- You are here:
-
Home

- k2 Feed
Infrared Radiation
Infrared radiation is that part of the non-ionizing radiation spectrum located between microwaves and visible light. It is a natural part of the human environment and thus people are exposed to it in small amounts in all areas of daily life—for example, at home or during recreational activities in the sun. Very intense exposure, however, may result from certain technical processes at the workplace.
Many industrial processes involve thermal curing of various kinds of materials. The heat sources used or the heated material itself will usually emit such high levels of infrared radiation that a large number of workers are potentially at risk of being exposed.
Concepts and Quantities
Infrared radiation (IR) has wavelengths ranging from 780 nm to 1 mm. Following the classification by the International Commission on Illumination (CIE), this band is subdivided into IRA (from 780 nm to 1.4 μm), IRB (from 1.4 μm to 3 μm) and IRC (from 3 μm to 1 mm). This subdivision approximately follows the wavelength-dependent absorption characteristics of IR in tissue and the resulting different biological effects.
The amount and the temporal and spatial distribution of infrared radiation are described by different radiometric quantities and units. Due to optical and physiological properties, especially of the eye, a distinction is usually made between small “point” sources and “extended” sources. The criterion for this distinction is the value in radians of the angle (α) measured at the eye that is subtended by the source. This angle can be calculated as a quotient, the light source dimension DL divided by the viewing distance r. Extended sources are those which subtend a viewing angle at the eye greater than αmin, which normally is 11 milliradians. For all extended sources there is a viewing distance where α equals αmin; at greater viewing distances, the source can be treated like a point source. In optical radiation protection the most important quantities concerning extended sources are the radiance (L, expressed in Wm–2sr–1) and the time-integrated radiance (Lp in Jm–2sr–1), which describe the “brightness” of the source. For health risk assessment, the most relevant quantities concerning point sources or exposures at such distances from the source where α< αmin, are the irradiance (E, expressed in Wm–2), which is equivalent to the concept of exposure dose rate, and the radiant exposure (H, in Jm–2), equivalent to the exposure dose concept.
In some bands of the spectrum, the biological effects due to exposure are strongly dependent on wavelength. Therefore, additional spectroradiometric quantities must be used (e.g., the spectral radiance, Ll, expressed in Wm–2 sr–1 nm–1) to weigh the physical emission values of the source against the applicable action spectrum related to the biological effect.
Sources and Occupational Exposure
Exposure to IR results from various natural and artificial sources. The spectral emission from these sources may be limited to a single wavelength (laser) or may be distributed over a broad wavelength band.
The different mechanisms for the generation of optical radiation in general are:
- thermal excitation (black-body radiation)
- gas discharge
- light amplification by stimulated emission of radiation (laser), with the mechanism of gas discharge being of lesser importance in the IR band.
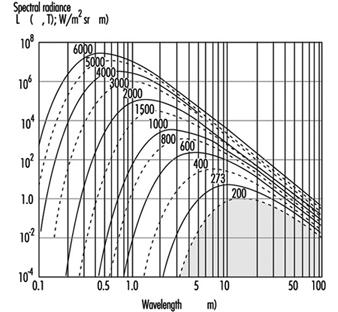
The emission from the most important sources used in many industrial processes results from thermal excitation, and can be approximated using the physical laws of black-body radiation if the absolute temperature of the source is known. The total emission (M, in Wm–2) of a black-body radiator (figure 1) is described by the Stefan-Boltzmann law:
M(T) = 5.67 x 10-8T4
and depends on the 4th power of the temperature (T, in K) of the radiating body. The spectral distribution of the radiance is described by Planck’s radiation law:

and the wavelength of maximum emission (λmax) is described according to Wien’s law by:
λmax = (2.898 x 10-8) / T
Figure 1. Spectral radiance λmaxof a black body radiator at the absolute temperature shown in degrees Kelvin on each curve
Many lasers used in industrial and medical processes will emit very high levels of IR. In general, compared with other radiation sources, laser radiation has some unusual features that may influence the risk following an exposure, such as very short pulse duration or extremely high irradiance. Therefore, laser radiation is discussed in detail elsewhere in this chapter.
Many industrial processes require the use of sources emitting high levels of visible and infrared radiation, and thus a large number of workers like bakers, glass blowers, kiln workers, foundry workers, blacksmiths, smelters and fire-fighters are potentially at risk of exposure. In addition to lamps, such sources as flames, gas torches, acetylene torches, pools of molten metal and incandescent metal bars must be considered. These are encountered in foundries, steel mills and in many other heavy industrial plants. Table 1 summarizes some examples of IR sources and their applications.
Table 1. Different sources of IR, population exposed and approximate exposure levels
|
Source |
Application or exposed population |
Exposure |
|
Sunlight |
Outdoor workers, farmers, construction workers, seafarers, general public |
500 Wm–2 |
|
Tungsten filament lamps |
General population and workers |
105–106 Wm–2sr–1 |
|
Tungsten halogen filament lamps |
(See tungsten filament lamps) |
50–200 Wm–2 (at 50 cm) |
|
Light emitting diodes (e.g. GaAs diode) |
Toys, consumer electronics, data transmission technology, etc. |
105 Wm–2sr–1 |
|
Xenon arc lamps |
Projectors, solar simulators, search lights |
107 Wm–2sr–1 |
|
Iron melt |
Steel furnace, steel mill workers |
105 Wm–2sr–1 |
|
Infrared lamp arrays |
Industrial heating and drying |
103 to 8.103 Wm–2 |
|
Infrared lamps in hospitals |
Incubators |
100–300 Wm–2 |
Biological Effects
Optical radiation in general does not penetrate very deeply into biological tissue. Therefore, the primary targets of an IR exposure are the skin and the eye. Under most exposure conditions the main interaction mechanism of IR is thermal. Only the very short pulses that lasers may produce, but which are not considered here, can also lead to mechanothermal effects. Effects from ionization or from the breakage of chemical bonds are not expected to appear with IR radiation because the particle energy, being less than approximately 1.6 eV, is too low to cause such effects. For the same reason, photochemical reactions become significant only at shorter wavelengths in the visual and in the ultraviolet region. The different wavelength-dependent health effects of IR arise mainly from the wavelength-dependent optical properties of tissue—for example, the spectral absorption of the ocular media (figure 2).
Figure 2. Spectral absorption of the ocular media

Effects on the eye
In general, the eye is well adapted to protect itself against optical radiation from the natural environment. In addition, the eye is physiologically protected against injury from bright light sources, such as the sun or high intensity lamps, by an aversion response that limits the duration of exposure to a fraction of a second (approximately 0.25 seconds).
IRA affects primarily the retina, because of the transparency of the ocular media. When directly viewing a point source or laser beam, the focusing properties in the IRA region additionally render the retina much more susceptible to damage than any other part of the body. For short exposure periods, heating of the iris from the absorption of visible or near IR is considered to play a role in the development of opacities in the lens.
With increasing wavelength, above approximately 1 μm, the absorption by ocular media increases. Therefore, absorption of IRA radiation by both the lens and the pigmented iris is considered to play a role in the formation of lenticular opacities. Damage to the lens is attributed to wavelengths below 3 μm (IRA and IRB). For infrared radiation of wavelengths longer than 1.4 μm, the aqueous humour and the lens are particularly strongly absorbent.
In the IRB and IRC region of the spectrum, the ocular media become opaque as a result of the strong absorption by their constituent water. Absorption in this region is primarily in the cornea and in the aqueous humour. Beyond 1.9 μm, the cornea is effectively the sole absorber. The absorption of long wavelength infrared radiation by the cornea may lead to increased temperatures in the eye due to thermal conduction. Because of a quick turnover rate of the surface corneal cells, any damage limited to the outer corneal layer can be expected to be temporary. In the IRC band the exposure can cause a burn on the cornea similar to that on the skin. Corneal burns are not very likely to occur, however, because of the aversion reaction triggered by the painful sensation caused by strong exposure.
Effects on the skin
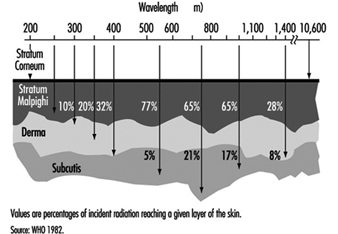
Infrared radiation will not penetrate the skin very deeply. Therefore, exposure of the skin to very strong IR may lead to local thermal effects of different severity, and even serious burns. The effects on the skin depend on the optical properties of the skin, such as wavelength-dependent depth of penetration (figure 3 ). Especially at longer wavelengths, an extensive exposure may cause a high local temperature rise and burns. The threshold values for these effects are time dependent, because of the physical properties of the thermal transport processes in the skin. An irradiation of 10 kWm–2, for example, may cause a painful sensation within 5 seconds, whereas an exposure of 2 kWm–2 will not cause the same reaction within periods shorter than approximately 50 seconds.
Figure 3. Depth of penetration into the skin for different wavelengths
If the exposure is extended over very long periods, even at values well below the pain threshold, the burden of heat to the human body may be great. Especially if the exposure covers the whole body as, for example, in front of a steel melt. The result may be an imbalance of the otherwise physiologically well balanced thermoregulation system. The threshold for tolerating such an exposure will depend on different individual and environmental conditions, such as the individual capacity of the thermoregulation system, the actual body metabolism during exposure or the environmental temperature, humidity and air movement (wind speed). Without any physical work, a maximum exposure of 300 Wm–2 may be tolerated over eight hours under certain environmental conditions, but this value decreases to approximately 140 Wm–2 during heavy physical work.
Exposure Standards
The biological effects of IR exposure which are dependent on wavelength and on the duration of exposure, are intolerable only if certain threshold intensity or dose values are exceeded. To protect against such intolerable exposure conditions, international organizations such as the World Health Organization (WHO), the International Labour Office (ILO), the International Committee for Non-Ionizing Radiation of the International Radiation Protection Association (INIRC/IRPA), and its successor, the International Commission on Non-Ionizing Radiation Protection (ICNIRP) and the American Conference of Governmental Industrial Hygienists (ACGIH) have suggested exposure limits for infrared radiation from both coherent and incoherent optical sources. Most of the national and international suggestions on guidelines for limiting human exposure to infrared radiation are either based on or even identical with the suggested threshold limit values (TLVs) published by the ACGIH (1993/1994). These limits are widely recognized and are frequently used in occupational situations. They are based on current scientific knowledge and are intended to prevent thermal injury of the retina and cornea and to avoid possible delayed effects on the lens of the eye.
The 1994 revision of the ACGIH exposure limits is as follows:
1. For the protection of the retina from thermal injury in case of exposure to visible light, (for example, in the case of powerful light sources), the spectral radiance Lλ in W/(m² sr nm) weighted against the retinal thermal hazard function Rλ (see table 2) over the wavelength interval Δλ and summed over the range of wavelength 400 to 1400 nm, should not exceed:
![]()
where t is the viewing duration limited to intervals from 10-3 to 10 seconds (that is, for accidental viewing conditions, not fixated viewing), and α is the angular subtense of the source in radians calculated by α = maximum extension of the source/distance to the source Rλ (table 2 ).
2. To protect the retina from the exposure hazards of infrared heat lamps or any near IR source where a strong visual stimulus is absent, the infrared radiance over the wavelength range 770 to 1400 nm as viewed by the eye (based on a 7 mm pupil diameter) for extended duration of viewing conditions should be limited to:
![]()
This limit is based on a pupil diameter of 7 mm since, in this case, the aversion response (closing the eye, for example) may not exist due to the absence of visible light.
3. To avoid possible delayed effects on the lens of the eye, such as delayed cataract, and to protect the cornea from overexposure, the infrared radiation at wavelengths greater than 770 nm should be limited to 100 W/m² for periods greater than 1,000 s and to:
![]()
or for shorter periods.
4. For aphakic patients, separate weighting functions and resulting TLVs are given for the wavelength range of ultraviolet and visible light (305–700 nm).
Table 2. Retinal thermal hazard function
|
Wavelength (nm) |
Rλ |
Wavelength (nm) |
Rλ |
|
400 |
1.0 |
460 |
8.0 |
|
405 |
2.0 |
465 |
7.0 |
|
410 |
4.0 |
470 |
6.2 |
|
415 |
8.0 |
475 |
5.5 |
|
420 |
9.0 |
480 |
4.5 |
|
425 |
9.5 |
485 |
4.0 |
|
430 |
9.8 |
490 |
2.2 |
|
435 |
10.0 |
495 |
1.6 |
|
440 |
10.0 |
500–700 |
1.0 |
|
445 |
9.7 |
700–1,050 |
10((700 - λ )/500) |
|
450 |
9.4 |
1,050–1,400 |
0.2 |
|
455 |
9.0 |
Source: ACGIH 1996.
Measurement
Reliable radiometric techniques and instruments are available that make it possible to analyse the risk to the skin and the eye from exposure to sources of optical radiation. For characterizing a conventional light source, it is generally very useful to measure the radiance. For defining hazardous exposure conditions from optical sources, the irradiance and the radiant exposure are of greater importance. The evaluation of broad-band sources is more complex than the evaluation of sources that emit at single wavelengths or very narrow bands, since spectral characteristics and source size must be considered. The spectrum of certain lamps consists of both a continuum emission over a wide wavelength band and emission on certain single wavelengths (lines). Significant errors may be introduced into the representation of those spectra if the fraction of energy in each line is not properly added to the continuum.
For health-hazard assessment the exposure values must be measured over a limiting aperture for which the exposure standards are specified. Typically a 1 mm aperture has been considered to be the smallest practical aperture size. Wavelengths greater than 0.1 mm present difficulties because of significant diffraction effects created by a 1 mm aperture. For this wavelength band an aperture of 1 cm² (11 mm diameter) was accepted, because hot spots in this band are larger than at shorter wavelengths. For the evaluation of retinal hazards, the size of the aperture was determined by an average pupil size and therefore an aperture of 7 mm was chosen.
In general, measurements in the optical region are very complex. Measurements taken by untrained personnel may lead to invalid conclusions. A detailed summary of measurement procedures is to be found in Sliney and Wolbarsht (1980).
Protective Measures
The most effective standard protection from exposure to optical radiation is the total enclosure of the source and all of the radiation pathways that may exit from the source. By such measures, compliance with the exposure limits should be easy to achieve in the majority of cases. Where this is not the case, personal protection is applicable. For example, available eye protection in the form of suitable goggles or visors or protective clothing should be used. If the work conditions will not allow for such measures to be applied, administrative control and restricted access to very intense sources may be necessary. In some cases a reduction of either the power of the source or the working time (work pauses to recover from heat stress), or both, might be a possible measure to protect the worker.
Conclusion
In general, infrared radiation from the most common sources such as lamps, or from most industrial applications, will not cause any risk to workers. At some workplaces, however, IR can cause a health risk for the worker. In addition, there is a rapid increase in the application and use of special-purpose lamps and in high temperature processes in industry, science and medicine. If the exposure from those applications is sufficiently high, detrimental effects (mainly in the eye but also on the skin) cannot be excluded. The importance of internationally recognized optical radiation exposure standards is expected to increase. To protect the worker from excessive exposure, protective measures like shielding (eye shields) or protective clothing should be mandatory.
The principal adverse biological effects attributed to infrared radiation are cataracts, known as glass blower’s or furnaceman’s cataracts. Long-term exposure even at relatively low levels causes heat stress to the human body. At such exposure conditions additional factors such as body temperature and evaporative heat loss as well as environmental factors must be considered.
In order to inform and instruct workers some practical guides were developed in industrial countries. A comprehensive summary can be found in Sliney and Wolbarsht (1980).
Ultraviolet Radiation
Like light, which is visible, ultraviolet radiation (UVR) is a form of optical radiation with shorter wavelengths and more energetic photons (particles of radiation) than its visible counterpart. Most light sources emit some UVR as well. UVR is present in sunlight and is also emitted from a large number of ultraviolet sources used in industry, science and medicine. Workers may encounter UVR in a wide variety of occupational settings. In some instances, at low ambient light levels, very intense near-ultraviolet (“black light”) sources can be seen, but normally UVR is invisible and must be detected by the glow of materials that fluoresce when illuminated by UVR.
Just as light can be divided into colours which can be seen in a rainbow, UVR is subdivided and its components are commonly denoted as UVA, UVB and UVC. Wavelengths of light and UVR are generally expressed in nanometres (nm); 1 nm is one-billionth (10–9) of a metre. UVC (very short-wavelength UVR) in sunlight is absorbed by the atmosphere and does not reach the Earth’s surface. UVC is available only from artificial sources, such as germicidal lamps, which emit most of their energy at a single wavelength (254 nm) that is very effective in killing bacteria and viruses on a surface or in the air.
UVB is the most biologically damaging UVR to the skin and eye, and although most of this energy (which is a component of sunlight) is absorbed by the atmosphere, it still produces sunburn and other biological effects. Long-wavelength UVR, UVA, is normally found in most lamp sources, and is also the most intense UVR reaching the Earth. Although UVA can penetrate deeply into tissue, it is not as biologically damaging as UVB because the energies of individual photons are less than for UVB or UVC.
Sources of Ultraviolet Radiation
Sunlight
The greatest occupational exposure to UVR is experienced by outdoor workers under sunlight. The energy of solar radiation is greatly attenuated by the earth’s ozone layer, limiting terrestrial UVR to wavelengths greater than 290-295 nm. The energy of the more dangerous short-wavelength (UVB) rays in sunlight is a strong function of the atmospheric slant path, and varies with the season and the time of day (Sliney 1986 and 1987; WHO 1994).
Artificial sources
The most significant artificial sources of human exposure include the following:
Industrial arc welding. The most significant source of potential UVR exposure is the radiant energy of arc-welding equipment. The levels of UVR around arc-welding equipment are very high, and acute injury to the eye and the skin can occur within three to ten minutes of exposure at close viewing distances of a few metres. Eye and skin protection is mandatory.
Industrial/workplace UVR lamps. Many industrial and commercial processes, such as photochemical curing of inks, paints and plastics, involve the use of lamps which strongly emit in the UV range. While the likelihood of harmful exposure is low due to shielding, in some cases accidental exposure can occur.
“Black lights”. Black lights are specialized lamps that emit predominantly in the UV range, and are generally used for non-destructive testing with fluorescent powders, for the authentication of banknotes and documents, and for special effects in advertising and discotheques. These lamps do not pose any significant exposure hazard to humans (except in certain cases to photosensitized skin).
Medical treatment. UVR lamps are used in medicine for a variety of diagnostic and therapeutic purposes. UVA sources are normally used in diagnostic applications. Exposures to the patient vary considerably according to the type of treatment, and UV lamps used in dermatology require careful use by staff members.
Germicidal UVR lamps. UVR with wavelengths in the range 250–265 nm is the most effective for sterilization and disinfection since it corresponds to a maximum in the DNA absorption spectrum. Low-pressure mercury discharge tubes are often used as the UV source, as more than 90% of the radiated energy lies at the 254 nm line. These lamps are often referred to as “germicidal lamps,” “bactericidal lamps” or simply “UVC lamps”. Germicidal lamps are used in hospitals to combat tuberculosis infection, and are also used inside microbiological safety cabinets to inactivate airborne and surface microorganisms. Proper installation of the lamps and the use of eye protection is essential.
Cosmetic tanning. Sunbeds are found in enterprises where clients may obtain a tan by special sun-tanning lamps, which emit primarily in the UVA range but also some UVB. Regular use of a sunbed may contribute significantly to a person’s annual UV skin exposure; furthermore, the staff working in tanning salons may also be exposed to low levels. The use of eye protection such as goggles or sunglasses should be mandatory for the client, and depending upon the arrangement, even staff members may require eye protectors.
General lighting. Fluorescent lamps are common in the workplace and have been used in the home for a long time now. These lamps emit small amounts of UVR and contribute only a few percent to a person’s annual UV exposure. Tungsten-halogen lamps are increasingly used in the home and in the workplace for a variety of lighting and display purposes. Unshielded halogen lamps can emit UVR levels sufficient to cause acute injury at short distances. The fitting of glass filters over these lamps should eliminate this hazard.
Biological Effects
The skin
Erythema
Erythema, or “sunburn”, is a reddening of the skin that normally appears in four to eight hours after exposure to UVR and gradually fades after a few days. Severe sunburn can involve blistering and peeling of the skin. UVB and UVC are both about 1,000 times more effective in causing erythema than UVA (Parrish, Jaenicke and Anderson 1982), but erythema produced by the longer UVB wavelengths (295 to 315 nm) is more severe and persists longer (Hausser 1928). The increased severity and time-course of the erythema results from deeper penetration of these wavelengths into the epidermis. Maximum sensitivity of the skin apparently occurs at approximately 295 nm (Luckiesh, Holladay and Taylor 1930; Coblentz, Stair and Hogue 1931) with much less (approximately 0.07) sensitivity occurring at 315 nm and longer wavelengths (McKinlay and Diffey 1987).
The minimal erythemal dose (MED) for 295 nm that has been reported in more recent studies for untanned, lightly pigmented skin ranges from 6 to 30 mJ/cm2 (Everett, Olsen and Sayer 1965; Freeman, et al. 1966; Berger, Urbach and Davies 1968). The MED at 254 nm varies greatly depending upon the elapsed time after exposure and whether the skin has been exposed much to outdoor sunlight, but is generally of the order of 20 mJ/cm2, or as high as 0.1 J/cm2. Skin pigmentation and tanning, and, most importantly, thickening of the stratum corneum, can increase this MED by at least one order of magnitude.
