarries, and the use of local exhaust ventilation systems makes it possible to maintain airborne dust concentrations within acceptable limits for 8-hour exposure. Ventilation of underground workings, drainage of groundwater into pits, lighting and work organization are improving the general hygiene of working conditions.
Circular sawing should be carried out under water jets, but planing does not usually give rise to dust provided the slivers of slate are not allowed to fall to the ground. Larger sheets are usually wet-polished; however, where dry-polishing is carried out, well-designed exhaust ventilation should be employed since slate dust is not easily collected even when using scrubbers. The dust readily clogs bag filters.
Workshops should be cleaned daily to prevent accumulation of dust deposits; in certain cases, it may be preferable to prevent deposited dust in gangways from becoming airborne again by covering dust with sawdust rather than by wetting it.
Talc
Occurrence and uses. Talc is a hydrous magnesium silicate whose basic formula is (Mg Fe+2)3Si4O10 (OH2), with theoretical weight percentages as follows: 63% SiO2, 32% MgO and 5% H2O. Talc is found in a variety of forms and is frequently contaminated with other minerals, including silica and asbestos. Talc production occurs in Australia, Austria, China, France and the United States.
The texture, stability and fibrous or flaky properties of the various talcs have made them useful for many purposes. The purest grades (i.e., those which most nearly approximate the theoretical composition) are fine in texture and colour, and are therefore widely used in cosmetics and toilet preparations. Other varieties, containing admixtures of different silicates, carbonates and oxides, and perhaps free silica, are relatively coarse in texture and are used in the manufacture of paint, ceramics, automobile tyres and paper.
Health hazards. Chronic inhalation may cause silicosis if silica is present, or asbestosis, lung cancer, and mesothelioma if asbestos or asbestos-like minerals are present. Investigations of workers exposed to talc without associated asbestos fibres revealed trends for higher mortality from silicosis, silicotuberculosis, emphysema and pneumonia. The major clinical symptoms and signs of talc pneumoconiosis include chronic productive cough, progressive shortness of breath, diminished breath sounds, limited chest expansion, diffuse rales and clubbing of the finger tips. Lung pathology has revealed various forms of pulmonary fibrosis.
Wollastonite (Calcium Silicate)
Occurrence and uses. Wollastonite (CaSiO3) is a natural calcium silicate found in metamorphic rock. It occurs in many different forms in New York and California in the United States, in Canada, Germany, Romania, Ireland, Italy, Japan, Madagascar, Mexico, Norway and Sweden.
Wollastonite is used in ceramics, welding-rod coatings, silica gels, mineral wool and paper coating. It is also used as a paint extender, a soil conditioner, and as a filler in plastics, rubber, cements and wallboard.
Health hazards. Wollastonite dust may cause skin, eye and respiratory irritation.
The GESTIS Chemical Information System: A Case Study
GESTIS, the hazardous substance information system of the Berufsgenossenschaften (BG, statutory accident insurance carriers) in Germany, is presented here as a case study of an integrated information system for the prevention of risks from workplace chemical substances and products.
With the enactment and application of the regulation on hazardous substances in Germany in the mid-1980s, there was a huge increase in demand for data and information on hazardous substances. This demand had to be met directly by the BG within the framework of their industrial advisory and supervisory activities.
Specialists, including persons working with technical inspection services of the BG, workplace safety engineers, occupational physicians and those cooperating with expert panels, require specific health data. However, information regarding chemical hazards and the necessary safety measures is no less important for the layperson working with hazardous products. In the factory the effectiveness of work protection rules is what finally counts; it is therefore essential that relevant information be easily accessible to the factory owner, safety personnel, workers and, if appropriate, the work committees.
Against this background GESTIS was set up in 1987. Individual BG institutions had maintained databases mostly for more than 20 years. Within the framework of GESTIS, these databases were combined and supplemented with new components, including a “fact” database on substances and products, and information systems specific to particular branches of industry. GESTIS is organized on a central and peripheral basis, with comprehensive data for and about industry in Germany. It is arranged and classified according to branches of industry.
GESTIS consists of four core databases located centrally with the Berufsgenossenschaften Association and their Institute for Occupational Safety (BIA), plus peripheral, branch-specific information systems and documentation on occupational medicine surveillance and interfaces with external databases.
The target groups for hazardous substance information, such as safety engineers and occupational physicians, require different forms and specific data for their work. The form of information directed towards employees should be understandable and related to the specific handling of substances. Technical inspectors may require other information. Finally, the general public has a right to and an interest in workplace health information, including the identification and status of particular risks and the incidence of occupational disease.
GESTIS must be able to satisfy the information needs of various target groups by providing accurate information that focuses on practice.
Which data and information are needed?
Core information on substances and products
Hard facts must be the primary foundation. In essence these are facts about pure chemical substances, based on scientific knowledge and legal requirements. The scope of the subjects and information in safety data sheets, as, for example, defined by the European Union in EU Directive 91/155/EEC, correspond to the requirements of work protection in the factory and provide a suitable framework.
These data are found in the GESTIS central substance and product database (ZeSP), an online database compiled since 1987, with an emphasis on substances and in cooperation with the governmental labour inspection services (i.e., the hazardous substance databases of the states). The corresponding facts on products (mixtures) are established only on the basis of valid data on substances. In practice, a large problem exists because producers of safety data sheets often do not identify the relevant substances in preparations. The above-mentioned EU directive provides for improvements in the safety data sheets and requires more precise data on the listing of components (depending on the concentration levels).
The compilation of safety data sheets within GESTIS is indispensable for combining the producer data with substance data that are independent of the producers. This result occurs both through the branch-specific recording activities of the BG and through a project in cooperation with producers, who ensure that the safety data sheets are available, up-to-date and largely in data-processed form (see figure 1) in the ISI database (Information System Safety datasheets).
Figure 1.Collection and information centre for safety data sheets - basic structure

Because safety data sheets often do not adequately consider the special use of a product, specialists in branches of industry compile information on product groups (e.g., cooling lubricants for practical work protection in the factory) from producers’ information and substance data. Product groups are defined according to their use and their chemical risk potential. The information made available on product groups is independent of the data provided by producers on the composition of individual products because it is based on general formulae of composition. Thus, the user has access to a supplementary independent information source in addition to the safety data sheet.
A characteristic feature of ZeSP is the provision of information on the safe handling of hazardous substances in the workplace, including specific emergency and preventive measures. Furthermore, ZeSP contains comprehensive information on occupational medicine in a detailed, understandable and practice-related form (Engelhard et al. 1994).
In addition to the practice-oriented information outlined above, further data are needed in connection with national and international expert panels in order to undertake risk assessments for chemical substances (e.g., the EU Existing Chemicals Regulation).
For the evaluation of risk, data are required for the handling of hazardous substances, including (1) the use category of substances or products; (2) the amounts used in production and handling, and the number of persons working with or exposed to the hazardous substance or product; and (3) exposure data. These data can be obtained from hazardous substance registers at the factory level, which are obligatory under European hazardous substance law, for pooling at a higher level to form branch or general trade registers. These registers are becoming increasingly indispensable for providing the required background for political decision- makers.
Exposure data
Exposure data (i.e., measurement values of hazardous substance concentrations) are obtained through the BG within the framework of the BG measurement system for hazardous substances (BGMG 1993), to carry out compliance measurements in view of threshold values in the workplace. Their documentation is necessary for considering the level of technology when establishing threshold values and for risk analyses (e.g., in connection with the determination of risks in existing substances), for epidemiological studies and for evaluating occupational diseases.
The measurement values determined as part of workplace surveillance are therefore documented in the Documentation for Measurement Data on Hazardous Substances in the Workplace (DOK-MEGA). Since 1972 more than 800,000 measurement values have become available from over 30,000 firms. At present about 60,000 of these values are being added annually. Particular features of the BGMG include a quality assurance system, education and training components, standardized procedures for sampling and analysis, a harmonized measurement strategy on a legal basis and tools supported by data processing for information gathering, quality assurance and evaluation (figure 2).
Figure 2. BG measurement system for hazardous substances (BGMG) —cooperation between the BIA and the BG.
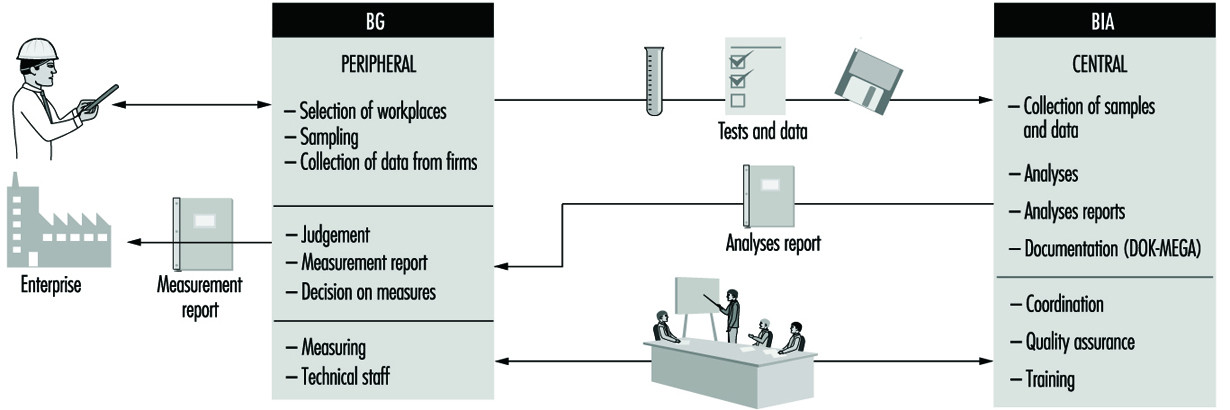
Exposure measurement values must be representative, repeatable and compatible. Exposure data from workplace surveillance in the BGMG are viewed strictly as “representative” of the individual factory situation, since the selection of measurement sites is carried out according to technical criteria in individual cases, not in accordance with statistical criteria. The question of representativeness arises, however, when measurement values for the same or a similar workplace, or even for entire branches of industry, have to be pooled statistically. Measurement data determined as part of surveillance activity generally give higher average values than data that have initially been collected to obtain a representative cross-section of a branch of industry.
For each measurement, differentiated recording and documentation of the relevant factory, process and sampling parameters are required so that the measured values can be combined in a way that is statistically reasonable, and evaluated and interpreted in a technically adequate manner.
In DOK-MEGA this goal is achieved on the following bases of data recording and documentation:
- a standard measurement strategy in accordance with the Technical Rules for Hazardous Substances (TRGS), with documentation of sampling and duration of exposure in particular
- comparable and reliable procedures for sampling, measuring and analysis
- classification of the measurement values according to industrial area, work process or workplace, and also according to activities in systematized and coded form (GESTIS code directories)
- documentation of process-specific or workplace-specific environmental conditions (e.g., local exhaust ventilation) and chemical substances used (e.g., type of electrodes in welding).
The BIA makes use of its experience with DOK-MEGA in a EU research project with representatives of other national exposure databases with the aim of improving the comparability of exposure and measurement results. In particular, an attempt is being made here to define core information as a basis for comparability and to develop a “protocol” for data documentation.
Health data
In addition to facts about chemical substances and products and about the results of exposure measurements, information is needed on the health effects of actual exposure to hazardous substances in the workplace. Adequate conclusions concerning occupational safety on and beyond the corporate level can be drawn only from an overall view of risk potential, actual risk and effects.
A further component of GESTIS is therefore the occupational disease documentation (BK-DOK), in which all cases of occupational disease reported since 1975 have been registered.
Essential to occupational disease documentation in the area of hazardous substances is the unambiguous, correct determination and recording of the relevant substances and products associated with each case. As a rule the determination is very time-consuming, but acquiring knowledge for prevention is impossible without the accurate identification of substances and products. Thus, for respiratory and skin diseases, which present a particular need for better understanding of possible causative agents, particular effort must be given to record substance and product use information as accurately as possible.
Literature data
The fourth component proposed for GESTIS was background information made available in the form of literature documents, so that the basic facts could be judged appropriately on the basis of current knowledge, and conclusions drawn. For this purpose an interface was developed with the literature database (ZIGUV-DOK), with a total of 50,000 references at present, of which 8,000 are on the subject of hazardous substances.
Linkage and Problem-oriented Preparation of Data
Information linkage
The components of GESTIS described above cannot stand in isolation if such a system is to be used efficiently. They require appropriate linkage possibilities, for example, between exposure data and cases of occupational disease. This linkage permits the creation of a truly integrated information system. The linkage occurs through core information that is available, coded in the standardized GESTIS coding system (see table 1).
Table 1. Standardized GESTIS code system
| Object | Individual | Group |
| Code | Code | |
| Substance, product | ZVG central allocation number (BG) | SGS/PGS, substance/product group code (BG) |
| Workplace | IBA sphere of activity of individual factory (BG) | AB sphere of activity (BIA) |
| Exposed person | Activity (BIA, on the basis of the Federal Statistical Office’s systematic listing of occupations) |
Origins of codes appear in parentheses.
With the help of the GESTIS code both individual items of information can be linked to each other (e.g., measurement data from a particular workplace with a case of occupational disease that has occurred in the same or similar workplace) and statistically condensed, “typified” information (e.g., diseases related to particular work processes with average exposure data) can be obtained. With individual linkages of data (e.g., using the pension insurance number) the data protection laws must of course be strictly observed.
It is clear, therefore, that only a systematic coding system is capable of meeting these linkage requirements within the information system. Attention must, however, also be drawn to the possibility of linkage between various information systems and across national boundaries. These possibilities of linkage and comparison are crucially dependent on the use of internationally unified coding standards, if necessary in addition to national standards.
Preparation of problem-oriented and use-oriented information
The structure of GESTIS has at its centre the fact databases on substances and products, exposures, occupational diseases and literature, the data compiled both through specialists active at the centre and through the peripheral activities of the BG. For the application and use of the data, it is necessary to reach the users, centrally through publication in relevant journals (e.g., on the subject of the incidence of occupational disease), but also specifically through the advisory activities of the BG in their member firms.
For the most efficient possible use of information made available in GESTIS, the question arises regarding the problem-specific and target-group-specific preparation of facts as information. User-specific requirements are addressed in the fact databases on chemical substances and products—for example, in the depth of information or in the practice-oriented presentation of information. However, not all the specific requirements of possible users can be directly addressed in the fact databases. Target-group-specific and problem-specific preparation, if necessary supported by data processing, is required. Workplace-oriented information must be made available on the handling of hazardous substances. The most important data from the database must be extracted in a generally understandable and workplace-oriented form, for example, in the form of “workplace instructions”, which are prescribed in the occupational safety laws of many countries. Frequently too little attention is paid to this user-specific preparation of data as information for workers. Special information systems can prepare this information, but specialized information points which respond to individual queries also provide information and give the necessary support to firms. Within the framework of GESTIS this information- gathering and preparation proceeds, for instance, through branch-specific systems such as GISBAU (Hazardous Substances Information System of the Building Industry BG), GeSi (Hazardous Substances and Safety System), and through specialized information centres in the BG, in the BIA or in the association of the Berufsgenossenschaften.
