- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- The Physical Environment and Health Care
Forms of Workers' Participation
The phrase workers’ participation is used loosely to encompass various forms of workers’ participation in decision making, usually at the enterprise level. They complement other forms that may exist at the industrial or sectoral level and the national level, such as bodies for tripartite cooperation. The types of workers’ participation arrangement differ widely with regard to their functions and powers, ranging from informal individual employee suggestion schemes to co-determination of certain matters by workers’ representatives together with management. The mechanisms used for encouraging employee participation vary so widely that it is impossible to review them fully here. The main forms that have attracted recent interest, particularly in the field of work organization, are reviewed below; to these could be added the historical example of self-management by workers in former Yugoslavia. As particularly relevant today, joint safety and health committees are examined as a special form of workers’ participation within the larger labour relations context.
The idea of workers’ participation arose in Europe, where collective bargaining has usually been at the branch or industry level; this often left a gap of employee representation at the enterprise or plant level, which became filled by bodies such as works councils, works committees, enterprise committees and so forth. Many developing countries have also adopted legislative initiatives with a view to having works councils or similar structures set up (e.g., Pakistan, Thailand, Zimbabwe) as a means of promoting labour-management cooperation. The relationship of these bodies to trade unions and collective bargaining has been the subject of considerable legislation and negotiation. This is reflected in a provision of the ILO Workers’ Representatives Convention, 1971 (No. 135), which states that where both trade union representatives and elected representatives exist in the same undertaking, measures shall be taken to ensure that the existence of those representatives is not used to undermine the position of the trade union (Article 5).
Direct Participation
Workers may participate in decision making either directly themselves or indirectly through their representatives – trade unions or elected employee representatives. Since the 1980s, there has been a spread of direct participation by workers, if the term participation is understood as the exercise of any influence on their work or how it is to be carried out. Thus workers may “participate” in work-related decisions not only when there is an institution, such as a quality circle, at the workplace. Accordingly, a simple exercise of work enrichment may be a form of promoting direct participation of workers.
Direct participation may be on an individual basis – for example, through suggestion schemes or “enriched” work. It may also be on a group basis – for example, in quality circles or similar small-group activities. Teamwork in itself constitutes a form of group-based direct participation. Direct participation may be integrated into decisions about daily work, or it may take place outside daily work, such as in a voluntary quality circle that cuts across the group structure habitually used. Direct participation may also be “consultative” or “deliberative”; research by the European Foundation for the Improvement of Living and Working Conditions has explored this particular aspect in some detail (Regalia and Gill 1996). With consultative participation, employees are encouraged and enabled, either as individuals or members of a group, to make their views known, but it is up to management to accept or reject their proposals. Deliberative participation, on the other hand, places some of traditional management responsibility in the employees’ hands, as in the case of teamworking or semi-autonomous work groups wherein some authority has been delegated to the workers.
Works Councils and Similar Structures; Co-determination
The term works councils describes arrangements for the represen-tation of employees, usually at the plant level although they also exist at higher levels (company, group of companies, industry, European Union). The relationship to trade unions is often delineated by legislation or clarified by collective agreement, but tensions between these institutions sometimes remain all the same. Extensive use of works councils, sometimes called workers’ committees, cooperation committees or otherwise, is well established in a number of European countries, such as Belgium, Denmark, France, Germany and the Netherlands and, under the impetus of Directive No. 94/45/EC of 1994 on European works councils, can be anticipated to spread in that region for large enterprises. Several Central and Eastern European countries, such as Hungary and Poland, have enacted legislation to encourage the emergence of works councils. They are found as well in some countries in Africa, Asia and Latin America; part of the post-apartheid labour law reform in South Africa, for instance, included establishing a form of works councils alongside trade union structures.
The possible powers of works councils are best illustrated by the example of Germany, although in some ways it is a unique case. Weiss (1992) describes the works council in that country as the form of institutionalized representation of interests for employees within an establishment. A works council enjoys certain rights to information, consultation (as in all countries) and co-determination (much more rare). As the most far-reaching form of participation, co-determination covers participation in arrangements on health and safety at work and the formal adoption of a reconciliation of interests and a “social plan” in the event of a substantial alteration in the establishment, such as a plant closure. Co-determination rights also extend to guidelines for staff selection and appraisal, in-service training and measures affecting individual workers such as grading, transfer and dismissal. The German works council is empowered to conclude works agreements at the enterprise level and can initiate complaints where it believes the agreement is not being honoured. Included in the areas of obligatory collective co-determination are accident prevention and health protection, works rules, working time, the fixing of performance-related pay rates, the manner of payment, general principles governing holidays and others. On these matters, the employer cannot take action without the works council’s agreement. The works council also has the right to take the initiative and can refer a matter to the establishment-level arbitration committee for enforcement. As Weiss (1992) characterizes it, the works council’s role is “participating in the ‘how’ after the employer has made a decision on the ‘whether’”. The right to consultation affords the works council a chance to play a part in the decisions made by the employer, but failure to consult will not invalidate the decision. The subjects on which consultation is required include protection against dismissal, protection against technical hazards, training and preparation of a social plan.
The works council must observe the principles of cooperation with the employer and the peace obligation (no work stoppages); it also must cooperate with trade unions present and with the appropriate employers’ organization. Works councils are bound to conduct their business impartially, without regard to race, religion or creed, nationality, origin, political or union activity, sex or age of the employees. The employer provides the facilities for the works council, funds it and is liable for its actions.
Works councils are elected separately for manual and non-manual workers in Germany. Special works council elections are held; while there is no legal connection between these representatives and trade union officers in fact, they often coincide. In Austria and Germany, special representation is ensured for disabled workers and young workers and trainees. Works council members receive no remuneration for this, but necessarily incurred expenses are reimbursed. Members are guaranteed retention of their pay level and job grading after the term of office has expired and enjoy special protection against dismissal. They are entitled to release from work to conduct works council business and attend training. Such protections are in line with the Workers’ Representatives Convention (No. 135), which calls for workers’ representatives in an undertaking to enjoy effective protection against any act prejudicial to them, including dismissal, based on their status or activities as a workers’ representative (Article 1).
Many countries feature less ambitious works council schemes that provide for information and consultation rights. Especially where trade unions have little presence on the shop floor level, there is considerable interest in introducing works councils or workers’ committees as a means for workers to have a voice at the workplace level.
Quality Circles and Total Quality Management
Quality circles and other similar group activities were rapidly introduced in a large number of enterprises in some Western European countries (e.g., the United Kingdom and France) at the start of the 1980s and in the United States a little earlier. They built upon “Quality of Working Life” (QWL) or “Humanization of Work” programmes that began in the early 1970s. Their spread was considerably later in some other Western countries (e.g., Germany) and still seems to be very limited in countries where joint project groups are the predominant means of dealing with work organization, such as Sweden. They were stimulated by a belief that Japan’s ability to produce innovative and high-quality products at low cost had something to do with the way human resources were managed in that country; quality circles were the most visible and easily transplantable feature of Japanese human resource management. Quality circles are generally expected to produce two types of effect: one is the enhancement of quality and productivity and the other is the fostering of a sense of participation in work-related decisions among workers, leading to increased job satisfaction and better industrial relations. In Japan the emphasis has been placed more on the first aspect and in Europe and North America on the second. There are also structural differences: while circle leaders are normally appointed by management in Japan, they are often elected in Germany. Today, the emphasis of QWL programmes is more on enhancing productivity and competitiveness (Ozaki 1996).
In some of the countries where quality circles were experimented with widely in the 1980s, such as France and the United Kingdom, there has been a certain disenchantment with their relative ineffectiveness in producing the expected results. Many circles disappeared a few years after their creation; many others exist on paper, but are in fact moribund. The failure has been attributed to many factors – their tendency to create confusion in the normal lines of command, non-management control over membership, circles’ determining their own agenda without heed for management priorities, lack of enthusiasm or hostility on the part of middle management, absence of durable commitment on the part of top management and restriction of scope to minor work-related issues.
Realization of these shortcomings led to the formation of a theory of “Total Quality Management” (TQM). Certain principles of TQM have implications for employee participation: all employees are to participate in the process of improving the business, and responsibility for quality is to be assigned to people who in fact control the quality of what they do. Thus TQM encourages job enlargement and enrichment leading to semi-autonomous work groups. It also promotes horizontal coordination in a firm through, for example, the use of ad hoc, multi functional or interdepartmental project teams.
Joint Project Groups
The practice of establishing joint project groups to study the best ways of introducing technological or organizational changes through the joint efforts of managers and workers is a traditional feature of labour relations in some countries, such as Sweden. A joint project group is normally composed of managers, workplace union representatives and shop-floor workers and often assisted by outside experts. The management and the union concerned often establish joint project groups separately on four issues: new technology, work organization, training and work environment. The Swedish model of joint project groups presents a notable example of direct participation of shop-floor workers within a framework of established collective labour relations. The system is also found in other countries, such as Germany and Japan.
Semi-autonomous Group Work and Teamwork
Semi-autonomous group work and teamwork are both forms of on-line direct participation of shop-floor workers in work-related decisions, unlike the above-mentioned joint project group work, which is a form of off-line participation. The main difference between the two forms of participation lies in the degree of autonomy which the members of the team or group enjoy in organizing their work. Semi-autonomous group work was used extensively in Scandinavia, although recently there has been a move back to a more traditional approach; there have been experiments with it elsewhere in Europe as well.
While experiments with semi-autonomous group work are generally declining, teamwork is spreading fast throughout Western countries. The degree of autonomy which a team enjoys varies widely from one company to another. Team structure also differs. In many countries, team leaders are usually appointed by management, but in a few countries (e.g., Germany) they are often elected by co-workers. Frequently, the creation of teams is accompanied by significant changes in the role of first-line supervisors; they tend to take on greater responsibility for advising team members and for both vertical and horizontal communication, but lose their supervisory role. Employers have shown increasing interest in teamwork because it tends to facilitate the upgrading of workers’ skills and widens the range of workers’ tasks, thus allowing greater flexibility in production processes. However, it is sometimes criticized by workers as a means of inducing them to work harder “voluntarily” by substituting co-workers’ pressure for management control.
Employee Representation on Supervisory Boards; Employee Shareholding
Some commentators include forms of employee ownership or representation on company boards as expressions of workers’ participation. In Germany and the Scandinavian countries, among others, workers have indirect participation above the enterprise level by the inclusion of workers’ representatives on supervisory boards. This involves incorporating workers’ representatives in the traditional company board structure, where they are in a minority (although sometimes, as in Germany, a numerous one). It does not necessarily imply participation in the active management of the company and the workers’ representatives have the same status as other board members. This means they are to put the interests of the company first and foremost and are bound by the same duty of secrecy as other board members. Holding positions on the board may provide access to additional information, however, and a number of trade unions have sought the right to have workers’ representatives on boards. It is a phenomenon now seen in Eastern and Western Europe and North America, but remains rather rare elsewhere.
Another expression of workers’ participation is as owners of shares in limited liability companies or corporations. Sometimes workers are able to scrape enough capital together to purchase a firm that would otherwise be going out of business. The rationale behind these situations is that a worker who identifies financially with a company will work harder for its success. Important variables are the form of participation (return on investment rights or control rights), its degree (amount and timing of returns) and the reasons behind financial participation. In any event, these practices are largely reserved to Europe and North America. If cooperative ventures are considered part of this phenomenon, however, the notion of workers being stakeholders in their work is much more widespread throughout the world. It would be interesting to study whether and to what extent employee ownership of a firm or of shares in it has an effect on the workplace safety and health record.
Health and Safety Committees and Representatives
A specialized form of workers’ participation is seen in the development of health and safety committees and health and safety representatives (for worker participation in Denmark, see also "Case Study: Denmark"). The legislation of a number of countries provides for the establishment of such committees and for such representatives (e.g., Belgium, several provinces of Canada, Denmark, France, the Netherlands, Sweden). Smaller companies, variously defined, are usually excluded from such mandatory measures, but they, like larger units, often set up health and safety committees on their own initiative. In addition, many collective bargaining agreements have led to the creation of such committees and to the designation of health and safety representatives (e.g., in Canada and the United States).
Often, collective bargaining agreements will strengthen the legislatively guaranteed powers afforded to workers’ safety and health representatives. The committees and representatives vary in regard to their relationship to trade unions and works councils, their election or appointment, their duties and functions and their impact. As a form of workers’ involvement in the specialized sphere of health and safety, such committees and representatives can be a contributing factor to improving both working conditions and the labour relations climate. They have been most successful when they form an integral part of management’s safety and health programme, have access to adequate information, involve rank-and-file workers in their activities to help ensure continuity and are backed up by effective government labour inspection. Where employers maintain occupational health services or have safety experts, a fruitful relationship with them can also promote the success of joint health and safety committees. A recent workplace survey in the United Kingdom, for instance, found that “joint consultative committees, with all employee representatives appointed by unions, significantly reduced workplace injuries relative to those establishments where the management alone determines health and safety arrangements” (Reilly, Paci and Holl 1995). They also reported an important role for joint consultative committees where employee representatives were appointed in other ways. However, some research also indicates that joint health and safety committees fall short of the expectations held out for them. The reasons suggested for this differ: insufficient support from management, participants who are not adequately informed or trained, workers not represented forcefully enough and so on.
Workers’ health and safety representatives may be appointed by management (as in many workplaces where no trade union is present), designated by the trade union (as in the United Kingdom) or elected directly by the workers at the enterprise or higher level (as in Denmark). A parallel system will be used for worker representatives on a joint labour-management health and safety committee which, while bipartite, will not always have equal representation from both sides. General institutions for workers’ representation are often complemented by special representative structures for health and safety (as in Spain). The mechanism chosen will often reflect the existence of other labour relations institutions in a country: in France, for instance, employee members of the joint health, safety and working conditions committees are appointed by a delegate elected from the works committee and staff representatives; in Germany, members designated by the works council will be among those serving on a joint health and safety committee. Works councils in the Netherlands may delegate their powers to a safety, health and welfare committee. A strong link, if not identity, between trade union representatives and health and safety representatives is usually seen as desirable (as in Quebec (Canada), Ireland, Norway and Sweden), but where trade union density is low this runs the risk of depriving large numbers of workers of representation rights in relation to health and safety. Speculation that joint health and safety committees might lead to extending greater workers’ participation to other fields has remained largely unfounded.
Workers’ health and safety representatives normally have the following rights: to have access to information on health and safety and the introduction of new technology, to be consulted on these matters, to be involved in monitoring workplace conditions, to accompany inspectors (sometimes called the “walkaround right”), to be involved in accident investigations and to make recommendations to management on the improvement of working conditions. In some countries their powers go beyond this to include the right to engage in co-decision making, to initiate inspections and accident investigations and to review management’s reports to government. Most importantly, some workers’ health and safety representatives are empowered to order the shut-down of an imminently hazardous operation (also called “red-tagging”, for the marker placed on the spot), as in Denmark, Finland, Norway and Sweden. They are in certain instances, such as in France and some provinces of Canada, directly involved in the enforcement of health and safety regulations. Prior consultation of the joint committee is sometimes necessary before an employer can make any significant change in health, safety or working conditions (as in France and the Netherlands). In Belgium intercompany health services are under the control of a joint committee. In Italy the committees’ role includes the promotion of prevention, and in Greece they can, with the employers’ agreement, call for expert opinions on health and safety questions.
