This article examines the role of human factors in the accident causation process and reviews the various preventive measures (and their effectiveness) by which human error may be controlled, and their application to the accident causation model. Human error is an important contributing cause in at least 90 of all industrial accidents. While purely technical errors and uncontrollable physical circumstances may also contribute to accident causation, human error is the paramount source of failure. The increased sophistication and reliability of machinery means that the proportion of causes of accidents attributed to human error increases as the absolute number of accidents decreases. Human error is also the cause of many of those incidents that, although not resulting in injury or death, nevertheless result in considerable economic damage to a company. As such, it represents a major target for prevention, and it will become increasingly important. For effective safety management systems and risk identification programmes it is important to be able to identify the human component effectively through the use of general failure type analysis.
The Nature of Human Error
Human error can be viewed as the failure to reach a goal in the way that was planned, either from a local or wider perspective, due to unintentional or intentional behaviour. Those planned actions may fail to achieve the desired outcomes for the following four reasons:
1. Unintentional behaviour:
- The actions did not go as planned (slips).
- The action was not executed (lapses).
2. Intentional behaviour:
- The plan itself was inadequate (mistakes).
- There were deviations from the original plan (violations).
Deviations can be divided in three classes: skill-, rule- and knowledge-based errors.
- At the skill-based level, behaviour is guided by pre-programmed action schemes. The tasks are routine and continuous, and feedback is usually lacking.
- At the rule-based level, behaviour is guided by general rules. They are simple and can be applied many times in specific situations. The tasks consist of relatively frequent action sequences that start after a choice is made among rules or procedures. The user has a choice: the rules are not automatically activated, but are actively chosen.
- Knowledge-based behaviour is shown in completely new situations where no rules are available and where creative and analytical thinking is required.
In some situations, the term human limitation would be more appropriate than human error. There also are limits to the ability to foresee the future behaviour of complex systems (Gleick 1987; Casti 1990).
Reason and Embrey’s model, the Generic Error Modelling System (GEMS) (Reason 1990), takes into account the error-correcting mechanisms on the skill-, rule- and knowledge-based levels. A basic assumption of GEMS is that day-to-day behaviour implies routine behaviour. Routine behaviour is checked regularly, but between these feedback loops, behaviour is completely automatic. Since the behaviour is skill-based, the errors are slips. When the feedback shows a deviation from the desired goal, rule-based correction is applied. The problem is diagnosed on the basis of available symptoms, and a correction rule is automatically applied when the situation is diagnosed. When the wrong rule is applied there is a mistake.
When the situation is completely unknown, knowledge-based rules are applied. The symptoms are examined in the light of knowledge about the system and its components. This analysis can lead to a possible solution the implementation of which constitutes a case of knowledge-based behaviour. (It is also possible that the problem cannot be solved in a given way and that further knowledge-based rules have to be applied.) All errors on this level are mistakes. Violations are committed when a certain rule is applied that is known to be inappropriate: the thinking of the worker may be that application of an alternative rule will be less time-consuming or is possibly more suitable for the present, probably exceptional, situation. The more malevolent class of violations involves sabotage, a subject that is not within the scope of this article. When organizations are attempting to eliminate human error, they should take into account whether the errors are on the skill-, rule- or knowledge-based level, as each level requires its own techniques (Groeneweg 1996).
Influencing Human Behaviour: An Overview
A comment often made with regard to a particular accident is, “Maybe the person did not realize it at the time, but if he or she had not acted in a certain way, the accident would not have happened.” Much of accident prevention is aimed at influencing the crucial bit of human behaviour alluded to in this remark. In many safety management systems, the solutions and policies suggested are aimed at directly influencing human behaviour. However, it is very uncommon that organizations assess how effective such methods really are. Psychologists have devoted much thought to how human behaviour can best be influenced. In this respect, the following six ways of exercising control over human error will be set forth, and an evaluation will be performed of the relative effectiveness of these methods in controlling human behaviour on a long-term basis (Wagenaar 1992). (See table 1.)
