- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- The Physical Environment and Health Care
Case Study: A Successful Information Experience in Thailand
Background
Thailand has a population of approximately 59 million people and a land area of 514,000 square kilometres. The population growth is 1.7% per annum. The labour force in 1995 was 34 million of whom 33 million were employed and 1 million unemployed. About 17 and 14 million people were employed in the agricultural and non-agricultural sectors respectively.
In the past, Thailand has been an agricultural economy, exporting more rice and tapioca combined than other country, but during the 30-year period 1960–90 the Thai economy underwent dramatic structural changes. Manufacturing has assumed the leading role in terms of its contribution to the GDP. These changes have made Thailand one of the fastest growing economies in the region, with a rapidly expanding manufacturing sector supplying textiles, garments, electrical and electronic goods, gems and jewels and dozens of other products for local and world markets.
The Royal Thai Government is greatly concerned for the welfare of Thai workers in both the industrial and the agricultural sectors. This concern has led to seminars stressing the need for effective measures to improve the working conditions and environments of workers in various sectors and work situations. In light of all the issues taken into consideration, the National Institute for the Improvement of Working Conditions and Environment (NICE) was established through collaborative arrangements between the Royal Thai Government and the United Nations. NICE became a division under the Department of Labour Protection and Welfare (DLPW), which has the primary responsibility for the protection of workers in Thailand and seeks to achieve its objectives through strengthening the existing institutional systems procedures and technical capabilities of DLPW.
The objective of NICE is to improve the protection of workers from occupational accidents and diseases and from unsatisfactory working conditions. Its main activities are as follows:
- the development and implementation of training programmes in occupational safety and health and in working conditions
- the development and operation of a management information system (MIS) to centralize all information collected and to provide a basis for planning, evaluation and coordinating policies and programmes for improving working conditions and the environment
- the development of a visible focal point for national exchange of information and expertise on working conditions and the environment
- providing technical support to increase the capability of those inspection staff who handle working conditions and the environment
- providing laboratory facilities in occupational hygiene, work physiology and ergonomics, and testing of safety equipment
- provision of support, through research and technical advisory services, for example, for extending protection to small-scale enterprises.
NICE has a staff of 50 professionals and is divided into the following sections: General Administration, Work Environment, Ergonomics and Work Physiology, Safety Technology, Safety Promotion and Training, Safety and Health Information Centre, Audiovisual and 12 regional centres in industrial estate areas throughout the country.
National Occupational Safety and Health Information Centre of Thailand
In order to improve NICE’s ability to meet its objective more effectively, NICE, in collaboration with the Geneva-based International Occupational Safety and Health Information Centre of the International Labour Office, established the National Occupational Safety and Health Information Centre of Thailand. The Centre is concerned primarily with collecting information on occupational safety, health and working conditions, from Thailand and abroad, processing and storing it and disseminating it to employers, workers, their respective organizations and related bodies and others having need for such information. This Information Centre comprises a reference library, a documentation unit, an inquiry service and a computer unit.
The library
When it opened, this library possessed only a few hundred books; now, the collection comprises approximately 3,000 book titles and 20,000 titles of microfiches on various topics on occupational safety and health such as occupational disease, safety and health engineering and working conditions. Furthermore, since 1983, the library has subscribed to 27 English-language publications and ten Thai journals. Thirty videotape titles on display and posters are available. The library’s outreach to safety and health professionals is continually expanding.
The documentation unit
The duty of this unit is to produce an occupational safety and health newsletter; guidelines, handbook and code of practice; a brochure; and information sheets.
1. The safety and health newsletter. Four newsletters are produced annually, each presenting such various offerings as safety and health updates, research news, interviews, statistics, and so on. There are 6,000 copies of each newsletter produced annually.
2. Information sheets. These are divided into four groups of topics including:
- safety and health in general, e.g., safety construction, fire prevention, and ventilation in the workplace
- practical use for safety, for example, the safe use of hand tools, or the safe use of electrical equipment
- chemical data such as might relate to sodium hydroxide or ammonia
- laws and legislation on safety, such as would concern safe working environments, and much more.
3. Recently, the documentation unit produced 109 titles of information sheets and 10,000 copies of each was printed, making an aggregate of over a million copies.
4. The guideline, handbook and code of practice. As of the mid-1990s 15 titles of this publication had been produced; for example, one of these included a guideline for the safe handling of pesticides and a handbook for first aid in industry. Each publication was printed in 3,000 copies.
5. Brochures. Ten titles of brochures were produced, having to do, for example, with the use of ear plugs at work. Of each title, 5,000 copies were printed, giving an aggregate of 50,000 copies.
The inquiry service
The inquiry service was set up with the purpose of seeking answers to questions on occupational safety and health from every person concerned in this field: labour inspectors, safety officers, employers, employees, students and others. All inquiries can reach the centre by post, telephone or facsimile. Before sending out every answer, all information is checked by NICE technical staff for correctness.
Each year, approximately 600 inquiries are sent to the centre.
The computer unit
As the focal point for collecting and exchanging information, expertise and practical experience in the area of occupational safety and health, NICE has built up several databases: on industrial establishment, accident investigation reports, labour inspection reports, safety officers, major hazards installation, boiler inspection reports, work environment inspection reports and workers’ health screening reports. In order to enhance the ability of this unit, NICE has developed a centralized computer system which will serve as the host database on occupational safety and health. This work has been done with assistance from the International Development Research Centre (IDRC) and the International Labour Organization. Meanwhile, the local area network (LAN) between NICE and the other Regional Centres on Occupational Safety and Health has been established. This linkage will help the staff from a Regional Centre to access information from NICE databases and from various CD-ROM databases in the NICE computer unit.
In order to promote as its direct concern the improved working conditions and the safety and health of Thai workers throughout the country, all the services of NICE are free of charge and NICE now supports all labour inspectors, approximately 5,000 safety officers, about 650 organized trade unions of medium- and large-size enterprises, employers and employees throughout the country. Therefore, NICE still moves on developing and strengthening its ability to protect workers from unsatisfactory performance and injuries due to unsafe working conditions and hazards in the environment.
Case Study: Malaysian Information Service on Pesticide Toxicity
Introduction
Unlike problems that command the attention of the industrialized countries with respect to pesticide hazards, namely, chronic occupational exposure and environmental contamination, the major threat posed by pesticides in many developing countries is acute poisoning itself. A recent estimate by the World Health Organization (WHO) puts the annual number of severe poisonings at 3 million, with about 220,000 deaths. It is a matter of further concern that, based on a survey of self-reported minor poisoning in four Asian countries, it was shown that each year 25 million agricultural workers in the developing countries are exposed to the danger of acute pesticide poisoning (Jeyaratnam 1990).
In Malaysia, a largely agricultural country, the use of pesticides is relatively prevalent. In Peninsular Malaysia alone, about 1.5 million hectares of land are devoted to the cultivation of rubber trees and 0.6 million hectares to oil palm trees. The employment of almost 4.3 million people is related to agriculture.
The principal legislation for the control of pesticides in Malaysia is the Pesticides Act of 1974. The main intent of this Act is the control of the manufacture and import of pesticides through registration. Other aspects of control include the licensing of premises selling pesticides and storing them for sale, the proper labelling of pesticides, and control of the import of unregistered pesticides for research and educational purposes (Tan et al. 1992).
Surveys carried out by the local agrochemical industry showed that in 1987, most of the estimated 715,000 rubber and oil palm smallholder farmers used paraquat (Shariff 1993). Over a ten-year period (1979–1988), pesticides accounted for 40.3% of the total number of 5,152 cases of human poisoning in Malaysia. Paraquat contributed 27.8%, other weed-killers 1.7%, malathion 4.7%, other organophosphates 2.1%, organochlorine compounds 2.6%, and other pesticides 1.4%. Annually, 230 million ringgit (MYR) is spent on weed-killers alone (Tara et al. 1989). It has been estimated that about 73% of poisonings involving paraquat are suicidal, compared with 14% due to accidents and 1% due to occupational exposure (Jeyaratnam 1990).
Poisoning cases due to pesticides have not been well documented. However, such incidents do occur, according to a number of selected studies. A survey showed that poisoning had occurred in 14.5% of the 4,531 farmers growing vegetables, flowers and fruits in the Cameron Highlands. Hospital admissions showed 32.1% were accidental pesticide poisoning and 67.9% suicidal cases. In Tanjung Karang, a paddy growing area, 72% of rice farmers experienced poisoning symptoms when handling pesticides, and proper clothing, goggles, shoes and respiratory masks were seldom worn. In 1989, 448 pesticide workers received medical treatment at government hospitals (Lee 1991).
In another study (Awang et al. 1991) conducted in a predominantly agricultural area, it was reported that 12.2% out of a total of 264 poisoning cases treated in a teaching hospital were due to pesticides. In yet another study (Majid et al. 1991) serum pseudocholinesterase levels, which were used as an indicator of exposure to the organophosphates, were found to be significantly lower in vegetable farmers: the degree of decrease in these blood levels is dependent upon the length of exposure to these pesticides.
The use of pesticides in Malaysia has caused serious concern. A recent report by the Malaysian Factories and Machinery Department, an agency that enforces the Occupational Safety and Health Act, revealed that the accident rate for improper handling of pesticides is four times higher than that of other industries, and is as high as 93 per 1,000 workers as compared with the national average of 23 per 1,000 (Rengam 1991). This seems to indicate that there is an insufficiency of educational materials and information on safety and an apparent lack of caution in the handling of pesticides. A 1994 report also highlighted the death of about 70 cattle, suspected to be due to paraquat poisoning as a consequence of the animals’ re-entry into a sprayed area (New Straits Times 1994).
Clearly there is an urgent need not only to collect data but also to facilitate education among those involved in the use of pesticides. It is with this in mind that a pesticide information service was developed and a pilot information system was launched throughout the country in 1989. It is part of the Integrated Drug and Poison Information Service (IDPIS) of the National Poison Centre based at the Universiti Sains Malaysia (USM) at Penang.
The primary aim of the IDPIS is to disseminate information concerning health-related matters, especially with regard to drug usage and poison control, to health professionals and the public alike (Razak et al. 1991).
The pesticide information service, which was launched through the videotex system, has had the welcome side-effect of opening up new possibilities for several other databases important for health care. IDPIS databases were continually being used as a guide for the development of other databases for the management of information relating to pesticides, industrial and household chemicals and food supplements. The Pestinfo system was one such product; it was initiated by IDPIS in collaboration with the Pesticide Board (the Malaysian pesticide regulatory body) and the Malaysian-German Pesticide Project. This arrangement has been conspicuously successful in terms of information validation and the evaluation of information needs in view of countrywide trends in pesticide use.
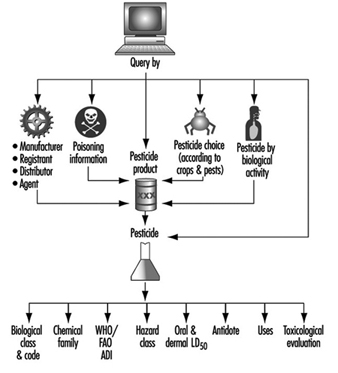
This system is focused on registered pesticides in Malaysia, but could also cater to those found throughout the Asia-Pacific region. To date, information on more that 500 biochemically active substances has been incorporated into the pesticide information system, with some 3,000 commercially available products and their profiles listed. The system is available in two modes, namely, via a videotex system and also through a computer network utilizing PCs. The former facility is called Pestinfo, while the latter is called the Pesticide Information System (see figure 1).
Figure 1. Information flow and relational access in the Pesticide Information System
Pestinfo
The Pestinfo system is the first to be made available in this region and operates via TELITA, Malaysia’s National Videotex System. Operated by Malaysia’s Telecommunication Company, TELITA provides nationwide access that is both cheap and fast. TELITA can be accessed through a television set and a decoder or a computer system equipped with a modem connected to a telephone network (Siraj 1990). Such a system is economical as each dial-up costs only MYR 0.13 (less than US$ 0.05) and access time is charged at only MYR 0.08 a minute. It is internationally unique in its approach in that it is both professional- and community-based. Information in Pestinfo is collectively packaged with two other closely interrelated on-line databases (called Drugline and Poisonline) to maximize the relational information provided to the end-user.
Pestinfo can be accessed by members of the public and by professionals alike, including those in the agricultural sectors, whether extension workers or field workers. All the databases are well integrated, and yet independent, so that all pertinent data can be easily accessed. For this reason, the USM’s Pestinfo is sequentially arranged into at least 15 subcategories.
End-users who are health care providers are also able to gain direct access to Poisonline, which carries further specialized details with regard to patient management in cases of poisoning.
Poisonline by itself is in fact a broad-base information module covering several classes of poisons, including pharmaceuticals, as well as industrial and household chemicals, food and cosmetics. It provides information on poisoning signs and symptoms according to anatomical systems, on treatment and management modalities, and on aspects of poisoning prevention. Also included are detailed antidote information and emergency treatment procedures.
The on-line Poisoning Reporting System is an outstanding feature incorporated in Pestinfo, and in Poisonline as well. This feature enables first-line reporting to be done electronically by the end-user, through a specially designed format, when any case of poisoning is encountered. It not only allows automatic documentation of all the cases reported, but simultaneously acts as an instant referral system which permits follow-up to be done systematically. Through the reporting system too, initiation of the appropriate immediate response can be undertaken to further assist the user in the management of the poisoning case. Data obtained via the Poisoning Reporting System will automatically be stored in a PC-based network system to make it possible to generate statistical reports.
Additionally, all users of Pestinfo will be able to access several other user-friendly databases on public education with emphasis on health, especially in pharmaceutical-related areas. These databases aim to educate the public on proper chemical and drug use and the maintenance of good health. The main database designed for this purpose is designated Public Infoline.
An attractive feature with regard to public education is the “Ask Your Pharmacist” service, which provides an electronic mail service for questions and answers concerning any topics relating to health. This is available free to all users.
The Pesticide Information System
The initial experience with Pestinfo has led to the development of the Pesticide Information System, which offers new possibilities of information processing for purposes of identification in cases of poisoning and can serve as a medium of reference for extension workers as well as a means of compiling poisoning events that could be of assistance in policy decision-making and planning for health centres. Because the videotex system was not fully equipped to meet these needs, an application that provides several flexible search functions was developed using the PC.
As mentioned earlier, the pesticide information service is complemented by a user-friendly network-based microcomputer system that runs on IBM-compatible PCs. This application is called the Pesticide Information System Version 2.3 and has been specially designed for maintenance of up-to-date documentation as well as for the processing of poisoning records received electronically or otherwise. It can be instructed to produce baseline statistical reports as well as to respond to other data manipulation requests as stipulated in the software. It is thus more flexible in retrieving information, given the added processing and interactive powers accorded to it by each PC. It was designed using dBase3 Plus and compiled under Clipper Summer 5.0.
The Pesticide Information System contains additional relevant information which can be readily accessed either by pesticide name, composition, registration number and name of the manufacturer or registrant of each and every product registered in the country. The main menu of the System is described in figure 1. The System is particularly suitable for use by health professionals as well as by agriculture-based personnel since it can be loaded on a portable computer.
To date, more than 50% of the poisoning cases received on-line have been pesticide-related (Latiff et al. 1991). The combination of the two modes of operation described above has undoubtedly enhanced the running of the Pesticide Information System, making possible an even faster response to a broader range of inquiries.
Future Directions
The task of compiling and disseminating pesticide information to users has been very successful even though it has been carried out on an informal basis. IDPIS has also taken new directions in the light of the rapid progress in hardware and communication technology. For instance, network-based applications will also be linked up to users nationwide through a collaboration with a network communications company that supports and provides communication link-ups for the whole country. This will further enhance the communicability of health information, as this sort of arrangement ensures economical solutions to both the user and to IDPIS as the information provider.
