General Profile
It has been estimated that over a million people work in approximately 150,000 salons and barber shops in the United States. These men and women, barbers and cosmetologists (also referred to as “technicians”), perform a wide range of services, including shaving; cutting and styling hair; giving manicures and pedicures; applying artificial nails; and performing a variety of chemical hair processes including bleaching, colouring, hair relaxing and permanent waving. In addition, some technicians provide facial treatments and removal of body hair.
Technicians may be exposed to a variety of potential health and safety hazards on the job, including:
Chemicals. According to an analysis conducted by the US National Institute for Occupational Safety and Health (NIOSH), 30% of the nearly 3,000 chemicals used in cosmetology are classified by the US government as toxic substances. Ventilation in many shops is often inadequate to eliminate chemical exposure.
Diseases. Because of their close contact with clients, technicians may be exposed to a variety of infectious diseases, ranging from colds and flu to impetigo, chicken pox and hepatitis.
Ergonomic hazards. Barbers and cosmetologists also suffer from a range of musculoskeletal disorders associated with repetitive motion, prolonged standing, cramped work spaces and poorly designed tools and equipment.
Scheduling. Working hours may be irregular and extended. Many technicians work in “split shifts”, splitting their work day to cover 12 to 14 hours of client services.
Other problems. These include poor housekeeping and electrical and fire hazards.
As a result of exposure to these and other hazards, an increasing number of people are being forced to leave their chosen profession. A recent study by Nellie Brown, director of the Chemical Hazards Information Program at Cornell University, found that 20% of US hair stylists leave their jobs because of work-related illness (New York Times Magazine, 7 March 1993).
Despite increasing evidence of risk, there are few regulations protecting barbers and cosmetologists. In the United States, cosmetic products are regulated by the Food and Drug Administration (FDA), which is oriented towards consumer protection and has a limited ability to address worker health and safety issues. Like regulatory agencies in many countries, the FDA does not require product manufacturers to conduct safety tests before public marketing, to list ingredients on the labels of products sold for professional use only or to give the FDA information on consumer complaints. Nor does the FDA routinely test products on its own initiative; any testing done by the FDA focuses on risks to consumers, not workers, although workers may be at greater risk due to their daily and prolonged use of cosmetic chemicals.
Attempts to regulate this industry are further complicated by the differing local, national and international definitions of the tasks barbers and cosmetologists perform. In the United States, licensing requirements vary from state to state. Many countries have no licensing requirements at all.
