Occupational Exposure
Occupational exposures to whole-body vibration mainly occur in transport but also in association with some industrial processes. Land, sea and air transport can all produce vibration that can cause discomfort, interfere with activities or cause injury. Table 1 lists some environments which may be most likely to be associated with a health risk.
Table 1. Activities for which it may be appropriate to warn of the adverse effects of whole-body vibration
Tractor driving
Armoured fighting vehicles (e.g., tanks) and similar vehicles
Other off-road vehicles:
Earth-moving machinery—loaders, excavators, bulldozers, graders,
- scrapers, dumpers, rollers
- Forest machines
- Mine and quarry equipment
- Forklift trucks
Some truck driving (articulated and non-articulated)
Some bus and tram driving
Some helicopter and fixed-wing aircraft flying
Some workers with concrete production machinery
Some railway drivers
Some use of high-speed marine craft
Some motor bicycle riding
Some car and van driving
Some sports activities
Some other industrial equipment
Source: Adapted from Griffin 1990.
The most common exposure to severe vibration and shocks may occur on off-road vehicles, including earth moving machinery, industrial trucks and agricultural tractors.
Biodynamics
Like all mechanical structures, the human body has resonance frequencies where the body exhibits a maximum mechanical response. Human responses to vibration cannot be explained solely in terms of a single resonance frequency. There are many resonances in the body, and the resonance frequencies vary among people and with posture. Two mechanical responses of the body are often used to describe the manner in which vibration causes the body to move: transmissibility and impedance.
The transmissibility shows the fraction of the vibration which is transmitted from, say, the seat to the head. The transmissibility of the body is highly dependent on vibration frequency, vibration axis and body posture. Vertical vibration on a seat causes vibration in several axes at the head; for vertical head motion, the transmissibility tends to be greatest in the approximate range of 3 to 10 Hz.
The mechanical impedance of the body shows the force that is required to make the body move at each frequency. Although the impedance depends on body mass, the vertical impedance of the human body usually shows a resonance at about 5 Hz. The mechanical impedance of the body, including this resonance, has a large effect on the manner in which vibration is transmitted through seats.
Acute Effects
Discomfort
The discomfort caused by vibration acceleration depends on the vibration frequency, the vibration direction, the point of contact with the body, and the duration of vibration exposure. For vertical vibration of seated persons, the vibration discomfort caused by any frequency increases in proportion to the vibration magnitude: a halving of the vibration will tend to halve the vibration discomfort.
The discomfort produced by vibration may be predicted by the use of appropriate frequency weightings (see below) and described by a semantic scale of discomfort. There are no useful limits for vibration discomfort: the acceptable discomfort varies from one environment to another.
Acceptable magnitudes of vibration in buildings are close to vibration perception thresholds. The effects on humans of vibration in buildings are assumed to depend on the use of the building in addition to the vibration frequency, direction and duration. Guidance on the evaluation of building vibration is given in various standards such as British Standard 6472 (1992) which defines a procedure for the evaluation of both vibration and shock in buildings.
Activity interference
Vibration can impair the acquisition of information (e.g., by the eyes), the output of information (e.g., by hand or foot movements) or the complex central processes that relate input to output (e.g., learning, memory, decision-making). The greatest effects of whole-body vibration are on input processes (mainly vision) and output processes (mainly continuous hand control).
Effects of vibration on vision and manual control are primarily caused by the movement of the affected part of the body (i.e., eye or hand). The effects may be decreased by reducing the transmission of vibration to the eye or to the hand, or by making the task less susceptible to disturbance (e.g., increasing the size of a display or reducing the sensitivity of a control). Often, the effects of vibration on vision and manual control can be much reduced by redesign of the task.
Simple cognitive tasks (e.g., simple reaction time) appear to be unaffected by vibration, other than by changes in arousal or motivation or by direct effects on input and output processes. This may also be true for some complex cognitive tasks. However, the sparsity and diversity of experimental studies does not exclude the possibility of real and significant cognitive effects of vibration. Vibration may influence fatigue, but there is little relevant scientific evidence, and none which supports the complex form of the “fatigue-decreased proficiency limit” offered in International Standard 2631 (ISO 1974, 1985).
