Lung function may be measured in a number of ways. However, the aim of the measurements has to be clear before the examination, in order to interpret the results correctly. In this article we will discuss lung function examination with special regard to the occupational field. It is important to remember the limitations in different lung function measurements. Acute temporary lung function effects may not be discernible in case of exposure to fibrogenic dust like quartz and asbestos, but chronic effects on lung function after long-term (>20 years) exposure may be. This is due to the fact that chronic effects occur years after the dust is inhaled and deposited in the lungs. On the other hand, acute temporary effects of organic and inorganic dust, as well as mould, welding fumes and motor exhaust, are well suited to study. This is due to the fact that the irritative effect of these dusts will occur after a few hours of exposure. Acute or chronic lung function effects also may be discernible in cases of exposure to concentrations of irritating gases (nitrogen dioxide, aldehydes, acids and acid chlorides) in the vicinity of well documented exposure limit values, especially if the effect is potentiated by particulate air contamination.
Lung function measurements have to be safe for the examined subjects, and the lung function equipment has to be safe for the examiner. A summary of the specific requirements for different kinds of lung function equipment are available (e.g., Quanjer et al. 1993). Of course, the equipment must be calibrated according to independent standards. This may be difficult to achieve, especially when computerized equipment is being used. The result of the lung function test is dependent on both the subject and the examiner. To provide satisfactory results from the examination, technicians have to be well trained, and able to instruct the subject carefully and also encourage the subject to carry out the test properly. The examiner should also have knowledge about the airways and lungs in order to interpret the results from the recordings correctly.
It is recommended that the methods used have a fairly high reproducibility both between and within subjects. Reproducibility may be measured as the coefficient of variation, that is, the standard deviation multiplied by 100 divided by the mean value. Values below 10% in repeated measurements on the same subject are deemed acceptable.
In order to determine if the measured values are pathological or not, they must be compared with prediction equations. Usually the prediction equations for spirometric variables are based on age and height, stratified for sex. Men have on the average higher lung function values than women, of the same age and height. Lung function decreases with age and increases with height. A tall subject will therefore have higher lung volume than a short subject of the same age. The outcome from prediction equations may differ considerably between different reference populations. The variation in age and height in the reference population will also influence the predicted values. This means, for example, that a prediction equation must not be used if age and/or height for the examined subject are outside the ranges for the population that is the basis for the prediction equation.
Smoking will also diminish lung function, and the effect may be potentiated in subjects who are occupationally exposed to irritating agents. Lung function used to be considered as not being pathological if the obtained values are within 80% of the predicted value, derived from a prediction equation.
Measurements
Lung function measurements are carried out to judge the condition of the lungs. Measurements may either concern single or multiple measured lung volumes, or the dynamic properties in the airways and lungs. The latter is usually determined through effort-dependent manoeuvres. The conditions in the lungs may also be examined with regard to their physiological function, that is, diffusion capacity, airway resistance and compliance (see below).
Measurements concerning ventilatory capacity are obtained by spirometry. The breathing manoeuvre is usually performed as a maximal inspiration followed by a maximal expiration, vital capacity (VC, measured in litres). At least three technically satisfactory recordings (i.e., full inspiration and expiration effort and no observed leaks) should be done, and the highest value reported. The volume may be directly measured by a water-sealed or a low-resistive bell, or indirectly measured by pneumotachography (i.e., integration of a flow signal over time). It is important here to note that all measured lung volumes should be expressed in BTPS, that is, body temperature and ambient pressure saturated with water vapour.
Forced expired vital capacity (FVC, in litres) is defined as a VC measurement performed with a maximally forced expiratory effort. Due to the simplicity of the test and the relatively inexpensive equipment, the forced expirogram has become a useful test in the monitoring of lung function. However, this has resulted in many poor recordings, of which the practical value is debatable. In order to carry out satisfactory recordings, the updated guideline for the collection and use of the forced expirogram, published by the American Thoracic Society in 1987, may be useful.
