- You are here:
-
Home

- k2 Feed
Diseases Associated with Hunting and Trapping
Hazards
The hazards associated with hunting and trapping are numerous—falls, drownings, frostbite, animal trap injuries, animal bites, reactions to insect bites and stings, wood-cutting wounds, sun glare and many others. However, it is usually the less experienced who suffer such mishaps. The most important factors contributing to the severity of these occupational hazards are isolation and distance. Hunters and trappers frequently work alone in rugged areas remote from any medical treatment centre, and their exact locations may often be unknown to anyone for weeks at a time. A wound, animal bite or other accident that would otherwise be a minor matter can have serious consequences under such circumstances.
Accidents
Since professional trappers work mainly in the winter season in northern climates, sun glare from snow can produce eye injuries, and cold temperatures can produce frostbite and a dangerous lowering of body temperature, known as hypothermia; symptoms of hypothermia include euphoria and lethargy, with fatal consequences if not recognized in time. Crossing frozen lakes and rivers requires extreme caution because breaking through a thin layer of ice can result in drowning or hypothermia in a matter of minutes. Prolonged exposure to even moderately cold weather without adequate clothing can lead to hypothermia. Other accidents include gunshot wounds, snowmobile mishaps, wounds from skinning and wood-chopping, the accidental tripping of traps, and bites or injuries from trapped animals, snakes or other animal encounters. In addition to risk of wounds becoming infected, there is also the possibility of contracting certain diseases from animals.
Diseases
Hunters and trappers are potentially exposed to a great variety of infectious agents that can cause illnesses. Among them are zoonotic diseases, transmitted from animals to people. Zoonotic diseases are caused by numerous types of bacteria, viruses, parasites and fungi. The risk of acquiring any zoonotic disease varies with location, season and living conditions. A person can become infected directly (e.g., from an animal bite or from contact with blood while skinning an animal) or indirectly (e.g., from an insect bite that transmits the disease from another animal to a human).
Rabies is one of the most serious diseases that can be contracted from wild animals, usually from a bite wound, because it is essentially 100% fatal without medical treatment. Rabies is endemic in many areas and can infect most warm-blooded animals, including foxes, dogs, cats, bats, raccoons, skunks, wolves, bears and beaver as well as larger animals such as caribou, moose, cattle and horses. The rabies virus affects the brain; therefore, any wild animal which appears to lose its fear of man or to show any other unusual behaviour should be considered hazardous. Because the rabies virus, as well as a number of other viruses and bacteria, is transmitted in saliva, all animal bites should be washed thoroughly with soap and water. Any hunter or trapper who is bitten by an animal suspected to be rabid should seek medical assistance immediately and should try to obtain the head of the animal for testing.
Tularaemia, also known as deer fly fever and rabbit fever, is a bacterial disease that can be transmitted indirectly (by ticks, deer flies and other biting flies) or directly (by bites of infected animals or by handling carcasses, furs and hides of infected animals). It can also infect water supplies and contaminate meat. Its symptoms, similar to those of undulant fever and plague, include fever, chills, fatigue and swollen lymph nodes. In areas in which the disease is suspected, water supplies should be disinfected. Wild game should be thoroughly cooked before eating. Arms and hands should be kept clean and disinfected. Rubber gloves should be worn if there are any cuts or abrasions. The area in which carcasses, hides and pelts are handled should be kept clean and disinfected.
Anthrax is another bacterial disease that may infect trappers and hunters, since it is endemic in both wild and domesticated animals in most parts of the world. A skin infection from contact with contaminated skins and hides is the most frequent form of anthrax; however, people are also infected by eating contaminated meat. Disease caused by inhalation is less common. Treatment should be sought at once.
Tuberculosis is an increasingly significant problem in many areas. Many species of animals can be a source of tuberculosis infection for hunters. Although most cases of human tuberculosis are due to exposure to coughs and sneezes from infected humans, many species of animals, including birds and cold-blooded animals, can be infected with the bacillum. Tuberculosis is also transmitted by consuming unpasteurized dairy products. It is also possible to become infected by inhaling airborne respiratory droplets or by eating the meat of infected animals. People who are immune suppressed (e.g., due to medication or human immunodeficiency virus infection) are at particular risk for the more common agents of tuberculosis, as well as those found in soil and water.
Hunters and trappers may also suffer from several fungal diseases carried by animals as well as soil fungi. Trichophyton verrucosum and T. mentagrophytes are the main ringworm agents affecting man. Also, dogs serve as a reservoir for Microsporum canis, the principal cause of animal ringworm in man. Hunters and trappers may be exposed to fungi that reside in soil and decaying vegetation, especially soils contaminated with bird or bat droppings; these fungi, which are not zoonotic diseases, inhabit specific habitats. Coccidioides immitis is common only in arid and semi-arid areas, whereas Blastomyces dermatitidis prefers moist soils along waterways and undisturbed areas. Cryptococcus neoformans and Histoplasma capsulatum are more common and live in soils enriched with bird and bat droppings. When inhaled, these fungi can cause pneumonia-like symptoms as well as serious systemic diseases in both people and animals.
Tetanus is another serious disease that infects both humans and animals. The tetanus bacteria are also very common in soils and other parts of the environment, and are normal inhabitants of many animals’ digestive tracts. Wounds, particularly deep puncture wounds, that are contaminated with dirt are the most likely to become infected. Prevention includes proper wound care and routine vaccination.
Wood ticks, mosquitoes, fleas and other biting insects often transmit infections from animals to man. Bubonic plague is an example of a bacterial disease transmitted by flea bites. A flea becomes infected when it takes a blood meal from an infected animal—usually a rodent, rabbit or hare, but also various carnivores. The flea then transmits the infection to the next animal it feeds on, including man. People can also become infected by handling tissues of infected animals, or by inhaling airborne droplets from humans or animals, usually cats, with pneumonic form of plague. The initial symptoms of bubonic plague are non-specific and include fever, chills, nausea and prostration. Later, the lymph nodes may become swollen and inflamed (the buboes for which the disease is named).
A more common disease transmitted by the bite of an insect is Lyme disease. Lyme disease is one of many transmitted by ticks. The first symptom is often a bull’s-eye rash, a red circle with a pale centre at the site of the bite. The rash disappears; however, without treatment, the disease can progress to arthritis and more serious complications.
Hantaviruses infect rodents worldwide, and human infections have been described for decades, most typically affecting the kidneys. In 1993, hantavirus pulmonary syndrome was newly recognized in the United States. This virus caused a rapidly fatal respiratory failure. Transmission of these viruses is likely to be via aerosolized rodent urine and faeces. It is thought that infected people were exposed to mice that contaminated cabins and houses.
In addition, hunters and trappers may be exposed to a wide variety of other viral, bacterial, fungal and parasitic infections that are at times found in wild animals (table 1). Standard reference works may be consulted for details.
Table 1. Examples of diseases potentially significant to hunters and trappers
|
Agent |
Disease |
Reservoir |
Mode of transmission |
Occurrence |
|
Bacterial diseases |
||||
|
Bacillus anthracis |
Anthrax |
Animals, hides, hair, bone, soil |
Direct and indirect contact, |
Americas, Europe, Asia, Africa |
|
Borellia spp. |
Lyme disease, relapsing fever |
Rodents, small mammals, deer, ticks |
Tick and louse bites |
Worldwide except Australia |
|
Brucella spp. |
Brucellosis, undulant fever |
Animals |
Contact, ingestion, inhalation |
Worldwide |
|
Campylobacter spp. |
Enteritis |
Animals |
Ingestion |
Worldwide |
|
Coxiella burnetii |
Q fever |
Animals |
Inhalation, contact |
Worldwide |
|
Clostridium tetani |
Tetanus |
Soil |
Contact |
Worldwide |
|
Ehrlichia spp. |
Ehrlichiosis |
Unknown |
Tick bite |
North America, Africa, Asia |
|
Francisella tularensis |
Tularemia |
Animals |
Insect bites, contact, ingestion, |
Worldwide except Australia |
|
Leptospira spp. |
Leptospirosis |
Animals |
Contact, ingestion, inhalation |
Worldwide |
|
Listeria monocytogenes |
Listeriosis |
Soil, animals, humans |
Ingestion |
USA |
|
Mycobacterium spp. |
Tuberculosis |
Humans, mammals, birds, |
Inhalation, ingestion, wound |
Worldwide |
|
Rickettsia spp. |
Tick-borne rickettsioses |
Ticks, rodents |
Tick and mite bites |
Worldwide |
|
Salmonella spp. |
Salmonellosis |
Mammals, birds, cold-blooded |
Ingestion |
Worldwide |
|
Vibrio cholera |
Cholera |
Humans |
Ingestion |
Worldwide |
|
Yersinia pestis |
Plague, bubonic plague |
Rodents, hares, rabbits, humans, |
Flea bites, inhalation, contact |
Worldwide |
|
Viral diseases |
||||
|
Arboviruses |
Fevers, rash, haemorrhagic fevers, |
Humans, animals, insects |
Insect bites: mosquitoes, ticks, midges, sandflies, others |
Worldwide |
|
Ebola/Marburg viruses |
Haemorrhagic fevers |
Unknown, monkeys |
Unknown, body-fluid contact |
Africa, exposure to monkeys |
|
Hantaviruses |
Haemorrhagic fever, renal and pulmonary syndromes |
Rodents |
Inhalation |
Asia, former Soviet Union, |
|
Lassa virus |
Lassa fever |
Rodents |
Inhalation, body-fluid contact |
West Africa |
|
Rabies virus |
Rabies |
Mammals |
Virus in saliva, usually a bite |
Worldwide except some island |
|
Fungal diseases |
||||
|
Blastomyces dermatitidis |
Blastomycosis |
Soil |
Inhalation |
Africa, India, Israel, North |
|
Coccidioides immitis |
Coccidioidomycosis, valley fever, desert fever |
Soil |
Inhalation |
Argentina, Paraguay, Colombia, |
|
Cryptococcus neoformans |
Cryptococcosis |
Soil, bird and bat droppings |
Inhalation |
Worldwide |
|
Histoplasma capsulatum |
Histoplasmosis |
Soil, bird and bat droppings |
Inhalation |
Americas, Africa, eastern Asia, |
|
Microsporum spp., |
Ringworm |
Humans, animals, soil |
Direct or indirect contact |
Worldwide |
|
Parasitic diseases |
||||
|
Babesia spp. |
Babesiosis |
Rodents, cattle |
Tick bites |
Europe, Mexico, Russia, |
|
Baylisascaris spp. |
Baylisascaris larva migrans |
Racoons, badgers, skunks, |
Ingestion |
North America |
|
Cryptosporidium parvum |
Cryptosporidiosis |
Humans, cattle, domestic animals |
Ingestion |
Worldwide |
|
Diphyllobothrium latum |
Tapeworm infection |
Humans, dogs, bears, fish-eating |
Ingestion |
Lake regions |
|
Echinococcus spp. |
Echinococcosis |
Animals |
Ingestion |
Worldwide |
|
Giardia spp. |
Giardiasis |
Humans, animals |
Ingestion |
Worldwide |
|
Leishmania spp. |
Leishmaniasis |
Humans, animals |
Sandfly bite |
Tropical and sub-tropical areas |
|
Trichinella spiralis |
Trichinellosis |
Animals |
Ingestion |
Worldwide |
|
Trypanosoma spp. |
Trypanosomiasis |
Humans, animals |
Insect bites |
Africa, Americas |
Most zoonotic diseases and other infectious agents can be avoided by using common sense and some general precautions. Water should be boiled or chemically treated. All foods should be adequately cooked, especially those of animal origin. Meats from all wild animals should be cooked to 71°C (160°F). Foods eaten raw should be thoroughly washed. Insect bites and stings should be avoided by tucking trousers into boots; wearing long-sleeved shirts; using repellants and mosquito netting as necessary. Ticks should be removed as soon as possible. Direct contact with animal tissues and bodily fluids should be avoided. Wearing gloves is recommended, particularly if one’s hands are cracked or abraded. Hands should be washed with soap and water after animal handling and always prior to eating. Bites and wounds should be washed with soap and water as soon as possible, with follow-up medical treatment especially if exposure to a rabies-infected animal is suspected. Hunters and trappers should be vaccinated against diseases common to their location. Having emergency first aid supplies on hand and a basic knowledge of first aid procedures may make the difference between a major and a minor incident.