Photosensitization
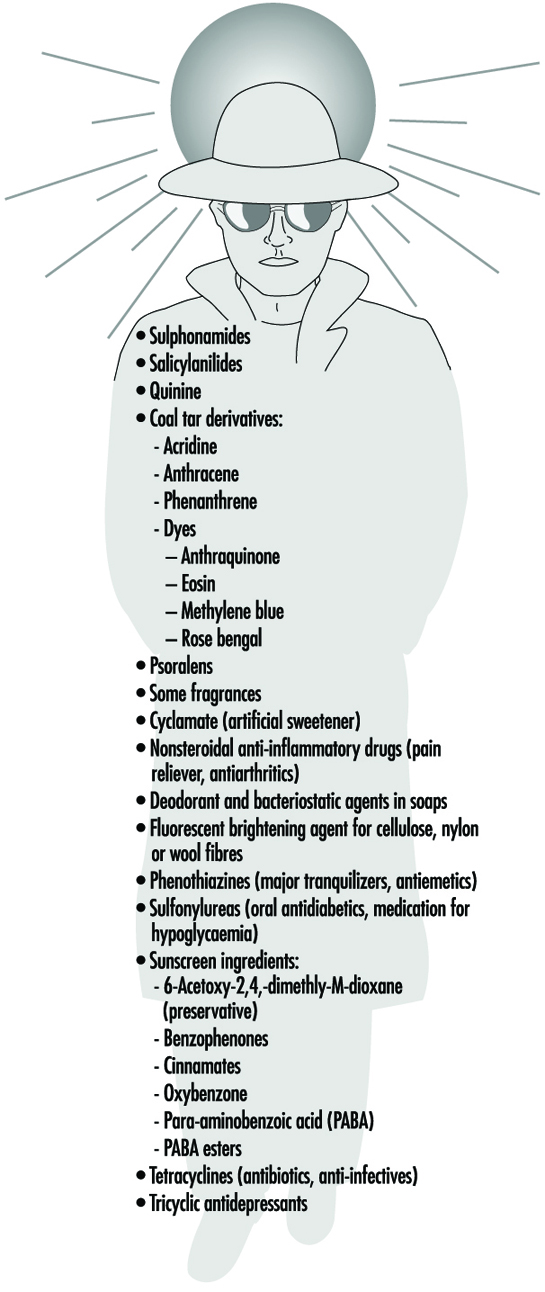
Occupational health specialists frequently encounter adverse effects from occupational exposure to UVR in photosensitized workers. The use of certain medicines may produce a photosensitizing effect on exposure to UVA, as may the topical application of certain products, including some perfumes, body lotions and so on. Reactions to photosensitizing agents involve both photoallergy (allergic reaction of the skin) and phototoxicity (irritation of the skin) after UVR exposure from sunlight or industrial UVR sources. (Photosensitivity reactions during the use of tanning equipment are also common.) This photosensitization of the skin may be caused by creams or ointments applied to the skin, by medications taken orally or by injection, or by the use of prescription inhalers (see figure 1 ). The physician prescribing a potentially photosensitizing medication should always warn the patient to take appropriate measures to ensure against adverse effects, but the patient frequently is told only to avoid sunlight and not UVR sources (since these are uncommon for the general population).
Figure 1. Some phonosensitizing substances
Delayed effects
Chronic exposure to sunlight—especially the UVB component—accelerates the ageing of the skin and increases the risk of developing skin cancer (Fitzpatrick et al. 1974; Forbes and Davies 1982; Urbach 1969; Passchier and Bosnjakovic 1987). Several epidemiological studies have shown that the incidence of skin cancer is strongly correlated with latitude, altitude and sky cover, which correlate with UVR exposure (Scotto, Fears and Gori 1980; WHO 1993).
Exact quantitative dose-response relationships for human skin carcinogenesis have not yet been established, although fair-skinned individuals, particularly those of Celtic origin, are much more prone to develop skin cancer. Nevertheless, it must be noted that the UVR exposures necessary to elicit skin tumours in animal models may be delivered sufficiently slowly that erythema is not produced, and the relative effectiveness (relative to the peak at 302 nm) reported in those studies varies in the same way as sunburn (Cole, Forbes and Davies 1986; Sterenborg and van der Leun 1987).
The eye
Photokeratitis and photoconjunctivitis
These are acute inflammatory reactions resulting from exposure to UVB and UVC radiation which appear within a few hours of excessive exposure and normally resolved after one to two days.
Retinal injury from bright light
Although thermal injury to the retina from light sources is unlikely, photochemical damage can occur from exposure to sources rich in blue light. This can result in temporary or permanent reduction in vision. However the normal aversion response to bright light should prevent this occurrence unless a conscious effort is made to stare at bright light sources. The contribution of UVR to retinal injury is generally very small because absorption by the lens limits retinal exposure.
Chronic effects
Long-term occupational exposure to UVR over several decades may contribute to cataract and such non-eye-related degenerative effects as skin ageing and skin cancer associated with sun exposure. Chronic exposure to infrared radiation also can increase the risk of cataract, but this is very unlikely, given access to eye protection.
Actinic ultraviolet radiation (UVB and UVC) is strongly absorbed by the cornea and conjunctiva. Overexposure of these tissues causes keratoconjunctivitis, commonly referred to as “welder’s flash”, “arc-eye” or “snow-blindness”. Pitts has reported the action spectrum and time course of photokeratitis in the human, rabbit and monkey cornea (Pitts 1974). The latent period varies inversely with the severity of exposure, ranging from 1.5 to 24 hours, but usually occurs within 6 to 12 hours; discomfort usually disappears within 48 hours. Conjunctivitis follows and may be accompanied by erythema of the facial skin surrounding the eyelids. Of course, UVR exposure rarely results in permanent ocular injury. Pitts and Tredici (1971) reported threshold data for photokeratitis in humans for wavebands 10 nm in width from 220 to 310 nm. The maximum sensitivity of the cornea was found to occur at 270 nm—differing markedly from the maximum for the skin. Presumably, 270 nm radiation is biologically more active because of the lack of a stratum corneum to attenuate the dose to the corneal epithelium tissue at shorter UVR wavelengths. The wavelength response, or action spectrum, did not vary as greatly as did the erythema action spectra, with thresholds varying from 4 to 14 mJ/cm2 at 270 nm. The threshold reported at 308 nm was approximately 100 mJ/cm2.
Repeated exposure of the eye to potentially hazardous levels of UVR does not increase the protective capability of the affected tissue (the cornea) as does skin exposure, which leads to tanning and to thickening of the stratum corneum. Ringvold and associates studied the UVR absorption properties of the cornea (Ringvold 1980a) and aqueous humour (Ringvold 1980b), as well as the effects of UVB radiation upon the corneal epithelium (Ringvold 1983), the corneal stroma (Ringvold and Davanger 1985) and the corneal endothelium (Ringvold, Davanger and Olsen 1982; Olsen and Ringvold 1982). Their electron microscopic studies showed that corneal tissue possessed remarkable repair and recovery properties. Although one could readily detect significant damage to all of these layers apparently appearing initially in cell membranes, morphological recovery was complete after a week. Destruction of keratocytes in the stromal layer was apparent, and endothelial recovery was pronounced despite the normal lack of rapid cell turnover in the endothelium. Cullen et al. (1984) studied endothelial damage that was persistent if the UVR exposure was persistent. Riley et al. (1987) also studied the corneal endothelium following UVB exposure and concluded that severe, single insults were not likely to have delayed effects; however, they also concluded that chronic exposure could accelerate changes in the endothelium related to ageing of the cornea.
Wavelengths above 295 nm can be transmitted through the cornea and are almost totally absorbed by the lens. Pitts, Cullen and Hacker (1977b) showed that cataracts can be produced in rabbits by wavelengths in the 295–320 nm band. Thresholds for transient opacities ranged from 0.15 to 12.6 J/cm2, depending on wavelength, with a minimum threshold at 300 nm. Permanent opacities required greater radiant exposures. No lenticular effects were noted in the wavelength range of 325 to 395 nm even with much higher radiant exposures of 28 to 162 J/cm2 (Pitts, Cullen and Hacker 1977a; Zuclich and Connolly 1976). These studies clearly illustrate the particular hazard of the 300-315 nm spectral band, as would be expected because photons of these wavelengths penetrate efficiently and have sufficient energy to produce photochemical damage.
Taylor et al. (1988) provided epidemiological evidence that UVB in sunlight was an aetiological factor in senile cataract, but showed no correlation of cataract with UVA exposure. Although once a popular belief because of the strong absorption of UVA by the lens, the hypothesis that UVA can cause cataract has not been supported by either experimental laboratory studies or by epidemiological studies. From the laboratory experimental data which showed that thresholds for photokeratitis were lower than for cataractogenesis, one must conclude that levels lower than those required to produce photokeratitis on a daily basis should be considered hazardous to lens tissue. Even if one were to assume that the cornea is exposed to a level nearly equivalent to the threshold for photokeratitis, one would estimate that the daily UVR dose to the lens at 308 nm would be less than 120 mJ/cm2 for 12 hours out of doors (Sliney 1987). Indeed, a more realistic average daily exposure would be less than half that value.
Ham et al. (1982) determined the action spectrum for photoretinitis produced by UVR in the 320–400 nm band. They showed that thresholds in the visible spectral band, which were 20 to 30 J/cm2 at 440 nm, were reduced to approximately 5 J/cm2 for a 10 nm band centred at 325 nm. The action spectrum was increasing monotonically with decreasing wavelength. We should therefore conclude that levels well below 5 J/cm2 at 308 nm should produce retinal lesions, although these lesions would not become apparent for 24 to 48 hours after the exposure. There are no published data for retinal injury thresholds below 325 nm, and one can only expect that the pattern for the action spectrum for photochemical injury to the cornea and lens tissues would apply to the retina as well, leading to an injury threshold of the order of 0.1 J/cm2.
Although UVB radiation has been clearly shown to be mutagenic and carcinogenic to the skin, the extreme rarity of carcinogenesis in the cornea and conjunctiva is quite remarkable. There appears to be no scientific evidence to link UVR exposure with any cancers of the cornea or conjunctiva in humans, although the same is not true of cattle. This would suggest a very effective immune system operating in the human eye, since there are certainly outdoor workers who receive a UVR exposure comparable to that which cattle receive. This conclusion is further supported by the fact that individuals suffering from a defective immune response, as in xeroderma pigmentosum, frequently develop neoplasias of the cornea and conjunctiva (Stenson 1982).
Safety Standards
Occupational exposure limits (EL) for UVR have been developed and include an action spectrum curve which envelops the threshold data for acute effects obtained from studies of minimal erythema and keratoconjunctivitis (Sliney 1972; IRPA 1989). This curve does not differ significantly from the collective threshold data, considering measurement errors and variations in individual response, and is well below the UVB cataractogenic thresholds.
The EL for UVR is lowest at 270 nm (0.003 J/cm2 at 270 nm), and, for example, at 308 nm is 0.12 J/cm2 (ACGIH 1995, IRPA 1988). Regardless of whether the exposure occurs from a few pulsed exposures during the day, a single very brief exposure, or from an 8-hour exposure at a few microwatts per square centimetre, the biological hazard is the same, and the above limits apply to the full workday.
Occupational Protection
Occupational exposure to UVR should be minimized where practical. For artificial sources, wherever possible, priority should be given to engineering measures such as filtration, shielding and enclosure. Administrative controls, such as limitation of access, can reduce the requirements for personal protection.
Outdoor workers such as agricultural workers, labourers, construction workers, fishermen and so on can minimize their risk from solar UV exposure by wearing appropriate tightly woven clothing, and most important, a brimmed hat to reduce face and neck exposure. Sunscreens can be applied to exposed skin to reduce further exposure. Outdoor workers should have access to shade and be provided with all the necessary protective measures mentioned above.
In industry, there are many sources capable of causing acute eye injury within a short exposure time. A variety of eye protection is available with various degrees of protection appropriate to the intended use. Those intended for industrial use include welding helmets (additionally providing protection both from intense visible and infrared radiation as well as face protection), face shields, goggles and UV-absorbing spectacles. In general, protective eyewear provided for industrial use should fit snugly on the face, thus ensuring that there are no gaps through which UVR can directly reach the eye, and they should be well-constructed to prevent physical injury.
The appropriateness and selection of protective eyewear is dependent on the following points:
- the intensity and spectral emission characteristics of the UVR source
- the behavioural patterns of people near UVR sources (distance and exposure time are important)
- the transmission properties of the protective eyewear material
- the design of the frame of the eyewear to prevent peripheral exposure of the eye from direct unabsorbed UVR.
In industrial exposure situations, the degree of ocular hazard can be assessed by measurement and comparison with recommended limits for exposure (Duchene, Lakey and Repacholi 1991).
Measurement
Because of the strong dependence of biological effects on wavelength, the principal measurement of any UVR source is its spectral power or spectral irradiance distribution. This must be measured with a spectroradiometer which consists of suitable input optics, a monochromator and a UVR detector and readout. Such an instrument is not normally used in occupational hygiene.
In many practical situations, a broad-band UVR meter is used to determine safe exposure durations. For safety purposes, the spectral response can be tailored to follow the spectral function used for the exposure guidelines of the ACGIH and the IRPA. If appropriate instruments are not used, serious errors of hazard assessment will result. Personal UVR dosimeters are also available (e.g., polysulphone film), but their application has been largely confined to occupational safety research rather than in hazard evaluation surveys.
Conclusions
Molecular damage of key cellular components arising from UVR exposure occurs constantly, and repair mechanisms exist to deal with the exposure of skin and ocular tissues to ultraviolet radiation. Only when these repair mechanisms are overwhelmed does acute biological injury become apparent (Smith 1988). For these reasons, minimizing occupational UVR exposure continues to remain an important object of concern among occupational health and safety workers.
The Electromagnetic Spectrum: Basic Physical Characteristics
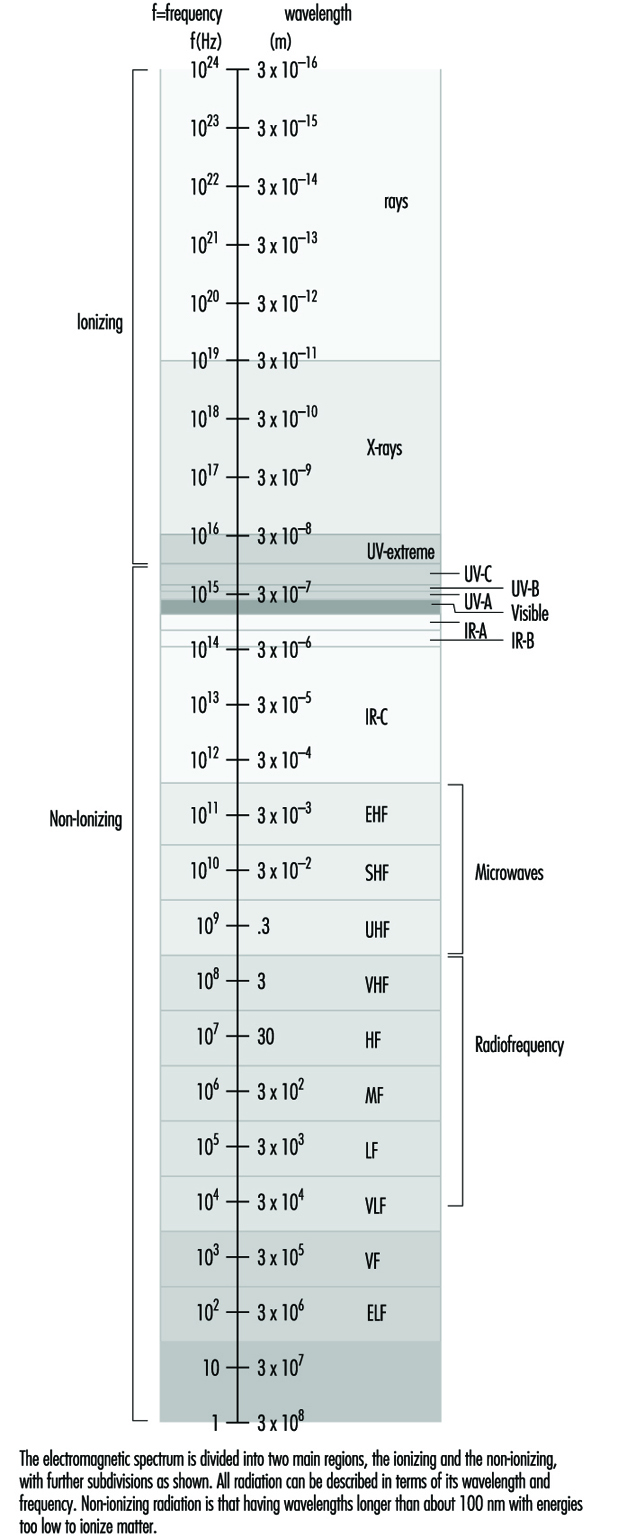
The most familiar form of electromagnetic energy is sunlight. The frequency of sunlight (visible light) is the dividing line between the more potent, ionizing radiation (x rays, cosmic rays) at higher frequencies and the more benign, non-ionizing radiation at lower frequencies. There is a spectrum of non-ionizing radiation. Within the context of this chapter, at the high end just below visible light is infrared radiation. Below that is the broad range of radio frequencies, which includes (in descending order) microwaves, cellular radio, television, FM radio and AM radio, short waves used in dielectric and induction heaters and, at the low end, fields with power frequency. The electromagnetic spectrum is illustrated in figure 1.
Figure 1. The electromagnetic spectrum
Just as visible light or sound permeates our environment, the space where we live and work, so do the energies of electromagnetic fields. Also, just as most of the sound energy we are exposed to is created by human activity, so too are the electromagnetic energies: from the weak levels emitted from our everyday electrical appliances—those that make our radio and TV sets work—to the high levels that medical practitioners apply for beneficial purposes—for example, diathermy (heat treatments). In general, the strength of such energies decreases rapidly with distance from the source. Natural levels of these fields in the environment are low.
Non-ionizing radiation (NIR) incorporates all radiation and fields of the electromagnetic spectrum that do not have enough energy to produce ionization of matter. That is, NIR is incapable of imparting enough energy to a molecule or atom to disrupt its structure by removing one or more electrons. The borderline between NIR and ionizing radiation is usually set at a wavelength of approximately 100 nanometres.
As with any form of energy, NIR energy has the potential to interact with biological systems, and the outcome may be of no significance, may be harmful in different degrees, or may be beneficial. With radiofrequency (RF) and microwave radiation, the main interaction mechanism is heating, but in the low-frequency part of the spectrum, fields of high intensity may induce currents in the body and thereby be hazardous. The interaction mechanisms for low-level field strengths are, however, unknown.
Quantities and Units
Fields at frequencies below about 300 MHz are quantified in terms of electric field strength (E) and magnetic field strength (H). E is expressed in volts per metre (V/m) and H in amperes per metre (A/m). Both are vector fields—that is, they are characterized by magnitude and direction at each point. For the low-frequency range the magnetic field is often expressed in terms of the flux density, B, with the SI unit tesla (T). When the fields in our daily environment are discussed, the subunit microtesla (μT) is usually the preferred unit. In some literature the flux density is expressed in gauss (G), and the conversion between these units is (for fields in air):
1 T = 104 G or 0.1 μT = 1 mG and 1 A/m = 1.26 μT.
Reviews of concepts, quantities, units and terminology for non-ionizing radiation protection, including radiofrequency radiation, are available (NCRP 1981; Polk and Postow 1986; WHO 1993).
The term radiation simply means energy transmitted by waves. Electromagnetic waves are waves of electric and magnetic forces, where a wave motion is defined as propagation of disturbances in a physical system. A change in the electric field is accompanied by a change in the magnetic field, and vice versa. These phenomena were described in 1865 by J.C. Maxwell in four equations which have come to be known as Maxwell’s Equations.
Electromagnetic waves are characterized by a set of parameters that include frequency (f), wavelength (λ), electric field strength, magnetic field strength, electric polarization (P) (the direction of the E field), velocity of propagation (c) and Poynting vector (S). Figure 2 illustrates the propagation of an electromagnetic wave in free space. The frequency is defined as the number of complete changes of the electric or magnetic field at a given point per second, and is expressed in hertz (Hz). The wavelength is the distance between two consecutive crests or troughs of the wave (maxima or minima). The frequency, wavelength and wave velocity (v) are interrelated as follows:
v = f λ
Figure 2. A plane wave propagating with the speed of light in the x-direction
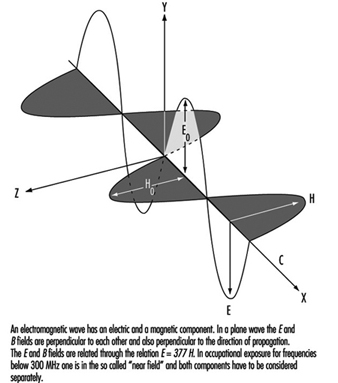
The velocity of an electromagnetic wave in free space is equal to the velocity of light, but the velocity in materials depends on the electrical properties of the material—that is, on its permittivity (ε) and permeability (μ). The permittivity concerns the material interactions with the electric field, and the permeability expresses the interactions with the magnetic field. Biological substances have permittivities that differ vastly from that of free space, being dependant on wavelength (especially in the RF range) and tissue type. The permeability of biological substances, however, is equal to that of free space.
In a plane wave, as illustrated in figure 2 , the electric field is perpendicular to the magnetic field and the direction of propagation is perpendicular to both the electric and the magnetic fields.
For a plane wave, the ratio of the value of the electric field strength to the value of the magnetic field strength, which is constant, is known as the characteristic impedance (Z):
Z = E/H
In free space, Z= 120π ≈ 377Ω but otherwise Z depends on the permittivity and permeability of the material the wave is travelling through.
Energy transfer is described by the Poynting vector, which represents the magnitude and direction of the electromagnetic flux density:
S = E x H
For a propagating wave, the integral of S over any surface represents the instantaneous power transmitted through this surface (power density). The magnitude of the Poynting vector is expressed in watts per square metre (W/m2) (in some literature the unit mW/cm2 is used—the conversion to SI units is 1 mW/cm2 = 10 W/m2) and for plane waves is related to the values of the electric and magnetic field strengths:
S = E2 / 120π = E2 / 377
and
S =120π H2 = 377 H2
Not all exposure conditions encountered in practice can be represented by plane waves. At distances close to sources of radio-frequency radiation the relationships characteristic of plane waves are not satisfied. The electromagnetic field radiated by an antenna can be divided into two regions: the near-field zone and the far-field zone. The boundary between these zones is usually put at:
r = 2a2 / λ
where a is the greatest dimension of the antenna.
In the near-field zone, exposure has to be characterized by both the electric and the magnetic fields. In the far-field one of these suffices, as they are interrelated by the above equations involving E and H. In practice, the near-field situation is often realized at frequencies below 300 Mhz.
