- You are here:
-
Home

-
Part XVII. Services and Trade
-
Transport Industry and Warehousing
- Water Transport
Strain in Health Care Work
Cognitive Strain
Continuous observation has revealed that nurses’ workdays are characterized by continual reorganization of their work schedules and frequent interruptions.
Belgian (Malchaire 1992) and French (Gadbois et al. 1992; Estryn-Béhar and Fouillot 1990b) studies have revealed that nurses perform 120 to 323 separate tasks during their workday (see table 1). Work interruptions are very frequent throughout the day, ranging from 28 to 78 per workday. Many of the units studied were large, short-term-stay units in which the nurses’ work consisted of a long series of spatially dispersed, short-duration tasks. Planning of work schedules was complicated by the presence of incessant technical innovation, close interdependence of the work of the various staff members and a generally haphazard approach to work organization.
Table 1. Number of separate tasks undertaken by nurses, and interruptions during each shift
|
Belgium |
France |
France |
|
|
Authors |
Malchaire 1992* |
Gadbois et al. 1992** |
Estryn-Béhar and |
|
Departments |
Cardiovascular |
Surgery (S) and |
Ten medical and |
|
Number of separate |
Morning 120/8 h |
S (day) 276/12 h |
Morning 323/8 h |
|
Number of |
S (day) 36/12 h |
Morning 78/8 h |
Number of hours of observation: * Morning: 80 h; afternoon: 80 h; night: 110 h. ** Surgery: 238 h; medicine: 220 h. *** Morning : 64 h; afternoon: 80 h; night: 90 h.
Gadbois et al. (1992) observed an average of 40 interruptions per workday, of which 5% were caused by patients, 40% by inadequate transmission of information, 15% by telephone calls and 25% by equipment. Ollagnier and Lamarche (1993) systematically observed nurses in a Swiss hospital and observed 8 to 32 interruptions per day, depending on the ward. On average, these interruptions represented 7.8% of the workday.
Work interruptions such as these, caused by inappropriate information supply and transmission structures, prevent workers from completing all their tasks and lead to worker dissatisfaction. The most serious consequence of this organizational deficiency is the reduction of time spent with patients (see table 2). In the first three studies cited above, nurses spent at most 30% of their time with patients on average. In Czechoslovakia, where multiple-bed rooms were common, nurses needed to change rooms less frequently, and spent 47% of their shift time with patients (Hubacova, Borsky and Strelka 1992). This clearly demonstrates how architecture, staffing levels and mental strain are all interrelated.
Table 2. Distribution of nurses’ time in three studies
|
Czechoslovakia |
Belgium |
France |
|
|
Authors |
Hubacova, Borsky and Strelka 1992* |
Malchaire 1992** |
Estryn-Béhar and |
|
Departments |
5 medical and surgical departments |
Cardiovascular surgery |
10 medical and |
|
Average time for the main postures and total distance walked by nurses: |
|||
|
Per cent working |
76% |
Morning 61% |
Morning 74% |
|
Including stooping, |
11% |
Morning 16% |
|
|
Standing flexed |
Morning 11% |
||
|
Distance walked |
Morning 4 km |
Morning 7 km |
|
|
Per cent working |
Three shifts: 47% |
Morning 38% |
Morning 24% |
Number of observations per shift: * 74 observations on 3 shifts. ** Morning: 10 observations (8 h); afternoon: 10 observations (8 h); night: 10 observations (11 h). *** Morning: 8 observations (8 h); afternoon: 10 observations (8 h); night: 9 observations (10-12 h).
Estryn-Béhar et al. (1994) observed seven occupations and schedules in two specialized medical wards with similar spatial organization and located in the same high-rise building. While work in one ward was highly sectorized, with two teams of a nurse and a nurses’ aide attending half of the patients, there were no sectors in the other ward, and basic care for all patients was dispensed by two nurses’ aides. There were no differences in the frequency of patient-related interruptions in the two wards, but team-related interruptions were clearly more frequent in the ward without sectors (35 to 55 interruptions compared to 23 to 36 interruptions). Nurses’ aides, morning-shift nurses and afternoon-shift nurses in the non-sectorized ward suffered 50, 70 and 30% more interruptions than did their colleagues in the sectorized one.
Sectorization thus appears to reduce the number of interruptions and the fracturing of work shifts. These results were used to plan the reorganization of the ward, in collaboration with the medical and paramedical staff, so as to facilitate sectorization of the office and the preparation area. The new office space is modular and easily divided into three offices (one for physicians and one for each of the two nursing teams), each separated by sliding glass partitions and furnished with at least six seats. Installation of two counters facing each other in the common preparation area means that nurses who are interrupted during preparation can return and find their materials in the same position and state, unaffected by their colleagues’ activities.
Reorganization of work schedules and technical services
Professional activity in technical departments is much more than the mere sum of tasks associated with each test. A study conducted in several nuclear medicine departments (Favrot-Laurens 1992) revealed that nuclear medicine technicians spend very little of their time performing technical tasks. In fact, a significant part of technicians’ time was spent coordinating activity and workload at the various workstations, transmitting information and making unavoidable adjustments. These responsibilities stem from technicians’ obligation to be knowledgeable about each test and to possess essential technical and administrative information in addition to test-specific information such as time and injection site.
Information processing necessary for the delivery of care
Roquelaure, Pottier and Pottier (1992) were asked by a manufacturer of electroencephalography (EEG) equipment to simplify the use of the equipment. They responded by facilitating the reading of visual information on controls which were excessively complicated or simply unclear. As they point out, “third-generation” machines present unique difficulties, due in part to the use of visual display units packed with barely legible information. Deciphering these screens requires complex work strategies.
On the whole, however, little attention has been paid to the need to present information in a manner that facilitates rapid decision-making in health care departments. For example, the legibility of information on medicine labels still leaves much to be desired, according to one study of 240 dry oral and 364 injectable medications (Ott et al. 1991). Ideally, labels for dry oral medication administered by nurses, who are frequently interrupted and attend several patients, should have a matte surface, characters at least 2.5 mm high and comprehensive information on the medication in question. Only 36% of the 240 medications examined satisfied the first two criteria, and only 6% all three. Similarly, print smaller than 2.5 mm was used in 63% of labels on the 364 injectable medications.
In many countries where English is not spoken, machine control panels are still labelled in English. Patient-chart software is being developed in many countries. In France, this type of software development is often motivated by a desire to improve hospital management and undertaken without adequate study of the software’s compatibility with actual working procedures (Estryn-Béhar 1991). As a result, the software may actually increase the complexity of nursing, rather than reduce cognitive strain. Requiring nurses to page through multiple screens of information to obtain the information they need to fill a prescription may increase the number of errors they make and memory lapses they suffer.
While Scandinavian and North American countries have computerized much of their patient records, it must be borne in mind that hospitals in these countries benefit from a high staff-to-patient ratio, and work interruptions and constant reshuffling of priorities are therefore less problematic there. In contrast, patient-chart software designed for use in countries with lower staff-to-patient ratios must be able to easily produce summaries and facilitate reorganization of priorities.
Human error in anaesthesia
Cooper, Newbower and Kitz (1984), in their study of the factors underlying errors during anaesthesia in the United States, found equipment design to be crucial. The 538 errors studied, largely drug administration and equipment problems, were related to the distribution of activities and the systems involved. According to Cooper, better design of equipment and monitoring apparatus would lead to a 22% reduction in errors, while complementary training of anaesthesiologists, using new technologies such as anaesthesia simulators, would lead to a 25% reduction. Other recommended strategies focus on work organization, supervision and communications.
Acoustic alarms in operating theatres and intensive-care units
Several studies have shown that too many types of alarms are used in operating theatres and intensive-care units. In one study, anaesthetists identified only 33% of alarms correctly, and only two monitors had recognition rates exceeding 50% (Finley and Cohen 1991). In another study, anaesthetists and anaesthesia nurses correctly identified alarms in only 34% of cases (Loeb et al. 1990). Retrospective analysis showed that 26% of nurses’ errors were due to similarities in alarm sounds and 20% to similarities in alarm functions. Momtahan and Tansley (1989) reported that recovery-room nurses and anaesthetists correctly identified alarms in only 35% and 22% of cases respectively. In another study by Momtahan, Hétu and Tansley (1993), 18 physicians and technicians were able to identify only 10 to 15 of 26 operating-theatre alarms, while 15 intensive-care nurses were able to identify only 8 to 14 of 23 alarms used in their unit.
De Chambost (1994) studied the acoustic alarms of 22 types of machines used in an intensive-care unit in the Paris region. Only the cardiogram alarms and those of one of the two types of automated-plunger syringes were readily identified. The others were not immediately recognized and required personnel first to investigate the source of the alarm in the patient’s room and then return with the appropriate equipment. Spectral analysis of the sound emitted by eight machines revealed significant similarities and suggests the existence of a masking effect between alarms.
The unacceptably high number of unjustifiable alarms has been the object of particular criticism. O’Carroll (1986) characterized the origin and frequency of alarms in a general intensive-care unit over three weeks. Only eight of 1,455 alarms were related to a potentially fatal situation. There were many false alarms from monitors and perfusion pumps. There was little difference between the frequency of alarms during the day and night.
Similar results have been reported for alarms used in anaesthesiology. Kestin, Miller and Lockhart (1988), in a study of 50 patients and five commonly used anaesthesia monitors, reported that only 3% indicated a real risk for the patient and that 75% of alarms were unfounded (caused by patient movement, interference and mechanical problems). On average, ten alarms were triggered per patient, equivalent to one alarm every 4.5 minutes.
A common response to false alarms is simply to disable them. McIntyre (1985) reported that 57% of Canadian anaesthetists admitted deliberately inactivating an alarm. Obviously, this could lead to serious accidents.
These studies underscore the poor design of hospital alarms and the need for alarm standardization based on cognitive ergonomics. Both Kestin, Miller and Lockhart (1988) and Kerr (1985) have proposed alarm modifications that take into account risk and the expected corrective responses of hospital personnel. As de Keyser and Nyssen (1993) have shown, the prevention of human error in anaesthesia integrates different measures—technological, ergonomic, social, organizational and training.
Technology, human error, patient safety and perceived psychological strain
Rigorous analysis of the error process is very useful. Sundström-Frisk and Hellström (1995) reported that equipment deficiencies and/or human error were responsible for 57 deaths and 284 injuries in Sweden between 1977 and 1986. The authors interviewed 63 intensive-care-unit teams involved in 155 incidents (“near-accidents”) involving advanced medical equipment; most of these incidents had not been reported to authorities. Seventy typical “near-accident” scenarios were developed. Causal factors identified included inadequate technical equipment and documentation, the physical environment, procedures, staffing levels and stress. The introduction of new equipment may lead to accidents if the equipment is poorly adapted to users’ needs and is introduced in the absence of basic changes in training and work organization.
In order to cope with forgetfulness, nurses develop several strategies for remembering, anticipating and avoiding incidents. They do still occur and even when patients are unaware of errors, near-accidents cause personnel to feel guilty. The article "Case Study: Human Error and Critical Taks" deals with some aspects of the problem.
Emotional or Affective Strain
Nursing work, especially if it forces nurses to confront serious illness and death, can be a significant source of affective strain, and may lead to burn-out, which is discussed more fully elsewhere in this Encyclopaedia. Nurses’ ability to cope with this stress depends on the extent of their support network and their possibility to discuss and improve patients’ quality of life. The following section summarizes the principal findings of Leppanen and Olkinuora’s (1987) review of Finnish and Swedish studies on stress.
In Sweden, the main motivations reported by health professionals for entering their profession were the “moral calling” of the work, its usefulness and the opportunity to exercise competence. However, almost half of nurses’ aides rated their knowledge as inadequate for their work, and one-quarter of nurses, one-fifth of registered nurses, one-seventh of physicians and one-tenth of head nurses considered themselves incompetent at managing some types of patients. Incompetence in managing psychological problems was the most commonly cited problem and was particularly prevalent among nurses’ aides, although also cited by nurses and head nurses. Physicians, on the other hand, consider themselves competent in this area. The authors focus on the difficult situation of nurses’ aides, who spend more time with patients than the others but are, paradoxically, unable to inform patients about their illness or treatment.
Several studies reveal the lack of clarity in delineating responsibilities. Pöyhönen and Jokinen (1980) reported that only 20% of Helsinki nurses were always informed of their tasks and the goals of their work. In a study conducted in a paediatric ward and an institute for disabled persons, Leppanen showed that the distribution of tasks did not allow nurses enough time to plan and prepare their work, perform office work and collaborate with team members.
Responsibility in the absence of decision-making power appears to be a stress factor. Thus, 57% of operating-room nurses felt that ambiguities concerning their responsibilities aggravated their cognitive strain; 47% of surgical nurses reported being unfamiliar with some of their tasks and felt that patients’ and nurses’ conflicting expectations were a source of stress. Further, 47% reported increased stress when problems occurred and physicians were not present.
According to three European epidemiological studies, burn-out affects approximately 25% of nurses (Landau 1992; Saint-Arnaud et al. 1992; Estryn-Béhar et al. 1990) (see table 3 ). Estryn-Béhar et al. studied 1,505 female health care workers, using a cognitive strain index that integrates information on work interruptions and reorganization and an affective strain index that integrates information on work ambience, teamwork, congruity of qualification and work, time spent talking to patients and the frequency of hesitant or uncertain responses to patients. Burn-out was observed in 12% of nurses with low, 25% of those with moderate and 39% of those with high cognitive strain. The relationship between burn-out and affective strain increases was even stronger: burn-out was observed in 16% of nurses with low, 25% of those with moderate and 64% of those with high affective strain. After adjustment by logistic multivariate regression analysis for social and demographic factors, women with a high affective strain index had an odds ratio for burn-out of 6.88 compared to those with a low index.
Table 3. Cognitive and affective strain and burn-out among health workers
|
Germany* |
Canada** |
France*** |
|
|
Number of subjects |
24 |
868 |
1,505 |
|
Method |
Maslach Burn-out |
Ilfeld Psychiatric |
Goldberg General |
|
High emotional |
33% |
20% |
26% |
|
Degree of burn-out, |
Morning 2.0; |
Morning 25%; |
|
|
Percentage suffering |
Cognitive and |
Cognitive strain: |
* Landau 1992. ** Saint Arnand et. al. 1992. *** Estryn-Béhar et al. 1990.
Saint-Arnaud et al. reported a correlation between the frequency of burn-out and the score on their composite cognitive and affective strain index. Landau’s results support these findings.
Finally, 25% of 520 nurses working in a cancer treatment centre and a general hospital in France were reported to exhibit high burn-out scores (Rodary and Gauvain-Piquard 1993). High scores were most closely associated with a lack of support. Feelings that their department did not regard them highly, take their knowledge of the patients into account or put the highest value on their patients’ quality of life were reported more frequently by nurses with high scores. Reports of being physically afraid of their patients and unable to organize their work schedule as they wished were also more frequent among these nurses. In light of these results, it is interesting to note that Katz (1983) observed a high suicide rate among nurses.