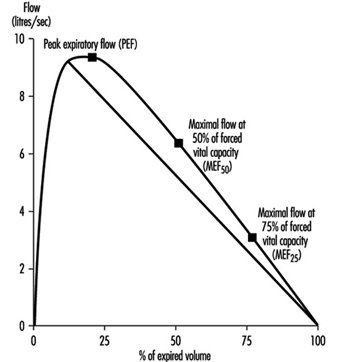
Instantaneous flows may be measured on flow-volume or flow-time curves, while time average flows or times are derived from the spirogram. Associated variables which can be calculated from the forced expirogram are forced expired volume in one second (FEV1, in litres per second), in percentage of FVC (FEV1%), peak flow (PEF, l/s), maximal flows at 50% and 75% of forced vital capacity (MEF50 and MEF25, respectively). An illustration of the derivation of FEV1 from the forced expirogram is outlined in figure 1. In healthy subjects, maximal flow rates at large lung volumes (i.e., at the beginning of expiration) reflect mainly the flow characteristics of the large airways while those at small lung volumes (i.e., the end of expiration) are usually held to reflect the characteristics of the small airways, figure 2. In the latter the flow is laminar, while in the large airways it may be turbulent.
Figure 1. Forced expiratory spirogram showing the derivation of FEV1 and FVC according to the extrapolation principle.
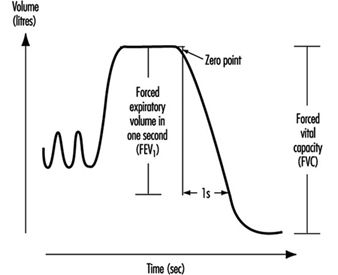
Figure 2. Flow-volume curve showing the derivation of peak expiratory flow (PEF), maximal flows at 50% and 75% of forced vital capacity (![]() and
and ![]() , respectively).
, respectively).
PEF may also be measured by a small portable device such as the one developed by Wright in 1959. An advantage with this equipment is that the subject may carry out serial measurements—for example, at the workplace. To get useful recordings, however, it is necessary to instruct the subjects well. Moreover, one should keep in mind that measurements of PEF with, for example, a Wright meter and those measured by conventional spirometry should not be compared due to the different blow techniques.
The spirometric variables VC, FVC and FEV1 show a reasonable variation between individuals where age, height and sex usually explain 60 to 70% of the variation. Restrictive lung function disorders will result in lower values for VC, FVC and FEV1. Measurements of flows during expiration show a great individual variation, since the measured flows are both effort and time dependent. This means, for example, that a subject will have extremely high flow in case of diminished lung volume. On the other hand, the flow may be extremely low in case of very high lung volume. However, the flow is usually decreased in case of a chronic obstructive disease (e.g., asthma, chronic bronchitis).
Figure 3. A principal outline of the equipment for determination of total lung capacity (TLC) according to the helium dilution technique.
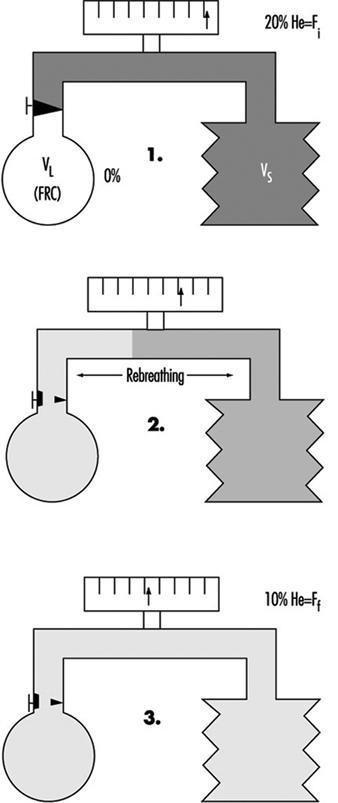
The proportion of residual volume (RV), that is, the volume of air which still is in the lungs after a maximal expiration, can be determined by gas dilution or by body plethysmography. The gas dilution technique requires less complicated equipment and is therefore more convenient to use in studies carried out at the workplace. In figure 3, the principle for the gas dilution technique has been outlined. The technique is based on dilution of an indicator gas in a rebreathing circuit. The indicator gas must be sparingly soluble in biological tissues so that it is not taken up by the tissues and blood in the lung. Hydrogen was initially used, but because of its ability to form explosive mixtures with air it was replaced by helium, which is easily detected by means of the thermal conductivity principle.