Table 1. Six ways to induce safe behaviour and assessment of their cost-effectiveness
|
No. |
Way of influencing |
Cost |
Long-term effect |
Assessment |
|
1 |
Don’t induce safe behaviour, |
High |
Low |
Poor |
|
2 |
Tell those involved what to do. |
Low |
Low |
Medium |
|
3 |
Reward and punish. |
Medium |
Medium |
Medium |
|
4 |
Increase motivation and awareness. |
Medium |
Low |
Poor |
|
5 |
Select trained personnel. |
High |
Medium |
Medium |
|
6 |
Change the environment. |
High |
High |
Good |
Do not attempt to induce safe behaviour, but make the system “foolproof”
The first option is to do nothing to influence the behaviour of people but to design the workplace in such a way that whatever the employee does, it will not result in any kind of undesirable outcome. It must be acknowledged that, thanks to the influence of robotics and ergonomics, designers have considerably improved on the user-friendliness of workplace equipment. However, it is almost impossible to anticipate all the different kinds of behaviour that people may evince. Besides, workers often regard so-called foolproof designs as a challenge to “beat the system”. Finally, as designers are human themselves, even very carefully foolproof-designed equipment can have flaws (e.g., Petroski 1992). The additional benefit of this approach relative to existing hazard levels is marginal, and in any event initial design and installation costs may increase exponentially.
Tell those involved what to do
Another option is to instruct all workers about every single activity in order to bring their behaviour fully under the control of management. This will require an extensive and not very practical task inventory and instruction control system. As all behaviour is de-automated it will to a large extent eliminate slips and lapses until the instructions become part of the routine and the effect fades away.
It does not help very much to tell people that what they do is dangerous - most people know that very well - because they will make their own choices concerning risk regardless of attempts to persuade them otherwise. Their motivation to do so will be to make their work easier, to save time, to challenge authority and perhaps to enhance their own career prospects or claim some financial reward. Instructing people is relatively cheap, and most organizations have instruction sessions before the start of a job. But beyond such an instruction system the effectiveness of this approach is assessed to be low.
Reward and punish
Although reward and punishment schedules are powerful and very popular means for controlling human behaviour, they are not without problems. Reward works best only if the recipient perceives the reward to be of value at the time of receipt. Punishing behaviour that is beyond an employee’s control (a slip) will not be effective. For example, it is more cost-effective to improve traffic safety by changing the conditions underlying traffic behaviour than by public campaigns or punishment and reward programmes. Even an increase in the chances of being “caught” will not necessarily change a person’s behaviour, as the opportunities for violating a rule are still there, as is the challenge of successful violation. If the situations in which people work invite this kind of violation, people will automatically choose the undesired behaviour no matter how they are punished or rewarded. The effectiveness of this approach is rated as of medium quality, as it usually is of short-term effectiveness.
Increase motivation and awareness
Sometimes it is believed that people cause accidents because they lack motivation or are unaware of danger. This assumption is false, as studies have shown (e.g., Wagenaar and Groeneweg 1987). Furthermore, even if workers are capable of judging danger accurately, they do not necessarily act accordingly (Kruysse 1993). Accidents happen even to people with the best motivation and the highest degree of safety awareness. There are effective methods for improving motivation and awareness which are discussed below under “Change the environment”. This option is a delicate one: in contrast with the difficulty to further motivate people it is almost too easy to de-motivate employees to the extent that even sabotage is considered.
The effects of motivation enhancement programmes are positive only when coupled with behaviour modification techniques such as employee involvement.
Select trained personnel
The first reaction to an accident is often that those involved must have been incompetent. With hindsight, the accident scenarios appear straightforward and easily preventable to someone sufficiently intelligent and properly trained, but this appearance is a deceptive one: in actual fact the employees involved could not possibly have foreseen the accident. Therefore, better training and selection will not have the desirable effect. A base level of training is however a prerequisite for safe operations. The tendency in some industries to replace experienced personnel with inexperienced and inadequately trained people is to be discouraged, as increasingly complex situations call for rule- and knowledge-based thinking that requires a level of experience that such lower-cost personnel often do not possess.
A negative side-effect of instructing people very well and selecting only the highest-classified people is that behaviour can become automatic and slips occur. Selection is expensive, while the effect is not more than medium.
Change the environment
Most behaviour occurs as a reaction to factors in the working environment: work schedules, plans, and management expectations and demands. A change in the environment results in different behaviour. Before the working environment can be effectively changed, several problems must be solved. First, the environmental factors that cause the unwanted behaviour must be identified. Second, these factors must be controlled. Third, management must allow discussion about their role in creating the adverse working environment.