Changes in Physiological Functions
Changes in physiological functions occur when subjects are exposed to a novel whole-body vibration environment in laboratory conditions. Changes typical of a “startle response” (e.g., increased heart rate) normalize quickly with continuing exposure, whereas other reactions either proceed or develop gradually. The latter can depend on all characteristics of vibration including the axis, the magnitude of acceleration, and the kind of vibration (sinusoidal or random), as well as on further variables such as circadian rhythm and characteristics of the subjects (see Hasan 1970; Seidel 1975; Dupuis and Zerlett 1986). Changes of physiological functions under field conditions often cannot be related to vibration directly, since vibration is often acting together with other significant factors, such as high mental strain, noise and toxic substances. Physiological changes are frequently less sensitive than psychological reactions (e.g., discomfort). If all available data on persistent physiological changes are summarized with respect to their first significant appearance depending on the magnitude and frequency of whole-body vibration, there is a boundary with a lower border around 0.7 m/s2 r.m.s. between 1 and 10 Hz, and rising up to 30 m/s2 r.m.s. at 100 Hz. Many animal studies have been performed, but their relevance to humans is doubtful.
Neuromuscular changes
During active natural motion, motor control mechanisms act as a feed-forward control that is constantly adjusted by additional feedback from sensors in muscles, tendons and joints. Whole-body vibration causes a passive artificial motion of the human body, a condition that is fundamentally different from the self-induced vibration caused by locomotion. The missing feed-forward control during whole-body vibration is the most distinct change of the normal physiological function of the neuromuscular system. The broader frequency range associated with whole-body vibration (between 0.5 and 100 Hz) compared to that for natural motion (between 2 and 8 Hz for voluntary movements, and below 4 Hz for locomotion) is a further difference that helps to explain reactions of the neuromuscular control mechanisms at very low and at high frequencies.
Whole-body vibration and transient acceleration cause an acceleration-related alternating activity in the electromyogram (EMG) of superficial back muscles of seated persons that requires a tonic contraction to be maintained. This activity is supposed to be of a reflex-like nature. It usually disappears completely if the vibrated subjects sit relaxed in a bent position. The timing of muscle activity depends on the frequency and magnitude of acceleration. Electromyographic data suggest that an increased spinal load can occur due to reduced muscular stabilization of the spine at frequencies from 6.5 to 8 Hz and during the initial phase of a sudden upward displacement. In spite of weak EMG activity caused by whole-body vibration, back muscle fatigue during vibration exposure can exceed that observed in normal sitting postures without whole-body vibration.
Tendon reflexes may be diminished or disappear temporarily during exposure to sinusoidal whole-body vibration at frequencies above 10 Hz. Minor changes of postural control after exposure to whole-body vibration are quite variable, and their mechanisms and practical significance are not certain.
Cardiovascular, respiratory, endocrine and metabolic changes
The observed changes persisting during exposure to vibration have been compared to those during moderate physical work (i.e., increases of heart rate, blood pressure and oxygen consumption) even at a vibration magnitude near to the limit of voluntary tolerance. The increased ventilation is partially caused by oscillations of the air in the respiratory system. Respiratory and metabolic changes may not correspond, possibly suggesting a disturbance of the respiration control mechanisms. Various and partially contradictory findings have been reported for changes of the adrenocorticotropic hormones (ACTH) and catecholamines.
Sensory and central nervous changes
Changes of vestibular function due to whole-body vibration have been claimed on the basis of an affected regulation of posture, although posture is controlled by a very complex system in which a disturbed vestibular function can be largely compensated by other mechanisms. Changes of the vestibular function seem to gain significance for exposures with very low frequencies or those near the resonance of the whole body. A sensory mismatch between vestibular, visual and proprioceptive (stimuli received within the tissues) information is supposed to be an important mechanism underlying physiological responses to some artificial motion environments.
Experiments with short-term and prolonged combined exposures to noise and whole-body vibration, seem to suggest that vibration has a minor synergistic effect on hearing. As a tendency, high intensities of whole-body vibration at 4 or 5 Hz were associated with higher additional temporary threshold shifts (TTS). There was no obvious relation between the additional TTS and exposure time. The additional TTS seemed to increase with higher doses of whole-body vibration.
Impulsive vertical and horizontal vibrations evoke brain potentials. Changes of the function of the human central nervous system have also been detected using auditory evoked brain potentials (Seidel et al. 1992). The effects were influenced by other environmental factors (e.g., noise), the difficulty of the task, and by the internal state of the subject (e.g., arousal, degree of attention towards the stimulus).