A Profile of Hunting and Trapping in the 1990s
Overview of the Sector
Hunting and trapping of wild animals are two very old human endavours that persist in a variety of forms throughout the world today. Both involve the capture and death of target species living in wild or relatively undeveloped habitats. A wide variety of species is hunted. Small game mammals like hares, rabbits and squirrels are hunted throughout the world. Examples of big game commonly pursued by hunters are deer, antelope, bears and the large cats. Waterfowl and pheasants are among the commonly hunted game birds. Trapping is limited to animals having fur with either commercial or some practical value for use by the trapper. In the north temperate zones, beaver, muskrat, mink, wolf, bobcat, and raccoons are often trapped.
Hunting is the stalking and killing of individual wild animals, usually for food, clothing or recreational reasons. Recently, hunting in some situations has been viewed as a way of maintaining the cultural continuity of an indigenous culture. Subsistence bowhead whaling in northern Alaska is an example. Hunters usually employ projectile weapons like shotguns, rifles or bow and arrow. Trappers are more specialized and have to obtain numbers of fur-bearing mammals without damaging the pelts. Snares and deadfalls have been used for millennia. Leghold traps (both padded and unpadded) are still commonly used for some species; killing traps like the Conibear are more widely used for other species.
Evolution and Structure of the Industry
In a few traditional societies throughout the world today, hunting continues as an individual survival activity, essentially unchanged since before the evolution of either animal husbandry or agriculture. However, most people hunt today as some form of leisure time activity; some earn partial incomes as professional hunters or trappers; and relatively few are employed in these occupations on a full-time basis. Commerce in hunting and trapping probably began with the trade of surplus animal food and skins. Trade has gradually evolved into specialized but related occupations. Examples include tanning; hide and fur preparation; clothing manufacture; production of hunting, trapping and outdoor equipment; professional guiding; and regulation of wildlife populations.
Economic Importance
In recent centuries the commercial search for furs influenced the course of history. Wildlife populations, the fate of indigenous people and the character of many nations have been shaped by the quest for wild furs. (For example, see Hinnis 1973.) An important continuing characteristic of the fur trade is that demand for fur, and resulting prices, can fluctuate widely over time. The change in European fashion from beaver felt to silk hats in the early decades of the 19th century brought an end to the era of the mountain men in the Rocky Mountains of North America. The impact on people dependent on fur harvest can be sudden and severe. Organized public protest against the clubbing of harp seal pups in the western North Atlantic in the 1970s wreaked severe economic and social impact on small communities along the Newfoundland coast of Canada.
Trapping and hunting continue to be important in many rural economies. The cumulative expenditures for these activities can be substantial. In 1991 an estimated 10.7 million big game hunters in the United States spent US$5.1 billion on trip and equipment expenditures (US Department of the Interior, Fish and Wildlife Service and US Department of Commerce, Bureau of the Census 1993).
Characteristics of the Workforce
Professional hunting is now rare (except for guiding activities) in developed nations, and confined generally to culling operations (e.g., for predators or overcapacity hooved animals) and nuisance population control (e.g., alligators). Thus, hunting is now largely for subsistence and/or recreation, while trapping remains an income-producing occupation for some rural residents. Most hunters and trappers are men. In 1991, 92% of the 14.1 million people (age 16 or older) hunting in the United States were male. Hunting and trapping attracts independent and vigorous people who enjoy working and living on the land. Both are traditional activities for many rural families, where young people are instructed by their parents or elders in hunting as they are for preparation of food, skins and clothing. It is a seasonal activity used to supplement food supplies and, in the case of trapping, to obtain cash. Consistent success depends upon in-depth knowledge about wildlife habits and competence with a range of outdoor skills. Efficient transportation to good hunting and trapping areas is also an important requirement.
Major Sectors and Processes
Hunting requires locating and closely approaching a wild animal, and then dispatching it, under a combination of formal and informal rules (Ortega y Gasset 1985). Transportation to the hunting area is often a major expense, particularly for recreational hunters who may live in urban centres. Transportation is also a primary source of occupational risk. Automobile, light aircraft and boat accidents as well as mishaps with horses, all-terrain and snow-travel vehicles are all sources of risk. Other sources are weather, exposure and terrain difficulties. Becoming lost in rough country is always a hazard. Injury from wounded dangerous game like bears, elephants and cape buffalo is always possible for hunters seeking those species. In small cabins or tents, fire, carbon monoxide and propane gas all present potential hazards. Both hunters and trappers must contend with self-inflicted injury from knives and, in the case of bowhunters, broad-head arrow points. Firearms accidents are also a well known source of injury and mortality to hunters despite continuing efforts to address the problem.
Trappers are generally exposed to the same hazards as hunters. Trappers in circumpolar areas have more opportunity for frostbite and hypothermia difficulties. The potential for breaking through ice-covered lakes and rivers during the winter months is a serious problem. Some trappers travel long distances alone and must safely operate their traps, often under difficult conditions. Mishandling results in bruised or broken fingers, perhaps a broken arm. Bites from live-trapped animals are always a potential problem. Attacks by rabid foxes or problems with large animals such as bears or moose during the breeding season are unusual but not unknown. Skinning and fur handling expose trappers to knife injuries and, sometimes, wildlife diseases.
Hunting Techniques
Firearms
Firearms are basic equipment for most hunters. Modern rifles and shotguns are the most popular, but hunting with handguns and more primitive muzzle-loading firearms has also increased in some developed countries since the 1970s. All are essentially launching and aiming platforms for a single projectile (a bullet) or, in the case of shotguns, a cloud of small, short-range projectiles (called shot). Effective range depends on the type of firearm used and the skill of the hunter. It can vary from a few to several hundred metres under most hunting conditions. Rifle bullets can travel thousands of metres and still cause damage or injury.
Most hunting accidents involving firearms are either accidental discharges or vision-related accidents, where the victim is not identified by the shooter. Modern manufacturers of firearms used for hunting and trapping have, with few exceptions, succeeded in producing mechanically safe and reliable equipment at competitive prices. Much effort has been expended at refining mechanical safeties to prevent accidental discharges, but safe operation by the firearm user is still essential. Manufacturers, governments and private groups such as hunting clubs have all worked to promote firearms and hunter safety. Their emphasis has been on safe storage, use and handling of firearms.
The International Hunter Education Association (IHEA) defines a hunting accident as “any event which is attributed directly or indirectly to a firearm or bow, and causes injury or death to any person or persons as a result of a person’s actions while hunting” (IHEA 1995). In 1995, 17 million people purchased hunting licenses in the United States (excluding Alaska). For 1995, the IHEA received reports of 107 deaths and 1,094 injuries from hunting accidents in the United States. The most common type of accident occurred when the victim was not identified by the shooter. The use of blaze- or hunter-orange clothing has been shown to reduce visibility-related accidents in states requiring its use. More extensive use of blaze-orange clothing is recommended by the IHEA. Forty states now require use of blaze orange, but in some of them, it is limited to use on public lands or only for big-game hunting. The IHEA reports that self-inflicted injuries are the second most common cause of hunting firearms accidents, accounting for 31% of the total number in 1995.
Governments encourage hunting and firearms safety in various ways. In some European countries, hunters must pass a written examination or demonstrate proficiency in hunting a particular species. The United States emphasizes hunter education, which is administered by each state. All states except Alaska require some form of mandatory hunter education card before allowing hunting in that state. A minimum of 10 hours of instruction is required. Course subjects include hunter responsibility, wildlife conservation, firearms, hunting ethics, specialty hunting, survival skills and first aid.