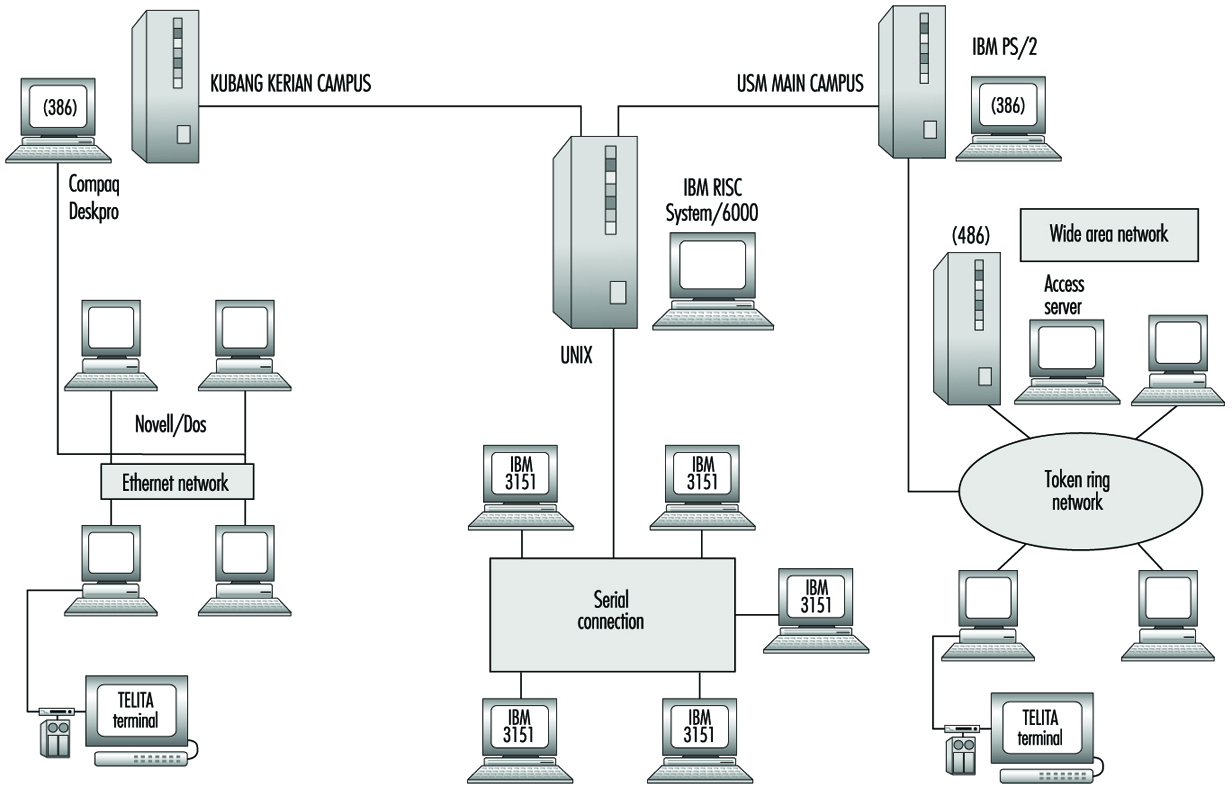
Currently, IDPIS operates on two networks, namely Token Ring and Ethernet, for the purpose of research and development work in information systems (figure 2). The former is installed at the University Teaching Hospital. Both networks are connected to an IBM RISC6000 so that information and resources within the servers of the two networks can be shared and coordinated to provide facilities for education, training and research. The networks will be designed to incorporate a tool for surveillance in the areas of pharmacoepidemiology and toxicovigilance.
Figure 2. The network-based Integrated Drug & Poison Information System (IDPIS)
In 1996 IDPIS set up its own Homepage on the Internet as the Malaysian Drug and Poison Net, at http://prn.usm.my.
Information Management
Reliable, comprehensive and intelligible information is essential for occupational health and safety. Users of such information are managers, workers, occupational safety and health professionals, safety and health representatives and occupational safety and health committee members. The responsibilities of professionals, representatives and committee members normally include providing information to others. Occupational safety and health laws in many countries require information to be provided to workers by governments, employers and chemical suppliers, among others, and to be generated by organizations such as companies to which the laws apply.
Enterprise Level Information
Viewed from within an organization, the information needed for occupational safety and health is of two basic types:
Table 1. Information required in occupational health and safety
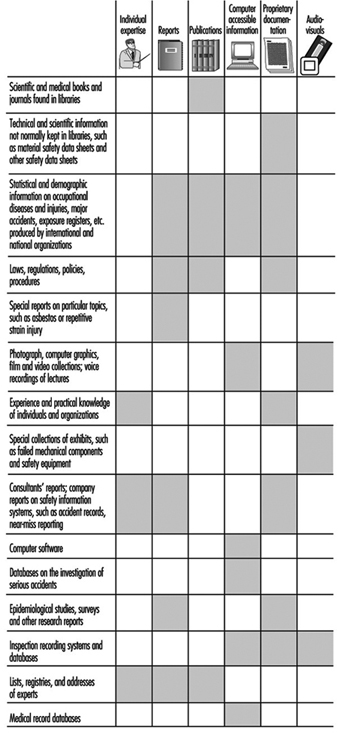
Externally generated information. This information is required within the organization to address specific needs and to solve problems. It is diverse and voluminous, and it comes from numerous sources (see table 1). To achieve the desired standards of reliability, comprehensiveness and intelligibility, it has to be managed. Information management involves three ongoing processes:
- analysing the information needs of the information users
- identifying and obtaining the information required
- supplying the information needed by the users.
Internally generated information. This information is used to help identify safety and health problems, to monitor performance and to comply with legal requirements.
Collecting, coding and storing information from accident investigations can help identify recurring accidents and highlight causal factors. For instance, records of individual workers’ exposure to particular chemicals may be important years later if questions of job-related disease arise.
Information is drawn from such data by analysis. For the analysis to yield reliable conclusions, the data must be comprehensive and trustworthy. To be trustworthy, the information must be collected and compiled according to scientific principles. For example, the question or problem should be set out clearly in advance so that all the appropriate data are collected, and that
- The types of data to be included in the compilation are strictly defined.
- Collection of the data is carried out in a consistent manner allowing for the checking of the data’s validity and integrity.
- The limitations of the data are understood and stated.
Information management involves the processes of data collection, storage, retrieval and analysis.
Organization of Information Management
The tasks of information management are often organized and conducted by an information service. The functions of such a service include:
- Ensuring that essential and up-to-date information is available when it is needed, and that users are not overburdened with excessive or redundant information.
- Making the information usable for the people who need it. Doing so often requires detailed knowledge of the needs of the persons seeking the information, and in-depth understanding of the information they seek.
- Helping users to find information for themselves.
- Actively disseminating information. Access to information in occupational health and safety is a matter of general right, not a privilege for a select group. Desk-top publishing has reduced the cost of producing pamphlets, newsletters and other materials for wide distribution.
- Collecting and providing information in an efficient and cost-effective manner. No information service has an unlimited budget.
- Keeping abreast of legal responsibilities for collecting and providing information.
- Providing or coordinating the resources and expertise required for production and analysis of internally generated information, including:
- company safety information systems (accident records, near-miss reporting)
- accident and disease statistics, registers of exposures (see also the chapter Record Systems and Surveillance)
- serious-accident investigation databases (see also the article “Audits, inspections and investigations”)
- specific data collection surveys (see also the chapter Epidemiology and Statistics)
- inspection recording systems and databases
- lists and registries of experts, addresses
- medical record databases (see also the chapters Occupational Health Services and Ethical Issues).
- Facilitating surveys and research. Methods will often be drawn from scientific disciplines such as epidemiology and statistics. The information service can help the researchers to gather the background information they need, provide computer facilities to store data, and disseminate the results of the research throughout the occupational health and safety community. In some types of study, the information service may also participate in data collection.
For the information service to fulfil all these functions successfully, it must overcome various problems. One continuing problem is the high rate of growth in the already considerable quantity of information potentially relevant to occupational health and safety. This problem is compounded by the many updates and revisions of existing information. An extension of this problem is that the apparent surfeit of information conceals a lack of multidisciplinary material. Much of the information resulting from research in medicine and engineering, for example, is communicated to specialists. It may be unintelligible to anybody else. The new knowledge is then not transferable to some potential users for whom it may be of great importance. One role of an information service is to stimulate production of multidisciplinary materials.
Other problems arise because of barriers that potential users experience in accessing or using information. For example:
- Human language. Much of the information available in occupational health and safety is framed in a language that many users do not understand well or at all. The information service should be able to transpose the information and the jargon into the everyday language of the user, and it should be able to do so without loss of quality of the information. Computers can help in overcoming such language barriers. They can assist in translation from one kind of language to another, and they can produce text automatically in one language while the user inputs information in another. By means of structured text generation computers may be able to write various reports automatically.
- Literacy. Another barrier to effective communication related to language may arise because the levels of literacy among the potential users are below the reading levels required to comprehend the more technical information in occupational health and safety. Computers offer help in overcoming this barrier with techniques that automatically analyse reading levels of written materials, which can then be assessed for suitability for particular users.
- Restrictions in distribution and availability. Some information of great importance in occupational health and safety may be classified as confidential. Examples include medical data, trade secrets, and some government documents. Copyright laws also restrict duplication of various types of information. In some circumstances, keeping information confidential is as important a responsibility as disseminating it. Confidentiality of information is a necessary consideration for persons and organizations generating information. Information management involves expertise in the avoidance of problems of confidentiality, for example by using aggregated rather than individual data, and by acquiring detailed knowledge of legitimate requirements to protect the privacy of information.
- Information access tools (finding aids) used in libraries to search for information. Not all users know how to use advanced information access tools, such as computerized catalogues (see below), and not all information is readily accessible by means of access tools. Most access tools require experience and skill, and good knowledge of the English language as well. Menu systems are an attempt to simplify the searcher’s task, but the simplification may act to conceal information. Such problems can be minimized if information professionals adopt the role of tutor.
- The computer keyboard. For some people, the computer keyboard is a barrier because they have not been trained to use it. Persons with disabilities such as repetitive strain injury cannot use it for long periods of time or at all. Voice recognition provides an alternative means of communication with the computer.
- The financial (and environmental) cost of information and document delivery. Paper is a costly medium for distributing information. Although computers are supposed to economize in paper, in practice they can be extremely wasteful of it. Carefully managed computer-based information systems are the most cost-effective (and least environmentally burdensome) way of distributing as well as storing information.
Information Services and Libraries
Information services and libraries work together. Large community and special libraries, such as law or medical libraries, often have information services. Specialized information services (including libraries) devoted to occupational health and safety are usually located within organizations such as occupational safety and health institutions, companies, universities and government departments.
The information service undertakes to answer the users’ questions and to keep them informed on important matters. It requires the support of library skills and resources to search for and to obtain the information, and to deal with some copyright matters. The information service analyses the information relative to the needs of the questioners. It compiles answers which frequently involve information from sources outside the scope of a community library (see table 1).
Some information and occupational health and safety experts differentiate between the community library and information services. They argue that unnecessary duplication of effort should be avoided for reasons of cost, if for no other. A rule of thumb is that materials on loan from a community library which is accessible to the information service’s user community should not also be available for loan from the information service. By the same token, the information service should specialize in occupational safety and health information that is not normally available through the community library. The information service should be able to focus on service to groups and individuals with defined needs in occupational safety and health. The information service may also support an organization’s legal obligation to provide or generate information, which a community library could not be expected to do.
Libraries rely on highly developed, computerized systems for the acquisition and cataloguing of materials, and for monitoring and controlling circulation. Information services access these systems through team work with specialist library personnel. The library and the information service need to cooperate closely in the organization of reference materials (materials not available for loan), interlibrary loans, on-line systems and audiovisual materials. The information service would normally have a core collection of important reference materials such as the ILO’s Encyclopaedia of Occupational Health and Safety.
Selective dissemination of information (SDI) is an aspect of information service in which cooperation is especially important between information services and community libraries. To operate a service of SDI, the information provider stores a personal search profile of the user’s needs. A group of profiles for researchers, for example, would be used for scanning the titles of scientific articles as these are published. Titles matching particular profiles are notified to the individuals concerned. While SDI can be an important service, it may be difficult to organize effectively when the information needs of the users vary considerably from time to time, as is often the case in occupational safety and health.
Training for Accessing Information
Workers and managers need to know from whom and from where they can obtain information. For example, Material Safety Data Sheets are an important source of health and safety information about chemicals used in the workplace. Workers and managers need training in seeking out and using this information. Because no occupational health and safety training can possibly cover all potential problems, knowledge about where to look for information is vital for workers and managers. Something about information sources and services should be included in all occupational health and safety training.
Information training is an essential part of the education of professionals, representatives and committee members.
The training assumption is that such people have a good grasp of occupational health and safety but need basic training in information management skills. Such skills include searching on-line information resources, and making effective use of an information service. The training should include practical experience of working as a team with professional library and information staff.
Professional library and information scientists represent the most advanced level of education and training in information work. But in their education they may have had little exposure to occupational health and safety. There is a need to increase this content, and perhaps develop appropriate specialization in the university and college education of this group.
The Computer in Information Management
All of the processes of information management increasingly involve computers. While much of the world’s information is still in paper form, and is likely to remain so for some time to come, the role of computers is increasing in every area. Computers continue to become smaller and less expensive while growing in capability. Inexpensive microcomputers, also called personal computers (PCs), can do the information management work that only a few years ago would have required an expensive mainframe computer. Three key concepts in computing are especially important in information management: databases, database management systems and computer communication.
Databases
A telephone directory is a simple example of a database. The telephone company keeps a master list of names and telephone numbers in a computer. This list is a computer database. Changes to it can be made quickly, so that it is always up to date. It is also used in the printing of the paper version of the telephone directory, which is a database for public access. Individuals and organizations often keep their own lists of frequently used telephone numbers. Such lists are personal or private databases.
The paper version of the telephone directory illustrates the basic form of a database. The information is organized by last (family) name, in alphabetical order. Initials and addresses distinguish individuals with the same last name. For each unique combination of name, initials and address there is at least one telephone number. In database terminology, each line (last name › telephone number) is a record. The names, initials, addresses and telephone numbers are called fields.
The paper form of a large database, such as a telephone directory, has major limitations. If all one has as a starting point is a telephone number, finding a name in a large city’s telephone directory is difficult, to say the least. But this task is easy for the telephone company’s computer. It simply rearranges all the records in numerical order of telephone number. The ease with which records can be rearranged is one of the most useful features of a computer database.
Library catalogues are databases which exist in both paper and electronic form. Each record corresponds to a particular book or article. The fields identify the date and place of publication, and show where a copy can be seen. Library catalogue databases exist for many subjects, including several of relevance to occupational health and safety. The ILO’s CISDOC is an example of such a bibliographic database.
In addition to the names of authors, reference data (such as title, date of publication, name of the journal), a bibliographic database often contains an abstract as well. The abstract serves to inform the searcher of the contents of the article. The user can then decide whether to obtain the full paper.
Databases can store not only abstracts, but also the full text of articles, as well as images (graphics) such as photographs and diagrams. Multimedia is a powerful application of database technology to combine sound, text, and still and moving visual images.
Advances in optical and magnetic storage media have brought down the cost of high-capacity storage. As a result, larger and increasingly complex databases are kept in personal computers or are accessible through them.
Database management systems
Arranging records in a database and many other important information management functions, such as performing a search for particular records, are carried out by means of a database management system (DBMS). The DBMS is software that enables the user to work with the data in the database. The DBMS is thus a vital element in information management. A special form of DBMS software is the personal information manager, used for personal telephone directories, to-do lists, meeting arrangements and other personal data kept by individuals.
The concept of the filter is a useful one for representing the way in which a search is structured by a DBMS. Each search can be seen as a filter which allows passage onwards only of those records that correspond to a particular profile. For example, the user could ask to see all records published on asbestos during the year 1985. The search would be expressed to the computer as an instruction to filter for all records that have the key word “asbestos” in the title and that were published in 1985. A typical instruction would read:
title key word = asbestos AND date of publication = 1985
The operator AND is known as a Boolean operator, named after George Boole (an English mathematician) who devised a system of algebraic logic in the 19th century known as Boolean Algebra. Other commonly used Boolean operators are OR and NOT. Using these, the search filters can be made highly specific.
Computer communications
Computer communications have created numerous networks, formal and informal, by which information is exchanged. Such networks often cover great distances. Many operate through the normal telephone system by means of a modem. Others use satellite communications.
In a typical network, the databases are held in one computer, the target, while a personal computer, the origin, issues the request for a search. The target’s response is to send back the records produced by the search. International standards have been evolved to ensure that this computer-to-computer communication takes place properly. Examples of such standards are ISO 10162 and 10163-1 (both 1993), which relate to search and retrieval.
In the past, computer communications required large and expensive computers. The power and capacity of personal computers is now so great that even an individual can organize networks from his or her own office or home. The network through which the individual connects to the world of information is the Internet. By 1996 this had become the fastest growing communications system the world has ever known, with a predicted one billion users by the end of the century.
An instrument of this growth is the World Wide Web. This software tool set simplifies the complexity of the Internet. With the Web the user needs no knowledge of computer languages or commands. Nor does the user have to rely on the services of an information professional, as was the case in the past. The key tool for the user is a Web browser, a computer program which permits the user to navigate through the Web. With this, millions of Web documents—the information resources of Web—become accessible. Web resources are not limited to text but are also full multimedia presentations that include sound and animation.
The multimedia capability turns the Web into an important training medium. By 1996, occupational health and safety training programmes had begun to appear on the Web. From the larger Web sites, computer programs could be downloaded for use in occupational health and safety. Other Web information resources included the increasing number of library sites of relevance to occupational health and safety on the Web. With the continuing growth of the Web, we could well see within the life span of this edition of the ILO Encyclopaedia the development of a worldwide “virtual university” of occupational health and safety.
The Internet provides the global electronic mail (e-mail) system by which individuals send private messages to each other. Increasingly the Internet is used for voice mail and video-conferencing, as well.