It is more practical to influence behaviour through creating the proper working environment. The problems that should be solved before this solution can be put into practice are (1) that it must be known which environmental factors cause the unwanted behaviour, (2) that these factors must be controlled and (3) that previous management decisions must be considered (Wagenaar 1992; Groeneweg 1996). All these conditions can indeed be met, as will be argued in the remainder of this article. The effectiveness of behaviour modification can be high, even though a change of environment may be quite costly.
The Accident Causation Model
In order to get more insight into the controllable parts of the accident causation process, an understanding of the possible feedback loops in a safety information system is necessary. In figure 1, the complete structure of a safety information system is presented that can form the basis of managerial control of human error. It is an adapted version of the system presented by Reason et al. (1989).
Figure 1. A safety information system
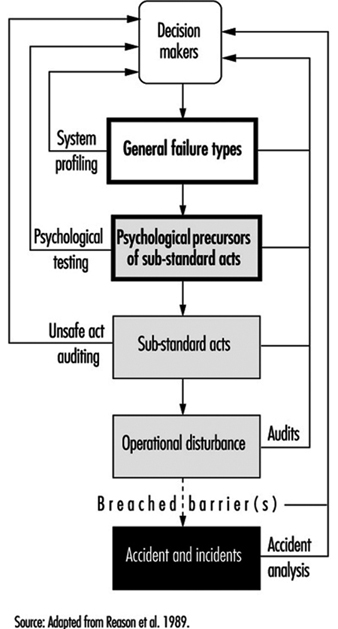
Accident investigation
When accidents are investigated, substantial reports are produced and decision-makers receive information about the human error component of the accident. Fortunately, this is becoming more and more obsolete in many companies. It is more effective to analyse the “operational disturbances” that precede the accidents and incidents. If an accident is described as an operational disturbance followed by its consequences, then sliding from the road is an operational disturbance and getting killed because the driver did not wear a safety belt is an accident. Barriers may have been placed between the operational disturbance and the accident, but they failed or were breached or circumvented.
Unsafe act auditing
A wrong act committed by an employee is called a “substandard act” and not an “unsafe act” in this article: the notion of “unsafe” seems to limit the applicability of the term to safety, whereas it can also be applied, for example, to environmental problems. Substandard acts are sometimes recorded, but detailed information as to which slips, mistakes and violations were performed and why they were performed is hardly ever fed back to higher management levels.
Investigating the employee’s state of mind
Before a substandard act is committed, the person involved was in a certain state of mind. If these psychological precursors, like being in a state of haste or feeling sad, could be adequately controlled, people would not find themselves in a state of mind in which they would commit a substandard act. Since these states of mind cannot be effectively controlled, such precursors are regarded as “black box” material (figure 1).
General failure types
The GFT (general failure type) box in figure 1 represents the generating mechanisms of an accident - the causes of substandard acts and situations. Because these substandard acts cannot be controlled directly, it is necessary to change the working environment. The working environment is determined by 11 such mechanisms (table 2). (In the Netherlands the abbreviation GFT already exists in a completely different context, and has to do with ecologically sound waste disposal, and to avoid confusion another term is used: basic risk factors (BRFs) (Roggeveen 1994).)
Table 2. General failure types and their definitions
|
General failures |
Definitions |
|
1. Design (DE) |
Failures due to poor design of a whole plant as well as individual |
|
2. Hardware (HW) |
Failures due to poor state or unavailability of equipment and tools |
|
3. Procedures (PR) |
Failures due to poor quality of the operating procedures with |
|
4. Error enforcing |
Failures due to poor quality of the working environment, with |
|
5. Housekeeping (HK) |
Failures due to poor housekeeping |
|
6. Training (TR) |
Failures due to inadequate training or insufficient experience |
|
7. Incompatible goals(IG) |
Failures due to the poor way safety and internal welfare are |
|
8. Communication (CO) |
Failures due to poor quality or absence of lines of communication |
|
9. Organization (OR) |
Failures due to the way the project is managed |
|
10. Maintenance |
Failures due to poor quality of the maintenance procedures |
|
11. Defences (DF) |
Failures due to the poor quality of the protection against hazardous |
The GFT box is preceded by a “decision-maker’s” box, as these people determine to a large extent how well a GFT is managed. It is management’s task to control the working environment by managing the 11 GFTs, thereby indirectly controlling the occurrence of human error.