Workers’ health and safety representatives necessarily enjoy protection from discrimination or retaliation in the exercise of their functions. They are entitled to at least some time off with pay, as well as to have the necessary means (the definition of which is often debated) to exercise their functions. In addition, while in office some are specially shielded from economic layoffs (redundancies) or given extra protection from dismissal (as in Belgium). Frequently, worker health and safety representatives have a right to receive specialized training (as in Denmark).
The effect that workers’ health and safety representatives and joint committees can have will of course depend not only on rights and duties set out in legislation or in a collective bargaining agreement, but on how they are exercised in practice. This is in turn influenced by factors that affect workers’ participation generally. Such representatives and joint committees are no substitute for the effective government enforcement of health and safety standards or for what may be achieved by means of collective bargaining. However, “most observers believe that [mandated joint health and safety] committees provide a more efficient regulatory regime for safety and health than inspectorate or civil liability schemes” (Kaufman and Kleiner 1993). In any event, the trend is definitely towards greater workers’ participation in health and safety matters, at least in terms of collective agreements covering larger enterprises and legislation. Where they operate as effective institutions, joint health and safety committees can be a valuable tool for identifying problems and raising awareness of hazards, thus potentially reducing the incidence of injury, disease and death on the job. The extent to which they are effective, however, depends on a large range of variables in the particular labour relations system and in the strategic approach taken to health and safety at the workplace.
Evaluation
Schregle (1994) has commented:
In practice, none of these workers’ participation schemes has produced the expected results. There are many reasons for this. One is that, in a general way, trade unions and employers do not have the same view of participation. While it is the workers’ desire to exert a tangible and concrete influence on employers’ decisions in the sense of power-sharing, employers insist on management rights or management prerogatives, derived from private ownership, to run the business according to their own criteria and decision-making power, affording to workers at most the right to express their views and positions without binding effect on management. The result of all this is confusion over such terms as consultation, workers’ participation, workers’ participation in management, co-determination, co-management, etc.
The fact remains that in most workplaces around the world, there is little effective employee participation at the enterprise level. The first level of participation and indeed a prerequisite for it, is the provision of information, followed by consultation. Within Europe, research has indicated a wide variation in the extent of implementation of the 1989 framework directive on health and safety, when it comes to workers’ participation; it may get a new lease on life with the impetus of the 1995 directive on European works councils. A high degree of non-participation also characterizes other regions. Nevertheless, high hopes continue to be held out for strengthening mechanisms for workers’ participation at the enterprise level.
The traditional approach to workers’ participation as promotional of greater worker-management cooperation falls short of being satisfactory in relation to health and safety issues, where the categorization of labour relations as conflictual or cooperative does not particularly advance the debate. As Vogel (1994) notes:
...the problem of worker participation is clearly not confined to the institutionalized forms of participation in or outside the undertaking. The basis of participation lies in the recognition that distinct interests are in play giving rise to specific rationales... The essential legitimacy of participation is to be found outside the firm in a democratic requirement which refuses to admit that the self-determination of individuals should be confined within the rules of political representation and in a view of health conceived as a purposeful, social process through which individuals and communities develop strategies for self-fulfilment and defence.
In the end, the differing functions of various workers’ participation schemes make it difficult to assess their comparative impact. As collective bargaining shrinks in coverage, however, greater use of management-led workers’ participation arrangements may be expected.
National Level Tripartite and Bipartite Cooperation on Health and Safety
Cooperation between workers, employers and government in the elaboration and implementation of occupational health and safety measures at the national or regional level is common in a significant number of countries. It is not unusual for interest groups and technical experts also to be involved in this process. Such cooperation is highly developed and has been institutionalized in a number of countries by the establishment of consultative and collaborative organizations. These organizations have normally been widely accepted by all labour market participants as there appears to be a general consensus that health and safety at work is a subject of common concern where dialogue between the social partners, the government and other interested parties is extremely important.
The institutions which have been established to facilitate this cooperation vary significantly in form. One approach is to establish consultative organizations either on an ad hoc or a permanent basis to give advice to the government on questions of occupational safety and health policy. The government is normally not obligated to follow the recommendations offered, but in practice they are difficult to ignore and are frequently taken into consideration in the elaboration of government policy.
The other approach is to have the social partners and other interested parties actively cooperate with the government in public institutions which have been established to implement occupational safety and health policy. Participation by non-governmental actors in public institutions with responsibility for health and safety questions at work is normally undertaken through the representation of employers’ and workers’ organizations and, in some cases, other parties, on the board of directors of the public institution concerned, although sometimes participation extends to the management and even the project level. In most cases these persons are nominated by the government on recommendation of the parties to be represented, although in some cases workers’ and employers’ organizations have the right to directly nominate their representatives to these collaborative institutions. Bodies at the national level (or regional, state or provincial level) are normally complemented by structures or arrangements at the industry, enterprise and plant level.
Advice on Policy and Standard Setting
Probably the most common form of cooperation involves the establishment of consultative organizations to give advice on policy and standard setting. Examples of this can vary between a modest approach, which involves the expenditure of relatively few resources, to more institutionalized approaches, which involve more significant amounts of resources. The United States is an example of a country where a more limited approach has been adopted. At the federal level, the National Advisory Committee on Occupational Safety and Health, established pursuant to the Occupational Safety and Health Act of 1970, is the principal permanent advisory committee. This committee, according to the Act, is to be composed of representatives of management, labor, occupational safety and health professionals and the public, with a member of the public acting as the chairperson. The committee makes recommendations to the Secretary of Labor and the Secretary of Health and Human Services. In practice, however, this committee has not met frequently. The members of the committee are not compensated and the Secretary of Labor has provided from its budget an executive secretary and other support services as needed. The costs of maintaining this committee in existence are therefore very low, although budgetary constraints now call even this support into question. A permanent committee of a similar character, the Federal Advisory Council on Occupational Safety and Health, was established in July 1971 pursuant to Executive Order 11612 to advise the Secretary of Labour on matters relating to the safety and health of federal workers.
The Occupational Safety and Health Act of 1970 also provides for the establishment of ad hoc advisory committees to assist in standard-setting functions. These advisory committees are appointed by the Secretary of Labor and are to consist of no more than 15 members, including one or more persons who are designated by the Secretary of Health and Human Services. Each standard-setting committee is to include an equal number of representatives of workers’ and employers’ organizations. The Secretary of Labor may also appoint one or more representatives of state health and safety agencies, as well as technical experts who could be, for example, representatives of professional organizations of technicians or professionals specializing in occupational health or safety, or of nationally recognized standards-producing organizations. Extensive use has been made of such standard-setting committees, which are sometimes in existence several years to accomplish the work that has been assigned to them. Meetings can be frequent, depending on the nature of the tasks to be performed. Although committee members are normally not paid, they are normally reimbursed for reasonable travel expenses and support services for the activity of these committees have been paid for by the Department of Labor as well in the past. Committees have been constituted to recommend standards with respect to agriculture, asbestos dust, carcinogens, coke oven emissions, cutaneous hazards, hazardous materials labelling, heat stress, marine terminal facilities, noise, longshoring safety and health, shipyard employment standards and steel erection rules, among other things.
Other ad hoc advisory committees of a similar character have been established pursuant to similar legislation which falls under the authority of the Secretary of Labor. For example, a number of standard-setting committees have been established pursuant to the Federal Mine Safety and Health Act of 1977. The costs involved in the establishment of such standard-setting committees, however, are relatively modest and are characterized by relatively low administrative costs, little infrastructure, voluntary participation by outside parties without compensation and dissolution of the committees upon completion of their tasks.
More elaborate institutionalized forms of consultation are, however, found in other countries. In the Netherlands, for example, the pre-eminent organization is the Working Environment Council, which was established pursuant to the Working Environmental Council Act 1990. The Council gives its views to the Ministry of Social Affairs and Employment, either when asked or on its own initiative, comments on proposed new acts and decrees and can bring forward its own proposals for new policy or legislation. The Council also gives its views about the advisability of making grants-in-aid for research on working environment issues, about the issuance of exemptions, the formulation of government guidance and the policy of the Labour Inspectorate. The Council is comprised of eight representatives from central employers’ organizations, eight from central workers’ organizations and seven from governmental bodies. Only the representatives of workers’ and employers’ organizations have the right to vote, however, and the chairperson of the Council is independent. The Council meets every month. In addition, the Council has approximately 15 different working committees for specific issues and, in addition, ad hoc working groups are established for detailed subjects when the subject matter justifies it. Within the working committees and working groups, external experts play an important role and these working organizations prepare reports and papers which are discussed at Council meetings and often form the basis for positions which are subsequently taken. The recommendations of the Council are comprehensive and are published. Although normally the parties try to achieve a consensus position, separate views can be expressed to the Minister of Social Affairs and Employment when employers’ and workers’ representatives cannot find common ground. More than 100 persons are involved in the work of the Council and its subsidiary organizations and thus it is supported by significant financial and administrative resources.
Other less prominent consultative organizations exist in the Netherlands for more specific occupational safety and health issues. These include the Foundation for the Working Environment in Building Construction, the Foundation for Health Care in Agriculture, the Commission for the Prevention of Disasters by Dangerous Substances and the Commission for the Labour Inspectorate and Enforcement Policy.
Examples of other countries which have consultative organizations of a bipartite, tripartite or multipartite character to give recommendations on occupational safety and health policy and standards include: Canada (ad hoc committees on legislative reform and standard setting – federal level; Forum for Action on Workplace Health and Safety – Alberta; Joint Steering Committee on Hazardous Substances in the Workplace – Ontario; Back Injury Prevention Advisory Committee – Newfoundland; Occupational Health and Safety Council – Prince Edward Island; Advisory Council on Workplace Safety and Health – Manitoba; Occupational Health and Safety Council – Saskatchewan; Logging Safety Forum – British Columbia); Denmark (Working Environment Council); France (the Central Council for the Prevention of Occupational Risks and the National Commission of Occupational Health and Safety in Agriculture); Italy (Permanent Consultative Commission for the Prevention of Work Accidents and Occupational Health); Germany (Advisory Board to the Federal Institute for Occupational Safety and Health); and Spain (General Council of the National Institute for Occupational Safety and Health).
Policy Implementation
A number of countries have bipartite, tripartite or multipartite organizations which are also active in policy implementation. These collaborative organizations normally are public establishments which incorporate representatives of employers’ and workers’ organizations and in some cases other persons or interest groups, in both policy making and policy implementation. Normally far larger than advisory committees, councils or commissions, these collaborative organizations have responsibility for implementing government policy, frequently manage large budgetary resources and often have significant numbers of personnel.
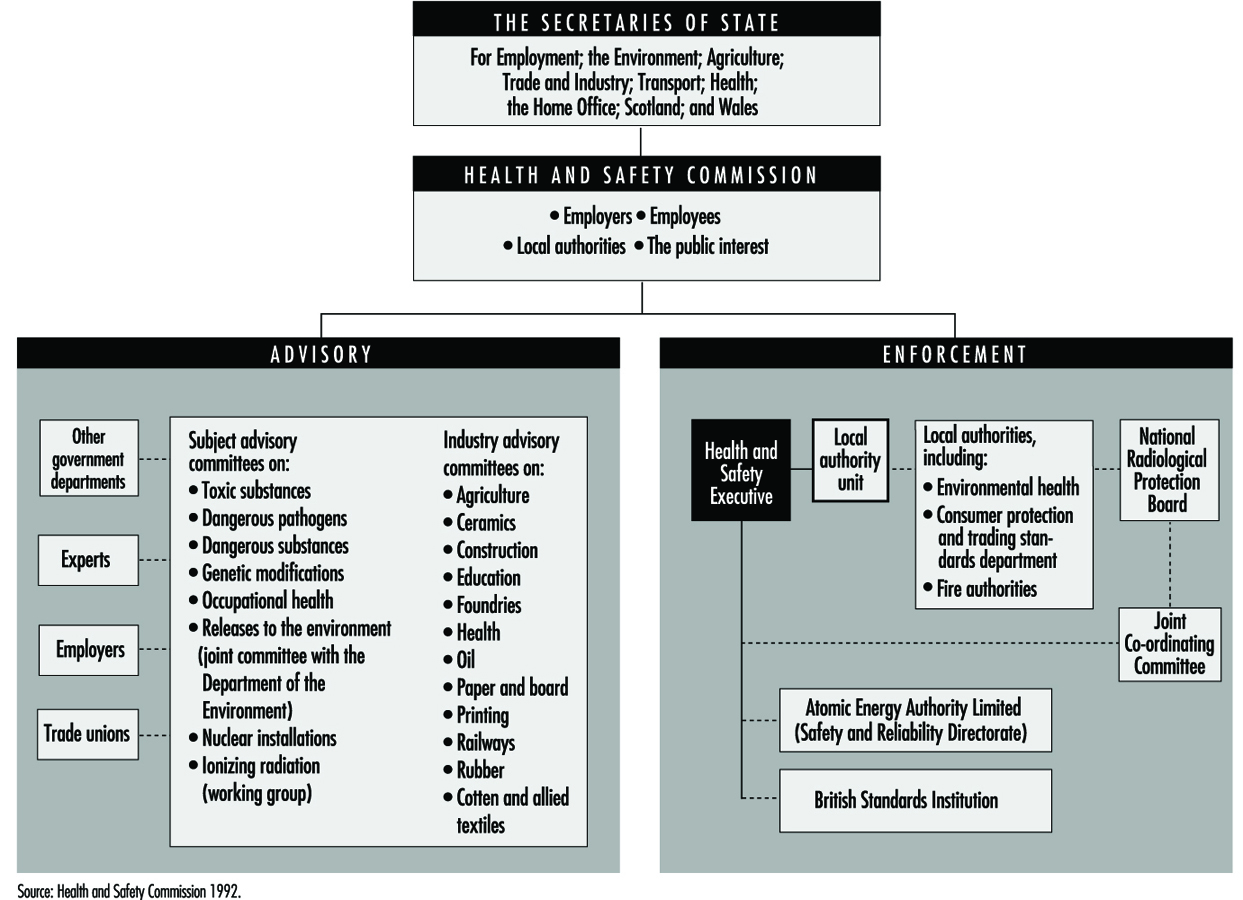
An example of such an organization is the Health and Safety Commission in Great Britain. The Commission was established pursuant to the provisions of the Health and Safety Act 1974. It has as its mandate to ensure that adequate measures are taken to secure the health, safety and welfare of persons at work; to protect the public against risks to health and safety arising out of work; to control storage and use of explosives, highly flammable materials and other dangerous substances; and to control the emission of noxious or offensive substances from the workplace. It is responsible to the Secretary of State for Education and Employment, but also to other Secretaries of State, including those of Trade and Industry, Transport, Environment and Agriculture. The Commission has nine persons, all of whom are appointed by the Secretary of State for Education and Employment. It consists of a chairperson, three members appointed after consultation with the principal central employers’ organization, three members appointed after consultation with the principal central workers’ organization and two members appointed after consultation with local authority associations.
