Raymond Hétu
* This article was written by Dr. Hétu shortly before his untimely death. His colleagues and friends consider it one memoriam to him.
Although this article deals with disability due to noise-exposure and hearing loss, it is included here because it also contains fundamental principles applicable to rehabilitation from disabilities arising from other hazardous exposures.
Psychosocial Aspects of Occupationally Induced Hearing Loss
Like all human experience, hearing loss caused by exposure to workplace noise is given meaning—it is qualitatively experienced and evaluated—by those whom it affects and by their social group. This meaning can, however, be a powerful obstacle to the rehabilitation of individuals suffering from occupationally induced hearing loss (Hétu and Getty 1991b). The chief reasons, as discussed below, are that the victims of hearing loss experience perceptual barriers related to the signs and effects of their deficiency and that the manifestation of overt signs of hearing loss is highly stigmatizing.
Communication problems due to the distorted perception of hearing
Difficulties in hearing and communication resulting from occupationally induced hearing loss are usually attributed to other causes, for example unfavourable conditions for hearing or communication or a lack of attention or interest. This erroneous attribution is observed in both the affected individual and among his or her associates and has multiple, although converging, causes.
- Internal ear injuries are invisible, and victims of this type of injury do not see themselves as physically injured by noise.
- Hearing loss per se progresses very insidiously. The virtually daily auditory fatigue due to workplace noise suffered by exposed workers makes the timely detection of irreversible alterations in hearing function a matter of the greatest difficulty. Individuals exposed to noise are never aware of tangible deteriorations of hearing capacity. In fact, in most workers exposed daily to harmful levels of noise, the increase in the auditory threshold is of the order of one decibel per year of exposure (Hétu, Tran Quoc and Duguay 1990). When hearing loss is symmetric and progressive, the victim has no internal reference against which to judge the induced hearing deficit. As a result of this insidious evolution of hearing loss, individuals undergo a very progressive change of habits, avoiding situations which place them at a disadvantage—without however explicitly associating this change with their hearing problems.
- The signs of hearing loss are very ambiguous and usually take the form of a loss of frequency discrimination, that is, a diminished ability to discriminate between two or more simultaneous acoustic signals, with the more intense signal masking the other(s). Concretely, this takes the form of varying degrees of difficulty in following conversations where reverberation is high or where background noise due to other conversations, televisions, fans, vehicle motors, and so forth, is present. In other words, the hearing capacity of individuals suffering from impaired frequency discrimination is a direct function of the ambient conditions at any given moment. Those with whom the victim comes into daily contact experience this variation in hearing capacity as inconsistent behaviour on the part of the affected individual and reproach him or her in terms like, “You can understand well enough when it suits your purpose”. The affected individual, on the other hand, considers his or her hearing and communication problems to be the result of background noise, inadequate articulation by those addressing him or her, or a lack of attention on their part. In this way, the most characteristic sign of noise-induced hearing loss fails to be recognized for what it is.
- The effects of hearing loss are usually experienced outside of the workplace, within the confines of family life. Consequently, problems are not associated with occupational exposure to noise and are not discussed with work colleagues suffering similar difficulties.
- Acknowledgement of hearing problems is usually triggered by reproaches from the victim’s family and social circles (Hétu, Jones and Getty 1993). Affected individuals violate certain implicit social norms, for example by speaking too loudly, frequently asking others to repeat themselves and turning the volume of televisions or radios up too high. These behaviours elicit the spontaneous—and usually derogatory—question, “Are you deaf?” from those around. The defensive behaviours that this triggers do not favour the acknowledgement of partial deafness.
As a result of the convergence of these five factors, individuals suffering from occupationally induced hearing loss do not recognize the effects of their affliction on their daily lives until the loss is well advanced. Typically, this occurs when they find themselves frequently asking people to repeat themselves (Hétu, Lalonde and Getty 1987). Even at this point, however, victims of occupationally induced hearing loss are very unwilling to acknowledge their hearing loss on account of the stigma associated with deafness.
Stigmatization of the signs of deafness
The reproaches elicited by the signs of hearing loss are a reflection of the extremely negative value construct typically associated with deafness. Workers exhibiting signs of deafness risk being perceived as abnormal, incapable, prematurely old, or handicapped—in short, they risk becoming socially marginalized in the workplace (Hétu, Getty and Waridel 1994). These workers’ negative self-image thus intensifies as their hearing loss progresses. They are obviously reluctant to embrace this image, and by extension, to acknowledge the signs of hearing loss. This leads them to attribute their hearing and communication problems to other factors and to become passive in the face of these factors.
