Human Factors in Accident Modelling
Human factors are a major component of the causes of accidents in the workplace. Estimates of the actual extent of the involvement vary markedly, but a study in the early 1980s of the causes of all work-related fatalities occurring in Australia over three years revealed that behavioural factors were involved in more than 90% of fatal accidents. In view of data like these, it is important to have an understanding of the role of human factors in accidents. Traditional models of accident causation placed superficial emphasis on human factors. Where human factors were included, they were depicted as linked to error occurring in the immediate sequence of events leading to the accident. A better understanding of how, why and when human factors become involved in accidents enhances our ability to make predictions about the role of human factors and helps to prevent accidents. A number of models have been put forward that attempt to describe the part that human factors play in accidents.
Accident Causation Models
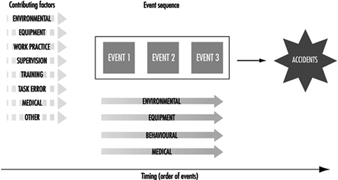
Recent models have extended the role of human factors beyond the immediate causal events leading to the accident. Models now tend to include additional factors in the wider circumstances of the accident. Figure 1 shows details of such an approach: For example, human factors, such as work practices and supervision, can be included both as error in the event sequence leading immediately to the accident and as pre-existing human factors contributing to the accident event sequence. The two main components (contributing factors and event sequences) of this human factors model should be envisaged as occurring on a notional time line on which the order—contributing factors followed by a sequence of errors—is fixed, but the time base on which they occur is not. Both of these components are essential parts of accident causation.
Figure 1. Model of accident causation
The Nature of Error
An essential component of accident prevention, therefore, is gaining an understanding of the nature, timing and causes of error. One of the important and unique characteristics of error, distinguishing it from other factors involved in accidents, is that error is a normal part of behaviour. Error plays a fundamental role in learning new skills and behaviours and in maintaining those behaviours. Through testing the boundaries of interactions with the environment, and consequently making errors, humans learn just what the boundaries are. This is essential not only for learning a new skill but also for updating and maintaining ones they have already learned. The degree to which humans test the boundaries of their skills is related to the level of risk that they are prepared to accept.
It seems that errors are a constant feature of all behaviour. Studies show also that they occur in the causes of approximately two-thirds of work-related fatal accidents. It is essential therefore to develop some ideas about the form they are likely to take, and when and why they might occur. While there are many aspects of human error that are not yet understood, our current level of understanding allows some predictions to be made about error types. Knowledge of these types of error will, it is to be hoped, guide our efforts to prevent error or at least to modify the adverse consequences of error.
One of the most important features of the nature of error is that it is not a unitary phenomenon. Even though traditional accident analysis often treats error as if it were a singular entity which cannot be dissected further, there are a number of ways that errors can occur. Errors differ depending on the information-processing function being challenged. For example, errors can take the form of false sensations due to poor or degraded stimulation of the sensory organs, attentional failures due to the demands of prolonged or very complex stimulation from the environment, various types of memory lapses, errors of judgement and reasoning errors. All of these types of errors are distinguishable in terms of the context or task characteristics in which they occur. They signify breakdown in different information-processing functions and consequently would require different approaches to overcoming each of them.
Different types of error can also be distinguished with respect to skilled and unskilled behaviour. Training is often said to be a solution to problems of human error since skilled behaviour means that the required sequence of actions can be performed without conscious, constant attention and feedback, requiring only intermittent conscious checking to ensure that the behaviour is on track. The advantages of skilled behaviour are that once triggered, it requires little effort from the operator. It allows other activities to be undertaken at the same time (for instance, one can drive an automobile and talk at the same time) and allows the operator to plan for future aspects of the task. Furthermore, skilled behaviour is usually predictable. Unfortunately, while greater skill reduces the likelihood of many types of error, it increases the likelihood of others. Errors during skilled behaviour occur as absent-minded or unintended actions or lapses and are distinct from the mistakes which occur during unskilled behaviour. Skill-based errors tend to be associated with switching in the nature of attentional control of the task. They can occur during the conscious checking mode or they may be due to conclusion of similar patterns of skilled behaviour.
A second characteristic of errors is that they are not novel or random. Error forms are limited. They take similar forms in all types of functions. For example, “place losing” errors occur in speech and perceptual tasks as well as in knowledge-related or problem-solving tasks. Similarly, the timing and location of error in the accident causation sequence does not appear to be random. An important characteristic of information processing is that it is expressed in the same way regardless of the setting. This means that the error forms that occur in everyday life in the kitchen, for example, occur in the same manner in the most high-risk industries. The consequences of these errors, however, are very different and are determined by the setting in which the error occurs, rather than by the nature of the error itself.
Models of Human Error
In the categorization of error and the development of models of human error, it is important to take all aspects of error into account to the extent possible. The resulting categorization, however, needs to be usable in practice. This is possibly the biggest constraint. What can be done in developing a theory of accident causation can be very difficult to apply in practice. In attempting to analyse the causes of an accident, or to predict the role of human factors in a process, it is not possible to understand all aspects of human information processing which contributed or might contribute. It may never be possible, for example, to know the role of intention before an accident occurred. Even afterwards, the very fact that the accident had occurred can change a person’s recall of the events surrounding it. The error categorizations that have been most successful to date therefore focus on the nature of the behaviour that was performed at the time the error occurred. This allows error analysis to be relatively objective and as reproducible as possible.
These categorizations of error distinguish between those occurring during skilled behaviour (slips, lapses or unintended acts) and those occurring during unskilled or problem-solving behaviour (mistakes).
Slips or skill-based errors are defined as unintended errors occurring when the behaviour is a highly practised routine or automatic in nature.
Mistakes have been further categorized into two types:
- rule-based errors, which occur when the behaviour requires the application of rules
- knowledge-based errors, which occur during problem solving when the person has no skill or rule to apply.
This means that knowledge-based errors occur through lack of expertise, rule-based errors through the failure to apply the expertise appropriately, and skill-based errors through a disruption of the execution of the programme of actions, usually due to changes in attentional level (Rasmussen 1982).
Application of these categories in a population study of work-related fatal accidents showed that they could be used reliably. The results showed that skill-based errors occurred most frequently overall and that occurrences of the three error types were distributed differently across the event sequence. Skill-based errors, for example, occurred most commonly as the last event immediately before the accident (79% of fatalities). Since, at this point, there is little time for recovery, their consequences may be more severe. Mistakes, on the other hand, appear to be distributed earlier in the accident sequence.
Human Factors in the Wider Circumstances of Accidents
Elaboration of the involvement of human factors other than human error in the circumstances immediately surrounding the accident represents a major advance in understanding accident genesis. While there is no question that error is present in most accident sequences, human factors are also involved in a broader sense, taking the form, for example, of standard operating work procedures and the influences that determine the nature and acceptability of work procedures, including the earliest decisions of management. Clearly, flawed work procedures and decisions are related to error since they involve errors of judgement and reasoning. However, flawed work procedures are distinguished by the characteristic that the errors of judgement and reasoning have been permitted to become standard ways of operating, since, having no immediate consequences, they do not make their presence urgently felt. They are, nevertheless, recognizable as unsafe work systems with fundamental vulnerabilities that provide the circumstances which may later, unintentionally, interact with human action and lead directly to accidents.
In this context, the term human factors covers a wide range of elements involved in the interaction between individuals and their working environment. Some of these are direct and observable aspects of the ways in which work systems function that do not have immediate adverse consequences. Design, use and maintenance of equipment, the provision, use and maintenance of personal protective and other safety equipment and standard operating procedures originating from management or workers, or both, are all examples of such ongoing practices.
These observable aspects of human factors in system functioning are to a large extent manifestations of the overall organizational setting, a human element even more removed from direct involvement in accidents. Characteristics of organizations have been collectively termed organizational culture or climate. These terms have been used to refer to the set of goals and beliefs an individual holds and the impact of the organization’s goals and beliefs on those of the individual. Ultimately, the collective or norm values, reflecting the characteristics of the organization, are likely to be influential determinants of attitude and motivation for safe behaviour at all levels. The level of risk tolerated in a work setting, for example, is determined by such values. Thus, the culture of any organization, clearly reflected in its work system and the standard operating procedures of its workers, is a crucial aspect of the role of human factors in accident causation.
The conventional view of accidents as a number of things suddenly going wrong at the time and the place of the accident, concentrates attention on the overt measurable event at the time of the accident. In fact, errors occur in a context which itself may allow the unsafe act or error to have its consequences. In order to reveal accident causes that originate in pre-existing conditions in work systems, we need to take into account all of the various ways in which the human element can contribute to accidents.This is perhaps the most important consequence of taking a broad view of the role of human factors in accident causation. Flawed decisions and practices in work systems, while not having an immediate impact, act to create the setting conducive to operator error—or to the error’s having consequences—at the time of the accident.
Traditionally, organizational aspects of accidents have been the most neglected aspect of accident analysis design and data collection. Because of their distant relationship in time from the occurrence of the accident, the causal link between accidents and organizational factors has often not been obvious. Recent conceptualizations have specifically structured analysis and data collection systems in such a way as to incorporate the organizational components of accidents. According to Feyer and Williamson (1991), who used one of the first systems designed to specifically include the organizational contribution to accidents, a considerable proportion of all occupational fatalities in Australia (42.0%) involved pre-existing and ongoing unsafe work practices as a causal factor. Waganaar, Hudson and Reason (1990), using a similar theoretical framework in which the organizational contribution to accidents was recognized, argued that organizational and managerial factors constitute latent failures in work systems that are analogous to resident pathogens in biological systems. Organizational flaws interact with triggering events and circumstances in the immediate circumstances surrounding accidents much as resident pathogens in the body combine with triggering agents such as toxic factors to bring about disease.
The central notion in these frameworks is that organizational and managerial flaws are present long before the onset of the accident sequence. That is, they are factors which have a latent or delayed-action effect. Thus, to understand how accidents occur, how people contribute to them and why they behave the way that they do, it is necessary to ensure that analysis does not begin and end with the circumstances that most directly and immediately lead to harm.
The Role of Human Factors in Accidents and Accident Prevention
In acknowledging the potential aetiological significance of the wider circumstances surrounding the accident, the model best describing accident causation has to take into account the relative timing of elements and how they relate to each other.
First, causal factors vary in terms of their causal importance, and also in terms of their temporal importance. Furthermore, these two dimensions can vary independently; that is, causes can be important because they occur very close in time to the accident and therefore they reveal something about the time of the accident, or they can be important because they are a prime cause underlying the accident, or both. By examining both the temporal and causal importance of factors involved in the wider circumstances as well as the immediate circumstances of the accident, analysis focuses on why the accident happened, rather than just describing how it happened.
Second, accidents are generally agreed to be multicausal. Human, technical and environmental components in the work system can interact in critical ways. Traditionally, accident analysis frameworks have been limited in terms of the range of categories defined. This, in turn, limits the nature of the information obtained and so limits the range of options highlighted for preventive action. When the wider circumstances of the accident are taken into consideration, the model has to deal with an even more extensive range of factors. Human factors are likely to interact with other human factors and also with non-human factors. The patterns of occurrences, co-occurrences and inter-relationships of the wide range of possible different elements within the causal network provides the most complete and therefore most informative picture of accident genesis.
Third, these two considerations, the nature of the event and the nature of its contribution to the accident, interact. Although multiple causes are always present, they are not equivalent in role. Accurate knowledge of the role of factors is the essential key to understanding why an accident happens and how to prevent it from recurring. For example, immediate environmental causes of accidents may have their impact because of earlier behavioural factors in the form of standard operating procedures. Similarly, pre-existing aspects of work systems may provide the context in which routine errors committed during skill-based behaviour can precipitate an accident with harmful consequences. Normally these routine errors would have benign consequences. Effective prevention would be best served if it were targeted towards the latent underlying causes, rather than the immediately precipitating factors. This level of understanding of the causal network and how it influences outcome is possible only if all types of factors are included for consideration, their relative timing is examined and their relative importance is determined.
Despite the potential for an almost infinite variety in the ways that human action can directly contribute to accidents, relatively few patterns of causal pathways account for the majority of accident causation. In particular, the range of underlying latent conditions which set the scene for later human and other factors to have their effect are limited predominantly to a small number of aspects of work systems. Feyer and Williamson (1991) reported that only four patterns of factors accounted for the causes of approximately two-thirds of all occupational fatalities in Australia over a 3-year period. Not surprisingly, almost all of these involved human factors at some point.
Summary
The nature of human involvement varies as to type and timing and as to its importance in terms of causing the accident (Williamson and Feyer 1990). Most commonly, human factors in the form of a limited range of pre-existing, flawed work systems create the underlying prime causes of the fatal accidents. These combine with later lapses during skilled performance or with hazards in environmental conditions to precipitate the accident. These patterns illustrate the layered role typical of the involvement of human factors in accident genesis. To be of use in preventive strategy formulation, however, the challenge is not to simply describe the various ways in which the human element is involved but rather to identify where and how it may be possible to intervene most effectively. This is possible only if the model used has the capacity to describe accurately and comprehensively the complex network of interrelated factors involved in accident causation, including the nature of the factors, their relative timing and their relative importance.
Theory of Accident Causes
Accidents are defined as unplanned occurrences which result in injuries, fatalities, loss of production or damage to property and assets. Preventing accidents is extremely difficult in the absence of an understanding of the causes of accidents. Many attempts have been made to develop a prediction theory of accident causation, but so far none has been universally accepted. Researchers from different fields of science and engineering have been trying to develop a theory of accident causation which will help to identify, isolate and ultimately remove the factors that contribute to or cause accidents. In this article, a brief outline of various accident causation theories is presented, followed by a structure of accidents.
Accident Causation Theories
The domino theory
According to W.H. Heinrich (1931), who developed the so-called domino theory, 88% of all accidents are caused by unsafe acts of people, 10% by unsafe actions and 2% by “acts of God”. He proposed a “five-factor accident sequence” in which each factor would actuate the next step in the manner of toppling dominoes lined up in a row. The sequence of accident factors is as follows:
- ancestry and social environment
- worker fault
- unsafe act together with mechanical and physical hazard
- accident
- damage or injury.
In the same way that the removal of a single domino in the row would interrupt the sequence of toppling, Heinrich suggested that removal of one of the factors would prevent the accident and resultant injury; with the key domino to be removed from the sequence being number 3. Although Heinrich provided no data for his theory, it nonetheless represents a useful point to start discussion and a foundation for future research.