The Commission is assisted by a number of subsidiary organizations (figure 1). The most important of these is the Health and Safety Executive, a distinct statutory body which consists of a governing body of three persons appointed by the Commission with the approval of the Secretary of State for Education and Employment. The Health and Safety Executive is responsible for carrying out the substantive work of the Commission, including the enforcement of health and safety standards under the Health and Safety Act 1974 and other functions delegated to it by the Commission. Local authorities also perform enforcement functions with respect to certain health and safety legislation as well. In addition, the Commission is assisted in its work by a number of advisory committees which are, depending on the committee, bipartite, tripartite or multipartite in character. These advisory committees are organized both by subject matter and industry. There are advisory committees for each of the following subjects: toxic substances, dangerous pathogens, dangerous substances, genetic modifications, occupational health, releases to the environment, nuclear installations and ionizing radiation. There are also advisory committees for the following industries: agriculture, ceramics, construction, education, foundries, health, petroleum, paper and board, printing, railways, rubber, cotton and textiles. Subject matter committees tend to have between 12 and 18 members plus a chairperson and are multipartite in character, frequently including technical experts as well as representatives of central workers’ and employers’ organizations, government and other interest groups. Industry committees, however, tend to be bipartite, with approximately 12 members drawn in equal numbers from central workers’ and employers’ organizations and with the chairperson being from the government. The resources at the disposition of the Commission and the Health and Safety Executive are substantial. For example, in 1993 these organizations together had approximately 4,538 staff members and a budget of £ 211.8 million.
Figure 1. Health & safety in Great Britain: the main institutions
Other examples of collaborative organizations in this field can be found in Canada. At the federal level, the Canadian Centre for Occupational Health and Safety is Canada’s main resource for information on this topic. The Centre also promotes health and safety in the workplace, facilitates the establishment of high standards of occupational health and safety and assists in the development of programmes and policies to reduce or eliminate occupational hazards. The Centre, created by an act of parliament in 1978, was given a tripartite governing body to ensure its impartiality in occupational health and safety matters, including being an unbiased source of information. Its governing council consists of a chairperson and 12 governors – four representing the federal, provincial and territorial governments; four representing labour; and four representing employers. The Centre manages significant human and financial resources and its total expenditures in 1993 were approximately C$8.3 million.
In some provinces there are also collaborative organizations. In Quebec, two prominent organizations are the Commission for Occupational Health and Safety and the Institute of Occupational Health and Safety Research. The Commission has two functions. The first is to develop and implement occupational health and safety policy, including the establishment of standards and their enforcement; the provision of support for the implementation of prevention programmes, participation mechanisms and health services; and the provision of training, information and research services. The second is to provide payment to workers injured on the job and to manage an insurance fund for this purpose to which employers must contribute. The Commission, which was established by law in 1981 and which succeeded the Commission of Occupational Accidents founded in 1931, has a bipartite board of directors which is composed of seven workers’ representatives, seven representatives of employers and a chairperson. The representatives of workers’ and employers’ organizations are chosen from lists supplied by the most representative labour and employer organizations. The Commission manages large human and financial resources and at the end of 1992 had expenditures of C$2,151.7 million and employed 3,013 persons as permanent staff and 652 as casual employees.
Quebec’s Institute of Occupational Health and Safety Research, founded in 1980, has as its mandate to contribute, through scientific research, to the identification and the elimination of sources of workplace hazards, as well as to the readaptation of workers who have suffered workplace injuries. The board of directors of the Institute is the same as that of the Commission for Occupational Health and Safety, notwithstanding that it is an independent institution. The Institute also has a scientific council which has advisory functions and is composed of four representatives of workers’ organizations, four from employers’ organizations, six representatives of the scientific and technical community and the Institute’s Director General. In 1992, the Institute had expenditures of C$17.9 million and approximately 126 employees.
The Ontario Workplace Health and Safety Agency, established in 1990 by amendment of the Occupational Health and Safety Act, also has responsibility for developing and implementing policy and for managing occupational health and safety programmes in Ontario. The governing body of the organization consists of a bipartite board of 18 persons with nine representatives each from workers’ and employers’ organizations. Of these representatives, one representative of labour and one of management serve as joint chief executive officers. The resources of this organization are substantial – total expenditures amounted to C$64.9 million in 1992.
One country with a long tradition of collaborative organizations in the field of occupational safety and health, Sweden, decided to reject this form of organization in 1992 and has subsequently used advisory organizations instead. It should be added that this decision was not confined to occupational safety and health, but included all collaborative organizations of any kind in which representatives of workers’ and employers’ organizations played a decision-making role at the national level. The impetus for this change came from the principal employers’ organization, which decided unilaterally to withdraw from participation in collaborative public institutions. The central employers’ organization argued that interest groups should not have political responsibility in terms of managing public institutions, but that the government and parliament should have this political role and responsibility; that the role of the employers’ organization was to represent its members’ interests, and that this role could be in conflict with a duty to serve the interests of the public institutions if the employers’ organization was represented on the governing boards of such institutions; and that participation weakened democracy and the development of public institutions. Although workers’ organizations were not in agreement with the employers’ organizations on these points, the government concluded that collaborative bodies with no representation from the principal employers’ organization were impractical and decided to have representation by workers’ and employers’ organizations as well as other interest groups only on advisory bodies. Hence, organizations in the field of occupational safety and health such as the National Board of Occupational Safety and Health, the National Institute of Occupational Health and the Working Life Fund, which had formerly been collaborative in character in terms of a tripartite or multipartite governing board, were restructured.
Although collaborative organizations in most countries are more rare than advisory organizations, which are quite widespread, the case of Sweden’s rejection of collaborative institutions, at least in the field of occupational safety and health, appears to be an isolated one. Although some collaborative institutions, dealing notably with questions of economic policy, training and employment, were dismantled in Great Britain during the 1980s and 1990s by successive conservative governments, the Health and Safety Commission was not affected. Some have advanced that this is because occupational safety and health is a subject of common concern to employers’ and workers’ organizations as well as the government and other interested parties and therefore there is a strong interest by all parties in finding a consensus in both policy formulation and implementation. Also, in Canada such collaborative institutions have been created at both the federal level and in some provinces precisely because a collaborative approach was deemed more useful in finding a consensus between the labour market parties and because administration of the occupational safety and health laws would appear more impartial and fair to those affected by them.
On a broader level, however, there are two national consultative bodies which are also concerned with occupational safety and health issues as part of their more general mandate to address all important social and economic questions of national importance. In the Netherlands, the Labour Foundation, established in May 1945, is a bipartite organization jointly managed by equal numbers of representatives from central employers’ and workers’ organizations (including farmers) and has a significant role as an advisory body to the Government. Although historically its main function has concerned questions of wage policy, it also expresses its views on other conditions of work. The other national consultative body of importance is the Social and Economic Council, which was founded in 1950 pursuant to the Act on Statutory Trade Associations. The tripartite Council consists of 15 representatives of central employers’ organizations, 15 representatives of central workers’ organizations and 15 independent experts. The employers’ and workers’ representatives are appointed by their organizations and the independent experts are appointed by the Crown. In making its appointments, the Crown also tries to have a balance between the major political parties. The Council is independent of the government and is financed by a mandatory tax on employers. The Council has a multimillion dollar budget and its own Secretariat. The Council normally meets once a month and is assisted by a number of permanent and ad hoc committees, which are frequently also constituted on a tripartite basis. The government is required by law to submit all proposals for social and economic legislation to the Council for its advice and any labour legislation – which would include proposals concerning occupational safety and health – comes before the Council.
It should be added that a number of countries require that workplace health and safety committees should or may be established for enterprises which have more than a certain number of employees. These committees are bipartite in nature and include representatives of the employers and the workers. These committees normally have as their function to investigate and propose all ways and means of actively contributing to measures undertaken to ensure the best possible health and safety conditions in the establishment, a role which can include the promotion and monitoring of health and safety conditions in the enterprise to ensure, among other things, adherence to applicable law and regulations. These joint committees are normally advisory in character. Workplace health and safety committees, for example, are legally required in Belgium, Canada, France, Germany, the Netherlands and Spain.
Collective Bargaining and Safety and Health
Collective bargaining is the process through which workers negotiate, as a group, with their employer; this can occur at various levels (enterprise, industry/sector, national). Traditionally, the subjects of the negotiation are wages, benefits, working conditions and fair treatment. However, collective bargaining can also address issues that do not directly affect the workers employed in the enterprise, such as increased old-age pensions for workers already retired. Less often, collective bargaining addresses issues that reach well beyond the workplace, such as protection of the external environment.
In a very small enterprise, it is possible for all the workers to negotiate as a body with their employer. This kind of informal collective bargaining has existed for centuries. Today, however, most collective bargaining is carried out by workers’ organizations, or unions.
The definition used in the ILO Convention concerning the promotion of collective bargaining, 1981 (No.154), Article 2, is broad:
...the term... extends to all negotiations which take place between an employer, a group of employers or one or more employers’ organizations, on the one hand, and one or more workers’ organizations, on the other, for –
(a) determining working conditions and terms of employment; and/or
(b) regulating relations between employers and workers; and/or
(c) regulating relations between employers or their organizations and a workers’ organization or workers’ organizations.
Collective bargaining is an important tool for raising living standards and improving working conditions. Even though safety and health is addressed in the national law of almost all countries, collective bargaining often provides the mechanism through which the law is implemented in the workplace. For example, the law may mandate joint safety and health committees or works councils, but leave the details to be negotiated between the employer and the workers’ organization.
Unfortunately, collective bargaining is under attack by authoritarian employers and repressive governments, both in developed and developing countries. It rarely exists in the informal sector or in small, traditional enterprises. As a result, the majority of the world’s workers do not yet enjoy the benefits of effective collective bargaining under a framework of worker rights guaranteed by law.
History of Union Action for Safety and Health
There is a long history of workers’ organizations taking collective action for safety and health. In 1775, Percival Pott, an English surgeon, made the first known report of occupational cancer – skin cancer in London chimney sweeps (Lehman 1977). Two years later the Danish Chimney Sweepers Guild, in what was the first known response by a workers’ organization to the threat of occupational cancer, ordered that apprentices be given the means for a daily bath.
The Labour Agreement between the Bethlehem Steel Corporation and the United Steelworkers of America
The agreement between Bethlehem Steel and the United Steelworkers of America is typical of company-wide agreements in large unionized manufacturing enterprises in the United States. Steel industry labour agreements have contained safety and health articles for more than 50 years. Many provisions negotiated in the past gave workers and the union rights that were later guaranteed by law. Despite this redundancy, the provisions still appear in the contract as a hedge against changes in the law, and to allow the union the option of taking violations to impartial arbitration rather than the courts.
The Bethlehem agreement runs from 1 August 1993 to 1 August 1999. It covers 17,000 workers in six plants. The full agreement is 275 pages long; 17 pages are devoted to safety and health.
Section 1 of the safety and health article pledges the company and the union to cooperate in the objective of eliminating accidents and health hazards. It obligates the company to provide safe and healthful workplaces, obey federal and state law, provide employees with the necessary protective equipment free of charge, provide chemical safety information to the union and inform workers of the hazards and controls for toxic substances. It grants the union’s central safety and health department the right to any information in the company’s possession that is “relevant and material” to an understanding of potential hazards. It requires the company to make air sampling tests and environmental investigations at the request of the union co-chairperson of the plant’s safety and health committee.
Section 2 sets up joint union-management safety and health committees at the plant and national levels, prescribes the rules under which they operate, mandates training for committee members, gives members of the committee access to all parts of the plant to facilitate the committee’s work and specifies the applicable rates of pay for committee members on committee business. The section also specifies how disputes over protective equipment are to be resolved, requires the company to notify the union of all potentially disabling accidents, sets up a system of joint accident investigation, requires the company to gather and supply to the union certain safety and health statistics, and establishes an extensive safety and health training programme for all employees.
Section 3 gives workers the right to remove themselves from work involving hazards beyond those “inherent in the operation” and provides an arbitration mechanism through which disputes over such work refusals can be resolved. Under this provision, a worker cannot be disciplined for acting in good faith and on the basis of objective evidence, even if a subsequent investigation shows that the hazard did not in fact exist.
Section 4 specifies that the committee’s role is advisory, and that committee members and officers of the union acting in their official capacity are not to be held liable for injuries or illnesses.
Section 5 states that alcoholism and drug abuse are treatable conditions, and sets up a programme of rehabilitation.
Section 6 establishes an extensive programme for controlling carbon monoxide, a serious hazard in primary steel production.
Section 7 provides workers with vouchers for the purchase of safety shoes.
Section 8 requires the company to keep individual medical records confidential except in certain limited circumstances. However, workers have access to their own medical records, and may release them to the union or to a personal physician. In addition, physicians for the company are required to notify workers of adverse medical findings.
Section 9 establishes a medical surveillance programme.
Section 10 establishes a programme for investigating and controlling the hazards of video display terminals.
Section 11 establishes full-time safety representatives in each plant, chosen by the union but paid by the company.
In addition, an appendix to the agreement commits the company and the union to review each plant’s safety programme for mobile equipment operating on rails. (Fixed rail equipment is the leading cause of death by traumatic injury in the American steel industry.)
However, safety and health seldom was an explicit issue in early labour struggles. Workers in dangerous jobs were overwhelmed by more pressing problems, such as low wages, crushing hours of work and the arbitrary power of factory and mine owners. Safety hazards were obvious in the daily toll of injury and death, but occupational health was not well understood. Workers’ organizations were weak and under constant attack by owners and governments. Simple survival was the primary goal of workers’ organizations. As a result, the grievances of nineteenth-century workers rarely manifested themselves in campaigns for safer conditions (Corn 1978).
However, safety and health sometimes joined other issues in early labour struggles. In the late 1820s, workers in the textile industry in the United States began to agitate for shorter working hours. Many of the workers were women, as were the leaders of such rudimentary unions as the female labour reform associations of New England. The proposed 10-hour day was seen mostly as an issue of general welfare. But in testimony before the Massachusetts legislature, workers also decried the effects of 12- and 14-hour days in badly ventilated mills, describing a “wasting sickness” they attributed to cotton dust and bad ventilation, in what are now recognized as some of the first reports of byssinosis. They had little success in winning recognition from the mill owners, or action from the legislature (Foner 1977).
Other union actions dealt more with the effects of occupational hazards than with their prevention. Many nineteenth-century unions adopted welfare programmes for their members, including disability payments to the injured and benefits for survivors. US and Canadian mining unions went one step further, establishing hospitals, clinics and even cemeteries for their members (Derickson 1988). While unions attempted to negotiate better conditions with employers, most agitation for safety and health in North America was in mines aimed at state and provincial legislatures (Fox 1990).