Other hunting techniques
In recent decades, refinement of the compound bow has made archery hunting available to millions of recreational hunters. Compound bows use a system of pulleys and cables to minimize the strength and training once needed to hunt with traditional bows. Bow hunters use razor-sharp broad-head arrows; cuts from broad heads and falling on unprotected arrowheads are two types of accident common to this hunting specialty. Effective bow hunting requires extensive wildlife knowledge and stalking skills. Bow hunters normally have to be within 30 metres of their prey in order to be able to shoot effectively.
Trapping Techniques
Most of the wild fur production in the world comes from two areas: North America and the former Soviet Union. Trappers normally operate a line or series of sets, each with one or more devices intended to restrain or kill the target species without damaging the pelt. Snares and traps (including box, leghold and body-gripping humane traps) are most commonly used. Traplines can vary from a few sets in a creekbed behind a residence to hundreds set out along several hundred miles of trail. The Alaska Trappers Manual (ATA 1991) is a recent description of trapping techniques currently in use in that region.
Pelt treatment techniques
Trappers normally skin their catches and sell the dried pelts to a fur buyer or directly to an auction house. The pelts will eventually be sold to a manufacturer who dresses or tans the skins. Afterwards they are prepared into garments. Fur prices vary considerably. The price paid for a pelt depends on size, desired colour, fur condition, the absence of defects and market conditions. Experienced trappers have to catch furbearers and prepare the pelts for sale in a manner that makes the entire process profitable enough to continue operating. For a thorough discussion of the wild fur industry see Novak et al. (1987).
Environmental and Public Health Issues
Technological advances since the Second World War have improved the lot of hunters and trappers in many ways. These improvements have alleviated, at least in the developed countries, the isolation, gruelling physical labour and occasional malnutrition that once had to be endured. Improved navigation and search and rescue methods have improved the safety levels of these occupations generally. Alaska Native walrus and whale hunters, for example, now almost always return home safely from the hunt.
In the 20th century, two major issues have seriously challenged these occupations. They are the continuing need to maintain healthy wildlife ecosystems and the ethical questions resulting from the way hunters and trappers interact with wild animals. Government-sponsored research and regulations are usually the front-line approach to addressing the very old problem of human exploitation of wildlife. The scientific discipline of wildlife management emerged in mid-century and has continued to evolve into the broader concept of conservation biology. The latter seeks to maintain ecosystem health and genetic diversity.
Early in the 20th century, habitat destruction and commercial exploitation in the United States had contributed to depletion of fish and game resources. Hunters, trappers and other outdoor advocates secured passage of legislation that created the US Federal Aid in Wildlife Restoration Act of 1937. This act imposes a 10 to 11% excise tax on the sale of rifles, pistols, shotguns, ammunition and archery equipment. The money is then used to augment revenue obtained from the sale of state hunting/trapping licenses, tags and stamps.
Since the late 1930s, US federal aid has directed millions of dollars into wildlife research, conservation, management and hunter education. One result of these efforts is that North American wildlife populations actively used by hunters and trappers now are generally healthy and capable of sustaining consumptive uses. The federal aid experience suggests that when wildlife has a constituency willing to pay research and management costs, the future for those species is relatively bright. Unfortunately there are many ecosystems and wildlife species throughout the world where this is not the case. As we are about to enter a new century, habitat alteration and species extinction are very real conservation issues.
The other continuing challenge is controversy about animal rights. Is hunting and trapping, especially for recreation or non-subsistence purposes, a socially acceptable activity in a 21st century world of growing human population and shrinking resources? This social debate has intensified in recent decades. One positive side of the dialogue is that those who participate in these activities have had to do a better job of articulating their positions and of maintaining high standards of hunting and trapping performance. Activities offending the sensibilities of the general public, such as the clubbing of baby harp seals off the coast of Newfoundland, have sometimes been eliminated—in this case at enormous social and economic cost to the Newfoundlanders who had for many generations participated in those activities. A recent ban threatened by European communities on importation of fur taken by steel leg-hold traps has intensified the search for practical and more humane methods of killing certain furbearers. This same proposed ban threatens a rural North American subsistence lifestyle that has existed for a long time. (For more details see Herscovici 1985.)
Health Effects and Disease Patterns
Hotels and restaurants constitute a large, diversified, labour-intensive service industry made up predominantly of small enterprises. While there are a number of giant corporations, some of which attempt to standardize procedures and working rules, their hotels and restaurants are usually operated individually, often on a franchise rather than a directly owned basis. Frequently, the eating and drinking establishments in hotels are leased to franchise operators.
There is a high degree of failure among the enterprises in this industry, with many being very close to the edge of financial insolvency for some time before closing their doors. This often dictates economies in staffing, in the purchase and maintenance of equipment and in the provision of necessary supplies. It also often forces neglect of employee training programmes and a reluctance to spend scarce resources on measures to promote and protect employee safety and health.
The majority of the jobs are unskilled and provide low or minimal wages (in some of the jobs, these may be supplemented by gratuities that depend on the largesse of the patrons). Consequently, they attract only workers with minimal education and experience, and because minimal language and literacy skills are required, many of the jobs are filled by immigrants and ethnic minorities. Many are entry-level positions with little or no opportunities for advancement. Shift work is required in hotels because they operate around the clock; in restaurants, the flurries of activity at meal times are often covered by part-time workers. Because their patronage is seasonal, many establishments curtail their operations or shut down entirely during the off-season, and, as a result, there may be little or no job security. The end result of all of this is a high rate of turnover in the workforce.
Job Stress
Because of the periods of intense activity and the necessity of pleasing the patrons on whose gratuities their livelihoods often depend, many of the workers in this industry are subject to high levels of job stress. They must often comply with seemingly unreasonable or even impossible requests and may be subjected to abusive behaviour on the part of supervisors as well as customers. Many of the jobs, particularly those in kitchens and laundries, must be carried out in stressful environments featuring high heat and humidity, poor ventilation, poor lighting and noise (Ulfvarson, Janbell and Rosen 1976).
Violence
Hotels and restaurants rank high on the lists of workplaces with the greatest incidence of occupational violent crime. According to one survey, over 50% of such incidents involving hotel and restaurant workers resulted in death (Hales et al. 1988). These workers are exposed to many of the risk factors for workplace homicide: exchange of money with the public, working alone or in small numbers, working late night or early morning hours and guarding valuable property or possessions (Warshaw and Messite 1996).
Types of Injuries and Diseases
According to the US Bureau of Labor Statistics, food and beverage preparation and housekeeping departments accounted for 76% of all work injuries and accidents in hotels (US Bureau of Labor Statistics 1967), while a Danish survey found that these were predominantly skin and musculoskeletal problems (Direktoratet for Arbejdstilsynet 1993). Most of the skin problems may be traced to exposure to soap and hot water, to the chemicals in detergents and other cleaning/polishing materials and, in some instances, to pesticides. Except for the special problems noted below, the majority of musculoskeletal injuries result from slips and falls and from lifting and handling heavy and/or bulky objects.
Sprains, strains and repetitive motion injuries
Back injuries and other sprains and strains commonly occur among doormen, porters and bellmen lifting and carrying luggage (a particular problem when large tour groups arrive and depart); kitchen workers and others receiving and storing bulk supplies; and housekeeping workers lifting mattresses, making beds and handling bundles of laundry. A unique type of injury is carpal tunnel syndrome among food service workers who use scoops to prepare servings of hard ice cream and other frozen desserts.
Cuts and lacerations
Cuts and lacerations are common among restaurant workers and dishwashers who deal with broken glass and crockery, and who handle or clean sharp knives and slicing machines. They are also common among chambermaids who encounter broken glasses and discarded razor blades in cleaning out waste baskets; they may be protected by lining the baskets with plastic bags which can be removed en masse.
Burns and scalds
Burns and scalds are common among chefs, dishwashers and other kitchen workers and laundry workers. Grease burns occur from splatters during cooking or as food is dropped into deep-fat fryers, when hot grease is added, filtered or removed, and when grills and fryers are cleaned while hot. Many result when workers slip on wet or slippery floors and fall on or against hot grills and open flames. A unique type of burn occurs in restaurants where flaming desserts, entrees and drinks are served (Achauer, Bartlett and Allyn 1982).
Industrial chemicals
Hotel and restaurant establishments share with other small enterprises a propensity for improper storage, handling and disposal of industrial chemicals. All too frequently cleaning supplies, disinfectants, pesticides and other “household” poisons are stored in unlabelled containers, are placed above open food containers or food preparation areas or, when used in spray form, are excessively inhaled.
The fast food industry
The fast food industry, one of the most rapidly growing in the United States and becoming increasingly popular in other countries, is one of the largest employers of young people. Lacerations and burns are common hazards in these establishments. It has also been noted that the home delivery of pizzas and other prepared food is often extremely hazardous because of policies which encourage reckless driving on bicycles as well as in motor vehicles (Landrigan et al. 1992).
Preventive Measures
Standardized work processes, adequate training and proper supervision are key elements in the prevention of work-related injuries and illnesses among workers in the hotel and restaurant industry. It is essential that, because of their generally low educational levels and language difficulties, the educational materials and training exercises be readily understood (they may have to be conducted in several languages). Also, because of the high turnover, training must be repeated at frequent intervals. The training exercises should be supplemented by frequent inspections to assure that the basic principles of good housekeeping and elimination of accident hazards are observed.
Emergency drills
In addition to regular inspections to verify that firefighting equipment (e.g., smoke alarms, sprinkler systems, fire extinguishers and hoses and emergency lighting equipment) is in good working order and that emergency exits are clearly marked and not blocked, frequent drills are necessary to train the workers in how to prevent themselves and the patrons from being trapped and overcome in the event of a fire or an explosion. It is desirable to hold at least some of these drills in concert with the community fire, rescue and police organizations.
Conclusion
Apropriately designed and diligently practised preventive measures will do much to lower the frequency of occupational injuries and illnesses among hotel and restaurant workers. Language barriers and relatively low educational levels often represent formidable challenges to the effectiveness of training and indoctrination programmes, while the high rate of turnover dictates the frequent repetition of these programmes. It is important to remember that the health and safety of the workers in this industry is an essential element in the enjoyment and satisfaction of the patrons, upon whose good will the success - and even the survival - of the enterprise depends.