Major Processes and Hazards
Chemical hazards
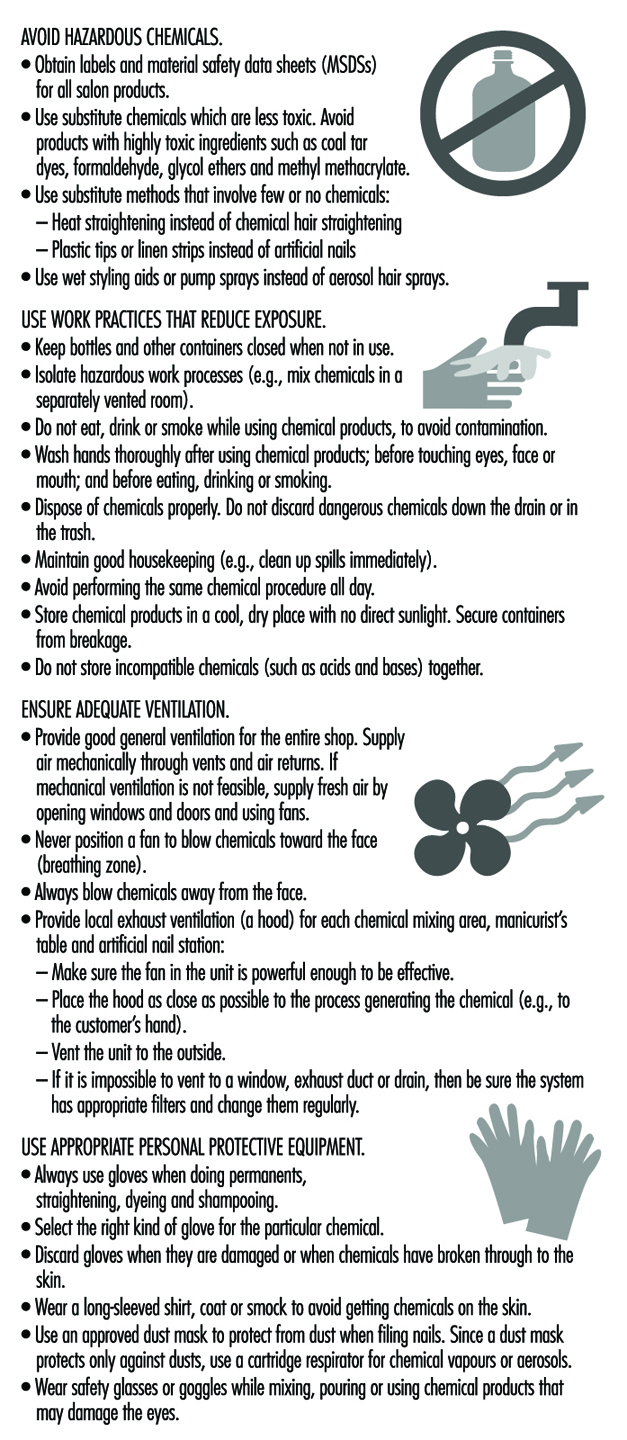
Barbers and cosmetologists are exposed to a wide variety of chemicals during the course of a working day. Technicians are at risk for absorbing chemicals through the skin or eyes, inhaling dangerous vapours or particulates and ingesting toxins that have contaminated food, drink or cigarettes. Some guidelines for reducing hazardous exposure are given in figure 1 .
Figure 1. Reducing exposure to chemical hazards.
Chemicals can affect the body in different ways depending on the concentration of the chemical in a product; how toxic the chemical is; the route by which it enters the body (inhalation, skin contact, ingestion); and the length of time of the exposure. Individual characteristics, such as general health status, pregnancy and smoking, can also affect a person’s risk.
There are thousands of different chemicals associated with cosmetology processes. In order to determine the specific chemicals contained in a product and their effects, it is important that technicians have access to, and understand, product labels and material safety data sheets (MSDSs).
Common chemical processes
Colouring hair. Hair colouring solutions are applied manually to the hair with an applicator bottle or brush. It also is becoming very common for clients to request an eyebrow or eyelash tints.
Chemicals used in hair colouring include synthetic organic colorants, complex metallic colorants and vegetable dyes. Synthetic hair colorants often include permanent oxidative dyes which use hydrogen peroxide to oxidize aromatic diamines. These chemicals are eye, nose and throat irritants. Synthetic organic hair dyes containing an amine group are also among the most frequent causes of allergic sensitization. Metallic dyes may include lead-containing compounds.
Coal tar-based hair dyes may contain mutagens. Hair dyes which have been found to be mutagenic in in vitro testing pose uncertain human health risks. However, the production of non-mutagenic hair dyes appears to be possible and should be encouraged. For example, henna, a vegetable dye, is one of the oldest hair dyes and is not known to be either a mutagen or a carcinogen.
Bleaching hair. Bleaching solutions are applied manually with an applicator bottle or brush. These solutions may contain hydrogen peroxide, sodium peroxide, ammonium hydroxide, ammonium persulphate or potassium persulphate. These chemicals can cause skin, eye, nose, throat or lung irritation. Persulphate bleach powders have also been associated with asthma among cosmetologists (Blainey et al. 1986).
Permanent waving. Permanent waves usually involve several steps: washing the hair; rolling the hair in curlers; applying a thioglycolate or similar solution; and rinsing and neutralizing with an oxidizing agent. Water sprays may also be used.