The subject and the apparatus form a closed system, and the initial concentration of the gas is thus reduced when it is diluted into the gas volume in the lungs. After equilibration, the concentration of indicator gas is the same in the lungs as in the apparatus, and functional residual capacity (FRC) can be calculated by means of a simple dilution equation. The volume of the spirometer (including the addition of the gas mixture into the spirometer) is denoted by VS, VL is the volume of the lung, Fi is the initial gas concentration and Ff is the final concentration.
FRC = VL = [(VS · Fi) / Ff] – VS
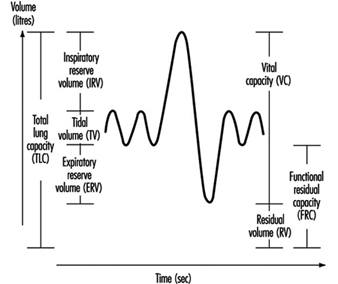
Two to three VC manoeuvres are carried out to provide a reliable base for the calculation of TLC (in litres). The subdivisions of the different lung volumes are outlined in figure 4.
Figure 4. Spirogram labelled to show the subdivisions of the total capacity.
Due to change in the elastic properties of the airways, RV and FRC increase with age. In chronic obstructive diseases, increased values of RV and FRC are usually observed, while VC is decreased. However, in subjects with badly ventilated lung areas—for example, subjects with emphysema—the gas dilution technique may underestimate RV, FRC and also TLC. This is due to the fact that the indicator gas will not communicate with closed-off airways, and therefore the decrease in the indicator gas concentration will give erroneously small values.
Figure 5. A principal outline of the recording of airway closure and the slope of the alveolar plateau (%![]() ).
).
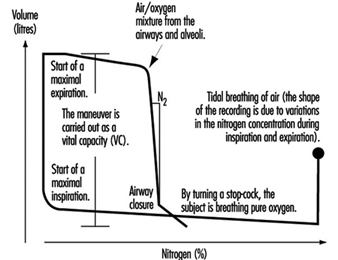
Measures of airway closure and gas distribution in the lungs can be obtained in one and the same manoeuvre by the single breath wash-out technique, figure 5. The equipment consists of a spirometer connected to a bag-in-box system and a recorder for continuous measurements of nitrogen concentration. The manoeuvre is carried out by means of a maximal inspiration of pure oxygen from the bag. In the beginning of the expiration, the nitrogen concentration increases as a result of emptying the subject’s deadspace, containing pure oxygen. The expiration continues with the air from the airways and alveoli. Finally, air from the alveoli, containing 20 to 40% nitrogen, is expired. When the expiration from the basal parts of the lungs increases, the nitrogen concentration will rise abruptly in case of airway closure in dependent lung regions, figure 5. This volume above RV, at which airways close during an expiration, is usually expressed as closing volume (CV) in percentage of VC (CV%). Distribution of the inspired air in the lungs is expressed as the slope of the alveolar plateau (%N2 or phase III, %N2/l). It is obtained by taking the difference in nitrogen concentration between the point when 30% of the air is exhaled and the point for airway closure, and dividing this by the corresponding volume.
Ageing as well as chronic obstructive disorders will result in increased values for both CV% and phase III. However, not even healthy subjects have a uniform gas distribution in the lungs, resulting in slightly elevated values for phase III, that is, 1 to 2% N2/l. The variables CV% and phase III are considered to reflect the conditions in the peripheral small airways with an internal diameter about 2 mm. Normally, the peripheral airways contribute to a small part (10 to 20%) of the total airway resistance. Quite extensive changes which are not detectable by conventional lung function tests like dynamic spirometry, may occur, for example, as a result of an exposure to irritating substances in the air in the peripheral airways. This suggests that airway obstruction begins in the small airways. Results from studies also have shown alterations in CV% and phase III before any changes from the dynamic and static spirometry have occurred. These early changes may go into remission when exposure to hazardous agents has ceased.