Hotels
Departmental operations within a hotel usually consist of: reception, which oversees reservations and guest reception services; housekeeping, which cleans and stocks guest rooms and public areas; maintenance, which does heavy cleaning, setup, painting, repair and remodelling; food and beverage; office and accounting; and other miscellaneous services such as health centres, beauty salons, barber shops and gift shops.
Hazards by Department
Reception
Reception includes the following job classifications: managers, desk clerks, telephone operators, bell and door staff, security personnel, concierges, drivers and parking attendants. Key job safety and health hazards include:
Visual display units (VDUs). Desk clerks, telephone operators and other front desk personnel often use computer terminals. It has been shown that computer use under some conditions can cause various repetitive strain injuries (RSIs), such as carpal tunnel syndrome (in the wrist) as well as shoulder, neck and back problems. Employees are at special risk if workstations are poorly adjusted and require awkward body postures, or if VDU work is continuous without adequate breaks. VDU work can also produce eyestrain and other visual problems. Preventive measures include providing adjustable computer workstations, training staff on how to adjust their equipment properly and maintain correct postures, and ensuring that employees take rest and stretch breaks.
Shift work. Many guest service employees work shifts that can vary according to the level of daily hotel occupancy. Staff members may be required to work both day and evening shifts, or split shifts with random days off. Physiological and psychological health effects of shift work can include disturbed sleep patterns, stomach trouble and stress. Staff may also use drugs or medicines as sleeping aids to adjust to unusual work hours. Workers should receive training on health hazards related to shift work. Whenever possible workers should have adequate time off between rotating shifts to allow for sleep adjustments.
Special consideration should also be paid to other issues associated with swing and graveyard shifts, such as safety concerns, access to healthy meals while on duty and proper ventilation (as air conditioning is often turned off in the evening).
Poor indoor-air quality. Employees can be exposed to second-hand smoke in the lobby, bar, dining rooms and guest rooms. Where ventilation is inadequate, second-hand smoke can pose a risk of cancer and heart disease.
Lifting. Lifting hazards affect staff who load, unload and carry luggage and convention supplies. Back, neck, knee and ankle injuries can result when staff are not trained on proper lifting techniques. Luggage carts should be available. They should be well maintained and equipped with smooth-rolling wheels and safety locks.
Parking and garage hazards. Garage jobs in hotels range from valet parking, to collecting fees, to site maintenance. Employees may work part time, and turnover is often high.
Workers can be struck by vehicles, can inhale exhaust fumes (which contain carbon monoxide among other toxins), or can be exposed to chemicals in automotive products, cleaning products and paints. They can be exposed to asbestos from brake dusts. They can fall from ladders or other maintenance equipment, and can trip or fall due to fluid spills, broken pavement or snow. They can also be assaulted or robbed.
Measures to prevent auto accidents include having clearly marked traffic lanes and walkways, warnings indicating the direction of traffic flow, stop signs for crossing lanes and roped-off areas wherever maintenance work is being done.
Workers exposed to car exhaust, paint fumes and other chemicals should have access to fresh air. Training should be provided about chemical hazards and health effects.
Kerosene heaters sometimes used to warm workers in parking garages can release toxic fumes, and should be prohibited. If heaters are necessary, properly guarded and grounded electric heaters should be used.
Oil spills, water and debris should be cleaned up immediately to prevent falls. Snow should be removed and not allowed to accumulate.
Housekeeping
This group includes housekeepers, laundry workers and supervisors. The department is usually responsible for cleaning and maintaining guest rooms, public areas and meeting and recreational facilities. It may also supply laundry services for guests. Typical safety and health hazards can include:
Repetitive strain injuries (RSIs). Housekeepers are subject to strains from repeated lifting, pushing, bending, reaching and wiping when cleaning bathrooms, changing bed linen, vacuuming rugs, wiping furniture and walls and pushing supply carts from room to room. Laundry workers are also at risk for to RSI injuries due to reaching and to rapid motions from folding, sorting and loading laundry.
Housekeeping carts help transport supplies and equipment, but carts need to be well maintained, with smooth-rolling wheels, and designed to carry heavy loads without tipping over. Carts also need to be relatively light and easy to manoeuvre, with sufficient clearance above the cart so housekeepers can see where they are going.
Training in both ergonomics and proper lifting should be available for housekeepers and laundry workers. Training should include RSI risk factors and methods for reducing them.
Chemical products. Housekeepers and maids use chemical cleaning products for sinks, tubs, toilets, floors and mirrors. Some products can cause dermatitis, respiratory distress and other problems. Some general cleaning agents containing ammonia, detergents and solvents can irritate the skin, eyes, nose and throat. Certain solvent-based products can damage the kidneys and reproductive organs. Disinfectants often contain phenol compounds, which can cause irritation and are suspected to cause cancer.
Preventive measures include supplying protective gloves and substituting with less hazardous products. Proper ventilation should be provided through open windows, mechanical air vents or fans. Chemical storage areas should be well maintained and away from break and eating areas.
Training should be provided about chemical hazards and health effects. It should be conducted in a way staff can understand. To be effective, some training procedures may need translation into workers’ first languages.
Trips and falls. Housekeepers are required to move quickly. Speed can result in slipping on wet floors, falling from tubs and other surfaces when cleaning, and tripping over cords, sheets and bed covers and debris. Laundry staff may slip on wet floors.
Training should be offered emphasizing safety measures to prevent falls and work methods that reduce the need to rush.
Cuts. Cuts from glass, discarded razor blades and debris can be reduced by using liners in wastebaskets and by installing razor blade disposal devices in bathrooms. Workers should be trained in proper waste-handling techniques.
Needlesticks. Used hypodermic needles left by guests in wastebaskets, linens or rooms put hotel staff at risk of getting infectious diseases from accidental punctures. Housekeeping and laundry personnel are the most likely to encounter a discarded needle. Staff should be instructed on how to report and dispose of needles. Staff should have access to approved types of needle receptacle boxes. Management should also have effective medical and counselling procedures to assist staff who have been stuck by a discarded needle.
Heat stress. Hotel laundry workers wash, iron, fold and deliver linen. Heat from machinery, combined with poor ventilation, can result in an oppressive work environment and cause heat stress. Symptoms may include headache, nausea, irritability, fatigue, fainting and accelerated pulse. Eventually these can lead to convulsions and more serious problems if early symptoms are not treated.
Heat stress can be prevented by installing air conditioning, insulating sources of heat, ventilating hot areas with hoods that draw hot air away, taking frequent short breaks in cool areas, drinking plenty of water and wearing loose-fitting clothes. If the work area is only moderately hot (below 35°C), fans may be useful.
Maintenance
Maintenance staff do heavy cleaning, set-up, painting, repair, remodelling and grounds work. Hazards include:
Chemical products. Maintenance staff may use toxic cleaning products to strip and polish floors as well as to clean carpets, walls, furniture, brass fixtures and marble. Certain products can irritate the skin, eyes, nose and throat; can affect the nervous system; and can damage the kidneys, lungs, liver and reproductive system.
Solvents may be present in painting and remodelling materials. Fast-drying paints are used to enable rooms and public areas to be available quickly, but these paints contain high solvent concentrations. Glues used in laying carpet and flooring and in other remodelling jobs may also contain toxic solvents. Solvents can irritate the skin, eyes, nose and throat. Some may damage the nervous system, kidneys, lungs, liver and reproductive organs. Certain solvents are known to cause cancer.
Pesticides and herbicides may be applied in kitchens, dining rooms, public areas, locker rooms and outside the hotel in gardens and driveways. Some of these chemicals can cause respiratory problems; can irritate the skin, eyes, nose and throat; and can damage the nervous system, kidneys, liver and other organs.
Preventive measures include training about chemicals, proper ventilation and proper use of personal protective equipment. If respirators are required, staff should be trained on how to select the proper respirator and cartridge, and how to fit test, use and maintain the equipment. In addition, employees should be given a medical exam to ensure that they are physically fit to work wearing a respirator. Wherever possible, less toxic chemicals should be used.
Asbestos. Asbestos is present in many hotels. Used for years as an insulator and fire retardant, it is found around pipes and in ceiling materials and floor coverings. This highly toxic substance can cause asbestosis, lung cancer or mesothelioma (another form of cancer).
Asbestos is most hazardous when it ages or is damaged. It may begin to break up, creating dust. Hotels should regularly inspect areas where asbestos-containing materials are present to ensure that the asbestos is in good condition.
Extreme caution must be used to protect workers and guests when asbestos dust is present (through ageing or damage or during asbestos abatement jobs). Hotel workers and guests must be kept away from the area, warning signs must be posted and only skilled and licensed personnel should be hired to abate the hazard. The area should be inspected by qualified professionals when work in completed. In new construction or renovation, substitute products should be used in lieu of asbestos.
Trips and falls. Maintenance staff may fall when using ladders and hoists to reach high places such as ceilings, chandeliers, light fixtures, walls and balconies. Training should be provided.
Food and beverage
These staff members include kitchen workers, dishwashers, restaurant servers, room service personnel, hosts and bartenders. Among the hazards are:
Repetitive strain injuries (RSIs). RSIs can occur when room service personnel or restaurant servers deliver food. Trays can be heavy and the server may have to walk long distances. To reduce the risk of injury, room service carts can be used to deliver orders. Carts should be easy to manoeuvre and well maintained. If carts are equipped with heating boxes, the staff should be trained on their proper use.
Trips and falls. Floor surfaces in the kitchen, as well as in all areas to which serving personnel must go, should be kept clean and dry to prevent falls. Spills should be cleaned up immediately. See also the article “Restaurants” in this chapter.
Miscellaneous services
Swimming pools and fitness centres. Many hotels provide swimming facilities or fitness centres for guests. Often showers, saunas, whirlpools, weight rooms and locker rooms are available.
Chemicals used to clean and disinfect showers and locker rooms can cause skin and respiratory irritation. In addition, employees who maintain swimming pools may handle solid or gaseous chlorine. Chlorine leaks can cause burns and severe respiratory problems. If mishandled, it can explode. Employees should be trained on how to handle all these chemicals properly.