The combined effect of the stigma of deafness and the distorted perception of the signs and effects of hearing loss on rehabilitation is illustrated in figure 1.
Figure 1. Conceptual framework for incapacity from handicap

When hearing problems progress to the point that it is no longer possible to deny or minimize them, individuals attempt to hide the problem. This invariably leads to social withdrawal on the part of the worker and exclusion on the part of the worker’s social group, which ascribes the withdrawal to a lack of interest in communicating rather than to hearing loss. The result of these two reactions is that the affected individual is not offered help or informed of coping strategies. Workers’ dissimulation of their problems may be so successful that family members and colleagues may not even realize the offensive nature of their jokes elicited by the signs of deafness. This situation only exacerbates the stigmatization and its resultant negative effects. As Figure 1 illustrates, the distorted perceptions of the signs and effects of hearing loss and the stigmatization which results from these perceptions are barriers to the resolution of hearing problems. Because affected individuals are already stigmatized, they initially refuse to use hearing aids, which unmistakably advertise deafness and so promote further stigmatization.
The model presented in Figure 1 accounts for the fact that most people suffering occupationally induced hearing loss do not consult audiology clinics, do not request modification of their workstations and do not negotiate enabling strategies with their families and social groups. In other words, they endure their problems passively and avoid situations which advertise their auditory deficit.
Conceptual Framework of Rehabilitation
For rehabilitation to be effective, it is necessary to overcome the obstacles outlined above. Rehabilitative interventions should therefore not be limited to attempts to restore hearing capacity, but should also address issues related to the way hearing problems are perceived by affected individuals and their associates. Because stigmatization of deafness is the greatest obstacle to rehabilitation (Hétu and Getty 1991b; Hétu, Getty and Waridel 1994), it should be the primary focus of any intervention. Effective interventions should therefore include both stigmatized workers and their circles of family, friends, colleagues and others with whom they come into contact, since it is they who stigmatize them and who, out of ignorance, impose impossible expectations on them. Concretely, it is necessary to create an environment which allows affected individuals to break out of their cycle of passivity and isolation and actively seek out solutions to their hearing problems. This must be accompanied by a sensitization of the entourage to the specific needs of affected individuals. This process is grounded in the ecological approach to incapacity and handicap illustrated in figure 2.
Figure 2. Model of restrictions due to hearing loss
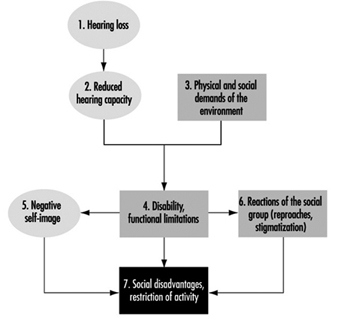
In the ecological model, hearing loss is experienced as an incompatibility between an individual’s residual capacity and the physical and social demands of his or her environment. For example, workers suffering from a loss of frequency discrimination associated with noise-induced hearing loss will have difficulty detecting acoustic alarms in noisy workplaces. If the alarms required at workstations cannot be adjusted to levels significantly louder than those appropriate for people with normal hearing, the workers will be placed in a handicapped position (Hétu 1994b). As a result of this handicap, workers may be at the obvious disadvantage of being deprived of a means to protect themselves. Yet, simply acknowledging hearing loss puts the worker at risk of being considered “abnormal” by his or her colleagues, and when labelled disabled he or she will fear being seen as incompetent by colleagues or superiors. In either case, workers will attempt to hide their handicap or deny the existence of any problems, placing themselves at a functional disadvantage at work.