In Europe, the situation began to change around the turn of the century with the rise of stronger workers’ organizations. In 1903, the German and French painters’ unions began a campaign against the hazards of lead paint. The Factory Workers Union of Germany had an active industrial hygiene programme by 1911, published education materials on chemical hazards and began a campaign for safeguards against chromate-induced lung cancer, ultimately leading to a change in the production method. Trade unions in the United Kingdom represented their members in workers’ compensation cases and fought for better laws and regulations. Their work showed the interplay between collective bargaining for safety and health and the factory inspection system. In 1905, for example, trade unions filed 268 complaints with the British factory inspectorate (Teleky 1948). As early as 1942, the Swedish Employers’ Confederation and the Swedish Confederation of Trade Unions reached a nationwide Working Environment Agreement regarding local safety and health services. The agreement has been revised and extended several times; in 1976 the original parties were joined by the Federation of Salaried Employees (Joint Industrial Safety Council of Sweden 1988).
North America lagged behind. Formal corporate safety programmes were instituted by some large employers around the turn of the century (for a description of such programmes in the steel industry see Brody (1960), or the self-congratulatory Year Book of the American Iron and Steel Institute for 1914 (AISI 1915)). The programmes were highly paternalistic, relied more on discipline than education and often were based on the premise that workers themselves were largely to blame for industrial accidents. Major disasters such as New York’s 1911 Triangle Shirtwaist Fire, which killed 146 workers, led to union campaigns for improvement and ultimately to improved fire safety laws. However, safety and health as a widespread labour issue came only with the rise of strong unions in the 1930s and 1940s. In 1942, for example, the founding Constitution of the United Steelworkers of America required every local union to establish a safety and health committee. By the mid-1950s, joint labour-management safety and health committees had been established in most unionized mines and manufacturing plants and in many other workplaces in the construction and service sector; most union contracts included a section on safety and health.
Process of Collective Bargaining
It is common to think of collective bargaining as a formal process that occurs at regular intervals and which results in a written agreement between the workers’ organization and the employer or employers. This kind of bargaining presupposes a succession of demands or proposals, counterproposals and extended deliberations. The process can produce a variety of results: a collective bargaining contract, letters of understanding, joint declarations or mutually agreed codes of practice.
However, collective bargaining can also be understood as a continuous process for solving problems as they arise. This kind of collective bargaining occurs every time a shop steward meets with an area supervisor to settle a dispute or grievance, every time a joint safety and health committee meets to discuss problems in the plant, every time a joint union-management team considers a new company programme.
It is this flexibility of collective bargaining which helps ensure its continued viability. There is, however, one precondition for formal or informal bargaining: for negotiations to be a success, the representatives of both sides must have the authority to bargain and to strike a deal that is meant to be honoured.
Collective bargaining is sometimes seen as a test of strength, in which a gain for one side is a loss for the other. A wage increase, for example, is seen as a threat to profits. A no-layoff agreement is seen as limiting management’s flexibility. If bargaining is seen as a contest, it follows that the most important determinant of the final outcome is the relative power of the parties. For the workers’ organization, this means the ability to halt production through a strike, organize a boycott of the employer’s product or service or bring some other form of pressure to bear, while maintaining the loyalty of the organization’s members. For an employer, power means the ability to resist such pressures, replace the striking workers in countries where this is permitted or hold out until hardship forces workers back to the job under management’s conditions.
Of course, the vast majority of labour negotiations end successfully, without a work stoppage. Nevertheless, it is the threat of one that leads both sides to seek a settlement. This kind of negotiation is sometimes called positional bargaining, because it begins with each side taking a position, after which both sides move by increments until a compromise is reached, based on their relative strengths.
A second model of collective bargaining describes it as a mutual search for an optimum solution (Fisher and Ury 1981). This kind of bargaining assumes that a proper agreement can lead to gains for both parties. A wage increase, for example, can be offset by greater productivity. A no-layoff agreement can encourage workers to improve efficiency, since their jobs will not be threatened as a result. Such bargaining is sometimes called “mutual gains” or “win-win” bargaining. What is most important is the ability of each side to understand the interests of the other and to find solutions that maximize both. Occupational safety and health is frequently seen as an ideal subject for mutual gains bargaining, since both sides are interested in avoiding occupational accidents and disease.
In practice, these models of bargaining are not mutually exclusive and both are important. Skilled bargainers will always seek to understand their counterparts and search for areas where both sides can benefit from a wise agreement. However, it is unlikely that a party without power will accomplish its objectives. There will always remain areas where the parties perceive their interests to be different. Good faith negotiation works best when both sides fear the alternative.
Power is important even in negotiations over safety and health. An enterprise may be less interested in reducing the accident rate if it can externalize the cost of the accidents. If injured workers can be replaced easily and cheaply, without substantial compensation, management may be tempted to avoid expensive safety improvements. This is especially true in the case of occupational diseases with long latency periods, where cost of controls is paid when the controls are installed, while the benefits may not accrue for many years. As a result, a workers’ organization is more likely to succeed if workers have the power to stop production or to call a government inspector if the parties fail to negotiate a solution.
Legal Framework
ILO Conventions on freedom of association, on protection of the rights to organize and to engage in collective bargaining and the ILO Conventions and Recommendations on occupational safety and health recognize the role of workers’ organizations. While these instruments provide an international framework, workers’ rights can be assured only through national law and regulation.
Of course, the legal basis for collective bargaining, the level at which bargaining occurs and even the process of bargaining all vary by country. The legislation of most industrialized countries includes a system for regulating collective bargaining. Even within Europe, the degree of regulation can differ widely, from a minimal approach in Germany to a much more developed one in France. The legal effect of a collective agreement also varies. In most countries an agreement is legally enforceable; in the United Kingdom, however, agreements are seen as informal, to be applied by virtue of the parties’ good faith backed up by the threat of a work stoppage. It is expected that this variability within Europe will diminish as a result of greater European unification.
The level of bargaining also varies. The United States, Japan and most Latin American countries feature bargaining at the level of the individual enterprise, although unions often attempt to negotiate “pattern” agreements with all the major employers in a given sector. At the other extreme, Austria, Belgium and the Nordic countries tend to have highly centralized bargaining in which most workplaces are subject to a framework agreement negotiated between national federations representing unions and employers. Sectoral agreements covering particular industries or occupations are common in some countries such as Germany and France.
French-speaking African countries tend to follow the example of France and bargain by industry. Some English-speaking developing countries also bargain by industry. In others, multiple trade unions bargain on behalf of different groups of workers in a single enterprise.
The level of bargaining partially determines the coverage of collective agreements. In France and Germany, for example, collective agreements are usually extended to cover everyone coming within the scope of the occupation or industry to which the agreement applies. On the other hand, in the United States and other countries with enterprise-level bargaining, collective agreements cover only those workplaces where the union has been recognized as the bargaining agent.
An even more important factor in determining the coverage of collective bargaining is whether national law facilitates or impedes unionization and collective bargaining. For example, public sector employees are not permitted to bargain collectively in some countries. In others, public sector unions are growing rapidly. As a result of such factors, the percentage of workers covered by collective agreements varies from a high of almost 90 per cent in Germany and the Nordic countries to under 10 per cent in many developing countries.
The legal framework also affects how collective bargaining applies to occupational safety and health. For example, the United States Occupational Safety and Health Act gives workers’ organizations the right to information on dangerous chemicals and other hazards in the plant, the right to accompany a workplace inspector and a limited right to participate in legal cases brought by the Government against an employer for a violation of standards.
Many countries go further. Most industrialized countries require most enterprises to establish joint safety and health committees. The Canadian Province of Ontario requires that certified safety and health representatives be chosen by the workers in most workplaces and given a standard course of training at employer expense. The Swedish Work Environment Act requires the appointment of safety delegates by the local trade union organization. Swedish safety delegates have broad rights to information and consultation. Most important, they have the power to suspend dangerous work pending a review by the Swedish Labour Inspectorate.
These laws strengthen the collective bargaining process on issues of safety and health. Mandatory joint safety committees provide a routine mechanism for negotiation. Training gives union representatives the knowledge they need to participate effectively. The right to suspend dangerous work helps keep both parties focused on eliminating the source of danger.
Contract and Labour Law Enforcement
Of course, labour agreements are of limited value without an enforcement mechanism. A strike is one method by which a workers’ organization can respond to an alleged violation by the employer; conversely, the employer can engage in a lockout, denying employment to members of the workers’ organization until the dispute is resolved. However, most labour agreements in developed countries rely on less disruptive methods of enforcement. In fact, many labour agreements bar strikes or lockouts during the life of the agreement (no-strike clauses or peace obligations). Some restrict them to a limited set of circumstances; for example, the contracts negotiated in the United States between the United Automobile Workers and the major auto companies allow strikes over unsafe working conditions, but not over wages or benefits during the term of the agreement.
A common enforcement mechanism in developed countries is a system of arbitration, in which disputes are referred to an impartial referee chosen jointly by the employer and the workers’ organization. In some cases, disputes may be resolved by the judicial system, either in the regular courts or in special labour courts or boards. In the United States, for example, a dispute over contract interpretation usually will go to arbitration. However, if the losing side refuses to abide by the arbitrator’s decision, the winning side can seek to have the decision enforced by the courts. A quasi-judicial body in the United States, the National Labor Relations Board, hears complaints concerning unfair labour practices, such as the failure of one side to bargain in good faith. In many other countries, labour courts fulfil this role.
Collective Bargaining Today
Collective bargaining is a dynamic process in all industrial relations systems where it is practised. The situation in Europe is changing rapidly. The Nordic countries are characterized by comprehensive working environment agreements negotiated on a national basis, integrated with highly developed national laws. Unionization is very high; labour agreements and the law establish joint committees and worker safety representatives in most workplaces. Collective bargaining mechanisms for safety and health and unionization rates, are less extensive in other European countries. Member States of the European Union face the task of harmonizing national laws under the Single European Act and the Framework Directive on safety and health (Hecker 1993). European trade unions are seeking to coordinate their efforts, primarily through the European Trade Union Confederation. There are some signs that national bargaining ultimately will be replaced or, more likely, supplemented by agreements at the European level, although employer resistance to this is high. The first example of such Europe-wide bargaining was over parental leave. In the area of safety and health, the GMB union in the United Kingdom has proposed an ambitious Europe-wide Work Environment Fund, based on similar funds in the Nordic Countries.
Central and Eastern Europe and the countries of the former Soviet Union, are changing even more rapidly. Safety and health regulations were extensive under Communism, but rarely enforced. Trade unions existed, but only under the control of the Communist Party. At the enterprise level, unions functioned as workplace labour relations departments, under the control of management, without any sort of bipartite negotiation. Newly formed independent unions helped precipitate the fall of Communism; sometimes their issues concerned working conditions or such basic sanitary measures as the provision of soap in coal mine wash houses. Today, the old unions are gone or are struggling to reconstitute themselves. The new independent unions are attempting to change from political organizations confronting the government, to collective bargaining organizations representing their members in the workplace. Bad and often deteriorating working conditions will continue to be an important issue.
The Japanese system of worker participation, continuous improvement and extensive training effectively promotes safety and health, but only where safety and health are explicit goals of the enterprise. Most Japanese unions exist only at the enterprise level; negotiations take place through a system of continuous joint consultation (Inohara 1990). Joint safety and health committees are established by the Labour Safety and Sanitation Law of 1972, as amended.
Labour agreements in the United States contain relatively extensive safety and health articles for two reasons. First, safety and health is an important issue for North American unions, as it is for workers’ organizations in all industrialized countries. However, safety and health laws in the United States lack many of the provisions found in the laws of other countries, forcing unions to bargain for rights and protections guaranteed elsewhere by law. For example, joint union-management safety and health committees are generally recognized as an important mechanism for day-to-day cooperation and negotiation between workers and employers. However, there is no requirement in the US Occupational Safety and Health Act for such committees. As a result, unions must bargain for them. And since the rate of unionization is low in the United States, most workers do not have access to joint committees. Many unions in the United States also have negotiated contract clauses barring retaliation against workers who refuse to work under abnormally hazardous conditions, since legal protections are weak and uncertain.
Canadian law varies from province to province, although it is generally stronger than in the United States. For example, unions in Canada do not need to negotiate for the existence of safety and health committees, although they may negotiate for larger ones, with more powers. Safety and health committees are also required under Mexican law.
The situation in developing countries is mixed. Workers’ organizations in developing countries like India, Brazil and Zimbabwe place a growing emphasis on safety and health through agitation for improved laws and through collective bargaining. For example, the Zimbabwe Congress of Trade Unions has fought to extend the national labour code, including its safety and health provisions, to the country’s export processing zones (see box). But trade unions are severely restricted or suppressed in many parts of the world and the vast majority of workers in developing countries do not belong to any workers’ organization or benefit from collective bargaining.
Trade Union Action in Zimbabwe
The Zimbabwe Congress of Trade Unions (ZCTU), has launched a National Campaign for the Rights of Injured Workers, which combines national level and shop floor action to seek amended laws and improved collective agreements.
Zimbabwean law has since 1990 provided for safety committees, health and safety representatives and health and safety supervisors at all workplaces. The Zimbabwe Congress of Trade Unions has insisted that worker health and safety representatives must be elected by workers. Its National Campaign covers these demands:
- Safe work. This involves identification of workplace hazards through surveys and accident investigation, as well as negotiating to improve conditions.
- Worker and union participation in workers’ health issues. This includes the rights of workers to elect their own health and safety representatives, to obtain information such as safety data sheets and factory inspector’s reports, and jointly to investigate and report accidents and injuries (as in Sweden).
- Adequate compensation and care for injured workers. This extends to a review of compensation levels.
- Job security for injured workers. Trade union representatives have negotiated a right to return to work and be assisted in placement.
For the ZCTU, a key step in accident prevention has been its training programme to increase effective worker participation in health and safety at the shop floor level. The training for worker representatives has been in carrying out walk-through surveys at workplaces and in reporting on any hazards identified - first to workers and then to management for discussion. Once in operation, union health and safety representatives have been involved in inspections and in ensuring that injuries are reported. This is particularly important in sectors that would otherwise be inaccessible, such as agriculture.
The ZCTU has also demanded an increase in penalties that may be imposed on employers found to have infringed health and safety laws.
by Chapter Editor (excerpted from Loewenson 1992).
The Future of Collective Bargaining
Workers’ organizations and collective bargaining face difficult challenges in the years ahead. Virtually all collective bargaining takes place at the enterprise, industry or national level. In contrast, the economy is increasingly global. Apart from Europe, however, workers’ organizations have yet to develop effective mechanisms for bargaining across national boundaries. Such bargaining is a top priority for international labour federations. It can best be promoted through stronger and more effective international union structures, strong social clauses in world trade agreements and appropriate international instruments, such as those of the International Labour Organization. For example, the ILO Tripartite Declaration on Multinational Enterprises refers specifically to both collective bargaining and occupational safety and health. Many unions are developing direct links with their counterparts in other countries in order to coordinate their bargaining and provide mutual assistance. One example is the relationship between mining unions in the United States and Colombia (Zinn 1995).