Workers who maintain pool and fitness facilities are exposed to injuries from slips and falls. Nonskid, well-maintained and well-drained walking surfaces are important. Water puddles should be wiped up immediately.
Gift shops. Hotels often provide gift and convenience shops for guests. Employees are subject to falls, strains and cuts associated with unpacking and stocking merchandise. They should be trained on proper lifting techniques and should have hand carts to aid in transporting merchandise. Aisles should be kept clear to avoid accidents.
Beauty salons and barber shops. Barbers and cosmetologists risk injuries including skin irritation from hair chemicals, burns from hot towels and curling irons, and cuts and punctures from scissors and razors.
Special hazards include a risk of respiratory problems and possibly even cancer from repeated exposure to certain chemicals such as some hair dye ingredients. There is also a risk of RSIs due to continual use of the hands in awkward postures. Employees should be trained to recognize chemical and ergonomic hazards, and to work in a way that minimizes the risk. They should be supplied with proper gloves and aprons when working with dyes, bleaches, permanent-wave solutions and other chemical products. Shop areas should be properly ventilated to provide fresh air and remove fumes, especially in areas where employees are mixing solutions. Scissors and razors should be properly maintained for ease in cutting, as discussed elsewhere in this Encyclopaedia.
All Occupations
Sexual harassment. Housekeepers and other hotel employees may be exposed to sexual advances from guests or others. Employees should be trained about sexual harassment issues.
Management should have a clear policy on how to report and respond to such incidents.
Fires and other emergencies. Emergencies and disasters can result in loss of life and injuries to both guests and staff. Hotels should have clear emergency response plans, including designated evacuation routes, emergency procedures, an emergency communication system and methods for clearing guests out of the hotel quickly. Certain managers as well as the switchboard operators should have clear instructions on how to coordinate emergency communication with guests and staff.
Staff training and joint labor-management safety meetings are vital components of an effective emergency prevention and response programme. Training sessions and meetings should include translation for staff who need it. Training should be frequent since there is high turnover among hotel workers. Periodic emergency drills should be scheduled, incorporating “walk-throughs” of evacuation routes, staff roles and other emergency procedures.
There should also be a fire prevention programme, including regular inspections. Management and staff members should ensure that exits are not blocked, flammable materials are properly stored, kitchen hoods are regularly cleaned and electrical equipment is well maintained (without frayed wires). Fire retardant materials should be used in interior decorating projects, and there should be screens around fireplaces. Ashtrays should be properly emptied, and candles should be used only in semi-enclosed containers.
Hotel accommodations as well as all facilities attached to the hotel, such as beauty shops, restaurants and gift shops, should be in compliance with all fire codes. Guest rooms and public areas should be equipped with smoke detectors and water sprinklers. Fire extinguishers should be available throughout the hotel. Exits should be well marked and illuminated. Back-up generators should be available to provide emergency lighting and other services.
Evacuation instructions should be posted in each guest room. Many hotels now provide in-room videos with information on fire safety. Guests who are hearing impaired should have rooms equipped with alarms using bright lights to alert them to an emergency. Visually impaired guests should receive emergency procedure information in Braille.
There should be a central alarm system which can display the exact location of a suspected fire. It should also automatically communicate to local emergency services, and broadcast messages over the public address system for guests and staff.
Restaurants
Restaurants can range in size from a small local diner to a large hotel restaurant, and generally consist of three main areas: the kitchen, where the preparation and cooking of meals takes place; the food service, which provides the service of food to guests in the restaurant; and the bar, a lounge which provides live or recorded entertainment and sales of alcoholic beverages and food.
Kitchens
Kitchen personnel include chefs and cooks, who are responsible for preparing and cooking food; pantry persons, who prepare the food for cooking and also keep an inventory of stock; and stewards, who are responsible for the cleaning and maintenance of the kitchen area.
Several different types of accidents can occur in the kitchen area, such as burns from deep fryers, slipping on grease and cuts from knives. Lack of maintenance or improper maintenance in the kitchen area can lead to accidents. Floors that have been mopped should always have a “Wet Floor” placard posted, or kitchen personnel may slip and injure themselves. Trays of food or dishes must be stored securely or they will topple over. Non-slip mats and non-slip floor waxes should be used at entrances and exits. Passageways should always be kept free of boxes, trash cans and other obstacles. Conditions that could cause an accident, such as loose floor tiles, exposed wiring, spills and so on, should always be reported and dealt with as soon as possible and a reporting mechanism should be in place in the workplace.
Another cause of accidents is not using the proper equipment to reach items kept on upper shelves. Items on high shelves should only be retrieved by using a ladder or step stool and not by climbing on boxes or chairs. This means that ladders and step stools must be kept in a convenient location and be in good repair.
Machines, cutting equipment and knives
Accidents and injuries can be common in the kitchen unless safety procedures are properly exercised. The type of machinery used and the high level of activity and pressure in restaurant kitchens during serving hours increase the risk of accidents.
Some common types of machinery used in kitchens are meat grinders, mixers, ice machines and dishwashing machines. Misuse or improper use of this machinery can result in cuts, limbs caught in moving parts and electric shock. To prevent these types of accidents from occurring, kitchen personnel should receive thorough training prior to using the equipment, and should follow the manufacturer’s instructions for safe operation. Other measures to prevent injury are: ensuring equipment is turned off and unplugged before cleaning; wearing snug-fitting clothing with no loose jewellery that can fall off or be caught in the equipment while operating the machinery (long-haired employees should wear hair nets for the same reason); and regular servicing by authorized personnel. One must always avoid pushing food through equipment with one’s hands.
Meat slicers are commonly used in kitchens for slicing meats, fruits and vegetables, and are potentially the most dangerous of any kitchen equipment. Mechanical machine guards must always be in place when slicers are being used. Caution must always be used when cleaning the equipment, particularly when the blades are exposed. When workers finish using the slicer, it should be returned to the zero position and unplugged.
Knives can inflict severe wounds if they are improperly used or stored. Kitchen personnel frequently use knives to chop and dice vegetables and meat prior to cooking. Methods to prevent injuries include: using knives only for the purpose for which they were intended (e.g., not as can openers); ensuring that knives are sharp, since a dull knife requires more pressure and is more likely to slip; carrying knives by the handle, with the blade pointed down; and storing knives in their proper place immediately after cleaning.
Stoves and ovens
Skin burns are the main hazard experienced by kitchen personnel using stoves and ovens. Burns can range from a slight scald to a third-degree burn. Preventive measures include always using oven mitts when lifting pot lids, when transporting pots and when removing hot items from the oven. Oven areas must always be kept free of grease build-up to prevent slipping or accidental fires. If gas ovens are being used, the pilot light must be lit before lighting the oven.
Deep fat fryers are commonly used in kitchens for deep frying various meats and vegetables. The most common hazard associated with these units is skin burns from the splashing of hot grease. Measures that can be taken to ensure the safe use of deep fat fryers are: ensuring that the oil does not overheat and start a fire; cleaning away any grease on the floor around the fryer; preventing overflows by not overfilling the fryer with oil; and using extreme care when filtering or changing the fat in the fryer. Personal protective equipment such as gloves, aprons and long sleeved shirts should always be worn.
Microwave ovens are frequently used in kitchens in order to quickly heat or cook food. The hazards associated with improperly maintained microwave ovens are electrical shock or exposure to leaked microwave radiation. Depending on the amount of leaked radiation and the length of exposure, microwave radiation can damage sensitive human organs. The radiation can also damage medical equipment implanted in the human body, such as pacemakers. Microwave ovens must be kept free of food and grease spills around the doors and seals, since these residues may prevent the oven doors from closing properly and lead to leakage of microwaves. Notices should be posted near the ovens with full instructions on their safe use. All ovens should be checked regularly for proper performance and microwave leakage. They should be repaired or adjusted by trained service personnel.
Tableside cooking
Tableside cooking or serving of flaming foods can result in severe burn injuries to both the server and the customer if improper techniques are used. This type of service should be performed only by staff trained in tableside cooking and in the use of liquid or semi-solid fuel. A carbon dioxide fire extinguisher should be available in case of fire.
Walk-in refrigerators and freezers
Large walk-in refrigerators and freezers are commonly used in restaurant kitchens to store prepared food and ingredients. In addition to the temperature, the major hazard associated with walk-in refrigeration units is that kitchen personnel can be trapped in them if the door accidentally closes behind them. All walk-in cooling equipment must be equipped with interior door opening handles and with alarm switches, and all personnel who use these units should be familiar with the location of these devices.
Care should be taken when walking inside refrigeration units since condensation can cause the floors to become very slippery. To further prevent falling injuries, refrigerator floors should always be kept clear of food scraps and grease. At closing time, a check should always be made to ensure that no one has remained behind in the refrigerators.
Temperature extremes
In the restaurant kitchen almost all personnel are exposed to heat stress; however, the chef or cook is the most exposed since he or she works in close proximity to hot stoves and ovens. Dangerously high air temperatures near stoves and ovens, combined with the heavy uniforms many chefs are required to wear, can cause a number of heat-related health problems. For example, high blood pressure, skin disorders, headaches and fatigue have often been experienced by kitchen personnel. Heat exhaustion and heat stroke can also occur. In extreme cases, fainting and loss of consciousness have been known to happen.
Methods to prevent heat stress include improving ventilation with oven hoods that draw away hot air, implementing work/rest schedules and drinking plenty of water while working. Kitchen personnel should also be educated in recognizing the symptoms of heat disorders.
Kitchen personnel are often exposed to temperature extremes when walking back and forth between walk-in refrigerators and hot kitchens. These sudden changes in temperature can result in respiratory problems. Some kitchen workers are required to work inside refrigerators for extended periods of time, unpacking produce, while arranging boxes of meats and cleaning the interior. These individuals should be given appropriate protective garments to wear while working in these areas.
Ventilation
Good ventilation systems are necessary to remove odour, grease and smoke from kitchen areas. Airborne grease can settle on kitchen equipment and cause it to become slippery. Ventilation systems include fans, air ducts and hoods. These systems should have filters removed and cleaned regularly.