Multiple causation theory
Multiple causation theory is an outgrowth of the domino theory, but it postulates that for a single accident there may be many contributory factors, causes and sub-causes, and that certain combinations of these give rise to accidents. According to this theory, the contributory factors can be grouped into the following two categories:
Behavioural. This category includes factors pertaining to the worker, such as improper attitude, lack of knowledge, lack of skills and inadequate physical and mental condition.
Environmental. This category includes improper guarding of other hazardous work elements and degradation of equipment through use and unsafe procedures.
The major contribution of this theory is to bring out the fact that rarely, if ever, is an accident the result of a single cause or act.
The pure chance theory
According to the pure chance theory, every one of any given set of workers has an equal chance of being involved in an accident. It further implies that there is no single discernible pattern of events that leads to an accident. In this theory, all accidents are treated as corresponding to Heinrich’s acts of God, and it is held that there exist no interventions to prevent them.
Biased liability theory
Biased liability theory is based on the view that once a worker is involved in an accident, the chances of the same worker becoming involved in future accidents are either increased or decreased as compared to the rest of workers. This theory contributes very little, if anything at all, towards developing preventive actions for avoiding accidents.
Accident proneness theory
Accident proneness theory maintains that within a given set of workers, there exists a subset of workers who are more liable to be involved in accidents. Researchers have not been able to prove this theory conclusively because most of the research work has been poorly conducted and most of the findings are contradictory and inconclusive. This theory is not generally accepted. It is felt that if indeed this theory is supported by any empirical evidence at all, it probably accounts for only a very low proportion of accidents without any statistical significance.
The energy transfer theory
Those who accept the energy transfer theory put forward the claim that a worker incurs injury or equipment suffers damage through a change of energy, and that for every change of energy there is a source, a path and a receiver. This theory is useful for determining injury causation and evaluating energy hazards and control methodology. Strategies can be developed which are either preventive, limiting or ameliorating with respect to the energy transfer.
Control of energy transfer at the source can be achieved by the following means:
- elimination of the source
- changes made to the design or specification of elements of the work station
- preventive maintenance.
The path of energy transfer can be modified by:
- enclosure of the path
- installation of barriers
- installation of absorbers
- positioning of isolators.
The receiver of energy transfer can be assisted by adopting the following measures:
- limitation of exposure
- use of personal protective equipment.
The “symptoms versus causes” theory
The “symptoms versus causes” theory is not so much a theory as an admonition to be heeded if accident causation is to be understood. Usually, when investigating accidents, we tend to fasten upon the obvious causes of the accident to the neglect of the root causes. Unsafe acts and unsafe conditions are the symptoms—the proximate causes—and not the root causes of the accident.
Structure of Accidents
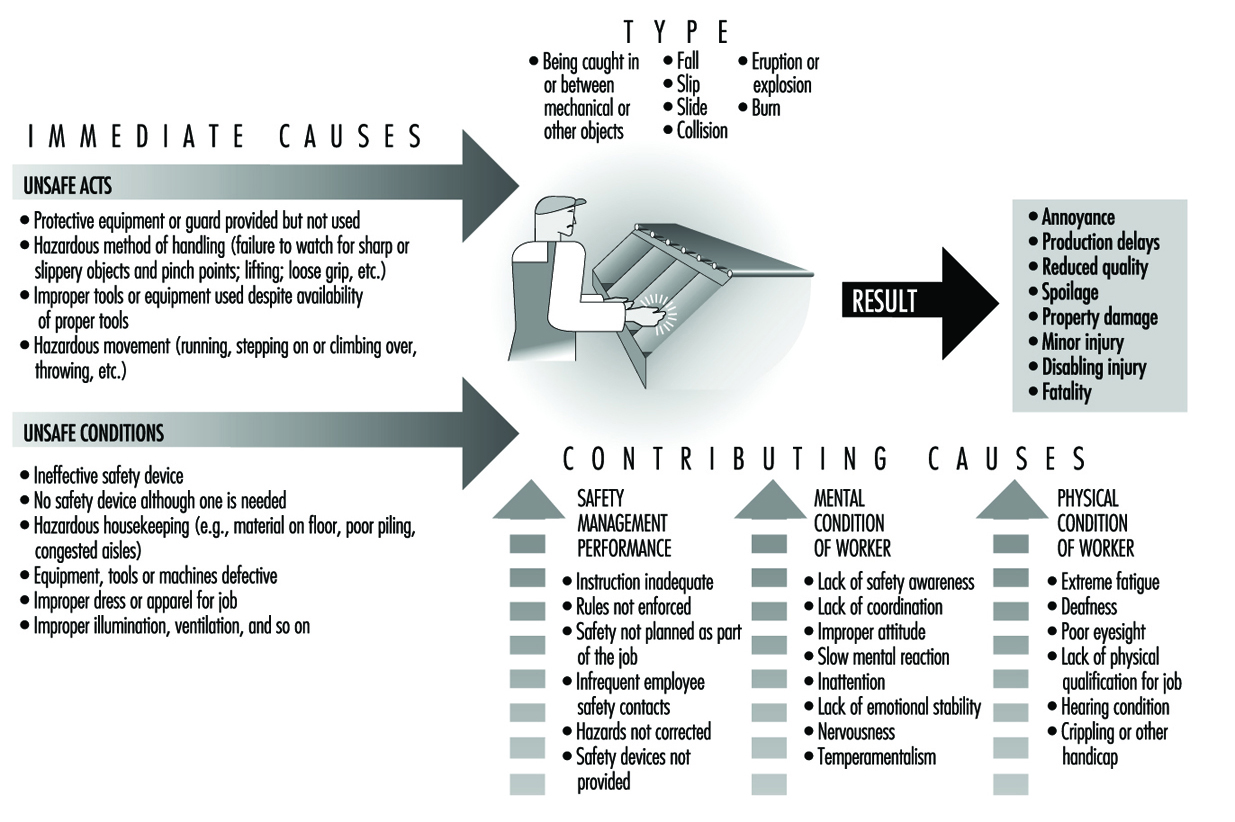
The belief that accidents are caused and can be prevented makes it imperative for us to study those factors which are likely to favour the occurrence of accidents. By studying such factors, the root causes of accidents can be isolated and necessary steps can be taken to prevent the recurrence of the accidents. These root causes of accidents can be grouped as “immediate” and “contributing”. The immediate causes are unsafe acts of the worker and unsafe working conditions. The contributing causes could be management-related factors, the environment and the physical and mental condition of the worker. A combination of causes must converge in order to result in an accident.
Figure 1 shows the structure of accidents, including the details of immediate causes, contributing causes, types of accidents and results of accidents. This accounting is not exhaustive by any means. However, an understanding of the “cause and effect” relation of the accident-causing factors is required before continuous improvement of safety processes can be undertaken.
Figure 1. Structure of Accidents
Summary
Accident causation is very complex and must be understood adequately in order to improve accident prevention. Since safety lacks a theoretical base, it cannot be regarded as being a science yet. This fact should not discourage us, as most of the scientific disciplines—mathematics, statistics and so on—passed through a similarly tentative phase at one time or the other. Accident causation study holds great promise for those who are interested in developing the pertinent theory. At present, theories of accident causation are conceptual in nature and, as such, are of limited use in preventing and controlling accidents. With such a diversity of theories, it will not be difficult to understand that there does not exist one single theory that is considered right or correct and is universally accepted. These theories are nonetheless necessary, but not sufficient, for developing a frame of reference for understanding accident occurrences.
Concepts of Accident Analysis
The purpose of this article is to provide a guide for calculating the magnitude of the accident problem; it is not a description of the magnitude itself. In dealing with occupational accidents, the magnitude of the problem can be estimated in different ways, depending on one’s need to estimate how big the problem has been or how big it will be in the future. (Some people may say that this distinction is an unnecessary one, since knowledge of the current extent of the problem will serve to indicate what is to be expected in the future.) The magnitude of the problem as well as its types differs from country to country, from industry to industry and from workplace to workplace.
An accident may be described as a result of a chain of events in which something has gone wrong, resulting in an undesired conclusion. It has been shown that human intervention may prevent the injury or damage to which such a chain of events would otherwise lead. However, given the fact of human intervention, the potential exists for far more dangerous possible chains of events than those actually leading to injury or damage. These possibilities must be considered in assessing the full extent of workplace risk. Assuming that events that might lead to injury or damage occur because of factors in the workplace, one is led to conclude that the magnitude of the problem has to be determined on the basis of the existence and frequency of such factors.
When dealing with accidents in the workplace, one can estimate the magnitude of the problem retrospectively by comparing the number of accidents (incidence rate) with the severity of the accidents (lost work days). However, if one wants to estimate the magnitude of the problem prospectively, it is done by evaluating the presence of risk factors in the workplace—that is, factors that might lead to accidents.
A sufficiently complete and accurate view of the state of affairs with respect to workplace accidents can be gained by means of a comprehensive reporting and record-keeping system. Analyses of well-prepared accident reports can give a picture of the basic relationships essential to understanding the causes of the accidents. In order to estimate the magnitude of the problem in detail, a determination of risk factors is essential. Knowledge of the relevant risk factors can be obtained by analysing the detailed information provided with each accident record as to where workers and operators were located when the accident occurred, what they were doing or handling, by what means, what damages or injuries occurred and other particulars surrounding the accident.
Risk
Risk measurement must be made on the basis of information regarding the number and seriousness of injuries that have occurred in the past, yielding a retrospective measurement. The risk of injury to individuals may be described by two types of data:
- Measurement of risk provides a calculated frequency of injuries and a measurement of the seriousness of the injury. This could be described as the number of lost work day cases (or fatalities) per number of workers (e.g., in Denmark, the risk of dying in an occupational accident is 3 fatalities per 100,000 employees).
- Type of risk or element of danger assessment provides not only an indication of the exposure sources and other harmful factors which may cause an accident, but also an indication of the circumstances leading to injury or damage. Work performed at a height, for example, will involve a risk of falling, with serious injury as a possible result. Similarly, work with cutting tools involves a risk of cuts from contact with sharp components, and work with noisy machines for a long period of time may result in hearing damage.
There exists a good deal of common-sense knowledge on many types of risks. For example, if you work at a height, you may fall; if it is slippery underfoot, then you may slip; and if there are sharp objects nearby, you may cut yourself. Many types of risk, not apparent to common sense, may be overlooked. With regard to these, the worker must be informed of the risk (e.g., that noise causes hearing damage, that some solvents cause brain damage and that certain chemicals cause acute poisoning by inhalation). Our knowledge of types of risk, from the most to the least conspicuous, whether gained through everyday experience or through research efforts, is based on past events. However, it is one thing to know what has happened, and another to assess what will happen in the future. It should be noted that the very knowledge of the exposure sources and other potentially harmful factors which may cause damage or injury in connection with tasks of various sorts, as well as knowledge of the factors that can either heighten or reduce those risk factors that influence risk measurement, can provide a basis for recognition of the risk.
Factors Determining Risk
The factors which are of greatest relevance in determining risk are:
- factors which determine the presence or absence (or potential) of risks of any sort
- factors which either increase or minimize the probability of these risks resulting in accidents or injuries
- factors affecting the seriousness of accidents associated with these risks.
To clarify the first point, it is necessary to identify the causes of the accident—namely, exposure sources and other harmful factors; the two latter points constitute the factors which influence the measurement of risk.
The primary factors in the working environment which are the direct causes of harm, either by way of occupational diseases or occupational accidents, are as follows:
Exposure sources and occupational disorders
The concept of injuries due to exposure sources is often linked to the concept of disease (or disorder) because a disease can be viewed as caused by exposure to one or several agents over a short (acute exposure) or long (chronic exposure) period of time. Chronic exposure agents are usually not directly harmful, but take effect rather after a relatively constant and extended period of exposure, whereas acute exposures are almost instantaneously harmful. The intensity, harmfulness and period of action is of importance to the development of the injury, which may often be a matter of a combination of the effects of several different agents. This fact makes it difficult to point out and determine the exposure sources because (among other reasons) monocausal correlations between specific disorders and specific exposure sources are almost never found.
Examples of exposure sources which may result in an injury in the form of a disease-like condition are:
- chemical exposures (solvents, cleaning agents, degreasing agents, etc.)
- physical exposures (noise, radiation, heat, cold, inadequate lighting, lack of oxygen, etc.)
- physiological exposures (heavy loads, bad work postures or repetitive work)
- biological exposures (viruses, bacteria, flour, animal blood or leather, etc.)
- psychological exposures (work in isolation, threat of violence, changing working hours, unusual job demands, etc.).
Harmful factors and occupational accidents
The concept of harmful factors (not including exposure sources) is linked to occupational accidents, because this is where damages occur and workers are exposed to the type of actions that cause instant injury. This type of action is easily identified because the damage or injury is recognized immediately when it occurs. The difficulty attached to this type of injury is the unexpected contact with the harmful factor.
Examples of harmful factors which may result in persons being injured by an accident are often linked to different energy forms, sources or activity, such as the following:
- energy that involves cutting, dividing or planing, usually in connection with such types of sharp objects as knives, saws and edged tools
- energy that involves pressing and compressing, usually in connection with different shaping means such as presses and clamping tools
- the conversion of kinetic energy into potential energy—for example, when something hits or falls against a worker
- the conversion of potential energy in a person into kinetic energy, such as occurs in falls from one level to another
- heat and cold, electricity, sound, light, radiation and vibration
- toxic and corrosive substances
- energy exposing the body to excessive stress in such actions, for example, as the moving of heavy loads or twisting of the body
- mental and psychological stresses such as the threat of violence.
Controlling Exposures
Exposure sources or other harmful factors are to a great extent governed by the nature of the processes, technologies, products and equipment to be found in the workplace, but may also be governed by the way in which the work is organized. From the point of view of measurable risk, it should be recognized that control of the probability of exposures and the seriousness of injuries to workers often depends on the following three factors:
- Elimination/substitution safety measures. Workplace hazards in the form of exposure sources or other harmful factors may be eliminated or mitigated by substitution (e.g., a less harmful chemical may replace a toxic chemical in a process). It should be noted that this is not totally possible, as exposure sources and other harmful factors will always be present in human surroundings (not least with respect to human working conditions).