Exposure to RF fields is further complicated by interactions of electromagnetic waves with objects. In general, when electromagnetic waves encounter an object some of the incident energy is reflected, some is absorbed and some is transmitted. The proportions of energy transmitted, absorbed or reflected by the object depend on the frequency and polarization of the field and the electrical properties and shape of the object. A superimposition of the incident and reflected waves results in standing waves and spatially non-uniform field distribution. Since waves are totally reflected from metallic objects, standing waves form close to such objects.
Since the interaction of RF fields with biological systems depends on many different field characteristics and the fields encountered in practice are complex, the following factors should be considered in describing exposures to RF fields:
- whether exposure occurs in the near- or far-field zone
- if near-field, then values for both E and H are needed; if far-field, then either E or H
- spatial variation of the magnitude of the field(s)
- field polarization, that is, the direction of the electric field with respect to the direction of wave propagation.
For exposure to low-frequency magnetic fields it is still not clear whether the field strength or flux density is the only important consideration. It may turn out that other factors are also important, such as the exposure time or the rapidity of the field changes.
The term electromagnetic field (EMF), as it is used in the news media and popular press, usually refers to electric and magnetic fields at the low-frequency end of the spectrum, but it can also be used in a much broader sense to include the whole spectrum of electromagnetic radiation. Note that in the low-frequency range the E and B fields are not coupled or interrelated in the same way that they are at higher frequencies, and it is therefore more accurate to refer to them as “electric and magnetic fields” rather than EMFs.
Electric and Magnetic Fields and Health Outcomes
In recent years interest has increased in the biological effects and possible health outcomes of weak electric and magnetic fields. Studies have been presented on magnetic fields and cancer, on reproduction and on neurobehavioural reactions. In what follows, a summary is given of what we know, what still needs to be investigated and, particularly, what policy is appropriate—whether it should involve no restrictions of exposure at all, “prudent avoidance” or expensive interventions.
What we Know
Cancer
Epidemiological studies on childhood leukaemia and residential exposure from power lines seem to indicate a slight risk increase, and excess leukaemia and brain tumour risks have been reported in “electrical” occupations. Recent studies with improved techniques for exposure assessment have generally strengthened the evidence of an association. There is, however, still a lack of clarity as to exposure characteristics—for example, magnetic field frequency and exposure intermittence; and not much is known about possible confounding or effect-modifying factors. Furthermore, most of the occupational studies have indicated one special form of leukaemia, acute myeloid leukaemia, while others have found higher incidences for another form, chronic lymphatic leukaemia. The few animal cancer studies reported have not given much help with risk assessment, and in spite of a large number of experimental cell studies, no plausible and understandable mechanism has been presented by which a carcinogenic effect could be explained.
Reproduction, with special reference to pregnancy outcomes
In epidemiological studies, adverse pregnancy outcomes and childhood cancer have been reported after maternal as well as paternal exposure to magnetic fields, the paternal exposure indicating a genotoxic effect. Efforts to replicate positive results by other research teams have not been successful. Epidemiological studies on visual display unit (VDU) operators, who are exposed to the electric and magnetic fields emitted by their screens, have been mainly negative, and animal teratogenic studies with VDU-like fields have been too contradictory to support trustworthy conclusions.
Neurobehavioural reactions
Provocation studies on young volunteers seem to indicate such physiological changes as slowing of heart rate and electroencephalogram (EEG) changes after exposure to relatively weak electric and magnetic fields. The recent phenomenon of hypersensitivity to electricity seems to be multifactorial in origin, and it is not clear whether the fields are involved or not. A great variety of symptoms and discomforts has been reported, mainly of the skin and the nervous system. Most of the patients have diffuse skin complaints in the face, such as flush, rosiness, ruddiness, heat, warmth, pricking sensations, ache and tightness. Symptoms associated with the nervous system are also described, such as headache, dizziness, fatigue and faintness, tingling and pricking sensations in the extremities, shortness of breath, heart palpitations, profuse sweatings, depressions and memory difficulties. No characteristic organic neurological disease symptoms have been presented.
Exposure
Exposure to fields occurs throughout society: in the home, at work, in schools and by the operation of electrically powered means of transport. Wherever there are electric wires, electric motors and electronic equipment, electric and magnetic fields are created. Average workday field strengths of 0.2 to 0.4 μT (microtesla) appear to be the level above which there could be an increased risk, and similar levels have been calculated for annual averages for subjects living under or near power lines.
Many people are similarly exposed above these levels, though for shorter periods, in their homes (via electric radiators, shavers, hair-dryers and other household appliances, or stray currents due to imbalances in the electrical grounding system in a building), at work (in certain industries and offices involving proximity to electric and electronic equipment) or while travelling in trains and other electrically driven conveyances. The importance of such intermittent exposure is not known. There are other uncertainties as to exposure (involving questions relating to the importance of field frequency, to other modifying or confounding factors, or to knowledge of the total exposure day and night) and effect (given the consistency in findings as to type of cancer), and in the epidemiological studies, which make it necessary to evaluate all risk assessments with great caution.
Risk assessments
In Scandinavian residential studies, results indicate a doubled leukaemia risk above 0.2 μT, the exposure levels corresponding to those typically encountered within 50 to 100 metres of an overhead power line. The number of childhood leukaemia cases under power lines are few, however, and the risk is therefore low compared to other environmental hazards in society. It has been calculated that each year in Sweden there are two cases of childhood leukaemia under or near power lines. One of these cases may be attributable to the magnetic field risk, if any.
Occupational exposures to magnetic fields are generally higher than residential exposures, and calculations of leukaemia and brain tumour risks for exposed workers give higher values than for children living close to power lines. From calculations based on the attributable risk discovered in a Swedish study, approximately 20 cases of leukaemia and 20 cases of brain tumours could be attributed to magnetic fields each year. These figures are to be compared with the total number of 40,000 annual cancer cases in Sweden, of which 800 have been calculated to have an occupational origin.
What Still Needs to be Investigated
It is quite clear that more research is needed in order to secure a satisfactory understanding of the epidemiological study results obtained so far. There are additional epidemiological studies in progress in different countries around the world, but the question is whether these will add more to the knowledge we already have. As a matter of fact it is not known which characteristics of the fields are causal to the effects, if any. Thus, we definitely need more studies on possible mechanisms to explain the findings we have assembled.
There are in the literature, however, a vast number of in vitro studies devoted to the search for possible mechanisms. Several cancer promotion models have been presented, based on changes in the cell surface and in the cell membrane transport of calcium ions, disruption of cell communication, modulation of cell growth, activation of specific gene sequences by modulated ribonucleic acid (RNA) transcription, depression of pineal melatonin production, modulation of ornithine decarboxylase activity and possible disruption of hormonal and immune-system anti-tumour control mechanisms. Each of these mechanisms has features applicable to explaining reported magnetic field cancer effects; however, none has been free of problems and essential objections.
Melatonin and magnetite
There are two possible mechanisms that may be relevant to cancer promotion and thus deserve special attention. One of these has to do with the reduction of nocturnal melatonin levels induced by magnetic fields and the other is related to the discovery of magnetite crystals in human tissues.
It is known from animal studies that melatonin, via an effect on circulating sex hormone levels, has an indirect oncostatic effect. It has also been indicated in animal studies that magnetic fields suppress pineal melatonin production, a finding that suggests a theoretical mechanism for the reported increase in (for example) breast cancer that may be due to exposure to such fields. Recently, an alternative explanation for the increased cancer risk has been proposed. Melatonin has been found to be a most potent hydroxyl radical scavenger, and consequently the damage to DNA that might be done by free radicals is markedly inhibited by melatonin. If melatonin levels are suppressed, for example by magnetic fields, the DNA is left more vulnerable to oxidative attack. This theory explains how the depression of melatonin by magnetic fields could result in a higher incidence of cancer in any tissue.
But do human melatonin blood levels diminish when individuals are exposed to weak magnetic fields? There exist some indications that this may be so, but further research is needed. For some years it has been known that the ability of birds to orient themselves during seasonal migrations is mediated via magnetite crystals in cells that respond to the earth’s magnetic field. Now, as mentioned above, magnetite crystals have also been demonstrated to exist in human cells in a concentration high enough theoretically to respond to weak magnetic fields. Thus the role of magnetite crystals should be considered in any discussions on the possible mechanisms that may be proposed as to the potentially harmful effects of electric and magnetic fields.
The need for knowledge on mechanisms
To summarize, there is a clear need for more studies on such possible mechanisms. Epidemiologists need information as to which characteristics of the electric and magnetic fields they should focus upon in their exposure assessments. In most epidemiological studies, mean or median field strengths (with frequencies of 50 to 60 Hz) have been used; in others, cumulative measures of exposure were studied. In a recent study, fields of higher frequencies were found to be related to risk. In some animal studies, finally, field transients have been found to be important. For epidemiologists the problem is not on the effect side; registers on diseases exist in many countries today. The problem is that epidemiologists do not know the relevant exposure characteristics to consider in their studies.
What Policy is Appropriate
Systems of protection
Generally, there are different systems of protection to be considered with respect to regulations, guidelines and policies. Most often the health-based system is selected, in which a specific adverse health effect can be identified at a certain exposure level, irrespective of exposure type, chemical or physical. A second system could be characterized as an optimization of a known and accepted hazard, which has no threshold below which the risk is absent. An example of an exposure falling within this kind of system is ionizing radiation. A third system covers hazards or risks where causal relationships between exposure and outcome have not been shown with reasonable certainty, but for which there are general concerns about possible risks. This lattermost system of protection has been denoted the principle of caution, or more recently prudent avoidance, which can be summarized as the future low-cost avoidance of unnecessary exposure in the absence of scientific certainty. Exposure to electric and magnetic fields has been discussed in this way, and systematic strategies have been presented, for instance, on how future power lines should be routed, workplaces arranged and household appliances designed in order to minimize exposure.
It is apparent that the system of optimization is not applicable in connection with restrictions of electric and magnetic fields, simply because they are not known and accepted as risks. The other two systems, however, are both presently under consideration.
Regulations and guidelines for restriction of exposure under the health-based system
In international guidelines limits for restrictions of field exposure are several orders of magnitude above what can be measured from overhead power lines and found in electrical occupations. The International Radiation Protection Association (IRPA) issued Guidelines on limits of exposure to 50/60 Hz electric and magnetic fields in 1990, which has been adopted as a basis for many national standards. Since important new studies were published thereafter, an addendum was issued in 1993 by the International Commission on Non-Ionizing Radiation Protection (ICNIRP). Furthermore, in 1993 risk assessments in agreement with that of IRPA were also made in the United Kingdom.
These documents emphasize that the state of scientific knowledge today does not warrant limiting exposure levels for the public and the workforce down to the μT level, and that further data are required to confirm whether or not health hazards are present. The IRPA and ICNIRP guidelines are based on the effects of field-induced currents in the body, corresponding to those normally found in the body (up to about 10 mA/m2). Occupational exposure to magnetic fields of 50/60 Hz is recommended to be limited to 0.5 mT for all-day exposure and 5 mT for short exposures of up to two hours. It is recommended that exposure to electric fields be limited to 10 and 30 kV/m. The 24-hour limit for the public is set at 5 kV/m and 0.1 mT.
These discussions on the regulation of exposure are based entirely on cancer reports. In studies of other possible health effects related to electric and magnetic fields (for example, reproductive and neurobehavioural disorders), results are generally considered insufficiently clear and consistent to constitute a scientific basis for restricting exposure.
The principle of caution or prudent avoidance
There is no real difference between the two concepts; prudent avoidance has been used more specifically, though, in discussions of electric and magnetic fields. As said above, prudent avoidance can be summarized as the future, low-cost avoidance of unnecessary exposure as long as there is scientific uncertainty about the health effects. It has been adopted in Sweden, but not in other countries.
In Sweden, five government authorities (the Swedish Radiation Protection Institute; the National Electricity Safety Board; the National Board of Health and Welfare; the National Board of Occupational Safety and Health; and the National Board of Housing, Building and Planning) jointly have stated that “the total knowledge now accumulating justifies taking steps to reduce field power”. Provided the cost is reasonable, the policy is to protect people from high magnetic exposures of long duration. During the installation of new equipment or new power lines that may cause high magnetic field exposures, solutions giving lower exposures should be chosen provided these solutions do not imply large inconveniences or costs. Generally, as stated by the Radiation Protection Institute, steps can be taken to reduce the magnetic field in cases where the exposure levels exceed the normally occurring levels by more than a factor of ten, provided such reductions can be done at a reasonable cost. In situations where the exposure levels from existing installations do not exceed the normally occurring levels by a factor of ten, costly rebuilding should be avoided. Needless to say, the present avoidance concept has been criticized by many experts in different countries, such as by experts in the electricity supply industry.
Conclusions
In the present paper a summary has been given of what we know on the possible health effects of electric and magnetic fields, and what still needs to be investigated. No answer has been given to the question of which policy should be adopted, but optional systems of protection have been presented. In this connection, it seems clear that the scientific database at hand is insufficient to develop limits of exposure at the μT level, which means in turn that there are no reasons for expensive interventions at these exposure levels. Whether some form of strategy of caution (e.g., prudent avoidance) should be adopted or not is a matter for decisions by public and occupational health authorities of individual countries. If such a strategy is not adopted it usually means that no restrictions of exposure are imposed because the health-based threshold limits are well above everyday public and occupational exposure. So, if opinions differ today as to regulations, guidelines and policies, there is a general consensus among standard setters that more research is needed to get a solid basis for future actions.
Case Study: Outdoor Markets
The informal sector accounts for between 20 and 70% of the urban workforce in developing countries (with the average being 40%); and the traders and hawkers of outdoor markets comprise a significant portion of this sector. Such work is by its very nature precarious. It involves long hours and low pay. Average earnings may not total 40% of levels found in the formal sector. Not only do many workers in outdoor markets lack permanent locations to conduct their business, they also may be compelled to do without supporting infrastructural facilities. They do not enjoy the same legal protection or social insurance as workers in the formal sector and are subject to harassment. Occupationally related morbidity and mortality rates generally go unrecorded (Bequele 1985).
Figure 1. Outdoor food market in Malatia, Solomon Islands, 1995

C. Geefhuyson
Workers in outdoor markets in both developing and developed countries, such as those shown in figure 1 and figure 2 , are exposed to numerous health and safety hazards. They are exposed to exhaust from motor vehicles, which contains such things as carbon monoxide and polycyclic aromatic hydrocarbons. Workers are also exposed to the weather. In tropical and desert locations they are subject to heat stress and dehydration. In cooler climates they are exposed to freezing temperatures, which can cause problems such as numbness, shivering and frostbite. Workers in outdoor markets may not have access to adequate hygiene facilities.
Figure 2. Heavy baskets of sea urchins being distributed by a small operator-owner, Japan, 1989

L. Manderson
The informal sector generally and outdoor markets specifically involve child labour. Roughly 250 million children are engaged in full- and part-time work around the world (ILO 1996); street traders are the most visible child workers. Children who work, including street traders, typically are denied education and often are forced to perform tasks, such as lifting heavy loads, which can result in permanent disabilities.
The Retail Industry
The retail trade is the selling of goods to consumers. Enterprises sell everything from automobiles to clothing, from food to television sets. In many countries what once was an industry comprised mainly of small shops and stores, now largely consists of multinational conglomerates which own huge megastores competing for the global market. Competition and technological changes have changed job descriptions, the hazards associated with those jobs and the nature of the workforce itself.
In the developed nations, small retailers struggle to compete with large corporate retailers. In the United States, Canada and throughout the European Community and the Pacific Rim, the retail trade has moved from the city centre to suburban shopping malls. Instead of the neighbourhood “mom and pop” stores, multinational chain stores sell the same products and the same brand names, effectively limiting consumer choice of product and forcing competition out of the market by their buying power, advertising capabilities and lower prices. Many times a large store will take a loss on certain products in order to bring customers into a store; this technique frequently generates other sales.
In developing countries with predominantly agrarian economies, bartering systems and open marketplaces are still common. However, in many developing countries, the large multinational retailers are beginning to enter the retail market.
Each type of establishment has its own hazards. Retail work in developing countries and countries in transition is often very different from retail work in developed countries; conglomerates with large chain stores are not yet dominant and retail work is mainly conducted in an open-air market, in all types of weather.
There is a trend among multinational conglomerates to try and change employment conditions: trade unionism is discouraged, staff is reduced to a bare minimum, wages go down, stores predominantly hire part-time workers, the average age of the workforce is lowered and benefit packages diminish.
Throughout the world store opening hours have changed so that some establishments even remain open 24 hours a day, 7 days per week. In the past, a worker who worked late at night or on a holiday received extra compensation; now, premium pay for working those hours has been taken away as such long hours become the norm. In the US, for example, traditional holidays are now negotiable when the store stays open on a 24-hour, 7-day basis.
The changes in the nature of how business is conducted has forced several fundamental changes in the workforce. Since many jobs have been marginalized to part-time work, the jobs themselves require little skill and workers receive no training. Workers who once saw a career in retail work, now find themselves changing jobs frequently or even leaving the field of retail work, which has become short term and part time.
The size of the workforce in the retail industry is difficult to estimate. The informal sector plays a significant role in developing countries (see “Case Study: Outdoor Markets”). Many times, health and safety problems go unnoticed, are not recorded by government and are considered to be part of the job.
In many of the countries that do keep statistics, retail, wholesale and restaurant and hotel workers are grouped into one category. Statistics from around the world show that the percentage of people who work in the wholesale, retail, restaurant and hotel trades ranges from over 20% in some countries in Asia to less than 3% in Burkina Faso (see table 1 ). Although men outnumber women in the labour force, the percentage of women in the retail industry is higher in at least half of the countries for which statistics are available.
Table 1. Labour statistics in the retail industry (selected countries)
|
Country |
Men in the labour force (%) |
Men in |
Women in the labour force (%) |
Women in |
Total population in |
Total number |
Injured people |
|
Burkina Faso |
51.3 |
1.0 |
48.7 |
1.5 |
2.6 |
1,858 |
8.71 |
|
Costa Rica |
69.9 |
11.0 |
30.1 |
7.4 |
18.4 |
156,782 |
7.02 |
|
Egypt |
75.9 |
7.3 |
24.1 |
1.2 |
8.4 |
60,859 |
2.52 |
|
Germany |
52.3 |
4.5 |
47.7 |
7.0 |
11.5 |
29,847 |
20.13 |
|
Greece |
63.0 |
10.9 |
37.0 |
7.0 |
17.0 |
23,959 |
10.54 |
|
Italy |
63.1 |
11.7 |
36.9 |
6.9 |
8.6 |
767,070 |
8.15 |
|
Japan |
59.5 |
11.0 |
40.5 |
10.9 |
21.9 |
2,245 |
9.7 |
|
Mexico |
69.1 |
10.8 |
30.9 |
9.6 |
20.5 |
456,843 |
16.96 |
|
Netherlands |
58.9 |
9.1 |
41.1 |
8.0 |
17.1 |
64,657 |
16.5 |
|
Norway |
54.5 |
7.9 |
45.5 |
8.9 |
16.7 |
26,473 |
5.0 |
|
Singapore |
59.8 |
13.2 |
40.2 |
9.0 |
22.0 |
4,019 |
0.27 |
|
Sweden |
52.0 |
6.8 |
48.0 |
6.5 |
13.3 |
43,459 |
6.6 |
|
Thailand |
55.5 |
5.8 |
49.5 |
6.8 |
12.6 |
103,296 |
3.18 |
|
United Kingdom |
56.2 |
8.3 |
43.8 |
9.5 |
17.8 |
157,947 |
11.09 |
|
United States |
54 |
11.1 |
46.0 |
10.0 |
21 |
295,340 |
23.610 |
1 Including commuting accidents; including occupational diseases.
2 Including commuting accidents; establishments employing 100 or more workers.
3 The series related to the territory of the Federal Republic of Germany before 1990;
including commuting accidents.
4 Including occupational diseases;.including non-fatal cases without lost workdays.
5 Including commuting accidents; persons losing more than three workdays
per period of disability.
6 Including non-fatal cases without lost workdays.
7 Including commuting accidents; including occupational diseases;
including non-fatal cases without lost workdays.
8 Including commuting accidents.
9 Employees only; excluding traffic accidents; year beginning April, 1993.
10 Including occupational diseases.
Sources: Country reports: Costa Rica 1994; Greece 1992, 1994; Mexico 1992, 1996; Singapore 1994, 1995; Thailand 1994, 1995; Euro-FIET Commerce Trade Section 1996; ILO 1994, 1995; Price Waterhouse 1991.
Operations, Hazards and Prevention
Cashiers
Many cashiers work at mechanized registers that require them to punch a keypad thousands of times per day to ring up the price of the article. The key punching is usually done with the right hand while products are moved from in front of the cashier to the rear of the cashier for packaging with the left hand. These work activities frequently involve poorly designed workstations, causing cashiers to lift heavy products, reach extensively for products and frequently twist the body in order to move products from one area to another. This job function places different burdens on each side of the body, causing lower-back pain, upper-extremity illnesses and repetitive-motion illnesses including tendinitis, carpal tunnel syndrome, tenosynovitis, thoracic outlet syndrome and hip, leg and foot problems.
Well-designed workstations, with automatic scanners, flexible work height conveyors, lowered bagging stations, extra personnel to bag the products and flexible seats (so that cashiers can sit to relieve lower-back and leg pressures) help eliminate upper- extremity pressures, strains and twisting motions.
Lasers
Bar-code readers and hand-held scanners in supermarkets are generally Class 2 lasers, which produce infrared radiation in the wavelength range of 760 to 1,400 nm; they are considered nonhazardous unless there is prolonged viewing of the laser beam. A laser produces a high-intensity light which can damage the retina of the eye. The eyes are vulnerable to heat, have no heat sensors and do not dissipate heat efficiently. Recommended safe practices should include, at a minimum, training workers about the hazards of looking into the beam of light and the damage to the eye that can result. Baseline eye examinations should be included in a worker protection programme to ensure that no damage has occurred.