Clean-up
Dish washing
Dishwashing machines can cause skin burns from handling hot dishes and can scald a worker who reaches into the machines before the dishwashing cycle is finished. Dishwashing machines should never be overloaded, since this could cause the machine to jam or to stop operating. Gloves should be used when removing hot dishes directly from the dishwasher.
Cleaning products
In order to keep restaurant kitchens as clean and hygienic as possible, several types of cleaning products and agents are used. Ammonia solutions are often used to clean grease from oven ranges and can be particularly irritating to skin and eyes. Good ventilation should always be provided by fans or oven hoods when using ammonia products.
Other products used include drain cleaners, which are caustic and can cause skin burns and damage to eyes. To protect against splashing, rubber gloves or a face mask should be worn when using these cleaners. Soaps and detergents that are present in floor cleaning products may cause dermatitis or throat irritation, if soap dust is inhaled. Disposable respirators (face masks) may be needed by employees who are sensitive to this type of dust.
To further ensure that cleaning products do not pose a risk to employees, proper handling procedures should always be followed. Cleaning products should always be stored in clearly labelled containers, far away from where food containers are stored. Cleaning products should never be combined, particularly with chlorine bleach, which can cause a hazardous situation if mixed with other cleaning products. Material safety data sheets (MSDSs) are available in many countries for learning about the contents of cleaning products, their effects and how to handle them properly.
Trash compactors
Trash compactors are used for compacting the large amounts of food waste generated in the kitchen into a much smaller volume. These machines should be designed not to operate with the lids open, in order to prevent catching hands or hair in them. The water supply should also be sufficient for the unit to operate safely and efficiently. Care should always be taken to ensure that glass, metal or plastics do not get into the compactor unit, since these materials will cause the machine to jam and lock out.
Pesticides
Pesticides are often used in restaurants to combat insects that are attracted by a food environment. Most pesticides used in restaurants and kitchens are of low hazard to humans. However, some individuals may be sensitive to such products and may develop skin irritation and other allergic reactions.
To prevent misuse of pesticides, training in the use of pesticides should be provided to janitors and other cleaning staff, and serious insect infestations should be treated by a licensed exterminator. Instructions should be printed on all pesticide containers and must be read prior to use, particularly to determine whether the pesticide can be used safely in food areas.
Food Service
Food service personnel include dining room waiters, cocktail waiters, bartenders, hosts, banquet waiters and buspersons. These individuals are responsible for serving meals and beverages, showing guests to their tables and cleaning and maintaining the dining room
Slips and falls
Injuries can result from slips on wet floors or falling over boxes, carts or garbage containers left in the kitchen or dining room area. These injuries could include sprains, broken limbs, injured necks and backs and cuts from falling on sharp objects. To help prevent these accidents, employees should wear sturdy, low-heeled, rubber-soled shoes at all times. All water, grease or food spills should be wiped up immediately, and loose electrical cords and wiring should always be taped down to the floor.
All area rugs in the dining room should be of the non-slip type, with a rubber or other appropriate backing. Carpeting should be checked for frayed or raised edges that can cause food service personnel to trip and fall. Areas where the flooring changes from carpet to tile should always be clearly marked to alert food service personnel of the surface change.
The layout of the dining room is also important in preventing accidents. Tight corners, dim lighting and small exits to the kitchen can result in collisions between food service personnel. Wider corners and clearly marked, well lit exits will lead to safer traffic patterns.
Burns
Food service personnel can suffer skin burns through spilling of hot liquids such as coffee or soup, or from melted wax if tables are candle lit. To prevent spilling of hot liquids, waiters should never overreach when serving hot beverages at a table. When filling soup bowls, food service personnel should be careful to avoid splashes and try not to overfill the bowls.
When carrying hot coffee pots and urns to the dining room, servers should use a small towel to protect hands.
Musculoskeletal injuries
Repetitive strain injuries (RSIs) and other musculoskeletal problems can be experienced by food service personnel who must routinely carry heavy trays, bend and reach to clear, wipe and set tables or carry boxes of restaurant supplies. Well designed workstations and work schedules, such as rotating tasks among food service personnel so that repetitiveness of tasks can be reduced, can diminish the risks.
Training in ergonomics (as well as training in identifying RSI risk factors) can also be helpful to all food service personnel in order to prevent strain injuries.
Many back and neck injuries occur because of improper lifting techniques. For many food service personnel, improper carrying of overloaded trays of dishes and glasses can cause strain on the back and increase the risk of dropping the tray and injuring someone. Training in proper loading and lifting of trays can reduce the risk of injury. For example, distributing the glasses and dishes evenly on the tray and placing one palm under the center of the tray while holding the front edge with the other hand will help create a safer dining room environment.
Stress
The restaurant dining room can be a very high stress environment because of the pressure of performing efficiently while working within tight schedules. Other causes of stress among food service personnel include working shifts, uncertain income because of dependence on gratuities and dealing with irate, difficult customers. Physical stressors such as noise and poor air quality can also be experienced in the restaurant environment. Some symptoms of stress can include headaches, racing heart, ulcers, irritability, insomnia and depression.
Methods to prevent or cope with stress include having workplace meetings that allow employees to share their views about improving work procedures, seminars on stress management techniques, improving air quality and reducing noise. These issues are discussed more fully elsewhere in this Encyclopaedia.
Bars and lounges
Bars or lounges can range in size from a small club or piano lounge to a vast dance/entertainment complex. Most of the hazards presented here are discussed in more detail elsewhere in this Encyclopaedia.
Broken glass is often a hazard in a bar environment because of the large amount of glassware used. Shards from broken glasses can accidentally be ingested by staff and customers. Glass fragments can cause cuts to fingers. There are several methods which can be used to minimize broken glass in the bar areas. Glasses should be inspected regularly for chips and cracks. Any damaged glasses should be discarded immediately. Picking up several glasses in one hand by placing fingers inside the glasses and bringing them together is hazardous since glasses carried in this manner may break.
A glass should never be used to scoop up the ice. A metal ice scoop should always be used when filling glasses with ice. If a glass does break in the ice area, the ice should be melted and all pieces of glass carefully removed. Broken glass should never be handled with bare hands.
Second-hand smoke. Bar personnel are exposed to heavy amounts of second-hand smoke due to the crowded conditions in many bars and lounges. These conditions can pose a risk since second-hand smoke has been linked to lung cancer and other respiratory problems. Every effort possible should be made to improve ventilation in bars and/or to set up non-smoking rooms in the bar areas.
Slips and falls. The rushed environment of a busy bar can contribute to slips and falls. Spilled drinks and leaking beverage containers can result in the area behind the bar being particularly hazardous for bartenders. Buspersons should regularly dry mop behind the bar throughout the evening. Outside the bar area, all spilled drinks should be cleaned up immediately. If the area is carpeted, there should be checks to ensure that there are no ragged edges where people could trip. All bar personnel should wear non-slip rubber-soled shoes.
If the bar has a dance floor, the floor should be made of wood or a material that allows gliding, but the floor should also be clearly distinct in colour from other walking surfaces.
Lifting. Bartenders are often required to lift heavy boxes or kegs of beer. Where possible, dollies should be used to transport kegs and boxes of beer. If proper lifting techniques are not used, back, neck and knee injuries can occur. All heavy lifting should be done using safe lifting techniques.
Bar waiters often carry heavy trays of drinks, which can put considerable stress on the back and neck. Proper tray carrying techniques should be shown to all bar waiters. Physical fitness is important for avoiding back injuries.
Noise. Excessive noise from live entertainment in bars and lounges can result in hearing damage among bar staff. Noise levels of 90 decibels (dB), which is the legal limit in some countries, like the United States, is a level that will lead to hearing loss in some individuals. Annual hearing testing (audiometric testing) is a requirement for all bar personnel exposed to 85 to 90 dB noise levels for 8 hours daily.
To prevent hearing damage among bar personnel, exposure to high noise levels should be limited to short periods of time, and attempts should be made to reduce the sound volume. If these methods are not feasible, then personal protective equipment such as ear plugs should be issued.
Compressed gases. Compressed gases are found in the bar areas where carbonated beverages are served. The canisters of gas must be kept in an upright position at all times or an explosion may occur.
Fire safety
All restaurant employees should be trained in the use of fire extinguishers and should know the location of all the fire alarms. An effective fire prevention programme includes training employees in spotting fire hazards and in proper procedures if a fire does occur. The telephone numbers of emergency-response personnel and instructions on how to summon them should be posted in a prominent area, and all employees should be familiar with an evacuation plan and escape routes. Kitchen personnel in particular should be trained in how to extinguish small fires that may occur in the kitchen.
Good housekeeping is key to fire prevention in restaurants. All areas of the restaurant should be checked for build-up of trash, grease and oil. Combustible materials such as aerosols and greasy rags should be kept in suitable covered containers and garbage cans when not in use. Ducts, filters and fans in the kitchen must be kept free of grease. This will also result in the equipment running more efficiently.
Fire exits from the restaurant must be clearly marked, and passageways to the exits must be free of boxes, trash and other debris. The use of fire detection devices and sprinkler systems should also be part of a good fire prevention programme.
Cashiers
Restaurant cashiers are generally responsible for operating the cash register, handling incoming cash, processing guest receipts and answering the phone. Restaurants can often be targets for hold-ups and robberies, resulting in injuries and even death for cashiers. Management should provide training to cashiers in proper cash-handling procedures and behaviour during a robbery. Other preventive measures are ensuring that the cashiers’ area is well lit and open, and furnishing the cashier area with alarms that can summon security during a robbery. The entire restaurant should be securable after closing, with all exits alarmed and labelled for emergency use only.
Ergonomics
Cashiers in fast food restaurants and cafeterias in particular may develop repetitive motion injuries due to the design of the job and the high workload. Precautions include well-designed work stations with cash registers at comfortable heights. Flexible seats will allow cashiers to sit and relieve lower-back and leg pressures.