- Technical safety measures. These measures, often called engineering controls, consist of separating persons from harmful factors by encapsulating the harmful elements, or installing barriers between workers and the factors which may cause injury. Examples of these measures include, but are not limited to, automation, remote control, use of ancillary equipment and machine protection (guarding).
- Organizational safety measures. Organizational safety measures, also known as administrative controls, include separating persons from harmful factors either by means of special working methods or by separation in time or space. Examples of these controls include, but are not limited to, reduced exposure time, preventive maintenance programmes, encapsulating the individual workers with personal protective equipment, and expedient organization of work.
Controlling Human Conduct
It is often not possible to isolate all hazards using the above control measures. It is commonly supposed that accident prevention analysis ends here because it is believed that the workers will then be able to take care of themselves by acting “according to the rules”. This means that safety and risk will at some point depend on factors which control human conduct—namely, whether the individual person has the knowledge, the skills, the opportunity and the will to act so as to ensure safety in the workplace. The following illustrates the role of these factors.
- Knowledge. Workers must first be aware of the types of risk, potential hazards and elements of danger that may be found in the workplace. This usually requires education, training and job experience. The risks also need to be identified, analysed, recorded and described in a readily understandable manner so that workers know when they are in a specific risk situation and what consequences are liable to follow from their actions.
- The opportunity to act. It must be possible for the workers to act safely. It is necessary for workers to be able to make use of the available technical and organizational—as well as physical and psychological—opportunities for action. Positive support of the safety programme must be forthcoming from management, supervisors and the surroundings, including concern about risk taking, designing and following working methods with safety in view, safe use of the proper tools, clearly defining tasks, establishing and following safe procedures, and providing clear instructions on how equipment and materials are to be safely handled.
- The will to act safely. Technical and organizational factors are important with respect to workers’ readiness to behave in ways that will ensure workplace safety, but social and cultural factors are at least equally important. Risks will arise if, for example, safe conduct is difficult or time-consuming, or if it is not desired by management or colleagues, or is not appreciated by them. Management must be clearly interested in safety, taking steps to prioritize it and displaying a positive attitude towards the need for safe conduct.
Information on the causes of accidents serves the following purposes:
- It can demonstrate where something is wrong and what needs to be changed.
- It indicates the types of harmful factors that cause accidents (or near accidents) and also describes the situations that result in damage and injuries.
- It identifies and describes the underlying circumstances that determine the presence of potential hazards and risky situations and that will result in optimum safety by their being altered or eliminated.
Information of a general sort can be obtained by a thorough analysis of the damage or injuries and the circumstances under which they occurred. Information obtained from other similar accidents may point out more general factors of importance, thus disclosing less immediately visible causal relationships. However, as very detailed and specific information can be obtained by analysing an individual accident, this information may help uncover the specific circumstances which should be addressed. Often, analysis of the individual accident will provide information which it is not possible to obtain from the general analysis, whereas the general analysis may point out factors which the specific analysis does not elucidate. Data from both of these kinds of analyses are important to help disclose obvious and direct causal relations at the individual level.
Analysis of Individual Accidents
Analysis of individual accidents has two primary purposes:
First, it can be used to determine the cause of an accident and the specific work factors that contributed to it. Following analysis, one can assess the extent to which the risk has been recognized. One may also decide upon technical and organizational safety measures and the degree to which more job experience might have diminished the risk. Furthermore, a clearer view is gained of the possible actions that might have been taken to avoid the risk, and the motivation that a worker must have to take these actions.
Second, one can gain knowledge which may be used for analyses of many similar accidents at both the enterprise level and at more comprehensive (e.g., organization-wide or national) levels. In this connection, it is important to assemble information such as the following:
- the identity of the workplace and the work itself (that is, information relating to the sector or the trade in which the workplace is positioned), and the work processes and the technology that characterize the work
- the nature and the seriousness of the accident
- factors causing the accident, such as exposure sources, the way in which the accident occurred and the specific working situation causing the accident
- general conditions at the workplace and the working situation (comprising the factors mentioned in the foregoing paragraph).
Types of Analyses
There are five primary types of analyses of accidents, each having a distinct purpose:
- Analyses and identification of where and which types of accidents occur. The goal is to determine the incidence of the injuries, as associated, for example, with sectors, trade groups, enterprises, work processes and types of technology.
- Analyses with respect to monitoring developments in the incidence of accidents. The purpose is to be warned of changes, both positive and negative. Measuring the effect of preventive initiatives may be the result of such analyses, and increases in new types of accidents within a specified area will constitute warning of new risk elements.
- Analyses to prioritize initiatives that call for high degrees of risk measurement, which in turn involve calculating the frequency and seriousness of accidents. The goal is to establish a basis for prioritization to determine where it is more important to carry out preventive measures than elsewhere.
- Analyses to determine how the accidents occurred and, especially, to establish both direct and underlying causes. This information is then applied to the selection, elaboration and implementation of concrete corrective action and preventive initiatives.
- Analyses for elucidation of special areas which have otherwise attracted attention (a sort of rediscovery or control analyses). Examples include analyses of incidences of a special injury risk or the discovery of a hitherto unrecognized risk identified in the course of examining an already known risk.
These types of analyses can be carried out at several different levels, ranging from the individual enterprise to the national level. Analyses at several levels will be necessary for preventive measures. Analyses involving general accident incident rates, monitoring, warning and prioritization will be carried out chiefly at higher levels, whereas analyses describing direct and underlying accident causes will be conducted at lower levels. The results of the analyses will accordingly be more specific at the individual level and more general at the higher level.
Phases of the Analysis
Irrespective of the level from which an analysis starts, it will usually have the following phases:
- identification of where the accidents occur at the general level selected
- specification of where the accidents occur at a more specific level within the general level
- determination of goals in view of the incidence (or frequency) and seriousness of the accidents
- description of exposure sources or other harmful factors—that is, the direct causes of damage and injury
- examination of the underlying causal relation and causal development.
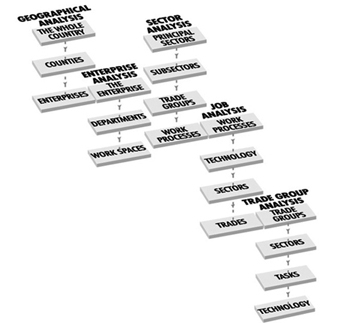
Examples of different levels of analysis are given in figure 1.
Figure 1. Different levels of accident analysis
Summary
Identification of accidents nationwide may provide knowledge of the sectors, trade groups, technologies and working processes within which damages and injuries occur. The goal is solely to identify where the accidents occurred. Measurement of accidents by frequency and seriousness partly establishes where something is wrong in particular and partly indicates where the risk has changed.
The type of workplace risk is established by descriptions of the types of accidents that take place and the way in which they arise within the individual workplace areas. In this way, knowledge is obtained of the exposure sources and other harmful factors present in the workplace in the event that preventive measures—attention to safety conditions, awareness of risk, providing opportunity for action and the appeal to the workers’ will—have proved insufficient to avert the accident.
Identification, measurement and description of accidents together provide the basis for what is to be done and who is to do it in order to reduce the risk. If, for example, specific exposure sources can be linked to specific technologies, it will help determine what special safety measures are necessary to control the risk. This information may also be used to influence manufacturers and suppliers associated with the technology in question. If it can be demonstrated that frequent and very serious accidents occur in connection with specific processes, the attempt may be made to adjust the nature of the equipment, machinery, operations or work procedures that are associated with these processes. Unfortunately, a typical feature of such initiatives and adjustments is that an almost unambiguous monocausal correlation between accidents and causes is required, and this is available for only a few cases.
Analyses of accidents within an enterprise may also be carried out from a general to a more specific level. However, the problem often is to assemble a sufficiently extensive database. If accident injury data covering a number of years are gathered at an enterprise (including information regarding minor injuries and near accidents), it will be possible to establish a useful database even at this level. The overall analysis of the enterprise will show whether there are special problems in specific sections of the enterprise, or in connection with specific tasks or with the use of specific types of technology. The detailed analysis will then show what is wrong and thus lead to an evaluation of preventive measures.
If workers’ conduct within a sector, trade group or enterprise, or the conduct of an individual is to be influenced, knowledge regarding many accidents is required in order to increase workers’ awareness. At the same time, information must be made available about the factors which increase the probability of accidents and about known possibilities of action that may minimize the risk of damage or injury. At this point, safety becomes a matter of motivating those responsible for people’s conduct at the level of a given sector, an industrial organization, a trade organization, the employer or the employee.
Introduction
According to International Labour Office statistics, 120 million occupational accidents occur annually at workplaces worldwide. Of these, 210,000 are fatal accidents. Every day, more than 500 men or women do not come home because they were killed by accidents at work. These are dramatic numbers which draw fairly little public attention. Considering the fact that accidents take a considerable economic toll from nations, companies and individuals, accidents do not get much publicity.
Fortunately there are people working with a sense of purpose, often behind the scenes, towards understanding and managing safety and accident prevention better, and their efforts have not been wasted. Our understanding of accident prevention and safety is on a far higher level than ever before. Many world-class researchers and safety practitioners share this new knowledge with us through their articles in this Encyclopaedia. During the past twenty decades, knowledge about accidents has evolved considerably. We have left behind the simplistic model of dividing behaviour and conditions into two categories: safe or unsafe. The rigid belief that any activity can be placed into either category has been put aside as more sophisticated systemic models have been developed and proven effective in managing safety.
The important observation is that two safe conditions which by themselves are safe, may not be safe together. Workers are the connecting link, as their behaviour changes according to the environment and their physical surroundings. As an example, power saws caused many accidents when they came into use in the 1960s due to a hazard known as “kickback”, which takes the operator by surprise when the chain-saw blades hit a branch, knot or harder point in wood. Kickback killed and injured hundreds of people before a guard was invented to protect the operator. When Sweden implemented regulations requiring the kickback guard, the number of power saw injuries went down from 2,600 in 1971 to 1,700 in 1972. This was a major breakthrough in power saw accident prevention.
Every user of power saws knows from personal experience that this noisy, vibrating and obviously sharp cutting tool appears to be very dangerous to use, and the beginner operator is very cautious. However, after hours of experience operators lose their sense of any hazard and start handling the saw less carefully. The kickback guard may produce a similar effect. Operators who know kickback is possible try to avoid it. When operators know that there is a mechanical device preventing the saw from hurting them in event of kickback, they become less cautious. In another forestry industry chain-saw example, studies have shown that leg protection makes workers less careful and they expose themselves more often to kickbacks, because they believe they are protected.
Despite the fact that kickback protection has helped prevent injuries, the mechanism is not straightforward. Even if these protective arrangements have been successful, in the final analysis their effects do not have a linear relationship with safety. Two safe conditions, kickback guard and leg protection, do not double the safety. The normal arithmetic of one plus one equals two (1 + 1 = 2), does not apply in this case, as one plus one makes less than two. Fortunately, one plus one (1 + 1) makes more than zero in some cases. In other cases, however, the sum may even be negative.
These are phenomena which safety practitioners have started to understand better than before. The simple division of behaviours and conditions into safe and unsafe does not lead very far toward prevention. The credit for progress has to be given to systems management. After understanding that humans, their tasks, their equipment and the environment make up a dynamic system, we have made considerable progress towards more effective accident prevention. The following examples demonstrate the dynamic nature of people and work. If one component is changed, the others do not remain the same, and the ultimate safety effect is hard to estimate in advance.
In aviation and in other highly engineered and automated systems, we have seen that increased automation may not necessarily result in improved safety. For example, operators may not get enough practice to maintain their skills in a highly automated system. When they then are required to intervene, they may not have the necessary competence or ability.
Some paper manufacturers have indicated that younger employees do not understand the functions of a paper machine as well as the older employees. The older employees have operated non-automated machines, and they have seen how these work. The new automated machines are operated from control rooms through computer keyboards and screens. The operators do not know the exact location of each component of the machines they operate. Therefore they may bring a component into a state which, for example, causes a hazard to the maintenance people in the vicinity. A technical improvement in the machinery or controls without simultaneous improvement in operators’ skills, knowledge and values may not result in improved safety.
Accident prevention has been traditionally based on learning from accidents and near accidents (near misses). By investigating every incident, we learn about causes and can take actions towards mitigating or removing the causes. The problem is that we have not been able to develop, in the absence of sufficiently good theories, investigation methods which would bring up all the relevant factors for prevention. An investigation may give a fairly good picture about the causes. However, this picture is usually relevant only for the specific case investigated. There may be conditions and factors which contributed to the accident whose connections the investigators do not recognize or understand. Generalizing from one accident to other situations bears a degree of risk.
The good news is that we have made considerable progress in the area of predictive safety management. A number of techniques have been developed and have become routine for industrial safety and risk analysis. These techniques allow us to study industrial production plants systematically for the identification of potential hazards and to institute appropriate action before anything happens.
The chemical and petrochemical industries have shown leadership in this area worldwide. As a result of major catastrophes, such as Bhopal and Chernobyl, the use of the new predictive techniques has increased. Remarkable progress has been made since the mid-1970s in the area of safety. Many governments have also been leaders in making safety analysis mandatory. Sweden, Finland, Japan and the Federal Republic of Germany have all reduced fatal occupational accidents by 60 to 70% during this time. Many other countries show similar progress. Now, the challenge is to transfer our knowledge from research into practical applications and further improve our preventive efforts.
One of the new steps in safety management is the notion of safety culture. It may be a difficult concept, since culture is not a visible entity. It is an abstract concept prevailing within an organization or society. There are no direct ways of adjusting it. Safety culture is, however, a crucial concept for understanding the possibilities of prevention. One of the goals of this edition is to explore this new concept.
This new edition of the Encyclopaedia provides a comprehensive review of accident prevention theories and models in order to develop better design and more effective preventive strategies. It is possible to prevent occupational accidents. We do not need to tolerate this unnecessary toll to our well-being and economy.
Respiratory Effects and other Disease Patterns in the Textile Industry
For nearly 300 years, work in the textile industry has been recognized as hazardous. Ramazzini (1964), in the early 18th century, described a peculiar form of asthma among those who card flax and hemp. The “foul and poisonous dust” which he observed “makes the workmen cough incessantly and by degrees brings on asthmatic troubles”. That such symptoms did in fact occur in the early textile industry was illustrated by Bouhuys and colleagues (1973) in physiological studies at Philipsburg Manor (a restoration project of life in the early Dutch colonies in North Tarrytown, New York, in the United States). While numerous authors throughout the 19th and early 20th centuries in Europe described the respiratory manifestations of work-related illness in textile mills with increasing frequency, the disease remained essentially unrecognized in the United States until preliminary studies in the middle of the 20th century under the direction of Richard Schilling (1981) indicated that, despite pronouncements to the contrary by both industry and government, characteristic byssinosis did occur (American Textile Reporter 1969; Britten, Bloomfield and Goddard 1933; DOL 1945). Many subsequent investigations have shown that textile workers around the world are affected by their work environment.