Clerks
Retail clerks move large quantities of product from trucks to the loading dock and then to the shelves in the sales area of the store. Products come packaged in cartons of various weights. Manually unloading trucks and moving the product cartons to the front of the store may cause musculoskeletal problems. Pricing the items and placing them on the shelves puts tremendous pressure on the back, legs and neck. Using a pricing gun can cause carpal tunnel syndrome and other RSIs by putting excessive and repeated strain on the wrist, fingers and palm of the hand. Opening cartons with a knife or blade can lead to cuts on the hands, arms and other parts of the body. Cutting through cardboard with a dull knife requires extra pressure, which puts extra strain on the palms of the hands.
Mechanical lifting aids, such as fork-lift trucks, manual high-low trucks, dollies and carts help move items from one part of the store to another. Tables, scissor jacks and movable carts can help bring the items to a good height and help clerks place product on the shelves without back strain from lifting and twisting. Automated pricing guns or packaged goods already labelled will prevent wrist and upper extremity strains from repeated motions. Sharp knives will prevent forceful motions when opening cartons.
Meat cutters and delicatessen workers
Meat cutters and delicatessen workers work with saws, grinders, slicers and knives (see figure 1). When machine blades are not guarded, get jammed or become loose, fingers can be severed, cut, crushed or bruised. Machines must be securely anchored to the floor to prevent tipping and moving. Blades must be kept free of debris. If a machine is jammed, wooden devices should be used to unjam the machine with the power off. No machines should be unjammed with the power still on. Knives should be kept sharp to avoid problems in the wrists, hands and arms. The handles of knives, cleavers and clubs should be kept clean and unslippery.
Figure 1. Small-scale manual cutting of dried meet for local sale, Japan, 1989

L. Manderson
When meat is mechanically weighed and packaged on a styrofoam tray in a plastic film sealed with a heating element, vapours and gases from the heated plastic may cause “meat wrapper’s asthma” and eye, nose and throat irritation, difficulty in breathing, chest pains, chills and fever. Local exhaust ventilation (LEV) should be placed near the heating element so that these vapours are not breathed in by workers, but are vented outside the workplace.
Meat cutters enter and leave freezers many times during the day. Work clothing should include heavy clothing for freezer work.
Floors and walkways can become slippery from meat, grease and water. Slips, trips and falls are common causes of injury. All waste material must be carefully discarded and kept off walking surfaces. Walking and standing mats must be cleaned daily or whenever they become soiled.
Chemical exposures
Retail workers are increasingly exposed to hazardous chemicals in cleaning products, pesticides, rodenticides, fungicides and preservatives. Hardware store workers, automotive distributive workers and others are potentially exposed to hazardous chemicals because of the stock of paints, solvents, acids, caustics and compressed gases. The hazardous or toxic chemicals vary depending on the nature of the products that are stocked in each establishment. These can include materials not necessarily considered hazardous. Department store workers, for example, can develop sensitivities and allergies to perfumes that are sprayed as demonstrations.
Cleaning products that are used to clean surfaces in supermarkets and other retail establishments may contain chlorine, ammonia, alcohols, caustics and organic solvents. These products may be used by cleaning crews during the night shift, in stores without natural ventilation and when the mechanical ventilation system is not working at full capacity. These chemical products affect the body when used in the workplace in industrial strengths and amounts. Chemical safety information must be readily available in the workplace for workers to read. Chemical containers must be labelled with the name of the chemical and how the product affects the body, as well as which protective equipment must be used to prevent illness. Workers need to be trained about the health hazards associated with the use of chemicals, how the chemicals enter the body and how to avoid exposure.
Retail workers who set up shop on the street are exposed to exhaust from motor vehicle traffic, as are the back-of-the-store workers who inhale exhaust from idling delivery trucks in the truck bays. The incomplete combustion products in motor vehicle exhaust include, among other things, carbon monoxide and polycyclic aromatic hydrocarbons. Exhaust gases and particulates affect the body is several ways. Carbon monoxide causes dizziness and nausea and acts as an asphyxiant, limiting the blood’s ability to use oxygen. Delivery trucks should turn off their engines while unloading. Mechanical general exhaust ventilation may be needed to vent the contaminated air away from workers. Routine scheduled maintenance and cleaning is needed to maintain the ventilation system.
Formaldehyde is frequently used on clothing and other textiles to prevent mildew. It can affect those who breathe it in. In stores with larger stocks of clothing and textiles without adequate natural or mechanical ventilation systems, formaldehyde gas can build up and irritate the eyes, nose and throat. Formaldehyde can cause skin and respiratory irritation and allergies and is considered a probable carcinogen.
Pesticides, rodenticides and fungicides are frequently used to keep vermin out of establishments. They can affect the nervous, respiratory and circulatory systems of human beings as well as insects, rodents and plants. It is important not to spray chemicals indiscriminately when people are present and to keep people away from sprayed areas until it is safe to enter them again. The pesticide applicator must be trained in safe work methods before pesticides are applied.
“Tight” buildings—those without windows that can open and without natural ventilation—are dependent on mechanical ventilation systems. These systems must provide an adequate exchange of air within the space and must include adequate fresh outdoor air. The air must be heated or cooled depending on the ambient temperature outside.
Sanitation
Personal hygiene is important in the retail industry, especially when employees handle food, money and hazardous chemicals. Toilets and washing and drinking facilities must be sanitary and available in areas where employees can use them while on duty. Facilities must have clean running water, soap and towels. Employees must be encouraged to wash their hands thoroughly after using the toilet and before returning to work. Clean, cool drinking water should be available throughout the work area. Good housekeeping is necessary to prevent vermin and accumulation of garbage. Trash should be picked up on a regular basis.
Sanitation facilities are difficult to maintain in open-air markets, but an attempt must be made to provide toilets and washing facilities.
Weather
In open-air markets, retail workers are exposed to the elements and subject to the problems relating to heat and cold. In supermarkets, cashiers often work at the front of the store close to the doors that the public uses to enter and exit, exposing cashiers to hot and cold air drafts. Air shields in front of the doors that go to the outside will help block drafts and keep the air temperature at the cash register consistent with the rest of the store.
Fire prevention
There are many fire hazards in retail stores, including locked or blocked exits, limited entry and exits, combustible and flammable materials and faulty or temporary electrical wiring and heating systems. If workers are required to fight a fire, they must be trained in how to call for help, use fire extinguishers and evacuate the space. Fire extinguishers must be of the appropriate type for the type of fire and must be inspected regularly and maintained. Fire drills are necessary so that workers know how to get out of the facility during an emergency.
Stress
A new trend in retail work, when the establishment is owned by a large conglomerate, is to change full-time work to part-time work. Many large retail stores are now staying open 24 hours per day, and many stay open every day of the year, forcing workers to work “unsocial” hours. Disruption of the internal biological clock which controls natural physical phenomena such as sleep, causes symptoms such as sleepiness, gastro-intestinal disturbances, headaches and depression. Changing shifts, working on holidays and part-time work cause emotional and physical stress on the job and at home. “Normal” family life is severely compromised and meaningful social life is restricted.
Late night hours are more and more prevalent, increasing the feeling of insecurity about personal safety and the fear of robberies and other types of violence on the job. In the United States, for example, homicide is a major cause of death on the job for women, with many of these deaths occurring during robberies. Handling money or working alone or during late night hours should be avoided. A regular review of security measures should be part of a violence prevention and security programme.
Part-time pay, with few or no benefits, increases job stress and forces many workers to find additional jobs in order to support their families and maintain health benefits.
Telework
Telework—or working out of one’s home—is a growing trend in businesses internationally. This article discusses the occupational health and safety hazards of telework (from the Greek tele, meaning “far off”). The employer’s responsibility to provide safe and healthy working conditions to such employees will vary depending on the contract or understanding that exists between each teleworker and employer and on the applicable labour laws.
While telework is most widespread in the United States, where it involves over 8 million workers and accounts for 6.5% of the workforce, other countries also have significant numbers of teleworkers. There are more than 560,000 in the United Kingdom, 150,000 in Germany and 100,000 in Spain. There are over 32,000 in Ireland, which amount to 3.8% of the workforce (ILO 1997).
The growing trend toward telework arrangements can be explained by the following factors:
- business efforts to reduce the time, expense and environmental impact of commuting
- legislative efforts to reduce traffic-induced air pollution trends
- changes in technology, computerization and electronic communication that enable businesses to employ workers in disparate geographic locations
- costs of maintaining large office spaces needed to accommodate large numbers of employees
- accommodation of workers who prefer telework due to physical disability, parenting needs or other family responsibilities or other reasons
- a strategy to reduce absenteeism
- recognition that workers have varying internal cycles of productivity and creativity.
Increased productivity is another factor, as a number of studies have demonstrated that telework can result in large productivity gains (ILO 1990b).
Telework may be contracted in several ways:
- The employee works full time (or part time) at home for their employer and is entitled to all of the same benefits provided by that employer to all onsite workers.
- The employee works full time for the employer but only works out of the home during a specified number of days per week or month.
- The worker is defined as an independent contractor and does not receive benefits or equipment provided by the employer.
Health and Safety Hazards of Telework
The health and safety hazards of telework can include all of the same hazards found in conventional office environments, with several additional concerns.
Indoor air quality
Most homes are not equipped with mechanical ventilation systems. Instead, air exchanges in the home rely on natural ventilation. The effectiveness of this can depend on such factors as the type of insulation of the building and so on. Provision of a fresh supply of outside air cannot be guaranteed. If the natural ventilation is inadequate to remove sources of indoor air pollutants in the home work environment, then additional ventilation may be necessary.
Indoor air pollutants in the home environment may include the following:
- natural gas or carbon monoxide exposure from inefficient heating systems or leaky stoves
- vapours and gases from photocopiers, printers or other office machines
- ongoing passive exposure to chemicals, gases or dusts resulting from renovation or construction in the worker’s home
- exposure to the effluents of other activities if housed in a multi-use building (such as an apartment building with a nail salon, dry cleaner or fast food restaurant on the ground floor).
- exposure to radon hazards if office is located in the basement in parts of the world where radon arises from construction materials or the earth.
Fire hazards
Home electrical wiring is rarely designed to accommodate the needs of the electrical equipment typically used in telework, such as printers, copiers and other office machines. Installing such equipment without assessing the wiring limits of the dwelling could create a fire hazard. Local building codes may prohibit the adjustments necessary to accommodate increased equipment needs.
Teleworkers who rent their apartments may live in multi-unit dwellings with inadequate fire evacuation plans, blocked means of egress to fire exits or locked exit doors.
Ergonomics hazards
Home work environments often rely on the employee’s personal furnishings such as chairs, tables, shelves and other items to perform required tasks. Computer workstations in the home environment may not allow for the adjustments necessary for computer-intensive work. A shortage of adequate surface area, shelf space or storage areas may result in excessive bending, awkward postures, excessive reaching and other risk factors for cumulative trauma disorders (CTDs). Working in cold or unevenly heated environments can also contribute to musculoskeletal injuries.
Lighting
Inadequate lighting may result in awkward body postures, eye strain and visual disturbances. Task lighting may be necessary for work surfaces or document holders. Wall and furniture surfaces should be neutral with a non-glare finish. While this glare-reducing strategy is increasingly utilized in office environments, it is not yet a standard of home decoration and design.
Occupational stress
Full-time employment in the home environment deprives the worker of the interpersonal and professional benefits of continuous interaction with co-workers, colleagues and mentors. The isolation created by telework can prevent the worker from engaging in professional development activities, taking advantage of promotional opportunities and contributing ideas to the organization. Gregarious workers in particular may depend on human contact and suffer personally and professionally without it. The lack of administrative support services for employees who require clerical assistance presents an additional burden to teleworkers. The employer should make an effort to incorporate the teleworker into staff meetings and other group activities, either in person or electronically (tele-conferencing) as per physical and geographical limitations.
Employees with children, disabled family members or ageing parents may perceive distinct advantages of working at home. But attending to the needs of dependent family members can affect the concentration needed to focus on job responsibilities. The ensuing stress can negatively impact on the worker who is unable to perform to capacity in the home and fails to meet employer expectations. Telework should not be considered as a substitute for child or elder care. Since workers vary tremendously in their capacity to balance work and other responsibilities in the home environment, the need for support services must be evaluated on a case-by-case basis to prevent excessive occupational stress and subsequent loss in productivity. No worker should be required to adopt a telework arrangement against his or her will.
Injury and Illness Compensation
Occupational illnesses often occur over long periods of time from cumulative exposures. Prevention of these illnesses depends on rapid identification of risk factors, fixing the problem using a variety of methods and medical management of the affected worker when the first signs or symptoms of illness appear.
To date, employer responsibility for accidents and injuries in the home environment have been debated on a case-by-case basis. Most national occupational health and safety standards do not include formal policies addressing the safety of teleworkers. The serious impact of this trend must be carefully evaluated and addressed via international standard-setting.
When telework arrangements shift the employee’s status to that of an independent contractor, the burden of many responsibilities shift to the employee as well. Once the work is performed in the home by an independent contractor, the employer no longer feels obligated to provide a healthy and safe workplace, access to preventive and curative medical care for the worker and his or her family, social security, disability insurance and compensation for injured workers who need to recuperate. This trend eliminates worker benefits and protections that were won after decades of struggle and negotiation.
Protection for the Teleworker
The contract between the teleworker and the employer must address the overall work environment, safety and health standards, training and equipment. Employers should inspect the home workspace (at agreed-upon times) to ensure worker safety and to identify and correct risk factors that could contribute to illness or injury. The inspection should evaluate indoor air, ergonomics, trip hazards, lighting, chemical exposure and other concerns. Clear policy must be established regarding the provision of office supplies required for job tasks. Liability issues must be clearly defined regarding employer (and worker) assets that are lost or damaged due to fire, natural disaster or theft. Employees must be exempt from financial liability unless found to be negligent.
In addition, telework arrangements should be evaluated on a regular basis in order to identify workers who discover that working at home does not work for them.
Summary
The advantages of telework are extensive, and beneficial telework arrangements should be encouraged for job tasks and mature workers who will have much to gain by working at home. Telework has enabled disabled workers to achieve greater independence and seek professional opportunities not previously offered or available. In return, employers are able to retain valuable workers. However, the telework arrangement must ensure continuation of employee benefits and occupational health and safety protections.
Bank Teller Safety: The Situation in Germany
Working in the Bank: Now Safer for the Personnel
What long-term measures can be taken to reduce the attraction of robbing a bank? The new provisions in Germany’s Accident Prevention Regulation (APR) for “Teller’s window” (VBG 120) significantly minimizes the risk to employees of being injured or killed in bank robberies.
A precise knowledge of the conduct of bank robbers is crucial. To this end, the Administration Trade Organization has been studying bank robberies since 1966. These studies have shown that, for example, bank robbers prefer small bank branches with few employees. Approximately one-third of bank robberies occur shortly after opening or just before closing. The goal is to leave the robbed bank as quickly as possible (after 2 or 3 minutes) and with the largest possible haul. Many bank robbers work under the wide-spread misconception that DM 100,000 and more can be taken from a teller’s window. The results of these and other studies are contained in the sections “Building and equipping” and “Operations” in the “Teller’s window” APR. Measures that drastically reduce the bank robbers’ expectations are proposed here to protect the employee. The success of these measures depends upon the employees strictly adhering to them in daily practice.
What basic requirements are set in the “Teller’s window” APR? In paragraph 7 of the “Teller’s window” APR, the central requirement is laid out: “Protecting the insured requires securing the banknotes so as to considerably reduce the incentive for robbery”.
What does that mean in daily practice? Easily accessible money should be kept and worked with in publicly accessible areas only within rooms separated from the public by bullet-proof or break-proof sections.
The maximum amount of accessible money allowed is given in paragraph 32: a combined maximum of DM 50,000 is allowed if there are bullet-proof tellers’ windows, other break-proof safeguards and at least 6 employees present. DM 10,000 may not be exceeded when using break-proof safeguards (but not bullet-proof tellers’ windows) in connection with containers equipped with time-staggered releases. There must be at least 2 employees present at all times, who must be in eye-contact.
To keep the incentive for bank robbery as low as possible, amounts of accessible money should be kept well below the maximums set in the “Teller’s window” APR. In addition, paragraph 25 calls for company instructions to set the maximum allowable accessible amounts for each branch. Larger amounts necessary for business and other needs should be secured in time-lock containers to make access by bank robbers more difficult.
Tellers’ windows that are not equipped with bullet-proof or break-proof safety guards and have no central money supply facility or employee-operated automatic teller machine should not have any accessible banknotes on hand.
Securing Windows and Doors
Personnel entrance and exit doors to teller areas containing cash must be secured against viewing or entering from outside, so that bank robbers cannot easily intercept employees entering and leaving bank rooms. The employee must be able to ensure, with built-in peepholes, that no danger exists.
To prevent unnoticed entrance by bank robbers into bank rooms, door closers must ensure that doors are always kept closed.
Since a considerable incentive for theft arises from viewing banknotes, windows behind which banknotes are handled must be secured against viewing or penetrating. Statistics show that holding strictly to this requirement results in very few bank robberies through windows or personnel entrances.
In contrast to personnel entrance and exit doors, doors for public traffic must have a clear view. Bank robbers can thereby be recognized early and an alarm sounded to bring assistance. Therefore it is important that the view not be obstructed by placards or the like.
Optimal Room Surveillance
In order to be able to identify the bank robber as quickly as possible, and to have effective evidence for court, optimal room surveillance equipment is prescribed in the “Teller’s window” APR. This is also important for determining whether the robber extorted money or threatened employees, since particularly brutal actions increase the penalty. Good pictures reduce the incentive to rob a bank.
The instruction “Installation directions for optimal room surveillance equipment (ORSE) SP 9.7/5” of July 1993 permitted only individual cameras as standard ORSE. Photographs are superior to video shots for identification because of greater detail recognition, resulting in better evidence. The disadvantage lies in the fact that photos are available only after the camera is triggered. Because of technical advances, the Administration technical committee now also permits the use of video cameras as possible ORSE. The corresponding instruction is now being prepared; it provides that the limited resolution of video pictures should be compensated for by using 2 views. For this, at least 2 cameras must be installed for recognizing the robber and for videotaping essential events.
Appropriate installation of the video technology can continuously record, and a “wanted” photo can thus be available without special triggering. The further advantages of the system include colour shots, quicker availability of “wanted” photos, transmission of the pictures to the police even during the robbery and the ability to constantly check the functioning of the camera.
Teller’s Window Security
The “Teller’s window” APR authorizes:
- bullet-proof and break-proof glass enclosures and tellers’ booths
- power-driven separations
- break-proof separations in connection with bullet-proof screens
- central money supply equipment
- employee-operated teller machines.
Furthermore, customer-operated teller machines support the requirements of paragraph 7, since their use can reduce the amount of money in the booth or separated room.
In order to comply with the “Teller’s window” APR, the number of employees needed at the counter and the amounts to be taken in and paid out (quantity and number) must be known before a tellers’ counter is built or remodeled. Optimal security can be achieved only when counter security corresponds to the actual flow of business.
Constant Presence with Eye contact
Certain teller security measures require a minimum of 2 to 6 employees having eye contact with each other. This requirement flows from the recognition that bank robbers prefer smaller branches with higher yields, where the tellers, when threatened with a gun, cannot withdraw behind bullet-proof shielding.
Break-proof teller shielding can be used only when 6 employees with eye contact are always present in the counter area. This does not mean a 6-person location, where not everyone is always at their workplace due to vacation, sickness, customer visits and so on. Experience shows that this condition can be fulfilled only when 8 to 10 employees work at the location. Alternatively, a floater service can possibly be used to ensure the necessary minimum number of employees.
To guarantee the constant presence of 2 employees with eye contact, the location must have 3 to 4 positions.
It is important that the facility not be opened before the required minimum number of employees are present. When consultations are taking place in adjoining rooms, the minimum number of employees at the windows must still be maintained.
Security through Separation
Small branches
“Small branches” are those where the presence of at least 2 employees with eye contact in the counter area is not ensured. For these branches, bullet-proof shielding in connection with break-proof separations offers good protection, since the employee does not have to leave the secured area in the event of a robbery. Consultations are carried on in an area protected by break-proof shielding. Good communication is possible here. The bullet-proof shield, behind which the accessible cash must be kept, should be placed so that employees cannot be threatened with a weapon from the customer area. Money transactions take place by way of a prescribed hatch or sliding drawer. Since the employee must go into the bullet-proof-secured area in the event of an attack, the necessary personal security is provided. This area must not be left under any circumstances, including while handing money over to the robber.
Bullet-proof full separation presents an alternative for 1- to 3-person teller operations. It offers mechanical protection against the typical bank robbery, since all employees are separated from the robber by bullet-proof shielding. The disadvantage here is that communication with customers is reduced in the interest of security. So full bullet-proof separation is appropriate only for small branches.
Larger branches
The teller’s booth is a form of security in which only the teller’s work station is separated from the customer area. This possibility makes sense only for teller jobs in which the teller is fully occupied by his or her work in the booth and does not have to leave it.
Before installing a booth, it is necessary to determine whether the teller is fully occupied handling money. In smaller branches with only 2 to 4 employees, this is often not the case. If the teller has other tasks outside the booth, the security requirements of the APR are not met, since the teller is supposed to always be separated from the customers for protection against bodily attack. In practice what repeatedly happens is that while the teller is performing tasks outside the booth, the door is held open with a wedge or the key is left in the lock. Thus the security of the teller’s booth is compromised, which is of great interest to potential robbers.
The bullet-proof teller’s booth does hinder communication between the teller and customers. But since longer discussions take place in unsecured workplaces anyway, this does not present a big problem. More serious problems include ensuring draft-free ventilation and air-conditioning in small teller’s booths.
For power-driven separations, a movable steel wall, built into the counter, is raised in emergencies by way of several arranged triggers in second intervals. This creates a bullet-proof separation, with the employees behind it in a secure area. To prevent a robber from entering unnoticed, it must be activated whenever there are no employees in the vault area, or when work is being done that requires personnel to turn away from the counters. In order to avoid constant activation of the steel wall, this type of security should be used only in 2- to 4-person teller areas.
Furthermore, the tellers’ workstations can be isolated with bullet-proof separations. For this, full separations for all employees as well as tellers’ booths can be installed. This form of security, however, requires the constant presence of at least 6 employees with constant eye contact in the main hall.