All these GFTs can contribute to accidents in subtle ways by allowing undesirable combinations of situations and actions to come together, by increasing the chance that certain persons will commit substandard acts and by failing to provide the means to interrupt accident sequences already in progress.
There are two GFTs that require some further explanation: maintenance management and defences.
Maintenance management (MM)
Since maintenance management is a combination of factors that can be found in other GFTs, it is not, strictly speaking, a separate GFT: this type of management is not fundamentally different from other management functions. It may be treated as a separate issue because maintenance plays an important role in so many accident scenarios and because most organizations have a separate maintenance function.
Defences (DF)
The category of defences is also not a true GFT, as it is not related to the accident causation process itself. This GFT is related to what happens after an operational disturbance. It does not generate either psychological states of mind or substandard acts by itself. It is a reaction that follows a failure due to the action of one or more GFTs. While it is indeed true that a safety management system should focus on the controllable parts of the accident causation chain before and not after the unwanted incident, nevertheless the notion of defences can be used to describe the perceived effectiveness of safety barriers after a disturbance has occurred and to show how they failed to prevent the actual accident.
Managers need a structure that will enable them to relate identified problems to preventive actions. Measures taken at the levels of safety barriers or substandard acts are still necessary, although these measures can never be completely successful. To trust “last line” barriers is to trust factors that are to a large extent out of management control. Management should not attempt to manage such uncontrollable external devices, but instead must try to make their organizations inherently safer at every level.
Measuring the Level of Control over Human Error
Ascertaining the presence of the GFTs in an organization will enable accident investigators to identify the weak and strong points in the organization. Given such knowledge, one can analyse accidents and eliminate or mitigate their causes and identify the structural weaknesses within a company and fix them before they in fact contribute to an accident.
Accident investigation
The task of an accident analyst is to identify contributing factors and to categorize them. The number of times a contributing factor is identified and categorized in terms of a GFT indicates the extent to which this GFT is present. This is often done by means of a checklist or computer analysis program.
It is possible and desirable to combine profiles from different but similar types of accidents. Conclusions based upon an accumulation of accident investigations in a relatively short time are far more reliable than those drawn from a study in which the accident profile is based upon a single event. An example of such a combined profile is presented in figure 2, which shows data relating to four occurrences of one type of accident.
Figure 2. Profile of an accident type
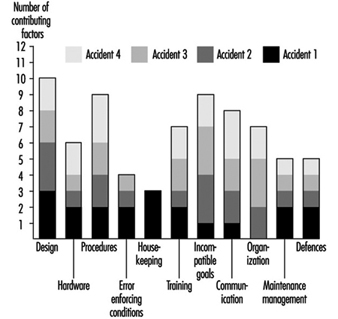
Some of the GFTs - design, procedures and incompatible goals - score consistently high in all four particular accidents. This means that in each accident, factors have been identified that were related to these GFTs. With respect to the profile of accident 1, design is a problem. Housekeeping, although a major problem area in accident 1, is only a minor problem if more than the first accident is analysed. It is suggested that about ten similar types of accidents be investigated and combined in a profile before far-reaching and possibly expensive corrective measures are taken. This way, the identification of the contributing factors and subsequent categorization of these factors can be done in a very reliable way (Van der Schrier, Groeneweg and van Amerongen 1994).
Identifying the GFTs within an organization pro-actively
It is possible to quantify the presence of GFTs pro-actively, regardless of the occurrence of accidents or incidents. This is done by looking for indicators of the presence of that GFT. The indicator used for this purpose is the answer to a straightforward yes or no question. If answered in the undesired way, it is an indication that something is not functioning properly. An example of an indicator question is: “In the past three months, did you go to a meeting that turned out to be cancelled?” If the employee answers the question in the affirmative, it does not necessarily signify danger, but it is indicative of a deficiency in one of the GFTs—communication. However, if enough questions that test for a given GFT are answered in a way that indicates an undesirable trend, it is a signal to management that it does not have sufficient control of that GFT.
To construct a system safety profile (SSP), 20 questions for each of the 11 GFTs have to be answered. Each GFT is assigned a score ranging from 0 (low level of control) to 100 (high level of control). The score is calculated relative to the industry average in a certain geographical area. An example of this scoring procedure is presented in the box.