GESTIS provides the relevant interfaces for data exchange and fosters cooperation by means of task-sharing:
- Direct on-line search is possible for the BG through the central substance and product database (ZeSP) and the literature database (ZIGUV-DOK).
- Off-line exchange between central and peripheral databases is accomplished with the help of appropriate interface formats.
- In the specialized information points within GESTIS, experts carry out targeted evaluations and research on request.
Outlook
The emphasis of further development will be on prevention. In cooperation with the producers, plans encompass a comprehensive and up-to-date preparation of product data; the establishment of statistically determined workplace characteristic values derived from the exposure measurement data and from the substance-specific and product-specific documentation; and an evaluation in the occupational disease documentation.
Methods for Localized Control of Air Contaminants
Occupational health professionals have generally relied on the following hierarchy of control techniques to eliminate or minimize worker exposures: substitution, isolation, ventilation, work practices, personal protective clothing and equipment. Usually a combination of two or more of these techniques is applied. Although this article focuses primarily on the application of ventilation techniques, the other approaches are briefly discussed. They should not be ignored when attempting to control exposure to chemicals by ventilation.
The occupational health professional should always think of the concept of source-path-receiver. The primary focus should be on control at the source with control of the path the second focus. Control at the receiver should be considered the last choice. Whether it is during the start-up or design phases of a process or during the evaluation of an existing process, the procedure for control of exposure to air contaminants should start at the source and progress to the receiver. It is likely that all or most of these control strategies will need to be used.
Substitution
The principle of substitution is to eliminate or reduce the hazard by substituting non-toxic or less toxic materials or redesigning the process to eliminate escape of contaminants into the workplace. Ideally, substitute chemicals would be non-toxic or the process redesign would completely eliminate exposure. However, since this is not always possible the subsequent controls in the above hierarchy of controls are attempted.
Note that extreme care should be taken to assure that substitution does not result in a more hazardous condition. While this focus is on the toxicity hazard, the flammable and chemical reactivity of substitutes must also be considered when assessing this risk.
Isolation
The principle of isolation is to eliminate or reduce the hazard by separating the process emitting the contaminant from the worker. This is accomplished by completely enclosing the process or locating it a safe distance away from people. However, to accomplish this, the process may need to be operated and/or controlled remotely. Isolation is particularly useful for jobs requiring few workers and when control by other methods is difficult. Another approach is to perform hazardous operations on off shifts where fewer workers may be exposed. Sometimes the use of this technique does not eliminate exposure but reduces the number of people who are exposed.
Ventilation
Two types of exhaust ventilation are commonly employed to minimize airborne exposure levels of contaminants. The first is called general or dilution ventilation. The second is referred to as source control or local exhaust ventilation (LEV) and is discussed in more detail later in this article.
These two types of exhaust ventilation should not be confused with comfort ventilation, whose main purpose is to provide measured amounts of outdoor air for breathing and to maintain design temperature and humidity. Various types of ventilation are discussed elsewhere in this Encyclopaedia.
Work Practices
Work practices control encompasses the methods workers employ to perform operations and the extent to which they follow the correct procedures. Examples of this control procedure are given throughout this Encyclopaedia wherever general or specific processes are discussed. General concepts such as education and training, principles of management and social support systems include discussions of the importance of work practices in controlling exposures.
Personal Protective Equipment
Personal protective equipment (PPE) is considered the last line of defence for control of worker exposure. It encompasses the use of respiratory protection and protective clothing. It is frequently used in conjunction with other control practices, particularly to minimize the effects of unexpected releases or accidents. These issues are discussed in more detail in the chapter Personal protection.
Local Exhaust Ventilation
The most efficient and cost-effective form of contaminant control is LEV. This involves capture of the chemical contaminant at its source of generation. There are three types of LEV systems:
- enclosures
- exterior hoods
- receiving hoods.
Enclosures are the preferable type of hood. Enclosures primarily are designed to contain the materials generated within the enclosure. The more complete the enclosure the more completely the contaminant will be contained. Complete enclosures are those that have no openings. Examples of complete enclosures include glove boxes, abrasive blasting cabinets and toxic gas storage cabinets (see figure 1, figure 2 and figure 3). Partial enclosures have one or more sides open but the source is still inside the enclosure. Examples of partial enclosures are a spray paint booth (see figure 4) and a laboratory hood. Often it might appear that the design of enclosures is more art than science. The basic principle is to design a hood with the smallest opening possible. The volume of air required is usually based on the area of all openings and maintaining an airflow velocity into the opening of 0.25 to 1.0 m/s. The control velocity chosen will depend on the operation’s characteristics, including the temperature and the degree to which the contaminant is propelled or generated. For complex enclosures, extreme care must be taken to assure that the exhaust flow is evenly distributed throughout the enclosure, particularly if the openings are distributed. Many enclosure designs are evaluated experimentally and if demonstrated to be effective are included as design plates in the American Conference of Governmental Industrial Hygienists’ industrial ventilation manual (ACGIH 1992).
Figure 1. Complete enclosure: Glovebox
Figure 2. Complete enclosure: Toxic gas storage cabinet

Figure 3. Complete enclosure: Abrasive blasting cabinet

Figure 4. Partial enclosure: Spray paint booth

Louis DiBernardinis
Often, total enclosure of the source is not possible, or is not necessary. In these cases, another form of local exhaust, an exterior or capture hood, can be used. An exterior hood prevents the release of toxic materials into the workplace by capturing or entraining them at or close to the source of generation, usually a work station or process operation. Considerably less air volume is usually required than for the partial enclosure. However, since the contaminant is generated outside the hood, it must be designed and used properly in order to be as effective as a partial enclosure. The most effective control is a complete enclosure.
To work effectively, the air inlet of an exterior hood must be of appropriate geometrical design and placed near the point of chemical release. The distance away will depend on the size and shape of the hood and the velocity of air needed at the generation source to capture the contaminant and bring it into the hood. Generally, the closer to the generation source, the better. Design face or slot velocities are typically in the range of 0.25 to 1.0 and 5.0 to 10.0 m/s, respectively. Many design guidelines exist for this class of exhaust hoods in Chapter 3 of the ACGIH manual (ACGIH 1992) or in Burgess, Ellenbecker and Treitman (1989). Two types of exterior hoods that find frequent application are “canopy” hoods and “slot” hoods.
Canopy hoods are used primarily for capture of gases, vapours and aerosols released in one direction with a velocity that can be used to aid capture. These are sometimes called “receiving” hoods. This type of hood is generally used when the process to be controlled is at elevated temperatures, to make use of the thermal updraft, or the emissions are directed upward by the process. Examples of operations that may be controlled in this manner include drying ovens, melting furnaces and autoclaves. Many equipment manufacturers recommend specific capture hood configurations that are suitable for their units. They should be consulted for advice. Design guidelines are also provided in the ACGIH manual, Chapter 3 (ACGIH 1992). For example, for an autoclave or oven where the distance between the hood and the hot source does not exceed approximately the diameter of the source or 1 m, whichever is smaller, the hood may be considered a low canopy hood. Under such conditions, the diameter or cross-section of the hot air column will be approximately the same as the source. The diameter or side dimensions of the hood therefore need only be 0.3 m larger than the source.
The total flow rate for a circular low canopy hood is
Qt=4.7 (Df)2.33 (Dt)0.42
where:
Qt = total hood air flow in cubic feet per minute, ft3/min
Df = diameter of hood, ft
Dt = difference between temperature of the hood source, and the ambient, °F.
Similar relationships exist for rectangular hoods and high canopy hoods. An example of a canopy hood can be seen in figure 5.
Figure 5. Canopy hood: Oven exhaust

Louis DiBernardinis
Slot hoods are used for control of operations that cannot be performed inside a containment hood or under a canopy hood. Typical operations include barrel filling, electroplating, welding and degreasing. Examples are shown in figure 6 and figure 7.
Figure 6. Exterior hood: Welding

Figure 7. Exterior hood: Barrel filling

Louis DiBernardinis
The required flow can be calculated from a series of equations determined empirically by the size and shape of the hood and the distance of the hood from the source. For example, for a flanged slot hood, the flow is determined by
Q = 0.0743LVX
where:
Q = total hood air flow, m3/min
L = the length of the slot, m
V = the velocity needed at the source to capture it, m/min
X = distance from the source to the slot, m.
The velocity needed at the source is sometimes called “capture velocity” and is usually between 0.25 and 2.5 m/s. Guidelines for selecting an appropriate capture velocity are provided in the ACGIH manual. For areas with excessive cross-drafts or for high-toxicity materials, the upper end of the range should be selected. For particulates, higher capture velocities will be necessary.
Some hoods may be some combination of enclosure, exterior and receiving hoods. For example, the spray paint booth shown in figure 4 is a partial enclosure that is also a receiving hood. It is designed to provide efficient capture of particles generated by making use of the particle momentum created by the rotating grinding wheel in the direction of the hood.
Care must be used in selecting and designing local exhaust systems. Considerations should include (1) ability to enclose the operation, (2) source characteristics (i.e., point source vs. widespread source) and how the contaminant is generated, (3) capacity of existing ventilation systems, (4) space requirements and (5) toxicity and flammability of contaminants.
Once the hood is installed, a routine monitoring and maintenance programme for the systems shall be implemented to assure its effectiveness in preventing exposure to workers (OSHA 1993). Monitoring of the standard laboratory chemical hood has become standardized since the 1970s. However, there is no such standardized procedure for other forms of local exhaust; therefore, the user must devise his or her own procedure. The most effective would be a continuous flow monitor. This could be as simple as a magnetic or water pressure gauge measuring static pressure at the hood (ANSI/AIHA 1993). The required hood static pressure (cm of water) will be known from the design calculations, and flow measurements can be made at the time of installation to verify them. Whether or not a continuous flow monitor is present, there should be some periodic evaluation of the hood performance. This can be done with smoke at the hood to visualize capture and by measuring total flow in the system and comparing that to the design flow. For enclosures it is usually advantageous to measure face velocity through the openings.
Personnel must also be instructed in the correct use of these types of hoods, particularly where the distance from the source and the hood can be easily changed by the user.
If local exhaust systems are designed, installed and used correctly they can be an effective and economical means of controlling toxic exposures.
Pregnancy and US Work Recommendations
Changes in family life over recent decades have had dramatic effects on the relationship between work and pregnancy. These include the following:
- Women, particularly those of childbearing age, continue to enter the labour force in considerable numbers.
- A tendency has developed on the part of many of these women to defer starting their families until they are older, by which time they have often achieved positions of responsibility and become important members of the productive apparatus.
- At the same time, there is an increasing number of teenage pregnancies, many of which are high-risk pregnancies.
- Reflecting increasing rates of separation, of divorce and of choices of alternative lifestyles, as well as an increase in the number of families in which both parents must work, financial pressures are forcing many women to continue working for as long as possible during pregnancy.
The impact of pregnancy-related absences and lost or impaired productivity, as well as concern over the health and well-being of both the mothers and their infants, have led employers to become more proactive in dealing with the problem of pregnancy and work. Where employers pay all or part of health insurance premiums, the prospect of avoiding the sometimes staggering costs of complicated pregnancies and neonatal problems is a potent incentive. Certain responses are dictated by laws and government regulations, for example, guarding against potential occupational and environmental hazards and providing maternity leave and other benefits. Others are voluntary: prenatal education and care programmers, modified work arrangements such as flex-time and other work schedule arrangements, dependant care and other benefits.
Management of pregnancy
Of primary importance to the pregnant woman—and to her employer—whether or not she continues working during her pregnancy, is access to a professional health management programme designed to identify and avert or minimize risks to the mother and her foetus, thus enabling her to remain on the job without concern. At each of the scheduled prenatal visits, the physician or midwife should evaluate medical information (childbearing and other medical history, current complaints, physical examinations and laboratory tests) and information about her job and work environment, and develop appropriate recommendations.
It is important that health professionals not rely on the simple job descriptions pertaining to their patients’ work, as these are often inaccurate and misleading. The job information should include details concerning physical activity, chemical and other exposures and emotional stress, most of which can be provided by the woman herself. In some instances, however, input from a supervisor, often relayed by the safety department or the employee health service (where there is one), may be needed to provide a more complete picture of hazardous or trying work activities and the possibility of controlling their potential for harm. This can also serve as a check on patients who inadvertently or deliberately mislead their physicians; they may exaggerate the risks or, if they feel it is important to continue working, may understate them.
Recommendations for Work
Recommendations regarding work during pregnancy fall into three categories:
The woman may continue to work without changes in her activities or the environment. This is applicable in most instances. After extensive deliberation, the Task Force on the Disability of pregnancy comprising obstetrical health professionals, occupational physicians and nurses, and women’s representatives assembled by ACOG (the American College of Obstetricians and Gynecologists) and NIOSH (the National Institute for Occupational Safety and Health) concluded that “the normal woman with an uncomplicated pregnancy who is in a job that presents no greater hazards than those encountered in normal daily life in the community, may continue to work without interruption until the onset of labor and may resume working several weeks after an uncomplicated delivery” (Isenman and Warshaw, 1977).
The woman may continue to work, but only with certain modifications in the work environment or her work activities. These modifications would be either “desirable” or “essential” (in the latter case, she should stop work if they cannot be made).
The woman should not work. It is the physician’s or midwife’s judgement that any work would probably be detrimental to her health or to that of the developing foetus.
The recommendations should not only detail the needed job modifications but should also stipulate the length of time they should be in effect and indicate the date for the next professional examination.
Non-medical Considerations
The recommendations suggested above are based entirely on considerations of the health of the mother and her foetus in relation to job requirements. They do not take into account the burden of such off-the-job activities as commuting to and from the workplace, housework and care of other children and family members; these may sometimes be even more demanding than those of the job. When modification or restriction of activities is called for, one should consider the question whether it should be implemented on the job, in the home or both.
In addition, recommendations for or against continuing work may form the basis of a variety of non-medical considerations, for example, eligibility for benefits, paid versus unpaid leave or guaranteed job retention. A critical issue is whether the woman is considered disabled. Some employers categorically consider all pregnant workers to be disabled and strive to eliminate them from the workforce, even though many are able to continue to work. Other employers assume that all pregnant employees tend to magnify any disability in order to be eligible for all available benefits. And some even challenge the notion that a pregnancy, whether or not it is disabling, is a matter for them to be concerned about at all. Thus, disability is a complex concept which, although fundamentally based on medical findings, involves legal and social considerations.