Bullet-proof full separation and tellers’ booths can also be used when a minimum of 2 employees are present with eye contact and the accessible cash does not exceed DM 10,000. A time-release money container is required in this case so that the teller does not constantly have to leave the secured area to restock. Bank robbers avoid teller positions where they can expect only a small amount of cash or have to wait a long time for it. In this case, notice of the time-release container at the entrance and in the tellers’ area is important for the employees’ protection. This makes immediately clear to the potential robber that the employee has no control over the container and that only a small haul can be expected.
Security without Accessible Banknotes in the Main Hall
Security is possible even without building a separation between the employees and the customer area. But for this to reduce the incentive, no accessible quantities of money can be in the tellers’ area. Money taken in must be immediately secured. The money is kept in a cash box in an area not open to the public, so it cannot be threatened by the robber. The employees receive the necessary amounts of money through a tube delivery system in the main hall. Money taken in is sent to the cash box by this means. No minimum number of employees in the main hall is prescribed in this case. This type of security, however, results in longer waiting times for customers. The advantage is that bank robbers have virtually no chance of getting anything in a robbery.
Employee-operated automatic teller machines (ATMs) are a second way to make payments with cash that is not accessible in the main hall. These, referred to by the bank as AKT-designated machines, contain 4 to 6 magazines for holding banknotes in a time-released secured container. For payments, the required amount is called up using a keyboard, with which an alarm can also be sounded in emergencies. The money is delivered to the employee after a time delay. The length of the delay depends upon the amount of money and is set in paragraph 32 of the “Teller’s window” APR. These are set so that good service is possible, but the robber is scared off by the longer waiting times for larger amounts. Cash receipts should be secured by use of time- or double-closing containers.
At least 2 employees with eye contact must be constantly present when using an employee-operated ATM. For this reason, this form of security is appropriate only for locations in which 3 to 4 employees work. Discussions can take place in a conference room only when 2 or more employees are present in the customer area during the discussion.
In the case of a technical problem in an employee-operated ATM, appropriate instructions and measures should be prepared. These should include an emergency cash box and corresponding organizational procedures to ensure that work proceeds in accordance with the “Teller’s window” APR.
Company Directives and Instructions
The employer must prepare company directives for every teller’s window and regularly check on compliance. These directives should outline the possible events during a robbery and describe what to do during and after the robbery. Furthermore, daily instructions should be given, and use of the installed security equipment should be mandated. This is especially true when larger amounts of accessible banknotes are present. Instructions should also prescribe the manner of safekeeping for other valuable objects. Employees at the windows should be instructed in these company policies at least twice a year.
The purpose of these instructions is clear—to ensure that the employees follow the requirements of the “Teller’s window” APR for their own protection, and to significantly reduce the incentive for robbing a teller’s window.
Offices: A Hazard Summary
Office workers may perform a wide variety of tasks, including: answering the telephone; interacting with the public; handling money; receiving and delivering mail; opening mail; typing and transcribing; operating office machinery (e.g., computers, adding machines, duplicating machines and so on); filing; lifting supplies, parcels and so on; and professional work such as writing, editing, accounting, research, interviewing and the like. Table 1 lists standard clerical jobs.
Table 1. Standard clerical jobs
Clerks
Secretaries and keyboard-operating clerks
Stenographers and typists
Word-processor and related operators
Data entry operators
Calculating-machine operators
Secretaries
Numerical clerks
Accounting and bookkeeping clerks
Statistical and finance clerks
Material-recording and transport clerks
Stock clerks
Production clerks
Transport clerks
Library, mail and related clerks
Library and filing clerks
Mail carriers and sorting clerks
Coding, proof-reading and related clerks
Scribes and related clerks
Other office clerks
Cashiers, tellers and related clerks
Cashiers and ticket clerks
Tellers and other counter clerks
Bookmakers and croupiers
Pawnbrokers and money-lenders
Debt-collectors and related workers
Client information clerks
Travel agency and related clerks
Receptionists and information clerks
Telephone and switchboard operators
Source: ILO 1990a.
Office workers are often thought to have pleasant, safe environments to work in. Even though office work is not as hazardous as many other workplaces, there are a variety of safety and health problems that may be present in an office. Some of these can pose significant risks to office workers.
Some Hazards and Health Problems
Slips, trips and falls are a common cause of office injuries. Poor weather conditions such as rain, snow and ice create slip hazards outside of buildings, and inside when wet floors are not cleaned up promptly. Electrical and telephone cords placed in aisles and walkways are a common cause of trips. Carpeted offices can create trip hazards when old, frayed and buckling carpet is not repaired and shoe heels catch on it. Electrical floor outlet boxes can cause trips when they are located in aisles and walkways.
Cuts and bruises are seen in office settings from a variety of causes. Paper cuts are common from file folders, envelopes and paper edges. Workers can be injured from walking into tables, doors or drawers that have been left open and are unseen. Office supplies and materials that are improperly stored can cause injury if they fall onto a worker or are placed where a worker would inadvertently walk into them. Cuts can also be caused by office equipment such as paper cutters and sharp edges of drawers, cabinets and tables.
Electrical hazards occur when electrical cords are placed across aisles and walkways, subjecting the cords to damage. Improper use of extension cords is often seen in offices, for example, when these cords are used in place of fixed (permanently installed) outlets, have too many items plugged into them (so that there could be an electrical overload) or are the wrong size (thin extension cords used to energize heavy-duty cords). Adapter or “cheater” plugs are used in many offices. Most often they are used to connect equipment that must be grounded (three-pronged plug) into two-pronged outlets without connecting the plug to ground. This creates an unsafe electrical connection. Ground pins are sometimes broken off a plug to allow for the same two-prong connection.
Stress is a significant psychosocial health problem for many offices. Stress is caused by many factors, including noise from overcrowding and equipment, poor relationships with supervisors and/or co-workers, increase in workload and lack of control of work.
Musculoskeletal problems and soft tissue injuries such as tendinitis result from office furniture and equipment which is not fitted to a worker’s individual physical needs. Tendinitis can occur from repeated movement of certain body parts, such as finger problems from constant writing, or filing and retrieving files from cabinets that are too full. Many office workers suffer from a variety of RSIs such as carpal tunnel syndrome, thoracic outlet syndrome and ulcer nerve damage because of the ill-fitting equipment and the lack of rest breaks from continuous keying (on a computer) or other repetitive activities. Poorly designed furniture and equipment also contribute to poor posture and nerve compression of lower extremities, since many office workers sit for long periods of time; all of these factors contribute to low-back and lower-extremity problems, as does constant standing.
Continual use of computers and poor overall lighting create eye strain for office workers. Because of this, many workers experience a worsening of vision, headaches, burning eyes and eye fatigue. Adjustments in lighting and computer screen contrast, as well as frequent breaks in eye focus, are necessary to help eliminate eye problems. Lighting must be appropriate for the task.
Fire and emergency procedures are essential in an office. Many offices lack adequate procedures for workers to exit a building in case of fire or other emergency. These procedures, or emergency plans, should be in writing and should be practised (through fire drills) so that office occupants are familiar with where to go and what to do. This insures that all workers will promptly and safely evacuate in the event of a real fire or other emergency. Fire safety is often compromised in offices by blocking of exits, lack of exit signage, storage of incompatible chemicals or combustible materials, inoperative alarm or firefighting systems or total lack of adequate means of notification of workers in emergencies.
Violence
Violence in the workplace is now being recognized as a significant workplace hazard. As discussed in the chapter Violence, in the United States, for example, homicide is the leading cause of death for women workers and the third-leading cause of death for all workers. Non-fatal assaults occur much more frequently than most people realize. Office workers who interact with the public—for example, cashiers—can be at greater risk of violence. Violence can also be internal (worker against worker). The vast majority of office workplace violence, however, comes from people coming to the office from the outside. Government office workers are much more at risk for workplace violence incidents because these workers administer laws and regulations to which many citizens have hostile reactions, be they verbal or physical. In the United States, 18% of the workforce are government workers, but they constitute 30% of the victims of workplace violence.
Offices can be made safer by restricting access to work areas, changing or creating policies and procedures which help eliminate sources of hostility and provide for emergency procedures and installing security equipment which is appropriate for the particular office being improved. Measures for improving safety are illustrated in the article describing German requirements for bank teller safety.
Indoor Air Quality
Poor indoor air quality (IAQ) is probably the most frequent safety and health complaint from office workers. The effect of poor IAQ on productivity, absenteeism and morale is substantial. The US Environmental Protection Agency (EPA) has listed poor IAQ in their top 5 public health problems of the 1990s. Many reasons exist for poor air quality. Among them are closed or sealed buildings with inadequate amounts of outside air, overcrowding of offices, inadequate maintenance of ventilation systems, presence of chemicals such as pesticides and cleaning compounds, water damage and mould growth, installation of cubicles and walls which block off air flow to work areas, too much or too little humidity and dirty work environments (or poor housekeeping).
Table 2 lists common indoor air pollutants found in many offices. Office machines are also a source of many indoor air pollutants. Unfortunately, most offices have not designed their ventilation systems to take into account emissions from office equipment.
Table 2. Indoor air pollutants that may be found in office buildings
|
Pollutant |
Sources |
Health effects |
|
Ammonia |
Blueprint machines, cleaning solutions |
Respiratory system, eye and skin irritation |
|
Asbestos |
Insulation products, spackling compounds, fire retardants, ceiling and floor tiles |
Pulmonary (lung) fibrosis, cancer |
|
Carbon dioxide |
Humans’ exhaled air, combustion |
Headache, nausea, dizziness |
|
Carbon monoxide |
Automobile exhaust, tobacco smoke, combustion |
Headache, weakness, dizziness, nausea; long-term exposure related to heart disease |
|
Formaldehyde |
Urea-formaldehyde foam insulation and urea-formaldehyde resin used to bind laminated wood products such as particleboard and plywood; tobacco smoke |
Respiratory system, eye and skin irritation, nausea, headache, fatigue, possibility of cancer |
|
Freons |
Leaking air conditioning systems |
Respiratory system irritation; heart arrhythmia at high concentrations |
|
Methyl alcohol |
Spirit duplicating machines |
Respiratory system and skin irritation |
|
Micro-organisms (viruses, bacteria, fungi) |
Humidifying and air conditioning systems, evaporative condensers, cooling towers, mildewed papers, old books, damp newsprint |
Respiratory infections, allergic responses |
|
Motor vehicle exhaust (carbon monoxide, nitrogen oxides, lead particulates, sulphur oxides) |
Parking garages, outside traffic |
Respiratory system and eye irritation, headache (see carbon monoxide), genetic damage |
|
Nitrogen oxides |
Gas heaters and stoves, combustion, motor vehicle exhaust, tobacco smoke |
Respiratory system and eye irritation |
|
Ozone |
Photocopying and other electrical machines |
Respiratory system and eye irritation, headache, genetic damage |
|
Paint vapours and dusts (organics, lead, mercury) |
Freshly painted surfaces, old, cracking paint |
Respiratory system and eye irritation; neurological, kidney and bone-marrow damage at high levels of exposure |
|
PCBs (polychlorinated biphenyls), dioxin, dibenzofuran |
Electrical transformers, old fluorescent light ballasts |
Sperm and foetal defects, skin rashes, liver and kidney damage, cancer |
|
Pesticides |
Spraying of plants and premises |
Depending on chemical components: liver damage, cancer, neurological damage, skin, respiratory system and eye irritation |
|
Radon and decay products |
Building construction materials such as concrete and stone; basements |
Genetic damage, cancer, foetal and sperm damage, etc., due to ionizing radiation |
|
Solvents (methylene chloride, 1,1,1-trichloro-ethane, perchloroethylene, hexane, heptane, ethyl alcohol, glycol ethers, xylene, etc.) |
Typewriter cleaners and correction fluids, spray adhesives, rubber cement, stamp pad inks, felt-tip markers, printing press inks and cleaners |
Depending upon solvent: skin, eye and respiratory system irritation; headaches, dizziness, nausea; liver and kidney damage |
|
Sterilant gases (such as ethylene oxide) |
Systems to sterilize humidifying and air-conditioning systems |
Depending on chemical components: respiratory system and eye irritation, genetic damage, cancer |
|
Tobacco smoke (passive exposure to particulates, carbon monoxide, formaldehyde, coal tars and nicotine) |
Cigarettes, pipes, cigars |
Respiratory system and eye irritation; may lead to diseases associated with smokers |
|
Volatile organic compounds (VOCs) |
Photocopiers and other office machines, carpets, new plastics |
Respiratory system and eye irritation, allergic reactions |
Source: Stellman and Henifin 1983.
The prevalence of poor IAQ has contributed to a rise in occupational asthma and other respiratory disorders, chemical sensitivity and allergies. Dry or irritated skin and eyes are also common health complaints that can be linked to poor IAQ. Action must be taken to investigate and correct problems that are causing poor IAQ according to air quality standards and recommendations.
Dermatitis (both allergic and irritant) can be caused by many of the air pollutants listed in table 2—for example, solvents, pesticide residues, inks, coated papers, typewriter ribbons, cleaners and so forth can cause skin problems. The best solutions for office workers are identification of the cause and substitution.
Professionals and Managers
The workplace, especially in industrialized countries, has become increasingly a world of white-collar workers. For example, in the United States in 1994, white-collar work was done by 57.9% of the workforce, and service occupations accounted for 13.7% of the workforce. The professional occupations have moved from the fourth to the third largest occupational group (AFL-CIO 1995). Table 1 lists standard professional jobs according to the International Standard Classification of Occupations (ISCO-88). White-collar membership in national unions and organizations has grown from 24% in 1973 to 45% in 1993 (AFL-CIO 1995). Professional, managerial and technical occupational employment is expected to grow faster than average.
Table 1. Standard professional jobs
Professionals
Physicists, chemists and related professionals
Physicists and astronomers
Meteorologists
Chemists
Geologists and geophysicists
Mathematicians, statisticians and related professionals
Mathematicians and related professionals
Statisticians
Computing professionals
Computer systems designers and analysts
Computer programmers
Other computing professionals
Architects, engineers and related professionals
Architects, town and traffic planners
Civil engineers
Electrical engineers
Electronics and telecommunications engineers
Mechanical engineers
Chemical engineers
Mining engineers, metallurgists and related professionals
Cartographers and surveyors
Other architects and engineers
Life science and health professionals
Biologists, zoologists and related professionals
Pharmacologists, pathologists and related professionals
Agronomists and related professionals
Health professionals (except nursing)
Medical doctors
Dentists
Veterinarians
Pharmacists
Other health professionals
Nursing and midwifery professionals
College, university and higher education teaching professionals
Secondary education teaching professionals
Primary and pre-primary education teaching professionals
Special education teaching professionals
Other teaching professionals
Education methods specialists
School inspectors
Business professionals
Accountants
Personnel and career professionals
Other business professionals
Legal professionals
Lawyers
Judges
Other legal professionals
Archivists, librarians and related information professionals
Archivists and curators
Librarians and related professionals
Social science and related professionals
Economists
Sociologists, anthropologists and related professionals
Philosophers, historians and political scientists
Philologists, translators and interpreters
Psychologists
Social work professionals
Writers and creative or performing artists
Authors, journalists and other writers
Sculptors, painters and related artists
Composers, musicians and singers
Choreographers and dancers
Film, stage and related actors and directors
Religious professionals
Source: ILO 1990a.
One characteristic of professional office staff and managers is that their work function may require decision-making and responsibility for the work of others. Some managers or professional staff (for example, engineers, nurse administrators or social workers) may be located in industry and experience industrial hazards shared with the line staff. Others with managerial and executive functions work in buildings and offices remote from the industry itself. Both groups of administrative workers have risk from the hazards of office work: occupational stress, poor indoor air quality, chemical and biological agents, repetitive strain injuries (RSIs), fire safety concerns, sexual harassment and violence or assault in the workplace. See also the article “Offices: A hazard summary” in this chapter.
Demographic Changes
In a study of executive “hardiness” in the 1970s, not enough women could be found in executive positions to be included in the study (Maddi and Kobasa 1984). In the 1990s, women and minorities have had increasing representation in positions of authority, professional jobs and non-traditional jobs. However, a “glass ceiling” clusters most women in the lower levels of the organizational hierarchy: only 2% of senior management positions are held by women in the United States, for example.
As women enter traditionally male occupations, the question arises as to whether their experience in the workplace will result in an increase in coronary heart disease similar to that of men. In the past, women have been less reactive than men in stress hormone secretions when faced with the pressure to achieve. However, in studies of women in non-traditional roles (female engineering students, bus drivers and lawyers) a laboratory experiment showed that women had almost as sharp an increase in epinephrine secretion as men exposed to a difficult task, considerably higher than female clerical workers in traditional roles. A study of male and female managers in 1989 showed that both sexes had a heavy workload, time pressure, deadlines and responsibility for others. Women managers reported lack of communication at work and conflict between work and family as sources of stress, whereas male managers did not. Male managers reported the highest work satisfaction. The female managers were not found to have the support of a strong work network. Studies of professional women and their spouses showed child care responsibilities to be more heavily borne by women, with men shouldering chores with less time-specific demands, such as lawn care (Frankenhaeuser, Lundberg and Chesney 1991).
Although studies do not indicate that working leads to smoking, workplace stress is associated with increased smoking rates and difficulties in smoking cessation. In 1988, a higher rate of smoking was observed among female professionals as compared to male professional workers (Biener 1988). Smoking is a behavioural style of coping with stress. For example, nurses who smoked cigarettes reported higher levels of job stress than non-smoking nurses. In the Women and Health study, salaried workers were more likely to report job strain (45%) than hourly wage workers (31%), and more difficulty unwinding after work (57%) than hourly workers (35%) (Tagliacozzo and Vaughn 1982).
International changes have caused political and social restructuring that lead to large numbers of people emigrating from their country of birth. Workplace adaptation to minority groups results in more diverse workers represented in managerial positions. Implications of these changes include human factor analyses, personnel policies and diversity education. Ergonomic changes may be needed to accommodate diverse body types and sizes. Cultures may clash; for example, values regarding high productivity or time management may vary among nations. Sensitivity to such cultural differences is taught more often today as a global economy is envisioned (Marsella 1994).
New Structures of Work Organization
An increase in the use of participative techniques for input and governance of organizations, such as joint labour-management committees and quality improvement programmes, have changed the typical hierarchical structures of some organizations. As a result, role ambiguity and new skill requirements are frequently mentioned as stressors for those in managerial positions.
If the condition of managerial and supervisory work remains challenging, then the high stress/low illness individual can be described as a “hardy executive”. Such executives have been characterized as being committed to various parts of their lives (e.g., family, work, interpersonal relationships), as feeling a greater sense of control over what occurs in their lives and as regarding challenge in a positive mode. If stressful life events (e.g., staff reductions) can debilitate a worker, the model of hardiness provides a buffering or protective effect. For example, during periods of organizational change, efforts to maintain a feeling of control among workers could include increased clarity in work activities and job descriptions, and perceptions of the change as having possibilities, rather than as a loss (Maddi and Kobasa 1984).
Change in Workplace Technology
Work has altered so that in addition to the mental skills required of the professional, technological expertise is expected. The use of the computer, fax, telephone and video-conferencing, electronic mail, audio-visual presentations and other new technology has both changed the function of many managers and created ergonomic and other hazards associated with the machines which assist these functions. The term techno-stress has been coined to describe the impact of the introduction of new information technologies. In 1991 for the first time in history, US companies spent more on computing and communications hardware than on industrial, mining, farm and construction machines.
Computers affect how professional work and work processes are organized today. Such effects can include eye strain, headaches, and other VDU effects. The World Health Organization (WHO) in 1989 reported that psychological and sociological factors are at least as important as physical ergonomics in working with computers. Unintended consequences of computer use include the isolation of the computer operator, and the increase in working with computers in remote locations using high-speed modems. (See also the article “Telework” in this chapter.)
Occupational Stress
A well-known hazard is that of occupational stress, now linked to physiological outcomes, especially cardiovascular diseases. Stress is discussed extensively in several chapters in this Encyclopaedia.
A Swedish study of professional telecommunication engineers suggests that most studies of stress, which have usually been based on low- and medium-skill jobs, are not applicable to skilled professionals. In this study, three stress-reduction interventions were applied to the professional workforce with the following beneficial results: a feeling of being in control of one’s own work (thought to protect against high mental strain work); a lessening of mental strain; a lasting effect on social interactions and support; an improvement in elevated prolactin levels; a lessening of circulating thrombocytes (which may be a factor in stroke); and an improvement in cardiovascular risk indicators (Arnetz 1996).
As the human and financial costs of occupational stress have become known, many organizations have introduced initiatives that reduce stress and improve employee health in the workplace. Such interventions can focus on the individual (relaxation techniques and employee assistance programmes); on the individual-organizational interface (person-environment fit, participation and autonomy); or on the organization (organizational structures, training, selection and placement).
Violence
Managerial and professional workers are at risk for violence and assault because of their visibility and the possibility of adverse reactions to their decisions. Most commonly, violence and assault occur where money changes hands in retail settings or where troubled clients are seen. Workplaces at greatest risk for homicide (in descending order) are taxicab establishments, liquor stores, gas stations, detective services, justice and public order establishments, grocery stores, jewellery stores, hotels/motels, and eating/drinking places. Homicide in the workplace was the leading cause of occupational death for women, and the third leading cause of death for all workers in the United States from the mid-1980s to the mid-1990s (NIOSH 1993; Stout, Jenkins and Pizatella 1989).
Travel Hazards
Approximately 30 million people travelled from industrialized countries to developing countries in 1991, many of these business travellers. One-half of the travellers were US and Canadian residents, most commonly travelling to Mexico. European travellers were 40% of the total, with the majority visiting Africa and Asia. Health risks to international travellers occur when travelling to developing countries with high endemic rates of disease for which the traveller may have low levels of protective antibodies. An example is the hepatitis A virus (HAV), which is transmitted to 3 in 1,000 for the average traveller to developing countries and which increases to 20 in 1,000 people for those who travel to rural areas and were not careful with food and hygiene. Hepatitis A is a food- and water-borne disease. A vaccine is available that was introduced in Switzerland in 1992 and is recommended by the Advisory Committee on Immunization Practices for individuals travelling to areas with a high incidence of HAV (Perry 1996). Background and references for such hazards are provided elsewhere in this Encyclopaedia.