Long-Term Effects
Spinal health risk
Epidemiological studies have frequently indicated an elevated health risk for the spine in workers exposed for many years to intense whole-body vibration (e.g., work on tractors or earth-moving machines). Critical surveys of the literature have been prepared by Seidel and Heide (1986), Dupuis and Zerlett (1986) and Bongers and Boshuizen (1990). These reviews concluded that intense long-term whole-body vibration can adversely affect the spine and can increase the risk of low-back pain. The latter may be a secondary consequence of a primary degenerative change of the vertebrae and disks. The lumbar part of the vertebral column was found to be the most frequently affected region, followed by the thoracic region. A high rate of impairments of the cervical part, reported by several authors, seems to be caused by a fixed unfavourable posture rather than by vibration, although there is no conclusive evidence for this hypothesis. Only a few studies have considered the function of back muscles and found a muscular insufficiency. Some reports have indicated a significantly higher risk of the dislocation of lumbar disks. In several cross-sectional studies Bongers and Boshuizen (1990) found more low-back pain in drivers and helicopter pilots than in comparable reference workers. They concluded that professional vehicle driving and helicopter flying are important risk factors for low-back pain and back disorder. An increase in disability pensioning and long-term sick leave due to intervertebral disc disorders was observed among crane operators and tractor drivers.
Due to incomplete or missing data on exposure conditions in epidemiological studies, exact exposure-effect relationships have not been obtained. The existing data do not permit the substantiation of a no-adverse-effect level (i.e., safe limit) so as to reliably prevent diseases of the spine. Many years of exposure below or near the exposure limit of the current International Standard 2631 (ISO 1985) are not without risk. Some findings have indicated an increasing health risk with increased duration of exposure, although selection processes have made it difficult to detect a relation in the majority of studies. Thus, a dose-effect relationship cannot currently be established by epidemiological investigations. Theoretical considerations suggest marked detrimental effects of high peak loads acting on the spine during exposures with high transients. The use of an “energy equivalent” method to calculate a vibration dose (as in International Standard 2631 (ISO 1985)) is therefore questionable for exposures to whole-body vibration containing high peak accelerations. Different long-term effects of whole-body vibration depending on the vibration frequency have not been derived from epidemiological studies. Whole-body vibration at 40 to 50 Hz applied to standing workers through the feet was followed by degenerative changes of the bones of the feet.
In general, differences between subjects have been largely neglected, although selection phenomena suggest they may be of major importance. There are no clear data showing whether the effects of whole-body vibration on the spine depend on gender.
The general acceptance of degenerative disorders of the spine as an occupational disease is debated. Specific diagnostic features are not known which would permit a reliable diagnosis of the disorder as an outcome of exposure to whole-body vibration. A high prevalence of degenerative spinal disorders in non-exposed populations hinders the assumption of a predominantly occupational aetiology in individuals exposed to whole-body vibration. Individual constitutional risk factors that might modify vibration-induced strain are unknown. The use of a minimal intensity and/or a minimal duration of whole-body vibration as a prerequisite for the recognition of an occupational disease would not take into account the expected considerable variability in individual susceptibility.
Other health risks
Epidemiological studies suggest that whole-body vibration is one factor within a causative set of factors which contribute to other health risks. Noise, high mental strain and shift work are examples of important concomitant factors which are known to be associated with health disorders. The results of investigations into disorders of other bodily systems have often been divergent or have indicated a paradoxical dependence of the prevalence of pathology on the magnitude of whole-body vibration (i.e., a higher prevalence of adverse effects with a lower intensity). A characteristic complex of symptoms and pathological changes of the central nervous system, the musculo-skeletal system and the circulatory system has been observed in workers standing on machines used for the vibro-compression of concrete and exposed to whole-body vibration beyond the exposure limit of ISO 2631 with frequencies above 40 Hz (Rumjancev 1966). This complex was designated as “vibration disease”. Although rejected by many specialists, the same term has sometimes been used to describe a vague clinical picture caused by long-term exposure to low-frequency whole-body vibration which, allegedly, is manifested initially as peripheral and cerebral vegeto-vascular disorders with a non-specific functional character. Based on the available data it can be concluded that different physiological systems react independently of one another and that there are no symptoms which might serve as an indicator of pathology induced by whole-body vibration.
