The problem of air pollution has grown steadily since the Industrial Revolution began 300 years ago. Four major factors have exacerbated air pollution: growing industrialization; increasing traffic; rapid economic development; and higher levels of energy consumption. The available information shows that the WHO guidelines for the major air pollutants are regularly exceeded in many major urban centres. Although progress has been made in controlling air pollution problems in many industrialized countries over the last two decades, air quality—particularly in the larger cities in the developing world—is worsening. Of major concern are the adverse health effects of ambient air pollutants in many urban areas, where levels are sufficiently high to contribute to increased mortality and morbidity, deficits in pulmonary function and cardiovascular and neurobehavioural effects (Romieu, Weizenfeld and Finkelman 1990; WHO/UNEP 1992). Indoor air pollution due to domestic combustion products is also a major issue in developing countries (WHO 1992b), but it is not part of this review, which considers only the sources, dispersion and health effects of outdoor air pollution, and includes a case study of the situation in Mexico.
Source of Air Pollutants
The most common air pollutants in urban environments include sulphur dioxide (SO2), suspended particulate matter (SPM), the nitrogen oxides (NO and NO2, collectively termed NOX), ozone (O3), carbon monoxide (CO) and lead (Pb). Combustion of fossil fuels in stationary sources leads to the production of SO2, NOX and particulates, including sulphate and nitrate aerosols formed in the atmosphere following gas to particle conversion. Petrol-fuelled motor vehicles are the principal sources of NOX, CO and Pb, whereas diesel-fuelled engines emit significant quantities of particulates, SO2 and NOX. Ozone, a photochemical oxidant and the main constituent of photochemical smog, is not emitted directly from combustion sources but is formed in the lower atmosphere from NOX and volatile organic compounds (VOCs) in the presence of sunlight (UNEP 1991b). Table 1 presents the major sources of outdoor air pollutants.
Table 1. Major sources of outdoor air pollutants
Pollutants Sources
Sulphur oxides Coal and oil combustion, smelters
Suspended particulate matter Combustion products (fuel, biomass), tobacco smoke
Nitrogen oxides Fuel and gas combustion
Carbon monoxide Incomplete petrol and gas combustion
Ozone Photochemical reaction
Lead Petrol combustion, coal combustion, producing batteries, cables, solder, paint
Organic substances Petrochemical solvents, vaporization of unburnt fuels
Source: Adapted from UNEP 1991b.
Dispersion and Transport of Air Pollutants
The two major influences on the dispersion and transport of air pollutant emissions are the meteorology (including microclimate effects such as “heat islands”) and the topography in relation to the population distribution. Many cities are surrounded by hills which may act as a downwind barrier, trapping pollution. Thermal inversions contribute to a particulate problem in temperate and cold climates. Under normal dispersion conditions, hot pollutant gases rise as they come into contact with colder air masses with increasing altitude. However, under certain circumstances the temperature may increase with altitude, and an inversion layer forms, trapping pollutants close to the emission source and delaying their diffusion. Long-range transport of air pollution from large urban areas may have national and regional impacts. Oxides of nitrogen and sulphur may contribute to acid deposition at great distances from the emission source. Ozone concentrations are often elevated downwind of urban areas due to the time lag involved in photochemical processes (UNEP 1991b).
Health Effects of Air Pollutants
Pollutants and their derivatives can cause adverse effects by interacting with and impairing molecules crucial to the biochemical or physiological processes of the human body. Three factors influence the risk of toxic injury related to these substances: their chemical and physical properties, the dose of the material that reaches the critical tissue sites and the responsiveness of these sites to the substance. The adverse health effects of air pollutants may also vary across population groups; in particular, the young and the elderly may be especially susceptible to deleterious effects. Persons with asthma or other pre-existing respiratory or cardiac diseases may experience aggravated symptoms upon exposure (WHO 1987).
Sulphur Dioxide and Particulate Matter
During the first half of the twentieth century, episodes of marked air stagnation resulted in excess mortality in areas where fossil-fuel combustion produced very high levels of SO2 and SMP. Studies of long-term health effects have also related the annual mean concentrations of SO2 and SMP to mortality and morbidity. Recent epidemiological studies have suggested an adverse effect of inhalable particulate levels (PM10) at relatively low concentrations (not exceeding the standard guidelines) and have shown a dose-response relationship between exposure to PM10 and respiratory mortality and morbidity (Dockery and Pope 1994; Pope, Bates and Razienne 1995; Bascom et al. 1996) as shown in table 2.
Table 2. Summary of short-term exposure-response relationship of PM10 with different health effects indicators
|
Health effect |
% changes for each 10 μg/m3 |
|
|
Mean |
Range |
|
|
Mortality |
||
|
Total |
1.0 |
0.5-1.5 |
|
Cardiovascular |
1.4 |
0.8-1.8 |
|
Respiratory |
3.4 |
1.5-3.7 |
|
Morbidity |
||
|
Hospital admission for respiratory condition |
1.1 |
0.8-3.4 |
|
Emergency visits for respiratory conditions |
1.0 |
0.5-4 |
|
Symptom exacerbations among asthmatics |
3.0 |
1.1-11.5 |
|
Changes in peak expiratory flow |
0.08 |
0.04-0.25 |
Nitrogen Oxides
Some epidemiological studies have reported adverse health effects of NO2 including increased incidence and severity of respiratory infections and increase in respiratory symptoms, especially with long-term exposure. Worsening of the clinical status of persons with asthma, chronic obstructive pulmonary disease and other chronic respiratory conditions has also been described. However, in other studies, investigators have not observed adverse effects of NO2 on respiratory functions (WHO/ECOTOX 1992; Bascom et al. 1996).