Rapid changes in technology and work organization can overwhelm existing labour agreements. Workers’ organizations are attempting to develop a form of continuous bargaining to respond to workplace change. Workers’ organizations have long recognized the links between the working environment and the external environment. Some unions have begun to address issues of the external environment in their collective bargaining agreements and in their membership education programmes. An example is the Model Environment Agreement proposed by the Manufacturing-Science-Finance (MSF) Union in the United Kingdom.
A fundamental purpose of trade unions is to take human rights and human welfare out of economic competition – to prevent an enterprise or a nation from seeking a competitive advantage by impoverishing its workers and forcing them to work under dangerous conditions. Collective bargaining is vital to safety and health. However, workers’ organizations are essential to collective bargaining and workers’ organizations are under attack in many developed and developing countries. The survival and growth of workers’ organizations will largely determine whether most workers enjoy rising living standards and improved working conditions, or face a deteriorating cycle of poverty, injury and disease.
Rights of Association and Representation
Relationship between Rights of Association and Representation and Occupational Safety and Health
Joint consultation and participation can be effective only in an environment where there is adequate recognition of and respect for the right of employers and workers to associate freely and for their organizations to be able to represent their interests effectively. In a very real sense, therefore, respect for the right to organize can be seen to be an essential precondition of an effective occupational safety and health strategy at both the national and international level and at the workplace. That being the case, it is necessary and appropriate to look more closely at ILO standards relating to freedom of association, bearing in mind their application in the context of the prevention of work-related injury and disease and the compensation and rehabilitation of those who have incurred such injury or disease. Freedom of association standards require that there be proper recognition in law and practice of the right of workers and employers to form and to join the organizations of their choice and of the right of those organizations, once established, to formulate and to implement freely their programmes.
Rights of association and representation also underpin tripartite (governments, employers and workers) cooperation in the field of occupational health and safety. Such cooperation is promoted in the context of ILO standard-setting, for example, by:
- enjoining governments to consult with representative organizations of employers and workers in relation to the formulation and implementation of policy on occupational health and safety at the national or regional level (e.g., Asbestos Convention, 1986 (No. 162), Article 4 and Occupational Safety and Health Convention, 1981 (No. 155), Articles 1 and 8)
- encouraging joint consultation and cooperation on occupational safety and health matters at the level of the workplace (e.g., Prevention of Major Industrial Accidents Convention, 1993 (No. 174), Article 9(f) and (g))
- requiring the joint participation of employers and workers in the formulation and implementation of occupational safety and health policy in the workplace (see especially Occupational Safety and Health Convention, 1981 (No. 155), Articles 19 and 20 and Occupational Safety and Health Recommendation, 1981 (No. 164), para 12).
ILO and Rights of Association and Representation
The “right of association for all lawful purposes by the employed as well as by the employers” was one of the methods and principles set out in Article 41 of the original Constitution of the ILO. This principle now finds express recognition in the Preamble to the Constitution as one of the essential preconditions of the establishment of social justice, which is itself seen as the essential precondition of universal and lasting peace. Together with the principle of tripartism, it is also accorded express recognition in Article I of the Declaration of Philadelphia, which was appended to the Constitution in 1946. This Constitutional endorsement of the importance of respect for the principles of freedom of association helps provide one of the juridical bases for the capacity of the Fact-Finding and Conciliation Commission on Freedom of Association and the Governing Body’s Committee on Freedom of Association to inquire into alleged breaches of the principles of freedom of association.
As early as 1921 the International Labour Conference adopted the Right of Association (Agriculture) Convention (No. 11), which requires ratifying States to “secure to all those engaged in agriculture the same rights of association and combination as to industrial workers”. It does not, however, say anything about the rights which are to be accorded to the industrial workers with whom those engaged in agriculture are to enjoy parity! Attempts to adopt a more general instrument dealing with freedom of association in the 1920s foundered upon the rocks of employer and government insistence that the right to form and join trade unions must be accompanied by a correlative right not to join. The matter was re-opened in the period immediately after the Second World War. This duly resulted in the adoption of the Right of Association (Non-Metropolitan Territories) Convention, 1947 (No. 84), the Freedom of Association and Protection of the Right to Organise Convention, 1948 (No. 87) and the Right to Organise and Collective Bargaining Convention, 1949 (No. 98).
Conventions Nos. 87 and 98 are among the most important and the most widely ratified of all ILO Conventions: as of 31 December 1996, Convention No. 87 had attracted 119 ratifications, while No. 98 had attracted 133. Between them they embody what can properly be regarded as the four key elements in the notion of freedom of association. They are regarded as the benchmark for the international protection of freedom of association for trade union purposes, as reflected, for example, in Article 8 of the International Covenant on Economic, Social and Cultural Rights and Article 22 of the International Covenant on Civil and Political Rights. Within the ILO structure, they form the basis for the principles of freedom of association as developed and applied by the Governing Body’s Committee on Freedom of Association and the Fact-Finding and Conciliation Commission on Freedom of Association, even though in technical terms those bodies derive their jurisdiction from the Constitution of the Organization rather than the Conventions. They also constitute a major focus for the deliberations of the Committee of Experts on the Application of Conventions and Recommendations and of the Conference Committee on the Application of Conventions and Recommendations.
Despite the pivotal role of Conventions Nos. 87 and 98, it should be appreciated that they are by no means the only formal standard-setting instruments which have been adopted under the auspices of the ILO in the field of freedom of association. On the contrary, since 1970 the Conference has adopted further four Conventions and four Recommendations dealing in greater detail with various aspects of the principles of freedom of association, or with their application in certain specific contexts:
- the Workers’ Representatives Convention (No. 135) and Recommendation (No. 143), 1971
- the Rural Workers’ Organizations Convention (No. 141) and Recommendation (No. 149), 1975
- the Labour Relations (Public Service) Convention (No. 151) and Recommendation (No. 158), 1978
- the Collective Bargaining Convention (No. 154) and Recommendation (No. 163), 1981
Principles of Freedom of Association
The core elements
The core elements of the principles of freedom of association as embodied in Conventions Nos. 87 and 98 are:
- that “workers and employers, without distinction whatsoever, shall have the right to establish and, subject only to the rules of the organization concerned, to join organizations of their own choosing without previous authorization” (Article 2 of Convention No. 87)
- that organizations of employers and workers, once established, should have the right “to draw up their constitutions and rules, to elect their representatives in full freedom, to organize their administration and activities and to formulate their programmes” (Article 3(1) of Convention No. 87). Furthermore, the public authorities must “refrain from any interference which would restrict this right or impede the lawful exercise thereof” (Article 3(2))
- that workers are to enjoy “adequate protection against acts of anti-union discrimination in respect of their employment” (Article 1(1) of Convention No. 98)
- that “measures appropriate to national conditions shall be taken, where necessary, to encourage and to promote the full development and utilization of machinery for voluntary negotiation between employers and employers’ organizations and workers’ organizations, with a view to the regulation of terms and conditions of employment by means of collective agreements” (Article 4 of Convention No. 98)
All of the guarantees provided by Convention No. 87 are subject to the proviso set out in Article 8(1): “in exercising the rights provided for in this Convention workers and employers and their respective organizations... shall respect the law of the land”. This in turn is subject to the further proviso that the “law of the land shall not be such as to impair, nor shall it be applied so as to impair, the guarantees provided for in this Convention.”
It should also be noted that by virtue of Article 9(1) of Convention No. 87 it is permissible, but not necessary, to qualify the application of the guarantees set out in that Convention to members of the police and of the armed forces. Article 5(1) of Convention No. 98 is to the same effect, while Article 6 of that instrument stipulates that the Convention “does not deal with the position of public servants engaged in the administration of the State, nor shall it be construed as prejudicing their rights or status in any way.”
The right to join
The right of workers and employers to form and to join the organizations of their choice is the pivot of all of the other guarantees provided by Conventions Nos. 87 and 98 and by the principles of freedom of association. It is subject only to the qualification set out in Article 9(1) of the Convention. This means that it is not permissible to deny any group of workers other than members of the police or the armed forces the right to form or join the trade unions of their choice. It follows that denial or restriction of the right of public servants, agricultural workers, school teachers and so on to form or join the organizations of their choice would not be consistent with the requirements of Article 2.
It is, however, permissible for the rules of a trade union or an employer organization to restrict the categories of workers or employers who may join the organization. The point is that any such restriction must be the result of the free choice of the members of the organization – it must not be imposed from outside.
The right to associate set out in Article 2 is not accompanied by any correlative right not to associate. It will be recalled that earlier attempts to adopt a general freedom of association convention failed because of the insistence by employer and some government delegates that the positive right to associate must carry with it a negative right not to associate. This issue was again raised in the context of the debates on Conventions Nos. 87 and 98. However on this occasion a compromise was effected whereby the Conference adopted a resolution to the effect that the extent to which trade union security devices (such as the “closed” or “agency” shop and check-off arrangements for trade union dues) were permissible or otherwise was a matter to be determined by national law and practice. In other words, the Conventions are considered neither to condone nor to condemn the closed shop and other forms of union security device, although such measures are not regarded as acceptable if they are imposed by law rather than adopted by agreement of the parties (ILO 1994b; ILO 1995a).
Perhaps the most difficult issue which has arisen in the context of Article 2 relates to the extent to which it can be said to endorse the notion of trade union pluralism. In other words, is it consistent with Article 2 for the law to limit, directly or indirectly, the right of workers (or employers) to form or join the organization of their choice through the application of administrative or legislative criteria?
There are two sets of competing interests in this context. On the one hand, Article 2 is clearly meant to protect the right of workers and employers to choose the organization to which they wish to belong and to choose not to belong to organizations with which they are out of sympathy on political, denominational or other grounds. On the other hand, governments (and indeed trade unions) may argue that the excessive proliferation of trade unions and employer organizations which may be an incident of unrestricted freedom of choice is not conducive to the development of free and effective organizations or the establishment and maintenance of orderly industrial relations processes. This was an issue of particular difficulty in the Cold War era, when governments often sought to restrict the range of unions to which workers could belong on ideological grounds. It remains a highly sensitive issue in many developing countries where governments, for good reason or ill, wish to prevent what they see as the excessive proliferation of trade unions by placing restrictions on the number and/or size of unions which can operate in a given workplace or sector of the economy. The ILO’s supervisory bodies have tended to adopt a fairly restrictive approach to this issue, permitting trade union monopolies where they are the result of the free choice of the workers in the country concerned and permitting the adoption of “reasonable” registration criteria, but taking exception to legally imposed monopolies and “unreasonable” registration criteria. In doing so, they have attracted considerable criticism, especially from governments in developing countries which accuse them of adopting a Eurocentric approach to the application of the Convention – the point being that the characteristically European concern with the rights of the individual is said to be inconsistent with the collectivist traditions of many non-European cultures.
Organizational autonomy and the right to strike
If Article 2 of Convention No. 87 protects the fundamental right of employers and workers to form and to join the organization of their choice, then Article 3 can be seen to provide its logical corollary by protecting the organizational autonomy of organizations once established.
As the wording of Article 3(1) clearly indicates, this would include the drafting, adoption and implementation of the constitutions and rules of organizations and the conduct of elections. However, the supervisory bodies have accepted that it is permissible for the public authorities to impose minimum conditions upon the content or administration of rules for the purpose of “ensuring a sound administration and preventing legal complications arising as a result of constitutions and rules being drawn up in insufficient detail” (ILO 1994b). However, if such conditions are excessively detailed or onerous in application then they are likely to be adjudged to be inconsistent with the requirements of Article 3.
Over the years the supervisory bodies have consistently taken the view that “the right to strike is an intrinsic corollary of the right to organize protected by Convention No. 87” (ILO 1994b):
The Committee [of Experts] considers that the right to strike is one of the essential means available to workers and their organizations for the protection of their economic and social interests. These interests not only have to do with obtaining better working conditions and pursuing collective demands of an occupational nature, but also with seeking solutions to economic and social policy questions and to labour problems of any kind which are of direct concern to the workers.
This is one of the most controversial aspects of the entire jurisprudence relating to freedom of association and in recent years in particular it has come in for vigorous criticism from employer and government members of the Conference Committee on the Application of Conventions and Recommendations. (See, for example, International Labour Conference, 80th Session (1993), Record of Proceedings, 25/10-12 and 25/58-64 and International Labour Conference, 81st Session (1994), Record of Proceedings, 25/92-94 and 25/179-180.) It is, however, a firmly entrenched feature of the jurisprudence on freedom of association. It finds clear recognition in Article 8(1) (d) of the International Covenant on Economic, Social and Cultural Rights and was endorsed by the Committee of Experts in its 1994 General Survey on Freedom of Association and Collective Bargaining (ILO 1994b).
It is important to appreciate, however, that the right to strike as recognized by the supervisory bodies is not an unqualified one. In the first place, it does not extend to those groups of workers in relation to whom it is permissible to attenuate the guarantees set out in Convention No. 87, namely members of the police and armed forces. Furthermore, it has also been determined that the right to strike may legitimately be denied to “public servants acting as agents of the public authority” and to workers engaged in essential services in the sense of “services whose interruption would endanger the life, personal safety or health of the whole or part of the population.” However, any restrictions upon the right to strike of workers in these latter categories must be offset by compensatory guarantees, such as “conciliation and mediation procedures leading, in the event of a deadlock, to arbitration machinery seen to be reliable by the parties concerned. It is essential that the latter be able to participate in determining and implementing the procedure, which should furthermore provide sufficient guarantees of impartiality and rapidity: arbitration awards should be binding on both parties and once issued should be implemented rapidly and completely” (ILO 1994b).
It is also permissible to impose temporary restrictions upon the right to strike in times of “acute national emergency”. More generally, it is permissible to impose preconditions such as balloting requirements, exhaustion of conciliation procedures and so on, upon the exercise of the right to strike. However, all such restrictions must “be reasonable and... not such as to place a substantial limitation on the means of action open to trade union organizations”.
The right to strike is often described as the weapon of last resort in collective bargaining. If Article 3 is interpreted so as to protect the weapon of last resort, it seems reasonable to suppose that it must also protect the process of collective bargaining itself. The supervisory bodies have indeed taken this view on a number of occasions, but in general they have preferred to base their jurisprudence on collective bargaining upon Article 4 of Convention No. 98. (For more detailed discussion of the ILO jurisprudence on the right to strike, see Hodges-Aeberhard and Odero de Dios 1987; Ben-Israel 1988).
The autonomy of organizations of employers and workers is also addressed in Articles 4 to 7 of Convention No. 87 and in Article 2 of Convention No. 98. Article 4 provides that such organizations must not be “liable to be dissolved or suspended by administrative authority”. This does not mean that trade unions or employers’ organizations cannot be deregistered or dissolved where they have, for example, engaged in gross industrial misconduct or have not been run in accordance with their rules. But it does mean that any such sanction must be imposed through a duly constituted court or other appropriate body, rather than by administrative diktat.
Article 5 protects the rights of organizations to form and join federations and confederations and also the right of organizations, federations and confederations to affiliate with international organizations of employers and workers. Furthermore, according to Article 6, the guarantees set out in Articles 2, 3 and 4 apply to federations and confederations in the same way as to first level organizations, while Article 7 stipulates that the acquisition of legal personality by organizations of employers or workers must not be made subject to “conditions of such a character as to restrict the application of the provisions of Articles 2, 3 and 4.”