General Profile
Hotels and restaurants are found in every country. The economy of hotels and restaurants is intimately tied to the tourism industry, to business travel and to conventions. In many countries, the tourism industry is a major part of the overall economy.
The primary function of a restaurant is to provide food and drink to people outside the home. Types of restaurants include restaurants (which are often costly) with dining rooms and extensive serving staffs; smaller, “family-style” restaurants and cafes which often service the local community; “diners”, or restaurants where serving short-order meals at counters is the major feature; fast food restaurants, where people line up at counters to place their orders and where meals are available in a few minutes, often for taking out to eat elsewhere; and cafeterias, where people go through serving lines and make their selections from a variety of already prepared foods, which are usually displayed in cases. Many restaurants have separate bar or lounge areas, where alcoholic beverages are served, and many larger restaurants have special banquet rooms for groups of people. Street vendors serving food from carts and stalls are common in most countries, often as part of the informal sector of the economy.
The primary function of a hotel is to provide lodging for guests. Types of hotels range from basic overnight facilities, such as inns and motels that cater to business travellers and tourists, to elaborate luxury complexes, such as resorts, spas and convention hotels. Many hotels offer auxiliary services such as restaurants, bars, laundries, health and fitness clubs, beauty salons, barber shops, business centres and gift shops.
Restaurants and hotels can be individually or family-owned and operated, owned by partnerships or owned by large corporate entities. Many corporations do not actually own individual restaurants or hotels in the chain but rather grant a franchise of a name and style to local owners.
The restaurant workforce can include chefs and other kitchen staff, waiters and head waiters, table busing staff, bartenders, a cashier and coatroom personnel. Larger restaurants have staffs which can be highly specialized in their job functions.
The workforce in large a hotel typically will include reception clerks, door and bell persons, security personnel, parking and garage staff, housekeepers, laundry workers, maintenance personnel, kitchen and restaurant workers and office staff.
Most hotel jobs are “blue collar” and require minimal language and literacy skills. Women and immigrant workers comprise the bulk of the workforce in most hotels in developed countries today. In developing countries, hotels tend to be staffed by local residents. Because hotel occupancy levels tend to be seasonal, there is usually a small group of full-time employees with a sizeable number of part-time and seasonal workers. Salaries tend to be in the middle to low income range. As a result of these factors, employee turnover is relatively high.
In restaurants, workforce characteristics are similar, although men comprise a larger proportion of the workforce in restaurants than in hotels. In many countries salaries are low, and the staff waiting on and busing tables may depend on gratuities for a major portion of their income. In many places, a service charge is automatically added to the bill. In fast food restaurants, the workforce are often teenagers and the pay is at the minimum wage.
Motion Sickness
Motion sickness, or kinetosis, is not a pathological condition, but is a normal response to certain motion stimuli with which the individual is unfamiliar and to which he or she is, therefore, unadapted; only those without a functioning vestibular apparatus of the inner ear are truly immune.
Motions producing sickness
There are many different types of provocative motion that induce the motion sickness syndrome. Most are associated with aids to locomotion—in particular, ships, hovercraft, aircraft, automobiles and trains; less commonly, elephants and camels. The complex accelerations generated by fairground amusements, such as swings, roundabouts (merry-go-rounds), roller-coasters and so on, can be highly provocative. In addition, many astronauts/cosmonauts suffer from motion sickness (space-motion sickness) when they first make head movements in the abnormal force environment (weightlessness) of orbital flight. The motion sickness syndrome is also produced by certain moving visual stimuli, without any physical motion of the observer; the external visual world display of fixed-base simulators (simulator sickness) or a large-screen projection of scenes taken from a moving vehicle (Cinerama or IMAX sickness) are examples.
Aetiology
The essential characteristics of stimuli that induce motion sickness is that they generate discordant information from the sensory systems that provide the brain with information about the spatial orientation and motion of the body. The principal feature of this discord is a mismatch between the signals provided, principally, by the eyes and inner ear, and those that the central nervous system “expects” to receive and to be correlated.
Several categories of mismatch can be identified. Most important is the mismatch of signals from the vestibular apparatus (labyrinth) of the inner ear, in which the semicircular canals (the specialized receptors of angular accelerations) and the otolith organs (the specialized receptors of translational accelerations) do not provide concordant information. For example, when a head movement is made in a car or aircraft which is turning, both the semicircular canals and the otoliths are stimulated in an atypical manner and provide erroneous and incompatible information, information that differs substantially from that generated by the same head movement in a stable, 1-G gravity environment. Likewise, low-frequency (below 0.5 Hz) linear accelerations, such as occur aboard ship in rough seas or in an aircraft during flight through turbulent air, also generate conflicting vestibular signals and, hence, are a potent cause of motion sickness.
The mismatch of visual and vestibular information can also be an important contributory factor. The occupant of a moving vehicle who cannot see out is more likely to suffer from motion sickness than one who has a good external visual reference. The passenger below deck or in an aircraft cabin senses motion of the vehicle by vestibular cues, but he or she receives visual information only of his or her relative movement within the vehicle. The absence of an “expected” and concordant signal in a particular sensory modality is also considered to be the essential feature of visually induced motion sickness, because the visual motion cues are not accompanied by the vestibular signals that the individual “expects” to occur when subjected to the motion indicated by the visual display.
Signs and symptoms
On exposure to provocative motion, the signs and symptoms of motion sickness develop in a definite sequence, the time scale being dependent upon the intensity of the motion stimuli and the susceptibility of the individual. There are, however, considerable differences among individuals not only in susceptibility, but also in the order in which particular signs and symptoms develop, or whether they are experienced at all. Typically, the earliest symptom is epigastric discomfort (“stomach awareness”); this is followed by nausea, pallor and sweating, and is likely to be accompanied by a feeling of bodily warmth, increased salivation and eructation (belching). These symptoms commonly develop relatively slowly, but with continuing exposure to the motion, there is a rapid deterioration in well-being, the nausea increases in severity and culminates in vomiting or retching. Vomiting may bring relief, but this is likely to be short-lived unless the motion ceases.
There are other more variable features of the motion sickness syndrome. Alteration of respiratory rhythm with sighing and yawning may be an early symptom, and hyperventilation may occur, particularly in those who are anxious about the cause or consequence of their disability. Headache, tinnitus and dizziness are reported, while in those with severe malaise, apathy and depression are not uncommon, and may be of such severity that personal safety and survival are neglected. A feeling of lethargy and somnolence may be dominant following the cessation of provocative motion, and these may be the only symptoms in situations where adaptation to unfamiliar motion takes place without malaise.
Adaptation
With continued or repeated exposure to a particular provocative motion, most individuals show a decrease in the severity of symptoms; typically after three or four days of continuous exposure (as aboard ship or in a space vehicle) they have adapted to the motion and can carry out their normal duties without disability. In terms of the “mismatch” model, this adaptation or habituation represents the establishment of a new set of “expectations” in the central nervous system. However, on return to a familiar environment, these will no longer be appropriate and symptoms of motion sickness can recur (mal de débarquement) until readaptation occurs. Individuals differ considerably in the rate at which they adapt, the way they retain adaptation and the degree to which they can generalize protective adaptation from one motion environment to another. Unfortunately, a small proportion of the population (probably about 5%) do not adapt, or adapt so slowly that they continue to experience symptoms throughout the period of exposure to provocative motion.
Incidence
The incidence of sickness in a particular motion environment is governed by a number of factors, notably:
- the physical characteristics of the motion (its intensity, frequency and direction of action)
- the duration of exposure
- the intrinsic susceptibility of the individual
- the task being performed
- other environmental factors (e.g., odour).
Not surprisingly, the occurrence of sickness varies widely in different motion environments. For example: nearly all the occupants of life rafts in rough seas will vomit; 60% of student aircrew members suffer from air sickness at some time during training, which in 15%is sufficiently severe to interfere with training; in contrast, less than 0.5% of passengers in civil transport aircraft are affected, although the incidence is higher in small commuter aircraft flying at low altitude in turbulent air.
Laboratory and field studies have shown that for vertical translational oscillatory motion (appropriately called heave), oscillation at a frequency of about 0.2 Hz is the most provocative (figure 1). For a given intensity (peak acceleration) of oscillation, the incidence of sickness falls quite rapidly with an increase in frequency above 0.2 Hz; motion at 1 Hz is less than one-tenth as provocative as that at 0.2 Hz. Likewise, for motion at frequencies below 0.2 Hz, although the relationship between incidence and frequency is not well defined because of a lack of experimental data; certainly, a stable, zero frequency, 1-G environment is not provocative.
Figure 1. Motion sickness incidence as a function of wave frequency and acceleration for 2 hour exposure to vertical sinusoidal motion

Relationships established between the incidence of symptoms of motion sickness and the frequency, magnitude and duration of heave (z-axis) motion have led to the development of simple formulae that can be used to predict incidence when the physical parameters of the motion are known. The concept, embodied in British Standard 6841 (BSI 1987b) and in ISO Draft International Standard 2631-1, is that the incidence of symptoms is proportional to the Motion Sickness Dose Value (MSDVz). The MSDVz (in m/s1.5) is defined:
MSDVz=(a2t)½
where a is the root-mean-square (r.m.s.) value of the frequency-weighted acceleration (in m/s2) determined by linear integration over the duration, t (in seconds), of exposure to the motion.
The frequency weighting to be applied to the stimulus acceleration is a filter having a centre frequency and attenuation characteristics similar to those depicted in figure 1. The weighting function is defined precisely in the standards.
The percentage of an unadapted adult population (P) who are likely to vomit is given by:
P =1/3 MSDVz
Furthermore, the MSDVz may also be used to predict the level of malaise. On a four-point scale of zero (I felt all right) to three (I felt absolutely dreadful) an “illness rating” (I) is given by:
I =0.02MSDVz
Given the large differences among individuals in their susceptibility to motion sickness, the relationship between MSDVz and the occurrence of vomiting in laboratory experiments and in sea trials (figure 2) is acceptable. It should be noted that the formulae were developed from data acquired on exposures lasting from about 20 minutes to six hours with vomiting occurring in up to 70% of individuals (mostly seated) exposed to vertical, heave, motion.