Impact of workload, autonomy and support networks
A study of 900 Canadian nurses revealed an association between workload and five indices of cognitive strain measured by the Ilfeld questionnaire: the global score, aggression, anxiety, cognitive problems and depression (Boulard 1993). Four groups were identified. Nurses with a high workload, high autonomy and good social support (11.76%) exhibited several stress-related symptoms. Nurses with a low workload, high autonomy and good social support (35.75%) exhibited the lowest stress. Nurses with high workload, little autonomy and little social support (42.09%) had a high prevalence of stress-related symptoms, while nurses with a low workload, little autonomy and little social support (10.40%) had low stress, but the authors suggest that these nurses may experience some frustration.
These results also demonstrate that autonomy and support, rather than moderating the relationship between workload and mental health, act directly on workload.
Role of head nurses
Classically, employee satisfaction with supervision has been considered to depend on the clear definition of responsibilities and on good communication and feedback. Kivimäki and Lindström (1995) administered a questionnaire to nurses in 12 wards of four medical departments and interviewed the wards’ head nurses. Wards were classified into two groups on the basis of the reported level of satisfaction with supervision (six satisfied wards and six dissatisfied wards). Scores for communication, feedback, participation in decision-making and the presence of a work climate that favours innovation were higher in “satisfied” wards. With one exception, head nurses of “satisfied” wards reported conducting at least one confidential conversation lasting one to two hours with each employee annually. In contrast, only one of the head nurses of the “dissatisfied” wards reported this behaviour.
Head nurses of the “satisfied” wards reported encouraging team members to express their opinions and ideas, discouraging team members from censuring or ridiculing nurses who made suggestions, and consistently attempting to give positive feedback to nurses expressing different or new opinions. Finally, all the head nurses in “satisfied” wards, but none of the ones in “dissatisfied” ones, emphasized their own role in creating a climate favourable to constructive criticism.
Psychological roles, relationships and organization
The structure of nurses’ affective relationships varies from team to team. A study of 1,387 nurses working regular night shifts and 1,252 nurses working regular morning or afternoon shifts revealed that shifts were extended more frequently during night shifts (Estryn-Béhar et al. 1989a). Early shift starts and late shift ends were more prevalent among night-shift nurses. Reports of a “good” or “very good” work ambience were more prevalent at night, but a “good relationship with physicians” was less prevalent. Finally, night-shift nurses reported having more time to talk to patients, although that meant that worries and uncertainties about the appropriate response to give patients, also more frequent at night, were harder to bear.
Büssing (1993) revealed that depersonalization was greater for nurses working abnormal hours.
Stress in physicians
Denial and suppression of stress are common defence mechanisms. Physicians may attempt to repress their problems by working harder, distancing themselves from their emotions or adopting the role of a martyr (Rhoads 1977; Gardner and Hall 1981; Vaillant, Sorbowale and McArthur 1972). As these barriers become more fragile and adaptive strategies break down, bouts of anguish and frustration become more and more frequent.
Valko and Clayton (1975) found that one-third of interns suffered severe and frequent episodes of emotional distress or depression, and that one-quarter of them entertained suicidal thoughts. McCue (1982) believed that a better understanding of both stress and reactions to stress would facilitate physician training and personal development and modify societal expectations. The net effect of these changes would be an improvement in care.
Avoidance behaviours may develop, often accompanied by a deterioration of interpersonal and professional relationships. At some point, the physician finally crosses the line into a frank deterioration of mental health, with symptoms which may include substance abuse, mental illness or suicide. In yet other cases, patient care may be compromised, resulting in inappropriate examinations and treatment, sexual abuse or pathological behaviour (Shapiro, Pinsker and Shale 1975).
A study of 530 physician suicides identified by the American Medical Association over a five-year period found that 40% of suicides by female physicians and less than 20% of suicides by male physicians occurred in individuals younger than 40 years (Steppacher and Mausner 1974). A Swedish study of suicide rates from 1976 to 1979 found the highest rates among some of the health professions, compared to the overall active population (Toomingas 1993). The standardized mortality ratio (SMR) for female physicians was 3.41, the highest value observed, while that for nurses was 2.13.
Unfortunately, health professionals with impaired mental health are often ignored and may even be rejected by their colleagues, who attempt to deny these tendencies in themselves (Bissel and Jones 1975). In fact, slight or moderate stress is much more prevalent among health professionals than are frank psychiatric disorders (McCue 1982). A good prognosis in these cases depends on early diagnosis and peer support (Bitker 1976).
Discussion groups
Studies on the effect of discussion groups on burn-out have been undertaken in the United States. Although positive results have been demonstrated (Jacobson and MacGrath 1983), it should be noted that these have been in institutions where there was sufficient time for regular discussions in quiet and appropriate settings (i.e., hospitals with high staff-patient ratios).
A literature review of the success of discussion groups has shown these groups to be valuable tools in wards where a high proportion of patients are left with permanent sequelae and must learn to accept modifications in their lifestyle (Estryn-Béhar 1990).
Kempe, Sauter and Lindner (1992) evaluated the merits of two support techniques for nurses near burn-out in geriatrics wards: a six-month course of 13 professional counselling sessions and a 12-month course of 35 “Balint group” sessions. The clarification and reassurance provided by the Balint group sessions were effective only if there was also significant institutional change. In the absence of such change, conflicts may even intensify and dissatisfaction increase. Despite their impending burn-out, these nurses remained very professional and sought ways of carrying on with their work. These compensatory strategies had to take into account extremely high workloads: 30% of nurses worked more than 20 hours of overtime per month, 42% had to cope with understaffing during more than two-thirds of their working hours and 83% were often left alone with unqualified personnel.
The experience of these geriatrics nurses was compared to that of nurses in oncology wards. Burnout score was high in young oncology nurses, and decreased with seniority. In contrast, burnout score among geriatrics nurses increased with seniority, attaining levels much higher than those observed in oncology nurses. This lack of decrease with seniority is due to the characteristics of the workload in geriatrics wards.
The need to act on multiple determinants
Some authors have extended their study of effective stress management to organizational factors related to affective strain.
For example, analysis of psychological and sociological factors was part of Theorell’s attempt to implement case-specific improvements in emergency, paediatric and juvenile psychiatry wards (Theorell 1993). Affective strain before and after the implementation of changes was measured through the use of questionnaires and the measurement of plasma prolactin levels, shown to mirror feelings of powerlessness in crisis situations.
Emergency-ward personnel experienced high levels of affective strain and frequently enjoyed little decisional latitude. This was attributed to their frequent confrontation with life-and-death situations, the intense concentration demanded by their work, the high number of patients they frequently attended and the impossibility of controlling the type and number of patients. On the other hand, because their contact with patients was usually short and superficial, they were exposed to less suffering.
The situation was more amenable to control in paediatric and juvenile psychiatry wards, where schedules for diagnostic procedures and therapeutic procedures were established in advance. This was reflected by a lower risk of overwork compared to emergency wards. However, personnel in these wards were confronted with children suffering from serious physical and mental disease.
Desirable organizational changes were identified through discussion groups in each ward. In emergency wards, personnel were very interested in organizational changes and recommendations concerning training and routine procedures—such as how to treat rape victims and elderly patients with no relations, how to evaluate work and what to do if a called physician doesn’t arrive—were formulated. This was followed by the implementation of concrete changes, including the creation of the position of head physician and the ensuring of the constant availability of an internist.
The personnel in juvenile psychiatry were primarily interested in personal growth. Reorganization of resources by the head physician and the county allowed one-third of the personnel to undergo psychotherapy.
In paediatrics, meetings were organized for all the personnel every 15 days. After six months, social support networks, decisional latitude and work content all had improved.
The factors identified by these detailed ergonomic, psychological and epidemiological studies are valuable indices of work organization. Studies which focus on them are quite different from in-depth studies of multi-factor interactions and instead revolve around the pragmatic characterization of specific factors.
Tintori and Estryn-Béhar (1994) identified some of these factors in 57 wards of a large hospital in the Paris region in 1993. Shift overlap of more than 10 minutes was present in 46 wards, although there was no official overlap between the night and morning shifts in 41 wards. In half the cases, these information communication sessions included nurses’ aides in all three shifts. In 12 wards, physicians participated in the morning-afternoon sessions. In the three months preceding the study, only 35 wards had held meetings to discuss patients’ prognoses, discharges and patients’ understanding of and reaction to their illnesses. In the year preceding the study, day-shift workers in 18 wards had received no training and only 16 wards had dispensed training to their night-shift workers.
Some new lounges were not used, since they were 50 to 85 metres from some of the patients’ rooms. Instead, the personnel preferred holding their informal discussions around a cup of coffee in a smaller but closer room. Physicians participated in coffee breaks in 45 day-shift wards. Nurses’ complaints of frequent work interruptions and feelings of being overwhelmed by their work are no doubt attributable in part to the dearth of seats (less than four in 42 of the 57 wards) and cramped quarters of the nursing stations, where more than nine people must spend a good part of their day.
The interaction of stress, work organization and support networks is clear in studies of the home-care unit of the hospital in Motala, Sweden (Beck-Friis, Strang and Sjöden 1991; Hasselhorn and Seidler 1993). The risk of burn-out, generally considered high in palliative care units, was not significant in these studies, which in fact revealed more occupational satisfaction than occupational stress. Turnover and work stoppages in these units were low, and personnel had a positive self-image. This was attributed to selection criteria for personnel, good teamwork, positive feedback and continuing education. Personnel and equipment costs for terminal-stage cancer hospital care are typically 167 to 350% higher than for hospital-based home care. There were more than 20 units of this type in Sweden in 1993.
Hospital Ergonomics: A Review
Author: Madeleine R. Estryn-Béhar
Ergonomics is an applied science that deals with the adaptation of work and the workplace to the characteristics and capabilities of the worker so that he or she may perform the duties of the job effectively and safely. It addresses the worker’s physical capacities in relation to the physical requirements of the job (e.g., strength, endurance, dexterity, flexibility, ability to tolerate positions and postures, visual and auditory acuity) as well as his or her mental and emotional status in relation to the way the work is organized (e.g., work schedules, workload and work-related stress). Ideally, adaptations are made to the furniture, equipment and tools used by the worker and to the work environment to enable the worker to perform adequately without risk to himself/herself, co-workers and the public. Occasionally, it is necessary to improve the worker’s adaptation to the job through, for example, special training and the use of personal protective equipment.
Since the mid 1970s, the application of ergonomics to hospital workers has broadened. It is directed now at those involved in direct patient care (e.g., physicians and nurses), those involved in ancillary services (e.g., technicians, laboratory staff, pharmacists and social workers) and those providing support services (e.g., administrative and clerical personnel, food service staff, housekeeping staff, maintenance workers and security staff).
Extensive research has been conducted into the ergonomics of hospitalization, with most studies attempting to identify the extent to which hospital administrators should allow hospital personnel latitude in developing strategies to reconcile an acceptable workload with good quality of care. Participatory ergonomics has become increasingly widespread in hospitals in recent years. More specifically, wards have been reorganized on the basis of ergonomic analyses of activity undertaken in collaboration with medical and paramedical personnel, and participatory ergonomics has been used as the basis for the adaptation of equipment for use in health care.
In studies of hospital ergonomics, workstation analysis must extend at least to the departmental level—the distance between rooms and the amount and location of equipment are all crucial considerations.
Physical strain is one of the primary determinants of the health of HCWs and the quality of care that they dispense. This being said, the frequent interruptions that hinder care-giving and the effect of psychological factors associated with confrontations with serious illness, ageing and death must also be addressed. Accounting for all these factors is a difficult task, but approaches focusing only on single factors will fail to improve either working conditions or the quality of care. Similarly, patients’ perception of the quality of their hospital stay is determined by the effectiveness of the care they receive, their relationship with physicians and other personnel, the food and the architectural environment.
Basic to hospital ergonomics is study of the sum and interaction of personal factors (e.g., fatigue, fitness, age and training) and circumstantial factors (e.g., work organization, schedule, floor layout, furniture, equipment, communication and psychological support within the work team), which combine to affect the performance of work. Precise identification of the actual work performed by health care workers depends on ergonomic observation of entire workdays and collection of valid and objective information on the movements, postures, cognitive performance and emotional control called upon to satisfy work requirements. This helps to detect factors that may interfere with effective, safe, comfortable and healthy work. This approach also sheds light on the potential for workers’ suffering or taking pleasure in their work. Final recommendations must take the interdependence of the various professional and ancillary personnel attending the same patient into account.
These considerations lay the groundwork for further, specific research. Analysis of strain related to the use of basic equipment (e.g., beds, meal carts and mobile x-ray equipment) may help clarify the conditions of acceptable use. Measurements of lighting levels may be complemented by information on the size and contrast of medication labels, for example. Where alarms emitted by different intensive-care-unit equipment can be confused, analysis of their acoustic spectrum may prove useful. Computerization of patient charts should not be undertaken unless the formal and informal information-support structures have been analysed. The interdependence of the various elements of the work environment of any given caregiver should therefore always be borne in mind when analysing isolated factors.
Analysis of the interaction of different factors influencing care—physical strain, cognitive strain, affective strain, scheduling, ambience, architecture and hygiene protocols—is essential. It is important to adapt schedules and common work areas to the needs of the work team when attempting to improve overall patient management. Participatory ergonomics is a way of using specific information to bring about wide-ranging and relevant improvements to the quality of care and to working life. Involving all categories of personnel in key stages of the search for solution helps ensure that the modifications finally adopted will have their full support.
Working Postures
Epidemiological studies of joint and musculoskeletal disorders. Several epidemiological studies have indicated that inappropriate postures and handling techniques are associated with a doubling of the number of back, joint and muscle problems requiring treatment and time off the job. This phenomenon, discussed in greater detail elsewhere in this chapter and Encyclopaedia, is related to physical and cognitive strain.
Working conditions differ from country to country. Siegel et al. (1993) compared conditions in Germany and Norway and found that 51% of German nurses, but only 24% of Norwegian nurses, suffered lower-back pain on any given day. Working conditions in the two countries differed; however, in German hospitals, the patient-nurse ratio was twice as high and the number of adjustable-height beds half that in Norwegian hospitals, and fewer nurses had patient handling equipment (78% versus 87% in Norwegian hospitals).