As figure 2 illustrates, disability is a complex state of affairs with several interrelated restrictions. In such a network of relationships, prevention or minimization of disadvantages or restrictions of activity require simultaneous interventions on many fronts. For example, hearing aids, while partially restoring hearing capacity (component 2), do not prevent either the development of a negative self-image or stigmatization by the worker’s entourage (components 5 and 6), both of which are responsible for isolation and avoidance of communication (component 7). Further, auditory supplementation is incapable of completely restoring hearing capacity; this is particularly true with regard to frequency discrimination. Amplification may improve the perception of acoustic alarms and of conversations but is incapable of improving the resolution of competing signals required for the detection of warning signals in the presence of significant background noise. The prevention of disability-related restrictions therefore necessitates the modification of the social and physical demands of the workplace (component 3). It should be superfluous to note that although interventions designed to modify perceptions (components 5 and 6) are essential and do prevent disability from arising, they do not palliate the immediate consequences of these situations.
Situation-specific Approaches to Rehabilitation
The application of the model presented in Figure 2 will vary depending on the specific circumstances encountered. According to surveys and qualitative studies (Hétu and Getty 1991b; Hétu, Jones and Getty 1993; Hétu, Lalonde and Getty 1987; Hétu, Getty and Waridel 1994; Hétu 1994b), the effects of disability suffered by victims of occupationally induced hearing loss are particularly felt: (1) at the workplace; (2) at the level of social activities; and (3) at the family level. Specific intervention approaches have been proposed for each of these situations.
The workplace
In industrial workplaces, it is possible to identify the following four restrictions or disadvantages requiring specific interventions:
- accident hazards related to the failure to detect warning signals
- efforts, stress and anxiety resulting from hearing and com-munication problems
- obstacles to social integration
- obstacles to professional advancement.
Accident hazards
Acoustic warning alarms are frequently used in industrial workplaces. Occupationally induced hearing loss may considerably diminish workers’ ability to detect, recognize or locate such alarms, particularly in noisy workplaces with high levels of reverberation. The loss of frequency discrimination which inevitably accompanies hearing loss may in fact be so pronounced as to require warning alarms to be 30 to 40db louder than background levels to be heard and recognized by affected individuals (Hétu 1994b); for individuals with normal hearing, the corresponding value is approximately 12 to 15db. Currently, it is rare that warning alarms are adjusted to compensate for background noise levels, workers’ hearing capacity or the use of hearing protection equipment. This puts affected workers at a serious disadvantage, especially as far as their safety is concerned.
Given these constraints, rehabilitation must be based on a rigorous analysis of the compatibility of auditory perception requirements with residual auditory capacities of affected workers. A clinical examination capable of characterizing an individual’s ability to detect acoustic signals in the presence of background noise, such as the DetectsoundTM software package (Tran Quoc, Hétu and Laroche 1992), has been developed, and is available to determine the characteristics of acoustic signals compatible with workers’ hearing capacity. These devices simulate normal or impaired auditory detection and take into account the characteristics of the noise at the workstation and the effect of hearing protection equipment. Of course, any intervention aimed at reducing the noise level will facilitate the detection of acoustic alarms. It is nevertheless necessary to adjust the alarms’ level as a function of the residual hearing capacity of affected workers.
In some cases of relatively severe hearing loss, it may be necessary to resort to other types of warning, or to supplement hearing capacity. For example, it is possible to transmit warning alarms over FM bandwidths and receive them with a portable unit connected directly to a hearing aid. This arrangement is very effective as long as: (1) the tip of the hearing aid fits perfectly (in order to attenuate background noise); and (2) the response curve of the hearing aid is adjusted to compensate for the masking effect of background noise attenuated by the hearing aid tip and the worker’s hearing capacity (Hétu, Tran Quoc and Tougas 1993). The hearing aid may be adjusted to integrate the effects of the full spectrum of background noise, the attenuation produced by the hearing aid’s tip, and the worker’s hearing threshold. Optimal results will be obtained if the frequency discrimination of the worker is also measured. The hearing aid-FM receptor may also be used to facilitate verbal communication with work colleagues when this is essential for worker safety.
In some cases, the workstation itself must be redesigned in order to ensure worker safety.
Hearing and communication problems
Acoustic warning alarms are usually used to inform workers of the state of a production process and as a means of inter operator communication. In workplaces where such alarms are used, individuals with hearing loss must rely upon other sources of information to perform their work. These may involve intense visual surveillance and discreet help offered by work colleagues. Verbal communication, whether over the telephone, in committee meetings or with superiors in noisy workshops, requires great effort on the part of affected individuals and is also highly problematic for affected individuals in industrial workplaces. Because these individuals feel the need to hide their hearing problems, they are also plagued by the fear of being unable to cope with a situation or of committing costly errors. Often, this may cause extremely high anxiety (Hétu and Getty 1993).