Photochemical Oxidants and Ozone
The health effects of photochemical oxidants exposure cannot be attributed only to oxidants, because photochemical smog typically consists of O3, NO2, acid and sulphate and other reactive agents. These pollutants may have additive or synergistic effects on human health, but O3 appears to be the most biologically active. Health effects of ozone exposure include decreased pulmonary function (including increased airway resistance, reduced air flow, decreased lung volume) due to airway constriction, respiratory symptoms (cough, wheezing, shortness of breath, chest pains), eye, nose and throat irritation, and disruption of activities (such as athletic performance) due to less oxygen availability (WHO/ECOTOX 1992). Table 3 summarizes the major acute health effects of ozone (WHO 1990a, 1995). Epidemiological studies have suggested a dose-response relationship between exposure to increasing ozone levels and the severity of respiratory symptoms and the decrement in respiratory functions (Bascom et al. 1996).
Table 3. Health outcomes associated with changes in peak daily ambient ozone concentration in epidemiological studies
|
Health outcome |
Changes in |
Changes in |
|
Symptom exacerbations among healthy children |
||
|
25% increase |
200 |
100 |
|
50% increase |
400 |
200 |
|
100% increase |
800 |
300 |
|
Hospital admissions for respiratory |
||
|
5% |
30 |
25 |
|
10% |
60 |
50 |
|
20% |
120 |
100 |
a Given the high degree of correlation between the 1-h and 8-h O3 concentrations in field studies, an improvement in health risk associated with decreasing 1- or 8-h O3 levels should be almost identical.
Source: WHO 1995.
Carbon Monoxide
The main effect of CO is to decrease oxygen transport to the tissues through the formation of carboxyhaemoglobin (COHb). With increasing levels of COHb in blood, the following health effects can be observed: cardiovascular effects in subjects with previous angina pectoris (3 to 5%); impairment of vigilance tasks (>5%); headache and dizziness (≥10%); fibrinolysis and death (WHO 1987).
Lead
Lead exposure principally affects haem biosynthesis, but also may act on the nervous system and other systems such as the cardiovascular system (blood pressure). Infants and young children less than five years old are particularly sensitive to lead exposure because of its effect on neurological development at blood lead levels close to 10 μg/dl (CDC 1991).
Several epidemiological studies have investigated the effect of air pollution, especially ozone exposure, on the health of the population of Mexico City. Ecological studies have shown an increase in mortality with respect to exposure to fine particulates (Borja-Arburto et al. 1995) and an increase in emergency visits for asthma among children (Romieu et al. 1994). Studies of the adverse effect of ozone exposure conducted among healthy children have shown an increase in school absenteeism due to respiratory illnesses (Romieu et al. 1992), and a decrease in lung function after both acute and subacute exposure (Castillejos et al. 1992, 1995). Studies conducted among asthmatic children have shown an increase in respiratory symptoms and a decrease in peak expiratory flow rate after exposure to ozone (Romieu et al. 1994) and to fine particulate levels (Romieu et al. in press). Although, it seems clear that acute exposure to ozone and particulates is associated with adverse health effects in the population of Mexico City, there is a need to evaluate the chronic effect of such exposure, in particular given the high levels of photo-oxidants observed in Mexico City and the ineffectiveness of control measures.
Case study: Air pollution in Mexico City
The metropolitan area of Mexico City (MAMC) is situated in the Mexican Basin at a mean altitude of 2,240 metres. The basin covers 2,500 square kilometres and is surrounded by mountains, two of which are over 5,000 metres high. The total population was estimated at 17 million in 1990. Due to the particular geographic characteristics and the light winds, ventilation is poor with a high frequency of thermic inversions, especially during the winter. More than 30,000 industries in the MAMC and the three million motor vehicles circulating daily are responsible for 44% of the total energy consumption. Since 1986, air pollution has been monitored, including SO2, NOx, CO, O3, particulate matter and non-methane hydrocarbon (HCNM). The main air pollutant problems are related to ozone, especially in the southwest part of the city (Romieu et al. 1991). In 1992 the Mexican norm for ozone (110 ppb one-hour maximum) was exceeded in the southwest part more than 1,000 hours and reached a maximum of 400 ppb. Particulate levels are high in the northeast section of the city, close to the industrial park. In 1992, the annual average of inhalable particulate (PM10) was 140 μg/m3. Since 1990, important control measures have been taken by the government to decrease air pollution, including a programme that prohibits use of cars one day a week depending on their terminating licence plate number, the closure of one of the most polluting refineries located in Mexico City, and the introduction of unleaded fuel. These measures have led to a decrease in various air pollutants, mainly SO2, particulate matter, NO2, CO and lead. However the ozone level remains a major problem (see figure 1, figure 2 and figure 3).
Figure 1. Ozone levels in two zones of Mexico City. One-hour daily maximum by month, 1994

Figure 2. Particulates (PM10) in two zones of Mexico City, 1988-1993
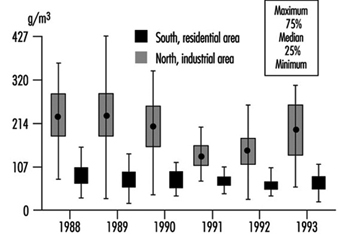
Figure 3. Air lead levels in two zones of Mexico City, 1988-1994
