A workplace hazard can be defined as any condition that may adversely affect the well-being or health of exposed persons. Recognition of hazards in any occupational activity involves characterization of the workplace by identifying hazardous agents and groups of workers potentially exposed to these hazards. The hazards might be of chemical, biological or physical origin (see table 1). Some hazards in the work environment are easy to recognize—for example, irritants, which have an immediate irritating effect after skin exposure or inhalation. Others are not so easy to recognize—for example, chemicals which are accidentally formed and have no warning properties. Some agents like metals (e.g., lead, mercury, cadmium, manganese), which may cause injury after several years of exposure, might be easy to identify if you are aware of the risk. A toxic agent may not constitute a hazard at low concentrations or if no one is exposed. Basic to the recognition of hazards are identification of possible agents at the workplace, knowledge about health risks of these agents and awareness of possible exposure situations.
Table 1. Hazards of chemical, biological and physical agents.
|
Type of hazard |
Description |
Examples |
|
CHEMICAL HAZARDS
|
Chemicals enter the body principally through inhalation, skin absorption or ingestion. The toxic effect might be acute, chronic or both., |
|
|
Corrosion |
Corrosive chemicals actually cause tissue destruction at the site of contact. Skin, eyes and digestive system are the most commonly affected parts of the body. |
Concentrated acids and alkalis, phosphorus |
|
Irritation |
Irritants cause inflammation of tissues where they are deposited. Skin irritants may cause reactions like eczema or dermatitis. Severe respiratory irritants might cause shortness of breath, inflammatory responses and oedema. |
Skin: acids, alkalis, solvents, oils Respiratory: aldehydes, alkaline dusts, ammonia, nitrogendioxide, phosgene, chlorine, bromine, ozone |
|
Allergic reactions |
Chemical allergens or sensitizers can cause skin or respiratory allergic reactions. |
Skin: colophony (rosin), formaldehyde, metals like chromium or nickel, some organic dyes, epoxy hardeners, turpentine Respiratory: isocyanates, fibre-reactive dyes, formaldehyde, many tropical wood dusts, nickel
|
|
Asphyxiation |
Asphyxiants exert their effects by interfering with the oxygenation of the tissues. Simple asphyxiants are inert gases that dilute the available atmospheric oxygen below the level required to support life. Oxygen-deficient atmospheres may occur in tanks, holds of ships, silos or mines. Oxygen concentration in air should never be below 19.5% by volume. Chemical asphyxiants prevent oxygen transport and the normal oxygenation of blood or prevent normal oxygenation of tissues. |
Simple asphyxiants: methane, ethane, hydrogen, helium Chemical asphyxiants: carbon monoxide, nitrobenzene, hydrogencyanide, hydrogen sulphide
|
|
Cancer |
Known human carcinogens are chemicals that have been clearly demonstrated to cause cancer in humans. Probable human carcinogens are chemicals that have been clearly demonstrated to cause cancer in animals or the evidence is not definite in humans. Soot and coal tars were the first chemicals suspected to cause cancer. |
Known: benzene (leukaemia); vinyl chloride (liver angio-sarcoma); 2-naphthylamine, benzidine (bladder cancer); asbestos (lung cancer, mesothelioma); hardwood dust (nasalor nasal sinus adenocarcinoma) Probable: formaldehyde, carbon tetrachloride, dichromates, beryllium |
|
Reproductive effects
|
Reproductive toxicants interfere with reproductive or sexual functioning of an individual. |
Manganese, carbon disulphide, monomethyl and ethyl ethers of ethylene glycol, mercury |
|
|
Developmental toxicants are agents that may cause an adverse effect in offspring of exposed persons; for example, birth defects. Embryotoxic or foetotoxic chemicals can cause spontaneous abortions or miscarriages. |
Organic mercury compounds, carbon monoxide, lead, thalidomide, solvents |
|
Systemic poisons
|
Systemic poisons are agents that cause injury to particular organs or body systems. |
Brain: solvents, lead, mercury, manganese Peripheral nervous system: n-hexane, lead, arsenic, carbon disulphide Blood-forming system: benzene, ethylene glycol ethers Kidneys: cadmium, lead, mercury, chlorinated hydrocarbons Lungs: silica, asbestos, coal dust (pneumoconiosis)
|
|
BIOLOGICAL HAZARDS
|
Biological hazards can be defined as organic dusts originating from different sources of biological origin such as virus, bacteria, fungi, proteins from animals or substances from plants such as degradation products of natural fibres. The aetiological agent might be derived from a viable organism or from contaminants or constitute a specific component in the dust. Biological hazards are grouped into infectious and non-infectious agents. Non-infectious hazards can be further divided into viable organisms, biogenic toxins and biogenic allergens. |
|
|
Infectious hazards |
Occupational diseases from infectious agents are relatively uncommon. Workers at risk include employees at hospitals, laboratory workers, farmers, slaughterhouse workers, veterinarians, zoo keepers and cooks. Susceptibility is very variable (e.g., persons treated with immunodepressing drugs will have a high sensitivity). |
Hepatitis B, tuberculosis, anthrax, brucella, tetanus, chlamydia psittaci, salmonella |
|
Viable organisms and biogenic toxins |