Nervous system, vestibular organ and hearing. Intense whole-body vibration at frequencies higher than 40 Hz can cause damage and disturbances of the central nervous system. Conflicting data have been reported on effects of whole-body vibration at frequencies below 20 Hz. In some studies only, an increase of non-specific complaints such as headache and increased irritability has been found. Disturbances of the electroencephalogram (EEG) after long-term exposure to whole-body vibration have been claimed by one author and denied by others. Some published results are consistent with a decreased vestibular excitability and a higher incidence of other vestibular disturbances, including dizziness. However, it remains doubtful whether there are causal links between whole-body vibration and changes in the central nervous system or vestibular system because paradoxical intensity-effect relationships were detected.
In some studies, an additional increase of the permanent threshold shifts (PTS) of hearing has been observed after a combined long-term exposure to whole-body vibration and noise. Schmidt (1987) studied drivers and technicians in agriculture and compared the permanent threshold shifts after 3 and 25 years on the job. He concluded that whole-body vibration can induce an additional significant threshold shift at 3, 4, 6 and 8 kHz, if the weighted acceleration according to International Standard 2631 (ISO 1985) exceeds 1.2 m/s2 r.m.s. with a simultaneous exposure to noise at an equivalent level of more than 80 decibels (dBA).
Circulatory and digestive systems. Four main groups of circulatory disturbances have been detected with a higher incidence among workers exposed to whole-body vibration:
- peripheral disorders, such as the Raynaud-syndrome, near to the site of application of whole-body vibration (i.e., the feet of standing workers or, with a low degree only, the hands of drivers)
- varicose veins of the legs, haemorrhoids and varicocele
- ischaemic heart disease and hypertension
- neurovascular changes.
The morbidity of these circulatory disturbances did not always correlate with the magnitude or duration of vibration exposure. Although a high prevalence of various disorders of the digestive system has often been observed, almost all authors agree that whole-body vibration is but one cause and possibly not the most important.
Female reproductive organs, pregnancy and male urogenital system. Increased risks of abortions, menstrual disturbances and anomalies of positions (e.g., uterine descent) have been assumed to be associated with long-term exposure to whole-body vibration (see Seidel and Heide 1986). A safe exposure limit in order to avoid a higher risk for these health risks cannot be derived from the literature. The individual susceptibility and its temporal changes probably co-determine these biological effects. In the available literature, a harmful direct effect of whole-body vibration on the human foetus has not been reported, although some animal studies suggest that whole-body vibration can affect the foetus. The unknown threshold value for adverse effects on pregnancy suggests a limitation on an occupational exposure to the lowest reasonable extent.
Divergent results have been published for the occurrence of diseases of the male urogenital system. In some studies, a higher incidence of prostatitis was observed. Other studies could not confirm these findings.
Standards
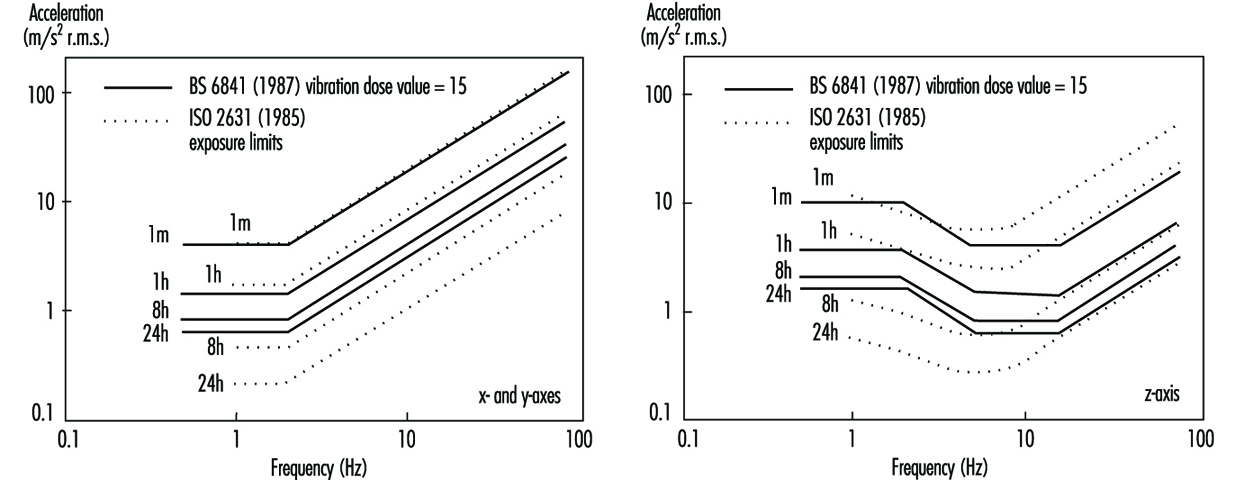
No precise limit can be offered to prevent disorders caused by whole-body vibration, but standards define useful methods of quantifying vibration severity. International Standard 2631 (ISO 1974, 1985) defined exposure limits (see figure 1) which were “set at approximately half the level considered to be the threshold of pain (or limit of voluntary tolerance) for healthy human subjects ”. Also shown in figure 1 is a vibration dose value action level for vertical vibration derived from British Standard 6841 (BSI 1987b); this standard is, in part, similar to a draft revision of the International Standard.