Under these circumstances, rehabilitation must first focus on eliciting explicit acknowledgement by the company and its representatives of the fact that some of their workers suffer from hearing difficulties caused by noise exposure. The legitimization of these difficulties helps affected individuals to communicate about them and to avail themselves of appropriate palliative means. However, these means must in fact be available. In this regard, it is astonishing to note that telephone receivers in the workplace are rarely equipped with amplifiers designed for individuals suffering from hearing loss and that conference rooms are not equipped with appropriate systems (FM or infrared transmitters and receptors, for example). Finally, a campaign to increase awareness of the needs of individuals suffering from hearing loss should be undertaken. By publicizing strategies which facilitate communication with affected individuals, communication-related stress will be greatly reduced. These strategies consist of the following phases:
- approaching the affected individual and facing him or her
- articulating without exaggeration
- repeating misunderstood phrases, using different words
- keeping as far away from sources of noise as possible
Clearly, any control measures that lead to lower noise and reverberation levels in the workplace also facilitate communication with individuals suffering from hearing loss.
Obstacles to social integration
Noise and reverberation in the workplace render communication so difficult that it is often limited to the strict minimum required by the tasks to be accomplished. Informal communication, a very important determinant of the quality of working life, is thus greatly impaired (Hétu 1994a). For individuals suffering from hearing loss, the situation is extremely difficult. Workers suffering from occupationally induced hearing loss are isolated from their work colleagues, not only at their workstation but even during breaks and meals. This is a clear example of the convergence of excessive work requirements and the fear of ridicule suffered by affected individuals.
The solutions to this problem lie in the implementation of the measures already described, such as the lowering of overall noise levels, particularly in rest areas, and the sensitization of work colleagues to the needs of affected individuals. Again, recognition by the employer of affected individuals’ specific needs itself constitutes a form of psychosocial support capable of limiting the stigma associated with hearing problems.
Obstacles to professional advancement
One of the reasons individuals suffering from occupationally induced hearing loss take such pains to hide their problem is the explicit fear of being disadvantaged professionally (Hétu and Getty 1993): some workers even fear losing their jobs should they reveal their hearing loss. The immediate consequence of this is a self-restriction with regard to professional advancement, for example, failure to apply for a promotion to shift supervisor, supervisor or foreman. This is also true of professional mobility outside the company, with experienced workers failing to take advantage of their accumulated skills since they feel that pre-employment audiometric examinations would block their access to better jobs. Self-restriction is not the only obstacle to professional advancement caused by hearing loss. Workers suffering from occupationally induced hearing loss have in fact reported instances of employer bias when positions requiring frequent verbal communication have become available.
As with the other aspects of disability already described, explicit acknowledgement of affected workers’ specific needs by employers greatly eliminates obstacles to professional advancement. From the standpoint of human rights (Hétu and Getty 1993), affected individuals have the same right to be considered for advancement as do other workers, and appropriate workplace modifications can facilitate their access to higher-level jobs.
In summary, the prevention of disability in the workplace requires sensitization of employers and work colleagues to the specific needs of individuals suffering from occupationally induced hearing loss. This can be accomplished by information campaigns on the signs and effects of noise-induced hearing loss aimed at dissipating the view of hearing loss as an improbable abnormality of little import. The use of technological aids is possible only if the need to use them has been legitimized in the workplace by colleagues, superiors and affected individuals themselves.
Social activities
Individuals suffering from occupationally induced hearing loss are at a disadvantage in any non-ideal hearing situation, for instance, in the presence of background noise, in situations requiring communication at a distance, in environments where reverberation is high and on the telephone. In practice, this greatly curtails their social life by limiting their access to cultural activities and public services, thus hindering their social integration (Hétu and Getty 1991b).
Access to cultural activities and public services
In accordance with the model in Figure 2, restrictions related to cultural activities involve four components (components 2, 3, 5 and 6) and their elimination relies on multiple interventions. Thus concert halls, auditoriums and places of worship can be made accessible to persons suffering from hearing loss by equipping them with appropriate listening systems, such as FM or infrared transmission systems (component 3) and by informing those responsible for these institutions of the needs of affected individuals (component 6). However, affected individuals will request hearing equipment only if they are aware of its availability, know how to use it (component 2) and have received the necessary psychosocial support to recognize and communicate their need for such equipment (component 5).