Pregnancy and Disability
In many jurisdictions, it is important to distinguish between the disability of pregnancy and pregnancy as a period in life that calls for special benefits and dispensations. The disability of pregnancy falls into three categories:
- Disability following delivery. From a purely medical standpoint, recovery following the termination of pregnancy through an uncomplicated delivery lasts only a few weeks, but conventionally it extends to six or eight weeks because that is when most obstetricians customarily schedule their first postnatal check-up. However, from a practical and sociological point of view, a longer leave is considered by many to be desirable in order to enhance family bonding, to facilitate breast-feeding, and so on.
- Disability resulting from medical complications. Medical complications such as eclamsia, threatened abortion, cardiovascular or renal problems and so on, will dictate periods of reduced activity or even hospitalization that will last as long as the medical condition persists or until the woman has recovered from both the medical problem and the pregnancy.
- Disability reflecting the necessity of avoiding exposure to toxicity hazards or abnormal physical stress. Because of the greater sensitivity of the foetus to many environmental hazards, the pregnant woman may be considered disabled even though her own health might not be in danger of being compromised.
Conclusion
The challenge of balancing family responsibilities and work outside the home is not new to women. What may be new is a modern society that values the health and well-being of women and their offspring while confronting women with the dual challenges of achieving personal fulfillment through employment and coping with the economic pressures of maintaining an acceptable standard of living. The increasing number of single parents and of married couples both of whom must work suggest that work-family issues cannot be ignored. Many employed women who become pregnant simply must continue to work.
Whose responsibility is it to meet the needs of these individuals? Some would argue that it is purely a personal problem to be dealt with entirely by the individual or the family. Others consider it a societal responsibility and would enact laws and provide financial and other benefits on a community-wide basis.
How much should be loaded on the employer? This depends largely on the nature, the location and often the size of the organization. The employer is driven by two sets of considerations: those imposed by laws and regulations (and sometimes by the need to meet demands won by organized labour) and those dictated by social responsibility and the practical necessity of maintaining optimal productivity. In the last analysis, it hinges on lacing a high value on human resources and acknowledging the interdependence of work responsibilities and family commitments and their sometimes counterbalancing effects on health and productivity.
Maternity Protection in Legislation
During pregnancy, exposure to certain health and safety hazards of the job or the working environment may have adverse effects on the health of a woman worker and her unborn child. Before and after giving birth, she also needs a reasonable amount of time off from her job to recuperate, breast-feed and bond with her child. Many women want and need to be able to return to work after childbirth; this is increasingly recognized as a basic right in a world where the participation of women in the labour force is continuously increasing and approaching that of men in many countries. As most women need to support themselves and their families, continuity of income during maternity leave is vital.
Over time, governments have enacted a range of legislative measures to protect women workers during pregnancy and at childbirth. A feature of more recent measures is the prohibition of discrimination in employment on the grounds of pregnancy. Another trend is to provide the right for mothers and fathers to share leave entitlements after the birth so that either may care for the child. Collective bargaining in many countries contributes to the more effective application of such measures and often improves upon them. Employers also lay an important role in furthering maternity protection through the terms of individual contracts of employment and enterprise policies.
The Limits of Protection
Laws providing maternity protection for working women are usually restricted to the formal sector, which may represent a small proportion of economic activity. These do not apply to women working in unregistered economic activities in the informal sector, who in many countries represent the majority of working women. While there is a trend worldwide to improve and extend maternity protection, how to protect the large segment of the population living and working outside the formal economy remains a major challenge.
In most countries, labour legislation provides maternity protection for women employed in industrial and non-industrial enterprises in the private and often also the public sector. Homeworkers, domestic employees, own-account workers and workers in enterprises employing only family members are frequently excluded. Since many women work in small firms, the relatively frequent exclusion of undertakings which employ less than a certain number of workers (e.g., five permanent workers in the Republic of Korea) is of concern.
Many women workers in precarious employment, such as temporary workers, or casual workers in Ireland, are excluded from the scope of labour legislation in a number of countries. Depending on the number of hours they work, part-time workers may also be excluded. Other groups of women may be excluded, such as women managers (e.g., Singapore, Switzerland), women whose earnings exceed a certain maximum (e.g., Mauritius) or women who are paid by results (e.g., the Philippines). In rare cases, unmarried women (e.g., teachers in Trinidad and Tobago) do not qualify for maternity leave. However, in Australia (federal), where parental leave is available to employees and their spouses, the term “spouse” is defined to include a de facto spouse. Where age limits are set (e.g., in Israel, women below the age of 18) they usually do not exclude very many women as they are normally fixed below or above the prime child-bearing ages.
Public servants are often covered by special rules, which may provide for more favourable conditions than those applicable to the private sector. For example, maternity leave may be longer, cash benefits may correspond to the full salary instead of a percentage of it, parental leave is more likely to be available, or the right to reinstatement may be more clearly established. In a significant number of countries, conditions in the public service can act as an agent of progress since collective bargaining agreements in the private sector are often negotiated along the lines of public service maternity protection rules.
Similar to labour legislation, social security laws may limit their application to certain sectors or categories of workers. While this legislation is often more restrictive than the corresponding labour laws in a country, it may provide access to maternity cash benefits to groups not covered by labour laws, such as self-employed women or women who work with their self-employed husbands. In many developing countries, owing to a lack of resources, social security legislation may only apply to a limited number of sectors.
Over the decades, however, the coverage of legislation has been extended to more economic sectors and categories of workers. Yet, while an employee may be covered by a law, the enjoyment of certain benefits, in particular maternity leave and cash benefits, may depend on certain eligibility requirements. Thus, while most countries protect maternity, working women do not enjoy a universal right to such protection.
Maternity Leave
Time off work for childbirth can vary from a few weeks to several months, often divided into two parts, before and after the birth. A period of employment prohibition may be stipulated for a part or the whole of the entitlement to ensure that women have sufficient rest. Maternity leave is commonly extended in case of illness, preterm or late birth, and multiple births, or shortened in case of miscarriage, stillbirth or infant death.
Normal duration
Under the ILO’s Maternity protection Convention, 1919 (No. 3), “a woman shall not be permitted to work during the six weeks following her confinement; [and] shall have the right to leave her work if she produces a medical certificate stating that her confinement will probably take lace within six weeks”. The Maternity protection Convention (Revised), 1952 (No. 103), confirms the 12-week leave, including an employment prohibition for six weeks after the birth, but does not prescribe the use of the remaining six weeks. The Maternity protection Recommendation, 1952 (No. 95), suggests a 14-week leave. The Maternity protection Recommendation, 2000 (No. 191) suggests a 18-week leave [Edited, 2011]. Most of the countries surveyed meet the 12-week standard, and at least one-third grant longer periods.
A number of countries afford a possibility of choice in the distribution of maternity leave. In some, the law does not prescribe the distribution of maternity leave (e.g., Thailand), and women are entitled to start the leave as early or as late as they wish. In another group of countries, the law indicates the number of days to be taken after confinement; the balance can be taken either before or after the birth.
Other countries do not allow flexibility: the law provides for two periods of leave, before and after confinement. These periods may be equal, especially where the total leave is relatively short. Where the total leave entitlement exceeds 12 weeks, the prenatal period is often shorter than the postnatal period (e.g., in Germany six weeks before and eight weeks after the birth).
In a relatively small number of countries (e.g., Benin, Chile, Italy), the employment of women is prohibited during the whole period of maternity leave. In others, a period of compulsory leave is prescribed, often after confinement (e.g., Barbados, Ireland, India, Morocco). The most common requirement is a six-week compulsory period after birth. Over the past decade, the number of countries providing for some compulsory leave before the birth has increased. On the other hand, in some countries (e.g., Canada) there is no period of compulsory leave, as it is felt that the leave is a right that should be freely exercised, and that time off should be organized to suit the individual woman’s needs and preferences.
Eligibility for maternity leave
The legislation of most countries recognizes the right of women to maternity leave by stating the amount of leave to which women are entitled; a woman needs only to be employed at the time of going on leave to be eligible for the leave. In a number of countries, however, the law requires women to have been employed for a minimum period prior to the date on which they absent themselves. This period ranges from 13 weeks in Ontario or Ireland to two years in Zambia.
In several countries, women must have worked a certain number of hours in the week or month to be entitled to maternity leave or benefits. When such thresholds are high (as in Malta, 35 hours per week), they can result in excluding a large number of women, who form the majority of part-time workers. In a number of countries, however, thresholds have been lowered recently (e.g., in Ireland, from 16 to eight hours per week).
A small number of countries limit the number of times a woman may request maternity leave over a given period (for example two years), or restrict eligibility to a certain number of pregnancies, either with the same employer or throughout the woman’s life (e.g., Egypt, Malaysia). In Zimbabwe, for example, women are eligible for maternity leave once in every 24 months and for a maximum of three times during the period that they work for the same employer. In other countries, the women who have more than the prescribed number of children are eligible for maternity leave, but not for cash benefits (e.g., Thailand), or are eligible for a shorter period of leave with benefits (e.g., Sri Lanka: 12 weeks for the first two children, six weeks for the third and subsequent children). The number of countries that limit eligibility for maternity leave or benefits to a certain number of pregnancies, children or surviving children (between two and four) appears to be growing, although it is by no means certain that the duration of maternity leave is a decisive factor in motivating decisions about family size.
Advance notice to the employer
In most countries, the only requirement for women to be entitled to maternity leave is the presentation of a medical certificate. Elsewhere, women are also required to give their employer notice of their intention to take maternity leave. The period of notice ranges from as soon as the pregnancy is known (e.g., Germany) to one week before going on leave (e.g., Belgium). Failure to meet the notice requirement may lose women their right to maternity leave. Thus, in Ireland, information regarding the timing of maternity leave is to be supplied as soon as reasonably practicable, but not later than four weeks before the commencement of the leave. An employee loses her entitlement to maternity leave if she fails to satisfy this requirement. In Canada (federal), the notice requirement is waived where there is a valid reason why the notice cannot be given; at provincial level, the notice period ranges from four months to two weeks. If the notice period is not complied with, a woman worker is still entitled to the normal maternity leave in Manitoba; she is entitled to shorter periods (usually six weeks as opposed to 17 or 18) in most other provinces. In other countries, the law does not clarify the consequences of failing to give notice.
Cash Benefits
Most women cannot afford to forfeit their income during maternity leave; if they had to, many would not use all their leave. Since the birth of healthy children benefits the whole nation, as a matter of equity, employers should not bear the full cost of their workers’ absences. Since 1919, ILO standards have held that during maternity leave, women should receive cash benefits, and that these should be paid out of public funds or through a system of insurance. Convention No. 103 requires that contributions due under a compulsory social insurance scheme be paid based on the total number of men and women employed by the undertakings concerned, without distinction based on sex. Although in a few countries, maternity benefits represent only a relatively small percentage of wages, the level of two-thirds called for in Convention No. 103 is reached in several and exceeded in many others. In more than half of the countries surveyed, maternity benefits constitute 100% of insured wages or of full wages.
Many social security laws may provide a specific maternity benefit, thus recognizing maternity as a contingency in its own right. Others provide that during maternity leave, a worker will be entitled to sickness or unemployment benefits. Treating maternity as a disability or the leave as a period of unemployment could be considered unequal treatment since, in general, such benefits are only available during a certain period, and women who use them in connection with maternity may find they do not have enough left to cover actual sickness or unemployment periods later. Indeed, when the 1992 European Council Directive was drafted, a proposal that during maternity leave women would receive sickness benefits was strongly challenged; it was argued that in terms of equal treatment between men and women, maternity needed to be recognized as independent grounds for obtaining benefits. As a compromise, the maternity allowance was defined as guaranteeing an income at least equivalent to what the worker concerned would receive in the event of sickness.
In nearly 80 of the countries surveyed, benefits are paid by national social security schemes, and in over 40, these are at the expense of the employer. In about 15 countries, the responsibility for financing maternity benefits is shared between social security and the employer. Where benefits are financed jointly by social security and the employer, each may be required to pay half (e.g., Costa Rica), although other percentages may be found (e.g., Honduras: two-thirds by social security and one-third by the employer). Another type of contribution may be required of employers: when the amount of maternity benefit paid by social security is based on a statutory insurable income and represents a low percentage of a woman’s full wage, the law sometimes provides that the employer will pay the balance between the woman’s salary and the maternity benefit paid by the social security fund (e.g., in Burkina Faso). Voluntary additional payment by the employer is a feature of many collective agreements, and also of individual employment contracts. The involvement of employers in the payment of cash maternity benefits may be a realistic solution to the problem posed by the lack of other funds.
Protection of the Health of Pregnant and Nursing Women
In line with the requirements of the Maternity protection Recommendation, 1952 (No. 95), many countries provide for various measures to protect the health of pregnant women and their children, seeking to minimize fatigue by the reorganization of working time or to protect women against dangerous or unhealthy work.
In a few countries (e.g., the Netherlands, Panama), the law specifies an obligation of the employer to organize work so that it does not affect the outcome of the pregnancy. This approach, which is in line with modern occupational health and safety practice, permits matching the needs of individual women with the corresponding preventive measures, and is therefore most satisfactory. Much more generally, protection is sought through prohibiting or limiting work which may be harmful to the health of the mother or child. Such a prohibition may be worded in general terms or may apply to certain types of hazardous work. However, in Mexico, the prohibition of employing women in unhealthy or dangerous work does not apply if the necessary health protection measures have, in the opinion of the competent authority, been taken; nor does it apply to women in managerial positions or those who possess a university degree or technical diploma, or the necessary knowledge and experience to carry on the work.
In many countries, the law provides that pregnant women and nursing mothers may not be allowed to do work that is “beyond their strength”, which “involves hazards”, “is dangerous to their health or that of their child”, or “requires a physical effort unsuited to their condition”. The application of such a general prohibition, however, can present problems: how, and by whom, shall it be determined that a job is beyond a person’s strength? By the worker concerned, the employer, the labour inspector, the occupational health physician, the woman’s own doctor? Differences in appreciation might lead to a woman being kept away from work which she could in fact do, while another might not be removed from work which is too taxing.
Other countries list, sometimes in great detail, the type of work that is prohibited to pregnant women and nursing mothers (e.g., Austria, Germany). The handling of loads is frequently regulated. Legislation in some countries specifically prohibits exposure to certain chemicals (e.g., benzene), biological agents, lead and radiation. Underground work is prohibited in Japan during pregnancy and one year after confinement. In Germany, piece-rate work and work on an assembly line with a fixed pace are prohibited. In a few countries, pregnant workers may not be assigned to work outside their permanent place of residence (e.g., Ghana, after the fourth month). In Austria, smoking is not permitted in places where pregnant women are working.