Epidemiological studies of pregnancy and its outcome. Because the hospital workforce is usually predominantly female, the influence of work on pregnancy often becomes an important issue (see articles on pregnancy and work elsewhere in this Encyclopaedia). Saurel-Cubizolles et al. (1985) in France, for example, studied 621 women who returned to hospital work after giving birth and found that a higher rate of premature births were associated with heavy housekeeping chores (e.g., cleaning windows and floors), carrying heavy loads and long periods of standing. When these tasks were combined, the rate of premature births was increased: 6% when only one of these factors was involved and up to 21% when two or three were involved. These differences remained significant after adjustment for seniority, social and demographic characteristics and professional level. These factors were also associated with a higher frequency of contractions, more hospital admissions during pregnancy and, on average, longer sick leave.
In Sri Lanka, Senevirane and Fernando (1994) compared 130 pregnancies borne by 100 nursing officers and 126 by clerical workers whose jobs presumably were more sedentary; socio-economic backgrounds and use of prenatal care were similar for both groups. Odds-ratios for complications of pregnancy (2.18) and preterm delivery (5.64) were high among nursing officers.
Ergonomic Observation of Workdays
The effect of physical strain on health care workers has been demonstrated through continuous observation of workdays. Research in Belgium (Malchaire 1992), France (Estryn-Béhar and Fouillot 1990a) and Czechoslovakia (Hubacova, Borsky and Strelka 1992) has shown that health care workers spend 60 to 80% of their workday standing (see table 1). Belgian nurses were observed to spend approximately 10% of their workday bent over; Czechoslovakian nurses spent 11% of their workday positioning patients; and French nurses spent 16 to 24% of their workday in uncomfortable positions, such as stooping or squatting, or with their arms raised or loaded.
Table 1. Distribution of nurses’ time in three studies
|
Czechoslovakia |
Belgium |
France |
|
|
Authors |
Hubacova, Borsky and Strelka 1992* |
Malchaire 1992** |
Estryn-Béhar and |
|
Departments |
5 medical and surgical departments |
Cardiovascular surgery |
10 medical and |
|
Average time for the main postures and total distance walked by nurses: |
|||
|
Per cent working |
76% |
Morning 61% |
Morning 74% |
|
Including stooping, |
11% |
Morning 16% |
|
|
Standing flexed |
Morning 11% |
||
|
Distance walked |
Morning 4 km |
Morning 7 km |
|
|
Per cent working |
Three shifts: 47% |
Morning 38% |
Morning 24% |
Number of observations per shift:* 74 observations on 3 shifts. ** Morning: 10 observations (8 h); afternoon: 10 observations (8 h); night: 10 observations (11 h). *** Morning: 8 observations (8 h); afternoon: 10 observations (8 h); night: 9 observations (10-12 h).
In France, night-shift nurses spent somewhat more time sitting, but they end their shift by making beds and dispensing care, both of which involve work in uncomfortable positions. They are assisted in this by a nurses’ aide, but this should be contrasted with the situation during the morning shift, where these tasks are usually performed by two nurses’ aides. In general, nurses working day shifts spend less time in uncomfortable positions. Nurses’ aides were on their feet constantly, and uncomfortable positions, due largely to inadequate equipment, accounted for 31% (afternoon shift) to 46% (morning shift) of their time. Patient facilities in these French and Belgian teaching hospitals were spread out over large areas and consisted of rooms containing one to three beds. Nurses in these wards walked an average of 4 to 7 km per day.
Detailed ergonomic observation of entire workdays (Estryn-Béhar and Hakim-Serfaty 1990) is useful in revealing the interaction of the factors that determine quality of care and the manner in which work is performed. Consider the very different situations in a paediatric intensive care unit and a rheumatology ward. In paediatric resuscitation units, the nurse spends 71% of her time in patients’ rooms, and each patient’s equipment is kept on individual carts stocked by nurses’ aides. The nurses in this ward change location only 32 times per shift, walking a total of 2.5 km. They are able to communicate with physicians and other nurses in the adjoining lounge or nurses’ station through intercoms which have been installed in all the patients’ rooms.
By contrast, the nursing station in the rheumatology ward is very far from patients’ rooms, and care preparation is lengthy (38% of shift time). As a result, the nurses spend only 21% of their time in patients’ rooms and change location 128 times per shift, walking a total of 17 km. This clearly illustrates the interrelationship between physical strain, back problems and organizational and psychological factors. Because they need to move rapidly and get equipment and information, nurses only have time for hallway consultations—there is no time to sit while dispensing care, listen to patients and give patients personalized and integrated responses.
Continuous observation of 18 Dutch nurses in long-term-stay wards revealed that they spent 60% of their time performing physically demanding work with no direct contact with their patients (Engels, Senden and Hertog 1993). Housekeeping and preparation account for most of the 20% of the time described as spent in “slightly hazardous” activities. In all, 0.2% of shift time was spent in postures requiring immediate modification and 1.5% of shift time in postures requiring rapid modification. Contact with patients was the type of activity most frequently associated with these hazardous postures. The authors recommend modifying patient-handling practices and other less hazardous but more frequent tasks.
Given the physiological strain of the work of nurses’ aides, continuous measurement of heart rate is a useful complement to observation. Raffray (1994) used this technique to identify arduous housekeeping tasks and recommended not restricting personnel to this type of task for the whole day.
Electro-myographical (EMG) fatigue analysis is also interesting when body posture must remain more or less static—for example, during operations using an endoscope (Luttman et al. 1996).
Influence of architecture, equipment and organization
The inadequacy of nursing equipment, particularly beds, in 40 Japanese hospitals was demonstrated by Shindo (1992). In addition, patients’ rooms, both those lodging six to eight patients and single rooms reserved for the very ill, were poorly laid out and extremely small. Matsuda (1992) reported that these observations should lead to improvements in the comfort, safety and efficiency of nursing work.
In a French study (Saurel 1993), the size of patient rooms was problematic in 45 of 75 medium- and long-term-stay wards. The most common problems were:
- lack of space (30 wards)
- difficulty in manoeuvring patient-transfer gurneys (17)
- inadequate space for furniture (13)
- the need to take beds out of the room to transfer patients (12)
- difficult access and poor furniture layout (10)
- doors that were too small (8)
- difficulty moving between beds (8).
The mean available area per bed for patients and nurses is at the root of these problems and decreases as the number of beds per room increases: 12.98 m2, 9.84 m2, 9.60 m2, 8.49 m2 and 7.25 m2 for rooms with one, two, three, four and more than four beds. A more accurate index of the useful area available to personnel is obtained by subtracting the area occupied by the beds themselves (1.8 to 2.0 m2) and by other equipment. The French Department of Health prescribes a useful surface area of 16 m2 for single rooms and 22 m2 for double rooms. The Quebec Department of Health recommends 17.8 m2 and 36 m2, respectively.
Turning to factors favouring the development of back problems, variable-height mechanisms were present on 55.1% of the 7,237 beds examined; of these, only 10.3% had electric controls. Patient-transfer systems, which reduce lifting, were rare. These systems were systematically used by 18.2% of the 55 responding wards, with over half the wards reporting using them “rarely” or “never”. “Poor” or “rather poor” manoeuvrability of meal carts was reported by 58.5% of 65 responding wards. There was no periodic maintenance of mobile equipment in 73.3% of 72 responding wards.
In almost half the responding wards, there were no rooms with seats that nurses could use. In many cases, this appears to have been due to the small size of the patient rooms. Sitting was usually possible only in the lounges—in 10 units, the nursing station itself had no seats. However, 13 units reported having no lounge and 4 units used the pantry for this purpose. In 30 wards, there were no seats in this room.
According to statistics for 1992 provided by the Confederation of Employees of the Health Services Employees of the United Kingdom (COHSE), 68.2% of nurses felt that there were not enough mechanical patient lifts and handling aides and 74.5% felt that they were expected to accept back problems as a normal part of their work.
In Quebec, the Joint Sectoral Association, Social Affairs Sector (Association pour la santé et la sécurité du travail, secteur afffaires sociales, ASSTAS) initiated its “Prevention-Planning-Renovation-Construction” project in 1993 (Villeneuve 1994). Over 18 months, funding for almost 100 bipartite projects, some costing several million dollars, was requested. This programme’s goal is to maximize investments in prevention by addressing health and safety concerns early in the design stage of planning, renovation and design projects.
The association completed the modification of the design specifications for patient rooms in long-term-care units in 1995. After noting that three-quarters of occupational accidents involving nurses occur in patient rooms, the association proposed new dimensions for patients’ rooms, and new rooms must now provide a minimum amount of free space around beds and accommodate patient lifts. Measuring 4.05 by 4.95 m, the rooms are more square than the older, rectangular rooms. To improve performance, ceiling-mounted patient lifts were installed, in collaboration with the manufacturer.
The association is also working on the modification of construction standards for washrooms, where many occupational accidents also occur, although to a lesser extent than in the rooms themselves. Finally, the feasibility of applying anti-skid coatings (with a coefficient of friction above the minimum standard of 0.50) on floors is being studied, since patient autonomy is best promoted by providing a non-skid surface on which neither they nor nurses can slip.
Evaluation of equipment that reduces physical strain
Proposals for improving beds (Teyssier-Cotte, Rocher and Mereau 1987) and meal carts (Bouhnik et al. 1989) have been formulated, but their impact is too limited. Tintori et al. (1994) studied adjustable-height beds with electric trunk-lifts and mechanical mattress-lifts. The trunk-lifts were judged satisfactory by the staff and patients, but the mattress-lifts were very unsatisfactory, since adjusting the beds required more than eight pedal strokes, each of which exceeded standards for foot force. Pushing a button located close to the patient’s head while talking to her or him is clearly preferable to pumping a pedal eight times from the foot of the bed (see figure 1). Because of time constraints, the mattress lift was often simply not used.
Figure 1. Electronically-operated trunk-lifts on beds effectively reduce lifting accidents

B. Floret
Van der Star and Voogd (1992) studied health care workers caring for 30 patients in a new prototype of bed over a period of six weeks. Observations of the workers’ positions, the height of work surfaces, physical interaction between nurses and patients and the size of the work space were compared to data collected on the same ward over a seven-week period prior to the introduction of the prototype. Use of the prototypes reduced the total time spent in uncomfortable positions while washing patients from 40% to 20%; for bed-making the figures were 35% and 5%. Patients also enjoyed greater autonomy and often changed positions on their own, raising their trunks or legs by means of electric control buttons.
In Swedish hospitals, each double room is equipped with ceiling-mounted patient lifts (Ljungberg, Kilbom and Goran 1989). Rigorous programmes such as the April Project evaluate the interrelation of working conditions, work organization, the establishment of a back school and the improvement of physical fitness (Öhling and Estlund 1995).
In Quebec, ASSTAS developed a global approach to the analysis of working conditions causing back problems in hospitals (Villeneuve 1992). Between 1988 and 1991, this approach led to modifications of the work environment and equipment used in 120 wards and a 30% reduction in the frequency and severity of occupational injuries. In 1994, a cost-benefit analysis performed by the association demonstrated that the systematic implementation of ceiling-mounted patient lifts would reduce occupational accidents and increase productivity, compared to the continued use of mobile, ground-based lifts (see figure 2).
Figure 2. Using ceiling-mounted patient lifts to reduce lifting accidents

Accounting for individual variation and facilitating activity
The female population in France is generally not very physically active. Of 1,505 nurses studied by Estryn-Béhar et al. (1992), 68% participated in no athletic activity, with inactivity more pronounced among mothers and unskilled personnel. In Sweden, fitness programmes for hospital personnel have been reported to be useful (Wigaeus Hjelm, Hagberg and Hellstrom 1993), but are feasible only if potential participants do not end their work day too tired to participate.
The adoption of better work postures is also conditioned by the possibility of wearing appropriate clothing (Lempereur 1992). The quality of shoes is particularly important. Hard soles are to be avoided. Anti-skid soles prevent occupational accidents caused by slips and falls, which in many countries are the second-leading cause of accidents leading to work absence. Ill-fitting overshoes or boots worn by operating room personnel to minimize the build-up of static electricity may be a hazard for falls.
Slips on level floors can be prevented by using low-slip floor surfaces that require no waxing. The risk of slips, particularly at doorways, can also be reduced by using techniques that do not leave the floor wet for long. The use of one mop per room, recommended by hygiene departments, is one such technique and has the additional advantage of reducing the handling of buckets of water.
In Vasteras County (Sweden), the implementation of several practical measures reduced painful syndromes and absenteeism by at least 25% (Modig 1992). In the archives (e.g., record or file rooms), ground- and ceiling-level shelves were eliminated, and an adjustable sliding board on which personnel can take notes while consulting the archives was installed. A reception office equipped with movable filing units, a computer and a telephone was also constructed. The height of the filing units is adjustable, allowing employees to adjust them to their own needs and facilitating the transition from sitting to standing during work.
Importance of “anti-lifting”
Manual patient-handling techniques designed to prevent back injuries have been proposed in many countries. Given the poor results of these techniques that have been reported to date (Dehlin et al. 1981; Stubbs, Buckle and Hudson 1983), more work in this area is needed.
The department of kinesiology of the University of Groningen (Netherlands) has developed an integrated patient-handling programme (Landewe and Schröer 1993) consisting of:
- recognition of the relationship between patient-handling and back strain
- demonstration of the value of the “anti-lifting” approach
- sensitization of nursing students throughout their studies to the importance of avoiding back strain
- the use of problem-resolution techniques
- attention to implementation and evaluation.
In the “anti-lifting” approach, the resolution of problems associated with patient transfers is based on the systematic analysis of all aspects of transfers, especially those related to patients, nurses, transfer equipment, teamwork, general working conditions and environmental and psychological barriers to the use of patient lifts (Friele and Knibbe 1993).
The application of European standard EN 90/269 of 29 May 1990 on back problems is an example of an excellent starting point for this approach. Besides requiring employers to implement appropriate work organization structures or other appropriate means, particularly mechanical equipment, to avoid manual handling of loads by workers, it also emphasizes the importance of “no-risk” handling policies that incorporate training. In practice, the adoption of appropriate postures and handling practices depends on the amount of functional space, presence of appropriate furniture and equipment, good collaboration on work organization and quality of care, good physical fitness and comfortable work clothing. The net effect of these factors is improved prevention of back problems.
Occupational Health and Safety Practice: The Russian Experience
The work of people in the medical profession has great social value, and in recent years the urgent problem of the labour conditions and the state of health of HCWs has been studied actively. However, the nature of this work is such that any preventive and ameliorating measures cannot eliminate or reduce the main source of the hazards in the work of physicians and other HCWs: contact with a sick patient. In this respect the problem of prevention of occupational illness in medical workers is rather complicated.
In many cases the diagnostic and medical equipment and the methods of treatment used in medical institutions can affect the health of HCWs. Therefore, it is necessary to follow hygienic standards and precautionary measures to control the levels of exposure to unfavourable factors. Studies carried out in a number of Russian medical institutions have revealed that the labour conditions at many workplaces were not optimum and could induce the deterioration of the health of medical and support personnel, and sometimes cause the development of occupational diseases.