Finally, Article 2(1) of Convention No. 98 requires that organizations of employers and workers are to enjoy “adequate protection against acts of interference by each other or each other’s agents or members in their establishment, functioning or administration”. In practical terms, it seems somewhat unlikely that trade unions would or could effectively interfere with the internal functioning of employer organizations. It is quite conceivable, however, that in certain circumstances employers or their organizations would seek to interfere with the internal affairs of workers’ organizations – for example, by providing some or all of their funds. This possibility finds express recognition in Article 2(2):
In particular, acts which are designed to promote the establishment of workers’ organizations under the domination of employers or employers’ organizations by financial or other means, with the object of placing such organizations under the control of employers or employers’ organizations, shall be deemed to constitute acts of interference within the meaning of this Article.
Protection against victimization
For the guarantees set out in Conventions Nos. 87 and 98 to be meaningful in practice, it is clearly necessary that individuals who exercise their right to form or join organizations of workers be protected against victimization on account of having done so. This logic finds recognition in Article 1(1) of Convention No. 98, which, as indicated, requires that “workers shall enjoy adequate protection against acts of anti-union discrimination in respect of their employment.” Article 1(2) takes the matter further:
Such protection shall apply more particularly in respect of acts calculated to:
(a) make the employment of a worker subject to the condition that he shall not join a union or shall relinquish trade union membership;
(b) cause the dismissal of or otherwise prejudice a worker by reason of union membership or because of participation in union activities outside working hours or, with the consent of the employer, within working hours.
Anti-union discrimination for these purposes would include refusal to employ, dismissal and other measures such as “transfer, relocation, demotion, deprivation or restrictions of all kinds (remuneration, social benefits, vocational training)” which may cause serious prejudice to the worker concerned (see also Termination of Employment Convention, 1982 (No. 158), Article 5(a), (b) and (c), as well as ILO 1994b, para.212).
Not only must there be comprehensive protection against anti-union discrimination as defined, but by virtue of Article 3 of Convention No. 98, there must also be effective means of enforcing those protections:
Legal standards are inadequate if they are not coupled with effective and expeditious procedures and with sufficiently dissuasive penal sanctions to ensure their application ... The onus placed on the employer to prove the alleged anti-union discriminatory measures are connected with questions other than trade union matters, or presumptions established in the worker’s favour are additional means of ensuring effective protection of the right to organize guaranteed by the Convention. Legislation which allows the employer in practice to terminate the employment of a worker on condition that he pay the compensation provided for by law in any case of unjustified dismissal... is inadequate under the terms of Article 1 of the Convention. Legislation should also provide effective means for implementing means of compensation, with the reinstatement of the dismissed worker, including retroactive compensation, being the most appropriate remedy in such cases of anti-union discrimination (ILO 1994b).
Collective bargaining
The guarantee set out in Article 4 of Convention No. 98 has been interpreted so as to protect both the right to engage in collective bargaining and the autonomy of the bargaining process. In other words it is not consistent with Article 4 for employers and workers to be denied the right to engage in collective bargaining if they wish to do so—bearing in mind that it is not inconsistent with the Convention to deny these rights to members of the police or the armed forces and that “the Convention does not deal with the position of public servants engaged in the administration of the State”. Not only must the parties be free to engage in collective bargaining if they so choose, but they must be permitted to reach their own agreement on their own terms without interference by the public authorities – subject to certain qualifications for “compelling reasons of national economic interest” (ILO 1994) and to reasonable requirements as to form, registration and so on.
Article 4 has not, however, been interpreted as protecting the right to recognition for purposes of collective bargaining. The supervisory bodies have repeatedly emphasized the desirability of such recognition, but have not been prepared to take the further step of determining that refusal to recognize and/or the absence of a mechanism whereby employers can be obliged to recognize the unions to which their employees belong constitutes a breach of Article 4 (ILO 1994b; ILO 1995a). They have justified this interpretation on the basis that compulsory recognition would deprive collective bargaining of its voluntary character as envisaged by Article 4 (ILO 1995a). As against that, it might be argued that the ostensible right to engage in collective bargaining must inevitably be compromised if employers are to be free to refuse to engage in such bargaining notwithstanding that they have the right so to bargain if they wish. Furthermore, permitting employers to refuse to recognize the unions to which their employees belong seems to sit somewhat uneasily with the duty to “promote” collective bargaining, which appears to be the principal purpose of Article 4 (Creighton 1994).
Application of Freedom of Association Principles in the Context of Occupational Safety and Health
It was suggested earlier that ILO standards relating to occupational safety and health endorse the concept of bipartite or tripartite involvement in three principal contexts: (1) the formulation and implementation of policy at national and regional level; (2) consultation between employers and workers at the level of the workplace; and (3) joint participation between employers and workers in the formulation and implementation of policy at the level of the workplace. It should be clear from the foregoing that the effective involvement of employers and (especially) workers in all three contexts is crucially dependent upon adequate recognition of their rights of association and representation.
Respect for the right to form and to join organizations is clearly an essential precondition of all three forms of joint involvement. Consultation and participation at the governmental level is feasible only where there are strong and effective organizations which can be seen to be representative of the interests of their constituencies. This is necessary both for ease of communication and so that government will feel constrained to take seriously the views expressed by the representatives of employers and workers. A fortiori, consultation and participation at the level of the workplace is a realistic proposition only if workers have the capacity to form and to join organizations which can represent their interests in discussions with employers and their organizations, provide back-up resources for worker representatives, assist in dealings with public inspectorates and so on. Theoretically, worker representatives could operate at the level of the workplace without having any necessary connection with a more broadly based organization, but the reality of power relations in most workplaces is such that they are unlikely to be able to do so in an effective manner without the support of an industrial organization. At the very least, workers must have the right to have their interests represented in this manner if they so choose.
The organizational autonomy of employer and worker organizations is also an essential precondition of meaningful participation at all levels. It is necessary, for example, that worker organizations should have the right to formulate and to implement their policies on occupational safety and health issues without outside interference, for purposes of consultation with government in relation to: (1) issues such as the legal regulation of hazardous processes or substances; or (2) the formulation of legislative policy relating to compensation for work-related injury or the rehabilitation of injured workers. Such autonomy is even more important at the level of the workplace, where worker organizations need to develop and maintain a capacity to represent the interests of their members in discussion with employers on occupational safety and health issues. This might include having rights of access to workplaces for union officials and/or health and safety specialists; invoking the assistance of the public authorities in relation to hazardous situations; and in certain circumstances organizing industrial action in order to protect the health and safety of their members.
To be effective, organizational autonomy also requires that trade union members and officials be accorded adequate protection against victimization on grounds of their trade union membership or activities, or on account of their having initiated or participated in legal proceedings relating to occupational safety and health matters. In other words, the guarantees against discrimination set out in Article 1 of Convention No. 98 are as relevant to trade union activity relating to occupational safety and health as to other forms of union activity such as collective bargaining, membership recruitment and so on.
The right to engage in autonomous collective bargaining is also a crucial element in effective worker participation in relation to occupational safety and health. The guarantees set out in Article 4 of Convention No. 98 are important in this context. However, as indicated, those guarantees do not extend to the right to be recognized for purposes of such bargaining. On the other hand provisions such as Article 19 of the Occupational Safety and Health Convention, 1981 (No. 155) may be seen as coming very close to requiring trade union recognition in the context of occupational safety and health:
There shall be arrangements at the level of the undertaking under which:
- representatives of workers in an undertaking are given adequate information on measures taken by the employer to secure occupational safety and health and may consult their representative organizations about such information provided they do not disclose commercial secrets;
- workers and their representatives in the undertaking are given appropriate training in occupational safety and health;
- workers or their representatives and, as the case may be, their representative organizations in an undertaking, in accordance with national law and practice, are enabled to inquire into, and are consulted by the employer on, all aspects of occupational safety and health associated with their work...
In practical terms it would be very difficult to give effect to these provisions without according some kind of formal recognition to the role of workers’ organizations. This in turn serves to emphasize yet again the importance of adequate recognition of rights of association and representation as a precondition of the development and implementation of effective occupational safety and health strategies at both the national and enterprise level.
Zirconium and Hafnium
Gunnar Nordberg
Occurrence and Uses
It has been estimated that zirconium (Zr) constitutes about 0.017% of the lithosphere. Because of its very high chemical activity at temperatures only slightly above normal atmospheric temperature, the element occurs only in combined states. The most common ores are zircon (ZrO2) and baddeleyite (ZrSiO4). Zirconium is found in all animal tissues.
Hafnium (Hf) is found associated with zirconium in all its terrestrial occurrences. The amount of hafnium varies but averages about 2% of the total zirconium plus hafnium. In only one ore, low in both elements, has hafnium been found in greater quantity than zirconium. Spectrographic evidence indicates that the distribution is also about 2% hafnium in the total zirconium-plus-hafnium in the universe. These two elements are more closely identical in their chemical properties than are any other pair in the periodic table. The similarity is so great that no qualitative differences have yet been found which would permit their separation. For this reason, it can be assumed that most of the zirconium which has been used, and on the basis of which physiological effects have been reported, has contained 0.5 to 2% hafnium.
Zircon has been valued since the earliest times as a gem stone, since it occurs quite commonly in large single crystals; however, most of the commercially useful deposits of zirconium ore are in beach sands or other places where the relatively heavy and chemically inert zirconium minerals have been deposited while the lighter portions of the rocks in which they occurred have been disintegrated and washed away by the action of water. Substantial deposits of such beach sands are known in India, Malaya, Australia and the United States. Baddeleyite in commercially useful deposits was first observed in Brazil, and has since been found in a number of other locations including Sweden, India and Italy. Some zirconium ores have also been mined commercially in Madagascar, Nigeria, Senegal and South Africa.
Zircon is used as a foundry sand, an abrasive, and as a component of zircon and zirconia refractory compositions for laboratory crucibles. It is found in ceramic compositions where it acts as an opacifier in glazes and enamels. Zircon and zirconia bricks are used as linings for glass furnaces. Zirconia forms are also used as dies for extrusion of both ferrous and non-ferrous metals and as spout linings for pouring metals, particularly for continuous casting.
More than 90% of zirconium metal is now used in nuclear power generation because zirconium has a low absorption cross-section for neutrons and a high resistance to corrosion inside atomic reactors, provided it is free of hafnium. Zirconium is also used in the manufacture of cast iron, steel and surgical appliances. It is employed in arc lamps, pyrotechnics, in special welding fluxes, and as a pigment in plastics.
Powdered zirconium metal is used as a “getter” in thermionic tubes to absorb the last traces of gas after pumping and out-gassing of the tube elements. In the form of fine ribbon or wool, the metal is also used as the filter in photographic flash-bulbs. The massive metal is used either pure or in alloy form for the lining of reaction vessels. It is also used as a lining for pumps and piping systems for chemical processes. An excellent super-conducting alloy of zirconium and columbium has been used in a magnet with a field of 6.7 T.
Zirconium carbide and zirconium diboride are both hard, refractory, metallic compounds which have been used in cutting tools for metals. The diboride has also been used as a thermocouple jacket in open-hearth furnaces, providing very long-lived thermocouples. Zirconium tetrachloride is used in organic synthesis and in water repellents for textiles. It is also useful as a tanning agent.
Hafnium metal has been used as a cladding on tantalum for rocket engine parts which must operate in very high-temperature, erosive conditions. Because of its high thermal-neutron cross-section, it is also used as a control rod material for nuclear reactors. In addition, hafnium is used in the manufacture of electrodes and light-bulb filaments.
Hazards
It is inaccurate to state that zirconium compounds are physiologically inert, but the tolerance of most organisms to zirconium appears to be great in comparison to the tolerance for most heavy metals. Zirconium salts have been used in the treatment of plutonium poisoning to displace the plutonium (and yttrium) from its deposition in the skeleton and to prevent the deposition when treatment was started early. In the course of this study, it was determined that the diet of rats could contain as much as 20% of zirconia for comparatively long periods without harmful effects, and that the intravenous LD50 of sodium zirconium citrate for rats is about 171 mg/kg body weight. Other investigators have found an intraperitoneal LD50 of 0.67 g/kg for zirconium lactate and 0.42 g/kg for barium zirconate in rats and 51 mg/kg of sodium zirconium lactate in mice.
Zirconium compounds have been recommended and used for the topical treatment of Rhus (poison ivy) dermatitis and for body deodorants. Some compounds which have been used are carbonated hydrous zirconia, hydrous zirconia and sodium zirconium lactate. There have been a number of reports of the production of persistent granulomatous conditions of the skin as the result of these applications.
Of more direct interest in connection with occupational exposures is the effect of inhalation of zirconium compounds, and this has been less extensively investigated than the other routes of administration. There have, however, been several experiments and at least one report of human exposure. In this instance, a chemical engineer with seven years’ exposure in a zirconium and hafnium processing plant was found to have a granulomatous lung condition. Since examination of all the other employees revealed no comparable lesions, it was concluded that the condition was most probably to be attributed to a relatively heavy beryllium exposure prior to zirconium exposure.
Exposure of experimental animals to zirconium compounds showed that zirconium lactate and barium zirconate both produced severe, persistent, chronic interstitial pneumonitis at atmospheric zirconium concentrations of about 5 mg/m3. Much higher atmospheric sodium zirconium lactate concentrations of 0.049 mg/cm3 for shorter exposures have been found to produce peribronchial abscesses, peribronchiolar granulomas and lobular pneumonia. Although documentation of zirconium pneumoconiosis in humans has been lacking, authors of one study conclude that zirconium should be considered a likely cause of pneumoconiosis, and recommend taking appropriate precautions in the workplace.
The small number of investigations on the toxicity of hafnium compounds has indicated an acute toxicity slightly higher than that of zirconium salts. Hafnium and its compounds cause liver damage. Hafnyl chloride at 10 mg/kg produced cardiovascular collapse and respiratory arrest in a cat in the same manner as soluble zirconium salts; the intraperitoneal LD50 of 112 mg/kg for hafnium is not much smaller than that for zirconium.
Safety and Health Measures
Fire and explosion. Zirconium metal in the form of a fine powder burns in air, nitrogen or carbon dioxide. The powders are explosive in air in the range of 45 to 300 mg/l, and are self-igniting if disturbed, probably because of static electricity generated by separation of the grains.
The powdered metals should be transported and handled in the wet state; water is usually used for wetting. When the powder is dried prior to use, the quantities employed should be kept as small as possible and operations should be carried out in separate cubicles to prevent propagation in the event of an explosion. All sources of ignition, including static electric charges, should be eliminated from areas in which the powder is to be handled.
All surfaces in the area should be impervious and seamless so that they can be washed down with water and kept completely free from dust. Any spilled powder should be cleaned up immediately with water so that it has no chance to dry in place. Used papers and cloths which have become contaminated with the powders should be kept wet in covered containers until they are removed to be burned, which should be done at least daily. The dried powders should be disturbed and handled as little as possible, and then only with non-sparking tools. Rubber or plastic aprons, if worn over work clothes, should be treated with an anti-static compound. Work clothing should be made from non-synthetic fibres unless effectively treated with antistatic materials.