Messaging differs from e-mail. In messaging, all members of the group can read and respond to a message. Messaging is used for computer conferencing in which many people participate in a discussion on a particular topic. It is an inexpensive way to create a network, for example, among occupational health and safety professionals with a common interest in a particular type of occupational hazard.
File transfer is a basic process in computing. In computer terminology, a file is the basic unit of storage that allows the computer to distinguish one set of information from another. A file could be a computer program, a word-processed document, an entire database or a filtered set of records produced by a search of a database. File transfer is the means whereby computers transfer information between themselves. Various file transfer protocols (FTPs) ensure that data are not changed in any way during transfer. The special importance of file transfer for information management in occupational health and safety is that any information service with even a modest personal computer can receive all types of information from information services all over the world. File transfer and associated services are usually the most cost-effective method of transferring information. As computer capabilities improve, the breadth and scope of the information that can be transferred increases apace.
An example of on-line transaction processing would be to order a publication through a personal computer. Another example is contributing an item of data to a computer in a distant city in connection with a research project involving several geographic regions.
Other forms of computer communication that play an increasingly important role in occupational health and safety are computer-based faxback services. The user telephones the computer to order specific information. The computer then sends the information to the caller’s fax machine.
In overview, it can be said that the computer is not only the main instrument for information management, but also the great facilitator of the information revolution that continues to gather momentum in the field of occupational safety and health, as in other important areas of human activity.
Finding and Using Information
As the fund of accumulated knowledge relating to safety and health grows and is publicized by general and specialized media alike, concerns having to do with personal health in general, with environmental hazards and with occupational safety and health have been receiving increasing attention. Especially with respect to the workplace, the principle that both employers and employees have a need and a right to be supplied with adequate safety and health information is becoming more and more clearly recognized and actively implemented.
Need for Information
Reliable, comprehensive, and intelligible information is essential to the securing of occupational safety and health (OSH) objectives. This information must be conveniently accessible, up-to-date, and directly applicable to the specific circumstances of the user. But the great variety of work settings and the enormous volume and diversity of OSH information, whether touching upon toxicology, biochemistry, behavioural science or engineering, challenge the providers of such information to attend to such needs as the following:
- academic or theoretical information, required by sophisticated technical or scientific specialists and researchers
- practical information, required by regulators, employers and employees
- legislative information, required for developing and implementing policies, training employees and employers, developing and implementing OSH programmes and complying with OSH requirements. The responsibilities of safety professionals and of representatives and committee members assigned to safety-related duties normally include providing information to others. Furthermore, in many countries safety and health laws require information: (a) to be provided to workers by governments, employers, and chemical suppliers, among others; and (b) to be generated by organizations such as the companies to which the laws apply.
Occupational safety and health information is needed in order:
- To make informed decisions. Occupational safety and health information enables regulators, legislators, OSH professionals, labour and industrial organizations, employers and workers to make sound decisions concerning a healthy and safe work environment. These decisions can include the development and implementation of occupational safety and health policies, regulatory requirements, and safety and health programmes appropriate for the workplace.
- To safely discharge duties. Workers need occupational safety and health information in order to take day-to-day decisions regarding the effective yet safe performance of their duties. Employers require it in order to train their employees to take these decisions.
- To meet legislative and regulatory requirements. Without complete and accurate occupational safety and health information, workers, employers, labour organizations and occupational safety and health professionals would be unable to meet these mandates.
- To exercise rights. Increasing numbers of workers have been accorded the right to know about the hazards involved in their duties and to participate in decision-making regarding their work environment. In some countries, they have the right to refuse dangerous work.
Effective Information Dissemination
The following considerations need to be addressed in order to ensure that a dissemination programme for occupational safety and health information will be effective.
- The information must be presented in a form that is suited to the needs, circumstances and background of the end-user. For example, documents containing technical information may be more useful to occupational safety and health professionals than to those employees and employers who usually are less familiar with technical language. However, consideration should always be given to converting technical material into lay language in order to effect a comprehensive occupational safety and health information programme. To be effective, occupational safety and health information must be useful and understandable.
- Alternative audiences should be considered. For example, an article on hazards in commercial restaurants should be of interest to schools, prisons and other institutions that have dining facilities.
- Information must reach the people who need it, and a comprehensive strategy should be developed to communicate it to them. Available methods include direct mail to individuals on a purchased or developed mailing list; presentations at seminars, symposiums and training courses; exhibits at professional conferences as well as at meetings of workers and small businesses; and advertisements in trade and professional periodicals.
- Frequently, secondary disseminators can be used to augment a dissemination strategy. These cooperative endeavours encourage consistency, reduce duplication and benefit from the secondary disseminators’ strengths. For example, after serving as a document reviewer, a trade association representative may be interested in making an employee-related publication available to the membership or, minimally, advising the members of the original document’s availability. Secondary disseminators can also reduce costs because they may be willing to reprint the material for those who may need it, particularly if they are loaned the camera copy or negatives.
[V. Morgan]
User Population
Occupational safety and health encompasses the full spectrum of work activities and occupations. Information on safety and health relating to these activities is needed by people who have responsibility under the law for ensuring safe and healthy working environments or who may be detrimentally affected by hazards originating—even remotely—in work activities. These include: people who are directly involved with hazards at work or who are engaged professionally in occupational safety and health; people from other organizations that provide services to a workplace; and communities and the general public who may be exposed, perhaps at a greater remove, to any deleterious effects of work processes. Consequently, the user profile for occupational safety and health information covers an extremely broad range of types.
First, there is the decision maker. In every establishment, several categories of people occupy key decision-making positions that directly (and, often enough, indirectly) affect the health and well-being of people associated with the particular workplace, those in the surrounding communities and others who may be affected by the establishment’s practices. These people may be employers, senior line managers, members of joint safety and health committees, safety and health representatives or specialist staff responsible for safety and health, purchasing, training and information management. All of these categories of people need adequate information in order to carry out their safety-related functions effectively and to take informed decisions concerning OSH problems and how to deal with them.
Employees themselves are by no means exempt from the need to acquire and act upon OSH information. All employees, whether self-employed, working in any other part of the private sector or for a government establishment, regardless of country, location, industry or role, have a responsibility towards safety and health that is associated with their work and that requires information according to their particular circumstances. All need to know what present or potential hazards they may be exposed to and to be familiar with possible solutions and preventive measures, what their rights and responsibilities are and what resources they have at their disposal that can help them carry out their duties in this connection.
In the field of safety and health itself, managers who are specifically responsible for safety and health in the workplace and practitioners in occupational safety and health and related fields—nurses and physicians (whether in-house or on-call), safety educators, safety inspectors and others whose expertise comprises workplace safety, health and hygiene—are constantly in need of information on various occupational safety and health concerns to carry out their daily responsibilities.
Although many people and organizations are in contact with workplaces only through the services they provide, it should be borne in mind that they may have a safety-related impact on the workplaces they serve and, in turn, may be affected by their contact with these environments. The suppliers of equipment, materials and chemicals to such consumers as factories and offices, industry associations, trade unions, transport services, inspection services or worker health services, must make it their concern to examine whether their mutual relationship may imply any potential for the development of unsuspected safety problems and in order to do so, they need information concerning the specific circumstances associated with providing their services to the various workplaces.
Academics and researchers working in subject areas associated with workplace safety and health are heavy users of information on those subjects, including review materials and reports of current and past research. Technical and scientific information is also needed by professionals in fields such as engineering, chemistry, medicine and information management itself. In addition, for purposes of reporting on specific events or concerns, professionals in the public media must seek background information on OSH topics so that they may in turn inform the general public.
Another category of OSH information users are governments at all levels—local, regional and national. Policy makers and legislators and regulators, planners and other bureaucrats all deal with occupational safety and health issues that bear upon their particular functions.
On perhaps the largest scale of information need and use as far as breadth of dissemination is concerned, there is society itself. Environmental and health concerns and greater recognition of citizens’ rights, together with the impact of modern means of communication, have heightened society’s awareness of occupational safety and health issues and created a vast demand for information so that society as a whole is now making increasing—and large—demands for information on various occupational safety and health concerns. Consumers, communities in proximity to work establishments and the public in general are concerned about the activities that are carried out in workplaces and about the products they produce, and want to know about their safety and health implications. In particular, citizens’ groups and lobbyists concerned about the safety and health of communities want information on all aspects of hazards related to workplace activities such as production, emissions to the environment, transportation and waste disposal that are relevant to their cause.
There are enormous complexities in informing this diverse spectrum of information users who represent different backgrounds, education levels, cultures, languages and levels of knowledge of OSH (not to mention work environments). In order to be effective, the content, presentation and accessibility of the information must be targeted to meet the specific needs of these various categories of user.
[V. Morgan and P.K. Abeytunga]
Nature of Safety and Health Information
Quality of information
OSH information needs to be authoritative and, more important, validated by experts. Authoritative information comes from official and recognized sources or organizations, but one must be aware that information from other sources, which does not appear to have been validated, is increasingly being produced. Some examples of errors due to lack of validation are:
- Measurements are not checked and appear with the wrong abbreviations (e.g., “m” (meaning metres) instead of “mm” (meaning millimetres).
- The decimal point is in the wrong place in an exposure limit.
- The wrong chemical name is used.
- Illustrations show incorrect safety and health practices.
Problems with occupational safety and health information
Although there is an overwhelming amount of occupational safety and health information, there are areas where the information is sparse or not collected in an accessible format. The necessary information is fragmented among various subject areas and sources, many information sources are biased and information is often not available or not in a usable form for the many people who need it. To save the information seeker time the following points should be noted.
Legislation: All legislation on occupational safety and health is available but there is not, as yet, a central database of legislation from all countries. The International Occupational Safety and Health Information Centre (CIS), headquartered at the International Labour Office (ILO), has made some efforts in this area, but CISDOC, the CIS database, is not fully comprehensive. In the United Kingdom, the University of Salford European Occupational Safety and Health Law Unit has a complete up-to-date collection of the full text of the occupational safety and health legislation of the European Union Member States including the European Directives in place in each country. This collection is widening to include the Scandinavian countries and ultimately the rest of the world. The UK Safety and Health Executive Information Service headquarters in Sheffield also has a complete set of the full text of the legislation of the European Union Member States, but it is correct only up to 1991. There are a number of databases available giving reference to legislation of different countries and also some printed updating services available in different countries.
Statistics: Most countries do not have a uniform or consistent way of collecting statistics. Therefore, it cannot be assumed that any two countries use the same methodology; consequently data from different countries cannot easily be used for comparative studies.
Ergonomics: While many databases include information on ergonomics no one database exists which brings together information available from world-wide sources. A useful printed abstracting journal is Ergonomics Abstracts which is available in CD-ROM format.
Research: There is no comprehensive source of information on international research on subjects on occupational safety and health, but there are numerous journals and databases containing the results of research and research programmes. The Institut National de Recherche et de Sécurité pour la Prevention des Accidents du Travail et des Maladies Professionnels (INRS) in France has a database but it does not contain all known occupational safety and health research.
Films and videos: Films and videos help to convey information in an easy and understandable way, but there is no comprehensive database of films and videos, although new titles appear in a neverending stream. CIS has attempted to collect information on the available material in the CISDOC database, as does the UK Safety and Health Executive Information Services in the HSELINE database. Some countries, such as the UK, the US and France, produce annual catalogues which contain new titles published the previous year.
Other considerations: Because of these problems and gaps the information seeker on occupational safety and health will not find a single complete source for answers to questions. There are a number of subject areas and disciplines involved which must be checked to obtain a full picture of any of these topics.
The information user should be aware that there can be a lack of knowledge on a particular topic, or even conflicting or biased opinions, and it is wise to obtain interpretations from specialists before reaching conclusions. Some information can be easily and quickly transferred in today’s world but consideration must be given to the local conditions and also the legal requirements of the country.
Cost of Information
While many large organizations which may be government based are willing to share information at no cost or very low cost, the seeker for information on occupational health and safety must be aware that the cost of good validated information is constantly rising as authoring, production, printing and distribution costs for both printed paper and electronic products continue to rise.
Therefore a cost-effective information service which has not only up-to-date information but also high quality, trained and qualified information professionals with relevant experience is becoming a rarity. Organizations such as the International Labour Organization with its increasing number of member countries are encouraging the setting-up of focal information centres or resources where the information seeker can use and also gain access to other worldwide centres. Improved direct telecommunications should increase the capacity for supporting regional centres.
Because prices change all the time, it did not seem appropriate to include them in the following section. However, the relative costs of documents will always depend on the amount of effort needed to assemble their contents, the number of copies printed and the extent to which the cost of buying a document will be offset by the benefit of applying its contents, although the price of high quality publications may be reduced by public subsidy.
[S. Pantry]
Types of Safety and Health Information and Where to Find Them
The range of users described above defines the range of document types that constitute “occupational safety and health information”. It is helpful to distinguish between those documents that deal exclusively with occupational safety and health issues (“core" publications) and those (“others”) that contain useful information but have a different focus. The number of publications presented in table 1 has been limited by space considerations. The journals listed have been chosen because of the frequency with which they have been cited in other publications or in bibliographic databases. (Inclusion of a source should not be taken as an endorsement by the ILO and is no reflection on a publication or series that is not named.)
Table 1. Examples of core periodicals in occupational health and safety
|
Language |
Name |
Subject area |
|
English |
American Industrial Hygiene Association Journal |
Occupational hygiene |
|
American Journal of Industrial Medicine |
Occupational health |
|
|
Applied Ergonomics |
Ergonomics |
|
|
Applied Industrial Hygiene |
Occupational hygiene |
|
|
Occupational and Environmental Medicine (formerly BJIM) |
Occupational health |
|
|
Ergonomics |
Ergonomics |
|
|
Journal of Hazardous Materials |
Chemical safety |
|
|
Safety Science |
Safety science |
|
|
Scandinavian Journal of Work, Environment and Health |
Occupational health and hygiene |
|
|
French |
Travail et sécurité |
Safety science |
|
Italian |
Medicina del Lavoro |
Occupational health |
|
Japanese |
Japanese Journal of Industrial Health |
Occupational health |
|
Russian |
Gigiena truda i professional’nye zabolevanija |
Occupational hygiene |
|
Spanish |
Salud y Trabajo |
Occupational safety and health |
Traditional paper sources
The most common vehicle for information is paper, in the form of books and periodicals. These periodicals appear regularly and the books have extensive, well-established distribution networks. The primary literature is the set of journals where new observations, discoveries or inventions are reported by the persons responsible. State-of-the-art reviews also appear in primary publications. To be published in a primary publication, an article must be reviewed by a number of experts in the given field, who ensure that it reflects good practice and that its conclusions follow from the facts presented. This process is called peer review.
Typical of the “other” category are among others, the Journal of the International Institute of Noise Control Engineering and the Journal of the American Medical Association (JAMA). Government agencies in many countries print statistical periodicals that count as primary literature, even though they do not use the peer review process of the research journalists. The Morbidity and Mortality Weekly Report issued by the Centers for Disease Control and Prevention in the US is one example. Primary serials can be found in the libraries of the relevant institutions ( the JAMA in medical school and hospital libraries, for example).
There are some core mass-circulation magazines that are not peer reviewed, but that do provide primary information in the form of news of recent or upcoming events, in addition to easy-to-read articles on topics of current interest. They often include advertisements for occupational safety and health products and services that are themselves useful information on sources of supply. They may be published by public authorities—for example, Australia Newsletter and Bezopasnost’ truda v promyshlennosti (Russia), by private non-profit safety councils—Australian Safety News, Safety and Health (USA), Promosafe (Belgium), Safety Management (UK), Arbetsmiljö (Sweden), SNOP (Italy) or by private enterprises—Occupational Safety and Health Letter (USA). There are also many publications in other specialities that include useful and interesting information—Chemical Week, Plant Engineer, Fire Prevention.
The difficulty in finding information on one particular topic in the mass of the primary literature has prompted the development of secondary sources. These are guides to the literature or to recent events, such as court cases, whose official write-ups appear elsewhere. They indicate where a given document on a topic is published and usually give a brief summary of its contents. There are also citation indexes, which list the publications that cite a given document; these permit efficient retrieval of relevant publications once one key reference has been identified (unfortunately, there is none devoted exclusively to occupational safety and health). Because they must be up to date, secondary sources use the latest electronic technology to speed their publication.
In order to improve access, particularly to areas with a limited number of computers, some databases are also made available in printed form. The ILO’s Safety and Health at Work—ILO/CIS bulletin is a printed version of CISDOC which is issued six times a year and includes annual and 5-year indexes. Similarly, Excerpta Medica is available as a journal. Some secondary source databases are also available on microfiche, such as RTECS, although it is more common that the paper-based bibliographic information is supported by full-text microfiche. In these cases the database is in two parts: bibliographic references and abstracts on paper (or in electronic format) and the full text on microfiche.
Some other titles of secondary sources are Occupational Health and Industrial Medicine, and CA Selects “Occupational Safety and Health”. Others include the Science Citation Index, Social Science Citation Index, Chemical Abstracts, and BIOSIS. Because of the number of highly trained people involved in their preparation, secondary sources tend to be expensive.