Among the physical factors that can substantially affect the health of medical personnel in the Russian Federation, ionizing radiation should be ranked as one of the first. Tens of thousands of Russian medical workers encounter sources of ionizing radiation at work. In the past, special laws were adopted to limit the doses and levels of irradiation at which specialists could work for a long period without health risk. In recent years x-ray control procedures were extended to cover not only radiologists, but surgeons, anaesthetists, traumatologists, rehabilitation specialists and mid-level personnel. The levels of radiation at worksites and the x-ray doses received by these individuals sometimes are even higher than the doses received by the radiologists and radiology laboratory assistants.
Instruments and equipment generating non-ionizing radiation and ultrasound are also widespread in modern medicine. Since many physiotherapy procedures are used precisely because of the therapeutic benefits of such treatment, the same biological effects may be hazardous to those involved in administering them. Persons encountering instruments and machines generating non-ionizing radiation are often reported to have functional disturbances in the nervous and cardiovascular systems.
Studies of working conditions where ultrasound is used for diagnostic or therapeutic procedures revealed that the personnel were exposed during as much as 85 to 95% of their working day to levels of high frequency, low intensity ultrasound comparable to the exposures experienced by operators of industrial ultrasonic defectoscopy. They experienced such impairments of the peripheral neuro-vascular system as angiodistonic syndrome, vegetative polyneuritis, vegetative vascular malfunction and so on.
Noise is rarely reported as a substantial factor of occupational risk in the work of Russian medical personnel, except at dental institutions. When using high-speed drills (200,000 to 400,000 rev/min) the maximum energy of the sound falls at a frequency of 800 Hz. The noise levels at a distance of 30 cm from the drill placed in the mouth of the patient vary from 80 to 90 dBA. One-third of the whole sound spectrum falls within the range most harmful to the ear (i.e., between 1000 and 2000 Hz).
Many noise sources gathered in one place can generate levels exceeding permissible limits. To create optimum conditions it is recommended that anaesthetizing machines, respiratory equipment and artificial blood circulation pumps be taken out of operating rooms.
In surgery departments, especially in operating rooms and in rehabilitation and intensive care departments, as well as in some other special rooms, it is necessary to maintain the required parameters of temperature, humidity and air circulation. The optimal layout of modern medical institutions and the installation of ventilation and air-conditioning plants provide the favourable microclimate.
However, in operating suites built without optimal planning, occlusive clothing (i.e., gowns, masks, caps and gloves) and exposure to heat from lighting and other equipment lead many surgeons and other members of the operating teams to complain of “overheating”. Perspiration is mopped from surgeons’ brows lest it interfere with their vision or contaminate the tissues in the surgical field.
As a result of the introduction into medical practice of treatment in hyperbaric chambers, physicians and nurses now are often exposed to heightened atmospheric pressure. In most cases this affects surgical teams performing operations in such chambers. Exposure to conditions of increased atmospheric pressure is believed to lead to unfavourable changes in a number of body functions, depending on the level of the pressure and the duration of the exposure.
Working posture is also of great importance for physicians. Although most tasks are performed in sitting or standing positions, some activities require long periods in awkward and uncomfortable positions. This is particularly the case with dentists, otologists, surgeons (especially microsurgeons), obstetricians, gynaecologists and physiotherapists. Work requiring long periods of standing in one position has been associated with the development of varicose veins in the legs and haemorrhoids.
Continual, intermittent or casual exposure to potentially hazardous chemicals used in medical institutions also can affect medical personnel. Among these chemicals, inhalation anaesthetics are considered to have the most unfavourable influence on humans. These gases can accumulate in large amounts not only in operating and delivery rooms but also in pre-op areas where anaesthesia is induced and in recovery rooms where they are exhaled by patients coming out of anaesthesia. Their concentration depends on the content of the gas mixtures being administered, the type of equipment being used and the duration of the procedure. Concentrations of anaesthetic gases in the breathing zones of surgeons and anaesthetists in the operating room have been found ranging from 2 to 14 times the maximum allowable concentration (MAC). Exposure to anaesthetic gases has been associated with impaired reproductive capacity of both male and female anaesthetists and abnormalities in the foetuses of pregnant female anaesthetists and the spouses of male anaesthetists (see chapter Reproductive system and the article “Waste anaesthetic gases" in this chapter).
In the treatment rooms where many injections are performed, the concentration of a medicine in the respiration zone of nurses can exceed permissible levels. Airborne drug exposure can happen when washing and sterilizing syringes, removing air bubbles from a syringe, and while dispensing aerosol therapy.
Among chemicals which could affect the health of medical personnel are hexachlorophene (possibly causing teratogenic effects), formalin (an irritant, sensitizer and carcinogen), ethylene oxide (which has toxic, mutagenic and carcinogenic characteristics), antibiotics that cause allergies and suppressed immune response, vitamins and hormones. There is also the possibility of exposure to industrial chemicals used in cleaning and maintenance work and as insecticides.
Many of the drugs used in the treatment of cancer are themselves mutagenic and carcinogenic. Special training programmes have been developed to prevent workers involved in preparing and administering them from exposure to such cytotoxic agents.
One of the features of job assignments of medical workers of many specialties is contact with infected patients. Any infectious disease incurred as a result of such contact is considered to be an occupational one. Viral serum hepatitis has proved to be the most dangerous for the staff of medical institutions. Viral hepatitis infections of laboratory assistants (from examining blood samples), staff members of haemodialysis departments, pathologists, surgeons, anaesthetists and other specialists who had occupational contact with the blood of infected patients have been reported (see the article “Prevention of occupational transmission of bloodborne pathogens” in this chapter).
There has apparently been no recent improvement in the health status of HCWs in the Russian Federation. The proportion of cases of work-related, temporary disability remained at the level of 80 to 96 per 100 working doctors and 65 to 75 per 100 mid-level medical workers. Although this measure of work loss is quite high, it should also be noted that self-treatment and informal, unreported treatment are widespread among HCWs, which means that many cases are not captured by the official statistics. This was confirmed by a survey among physicians which found that 40% of the respondents were ill four times a year or more but did not apply to a practising physician for medical care and did not submit a disability form. These data were corroborated by medical examinations which found evidence of disability in 127.35 cases per 100 workers examined.
Morbidity also increases with age. In these examinations, it was six times more frequent among HCWs with 25 years of service than among those with less than 5 years of service. The most common diseases included circulatory impairments (27.9%), diseases of the digestive organs (20.0%) and musculoskeletal disorders (20.72%). Except for the last, most of the cases were non-occupational in origin.
Sixty per cent of doctors and 46% of mid-level personnel were found to have chronic diseases. Many of these were directly associated with job assignments.
Many of the observed diseases were directly associated with job assignments of those examined. Thus, microsurgeons working in an awkward posture were found to have frequent osteochondroses; chemotherapists were found to suffer frequently from chromosome abnormalities and anaemia; nurses who were in contact with a large variety of medicines suffered various allergic diseases, ranging from dermatoses to bronchial asthma and immunodeficiency.
In Russia, health problems of medical workers were first addressed in the 1920s. In 1923 a special scientific-consultative bureau was founded in Moscow; the results of its studies were published in five collections entitled Labour and Life of Medical Workers of Moscow and Moscow Province. Since that time other studies have appeared devoted to this problem. But this work has been carried on in the most fruitful way only since 1975, when the Laboratory of Labour Hygiene of Medical Workers was established in the RAMS Institute of Occupational Health, which coordinated all the studies of this problem. After analysis of the then-current situation, research was directed at:
- studies of the features of labour processes in the main medical specialties
- assessment of the factors of the occupational environment
- analysis of the morbidity of medical workers
- elaboration of measures for optimization of labour conditions, reduction of fatigue and prevention of morbidity.
Based on the studies carried out by the Laboratory and other institutions, a number of recommendations and suggestions were prepared, aimed at reduction and prevention of the occupational diseases of medical workers.
Instructions were established for pre-employment and periodic medical examinations of health care workers. The aim of these examinations was to determine the fitness of the worker for the job and to prevent common and occupational diseases as well as occupational accidents. A list of hazardous and dangerous factors in the work of medical personnel was prepared which included recommendations for frequency of examinations, the range of specialists to take part in the examinations, the number of laboratory and functional studies as well as a list of medical contra-indications for work with a specific hazardous occupational factor. For every studied group there was a list of occupational diseases, enumerating the nosological forms, approximate list of job assignments and hazardous factors which can cause the respective occupational conditions.
In order to control the working conditions in treatment and prevention institutions, a Certificate of Sanitary and Technical Conditions of Labour in the health care institutions was developed. The certificate can be used as a guide for conducting sanitary measures and improvement of labour safety. For an institution to complete the certificate, it is necessary to carry out a study, with the help of specialists in sanitary service and other respective organizations, of the general situation in the departments, rooms and wards, to measure the levels of health and safety hazards.
Departments of hygiene of the preventive medicine institutions have been established in the modern centres of sanitary-epidemic inspections. The mission of these departments includes perfecting measures for the prevention of nosocomial infections and their complications in hospitals, creating optimal conditions for treatment and protecting the safety and health of HCWs. Public health doctors and their assistants conduct the preventive monitoring of design and construction of buildings for health care institutions. They see to the compliance of the new premises with the climate conditions, required arrangement of worksites, comfortable labour conditions and systems of rest and nutrition during the work shifts (see the article “Buildings for health care facilities” in this chapter). They also control technical documentation for the new equipment, technological procedures and chemicals. The routine sanitary inspection includes the monitoring of the occupational factors at the worksites and accumulation of the received data in the above-mentioned Certificate of Sanitary and Technical Conditions of Labour. Quantitative measurement of working conditions and prioritization of health improvement measures are established according to hygienic criteria for assessments of labour conditions which are based on indicators of the hazard and danger of labour environment factors and the heaviness and intensity of the working process. The frequency of laboratory studies is determined by the specific needs of each case. Each study usually includes measurement and analysis of microclimate parameters; measurement of indicators of air environment (e.g., content of bacteria and hazardous substances); assessment of the effectiveness of ventilation systems; assessment of the levels of natural and artificial illumination; and measurement of noise levels, ultrasound, ionizing radiation and so on. It is also recommended that time-keeping monitoring of the exposures of the unfavourable factors be conducted, based on the guideline documents.
According to instructions of the Russian government, and in keeping with current existing practice, the hygienic and medical standards should be revised following the accumulation of new data.
Case Study: Violence in Health Care Work
A psychotic patient in his thirties had been forcibly committed to a large psychiatric hospital in the suburbs of a city. He was not regarded as having violent tendencies. After a few days he escaped from his secure ward. The hospital authorities were informed by his relatives that he had returned to his own house. As was routine an escort of three male psychiatric nurses set out with an ambulance to bring the patient back. En route they stopped to pick up a police escort as was routine in such cases. When they arrived at the house, the police escort waited outside, in case a violent incident developed. The three nurses entered and were informed by the relatives that the patient was sitting in an upstairs bedroom. When approached and quietly invited to come back to hospital for treatment the patient produced a kitchen knife which he had hidden. One nurse was stabbed in the chest, another a number of times in the back and the third in the hand and the arm. All three nurses survived but had to spend time in hospital. When the police escort entered the bedroom the patient quietly surrendered the knife.
Home Care Workers: The New York City Experience
Massive use of home care workers in New York City began in 1975 as a response to the needs of the growing population of chronically ill and frail elderly and as an alternative to more expensive care in nursing homes, many of which had long lists of such people waiting for admission. Additionally, it allowed for more personal assistance at a time when nursing homes were perceived as impersonal and uncaring. It also provided entry-level employment to unskilled individuals, mostly women, many of whom were recipients of welfare.
Initially, these workers were employees of the City’s Department of Human Resources but, in 1980, this service was “privatized” and they were recruited, trained and employed by non-profit, community-based social agencies and traditional health care organizations such as hospitals which had to be certified by the State of New York as providers of home care services. The workers are categorized as home makers, personal care workers, health aides, home care attendants and housekeepers, depending on their levels of skills and the kinds of services they provide. Which of these services a particular client uses depends on an evaluation of that person’s health status and needs which is conducted by a licensed health professional, such as a physician, nurse or social worker.
The Home Care Workforce
Home care workers in New York City present a conglomerate of characteristics that provide a unique profile. A recent survey by Donovan, Kurzman and Rotman (1993) found that 94% are female with an average age of 45. About 56% were not born within the continental US and about 51% never completed high school. Only 32% were identified as married, 33% were separated or divorced and 26% were single, while 86% have children, 44% with children under 18 years of age. According to the survey, 63% live with their children and 26% live with a spouse.
The median family income for this group in 1991 was $12,000 per year. In 81% of these families, the home care worker was the primary breadwinner. In 1996, the annual salary of full-time home care workers’ ranged between $16,000 and $28,000; part-time workers earned less.
Such low earnings represent significant economic hardship to the survey respondents: 56% said they could not afford adequate housing; 61% reported being unable to afford furniture or household equipment; 35% said they lacked funds to purchase enough food for their families; and 36% were ineligible for Medicare and unable to afford needed medical care for themselves and their families. As a group, their financial status will inevitably worsen as cuts in government funding force curtailment of the amount and intensity of home care services being provided.
Home Care Services
The services provided by home care workers depend on the needs of the clients being served. Those with greater disability require assistance with the “basic activities of daily living”, which consist of bathing, dressing, toileting, transferring (moving in or out of bed and chairs) and feeding. Those with higher levels of functional capacity need help with the “instrumental activities of daily living”, which comprise housekeeping (cleaning, bed making, dishwashing, and so forth), shopping, food preparation and serving, laundry, using public or private transportation and managing finances. Home care workers may give injections, dispense medications and provide such treatments as passive exercise and massage as prescribed by the client’s physician. A most appreciated service is companionship and assisting the client to participate in recreational activities.
The difficulty of the home care worker’s job is directly related to the home environment and, in addition to physical status, the behaviour of the client and any family members who may be on the scene. Many clients (and the workers as well) live in poor neighbourhoods where crime rates are high, public transportation often marginal and public services substandard. Many live in deteriorated housing with no or non-functioning elevators, dark and dirty stairwells and hallways, lack of heat and hot water, dilapidated plumbing and poorly functioning household appliances. Commuting to and from the client’s home may be arduous and time-consuming.
Many of the clients may have very low levels of functional capacity and require assistance at every turn. Clients’ muscle weakness and lack of coordination, loss of vision and hearing and incontinence of bladder and/or bowels add to the burden of care. Mental difficulties such as senile dementia, anxiety and depression and difficulties in communication because of memory loss and language barriers may also magnify the difficulty. Finally, abusive and demanding behaviour on the part of both clients and their family members may sometimes escalate into acts of violence.