Figure 1. Frequency dependencies for human response to whole-body vibration
The vibration dose value can be considered to be the magnitude of a one-second duration of vibration which will be equally severe to the measured vibration. The vibration dose value uses a fourth-power time dependency to accumulate vibration severity over the exposure period from the shortest possible shock to a full day of vibration (e.g., BSI 6841):
Vibration dose value = 
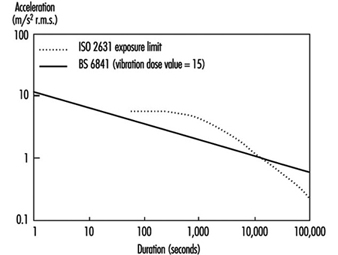
The vibration dose value procedure can be used to evaluate the severity of both vibration and repetitive shocks. This fourth-power time dependency is simpler to use than the time dependency in ISO 2631 (see figure 2).
Figure 2. Time dependencies for human response to a whole-body vibration
British Standard 6841 offers the following guidance.
High vibration dose values will cause severe discomfort, pain and injury. Vibration dose values also indicate, in a general way, the severity of the vibration exposures which caused them. However there is currently no consensus of opinion on the precise relation between vibration dose values and the risk of injury. It is known that vibration magnitudes and durations which produce vibration dose values in the region of 15 m/s1.75 will usually cause severe discomfort. It is reasonable to assume that increased exposure to vibration will be accompanied by increased risk of injury (BSI 1987b).
At high vibration dose values, prior consideration of the fitness of the exposed persons and the design of adequate safety precautions may be required. The need for regular checks on the health of routinely exposed persons may also be considered.
The vibration dose value provides a measure by which highly variable and complex exposures can be compared. Organizations may specify limits or action levels using the vibration dose value. For example, in some countries, a vibration dose value of 15 m/s1.75 has been used as a tentative action level, but it may be appropriate to limit vibration or repeated shock exposures to higher or lower values depending on the situation. With current understanding, an action level merely serves to indicate the approximate values that might be excessive. Figure 2 illustrates the root-mean-square accelerations corresponding to a vibration dose value of 15 m/s1.75 for exposures between one second and 24 hours. Any exposure to continuous vibration, intermittent vibration, or repeated shock may be compared with the action level by calculating the vibration dose value. It would be unwise to exceed an appropriate action level (or the exposure limit in ISO 2631) without consideration of the possible health effects of an exposure to vibration or shock.
The Machinery Safety Directive of the European Economic Community states that machinery must be designed and constructed so that hazards resulting from vibration produced by the machinery are reduced to the lowest practicable level, taking into account technical progress and the availability of means of reducing vibration. The Machinery Safety Directive (Council of the European Communities 1989) encourages the reduction of vibration by means additional to reduction at source (e.g., good seating).
Measurement and Evaluation of Exposure
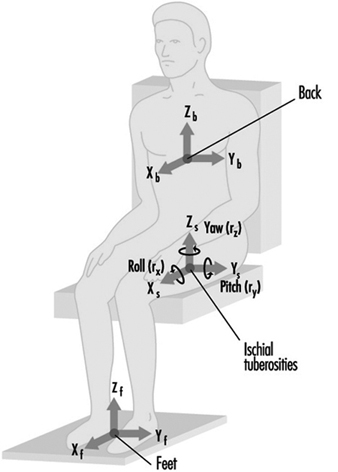
Whole-body vibration should be measured at the interfaces between the body and the source of vibration. For seated persons this involves the placement of accelerometers on the seat surface beneath the ischial tuberosities of subjects. Vibration is also sometimes measured at the seat back (between the backrest and the back) and also at the feet and hands (see figure 3).