Some newsletters are valuable secondary sources, as they cite important recent publications, laws or court decisions. Examples include: Core publications: OSHA Compliance Advisor (USA); Other: Chemicals in Progress Bulletin (US EPA). Whereas many government publications of this type are free, the privately researched and compiled newsletters tend to be expensive. They are rarely found in libraries; those who need them may find them worth the price of subscription.
A third major type of information source includes textbooks, encyclopaedias and compendia. Whereas reviews in the primary literature describe a domain of knowledge at the time of their writing, tertiary-source reviews recount the evolution of that knowledge and its larger context. Compendia of data bring together values originally measured and reported at different times over many years.
Core publications in this “tertiary category” include Patty’s Industrial Hygiene and Toxicology (Patty 1978), Reactive Chemical Hazards (Bretherick 1979), Dangerous Properties of Industrial Materials (Sax 1989), Handbuch der gefährlichen Güter (Hommel 1987), The Diseases of Occupations (Hunter 1978), and this Encyclopaedia. Examples of tertiary publications in the “other” category are the McGraw-Hill one-volume encyclopaedias that cover various areas of science and technology and the Kirk-Othmer Concise Encyclopedia of Chemical Technology (Grayson and Eckroth 1985), 4th edition in 27 volumes (volumes 1 to 5 are published). Readers should not overlook the large quantity of occupational safety- and health-related information to be found in the large general encyclopaedias: Britannica, Universalis, Brockhaus, etc.
Grey literature
There are many books and periodicals that do not have the same highly organized system of publication and distribution as the traditional paper literature, for example reports, data sheets and catalogues; these are referred to as grey literature because they are hard to find. Primary literature in the grey category includes government agency reports (research reports, statistics, accident investigations, etc.), theses and reports from university and commercial research institutes, such as the State Research Institute (VTT) in Finland or the European Chemical Industry Ecology-Toxicology Research Centre (ECETOC) in Belgium. A good source of information on occupational safety and health in developing countries can be found in reports of public and private agencies. Manufacturers’ catalogues can provide a wealth of information. Many exist in more than one language, so that a full set provides a guide to a kind of terminology that is rarely found in dictionaries.
To help the occupational safety and health professional find these irregularly published documents, a number of secondary sources have been created. They include government reports, announcements, index journals and dissertation abstracts. The publishers of reports may occasionally include a catalogue of previously published documents in the reports series itself. The secondary sources are not grey literature: they are published regularly and are easy to find in libraries.
A major type of grey literature is tertiary: Material Safety Data Sheets (MSDS) and criteria documents. (Some data sheets are periodicals; e.g., the Industrial Safety Data File, published monthly by Wilmington Publishers in the UK). Core sources are: national authorities (NIOSH, Arbetsmiljöinstitutet), international programmes such as the International Programme on Chemical Safety (IPCS), manufacturers´ product (MSDSs).
Laws, standards and patents in print
Most countries and regional groupings (for example, the European Union) have as a primary source an official gazette where new laws, derived regulations and patents are printed. Offprints of individual laws, patents, etc., are also issued by government printers. Standards are a more complicated case. Technical standards are frequently developed by officially recognized voluntary associations such as the American Society for Testing and Materials (ASTM) or independent government-chartered institutes (such as the German Deutsche Industrie Normen (DIN)); these bodies cover their operating costs from the sale of copies of their standards. Health and welfare standards (such as limits on working hours or on exposure to certain substances) are more often set by government agencies, so the texts appear in official journals.
The American Association of Law Libraries has begun to publish Foreign Law: Current Sources of Codes and Legislation in Jurisdictions of the World. Two of the projected three volumes have appeared (The Western Hemisphere, 1989 and Western and Eastern Europe and the European Communities, 1991). The looseleaf volumes are updated annually. This work describes the legal systems of all the Member States of the United Nations and of those dependencies that have their own legal regimes. It identifies the relevant texts under various subject headings (occupational safety and health texts are found under “labour” and industrial sector headings). The editors note numerous other secondary sources, and include a list of foreign legal publications vendors.
The compendium is the normal tool for work with laws and derived regulations—the time lag between publication of a new law in the official gazette and its inclusion in collections is generally very short, and the text may only have meaning in the context of other regulations. With standards, too, it is frequently the case that an individual standard (say, the International Electrochemical Standard (IEC) 335-2-28 on sewing machines) does not state all the applicable requirements, but cites a “parent” standard in the same series that states universal requirements (IEC 335-1, Safety of household and similar electrical appliances). Many countries have consolidated editions of their labour codes in which the central occupational safety and health legislation can be found. Similarly, the ILO and the International Organization for Standardization (ISO) publish collections of standards, while the International Register of Potentially Toxic Chemicals (IRPTC) Legal File contains information from thirteen countries.
Information in Electronic Form
The study of occupational safety and health practices and the disciplines that support them grew vigorously from 1950 to 1990. Organizing and indexing the resulting mass of publications was one of the earliest applications of computers.
Databases
As of 1996, only a few full-text databases devoted exclusively to occupational safety and health exist but the number is growing rapidly. Relevant information, however, can be found in others, such as on-line databases of the American Chemical Society Journals Online and the Dow-Jones and other news services. On the other hand, there are many secondary sources in occupational safety and health available online: CISDOC, NIOSHTIC, HSELINE, INRS, CSNB, and parts of HEALSAFE. Other sources include ERIC (Educational Resources Information Center), which is a US service; MEDLINE, which includes abstracts of the world medical literature prepared by the United States National Library of Medicine; NTIS, which indexes US “grey literature”; and SIGLE, which does the same for Europe.
Different types of existing database on occupational safety and health include the following:
- Bibliographic databases. These are databases of already published documents, where one entry (record) may include such items (fields) as author name, title of document, name of publisher or source, and location of document and its abstract. The records generally include classification indicators which are primary or secondary descriptors or keywords describing the record. Keywords are often taken from a controlled vocabulary, or thesaurus. The document itself is not stored in the database.
- Full-text databases. Unlike the bibliographic database, which contains only bibliographic information and perhaps an abstract, all relevant text (the full text) of the document is included in this kind of database. There are usually some classifiers and descriptors as well, to help in retrieval. Databases on chemical safety data sheets, each containing one to ten pages, and even entire encyclopaedias and other large documents, may be kept in such a format. Full-text databases correspond to primary and tertiary sources of printed information—they are collections of facts and full sets of data—whereas bibliographic databases are secondary sources which describe or refer to other documents. Like secondary sources in print, they may contain abstracts of the cited information.
- Factual databases. These contain measures or numerical values, such as threshold limit values of chemical substances.
- Multimedia databases. These hold pictures, drawings, illustrations, sound and video (or references and links to it) as well as the text of the document (Abeytunga and de Jonge 1992).
- Mixed databases. Elements of each of the databases described above are included in a mixed database.
Any of these databases allows a person with a question to be answered to gain access to the relevant electronic information in two ways: by using telephone lines connected to a computer where the information is stored, or by acquiring a diskette or compact disc containing the information and installing it on the user’s personal computer.
On-line services
Large safety databases that can be accessed through large computers and are always accessible whenever the computers are running are called on-line databases. The organizations that run on-line systems are referred to as their hosts (Takala et al. 1992). Until recently, on-line databases have been the only feasible means for the storage and dissemination of information via magnetic media that allows the use of computers and specially designed search software for the retrieval and downloading of data (Wood, Philipp, and Colley 1988). Practically anybody who has access to a video display (or microcomputer) terminal and telecommunication (data or telephone) line may make use of an on-line database.
With the proliferation of commercially available on-line services since the early 1970s, information has become more easily accessible. It has been estimated that as of 1997 there were well over 6,000 databases available for information retrieval in the world, covering many subjects and totalling over 100 million references. In addition, there are over 3,000 CD-ROM sources, including an ever-increasing number of full-text CD-ROMs.
On-line services, which started with bibliographic databases, rely on huge central mainframe computers which are costly to establish and maintain. As the volume of information and user population grows, the upgrading of the systems alone involves heavy investments.
Open systems, which allow computers to talk to computers anywhere in the world, are increasingly becoming a standard feature of the workplace environment, eliminating the need to host all the necessary safety data on an “in-house” computer.
Telecommunication problems and the limited number of terminals available in developing countries restrict services such as these, mostly to the industrialized world. The level of existing infrastructure; political concerns such as security, secrecy and centralization; and cultural peculiarities may severely restrict the use of on-line services. In addition, the complexity of the access and search systems further limits the number of users. Those who are only occasionally interested in the information will most likely be insufficiently skilled in the necessary techniques, or may perhaps forget the correct procedures entirely. Consequently, it is trained information specialists who tend most often to use these computerized systems. Safety professionals, particularly at the factory level, rarely use them. On-line databases are not much used for safety training purposes because of expensive, by-the-minute, user charges. On-line databases are, however, irreplaceable when the database size is so great that a CD-ROM or even several of them cannot accommodate all the desired data.
Guides to on-line searching
There are a number of useful published guides to on-line searching and databases which the OHS information seeker may wish to consult. A public or university library and information service may supply them or they may be purchased from the publisher.
Large hosts keep hundreds of different databases available 24 hours a day. In running an on-line search, various search strategies combining a number of technical requirements can be carried out. Using special searching techniques such as descriptor or keyword searching, one can range over a large amount of available materials, concentrating on the information most relevant to one’s needs. In addition to search by keyword, freetext searching, in which a search is made for specified words located in almost any field of the database text, can provide further information. Practically no limitations exist as to the size of a database, and several large databases may be put together to form a cluster. A cluster can be used as if it were a single database, so that one search strategy can be applied to all or to selected databases simultaneously. This type of All Safety database is currently being set up by one of the large hosts, the European Space Agency’s Information Retrieval System (ESA-IRS). This cluster is intended to include many large databases and its size is in the range of gigabytes, or billions of characters. Such clusters are, of course, completely computer-dependent.
Full lists of available on-line databases may be obtained from the major international hosts, namely, ESA-IRS, DIALOG, ORBIT, STN, CCINFOline and Questel. Each host identifies only its own databases; more extensive listings can be found in directories like Gale Research’s Directory of Databases (including CD-ROMs and diskettes), which is available on-line on ORBIT and Questel as well as in print.
Several compact discs offer databases devoted to occupational safety and health: the OSHA CD-ROM from the United States Occupational Safety and Health Administration (OSHA), the CCINFO discs of the Canadian Centre for Occupational Health and Safety (CCOHS) in English and in French (CCOHS 1996), the UK’s Health and Safety Executive Information Service full text CD-ROMs OSH-CD and OSH-OFFSHORE, published by SilverPlatter, which also publishes many other occupational safety and health related CD-ROMs such as CHEMBANK, EINECS, TOXLINE, and EXCERPTA MEDICA. Springer-Verlag also publish GEFAHRGUT, a CD-ROM in German. The full text of ILO Conventions and Recommendations relating to occupational safety and health can be found on ILOLEX, a CD-ROM published by Kluwer. Secondary information can also be found in the CCINFOdiscs as well as on the OSH-ROM from SilverPlatter. MEDLINE and PESTBANK are two further CD-ROMs of interest.
Many kinds of useful information sources can be obtained in this way on diskette. GLOVES lists properties of the materials used for protective gloves to help users choose the most resistant ones for a given job. Bretherick’s Reactive Chemical Hazards is available on diskette, as is an ILO collection of information on regulated workplace chemicals, exposure limits in 13 countries, risk and safety phrases to be used in labelling and citations of relevant publications.
Other diskette sources include UN-Earth, which supplies data on UN agencies, programmes and areas of competence. There exist, too, secondary guides to data. A core source is FACTS, containing abstracts of industrial accident reports held at the Dutch National Technical Institute (TNO). There are other programmes to assist the practitioner, for example, ACCUSAFE (a safety auditing system from the United States National Safety Council); EBE, an information management system developed by the CIS Regional Technical Co-operation Project for Asia.
Subject Specialists
Solving occupational safety and health problems is not simply a matter of amassing facts, someone has to use the facts to devise solutions. All occupational safety and health specialists have areas of expertise, and when problems lie outside one person’s competence it is time to call for help. Major industries often have dedicated safety and health operations, such as the Center for Chemical Process Safety of the American Institute of Chemical Engineers. Local poison control centres can help with product identification as well as workplace emergencies. Professional societies (e.g., The American Society for Testing and Materials) may publish registers of recognized experts. Specialist publications (e.g., Fire Prevention) include useful advertisements. In many countries, national agencies offer consultancy services.
Every library in the world is an information centre where the facts relevant to occupational safety and health can be found. However, not every possible question can be answered in any single library. In general, information specialists or reference librarians will know the specialized sources in their regions and can advise patrons appropriately. There are also printed guides, such as Gale Research Inc.’s Directory of Special Libraries and Information Centres (16th ed., 1993). The country-level institutions that serve as CIS National and Collaborating Centres form a network that can route requests for information to the most appropriate source of expertise.
Workplace Safety Information
Because these “publications”—posters, signs, brochures, etc.—are images rather than words or numbers, they have not been amenable to electronic storage and retrieval in the past. At the time of writing, that is changing, but the OSH specialist seeking appropriate leaflets to hand out at a half-day course in fire safety should probably turn to the local fire department before turning on a computer. Of the core OSH databases, only CISDOC systematically includes references to training materials, and the CISDOC collection is indicative rather than exhaustive.
As libraries do not normally stock catalogues, the interested individual must build up a personal collection by contacting suppliers. These include commercial firms (e.g., Lab Safety Supply International), national or government-chartered private agencies (insurers, unions). An initial set of addresses can be compiled from the source information in CISDOC.
[E. Clevenstine]
Implications for Information Access
Search strategies
Searching for information can be very frustrating. The following advice is offered, especially to those who do not enjoy the benefits of a full-fledged information service or library onsite.
How to obtain a loan or photocopy of an article, book, or report
One may make use of a local public, college, polytechnic, university or hospital library. Many provide material for reference only, but have photocopiers onsite so that items may be reproduced (with attention to copyright conditions). First one should check the indexes or catalogues of the library: if the item sought is not in stock, the information specialist or librarian will indicate another library which may be able to help. The safety specialist in one’s trade union, professional association or employing institution may be approached for assistance. Any request should be framed as helpfully as possible, with attention to the information specialist’s or librarian’s need for the following sorts of information:
- title and author(s) of article, book or report
- publisher
- year of publication
- edition
- International Standard Book Number (ISBN)—this is a unique identifier given to every document published
- title of periodical or journal
- date of periodical or journal and volume, part number and pages required
- name of database.
It can take up to three weeks or more if an item has to be borrowed from another source, but it may be obtained more quickly if one is prepared to pay for a “premium” service.
How to search for information on a particular subject.
Again one should make use of local services and contacts. Information specialists or librarians will assist the information seeker in using the various traditional indexes and abstracts. Further information given in this chapter will be of use in any search, and one might check various bibliographies, yearbooks, guides, other encyclopaedias, dictionaries and books and write to relevant organizations for further information. Using established networks pays dividends. A local information specialist or local library should be able to carry out an on-line or CD-ROM search on one or more of the computerized databases listed in this chapter.
Search techniques
The information sought should be specified clearly; for example, “injuries” is too broad a term for seeking information on a subject like “low back pain problems among nurses”. Particular aspects of a subject should be defined accurately, with mention of whatever keywords, related terms, synonyms, chemical name(s) or chemical abstracts registry numbers, and so on, that may be available to the inquirer. The name of an author who is a known expert in an area of concern may be checked to find further, more recent publications under his or her name. One should decide how much information is needed—a few references or an exhaustive search. Information published in other languages should not be overlooked; the British Library Document Supply Centre (BLDSC) collects translations on all subjects. NIOSH in the United States, CCOHS in Canada and the Health and Safety Executive (HSE) in the United Kingdom have extensive translation programmes. The HSE deposits more than 700 translations with BLDSC each year.
It is useful to keep a standard search form (see table 2), at one’s disposal to ensure that each search is carried out systematically and consistently.
Table 2. Standard search form
SEARCH FOR
|
Keywords |
______________________________ |
|
Synonyms |
______________________________ |
|
Chemical registry number |
______________________________ |
|
Known author(s) |
______________________________ |
|
How far back in time to search? |
______________________________ |
|
How many references required? |
______________________________ |
|
Where to search (e.g., indexes, libraries) |
______________________________ |
|
Journals/periodicals checked |
______________________________ |
|
Books/reports checked |
______________________________ |
|
Databases/CD-ROMs checked |
______________________________ |
|
Terms used in search |
______________________________ |
|
Number of references found |
______________________________ |
|
Date |
______________________________ |
The flow-chart in figure 1 illustrates a typical route to locating information.