Other travel hazards include motor vehicle accidents (the highest rated cause of workplace fatality in the United States), jet lag due to diurnal disturbances, extended family absences, gastrointestinal disturbances, public transport accidents, crime, terrorism or violence. Traveller advisories for specific hazards are available from disease control agencies and embassies.
Health and Safety Interventions
Measure for the improvement of professional and managerial workers’ working conditions include the following:
- All managerial, supervisory and professional workers should be included in health and safety training on the worksite.
- Worksite smoking cessation programmes are appropriate as they are convenient, allow practice of cessation behaviours during working hours (when they are often most needed to cope with stressful events) and provide incentive to quit smoking.
- Stress- and time-management programmes lead to improved worker satisfaction and productivity.
- Diversity in the workplace will be commonplace in the coming century. Diversity training improves cross-cultural understanding.
- Female professional and managerial staff need workplace support for their demanding roles at home and in the workplace: family leave, support groups and increased opportunities for advancement and control over their work.
- Employee assistance programmes that are non-judgemental and confidential should be provided to all workers.
- Computer work hazards require organizational, environmental, equipment and training emphasis, as well as engineering improvements in workstation, monitor and remote worksite designs.
- Travellers need time to reorient to other time zones and countries, updated health information to protect them, time off to provide for family needs and security protections.
- All workers need engineering, work practice and protective equipment controls to protect against violent acts and assaults by others. Training in personal and office protection should deal with prevention, personal protection, and post-assault help and counselling.
More...
The Nature of Office and Clerical Work
Work Organization and Stress
Office and sales work are traditionally thought of as clean, easy, safe work. While life-threatening, acute injuries are rare in these fields, occupational hazards exist that diminish the quality of life and in some cases, cause serious injury and death.
Stress can be defined as a physical or psychological stimulus that produces strain or disruption of the individual’s normal physiological equilibrium. Stress reactions include headaches, gastro-intestinal and sleep disturbances, high blood pressure and other cardiovascular disease, anxiety, depression and increased use of alcohol and drugs. Work in offices and retail trades is stressful both because of the structure of the industries and because of the organization of work.
The Structure of Work
Employers are increasingly using part-time and temporary workers (“temps” or contract workers). Often, this arrangement provides the desired flexibility in working hours. But there are costs. Government labour statistics show that the average part-time worker in the United States, for example, earns only 60% as much as a full-time worker on an hourly basis. Not only are they paid less, but their benefits, like health insurance, pensions, paid sick leave and vacation, are substantially less than those received by full-time workers. Fewer than 25% of part-time workers have employer-paid health insurance, compared to nearly 80% of full-time workers. Sixty per cent of full-time workers have pensions, while only 25% of part-time workers have this coverage. In 1990 in the US, there were nearly 5 million part-time workers who would have preferred to be employed full time. Other countries are also undergoing similar transformations of work. For example, in the European Union, 15% of the workforce and roughly 20% of clerical and sales worked had part-time jobs in 1991, and 8.4% of clerical workers were temps (De Grip, Hovenberg and Willems 1997).
In addition to lower pay and few benefits, there are other negative aspects of this restructuring of work. Temps often live with the stress of not knowing when they will be working. They also tend to work more overtime because they are often hired for “crunch” periods. Neither part-time workers nor temps receive equal protection under many government laws, including occupational safety and health regulations, unemployment insurance and pension regulations. Few are represented by labour unions. A case study commissioned by the US Occupational Safety and Health Administration of contract labour in the petrochemical industry shows that contract workers get less health and safety training and have higher injury rates than non-contract workers (Murphy and Hurrell 1995). The health consequences of an increasingly non-unionized, temporary workforce should not be underestimated.
Work organization
When the well-known long-term study of heart disease, the US Framingham Heart Study, examined the relationship between employment status and the incidence of coronary heart disease, it found that 21% of women clerical workers develop coronary heart disease, a rate almost twice that of non-clerical workers or housewives. According to Karasek’s demand control model of job stress, work that is characterized by high demands and low control, or decision-making latitude, is the most stressful, because of the imbalance between responsibility and ability to respond (Karasek 1979, 1990). Occupations such as clerical work, electronics manufacturing, garment work and poultry processing are characterized by tedium, ergonomic hazards and low job control. Clerical work ranked among the most stressful in this regard.
Recognizing the social, economic and physical determinants of health effects related to occupational stressors instead of focusing solely on personal pathology is a first step in the complete and long-term management of stress-related problems. While many people may benefit from programmes that provide individual coping and relaxation exercises, workplace stress management programmes should also acknowledge the broader social and economic constraints that provide the context for the daily lives of working people.
Air Quality
Many buildings have serious indoor air pollution problems. In offices, the combination of poor ventilation design, sealed buildings and the build-up of chemicals from building materials, office machines and cigarette smoke has resulted in an office smog in many buildings. Micro-organisms (e.g., moulds, bacteria) can flourish in the air-conditioning and humidifying systems, evaporative condensers and cooling towers in many office buildings. The result may be “tight building syndrome”, which can involve a wide range of symptoms depending on the situation, including allergies and respiratory infections, such as legionnaires’ disease, that sometimes can reach epidemic proportions. Perhaps the most common office air pollutant is cigarette smoke, which can increase the level of respirable particles in the air to 5 times that of a non-smoking office. Since research has linked the cigarette smoking of a spouse with the increased lung cancer risk of a non-smoking spouse, non-smoking office workers may also be at risk.
Ergonomic Hazards
Ergonomic hazards in the retail trade have risen in recent years as new technologies and organizational structures have been introduced. The trend in retail has been towards self-service operations and towards larger retail outlets. The introduction of the electronic scanner has created shorter cycle times and increased repetitiveness. In addition, the work space is often not adapted to the new technology, and many work practices can lead to musculoskeletal stress.
Many studies and investigations have found a higher rate of cumulative trauma disorders in cashiers than in non-cashiers, and a dose-response relationship between the work and these disorders. These jobs usually require high levels of upper extremity activity, and, as a result, carpal tunnel syndrome, tendinitis and tenosynovitis are experienced by a large proportion of cashiers. General merchandise clerks have been shown to have moderate levels of wrist activity and high levels of ankle activity. The check stand design can greatly influence the cashier’s posture and movement patterns, causing awkward positions, long reaches and frequent lifts. As a result other common areas of discomfort are the neck, shoulder, elbow and back. Prolonged standing for cashiers and clerks can also lead to back pain from the compressive forces associated with the activity. Additionally, prolonged standing may cause discomfort in the legs, knees and feet, and varicose veins. Further risk to the back comes from moving stacks which can be too heavy and/or too large.
There are many other sectors within the retail trades that experience these disorders as well as many more. For example, retail floristry and hairdressing are frequently associated with skin problems such as rashes and chronic dermatitis. The most common injuries in eating and drinking establishments are lacerations and burns. Take these factors into account along with the high turnover rate of employees and the inadequate training that can occur as a consequence, and the result is a setting that is conducive to chronic pain, discomfort and eventual cumulative trauma disorders.
Office Trades
The image of white-collar work being safe and clean is often deceptive. The dramatic change in workforce characteristics where job specialization, the repetitiveness of tasks and physical demands have all increased and available work space has decreased has led to many ergonomic injuries and illnesses. The most obvious injuries are associated with safety, such as falls on slippery floors, trips over electrical cords, collisions with open file cabinet drawers and moving heavy objects such as boxes of paper and furniture. However, with the ubiquitous use of computers in offices today, a new pattern of health problems exists. The areas of the body most frequently affected by cumulative trauma disorders are the upper limbs and neck. However, prolonged visual disply unit (VDU) use can lead to inflammation in the muscles, joints and tendons of the back and legs as well. Serious wrist disorders such as carpal tunnel syndrome, tendinitis and tenosynovitis are often associated with VDU use. These conditions can result from continuous wrist extension during keyboard use or from direct mechanical pressure on the wrist from such things as the sharp edge of the desk. Disorders of the fingers may result from the numerous, rapid fine finger movements that occur during typing. Shoulders being held in a static elevated position, resulting from too high a work surface, can possibly lead to tendinitis. As is often the case, prolonged sitting, which is characteristic of VDU use, can reduce the blood circulation and increase blood pooling in the legs and feet as the soft tissue in the legs is compressed. Lower-back pain is often a disorder associated with prolonged sitting, as the compressive forces in the spine can be elevated, especially if the chair is poorly designed. Other common health effects of VDU use are eye strain and headaches from improper lighting or VDU flicker. The computer is rarely the only piece of equipment in large offices. The noise level generated by the combination of copiers, typewriters, printers, phones and the ventilation system is often higher than the 45 to 55 dBA recommended for easy office and phone conservation and can interfere with concentration and elevate annoyance and stress levels, which have been associated with heart disease.
Environmental Hazards
The leading environmental hazards related to office and retail trades are primarily concerned with the consumer society: mall development and groundwater problems related to “green fields” development. In many suburban communities in advanced industrial nations, retail trade and office development in malls threatens the viability of both downtown urban areas and open space in the suburbs. In Asia and Africa the problems are different: along with the vast, unplanned growth of urban areas has come even sharper geographic division of social classes. But in the North and in the South, some cities have become dumping grounds for the poor and disenfranchised, as shopping centres and office complexes—and the more privileged classes—have abandoned urban areas. Neither the work of the future nor the consumption possibilities associated with it are available, and the urban environment has deteriorated accordingly. The new efforts of environmental justice organizations have sharpened the discussion of urban development, living, shopping and work.
The development of offices also presents the problem of wasteful uses of paper. Paper presents a problem of resource depletion (the cutting of forests for paper pulp) and the problem of solid waste. An international campaign against chlorine has also pointed out the chemical hazards associated with paper production. The recycling of paper, however, has captured the imagination of the environmentally conscious, and the paper and pulp industry has been induced to increase production of recycled paper products, as well as to find alternatives to the use of chlorine compounds. Electronic communication and record keeping may very well pose a long-term solution to this problem.
The enormous problem of excess packaging materials is a critical environmental concern. For example, Fresh Kills landfill, New York City’s dump for residential garbage, the largest landfill in the United States, covers about 3,000 acres and receives approximately 14,000 tons of trash a day. At present, in some places, the landfill reaches 150 feet (about 50 m) deep, but is projected to go to 450 feet (about 140 m) in 10 years. This does not include commercial or industrial non-toxic waste. Much of this waste is paper and plastic, which could be recycled. In Germany, producers of goods are required to take back packaging materials. Thus, companies are strongly encouraged to reduce their own wasteful retail marketing practices.
Disregarding Ergonomic Design Principles: Chernobyl
The causes of the 1986 Chernobyl disaster have been variously attributed to the operating personnel, the plant management, the design of the reactor and the lack of adequate safety information in the Soviet nuclear industry. This article considers a number of design faults, operational shortcomings and human errors that combined in the accident. It examines the sequence of events leading up to the accident, design problems in the reactor and cooling rods, and the course of the accident itself. It considers the ergonomics aspects, and expresses the view that the main cause of the accident was inadequate user-machine interaction. Finally, it stresses the continuing inadequacies, and emphasizes that unless the ergonomics lessons are fully learned, a similar disaster could still occur.
The full story of the Chernobyl disaster is yet to be disclosed. To speak candidly, the truth is still veiled by self-serving reticence, half-truths, secrecy and even falsehood. A comprehensive study of the causes of the accident appears to be a very difficult task. The main problem faced by the investigator is the need to reconstruct the accident and the role of the human factors in it on the basis of the tiny bits of information that have been made available for study. The Chernobyl disaster is more than a severe technological accident, part of the reasons for the disaster also lie with the administration and the bureaucracy. However, the chief aim of this article is to consider the design faults, the operational shortcomings and the human errors that combined in the Chernobyl accident.
Who is to blame?
The chief designer for the pressure tube large power boiling water reactors (RBMK) used at the Chernobyl nuclear power plant (NPP), in 1989, presented his view on the causes of the Chernobyl accident. He attributed the disaster to the fact that the personnel failed to observe the correct procedures, or “production discipline”. He pointed out that the lawyers investigating the accident had arrived at the same conclusion. According to his view, “the fault lies with the personnel rather than some design or manufacturing failings.” The research supervisor for the RBMK development supported this view. The possibility of ergonomic inadequacy as a causative factor was not considered.
The operators themselves expressed a different opinion. The shift supervisor of the fourth unit, A.F. Akimov, when dying in a hospital as a result of receiving a dose of radiation of more than 1,500 rads (R) in a short period of time during the accident, kept telling his parents that his actions had been correct and he could not understand what had gone wrong. His persistence reflected absolute trust in a reactor that was supposedly completely safe. Akimov also said that he had nothing to blame his crew for. The operators were sure that their actions were in accord with regulations, and the latter did not mention the eventuality of an explosion at all. (Remarkably, the possibility of the reactor’s becoming dangerous under certain conditions was introduced into the safety regulations only after the Chernobyl accident.) However, in light of design problems revealed subsequently, it is significant that the operators could not understand why inserting rods into the core caused such a terrible explosion instead of instantly stopping the nuclear reaction as designed. In other words, in this case they acted correctly according to the maintenance instructions and to their mental model of the reactor system, but the design of the system failed to correspond to that model.
Six persons, representing only the plant management, were convicted, in view of the human losses, on the grounds of having violated safety regulations for potentially explosive facilities. The chairman presiding over the court said some words to the effect of proceeding with the investigations as regards “those who failed to take measures to improve the plant design”. He also mentioned the responsibility of department officials, local authorities and medical services. But, in fact, it was clear that the case was closed. Nobody else was held responsible for the greatest disaster in the history of nuclear technology.
However, it is necessary to investigate all causative factors that combined in the disaster to learn important lessons for safe future operation of NPPs.
Secrecy: The information monopoly in research and industry
The failure of the user-machine relationship that resulted in “Chernobyl-86” can be attributed in some measure to the policy of secrecy—the enforcement of an information monopoly—that governed technological communication in the Soviet nuclear energy establishment. A small group of scientists and researchers were given an exhaustive right to define the basic principles and procedures in nuclear power, a monopoly reliably protected by the policy of secrecy. As a result, reassurances by Soviet scientists as regards the absolute safety of NPPs remained unchallenged for 35 years, and secrecy veiled the incompetence of the civil nuclear leaders. Incidentally, it became known recently that this secrecy was extended to information relating to the Three Mile Island accident as well; the operating personnel of Soviet NPPs were not fully informed about this accident—only selected items of information, which did not contradict the official view on NPP safety, were made known. A report on the human engineering aspects of the Three Mile Island accident, presented by the author of this paper in 1985, was not distributed to those involved with safety and reliability of NPPs.
No Soviet nuclear accidents were ever made public except for the accidents at the Armenian and Chernobyl (1982) nuclear power plants, which were casually mentioned in the newspaper Pravda. By concealing the true state of affairs (thus failing to make use of lessons based on the accident analyses) the leaders of the nuclear power industry were setting it straight on the path to Chernobyl-86, a path that was further smoothed by the fact that a simplified idea of the operator activities had been implanted and the risk of operating NPPs was underestimated.
As a member of the State Expert Committee on the Consequences of the Chernobyl accident stated in 1990: “To err no more, we have to admit all our errors and analyse them. It is essential to determine which errors were due to our inexperience and which ones were actually a deliberate attempt to hide the truth.”
The Chernobyl Accident of 1986
Faulty planning of the test
On 25 April 1986, the fourth unit of the Chernobyl NPP (Chernobyl 4) was being prepared for routine maintenance. The plan was to shut the unit down and perform an experiment involving inoperative safety systems totally deprived of power from normal sources. This test should have been carried out before the initial Chernobyl 4 startup. However, the State Committee was in such a hurry to start up the unit that they decided to postpone indefinitely some “insignificant” tests. The Acceptance Certificate was signed at the end of 1982. Hence, the deputy chief engineer was acting according to the earlier plan, which presupposed a wholly inactive unit; his planning and timing of the test proceeded according to this implicit assumption. This test was in no way carried out on his own initiative.
The programme of the test was approved by the chief engineer. The power during the test was supposed to be generated from the rundown energy of the turbine rotor (during its inertia-induced rotation). When still rotating, the rotor provides electric power generation which could be used in an emergency. Total loss of power at a nuclear plant causes all mechanisms to stop, including the pumps which provide for the coolant circulation in the core, which in turn results in core meltdown—a grave accident. The above experiment was aimed at testing the possibility of using some other available means—the inertial rotation of the turbine—to produce power. It is not forbidden to perform such tests at operating plants provided that an adequate procedure has been developed and additional safety precautions have been worked out. The programme must ensure that a back-up power supply for the whole test period is provided. In other words, the loss of power is only implied but never actualized. The test may be performed only after the reactor is shut down, that is, when the “scram” button is pushed and the absorbing rods are inserted in the core. Prior to this, the reactor must be in a stable controlled condition with the reactivity margin specified in the operating procedure, with at least 28 to 30 absorbing rods inserted in the core.
The programme approved by the chief engineer of the Chernobyl plant satisfied none of the above requirements. Moreover, it called for the shutting off of the emergency core cooling system (ECCS), thus jeopardizing the safety of the plant for the whole test period (about four hours). When developing the programme, the initiators took into account the possibility of triggering the ECCS, an eventuality which would have prevented them from completing the rundown test. The bleed-off method was not specified in the programme since the turbine no longer needed steam. Clearly, the people involved were completely ignorant of reactor physics. The nuclear power leaders obviously included similarly unqualified people as well, which would account for the fact that when the above programme was submitted for approval to the responsible authorities in January 1986, it was never commented on by them in any way. The dulled feeling of danger also made its contribution. Owing to the policy of secrecy surrounding nuclear technology the opinion had formed that nuclear power plants were safe and reliable, and that their operation was accident-free. Lack of official response to the programme did not, however, alert the director of the Chernobyl plant to the possibility of danger. He decided to proceed with the test using the uncertified programme, even though it was not permitted.
Change in the test programme
While performing the test, the personnel violated the programme itself, thus creating further possibilities for an accident. The Chernobyl personnel committed six gross errors and violations. According to the programme the ECCS was made inoperative, this being one of the gravest and most fatal errors. The feedwater control valves had been cut off and locked beforehand so that it would be impossible even to open them manually. The emergency cooling was deliberately put out of action in order to prevent possible thermal shock resulting from cold water entering the hot core. This decision was based on the firm belief that the reactor would hold out. The “faith” in the reactor was strengthened by the comparatively trouble-free ten years’ operation of the plant. Even a serious warning, the partial core meltdown at the first Chernobyl unit in September 1982, was ignored.
According to the test programme the rotor rundown was to be carried out at a power level of 700 to 1000 MWth (megawatts of thermal power). Such a rundown should have been performed as the reactor was being shut down, but the other, disastrous, way was chosen: to proceed with the test with the reactor still operating. This was done to ensure the “purity” of the experiment.
In certain operating conditions, it becomes necessary to change or turn off a local control for clusters of absorbing rods. When turning off one of these local systems (the means of doing this are specified in the procedure for low-power operation), the senior reactor control engineer was slow to correct the imbalance in the control system. As a result, the power fell below 30 MWth which led to fission-product reactor poisoning (with xenon and iodine). In such an event, it is next to impossible to restore normal conditions without interrupting the test and waiting a day until the poisoning is overcome. The deputy chief engineer for operations did not want to interrupt the test and, by means of shouting at them, forced the control-room operators to begin raising the power level (which had been stabilized at 200 MWth). The reactor poisoning continued, but further power increase was impermissible owing to the small operating reactivity margin of only 30 rods for a large power pressure-tube reactor (RBMK). The reactor became practically uncontrollable and potentially explosive because, in trying to overcome the poisoning, the operators withdrew several rods needed to maintain the reactivity safety margin, thus making the scram system ineffective. Nevertheless, it was decided to proceed with the test. Operator behaviour was evidently motivated mainly by the desire to complete the test as soon as possible.
Problems due to the inadequate design of the reactor and absorbing rods
To give a better understanding of the causes of the accident, it is necessary to point out the major design deficiencies of the absorbing rods of the control and scram system. The core height is 7 m, while the absorbing length of the rods amounts to 5 m with 1 m hollow parts above and below it. The bottom ends of the absorbing rods, which go under the core when fully inserted, are filled with graphite. Given such a design, the control rods enter the core followed by one-metre hollow parts and, finally, come the absorbing parts.
At Chernobyl 4 , there were a total of 211 absorbing rods, 205 of which were fully withdrawn. Simultaneous reinsertion of so many rods initially results in reactivity overshoot (a peak in fission activity), since at first the graphite ends and hollow parts enter the core. In a stable controlled reactor such a burst is nothing to worry about, but in the event of a combination of adverse conditions, such an addition may prove fatal since it leads to prompt neutron reactor runaway. The immediate cause of initial reactivity growth was the initiation of water boiling in the core. This initial reactivity growth reflected one particular drawback: a positive steam void coefficient, which resulted from the core design. This design deficiency is one of the faults which caused operator errors.
Grave design faults in the reactor and the absorbing rods actually predetermined the Chernobyl accident. In 1975, after the accident at the Leningrad plant, and later on, specialists warned about the possibility of another accident in view of deficiencies in core design. Six months before the Chernobyl disaster, a safety inspector at the Kursk plant sent a letter to Moscow in which he pointed out to the chief researcher and chief designer certain design inadequacies of the reactor and the control and protection system rods. The State Supervising Committee for Nuclear Power, however, called his argument groundless.
The course of the accident itself
The course of the events was as follows. With the onset of the reactor coolant pump cavitation, which led to reduced flow rate in the core, the coolant boiled in the pressure tubes. Just then, the shift supervisor pushed the button of the scram system. In response, all the control rods (which had been withdrawn) and the scram rods dropped into the core. However, first to enter the core were the graphite and hollow ends of the rods, which cause reactivity growth; and they entered the core just at the beginning of intensive steam generation. The rise of the core temperature also produced the same effect. Thus there were combined three conditions unfavourable for the core. Immediate reactor runaway began. This was due primarily to gross design deficiencies of the RBMK. It should be recalled here that the ECCS had been made inoperative, locked and sealed.