In a number of countries (e.g., Angola, Bulgaria, Haiti, Germany), the employer is required to transfer the worker to suitable work. Often, the worker must retain her former salary even if the salary of the post to which she is transferred is lower. In the Lao people’s Democratic Republic, the woman keeps her former salary during a three-month period, and is then paid at the rate corresponding to the job she is actually performing. In the Russian Federation, where a suitable post is to be given to a woman who can no longer perform her work, she retains her salary during the period in which a new post is found. In certain cases (e.g., Romania), the difference between the two salaries is paid by social security, an arrangement which is to be referred, since the cost of maternity protection should not, as far as feasible, be borne by individual employers.
Transfer may also be available from work that is not dangerous in itself but which a medical practitioner has certified to be harmful to a particular woman’s state of health (e.g., France). In other countries, a transfer is possible at the request of the worker concerned (e.g., Canada, Switzerland). Where the law enables the employer to suggest a transfer, if there is a disagreement between the employer and the worker, an occupational physician will determine whether there is any medical need for changing jobs and whether the worker is fit to take up the job that has been suggested to her.
A few countries clarify the fact that the transfer is temporary and that the worker must be reassigned to her former job when she returns from maternity leave or at a specified time thereafter (e.g., France). Where a transfer is not possible, some countries provide that the worker will be granted sick leave (e.g., Seychelles) or, as was discussed above, that maternity leave will start early (e.g., Iceland).
Non-discrimination
Measures are taken in a growing number of countries to ensure that women do not suffer discrimination on account of pregnancy. Their aim is to ensure that pregnant women are considered for employment and treated during employment on an equal basis with men and with other women, and in particular are not demoted, do not lose seniority or are not denied promotion solely on the grounds of pregnancy. It is now more and more common for national legislation to prohibit discrimination on account of sex. Such a prohibition could be and indeed has been in many cases interpreted by the courts as a prohibition to discriminate on account of pregnancy. The European Court of Justice has followed this approach. In a 1989 judgement, the Court ruled that an employer who dismisses or refuses to recruit a woman because she is pregnant is in breach of Directive 76/207/EEC of the European Council on equal treatment. This judgement was important in clarifying the fact that sex discrimination exists when employment decisions are made on the basis of pregnancy even though the law does not specifically cite pregnancy as prohibited grounds for discrimination. It is customary in sex equality cases to compare the treatment given to a woman with the treatment given to a hypothetical man. The Court ruled that such comparison was not called for in the case of a pregnant woman, since pregnancy was unique to women. Where unfavourable treatment is made on grounds of pregnancy, there is by definition discrimination on grounds of sex. This is consistent with the position of the ILO Committee of Exerts on the Application of Conventions and Recommendations concerning the scope of the Discrimination (Employment and Occupation) Convention, 1958 (No. 111), which notes the discriminatory nature of distinctions on the basis of pregnancy, confinement and related medical conditions (ILO 1988).
A number of countries provide for an explicit prohibition of discrimination on the grounds of pregnancy (e.g., Australia, Italy, US, Venezuela). Other countries define discrimination on grounds of sex to include discrimination on grounds of pregnancy or absence on maternity leave (e.g., Finland). In the US, protection is further ensured through treating pregnancy as a disability: in undertakings with more than 15 workers, discrimination is prohibited against pregnant women, women at childbirth and women who are affected by related medical conditions; and policies and practices in connection with pregnancy and related matters must be applied on the same terms and conditions as applied to other disabilities.
In several countries, the law contains precise requirements which illustrate instances of discrimination on the grounds of pregnancy. For example, in the Russian Federation, an employer may not refuse to hire a woman because she is pregnant; if a pregnant woman is not hired, the employer must state in writing the reasons for not recruiting her. In France, it is unlawful for an employer to take pregnancy into account in refusing to employ a woman, in terminating her contract during a period of probation or in ordering her transfer. It is also unlawful for the employer to seek to determine whether an applicant is pregnant, or to cause such information to be sought. Similarly, women cannot be required to reveal the fact that they are pregnant, whether they apply for a job or are employed in one, except when they request to benefit from any law or regulation governing the protection of pregnant women.
Transfers unilaterally and arbitrarily imposed on a pregnant woman can constitute discrimination. In Bolivia, as in other countries in the region, a woman is protected against involuntary transfer during pregnancy and up to a year after the birth of her child.
The issue of combining the right of working women to health protection during pregnancy and their right not to suffer discrimination poses a special difficulty at the time of recruitment. Should a pregnant applicant reveal her condition, especially one who applies for a position involving work which is prohibited to pregnant women? In a 1988 judgement, the Federal Labour Court of Germany held that a pregnant woman applying for a job involving exclusively night work, which is prohibited to pregnant women under German legislation, should inform a potential employer of her condition. The judgement was overruled by the European Court of Justice as being contrary to the 1976 EC Directive on equal treatment. The Court found that the Directive precluded an employment contract from being held to be void on account of the statutory prohibition of night work, or from being avoided by the employer on account of a mistake on his or her part as to an essential personal characteristic of the woman at the time of the conclusion of the contract. The employee’s inability, due to pregnancy, to perform the work for which she was being recruited was temporary since the contract was not concluded with a fixed term. It would therefore be contrary to the objective of the Directive to hold it invalid or void because of such an inability.
Employment Security
Many women have lost their jobs because of a pregnancy. Nowadays, although the extent of protection varies, employment security is a significant component of maternity protection policies.
International labour standards address the issue in two different ways. The maternity protection Conventions prohibit dismissal during maternity leave and any extension thereof, or at such time as a notice of dismissal would expire during the leave under the terms of Convention No. 3, Article 4 and Convention No. 103, Article 6. Dismissal on grounds that might be regarded as legitimate is not considered to be permitted during this period (ILO 1965). In the event that a woman has been dismissed before going on maternity leave, the notice should be suspended for the time she is absent and continue after her return. The Maternity protection Recommendation, 1952 (No. 95), calls for the protection of a pregnant woman’s employment from the date the employer is informed of the pregnancy until one month after her return from maternity leave. It identifies cases of serious fault by the employed woman, the shutting down of the undertaking and the expiry of a fixed-term contract as legitimate grounds for dismissal during the protected period. The Termination of Employment Convention, 1982 (No. 158; Article 5(d)–(e)), does not prohibit dismissal, but provides that pregnancy or absence from work on maternity leave shall not constitute valid reasons for termination of employment.
At the level of the European Union, the 1992 Directive prohibits dismissal from the beginning of pregnancy until the end of the maternity leave, save in exceptional cases not connected with the worker’s condition.
Usually, countries provide for two sets of rules regarding dismissal. Dismissal with notice applies in such cases as the closure of the enterprise, redundancy and where, for a variety of reasons, the worker is unable to perform the work for which he or she has been recruited or fails to perform such work to the employer’s satisfaction. Dismissal without notice is used to terminate the services of a worker who is guilty of gross negligence, serious misconduct or other grave instances of behaviour, usually comprehensively listed in the legislation.
Where dismissal with notice is concerned, it is clear that employers could arbitrarily decide that pregnancy is incompatible with a worker’s tasks and dismiss her on grounds of pregnancy. Those who wish to avoid their obligations to pregnant women, or even simply do not like to have pregnant women around the workplace, could find a pretext to dismiss workers during pregnancy even if, in view of the existence of non-discrimination rules, they would refrain from using pregnancy as grounds for dismissal. Many people agree that it is legitimate to protect workers against such discriminatory decisions: the prohibition of dismissal with notice on grounds of pregnancy or during pregnancy and maternity leave is often viewed as a measure of equity and is in force in many countries.
The ILO Committee of Exerts on the Application of Conventions and Recommendations considers that protection against dismissal does not preclude an employer from terminating an employment relationship because he or she has detected a serious fault on the part of a woman employee: rather, when there are reasons such as this to justify dismissal, the employer is obliged to extend the legal period of notice by any period required to complete the period of protection under the Conventions. This is the situation, for example, in Belgium, where an employer who has legal grounds for dismissing a woman cannot do so while she is on maternity leave, but can serve notice so that it expires after the woman returns from leave.
The protection of pregnant women against dismissal in case of closure of the undertaking or economic retrenchment poses a similar problem. It is indeed a burden for a firm which ceases operation to continue to pay the salary of a person who is not working for them any more, even for a short period. However, recruitment prospects are often bleaker for women who are pregnant than for women who are not, or for men, and pregnant women particularly need the emotional and financial security of continuing to be employed. Where women may not be dismissed during pregnancy, they can put off looking for a job until after the birth. In fact, where legislation provides for the order in which various categories of workers to be retrenched are to be dismissed, pregnant women are among those to be dismissed last or next to last (e.g., Ethiopia).
Leave and Benefits for Fathers and Parents
Going beyond the protection of the health and employment status of pregnant and nursing women, many countries provide for paternity leave (a short period of leave at or about the time of birth). Other forms of leave are linked to the needs of children. One type is adoption leave, and another is leave to facilitate child-rearing. Many countries foresee the latter type of leave, but use different approaches. One group provides for time off for the mother of very young children (optional maternity leave), while another provides additional leave for both parents (parental education leave). The view that both the father and mother need to be available to care for young children is also reflected in integrated parental leave systems, which provide a long period of leave available to both parents.
Occupational and Environmental Exposures to the Newborn
Environmental hazards pose a special risk for infants and young children. Children are not “little adults”, either in the way they absorb and eliminate chemicals or in their response to toxic exposures. Neonatal exposures may have a greater impact because the body surface area is disproportionately large and metabolic capacity (or the ability to eliminate chemicals) is relatively underdeveloped. At the same time, the potential toxic effects are greater, because the brain, the lungs and the immune system are still developing during the early years of life.
Opportunities for exposure exist at home, in day care facilities and on playgrounds:
- Young children can absorb environmental agents from the air (by inhalation) or through the skin.
- Ingestion is a major route of exposure, especially when children begin to exhibit hand-to-mouth activity.
- Substances on the hair, clothes or hands of the parents can be transferred to the young child.
- Breast milk is another potential source of exposure for infants, although the potential benefits of nursing far outweigh the potential toxic effects of chemicals in breast milk.
For a number of the health effects discussed in connection with neonatal exposures, it is difficult to distinguish prenatal from postnatal events. Exposures taking lace before birth (through the placenta) can continue to be manifest in early childhood. Both lead and environmental tobacco smoke have been associated with deficits in cognitive development and lung function both before and after birth. In this review, we have attempted to focus on postnatal exposures and their effects on the health of very young children.
Lead and Other Heavy Metals
Among the heavy metals, lead (b) is the most important elemental exposure for humans in both environmental and occupational circumstances. Significant occupational exposures occur in battery manufacture, smelters, soldering, welding, construction and paint removal. parents employed in these industries have long been known to bring dust home on their clothes that can be absorbed by their children. The primary route of absorption by children is through ingestion of lead-contaminated paint chips, dust and water. Respiratory absorption is efficient, and inhalation becomes a significant exposure pathway if an aerosol of lead or alkyl lead is resent (Clement International Corporation 1991).
Lead poisoning can damage virtually every organ system, but current levels of exposure have been associated chiefly with neurological and developmental changes in children. In addition, renal and haematological disease have been observed among both adults and children intensely exposed to lead. Cardiovascular disease as well as reproductive dysfunction are known sequelae of lead exposure among adults. Subclinical renal, cardiovascular and reproductive effects are suspected to arise from lower, chronic lead exposure, and limited data support this idea. Animal data support human findings (Sager and Girard 1994).
In terms of measurable dose, neurological effects range from IQ deficits at low exposures (blood lead = 10 μg/dl) to enceha-loathy (80 μg/dl). Levels of concern in children in 1985 were 25 μg/dl, which was lowered to 10 μg/dl in 1993.
Neonatal exposure, as it resulted from dust brought home by working parents, was described as “fouling the nest” by Chisholm in 1978. Since that time, preventive measures, such as showering and changing clothing before leaving the workplace, have reduced the take-home dust burden. However, occupationally derived lead is still an important potential source of neonatal exposure today. A survey of children in Denmark found that blood lead was approximately twice as high among children of exposed workers than in homes with only non-occupational exposures (Grandjean and Bach 1986). Exposure of children to occupationally derived lead has been documented among electric cable splicers (Rinehart and Yanagisawa 1993) and capacitor manufacturing workers (Kaye, Novotny and Tucker 1987).
Non-occupational sources of environmental lead exposure continue to be a serious hazard to young children. Since the gradual ban of tetraethyl lead as a fuel additive in the United States (in 1978), average blood lead levels in children have declined from 13 to 3 μg/dl (Pirkle et al. 1994). paint chips and paint dust are now the principal cause of childhood lead poisoning in the United States (Roer 1991). For example in one report, younger children (neonates aged less than 11 months) with excessive lead in their blood were at greatest risk of exposure through dust and water while older children (aged 24 months) were at risk more from ingestion of paint chips (ica) (Shannon and Graef 1992). Lead abatement through paint removal has been successful in protecting children from exposure to dust and paint chips (Farfel, Chisholm and Rohde 1994). Ironically, workers engaged in this enterprise have been shown to carry lead dust home on their clothes. In addition, it has been noted that the continuing exposure of young children to lead disproportionately affects economically disadvantaged children (Brody et al. 1994; Goldman and Carra 1994). art of this inequity arises from the poor condition of housing; as early as 1982, it was shown that the extent of deterioration of housing was directly related to blood lead levels in children (Clement International Corporation 1991).
Another potential source of occupationally derived exposure for the neonate is lead in breast milk. Higher levels of lead in breast milk have been linked to both occupational and environmental sources (Ryu, Ziegler and Fomon 1978; Dabeka et al. 1986). The concentrations of lead in milk are small relative to blood (approximately 1/5 to 1/2) (Wolff 1993), but the large volume of breast milk ingested by an infant can add milligram quantities to the body burden. In comparison, there is normally less than 0.03 mg b in the circulating blood of an infant and the usual intake is less than 20 mg per day (Clement International Corporation 1991). Indeed, absorption from breast milk is reflected in the blood lead level of infants (Rabinowitz, Leviton and Needleman 1985; Ryu et al. 1983; Ziegler et al. 1978). It should be noted that normal lead levels in breast milk are not excessive, and lactation contributes an amount similar to that from other sources of infant nutrition. By comparison, a small paint chi could contain more than 10 mg (10,000 mg) of lead.
Developmental decrements in children have been linked with both prenatal and postnatal exposures to lead. prenatal exposure is thought to be responsible for lead-related deficits in mental and behavioural development that have been found in children until the age of two to four years (Landrigan and Cambell 1991; Bellinger et al. 1987). The effects of postnatal lead exposure, such as that experienced by the neonate from occupational sources, may be detected in children from ages two to six and even later. Among these are problem behaviour and lower intelligence (Bellinger et al. 1994). These effects are not confined only to high exposures; they have been observed at relatively low levels, e.g., where blood lead levels are in the range of 10 mg/dl (Needleman and Bellinger 1984).