Permanent-wave solutions may contain alcohol, bromates, sodium hydroxide, boric acid (perborate or borate), ammonium thioglycolate or glycerol monothioglycolate. Some of these chemicals may cause central nervous system effects (headache, dizziness, nausea, drowsiness); eye, nose and throat irritation; lung problems (breathing difficulty or coughing); skin irritation; burns; or allergic reactions (stuffy or runny nose, sneezing, asthma or allergic dermatitis).
Manicures, pedicures and artificial nails. Nail care involves soaking the cuticles in softening agents, using nail clippers, using emery boards or nail files to file the nails, using hand lotions and applying and removing polish. Artificial nails (acrylics, gels, fibreglass, porcelains and fabric wraps and tips) may be brushed onto the nail or attached to it with glue. They are allowed to harden and then filed to the desired shape.
The many chemicals found in nail products include acetone, ethyl methacrylate and other acrylates, methyl ethyl ketone, ethyl acetate, lanolin and dimethyl-p-toluidine. These can cause skin, eye, nose, throat and lung irritation, as well as central nervous system effects. Some nail products also contain formaldehyde, associated with allergies as well as cancer with long term use. Some products contain glycol ethers, xylene and toluene, all linked to reproductive problems in laboratory animals.
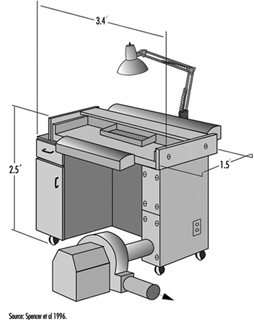
The use of methyl methacrylate (MMA) in artificial nail products was banned in the United States in 1974. Despite the ban, this chemical continues to be used. A 1982 study found that methyl methacrylate was present in 8 of 29 artificial nail products, and a 1986 study found measurable levels of MMA in the air of some nail salons. This chemical, if in contact with the skin, can cause tingling, numbness and whitening of the fingers. It also causes skin allergy in many people. An allergy to MMA can result in cross-sensitivity to other more commonly used methacrylates. In some products MMA has been replaced by other acrylates that may also be sensitizers. Figure 2 shows a downdraft table designed to minimize a manicurist’s exposure to the chemicals.
Figure 2. A modified commercial downdraft manicure table for application of artificial fingernails.
Washing and styling hair. Hair washing involves shampooing and rinsing with water. During this service, conditioners and other hair treatment products may also be applied. Hair drying is done in many ways: drying manually with towels, using a hand-held dryer or having the client sit under a fixed dryer. Styling generally involves the use of gels, creams or aerosol sprays. Washing the hair is often the first step for other services such as setting the hair, hair colouring and permanent waving. In large salons, one person may be assigned the job of washing clients’ hair, and do nothing other than that.
Shampoos and conditioners may contain alcohol, petroleum distillates and formaldehyde. All have been linked to dermatitis and allergies, including asthma. Long-term use of formaldehyde has also been linked to cancer.
Aerosol hair sprays may contain polyvinylpyrrolidone, which has been associated with lung and other respiratory diseases, including thesaurosis. They also contain a variety of solvents.
Straightening hair. Hair-straightening or hair-relaxing solutions are applied to the hair with a brush; then the hair is stretched to relax the natural curl. Hair straightener may contain sodium hydroxide, hydrogen peroxide, bromates, ammonium, thioglycolate and glycerol monothioglycolate. These chemicals may cause eye, nose and throat irritation, central nervous system effects and dermatitis.
Other chemical processes. A variety of cosmetics, including face creams and powders, mascara, eye liners, lipsticks and other products, may also be applied by cosmetologists. These can contain a wide variety of solvents, dyes, pigments, preservatives, oils, waxes and other chemicals that can cause skin allergies and/or irritation.
Cosmetologists may also remove body hair. Hair removal treatments can involve the application of hot wax and use of chemical depilatory products. These products often contain alkaline ingredients that can cause dermatitis.