Home Care Work Hazards
Work hazards commonly encountered by home care workers include:
- working alone without assistance
- lack of education and training and remote, if any, supervision
- working in substandard housing in high risk neighbourhoods
- back pain and musculoskeletal injuries incurred while lifting, transferring and supporting clients who may be heavy, weak and poorly coordinated
- violence in the home and in the neighbourhood
- infectious diseases (the health care worker may not have been fully informed of the client’s medical status; recommended gloves, gowns and masks may not be available)
- household chemicals and cleaning supplies (often incorrectly labelled and stored)
- sexual harassment
- work stress.
Stress is probably the most ubiquitous hazard. It is compounded by the fact the worker is usually alone in the home with the client with no simple way to report trouble or summon assistance. Stress is being exacerbated as cost-containment efforts are reducing the hours of service allowed for individual clients.
Prevention Strategies
A number of strategies have been suggested to promote occupational health and safety for home care workers and to improve their lot. They include:
- development and promulgation of standards of practice for home care accompanied by improved education and training so that home care workers can meet them
- education and training in the recognition and avoidance of chemical and other hazards in the home
- training in lifting, carrying and giving physical support to clients as needed in the course of providing services
- preliminary needs assessment of clients supplemented by inspections of their homes so that potential hazards can be identified and eliminated or controlled and needed materials and equipment can be procured
- periodic meetings with supervisors and other home care workers to compare notes and receive instruction. Videotapes may be developed and used for skills demonstrations. The meetings may be supplemented by telephone networks through which workers may communicate with each other to exchange information and alleviate any feelings of isolation.
- establishment of a health and safety committee within each agency to review work-related accidents and problems and develop appropriate preventive interventions
- establishment of an Employee Assistance Programme (EAP) through which the workers may receive counselling for their own psychosocial problems both on- and off-the-job.
Educational and training sessions should be conducted during working hours at a place and time convenient for the workers. They should be supplemented by the distribution of instructional materials designed for the low educational levels of most of the workers and, when necessary, they should be multilingual.
Case study: Violence in health care work
A psychotic patient in his thirties had been forcibly committed to a large psychiatric hospital in the suburbs of a city. He was not regarded as having violent tendencies. After a few days he escaped from his secure ward. The hospital authorities were informed by his relatives that he had returned to his own house. As was routine an escort of three male psychiatric nurses set out with an ambulance to bring the patient back. En route they stopped to pick up a police escort as was routine in such cases. When they arrived at the house, the police escort waited outside, in case a violent incident developed. The three nurses entered and were informed by the relatives that the patient was sitting in an upstairs bedroom. When approached and quietly invited to come back to hospital for treatment the patient produced a kitchen knife which he had hidden. One nurse was stabbed in the chest, another a number of times in the back and the third in the hand and the arm. All three nurses survived but had to spend time in hospital. When the police escort entered the bedroom the patient quietly surrendered the knife.
Daniel Murphy
Social Services
Overview of the Social Work Profession
Social workers function in a wide variety of settings and work with many different kinds of people. They work in community health centres, hospitals, residential treatment centres, substance-abuse programmes, schools, family service agencies, adoption and foster care agencies, day-care facilities and public and private child welfare organizations. Social workers often visit homes for interviews or inspections of home conditions. They are employed by businesses, labour unions, international aid organizations, human rights agencies, prisons and probation departments, agencies for the ageing, advocacy organizations, colleges and universities. They are increasingly entering politics. Many social workers have full- or part-time private practices as psychotherapists. It is a profession that seeks to “improve social functioning by the provision of practical and psychological help to people in need” (Payne and Firth-Cozens 1987).
Generally, social workers with doctorates work in community organization, planning, research, teaching or combined areas. Those with bachelor’s degrees in social work tend to work in public assistance and with the elderly, mentally retarded and developmentally disabled; social workers with master’s degrees are usually found in mental health, occupational social work and medical clinics (Hopps and Collins 1995).
Hazards and Precautions
Stress
Studies have shown that stress in the workplace is caused, or contributed to, by job insecurity, poor pay, work overload and lack of autonomy. All of these factors are features of the work life of social workers in the late 1990s. It is now accepted that stress is often a contributing factor to illness. One study has shown that 50 to 70% of all medical complaints among social workers are linked to stress (Graham, Hawkins and Blau 1983).
As the social work profession has attained vendorship privileges, managerial responsibilities and increased numbers in private practice, it has become more vulnerable to professional liability and malpractice suits in countries such as the United States which permit such legal actions, a fact which contributes to stress. Social workers are also increasingly dealing with bioethical issues—those of life and death, of research protocols, of organ transplantation and of resource allocation. Often there is inadequate support for the psychological toll confronting these issues can take on involved social workers. Increased pressures of high caseloads as well as increased reliance on technology makes for less human contact, a fact which is likely true for most professions, but particularly difficult for social workers whose choice of work is so related to having face to face contact.
In many countries, there has been a shift away from government-funded social programmes. This policy trend directly affects the social work profession. The values and goals generally held by social workers—full employment, a “safety net” for the poor, equal opportunity for advancement—are not supported by these current trends.
The movement away from spending on programmes for the poor has produced what has been called an “upside-down welfare state” (Walz, Askerooth and Lynch 1983). One result of this, among others, has been increased stress for social workers. As resources decline, demand for services is on the rise; as the safety net frays, frustration and anger must rise, both for clients and for social workers themselves. Social workers may increasingly find themselves in conflict over respecting the values of the profession versus meeting statutory requirements. The code of ethics of the US National Association of Social Workers, for example, mandates confidentiality for clients which may be broken only when it is for “compelling professional reasons”. Further, social workers are to promote access to resources in the interest of “securing or retaining social justice”. The ambiguity of this could be quite problematic for the profession and a source of stress.
Violence
Work-related violence is a major concern for the profession. Social workers as problem-solvers on the most personal level are particularly vulnerable. They work with powerful emotions, and it is the relationship with their clients which becomes the focal point for expression of these emotions. Often, an underlying implication is that the client is unable to manage his or her own problems and needs the help of social workers to do so. The client may, in fact, be seeing social workers involuntarily, as, for example, in a child welfare setting where parental abilities are being evaluated. Cultural mores might also interfere with accepting offers of help from someone of another cultural background or sex (the preponderence of social workers are women) or outside of the immediate family. There may be language barriers, necessitating the use of translators. This can be distracting at least or even totally disruptive and may present a skewed picture of the situation at hand. These language barriers certainly affect the ease of communication, which is essential in this field. Further, social workers may work in locations which are in high-crime areas, or the work might take them into the “field” to visit clients who live in those areas.
Application of safety procedures is uneven in social agencies, and, in general, insufficient attention has been paid to this area. Prevention of violence in the workplace implies training, managerial procedures and modifications of the physical environment and/or communication systems (Breakwell 1989).
A curriculum for safety has been suggested (Griffin 1995) which would include:
- training in constructive use of authority
- crisis intervention
- field and office safety
- physical plant set-up
- general prevention techniques
- ways to predict potential violence.
Other Hazards
Because social workers are employed in such a variety of settings, they are exposed to many of the hazards of the workplace discussed elsewhere in this Encyclopaedia. Mention should be made, however, that these hazards include buildings with poor or unclean air flow (“sick buildings”) and exposures to infection. When funding is scarce, maintenance of physical plants suffers and risk of exposure increases. The high percentage of social workers in hospital and out-patient medical settings suggests vulnerability to infection exposure. Social workers see patients with conditions like hepatitis, tuberculosis and other highly contagious diseases as well as human immunodeficiency virus (HIV) infection. In response to this risk for all health workers, training and measures for infection control are necessary and have been mandated in many countries. The risk, however, persists.
It is evident that some of the problems faced by social workers are inherent in a profession which is so centred on lessening human suffering as well as one which is so affected by changing social and political climates. At the end of the twentieth century, the profession of social work finds itself in a state of flux. The values, ideals and rewards of the profession are also at the heart of the hazards it presents to its practitioners.
Are They Health Care Workers, Too?
Often overlooked when considering the safety and well-being of health care workers are students attending medical, dental, nursing and other schools for health professionals and volunteers serving pro bono in healthcare facilities. Since they are not “employees” in the technical or legal sense of the term, they are ineligible for workers’ compensation and employment-based health insurance in many jurisdictions. Health care administrators have only a moral obligation to be concerned about their health and safety.
The clinical segments of their training bring medical, nursing and dental students into direct contact with patients who may have infectious diseases. They perform or assist in a variety of invasive procedures, including taking blood samples, and often do laboratory work involving body fluids and specimens of urine and faeces. They are usually free to wander about the facility, entering areas containing potential hazards often, since such hazards are rarely posted, without an awareness of their presence. They are usually supervised very loosely, if at all, while their instructors are often not very knowledgeable, or even interested, in matters of safety and health protection.
Volunteers are rarely permitted to participate in clinical care but they do have social contacts with patients and they usually have few restrictions with respect to areas of the facility they may visit.
Under normal circumstances, students and volunteers share with health care workers the risks of exposure to potentially harmful hazards. These risks are exacerbated at times of crisis and in emergencies when they step into or are ordered into the breech. Clearly, even though it may not be spelled out in laws and regulations or in organizational procedure manuals, they are more than entitled to the concern and protection extended to “regular” health care workers.
Health Care: Its Nature and its Occupational Health Problems
Health care is a labour intensive industry and, in most countries, health care workers (HCWs) constitute a major sector of the workforce. They comprise a wide range of professional, technical and support personnel working in a large variety of settings. In addition to health professionals, laboratory technicians, pharmacists, social workers and others involved in clinical services, they include administrative and clerical personnel, housekeeping and dietary staff, laundry workers, engineers, electricians, painters and maintenance workers who repair and refurbish the building and the equipment it contains. In contrast with those providing direct care, these support workers usually have only casual, incidental contact with patients.
HCWs represent diverse educational, social and ethnic levels and are usually predominantly female. Many, particularly in home care, are employed in entry-level positions and require considerable basic training. Table 1 lists samples of health care functions and associated occupations.
Table 1. Examples of health care functions and associated occupations
|
Functions |
Occupational category * |
Specific occupations |
|
Direct patient care |
Health-diagnosing occupations |
Physicians |
|
Technical support |
Health technicians |
Clinical laboratory technicians |
|
Services |
Health services |
Dental assistants |
|
Administrative support |
Clerical services |
Billing clerks |
|
Research |
Scientific occupations |
Scientists and research |
* Occupational categories are, in part, adapted from those used by the US Department of Labor, Bureau of Labor Statistics.
A segment of the health sector (unfortunately, often too small and under-resourced in most communities) is devoted to direct and indirect preventive services. The major focus of the health care industry, however, is the diagnosis, treatment and care of the sick. This creates a special set of dynamics, for the sick exhibit varying levels of physical and emotional dependencies that set them apart from the customers in such personal services industries as, for example, retail trade, restaurants and hotels. They require, and traditionally receive, special services and considerations, often on an emergency basis, provided frequently at the expense of the HCWs’ personal comfort and safety.
Reflecting their size and numbers of employees, acute and long-term care facilities constitute perhaps the most prominent elements in the health care industry. They are supplemented by outpatient clinics, “surgicenters” (facilities for outpatient surgery), clinical and pathological laboratories, pharmacies, x-ray and imaging centres, ambulance and emergency care services, individual and group offices, and home care services. These may be located within a hospital or operated elsewhere under its aegis, or they may be free-standing and operated independently. It should be noted that there are profound differences in the way health services are delivered, ranging from the well-organized, “high tech” care available in urban centres in developed countries to the underserved areas in rural communities, in developing countries and in inner-city enclaves in many large cities.
Superimposed on the health care system is a massive educational and research establishment in which students, faculty, researchers and support staffs often come in direct contact with patients and participate in their care. This comprises schools of medicine, dentistry, nursing, public health, social work and the variety of technical disciplines involved in health care.
The health care industry has been undergoing profound changes during the past few decades. Ageing of the population, especially in developed countries, has amplified the use of nursing homes, domiciliary facilities and home care services. Scientific and technological developments have not only led to the creation of new types of facilities staffed by new classes of specially-trained personnel, but they have also de-emphasized the role of the acute care hospital. Now, many services requiring inpatient care are being provided on an ambulatory basis. Finally, fiscal constraints dictated by the continuing escalation of health care costs have been reconfiguring the health care industry, at least in developing countries, resulting in pressure for cost-containment to be achieved through changes in the organization of health care services.
HCWs who are in direct contact with the sick, wherever they work, are exposed to a number of unique hazards. They face the risk of acquiring infections from the patients they serve, as well as the risk of musculoskeletal injuries when lifting, transferring or restraining them. Support staff not directly involved in patient care (e.g., laundry and housekeeping and materials handling workers) are not only routinely exposed to chemicals, such as cleaning agents and disinfectants of industrial strength, but are also exposed to biological hazards from contaminated linens and wastes (see figure 1). There is also the ethos of health care which, especially in emergency situations, requires HCWs to put the safety and comfort of their patients above their own. Coping with the stress of therapeutic failures, death and dying often takes its toll in worker burnout. All this is compounded by shift work, deliberate or inadvertent understaffing and the necessity of catering to the sometimes unreasonable demands from patients and their families. Finally, there is the threat of abuse and violence from patients, particularly when the job requires them to work alone or takes them into unsafe areas. All these are described in greater detail in other articles in this chapter and elsewhere in this Encyclopaedia.
Figure 1. Handling contaminated biological material
Health Sciences Centre, Winnipeg, Manitoba, Canada
The US National Institute for Occupational Safety and Health (NIOSH) reported that needle punctures, musculoskeletal sprains and back injuries probably were the most common injuries in the health care industry (Wugofski 1995). The World Health Organization (WHO) Conference on Occupational Hazards in 1981 identified as its five main areas of concern:
- cuts, lacerations and fractures
- back injuries
- lack of personal safety equipment
- poor maintenance of mechanical and electrical systems
- assault by patients.
Are they health care workers, too?
Often overlooked when considering the safety and well-being of health care workers are students attending medical, dental, nursing and other schools for health professionals and volunteers serving pro bono in healthcare facilities. Since they are not “employees” in the technical or legal sense of the term, they are ineligible for workers’ compensation and employment-based health insurance in many jurisdictions. Health care administrators have only a moral obligation to be concerned about their health and safety.
The clinical segments of their training bring medical, nursing and dental students into direct contact with patients who may have infectious diseases. They perform or assist in a variety of invasive procedures, including taking blood samples, and often do laboratory work involving body fluids and specimens of urine and faeces. They are usually free to wander about the facility, entering areas containing potential hazards often, since such hazards are rarely posted, without an awareness of their presence. They are usually supervised very loosely, if at all, while their instructors are often not very knowledgeable, or even interested, in matters of safety and health protection.