Mercury (Hg) exposure from the environment may occur as inorganic and organic (mainly methyl) forms. Recent occupational exposures to mercury have been found among workers in thermometer manufacture and in repair of high-voltage equipment containing mercury. Other occupations with potential exposures include painting, dentistry, plumbing and chlorine manufacture (Agency for Toxic Substance and Disease Registry 1992).
prenatal and postnatal mercury poisoning has been well documented among children. Children are more susceptible to effects of methylmercury than adults. This is largely because the developing human central nervous system is so “remarkably sensitive” to methylmercury, an effect also seen at low levels in animals (Clarkson, Nordberg and Sager 1985). Methylmercury exposures in children arise chiefly from ingestion of contaminated fish or from breast milk, while elemental mercury is derived from occupational exposures. Household exposure incidental to occupational exposure has been noted (Zirschky and Wetherell 1987). Accidental exposures in the home have been reported in recent years in domestic industries (Meeks, Keith and Tanner 1990; Rowens et al. 1991) and in an accidental sill of metallic mercury (Florentine and Sanfilio 1991). Elemental mercury exposure occurs mainly by inhalation, while alkyl mercury can be absorbed by ingestion, inhalation or dermal contact.
In the best-studied episode of poisoning, sensory and motor dysfunction and mental retardation were found following very high exposures to methylmercury either in utero or from breast milk (Bakir et al. 1973). Maternal exposures resulted from ingestion of methylmercury that had been used as a fungicide on grain.
pesticides and Related Chemicals
Several hundred million tons of pesticides are produced worldwide each year. Herbicides, fungicides and insecticides are employed mainly in agriculture by developed countries to improve crop yield and quality. Wood preservatives are a much smaller, but still a major, art of the market. Home and garden use represents a relatively minor proportion of total consumption, but from the point of view of neonatal toxicity, domestic poisonings are perhaps the most numerous. Occupational exposure is also a potential source of indirect exposure to infants if a parent is involved in work that uses pesticides. Exposure to pesticides is possible through dermal absorption, inhalation and ingestion. More than 50 pesticides have been declared carcinogenic in animals (McConnell 1986).
Organochlorine pesticides include aromatic compounds, such as DDT (bis(4-chlorohenyl)-1,1,1-trichloroethane), and cyclodienes, such as dieldrin. DDT came into use in the early 1940s as an effective means to eliminate mosquitoes carrying malaria, an application that is still widely employed today in developing countries. Lindane is an organochlorine used widely to control body lice and in agriculture, especially in developing countries. olychlorinated bihenyls (CBs), another fat-soluble organochlorine mixture used since the 1940s, pose a potential health risk to young children exposed through breast milk and other contaminated foods. Both lindane and CBs are discussed separately in this chapter. olybrominated bihenyls (BBs) also have been detected in breast milk, almost exclusively in Michigan. Here, a fire-retardant inadvertently mixed into livestock feed in 1973-74 became widely dispersed across the state through dairy and meat products.
Chlordane has been used as a pesticide and as a termiticide in houses, where it is effective for decades, no doubt because of its persistence. Exposure to this chemical can be from dietary and direct respiratory or dermal absorption. Levels in human milk in Japan could be related both to diet and to how recently homes had been treated. Women living in homes treated more than two years earlier had chlordane levels in milk three times those of women living in untreated homes (Taguchi and Yakushiji 1988).
Diet is the main source of persistent organochlorines, but smoking, air and water may also contribute to exposure. This class of pesticides, also termed halogenated hydrocarbons, is quite persistent in the environment, since these are lipophilic, resistant to metabolism or biodegradation and exhibit low volatility. Several hundreds of m have been found in human and animal fat among those with highest exposures. Because of their reproductive toxicity in wildlife and their tendency to bioaccumulate, organochlorines have been largely banned or restricted in developed countries.
At very high doses, neurotoxicity has been observed with organochlorines, but potential long-term health effects are of more concern among humans. Although chronic health effects have not been widely documented, heatotoxicity, cancer and reproductive dysfunction have been found in experimental animals and in wildlife. Health concerns arise mainly from observations in animal studies of carcinogenesis and of profound changes in the liver and the immune system.
Organohoshates and carbamates are less persistent than the organochlorines and are the most widely used class of insecticides internationally. pesticides of this class are degraded relatively quickly in the environment and in the body. A number of the organohoshates and carbamates exhibit high acute neurotoxicity and in certain cases chronic neurotoxicity as well. Dermatitis is also a widely reported symptom of pesticide exposure.
The petroleum-based products used to apply some pesticides are also of potential concern. Chronic effects including haematooietic and other childhood cancers have been associated with parental or residential exposures to pesticides, but the epidemiological data are quite limited. Nevertheless, based on the data from animal studies, exposures to pesticides should be avoided.
For the newborn, a wide spectrum of exposure possibilities and toxic effects have been reported. Among children who required hospitalization for acute poisoning, most had inadvertently ingested pesticide products, while a significant number had been exposed while laying on sprayed carets (Casey, Thomson and Vale 1994; Zwiener and Ginsburg 1988). Contamination of workers’ clothing by pesticide dust or liquid has long been recognized. Therefore, this route provides ample opportunity for home exposures unless workers take proper hygienic precautions after work. For example, an entire family had elevated levels of chlordecone (Keone) in their blood, attributed to home laundering of a worker’s clothes (Grandjean and Bach 1986). Household exposure to TCDD (dioxin) has been documented by the occurrence of chloracne in the son and wife of two workers exposed in the aftermath of an explosion (Jensen, Sneddon and Walker 1972).
Most of the possible exposures to infants arise from pesticide applications within and around the home (Lewis, Fortmann and Camann 1994). Dust in home carets has been found to be extensively contaminated with numerous pesticides (Fenske et al. 1994). Much of reported home contamination has been attributed to flea extermination or to lawn and garden application of pesticides (Davis, Bronson and Garcia 1992). Infant absorption of chloryrifos after treatment of homes for fleas has been predicted to exceed safe levels. Indeed, indoor air levels following such fumigation procedures do not always rapidly diminish to safe levels.
Breast milk is a potential source of pesticide exposure for the neonate. Human milk contamination with pesticides, especially the organochlorines, has been known for decades. Occupational and environmental exposures can lead to significant pesticide contamination of breast milk (D’Ercole et al. 1976; McConnell 1986). Organochlorines, which in the past have been resent in breast milk at excessive levels, are declining in developed countries, paralleling the decline in adipose concentrations that has occurred after restriction of these compounds. Therefore, DDT contamination of human milk is now highest in developing countries. There is little evidence of organohoshates in breast milk. This may be attributable to properties of water solubility and raid metabolism of these compounds in the body.
Ingestion of water contaminated with pesticides is also a potential health risk for the neonate. This problem is most renounced where infant formula must be reared using water. Otherwise, commercial infant formulae are relatively free of contaminants (National Research Council 1993). Food contamination with pesticides may also lead to infant exposure. Contamination of commercial milk, fruits and vegetables with pesticides exists at very low levels even in developed countries where regulation and monitoring are most vigorous (The Referee 1994). Although milk comprises most of the infant diet, fruits (especially ales) and vegetables (especially carrots) are also consumed in a significant amount by young children and therefore represent a possible source of pesticide exposure.
In the industrialized countries, including the United States and western Europe, most of the organochlorine pesticides, including DDT, chlordane, dieldrin and lindane, have been either banned, suspended or restricted since the 1970s (Maxcy Rosenau-Last 1994). pesticides still used for agricultural and non-agricultural purposes are regulated in terms of their levels in foods, water and pharmaceutical products. As a result of this regulation, the levels of pesticides in adipose tissue and human milk have significantly declined over the past four decades. However, the organochlorines are still widely used in developing countries, where, for example, lindane and DDT are among the most frequently employed pesticides for agricultural use and for malaria control (Awumbila and Bokuma 1994).
Lindane
Lindane is the γ-isomer and active ingredient of the technical grade of benzene hexachloride (BHC). BHC, also known as hexachlorocyclohexane (HCH), contains 40 to 90% of other isomers— α, β and δ. This organochlorine has been used as an agricultural and non-agricultural pesticide throughout the world since 1949. Occupational exposures may occur during the manufacture, formulation and application of BHC. Lindane as a pharmaceutical reparation in creams, lotions and shampoos is also widely used to treat scabies and body lice. Because these skin conditions commonly occur among infants and children, medical treatment can lead to absorption of BHC by infants through the skin. Neonatal exposure can also occur by inhalation of vapour or dust that may be brought home by a parent or that may linger after home use. Dietary intake is also a possible means of exposure to infants since BHC has been detected in human milk, dairy products and other foods, as have many organochlorine insecticides. Exposure through breast milk was more prevalent in the United States prior to the ban on the commercial production of lindane. According to the IARC (International Agency for Research on Cancer 1987), it is possible that hexachlorocyclohexane is carcinogenic to humans. However, evidence for adverse health outcomes among infants has been reported chiefly as effects on the neurological and haematooietic systems.
Household exposure to lindane has been described in the wife of a pesticide formulator, demonstrating the potential for similar neonatal exposures. The wife had 5 ng/ml of γ-BHC in her blood, a concentration lower than that of her husband (table 1) (Starr et al. 1974). presumably, γ-BHC was brought into the home on the body and/or clothes of the worker. Levels of γ-BHC in the woman and her husband were higher than those reported in children treated with lotion containing 0.3 to 1.0% BHC.
BHC in breast milk exists mainly as the β-isomer (Smith 1991). The half-life of the γ-isomer in the human body is approximately one day, while the β-isomer accumulates.
Table 1. Potential sources and levels of exposure to newborns
| Source of exposure | g-BHC in blood (ng/ml; ppb) |
|
| Occupational exposures | Low exposures High exposures |
5 36 |
| Adult male | Attempted suicide | 1300 |
| Child | Acute poisoning | 100-800 |
| Children | 1% BHC lotion (average) | 13 |
| Case report of home exposure1 | Husband Wife |
17 5 |
| Unexposed populations since1980 | Yugoslavia Africa Brazil India |
52 72 92 752 |
1Starr et al. (1974); other data from Smith (1991).
2Largely b-isomer.
Dermal absorption of lindane from pharmaceutical products is a function of the amount applied to the skin and duration of exposure. Compared with adults, infants and young children appear to be more susceptible to the toxic effects of lindane (Clement International Corporation 1992). One reason may be that dermal absorption is enhanced by increased permeability of the infant’s skin and a large surface-to-volume ratio. Levels in the neonate may persist longer because the metabolism of BHC is less efficient in infants and young children. In addition, exposure in neonates may be increased by licking or mouthing treated areas (Kramer et al. 1990). A hot shower or bath before dermal application of medical products may facilitate dermal absorption, thereby exacerbating toxicity.
In a number of reported cases of accidental lindane poisoning, overt toxic effects have been described, some in young children. In one case, a two-month-old infant died after multiple exposures to 1% lindane lotion, including a full-body application following a hot bath (Davies et al. 1983).
Lindane production and use is restricted in most developed countries. Lindane is still used extensively in other countries for agricultural purposes, as noted in a study of pesticide use on farms in Ghana, where lindane accounted for 35 and 85% of pesticide use for farmers and herdsmen, respectively (Awumbila and Bokuma 1994).
olychlorinated bihenyls
olychlorinated bihenyls were used from the mid-1940s until the late 1970s as insulating fluids in electrical capacitors and transformers. Residues are still resent in the environment because of pollution, which is due largely to improper disposal or accidental sills. Some equipment still in use or stored remains a potential source of contamination. An incident has been reported in which children had detectable levels of CBs in their blood following exposure while laying with capacitors (Wolff and Schecter 1991). Exposure in the wife of an exposed worker has also been reported (Fishbein and Wolff 1987).
In two studies of environmental exposures, re- and postnatal exposure to CBs has been associated with small but significant effects in children. In one study, slightly impaired motor development was detected among children whose mothers had immediate postnatal breast milk CB levels in the upper 95th percentile of the study group (Rogan et al. 1986). In the other, sensory deficits (as well as smaller gestational size) were seen among children with blood levels in approximately the to 25% (Jacobson et al. 1985; Fein et al. 1984). These exposure levels were in the upper range for the studies (above 3 m in mother’s milk (fat basis) and above 3 ng/ml in children’s blood), yet these are not excessively high. Common occupational exposures result in levels ten to 100 times higher (Wolff 1985). In both studies, effects were attributed to prenatal exposure. Such results however sound a cautionary note for unduly exposing neonates to such chemicals both pre- and postnatally.
Solvents
Solvents are a group of volatile or semi-volatile liquids that are used mainly to dissolve other substances. Exposure to solvents can occur in manufacturing processes, for example hexane exposure during distillation of petroleum products. For most persons, exposures to solvents will arise while these are being used on the job or in the home. Common industrial applications include dry cleaning, degreasing, painting and paint removal, and printing. Within the home, direct contact with solvents is possible during use of products such as metal cleaners, dry cleaning products, paint thinners or sprays.
The major routes of exposure for solvents in both adults and infants are through respiratory and dermal absorption. Ingestion of breast milk is one means of neonatal exposure to solvents derived from the parent’s work. Because of the brief half-life of most solvents, their duration in breast milk will be similarly short. However, following maternal exposure, some solvents will be resent in breast milk at least for a short time (at least one half-life). Solvents that have been detected in breast milk include tetrachloroethylene, carbon disulhide and halothane (an anaesthetic). A detailed review of potential infant exposure to tetrachloroethylene (TCE) has concluded that levels in breast milk can easily exceed recommended health risk guidelines (Schreiber 1993). Excess risk was highest for infants whose mothers might be exposed in the workplace (58 to 600 per million persons). For the highest non-occupational exposures, excess risks of 36 to 220 per 10 million persons were estimated; such exposures can exist in homes directly above dry-cleaners. It was further estimated that milk concentrations of TCE would return to “normal” (re-exposure) levels four to eight weeks after cessation of exposure.
Non-occupational exposures are possible for the infant in the home where solvents or solvent-based products are used. Indoor air has very low, but consistently detectable, levels of solvents like tetrachloroethylene. Water may also contain volatile organic compounds of the same type.
Mineral Dusts and Fibres: Asbestos, Fibreglass, Rock Wool, Zeolites, Talc
Mineral dust and fibre exposure in the workplace causes respiratory disease, including lung cancer, among workers. Dust exposure is a potential problem for the newborn if a parent carries articles into the home on the clothes or body. With asbestos, fibres from the workplace have been found in the home environment, and resulting exposures of family members have been termed bystander or family exposures. Documentation of familial asbestos disease has been possible because of the occurrence of a signal tumour, mesothelioma, that is primarily associated with asbestos exposure. Mesothelioma is a cancer of the leura or eritoneum (linings of lung and abdomen, respectively) that occurs following a long latency period, typically 30 to 40 years after the first asbestos exposure. The aetiology of this disease appears to be related only to the length of time after initial exposure, not to intensity or duration, nor to age at first exposure (Nicholson 1986; Otte, Sigsgaard and Kjaerulff 1990). Respiratory abnormalities have also been attributed to bystander asbestos exposure (Grandjean and Bach 1986). Extensive animal experiments support the human observations.