Figure 1. Simple routes to information
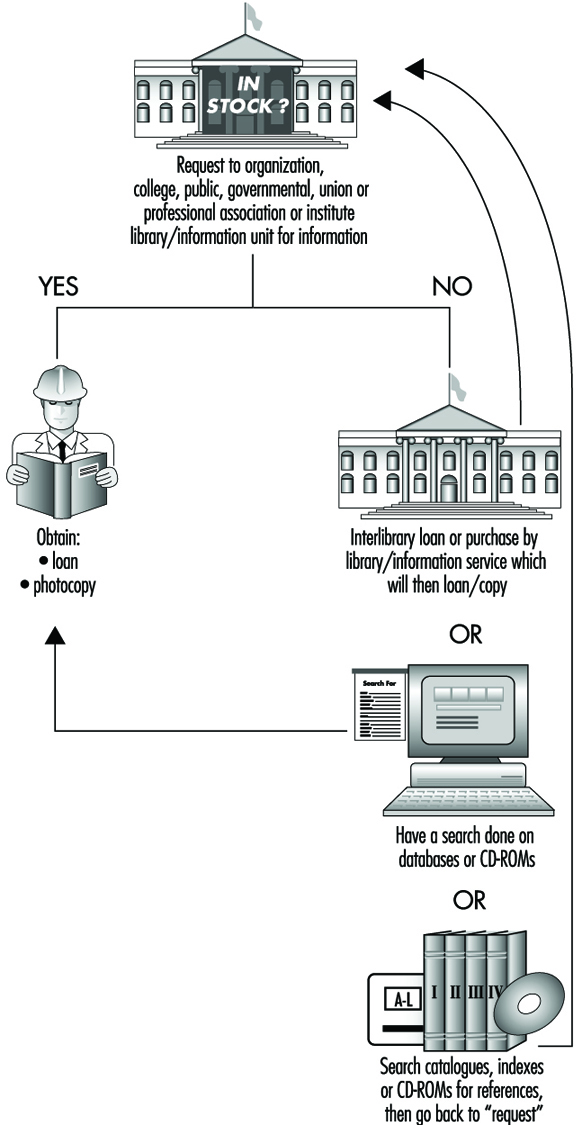
Technology advancement
Technology continues to advance rapidly, with such new developments as the worldwide delivery of high-bandwidth information at high-speed transmission speeds becoming more available at ever-lowering costs. The use of electronic mail is also making access to information easier, so that seeking guidance and advice from specialists around the world is becoming much simpler. The take-up and use of facsimile transmission of data have made a valuable contribution, again at low cost. The potential of these new informational technologies is enormous. Their facilities for accessing information at ever lower cost can increasingly help to reduce existing disparities in the availability of information between countries and between regions in a country. As the information delivery networks expand and further innovative applications are created using these beneficial technologies, more and more people will be reached, so that the role of information as a means of accomplishing desired changes in the workplace can be realized.
Cost benefit of technology
New technologies are also a boon to developing countries. It is well known that knowledge and information are vital to achieving improved quality of life and quality of the environment. Information technologies present one of the most cost-effective means for developing countries to keep pace with progress in various fields of activity. Electronic technologies may substantially enhance the ability of developing countries to achieve the benefits of improved information dissemination in a cost-effective manner.
Mainframes and on-line systems, while by no means obsolete, are costly for many institutions. Costs such as data production and telecommunications charges are high and often prohibitive. Today’s technologies, such as CD-ROM and Internet, are the best way for these countries to be informed and to come to terms with current knowledge in many areas, especially the very critical ones relating to health. The advantages that they offer for presenting large collections of information in forms that speak directly to the users and quickly and conveniently meet their diverse needs are undeniable.
Costs of an entire workstation—personal computer, CD-ROM reader and their applications—are falling rapidly. The affordability of PC-based information and the local skills in information technologies, provide developing countries with an opportunity to conduct activities on vital information at the same level as the developed world.
[S. Pantry and P.K. Abeytunga]
Information: A Precondition for Action
Production entails human activities that result in material, energy, information or other entities that are useful to individuals and to society; its development depends upon the collection, processing, dissemination and use of information. Work may be described as human activity directed to pre-set goals in the production process, with tools and equipment serving as the material instrumentality of such activity. But it should be borne in mind that in the work process the information that is continually received and organized affects and directs the process.
The work process itself contains information in the form of accumulated experience which is stored by the worker (as knowledge and skills); embodied, as it were, in tools, equipment, machinery and, in particular, by complex technological systems; and made explicit through the medium of information processing equipment. The work process is a concrete and dynamic way of using information to achieve certain set objectives. The safety components of this information are equally distributed among the various elements of work—the worker, the tools and equipment, the working environment and the objects of production; indeed, safety information should ideally be an integral part of the information needed for the production itself: instead of “how to produce something” it should be “how to safely (with lower risk) produce something”. Several experiments have demonstrated that information linking safety to production is not merely necessary but is increasingly being perceived as such.
Production entails not only the obvious technical creation of new output out of either natural raw materials or pre-existing man-made materials and goods, but also includes the modification and reorganization of information that pertains to the material production process and to the information cycle itself. The scope of the information element of a developing production process increases rapidly. Following the familiar practice of dividing the process of production into three parts, namely, energy production, materials production and information production, we may also divide its products into similar categories. However, these are usually of a mixed character. Energy is generally carried by matter, and information is either associated with matter—printed matter, for instance—or with energy, such as electrical charge or the optical and electronic impulses carried by fibre-optic lines. But, unlike material products, information does not necessarily lose its value when it undergoes reproductive processes. It is a product which can be reproduced in mass, yet its copies can be exactly as valid as the original.
Safety Information and Its Use in Production Systems
Safety information ranges over a great breadth of subjects and may assume a correspondingly great variety of forms. It can be classified as to whether it conveys statistical figures, descriptive information, reference data, original texts or quantitative or qualitative matter. It may be a statistical table setting forth a collection of quantitative data relating to accident incidence, or a chemical safety data sheet. It may be a computer-readable database, ready-to-use materials (including illustrations and drawings), model legislation and regulations, or the research results pertaining to a particular safety problem. Historically, most information needs were covered by conventional communication methods, oral and written, until the relatively recent advent of photography, radio communication, films, television and video productions. Although the methods of mass media were to facilitate electronic copying, they nevertheless lacked selectivity. Plainly, not all people need or are interested in the same type of safety information. Libraries and, in particular, specialized safety documentation centres provide a fairly comprehensive selection of documents which could provide specific details for each user of information, but their resources are not readily accessible in the form of copied matter. The latest methods of information collection, storage and retrieval, however, have solved this problem. Electronically managed information may contain the same amount of or more information than a full specialized library and it can be easily and quickly duplicated.
Safety professionals, namely, inspectors, industrial hygienists, safety engineers, safety representatives, managers, supervisors, researchers, and workers as well, will make use of information to the greatest desirable extent only if it is easily available. All that they need should be accessible right on their desks or bookshelves. Existing documentation could be converted into electronic form and organized in such a way that retrieval will be quick and reliable. These tasks are already being carried out and represent an enormous undertaking. First, selection is essential. Information should be assembled and provided on a priority basis and the retrieval process should be convenient and reliable. These goals require better organization of databases and more intelligent software and hardware.
Quantitative Safety Information
Information in factual, quantitative form is essentially expressed as numerical figures. Quantitative measures may record nominal values, such as a given number of accidents; ordinal values that define priorities; or ratios, such as may describe the frequency of accidents relative to their severity. The chief problem is to define criteria for the effectiveness of safety practices and to find the best ways to measure them (Tarrants 1980). Another problem is to design forms of information that are effective in setting forth the nature of (and the need for) safety measures and that, at the same time, are understandable to all concerned—workers, for example, or users of chemicals and chemical equipment. It has been shown that safety information will influence behaviour, but that the change in behaviour is influenced not only by the content of the information, but also by the form in which it is presented, for example, by its attractiveness and intelligibility. If risks are not effectively presented and correctly understood and recognized, one cannot expect rational and safe behaviour on the part either of workers, managers, designers, suppliers or others concerned with safety.
Quantitative risk data are not, in general, well understood. There is broad public confusion about which are the greater hazards and which the lesser, because there exists no uniform measure of risk. One of the reasons for this state of affairs is that the public media do not emphasize continually occurring problems, even the more serious ones, but tend to highlight relatively rare and striking “shocking” news.
Another factor limiting the effectiveness of safety education is that processing complex quantitative risk information may exceed the cognitive abilities of individuals to the extent that they rely on heuristics, unsystematically absorbing the lessons of experience, to make safety-related tasks manageable. In general, low risks are overestimated and high risks underestimated (Viscusi 1987). This bias may be understood if we consider that without any information, all risks would be considered as equal. Every piece of information obtained through experience will then encourage a skewed risk perception, with the more frequent but less harmful incidents receiving more attention (and more cautiously avoided) than the rarer but graver accidents.
Qualitative Safety Information
While quantitative safety information, with its sharp focus on particular hazards, is needed to concentrate our efforts on essential safety problems, we need qualitative information, conveying its fund of relevant expertise, in order to find practical solutions (Takala 1992). By its nature this sort of information cannot be precise and quantitative but is heterogeneous and descriptive. It comprises such diverse sources as legal information, training materials, audiovisuals, labels, signs and symbols, chemical and technical safety data sheets, standards, codes of practices, textbooks, scientific periodical articles, dissertation theses, posters, newsletters and even leaflets. The variety of materials makes it quite difficult to classify and subsequently retrieve these materials when needed. But it can be done and has indeed been successfully carried out: the preparation of company-, branch-, industry- and even nation-wide hazard profiles represents a practical example of the provision of qualitative information in a systematic way that at the same time attaches quantitative measures to the relative importance of the problems in question.
Another key issue is that of intelligibility. Comprehension requires that information be presented in a way that will be understood by the end user. The improper use of language, whether that of everyday speech or special technical terminology (including jargon), can create perhaps the greatest barrier to the global dissemination of safety information. Texts must be conscientiously and deliberately framed so as to make a strongly positive appeal to their intended audience.
It would be desirable to establish a comprehensive knowledge base of all accumulated safety and health information, accessible to users through interfaces tailored specially to each user group. Ideally, such interfaces would translate the desired elements of this information, without redundancy, into a format understood by the user, whether it should involve natural language, specified terminology (or absence of it), images, illustrations, drawings or sound, and would be adapted to the needs and abilities of the end user.
Impact, Presentation and Types of Safety Information
Company-level safety information and the information cycle
Studies of safety information systems within companies suggest that information flow within enterprises follows a cyclical pattern:
data collection →
data analysis and storage →
distribution of safety information →
developing preventive measures →
production of goods and materials (risks and accidents) →
data collection, etc.
The main methods used to collect data are accident investigations, safety inspections by enterprise personnel and the reporting of near-accidents. These methods concentrate on safety problems and do not pay much attention to health and industrial hygiene problems. They do not provide information on experience accumulated outside the enterprise either. It is essential to share such experience from elsewhere, since accidents are rare events and it is not likely that a sufficient number of similar incidents, especially major accidents (e.g., the disasters at Bhopal, Flixborough, Seveso and Mexico City), will occur in any one enterprise, or even in any one country, to serve as a basis for effective preventive efforts. They might, however, re-occur somewhere in the world (ILO 1988).
Safety-related activities that industry may undertake can assume a variety of forms. Information campaigns aimed at improving safety information dissemination may include safety slogans, development of a housekeeping index, positive reinforcement and training programmes for workers (Saarela 1991). In some countries, occupational health services have been established to involve health personnel in the company’s work of accident prevention. These services must have the capability to collect workplace information—to carry out job load and hazard analyses, for instance—in order to perform their everyday tasks. Further, many companies have established computerized systems for the recording and reporting of accidents. Similar systems, adapted to record accidents at workplaces according to a standard format required by workmen’s compensation bodies, have been established in several countries.
National and global safety information and theinformation cycle
Just as the safety information cycle exists within a company, there is a similar information cycle on a national, and international, level. The flow of safety information from nation to nation may be understood as a circle representing various phases in the movement of information where safety information may be either needed, processed or disseminated.
In order to assess the relative merits of various information systems, it is useful to discuss the dissemination of information in terms of the “information cycle”. The flow of safety information internationally is represented schematically in figure 1, based on Robert’s model (Robert 1983; Takala 1993). As a first step, safety information is identified or described by the author of a document, where the word “document” is used in its broadest sense, and may denote indifferently a scientific article, textbook, statistical report, piece of legislation, audiovisual training material, chemical safety data sheet or even a floppy disc or an entire database. Whatever its type, however, information may enter the cycle in either electronic or printed form.
Figure 1. The information cycle
MISSING
- Information is sent to a publisher or editor, who will evaluate its validity for publication. The publication of a document is, plainly, an important factor in its usefulness and general accessibility simply because unpublished materials are difficult to locate.
- Published documents can be used directly by a safety professional or they may target a non-professional end-user such as the worker at the workplace (for example, chemical safety data sheets).
- The document may then be sent to an information centre. In the case of documents that convey primary information (results of original research, for example), the centre will systematically collect, screen and select whatever useful information they may contain, thus carrying out the first rough reading of large volumes of documents. A regularly published or updated secondary publication, such as a periodical or database containing abstracts or reviews, may be published or made available by the information centre. This will draw attention on a continuous basis to significant developments in occupational safety and health.
- Such secondary publications or databases target mainly safety professionals. Examples of such secondary databases and publications are the CISDOC database and the Safety and Health at Work bulletin from the International Labour Organization, and the NIOSHTIC database from the National Institute for Occupational Safety and Health (NIOSH) in the United States. The interchange vehicle between a given institutional entity (e.g., a company) and the national or global information cycle is in all cases the user. The user is not necessarily an individual safety professional, but may also be the institution’s safety management system. A user of published material may furthermore communicate feedback directly to the author or publisher, a practice common for scientific publications.
- At this point in the information cycle, the published document may be modified as a result of “reality testing”, the stage at which the safety professional puts the information to actual use in order to reduce the number of accidents or work-related diseases, or to solve other problems at work.
- Experience contributes to better anticipation of health hazards and accidents.
- Experience may result in new research findings in the form of reports and documents which are sent to the publisher: thus the cycle is completed.
Applications of safety information
Information may be used for a number of purposes: training within and outside the company; design of machinery, processes, materials and methods; inspection and control operations. The varied character of such uses implies that the information must be prepared in a suitable form for each type of user. Users themselves modify and reprocess the information into new information products. For example, an inspectorate may draft new rules and regulations, machine manufacturers may set new guidelines in the light of their involvement in safety standardization activities, producers of chemicals may compile their own Material Safety Data Sheets and labels, and trainers may produce manuals, audiovisuals and handouts. Some information may be of a specific, ready-to-use type that offers direct solutions to individual safety and health problems, while other pieces of information may set forth improvements in the production process, such as a safer method, machine or material. Despite their variety, the common element among all of these information products is that in order to be useful, in the end they will have to be employed by a company safety management system. Resources involving processes, materials and methods must be selected, purchased, transported and installed; people to use them selected and trained; follow-up and supervision exercised; and outputs must be distributed with steady attention to a wide range of information needs.
Computerized Safety Information Systems
Computers are the latest link in the developmental process that ranges over all the information media, from spoken and written language to contemporary electronic systems. In fact, they may be able to do the work of all of the preceding types of information manipulation. Computers are particularly suitable for this purpose because of their ability to handle highly specific tasks involving large volumes of information. In the field of safety information, they may be especially useful for the types of need listed in figure 2.
Figure 2. Possible applications for computerized information
Individual Disputes over Health and Safety Issues
Types of Disputes
An individual dispute arises from a disagreement between an individual worker and his or her employer over an aspect of their employment relationship. An individual dispute exemplifies a “rights dispute”, that is a dispute over the application of the terms of legislation or an existing agreement, whether a collective bargaining agreement or an individual written or oral contract of employment. Thus there could be a dispute over the amount of wages paid or their manner of payment, work schedules, working conditions, entitlement to leave and so forth. In the field of health and safety an individual dispute may arise in relation to the use of personal protective equipment, extra payments for carrying out dangerous work (hazard pay – a practice now frowned upon in favour of eliminating hazards), refusal to perform work that poses an imminent danger and observance of health and safety rules.
An individual dispute may be initiated by a worker complaining to vindicate what he or she believes to be a right, or reacting to employer-imposed disciplinary action or dismissal. If a dispute involves similar claims on behalf of individual workers, or if an individual dispute raises a point of important principle for a trade union, an individual dispute can also lead to collective action and, where new rights are then sought, to an interests dispute. For instance, a single worker who refuses to perform work that he or she thinks is too hazardous may be disciplined or even dismissed by the employer; if the trade union sees that this work poses a continuing danger for other workers, it may take up the issue with collective action, including a work stoppage (i.e., a lawful strike or a wildcat strike). In this way, an individual dispute may lead to and become a collective dispute. Similarly, the union may see a point of principle which, if not recognized, will lead it to make new demands, thus giving rise to an interests dispute in future negotiations.
The resolution of an individual dispute will depend largely upon three factors: (1) the extent of legal protection afforded to workers in a particular country; (2) whether or not a worker falls under the umbrella of a collective agreement; and (3) the ease with which a worker can have enforcement of his or her rights, whether they are afforded by law or collective agreement.
