The connection between the use of a building either as a workplace or as a dwelling and the appearance, in certain cases, of discomfort and symptoms that may be the very definition of an illness is a fact that can no longer be disputed. The main culprit is contamination of various kinds within the building, and this contamination is usually referred to as “poor quality of indoor air”. The adverse effects due to poor air quality in closed spaces affect a considerable number of people, since it has been shown that urban dwellers spend between 58 and 78% of their time in an indoor environment which is contaminated to a greater or lesser degree. These problems have increased with the construction of buildings that are designed to be more airtight and that recycle air with a smaller proportion of new air from the outside in order to be more energy efficient. The fact that buildings that do not offer natural ventilation present risks of exposure to contaminants is now generally accepted.
The term indoor air is usually applied to nonindustrial indoor environments: office buildings, public buildings (schools, hospitals, theatres, restaurants, etc.) and private dwellings. Concentrations of contaminants in the indoor air of these structures are usually of the same order as those commonly found in outdoor air, and are much lower than those found in air in industrial premises, where relatively well-known standards are applied in order to assess air quality. Even so, many building occupants complain of the quality of the air they breathe and there is therefore a need to investigate the situation. Indoor air quality began to be referred to as a problem at the end of the 1960s, although the first studies did not appear until some ten years later.
Although it would seem logical to think that good air quality is based on the presence in the air of the necessary components in suitable proportions, in reality it is the user, through respiration, who is the best judge of its quality. This is because inhaled air is perceived perfectly through the senses, as human beings are sensitive to the olfactory and irritant effects of about half a million chemical compounds. Consequently, if the occupants of a building are as a whole satisfied with the air, it is said to be of high quality; if they are unsatisfied, it is of poor quality. Does this mean that it is possible to predict on the basis of its composition how the air will be perceived? Yes, but only in part. This method works well in industrial environments, where specific chemical compounds related to production are known, and their concentrations in the air are measured and compared with threshold limit values. But in nonindustrial buildings where there may be thousands of chemical substances in the air but in such low concentrations that they are, perhaps, thousands of times less than the limits set for industrial environments, the situation is different. In most of these cases information about the chemical composition of indoor air does not allow us to predict how the air will be perceived, since the combined effect of thousands of these contaminants, together with temperature and humidity, can produce air that is perceived as irritating, foul, or stale—that is, of poor quality. The situation is comparable to what happens with the detailed composition of an item of food and its taste: chemical analysis is inadequate to predict whether the food will taste good or bad. For this reason, when a ventilation system and its regular maintenance are being planned, an exhaustive chemical analysis of indoor air is rarely called for.
Another point of view is that people are considered the only sources of contamination in indoor air. This would certainly be true if we were dealing with building materials, furniture and ventilation systems as they were used 50 years ago, when bricks, wood and steel predominated. But with modern materials the situation has changed. All materials contaminate, some a little and others much, and together they contribute to a deterioration in the quality of indoor air.
The changes in a person’s health due to poor indoor air quality can show up as a wide array of acute and chronic symptoms and in the form of a number of specific illnesses. These are illustrated in figure 1. Although poor indoor air quality results in fully developed illness in only a few cases, it can give rise to malaise, stress, absenteeism and loss of productivity (with concomitant increases in production costs); and allegations about problems related to the building can develop rapidly into conflict between the occupants, their employers and the owners of the buildings.
Figure 1. Symptoms and illnesses related to the quality of indoor air.

Normally it is difficult to establish precisely to what extent poor indoor air quality can harm health, since not enough information is available concerning the relationship between exposure and effect at the concentrations in which the contaminants are usually found. Hence, there is a need to take information obtained at high doses—as with exposures in industrial settings—and extrapolate to much lower doses with a corresponding margin of error. In addition, for many contaminants present in the air, the effects of acute exposure are well known, whereas there are considerable gaps in the data regarding both long-term exposures at low concentrations and mixtures of different contaminants. The concepts of no-effect-level (NOEL), harmful effect and tolerable effect, already confusing even in the sphere of industrial toxicology, are here even more difficult to define. There are few conclusive studies on the subject, whether relating to public buildings and offices or private dwellings.