Historical Overview of Clinical Syndromes in the Textile Industry
Work in the textile industry has been associated with many symptoms involving the respiratory tract, but by far the most prevalent and the most characteristic are those of byssinosis. Many but not all vegetable fibres when processed to make textiles may cause byssinosis, as discussed in the chapter Respiratory system. The distinguishing feature of the clinical history in byssinosis is its relationship to the work week. The worker, typically after having worked a number of years in the industry, describes chest tightness beginning on Monday (or the first day of the work week) afternoons. The tightness subsides that evening and the worker is well for the remainder of the week, only to re-experience the symptoms on the following Monday. Such Monday dyspnoea may continue unchanged for years or may progress, with symptoms occurring on subsequent workdays, until chest tightness is present throughout the work week, and ultimately also while away from work on weekends and during vacation. When the symptoms become permanent, dyspnoea is described as effort dependent. At this stage a non-productive cough may be present. Monday symptoms are accompanied by across-shift decreases in lung function, which may be present on other workdays even in the absence of symptoms, but the physiological changes are not so marked (Bouhuys 1974; Schilling 1956). Baseline (Monday pre-shift) lung function deteriorates as the disease progresses. The characteristic respiratory and physiological changes seen in byssinotic workers have been standardized into a series of grades (see table 1) which currently form the basis of most clinical and epidemiological investigations. Symptoms other than chest tightness, particularly cough and bronchitis, are frequent among textile workers. These symptoms probably represent variants of the airway irritation brought on by dust inhalation.
Table 1. Grades of byssinosis
|
Grade 0 |
Normal—no symptoms of chest tightness or cough |
|
Grade 1/2 |
Occasional chest tightness or cough or both on first day of the working week |
|
Grade 1 |
Chest tightness on every first day of the working week |
|
Grade 2 |
Chest tightness on every first day and other days of the working week |
|
Grade 3 |
Grade 2 symptoms, accompanied by evidence of permanent incapacity from reduced ventilatory capacity |
Source: Bouhuys 1974.
There is unfortunately no simple test capable of establishing the diagnosis of byssinosis. The diagnosis must be made on the basis of worker symptoms and signs as well as on the physician’s awareness of and familiarity with the clinical and industrial settings in which the disease is likely to occur. Lung function data, although not always specific, may be very helpful in establishing the diagnosis and in characterizing the degree of impairment.
In addition to classic byssinosis, textile workers are subject to several other symptom complexes; in general, these are associated with fever and not related to the initial day of the work week.
Mill fever (cotton fever, hemp fever) is associated with fever, cough, chills and rhinitis which occurs with the worker’s first contact with the mill or with return after a prolonged absence. Chest tightness does not appear to be associated with this syndrome. The frequency of these findings among workers is quite variable, from as low as 5% of the workers (Schilling 1956) to a majority of those employed (Uragoda 1977; Doig 1949; Harris et al. 1972). Characteristically, symptoms subside after a few days despite continued exposure in the mill. Endotoxin in vegetable dust is thought to be a causative agent. Mill fever has been associated with an entity now commonly described in industries using organic materials, the organic dust toxic syndrome (ODTS), which is discussed in the chapter Respiratory system.
“Weaver’s cough” is primarily an asthmatic condition characteristically associated with fever; it occurs in both new and senior workers. The symptoms (unlike mill fever) can persist for months. The syndrome has been associated with materials used to treat the yarn—for example, tamarind seed powder (Murray, Dingwall-Fordyce and Lane 1957) and locust bean gum (Vigliani, Parmeggiani and Sassi 1954).
The third non-byssinotic syndrome associated with textile processing is “mattress maker’s fever” (Neal, Schneiter and Caminita 1942). The name refers to the context in which the disease was described when it was characterized by an acute outbreak of fever and other constitutional symptoms, including gastrointestinal symptoms and retrosternal discomfort in workers who were using low-grade cotton. The outbreak was attributed to contamination of the cotton with Aerobacter cloacae.
In general, these febrile syndromes are thought to be clinically distinct from byssinosis. For example, in studies of 528 cotton workers by Schilling (1956), 38 had a history of mill fever. The prevalence of mill fever among workers with “classic” byssinosis was 10% (14/134), compared to 6% (24/394) among workers who did not have byssinosis. The differences were not statistically significant.
Chronic bronchitis, as defined by medical history, is very prevalent among textile workers, and in particular among non-smoking textile workers. This finding is not surprising since the most characteristic histological feature of chronic bronchitis is mucous gland hyperplasia (Edwards et al. 1975; Moran 1983). Chronic bronchitis symptomatology should be carefully distinguished from classic byssinosis symptoms, although byssinotic and bronchitic complaints frequently overlap and in textile workers are probably different pathophysiological manifestations of the same airway inflammation.
Pathology studies of textile workers are limited, but reports have shown a consistent pattern of disease involving the larger airways (Edwards et al. 1975; Rooke 1981a; Moran 1983) but no evidence suggestive of destruction of lung parenchyma (e.g., emphysema) (Moran 1983).
Clinical Course of Byssinosis
Acute versus chronic disease
Implicit in the grading system given in table 1 is a progression from acute “Monday symptoms” to chronic and essentially irreversible respiratory disease in workers with byssinosis. That such a progression occurs has been suggested in cross-sectional data beginning with the early study of Lancashire, United Kingdom, cotton workers, which found a shift toward higher byssinosis grades with increasing exposure (Schilling 1956). Similar findings have since been reported by others (Molyneux and Tombleson 1970). Moreover, this progression may begin relatively soon after employment (e.g., within the first few years) (Mustafa, Bos and Lakha 1979).
Cross-sectional data have also shown that other chronic respiratory symptoms and symptom complexes, such as wheeze or chronic bronchitis, are much more prevalent in older cotton textile workers than in similar control populations (Bouhuys et al. 1977; Bouhuys, Beck and Schoenberg 1979). In all cases the cotton textile workers have displayed more chronic bronchitis than the controls, even when adjusting for sex and smoking status.
Grade 3 byssinosis indicates that, in addition to symptoms, textile workers demonstrate changes in respiratory function. The progression from early byssinosis (grade 1) to late byssinosis (grade 3) is suggested by the association of lung function loss with the higher grades of byssinosis in cross-sectional studies of textile workers. Several of these cross-sectional studies have given support to the concept that across-shift changes in lung function (which correlate with the acute findings of chest tightness) are related to chronic irreversible changes.
Underlying the association between acute and chronic disease in textile workers is a dose-response relationship in acute symptoms, which was first documented by Roach and Schilling in a study reported in 1960. These authors found a strong linear relation between biological response and total dust concentrations in the workplace. Based on their findings they recommended 1 mg/m3 gross dust as a reasonably safe level of exposure. This finding was later adopted by the ACGIH and was, until the late 1970s, the value used as the threshold limit value (TLV) for cotton dust in the United States. Subsequent observations demonstrated that the fine dust fraction (<7 μm) accounted for practically all of the prevalence of byssinosis (Molyneux and Tombleson 1970; Mckerrow and Schilling 1961; McKerrow et al. 1962; Wood and Roach 1964). A 1973 study by Merchant and colleagues of respiratory symptoms and lung function in 1,260 cotton, 803 blend (cotton-synthetic) and 904 synthetic-wool workers was undertaken in 22 textile manufacturing plants in North Carolina (United States). The study confirmed the linear association between byssinosis prevalence (as well as decrements in lung function) and concentrations of lint-free dust.
The validation of changes in respiratory function suggested by cross-sectional studies has come from a number of longitudinal investigations which complement and extend the results of the earlier studies. These studies have highlighted the accelerated loss of lung function in cotton textile workers as well as the high incidence of new symptoms.
In a series of investigations involving several thousand mill workers examined in the late 1960s over a 5-year span of time, Fox and colleagues (1973a; 1973b) found an increase in byssinosis rates which correlated with years of exposure, as well as a sevenfold greater annual decrease in forced expired volume in 1 second (FEV1) (as a per cent of predicted) when compared to controls.
A unique study of chronic lung disease in textile workers was initiated in the early 1970s by the late Arend Bouhuys (Bouhuys et al. 1977). The study was novel because it included both active and retired workers. These textile workers from Columbia, South Carolina, in the United States, worked in one of four local mills. The selection of the cohort was described in the original cross-sectional analysis. The original group of workers consisted of 692 individuals, but the analysis was restricted to 646 whites aged 45 years or older as of 1973. These individuals had worked an average of 35 years in the mills. The control group for the cross-sectional results consisted of whites aged 45 years and older from three communities studied cross-sectionally: Ansonia and Lebanon, Connecticut, and Winnsboro, South Carolina. In spite of geographic, socio-economic and other differences, the community residents did not differ in lung function from textile workers who held the least dusty jobs. Since no differences in lung function or respiratory symptoms were noted between the three communities, only Lebanon, Connecticut, which was studied in 1972 and 1978, was used as the control for the longitudinal study of textile workers studied in 1973 and in 1979 (Beck, Doyle and Schachter 1981; Beck, Doyle and Schachter 1982).
Both symptoms and lung function have been extensively reviewed. In the prospective study it was determined that the incidence rates for seven respiratory symptoms or symptom complexes (including byssinosis) were higher in textile workers than in controls, even when controlling for smoking (Beck, Maunder and Schachter 1984). When textile workers were separated into active and retired workers, it was noted that those workers retiring during the course of the study had the highest incidence rates of symptoms. These findings suggested that not only were active workers at risk for impairing respiratory symptoms but retired workers, presumably because of their irreversible lung damage, were at continuing risk.
In this cohort, loss of lung function was measured over a 6-year period. The mean decline for male and female textile workers (42 ml/yr and 30 ml/yr, respectively) was significantly greater than the decline in male and female controls (27 ml/yr and 15 ml/yr). When classified by smoking status, the cotton textile workers in general still had greater losses in FEV1 than did the controls.
Many authors have previously raised the potential confounding issue of cigarette smoking. Because many textile workers are cigarette smokers, it has been claimed that the chronic lung disease associated with exposure to textile dust can in large part be attributed to cigarette smoking. Using the Columbia textile-worker population, this question was answered in two ways. One study by Beck, Maunder and Schachter (1984) used a two-way analysis of variance for all lung function measurements and demonstrated that the effects of cotton dust and smoking on lung function were additive—that is, the amount of lung function loss due to one factor (smoking or cotton dust exposure) was not changed by the presence or absence of the other factor. For FVC and FEV1 the effects were similar in magnitude (average smoking history 56 pack-years, average mill exposure 35 years). In a related study, Schachter et al. (1989) demonstrated that using a parameter which described the shape of the maximum expiratory flow volume curve, angle beta, distinct patterns of lung function abnormalities could be shown for a smoking effect and for a cotton effect, similar to conclusions reached by Merchant earlier.
Mortality
Studies of cotton-dust exposure on mortality have not consistently demonstrated an effect. Review of experience in the late 19th and early 20th centuries in the United Kingdom suggested an excess of cardiovascular mortality in older textile workers (Schilling and Goodman 1951). By contrast, review of the experience in New England mill towns from late in the 19th century failed to demonstrate excess mortality (Arlidge 1892). Similar negative findings were observed by Henderson and Enterline (1973) in a study of workers who had been employed in Georgia mills from 1938 to 1951. By contrast, a study by Dubrow and Gute (1988) of male textile workers in Rhode Island who died during the period 1968 to 1978, showed a significant increase in proportionate mortality rate (PMR) for non-malignant respiratory disease. The elevations in PMR were consistent with increased dust exposure: carding, lapping and combing operatives had higher PMRs than did other workers in the textile industry. An interesting finding of this and other studies (Dubrow and Gute 1988; Merchant and Ortmeyer 1981) is the low mortality from lung cancer among these workers, a finding that has been used to argue that smoking is not a major cause of mortality in these groups.
Observations from a cohort in South Carolina suggest that chronic lung disease is indeed a major cause (or predisposing factor) for mortality, since among those workers aged 45 to 64 who died during a 6-year follow-up, lung function measured as residual FEV1 (observed-to-predicted) showed marked impairment at the initial study (mean RFEV1 = -0.9l) in male non-smokers who died during the 6-year follow-up (Beck et al. 1981). It may well be that the effect of mill exposure on mortality has been obscured by a selection effect (healthy worker effect). Finally, in terms of mortality, Rooke (1981b) estimated that of the average 121 deaths he observed annually among disabled workers, 39 had died as a result of byssinosis.
Increased Control, Decreased Disease
Recent surveys from the United Kingdom and the United States suggest that the prevalence as well as the pattern of lung disease seen in textile workers has been affected by the implementation of stricter air-quality standards in the mills of these countries. In 1996, Fishwick and his colleagues, for example, describe a cross-sectional study of 1,057 textile spinning operatives in 11 spinning mills in Lancashire. Ninety-seven per cent of the workforce was tested; the majority (713) worked with cotton and the remainder with synthetic fibre). Byssinosis was documented in only 3.5% of the operatives and chronic bronchitis in 5.3%. FEV1, however, was reduced in workers exposed to high dust concentrations. These prevalences are much reduced from those reported in earlier surveys of these mills. This low prevalence of byssinosis and related bronchitis appears to follow the trend of decreasing dust levels in the United Kingdom. Both smoking habits and cotton dust exposures contributed to the lung function loss in this cohort.
In the United States, results of a 5-year prospective study of workers in 9 mills (6 cotton and 3 synthetic) was conducted between 1982 and 1987 by Glindmeyer and colleagues (1991; 1994), where 1,817 mill workers who were employed exclusively in cotton yarn manufacturing, slashing and weaving or in synthetics were studied. Overall, fewer than 2% of these workers were found to have byssinotic complaints. Nevertheless, workers in yarn manufacturing exhibited a greater annual loss of lung function than workers in slashing and weaving. The yarn workers exhibited dose-related lung function loss which was also associated with the grade of cotton used. These mills were in compliance with then current OSHA standards, and the mean airborne lint-free respirable cotton dust concentrations averaged over 8 hours were 196 mg/m3 in yarn manufacture and 455 mg/m3 in slashing and weaving. The authors (1994) related across-shift changes (the objective lung function equivalent of byssinotic symptoms) with longitudinal declines in lung function. Across-shift changes were found to be significant predictors of longitudinal changes.