Effective communication, training and psychosocial support channels for hearing-impaired workers have been developed in an experimental rehabilitation programme (Getty and Hétu 1991, Hétu and Getty 1991a), discussed in “Family life”, below.
As regards the hearing-impaired, access to public services such as banks, stores, government services and health services is hindered primarily by a lack of knowledge on the part of the institutions. In banks, for example, glass screens may separate clients from tellers, who may be occupied in entering data or filling out forms while talking to clients. The resulting lack of face-to-face visual contact, coupled with unfavourable acoustic conditions and a context in which misunderstanding can have very serious consequences, render this an extremely difficult situation for affected individuals. In health service facilities, patients wait in relatively noisy rooms where their names are called by an employee located at a distance or via a public address system that may be difficult to comprehend. While individuals with hearing loss worry a great deal about being unable to react at the correct time, they generally neglect to inform staff of their hearing problems. There are numerous examples of this type of behaviour.
In most cases, it is possible to prevent these handicap situations by informing staff of the signs and effects of partial deafness and of ways to facilitate communication with affected individuals. A number of public services have already undertaken initiatives aimed at facilitating communication with individuals suffering from occupationally induced hearing loss (Hétu, Getty and Bédard 1994) with results as follows. The use of appropriate graphical or audio visual material allowed the necessary information to be communicated in less than 30 minutes and the effects of such initiatives were still apparent six months after the information sessions. These strategies greatly facilitated communication with the personnel of the services involved. Very tangible benefits were reported not only by clients with hearing loss but also by the staff, who saw their tasks simplified and difficult situations with this type of client prevented.
Social integration
Avoidance of group encounters is one of the most severe consequences of occupationally induced hearing loss (Hétu and Getty 1991b). Group discussions are extremely demanding situations for affected individuals, In this case, the burden of accommodation rests with the affected individual, as he or she can rarely expect the entire group to adopt a favourable rhythm of conversation and mode of expression. Affected individuals have three strategies available to them in these situations:
- reading facial expressions
- using specific communication strategies
- using a hearing aid.
The reading of facial expressions (and lip-reading) can certainly facilitate comprehension of conversations, but requires considerable attention and concentration and cannot be sustained over long periods. This strategy can, however, be usefully combined with requests for repetition, reformulation and summary. Nevertheless, group discussions occur at such a rapid rhythm that it is often difficult to rely upon these strategies. Finally, the use of a hearing aid may improve the ability to follow conversation. However, current amplification techniques do not allow the restoration of frequency discrimination. In other words, both signal and noise are amplified. This often worsens rather than improves the situation for individuals with serious frequency discrimination deficits.
The use of a hearing aid as well as the request for accommodation by the group presupposes that the affected individual feels comfortable revealing his or her condition. As discussed below, interventions aimed at strengthening self-esteem are therefore prerequisites for attempts to supplement auditory capacity.
Family life
The family is the prime locus of the expression of hearing problems caused by occupational hearing loss (Hétu, Jones and Getty 1993). A negative self-image is the essence of the experience of hearing loss, and affected individuals attempt to hide their hearing loss in social interactions by listening more intently or by avoiding overly demanding situations. These efforts, and the anxiety which accompanies them, create a need for release in the family setting, where the need to hide the condition is less strongly felt. Consequently, affected individuals tend to impose their problems on their families and coerce them to adapt to their hearing problems. This takes a toll on spouses and others and causes irritation at having to repeat oneself frequently, tolerate high television volumes and “always be the one to answer the telephone”. Spouses must also deal with serious restrictions in the couples’ social life and with other major changes in family life. Hearing loss limits companionship and intimacy, creates tension, misunderstandings and arguments and disturbs relations with children.
Not only does hearing and communication impairment affect intimacy, but its perception by affected individuals and their family (components 5 and 6 of figure 2) tends to feed frustration, anger and resentment (Hétu, Jones and Getty 1993). Affected individuals frequently do not recognize their impairment and do not attribute their communications problems to a hearing deficit. As a result, they may impose their problems on their families rather than negotiate mutually satisfactory adaptations. Spouses, on the other hand, tend to interpret the problems as a refusal to communicate and as a change in the affected individual’s temperament. This state of affairs may lead to mutual reproaches and accusations, and ultimately to isolation, loneliness and sadness, particularly on the part of the unaffected spouse.
