It is a paradox that the prevention of work-related accidents did not emerge very early as an absolute necessity, since health and safety is fundamental to work itself. In fact it was not until the beginning of the twentieth century that accidents at work ceased to be considered inevitable and their causation became a subject to be investigated and used as a basis for prevention. However, accident investigation long remained cursory and empirical. Historically, accidents were first conceived of as simple phenomena—that is, as resulting from a single (or principal) cause and a small number of subsidiary causes. It is now recognized that accident investigation, which is aimed at identifying the causes of the phenomenon so as to avert its reoccurrence, depends both on the concept underlying the process of investigation and on the complexity of the situation to which it is applied.
Causes of Accidents
It is indeed true that in the most precarious situations, accidents are often the result of a fairly simple sequence of a few causes that can be rapidly traced to basic technical problems that even a summary analysis can reveal (equipment badly designed, working methods undefined, etc.). On the other hand, the more closely that the material elements of work (machines, installations, the arrangement of the workplace, etc.) conform with the requirements of safe work procedures, standards and regulations, the safer the work situation becomes. The result is that an accident can then occur only when a group of exceptional conditions are present simultaneously—conditions that are becoming ever more numerous. In such cases, the injury or damage appears as the final result of a frequently complex network of causes. This complexity is actually evidence of progress in prevention, and requires appropriate methods of investigation. Table 1 lists the principal concepts of the accident phenomenon, their characteristics and implications for prevention.
Table 1. Principal concepts of the accident phenomenon, their characteristics and the implications for prevention
|
Concept or “accident phenomenon” |
Significant elements (objectives, procedures, limits, etc.) |
Main consequences for prevention |
|
Basic concept (accident as |
The objective is to identify “the” single or main cause |
Simple prevention measures concerning the immediate antecedent of the injury (individual protection, instructions about taking care, protection of dangerous machines) |
|
Concept focused on regulatory measures |
Focus on looking for who is responsible; the “enquiry” essentially identifies infringements and faults Rarely concerned about the conditions generating the situations examined |
Prevention usually limited to reminders about existing regulatory requirements or formal instructions |
|
Linear (or quasi-linear) concept (“domino” model) |
Identification of a chronological succession of “dangerous conditions” and “dangerous acts” |
Conclusions generally concerned with the dangerous acts |
|
Multifactorial concept |
Exhaustive research to gather the facts (circumstances, causes, factors, etc.) |
Concept not conducive to the search for solutions case by case (clinical analysis) and better adapted to the identification of statistical aspects (trends, tables, graphs, etc.) |
|
Systematic concept |
Identification of the network of factors of each accident |
Methods centred on clinical analysis |
Nowadays, a work accident is generally viewed as an index (or symptom) of dysfunction in a system consisting of a single production unit, such as a factory, workshop, team or work position. It is the nature of a system that its analysis requires the investigator to examine not only the elements that make up the system but also their relationships with one another and with the work environment. Within the framework of a system, the accident investigation seeks to trace to its origins the sequence of basic dysfunctions that have resulted in the accident and, more generally, the network of antecedents of the undesired event (accident, near accident or incident).
The application of methods of this kind, such as the STEP method (sequentially timed events plotting procedures) and the “tree of causes” method (similar to fault or event trees analyses), allows the accident process to be visualized in the form of an adjusted graph that illustrates the multicausality of the phenomenon. Because these two methods are so similar, it would represent a duplication of effort to describe them both; accordingly, this article concentrates on the tree of causes method and, where applicable, notes its main differences from the STEP method.
Information Useful for the Investigation
The initial phase of the investigation, the gathering of information, must allow the course of the accident to be described in concrete, precise and objective terms. The investigation therefore sets out to ascertain the tangible facts, taking care not to interpret them or to express an opinion about them. These are the antecedents of the accident, of which there are two types:
- those of an unusual nature (changes or variations) in relation to the “normal” or expected course of the work
- those of a permanent nature that have played an active part in the occurrence of the accident through the medium of or in combination with the unusual antecedents.
For example, insufficient protection of a machine (a permanent antecedent) can turn out to be a factor in an accident if it allows the operator to take up a position in a dangerous area in order to deal with a particular incident (unusual antecedent).
The information gathering is carried out at the location of the accident itself as soon as possible after its occurrence. It is preferably carried out by persons who know the operation or process and who try to obtain a precise description of the work without limiting themselves to the immediate circumstances of the damage or injury. The investigation is initially effected mainly by means of interviews, if possible with the worker or operator, victims and eyewitnesses, other members of the work team, and the hierarchical supervisors. If appropriate it is completed by means of a technical investigation and the use of outside expertise.