All processes using zirconium and or hafnium should be designed and ventilated to keep airborne contamination below the exposure limits.
Zinc
Gunnar Nordberg
Occurrence and Uses
Zinc (Zn) is widely distributed in nature in quantities which amount to approximately 0.02% of the earth’s crust. It is found in nature as the sulphide (sphalerite), carbonate, oxide or silicate (calamine) in combination with many minerals. Sphalerite, the principal zinc mineral and the source of at least 90% of metallic zinc, contains iron and cadmium as impurities. It is almost always accompanied by galena, the sulphide of lead, and occasionally is found in association with ores containing copper or other base metal sulphides.
On exposure to air, zinc becomes covered with a tenacious film of oxide which protects the metal from further oxidation. This resistance to atmospheric corrosion forms the basis for one of the most common uses of the metal, the protection of steelwork by galvanizing. Zinc’s ability to protect ferrous metals against corrosion is reinforced by electrolytic action. It acts as an anode with respect to iron and other structural metals, except aluminium and magnesium, and is thus preferentially attacked by corrosive agents. This property is used in many other important applications of zinc—for example, in the use of zinc plates as anodes for cathodic protection of ships’ hulls, underground tanks and so on. Zinc metal is die cast for components in the automobile industry, electrical equipment industry, and in the light machine tool, hardware, toys and fancy goods industries. It is rolled into sheets in rolling mills for the manufacture of roofing, weather stripping, cases for dry batteries, printing plates and so on. Zinc is also alloyed with copper, nickel, aluminium and magnesium. When it is alloyed with copper, it forms the important groups of alloys known as the brasses.
Zinc oxide (ZnO), or zinc white (flowers of zinc) is produced by the oxidation of vaporized pure zinc or by the roasting of zinc oxide ore. It is used as a pigment in paints, lacquers and varnishes, as well as a filler for plastics and rubber. Zinc oxide is found in cosmetics, quick-setting cements, and in pharmaceuticals. It is useful in the manufacture of glass, automobile tyres, matches, white glue and printing inks. Zinc oxide is also used as a semiconductor in the electronics industry.
Zinc chromate (ZnCrO4), or zinc yellow, is produced by the action of chromic acid on slurries of zinc oxide, or on zinc hydroxide. It is used in pigments, paints, varnishes and lacquers, and in the manufacture of linoleum. Zinc chromate acts as a corrosion inhibitor for metals and epoxy laminates.
Zinc cyanide (Zn(CN)2) is produced by precipitation of a solution of zinc sulphate or chloride with potassium cyanide. It is used for metal plating and for gold extraction. Zinc cyanide acts as a chemical reagent and as a pesticide. Zinc sulphate (ZnSO4·7H2O), or white vitriol, is produced by roasting zinc blende or by the action of sulphuric acid on zinc or zinc oxide. It is used as an astringent, a preservative for hides and wood, a bleach for paper, a pesticide adjuvant and a fungicide. Zinc sulphate also serves as a fireproofing agent and as a depressant in froth flotation. It is used in water treatment and in textile dyeing and printing. Zinc sulphide is used as a pigment for paints, oilcloths, linoleum, leather, inks, lacquers, and cosmetics. Zinc phosphide (Zn3P2) is produced by passing phosphine through a solution of zinc sulphate. It is used mainly as a rodenticide.
Zinc chloride (ZnCl2), or butter of zinc, has numerous uses in the textile industry, including dyeing, printing, sizing and weighting fabrics. It is a component of cement for metals, dentifrices, and soldering fluxes. It is used alone or with phenol and other antiseptics for preserving railway ties. Zinc chloride is useful for glass etching and for the manufacture of asphalt. It is a vulcanizing agent for rubber, a flame retardant for wood, and a corrosion inhibitor in water treatment.
Hazards
Zinc is an essential nutrient. It is a constituent of metalloenzymes, which play an important role in nucleic acid metabolism and protein synthesis. Zinc is not stored in the body, and a minimum daily intake of zinc is recommended by nutritional experts. Absorption of zinc takes place more readily from animal protein sources than from plant products. The phytate content of plants binds zinc, rendering it unavailable for absorption. Zinc deficiency states have been reported from countries where cereals are the major source of protein consumed by the population. Some of the recognized clinical manifestations of chronic zinc deficiency in humans are growth retardation, hypogonadism in males, skin changes, poor appetite, mental lethargy and delayed wound healing.
In general, zinc salts are astringent, hygroscopic, corrosive and antiseptic. Their precipitating action on proteins forms the basis of their astringent and antiseptic effects, and they are absorbed relatively easily through the skin. The taste threshold for zinc salts is approximately 15 ppm; water containing 30 ppm of soluble zinc salts has a milky appearance, and a metallic taste when the concentration reaches 40 ppm. Zinc salts are irritating to the gastrointestinal tract, and the emetic concentrations for zinc salts in water range from 675 to 2,280 ppm.
The solubility of zinc in weakly acidic solutions, in the presence of iron, has led to accidental ingestion of large quantities of zinc salts when acid foods such as fruit drinks were prepared in worn galvanized iron vessels. Fever, nausea, vomiting, stomach cramps and diarrhoea occurred in 20 minutes to 10 hours following ingestion.
A number of zinc salts may enter the body by inhalation, through the skin or by ingestion and produce intoxication. Zinc chloride has been found to cause skin ulcers. A number of zinc compounds present fire and explosion hazards. The electrolytic manufacturing of zinc can produce mists containing sulphuric acid and zinc sulphate that can irritate the respiratory or digestive systems and lead to dental erosion. Metallurgic processes involving zinc can lead to arsenic, cadmium, manganese, lead and possibly chromium and silver exposures, with their associated hazards. Since arsenic is frequently present in zinc, it can be a source of exposure to highly toxic arsine gas whenever zinc is dissolved in acids or alkalis.
In zinc metallurgy and manufacturing, welding and cutting of galvanized or zinc-coated metal, or melting and casting of brass or bronze, the most frequently encountered hazard from zinc and its compounds is exposure to zinc oxide fumes, which cause metal-fume fever. Symptoms of metal-fume fever include shivering attacks, irregular fever, profuse sweating, nausea, thirst, headache, pains in the limbs and a feeling of exhaustion. Attacks are of short duration (most cases are on the way to complete recovery within 24 hours of the onset of symptoms), and tolerance seems to be acquired. A significant increase in free erythrocyte protoporphyrin has been reported in zinc oxide packing operations.
Zinc chloride fumes are irritating to the eyes and mucous membranes. In an accident involving smoke generators, 70 exposed persons experienced varying degrees of irritation of the eyes, nose, throat and lungs. Of the 10 fatalities, some died within a few hours with pulmonary oedema, and others died later of bronchopneumonia. On another occasion, two firemen were exposed to zinc chloride fumes from a smoke generator during a firefighting demonstration, one briefly, the other for several minutes. The former recovered rapidly while the latter died after 18 days, due to respiratory failure. There was a rapid rise of temperature and marked upper respiratory tract inflammation soon after exposure. Diffuse pulmonary infiltrations were seen on the chest radiograph, and autopsy revealed active fibroblastic proliferation and cor pulmonale.
In an experiment primarily designed to evaluate carcinogenesis, groups of 24 mice received 1,250 to 5,000 ppm of zinc sulphate in drinking water for one year. Apart from severe anaemia in animals receiving 5,000 ppm, there were no adverse effects from zinc. Tumour incidence was not significantly different from that seen in the controls.
Zinc phosphide, which is used as a rodenticide, is toxic to humans whether swallowed, inhaled or injected, and, together with zinc chloride, is the most dangerous of the zinc salts; these two substances have been responsible for the only deaths definitely due to zinc poisoning.
Skin effects. Zinc chromate in primer paints used by car-body builders, tinsmiths and steel cupboard makers has been reported to cause nasal ulceration and dermatitis in exposed workers. Zinc chloride has a caustic action, which may result in ulceration of the fingers, hands and forearms of those who handle timber impregnated with it or use it as a flux in soldering. It has been reported that zinc oxide dust may block the ducts of the sebaceous glands and give rise to a papular, pustular eczema in humans packaging this compound.
Safety and Health Measures
Fire and explosion. Finely divided zinc powder, and other zinc compounds, can be fire and explosion hazards if stored in damp places, sources of spontaneous combustion. Residues from reduction reactions may ignite combustible materials. Zinc ammonium nitrate, zinc bromate, zinc chlorate, zinc ethyl, zinc nitrate, zinc permanganate and zinc picrate are all dangerous fire and explosion hazards. In addition, zinc ethyl will ignite spontaneously in contact with air. It should, therefore, be stored in a cool, dry, well-ventilated place away from acute fire risks, open flames and powerful oxidizing agents.
In all cases where zinc is heated to the point where fumes are produced, it is most important to ensure that adequate ventilation is provided. Individual protection is best ensured by education of the worker concerning metal-fume fever and the provision of local exhaust ventilation, or, in some situations, by wearing of a supplied-air hood or mask.
Workers who are none the less exposed to zinc chloride fumes should wear personal protective equipment including protective clothing, chemical eye and face protection and appropriate respiratory protective equipment. Exposure to zinc chloride fumes should be treated by copious irrigation of the exposed areas.
Vanadium
Occurrence and Uses
The most important vanadium (V) ores are patronite (vanadium sulphide), found in Peru, and descloizite (lead-zinc vanadate), found in South Africa. Other ores, such as vanadinite, roscoelite and carnotite, contain vanadium in sufficient quantities for economic extraction. Crude petroleum may contain small amounts of vanadium, and flue-gas deposits from oil-fired furnaces may contain over 50% vanadium pentoxide. Slags from ferrovanadium are another source of the metal. One of the most important sources of human exposure to vanadium is vanadium oxides released when burning fuel oils.
Normally, small amounts of vanadium are found in the human body, particularly in adipose tissue and in the blood.
The larger amount of the vanadium produced is used in ferrovanadium, the most important direct use of which is in high-speed steel and tool steelmaking. Addition of 0.05 to 5% of vanadium removes occluded oxygen and nitrogen from the steel, enhances the tensile strength and improves the modulus of elasticity and the rust resistance of the final alloy. In the past vanadium compounds have been used as therapeutic agents in medicine. The vanadium-gallium alloy has shown interesting properties for production of high magnetic fields.
Certain vanadium compounds have a limited use in industry. Vanadium sulphate (VSO4·7H2O) and vanadium tetrachloride (VCl4) are used as mordants in the dyeing industry. Vanadium silicates are used as catalysts. Vanadium dioxide (VO2) and vanadium trioxide (V2O3) are employed in metallurgy. However, the most significant compounds in terms of industrial health hazards are vanadium pentoxide (V2O5) and ammonium metavanadate (NH4VO3).
Vanadium pentoxide is obtained from patronite. It has for a long time been an important industrial catalyst used in a number of oxidation processes such as those involved in the manufacture of sulphuric acid, phthalic acid, maleic acid and so on. It serves as a photographic developer and as a dyeing agent in the textile industry. Vanadium pentoxide is also used in ceramic colouring materials.
Ammonium metavanadate is employed as a catalyst in the same way as vanadium pentoxide. It is a reagent in analytical chemistry and a developer in the photography industry. Ammonium metavanadate is also used in dyeing and printing in the textile industry.
Hazards
Experience has shown that vanadium oxides and, in particular, the pentoxide and its derivative ammonium metavanadate cause harmful effects in humans. Exposure to vanadium pentoxide is possible at the following points in industry: when vanadium pentoxide is used in particulate form in the production of metallic vanadium; during the repair of installations where vanadium pentoxide is used as a catalyst; and during the cleaning of oil-fired furnace flues in power stations, ships and so on. The presence of vanadium compounds in petroleum products is of particular significance and, because of the possibility of air pollution in the environment of oil-fired power stations, it receives attention from public health authorities as well as from those concerned with industrial health.
The inhalation of vanadium compounds may produce severe toxic effects. The severity of the effects depends on the atmospheric concentration of the vanadium compounds and the duration of exposure. Health impairment may occur after even brief exposure (e.g., 1 hour), and the initial symptoms are profuse lacrimation, burning sensation in the conjunctivae, serous or haemorrhageous rhinitis, sore throat, cough, bronchitis, expectoration and chest pain.
Severe exposure may result in pneumonia with fatal outcome; however, following one-time exposure, complete recovery usually occurs within 1 to 2 weeks; prolonged exposure may produce chronic bronchitis with or without emphysema. The tongue may present a greenish discolouration and also the cigarette ends of vanadium workers may show a greenish colour, resulting from chemical interactions.
Local effects in experimental animals are mainly observed in the respiratory tract. Systemic effects have been observed in the liver, kidney, nervous system, cardiovascular system and blood-forming organs. Metabolic effects include interference with biosynthesis of cystine and cholestrol, depression and stimulation of phospholipid synthesis. Higher concentrations have produced inhibition of serotonin oxidation. In addition, vanadate has been shown to inhibit several enzyme systems. In humans, systemic effects of vanadium exposure are less well documented, but reduction of serum cholestrol has been demonstrated. In the work environment, vanadium and its compounds are taken up in the human body by inhalation, mainly during production and boiler cleaning operations. Absorption of vanadium from the gastrointestinal tract is poor, not exceeding 1 to 2%; ingested vanadium compounds are largely eliminated with faeces.
A study was conducted to evaluate the level of bronchial responsiveness among workers recently exposed to vanadium pentoxide during periodic removal of ashes and clinker from boilers of an oil-fired power station. This study suggests that exposure to vanadium increases bronchial responsiveness even without the appearance of bronchial symptoms.
Safety and Health Measures
It is important to prevent the inhalation of airborne particulate vanadium pentoxide. For use as a catalyst, vanadium pentoxide can be produced in an agglomerated or pelleted form which is dust free; however, vibration in the plant may, in time, reduce a certain proportion to dust. In the processes associated with the manufacture of metallic vanadium, and in the sieving of used catalyst during maintenance operations, the escape of dust should be prevented by the enclosure of the process and by the provision of exhaust ventilation. In boiler cleaning in power stations and on ships, maintenance workers may have to enter the boilers to remove soot and to make repairs. These workers should wear adequate respiratory protective equipment with full face mask and eye protection. Wherever possible, on-load cleaning should be improved to reduce the need for workers to enter furnaces; where off-load cleaning proves essential, methods such as water lancing, which do not necessitate physical entry, should be tried.
Tungsten
Gunnar Nordberg
Occurrence and Uses
Tungsten (W) never occurs free in nature and is found only in a few minerals as tungstate of calcium, iron or manganese. Of the known tungsten-bearing minerals, scheelite (CaWO4), wolframite ((Fe,Mn)WO4), hubnerite (MnWO) and ferberite (FeWO4) are commercially important. Total world reserves of tungsten trioxide (WO3 ) are estimated to be about 175,000,000 t. These tungsten minerals are mostly mined from underground workings, but open-cut operations and more primitive methods are also applied. The tungsten content of the ore mined is usually 0.5 to 2.0%. The more common impurities are gangue minerals such as quartz and calcite, and metallic minerals of copper, bismuth, tin and molybdenum.