Series of standards for outdoor air quality exist and are relied on to protect the general population. They have been obtained by measuring adverse effects on health resulting from exposure to contaminants in the environment. These standards are therefore useful as general guidelines for an acceptable quality of indoor air, as is the case with those proposed by the World Health Organization. Technical criteria such as the threshold limit value of the American Conference of Governmental Industrial Hygienists (ACGIH) in the United States and the limit values legally established for industrial environments in different countries have been set for the working, adult population and for specific lengths of exposure, and cannot therefore be applied directly to the general population. The American Society of Heating, Refrigeration and Air Conditioning Engineers (ASHRAE) in the United States has developed a series of standards and recommendations that are widely used in assessing indoor air quality.
Another aspect that should be considered as part of the quality of indoor air is its smell, because smell is often the parameter that ends up being the defining factor. The combination of a certain smell with the slight irritating effect of a compound in indoor air can lead us to define its quality as “fresh” and “clean” or as “stale” and “polluted”. Smell is therefore very important when defining the quality of indoor air. While odours objectively depend on the presence of compounds in quantities above their olfactory thresholds, they are very often evaluated from a strictly subjective point of view. It should also be kept in mind that the perception of an odour may result from the smells of many different compounds and that temperature and humidity may also affect its characteristics. From the standpoint of perception there are four characteristics that allow us to define and measure odours: intensity, quality, tolerability and threshold. When considering indoor air, however, it is very difficult to “measure” odours from a chemical standpoint. For that reason the tendency is to eliminate odours that are “bad” and to use, in their place, those considered good in order to give air a pleasant quality. The attempt to mask bad odours with good ones usually ends in failure, because odours of very different qualities can be recognized separately and lead to unforeseeable results.
A phenomenon known as sick building syndrome occurs when more than 20% of the occupants of a building complain about air quality or have definite symptoms. It is evidenced by a variety of physical and environmental problems associated with non-industrial indoor environments. The most common features seen in cases of sick building syndrome are the following: those affected complain of non-specific symptoms similar to the common cold or respiratory illnesses; the buildings are efficient as regards energy conservation and are of modern design and construction or recently remodelled with new materials; and the occupants cannot control the temperature, humidity and illumination of the workplace. The estimated percentage distribution of the most common causes of sick building syndrome are inadequate ventilation due to lack of maintenance; poor distribution and insufficient intake of fresh air (50 to 52%); contamination generated indoors, including from office machines, tobacco smoke and cleaning products (17 to 19%); contamination from the outside of the building due to inadequate placement of air intake and exhaust vents (11%); microbiological contamination from stagnant water in the ducts of the ventilation system, humidifiers and refrigeration towers (5%); and formaldehyde and other organic compounds emitted by building and decoration materials (3 to 4%). Thus, ventilation is cited as an important contributory factor in the majority of cases.
Another question of a different nature is that of building-related illnesses, which are less frequent, but often more serious, and are accompanied by very definite clinical signs and clear laboratory findings. Examples of building-related illnesses are hypersensitivity pneumonitis, humidifier fever, legionellosis and Pontiac fever. A fairly general opinion among investigators is that these conditions should be considered separately from sick building syndrome.
Studies have been done to ascertain both the causes of air quality problems and their possible solutions. In recent years, knowledge of the contaminants present in indoor air and the factors contributing to a decline in indoor air quality has increased considerably, although there is a long way to go. Studies carried out in the last 20 years have shown that the presence of contaminants in many indoor environments is higher than anticipated, and moreover, different contaminants have been identified from those that exist in outside air. This contradicts the assumption that indoor environments without industrial activity are relatively free of contaminants and that in the worst of cases they may reflect the composition of outside air. Contaminants such as radon and formaldehyde are identified almost exclusively in the indoor environment.