The investigation seeks to identify, in order of priority, the unusual antecedents, and to determine their logical connections. An effort is made at the same time to reveal the permanent antecedents that have allowed the accident to occur. In this way the investigation is able to go back to a stage more remote than the immediate antecedents of the accident. These more remote antecedents may concern individuals, their tasks, the equipment that they use, the environment in which they function and the safety culture. By proceeding in the way just described, it is generally possible to draw up a lengthy list of antecedents, but it will usually be difficult to make immediate use of the data. The interpretation of the data is made possible thanks to a graphic representation of all the antecedents involved in the genesis of the accident—that is, a tree of causes.
Constructing a Tree of Causes
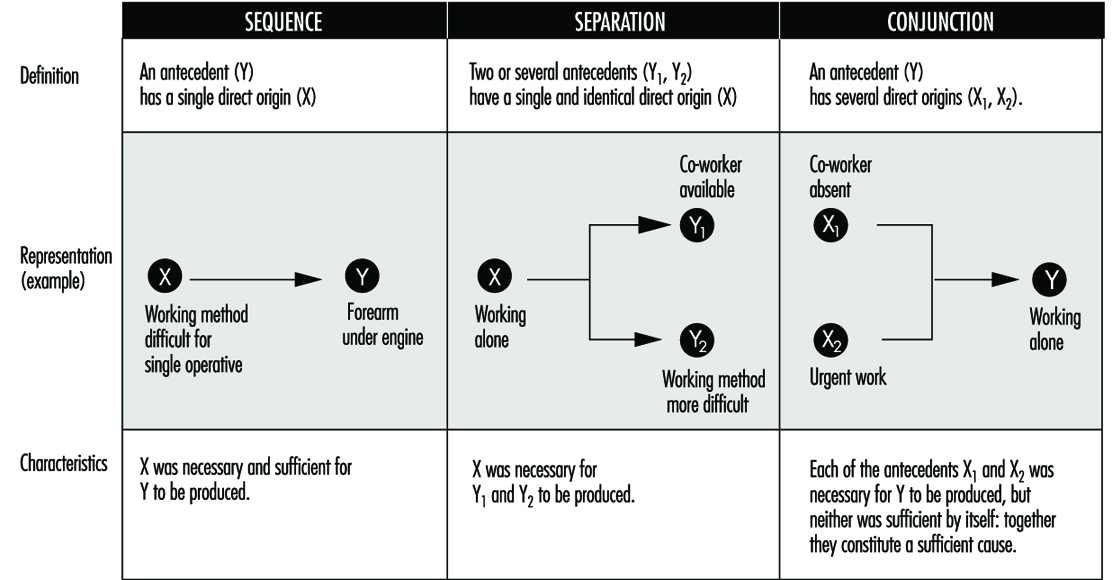
The tree of causes presents all the antecedents that have been gathered which have given rise to the accident, as well as the logical and chronological links that connect them; it is a representation of the network of antecedents that have directly or indirectly caused the injury. The tree of causes is constructed starting from the end-point of the event - that is, the injury or damage—and working backwards toward the cause by systematically asking the following questions for each antecedent that has been gathered:
- By which antecedent X was antecedent Y directly caused?
- Was antecedent X sufficient in itself to give rise to antecedent Y?
- If not, have there been other antecedents (X1, X2 Xn) that were equally necessary in order to give rise directly to antecedent Y?
This set of questions can reveal three types of logical connection, summarized in figure 1, among the antecedents.
Figure 1. Logical links used in the "tree of causes" method
The logical coherence of the tree is checked by asking the following questions for each antecedent:
- If X had not taken place, would Y nevertheless have occurred?
- In order for Y to occur, was X, and only X, necessary?
Moreover, the construction of the tree of causes in itself induces the investigators to pursue the information-gathering, and therefore the investigation, to a point well before the accident occurred. When completed, the tree represents the network of antecedents that have given rise to the injury—they are in fact the accident factors. As an example, the accident summarized below produced the tree of causes shown in figure 2.
Figure 2. Tree of causes of an accident suffered by an apprentice mechanic when remounting an engine in a car
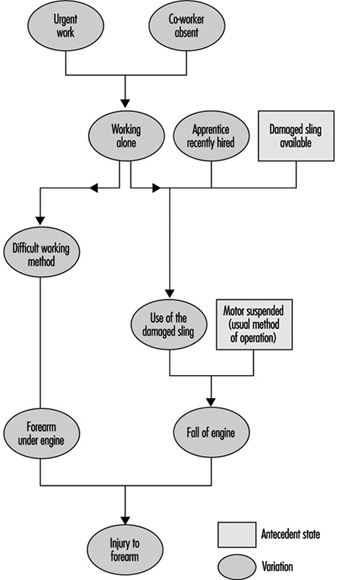
Accident Summary Report: An apprentice mechanic, recently recruited, had to work alone in an emergency. A worn sling was being used to suspend an engine that had to be remounted, and during this operation the sling broke and the engine fell and injured the mechanic’s arm.