The solution of this interpersonal dilemma requires the participation of both partners. In fact, both require:
- information on the auditory basis of their problems.
- psychosocial support
- training in the use of appropriate supplemental means of communication.
With this in mind, a rehabilitation programme for affected individuals and their spouses has been developed (Getty and Hétu 1991, Hétu and Getty 1991a). The goal of the programme is to stimulate research on the resolution of problems caused by hearing loss, taking into account the passivity and social withdrawal that characterize occupationally induced hearing loss.
Since the stigma associated with deafness is the principal source of these behaviours, it was essential to create a setting in which self-esteem could be restored so as to induce affected individuals to seek out actively solutions to their hearing-related problems. The effects of stigmatization can be overcome only when one is perceived by others as normal regardless of any hearing deficit. The most effective way to achieve this consists of meeting other people in the same situation, as was suggested by workers asked about the most appropriate aid to offer their hearing-impaired colleagues. However, it is essential that these meetings take place outside the workplace, precisely to avoid the risk of further stigmatization (Hétu, Getty and Waridel 1994).
The rehabilitation programme mentioned above was developed with this in mind, the group encounters taking place in a community health department (Getty and Hétu 1991). Recruitment of participants was an essential component of the programme, given the withdrawal and passivity of the target population. Accordingly, occupational health nurses first met with 48 workers suffering from hearing loss and their spouses at their homes. Following an interview on hearing problems and their effects, every couple was invited to a series of four weekly meetings lasting two hours each, held in the evening. These meetings followed a precise schedule aimed at meeting the objectives of information, support and training defined in the programme. Individual follow-up was provided to participants in order to facilitate their access to audio-logical and audioprosthetic services. Individuals suffering from tinnitus were referred to the appropriate services. A further group meeting was held three months after the last weekly meeting.
The results of the programme, collected at the end of the experimental phase, demonstrated that participants and their spouses were more aware of their hearing problems, and were also more confident of resolving them. Workers had undertaken various steps, including technical aids, revealing their impairment to their social group, and expressing their needs in an attempt to improve communication.
A follow-up study, performed with this same group five years after their participation in the programme, demonstrated that the programme was effective in stimulating participants to seek solutions. It also showed that rehabilitation is a complex process requiring several years of work before affected individuals are able to avail themselves of all the means at their disposal to regain their social integration. In most cases, this type of rehabilitation process requires periodic follow-up.
Conclusion
As figure 2 indicates, the meaning that individuals suffering from occupationally induced hearing loss and their associates give to their condition is a key factor in handicap situations. The approaches to rehabilitation proposed in this article explicitly take this factor into account. However, the manner in which these approaches are applied concretely will depend on the specific sociocultural context, since the perception of these phenomena may vary from one context to another. Even within the sociocultural context in which the intervention strategies described above were developed, significant modifications may be necessary. For example, the programme developed for individuals suffering from occupationally induced hearing loss and their spouses (Getty and Hétu 1991) was tested in a population of affected males. Different strategies would probably be necessary in a population of affected females, especially when one considers the different social roles men and women occupy in conjugal and parental relations (Hétu, Jones and Getty 1993). Modifications would be necessary a fortiori when dealing with cultures which differ from that of North America from which the approaches emerged. The conceptual framework proposed (figure 2) can nevertheless be used effectively to orient any intervention aimed at rehabilitating individuals suffering from occupationally induced hearing loss.
Furthermore, this type of intervention, if applied on a large scale, will have important preventive effects on hearing loss itself. The psychosocial aspects of occupationally induced hearing loss hinder both rehabilitation (figure 1) and prevention. The distorted perception of hearing problems delays their recognition, and their dissimulation by severely affected individuals fosters the general perception that these problem are rare and relatively innocuous, even in noisy workplaces. This being so, noise-induced hearing loss is not perceived by workers at risk or by their employers as an important health problem, and the need for prevention is thus not strongly felt in noisy workplaces. On the other hand, individuals already suffering from hearing loss who reveal their problems are eloquent examples of the severity of the problem. Rehabilitation can thus be seen as the first step of a prevention strategy.