Most cases of familial mesothelioma have been reported among wives of exposed miners, millers, manufacturers and insulators. However, a number of childhood exposures have also been associated with disease. Quite a few of these children had initial contact that occurred at an early age (Dawson et al. 1992; Anderson et al. 1976; Roggli and Longo 1991). For example, in one investigation of 24 familial contacts with mesothelioma who lived in a crocidolite asbestos mining town, seven cases were identified whose ages were 29 to 39 years at diagnosis or death and whose initial exposure had occurred at less than one year of age (n=5) or at three years (n=2) (Hansen et al. 1993).
Exposure to asbestos is clearly causative for mesothelioma, but an epigenetic mechanism has been further pro[osed to account for unusual clustering of cases within certain families. Thus, the occurrence of mesothelioma among 64 persons in 27 families suggests a genetic trait that may render certain individuals more sensitive to the asbestos insult leading to this disease (Dawson et al. 1992; Bianchi, Brollo and Zuch 1993). However, it also has been suggested that exposure alone may provide an adequate explanation for the reported familial aggregation (Alderson 1986).
Other inorganic dusts associated with occupational disease include fibreglass, zeolites and talc. Both asbestos and fibreglass have been widely used as insulating materials. pulmonary fibrosis and cancer are associated with asbestos and much less clearly with fibreglass. Mesothelioma has been reported in areas of Turkey with indigenous exposures to natural zeolites. Exposures to asbestos may also arise from non-occupational sources. Diaers (“naies”) constructed from asbestos fibre were implicated as a source of childhood asbestos exposure (Li, Dreyfus and Antman 1989); however, parental clothing was not excluded as a source of asbestos contact in this report. Asbestos also has been found in cigarettes, hairdryers, floor tiles and some types of talcum powder. Its use has been eliminated in many countries. However, an important consideration for children is residual asbestos insulation in schools, which has been widely investigated as a potential public health problem.
Environmental Tobacco Smoke
Environmental tobacco smoke (ETS) is a combination of exhaled smoke and smoke emitted from the smoldering cigarette. Although ETS is not itself a source of occupational exposure that may affect the neonate, it is reviewed here because of its potential to cause adverse health effects and because it provides a good example of other aerosol exposures. Exposure of a non-smoker to ETS is often described as passive or involuntary smoking. prenatal exposure to ETS is clearly associated with deficits or impairments in foetal growth. It is difficult to distinguish postnatal outcomes from effects of ETS in the prenatal period, since parental smoking is rarely confined to one time or the other. However, there is evidence to support a relationship of postnatal exposure to ETS with respiratory illness and impaired lung function. The similarity of these findings to experiences among adults strengthens the association.
ETS has been well characterized and extensively studied in terms of human exposure and health effects. ETS is a human carcinogen (US Environmental protection Agency 1992). ETS exposure can be assessed by measuring levels of nicotine, a component of tobacco, and cotinine, its major metabolite, in biological fluids including saliva, blood and urine. Nicotine and cotinine have also been detected in breast milk. Cotinine has also been found in the blood and urine of infants who were exposed to ETS only by breast-feeding (Charlton 1994; National Research Council 1986).
Exposure of the neonate to ETS has been clearly established to result from paternal and maternal smoking in the home environment. Maternal smoking provides the most significant source. For example, in several studies urinary cotinine in children has been shown to correlate with the number of cigarettes smoked by the mother per day (Marbury, Hammon and Haley 1993). The major routes of ETS exposure for the neonate are respiratory and dietary (through breast milk). Day care centers represent another potential exposure situation; many child care facilities do not have a no-smoking policy (Sockrider and Coultras 1994).
Hospitalization for respiratory illness occurs more often among newborns whose parents smoke. In addition, the duration of hospital visits is longer among infants exposed to ETS. In terms of causation, ETS exposure has not been associated with specific respiratory diseases. There is evidence, however, that passive smoking increases the severity of re-existing illnesses such as bronchitis and asthma (Charlton 1994; Chilmonczyk et al. 1993; Rylander et al. 1993). Children and infants exposed to ETS also have higher frequencies of respiratory infections. In addition, smoking parents with respiratory illnesses can transmit airborne infections to infants by coughing.
Children exposed to ETS postnatally show small deficits in lung function which appear to be independent of prenatal exposures (Frischer et al. 1992). Although the ETS-related changes are small (0.5% decrement per year of forced expiratory volume), and while these effects are not clinically significant, they suggest changes in the cells of the developing lung that may portend later risk. parental smoking has also been associated with increased risk of otitis media, or middle ear effusion, in children from infancy to age nine. This condition is a common cause of deafness among children which can cause delays in educational progress. Associated risk is supported by studies attributing one-third of all cases of otitis media to parental smoking (Charlton 1994).
Radiation Exposures
Ionizing radiation exposure is an established health hazard which is generally the result of intense exposure, either accidental or for medical purposes. It can be damaging to highly proliferative cells, and can therefore be very harmful to the developing foetus or neonate. Radiation exposures that result from diagnostic x rays are generally very low level, and considered to be safe. A potential household source of exposure to ionizing radiation is radon, which exists in certain geographic areas in rock formations.
prenatal and postnatal effects of radiation include mental retardation, lower intelligence, growth retardation, congenital malformations and cancer. Exposure to high doses of ionizing radiation is also associated with increased prevalence of cancer. Incidence for this exposure is dependent upon dose and age. In fact, the highest relative risk observed for breast cancer (~9) is among women who were exposed to ionizing radiation at a young age.
Recently, attention has focused on the possible effects of non-ionizing radiation, or electromagnetic fields (EMF). The basis of a relationship between EMF exposure and cancer is not yet known, and the epidemiological evidence is still unclear. However, in several international studies an association has been reported between EMF and leukaemia and male breast cancer.
Childhood exposure to excessive sunlight has been associated with skin cancer and melanoma (Marks 1988).
Childhood Cancer
Although specific substances have not been identified, parental occupational exposures have been linked to childhood cancer. The latency period for developing childhood leukaemia can be two to 10 years following the onset of exposure, indicating that exposures in utero or in the early postnatal period may be implicated in the cause of this disease. Exposure to a number of organochlorine pesticides (BHC, DDT, chlordane) has been tentatively associated with leukaemia, although these data have not been confirmed in more detailed studies. Moreover, elevated risk of cancer and leukaemia has been reported for children whose parents engage in work that involves pesticides, chemicals and fumes (O’Leary et al. 1991). Similarly, risk of Ewing’s bone sarcoma in children was associated with parental occupations in agriculture or exposure to herbicides and pesticides (Holly et al. 1992).
Summary
Many nations attempt to regulate safe levels of toxic chemicals in ambient air and food products and in the workplace. Nevertheless, opportunities for exposure abound, and children are particularly susceptible to both absorption and to effects of toxic chemicals. It has been noted that “many of the 40,000 child lives lost in the developing world every day are a consequence of environmental abuses reflected in unsafe water supplies, disease, and malnutrition” (Schaefer 1994). Many environmental exposures are avoidable. Therefore, prevention of environmental diseases takes high priority as a defence against adverse health effects among children.
Preterm Delivery and Work
The reconciliation of work and maternity is an important public health issue in industrialized countries, where more than 50% of women of child-bearing age work outside the home. Working women, unions, employers, politicians and clinicians are all searching for ways of preventing work-induced unfavourable reproductive outcomes. Women want to continue working while pregnant, and may even consider their physician’s advice about lifestyle modifications during pregnancy to be overprotective and unnecessarily restrictive.
physiological Consequences of pregnancy
At this point, it would be useful to review a few of the physiological consequences of pregnancy that may interfere with work.
A pregnant woman undergoes profound changes which allow her to adapt to the needs of the foetus. Most of these changes involve the modification of physiological functions that are sensitive to changes of posture or physical activity—the circulatory system, the respiratory system and water balance. As a result, physically active pregnant women may experience unique physiological and physiopathological reactions.
The main physiological, anatomical, and functional modifications undergone by pregnant women are (Mamelle et al. 1982):
- An increase in peripheral oxygen demand, leading to modification of the respiratory and circulatory systems. Tidal volume begins to increase in the third month and may amount to 40% of re-pregnancy values by the end of the pregnancy. The resultant increase in gas exchange may increase the hazard of the inhalation of toxic volatiles, while hyperventilation related to increased tidal volume may cause shortness of breath on exertion.
- Cardiac output increases from the very beginning of pregnancy, as a result of an increase in blood volume. This reduces the heart’s ability to adapt to exertion and also increases venous pressure in the lower limbs, rendering standing for long periods difficult.
- Anatomical modifications during pregnancy, including exaggeration of dorsolumbar lordosis, enlargement of the polygon of support and increases in abdominal volume, affect static activities.
- A variety of other functional modifications occur during pregnancy. Nausea and vomiting result in fatigue; daytime sleepiness results in inattention; mood changes and feelings of anxiety may lead to interpersonal conflicts.
- Finally, it is interesting to note that the daily energy requirements during pregnancy are equivalent to the requirements of two to four hours of work.
Because of these profound changes, occupational exposures may have special consequences in pregnant women and may result in unfavourable pregnancy outcomes.
Epidemiological Studies of Working Conditions and preterm Delivery
Although there are many possible unfavourable pregnancy outcomes, we review here the data on preterm delivery, defined as the birth of a child before the 37th week of gestation. preterm birth is associated with low birth weight and with significant complications for the newborn. It remains a major public health concern and is an ongoing reoccupation among obstetricians.
When we began research in this field in the mid-1980s, there was relatively strong legislative protection of pregnant women’s health in France, with prenatal maternity leave mandated to start six weeks prior to the due date. Although the preterm delivery rate has fallen from 10 to 7% since then, it appeared to have levelled off. Because medical prevention had apparently reached the limit of its powers, we investigated risk factors likely to be amenable to social intervention. Our hypotheses were as follows:
- Is working per se a risk factor for preterm birth?
- Are certain occupations associated with an increased risk of preterm delivery?
- Do certain working conditions constitute a hazard to the pregnant woman and foetus?
- Are there social preventive measures which could help reduce the risk of preterm birth?
Our first study, conducted in 1977–78 in two hospital maternity wards, examined 3,400 women, of whom 1,900 worked during pregnancy and 1,500 remained at home (Mamelle, Laumon and Lazar 1984). The women were interviewed immediately after delivery and asked to describe their home and work lifestyle during pregnancy as accurately as possible.
We obtained the following results:
Work per se
The mere fact of working outside the home cannot be considered to be a risk factor for preterm delivery, since women remaining at home exhibited a higher prematurely rate than did women who worked outside the home (7.2 versus 5.8%).
Working conditions
An excessively long work week appears to be a risk factor, since there was a regular increase in preterm delivery rate with the number of work hours. Retail-sector workers, medical social workers, specialized workers and service personnel were at higher risk of preterm delivery than were office workers, teachers, management, skilled workers or supervisors. The prematurely rates in the two groups were 8.3 and 3.8% respectively.
Table 1. Identified sources of occupational fatigue
| Occupational fatigue index | “HIGH” index if: |
| Posture | Standing for more than 3 hours per day |
| Work on machines | Work on industrial conveyor belts; independent work on industrial machines with strenuous effort |
| Physical load | Continuous or periodical physical effort; carrying loads of more than 10kg |
| Mental load | Routine work; varied tasks requiring little attention without stimulation |
| Environment | Significant noise level; cold temperature; very wet atmosphere; handling of chemical substances |
Source: Mamelle, Laumon and Lazar 1984.
Task analysis allowed identification of five sources of occupation fatigue: posture, work with industrial machines, physical workload, mental workload and the work environment. Each of these sources of occupational fatigue constitutes a risk factor for preterm delivery (see tables 1 and 2).
Table 2. Relative risks (RR) and fatigue indices for preterm delivery
| Index | Low index % | High index % | RR | Statistical significance |
| Posture | 4.5 | 7.2 | 1.6 | Significant |
| Work on machines | 5.6 | 8.8 | 1.6 | Significant |
| Physical load | 4.1 | 7.5 | 1.8 | Highly significant |
| Mental load | 4.0 | 7.8 | 2.0 | Highly significant |
| Environment | 4.9 | 9.4 | 1.9 | Highly significant |
Source: Mamelle, Laumon and Lazar 1984.
Exposure to multiple sources of fatigue may result in unfavourable pregnancy outcomes, as evidenced by the significant increase of the rate of preterm delivery with an increased number of sources of fatigue (table 3). Thus, 20% of women had concomitant exposure to at least three sources of fatigue, and experienced a preterm delivery rate twice as high as other women. Occupational fatigue and excessively long work weeks exert cumulative effects, such that women who experience intense fatigue during long work weeks exhibit an even higher prematurely rate. preterm delivery rates increase further if the woman also has a medical risk factor. The detection of occupational fatigue is therefore even more important than the detection of medical risk factors.
Table 3. Relative risk of prematurity according to number of occupational fatigue indices
| Number of high fatigue indices |
Proportion of exposed women % |
Estimated relative risk |
| 0 | 24 | 1.0 |
| 1 | 28 | 2.2 |
| 2 | 25 | 2.4 |
| 3 | 15 | 4.1 |
| 4-5 | 8 | 4.8 |
Source: Mamelle, Laumon and Lazar 1984
European and North American studies have confirmed our results, and our fatigue scale has been shown to be reproducible in other surveys and countries.
In a case-control follow-u study conducted in France a few years later in the same maternity wards (Mamelle and Munoz 1987) , only two of the five previously defined indices of fatigue were significantly related to preterm delivery. It should however be noted that women had a greater opportunity to sit down and were withdrawn from physically demanding tasks as a result of preventive measures implemented in the workplaces during this period. The fatigue scale nevertheless remained a predictor of preterm delivery in this second study.
In a study in Montreal, Quebec (McDonald et al. 1988), 22,000 pregnant women were interviewed retrospectively about their working conditions. Long work weeks, alternating shift work and carrying heavy loads were all shown to exert significant effects. The other factors studied did not appear to be related to preterm delivery, although there appears to be a significant association between preterm delivery and a fatigue scale based on the total number of sources of fatigue.
With the exception of work with industrial machines, no significant association between working conditions and preterm delivery was found in a French retrospective study of a representative sample of 5,000 pregnant women (Saurel-Cubizolles and Kaminski 1987). However, a fatigue scale inspired by our own was found to be significantly associated with preterm delivery.
In the United States, Homer, Beredford and James (1990), in a historical cohort study, confirmed the association between physical workload and an increased risk of preterm delivery. Teitelman and co-workers (1990), in a prospective study of 1,200 pregnant women, whose work was classified as sedentary, active or standing, on the basis of job description, demonstrated an association between work in a standing position and preterm delivery.