Indoor air quality, including that of dwellings, has become a question of environmental health in the same way as has happened with control of outdoor air quality and exposure at work. Although, as already mentioned, an urban person spends 58 to 78% of his or her time indoors, it should be remembered that the most susceptible persons, namely the elderly, small children and the sick, are the ones who spend most of their time indoors. This subject began to be particularly topical from around 1973 onwards, when, because of the energy crisis, efforts directed at energy conservation concentrated on reducing the entry of outside air into indoor spaces as much as possible in order to minimize the cost of heating and cooling buildings. Although not all the problems relating to indoor air quality are the result of actions aimed at saving energy, it is a fact that as this policy spread, complaints about indoor air quality began to increase, and all the problems appeared.
Another item requiring attention is the presence of micro-organisms in indoor air which can cause problems of both an infectious and an allergic nature. It should not be forgotten that micro-organisms are a normal and essential component of ecosystems. For example, saprophytic bacteria and fungi, which obtain their nutrition from dead organic material in the environment, are found normally in the soil and atmosphere, and their presence can also be detected indoors. In recent years problems of biological contamination in indoor environments have received considerable attention.
The outbreak of Legionnaire’s disease in 1976 is the most discussed case of an illness caused by a micro-organism in the indoor environment. Other infectious agents, such as viruses that can cause acute respiratory illness, are detectable in indoor environments, especially if the occupation density is high and much recirculation of air is taking place. In fact, the extent to which micro-organisms or their components are implicated in the outbreak of building-associated conditions is not known. Protocols for demonstrating and analysing many types of microbial agents have been developed only to a limited degree, and in those cases where they are available, the interpretation of the results is sometimes inconsistent.
Aspects of the Ventilation System
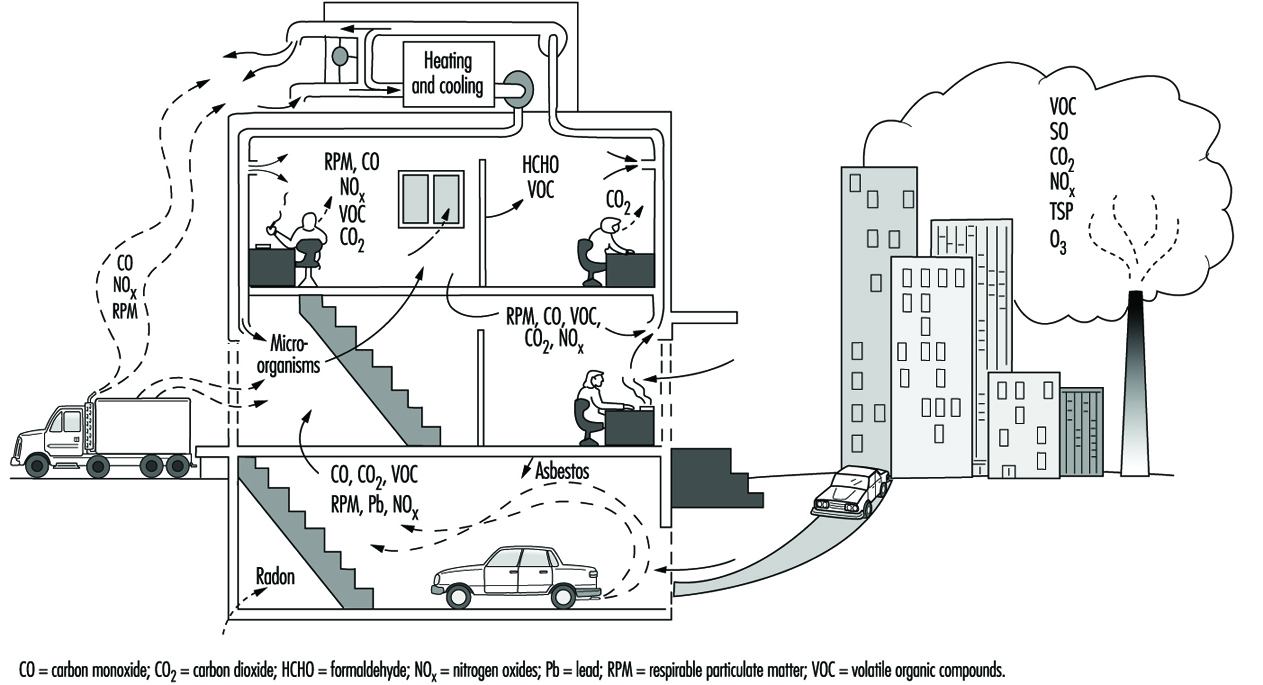
Indoor air quality in a building is a function of a series of variables which include the quality of the outdoor air, the design of the ventilation and air-conditioning system, the conditions in which this system operates and is serviced, the compartmentalization of the building and the presence of indoor sources of contaminants and their magnitude. (See figure 2) By way of summary it may be noted that the most common defects are the result of inadequate ventilation, contamination generated indoors and contamination coming from outside.