Analysis by the STEP Method
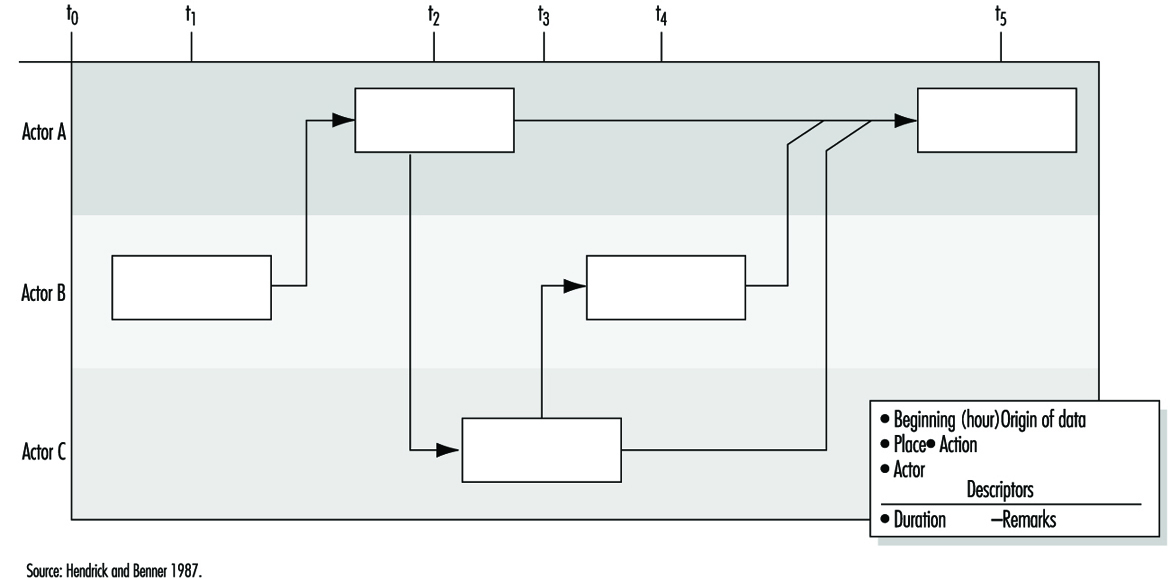
According to the STEP method (figure 3), each event is set out graphically so as to show the chronological order of its appearance, keeping one line per “agent” concerned (an agent is the person or thing that determines the course of events constituting the accident process). Each event is described precisely by indicating its beginning, duration, starting and ending place and so on. When there are several plausible hypotheses, the investigator can show them in the network of events by using the logical relationship “or”.
Figure 3. Example of representation possible by the STEP method
Analysis by the Tree of Causes Method
Making use of the tree of causes for the purposes of accident analysis has two objectives:
- making the reoccurrence of the same accident impossible
- averting the occurrence of more or less similar accidents - that is, accidents whose investigation would reveal common factors with the accidents that have already occurred.
Given the logical structure of the tree, the absence of a single antecedent would have prevented the occurrence of the accident. One judicious prevention measure would therefore suffice, in principle, to satisfy the first objective by preventing the reoccurrence of the same accident. The second objective would require that all the factors discovered should be eliminated, but in practice the antecedents are not all of equal importance for the purposes of prevention. It is therefore necessary to draw up a list of antecedents requiring reasonable and realistic preventive action. If this list is long, a choice has to be made. This choice has more chance of being appropriate if it is made within the framework of a debate between the partners concerned in the accident. Moreover, the debate will gain in clarity to the extent that it is possible to assess the cost-effectiveness of each measure proposed.
Effectiveness of Preventive Measures
The effectiveness of a preventive measure can be judged with the help of the following criteria:
The stability of the measure. The effects of a preventive measure must not disappear with time: informing the operators (in particular, reminding them of instructions) is not a very stable measure because its effects are often transient. The same is moreover true of some protective devices when they are easily removable.
The possibility of integrating safety. When a safety measure is added on - that is, when it does not contribute directly to production - it is said that safety is not integrated. Whenever this is so, it is observed that the measure tends to disappear. Generally speaking, any preventive measure entailing an additional cost for the operator should be avoided, whether it is a physiological cost (increasing the physical or nervous load), a psychological cost, a financial cost (in the case of salary or output) or even a simple loss of time.