Volunteers are rarely permitted to participate in clinical care but they do have social contacts with patients and they usually have few restrictions with respect to areas of the facility they may visit.
Under normal circumstances, students and volunteers share with health care workers the risks of exposure to potentially harmful hazards. These risks are exacerbated at times of crisis and in emergencies when they step into or are ordered into the breech. Clearly, even though it may not be spelled out in laws and regulations or in organizational procedure manuals, they are more than entitled to the concern and protection extended to “regular” health care workers.
Leon Warshaw
Biological Hazards
Biological hazards, which pose a risk for infectious disease, are common throughout the world, but they are particularly problematic in developing countries. While the hepatitis B virus (HBV) is a nearly universal threat to HCWs, it is particularly important in African and Asian countries where this virus is endemic. As discussed later in this chapter, the risk of HBV transmission after percutaneous exposure to hepatitis B surface antigen (HBsAg) positive blood is approximately 100-fold higher than the risk of transmitting the human immunodeficiency virus (HIV) through percutaneous exposure to HIV-infected blood (i.e., 30% versus 0.3%). Nonetheless, there has indeed been an evolution of concern regarding parenteral exposure to blood and body fluids from the pre-HIV to the AIDS era. McCormick et al. (1991) found that the annual reported incidents of injuries from sharp instruments increased more than threefold during a 14-year period and among medical house officers the reported incidents increased ninefold. Overall, nurses incur approximately two-thirds of the needlestick injuries reported. Yassi and McGill (1991) also noted that nursing staff, particularly nursing students, are at highest risk for needlestick injuries, but they also found that approximately 7.5% of medical personnel reported exposures to blood and body fluids, a figure that is probably low because of underreporting. These data were consistent with other reports which indicated that, while there is increased reporting of needlesticks reflecting concerns about HIV and AIDS, certain groups continue to underreport. Sterling (1994) concludes that underreporting of needlestick injuries ranges from 40 to 60%.
Certain risk factors clearly enhance the likelihood of transmission of bloodborne diseases; these are discussed in the article “Prevention of occupational transmission of bloodborne pathogens”. Frequent exposure has indeed been associated with high seroprevalence rates of hepatitis B among laboratory workers, surgeons and pathologists. The risk of hepatitis C is also increased. The trend towards greater attention to prevention of needlestick injuries is, however, also noteworthy. The adoption of universal precautions is an important advance. Under universal precautions, it is assumed that all blood-containing fluid is potentially infectious and that appropriate safeguards should always be invoked. Safe disposal containers for needles and other sharp instruments are increasingly being placed in conveniently accessible locations in treatment areas, as illustrated in figure 2. The use of new devices, such as the needle-less access system for intravenous treatment and/or blood sampling has been shown to be a cost-effective method of reducing needlestick injuries (Yassi and McGill 1995).
Figure 2. Disposal container for sharp instruments and devices
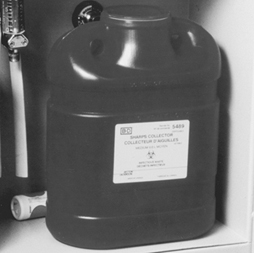
Health Sciences Centre, Winnipeg, Manitoba, Canada
Blood and body fluids are not the only source of infection for HCWs. Tuberculosis (TB) is also on the rise again in parts of the world where previously its spread had been curtailed and, as discussed later in this chapter, is a growing occupational health concern. In this, as in other nosocomial infections, such concern is heightened by the fact that so many of the organisms involved have become drug-resistant. There is also the problem of new outbreaks of deadly infectious agents, such as the Ebola virus. The article “Overview of infectious diseases” summarizes the major infectious disease risks for HCWs.
Chemical Hazards
HCWs are exposed to a wide variety of chemicals, including disinfectants, sterilants, laboratory reagents, drugs and anaesthetic agents, to name just a few of the categories. Figure 3 shows a storage cabinet in an area of a large hospital where prosthetics are fabricated and clearly illustrates the vast array of chemicals that are present in health care facilities. Some of these substances are highly irritating and may also be sensitizing. Some disinfectants and antiseptics also tend to be quite toxic, also with irritating and sensitizing propensities that may induce skin or respiratory tract disease. Some, like formaldehyde and ethylene oxide, are classified as mutagens, teratogens and human carcinogens as well. Prevention depends on the nature of the chemical, the maintenance of the apparatus in which it is used or applied, environmental controls, worker training and, in some instances, the availability of correct personal protective equipment. Often such control is straightforward and not very expensive. For example, Elias et al. (1993) showed how ethylene oxide exposure was controlled in one health care facility. Other articles in this chapter address chemical hazards and their management.
Figure 3. Storage cabinet for hazardous chemicals

Health Sciences Centre, Winnipeg, Manitoba, Canada
Physical Hazards and the Building Environment
In addition to the specific environmental contaminants faced by HCWs, many health care facilities also have documented indoor air quality problems. Tran et al. (1994), in studying symptoms experienced by operating room personnel, noted the presence of the “sick building syndrome” in one hospital. Building design and maintenance decisions are, therefore, extremely important in health care facilities. Particular attention must be paid to correct ventilation in specific areas such as laboratories, operating rooms and pharmacies, the availability of hoods and avoidance of the insertion of chemical-laden fumes into the general air-conditioning system. Controlling the recirculation of air and using special equipment (e.g., appropriate filters and ultraviolet lamps) is needed to prevent the transmission of air-borne infectious agents. Aspects of the construction and planning of health care facilities are discussed in the article “Buildings for health care facilities”.
Physical hazards are also ubiquitous in hospitals (see “Exposure to physical agents” in this chapter). The wide variety of electrical equipment used in hospitals can present an electrocution hazard to patients and staff if not properly maintained and grounded (see figure 4). Especially in hot and humid environments, heat exposure may present a problem to workers in such areas as laundries, kitchens and boiler rooms. Ionizing radiation is a special concern for staff in diagnostic radiology (i.e., x ray, angiography, dental radiography and computerized axial tomography (CAT) scans) as well as for those in therapeutic radiology. Controlling such radiation exposures is a routine matter in designated departments where there is careful supervision, well-trained technicians and properly shielded and maintained equipment, but it can be a problem when portable equipment is used in emergency rooms, intensive care units and operating rooms. It can also be a problem to housekeeping and other support staff whose duties take them into areas of potential exposure. In many jurisdictions these workers have not been properly trained to avoid this hazard. Exposure to ionizing radiation may also present a problem in diagnostic and therapeutic nuclear medicine units and in preparing and distributing doses of radioactive pharmaceuticals. In some cases, however, radiation exposure remains a serious problem (see the article “Occupational health and safety practice: The Russian experience” in this chapter).
Figure 4. Electrical equipment in hospital
Health Sciences Centre, Winnipeg, Manitoba, Canada
Contradicting the prevailing impression of hospitals as quiet workplaces, Yassi et al. (1991) have documented the surprising extent of noise-induced hearing loss among hospital workers (see table 2). The article “Ergonomics of the physical work environment” in this chapter offers useful recommendations for controlling this hazard, as does table 3.
Table 2. 1995 integrated sound levels
|
Area monitored |
dBA (lex) Range |
|
Cast room |
76.32 to 81.9 |
|
Central energy |
82.4 to 110.4 |
|
Nutrition and food services (main kitchen) |
|
|
Housekeeping |
|
|
Laundry |
|
|
Linen service |
76.3 to 91.0 |
|
Mailroom |
|
|
Maintenance |
|
|
Materials handling |
|
|
Print shop |
|
|
Rehabilitation engineering |
|
Note: “Lex” means the equivalent sound level or the steady sound level in dBA which, if present in a workplace for 8 hours, would contain the same acoustic energy.
Table 3. Ergonomic noise reduction options
|
Work area |
Process |
Control options |
|
Central energy |
General area |
Enclose the source |
|
Dietetics |
Pot washer |
Automate process |
|
Housekeeping |
Burnishing |
Purchasing criteria |
|
Laundry |
Dryer/washer |
Isolate and reduce vibration |
|
Mailroom |
Tuberoom |
Purchasing criteria |
|
Maintenance |
Various equipment |
Purchasing criteria |
|
Materiel handling and |
Carts |
Maintenance |
|
Print shop |
Press operator |
Maintenance |
|
Rehabilitation |
Orthotics |
Purchasing criteria |
By far the most common and most costly type of injury faced by HCWs is back injury. Nurses and attendants are at greatest risk of musculoskeletal injuries due to the large amount of patient lifting and transferring that their jobs require. The epidemiology of back injury in nurses was summarized by Yassi et al. (1995a) with respect to one hospital. The pattern they observed mirrors those that have been universally reported. Hospitals are increasingly turning to preventive measures which may include staff training and the use of mechanical lifting devices. Many are also providing up-to-date diagnostic, therapeutic and rehabilitation health services that will minimize lost time and disability and are cost-effective (Yassi et al. 1995b). Hospital ergonomics has taken on increasing importance and, therefore, is the subject of a review article in this chapter. The specific problem of the prevention and management of back pain in nurses as one of the most important problems for this cohort of HCWs is also discussed in the article “Prevention and management of back pain in nurses” in this chapter. Table 4 lists the total number of injuries in a one-year period.
Table 4. Total number of injuries, mechanism of injury and nature of industry (one hospital, all departments), 1 April 1994 to 31 March 1995
|
Nature of injury sustained |
Total |
||||||||||||
|
Mechanism |
Blood/ |
Cut/ |
Bruise/ |
Sprain/ |
Fracture/ |
Burn/ |
Human |
Broken |
Head- |
Occupa- |
Other3 |
Un- |
|
|
Exertion |
|||||||||||||
|
Transferring |
105 |
105 |
|||||||||||
|
Lifting |
83 |
83 |
|||||||||||
|
Assisting |
4 |
4 |
|||||||||||
|
Turning |
27 |
27 |
|||||||||||
|
Breaking fall |
28 |
28 |
|||||||||||
|
Pushing |
1 |
25 |
26 |
||||||||||
|
Lifting |
1 |
52 |
1 |
54 |
|||||||||
|
Pulling |
14 |
14 |
|||||||||||
|
Combination- |
38 |
38 |
|||||||||||
|
Other |
74 |
74 |
|||||||||||
|
Fall |
3 |
45 |
67 |
3 |
1 |
119 |
|||||||
|
Struck/ |
66 |
76 |
5 |
2 |
2 |
1 |
152 |
||||||
|
Caught in/ |
13 |
68 |
8 |
1 |
1 |
91 |
|||||||
|
Exp. |
3 |
1 |
4 |
19 |
16 |
12 |
55 |
||||||
|
Staff abuse |
|||||||||||||
|
Patient |
16 |
11 |
51 |
28 |
8 |
3 |
1 |
2 |
120 |
||||
|
Spill/splashes |
80 |
1 |
81 |
||||||||||
|
Drug/ |
2 |
2 |
|||||||||||
|
Exp. |
5 |
5 |
10 |
||||||||||
|
Needlesticks |
159 |
22 |
181 |
||||||||||
|
Scalpel cuts |
34 |
14 |
48 |
||||||||||
|
Other5 |
3 |
1 |
29 |
1 |
6 |
40 |
|||||||
|
Unknown (no |
8 |
8 |
|||||||||||
|
Total |
289 |
136 |
243 |
558 |
5 |
33 |
8 |
7 |
19 |
25 |
29 |
8 |
1,360 |
1 No blood/body fluid. 2 This includes rashes/dermatitis/work-related illness/burning eyes, irritated eyes. 3 Exposure to chemical or physical agents but with no documented injuries affects. 4 Accident not reported. 5 Exposure to cold/heat, unknown.
In discussing musculoskeletal and ergonomic problems, it is important to note that while those engaged in direct patient care may be at greatest risk (see figure 5) many of the support personnel in hospital must contend with similar ergonomic burdens (see figure 6 and figure 7). The ergonomic problems facing hospital laundry workers have been well-documented (Wands and Yassi 1993) (see figure 8, figure 9 and figure 10) and they also are common among dentists, otologists, surgeons and especially microsurgeons, obstetricians, gynaecologists and other health personnel who often must work in awkward postures.
Figure 5. Patient lifting is an ergonomic hazard in most hospitals
Health Sciences Centre, Winnipeg, Manitoba, Canada
Figure 6. Overhead painting: A typical ergonomic hazard for a tradesworker

Health Sciences Centre, Winnipeg, Manitoba, Canada
Figure 7. Cast-making involves many ergonomic stresses

Health Sciences Centre, Winnipeg, Manitoba, Canada
Figure 8. Laundry work such as this can cause repetitive stress injury to the upper limbs

Health Sciences Centre, Winnipeg, Manitoba, Canada
Figure 9. This laundry task requires working in an awkward position

Health Sciences Centre, Winnipeg, Manitoba, Canada
Figure 10. A poorly designed laundry operation can cause back strain
Health Sciences Centre, Winnipeg, Manitoba, Canada
Organizational Problems
The article “Strain in health care work” contains a discussion of some of the organizational problems in hospitals and a summary of the principal findings of Leppanen and Olkinuora (1987), who reviewed Finnish and Swedish studies of stress among HCWs. With the rapid changes currently under way in this industry, the extent of alienation, frustration and burnout among HCWs is considerable. Added to that is the prevalence of staff abuse, an increasingly troublesome problem in many facilities (Yassi 1994). While it is often thought that the most difficult psychosocial problem faced by HCWs is dealing with death and dying, it is being recognized increasingly that the nature of the industry itself, with its hierarchical structure, its growing job insecurity and the high demands unsupported by adequate resources, is the cause of the variety of stress-related illness faced by HCWs.
The Nature of the Health Care Sector
In 1976, Stellman wrote, “If you ever wondered how people can manage to work with the sick and always stay healthy themselves, the answer is that they can’t” (Stellman 1976). The answer has not changed, but the potential hazards have clearly expanded from infectious diseases, back and other injuries, stress and burnout to include a large variety of potentially toxic environmental, physical and psychosocial exposures. The world of the HCW continues to be largely unmonitored and largely unregulated. None the less, progress is being made in addressing occupational health and safety hazards in hospitals. The International Commission on Occupational Health (ICOH) has a sub-committee addressing this problem, and several international conferences have been held with published proceedings that offer useful information (Hagberg et al. 1995). The US Centers for Disease Control and Prevention (CDC) and NIOSH have proposed guidelines to address many of the problems of the health care industry discussed in this article (e.g., see NIOSH 1988). The number of articles and books addressing health and safety issues for HCWs has been growing rapidly, and good overviews of health and safety in the US health care industry have been published (e.g., Charney 1994; Lewy 1990; Sterling 1994). The need for systematic data collection, study and analysis regarding hazards in the health care industry and the desirability of assembling interdisciplinary occupational health teams to address them have become increasingly evident.