Tungsten is a component in hard metals. It is used to increase the hardness, toughness, elasticity and tensile strength of steel. It is used in the production of tungsten steels for automobiles and high-speed cutting tools. Tungsten is also used in lamps, vacuum tubes, electric contacts, x-ray tubes and fluorescent light tubes. It serves as a flame retardant in the textile industry.
Tungsten carbide (WC) has replaced diamond in large drawing dies and rock drills because of its extreme hardness. Tungsten compounds are also used in lasers, dyes, inks and ceramic frits. Some tungsten alloys are used in the nuclear and space industries for nozzles of rocket motors and for protecting shields for spacecraft.
Hazards
Little is known of the toxicity of tungsten. The LD50 of sodium tungstate for 66-day-old rats was between 223 and 255 mg/kg and showed significant postprandial and age effect. Of three tungsten compounds, sodium tungstate is most toxic, tungstic oxide is intermediate, and ammonium paratungstate is least toxic. The feeding of 2.5 and 10% of diet as tungsten metal over a period of 70 days has been shown to be without marked effect upon the growth of male rats, as measured in terms of gain in weight, though it caused a 15% reduction in weight gain for female rats from that of control.
Industrial exposure is related chiefly to substances associated with the production and uses of tungsten, its alloys and compounds, rather than tungsten itself. In the mining and milling processes, the main hazards seem to be exposure to quartz-containing dust, noise, hydrogen sulphide, sulphur dioxide and chemicals such as sodium cyanide and sodium hydroxide. The exposure may be associated with other metals in the ore, such as nickel.
Hard metal is the mixture of tungsten carbide and cobalt, to which small amounts of other metals may be added. In the tool-cutting industry workers may be exposed to dust of tungsten carbide, cobalt fumes and dust, and carbides of nickel, titanium and tantalum. Following occupational exposure to tungsten carbide dust by inhalation, cases of pneumoconiosis or pulmonary fibrosis have been reported, but it is generally agreed that this “hard-metal disease” is more likely to be caused by the cobalt with which tungsten carbide is fused. Where machining and grinding of tungsten carbide tools is performed, the hard-metal workers may be at risk for the development of interstitial obstructive lung disease, a serious hazard associated with elevated air concentrations of cobalt. The effects of hard metals on the lungs are discussed elsewhere in this Encyclopaedia.
Tungsten carbonyl is a moderate fire hazard when exposed to flame. When heated to decomposition, it emits carbon monoxide. The incidence of accidents and diseases in tungsten mines and mills is not well documented. However, from the scarce data available it can be said that it is less than that of coal mines.
Titanium
Gunnar Nordberg
Occurrence and Uses
Titanium (Ti) is contained in many minerals, but only a few of them are of industrial significance. These include ilmenite (FeTiO3), which contains 52.65% Ti and 47.4% FeO; rutile (TiO2), with admixtures of ferrous oxide; perovskite (CaTiO3), which contains 58.7% TiO2 and 41.3% CaO; and sphene, or titanite, (CaOTiO2·SiO2), which contains 38.8% TiO2. Some heterogeneous minerals, such as loparite, pyrochlor, and tailings from bauxite and copper ore processing may also be sources of titanium.
Titanium is used as a pure metal, in alloys, and in the form of various compounds. The bulk of titanium is needed in the iron and steel industry, in shipbuilding, for aircraft and rocket construction, and for the fabrication of chemical plants. Titanium is used as a protective surface on mixers in the pulp and paper industry. It is also found in surgical appliances. Titanium has been employed for the manufacture of electrodes, lamp filaments, paints, dyes and welding rods. Titanium powder is used in pyrotechnics and in vacuum engineering. Titanium is also used in dentistry and in surgery for implants or prostheses.
Titanium carbide and titanium nitride are used in powder metallurgy. Barium titanate is used for making heavy-duty capacitors. Titanium dioxide is utilized as a white pigment in paints, floor coverings, upholstery, electronics, adhesives, roofing, plastics and in cosmetics. It is also useful as a component of porcelain enamels and glazes, as a shrinking agent for glass fibres, and as a delustering agent for synthetic fibre. Titanium tetrachloride acts as an intermediate in the production of titanium metal and titanium pigments, and as a catalyst in the chemical industry.
Hazards
The formation of titanium dioxide (TiO2) and concentrate dust, pitch briquette dust arising from crushing, mixing and charging of bulk raw materials, and radiant heat from coking furnaces are hazards in titanium production. There may be chlorine, titanium tetrachloride (TiCl4) vapours and their pyrolysis products in the air of the chlorination and rectification plants, arising from leaking or corroded equipment. Magnesium oxide may be present in the air of the reduction area. Titanium dust becomes airborne when titanium sponge is knocked out, crushed, separated and bagged. Exposure to heat and infrared radiation occurs in the arc furnace area (up to 3 to 5 cal/cm2 per min).
Maintenance and repair of the chlorination and rectification installations, which includes disassembly and cleaning of the equipment and pipework, create particularly adverse conditions of work: high concentrations of TiCl4 vapours and hydrolysis products (HCl, Ti(OH)4), which are highly toxic and irritant. Workers in these plants often suffer from upper-airway disease and acute or chronic bronchitis. Liquid TiCl4 splashed on the skin causes irritation and burns. Even very short contact of the conjunctiva with TiCl4 leads to suppurative conjunctivitis and keratitis, which may result in corneal opacities. Animal experiments have shown that dust of metallic titanium, titanium concentrates, titanium dioxide and titanium carbide is slightly toxic. While titanium dioxide has not been found to be fibrogenic in animals, it seems to increase the fibrogenicity of quartz when given as combined exposure. Long-term exposure to titanium-containing dust may result in mild forms of chronic lung disease (fibrosis). There is radiological evidence that workers who have handled TiO2 for long periods develop lung changes resembling those observed in mild forms of silicosis. In one worker who had worked in contact with titanium dioxide for several years and died from brain cancer, the lungs displayed accumulations of TiO2 and changes analogous to anthracosis. Medical examinations of powder metallurgy workers in various countries have disclosed cases of chronic pneumonitis due to mixed dust including titanium carbide. The degree of this disease varied according to conditions of work, length of dust exposure and individual factors.
Workers who have been chronically exposed to titanium and titanium dioxide dust show a high incidence of chronic bronchitis (endobronchitis and peribronchitis). The early stages of the disease are characterized by impaired pulmonary respiration and ventilatory capacity, and by reduced blood alkalinity. Electrocardiographic tracings of these titanium workers revealed cardiac changes characteristic of pulmonary disease with hypertrophy of the right auricle. A considerable number of these cases presented myocardial hypoxia of various degrees, inhibited atrioventricular and intraventricular conductivity, and bradycardia.
Airborne metallic titanium dust is explosive.
Other hazards in titanium production are carbon monoxide exposures at the coking and arc furnaces, and burns.
Safety and Health Measures
Control dust during ore crushing by moistening the material to be processed (up to 6 to 8% moisture content), and by adopting a continuous process, which enables the equipment to be enclosed with exhaust devices at all points where dust may form; the dust-laden air exhausted should be filtered and the dust collected should be recycled. Dust exhaust systems must be provided at the knock-out stations; crushers, separators and baggers in the titanium sponge plant. Knocking out with pneumatic chipping hammers should be replaced by machining out on special milling or turning machines.
Tin
Gunnar Nordberg
Tin has been used through the ages up to modern industrial times because it is pliable and easily shaped at normal temperatures, and it mixes readily with other metals to form alloys. One of its outstanding characteristics is its resistance to acids and atmospheric influences.
Occurrence and Uses
Although deposits of tin are widely distributed throughout the world, up to the eighteenth century the world’s supply of tin was mainly from England, Saxony and Bohemia. Today, except for some deposits in Nigeria, China, the Congo and Australia, the principal sources are found in Southeast Asia and Bolivia.
Of minerals containing tin, cassiterite (SnO2) or tinstone is of the greatest commercial importance. It is present in veins closely connected with granite or acid eruptive rocks, but five-sixths of the world’s total production is derived from secondary alluvial deposits resulting from the disintegration of the primary deposits. In Bolivia, sulphide ores, such as stannite (Cu2FeSnS2) and tealite (PbZnSnS2) are of commercial significance.
Metallic tin is used for Babbitt type metals and for collapsible tubes in the pharmaceutical and cosmetic industries. Because of its resistance to corrosion, tin is used as a protective coating for other metals. Tinplate is sheet iron or steel which has been thickly coated with tin by dipping in a molten bath of that metal. It is used mainly for making household utensils and for utensils in food and beverage canning industries. It is often used for decorating purposes. Terneplate is sheet iron or steel coated with a lead-tin alloy containing 85% lead and 15% tin. It is used mainly for making roofing tile. Speculum is a tin-copper alloy containing 33 to 50% tin, that can be polished to a high degree of reflection. It is used as a coating applied by electrolytic deposition to impart brightness to silverware and similar articles, and for making telescope mirrors. A molten tin bath is also used in the production of window glass.
An important property of tin is its ability to form alloys with other metals, and it has a number of uses in this field. A tin-lead alloy known as soft solder is widely used for joining other metals and alloys in the plumbing, automobile, electrical and other industries, and as a filler in the finishing of car bodies. Tin is a constituent of a large number of non-ferrous alloys, including phosphor bronze, light brass, gun-metal, high-tensile brass, manganese bronze, die-casting alloys, bearing metals, type metal and pewter. The tin-niobium alloy is superconductive, and it is used in the manufacture of powerful electromagnets.
Stannic chloride (SnCl4), or tin chloride, is prepared by heating powdered tin with mercuric chloride or by passing a stream of chlorine over molten tin. It is used as a dehydrating agent in organic syntheses, a stabilizer for plastics, and as a chemical intermediate for other tin compounds. Stannic chloride is found in colours and perfumes in the soap industry. It is also employed in ceramics to produce abrasion-resistant or light-reflecting coatings. It is used for the bleaching of sugar and for the surface treatment of glass and other non-conductive materials. The pentahydrate of this salt is used as a mordant. It is also used in treating silk for the purpose of giving weight to the fabric.
Stannous chloride dihydrate (SnCl2·2H2O), or tin salt, is produced by dissolving metallic tin in hydrochloric acid and evaporating until crystallization begins. It is used in dye works as a mordant. It also serves as a reducing agent in the manufacture of glass, ceramics and inks.
The use of organotin (alkyl and aryl) compounds has greatly increased in recent years. Disubstituted compounds and, to a lesser degree, monosubstituted compounds, are used as stabilizers and catalysts in the plastics industry. Trisubstituted compounds are used as biocides, and tetrasubstitutes are intermediates in the production of other derivatives. Butyltin trichloride, or trichlorobutyltin; dibutyltin dichloride, or dichlorodibutyltin; trimethyltin; triethyltin chloride; triphenyltin chloride, or TPTC; tetraisobutyltin, or tetraisobutylstannane are among the most important.
Hazards
In the absence of precautions, mechanical injury can be caused by the heavy, powerful plant and machinery used in the dredging and washing operations. Serious burn hazards are present in the smelting processes when molten metal and hot slags are manipulated.
At the final stage of upgrading of cassiterite concentrate and during the roasting of sulphide ore, sulphur dioxide is evolved. Sulphur dioxide and stannous sulphide constitute a hazard when the rough molten tin is separated from the rest of the charge during refining. This work is done in a very hot environment, and heat exhaustion could arise. The noise on a dredger caused by the discharge from the dredging buckets to the primary washing plant may cause damage to the hearing of the workers.
Several studies report the hazards associated with exposure to radon, radon decay products and silica in tin mines. While most of the operations associated with the extraction and treatment of tin ore are wet processes, tin dust and oxide fumes may escape during bagging of concentrate, in ore rooms and during smelting operations (mixing-plant and furnace tapping), as well as during the periodic cleaning of bag filters used to remove particulate matter from smelter furnace flue gas before release to the atmosphere. The inhalation of tin oxide dust without silica leads to a benign nodular pneumoconiosis without pulmonary disability. The radiological picture is similar to baritosis. This benign pneumoconiosis has been called stannosis.
Tin powder is a moderate irritant to the eyes and airways; it is combustible and reacts violently with oxidants, strong acids, powdered sulphur and some extinguishing agents such as bicarbonate powder and carbon dioxide.
Tin ingested in small (mg) quantities is non-toxic (hence, the widespread use of tinplate in the food canning industry). The results of animal experiments indicate that the lethal dose by intravenous injection is about 100 mg/kg body weight, and that the ingestion of considerable quantities of powdered tin may cause vomiting but not permanent injury. It appears that humans can tolerate a daily intake of 800 to 1,000 mg without ill effect. The absorption of metallic tin or its inorganic salts from the alimentary tract seems to be small.
A number of tin alloys are injurious to health (particularly at high temperatures) because of the harmful characteristics of the metals with which may be alloyed (e.g., lead, zinc, manganese).
Organotin compounds are, in general, strong irritants, and acute conjunctivitis has been observed as a result of eye splashes, even when followed by immediate lavage; corneal opacities have also been reported. Prolonged contact of the skin with clothes moistened with vapour, or direct spillage on the skin, have been responsible for acute local burns, subacute diffuse erythematoid dermatitis with pruritus and some pustular eruption in the hair-covered areas. The irritation of the airways and pulmonary tissue can lead to lung oedema; the gastrointestinal tract can also be involved, and inflammatory reactions of the bile duct have been observed, mainly with the dialkyl compounds. Organotin compounds can injure liver and kidneys; they can depress the immune response and have haemolytic activity. In experimental animals they have been in some instances held responsible for reduction in fertility.
Tri- and tetralkyl compounds, in particular triethyltin chloride, cause encephalopathy and brain oedema, with clinical effects of depression, convulsions, flaccid paralysis and urinary retention, as seen in therapeutic use following oral administration.
Safety and Health Measures
Wherever possible, safer substitutes should be used in the place of alkyl tin compounds. When it is necessary to make and use them, the widest possible use should be made of enclosed systems and exhaust ventilation. Engineering control should ensure that exposure limits are not exceeded. Personal protective equipment should be worn, and in appropriate circumstances respiratory protection should be used. Emergency showers should be installed at workplaces in order to allow workers to wash immediately after splashes.
Medical surveillance should focus on eyes, skin and chest x rays in the exposure to inorganic tin compounds, and on eyes, skin, central nervous system, liver and kidney function, and blood in the exposure to organic tin compounds. Mercaprol has been reported as useful in the treatment of dialkyltin intoxications. Steroids have been suggested for the treatment of triethyltin poisoning; however only surgical decompression seems to be of value in encephalopathy and brain oedema provoked by tri- and tetraalkyl tin compounds.
Taking into consideration the fact that most tin mines are located in developing countries, attention should also be paid to climatic and other factors influencing the health, well-being and productive capacity of the workers. Where mines are geographically isolated, good housing should be provided for all personnel. Nutritional standards should be upgraded by health education, and workers should be provided with adequate food supplies and good medical care.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."