The subsequent events are well known. The reactor was damaged. The major part of the fuel, graphite and other in-core components were blown out. Radiation levels in the vicinity of the damaged unit amounted to 1,000 to 15,000 R/h, although there were some more distant or sheltered areas where radiation levels were considerably lower.
At first the personnel failed to realize what had happened and just kept on saying, “It is impossible! Everything was done properly.”
Ergonomics considerations in connection with the Soviet report on the accident
The report presented by the Soviet delegation at the International Atomic Energy Association (IAEA) meeting in summer 1986 evidently gave truthful information on the Chernobyl explosion, but a doubt keeps on returning as to whether the emphasis was put in the right places and whether the design inadequacies were not treated much too gently. The report stated that the behaviour of the personnel was caused by the desire to complete the test as soon as possible. Judging from the facts that the personnel violated the procedure for preparing and carrying out tests, violated the test programme itself, and were careless when performing the reactor control, it would seem that the operators were not fully aware of the processes taking place in the reactor and had lost all feeling of danger. According to the report:
The reactor designers failed to provide safety systems designed to prevent an accident in the case of deliberate shut-off of the engineered safety means combined with violations of the operating procedures since they regarded such a combination as unlikely. Hence the initial cause of the accident was a very unlikely violation of the operating procedure and conditions by the plant personnel.
It has become known that in the initial text of the report the words “plant personnel” were followed by the phrase “which showed the design faults of the reactor and the control and protection system rods”.
The designers considered the interference of “clever fools” in plant control unlikely, and therefore failed to develop the corresponding engineered safety mechanisms. Given the phrase in the report stating that the designers considered the actual combination of events unlikely, some questions arise: Had the designers considered all possible situations associated with human activity at the plant? If the answer is positive, then how were they taken into account in the plant design? Unfortunately, the answer to the first question is negative, leaving areas of user-machine interaction undetermined. As a result, onsite emergency training and theoretical and practical training were carried out mainly within a primitive control algorithm.
Ergonomics was not used when designing computer-assisted control systems and control rooms for nuclear plants. As a particularly serious example, an essential parameter indicative of the core state, that is, the number of the control and protection system rods in the core, was displayed on the control board of Chernobyl 4 in a manner inappropriate for perception and comprehension. This inadequacy was overcome only by operator experience in interpreting displays.
Project miscalculations and ignoring human factors had created a delayed-action bomb. It should be emphasized that the design fault of the core and the control system served as a fatal basis for further erroneous actions by operators, and thus the main cause of the accident was the inadequate design of user-machine interaction. Investigators of the disaster called for “respect to human engineering and man-machine interaction, it being the lesson Chernobyl taught us.” Unfortunately, it is difficult to abandon old approaches and stereotyped thinking.
As early as 1976, academician P.L. Kapitza seemed to foresee a disaster for reasons that might have been relevant to preventing a Chernobyl, but his concerns were made known only in 1989. In February 1976, US News and World Report, a weekly news magazine, published a report on the fire at the Browns Ferry nuclear facility in California. Kapitza was so concerned about this accident that he mentioned it in his own report, “Global problems and energy”, delivered in Stockholm in May 1976. Kapitza said in particular:
The accident highlighted the inadequacy of the mathematical methods used to calculate the probability of such events, since these methods do not take into account the probability due to human errors. To solve this problem, it is necessary to take measures to prevent any nuclear accident from taking on a disastrous course.
Kapitza tried to publish his paper in the magazine Nauka i Zhizn (Science and Life), but the paper was rejected on the grounds that it was not advisable “to frighten the public”. The Swedish magazine Ambio had asked Kapitza for his paper but in the long run did not publish it either.
The Academy of Sciences assured Kapitza that there could be no such accidents in the USSR and as an ultimate “proof” gave him the just published Safety Rules for NPPs. These rules contained, for example, such items as “8.1. The actions of the personnel in case of a nuclear accident are determined by the procedure for dealing with the consequences of the accident”!
After Chernobyl
As a direct or indirect consequence of the Chernobyl accident, measures are being developed and put into effect to ensure safe operation of current NPPs and to improve the design and construction of future ones. In particular, measures have been taken to make the scram system more fast-operating and to exclude any possibility of its being deliberately shut off by the personnel. The design of the absorbing rods has been modified and they have been made more numerous.
Furthermore, the pre-Chernobyl procedure for abnormal conditions instructed operators to keep the reactor operating, while according to the current one the reactor must be shut down. New reactors that, basically speaking, are in fact inherently safe are being developed. There have appeared new areas of research which were either ignored or non-existent before Chernobyl, including probabilistic safety analysis and experimental safety bench tests.
However, according to the former USSR Minister of Nuclear Power and Industry, V. Konovalov, the number of failures, shutdowns and incidents at nuclear power plants is still high. Studies show that this is due mainly to the poor quality of the delivered components, to human error and to inadequate solutions by design and engineering bodies. The quality of construction and installation work leaves much to be desired as well.
Various modifications and design changes have become common practice. As a result, and in combination with inadequate training, qualifications of the operating personnel are low. The personnel have to improve their knowledge and skills in the course of their work, based on their experience in plant operation.
Ergonomics lessons are still to be learned
Even the most effective, sophisticated safety control system will fail to provide for plant reliability if human factors are not taken into account. Work is being prepared for the vocational training of personnel in the All-Union Scientific and Research Institute of NPPs, and there are plans to considerably enlarge this effort. It should be admitted, however, that human engineering still is not an integral part of plant design, construction, testing and operation.
The former USSR Ministry of Nuclear Power replied in 1988 to an official inquiry that in the period 1990-2000 there was no need for specialists in human engineering with secondary and higher education as there were no corresponding requests for such personnel from nuclear plants and enterprises.
To solve many of the problems mentioned in this article it is necessary to carry out combined research and development involving physicists, designers, industrial engineers, operating personnel, specialists in human engineering, psychology and other fields. Organizing such joint work entails great difficulties, one particular difficulty being the remaining monopoly of some scientists and groups of scientists on “truth” in the field of nuclear energy and the monopoly of the operating personnel on the information concerning NPP operation. Without available comprehensive information, it is impossible to give a human engineering diagnosis of a NPP and, if necessary, propose ways to eliminate its shortcomings as well as to develop a system of measures to prevent accidents.
In the NPPs of the former Soviet Union the current means for diagnosis, control and computerization are far from accepted international standards; plant control methods are needlessly complicated and confusing; there are no advanced programmes of personnel training; there is poor support of plant operation by designers and highly outdated formats for operating manuals.
Conclusions
In September 1990, after further investigations, two former Chernobyl employees were freed from prison before the end of their terms. Some time later all the imprisoned operating personnel were freed before the appointed time. Many people involved with the reliability and safety of NPPs now believe that the personnel had acted correctly, even though these correct actions resulted in the explosion. The Chernobyl personnel cannot be held responsible for the unexpected magnitude of the accident.
In an attempt to identify those who were responsible for the disaster, the court mainly relied on the opinion of technical specialists who, in this case, were the designers of Chernobyl nuclear power plant. As a result of this one more important Chernobyl lesson is learned: As long as the main legal document that is used to identify responsibility for disasters at such complicated establishments as NPP is something like maintenance instructions produced and changed exclusively by designers of these establishments, it is too technically difficult to find the real reasons for disasters, as well as to take all the necessary precautions to avoid them.
Further, a question still remains as to whether operating personnel should strictly follow the maintenance instructions in the case of disaster or whether they should act according to their knowledge, experience or intuition, which may even contradict the instructions or be unconsciously associated with the threat of severe punishment.
We must state, regrettably, that the question “Who is guilty of the Chernobyl accident?” has not been cleared up. Those responsible should be sought among politicians, physicists, administrators and operators, as well as among development engineers. Convicting mere “switchmen” as in the Chernobyl case, or having clergymen sanctify NPPs with holy water, such as was done with the incident-plagued unit in Smolensk in 1991, cannot be the correct measures to ensure safe and reliable operation of NPPs.
Those considering the Chernobyl disaster merely an unfortunate nuisance of a sort which will never happen again, have to realize that one basic human characteristic is that people do make mistakes—not only operating personnel but also scientists and engineers. Ignoring ergonomic principles about user-machine interactions in any technical or industrial field will result in more frequent and more severe errors.
It is therefore necessary to design technical facilities such as NPPs in such a way that possible errors are discovered before a severe accident can happen. Many ergonomic principles have been derived trying to prevent errors in the first place, for instance in the design of indicators and controls. However, still today these principles are violated in many technical facilities all over the world.
The operating personnel of complex facilities need to be highly qualified, not only for the routine operations but also in the procedures necessary in the case of a deviation from normal status. A sound understanding of the physics and the technologies involved will help the personnel to react better under critical conditions. Such qualifications can only be attained through intensive training.
The constant improvements of user-machine interfaces in all kinds of technical applications, often as a result of minor or major accidents, show that the problem of human errors and thus of user-machine interaction is far from being solved. Continuous ergonomic research and the consequent application of the obtained results aimed at making user-machine interaction more reliable is necessary, especially with technologies that bear a highly destructive power, such as nuclear power. Chernobyl is a severe warning of what can happen if people—scientists and engineers, as well as administrators and politicians—disregard the necessity of including ergonomics in the process of designing and operating complex technical facilities.
Hans Blix, Director General of the IAEA, has stressed this problem with an important comparison. It has been said that the problem of war is much too serious to be left solely to generals. Blix added “that the problems of nuclear power are much too serious to leave them solely to nuclear experts”.
System Design in Diamond Manufacturing
The author acknowledges the assistance of Mr. E. Messer and Prof. W. Laurig for their contribution to the biomechanical and design aspects, and to Prof. H. Stein and Dr. R. Langer for their help with the physiological aspects of the polishing process. The research was supported by a grant from the Committee for Research and Prevention in Occupational Safety and Health, Ministry of Labor and Social Affairs, Israel.
The design of manually operated work benches and working methods in the diamond polishing industry has not changed for hundreds of years. Occupational health studies of diamond polishers have identified high rates of musculoskeletal disorders of the hands and arms, specifically, ulnar neuropathy at the elbow. These are due to the high musculoskeletal demands placed on the upper body in the practice of this manually intensive profession. A study conducted at the Technion Israel Institute of Technology addressed itself to the investigation of the ergonomic aspects and occupational diseases relating to safety issues among craftsmen in the diamond polishing industry. The tasks in this industry, with its high demands for manipulative movements, include movements that require frequent, rapid hand exertions. An epidemiological review conducted during the years 1989-1992 in the Israeli diamond industry has pointed out that the manipulative movements experienced in diamond polishing very often cause serious health problems to the worker in the upper extremities and in the upper and lower back. When such occupational hazards affect workers, it produces a chain reaction that eventually affects the industry’s economy as well.
For thousands of years, diamonds have been objects of fascination, beauty, richness and capital value. Skillful craftsmen and artists have tried, through the ages, to create beauty by enhancing the shape and values of this unique form of hard carbon crystal formation. In contrast to the continuing achievements of artistic creation with the native stone and the emergence of a great international industry, very little has been done to improve some questionable working conditions. A survey of the diamond museums in England, South Africa and Israel allows one to draw the historical conclusion that the traditional polishing workplace has not changed for hundreds of years. The typical diamond polishing tools, working bench and work processes are described by Vleeschdrager (1986), and they have been found to be universally common to all polishing setups.
Ergonomic evaluation performed at diamond manufacturing setups points to a great lack of engineering design of the polishing workstation, which causes back pain and neck and arm stress due to working posture. A micromotion study and biomechanical analysis of motion patterns involved in the diamond polishing profession indicate extremely intense hand and arm movements that involve high acceleration, rapid movement and a great degree of repetitiveness in short-period cycles. A symptom survey of diamond polishers indicated that 45% of the polishers were younger than 40 years of age, and although they represent a young and healthy population, 64% reported pain in the shoulders, 36% pain in the upper arm and 27% pain in the lower arm. The act of polishing is performed under an extensive amount of “hand on tool” pressure which is applied to a vibrating polishing disk.
The first known description of a diamond polishing workstation was given in 1568 by the Italian goldsmith, Benvenuto Cellini, who wrote: “One diamond is rubbed against another until by mutual abrasion both take a form which the skilled polisher wishes to achieve.” Cellini’s description could have been written today: the role of the human operator has not changed over these 400 years. If one examines the working routines, hand tools and the nature of the decisions involved in the process one can see that the user-machine relationship has also hardly changed. This situation is unique among most industries where enormous changes have occurred with the entry of automation, robotics and computer systems; these have completely changed the role of the worker in the world today. Yet the polishing work cycle has been found to be very similar, not only in Europe where the polishing craft started, but in most industries all over the globe, whether in advanced facilities in the United States, Belgium or Israel—which specialize in fancy geometry and higher-value diamond products—or the facilities in India, China and Thailand, which generally produce popular shapes and mid-value products.
The polishing process is based on grinding the fixed rough diamond over diamond dust bonded to the polishing disk’s surface. Owing to its hardness, only grinding by friction against similar carbon material is effective in manipulating the diamond’s shape to its geometric and brilliant finish. The workstation hardware is composed of two basic groups of elements: workstation mechanisms and hand-held tools. The first group includes an electric motor, which rotates a polishing disk on a vertical cylindrical shaft, perhaps by a single direct drive; a solid flat table which surrounds the polishing disk; a bench seat and a source of light. The hand-held operating tools consist of a diamond holder (or tang) which houses the rough stone during all polishing phases and is usually held in the left palm. The work is magnified with a convex lens which is held between the first, second and third fingers of the right hand and viewed with the left eye. This method of operation is imposed by a strict training process which in most cases does not take handedness into account. During work the polisher assumes a reclining posture, pressing the holder to the grinding disk. This posture requires the support of the arms on the working table in order to stabilize the hands. As a result, the ulnar nerve is vulnerable to external lesions due to its anatomical position. Such an injury is common among diamond polishers and has been accepted as an occupational disease since the 1950s. The number of polishers worldwide today is around 450,000, of whom approximately 75% are located in the Far East, primarily India, which has dramatically expanded its diamond industry in the last two decades. The act of polishing is done manually, with each of the diamond facets being produced by polishers who are trained and skilled with respect to a certain part of the stone’s geometry. The polishers are a clear majority of the diamond craft force, composing about 80% of the overall industry’s workforce. Therefore, most of the occupational risks of this industry can be addressed through improving the operation of the diamond polishing workstation.
Analysis of the motion patterns involved in polishing shows that the polishing routine consists of two subroutines: a simpler routine called the polish cycle, which represents the basic diamond polishing operation, and a more important one called the facet cycle, which involves a final inspection and a change of the stone’s position in the holder. The overall procedure includes four basic work elements:
- Polishing. This is simply the actual polishing operation.
- Inspection. Every few seconds the operator, using a magnifying glass, visually inspects the progress made on the polished facet.
- Dop adjustment. An angular adjustment is made to the diamond holder’s head (dop).
- Stone change. The act of changing facets, which is done by turning the diamond through a predetermined angle. It takes about 25 repetitions of these four elements to polish a diamond’s facet. The number of such repetitions depends upon such aspects as operator’s age, stone hardness and characteristics, time of day (owing to operator fatigue), and so on. On average, each repetition takes about four seconds. A micromotion study as performed on the polishing process and the methodology used is given by Gilad (1993).
Two of the elements—polishing and inspection—are performed in relatively static working postures while so-called “hand to polish” (H to P) and “hand to inspect” (H to I) actions require short and fast movements of the shoulder, elbow and wrist. Most of the actual movements of both hands are performed by flexion and extension of the elbow and pronation and supination of the elbow. Body posture (back and neck) and all other movements except wrist deviation are relatively unchanged during normal work. The stone holder, which is constructed of a square cross-sectional steel rod, is held so that it presses on blood vessels and bone, which can result in a reduction of blood flow to the ring and little fingers. The right hand holds the magnifying glass all during the polishing cycle, exerting isometric pressure on the three first fingers. For most of the time the right and left hands follow parallel movement patterns, while in the “hand to grind” movement the left hand leads and the right hand starts moving after a short delay, and in the “hand to inspect” movement the order is reversed. Right-hand tasks involve either holding the magnifying glass to the inspecting left eye while supporting the left hand (elbow flexion), or by putting pressure on the diamond holder head for better grinding (elbow extension). These fast movements result in rapid accelerations and decelerations that end up in a very precise placing of the stone on the grinding disk, which requires a high level of manual dexterity. It should be noted that it takes long years to become proficient to the point where work movements are almost embedded reflexes executed automatically.
On the face of it, diamond polishing is a simple straightforward task, and in a way it is, but it requires much skill and experience. In contrast to all other industries, where raw and processed material is controlled and manufactured according to exact specifications, the diamond in the rough is not homogeneous and each diamond crystal, large or small, has to be checked, categorized and treated individually. Apart from the needed manual skill, the polisher has to make operational decisions at every polishing phase. As a result of the visual inspection, decisions must be made on such factors as angular spatial correction—a three-dimensional judgment—amount and duration of pressure to be applied, angular positioning of the stone, contact point on the grinding disk, among others. Many points of significance have to be considered, all in the average time of four seconds. it is important to understand this decision-making process when improvements are designed.
Before one can advance to the stage at which motion analysis can be used for setting better ergonomic design and engineering criteria for a polishing workstation, one has to be aware of yet further aspects involved in this unique user-machine system. In this post-automation age, we still find the production part of the successful and expanding diamond industry almost untouched by the enormous technological advances made in the last few decades. While almost all other sectors of industry have undergone continuing technology change that defined not only production methods but the products themselves, the diamond industry has remained virtually static. A plausible reason for this stability may be the fact that neither the product nor the market have changed through the ages. The design and shapes of diamonds have in practice remained almost unchanged. From the business point of view, there was no reason to change the product or the methods. Furthermore, since most of the polishing work is done by subcontracting to individual workers, the industry had no problem in regulating the labour force, adjusting the flow of work and the supply of rough diamonds according to market fluctuations. As long as the production methods do not change, the product will not change either. Once the use of more advanced technology and automation are adopted by the diamond industry, the product will change, with a greater variety of forms available in the market. But a diamond still has a mystic quality that sets it apart from other products, a value that may well decrease when it comes to be regarded as merely another mass-produced item. Recently though, market pressures and the arrival of new production centres, mainly in the Far East, are challenging the old established European centres. These are forcing the industry to examine new methods and production systems and the role of the human operator.
When considering improving the polishing workstation, one must look upon it as part of a user-machine system that is governed by three main factors: the human factor, the technology factor and the business factor. A new design that takes account of ergonomic principles will provide a springboard to a better production cell in the broad sense of the term, meaning comfort over long working hours, a better quality product and higher production rates. Two different design approaches have been considered. One involves a redesign of the existing workstation, with the worker given the same tasks to perform. The second approach is to look at the polishing task in an unbiased manner, aiming at an optimal, total station and task design. A total design should not be based on the present workstation as input but on the future polishing task, generating design solutions that integrate and optimize the needs of the three above-mentioned system factors.
At present, the human operator performs most of the tasks involved in the polishing act. These human-performed tasks rely on “filling” and working experience. This is a complex psychophysiological process, only partially conscious, based on trial and error input which enables an operator to execute complex operations with a good prediction of the outcome. During periodic daily work cycles of thousands of identical movements, “filling” manifests itself in the human-automatic operation of motor memory executed with great precision. For each of these automatic motions, tiny corrections are made in response to feedback received from the human sensors, like the eyes, and the pressure sensors. In any future diamond polishing workstation these tasks will continue to be performed in a different way. As to the material itself, in the diamond industry, by contrast with most other industries, the relative value of the raw material is very high. This fact explains the importance of making maximal use of the rough diamond’s volume (or stone weight) in order to get the largest net stone possible after polishing. This emphasis is paramount throughout all the stages of diamond processing. Productivity and efficiency are not measured by reference to time only, but also by the size and precision achieved.
The four repetitive work elements—“polish”, “hand to inspect”, “inspect” and “hand to polish”—as performed in the polishing act, can be classified under the three main task categories: motor tasks for motion elements, visual tasks as sensing elements, and control and management as decision-content elements. Gilad and Messer (1992) discuss design considerations for an ergonomic workstation. Figure 1 presents an outline of an advanced polishing-cell. Only the general construction is indicated, since the details of such a design are guarded as a professionally restricted “know-how”. The term polishing cell is used since this user-machine system includes a totally different approach to polishing diamonds. In addition to ergonomic improvements, the system consists of mechanical and optoelectronic devices that enable the manufacture of three to five stones at the same time. Parts of visual and control tasks have been transferred to technical operators and management of the production cell is mediated via a display unit that provides momentary information about geometry, weight and optional operation moves in order to support optimal operating acts. Such a design takes the polishing workstation a few steps ahead into modernization, incorporating an expert system and a visual control system to replace the human eye in all routine work. Operators will still be able to intervene at any point, set up data and make human judgements on machine performance. The mechanical manipulator and the expert system will form a closed-loop system capable of performing all polishing tasks. Material handling, quality control and final approval will still reside with the operator. At this stage of an advanced system, it would be appropriate to consider the employment of higher technology such as a laser polisher. At present, lasers are being used extensively to saw and cut diamonds. Using a technologically advanced system will radically change the human task description. The need for skilled polishers will diminish until they will deal only with polishing larger, top-valued diamonds, probably with supervision.
Figure 1. Schematic presentation of a polishing-cell
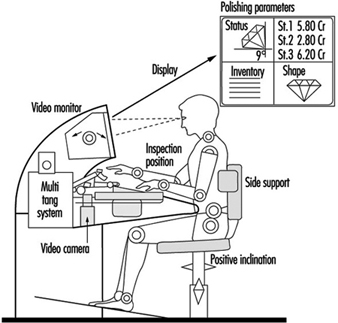
Workers with Special Needs
Designing for Disabled Persons is Designing for Everyone
There are so many products on the market that readily reveal their unfitness for the general population of users. What evaluation should one make of a doorway too narrow to comfortably accommodate a stout person or pregnant woman? Shall its physical design be faulted if it satisfies all relevant tests of mechanical function? Certainly such users cannot be regarded as disabled in any physical sense, since they may be in a state of perfect health. Some products need considerable handling before one can force them to perform as desired—certain inexpensive can openers come, not altogether trivially, to mind. Yet a healthy person who may experience difficulty operating such devices need not be considered disabled. A designer who successfully incorporates considerations of human interaction with the product enhances the functional utility of his or her design. In the absence of good functional design, people with a minor disability may find themselves in the position of being severely hampered. It is thus the user-machine interface that determines the value of design for all users.