The transfer factor of the lung (mmol/min; kPa) is an expression of the diffusion capacity of oxygen transport into the pulmonary capillaries. The transfer factor can be determined using single or multiple breath techniques; the single breath technique is considered to be most suitable in studies at the workplace. Carbon monoxide (CO) is used since the back pressure of CO is very low in the peripheral blood, in contrast to that of oxygen. The uptake of CO is assumed to follow an exponential model, and this assumption can be used to determine the transfer factor for the lung.
Determination of TLCO (transfer factor measured with CO) is carried out by means of a breathing manoeuvre including a maximal expiration, followed by a maximal inspiration of a gas mixture containing carbon monoxide, helium, oxygen and nitrogen. After a breath-holding period, a maximal exhalation is done, reflecting the content in the alveolar air, Figure 10. Helium is used for the determination of the alveolar volume (VA). Assuming that the dilution of CO is the same as for helium, the initial concentration of CO, before the diffusion has started, can be calculated. TLCO is calculated according to the equation outlined below, where k depends on the dimensions of the component terms, t is the effective time for breath-holding and log is base 10 logarithm. Inspired volume is denoted Vi and the fractions F of CO and helium are denoted by i and a for inspired and alveolar, respectively.
TLCO = k Vi (Fa,He/Fi,He) log (Fi,CO Fa,He/Fa,CO Fi,He) (t)-1
Figure 6. A principal outline of the recording of transfer factor

The size of TLCO will depend on a variety of conditions—for example, the amount of available haemoglobin, the volume of ventilated alveoli and perfused lung capillaries and their relation to each other. Values for TLCO decrease with age and increase with physical activity and increased lung volumes. Decreased TLCO will be found in both restrictive and obstructive lung disorders.
Compliance (l/kPa) is a function, inter alia, of the elastic property of the lungs. The lungs have an intrinsic tendency to collaborate—that is, to collapse. The power to keep the lungs stretched will depend on the elastic lung tissue, the surface tension in the alveoli, and the bronchial musculature. On the other hand, the chest wall tends to expand at lung volumes 1 to 2 litres above the FRC level. At higher lung volumes, power has to be applied to further expand the chest wall. At the FRC level, the corresponding tendency in the lungs is balanced by the tendency to expand. The FRC level is therefore denoted by the resting level of the lung.
The compliance of the lung is defined as the change in volume divided by the change in transpulmonary pressure, that is, the difference between the pressures in the mouth (atmospheric) and in the lung, as the result of a breathing manoeuvre. Measurements of the pressure in the lung are not easily carried out and are therefore replaced by measurements of the pressure in the oesophagus. The pressure in the oesophagus is almost the same as the pressure in the lung, and it is measured with a thin polyethylene catheter with a balloon covering the distal 10 cm. During inspiratory and expiratory manoeuvres, the changes in volume and pressure are recorded by means of a spirometer and pressure transducer, respectively. When the measurements are performed during tidal breathing, dynamic compliance can be measured. Static compliance is obtained when a slow VC manoeuvre is carried out. In the latter case, the measurements are carried out in a body plethysmograph, and the expiration is intermittently interrupted by means of a shutter. However, measurements of compliance are cumbersome to perform when examining exposure effects on lung function at the worksite, and this technique is considered to be more appropriate in the laboratory.
A decreased compliance (increased elasticity) is observed in fibrosis. To cause a change in volume, large changes in pressure are required. On the other hand, a high compliance is observed, for example, in emphysema as the result of loss of elastic tissue and therefore also elasticity in the lung.
The resistance in the airways essentially depends on the radius and length of the airways but also on air viscosity. The airway resistance (RL in (kPa/l) /s), can be determined by use of a spirometer, pressure transducer and a pneumotachograph (to measure the flow). The measurements may also be carried out using a body plethysmograph to record the changes in flow and pressure during panting manoeuvres. By administration of a drug intended to cause broncho-constriction, sensitive subjects, as a result of their hyperreactive airways, may be identified. Subjects with asthma usually have increased values for RL.