When considering occupational health and safety in the health care industry, it is crucial to appreciate the enormous changes currently taking place in it. Health care “reform”, being instituted in most of the developed countries of the world, is creating extraordinary turbulence and uncertainty for HCWs, who are being asked to absorb rapid changes in their work tasks often with greater exposure to risks. The transformation of health care is spurred, in part, by advances in medical and scientific knowledge, the development of innovative technological procedures and the acquisition of new skills. It is also being driven, however, and perhaps to an even greater extent, by concepts of cost-effectiveness and organizational efficiency, in which “downsizing” and “cost control” have often seemed to become goals in themselves. New institutional incentives are being introduced at different organizational levels in different countries. The contracting out of jobs and services that had traditionally been carried out by a large stable workforce is now increasingly becoming the norm. Such contracting out of work is reported to have helped the health administrators and politicians achieve their long-term goal of making the process of health care more flexible and more accountable. These changes have also brought changes in roles that were previously rather well-defined, undermining the traditional hierarchical relationships among planners, administrators, physicians and other health professionals. The rise of investor-owned health care organizations in many countries has introduced a new dynamic in the financing and management of health services. In many situations, HCWs have been forced into new working relationships that involve such changes as downgrading services so that they can be performed by less-skilled workers at lower pay, reduced staffing levels, staff redeployments involving split shifts and part-time assignments. At the same time, there has been a slow but steady growth in the numbers of such physician surrogates as physician assistants, nurse practitioners, midwives and psychiatric social workers who command lower rates of pay than the physicians they are replacing. (The ultimate social and health costs both to HCWs and to the public, as patients and payers, is still to be determined.)
A growing trend in the US that is also emerging in the UK and northern European countries is “managed care”. This generally involves the creation of organizations paid on a per capita basis by insurance companies or government agencies to provide or contract for the provision of a comprehensive range of health services to a voluntarily-enrolled population of subscribers. Their aim is to reduce the costs of health care by “managing” the process: using administrative procedures and primary care physicians as “gatekeepers” to control the utilization of expensive in-patient hospital days, reducing referrals to high-priced specialists and use of costly diagnostic procedures, and denying coverage for expensive new forms of “experimental” treatment. The growing popularity of these managed care systems, fuelled by aggressive marketing to employer- and government-sponsored groups and individuals, has made it difficult for physicians and other health care providers to resist becoming involved. Once engaged, there is a variety of financial incentives and disincentives to influence their judgement and condition their behaviour. The loss of their traditional autonomy has been particularly painful for many medical practitioners and has had a profound influence on their patterns of practice and their relationships with other HCWs.
These rapid changes in the organization of the health care industry are having profound direct and indirect effects on the health and safety of HCWs. They affect the ways health services are organized, managed, delivered and paid for. They affect the ways HCWs are trained, assigned and supervised and the extent to which considerations of their health and safety are addressed. This should be kept in mind as the various occupational health hazards faced by HCWs are discussed in this chapter. Finally, although it may not appear to be directly relevant to the content of this chapter, thought should be given to the implications of the well-being and performance of HCWs to the quality and effectiveness of the services they provide to their patients.
Statistical Methods
There is much debate on the role of statistics in epidemiological research on causal relationships. In epidemiology, statistics is primarily a collection of methods for assessing data based on human (and also on animal) populations. In particular, statistics is a technique for the quantification and measurement of uncertain phenomena. All the scientific investigations which deal with non-deterministic, variable aspects of reality could benefit from statistical methodology. In epidemiology, variability is intrinsic to the unit of observation—a person is not a deterministic entity. While experimental designs would be improved in terms of better meeting the assumptions of statistics in terms of random variation, for ethical and practical reasons this approach is not too common. Instead, epidemiology is engaged in observational research which has associated with it both random and other sources of variability.
Statistical theory is concerned with how to control unstructured variability in the data in order to make valid inferences from empirical observations. Lacking any explanation for the variable behaviour of the phenomenon studied, statistics assumes it as random—that is, non-systematic deviations from some average state of nature (see Greenland 1990 for a criticism of these assumptions).
Science relies on empirical evidence to demonstrate whether its theoretical models of natural events have any validity. Indeed, the methods used from statistical theory determine the degree to which observations in the real world conform to the scientists’ view, in mathematical model form, of a phenomenon. Statistical methods, based in mathematics, have therefore to be carefully selected; there are plenty of examples about “how to lie with statistics”. Therefore, epidemiologists should be aware of the appropriateness of the techniques they apply to measure the risk of disease. In particular, great care is needed when interpreting both statistically significant and statistically non-significant results.
The first meaning of the word statistics relates to any summary quantity computed on a set of values. Descriptive indices or statistics such as the arithmetic average, the median or the mode, are widely used to summarize the information in a series of observations. Historically, these summary descriptors were used for administrative purposes by states, and therefore they were named statistics. In epidemiology, statistics that are commonly seen derive from the comparisons inherent to the nature of epidemiology, which asks questions such as: “Is one population at greater risk of disease than another?” In making such comparisons, the relative risk is a popular measure of the strength of association between an individual characteristic and the probability of becoming ill, and it is most commonly applied in aetiological research; attributable risk is also a measure of association between individual characteristics and disease occurrence, but it emphasizes the gain in terms of number of cases spared by an intervention which removes the factor in question—it is mostly applied in public health and preventive medicine.
The second meaning of the word statistics relates to the collection of techniques and the underlying theory of statistical inference. This is a particular form of inductive logic which specifies the rules for obtaining a valid generalization from a particular set of empirical observations. This generalization would be valid provided some assumptions are met. This is the second way in which an uneducated use of statistics can deceive us: in observational epidemiology, it is very difficult to be sure of the assumptions implied by statistical techniques. Therefore, sensitivity analysis and robust estimators should be companions of any correctly conducted data analysis. Final conclusions also should be based on overall knowledge, and they should not rely exclusively on the findings from statistical hypothesis testing.
Definitions
A statistical unit is the element on which the empirical observations are made. It could be a person, a biological specimen or a piece of raw material to be analysed. Usually the statistical units are independently chosen by the researcher, but sometimes more complex designs can be set up. For example, in longitudinal studies, a series of determinations is made on a collection of persons over time; the statistical units in this study are the set of determinations, which are not independent, but structured by their respective connections to each person being studied. Lack of independence or correlation among statistical units deserves special attention in statistical analysis.
A variable is an individual characteristic measured on a given statistical unit. It should be contrasted with a constant, a fixed individual characteristic—for example, in a study on human beings, having a head or a thorax are constants, while the gender of a single member of the study is a variable.
Variables are evaluated using different scales of measurement. The first distinction is between qualitative and quantitative scales. Qualitative variables provide different modalities or categories. If each modality cannot be ranked or ordered in relation to others—for example, hair colour, or gender modalities—we denote the variable as nominal. If the categories can be ordered—like degree of severity of an illness—the variable is called ordinal. When a variable consists of a numeric value, we say that the scale is quantitative. A discrete scale denotes that the variable can assume only some definite values—for example, integer values for the number of cases of disease. A continuous scale is used for those measures which result in real numbers. Continuous scales are said to be interval scales when the null value has a purely conventional meaning. That is, a value of zero does not mean zero quantity—for example, a temperature of zero degrees Celsius does not mean zero thermal energy. In this instance, only differences among values make sense (this is the reason for the term “interval” scale). A real null value denotes a ratio scale. For a variable measured on that scale, ratios of values also make sense: indeed, a twofold ratio means double the quantity. For example, to say that a body has a temperature two times greater than a second body means that it has two times the thermal energy of the second body, provided that the temperature is measured on a ratio scale (e.g., in Kelvin degrees). The set of permissible values for a given variable is called the domain of the variable.
Statistical Paradigms
Statistics deals with the way to generalize from a set of particular observations. This set of empirical measurements is called a sample. From a sample, we calculate some descriptive statistics in order to summarize the information collected.
The basic information that is generally required in order to characterize a set of measures relates to its central tendency and to its variability. The choice between several alternatives depends on the scale used to measure a phenomenon and on the purposes for which the statistics are computed. In table 1 different measures of central tendency and variability (or, dispersion) are described and associated with the appropriate scale of measurement.
Table 1. Indices of central tendency and dispersion by scale of measurement
|
Scale of measurement |
||||
|
Qualitative |
Quantitative |
|||
|
Indices |
Definition |
Nominal |
Ordinal |
Interval/ratio |
|
Arithmetic mean |
Sum of the observed values divided by the total number of observations |
|
|
x |
|
Median |
Midpoint value of the observed distribution |
|
x |
x |
|
Mode |
Most frequent value |
x |
x |
x |
|
Range |
Lowest and highest values of the distribution |
|
x |
x |
|
Variance |
Sum of the squared difference of each value from the mean divided by the total number of observations minus 1 |
|
|
x |
The descriptive statistics computed are called estimates when we use them as a substitute for the analogous quantity of the population from which the sample has been selected. The population counterparts of the estimates are constants called parameters. Estimates of the same parameter can be obtained using different statistical methods. An estimate should be both valid and precise.
The population-sample paradigm implies that validity can be assured by the way the sample is selected from the population. Random or probabilistic sampling is the usual strategy: if each member of the population has the same probability of being included in the sample, then, on average, our sample should be representative of the population and, moreover, any deviation from our expectation could be explained by chance. The probability of a given deviation from our expectation also can be computed, provided that random sampling has been performed. The same kind of reasoning applies to the estimates calculated for our sample with regard to the population parameters. We take, for example, the arithmetic average from our sample as an estimate of the mean value for the population. Any difference, if it exists, between the sample average and the population mean is attributed to random fluctuations in the process of selection of the members included in the sample. We can calculate the probability of any value of this difference, provided the sample was randomly selected. If the deviation between the sample estimate and the population parameter cannot be explained by chance, the estimate is said to be biased. The design of the observation or experiment provides validity to the estimates and the fundamental statistical paradigm is that of random sampling.
In medicine, a second paradigm is adopted when a comparison among different groups is the aim of the study. A typical example is the controlled clinical trial: a set of patients with similar characteristics is selected on the basis of pre-defined criteria. No concern for representativeness is made at this stage. Each patient enrolled in the trial is assigned by a random procedure to the treatment group—which will receive standard therapy plus the new drug to be evaluated—or to the control group—receiving the standard therapy and a placebo. In this design, the random allocation of the patients to each group replaces the random selection of members of the sample. The estimate of the difference between the two groups can be assessed statistically because, under the hypothesis of no efficacy of the new drug, we can calculate the probability of any non-zero difference.
In epidemiology, we lack the possibility of assembling randomly exposed and non-exposed groups of people. In this case, we still can use statistical methods, as if the groups analysed had been randomly selected or allocated. The correctness of this assumption relies mainly on the study design. This point is particularly important and underscores the importance of epidemiological study design over statistical techniques in biomedical research.
Signal and Noise
The term random variable refers to a variable for which a defined probability is associated with each value it can assume. The theoretical models for the distribution of the probability of a random variable are population models. The sample counterparts are represented by the sample frequency distribution. This is a useful way to report a set of data; it consists of a Cartesian plane with the variable of interest along the horizontal axis and the frequency or relative frequency along the vertical axis. A graphic display allows us to readily see what is (are) the most frequent value(s) and how the distribution is concentrated around certain central values like the arithmetic average.
For the random variables and their probability distributions, we use the terms parameters, mean expected value (instead of arithmetic average) and variance. These theoretical models describe the variability in a given phenomenon. In information theory, the signal is represented by the central tendency (for example, the mean value), while the noise is measured by a dispersion index (such as the variance).
To illustrate statistical inference, we will use the binomial model. In the sections which follow, the concepts of point estimates and confidence intervals, tests of hypotheses and probability of erroneous decisions, and power of a study will be introduced.
Table 2. Possible outcomes of a binomial experiment (yes = 1, no = 0) and their probabilities (n = 3)
|
Worker |
Probability |
||
|
A |
B |
C |
|
|
0 |
0 |
0 |
|
|
1 |
0 |
0 |
|
|
0 |
1 |
0 |
|
|
0 |
0 |
1 |
|
|
0 |
1 |
1 |
|
|
1 |
0 |
1 |
|
|
1 |
1 |
0 |
|
|
1 |
1 |
1 |
|
An Example: The Binomial Distribution
In biomedical research and epidemiology, the most important model of stochastic variation is the binomial distribution. It relies on the fact that most phenomena behave as a nominal variable with only two categories: for example, the presence/absence of disease: alive/dead, or recovered/ill. In such circumstances, we are interested in the probability of success—that is, in the event of interest (e.g., presence of disease, alive or recovery)—and in the factors or variables that can alter it. Let us consider n = 3 workers, and suppose that we are interested in the probability, p, of having a visual impairment (yes/no). The result of our observation could be the possible outcomes in table 2.
Table 3. Possible outcomes of a binomial experiment (yes = 1, no = 0) and their probabilities (n = 3)
|
Number of successes |
Probability |
|
0 |
|
|
1 |
|
|
2 |
|
|
3 |
|
The probability of any of these event combinations is easily obtained by considering p, the (individual) probability of success, constant for each subject and independent from other outcomes. Since we are interested in the total number of successes and not in a specific ordered sequence, we can rearrange the table as follows (see table 3) and, in general, express the probability of x successes P(x) as:
![]()
where x is the number of successes and the notation x! denotes the factorial of x, i.e., x! = x×(x–1)×(x–2)…×1.
When we consider the event “being/not being ill”, the individual probability, ![]() refers to the state in which the subject is presumed; in epidemiology, this probability is called “prevalence”. To estimate p, we use the sample proportion:
refers to the state in which the subject is presumed; in epidemiology, this probability is called “prevalence”. To estimate p, we use the sample proportion:
p = x/n
with variance:
![]()
In an hypothetical infinite series of replicated samples of the same size n, we would obtain different sample proportions p = x/n, with probabilities given by the binomial formula. The “true” value of ![]() is estimated by each sample proportion, and a confidence interval for p, that is, the set of likely values for p, given the observed data and a pre-defined level of confidence (say 95%), is estimated from the binomial distribution as the set of values for p which gives a probability of x greater than a pre-specified value (say 2.5%). For a hypothetical experiment in which we observed x = 15 successes in n = 30 trials, the estimated probability of success is:
is estimated by each sample proportion, and a confidence interval for p, that is, the set of likely values for p, given the observed data and a pre-defined level of confidence (say 95%), is estimated from the binomial distribution as the set of values for p which gives a probability of x greater than a pre-specified value (say 2.5%). For a hypothetical experiment in which we observed x = 15 successes in n = 30 trials, the estimated probability of success is:
Table 4. Binomial distribution. Probabilities for different values of ![]() for x = 15 successes in n = 30 trials
for x = 15 successes in n = 30 trials
|
|
Probability |
|
0.200 |
0.0002 |
|
0.300 |
0.0116 |
|
0.334 |
0.025 |
|
0.400 |
0.078 |
|
0.500 |
0.144 |
|
0.600 |
0.078 |
|
0.666 |
0.025 |
|
0.700 |
0.0116 |
The 95% confidence interval for p, obtained from table 4, is 0.334 – 0.666. Each entry of the table shows the probability of x = 15 successes in n = 30 trials computed with the binomial formula; for example, for![]() = 0.30, we obtain from:
= 0.30, we obtain from:
![]()
For n large and p close to 0.5 we can use an approximation based on the Gaussian distribution:
![]()
where za /2 denotes the value of the standard Gaussian distribution for a probability
P (|z| ³ za /2) = a/2;
1 – a being the chosen confidence level. For the example considered,![]() = 15/30 = 0.5; n = 30 and from the standard Gaussian table z0.025 = 1.96. The 95% confidence interval results in the set of values 0.321 – 0.679, obtained by substituting p = 0.5, n = 30, and z0.025 = 1.96 into the above equation for the Gaussian distribution. Note that these values are close to the exact values computed before.