Disputes over Victimization and Dismissal
In most countries, however, certain rights enjoyed by an individual will be the same no matter what the length of his or her engagement or the size of the enterprise. These normally include protection against victimization for trade union activity or for reporting to the authorities an employer’s alleged infringement of the law, called “whistle-blower” protection. In most countries, the law affords protection to all workers against discrimination on the basis of race or sex (including pregnancy) and, in many cases, religion, political opinion, national extraction or social origin, marital status and family responsibilities. Those grounds are all listed as improper bases for dismissal by the ILO Termination of Employment Convention, 1982 (No. 158), which also adds to them: union membership and participation in union activities; seeking office as, or acting or having acted as, a workers’ representative; and filing a complaint, or participating in proceedings against an employer involving alleged violation of laws or regulations, or having recourse to administrative authorities. These last three are clearly of particular relevance to the protection of workers’ rights in the field of safety and health. The ILO Committee of Experts on the Application of Conventions and Recommendations recently highlighted the seriousness of retaliatory measures, in particular in the form of termination of employment, taken against a worker who reports the employer’s failure to apply occupational safety and health rules while the workers’ physical integrity, health and even lives may be at risk. When fundamental rights or the physical integrity of lives of workers are at stake, it would be desirable for conditions as to proof (reversal of the burden of proof) and measures of redress (reinstatement) to be such as to allow the worker to report illegal practices without fearing reprisals (ILO 1995c).
However, when it comes to retention of employment in practice, two major determinants of an individual’s employment rights are the enforcement mechanism available to vindicate these rights and the type of contract of employment under which he or she has been engaged. The longer the term of the engagement, generally the stronger the protection. Thus a worker still in the probationary period (in most countries a matter of a few months) will have little or no protection from dismissal. The same is true for a casual worker (i.e., a person engaged on a day-to-day basis) or a seasonal worker (i.e., one employed for a limited, recurring period). A worker with a contract of employment for a fixed term will have protection during the period covered by the contract, but will normally not have a right to its renewal. Workers engaged on contracts that are without limit of time are in the most secure position, but they may still be dismissed for specified reasons or more generally for what is often termed “gross misconduct”. Their jobs may also be eliminated in the course of company restructuring. With increasing pressures for greater flexibility in the labour market, the recent trend in legislation governing contracts of employment has been to make it easier for employers to “shed labour” in the restructuring process. In addition, a number of new forms of work relationships have arisen outside the traditional one of employer/employee. Without employee status, the individual concerned may have little legal protection.
Disputes over a Worker’s Refusal to Perform Hazardous Work
An individual dispute may often arise around the question of an employee’s refusal to perform work that he or she believes to pose an imminent hazard; the belief must be that of a reasonable person and/or be held in good faith. In the United States the reasonable belief must be that performance of the work constitutes an imminent danger of death or serious physical injury. In some countries, this right is negotiated in collective bargaining; in others, it exists by virtue of legislation or court interpretations. Unfortunately, this important right is not yet universally recognized, despite its inclusion as a basic principle in Article 13 of the ILO Occupational Health and Safety Convention, 1981 (No. 155). And even where the right exists in law, employees may fear retaliation or job loss for exercising it, particularly where they do not enjoy the backing of a trade union or an effective labour inspectorate.
The right to refuse such work is normally accompanied by a duty to inform the employer immediately of the situation; sometimes the joint safety committee must be informed as well. Neither the worker who refused nor another in his or her place should be (re)assigned to the work until the problem has been resolved. If this happens nonetheless and a worker is injured, the law may (as in France and Venezuela) subject the employer to severe civil and criminal penalties. In Canada, both the worker who refused the work and the health and safety representative have rights to be present while the employer undertakes an on-the-spot investigation. If the employee still refuses to do the work after the employer has taken remedial measures, an expedited government inspection can be triggered; until that has led to a decision, the employer cannot require the worker to do that work and is supposed to provide him or her with an alternative assignment to avoid earnings loss. A worker designated to replace the one who refused must be advised of the other’s refusal.
Recognition of a right to refuse hazardous work is an important exception to the general rule that the employer is the one who assigns work and that an employee is not to abandon his or her post or refuse to carry out instructions. Its conceptual justification lies in the urgency of the situation and the presence of interests of public order to save life (Bousiges 1991; Renaud and St. Jacques 1986).
Participation in a Strike
Another way in which an individual dispute can arise in connection with a health and safety issue is the participation of an individual in strike action to protest unsafe working conditions. His or her fate will depend on whether the work stoppage was lawful or unlawful and the extent to which the right to strike is guaranteed in the particular circumstances. This will involve not only its status as a collective right, but how the legal system views the employee’s withdrawal of labour. In many countries, going on strike constitutes a breach of the employment contract on the part of the employee and whether this will be forgiven or not may well be influenced by the overall power of his or her trade union vis-à-vis the employer and possibly the government. A worker who has a strong theoretical right to strike but who can be temporarily or permanently replaced will be reluctant to exercise that right for fear of job loss. In other countries, engaging in a lawful strike is explicitly made one of the grounds on which a worker’s employment may not be brought to an end (Finland, France).
Means of Dispute Resolution
The ways in which an individual dispute can be resolved are in general the same as those available for the resolution of collective disputes. However, different labour relations systems offer varying approaches. Some countries (e.g., Germany, Israel, Lesotho and Namibia) provide labour courts for the resolution of both collective and individual disputes. The labour courts in Denmark and Norway hear only collective disputes; individual workers’ claims must go through the regular civil courts. In other countries, such as France and the United Kingdom, special machinery is reserved for disputes between individual workers and their employers. In the United States, individuals have rights to bring actions claiming unlawfùl employment discrimination before bodies that are distinct from those before which unfair labour practice claims are pressed. However, in non-union situations, employer mandated arbitration for individual disputes is enjoying popularity despite criticism from labour practitioners. Where an individual is covered by a collective bargaining agreement, his or her grievance can be pursued by the trade union under that agreement, which usually refers disputes to voluntary arbitration. An individual’s ability to win a claim may ofien depend on his or her access to procedures that are fair, affordable and rapid and whether he or she has the support of a trade union or an able labour inspectorate.
Collective Disputes Over Health and Safety Issues
In recent years, legislation, international instruments and general literature on occupational health and safety have highlighted the importance of information, consultation and cooperation between workers and employers. The focus has been on averting disputes rather than their settlement. Some contend that in the area of occupational safety and health, the interests of workers and employers converge and thus disputes can be more easily avoided. Yet disputes still arise.
The employment relationship is subject to diverging interests and priorities as well as changing concerns, including with respect to health and safety considerations. The potential thus exists for disagreement or conflicts which may harden into labour disputes. Although there may be a consensus regarding the importance of health and safety issues in general, disagreement may arise regarding the need for specific measures or their implementation, particularly where extra time or money is involved or production will be decreased. When dealing with health and safety, there are few absolutes: what is an “acceptable” risk, for instance, is relative. Where to draw the line on a number of issues is open to debate, particularly since complicated situations may have to be addressed with limited technical assistance and a lack of conclusive scientific evidence. Also, perceptions in this area are continually shifting as a result of the use of new technology, medical and scientific research, changing societal attitudes and so on. The potential for diverging views and dispute in this area is, therefore, considerable.
In all areas of labour relations, but perhaps particularly with respect to health and safety concerns, the equitable and efficient resolution of disputes is essential. Disputes may be resolved at an early stage as a result of one side to the dispute making the other aware of relevant facts. This may be done formally or informally. Disputes may also be dealt with through internal complaints procedures, usually involving progressively higher levels of management. Conciliation or mediation may be needed to facilitate the resolution of the dispute, or a solution may be imposed by a court or an arbitrator. In the health and safety area, the labour inspector may also play an important role in dispute settlement. Some disputes may lead to work stoppages, which in the case of health and safety issues may or may not be considered a strike under the law.
Categories of Disputes
Within the purview of health and safety considerations, a variety of types of dispute may arise. Although the categories may not always be obvious, giving the dispute a particular definition is often important for determining the mechanisms for settlement that will be applied. Disputes in general can be classified as individual or collective, depending on who initiates, or has the authority to initiate, the dispute. Generally, an individual dispute is one involving an individual worker and a collective dispute involves a group of workers, usually represented by a trade union. A further distinction is often made between rights disputes and interest disputes. A rights dispute (also called a legal dispute) involves the application or interpretation of rights under law or an existing provision set out in a contract of employment or a collective agreement. An interest dispute, on the other hand, is a dispute regarding the creation of rights or obligations or the modification of those already in existence. Interest disputes primarily arise in relation to collective bargaining.
Sometimes defining a dispute as collective or individual will determine the resolution procedures; however, it is usually the interaction between the categories that is relevant – collective rights disputes, collective interest disputes and individual rights disputes are usually given distinct treatment. This article deals only with the first two categories, but it should be kept in mind that some stages in the process of collective disputes will coincide with those for individual claims.
Whether a dispute is considered to be collective or individual may depend on whether the law allows the trade union to raise a dispute on the issue in question. To obtain authority to negotiate over health and safety and other issues, in a number of countries a trade union needs to be registered with the public authorities or to be recognized as being representative of a given percentage of the employees concerned. In some countries, these prerequisites also apply with respect to the authority to raise rights disputes. In others, the employer must voluntarily agree to deal with the trade union before the trade union can act on behalf of the employees.
A trade union may be able to initiate procedures to settle a collective rights dispute where health and safety obligations affecting the workplace as a whole are at issue: for example, if there is a provision in the collective agreement or in legislation providing that noise levels are not to exceed a certain limit, particular precautions are to be taken with respect to machinery, or personal protective equipment is to be provided and the employer does not comply with these provisions. Collective rights disputes may also arise, for example, where the employer fails to consult with or provide information to the health and safety committee or representative as required by law or the collective agreement. Due to its inherently collective nature, an alleged breach of the collective agreement may in some countries be considered a collective dispute, particularly if it concerns the implementation of provisions of general applicability such as those on safety and health, even if in reality only one worker is immediately and directly affected by the employer’s breach. Breach of legal provisions may be considered collective where the trade union acts on behalf of all affected workers, where it is entitled to do so as a result of the breach.
Collective interest disputes over health and safety matters may also take many forms. Such disputes could arise out of negotiations between a trade union and an employer over the formation or responsibilities of a health and safety committee, the introduction of new technology, specific measures for dealing with hazardous materials, environmental control and so on. The negotiations may involve general statements of principle regarding health and safety or specific improvements or limits. Where the parties reach an impasse in the negotiations, dealing with the dispute is considered an extension of the freedom to bargain collectively. In the Collective Bargaining Convention, 1981 (No. 154), the ILO has noted the importance of setting up bodies and procedures for the settlement of labour disputes as part of the process of promoting collective bargaining (Article 5(2) (e)).
Grievance Procedures
The term grievance procedure is generally used to mean internal procedures set out in the collective agreement to resolve disputes regarding the application or interpretation of the collective agreement (rights disputes). Similar procedures are, however, often set up even in the absence of a union or collective agreement to address problems and complaints of workers, as they are seen to be a fairer and less costly means of dispute resolution than litigation (McCabe 1994). The collective agreement normally provides that the complaint is to be dealt with through a multi-stage procedure involving increasingly higher levels within the organization. For example, a dispute on a health and safety matter may go first to the immediate supervisor. If not resolved at the first stage, the supervisor and the health and safety representative may then undertake an investigation, the findings of which are submitted to a manager or perhaps the health and safety committee. If the dispute remains unresolved, a senior level of management may then intervene. There may be several stages which need to be exhausted before outside procedures are set in motion. The agreement may go on to provide for third party intervention in the form of inspection, conciliation and arbitration, which will be discussed in more detail below.
The Examination of Grievances Recommendation (No. 130), adopted by the ILO in 1967, underlines the importance of grievance procedures for rights disputes, whether individual or collective. It states that workers’ organizations or the representatives of workers in the undertaking should be associated with the employers in the establishment and implementation of the grievance procedures within the undertaking. Rapid, uncomplicated and informal procedures are urged. Where procedures within the undertaking are exhausted without a mutually acceptable resolution being reached, the Recommendation goes on to set out procedures for final settlement, including joint examination of the case by the employers’ and workers’ organizations, conciliation or arbitration and recourse to a labour court or other judicial authority.
Conciliation and Mediation
The collective agreement or law may require collective disputes to be submitted to conciliation or mediation before further dispute settlement procedures can be invoked. Even without being required to submit a dispute to conciliation, the parties may voluntarily ask a conciliator or mediator, an impartial third party, to assist them in reducing their differences and ultimately reaching an agreement. In some industrial relations systems, a distinction is made, at least in theory, between conciliation and mediation, though in practice the line is difficult to draw. The role of conciliators is to re-open the lines of communication, if they have been broken, to help the parties to find common ground so that an agreement can be reached and perhaps make findings of fact. The conciliator does not, however, present formal proposals to resolve the dispute (although in practice such a passive role is seldom adopted). A mediator, on the other hand, is expected to propose terms of settlement, though the parties remain free to accept or reject the proposals. In many countries there is no real distinction between conciliation and mediation, with both mediators and conciliators seeking to assist the parties to a dispute to find a solution, using the most appropriate tactics of the moment, sometimes remaining passive, sometimes putting forth proposals for settlement.
Conciliation is one of the most widely used and is considered to be one of the most effective procedures for the settlement of disputes over interests. In the process of collective bargaining, conciliation can be seen as the continuation of negotiations with the assistance of a neutral party. In a growing number of countries, conciliation is also used at the initial stages of settling rights disputes. The government may make conciliation services available or may set up an independent body to provide such services. In some countries, labour inspectors are involved in conciliation.
The ILO, through the adoption of the Voluntary Conciliation and Arbitration Recommendation, 1951 (No. 92), has advocated that free and expeditious voluntary conciliation machinery be “made available to assist in the prevention and settlement of industrial disputes between employers and workers” (Paras. 1 and 3). The role of conciliation in ensuring the effective exercise of the right to bargain collectively is reflected in the European Social Charter (10 October 1961, Article 6(3)).
Arbitration
Arbitration involves the intervention of a neutral third party who, though not a member of the established judiciary, is authorized to impose a decision. In several countries, virtually all rights disputes arising out of the application or interpretation of the collective agreement are dealt with through binding arbitration, sometimes following an obligatory and unsuccessful conciliation stage. Arbitration is available in many countries as a voluntary procedure, while in others it is compulsory. Where arbitration is imposed as a method of resolving disputes over interests it is usually limited to the public service or essential services. In some countries, however, particularly developing countries, arbitration of interest disputes is more generally applicable.
Arbitration is dealt with in the Voluntary Conciliation and Arbitration Recommendation, 1951 (No. 92). As with conciliation, the Recommendation concerns itself with disputes that are voluntarily submitted to arbitration and provides that in such cases the parties should abstain during the proceedings from striking or locking out and should accept the arbitration award. The voluntary nature of submission to arbitration is also stressed in the European Social Charter (ibid.). If one of the parties or public authorities can initiate arbitration proceedings, arbitration is considered to be compulsory. The ILO’s Committee of Experts on the Application of Conventions and Recommendations has stated that, in the case of interest disputes, compulsory arbitration is generally contrary to the principles of the Right to Organize and Collective Bargaining Convention, 1949 (No. 98), as it vitiates the autonomy of the bargaining parties (ILO 1994b). A final award binding on the parties concerned, if they have not voluntarily submitted a dispute to arbitration, may also be viewed as unreasonably limiting the right to strike. The Committee of Experts has stated that “such a prohibition seriously limits the means available to trade unions to further and defend the interests of their members, as well as their right to organize their activities and to formulate their programmes, and is not compatible with Article 3 of Convention No. 87 [the Freedom of Association and Protection of the Right to Organize Convention, 1948].” (ibid., para. 153.)
Labour Administration Authorities
The labour administration in most countries has a variety of responsibilities, of which one of the most important is inspecting work premises to ensure compliance with the laws on employment, in particular those on health and safety. Inspectors do not require a labour dispute in order to intervene. However, where a dispute alleges a violation of the law or agreement, they may play an important role in achieving its settlement.
In dispute settlement, labour administration authorities generally play a more active role in health and safety matters than in other areas. The role of the inspector in disputes may be defined in collective agreements or legislation involving health and safety, general labour law, workers’ compensation or a specific industry. In some countries, the health and safety representative or committee is entitled to lodge complaints with the labour inspector, or other public labour or health and safety officer, against the employer. The inspector may be requested to intervene where there is an allegation that health and safety regulations are not being observed. The labour administration authorities may also be required to intervene due to their competence under state workers’ compensation schemes.
The inspectors may have authority to issue improvement, prohibition or stop-work orders, levy fines or penalties or even initiate prosecutions. Civil or criminal proceedings may be available depending on the nature of the violation, the seriousness of the consequences, prior knowledge of the likely consequences and whether the violation has been repeated. An inspector’s decision can normally be reviewed on appeal to a higher public officer, a specialized labour or health and safety body or the court. Separate administrative and appeal mechanisms may exist for different industries (e.g., mining).