Figure 2. Diagram of building showing sources of indoor and outdoor pollutants.
Regarding the first of these problems, causes of inadequate ventilation can include: an insufficient supply of fresh air due to a high level of recirculation of the air or a low volume of intake; incorrect placement and orientation in the building of intake points for outside air; poor distribution and consequently incomplete mixing with the air of the premises, which can produce stratification, unventilated zones, unforeseen pressure differences giving rise to unwanted air currents and continuous changes in the thermohygrometric characteristics noticeable as one moves about the building—and incorrect filtration of the air because of lack of maintenance or inadequate design of the filtering system—a deficiency which is particularly serious where the outdoor air is of poor quality or where there is a high level of recirculation.
Origins of Contaminants
Indoor contamination has different origins: the occupants themselves; inadequate materials or materials with technical defects used in the construction of the building; the work performed within; excessive or improper use of normal products (pesticides, disinfectants, products used for cleaning and polishing); combustion gases (from smoking, kitchens, cafeterias and laboratories); and cross-contamination coming from other poorly ventilated zones which then diffuses towards neighbouring areas and affects them. It should be borne in mind that substances emitted in indoor air have much less opportunity of being diluted than those emitted in outdoor air, given the difference in the volumes of air available. As regards biological contamination, its origin is most frequently due to the presence of stagnant water, materials impregnated with water, exhausts and so on, and to defective maintenance of humidifiers and refrigeration towers.
Finally, contamination coming from outside must also be considered. As regards human activity, three main sources may be mentioned: combustion in stationary sources (power stations); combustion in moving sources (vehicles); and industrial processes. The five main contaminants emitted by these sources are carbon monoxide, oxides of sulphur, oxides of nitrogen, volatile organic compounds (including hydrocarbons), polycyclic aromatic hydrocarbons and particles. Internal combustion in vehicles is the principal source of carbon monoxide and hydrocarbons and is an important source of oxides of nitrogen. Combustion in stationary sources is the main origin of oxides of sulphur. Industrial processes and stationary sources of combustion generate more than half of the particles emitted into the air by human activity, and industrial processes can be a source of volatile organic compounds. There are also contaminants generated naturally that are propelled through the air, such as particles of volcanic dust, soil and sea salt, and spores and micro-organisms. The composition of outdoor air varies from place to place, depending both on the presence and the nature of the sources of contamination in the vicinity and on the direction of the prevailing wind. If there are no sources generating contaminants, the concentration of certain contaminants that will typically be found in “clean” outdoor air are as follows: carbon dioxide, 320 ppm; ozone, 0.02 ppm: carbon monoxide, 0.12 ppm; nitric oxide, 0.003 ppm; and nitrogen dioxide, 0.001 ppm. However, urban air always contains much higher concentrations of these contaminants.
Apart from the presence of the contaminants originating from outside, it sometimes happens that contaminated air from the building itself is expelled to the exterior and then returns inside again through the intakes of the air-conditioning system. Another possible way by which contaminants may enter from the exterior is by infiltration through the foundations of the building (e.g., radon, fuel vapors, sewer effluvia, fertilizers, insecticides and disinfectants). It has been shown that when the concentration of a contaminant in the outdoor air increases, its concentration in the air inside the building also increases, although more slowly (a corresponding relationship obtains when the concentration decreases); it is therefore said that buildings exert a shielding effect against external contaminants. However, the indoor environment is not, of course, an exact reflection of the conditions outside.