It is a truism to remind oneself that technology exists to serve human beings; its use is to enlarge their own capabilities. For disabled persons, this enlargement has to be taken some steps further. For instance in the 1980s, a good deal of attention was paid to the design of kitchens for disabled people. The experience gained in this work penetrated design features for “normal” kitchens; the disabled person in this sense may be considered a pioneer. Occupationally-induced impairments and disabilities—one has but to consider the musculoskeletal and other complaints suffered by those confined to sedentary tasks so common in the new workplace—similarly call for design efforts aimed not only also preventing the recurrence of such conditions, but at the development of user-compatible technology adapted to the needs of workers already affected by work-related disorders.
The Broader Average Person
The designer should not focus on a small, unrepresentative population. Among certain groups it is most unwise to entertain assumptions concerning similarities among them. For example, a worker injured in a certain way as an adult may not necessarily be anthropometrically quite so different from an otherwise comparable, healthy person, and may be considered as part of the broad average. A young child so injured will display a considerably different anthropometry as an adult since his muscular and mechanical development will be steadily and sequentially influenced by preceding growth stages. (No conclusions as to comparability as adults ought to be ventured as regards the two cases. They must be regarded as two distinct, specific groups, only the one being included among the broad average.) But as one strives for a design suitable for, say, 90% of the population, one should exert fractionally greater pains to increase this margin to, say, 95%, the point being that in this way the need for design for specific groups can be reduced.
Another way to approach design for the broader average population is to produce two products, each one designed roughly to fit the two percentile extremes of human differences. Two sizes of chair, for instance, might be built, the one with brackets allowing it to be adjusted in height from 38 to 46 cm, and the other one from 46 to 54 cm; two sizes of pliers already exist, one fitting larger and average sizes of men’s hands and the other fitting average women’s hands and hands of smaller men.
It would be a well-advised company policy to reserve annually a modest amount of money to have worksites analysed and made more suitable for workers, a move that would prevent illness and disability due to excessive physical load. It also increases the motivation of workers when they understand that management is actively trying to improve their work environment, and more impressively so when elaborate measures sometimes have to be undertaken: thorough work analysis, the construction of mock-ups, anthropometrical measurements, and even the specific design of units for the workers. In a certain company, in fact, the conclusion was that the units should be redesigned at every worksite because they caused physical overload in the form of too much standing, there were unsuitable dimensions associated with the seated positions, and there were other deficiencies as well.
Costs, Benefits and Usability of Design
Cost/benefit analyses are developed by ergonomists in order to gain insight into the results of ergonomic policies other than those that are economic. In the present day, evaluation in the industrial and commercial realms includes the negative or positive impact of a policy on the worker.
Methods of evaluating quality and usability are currently the subject of active research. The Rehabilitation Technology Useability Model (RTUM), as shown in figure 1, can be utilized as a model for evaluating the usability of a product within rehabilitation technology and to illuminate the various aspects of the product which determine its usability.
Figure 1. The Rehabilitation Technology Useability Model (RTUM)
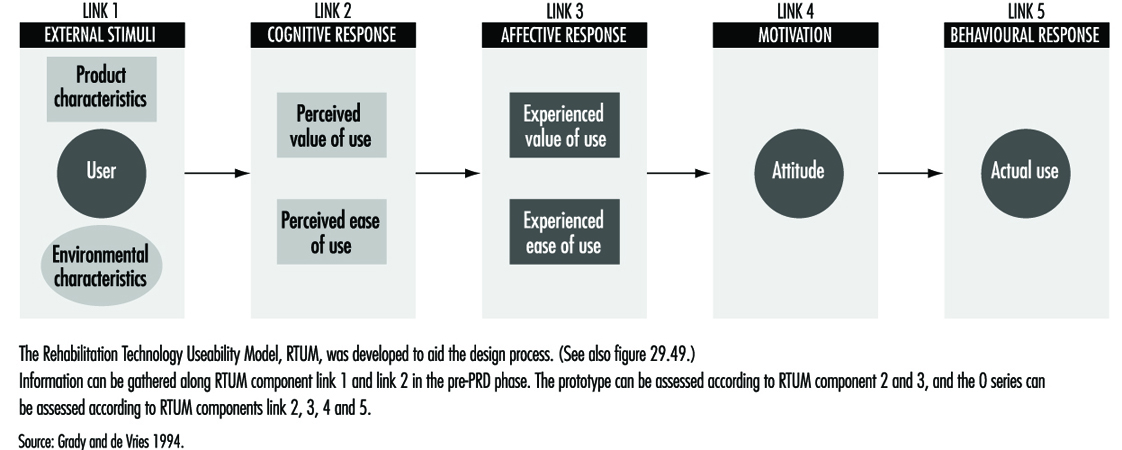
From the strictly economic point of view, the costs of creating a system in which a given task can be performed or in which a certain product can be made can be specified; it scarcely needs mentioning that in these terms each company is interested in a maximum return on its investment. But how can the real costs of task performance and product manufacturing in relation to financial investment be determined when one takes into account the varying exertions of workers’ physical, cognitive and mental systems? In fact, the judging of human performance itself is, among other factors, based on the workers’ perception of what has to be done, their view of their own value in doing it, and their opinion of the company. It is actually the intrinsic satisfaction with work that is the norm of value in this context, and this satisfaction, together with the aims of the company, constitute one’s reason for performing. Worker well-being and performance are thus based on a wide spectrum of experiences, associations and perceptions that determine attitudes towards work and the ultimate quality of performance—an understanding upon which the RTUM model is predicated.
If one does not accept this view, it becomes necessary to regard investment only in relation to doubtful and unspecified results. If ergonomists and physicians wish to improve the work environment of disabled people—to produce more from machine operations and enhance the usability of the tools used—they will encounter difficulties in finding ways to justify the financial investment. Typically, such justification has been sought in savings realized by prevention of injury and illness due to work. But if the costs of illness have been borne not by the company but by the state, they become financially invisible, so to speak, and are not seen as work-related.
Nevertheless, the awareness that investment in a healthy working environment is money well spent has been growing with the recognition that the “social” costs of incapacities are translatable in terms of ultimate costs to a country’s economy, and that value is lost when a potential worker is sitting about at home making no contribution to society. Investing in a workplace (in terms of adapting a work station or providing special tools or perhaps even help in personal hygiene) can not only reward a person with job satisfaction but can help make him or her self-sufficient and independent of social assistance.
Cost/benefit analyses can be carried out in order to determine whether special intervention in the workplace is justified for disabled persons. The following factors represent sources of data that would form the object of such analyses:
1. Personnel
- Absence. Will the disabled worker have a satisfactory attendance record?
- Is it likely that extra costs may be incurred for special task instruction?
- Are personnel changes called for? Their costs must be considered also.
- Can accident compensation rates be expected to increase?
2. Safety
- Will the job being considered for the disabled worker involve safety regulations?
- Will special safety regulations be involved?
- Is the work characterized by a considerable frequency of accidents or near accidents?
3. Medical
- As regards the worker whose disability is being examined with a view to his or her re-entry into the workplace, the nature and seriousness of the incapacity must be assessed.
- The extent of the disabled worker’s absence must also be taken into account.
- What is the character and frequency of the worker’s “minor” symptoms, and how are they to be dealt with? Can the future development of related “minor” illnesses capable of hampering the worker’s efficiency be foreseen?
As concerns time lost from work, these calculations can be made in terms of wages, overhead, compensation and lost production. The sort of analyses just described represents a rational approach by which an organization can arrive at an informed decision as to whether a disabled worker is better off back on the job and whether the organization itself will gain by his or her return to work.
In the preceding discussion, designing for the broader population has received a focus of attention heightened by emphasis on specific design in relation to usability and the costs and benefits of such design. It is still a difficult task to make the needed calculations, including all relevant factors, but at present, research efforts are continuing that incorporate modelling methods in their techniques. In some countries, for example the Netherlands and Germany, government policy is making companies more responsible for job-related personal harm; fundamental changes in regulatory policies and insurance structures are, clearly, to be expected to result from trends of this sort. It has already become a more or less settled policy in these countries that a worker who suffers a disabling accident at work should be provided with an adapted work station or be able to perform other work within the company, a policy that has made the treatment of the disabled a genuine achievement in the humane treatment of the worker.
Workers with Limited Functional Capacity
Whether design is aimed at the disabled or at the broader average, it is hindered by a scarcity of research data. Handicapped people have been the subjects of virtually no research efforts. Therefore, in order to set up a product requirements document, or PRD, a specific empirical research study will have to be undertaken in order to gather that data by observation and measurement.
In gathering the information needed about the disabled worker or user it is necessary to consider not only the current functional status of the disabled person, but to make the attempt to foresee whatever changes might be the result of the progression of a chronic condition. This kind of information can, in fact, be elicited from the worker directly, or a medical specialist can supply it.
In designing, for instance, a work action to which data about the worker’s physical strength is relevant, the designer will not choose as a specification the maximum strength which the disabled person can exert, but will take into account any possible diminution in strength that a progression in the worker’s condition might bring about. Thus the worker will be enabled to continue to use the machines and tools adapted or designed for him or at the work station.
Furthermore, designers should avoid designs that involve manipulations of the human body at the far extremes of, say, the range of motion of a body part, but should accommodate their designs to the middle ranges. A simple but very common illustration of this principle follows. A very common part of the drawers of kitchen and office cabinets and desks is a handle that has the form of a little shelf under which one places the fingers, exerting upward and forward force to open the drawer. This manoeuvre requires 180 degrees of supination (with the palm of the hand up) in the wrist—the maximum point for the range of this sort of motion of the wrist. This state of affairs may present no difficulty for a healthy person, provided that the drawer can be opened with a light force and is not awkwardly situated, but makes for strain when the action of the drawer is tight or when the full 180-degree supination is not possible, and is a needless burden on a disabled person. A simple solution—a vertically placed handle—would be mechanically far more efficient and more easily manipulated by a larger portion of the population.
Physical Functioning Ability
In what follows, the three chief areas of limitation in physical functional ability, as defined by the locomotion system, the neurological system and the energy system, will be discussed. Designers will gain some insight into the nature of user/worker constraints in considering the following basic principles of bodily functions.
The locomotion system. This consists of the bones, joints, connective tissues and muscles. The nature of the joint structure determines the range of motion possible. A knee joint, for example, shows a different degree of movement and stability than the joint of the hip or the shoulder. These varying joint characteristics determine the actions possible to the arms, hands, feet, and so on. There are also different types of muscle; it is the type of muscle, whether the muscle passes over one or two joints, and the location of the muscle that determines, for a given body part, the direction of its movement, its speed, and the strength which it is capable of exerting.
The fact that this direction, speed and strength can be characterized and calculated is of great importance in design. For disabled people, one has to take it into account that the “normal” locations of muscles have been disturbed and that the range of motion in joints has been changed. In an amputation, for instance, a muscle may function only partly, or its location may have changed, so that one has to examine the physical ability of the patient carefully to establish what functions remain and how reliable they may be. A case history follows.
A 40-year-old carpenter lost his thumb and the third finger of his right hand in an accident. In an effort to restore the carpenter’s capacity for work, a surgeon removed one of the patient’s great toes and he replaced the missing thumb with it. After a period of rehabilitation, the carpenter returned to work but found it impossible to do sustained work for more than three to four hours. His tools were studied and found to be unfitted to the “abnormal” structure of his hand. The rehabilitation specialist, examining the “redesigned” hand from the point of view of its new functional ability and form was able to have new tools designed that were more appropriate and usable with respect to the altered hand. The load on the worker’s hand, previously too heavy, was now within a usable range, and he regained his ability to continue work for a longer time.
The neurological system. The neurological system can be compared to a very sophisticated control room, complete with data collectors, whose purpose it is to initiate and govern one’s movements and actions by interpreting information relating to those aspects of the body’s components relating to position and mechanical, chemical and other states. This system incorporates not only a feedback system (e.g., pain) that provides for corrective measures, but a “feed-forward” capability which expresses itself anticipatorily so as to maintain a state of equilibrium. Consider the case of a worker who reflexively acts so as to restore a posture in order to protect himself from a fall or from contact with dangerous machine parts.
In disabled persons, the physiological processing of information can be impaired. Both the feedback and the feed-forward mechanisms of visually impaired people are weakened or absent, and the same is true, on an acoustic level, among the hearing-impaired. Furthermore the important governing circuits are interactive. Sound signals have an effect on the equilibrium of a person in conjunction with proprioceptive circuits that situate our bodies in space, so to speak, via data gathered from muscles and joints, with the further help of visual signals. The brain can function to overcome quite drastic deficiencies in these systems, correcting for errors in the coding of information and “filling in” missing information. Beyond certain limits, to be sure, incapacity supervenes. Two case histories follow.
Case 1. A 36-year-old woman suffered a lesion of the spinal cord due to an automobile accident. She is able to sit up without assistance and can move a wheelchair manually. Her trunk is stable. The feeling in her legs is gone, however; this defect includes an inability to sense temperature changes.
She has a sitting workplace at home (the kitchen is designed to allow her to work in a seated position). The safety measure has been taken of installing a sink in a position sufficiently isolated that the risk of burning her legs with hot water is minimized, since her inability to process temperature information in the legs leaves her vulnerable to being unaware of being burned.
Case 2. A five-year-old boy whose left side was paralysed was being bathed by his mother. The doorbell rang, the mother left the boy alone to go to the front door, and the boy, turning on the hot-water tap, suffered burns. For safety reasons, the bath should have been equipped with a thermostat (preferably one that the boy could not have overridden).
The energy system. When the human body has to perform physical labour, physiological changes, notably in the form of interactions in the muscle cells, take place, albeit relatively inefficiently. The human “motor” converts only about 25% of its energy supply to mechanical activity, the remainder of the energy representing thermal losses. The human body is therefore not especially suited to heavy physical labour. Exhaustion sets in after a certain time, and if heavy labour has to be performed, reserve energy sources are drawn upon. These sources of reserve energy are always used whenever work is carried out very rapidly, is started suddenly (without a warm-up period) or involves heavy exertion.
The human organism obtains energy aerobically (via oxygen in the bloodstream) and anaerobically (after depleting aerobic oxygen, it calls upon small, but important reserve units of energy stored in muscle tissue). The need for fresh air supplies in the workplace naturally draws the focus of discussion of oxygen usage toward the aerobic side, working conditions that are strenuous enough to call forth anaerobic processes on a regular basis being extraordinarily uncommon in most workplaces, at least in the developed countries. The availability of atmospheric oxygen, which relates so directly to human aerobic functioning, is a function of several conditions:
- Ambient air pressure (approximately 760 torr, or 21.33 kPa at sea level). High-altitude task performance can be profoundly affected by oxygen deficiency and is a prime consideration for workers in such conditions.
- For workers doing heavy labour, ventilation is necessary to ensure refreshment of the air supply, allowing the volume of air respired per minute to be increased.
- Ambient oxygen makes its way into the bloodstream via the alveoli by diffusion. At higher blood pressures, the diffusion surface is enlarged and thereby the oxygen capacity of the blood.
- An increase in oxygen diffusion to the tissues causes an increase of the diffusion surface and consequently of the oxygen level.
- People with certain heart problems suffer when, with increased cardiac output (together with the oxygen level), the blood circulation changes in favour of the muscles.
- By contrast with oxygen, because of the large reserves of glucose, and especially fat, the energy source (“fuel”) need not be continuously delivered from the outside. In heavy labour, it is merely glucose, with its high energy value, that is used. With lighter work, fat is called upon, at a rate varying with the individual. A brief, general case history follows.
A person suffering from asthma or bronchitis, both of which are diseases affecting the lungs, causes the worker severe limitation in his or her work. The work assignment of this worker should be analysed with respect to factors such as physical load. The environment should be analysed as well: clean ambient air will contribute substantially to workers’ well-being. Furthermore, the workload should be balanced through the day, avoiding peak loads.
Specific Design
In some cases, however, there is still a need for specific design, or design for very small groups. Such a need arises when the tasks to be performed and the difficulties a disabled person is experiencing are excessively large. If the needed specific requirements cannot be made with the available products on the market (even with adaptations), specific design is the answer. Whether this sort of solution may be costly or cheap (and aside from humanitarian issues) it must be nonetheless regarded in the light of workability and support to the firm’s viability. A specially designed worksite is worthwhile economically only when the disabled worker can look forward to working there for years and when the work he or she does is, in production terms, an asset to the company. When this is not the case, although the worker may indeed insist upon his or her right to the job, a sense of realism should prevail. Such touchy problems should be approached in a spirit of seeking a solution by cooperative endeavours at communication.
The advantages of specific design are as follows:
- The design is custom made: it fits the problems to be solved to perfection.
- The worker so served can return to work and a life of social participation.
- The worker can be self-sufficient, independent of welfare.
- The costs of any personnel changes that the alternative might involve are avoided.
The disadvantages of specific design are:
- The design is unlikely to be used for even one other person, let alone a larger group.
- Specific design is often costly.
- Specifically designed products must often be handmade; savings owing to mass methods are most often not realizable.
Case 1. For example, there is the case of a receptionist in a wheelchair who had a speech problem. Her speech difficulty made for rather slow conversations. While the firm remained small, no problems arose and she continued to work there for years. But when the firm enlarged, her disabilities began to make themselves problematic. She had to speak more rapidly and to move about considerably faster; she could not cope with the new demands. However, solutions to her troubles were sought and reduced themselves to two alternatives: special technical equipment might be installed so that the deficiencies that degraded the quality of some of her tasks could be compensated for, or she could simply choose a set of tasks involving a more desk-bound workload. She chose the latter course and still works for the same company.
Case 2. A young man, whose profession was the production of technical drawings, suffered a high level spinal cord lesion due to diving in shallow waters. His injury is severe enough for him to require help with all his daily activities. Nevertheless, with the help of a computer-aided design (CAD) software, he continues to be able make his living at technical drawing and lives, financially independent, with his partner. His work space is a study adapted for his needs and he works for a firm with which he communicates by computer, phone and fax. To operate his personal computer, he had to have certain adaptations made to the keyboard. But with these technical assets he can earn a living and provide for himself.
The approach for specific design is not different from other design as described above. The only insurmountable problem that may arise during a design project is that the design objective cannot be achieved on purely technical grounds—in other words, it can’t be done. For example, a person suffering from Parkinson’s disease is prone, at a certain stage in the progression of his or her condition, to fall over backwards. An aid which would prevent such an eventuality would of course represent the desired solution, but the state of the art is not such that such a device can yet be built.
System Ergonomic Design and Workers with Special Physical Needs
One can treat bodily impairment by medically intervening to restore the damaged function, but the treatment of a disability, or deficiency in the ability to perform tasks, can involve measures far less developed in comparison with medical expertise. As far as the necessity of treating a disability is concerned, the severity of the handicap strongly influences such a decision. But given that treatment is called for, however, the following means, taken singly or in combination, form the choices available to the designer or manager:
- leaving out a task
- compensating for a worker’s deficiency in performing a task element by using a machine or another person’s help
- differentiation of the task order, that is, dividing the task into more manageable subtasks
- modification of the tools used in the task
- special design of tools and machines.
From the specific ergonomic point of view, treatment of a disability includes the following:
- modification of the task
- modification of a tool
- design of new tools or new machines.
The issue of efficacy is always the point of departure in the modification of tools or machines, and is often related to the costs devoted to the modification in question, the technical features to be addressed, and the functional changes to be embodied in the new design. Comfort and attractiveness are qualities that by no means deserve to be neglected among these other characteristics.
The next consideration relating to design changes to be made to a tool or machine is whether the device is one already designed for general use (in which case, modifications will be made to a pre-existing product) or is to be designed with an individual type of disability in mind. In the latter case, specific ergonomic considerations must be devoted to each aspect of the worker’s disability. For example, given a worker suffering from limitations in brain function after a stroke, impairments such as aphasia (difficulty in communication), a paralysed right arm, and a spastic paresis of the leg preventing its being moved upwards might require the following adjustments:
- a personal computer or other device enabling the worker to communicate
- tools that can be operated with the remaining useful arm
- a prosthetic system that would serve to restore the function of the impaired foot as well as to compensate for the patient’s loss of ability to walk.
Is there any general answer to the question of how to design for the disabled worker? The system ergonomic design (SED) approach is an eminently suitable one for this task. Research related to the work situation or to the kind of product at issue requires a design team for the purpose of gathering special information relating either to a special group of disabled workers or to the unique case of an individual user disabled in a particular way. The design team will, by virtue of including a diversity of qualified people, be in possession of expertise beyond the technical sort expected of a designer alone; the medical and ergonomic knowledge shared among them will be as fully applicable as the strictly technical.
Design constraints determined by assembling data related to disabled users are treated with the same objectivity and in the same analytical spirit as are counterpart data relating to healthy users. Just as for the latter, one has to determine for disabled persons their personal patterns of behavioural response, their anthropometrical profiles, biomechanical data (as to reach, strength, range of motion, handling space used, physical load and so forth), ergonomic standards and safety regulations. But one is most regretfully obliged to concede that very little research indeed is done on behalf of disabled workers. There exist a few studies on anthropometry, somewhat more on biomechanics in the field of prostheses and orthoses, but hardly any studies have been carried on physical load capabilities. (The reader will find references to such material in the “Other relevant reading” list at the end of this chapter.) And while it is sometimes easy to gather and apply such data, frequently enough the task is difficult, and in fact, impossible. To be sure, one must obtain objective data, however strenuous the effort and unlikely the chances of doing so, given that the numbers of disabled persons available for research is small. But they are quite often more than willing to participate in whatever research they are offered the opportunity of sharing in, since there is great consciousness of the importance of such a contribution towards design and research in this field. It thus represents an investment not only for themselves but for the larger community of disabled people.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."