Figure 3. Axes for measuring vibration exposures of seated persons
Epidemiological data alone are not sufficient to define how to evaluate whole-body vibration so as to predict the relative risks to health from the different types of vibration exposure. A consideration of epidemiological data in combination with an understanding of biodynamic responses and subjective responses is used to provide current guidance. The manner in which the health effects of oscillatory motions depend upon the frequency, direction and duration of motion is currently assumed to be the same as, or similar to, that for vibration discomfort. However, it is assumed that the total exposure, rather than the average exposure, is important, and so a dose measure is appropriate.
In addition to evaluating the measured vibration according to current standards, it is advisable to report the frequency spectra, magnitudes in different axes and other characteristics of the exposure, including the daily and lifetime exposure durations. The presence of other adverse environmental factors, especially sitting posture, should also be considered.
Prevention
Wherever possible, reduction of vibration at the source is to be preferred. This may involve reducing the undulations of the terrain or reducing the speed of travel of vehicles. Other methods of reducing the transmission of vibration to operators require an understanding of the characteristics of the vibration environment and the route for the transmission of vibration to the body. For example, the magnitude of vibration often varies with location: lower magnitudes will be experienced in some areas. Table 2 lists some preventive measures that may be considered.
Table 2. Summary of preventive measures to consider when persons are exposed to whole-body vibration
|
Group |
Action |
|
Management |
Seek technical advice |
|
|
Seek medical advice |
|
|
Warn exposed persons |
|
|
Train exposed persons |
|
|
Review exposure times |
|
|
Have policy on removal from exposure |
|
Machine manufacturers |
Measure vibration |
|
|
Design to minimize whole-body vibration |
|
|
Optimize suspension design |
|
|
Optimize seating dynamics |
|
|
Use ergonomic design to provide good posture etc. |
|
|
Provide guidance on machine maintenance |
|
|
Provide guidance on seat maintenance |
|
|
Provide warning of dangerous vibration |
|
Technical-at workplace |
Measure vibration exposure |
|
|
Provide appropriate machines |
|
|
Select seats with good attenuation |
|
|
Maintain machines |
|
|
Inform management |
|
Medical |
Pre-employment screening |
|
|
Routine medical checks |
|
|
Record all signs and reported symptoms |
|
|
Warn workers with apparent predisposition |
|
|
Advise on consequences of exposure |
|
|
Inform management |
|
Exposed persons |
Use machine properly |
|
|
Avoid unnecessary vibration exposure |
|
|
Check seat is properly adjusted |
|
|
Adopt good sitting posture |
|
|
Check condition of machine |
|
|
Inform supervisor of vibration problems |
|
|
Seek medical advice if symptoms appear |
|
|
Inform employer of relevant disorders |
Source: Adapted from Griffin 1990.
Seats can be designed to attenuate vibration. Most seats exhibit a resonance at low frequencies, which results in higher magnitudes of vertical vibration occurring on the seat than on the floor! At high frequencies there is usually attenuation of vibration. In use, the resonance frequencies of common seats are in the region of 4 Hz. The amplification at resonance is partially determined by the damping in the seat. An increase in the damping of the seat cushioning tends to reduce the amplification at resonance but increase the transmissibility at high frequencies. There are large variations in transmissibility between seats, and these result in significant differences in the vibration experienced by people.
A simple numerical indication of the isolation efficiency of a seat for a specific application is provided by the seat effective amplitude transmissibility (SEAT) (see Griffin 1990). A SEAT value greater than 100% indicates that, overall, the vibration on the seat is worse than the vibration on the floor. Values below 100% indicate that the seat has provided some useful attenuation. Seats should be designed to have the lowest SEAT value compatible with other constraints.
A separate suspension mechanism is provided beneath the seat pan in suspension seats. These seats, used in some off-road vehicles, trucks and coaches, have low resonance frequencies (around 2 Hz) and so can attenuate vibration at frequencies above about 3 Hz. The transmissibilities of these seats are usually determined by the seat manufacturer, but their isolation efficiencies vary with operating conditions.