The indicators are pseudo-randomly drawn from a database with a few hundred questions. No two subsequent checklists have questions in common, and questions are drawn in such a way that each aspect of the GFT is covered. Failing hardware could, for instance, be the result of either absent equipment or defective equipment. Both aspects should be covered in the checklist. The answering distributions of all questions are known, and checklists are balanced for equal difficulty.
It is possible to compare scores obtained with different checklists, as well as those obtained for different organizations or departments or the same units over a period of time. Extensive validation tests have been done to ensure that all questions in the database have validity and that they are all indicative of the GFT to be measured. Higher scores indicate a higher level of control - that is, more questions have been answered in the “desired” way. A score of 70 indicates that this organization is ranked among the best 30 (i.e., 100 minus 70) of comparable organizations in this kind of industry. Although a score of 100 does not necessarily mean that this organization has total control over a GFT, it does means that with regard to this GFT the organization is the best in the industry.
An example of an SSP is shown in figure 3. The weak areas of Organization 1, as exemplified by the bars in the chart, are procedures, incompatible goals, and error enforcing conditions, as they score below the industry average as shown by the dark grey area. The scores on housekeeping, hardware and defences are very good in Organization 1. On the surface, this well-equipped and tidy organization with all safety devices in place appears to be a safe place to work. Organization 2 scores exactly at the industry average. There are no major deficiencies, and although the scores on hardware, housekeeping and defences are lower, this company manages (on the average) the human error component in accidents better than Organization 1. According to the accident causation model, Organization 2 is safer than Organization 1, although this would not necessarily be apparent in comparing the organizations in “traditional” audits.
Figure 3. Example of a system safety profile
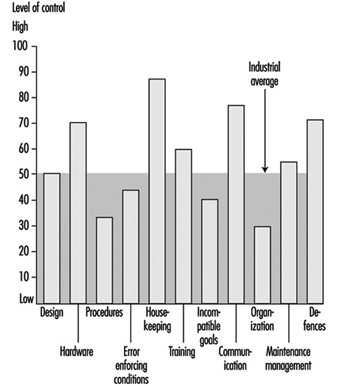
If these organizations had to decide where to allocate their limited resources, the four areas with below average GFTs would have priority. However, one cannot conclude that, since the other GFT scores are so favourable, resources may be safely withdrawn from their upkeep, since these resources are what have most probably kept them at so high a level in the first place.
Conclusions
This article has touched upon the subject of human error and accident prevention. The overview of the literature regarding control of the human error component in accidents yielded a set of six ways by which one can try to influence behaviour. Only one, restructuring the environment or modifying behaviour in order to reduce the number of situations in which people are liable to commit an error, has a reasonably favourable effect in a well-developed industrial organization where many other attempts have already been made. It will take courage on the part of management to recognize that these adverse situations exist and to mobilize the resources that are needed to effect a change in the company. The other five options do not represent helpful alternatives, as they will have little or no effect and will be quite costly.
“Controlling the controllable” is the key principle supporting the approach presented in this article. The GFTs must be discovered, attacked and eliminated. The 11 GFTs are mechanisms that have proven to be part of the accident causation process. Ten of them are aimed at preventing operational disturbances and one (defences) is aimed at the prevention of the operational disturbance’s turning into an accident. Eliminating the impact of the GFTs has a direct bearing upon the abatement of contributing causes of accidents. The questions in the checklists are aimed at measuring the “health state” of a given GFT, from both a general and a safety point of view. Safety is viewed as an integrated part of normal operations: doing the job the way it should be done. This view is in accordance with the recent “quality oriented” management approaches. The availability of policies, procedures and management tools is not the chief concern of safety management: the question is rather whether these methods are actually used, understood and adhered to.
The approach described in this article concentrates upon systemic factors and the way in which management decisions can be translated into unsafe conditions at the workplace, in contrast to the conventional belief that attention should be directed towards the individual workers who perform unsafe acts, their attitudes, motivations and perceptions of risk.