= 15/30 = 0.5; n = 30 and from the standard Gaussian table z0.025 = 1.96. The 95% confidence interval results in the set of values 0.321 – 0.679, obtained by substituting p = 0.5, n = 30, and z0.025 = 1.96 into the above equation for the Gaussian distribution. Note that these values are close to the exact values computed before.
Statistical tests of hypotheses comprise a decision procedure about the value of a population parameter. Suppose, in the previous example, that we want to address the proposition that there is an elevated risk of visual impairment among workers of a given plant. The scientific hypothesis to be tested by our empirical observations then is “there is an elevated risk of visual impairment among workers of a given plant”. Statisticians demonstrate such hypotheses by falsifying the complementary hypothesis “there is no elevation of the risk of visual impairment”. This follows the mathematical demonstration per absurdum and, instead of verifying an assertion, empirical evidence is used only to falsify it. The statistical hypothesis is called the null hypothesis. The second step involves specifying a value for the parameter of that probability distribution used to model the variability in the observations. In our examples, since the phenomenon is binary (i.e., presence/absence of visual impairment), we choose the binomial distribution with parameter p, the probability of visual impairment. The null hypothesis asserts that![]() = 0.25, say. This value is chosen from the collection of knowledge about the topic and a priori knowledge of the usual prevalence of visual impairment in non-exposed (i.e., non-worker) populations. Suppose our data produced an estimate
= 0.25, say. This value is chosen from the collection of knowledge about the topic and a priori knowledge of the usual prevalence of visual impairment in non-exposed (i.e., non-worker) populations. Suppose our data produced an estimate![]() = 0.50, from the 30 workers examined.
= 0.50, from the 30 workers examined.
Can we reject the null hypothesis?
If yes, in favour of what alternative hypothesis?
We specify an alternative hypothesis as a candidate should the evidence dictate that the null hypothesis be rejected. Non-directional (two-sided) alternative hypotheses state that the population parameter is different from the value stated in the null hypothesis; directional (one-sided) alternative hypotheses state that the population parameter is greater (or lesser) than the null value.
Table 5. Binomial distribution. Probabilities of success for ![]() = 0.25 in n = 30 trials
= 0.25 in n = 30 trials
|
X |
Probability |
Cumulative probability |
|
0 |
0.0002 |
0.0002 |
|
1 |
0.0018 |
0.0020 |
|
2 |
0.0086 |
0.0106 |
|
3 |
0.0269 |
0.0374 |
|
4 |
0.0604 |
0.0979 |
|
5 |
0.1047 |
0.2026 |
|
6 |
0.1455 |
0.3481 |
|
7 |
0.1662 |
0.5143 |
|
8 |
0.1593 |
0.6736 |
|
9 |
0.1298 |
0.8034 |
|
10 |
0.0909 |
0.8943 |
|
11 |
0.0551 |
0.9493 |
|
12 |
0.0291 |
0.9784 |
|
13 |
0.0134 |
0.9918 |
|
14 |
0.0054 |
0.9973 |
|
15 |
0.0019 |
0.9992 |
|
16 |
0.0006 |
0.9998 |
|
17 |
0.0002 |
1.0000 |
|
. |
. |
. |
|
30 |
0.0000 |
1.0000 |
Under the null hypothesis, we can calculate the probability distribution of the results of our example. Table 5 shows, for![]() = 0.25 and n = 30, the probabilities (see equation (1)) and the cumulative probabilities:
= 0.25 and n = 30, the probabilities (see equation (1)) and the cumulative probabilities:
![]()
From this table, we obtain the probability of having x ³15 workers with visual impairment
P(x ³15) = 1 – P(x <15) = 1 – 0.9992 = 0.0008
This means that it is highly improbable that we would observe 15 or more workers with visual impairment if they experienced the prevalence of disease of the non-exposed populations. Therefore, we could reject the null hypothesis and affirm that there is a higher prevalence of visual impairment in the population of workers that was studied.
When n×p ³ 5 and n×(1-![]() ) ³ 5, we can use the Gaussian approximation:
) ³ 5, we can use the Gaussian approximation:

From the table of the standard Gaussian distribution we obtain:
P(|z|>2.95) = 0.0008
in close agreement with the exact results. From this approximation we can see that the basic structure of a statistical test of hypothesis consists of the ratio of signal to noise. In our case, the signal is (p–![]() ), the observed deviation from the null hypothesis, while the noise is the standard deviation of P:
), the observed deviation from the null hypothesis, while the noise is the standard deviation of P:
![]()
The greater the ratio, the lesser the probability of the null value![]() .
.
In making decisions about statistical hypotheses, we can incur two kinds of errors: a type I error, rejection of the null hypothesis when it is true; or a type II error, acceptance of the null hypothesis when it is false. The probability level, or p-value, is the probability of a type I error, denoted by the Greek letter a. This is calculated from the probability distribution of the observations under the null hypothesis. It is customary to predefine an a-error level (e.g., 5%, 1%) and reject the null hypothesis when the result of our observation has a probability equal to or less than this so-called critical level.
The probability of a type II error is denoted by the Greek letter β. To calculate it, we need to specify, in the alternative hypothesis, α value for the parameter to be tested (in our example, α value for![]() ). Generic alternative hypotheses (different from, greater than, less than) are not useful. In practice, the β-value for a set of alternative hypotheses is of interest, or its complement, which is called the statistical power of the test. For example, fixing the α-error value at 5%, from table 5, we find:
). Generic alternative hypotheses (different from, greater than, less than) are not useful. In practice, the β-value for a set of alternative hypotheses is of interest, or its complement, which is called the statistical power of the test. For example, fixing the α-error value at 5%, from table 5, we find:
P(x ³12) <0.05
under the null hypothesis![]() = 0.25. If we were to observe at least x = 12 successes, we would reject the null hypothesis. The corresponding β values and the power for x = 12 are given by table 6.
= 0.25. If we were to observe at least x = 12 successes, we would reject the null hypothesis. The corresponding β values and the power for x = 12 are given by table 6.
Table 6. Type II error and power for x = 12, n = 30, α = 0.05
|
|
β |
Power |
|
0.30 |
0.9155 |
0.0845 |
|
0.35 |
0.7802 |
0.2198 |
|
0.40 |
0.5785 |
0.4215 |
|
0.45 |
0.3592 |
0.6408 |
|
0.50 |
0.1808 |
0.8192 |
|
0.55 |
0.0714 |
0.9286 |
In this case our data cannot discriminate whether![]() is greater than the null value of 0.25 but less than 0.50, because the power of the study is too low (<80%) for those values of
is greater than the null value of 0.25 but less than 0.50, because the power of the study is too low (<80%) for those values of![]() <0.50—that is, the sensitivity of our study is 8% for
<0.50—that is, the sensitivity of our study is 8% for![]() = 0.3, 22% for
= 0.3, 22% for![]() = 0.35,…, 64% for
= 0.35,…, 64% for![]() = 0.45.
= 0.45.
The only way to achieve a lower β, or a higher level of power, would be to increase the size of the study. For example, in table 7 we report β and power for n = 40; as expected, we should be able to detect a ![]() value greater than 0.40.
value greater than 0.40.
Table 7. Type II error and power for x = 12, n = 40, α = 0.05
|
|
β |
Power |
|
0.30 |
0.5772 |
0.4228 |
|
0.35 |
0.3143 |
0.6857 |
|
0.40 |
0.1285 |
0.8715 |
|
0.45 |
0.0386 |
0.8614 |
|
0.50 |
0.0083 |
0.9917 |
|
0.55 |
0.0012 |
0.9988 |
Study design is based on careful scrutiny of the set of alternative hypotheses which deserve consideration and guarantee power to the study providing an adequate sample size.
In the epidemiological literature, the relevance of providing reliable risk estimates has been emphasized. Therefore, it is more important to report confidence intervals (either 95% or 90%) than a p-value of a test of a hypothesis. Following the same kind of reasoning, attention should be given to the interpretation of results from small-sized studies: because of low power, even intermediate effects could be undetected and, on the other hand, effects of great magnitude might not be replicated subsequently.
Advanced Methods
The degree of complexity of the statistical methods used in the occupational medicine context has been growing over the last few years. Major developments can be found in the area of statistical modelling. The Nelder and Wedderburn family of non-Gaussian models (Generalized Linear Models) has been one of the most striking contributions to the increase of knowledge in areas such as occupational epidemiology, where the relevant response variables are binary (e.g., survival/death) or counts (e.g., number of industrial accidents).
This was the starting point for an extensive application of regression models as an alternative to the more traditional types of analysis based on contingency tables (simple and stratified analysis). Poisson, Cox and logistic regression are now routinely used for the analysis of longitudinal and case-control studies, respectively. These models are the counterpart of linear regression for categorical response variables and have the elegant feature of providing directly the relevant epidemiological measure of association. For example, the coefficients of Poisson regression are the logarithm of the rate ratios, while those of logistic regression are the log of the odds ratios.
Taking this as a benchmark, further developments in the area of statistical modelling have taken two main directions: models for repeated categorical measures and models which extend the Generalized Linear Models (Generalized Additive Models). In both instances, the aims are focused on increasing the flexibility of the statistical tools in order to cope with more complex problems arising from reality. Repeated measures models are needed in many occupational studies where the units of analysis are at the sub-individual level. For example:
- The study of the effect of working conditions on carpal tunnel syndrome has to consider both hands of a person, which are not independent from one other.
- The analysis of time trends of environmental pollutants and their effect on children’s respiratory systems can be evaluated using extremely flexible models since the exact functional form of the dose-response relationship is difficult to obtain.
A parallel and probably faster development has been seen in the context of Bayesian statistics. The practical barrier of using Bayesian methods collapsed after the introduction of computer-intensive methods. Monte Carlo procedures such as Gibbs sampling schemes have allowed us to avoid the need for numerical integration for computing the posterior distributions which represented the most challenging feature of Bayesian methods. The number of applications of Bayesian models in real and complex problems have found increasing space in applied journals. For example, geographical analyses and ecological correlations at the small area level and AIDS prediction models are more and more often tackled using Bayesian approaches. These developments are welcomed because they represent not only an increase in the number of alternative statistical solutions which could be employed in the analysis of epidemiological data, but also because the Bayesian approach can be considered a more sound strategy.
Impact of Random Measurement Error
Errors in exposure measurement may have different impacts on the exposure-disease relationship being studied, depending on how the errors are distributed. If an epidemiological study has been conducted blindly (i.e., measurements have been taken with no knowledge of the disease or health status of the study participants) we expect that measurement error will be evenly distributed across the strata of disease or health status.
Table 1 provides an example: suppose we recruit a cohort of people exposed at work to a toxicant, in order to investigate a frequent disease. We determine the exposure status only at recruitment (T0), and not at any further points in time during follow-up. However, let us say that a number of individuals do, in fact, change their exposure status in the following year: at time T1, 250 of the original 1,200 exposed people have ceased being exposed, while 150 of the original 750 non-exposed people have started to be exposed to the toxicant. Therefore, at time T1, 1,100 individuals are exposed and 850 are not exposed. As a consequence, we have “misclassification” of exposure, based on our initial measurement of exposure status at time T0. These individuals are then traced after 20 years (at time T2) and the cumulative risk of disease is evaluated. (The assumption being made in the example is that only exposure of more than one year is a concern.)
Table 1. Hypothetical cohort of 1950 individuals (exposed and unexposed at work), recruited at time T0 and whose disease status is ascertained at time T2
|
Time |
|||
|
T0 |
T1 |
T2 |
|
Exposed workers 1200 250 quit exposure 1100 (1200-250+150)
Cases of disease at time T2 = 220 among exposed workers
Non-exposed workers 750 150 start exposure 850 (750-150+250)
Cases of disease at time T2 = 85 among non-exposed workers
The true risk of disease at time T2 is 20% among exposed workers (220/1100),
and 10% in non-exposed workers (85/850) (risk ratio = 2.0).
Estimated risk at T2 of disease among those classified as exposed at T0: 20%
(i.e., true risk in those exposed) ´ 950 (i.e., 1200-250)+ 10%
(i.e., true risk in non-exposed) ´ 250 = (190+25)/1200 = 17.9%
Estimated risk at T2 of disease among those classified as non-exposed at
T0: 20% (i.e., true risk in those exposed) ´ 150 +10%
(i.e., true risk innon-exposed) ´ 600 (i.e., 750-150) = (30+60)/750 = 12%
Estimated risk ratio = 17.9% / 12% = 1.49
Misclassification depends, in this example, on the study design and the characteristics of the population, rather than on technical limitations of the exposure measurement. The effect of misclassification is such that the “true” ratio of 2.0 between the cumulative risk among exposed people and non-exposed people becomes an “observed” ratio of 1.49 (table 1). This underestimation of the risk ratio arises from a “blurring” of the relationship between exposure and disease, which occurs when the misclassification of exposure, as in this case, is evenly distributed according to the disease or health status (i.e., the exposure measurement is not influenced by whether or not the person suffered from the disease that we are studying).
By contrast, either underestimation or overestimation of the association of interest may occur when exposure misclassification is not evenly distributed across the outcome of interest. In the example, we may have bias, and not only a blurring of the aetiologic relationship, if classification of exposure depends on the disease or health status among the workers. This could arise, for example, if we decide to collect biological samples from a group of exposed workers and from a group of unexposed workers, in order to identify early changes related to exposure at work. Samples from the exposed workers might then be analysed in a more accurate way than samples from those unexposed; scientific curiosity might lead the researcher to measure additional biomarkers among the exposed people (including, e.g., DNA adducts in lymphocytes or urinary markers of oxidative damage to DNA), on the assumption that these people are scientifically “more interesting”. This is a rather common attitude which, however, could lead to serious bias.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."