The Labour Inspection Recommendation (No. 81), adopted by the ILO in 1947, encourages collaboration between officials of the labour inspectorate and workers’ and employers’ representatives. European Union Framework Directive No. 89/391/EEC on Health and Safety adopted in 1989 provides that workers and their representatives are entitled to appeal to the authority responsible for health and safety protection at work if they are not satisfied that the measures taken by the employer will ensure safety and health at work. According to the Directive, workers’ representatives are to have the opportunity to submit their observations during inspection visits by the competent authority (Article 11(6)).
Regular and Labour Courts
Since rights disputes involve rights or obligations that are already in existence, the general principle underlying their settlement is that they are to be resolved ultimately by courts or arbitrators and not through industrial action, such as a strike. Some countries leave ordinary courts to deal with all disputes over rights, irrespective of their labour relations character. However, in many countries, labour courts (called in some countries “industrial courts”) or specialized tribunals will deal with rights disputes. They may deal with rights disputes generally or only certain types of disputes, such as claims of unjustified discipline or dismissal. The principal reason for having such specialized judicial bodies is the need for speedy, inexpensive and informal procedures and specialized capacity in labour matters. The delays and expenses involved in the ordinary court system are not considered acceptable when dealing with employment, which is an area of crucial importance to a person’s life and often involves a relationship that must continue even after the dispute is settled. Jurisdiction over collective rights disputes may be divided between the ordinary and the labour courts: for instance in some countries the only collective disputes that a labour court is competent to adjudicate are those arising out of an alleged breach of a collective agreement, leaving breaches of legal provisions to the regular courts.
Often representatives of workers and employers as well as an independent judge sit on labour courts or tribunals. Labour courts consisting of only workers’ and employers’ representatives also exist. This bipartite or tripartite composition is aimed at ensuring that the members have expertise in industrial relations matters and, therefore, that relevant issues will be canvassed and dealt with in light of practical realities. Such composition also assists in giving credibility and persuasiveness to the decision. The workers’ and employers’ representatives may have an equal voice in determining the outcome of the dispute or they may be entitled to act only in an advisory capacity. In other countries, judges unaffiliated to either side of industry resolve collective rights disputes.
In a few countries, labour courts deal both with collective rights disputes and interest disputes. As discussed above with respect to arbitration, where adjudication is compulsory for interest disputes, the voluntary nature of collective bargaining is undermined.
Work Stoppages
A concerted work stoppage may take place for a variety of reasons. Most commonly it is understood as a form of pressure on the employer to agree to terms and conditions once an impasse has been reached in the collective bargaining process. This is considered to be a strike in most countries and is normally viewed as a legitimate means of workers and their organizations to promote and protect their interests.
The right to strike is expressly recognized as a general right under the International Covenant on Economic, Social and Cultural Rights (16 December 1966, Article 8(1) (d)). The European Social Charter (supra, Article 6(4)) links the right to strike to the right to bargain collectively and states that workers and employers are to have the right to collective action in cases of conflicts of interest, subject to obligations arising out of the collective agreement. The Charter of the Organization of American States (30 April 1948, Article 43(c)) defines the right to strike as an integral element of freedom of association, along with the right to collective bargaining. The ILO’s Committee of Experts on the Application of Conventions and Recommendations and Governing Body Committee on Freedom of Association have recognized the right to strike as arising out of the general principles of freedom of association set out in the Freedom of Association and Right to Organize Convention, 1948 (No. 87), though the right to strike is not mentioned specifically in the text of the Convention. The Committee of Experts has stated that “a general prohibition of strikes constitutes a considerable restriction of the opportunities opened to trade unions for furthering and defending the interests of their members... and of the right of trade unions to organize their activities” (ILO 1994b, para. 147).
In some countries the right to strike is a right of a trade union and thus strikes not organized or authorized by the trade union are considered “unofficial” and unlawful. In other countries, however, the right to strike is a right of the individual, even though it is normally exercised by a group, in which case the distinction between “official” and “unofficial” strikes is of little significance.
Even where the right to strike is recognized in principle, certain categories of workers may be excluded from enjoying the right, such as members of the police or armed forces, or senior public servants. The right may also be subject to certain procedural limitations, such as requiring prior notice to be given or a ballot to be taken in support of the strike. In a number of countries, the parties are obliged to refrain from striking or locking out, either absolutely or on issues regulated in the agreement, while the collective agreement is in force. This “peace obligation” is often set out specifically in legislation or collective agreements, or may be implied through judicial interpretation. The right to strike in many countries is severely restricted, or even prohibited, in essential services. This restriction is permitted under ILO principles if the services to which it applies are limited to those the interruption of which would endanger the life, personal safety or health of the whole or part of the population. (ILO 1994b, para. 159.)
In the field of disputes over health and safety issues, a distinction must be made between those relating to negotiating for certain rights (for instance, determining the precise functions of a safety representative in the implementation of a general health and safety policy) and those relating to situations of imminent danger. Where a dangerous situation exists, or is believed to exist, legislation or collective agreements generally give workers the right to stop work. This is often expressed as an individual right of the worker or workers who are directly at risk. A variety of formulas exist for justifying a work stoppage. An honest belief that a danger exists may suffice, or an objective danger may need to be shown. Regarding who is in danger, workers may cease working if they are immediately threatened, or the right may be broader and include causing danger to others. Collective work stoppages in solidarity (sympathy strikes) are not generally envisaged by the provisions (and therefore may be considered unlawful), but in fact they do take place. Authority to stop work may also be vested in the workplace health and safety representatives. Work may then be suspended pending a final decision by labour administration authorities.
The Occupational Safety and Health Convention, 1981 (No. 155), provides that workers shall not suffer undue consequences from having removed themselves from a work situation which they believe presents an imminent and serious danger to their life or health (Article 13). A similar provision can be found in Article 8(4) of the European Union’s 1989 Framework Directive, which refers to “serious, imminent and unavoidable danger”. Often the right to stop work due to imminent danger is contained in health and safety legislation. In some countries, the right is embodied in labour legislation and conceived as a work stoppage that does not constitute a strike; therefore, the procedural prerequisites for a strike do not need to be met and the peace obligation is not breached. Similarly, where an employer closes the workplace in compliance with a stop-work order or because of a reasonable belief that a dangerous situation exists, it is generally not considered to give rise to a lockout.
Labour Relations Aspects of Labour Inspection
The key role played by labour inspection in the development of labour relations is indisputable; in fact, the history of labour law is the history of the labour inspection system. Before the establishment of the first labour inspectorates, labour laws were mere declarations of goals whose infringement resulted in no sanctions. True labour law arose when a specific body was charged with ensuring compliance with the rules, thereby giving effect to the law by means of legal sanctions.
The first national attempts to establish a system of labour inspection centred on the creation of voluntary bodies which acted without remuneration to protect women and children employed in industry and which were a response to the peculiar nature of economic liberalism. Experience soon imposed the necessity to create a body of a coercive nature that would really be able to protect the working population as a whole. The first law introducing an official factory inspectorate was passed in Great Britain in 1878 on the grounds that the requirements relating to the appointment of honorary enforcers had not been faithfully carried out and therefore the protection measures had not been applied. The law conferred on factory inspectors the following basic powers: unrestricted entry into factories, free questioning of workers and employers, requiring the production of documents and the capacity to settle disputes and ascertain infringements of the laws.
The evolution of the various regulations had the result in subsequent years of reaffirming the authority of factory inspectors as administrative officials, separating out and gradually eliminating their function as judges. The idea emerged of the inspector as a paid civil servant but also a participant in the labour relations system, an official of the state who ensures that the government shows its human side through his or her direct presence in the workplace. With this goal in mind, the inspectorate was converted into a basic organ for the development and application of legislation; it became, in fact, a fundamental pillar of social reform.
This dual concept of its activities (strict control and active observation of the facts) reveals the origins of inspectoral activity within legal institutions. On the one hand, the labour inspectorate works with clear, specific legal texts which have to be applied; and, on the other hand, the correct articulation and exercise of its functions lead it to interpret the letter of the law by means of direct action. The inspector has to know not only the letter of the law, but also the spirit behind it and he or she must therefore be sensitive to the world of work and have a profound knowledge not only of the rules but also of the technical and production procedures. Thus the inspectorate is an organ of labour policy, but also a creative institution of progress, progress that is fundamental to the very evolution of labour law and labour relations.
The evolution of the world of work has continued to deepen and reinforce the role of the inspectorate as an independent organ of control at the centre of the labour relations sphere. In a parallel way, modification and change in the world of work generate new aims and forms of internal relationships in the complex microcosm that is the workplace. The original concept of a paternalistic type of relationship between the inspector and those subject to inspection gave way early on to more participatory action by the representatives of employers and workers, with the inspector involving the interested parties in his or her activities. Hence the role of conciliator in collective disputes was assigned to labour inspectors right from the beginning in the legislation of many countries.
Together with the consolidation of the role of the state inspector, advances in the trade union movement and professional organizations aroused a greater interest on the part of the workers themselves in active participation in inspection. After various attempts by the workers to incorporate themselves in direct inspectorial action (e.g., attempts to establish worker-inspectors as existed in Communist countries), the independent and objective status of the inspectorate came to be favoured, with its definitive transformation into a state organ consisting of civil servants. However, the participatory attitude of the workers’ and employers’ representatives was not lost in their contacts with the new institution: the inspectorate, in addition to being an independent entity, was also converted into a participant holding a special place in the dialogue between those representatives.
From this perspective the inspectorate developed progressively and in parallel with social and economic evolution. For example, the protectionist tendency of the state during the first third of the twentieth century resulted in substantial modifications in labour law, adding a considerable number of graduates to those already enrolled as inspectors. One immediate consequence of these developments was the creation of a true labour administration. Similarly, the emergence of new forms of work organization and the pressure of market forces on the public service at the end of the twentieth century have of course also affected the labour inspectorate in many countries.
The inspectorate, originally conceived as a body of legal controllers, has modified its own activity over time and converted itself into a useful and integrated mechanism responsive to the technological needs of new forms of work. In this way labour law has also grown, adapting itself to the new needs of production/services and incorporating regulations of a technical nature. Hence the appearance of related sciences: the sociology of labour, ergonomics, occupational safety and health, labour economics and so on. With new emphases and perspectives going beyond the purely legal sphere, the inspector became an active element of the true application of rules in workplaces, not only by virtue of applying sanctions but also by advising employers’ and workers’ representatives.
Generalist versus Specialist
The national regulations themselves have adopted two different organizational approaches to inspection: the generalist inspectorate (which arose in continental Europe) and the specialist inspectorate (which originated in the United Kingdom). Without entering into the arguments concerning the advantages of one or the other system, the terminology of the titles reveals two quite different perspectives. On the one hand, the generalist (also called unitary) approach involves inspectorial action performed by a single person, assisted by various technical institutions, on the assumption that the general appreciation of a single inspector can provide a more logical and coherent basis for the solution of various labour problems. The generalist inspector is an arbiter (in the sense of the word used in ancient Rome) who, having consulted with the relevant specialized bodies, tries to respond to the difficulties and problems posed by the particular workplace. The generalist inspector handles labour relations disputes directly. The specialist inspectorate, on the other hand, takes direct action through the use of a pre-eminently technical inspector, who has to resolve specific problems within a more narrow scope. In a parallel manner, purely labour relations questions are dealt with by bipartite or sometimes tripartite mechanisms (employers, trade unions, other government agencies), which try to resolve conflicts through a dialogue among them.
Despite the differences between the two trends, the point of convergence lies in the fact that the inspector continues to be a living expression of the law. In the generalist inspection system, the inspector’s central position allows him or her to recognize immediate needs and make modifications accordingly. The Italian situation is particularly illustrative of this: the law empowers the inspector to issue executory rules to complement the general regulations, or to substitute more specific regulations. In the case of the specialist inspectorate, the inspector’s in-depth knowledge of the problem and of the technical standards allows him or her to assess possible non-compliance with reference to the legal requirements and prevention of hazards and also to propose alternative solutions for immediate application.
The Present Role of Inspection
The central role of the inspector means that, in addition to his or her supervisory function, the inspector frequently becomes a pillar of support for existing social institutions in the labour field. Apart from the function of general control as regards legal requirements concerning working conditions and workers’ protection, the inspectorate in many countries supervises the fulfilment of other requirements relating to social services, the employment of foreign workers, vocational training, social security and so on. To be effective, a labour inspectorate should have the characteristics embodied in the ILO’s Labour Inspection Convention, 1947 (No. 81): sufficient staffing levels, independence, adequate training and resources and the powers necessary to carry out inspections and to achieve solutions to the problems found.
In many countries the inspection services are also given responsibilities in the resolution of labour disputes, participation in the negotiation of collective agreements at the request of the parties, activities relating to the gathering and evaluation of socio-economic data, drafting memoranda and expert technical advice in their fields for the labour authorities and other functions of a purely administrative nature. This extension and multiplicity of tasks arises from the concept of the inspector as an expert in labour relations with specific technical knowledge. It also reflects a special vision of a framework for the operation of enterprises which sees the inspectorate as the ideal institution for evaluating and solving the difficulties of the world of work. However, this multidisciplinary character in some cases gives rise to a basic problem: dispersion. It may be asked whether labour inspectors, being obliged to assume multiple responsibilities, do not run the risk of having to favour activities of an economic or other nature to the detriment of those which should be the essence of their mission.
The major controversy over the determination of the typical and priority functions of the inspectorate relates to the function of conciliation of labour disputes. Although surveillance and supervision surely make up the daily activity of the inspector, it is no less certain that the workplace is the centre of labour conflict, whether individual or collective. The question thus arises as to whether all the control and evaluation activity of the inspectorate does not imply, in some measure, “palliative” action as regards conflict itself. Let us examine an example: the inspector who suggests the application of legal requirements concerning noise is in many cases responding to a complaint from the workers’ representatives, who consider that the high decibel level affects work performance. When advising the employer, the inspector is proposing a measure for resolving an individual conflict generated within day-to-day working relationships. The solution may or may not be adopted by the employer, without prejudice to the subsequent initiation of legal action in case of non-compliance. In a similar manner, an inspector’s visit to a workplace to examine whether an act of anti-union discrimination has occurred is aimed at diagnosing and if possible eliminating, internal differences that have arisen in that respect.
To what extent are the prevention and solution of conflicts different in the daily activity of the inspector? The answer is not clear. The close intermeshing of all the spheres that form part of the labour field means that the inspectorate is not only a living expression of the law but also a central institution in the labour relations system. An inspectorial body that examines the world of work as a whole will be able to assist in securing better conditions of work, a safe working environment and, as a result, improved labour relations.
Labour Relations Aspects of Training
A training system should be a constituent of an overall human resource development policy and programme. This may be at the enterprise, industry or national level. Its practical implementation will be greatly assisted if paid educational leave is available (see box). Where such arrangements are not incorporated into national legislation (as they are in the Labour Codes of France and Spain, for example), then leave entitlement to attend appropriate occupational safety and health training should be negotiated by representatives of employers and workers as part of the collective bargaining process.
Highlights of the ILO Paid Educational Leave Convention, 1974 (No. 140)
Aim of the standard
To promote education and training during working hours, with financial entitlements.
Obligations
A ratifying State is to formulate and apply a policy designed to promote the granting of paid educational leave for training at any level; general, social and civic education; trade union education.
This policy is to take account of the stage of development and the particular needs of the country and shall be coordinated with general policies concerning employment, education and training, and hours of work.
Paid educational leave shall not be denied to workers on the grounds of race, colour, sex, religion, political opinion, national extraction or social origin.
Financing shall be on a regular and adequate basis.
The period of paid educational leave shall be treated as a period of effective service for the purpose of establishing claims to social benefits and other rights deriving from the employment relationship.
by Chapter Editor (excerpted from ILO Convention No. 140, 1974).
Any negotiated arrangements for training would identify appropriate subject matter as well as administrative, financial and organizational arrangements. Training on occupational safety and health should embrace the following:
- health and safety laws and means of enforcement
- employers’ attitudes to health and safety
- workers’ attitudes to health and safety
- health and safety issues and the means of improving health and safety practices.
The two key components of any training approach are content and process. These will be determined by the objectives of the training activity and the aspirations of the participants and trainers. The overall objective here would be to contribute to the improvement of health and safety at the workplace and so content should be based on identifying practical means of achieving improvement. Such an approach would require an assessment of the health and safety problems faced by workers. In general terms these should include:
- safety hazards, such as lifting, carrying, machinery, falls, ladders
- health hazards and problems, such as eyestrain, chemicals, noise, dust, aches, pains
- welfare issues, such as washing facilities, first aid, housing.
This methodological approach would allow for the systematic treatment of issues by means of describing the problem and reviewing how it came to be known, who was involved, what action was taken and the result of the action.
An important outcome of this approach is the identification of “good” and “bad” occupational safety and health practices, which, theoretically at least, can provide the basis for common action by employers and workers. To sustain this methodology, important information requirements need to be addressed. These include securing documentation on health and safety laws, standards and technical information and identifying the further information required to resolve the hazard/problem, such as policies or agreements produced by other trade unions and employers and alternative solutions and strategies.