Ergonomic hazards
Barbers and cosmetologists are at risk for musculoskeletal disorders due to the physical demands of their work and to poorly designed equipment, tools and work spaces. Such disorders can include:
- Wrist and hand problems, such as tendinitis and carpal tunnel syndrome. Risk factors include bending and twisting of the wrist while cutting and styling hair, holding hair dryers and using a round brush or curling iron. These disorders are also linked to forceful gripping or pinching caused by cutting with dull and/or poorly fitting shears.
- Shoulder problems, including tendinitis and bursitis. These are associated with constant reaching for supplies, or holding arms above shoulder height while cutting or styling hair. See figure 3.
- Neck and back problems, ranging from common aches and pains to serious conditions such as pinched nerves and ruptured discs. These are associated with frequent bending or twisting during activities such as shampooing, cutting hair below ear level, and performing manicures and pedicures.
- Foot and leg problems, including swelling, calluses and varicose veins. These may occur as a result of long periods of standing on hard floors in shoes with poor arch support.
Figure 3. Working with arms above shoulder level in a hairdressing salon in Zimbabwe.

Preventing musculoskeletal disorders
To prevent musculoskeletal disorders, it is important to apply ergonomic principles to the design of tasks, tools and workstations. Ergonomics is the science of adapting the workplace to the needs of the human body. It suggests ways to minimize awkward postures and repetitive motions, as well as the use of excessive force. It maximizes safety, health and comfort.
Ergonomic solutions may include:
- Adjustable furniture. For example, client chairs are available that can be raised, lowered and swiveled. Manicurist chairs are available with back support, armrests and seat pans that can be tilted to accommodate forward bending.
- Shears that are sharp, well-lubricated and designed to fit the individual’s hand.
- Curling irons and hair dryers with flexible handles. These can be used without excessive bending or twisting of the wrist.
- Free-standing sinks that allow technicians to wash hair without twisting and bending their backs.
- Rolling seats or stools that allow technicians to perform many procedures while seated, or to alternate between sitting and standing.
- Proper workstation designs such as storing commonly used supplies within easy reach; providing cushioned floor mats; and ensuring that cabinets are at the correct height to minimize reaching or bending.
- Client scheduling that varies the tasks and processes that a technician performs throughout the day.
- Training for technicians in good body mechanics and work practices such as proper lifting methods; bending at the hips instead of the waist; and using hair-cutting techniques that minimize reaching and bending of the wrist.
Infectious diseases
Work performed by barbers and cosmetologists involves close contact with clients. Understanding how infectious diseases are transmitted will help technicians prevent infection. Infectious diseases may be spread in the salon in the following ways:
- Through the air (e.g., upper respiratory illnesses such as colds and flu)
- Through contaminated water or food (e.g., hepatitis A, salmonella and giardia)
- Through insect or animal bites (e.g., lice)
- Through direct skin contact with infected persons (e.g., scabies, lice, ringworm, impetigo, herpes simplex, colds and chickenpox)
- Rarely, through exposure to the blood of an infected person (e.g., hepatitis B and HIV/AIDS)
While there is no recorded case of a barber or cosmetologist becoming infected with HIV/AIDS on the job, and work-related hepatitis B infection is extremely rare in these occupations, exposure to these bloodborne pathogens could possibly occur in rare instances of blood contact. Possible sources of exposure could include puncturing the skin with tools that carry infected blood (razors, tweezers, tattoo needles or clippers), or infected blood entering the body through an open wound, sore or skin rash.
This is one reason that shaving clients with razors has become uncommon in many countries. In addition to the risk to technicians, there is the possibility of skin and other infections being transferred from one client to another through unsterilized equipment.
Exposure to harmful organisms can be prevented by taking simple precautions:
- Hands should be washed frequently with soap and water.
- Latex gloves should be worn to protect technician and client if either has sores, lesions or skin rashes.