While textile manufacture in the developed world appears now to be associated with less prevalent and less severe disease, this is not the case for developing countries. High prevalences of byssinosis can still be found worldwide, particularly where governmental standards are lax or non-existent. In his recent literature survey, Parikh (1992) noted byssinosis prevalences well above 20% in such countries as India, Cameroon, Ethiopia, Sudan and Egypt. In a study by Zuskin et al. (1991), 66 cotton textile workers were followed in a mill in Croatia where mean respirable dust concentrations remained at 1.0 mg/m3. Byssinosis prevalences doubled, and annual declines in lung function were nearly twice those estimated from prediction equations for healthy non-smokers.
Non-Respiratory Disorders Associated with Work in the Textile Industry
In addition to the well-characterized respiratory syndromes which can affect textile workers, there are a number of risks that have been associated with working conditions and hazardous products in this industry.
Oncongenesis has been associated with work in the textile industry. A number of early studies indicate a high incidence of colorectal cancer among workers in synthetic textile mills (Vobecky et al. 1979; Vobecky, Devroede and Caro 1984). A retrospective study of synthetic textile mills by Goldberg and Theriault (1994a) suggested an association with length of employment in the polypropylene and cellulose triacetate extrusion units. Other associations with neoplastic diseases were noted by these authors but were felt to be “not persuasive” (1994b).
Exposure to azo dyes have been associated with bladder cancer in numerous industries. Siemiatycki and colleagues (1994) found a weak association between bladder cancer and work with acrylic fibres and polyethylene. In particular, workers who dye these textiles were found to be at an increased risk. Long-term workers in this industry presented a 10-fold excess risk (marginal statistical significance) for bladder cancer. Similar findings have been reported by other authors, although negative studies are also noted (Anthony and Thomas 1970; Steenland, Burnett and Osorio 1987; Silverman et al. 1989).
Repetitive-motion trauma is a recognized hazard in the textile industry related to high-speed manufacturing equipment (Thomas 1991). A description of carpal tunnel syndrome (Forst and Hryhorczuk 1988) in a seamstress working with an electrical sewing machine illustrates the pathogenesis of such disorders. A review of hand injuries referred to the Regional Plastic Surgery Unit treating Yorkshire wool workers between 1965 and 1984 revealed that while there was a fivefold decrease in employment in this industry, the yearly incidence of hand injuries remained constant, indicating increased risk in this population (Myles and Roberts 1985).
Hepatic toxicity in textile workers has been reported by Redlich and colleagues (1988) as a result of exposure to the solvent dimethylformanide in a fabric-coating factory. This toxicity was recognized in the context of an “outbreak” of liver disease in a New Haven, Connecticut, factory that produces polyurethane-coated fabrics.
Carbon disulphide (CS2) is an organic compound used in the preparation of synthetic textiles which has been associated with increased mortality from ischemic heart disease (Hernberg, Partanen and Nordman 1970; Sweetnam, Taylor and Elwood 1986). This may relate to its effects on blood lipids and diastolic blood pressure (Eyeland et al. 1992). Additionally, this agent has been associated with peripheral neurotoxicity, injury to sensory organs and disturbances in hormonal and reproductive function. It is generally believed that such toxicity results from long-term exposure to concentrations in excess of 10 to 20 ppm (Riihimaki et al. 1992).
Allergic responses to reactive dyes including eczema, uticaria and asthma have been reported in textile-dyeing workers (Estlander 1988; Sadhro, Duhra and Foulds 1989; Seidenari, Mauzini and Danese 1991).
Infertility in men and women has been described as a result of exposures in the textile industry (Rachootin and Olsen 1983; Buiatti et al. 1984).
Hand-Woven and Hand-Tufted Carpets
Adapted from 3rd edition, Encyclopaedia of Occupational Health and Safety.
All “oriental” carpets are hand woven. Many are made in family workplaces, with all the members of the household, often including very small children, working long days and often into the night on the loom. In some cases it is only a part-time occupation of the family, and in some areas the carpet weaving has been moved from the home into factories that are usually small.
Processes
The processes involved in the manufacture of a carpet are: yarn preparation, consisting of wool sorting, washing, spinning and dyeing; designing; and the actual weaving.
Yarn preparation
In some cases the yarn is received at the weaving place already spun and dyed. In others, the raw fibre, usually wool, is prepared, spun and dyed at the weaving place. After the sorting of the wool fibre into grades, usually done by women sitting on the floor, it is washed and spun by hand. The dyeing is carried out in open vessels using mostly aniline-based or alizarine dyestuffs; natural dyestuffs are no longer being used.
Designing and weaving
In handicraft weaving (or tribal weaving, as it is sometimes called), the designs are traditional, and no new designs need to be made. In industrial establishments employing a number of workers, however, there may be a designer who first sketches the design of a new carpet on a sheet of paper and then transfers it in colours onto squared paper from which the weaver can ascertain the number and arrangement of the various knots to be woven into the carpet.
In most cases the loom consists of two horizontal wooden rollers supported on uprights, one about 10 to 30 cm above floor level and the other about 3 m above it. The warp yarn passes from the top roller to the bottom roller in a vertical plane. There is usually one weaver working at the loom, but for wide carpets there may be as many as six weavers working side by side. In about 50% of the cases, the weavers squat on the floor in front of the bottom roller. In other cases, they may have a narrow horizontal plank on which to sit, which is raised up to 4 m above the floor as weaving proceeds. The weaver has to tie short pieces of woollen or silk yarn into knots around pairs of warp threads and then move the thread by hand across the whole length of the carpet. Picks of weft are beaten up into the fibre of the carpet by means of a beater or hand comb. The tufts of yarn protruding from the fibre are trimmed or cut down by scissors.
As the carpet is woven, it is usually wound onto the lower roller, which increases its diameter. When the workers squat on the floor, the position of the lower roller prevents them from stretching their legs, and as the diameter of the rolled-up carpet increases, they have to sit further back but must still lean forward to reach the position in which they tie in the knots of yarn (see figure 1). This is avoided when the weavers sit or squat on the plank, which may be raised as high as 4 m above the floor, but there may still not be enough room for their legs, and they are often forced into uncomfortable positions. In some instances, however, the weaver is provided with a back rest and a pillow (in effect, a legless chair), which may be moved horizontally along the plank as the work progresses. Recently, improved types of elevated looms have been developed that allow the weaver to sit on a chair, with ample room for his or her legs.
Figure 1. Squat loom
In some parts of the Islamic Republic of Iran, the warp in the carpet loom is horizontal instead of being vertical, and the worker sits on the carpet itself whilst working; this makes the task even more difficult.
Hazards of Carpet Weaving
As a largely cottage industry, carpet weaving is fraught with the hazards imposed by impoverished homes with small, crowded rooms that have poor lighting and inadequate ventilation. The equipment and processes are passed along from generation to generation with little or no opportunity for the education and training that might spark a break with the traditional methods. Carpet weavers are subject to skeletal deformations, eyesight disorders and mechanical and toxic hazards.
Skeletal deformation
The squatting position that the weavers must occupy on the old type of loom, and the need for them to lean forward to reach the place into which they knot the yarn, may, over time, lead to some very serious skeletal problems. These are often compounded by the nutritional deficiencies associated with poverty. Especially among those who start as young children, the legs may become deformed (genu valgum), or a crippling arthritis of the knee may develop. The constriction of the pelvis that sometimes occurs in females may make it necessary for them to have a Cesarean delivery when giving birth. Lateral curvature of the spinal column (scoliosis) and lordosis are also common maladies.
Vision disorders
The constant close focus on the point of weaving or knotting may cause considerable eyestrain, particularly when the lighting is inadequate. It should be noted that electric lighting is not available in many home workplaces, and the work, which is often continued into the night, must be performed by the light of oil lamps. There have been cases of almost total blindness occurring after only about 12 years of employment at this work.
Hand and finger disorders
The constant tying of small knots and the threading of the weft yarn through the warp threads may result in swollen finger joints, arthritis and neuralgia causing permanent disabilities of the fingers.
Stress
The high degree of skill and constant attention to detail over long hours are potent psychosocial stressors, which may be compounded by exploitation and harsh discipline. Children are often “robbed of their childhood”, while adults, who often lack the social contacts essential for emotional balance, may develop nervous illness manifested by trembling of the hands (which may hamper their work performance) and sometimes mental troubles.
Mechanical hazards
As no power machinery is used, there are practically no mechanical hazards. If the looms are not properly maintained, the wooden lever tensioning the warp may break and strike the weaver as it falls. This hazard may be avoided by using special thread tensioning gears.
Chemical hazards
The dyestuffs used, particularly if they contain potassium or sodium bichromate, may cause skin infections or dermatitis. There is also the risk from the use of ammonia, strong acids and alkalis. Lead pigments are sometimes used by designers, and there have been cases of lead poisoning due to their practice of smoothing the tip of the paintbrush by placing it between the lips; lead pigments should be replaced by non-toxic colours.
Biological hazards
There is a danger of anthrax infection from contaminated raw wool from areas where the bacillus is endemic. The appropriate governmental authority should ensure that such wool is properly sterilized before it is delivered to any workshops or factories.
Preventive Measures
The sorting of the raw material—wool, camel hair, goat hair and so on—should be done over a metal grid fitted with exhaust ventilation to draw any dust into a dust collector located outside the workplace.
The rooms in which the wool-washing and dyeing processes take place should be adequately ventilated, and the workers provided with rubber gloves and waterproof aprons. All waste liquors should be neutralized before being discharged into waterways or sewers.
Good lighting is required for the designing room and for weaving work. As noted above, inadequate light is a serious problem where there is no electricity and when the work is continued after sundown.
Perhaps the most important mechanical improvement would be mechanisms that raise the lower roller of the loom. This would obviate the necessity of weavers having to squat on the floor in an unhealthy and uncomfortable fashion and allow them to sit in a comfortable chair. Such an ergonomic improvement will not only improve the health of the workers but, once adopted, will increase their efficiency and productivity.
The workrooms should be kept clean and well ventilated, and properly boarded or covered floors substituted for earth floors. Adequate heating is required during cold weather. Manual manipulation of the warp places great strain on the fingers and may cause arthritis; wherever possible, hooked knives should be used for holding and weaving operations. Pre-employment and annual medical examinations of all workers are highly desirable.
Hand-tufted Carpets
The manufacture of carpets by the tying of knots of yarn by hand is a very slow process. The number of knots varies from 2 to 360 per square centimetre according to the quality of the carpet. A very large carpet with an intricate design may take over a year to make and involve the tying of hundreds of thousands of knots.
Hand tufting is an alternative method of rug manufacture. It uses a special kind of hand tool fitted with a needle through which the yarn is threaded. A sheet of coarse cotton cloth on which the design of the carpet has been traced is suspended vertically, and when the weaver places the tool against the cloth and presses a button, the needle is forced through the cloth and retracts, leaving a loop of yarn about 10 mm deep on the reverse side. The tool is moved horizontally about 2 or 3 mm, leaving a loop on the face of the cloth, and the trigger button is pressed again to form another loop on the reverse side. With acquired dexterity, as many as 30 loops on each side can be made in 1 minute. Depending on the design, the weaver has to stop from time to time to change the colour of yarn as called for in different parts of the pattern. When the looping operation has been finished, the carpet is taken down and placed reverse side up on the floor. A rubber solution is applied to the back and a covering or backing of stout jute canvas placed over it. The carpet is then placed face upwards and the protruding loops of yarn are trimmed by portable electric clippers. In some cases the design of the carpet is made by cutting or trimming the loops to varying depths.
Hazards in this type of carpet making are considerably less than in the manufacture of hand-knotted carpets. The operator usually sits on a plank in front of the canvas and has plenty of leg room. The plank is raised as the work proceeds. The weaver would be made more comfortable by provision of a backrest and a cushioned seat which could be moved horizontally along the plank as work proceeds. There is less visual strain, and no hand or finger movements that are likely to cause trouble.
The rubber solution used for this carpet usually contains a solvent which is both toxic and highly flammable. The backing process should be carried out in a separate workroom with good exhaust ventilation, at least two fire exits, and with no open flames or lights. Any electrical connections and equipment in this room should be certified as meeting sparkproof/flameproof standards. No more than a minimum amount of the flammable solution should be kept in this room, and appropriate fire extinguishers should be provided. A fire-resistant storage facility for the flammable solutions should not be situated inside any occupied building, but preferably in an open yard.
Legislation
In most countries, the general provisions of factory legislation cover the necessary standards required for the safety and health of workers in this industry. They may not be applicable, however, to family undertakings and/or home work, and they are difficult to enforce in the scattered small enterprises which, in the aggregate, employ many workers. The industry is notorious for the exploitation of its workers and for its use of child labour, often in defiance of existing regulations. A nascent worldwide trend (mid-1990s) among purchasers of hand-woven and tufted carpets to refrain from buying products produced by illegal or overly exploited workers will, it is hoped by many, eliminate such servitude.
Carpets and Rugs
The Carpet and Rug Institute
Hand-woven or hand-knotted carpets originated several centuries BC in Persia. The first US woven carpet mill was built in 1791 in Philadelphia. In 1839, the industry was reshaped with Erastus Bigelow’s invention of the power loom. The majority of carpet is machine-made in modern mills by one of two processes: tufted or woven.
Tufted carpet is now the predominant method of carpet production. In the United States, for example, approximately 96% of all carpet is machine tufted, a process that developed from tufted bedspread manufacturing centred in northwest Georgia. Tufted carpet is made by inserting a pile yarn into a primary backing fabric (usually polypropylene) and then attaching a secondary backing fabric with a synthetic latex to hold the yarns in place and attach the backings to each other, adding stability to the carpet.