Barbara Luke and co-workers (in press) conducted a retrospective study of US nurses who worked during pregnancy. Using our occupational risk scale, she obtained similar results to ours, that is, an association between preterm delivery and long work weeks, standing work, heavy workload and unfavourable work environment. In addition, the risk of preterm delivery was significantly higher among women with concomitant exposure to three or four sources of fatigue. It should be noted that this study included over half of all nurses in the United States.
Contradictory results have however been reported. These may be due to small sample sizes (Berkowitz 1981), different definitions of prematurely (Launer et al. 1990) and classification of working conditions on the basis of job description rather than actual workstation analysis (Klebanoff, Shiono and Carey 1990). In some cases, workstations have been characterized on a theoretical basis only—by the occupational physician, for example, rather than by the women themselves (peoples-Shes et al. 1991). We feel that it is important to take subjective fatigue—that is, fatigue as it is described and experienced by women—into account in the studies.
Finally, it is possible that the negative results are related to the implementation of preventive measures. This was the case in the prospective study of Ahlborg, Bodin and Hogstedt (1990), in which 3,900 active Swedish women completed a self-administered questionnaire at their first prenatal visit. The only reported risk factor for preterm delivery was carrying loads weighing more than 12 kg more often than 50 times per week, and even then the relative risk of 1.7 was not significant. Ahlborg himself points out that preventive measures in the form of aid maternity leave and the right to perform less tiring work during the two months receding their due date had been implemented for pregnant women engaged in tiring work. Maternity leaves were five times as frequent among women who described their work as tiring and involving the carrying of heavy loads. Ahlborg concludes that the risk of preterm delivery may have been minimized by these preventive measures.
preventive Interventions: French Examples
Are the results of aetiological studies convincing enough for preventive interventions to be applied and evaluated? The first question which must be answered is whether there is a public health justification for the application of social preventive measures designed to reduce the rate of preterm delivery.
Using data from our previous studies, we have estimated the proportion of preterm births caused by occupational factors. Assuming a rate of preterm delivery of 10% in populations exposed to intense fatigue and a rate of 4.5% in non-exposed populations, we estimate that 21% of premature births are caused by occupational factors. Reducing occupational fatigue could therefore result in the elimination of one-fifth of all preterm births in French working women. This is ample justification for the implementation of social preventive measures.
What preventive measures can be applied? The results of all the studies lead to the conclusion that working hours can be reduced, fatigue can be lessened through workstation modification, work breaks can be allowed and prenatal leave can be lengthened. Three cost-equivalent alternatives are available:
- reducing the work week to 30 hours starting from the 20th week of gestation
- prescribing a work break of one week each month starting in the 20th week of gestation
- beginning prenatal leave at the 28th week of gestation.
It is relevant to recall here that French legislation provides the following preventive measures for pregnant women:
- guaranteed employment after childbirth
- reduction of the workday by 30 to 60 minutes, applied through collective agreements
- workstation modification in cases of incompatibility with pregnancy
- work breaks during pregnancy, prescribed by attending physicians
- prenatal maternity leave six weeks prior to the due date, with a further two weeks available in case of complications
- postnatal maternity leave of ten weeks.
A one-year prospective observational study of 23,000 women employed in 50 companies in the Rhône-Ales region of France (Bertucat, Mamelle and Munoz 1987) examined the effect of tiring work conditions on preterm delivery. Over the period of the study, 1,150 babies were born to the study population. We analysed the modifications of working conditions to accommodate pregnancy and the relation of these modifications to preterm delivery (Mamelle, Bertucat and Munoz 1989), and observed that:
- Workstation modification was reformed for only 8% of women.
- 33% of women worked their normal shifts, with the others having their workday reduced by 30 to 60 minutes.
- 50% of women took at least one work break, apart from their prenatal maternity leave; fatigue was the cause in one-third of cases.
- 90% of women stopped working before their legal maternity leave began and obtained at least the two weeks leave allowed for in the case of complications of pregnancy; fatigue was the cause in half the cases.
- In all, given the legal prenatal leave period of six weeks prior to the due date (with an additional two weeks available in some cases), the real duration of prenatal maternity leave was 12 weeks in this population of women subjected to tiring work conditions.
Do these modifications of work have any effect on the outcome of pregnancy? Workstation modification and the slight reduction of the workday (30 to 60 min) were both associated with non-significant reductions of the risk of preterm delivery. We believe that further reductions of the work week would have a greater effect (table 4).
Table 4. Relative risks of prematurity associated with modifications in working conditions
| Modifications in working conditions |
Number of women | Preterm birth rates (%) |
Relative risk (95% confidence intervals) |
| Change in work situation | |||
| No Yes |
1,062 87 |
6.2 3.4 |
0.5 (0.2-1.6) |
| Reduction of weekly working hours | |||
| No Yes |
388 761 |
7.7 5.1 |
0.7 (0.4-1.1) |
| Episodes of sick leave1 | |||
| No Yes |
357 421 |
8.0 3.1 |
0.4 (0.2-0.7) |
| Increase of antenatal maternity leave1 | |||
| None or only additional 2 weeks Yes |
487 291 |
4.3 7.2 |
1.7 (0.9-3.0) |
1 In a reduced sample of 778 women with no previous or present obstetric pathology.
Source: Mamelle, Bertucat and Munoz 1989.
To analyse the relation between prenatal leave, work breaks and preterm delivery, it is necessary to discriminate between preventive and curative work breaks. This requires restriction of the analysis to women with uncomplicated pregnancies. Our analysis of this subgroup revealed a reduction of the preterm delivery rate among women who took work breaks during their pregnancy, but not in those who took prolonged prenatal leave (Table 9).
This observational study demonstrated that women who work in tiring conditions take more work breaks during their pregnancies than do other women, and that these breaks, particularly when motivated by intense fatigue, are associated with reductions of the risk of preterm delivery (Mamelle, Bertucat and Munoz 1989).
Choice of preventive Strategies in France
As epidemiologists, we would like to see these observations verified by experimental preventive studies. We must however ask ourselves which is more reasonable: to wait for such studies or to recommend social measures aimed at preventing preterm delivery now?
The French Government recently decided to include a “work and pregnancy guide”, identical to our fatigue scale, in each pregnant woman’s medical record. Women can thus calculate their fatigue score for themselves. If work conditions are arduous, they may ask the occupational physician or the person responsible for occupational safety in their company to implement modifications aimed at alleviating their workload. Should this be refused, they can ask their attending physician to prescribe rest weeks during their pregnancy, and even to prolong their prenatal maternity leave.
The challenge is now to identify preventive strategies that are well adapted to legislation and social conditions in every country. This requires a health economics approach to the evaluation and comparison of preventive strategies. Before any preventive measure can be considered generally applicable, many factors have to be taken into consideration. These include effectiveness, of course, but also low cost to the social security system, resultant job creation, women’s references and the acceptability to employers and unions.
This type of problem can be resolved using multicriteria methods such as the Electra method. These methods allow both the classification of preventive strategies on the basis of each of a series of criteria, and the weighting of the criteria on the basis of political considerations. Special importance can thus be given to low cost to the social security system or to the ability of women to choose, for example (Mamelle et al. 1986). While the strategies recommended by these methods vary depending on the decision makers and political options, effectiveness is always maintained from the public health standpoint.
Maternal Occupational Exposures and Adverse Pregnancy Outcomes
Paid employment among women is growing worldwide. For example, almost 70% of women in the United States are employed outside the home during their predominant childbearing years (ages 20 to 34). Furthermore, since the 1940s there has been an almost linear trend in synthetic organic chemical production, creating a more hazardous environment for the pregnant worker and her offspring.
Ultimately, a couple’s reproductive success depends on a delicate physiochemical balance within and between the father, the mother and the foetus. Metabolic changes occurring during a pregnancy can increase exposure to hazardous toxicants for both worker and concetus. These metabolic changes include increased pulmonary absorption, increased cardiac output, delayed gastric emptying, increased intestinal motility and increased body fat. As shown in figure 1, exposure of the concetus can produce varying effects depending on the phase of development—early or late embryogenesis or the foetal period.
Figure 1. Consequences of maternal exposure to toxicants on the offspring.
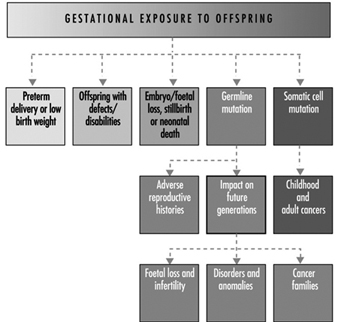
Transport time of a fertilized ovum before implantation is between two and six days. During this early stage the embryo may be exposed to chemical compounds that penetrate into the uterine fluids. Absorption of xenophobic compounds may be accompanied by degenerative changes, alteration in the blastocystic protein profile or failure to implant. Insult during this period is likely to lead to a spontaneous abortion. Based on experimental data, it is thought that the embryo is fairly resistant to teratogenic insult at this early stage because the cells have not initiated the complex sequence of chemical differentiation.
The period of later embryogenesis is characterized by differentiation, mobilization and organization of cells and tissue into organ rudiments. Early pathogenesis may induce cell death, failed cellular interaction, reduced biosynthesis, impaired morphogenic movement, mechanical disruption, adhesions or oedema (Paul 1993). The mediating factors that determine susceptibility include route and level of exposure, pattern of exposure and foetal and maternal genotype. Extrinsic factors such as nutritional deficiencies, or the additive, synergistic or antagonistic effects associated with multiple exposures may further impact the response. Untoward responses during late embryogenesis may culminate in spontaneous abortion, gross structural defects, foetal loss, growth retardation or developmental abnormalities.
The foetal period extends from embryogenesis to birth and is defined as beginning at 54 to 60 gestational days, with the concetus having a crown-rum length of 33 mm. The distinction between the embryonic and foetal period is somewhat arbitrary. The foetal period is characterized developmentally by growth, histogenesis and functional maturation. Toxicity may be manifested by a reduction in cell size and number. The brain is still sensitive to injury; myelination is incomplete until after birth. Growth retardation, functional defects, disruption in the pregnancy, behavioural effects, translacental carcinogenesis or death may result from toxicity during the foetal period. This article discusses the biological, sociological and epidemiological effects of maternal environmental/occupational exposures.
Embryonic/Foetal Loss
The developmental stages of the zygote, defined in days from ovulation (DOV), proceed from the blastocyst stage at days 15 to 20 (one to six DOV), with implantation occurring on day 20 or 21 (six or seven DOV), to the embryonic period from days 21 to 62 (seven to 48 DOV), and the foetal period from day 63 (49+ DOV) until the designated period of viability, ranging from 140 to 195 days. Estimates of the probability of pregnancy termination at one of these stages depend on both the definition of foetal loss and the method used to measure the event. Considerable variability in the definition of early versus late foetal loss exists, ranging from the end of week 20 to week 28. The definitions of foetal and infant death recommended by the World Health Organization (1977) are listed in table 1. In the United States the gestational age setting the lower limit for stillbirths is now widely accepted to be 20 weeks.
Table 1. Definition of foetal loss and infant death
| Spontaneous abortion | ≤500 g or 20-22 weeks or 25 cm length |
| Stillbirth | 500 g (1000 g International) nonviable |
| Early neonatal death | Death of a live-born infant ≤7 days (168 hours) |
| Late neonatal death | 7 days to ≤28 days |
Source: World Health Organization 1977.
Because the majority of early aborted foetuses have chromosomal anomalies, it has been suggested that for research purposes a finer distinction should be made—between early foetal loss, before 12 weeks’ gestation, and later foetal loss (Källén 1988). In examining late foetal losses it also may be appropriate to include early neonatal deaths, as the cause may be similar. WHO defines early neonatal death as the death of an infant aged seven days or younger and late neonatal death as occurring between seven and 29 days. In studies conducted in developing countries, it is important to distinguish between prepartum and intrapartum deaths. Because of problematic deliveries, intrapartum deaths account for a large portion of stillbirths in less developed countries.
In a review by Kline, Stein and Susser (1989) of nine retrospective or cross-sectional studies, the foetal loss rates before 20 weeks’ gestation ranged from 5.5 to 12.6%. When the definition was expanded to include losses u to 28 weeks’ gestation, the foetal loss rate varied between 6.2 and 19.6%. The rates of foetal loss among clinically recognized pregnancies in four prospective studies, however, had a relatively narrow range of 11.7 to 14.6% for the gestational period u to 28 weeks. This lower rate, seen in prospective versus retrospective or cross-sectional designs, may be attributable to differences in underlying definitions, misreporting of induced abortions as spontaneous or misclassification of delayed or heavy menses as foetal loss.
When occult abortions or early “chemical” losses identified by an elevated level of human chorionic gonadotrohins (hCG) are included, the total spontaneous abortion rate jumps dramatically. In a study using hCG methods, the incidence of post-implantation subclinical loss of fertilized ova was 22% (Wilcox et al. 1988). In these studies urinary hCG was measured with immunoradiometric assay using a detection antibody. The assay originally used by Wilcox employed a now extinct high affinity, polyclonal rabbit antibody. More recent studies have used an inexhaustible monoclonal antibody that requires less than 5 ml of urine for replicate samples. The limiting factor for use of these assays in occupational field studies is not only the cost and resources needed to coordinate collection, storage and analysis of urine samples but the large population needed. In a study of early pregnancy loss in women workers exposed to video display terminals (VDTs), approximately 7,000 women were screened in order to acquire a usable population of 700 women. This need for ten times the population size in order to achieve an adequate sample stems from reduction in the available number of women because of ineligibility due to age, sterility and the enrollment exclusively of women who are using either no contraceptives or relatively ineffective forms of contraception.
More conventional occupational studies have used recorded or questionnaire data to identify spontaneous abortions. Recorded data sources include vital statistics and hospital, private practitioner and outpatient clinic records. Use of record systems identifies only a subset of all foetal losses, principally those that occur after the start of prenatal care, typically after two to three missed periods. Questionnaire data are collected by mail or in personal or telephone interviews. By interviewing women to obtain reproductive histories, more complete documentation of all recognized losses is possible. Questions that are usually included in reproductive histories include all pregnancy outcomes; prenatal care; family history of adverse pregnancy outcomes; marital history; nutritional status; re-pregnancy weight; height; weight gain; use of cigarettes, alcohol and prescription and nonprescription drugs; health status of the mother during and prior to a pregnancy; and exposures at home and in the workplace to physical and chemical agents such as vibration, radiation, metals, solvents and pesticides. Interview data on spontaneous abortions can be a valid source of information, particularly if the analysis includes those of eight weeks’ gestation or later and those that occurred within the last 10 years.