Contaminants present in indoor air are diluted in the outdoor air that enters the building and they accompany it when it leaves. When the concentration of a contaminant is less in the outdoor air than the indoor air, the interchange of indoor and outdoor air will result in a reduction in the concentration of the contaminant in the air inside the building. If a contaminant originates from outside and not inside, this interchange will result in a rise in its indoor concentration, as mentioned above.
Models for the balance of amounts of contaminants in indoor air are based on the calculation of their accumulation, in units of mass versus time, from the difference between the quantity that enters plus what is generated indoors, and what leaves with the air plus what is eliminated by other means. If appropriate values are available for each of the factors in the equation, the indoor concentration can be estimated for a wide range of conditions. Use of this technique makes possible the comparison of different alternatives for controlling an indoor contamination problem.
Buildings with low interchange rates with outdoor air are classified as sealed or energy-efficient. They are energy-efficient because less cold air enters in winter, reducing the energy required to heat the air to the ambient temperature, thus cutting the cost of heating. When the weather is hot, less energy is also used to cool the air. If the building does not have this property, it is ventilated through open doors and windows by a process of natural ventilation. Although they may be closed, differences of pressure, resulting both from the wind and from the thermal gradient existing between the interior and the exterior, force the air to enter through crevices and cracks, window and door joints, chimneys and other apertures, giving rise to what is called ventilation by infiltration.
The ventilation of a building is measured in renewals per hour. One renewal per hour means that a volume of air equal to the volume of the building enters from outside every hour; in the same way, an equal volume of indoor air is expelled to the exterior every hour. If there is no forced ventilation (with a ventilator) this value is difficult to determine, although it is considered to vary between 0.2 and 2.0 renewals per hour. If the other parameters are assumed to be unchanged, the concentration of contaminants generated indoors will be less in buildings with high renewal values, although a high renewal value is not a complete guarantee of indoor air quality. Except in areas with marked atmospheric pollution, buildings that are more open will have a lower concentration of contaminants in the indoor air than those constructed in a more closed manner. However, buildings that are more open are less energy-efficient. The conflict between energy efficiency and air quality is of great importance.
Much action undertaken to reduce energy costs affects indoor air quality to a greater or lesser extent. In addition to reducing the speed with which the air circulates within the building, efforts to increase the insulation and waterproofing of the building involve the installation of materials that may be sources of indoor contamination. Other action, such as supplementing old and frequently inefficient central heating systems with secondary sources that heat or consume the indoor air can also raise contaminant levels in indoor air.
Contaminants whose presence in indoor air is most frequently mentioned, apart from those coming from outside, include metals, asbestos and other fibrous materials, formaldehyde, ozone, pesticides and organic compounds in general, radon, house dust and biological aerosols. Together with these, a wide variety of types of micro-organisms can be found, such as fungi, bacteria, viruses and protozoa. Of these, the saprophytic fungi and bacteria are relatively well known, probably because a technology is available for measuring them in air. The same is not true of agents such as viruses, rickettsiae, chlamydias, protozoa and many pathogenic fungi and bacteria, for the demonstration and counting of which no methodology is as yet available. Among the infectious agents, special mention should be made of: Legionella pneumophila, Mycobacterium avium, viruses, Coxiella burnetii and Histoplasma capsulatum; and among the allergens: Cladosporium, Penicillium and Cytophaga.
Investigating Indoor Air Quality
Experience so far suggests that the traditional techniques used in industrial hygiene and heating, ventilation and air-conditioning do not always provide satisfactory results at present for solving the ever more common problems of indoor air quality, although basic knowledge of these techniques permits good approximations for dealing with or reducing problems rapidly and inexpensively. The solution to problems of indoor air quality often requires, in addition to one or more experts in heating, ventilation and air-conditioning and industrial hygiene, specialists in indoor air quality control, analytical chemistry, toxicology, environmental medicine, microbiology, and also epidemiology and psychology.
When a study is carried out on indoor air quality, the objectives set for it will profoundly affect its design and the activities directed at sampling and evaluation, since in some cases procedures giving a rapid response will be required, while in others overall values will be of interest. The duration of the programme will be dictated by the time required to obtain representative samples, and will also depend on the season and on meteorological conditions. If the aim is to carry out an exposure-effect study, in addition to long-term and short-term samples for evaluating peaks, personal samples will be required for ascertaining the direct exposure of individuals.