Viable organisms include fungi, spores and mycotoxins; biogenic toxins include endotoxins, aflatoxin and bacteria. The products of bacterial and fungal metabolism are complex and numerous and affected by temperature, humidity and kind of substrate on which they grow. Chemically they might consist of proteins, lipoproteins or mucopolysaccharides. Examples are Gram positive and Gram negative bacteria and moulds. Workers at risk include cotton mill workers, hemp and flax workers, sewage and sludge treatment workers, grain silo workers. |
Byssinosis, “grain fever”, Legionnaire’s disease |
|
Biogenic allergens |
Biogenic allergens include fungi, animal-derived proteins, terpenes, storage mites and enzymes. A considerable part of the biogenic allergens in agriculture comes from proteins from animal skin, hair from furs and protein from the faecal material and urine. Allergens might be found in many industrial environments, such as fermentation processes, drug production, bakeries, paper production, wood processing (saw mills, production, manufacturing) as well as in bio-technology (enzyme and vaccine production, tissue culture) and spice production. In sensitized persons, exposure to the allergic agents may induce allergic symptoms such as allergic rhinitis, conjunctivitis or asthma. Allergic alveolitis is characterized by acute respiratory symptoms like cough, chills, fever, headache and pain in the muscles, which might lead to chronic lung fibrosis. |
Occupational asthma: wool, furs, wheat grain, flour, red cedar, garlic powder Allergic alveolitis: farmer’s disease, bagassosis, “bird fancier’s disease”, humidifier fever, sequoiosis
|
|
PHYSICAL HAZARDS |
|
|
|
Noise |
Noise is considered as any unwanted sound that may adversely affect the health and well-being of individuals or populations. Aspects of noise hazards include total energy of the sound, frequency distribution, duration of exposure and impulsive noise. Hearing acuity is generally affected first with a loss or dip at 4000 Hz followed by losses in the frequency range from 2000 to 6000 Hz. Noise might result in acute effects like communication problems, decreased concentration, sleepiness and as a consequence interference with job performance. Exposure to high levels of noise (usually above 85 dBA) or impulsive noise (about 140 dBC) over a significant period of time may cause both temporary and chronic hearing loss. Permanent hearing loss is the most common occupational disease in compensation claims. |
Foundries, woodworking, textile mills, metalworking |
|
Vibration |
Vibration has several parameters in common with noise-frequency, amplitude, duration of exposure and whether it is continuous or intermittent. Method of operation and skilfulness of the operator seem to play an important role in the development of harmful effects of vibration. Manual work using powered tools is associated with symptoms of peripheral circulatory disturbance known as “Raynaud’s phenomenon” or “vibration-induced white fingers” (VWF). Vibrating tools may also affect the peripheral nervous system and the musculo-skeletal system with reduced grip strength, low back pain and degenerative back disorders. |
Contract machines, mining loaders, fork-lift trucks, pneumatic tools, chain saws |
|
Ionizing radiation
|
The most important chronic effect of ionizing radiation is cancer, including leukaemia. Overexposure from comparatively low levels of radiation have been associated with dermatitis of the hand and effects on the haematological system. Processes or activities which might give excessive exposure to ionizing radiation are very restricted and regulated. |
Nuclear reactors, medical and dental x-ray tubes, particle accelerators, radioisotopes |
|
Non-ionizing radiation
|
Non-ionizing radiation consists of ultraviolet radiation, visible radiation, infrared, lasers, electromagnetic fields (microwaves and radio frequency) and extreme low frequency radiation. IR radiation might cause cataracts. High-powered lasers may cause eye and skin damage. There is an increasing concern about exposure to low levels of electromagnetic fields as a cause of cancer and as a potential cause of adverse reproductive outcomes among women, especially from exposure to video display units. The question about a causal link to cancer is not yet answered. Recent reviews of available scientific knowledge generally conclude that there is no association between use of VDUs and adverse reproductive outcome. |
Ultraviolet radiation: arc welding and cutting; UV curing of inks, glues, paints, etc.; disinfection; product control Infrared radiation: furnaces, glassblowing Lasers: communications, surgery, construction
|
Identification and Classification of Hazards
Before any occupational hygiene investigation is performed the purpose must be clearly defined. The purpose of an occupational hygiene investigation might be to identify possible hazards, to evaluate existing risks at the workplace, to prove compliance with regulatory requirements, to evaluate control measures or to assess exposure with regard to an epidemiological survey. This article is restricted to programmes aimed at identification and classification of hazards at the workplace. Many models or techniques have been developed to identify and evaluate hazards in the working environment. They differ in complexity, from simple checklists, preliminary industrial hygiene surveys, job-exposure matrices and hazard and operability studies to job exposure profiles and work surveillance programmes (Renes 1978; Gressel and Gideon 1991; Holzner, Hirsh and Perper 1993; Goldberg et al. 1993; Bouyer and Hémon 1993; Panett, Coggon and Acheson 1985; Tait 1992). No single technique is a clear choice for everyone, but all techniques have parts which are useful in any investigation. The usefulness of the models also depends on the purpose of the investigation, size of workplace, type of production and activity as well as complexity of operations.