The non-displacement of the risk. Some preventive measures may have indirect effects that are detrimental to safety. It is therefore always necessary to foresee the possible repercussions of a preventive measure on the system (job, team or workshop) in which it is inserted.
The possibility of general application (the notion of potential accident factor). This criterion reflects the concern that the same preventive action may be applicable to other jobs than the one affected by the accident under investigation. Whenever possible, an effort should be made to go beyond the particular case that has given rise to the investigation, an effort that often requires a reformulation of the problems discovered. The information obtained from an accident may thus lead to preventive action relating to factors that are unknown but present in other work situations where they have not yet given rise to accidents. For this reason they are called “potential accident factors”. This notion opens the way to the early detection of risks, mentioned later.
The effect on root “causes”. As a general rule, the prevention of accident factors near to the point of injury eliminates certain effects of dangerous situations, while prevention acting well upstream of the injury tends to eliminate the dangerous situations themselves. An in-depth investigation of accidents is justified to the extent that the preventive action is equally concerned with the upstream factors.
The time taken for application. The need to act as rapidly as possible after the occurrence of an accident so as to avoid its reoccurrence is often reflected in the application of a simple preventive measure (an instruction, for example), but this does not eliminate the need for other more lasting and more effective action. Every accident must therefore give rise to a series of proposals whose implementation is the subject of follow-up.
The above criteria are intended to give a better appreciation of the quality of preventive action proposed after each accident investigation. However, the final choice is not made solely on this basis, as other considerations, such as economic, cultural or social ones, must also be taken into account. Finally, the measures decided upon must obviously respect the regulations in force.
Accident Factors
The lessons drawn from each accident analysis deserve to be recorded systematically so as to facilitate passing from knowledge to action. Thus figure 4 consists of three columns. In the left-hand column are noted the accident factors requiring preventive measures. Possible preventive action is described in the middle column for each factor decided upon. After the discussion mentioned above, the action selected is recorded in this part of the document.
Figure 4. Lessons drawn from accidents and the use of these lessons

The right-hand column covers the potential accident factors suggested by the factors listed in the left-hand column: it is considered that each accident factor discovered is often only a particular case of a more general factor known as a potential accident factor. The passage from the particular case to the more general case is often made spontaneously. However, each time that an accident factor is expressed in such a fashion that it is not possible to encounter it elsewhere than in the situation in which it has appeared, a more general formulation must be considered. In doing this, it is necessary to avoid two opposite pitfalls so as to utilize the notion of potential accident factor effectively in the early detection of risks arising later. A formulation that is too circumscribed does not permit systematic detection of the factors, whereas one that is too wide makes the notion unworkable and is of no further practical interest. The detection of potential accident factors thus presupposes their being well formulated. This detection can then be carried out in two ways, which are moreover complementary:
- either by looking for the possible presence of potential factors already known at the level of a job or a wider area (workshop, service)
- or by looking for jobs where a factor already determined may be observed.
Usefulness, Effectiveness and Limitations of Accident Investigation
Usefulness. As compared to non-systematic investigations, methods of accident investigation based on a systematic concept have numerous advantages, which include the following:
- They allow the causal network of each accident to be defined collectively, from which it is easier to devise new preventive measures and foresee their impact without being limited to the direct causes of the injury.
- They provide those involved in the analysis with a richer and more realistic mental representation of the “accident phenomenon” that permits a global understanding of work situations.
- In-depth accident investigations (especially when they are extended to cover incidents and undesired events) can become a means and appropriate occasion for dialogue between management and operators.
Effectiveness. In order to be effective, accident investigation requires that four conditions are satisfied concurrently:
- an evident commitment on the part of the top management of the establishment, who must be able to ensure the systematic implementation of such procedures
- training of the investigators
- management, supervisors and workers fully informed concerning the aims of the investigation, its principles, the requirements of the method and the results expected
- real improvements in safety conditions that will encourage those involved in future investigations.
Limitations. Even when carried out very well, accident investigation suffers from a double limitation:
- It remains a procedure for investigating risks a posteriori (in the manner of systems analysis), with the aim of correcting existing situations. It does not therefore dispense with the need for a priori (prospective) investigations, such as the ergonomic investigation of jobs or, for complex systems, safety investigations.
- The usefulness of accident investigations also varies with the safety level of the establishment where they are applied. In particular, when the safety level is high (the accident rate is low or very low), it is evident that serious accidents result from the conjunction of numerous independent random factors that are relatively harmless from the safety viewpoint when considered outside the context under investigation.