Acute and Chronic Effects of Occupational Exposure on Pulmonary Function
Lung function measurement may be used to disclose an occupational exposure effect on the lungs. Pre-employment examination of lung function should not be used to exclude job-seeking subjects. This is because the lung function of healthy subjects varies within wide limits and it is difficult to draw a borderline below which it can safely be stated that the lung is pathological. Another reason is that the work environment should be good enough to allow even subjects with slight lung function impairment to work safely.
Chronic effects on the lungs in occupationally exposed subjects may be detected in a number of ways. The techniques are designed to determine historical effects, however, and are less suitable to serve as guidelines to prevent lung function impairment. A common study design is to compare the actual values in exposed subjects with the lung function values obtained in a reference population without occupational exposure. The reference subjects may be recruited from the same (or nearby) workplaces or from the same city.
Multivariate analysis has been used in some studies to assess differences between exposed subjects and matched unexposed referents. Lung function values in exposed subjects may also be standardized by means of a reference equation based on lung function values in the unexposed subjects.
Another approach is to study the difference between the lung function values in exposed and unexposed workers after adjustment for age and height with the use of external reference values, calculated by means of a prediction equation based on healthy subjects. The reference population may also be matched to the exposed subjects according to ethnic group, sex, age, height and smoking habits in order to further control for those influencing factors.
The problem is, however, to decide if a decrease is large enough to be classified as pathological, when external reference values are being used. Although the instruments in the studies have to be portable and simple, attention must be paid both to the sensitivity of the chosen method for detecting small anomalies in airways and lungs and the possibility of combining different methods. There are indications that subjects with respiratory symptoms, such as exertion dyspnoea, are at a higher risk of having an accelerated decline in lung function. This means that the presence of respiratory symptoms is important and so should not be neglected.
The subject may also be followed-up by spirometry, for example, once a year, for a number of years, in order to give a warning against the development of illness. There are limitations, however, since this will be very time-consuming and the lung function may have deteriorated permanently when the decrease can be observed. This approach therefore must not be an excuse for delay in carrying out measures in order to decrease harmful concentrations of air pollutants.
Finally, chronic effects on lung function may also be studied by examining the individual changes in lung function in exposed and unexposed subjects over a number of years. One advantage of the longitudinal study design is that the intersubject variability is eliminated; however, the design is considered to be time-consuming and expensive.
Susceptible subjects may also be identified by comparing their lung function with and without exposure during working shifts. In order to minimize possible effects of diurnal variations, lung function is measured at the same time of day on one unexposed and one exposed occasion. The unexposed condition can be obtained, for example, by occasionally moving the worker to an uncontaminated area or by use of a suitable respirator during a whole shift, or in some cases by performing lung function measurements in the afternoon of a worker’s day off.
One special concern is that repeated, temporary effects can result in chronic effects. An acute temporary lung function decrease may not only be a biological exposure indicator but also a predictor of a chronic lung function decrement. Exposure to air pollutants may result in discernible acute effects on lung function, although the mean values of the measured air pollutants are below the hygienic limit values. The question thus arises, whether these effects really are harmful in the long run. This question is hard to answer directly, especially since the air pollution in workplaces often has a complex composition and the exposure cannot be described in terms of mean concentrations of single compounds. The effect of an occupational exposure is also partly due to the sensitivity of the individual. This means that some subjects will react sooner or to a larger extent than others. The underlying pathophysiological ground for an acute, temporary decrease in lung function is not fully understood. The adverse reaction upon exposure to an irritating air contaminant is, however, an objective measurement, in contrast to subjective experiences like symptoms of different origin.
The advantage of detecting early changes in airways and lungs caused by hazardous air pollutants is obvious—the prevailing exposure may be reduced in order to prevent more severe illnesses. Therefore, an important aim in this respect is to use the measurements of acute temporary effects on lung function as a sensitive early warning system that can be used when studying groups of healthy working people.
Monitoring of Irritants
Irritation is one of the most frequent criteria for setting exposure limit values. It is, however, not certain that compliance with an exposure limit based on irritation will protect against irritation. It should be considered that an exposure limit for an air contaminant usually contains at least two parts—a time-weighted average limit (TWAL) and a short-term exposure limit (STEL), or at least rules for exceeding the time-weighted average limit, “excursion limits”. In the case of highly irritating substances, such as sulphur dioxide, acrolein and phosgene, it is important to limit the concentration even during very short periods, and it has therefore been common practice to fix occupational exposure limit values in the form of ceiling limits, with a sampling period that is kept as short as the measuring facilities will allow.