Identification and classification of hazards can be divided into three basic elements: workplace characterization, exposure pattern and hazard evaluation.
Workplace characterization
A workplace might have from a few employees up to several thousands and have different activities (e.g., production plants, construction sites, office buildings, hospitals or farms). At a workplace different activities can be localized to special areas such as departments or sections. In an industrial process, different stages and operations can be identified as production is followed from raw materials to finished products.
Detailed information should be obtained about processes, operations or other activities of interest, to identify agents utilized, including raw materials, materials handled or added in the process, primary products, intermediates, final products, reaction products and by-products. Additives and catalysts in a process might also be of interest to identify. Raw material or added material which has been identified only by trade name must be evaluated by chemical composition. Information or safety data sheets should be available from manufacturer or supplier.
Some stages in a process might take place in a closed system without anyone exposed, except during maintenance work or process failure. These events should be recognized and precautions taken to prevent exposure to hazardous agents. Other processes take place in open systems, which are provided with or without local exhaust ventilation. A general description of the ventilation system should be provided, including local exhaust system.
When possible, hazards should be identified in the planning or design of new plants or processes, when changes can be made at an early stage and hazards might be anticipated and avoided. Conditions and procedures that may deviate from the intended design must be identified and evaluated in the process state. Recognition of hazards should also include emissions to the external environment and waste materials. Facility locations, operations, emission sources and agents should be grouped together in a systematic way to form recognizable units in the further analysis of potential exposure. In each unit, operations and agents should be grouped according to health effects of the agents and estimation of emitted amounts to the work environment.
Exposure patterns
The main exposure routes for chemical and biological agents are inhalation and dermal uptake or incidentally by ingestion. The exposure pattern depends on frequency of contact with the hazards, intensity of exposure and time of exposure. Working tasks have to be systematically examined. It is important not only to study work manuals but to look at what actually happens at the workplace. Workers might be directly exposed as a result of actually performing tasks, or be indirectly exposed because they are located in the same general area or location as the source of exposure. It might be necessary to start by focusing on working tasks with high potential to cause harm even if the exposure is of short duration. Non-routine and intermittent operations (e.g., maintenance, cleaning and changes in production cycles) have to be considered. Working tasks and situations might also vary throughout the year.
Within the same job title exposure or uptake might differ because some workers wear protective equipment and others do not. In large plants, recognition of hazards or a qualitative hazard evaluation very seldom can be performed for every single worker. Therefore workers with similar working tasks have to be classified in the same exposure group. Differences in working tasks, work techniques and work time will result in considerably different exposure and have to be considered. Persons working outdoors and those working without local exhaust ventilation have been shown to have a larger day-to-day variability than groups working indoors with local exhaust ventilation (Kromhout, Symanski and Rappaport 1993). Work processes, agents applied for that process/job or different tasks within a job title might be used, instead of the job title, to characterize groups with similar exposure. Within the groups, workers potentially exposed must be identified and classified according to hazardous agents, routes of exposure, health effects of the agents, frequency of contact with the hazards, intensity and time of exposure. Different exposure groups should be ranked according to hazardous agents and estimated exposure in order to determine workers at greatest risk.
Qualitative hazard evaluation
Possible health effects of chemical, biological and physical agents present at the workplace should be based on an evaluation of available epidemiological, toxicological, clinical and environmental research. Up-to-date information about health hazards for products or agents used at the workplace should be obtained from health and safety journals, databases on toxicity and health effects, and relevant scientific and technical literature.
Material Safety Data Sheets (MSDSs) should if necessary be updated. Data Sheets document percentages of hazardous ingredients together with the Chemical Abstracts Service chemical identifier, the CAS-number, and threshold limit value (TLV), if any. They also contain information about health hazards, protective equipment, preventive actions, manufacturer or supplier, and so on. Sometimes the ingredients reported are rather rudimentary and have to be supplemented with more detailed information.