The principal physical, genetic, social and environmental factors associated with spontaneous abortion are summarized in table 2. To ensure that the observed exposure-effect relationship is not due to a confounding relationship with another risk factor, it is important to identify the risk factors that may be associated with the outcome of interest. Conditions associated with foetal loss include syphilis, rubella, genital Mycolasma infections, herpes simplex, uterine infections and general hyperpyrexia. One of the most important risk factors for clinically recognized spontaneous abortion is a history of pregnancy ending in foetal loss. Higher gravidity is associated with increased risk, but this may not be independent of a history of spontaneous abortion. There are conflicting interpretations of gravidity as a risk factor because of its association with maternal age, reproductive history and heterogeneity of women at different gravidity ranks. Rates of spontaneous abortion are higher for women younger than 16 and older than 36 years. After adjusting for gravidity and a history of pregnancy loss, women older than 40 were shown to have twice the risk of foetal loss of younger women. The increased risk for older women has been associated with an increase in chromosomal anomalies, particularly trisomy. possiblemale-mediated effects associated with foetal loss have been recently reviewed (Savitz, Sonnerfeld and Olshaw 1994). A stronger relationship was shown with paternal exposure to mercury and anaesthetic gases, as well as a suggestive but inconsistent relationship with exposure to lead, rubber manufacturing, selected solvents and some pesticides.
Table 2. Factors associated with small for gestational age and foetal loss
| Small for gestational age | |
| Physical-genetic | Environmental-social |
| Preterm delivery Multiple births Malformed foetus Hypertension Placental or cord anomaly Maternal medical history History of adverse pregnancy outcomes Race Chromosome anomalies Sex Maternal height, weight, weight gain Paternal height Parity Length of gestation Short interval between pregnancies |
Malnutrition Low income/poor education Maternal smoking Maternal alcohol consumption Occupational exposure Psychosocial stress Altitude History of infections Marijuana use |
| Foetal loss | |
| Physical-genetic | Environmental-social |
| Higher gravidity Maternal age Birth order Race Repeat spontaneous abortion Insulin dependent diabetes Uterine disorders Twinning Immunological factor Hormonal factors |
Socio-economic status Smoking history Prescribed and recreational drugs Alcohol use Poor nutrition Infections/maternal fever Spermicides Employment factors Chemical exposure Irradiation |
Employment status may be a risk factor regardless of a specific physical or chemical hazard and may act as a confounder in assessment of occupational exposure and spontaneous abortion. Some investigators suggest that women who stay in the workforce are more likely to have an adverse pregnancy history and as a result are able to continue working; others believe this group is an inherently more fit subpopulation due to higher incomes and better prenatal care.
Congenital Anomalies
During the first 60 days after conception, the developing infant may be more sensitive to xenobiotic toxicants than at any other stage in the life cycle. Historically, terata and congenital malformations referred to structural defects resent at birth that may be gross or microscopic, internal or external, hereditary or nonhereditary, single or multiple. Congenital anomaly, however, is more broadly defined as including abnormal behaviour, function and biochemistry. Malformations may be single or multiple; chromosomal defects generally produce multiple defects, whereas single-gene changes or exposure to environmental agents may cause either single defects or a syndrome.
The incidence of malformations depends on the status of the concetus—live birth, spontaneous abortus, stillbirth. Overall, the abnormality rate in spontaneous abortuses is approximately 19%, a tenfold increase in what is seen in the live born (Sheard, Fantel and Fitsimmons 1989). A 32% rate of anomalies was found among stillborn foetuses weighing more than 500 g. The incidence of major defects in live births is about 2.24% (Nelson and Holmes 1989). The prevalence of minor defects ranges between 3 and 15% (averaging about 10%). Birth anomalies are associated with genetic factors (10.1%), multifactorial inheritance (23%), uterine factors (2.5%), twinning (0.4%) or teratogens (3.2%). The causes of the remaining defects are unknown. Malformation rates are approximately 41% higher for boys than for girls and this is explained by the significantly higher rate of anomalies for male genital organs.
One challenge in studying malformations is deciding how to group defects for analysis. Anomalies can be classified by several parameters, including seriousness (major, minor), pathogenesis (deformation, disruption), associated versus isolated, anatomic by organ system, and aetiological (e.g., chromosomal, single gene defects or teratogen induced). Often, all malformations are combined or the combination is based either on major or minor categorization. A major malformation can be defined as one that results in death, requires surgery or medical treatment or constitutes a substantial physical or psychological handicap. The rationale for combining anomalies into large groups is that the majority arise, at approximately the same time period, during organogenesis. Thus, by maintaining larger sample sizes, the total number of cases is increased with a concomitant increase in the statistical power. If, however, the exposure effect is specific to a particular type of malformation (e.g., central nervous system), such grouping may mask the effect. Alternatively, malformations may be grouped by organ system. Though this method may be an improvement, certain defects may dominate the class, such as varus deformities of the feet in the musculoskeletal system. Given a sufficiently large sample, the optimal approach is to divide the defects into embryologically or pathogenetically homogenous groups (Källén 1988). Considerations should be given to the exclusion or inclusion of certain malformations, such as those that are likely caused by chromosomal defects, autosomal dominant conditions or malposition in utero. Ultimately, in analysing congenital anomalies, a balance has to be maintained between maintaining precision and compromising statistical power.
A number of environmental and occupational toxicants have been associated with congenital anomalies in offspring. One of the strongest associations is maternal consumption of food contaminated with methylmercury causing morphological, central nervous system and neurobehavioural abnormalities. In Japan, the cluster of cases was linked to consumption of fish and shellfish contaminated with mercury derived from the effluent of a chemical factory. The most severely affected offspring developed cerebral palsy. Maternal ingestion of polychlorinated biphenyl’s (CBs) from contaminated rice oil gave rise to babies with several disorders, including growth retardation, dark brown skin pigmentation, early eruption of teeth, gingival hyperplasia, wide sagittal suture, facial oedema and exophthalmoses. Occupations involving exposures to mixtures have been linked with a variety of adverse outcomes. The offspring of women working in the ul and aer industry, in either laboratory work or jobs involving “conversions” or aer refinement, also had increased risk of central nervous system, heart and oral cleft defects. Women working in industrial or construction work with unspecified exposures had a 50% increase in central nervous system defects, and women working in transportation and communication had two times the risk of having a child with an oral cleft. Veterinarians represent a unique group of health care personnel exposed to anaesthetic gases, radiation, trauma from animal kicks, insecticides and zoonotic diseases. Though no difference was found in the rate of spontaneous abortions or in birth weight of the offspring between female veterinarians and female lawyers, there was a significant excess of birth defects among veterinarians (Schenker et al. 1990). Lists of known, possible and unlikely teratogens are available as well as computer databases and risk lines for obtaining current information on potential teratogens (Paul 1993). Evaluating congenital anomalies in an occupational cohort is particularly difficult, however, because of the large sample size needed for statistical power and our limited ability to identify specific exposures occurring during a narrow window of time, primarily the first 55 days of gestation.
Small for Gestational Age
Among the many factors linked with infant survival, physical underdevelopment associated with low birth weight (LBW) resents one of the greatest risks. Significant weight gain of the foetus does not begin until the second trimester. The concetus weighs 1 g at eight weeks, 14 g at 12 weeks, and reaches 1.1 kg at 28 weeks. An additional 1.1 kg is gained every six weeks thereafter until term. The normal newborn weighs approximately 3,200 g at term. The newborn’s weight is dependent on its rate of growth and its gestational age at delivery. An infant that is growth retarded is said to be small for gestational age (SGA). If an infant is delivered prior to term it will have a reduced weight but will not necessarily be growth retarded. Factors associated with a preterm delivery are discussed elsewhere, and the focus of this discussion is on the growth-retarded newborn. The terms SGA and LBW will be used interchangeably. A low birth-weight infant is defined as an infant weighing less than 2,500 g, a very low birth weight is defined as less than 1,500 g, and extremely low birth weight is one that is less than 1,000 g (WHO 1969).
When examining causes of reduced growth, it is important to distinguish between asymmetrical and symmetrical growth retardation. Asymmetrical growth retardation, i.e., where the weight is affected more than the skeletal structure, is primarily associated with a risk factor operating during late pregnancy. On the other hand, symmetrical growth retardation may more likely be associated with an aetiology that operates over the entire period of gestation (Kline, Stein and Susser 1989). The difference in rates between asymmetrical and symmetrical growth retardation is especially apparent when comparing developing and developed countries. The rate of growth retardation in developing countries is 10 to 43%, and is primarily symmetrical, with the most important risk factor being poor nourishment. In developed countries foetal growth retardation is usually much lower, 3 to 8%, and is generally asymmetrical with a multifactorial aetiology. Hence, worldwide, the proportion of low birth-weight infants defined as intrauterine growth retarded rather than preterm varies dramatically. In Sweden and the United States, the proportion is approximately 45%, while in developing countries, such as India, the proportion varies between approximately 79 and 96% (Villar and Belizan 1982).
Studies of the Dutch famine showed that starvation confined to the third trimester depressed foetal growth in an asymmetric pattern, with birth weight being primarily affected and head circumference least affected (Stein, Susser and Saenger 1975). Asymmetry of growth also has been observed in studies of environmental exposures. In a study of 202 expectant mothers residing in neighbourhoods at high risk for lead exposures, prenatal maternal blood samples were collected between the sixth and the 28th week of gestation (Bornschein, Grote and Mitchell 1989). Blood lead levels were associated with both a decreased birth weight and length, but not head circumference, after adjustment for other relevant risk factors including length of gestation, socioeconomic status and use of alcohol or cigarettes. The finding of maternal blood lead as a factor in birth length was seen entirely in Caucasian infants. The birth length of Caucasian infants decreased approximately 2.5 cm per log unit increment in maternal blood lead. Care should be given to selection of the outcome variable. If only birth weight had been selected for study, the finding of the effects of lead on other growth parameters might have been missed. Also, if Caucasians and African Americans had been pooled in the above analysis, the differential effects on Caucasians, perhaps due to genetic differences in the storage and binding capacity of lead, may have been missed. A significant confounding effect also was observed between prenatal blood lead and maternal age and the birth weight of the offspring after adjustment for other covariables. The findings indicate that for a 30-year-old woman with an estimated blood lead level of about 20 mg/dl, the offspring weighed proximately 2,500 g compared with proximately 3,000 g for a 20-year-old with similar lead levels. The investigators speculated that this observed difference may indicate that older women are more sensitive to the additional insult of lead exposure or that older women may have had higher total lead burden from greater numbers of years of exposure or higher ambient lead levels when they were children. Another factor may be increased blood pressure. Nonetheless, the important lesson is that careful examination of high-risk subpopulations by age, race, economic status, daily living habits, sex of the offspring and other genetic differences may be necessary in order to discover the more subtle effects of exposures on foetal growth and development.
Risk factors associated with low birth weight are summarized in Table 5. Social class as measured by income or education persists as a risk factor in situations in which there are no ethnic differences. Other factors that may be operating under social class or race may include cigarette smoking, physical work, prenatal care and nutrition. Women between the ages of 25 and 29 are least likely to deliver a growth-retarded offspring. Maternal smoking increases the risk of low birth-weight offspring by about 200% for heavy smokers. Maternal medical conditions associated with LBW include placental abnormalities, heart disease, viral pneumonia, liver disease, re-eclamsia, eclamsia, chronic hypertension, weight gain and hyeremesis. An adverse pregnancy history of foetal loss, preterm delivery or prior LBW infant increases the risk of a current preterm low birth-weight infant two- to fourfold. An interval between births of less than a year triples the risk of having a low birth-weight offspring. Chromosomal anomalies associated with abnormal growth include Down’s syndrome, trisomy 18 and most malformation syndromes.
Smoking cigarettes is one of the primary behaviours most directly linked with lower weight offspring. Maternal smoking during pregnancy has been shown to increase the risk of a low birth-weight offspring two to three times and to cause an overall weight deficit of between 150 and 400 g. Nicotine and carbon monoxide are considered the most likely causative agents since both are rapidly and referentially transferred across the placenta. Nicotine is a powerful vasoconstrictor, and significant differences in the size of umbilical vessels of smoking mothers have been demonstrated. Carbon monoxide levels in cigarette smoke range from 20,000 to 60,000 m. Carbon monoxide has an affinity for haemoglobin 210 times that of oxygen, and because of lower arterial oxygen tension the foetus is especially compromised. Others have suggested that these effects are not due to smoking but are attributable to characteristics of smokers. Certainly occupations with potential carbon monoxide exposure, such as those associated with ul and aer, blast furnaces, acetylene, breweries, carbon black, coke ovens, garages, organic chemical synthesizers and petroleum refineries should be considered possible high risk occupations for pregnant employees.
Ethanol is also a widely used and researched agent associated with foetal growth retardation (as well as congenital anomalies). In a prospective study of 9,236 births, it was found that maternal alcohol consumption of more than 1.6 oz per day was associated with an increase in stillbirths and growth-retarded infants (Kaminski, Rumeau and Schwartz 1978). Smaller infant length and head circumference also are related to maternal alcohol ingestion.
In evaluating the possible effects of exposures on birth weight, some problematic issues must be considered. preterm delivery should be considered as a possible mediating outcome and the potential effects on gestational age considered. In addition, pregnancies having longer gestational length also have a longer opportunity for exposure. If enough women work late in pregnancy, the longest cumulative exposure may be associated with the oldest gestational ages and heaviest babies purely as an artifact. There are a number of procedures that can be used to overcome this problem including a variant of the Cox life-table regression model, which has the ability to handle time-dependent covariables.
Another problem centres on how to define lowered birth weight. Often studies define lower birth weight as a dichotomous variable, less than 2,500 g. The exposure, however, must have a very powerful effect in order to produce a drastic drop in the infant’s weight. Birth weight defined as a continuous variable and analysed in a multiple regression model is more sensitive for detecting subtle effects. The relative paucity of significant findings in the literature in relationship to occupational exposures and SGA infants may, in art, be caused by ignoring these design and analysis issues.
Conclusions
Studies of adverse pregnancy outcomes must characterize exposures during a fairly narrow window of time. If the woman has been transferred to another job or laid off work during a critical period of time such as organogenesis, the exposure-effect relationship can be severely altered. Therefore, the investigator is held to a high standard of identifying the woman’s exposure during a critical small time period as compared with other studies of chronic diseases, where errors of a few months or even years may have minimal impact.
Uterine growth retardation, congenital anomaly and spontaneous abortions are frequently evaluated in occupational exposure studies. There is more than one approach available to assess each outcome. These end-points are of public health importance due to both the psychological and the financial costs. Generally, nonsecificity in the exposure-outcome relationships has been observed, e.g., with exposure to lead, anaesthetic gases and solvents. Because of the potential for nonsecificity in the exposure-effect relationship, studies should be designed to assess several end-points associated with a range of possible mechanisms.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."