Successful training activity will require the use of active learning methods, which are developed by drawing on the experience, skills, knowledge, attitudes and objectives of participants. Experience and knowledge are reviewed, attitudes are analysed and skills are developed and improved through working collectively. As part of this process, participants are encouraged to apply the results of their training activity to their work environment. This focuses training activity on practical outcomes and relevant content.
Questions that the trainer and trainees need to ask of process and content are: What are we gaining that can be applied to our work environment? Is the training improving our skills and knowledge? Is it helping us to operate more effectively in our work environment?
The trainer should address these questions at the planning, implementation and evaluation stages of any training programme and the methodological process encourages participants to make the same demands during the process of training activity.
Such a method, often referred to as “learning through doing”, draws widely upon the participants’ experiences, attitudes, skills and knowledge. The objectives of training activity should always refer back to practical outcomes; therefore, training activities should integrate this method. In occupational safety and health programmes this could include the activities outlined in table 1.
Table 1. Practical activities-health and safety training
|
Activity |
Related skills |
|
Identifying hazards |
Critical analysis Sharing information Reviewing information |
|
Problem solving |
Critical analysis Sharing information Working collectively Developing strategies |
|
Finding information |
Using resources Researching skills Re-using information |
|
Forming attitudes |
Critical analysis Re-evaluation of attitudes Effective argument and debate |
Occupational safety and health training has the potential to develop workers’ and employers’ awareness of issues and to provide a basis for common action and agreement on how problems can be overcome. In practical terms, good health and safety practice not only provides for improvement in the working environment and potential productivity gains, but also encourages a more positive attitude to labour relations on the part of the social partners.
Consultation and Information on Health and Safety
Worker Participation in Health and Safety Matters
Worker participation in safety organization in plants can be planned in many ways, depending on national law and practice. This article refers only to consultation and information arrangements, not related forms of employee involvement. Additional coverage of specific aspects somewhat linked with consultation and information (e.g., participation in or initiation of inspections, participation in training activities) is offered elsewhere in this chapter.
The idea of employers and employees working jointly to improve health and safety at work is based on several principles:
- Workers can contribute to prevention of industrial accidents by spotting and warning about potential hazards and giving notice of imminent dangers.
- Involving employees educates and motivates them to cooperate in the promotion of safety.
- Ideas and experiences of workers are regarded as a useful contribution to safety improvement.
- People have a right to be involved in decisions that affect their working life, particularly their health and well-being.
- Cooperation between the two sides of industry, essential to improve working conditions, should be based on an equal partnership.
These principles have been laid down in the ILO Occupational Safety and Health Convention, 1981 (No. 155). Article 20 provides that “co-operation between management and workers and/or their representatives within the undertaking shall be an essential element of organizational and other measures” in the area of occupational health and safety. Also the ILO Communications within the Undertaking Recommendation, 1967 (No. 129), Paragraph 2(1), underlines that:
...employers and their organizations as well as workers and their organizations should, in their common interest, recognise the importance of a climate of mutual understanding and confidence within undertakings that is favourable both to the efficiency of the undertaking and to the aspirations of the workers.
The underlying philosophy is that employers and employees have a common interest in a self-regulating system in industrial accident prevention; actually they are more interested in occupational safety than in occupational health, since the occupational origin of accidents is more simple to establish and they are thus compensated more easily. Also for this reason safety representatives in many countries were historically the first employee representatives at the workplace to have their rights and duties determined by law or collective agreements. Today there is probably no subject in labour relations and human resources management on which the social partners are so ready to collaborate as in health and safety matters. But in some national contexts trade unions have not put sufficient resources into the safety and health effort to make it a major issue in either negotiations or contract administration.
Information and Consultation Rights in Legislation in ILO and European Union.
The general obligation for employers to disclose information in health and safety matters to workers and/or their representatives and seek their opinion via consultative arrangements is provided by Article 20 of the ILO Prevention of Major Industrial Accidents Convention, 1993 (No. 174). This norm prescribes that “the workers and their representatives at a major hazard installation shall be consulted through appropriate cooperative mechanisms in order to ensure a safe system of work”. More specifically workers and their representatives have the right to:
(a) be adequately and suitably informed of the hazards associated with the major hazard installation and their likely consequences; (b) be informed of any orders, instructions or recommendations made by the competent authority; (c) be consulted in the preparation of and have access to, the following documents: (i) safety reports, (ii) emergency plans and procedures, (iii) accident reports.
As a consequence of these information and consultation rights, workers are entitled “to discuss with the employer any potential hazards they consider capable of generating a major accident” (Article 20(f)).
More generally ILO Convention No. 155 lays down rules concerning occupational safety and health and the working environment, providing for effective arrangements at the level of the undertaking (be they regulated by law or collective bargaining or even left to local/domestic practices) under which “(c) representatives of workers... are given adequate information on measures taken by the employer to secure occupational safety and health and may consult their representative organizations about such information provided they do not disclose commercial secrets” (Article 19). The same norm adds that under these arrangements workers or their representatives must be “enabled to enquire into and are consulted by the employer, on all aspects of occupational safety and health associated with their work”. And for this purpose “technical advisers may, by mutual agreement, be brought in from outside the undertaking”.
ILO Recommendation No. 164 supplementing Convention No. 155 (Paragraph 12) clarifies that information and consultation rights on safety and health matters should be granted to a variety of participatory institutions: workers’ safety delegates, workers’ safety and health committees, joint safety and health committees and other workers’ representatives. This text also states important principles affecting the nature and the content of information/consultation. These practices should first of all enable the above-mentioned specialized forms of workers’ representation “to contribute in the decision-making process at the level of the undertaking regarding matters of safety and health” (Article 12(e)).
These are not simply rights to know and to be heard: workers and their representatives should “(a) be given adequate information on safety and health matters, enabled to examine factors affecting safety and health and encouraged to propose measures on the subject”. They should also “(b) be consulted when major new safety and health measures are envisaged and before they are carried out and seek to obtain the support of the workers for such measures” and “(c)... in planning alterations to work processes, work content or organization of work, which may have safety or health implications for the workers”.
The principle under which “representatives of the workers... should be informed and consulted in advance by the employer on projects, measures and decisions which are liable to have harmful consequences on the health of workers” (ILO Working Environment (Air Pollution, Noise and Vibration) Recommendation, 1977 (No. 156), Paragraph 21) reflects the idea of an “effective policy of communication” stated in general terms by Paragraph 3 of ILO Recommendation No. 129, which prescribes that “information is given and that consultation takes place between the parties concerned before decisions on matters of major interest are taken by management”. And in order to make these practices effective, “steps should be taken to train those concerned in the use of communications methods” (Para. 6).
The participative approach in labour relations in the area of health and safety is confirmed by other international legal texts. A meaningful example in this respect is offered by the Framework Directive 89/391/EEC on the introduction of measures to encourage improvements in the safety and health of people working in countries of the European Union. Article 10 provides for the employer an obligation to take appropriate measures so that workers and/or their representatives receive, in accordance with national law and/or practices, all necessary information” concerning safety and health risks, protective and preventive measures (also for first aid, fire-fighting and evacuation of workers and in case of serious and imminent danger). This information has to be “provided in a suitable form to temporary workers and hired workers present in the establishment or enterprise”. Additionally “workers with specific functions in protecting the safety and health of workers, or workers’ representatives with specific responsibility for the safety and health of workers” must have access to risk assessment and protective measures, reports on occupational accidents and illnesses suffered by workers and all information yielded by protective and preventive measures, inspection agencies and bodies responsible for safety and health.
Article 11 of the EC Directive links consultation and participation. In fact employers are under the obligation to “consult workers and/or their representatives and allow them to take part in discussions on all questions relating to safety and health at work”. That presupposes “the consultation of workers, the right of workers and/or their representatives to make proposals [and] balanced participation in accordance with national laws and/or practices”. The document continues, prescribing that:
workers with specific functions in protecting the safety and health of workers or workers’ representatives with specific responsibility for the safety and health of workers shall participate in a balanced way, in accordance with national laws and/or practices, or be consulted in advance and in due time by the employer...
The objective of these rights is to cover all measures which may substantially affect health and safety, including the designation of employees required to implement certain measures (first-aid, fire-fighting and evacuation of workers) and the planning and organization of adequate health and safety training throughout the employment relationship (upon hiring, job transfer, introduction of new working equipment, introduction of any new technology).
The choice is clear: no to conflict, yes to participation in health and safety labour relations. This is the meaning of the EC Framework Directive, which goes beyond the simple logic of the right to information. The system is based on a genuine form of consultation, since it must take place “in advance and in good time” – in other words, not only prior to decisions being adopted by the employer but also soon enough for proposals and comments to be made about them.
The Directive also uses the ambiguous expression “balanced participation”, a formula open to various interpretations. The notion is broader than (or, at least, different from) that of consultation, but not to the extent of constituting a form of joint decision making, which would prevent employers from taking measures which had not been approved by the workers or their representatives. It seems quite clearly to be a form of participation going beyond mere consultation (otherwise the article heading “consultation and participation” would be nonsense) but not necessarily as far as joint decision making. The concept is left somewhat vague: it embraces a range of multiple forms of worker participation which vary considerably between Member States of the European Union. And in any case the Directive does not place any obligation to provide a specific form of balanced participation.
In both the ILO and EC texts, information seems to be a concept whereby management informs the employees’ representatives body in writing or in a meeting. Consultation means that normally joint committees are set up in which employees’ representatives are not merely informed by management, but can also comment and expect justification from management in the event of differing opinions. Certainly these concepts differ from negotiation (when a contractually binding outcome is worked out in joint negotiating committees at company or inter-company level) and co-determination (where the employee has a right of veto and decisions require the agreement of both parties).
For Community-scale undertakings and groups thereof, EU Council Directive No. 94/45/EC of 22 September 1994 requires setting up European Works Council or an information and consultation procedure. The information relates “in particular to transnational questions which significantly affect workers’ interests” (Article 6(3)). Time will tell if this is used for safety and health purposes.
Role of Workers’ Representatives in Risk Assessment and Improvement of Work Environment: Record-keeping
The active nature of consultation is also stressed in Article 11(3) of the EC Framework Directive, which states that either workers with specific functions in this area or workers’ representatives in general “may call on the employer to take appropriate measures and submit to him relevant proposals by means of which all risks to workers may be reduced and/or sources of danger eliminated”.
The Framework Directive, with its provisions on risk management, while placing clear responsibilities on employers, also favours the greater involvement of workers and their representatives in consultations on management strategies in health and safety. Employers must assess risks and present their risk-control management systems in a plan or statement. In all cases they are expected to consult with and involve workers and/or their representatives in all the design, implementation and monitoring of these systems. But it is undeniable that this Directive, by conferring relevant participative rights to workers, has at the same time adopted an approach of “self-assessment”. Other EC Directives require, among other things, the recording of the results of measurements and examinations and lay down the employees’ rights of access to these records.
Also ILO Recommendation No. 164 (Para. 15(2)) provides that:
...employers should be required to keep such records relevant to occupational safety and health and the working environment as are considered necessary by the competent authority or authorities; these might include records of all notifiable occupational accidents and injuries to health which arise in the course of or in connection with work, records of authorisation and exemptions under laws or regulations in the field and any conditions to which they may be subject, certificates relating to supervision of the health of workers in the undertaking and data concerning exposure to specified substances and agents.
It is a general principle worldwide that employers are required to keep records, for instance of accidents and occupational diseases, or on the use or presence of biological and environmental monitoring.
National Laws and Practices
By comparison, labour relations systems exist (e.g., Italy) where statutory law provides no specific right to information and consultation in occupational safety and health for workers’ representatives, although such a right is often included in collective agreements. Italian legislation gives the workers themselves the right to control the implementation of standards relating to the prevention of accidents and occupational diseases, as well as the right to develop studies and adopt adequate measures in order to safeguard health and safety at work. In other systems (e.g., in the United Kingdom) in order to obtain disclosure of information on matters of health and safety as provided by law, it is necessary first to have safety representatives appointed; but this is possible only if there is a recognized trade union in existence at the undertaking. In situations where the employer refuses or withdraws the necessary status of a recognized trade union, information and consultation rights cannot be exercised.
These national experiences raise the question: To what extent is effective workers’ participation in health and safety conditional on the adoption of statutory arrangements? Certainly some legal backing seems to be helpful, the optimum amount of legislation being probably at a point where it provides for the election of workers’ representatives with sufficiently strong rights to allow them to function independently of management, while at the same time leaving room for a certain variety in the organizational arrangements for participation in different sectors and corporations.
In general labour relations systems provide by law that workers’ representatives are to be informed and consulted in health and safety matters. When joint committees composed of management and employee representatives are established, they enjoy considerable powers. For instance in France the committee for health, safety and working conditions may propose preventive measures: an employer declining to accept them must give detailed reasons. But empirical evidence demonstrates that sometimes safety representatives seem more efficient than joint committees since they are less dependent on the existence of a cooperative relationship.
Through various forms of representational participation, employees in general enjoy rights recognized by ILO Conventions and Recommendations (plus EC directives, when applicable) mentioned earlier with special reference to industrialized free-market economies. Safety representatives and/or works councillors have a right to be informed and consulted by the employer on all issues relating to the company’s operations and the improvement of working conditions, including health and safety matters. They have the right to see all relevant documents that the employer is statutorily obliged to keep and also to see any statements on the subject and the results of any research. They may also have copies of any of these documents if required.
Effectiveness of Information and Consultation Rights
Apart from specific aspects (such as use of experts, participation in or initiation of inspections, protection from victimization) which strongly affect the effectiveness of information and consultation rights in health and safety, there are general factors which have to be taken into account in this respect. First, the size of the undertaking: the effectiveness of controls is on the wane in small units, where trade unions and other forms of workers’ representation are almost absent. Small-sized establishments are also least likely to implement statutory requirements.
Secondly, where safety representatives are integrated into the formal trade union organization at the workplace, they are more likely to achieve the expected improvements in the working environment. Thirdly, consultation and information arrangements in health and safety reflect the more conflictual (e.g., UK, Italy) or cooperative (e.g., Germany, Scandinavian countries, Japan) nature of the surrounding labour relations system. And in general, collaboration between management and labour favours the disclosing of information and consultation.
Fourthly, the role of managerial initiative should not be underestimated. More than the existence of statutory rights, consultation and information are effective when there is the presence of a managerial culture which supports them. Employers—by their attitude towards training, their commitment to disclosing information and their speed in answering queries—are able to create an adversarial or cooperative climate. Legal backing is essential to guarantee full independence to worker representatives to act in this field, but then the success of information/consultation arrangements depends largely on the voluntary choice of both sides of industry.
Lastly it must be said that a precondition for successful worker representation in health and safety at the workplace is public awareness. It is fundamental for this specialized form of employee involvement that such a need is perceived and valued by people at work. There is empirical evidence that workers identify health and safety as one of the most significant concerns in their working life.
Highlights of the ILO Paid Educational Leave Convention,
1974 (No. 140)
Aim of the standard
To promote education and training during working hours, with financial entitlements.Obligations
A ratifying State is to formulate and apply a policy designed to promote the granting of paid educational leave for training at any level; general, social and civic education; trade union education.
This policy is to take account of the stage of development and the particular needs of the country and shall be coordinated with general policies concerning employment, education and training, and hours of work.
Paid educational leave shall not be denied to workers on the grounds of race, colour, sex, religion, political opinion, national extraction or social origin.
Financing shall be on a regular and adequate basis.
The period of paid educational leave shall be treated as a period of effective service for the purpose of establishing claims to social benefits and other rights deriving from the employment relationship.
by Chapter Editor
(excerpted from ILO Convention No. 140, 1974).
Safeguards on Use of Information
Comparative experience demonstrates that in general safety representatives are considered to be in breach of confidence if they reveal any information relating to an employer’s production processes and other professional secrets. Furthermore, they are obliged to use discretion with regard to any information provided to them which the employer indicates is confidential. ILO Convention No. 155 recognizes this by providing that enterprise-level representatives may consult their representative organizations about occupational health and safety information “provided they do not disclose commercial secrets” (Article 19(c)).
In some systems (e.g., Greece) employee representatives on works councils are obliged not to communicate to third parties information acquired which is of fundamental importance to the enterprise and which, if disclosed, would harm the enterprise’s competitiveness. The employee representatives and the employer are supposed to decide jointly what information can be disclosed. Under other systems (e.g., Luxembourg), where if employee representatives disagree with an employer’s classification of information as confidential, they may refer the matter to the inspectorate for a decision.
In some countries the duty of confidentiality is only implicit (e.g., Italy). Also when there is no specific requirement in this respect (e.g., United Kingdom), employee representatives cannot receive from the employer information relating to the health of individuals (unless their consent is given), information that would damage national security or information that would damage the employer’s undertaking. Finally (e.g., Sweden) the duty to observe confidentiality may not prevent safety representatives from passing on the information received to the executive board of their trade union, which will also be bound to observe confidentiality.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."