For some contaminants, well-validated and widely used methods are available, but for the majority this is not the case. Techniques for measuring levels of many contaminants found indoors are normally derived from applications in industrial hygiene but, given that the concentrations of interest in indoor air are usually much lower than those occurring in industrial environments, these methods are frequently inappropriate. As for the measurement methods used in atmospheric contamination, they operate with margins of similar concentrations, but are available for relatively few contaminants and present difficulties in indoor use, such as would arise, for example, with a high-volume sampler for determining particulate matter, which on the one hand would be too noisy and on the other could modify the quality of the indoor air itself.
The determination of contaminants in indoor air is usually carried out by using different procedures: with continuous monitors, whole-time active samplers, whole-time passive samplers, direct sampling and personal samplers. Adequate procedures exist at present for measuring levels of formaldehyde, oxides of carbon and nitrogen, volatile organic compounds and radon, among others. Biological contaminants are measured using techniques of sedimentation on open culture plates or, more frequently nowadays, by using active systems that cause the air to impact on plates containing nutrient, which are subsequently cultured, the quantity of micro-organisms present being expressed in colony-forming units per cubic meter.
When a problem of indoor air quality is being investigated, it is usual to design beforehand a practical strategy consisting of an approximation in phases. This approximation begins with a first phase, the initial investigation, which can be carried out using industrial hygiene techniques. It must be structured so that the investigator does not need to be a specialist in the field of indoor air quality in order to carry out his work. A general inspection of the building is undertaken and its installations are checked, particularly as regards the regulation and adequate functioning of the heating, ventilation and air-conditioning system, according to the standards set at the time of its installation. It is important in this respect to consider whether the persons affected are able to modify the conditions of their surroundings. If the building does not have systems of forced ventilation, the degree of effectiveness of the existing natural ventilation must be studied. If after revision—and adjustment if necessary—the operational conditions of the ventilation systems are adequate for the standards, and if despite this the complaints continue, a technical investigation of a general kind will have to ensue to determine the degree and nature of the problem. This initial investigation should also allow an assessment to be made as to whether the problems can be considered solely from the functional point of view of the building, or whether the intervention of specialists in hygiene, psychology or other disciplines will be necessary.
If the problem is not identified and resolved in this first phase, other phases can follow involving more specialized investigations concentrating on potential problems identified in the first phase. The subsequent investigations may include a more detailed analysis of the heating, ventilation and air-conditioning system of the building, a more extensive evaluation of the presence of materials suspected of emitting gases and particles, a detailed chemical analysis of the ambient air in the building and medical or epidemiological assessments to detect signs of disease.
As regards the heating, ventilation and air-conditioning system, the refrigeration equipment should be checked in order to ensure that there is no microbial growth in them or accumulation of water in their drip trays, the ventilation units must be checked to see that they are functioning correctly, the air intake and return systems must be examined at various points to see that they are watertight, and the interior of a representative number of ducts must be checked to confirm the absence of micro-organisms. This last consideration is particularly important when humidifiers are used. These units require particularly careful programmes of maintenance, operation and inspection in order to prevent the growth of micro-organisms, which can propagate themselves throughout the air-conditioning system.
The options generally considered for improving indoor air quality in a building are the elimination of the source; its insulation or independent ventilation; separating the source from those who may be affected; general cleaning of the building; and increased checking and improvement of the heating, ventilation and air-conditioning system. This may require anything from modifications at particular points to a new design. The process is frequently of a repetitive nature, so that the study has to be started again several times, using more sophisticated techniques on each occasion. A more detailed description of control techniques will be found elsewhere in this Encyclopaedia.
Finally, it should be emphasized that, even with the most complete investigations of indoor air quality, it may be impossible to establish a clear relationship between the characteristics and composition of the indoor air and the health and comfort of the occupants of the building under study. Only the accumulation of experience on the one hand, and the rational design of ventilation, occupation and compartmentalization of buildings on the other, are possible guarantees from the outset of obtaining indoor air quality that is adequate for the majority of the occupants of a building.