Monitored data and records of measurements should be studied. Agents with TLVs provide general guidance in deciding whether the situation is acceptable or not, although there must be allowance for possible interactions when workers are exposed to several chemicals. Within and between different exposure groups, workers should be ranked according to health effects of agents present and estimated exposure (e.g., from slight health effects and low exposure to severe health effects and estimated high exposure). Those with the highest ranks deserve highest priority. Before any prevention activities start it might be necessary to perform an exposure monitoring programme. All results should be documented and easily attainable. A working scheme is illustrated in figure 1.
Figure 1. Elements of risk assessment
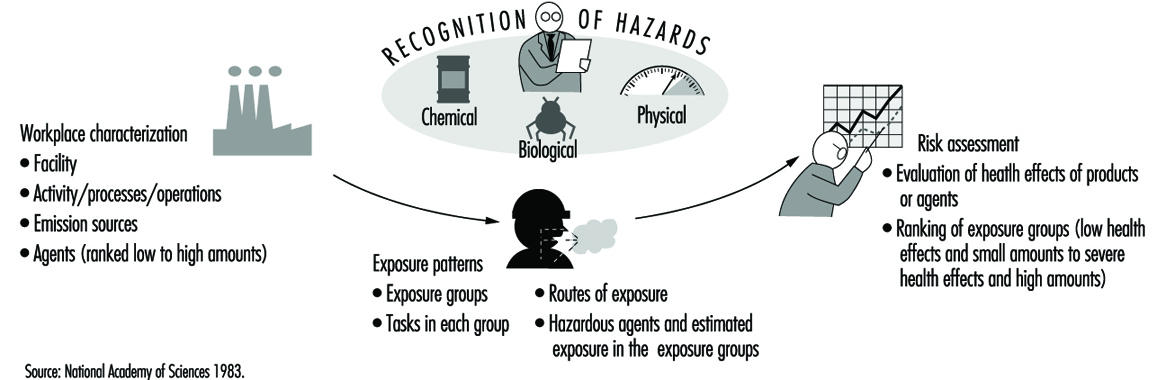
In occupational hygiene investigations the hazards to the outdoor environment (e.g., pollution and greenhouse effects as well as effects on the ozone layer) might also be considered.
Chemical, Biological and Physical Agents
Hazards might be of chemical, biological or physical origin. In this section and in table 1 a brief description of the various hazards will be given together with examples of environments or activities where they will be found (Casarett 1980; International Congress on Occupational Health 1985; Jacobs 1992; Leidel, Busch and Lynch 1977; Olishifski 1988; Rylander 1994). More detailed information will be found elsewhere in this Encyclopaedia.
Chemical agents
Chemicals can be grouped into gases, vapours, liquids and aerosols (dusts, fumes, mists).
Gases
Gases are substances that can be changed to liquid or solid state only by the combined effects of increased pressure and decreased temperature. Handling gases always implies risk of exposure unless they are processed in closed systems. Gases in containers or distribution pipes might accidentally leak. In processes with high temperatures (e.g., welding operations and exhaust from engines) gases will be formed.
Vapours
Vapours are the gaseous form of substances that normally are in the liquid or solid state at room temperature and normal pressure. When a liquid evaporates it changes to a gas and mixes with the surrounding air. A vapour can be regarded as a gas, where the maximal concentration of a vapour depends on the temperature and the saturation pressure of the substance. Any process involving combustion will generate vapours or gases. Degreasing operations might be performed by vapour phase degreasing or soak cleaning with solvents. Work activities like charging and mixing liquids, painting, spraying, cleaning and dry cleaning might generate harmful vapours.
Liquids
Liquids may consist of a pure substance or a solution of two or more substances (e.g., solvents, acids, alkalis). A liquid stored in an open container will partially evaporate into the gas phase. The concentration in the vapour phase at equilibrium depends on the vapour pressure of the substance, its concentration in the liquid phase, and the temperature. Operations or activities with liquids might give rise to splashes or other skin contact, besides harmful vapours.
Dusts
Dusts consist of inorganic and organic particles, which can be classified as inhalable, thoracic or respirable, depending on particle size. Most organic dusts have a biological origin. Inorganic dusts will be generated in mechanical processes like grinding, sawing, cutting, crushing, screening or sieving. Dusts may be dispersed when dusty material is handled or whirled up by air movements from traffic. Handling dry materials or powder by weighing, filling, charging, transporting and packing will generate dust, as will activities like insulation and cleaning work.
Fumes
Fumes are solid particles vaporized at high temperature and condensed to small particles. The vaporization is often accompanied by a chemical reaction such as oxidation. The single particles that make up a fume are extremely fine, usually less than 0.1 μm, and often aggregate in larger units. Examples are fumes from welding, plasma cutting and similar operations.
Mists
Mists are suspended liquid droplets generated by condensation from the gaseous state to the liquid state or by breaking up a liquid into a dispersed state by splashing, foaming or atomizing. Examples are oil mists from cutting and grinding operations, acid mists from electroplating, acid or alkali mists from pickling operations or paint spray mists from spraying operations.