Carpet Construction
Machine tufting
The tufting machine is comprised of hundreds of needles (up to 2,400) in a horizontal bar across the width of the machine (see figure 1). The creel, or yarn on cones arranged in racks, are passed overhead through small-diameter guide tubes to the machine needles on a jerker bar. Generally, two yarn spools are provided for each needle. The yarn end of the first spool is spliced together with the leading end of the second one, so that when yarn from the first spool has been used, yarn is supplied from the second without stopping the machine. A guide tube is provided for each yarn end, in order to prevent the yarns from becoming entangled. The yarns pass through a series of vertically aligned, fixed guides attached to the machine body and a guide located on the end of an arm extending from the moving needle bar of the machine. When the needle bar moves up and down, the relationship between the two guides is changed. Tufted product used for residential carpet is shown in figure 2.
Figure 1. Tufting machine
Carpet and Rug Institute
Figure 2. Residential carpet profile
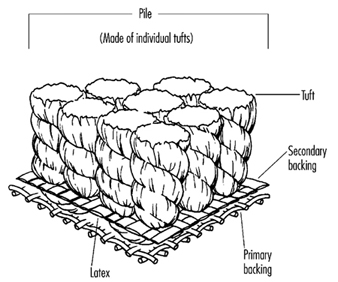
Carpet and Rug Institute
The jerker bar takes up the slack yarn delivered during the upward stroke of the needles. The yarns are threaded through their respective needles in the needle bar. The needles are operated simultaneously at 500 or more strokes per minute in a vertical, reciprocating motion. A tufting machine can produce 1,000 to 2,000 square metres of carpet in 8 hours of operation.
The primary backing into which the yarns are inserted is supplied from a roll located in front of the machine. The speed of the roll of carpet backing controls the stitch length and the number of stitches per inch. The number of needles in the width per inch or cm of the machine determines the gauge of the fabric, such as 3/16 gauge or 5/32 gauge.
Located below the needle plate of the tufting machine are loopers or looper-and-knife combinations, which pick up and hold momentarily the yarns carried by the needles. When forming loop pile, loopers shaped like inverted hockey sticks are positioned in the machine so that the formed pile loops move away from the loopers as the backing is advanced through the machine.
Loopers for cut pile are a reversed “C” shape, with a cutting surface on the top inside edge of the crescent shape. They are used in combination with knives having a ground cutting edge on one end. As the backing advances through the machine toward the cut pile loopers, the yarns picked up from the needles are cut with a scissor-like action between the looper and knife cutting edge. Figure 3 and figure 4 show the tufts on a backing and the kinds of loops available.
Figure 3. Commercial carpet profile
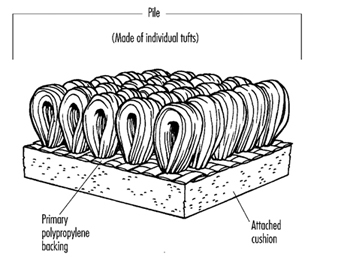
Carpet and Rug Institute
Figure 4. Level loop; cut and loop; velvet plush; saxony
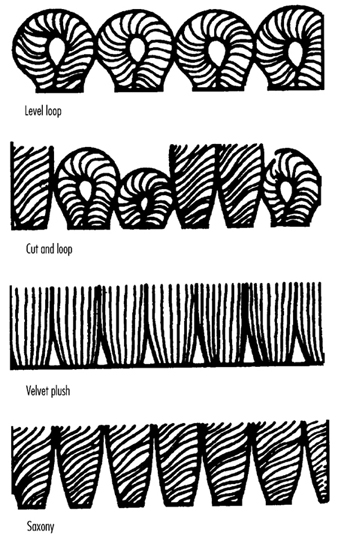
Carpet and Rug Institute
Weaving
Woven carpet has a pile surface yarn woven simultaneously with warp and weft threads that form the integrated backing. Backing yarns are usually jute, cotton or polypropylene. Pile yarns can be wool, cotton or any of the synthetic fibres, such as nylon, polyester, polypropylene, acrylic and so on. A back coating is applied to add stability; however, a secondary back is unnecessary and is rarely applied. Variations of woven carpet include velvet, Wilton and Axminster.
There are other methods of making carpet—knitted, needlepunched, fusion bonded—but those methods are used less often and for more specialized markets.
Fibre and Yarn Production
Carpet is manufactured primarily from synthetic yarns—nylon, polypropylene (olefin) and polyester—with lesser quantities of acrylic, wool, cotton and blends of any of these yarns. In the 1960s, synthetic fibres became predominant because they provide a durable, quality product in an affordable price range.
Synthetic yarns are formed by the extrusion of a molten polymer forced through the tiny holes of a metal plate, or spinneret. Additives to the molten polymer may provide solution-dyed colour or less transparent, whiter, more durable fibres and various other performance attributes. After the filaments emerge from the spinneret, they are cooled, drawn and texturized.
Synthetic fibres can be extruded in different shapes or cross-sections, such as round, trilobal, pentalobal, octalobal or square, depending upon the design and shape of the spinneret holes. These cross-sectional shapes can affect many properties of carpet, including lustre, bulkiness, texture retention, and soil-hiding abilities.
After fibre extrusion, post-treatments, such as drawing and annealing (heating/cooling), increase tensile strength and generally enhance the fibre’s physical properties. The filament bundle then goes through a crimping or texturing process, which converts straight filaments to fibres with a repeating kinked, curled or sawtooth configuration.
Yarn can be produced as either bulked continuous filament (BCF) or staple. The BCF is continuous strands of synthetic fibre formed into yarn bundles. Extruded yarn is made by winding the proper number of filaments for the desired yarn denier directly onto “take-up” packages.
Staple fibres are converted into spun yarns by textile yarn spinning processes. When staple fibre is produced, large bundles of fibre called “tow” are extruded. After the crimping process, the tow is cut into fibre lengths of 10 to 20 cm. There are three critical preparation steps—blending, carding and drafting—before the staple fibres are spun. Blending carefully mixes bales of staple fibre to ensure that the fibres intermingle in a way so that yarn streaking will not occur in subsequent dyeing operations. Carding straightens the fibres and puts them in a continuous sliver (rope-like) configuration. Drafting has three main functions: it blends fibres, places them in a parallel form and continues to decrease the weight per unit length of the total fibre bundle to make it easy to spin into the final yarn.
After spinning, which draws the sliver down to the desired yarn size, the yarn is plied and twisted to provide various effects. The yarn is then wound onto yarn cones to prepare it for the heat-setting and yarn-twisting processes.
Colouration Techniques
Because the synthetic fibres have various shapes, they take dyestuffs differently and may have varying colouration performance characteristics. Fibres of the same generic type can be treated or modified so that their affinity for certain dyes is changed, producing a multicolour or two-toned effect.
Colouration for carpet can be achieved at two possible times in the manufacturing process—either by dyeing the fibre or yarn before the fabric is tufted (pre-dyeing) or by dyeing the tufted fabric (post-dyeing of greige goods) before the application of the secondary backing and the finishing process. Methods of pre-dyeing include solution dyeing, stock dyeing and yarn dyeing. Post-dyeing methods include piece dyeing, the application of colour from an aqueous dye bath onto unfinished carpet; beck dyeing, which handles batches of greige goods of approximately 150 running metres; and continuous dyeing, a continuous process of dyeing almost unlimited quantities by distributing dye with an injection applicator across the full width of the carpet as it moves in open-width form under the applicator. Carpet printing uses machinery that is essentially enlarged, modified textile printing equipment. Both flat-bed and rotary-screen printers are used.
Carpet Finishing
Carpet finishing has three separate purposes: to anchor the individual tufts into the primary backing, to adhere the tufted primary backing to a secondary backing and to shear and clean the surface pile to give an attractive surface appearance. Adding a secondary backing material, such as woven polypropylene, jute or attached cushion material, adds dimensional stability to the carpet.
First, the back of the carpet is coated, usually by means of a roller rotating in a synthetic latex mix, and the latex is spread by a doctor blade. The latex is a viscous solution, usually from 8,000 to 15,000 centipose viscosity. Normally, between 22 and 28 ounces (625–795 g) of latex per square yard is applied.
A separate roll of secondary backing is positioned carefully onto the latex coating. The two materials are then carefully pressed together by a marriage roller. This laminate, remaining flat and unflexed, then passes through a long oven, usually 24 to 49 m long, where it is dried and cured at temperatures from 115 to 150 C for 2 to 5 minutes through three zones of heating. A high rate of evaporation is important for carpet drying, with forced hot air moving along precisely controlled heating zones.
In order to clean the surface yarns that may have developed fuzzing on the tips of the fibre during the dyeing and finishing stages, the carpet is lightly sheared. The shear is a unit that heavily brushes the carpet pile to make it both erect and uniform; it passes the carpet through a series of rotary knives or blades that shear or cut off the fibre tips at a precise, adjustable height. Two or four shear blades operate in tandem. The “double shear” has a double set of hard bristle or nylon brushes and two shear blade heads per unit, used in tandem.
The carpet goes through an intense inspection process and is packaged and stored, or cut, packaged and shipped.
Safe Practices in Carpet Mills
Modern carpet and yarn mills provide safety policies, monitoring of safety performance and, when necessary, prompt and thorough accident investigation. Carpet manufacturing machinery is well guarded to protect employees. Keeping the equipment serviced and safe is of primary importance for enhancing quality and productivity and for protection of the workers.
Workers should be trained in the safe use of electrical equipment and work practices to avoid injuries resulting from the unexpected start-up of machines. They need training to recognize hazardous energy sources, the type and magnitude of the energy available and the methods necessary for energy isolation and control. They also should be trained to distinguish exposed live parts from other parts of electrical equipment; to determine the nominal voltage of exposed, energized parts; and to know the required clearance distances and corresponding voltages. In areas where lockout/tagout will be in effect, employees are instructed in the prohibition against restarting or re-energizing equipment.
Where older equipment is in use, careful inspections should be frequent and upgrades made when advisable. Rotating shafts, v-belts and pulley drives, chain and sprocket drives, and overhead hoists and rigging should be periodically inspected, and guards installed whenever possible.
Because hand-pushed yarn buggies are used to move material in a yarn mill, and because yarn fly waste or lint (the scrap from yarn production) accumulates on the floor, the wheels of the yarn buggies must be kept clean and free to roll.
Employees should be trained in the safe use of compressed air, which is frequently used in clean-up procedures.
Fork-lift trucks, either electric- or propane-powered, are used throughout the carpet manufacturing and warehouse facilities. Proper maintenance and attention to safe refuelling, battery changing and so on are essential. Because fork-lift trucks are used where other personnel are working, various ways may be employed to avoid accidents (e.g., walkways reserved exclusively for workers, in which the trucks are prohibited); portable stop signs where employees are required to work in aisles with heavy fork-lift truck traffic; limiting the warehouse/shipping-dock areas to fork-lift truck operators and shipping personnel; and/or instituting a one-way traffic system.
Redesign of machines to minimize repetitive motions should help to reduce the incidence of repetitive-motion injuries. Encouraging workers to regularly practise simple hand and wrist exercises along with adequate work breaks and frequent changes in work tasks may also be helpful.
Musculoskeletal injuries from lifting and carrying may be reduced by the use of mechanical lifting devices, hand-trucks and rolling carts, and by stacking materials on platforms or tables and, where possible, keeping their bulk and weight to more easily manageable dimensions. Training in proper lifting techniques and muscle strengthening exercises can also be helpful, especially for workers returning after an episode of back pain.
A hearing conservation programme is advisable to avoid injury from the noise levels created in some mill operations. Sound-level surveys of the manufacturing equipment will identify those areas in which engineering controls are not sufficiently effective and in which workers may be required to wear hearing-protection equipment and have annual audiometric testing.
Contemporary standards of ventilation and exhaust of heat, lint and dust should be met by the mills.
Weaving and Knitting
Weaving and knitting are the two primary textile processes for manufacturing fabrics. In the modern textile industry, these processes take place on electrically powered automated machines, and the resulting fabrics find their way into a wide range of end-uses, including wearing apparel, home furnishings and industrial applications.
Weaving
The weaving process consists of interlacing straight yarns at right angles to one another. It is the oldest technology of manufacturing fabric: hand-powered looms were used in pre-Biblical times. The basic concept of interlacing the yarns is still followed today.
Warp yarns are supplied from a large reel, called a warp beam, mounted at the back of the weaving machine. Each warp yarn end is threaded through a heddles harness. The harness is used to lift or depress the warp yarns to allow the weaving to be done. The simplest weaving requires two harnesses, and more intricate woven fabrics require as many as six harnesses. Jacquard weaving equipment is used to manufacture the most decorative fabrics and has features to enable each individual warp yarn to be lifted or depressed. Each yarn end then is threaded through a reed of closely spaced thin parallel metal pieces mounted on the machine’s lay, or sley. The lay is designed to move in a reciprocating arc around a pivotal anchor point. The yarn ends are attached to the take-up roll. The woven fabric is wound on this roll.
The oldest technology for feeding the filling yarn across the width of the warp yarns is the shuttle, which is propelled in a free-flight fashion from one side of the warp yarn to the other side and pays out the filling yarn from a small bobbin mounted in it. New and faster technology, shown in figure 1, called shuttleless weaving, uses air jets, water jets, small projectiles that ride in a guidetrack, or small, sword-like devices called rapiers to carry the filling yarn.
Figure 1. Air-jet weaving machines
Tsudakoma Corp
Employees in weaving are typically grouped into one of four job functions:
- machine operators, commonly called weavers, who patrol their assigned production area to check on fabric production, correct some basic machine malfunctions such as yarn breaks and restart stopped machines
- machine technicians, sometimes called fixers, who adjust and repair the weaving machines
- direct production service workers, who transport and load raw materials (warp and filling yarn) onto the weaving machines and who unload and transport finished products (fabric rolls)
- indirect production service workers, who perform cleaning, machine lubrication and so on.
Safety risks
Weaving presents only a moderate worker safety risk. However, there are a number of typical safety hazards and minimization measures.
Falls
Objects on the floor that cause worker falls include machine parts and oil, grease and water spots. Good housekeeping is particularly important in weaving, since many of the process workers spend most of their workday patrolling the area with eyes directed to the production process rather than toward objects on the floor.
Machinery
Power transmission devices and most other pinch points are typically guarded. The machine lay, harnesses and other parts that must be frequently accessed by weavers, however, are only partially enclosed. Ample walking and working space must be provided around the machines, and good work procedures help workers avoid these exposures. In shuttle weaving, guards mounted on the lay are needed to prevent the shuttle from being thrown out, or to deflect it in a downward direction. Lockouts, mechanical blocks and so on are also required in order to prevent the introduction of hazardous energy into areas when technicians or others are performing job duties on stopped machines.
