Firefighting is one of the world’s most honoured but hazardous operations. By becoming fire-fighters, people join an organization rich in heritage of dedication, unselfish sacrifice and inspired human action. The job of a fire-fighter is not comfortable or easy. It is one that requires a high sense of personal dedication, a genuine desire to help people and a devotion to a profession that requires a high level of skill. It is also a profession that exposes an individual to a high level of personal danger.
Whenever there is a disaster, the fire department is one of the first called to the scene. Because it is a disaster, the conditions will not always be favourable. There will be hard, fast work that will drain energy and test endurance. The situation will not always involve fire. There will be cave-ins, building collapses, auto accidents, aircraft crashes, tornadoes, dangerous-goods incidents, civil disturbances, rescue operations, explosions, water incidents and medical emergencies. The emergency list is unlimited.
All fire-fighters use the same tactics and strategies to combat a fire. The strategies are simple—fight this fire offensively or defensively. Regardless, the goal is the same—extinguishment of the fire. Urban firefighting deals with structural firefighting. (The management of forest fires is dealt with in the chapter Forestry). It includes dealing with hazardous goods, water and ice, as well as high-angle rescue and emergency medicine. Fire service personnel must respond day and night to emergencies.
The tactical priorities that fire-fighters engage in during the course of the fire are shown in figure 1. It is during these operations that hose lays using attack lines, back up lines and supply lines can be employed. Other commonly used equipment are ladders and pushing/pulling and striking tools like axes and pike poles. Specialty equipment includes tarps that are used for salvage or hydraulic tools used for a rescue. The fire-fighter must use and be familiar with all of them. See figure 1.
Figure 1. The tactical priorities of structural firefighting operations.
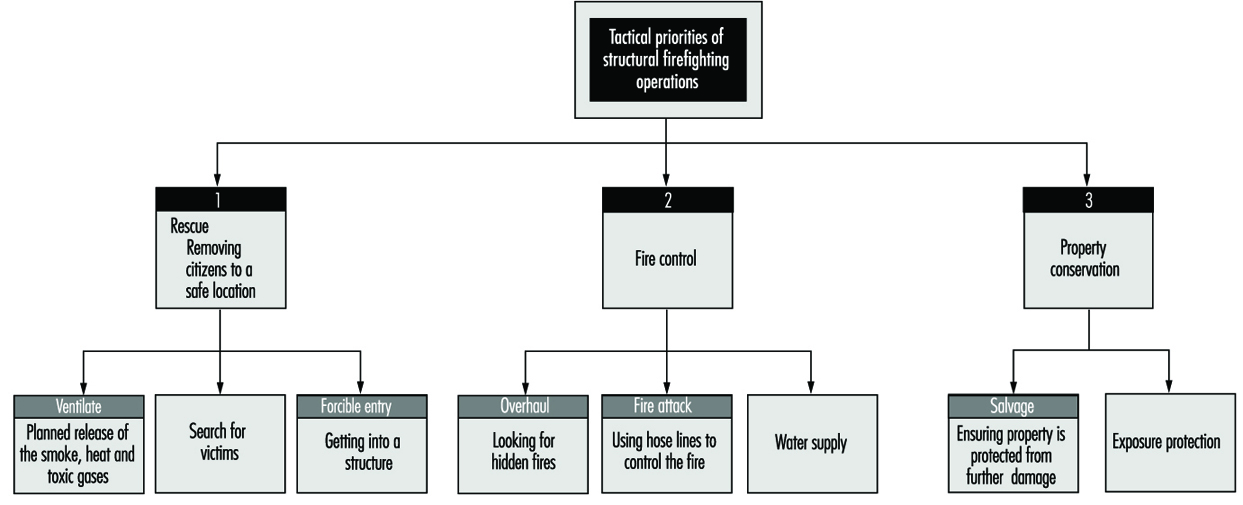
Figure 2 shows a fire-fighter with appropriate personal protection laying water on a structural fire with a fire hose.
Figure 2. Firefighter laying water on a structural fire.

These operations expose the fire-fighter to the greatest risks and injuries regardless of the tool used or the operation engaged in. Back injuries, sprains, fall-related injuries and heat stress commonly occur. Heart and lung diseases are quite common among fire-fighters, which is thought to be due, in part, to the toxic gases and the level of physical activity required on the fire ground. Therefore, many departments are aggressively pursuing the addition of fitness programmes within their departments’ overall safety programme. Many jurisdictions have programmes in place to deal with critical incident stress, because the fire-fighter faces incidents that can create severe emotional reactions. Such reactions are normal reactions in the face of very abnormal situations.
The mission of every fire department is the preservation of life and property; therefore, safety on the fire ground is of paramount importance. Many of the operations discussed here have an underlying goal of providing greater safety on the fire ground. Many of the dangers that exist on the fire ground are due to the nature of fire. Backdraft and flashover kill fire-fighters. Backdraft is caused by the introduction of air into a superheated oxygen-starved area. Flashover is the build-up of heat within an area until it suddenly ignites everything within that area. These two conditions reduce the level of safety and increase property damage. Ventilation is one method of control that fire-fighters use. Increasing ventilation can lead to much damage to property. The fire-fighter is often observed breaking windows or cutting holes in the roof and intensity of the fire appears to grow. This is because smoke and toxic gases are released from the fire area. But this is a necessary part of firefighting. Special attention must be paid to roof collapse, to establishing a quick means of egress and to back-up hose lines for protection of the personnel and property.
The fire-fighter must put safety first and must work with a safety-conscious attitude and within organizational environments that promote safety. In addition, proper protective clothing must be provided and maintained. Clothing should be designed for freedom of movement and protection from heat. The structural fire-fighter must be outfitted with heavy fire-resistant fibre suits and a self-contained breathing apparatus.
The type of clothing worn is generally specific to the types of hazards faced by the fire-fighter outside the fire area on the fire line; the urban fire-fighter is generally inside a structure where intense heat and toxic gases are present. Helmets, boots and gloves designed specifically for the hazard that is faced by the fire-fighter provide head, foot and hand protection. Fire crews need training to ensure that fire-fighters have the knowledge and skills necessary to perform safely and efficiently. Training is usually provided through an in-house training programme, which can consist of a combination of on-the-job training and a formalized theory programme. Most provincial and state governments have agencies that promote various types of training programmes.
North America leads the world in property loss and many North American departments engage in preventive programmes to reduce the life and property losses within their jurisdictions. Public education and enforcement programmes are aggressively pursued by the most pro-active departments because, according to available statistics, the cost of prevention is cheaper than the cost of rebuilding. Furthermore, only 10% of businesses that suffer a total fire loss successfully rebuild. Thus the costs of a fire loss to a community can be staggering, since in addition to the cost to rebuild, sources of tax revenue, jobs and lives may also be lost forever. It is important, therefore, that both the community and the fire service work together to ensure that lives and property are preserved.