Time-weighted average limit values for an eight-hour day combined with rules for excursion above these values are given for most of the substances in the American Conference of Governmental Industrial Hygienists (ACGIH) threshold limit value (TLV) list. The TLV list of 1993-94 contains the following statement concerning excursion limits for exceeding limit values:
“For the vast majority of substances with a TLV-TWA, there is not enough toxicological data available to warrant a STEL = short-term exposure limit). Nevertheless, excursions above the TLV-TWA should be controlled even where the eight-hour TWA is within recommended limits.”
Exposure measurements of known air contaminants and comparison with well documented exposure limit values should be carried out on a routine basis. There are, however, many situations when the determination of compliance with exposure limit values is not enough. This is the case in the following circumstances (inter alia):
- when the limit value is too high to safeguard against irritation
- when the irritant is unknown
- when the irritant is a complex mixture and there is no suitable indicator known.
As advocated above, the measurement of acute, temporary effects on lung function can be used in these cases as a warning against over-exposure to irritants.
In cases (2) and (3), acute, temporary effects on lung function may be applicable also in testing the efficiency of control measures to decrease exposure to air contamination or in scientific investigations, for example, in attributing biological effects to components of air contaminants. A number of examples follow in which acute, temporary lung function effects have been successfully employed in occupational health investigations.
Studies of Acute, Temporary Lung Function Effects
Work-related, temporary decrease of lung function over a work shift was recorded in cotton workers at the end of 1950. Later, several authors reported work-related, acute, temporary changes of lung function in hemp and textile workers, coal miners, workers exposed to toluene di-isocyanate, fire-fighters, rubber processing workers, moulders and coremakers, welders, ski waxers, workers exposed to organic dust and irritants in water-based paints.
However, there are also several examples where measurements before and after exposure, usually during a shift, have failed to demonstrate any acute effects, despite a high exposure. This is probably due to the effect of normal circadian variation, mainly in lung function variables depending on the size of airway calibre. Thus the temporary decrease in these variables must exceed the normal circadian variation to be recognized. The problem may be circumvented, however, by measuring lung function at the same time of the day at each study occasion. By using the exposed employee as his or her own control, the interindividual variation is further decreased. Welders were studied in this way, and although the mean difference between unexposed and exposed FVC values was less than 3% in 15 examined welders, this difference was significant at the 95% confidence level with a power of more than 99%.
The reversible transient effects on the lungs can be used as an exposure indicator of complicated irritating components. In the study cited above, particles in the work environment were crucial for the irritating effects on the airways and lungs. The particles were removed by a respirator consisting of a filter combined with a welding helmet. The results indicated that the effects on the lungs were caused by the particles in welding fumes, and that the use of a particulate respirator might prevent this effect.
Exposure to diesel exhaust also gives measurable irritative effects on the lungs, shown as an acute, temporary lung function decrease. Mechanical filters mounted on the exhaust pipes of trucks used in loading operations by stevedores relieved subjective disorders and reduced the acute, temporary lung function decrease observed when no filtration was done. The results thus indicate that the presence of particles in the work environment does play a role in the irritative effect on airways and lungs, and that it is possible to assess the effect by measurements of acute changes in lung function.
A multiplicity of exposures and a continually changing work environment may present difficulties in discerning the causal relationship of the different agents existing in a work environment. The exposure scenario in sawmills is an illuminating example. It is not possible (e.g., for economical reasons) to carry out exposure measurements of all possible agents (terpenes, dust, mould, bacteria, endotoxin, mycotoxins, etc.) in this work environment. A feasible method may be to follow the development of lung function longitudinally. In a study of sawmill workers in the wood-trimming department, lung function was examined before and after a working week, and no statistically significant decrease was found. However, a follow-up study carried out a few years later disclosed that those workers who actually had a numerical decrease in lung function during a working week also had an accelerated long-term decline in lung function. This may indicate that vulnerable subjects can be detected by measuring changes in lung function during a working week.