Materials handling
These can include lifting and moving heavy cloth rolls, warp beams and so on. Hand-trucks to help unload, or doff, and transport small cloth rolls from take-ups on the weaving machine reduce the risk of worker strain injuries by alleviating the need to lift the full weight of the roll. Powered industrial trucks can be used to doff and transport large cloth rolls from bulk take-ups placed at the front of the weaving machine. Wheeled trucks with powered or manual hydraulic assists can be used to handle warp beams, which usually weigh several hundred kg. Warp-handling workers should wear safety shoes.
Fires and ignition
Weaving creates a fair amount of lint, dust and fibre flyings which can represent fire hazards if the fibres are combustible. Controls include dust-collection systems (located under the machines in modern facilities), regular machine cleanings by service workers and use of electrical equipment designed to prevent sparking (e.g., Class III, Division 1, Hazardous Locations).
Health risks
Health risks in modern weaving are generally limited to noise-induced hearing loss and to pulmonary disorders associated with some types of fibres used in the yarn.
Noise
Most weaving machines, operating in the numbers found in a typical production facility, produce noise levels that generally exceed 90 dBA. In some shuttle and high-speed shuttleless weaving, levels may even exceed 100 dBA. Appropriate hearing protectors and a hearing conservation programme are nearly always necessary for weaving workers.
Fibre dust
Pulmonary disorders (byssinosis) have long been linked with dusts associated with the processing of raw cotton and flax fibres, and are discussed elsewhere in this chapter and this Encyclopaedia. Generally, ventilation and room air filtration cleaning systems with dust collection points under the weaving machines and at other points in the weaving area maintain dusts at or below required maximum levels (e.g., 750 mg/m3 of air in the OSHA cotton dust standard) in modern facilities. Additionally, dust respirators are needed for temporary protection during cleaning activities. A worker medical surveillance programme should be in place to identify workers who might be especially sensitive to the effects of these dusts.
Machine Knitting
There is a major cottage industry for the production of hand-knitted items. There are inadequate data on numbers of workers, generally women, thus engaged. The reader is referred to the chapter Entertainment and the arts for an overview of likely hazards. Editor.
The mechanical knitting process consists of interconnecting loops of yarn on powered automated machines (see figure 2). The machines are equipped with rows of small, hooked needles to draw formed yarn loops through previously formed loops. The hooked needles have a unique latch feature that closes the hook to easily allow the loop drawing and then opens to allow the yarn loop to slide off the needle.
Figure 2. Circular-knitting machine
Sulzer Morat
Circular-knitting machines have needles arranged in a circle, and the fabric produced on them comes off the machine in the shape of a large tube that is wound onto a take-up roll. Flat-knitting machines and warp-knitting machines, on the other hand, have needles arranged in a straight row, and fabric comes off the machine in a flat sheet for roll take-up. Circular- and flat-knitting machines are generally fed from yarn cones, and warp-knitting machines are generally fed from warp beams that are smaller but similar to those used in weaving.
Employees in knitting are grouped into job functions with duties similar to those in weaving. Job titles appropriately parallel the process name.
Safety risks
Safety risks in knitting are similar to those in weaving though generally of a lesser degree. Oil on the floor often is a little more prevalent in knitting due to the high lubrication needs of the knitting needles. Machine entrapment risks are less in knitting since there are fewer pinch points on the machines than those found in weaving, and much of the machinery lends itself well to enclosure guarding. Energy-control lockout procedures remain a must.
Cloth roll handling still presents a worker strain injury risk, but the heavy warp-beam handling risks are not present except in warp knitting. Risk control measures are similar to those in weaving. Knitting does not produce the levels of lint, flyings and dust that are found in weaving, but the oil from the process helps keep the fire fuel load at a level that needs attention. Controls are similar to those in weaving.
Health risks
Health risks in knitting are also generally lower than those in weaving. Noise levels range in the mid-80-dBA to low-90-dBA levels. Respiratory disorders for knitting workers processing raw cotton and flax do not appear to be especially prevalent, and regulatory standards for these materials are often not applicable in knitting.
Nonwoven Textile Fabrics
The nonwoven textile fabric industry had an exploratory beginning in the late 1940s which entered into a development phase in the 1950s followed by commercial expansion in the 1960s. During the next 35 years, the nonwoven industry matured and established markets for nonwoven fabrics by either providing cost-effective performance as alternatives to conventional textiles or providing products specifically developed for targeted end-uses. The industry has survived recessions better than conventional textiles and has grown at a faster rate. Its health and safety problems are similar to those of the rest of the textile industry (i.e., noise, airborne fibres, chemicals used in bonding fibres, safe working surfaces, pinch points, burns from thermal exposures, back injuries and so on).
The industry generally has a good safety record, and the number of injuries per standard work unit is low. The industry has responded to challenges associated with clean water and clean air acts. In the United States, the Occupational Safety and Health Administration (OSHA) has promulgated a number of worker protection rules which require safety training and manufacturing practices that have improved worker protection significantly. Responsible companies throughout the world are adopting similar practices.
The raw materials used by the industry are generally similar to those used in conventional textiles. The industry has been estimated to use almost 1 billion kg of a mix of raw materials annually. The natural fibres used are predominately cotton and wood pulp. The manufactured fibres include rayon, polyolefins (both polyethylene and polypropylene), polyesters and, to a smaller degree, nylons, acrylics, aramids and others.
There was an early growth in the number of nonwoven processes to approximately ten. These include; spunbond, melt blown, air-laid pulp and blends, wet laid, dry laid (bonded by either needlepunching, thermal bonding or chemical bonding) and stitch bonding processes. In the United States, the industry has saturated many of its end-use markets and is currently searching for new ones. A major growth area for nonwovens is developing in the area of composites. Laminates of nonwovens with films and other coatings are broadening markets for nonwoven materials. The storage of nonwoven roll goods has recently come under scrutiny because of the flammability of some products that have very low densities and high surface areas. Rolls whose volume-to-weight ratio is greater than a certain roll loft factor are considered to pose storage problems.
Raw Materials
Cellulosic fibres
The volume of bleached cotton used in nonwoven fabrics has been steadily increasing, and cotton-polyester and rayon-polyester blends in nonwoven fabrics, bonded by hydroentangling, have become attractive combinations for medical and feminine hygiene applications. There has been an interest in using unbleached cotton in nonwoven processes, and some attractive experimental fabrics have been produced through the use of the hydroentangling process.
Rayon has encountered some pressure from environmentalists who are concerned about the impact that by-products of the process have on the environment. Some rayon-producing companies in the United States abandoned the industry rather than face the cost of complying with regulatory requirements imposed by the clean water and air acts. Those companies that chose to meet the requirements now appear to be comfortable with their modified processes.
Wood pulp fibres are a major component of disposable diapers, incontinence products and other absorbent products. Fibres from hardwood and kraft fibres are employed. In the United States alone, use of pulp fibres totals more than 1 billion kg annually. A small percentage is used in air-laid nonwoven processes. The products are popular as towels in applications which range from the kitchen to sports.
Synthetic fibres
The two most popular polyolefin fibres are polyethylene and polypropylene. These polymers are either converted into staple-length fibres which are subsequently converted into nonwoven fabrics, or else converted into spunbonded nonwoven fabrics by extruding the polymers to form filaments which are formed into webs and bonded by thermal processes. Some of the fabrics produced are converted into protective apparel, and by 1995, more than 400,000,000 coveralls had been made using a popular spunbonded polyethylene fabric.
The largest single use for a nonwoven fabric in the United States (approximately 10 billion square metres) is as the cover sheet in disposable diapers. This is the fabric which contacts the baby’s skin and separates the baby from the other diaper components. Fabrics from these fibres are also used in durable products and in some geotextile applications where they are expected to last indefinitely. The fabrics will degrade in ultraviolet light or some other types of radiation.
Thermoplastic fibres from polyester polymers and copolymers are widely used in nonwovens in both staple fibre and spunbonded processes. The combined volume of polyester and polyolefin polymers used in the United States in nonwoven fabrics has been estimated to be more than 250 million kg annually. Blends of polyester fibres with wood pulp which are wet laid and then bonded by hydroentangling and subsequently treated with a repellent coating are widely used in disposable surgical gowns and drapes. By 1995, the use of disposable medical nonwovens in the United States alone exceeded 2 billion square metres annually.
Nylon fibres are used only sparingly in the form of staple fibres and in a limited volume in spunbonded nonwovens. One of the largest uses for spundbonded nylon nonwovens is in the reinforcement of carpet pads and in fibreglass filters. The fabrics provide a low friction surface to carpet pads that facilitates the installation of carpets. In fibreglass filters, the fabric helps retain the fibreglass in the filter and prevents glass fibres from entering the filtered air stream. Other specialty nonwovens, such as aramids, are used in niche markets where their properties, such as low flammability, recommend their use. Some of these nonwovens are used in the furniture industry as flame blockers, to reduce the flammability of sofas and chairs.
Processes
Spunbonded and meltblown
In the spunbonded and meltblown processes, suitable synthetic polymers are melted, filtered, extruded, drawn, charged electrostatically, laid down in web form, bonded and taken up as rolls. The process requires good safety practices common to working with hot extruders, filters, spinnerets and heated rolls used for bonding.
Workers should wear proper eye protection and avoid wearing loose clothing, neckties, rings or other jewellery that may be caught in moving equipment. Also, these processes almost always involve the use of large volumes of air, and special precautions must be taken to avoid designs that might lead to fires, such as placing light ballasts in an air duct. Extinguishing a fire in an air duct is difficult. It is important to maintain safe working-floor surfaces, and the floors around any nonwoven equipment should be free of contamination that can lead to unsafe footing.
Spunbonded and meltblown processes call for cleaning some of the process equipment by burning away any accumulated polymer residue. This usually involves the use of very hot ovens for both cleaning and storing the cleaned parts. Obviously, these operations require proper gloves and other thermal protection, as well as appropriate ventilation to reduce heat and exhaust fumes.
Spunbonded processes owe their economic advantages in part to the fact that they are relatively fast and the take-up rolls can be changed while the process continues to run. The design of the roll-changing equipment and the training of the operators should provide for an adequate margin of safety to handle these changeovers.
Dry laid
Processes that involve opening of bales of fibres, blending the fibres to provide a uniform feed to a carding machine, carding to form webs, cross-lapping the webs to provide optimum strength in all directions and then forwarding the web to some bonding process are similar in their safety requirements to conventional textile processes. All exposed points that could trap a worker’s hands in roll interfaces need protection. Some dry-laid processes involve the generation of small amounts of airborne fibres. The worker should be provided with adequate respiratory PPE in order to avoid inhalation of any respirable part of these fibres.
If the webs formed are to be bonded thermally, there will normally be a small amount (on the order of 10% by weight) of a lower-melting fibre or powder that has been blended into the web. This material is melted by exposure to a hot air oven or to heated rollers and then cooled to form the fabric’s bonds. Protection against exposure to the heated environments should be provided. In the United States, approximately 100 million kg of thermally bonded nonwovens are produced annually.
If the webs are bonded by needle punching, a needle loom is used. An array of needles is mounted in needle boards, and the needles are driven through the web. Needles capture surface fibres, carry them from the top to the bottom of the fabric and then release the fibres on the return stroke. The number of penetrations per unit area can range from a small number (in the case of high-loft fabrics) to a large number (in the case of needled felts). A loom may be used for needling from both the top and bottom sides of the web and for use with multiple boards. Broken needles must be replaced. Safety-locking the looms is required in order to prevent accidents during such maintenance. As in the case of carding, some small fibres may be generated by these processes, and ventilation and respirators are recommended. In addition, eye protection is advised to protect against flying debris from broken needles. In the United States, approximately 100 million kg of needlepunched nonwovens are manufactured annually.
If the webs are bonded by chemical adhesive, the process normally calls for spraying the adhesive on one side of the web and passing it through a curing area, normally a through-air oven. The web direction is then reversed, another application of the adhesive is made and the web is sent back through the oven. A third pass through the oven is sometimes used if needed to complete the curing process. Obviously, the area must exhaust the oven gases and it is necessary to capture and remove any toxic effluents (in the United States, this is required by various state and federal clean air acts). In the case of adhesive bonding, there has been worldwide pressure to reduce the release of formaldehyde into the environment. In the United States, the EPA has recently tightened limits on the release of formaldehyde to one tenth of the previously acceptable limits. There are concerns that the new limits challenge the precision of currently available laboratory methods. The adhesive industry has responded by offering new binders which are formaldehyde free.
Air laid
There is some nomenclature confusion in regard to air-laid nonwovens. One of the variations of carding processes includes a card that includes a section that randomizes the fibres being processed in an air stream. This process is often referred to as an “air-laid nonwoven process”. Another, very different, process, also called air laid, involves the dispersion of fibres in an air stream, usually using a hammer mill, and directing the airborne fibre dispersion to a device that deposits the fibres on a moving belt. The web formed is then spray bonded and cured. The laydown process may be repeated in line with different types of fibres to produce nonwoven fabrics from layers with different fibre compositions. The fibres used in this case can be very short, and protection to prevent exposure to such airborne fibres must be taken.
Wet laid
The wet laid nonwoven process borrows technology developed for making paper and calls for the formation of webs from dispersions of fibres in water. This process is assisted by the use of dispersion aids that help avoid non-uniform clumps of fibres. The fibre dispersion is filtered through moving belts and dewatered by pressing between felts. At some point in the process a binder is often added which bonds the web during the heat of drying. Alternatively, in a newer method, the web is bonded by hydroentangling using high-pressure jets of water. The final step involves drying and may include steps to soften the fabric by microcreping or some other similar technique. There are no known major hazards associated with this process, and the safety programmes normally are based on common good manufacturing practices.
Stitchbonding
This process is often excluded from some definitions of nonwovens because it can involve the use of yarns to stitch webs into fabrics. Some definitions of nonwovens exclude any fabrics which contain “yarn”. In this process a web is presented to conventional stitchbonding machines to produce knit-like structures that offer a wide variety of combinations including the use of elastic yarns to produce fabrics with attractive stretch and recovery properties. Again, no exceptional hazards are associated with this process.