- Sharp instruments should be handled carefully and disposed of in approved puncture-proof containers.
- All tools, equipment and surfaces should be disinfected properly.
- Towels should be sanitized.
- Workers should be vaccinated against hepatitis B.
Other hazards
Fire hazards
Some products used in the salon may contain flammable or combustible chemicals. Sources of ignition can include flame from a cigarette, match or burner; a spark from a light switch, electric plug or frayed cord; or a hot object such as a curling iron, stove, light bulb or hotplate. To prevent accidents, it should be made sure that chemicals are used and stored properly. Flammables and combustibles should be kept away from flames, sparks or hot objects, and electrical equipment should be checked for broken or frayed cords that might spark or get hot. Each shop should also have a fire-prevention and evacuation plan, and appropriate and functioning fire extinguishers.
General housekeeping
Salons are often cramped and crowded work environments. Overstocked shelves may be unstable. Technicians may be at risk for slips and falls as a result of spilled liquids, poorly stored equipment or poorly positioned cords or wires. Narrow, crowded aisles limit workers’ ability to move freely without obstruction. All shops should practice good housekeeping, including: keeping aisles clear, cleaning up spills immediately, storing heavy objects on low shelves and making sure people can move freely through their workspace.
Electrical hazards
Electrical devices in the salon can include hair clippers, hair dryers, facial machines and electrolysis equipment and they should be checked for frayed wires and proper grounding. Since electrical equipment and outlets are often within splash range of water, red ground fault circuit interrupters to prevent shock should be used.
Health Problems and Disease Patterns
Skin diseases
Irritant and allergic dermatitis of the hands alone, or of hands and face together, is a common problem, experienced by 10 to 20% of cosmetologists (van der Walle and Brunsveld 1994). It often produces a characteristic rash in the spaces between the fingers. Signs of dermatitis generally include redness, drying and cracking on the skin of the hands. Eczema of the tips of the fingers may also occur, with ridging of the nail folds. Younger workers appear to be at highest risk, possibly because those with lower seniority tend to be assigned most often to shampooing and permanent-waving jobs. Most frequent causes of allergic skin rash in cosmetologists include glycerol thioglycolate, ammonium thioglycolate, nickel sulphate, ammonium persulphate preservatives and hair dyes (p-phenylenediamine or resorcinol) (Villaplana, Romaguera and Grimalt 1991).
In most cases, once an allergic dermatitis develops it does not improve, even with the wearing of gloves. Rubber latex glove use may itself be a significant risk factor for allergic responses, and vinyl gloves may need to be substituted if latex allergy develops. If one worker in a salon develops latex allergy, the entire salon may need to become latex-free to protect that worker from repeated allergic responses.
Other skin diseases of hairdressers include granuloma from hair implantation, and hot water burns. Also, varicose veins may result from the prolonged standing common to this occupation. Sharp tools such as scissors, shaving equipment and electric hair-cutting tools can cause skin lacerations. Such cuts may predispose the cosmetologist to dermatitis due to chemical exposures.
Lung problems
Allergic rhinitis (“hay fever”) and asthma have been associated with exposure to permanent-wave solution (Schwartz, Arnold and Strohl 1990), and in particular to ammonium persulphate (Gamboa et al. 1989). Hair bleach as well as henna (Starr, Yunginger and Brahser 1982) have been associated with occupational asthma in cosmetologists.
Reproductive health
A recent study found a moderately increased risk of spontaneous abortion among cosmetologists who worked full time and performed a large number of chemical services. The use of formaldehyde and exposure to manicuring and nail-sculpting chemicals were specifically associated with an increased risk of spontaneous abortion (John, Savitz and Shy 1994).
Cancer
Cosmetologists have been found to have a possible increased risk of developing certain types of cancer, including non-Hodgkin’s lymphoma (Zahm et al. 1992; Pearce 1992), bladder/urothelial cancer (Steineck et al. 1990) and breast cancer (Koenig 1994).