An indication of the level of control your organization has over the GFT “Communication”
In this box a list of 20 questions is presented. The questions in this list have been answered by employees of more than 250 organizations in Western Europe. These organizations were operating in different fields, ranging from chemical companies to refineries and construction companies. Normally, these questions would be tailor-made for each branch. This list serves as an example only to show how the tool works for one of the GFTs. Only those questions have been selected that have proved to be so “general” that they are applicable in at least 80% of the industries.
In “real life” employees would not only have to answer the questions (anonymously), they would also have to motivate their answers. It is not sufficient to answer “Yes” on, for example, the indicator “Did you have to work in the past 4 weeks with an outdated procedure?” The employee would have to indicate which procedure it was and under which conditions it had to be applied. This motivation serves two goals: it increases the reliability of the answers and it provides management with information it can act upon.
Caution is also necessary when interpreting the percentile score: in a real measurement, each organization would be matched against a representative sample of branch-related organizations for each of the 11 GFTs. The distribution of percentiles is from May 1995, and this distribution does change slightly over time.
How to measure the “level of control”
Answer all 20 indicators with your own situation in mind and beware of the time limits in the questions. Some of the questions might not be applicable for your situation; answer them with “n.a.” It might be impossible for you to answer some questions; answer them with a question mark“?”.
After you have answered all questions, compare your answers with the reference answers. You get a point for each “correctly” answered question.
Add the number of points together. Calculate the percentage of correctly answered questions by dividing the number of points by the number of questions you have answered with either “Yes” or “No”. The “n.a.” and “?” answers are not taken into account. The result is a percentage between 0 and 100.
The measurement can be made more reliable by having more people answering the questions and by averaging their scores over the levels or functions in the organization or comparable departments.
Twenty questions about the GFT “Communication”
Possible answers to the questions: Y = Yes; N = No; n.a. = not applicable; ? = don’t know.
- In the past 4 weeks has the telephone directory provided you with incorrect or insufficient information?
- In the past 2 weeks has your telephone conversation been interrupted due to a malfunctioning of the telephone system?
- Have you received mail in the past week that was not relevant to you?
- Has there been an internal or external audit in the past 9 months of your office paper trail?
- Was more than 20% of the information you received in the past 4 weeks labelled “urgent”?
- Did you have to work in the past 4 weeks with a procedure that was difficult to read (e.g., phrasing or language problems)?
- Have you gone to a meeting in the past 4 weeks that turned out not to be held at all?
- Has there been a day in the past 4 weeks that you had five or more meetings?
- Is there a “suggestion box” in your organization?
- Have you been asked to discuss a matter in the past 3 months that later turned out to be already decided upon?
- Have you sent any information in the past 4 weeks that was never received?
- Have you received information in the past 6 months about changes in policies or procedures more than a month after it had been put into effect?
- Have the minutes of the last three safety meetings been sent to your management?
- Has “office” management stayed at least 4 hours at the location when making the last site visit?
- Did you have to work in the past 4 weeks with procedures with conflicting information?
- Have you received within 3 days feedback on requests for information in the past 4 weeks?
- Do people in your organization speak different languages or dialects (different mother tongue)?
- Was more than 80% of the feedback you received (or gave) from management in the past 6 months of a “negative nature”?
- Are there parts of the location/workplace where it is difficult to understand each other due to extreme noise levels?
- In the past 4 weeks, have tools and/or equipment been delivered that not had been ordered?
Reference answers:
1 = N; 2 = N; 3 = N; 4 = Y; 5 = N; 6 = N; 7 = N; 8 = N; 9 = N; 10 = N; 11 = N; 12 = N; 13 = Y; 14 = N; 15 = N; 16 = Y; 17 = N; 18 = N; 19 = Y; 20 = N.
Scoring GFT “Communication”
Percent score = (a/b) x 100
where a = no. of questions answered correctly
where b = no. of questions answered “Y” or “N”.
|
Your score % |
Percentile |
% |
Equal or better |
|
0-10 |
0-1 |
100 |
99 |
|
11-20 |
2-6 |
98 |
94 |
|
21-30 |
7-14 |
93 |
86 |
|
31-40 |
15-22 |
85 |
78 |
|
41-50 |
23-50 |
79 |
50 |
|
51-60 |
51-69 |
49 |
31 |
|
61-70 |
70-85 |
30 |
15 |
|
71-80 |
86-97 |
14 |
3 |
|
81-90 |
98-99 |
2 |
1 |
|
91-100 |
99-100 |