Finishing
Finishes for nonwoven fabrics include flame retardant, fluid repellent, antistatic, softeners, anti-bacterial, fusible, lubricants and other surface treatments. Finishes for nonwovens are applied either on-line or as off-line, post-manufacturing treatments, depending on the process and the type of finish. Frequently, antistatic finishes are added on-line, and surface treatment such as corona etching is normally an on-line process. Flame-retardant and -repellent finishes are often applied off-line. Some specialized fabric treatments include exposing the web to a high-energy plasma treatment to influence the polarity of fabrics and improve their performance in filtration applications. The safety of these chemical and physical processes varies with each application and must be considered separately.
Dyeing, Printing and Finishing
The section on dyeing is adapted from A.K. Niyogi’s contribution to the 3rd edition of the Encyclopaedia of Occupational Health and Safety.
Dyeing
Dyeing involves a chemical combination or a powerful physical affinity between the dye and the fibre of the fabric. An extensive variety of dyes and processes is used, depending on the type of fabric and the end-product desired.
Classes of dyes
Acid or basic dyes are used in a weak acid bath for wool, silk or cotton. Some acid dyes are used after mordanting the fibres with metallic oxide, tannic acid or dichromates. Direct dyes, which are not fast, are used for the dyeing of wool, rayon and cotton; they are dyed at the boil. For dyeing cotton fabrics with sulphur dyes, the dyebath is prepared by pasting the dye with soda ash and sodium sulphide and hot water. This dyeing is also carried out at the boil. For dyeing cotton with azo dyes, naphthol is dissolved in aqueous caustic soda. The cotton is impregnated with the solution of the sodium naphthoxide that is formed, and it is then treated with a solution of a diazo compound to develop the dye in the material. Vat dyes are made into leuco-compounds with sodium hydroxide and sodium hydrosulphite; this dyeing is done at 30 to 60 ºC. Disperse dyes are used for the dyeing of all synthetic fibres which are hydrophobic. Swelling agents or carriers which are phenolic in nature must be used to enable the disperse dyes to act. Mineral dyes are inorganic pigments which are salts of iron and chromium. After impregnation, they are precipitated by addition of hot alkaline solution. Reactive dyes for cotton are used in a hot or a cold bath of soda ash and common salt.
Preparing fabrics for dyeing
The preparatory processes before dyeing cotton fabrics consist of the following sequence of steps: The cloth is passed through a shearing machine to cut the loosely adhering fibres and then, to complete the trimming process, it is passed rapidly over a row of gas flames and the sparks are extinguished by passing the material through a water box. Desizing is carried out by passing the cloth through a diastase solution which removes the size completely. To remove other impurities, it is scoured in a kier with dilute sodium hydroxide, sodium carbonate or turkey red oil for 8 to 12 hours at high temperature and pressure.
For coloured woven material, an open kier is used and sodium hydroxide is avoided. The natural colouring in the cloth is removed by hypochlorite solution in the bleaching pits, after which the cloth is aired, washed, dechlorinated by means of a sodium bisulphite solution, washed again and scoured with dilute hydrochloric or sulphuric acid. After a final, thorough washing, the cloth is ready for the dyeing or printing process.
Dyeing process
Dyeing is carried out in a jig or padding machine, in which the cloth is moved through a stationary dye solution prepared by dissolving the dyestuff powder in a suitable chemical and then diluting with water. After dyeing, the cloth is subjected to a finishing process.
Nylon dyeing
The preparation of polyamide (nylon) fibres for dyeing involves scouring, some form of setting treatment and, in some cases, bleaching. The treatment adopted for the scouring of woven polyamide fabrics depends mainly on the composition of the size used. Water-soluble sizes based on polyvinyl alcohol or polyacrylic acid can be removed by scouring in a liquor containing soap and ammonia or Lissapol N or similar detergent and soda ash. After scouring, the material is rinsed thoroughly and is then ready for dyeing or printing, usually in a jigger or winch dyeing machine.
Wool dyeing
The raw wool is first scoured by the emulsification process, in which soap and a soda ash solution are used. The operation is carried out in a washing machine which consists of a long trough provided with rakes, a false bottom and, at the exit, wringers. After thorough washing, the wool is bleached with hydrogen peroxide or with sulphur dioxide. If the latter is used, the damp goods are left exposed to the sulphur dioxide gas overnight. The acid gas is neutralized by passing the fabric through a sodium carbonate bath, and then it is thoroughly washed. After dyeing, the goods are rinsed, hydroextracted and dried.
Hazards in Dyeing and Their Prevention
Fire and explosion
The fire hazards found in a dye works are the flammable solvents used in the processes and certain flammable dyestuffs. Safe storage facilities should be provided for both: properly designed storerooms constructed of fire-resisting materials with a raised and ramped sill at the doorway so that escaping liquid is contained within the room and prevented from flowing to a place where it may be ignited. It is preferable that stores of this nature be located outside the main factory building. If large quantities of flammable liquids are kept in tanks outside the building, the tank area should be mounded to contain escaping liquid.
Similar arrangements should be made when the gaseous fuel used on the singeing machines is obtained from a light petroleum fraction. The gas-making plant and the storage facilities for the volatile petroleum spirit should preferably be outside the building.
Chemical hazards
Many factories use hypochlorite solution for bleaching; in others, the bleaching agent is gaseous chlorine or bleaching powder which releases chlorine when it is charged into the tank. In either case, workers may be exposed to dangerous levels of chlorine, a skin and eye irritant and a dangerous pulmonary tissue irritant causing delayed lung oedema. To limit the escape of chlorine into the workers’ atmosphere, bleaching vats should be designed as closed vessels provided with vents that limit the escape of chlorine so that the relevant recommended maximum exposure levels are not exceeded. Atmospheric chlorine levels should be checked periodically to ensure that the exposure limit is not being exceeded.
The valves and other controls of the tank from which the liquid chlorine is supplied to the dyeworks should be controlled by a competent operator, since the possibilities of an uncontrolled leak could well be disastrous. When a vessel that has contained chlorine or any other dangerous gas or vapour has to be entered, all of the precautions advised for work in confined places should be taken.
The use of corrosive alkalis and acids and the treatment of cloth with boiling liquor expose the workers to the risk of burns and scalds. Both hydrochloric acid and sulphuric acid are used extensively in dyeing processes. Caustic soda is used in bleaching, mercerizing and dyeing. Chips from the solid material fly and create hazards for the workers. Sulphur dioxide, which is used in bleaching, and carbon disulphide, which is used as a solvent in the viscose process, can also pollute the workroom. Aromatic hydrocarbons such as benzol, toluol and xylol, solvent naphthas and aromatic amines such as aniline dyes are dangerous chemicals to which workers are likely to be exposed. Dichlorobenzene is emulsified with water with the help of an emulsifying agent, and is used for dyeing of polyester fibres. LEV is essential.
Many dyestuffs are skin irritants that cause dermatitis; in addition, workers are tempted to use harmful mixtures of abrasive, alkali and bleaching agents to remove dye stains from their hands.
Organic solvents used in the processes and for the cleaning of machines may themselves cause dermatitis or render the skin vulnerable to the irritant action of the other harmful substances that are used. Furthermore, they may be the cause of peripheral neuropathy—for example, methyl butyl ketone (MBK). Certain dyes, such as rhodamine B, magenta, β-naphthylamine and certain bases such as dianisidine, have been found to be carcinogenic. The use of β-naphthylamine has generally been abandoned in dyestuffs, which are discussed more fully elsewhere in this Encyclopaedia.
In addition to the fibre materials and their contaminants, allergy may be caused by the sizing and even by the enzymes used to remove the sizing.
Suitable PPE, including eye-protective equipment, should be provided to prevent contact with these hazards. In certain circumstances when barrier creams have to be used, care should be taken to ensure that they are effective for the purpose and that they can be removed by washing. At best, however, the protection they provide is rarely as reliable as that afforded by properly designed gloves. Protective clothing should be cleaned at regular intervals, and when splashed or contaminated by dyestuffs, it should be replaced by clean clothing at the earliest opportunity. Sanitary facilities for washing, bathing and changing should be provided, and the workers should be encouraged to use them; personal hygiene is particularly important for dye workers. Unfortunately, even when all protective measures have been taken, some workers are found to be so sensitive to the effects of these substances that transfer to other work is the only alternative.
Accidents
Serious scalding accidents have occurred when hot liquor has been accidentally admitted to a kier in which a worker has been arranging the cloth to be treated. This can occur when a valve is accidentally opened or when hot liquor is discharged into a common discharge duct from another kier on the range and enters the occupied kier through an open outlet. When a worker is inside a kier for any purpose, the inlet and outlet should be closed, isolating that kier from the other kiers on the range. If the locking device is operated by a key, it should be retained by the worker who might be injured by an accidental admission of hot liquid until he or she leaves the vessel.
Printing
Printing is carried out on a roller printing machine. The dye or pigment is thickened with starch or made into emulsion which, in the case of pigment colours, is prepared with an organic solvent. This paste or emulsion is taken up by the engraved rollers which print the material, and the colour is subsequently fixed in the ager or curing machine. The printed cloth then receives the appropriate finishing treatment.
Wet printing
Wet printing is performed with dyeing systems similar to those used in dyeing, such as vat printing and fibre-reactive printing. These printing methods are used only for 100% cotton fabric and for rayon. The health hazards associated with this type of printing are the same as those discussed above.
Solvent-based pigment printing
Solvent-based printing systems use large amounts of solvents such as mineral spirits in the thickening system. The major hazards are:
- Flammability. The thickening systems contain up to 40% solvents and are highly flammable. They should be stored with extreme caution in properly ventilated and electrically grounded areas. Care should also be taken in transferring these products to avoid creating a spark from static electricity.
- Air emissions. Solvents in this print system will be flashed off from the oven during drying and curing. Local environmental regulations will dictate the permissible levels of volatile organic compound (VOC) emissions that can be tolerated.
- Sludge. Since this print system is solvent based, the print paste cannot be allowed to enter the wastewater treatment system. It must be disposed of as a solid waste. Sites where sludge piles are used can have environmental problems with ground and groundwater contamination. These sludge storage areas should be equipped with waterproof linings to prevent this from occurring.
Aqueous-based pigment printing
None of the health hazards for solvent-based pigment printing apply to the aqueous-based printing systems. Although some solvents are used, the amounts are so small that they are not significant. The primary health hazard is the presence of formaldehyde.
Pigment printing requires the use of a cross-linker to assist in the bonding of the pigments to the fabric. These cross-linkers exist as stand-alone products (e.g., melamine) or as part of other chemicals such as binders, antiwicks, and even in the pigments themselves. Formaldehyde plays a necessary role in the function of the cross-linkers.
Formaldehyde is a sensitizer and an irritant that may produce reactions, sometimes violent, in workers who are exposed to it either by inhaling the air around the printing machine as it is operating or by coming into contact with the printed fabric. These reactions may range from simple eye irritation to welts on the skin and severe difficulty with breathing. Formaldehyde has been found to be carcinogenic in mice but it has not yet been conclusively associated with cancer in humans. It is classified as a Group 2A Carcinogen, “Probably Carcinogenic to Humans”, by the International Agency for Research on Cancer (IARC).
To protect the local environment, emissions from the plant have to be monitored to ensure that levels of formaldehyde do not exceed those stipulated by applicable regulations.
Another potential hazard is ammonia. Since the print paste is pH (acidity) sensitive, ammonia is often used as a print-paste thickener. Care should be taken to handle ammonia in a well-ventilated area and to wear respiratory protection if necessary.
Since all dyes and pigments used in printing are usually in a liquid form, dust exposure is not a hazard in printing as it is in dyeing.
Finishing
Finishing is a term applied to a very broad range of treatments that are usually performed during the last manufacturing process before fabrication. Some finishing can also be performed after fabrication.
Mechanical finishing
This type of finishing involves processes that change the texture or appearance of a fabric without the use of chemicals. They include:
- Sanforizing. This is a process where a fabric is overfed between a rubber belt and a heated cylinder and then fed between a heated cylinder and an endless blanket to control shrinkage and create a soft hand.
- Calendering. This is a process where fabric is fed between large steel rollers under pressures that range up to 100 tonnes. These rolls can be heated with either steam or gas to temperatures up to 232 °C. This process is used to change the hand and appearance of the fabric.
- Sanding. In this process, fabric is fed over rolls which are covered with sand to change the surface of the fabric and give a softer hand.
- Embossing. This is a process where fabric is fed between heated steel rollers which have been engraved with a pattern which is permanently transferred to the fabric.
- Heat-setting. This is a process where synthetic fabric, usually polyester, is run through either a tenter frame or a semi-contact heat-set machine at temperatures that are high enough to begin the molecular melting of the fabric. This is done to stabilize the fabric for shrinkage.
- Brushing. This is a process where fabric is run across brushes revolving at high speeds to change the surface appearance and the hand of the fabric.
- Sueding. In this process, fabric is run between a small steel roller and a larger roller that is covered with sandpaper to change the appearance and the hand of the fabric.
The principal hazards are the presence of heat, the very high temperatures being applied and nip points in the moving machine parts. Care should be taken to properly guard the machinery to prevent accidents and physical injury.
Chemical finishing
Chemical finishing is performed on a variety of types of equipment (e.g., pads, jigs, jet dye machines, becks, spray bars, kiers, paddle machines, kiss roll applicators and foamers).
One type of chemical finishing does not involve a chemical reaction: the application of a softener or a hand builder to modify the feel and texture of the fabric, or to improve its sewability. This presents no significant hazards except for the possibility of irritation from skin and eye contact, which can be prevented by the use of proper gloves and eye protection.
The other type of chemical finishing involves a chemical reaction: resin finishing of cotton fabric to produce desired physical properties in the fabric such as low shrinkage and a good smoothness appearance. For cotton fabric, for example, a dimethyldihydroxyethylene urea (DMDHEU) resin is catalysed and bonds with the cotton molecules of the fabric to create a permanent change in the fabric. The primary hazard associated with this type of finishing is that most resins release formaldehyde as part of their reaction.
Conclusion
As in the rest of the textile industry, dyeing, printing and finishing operations present a mixture of old, generally small establishments in which worker safety, health and welfare are given little if any attention, and newer, larger establishments with ever-improving technology in which, to the extent possible, hazard control is built into the design of the machinery. In addition to the specific hazards outlined above, such problems as substandard lighting, noise, incompletely guarded machinery, lifting and carrying of heavy and/or bulky objects, poor housekeeping and so on remain ubiquitous. Therefore, a well-formulated and implemented safety and health programme that includes the training and effective supervision of workers is a necessity.