Figure 2. Relationship between incidence of vomiting and stimulus dose (MSDV2), calculated by the procedure described in the text. Data from laboratory experiments volving vertical oscillation (x) and sea trials (+)

Knowledge about the effectiveness of translational oscillation acting in other body axes and other than in a vertical direction is fragmentary. There is some evidence from laboratory experiments on small groups of subjects that translational oscillation in a horizontal plane is more provocative, by a factor of about two, than the same intensity and frequency of vertical oscillation for seated subjects, but is less provocative, also by a factor of two, when the subject is supine and the stimulus acts in the longitudinal (z) body axis. Application of formulae and weighting characteristics embodied in standards to the prediction of sickness incidence should, therefore, be made with caution and due concern for the constraints noted above.
The considerable variability between individuals in their response to provocative motion is an important feature of motion sickness. Differences in susceptibility can, in part, be related to constitutional factors. Infants much below the age of about two years are rarely affected, but with maturation, susceptibility increases rapidly to reach a peak between four and ten years. Thereafter, susceptibility falls progressively so that the elderly are less likely to be affected, but are not immune. In any age group, females are more sensitive than males, the incidence data suggesting a ratio of approximately 1.7:1. Certain dimensions of personality, such as neuroticism, introversion and perceptual style have also been shown to be correlated, albeit weakly, with susceptibility. Motion sickness can also be a conditioned response and a manifestation of phobic anxiety.
Preventive measures
Procedures which minimize the provocative stimulus or increase the tolerance are available. These may prevent sickness in a proportion of the population, but none, other than withdrawal from the motion environment, is 100%effective. In the design of a vehicle, attention to factors which raise the frequency and reduce the magnitude of the oscillations (see figure 1) experienced by occupants during normal operation is beneficial. The provision of head support and body restraint to minimize the unnecessary head movements is advantageous, and is further aided if the occupant can assume a reclined or supine position. Sickness is less if the occupant can be given a view of the horizon; for those deprived of an external visual reference, closing the eyes reduces visual/vestibular conflict. Involvement in a task, particularly control of the vehicle, is also helpful. These measures can be of immediate benefit, but in the longer term the development of protective adaptation is of the greatest value. This is achieved by continued and repeated exposure to the motion environment, though it can be facilitated by ground-based exercises in which provocative stimuli are generated by making head movements whilst rotating on a spin table (desensitization therapy).
There are several drugs which increase tolerance, though all have side-effects (in particular, sedation), so that they should not be taken by those in primary control of a vehicle or when optimum performance is mandatory. For short-term (less than four hours) prophylaxis, 0.3 to 0.6 mg hyoscine hydrobromide (scopolamine) is recommended; longer acting are the antihistaminics, promethazine hydrochloride (25 mg), meclozine hydrochloride (50 mg), dimenhydrinate (50 mg) and cinnarizine (30 mg). The combination of either hyoscine or promethazine with 25 mg ephedrine sulphate increases prophylactic potency with some reduction of side-effects. Prophylaxis for up to 48 hours can be achieved using a scopolamine patch, which allows the drug to be slowly absorbed through the skin at a controlled rate. Effective concentrations of the drug in the body are not achieved until six to eight hours after application of the patch, so the need for this type of therapy must be anticipated.
Treatment
Those suffering from established motion sickness with vomiting should, when practicable, be placed in a position where the motion stimulus is minimized, and be given an anti–motion sickness drug, preferably promethazine by injection. Should vomiting be prolonged and repeated, intravenous replacement of fluid and electrolytes may be necessary.
Hand-Transmitted Vibration
Occupational Exposure
Mechanical vibration arising from powered processes or tools and entering the body at the fingers or the palm of the hands is called hand-transmitted vibration. Frequent synonyms for hand-transmitted vibration are hand-arm vibration and local or segmental vibration. Powered processes and tools which expose operators’ hands to vibration are widespread in several industrial activities. Occupational exposure to hand-transmitted vibration arises from hand-held powered tools used in manufacturing (e.g., percussive metal-working tools, grinders and other rotary tools, impact wrenches), quarrying, mining and construction (e.g., rock-drills, stone-hammers, pick-hammers, vibrocompactors), agriculture and forestry (e.g., chain saws, brush saws, barking machines) and public utilities (e.g., road and concrete breakers, drill-hammers, hand-held grinders). Exposure to hand-transmitted vibration can also occur from vibrating workpieces held in the hands of the operator as in pedestal grinding, and from hand-held vibrating controls as in operating lawn mowers or in controlling vibrating road compactors. It has been reported that the number of persons exposed to hand-transmitted vibration at work exceeds 150,000 in the Netherlands, 0.5 million in Great Britain, and 1.45 million in the United States. Excessive exposure to hand-transmitted vibration can cause disorders in the blood vessels, nerves, muscles, and bones and joints of the upper limbs. It has been estimated that 1.7 to 3.6% of the workers in European countries and the United States are exposed to potentially harmful hand-transmitted vibration (ISSA International Section for Research 1989). The term hand-arm vibration (HAV) syndrome is commonly used to refer to signs and symptoms associated with exposure to hand-transmitted vibration, which include:
- vascular disorders
- peripheral neurological disorders
- bone and joint disorders
- muscle disorders
- other disorders (whole body, central nervous system).
Leisure activities such as motorcycling or using domestic vibrating tools can occasionally expose the hands to vibration of high amplitude, but only long daily exposures may give rise to health problems (Griffin 1990).
The relationship between occupational exposure to hand-transmitted vibration and adverse health effects is far from simple. Table 1 lists some of the most important factors which concur to cause injuries in the upper limbs of vibration-exposed workers.
Table 1. Some factors potentially related to injurious effects during hand-transmitted vibration exposures
Vibration characteristics
- Magnitude (r.m.s., peak, weighted/unweighted)
- Frequency (spectra, dominant frequencies)
- Direction (x-, y-, z- axes)
Tools or processes
- Tool design (portable, fixed)
- Tool type (percussive, rotary, rotating percussive)
- Condition
- Operation
- Material being worked
Exposure conditions
- Duration (daily, yearly exposures)
- Pattern of exposure (continuous, intermittent, rest periods)
- Cumulative exposure duration
Environmental conditions
- Ambient temperature
- Airflow
- Humidity
- Noise
- Dynamic response of the finger-hand-arm system
- Mechanical impedance
- Vibration transmissibility
- Absorbed energy
Individual characteristics
- Method of working (grip force, push force, hand-arm posture, body position)
- Health
- Training
- Skill
- Use of gloves
- Individual susceptibility to injury
Biodynamics
It may be presumed that factors influencing the transmission of vibration into the finger-hand-arm system play a relevant role in the genesis of vibration injury. The transmission of vibration depends on both the physical characteristics of vibration (magnitude, frequency, direction) and the dynamic response of the hand (Griffin 1990).
Transmissibility and impedance
Experimental results indicate that the mechanical behaviour of the human upper limb is complex, as the impedance of the hand-arm system—that is, its resistance to vibrate—shows pronounced variations with the change in vibration amplitude, frequency and direction, applied forces, and orientation of the hand and arm with respect to the axis of the stimulus. Impedance is also influenced by body constitution and structural differences of the various parts of the upper limb (e.g., the mechanical impedance of the fingers is much lower than that of the palm of the hand). In general, higher vibration levels, as well as tighter hand-grips, result in greater impedance. However, the change in impedance has been found to be highly dependent on the frequency and direction of the vibration stimulus and various sources of both intra- and inter-subject variability. A resonance region for the finger-hand-arm system in the frequency range between 80 and 300 Hz has been reported in several studies.
Measurements of the transmission of vibration through the human arm have shown that lower frequency vibration (>50 Hz) is transmitted with little attenuation along the hand and forearm. The attenuation at the elbow is dependent on the arm posture, as the transmission of vibration tends to decrease with the increase of the flexion angle at the elbow joint. For higher frequencies (>50 Hz), the transmission of vibration progressively decreases with increasing frequency, and above 150 to 200 Hz most of the vibrational energy is dissipated in the tissues of the hand and fingers. From transmissibility measurements it has been inferred that in the high-frequency region vibration may be responsible for damage to the soft structures of the fingers and hands, while low-frequency vibration of high amplitude (e.g., from percussive tools) might be associated with injuries to the wrist, elbow and shoulder.
Factors influencing finger and hand dynamics
The adverse effects from vibration exposure may be assumed to be related to the energy dissipated in the upper limbs. Energy absorption is highly dependent on factors affecting the coupling of the finger-hand system to the vibration source. Variations in grip pressure, static force and posture modify the dynamic response of the finger, hand and arm, and, consequently, the amount of energy transmitted and absorbed. For instance, grip pressure has a considerable influence on energy absorption and, in general, the higher the hand grip the greater the force transmitted to the hand-arm system. Dynamic response data can provide relevant information to assess the injury potential of tool vibration and to assist in the development of anti-vibration devices such as hand-grips and gloves.
Acute Effects
Subjective discomfort
Vibration is sensed by various skin mechanoreceptors, which are located in the (epi)dermal and subcutaneous tissues of the smooth and bare (glabrous) skin of the fingers and hands. They are classified into two categories—slow and fast adapting—according to their adaptation and receptive field properties. Merkel discs and Ruffini endings are found in the slow-adapting mechanoreceptive units, which respond to static pressure and slow changes in pressure and are excited at low frequency (<16 Hz). Fast-adapting units have Meissner’s corpuscles and Pacinian corpuscles, which respond to rapid changes in stimulus and are responsible for vibratory sensation in the frequency range between 8 and 400 Hz. The subjective response to hand-transmitted vibration has been used in several studies to obtain threshold values, contours of equivalent sensation and unpleasant or tolerance limits for vibratory stimuli at different frequencies (Griffin 1990). Experimental results indicate that human sensitivity to vibration decreases with increasing frequency for both comfort and annoyance vibration levels. Vertical vibration appears to cause more discomfort than vibration in other directions. Subjective discomfort has also been found to be a function of the spectral composition of vibration and the grip force exerted on the vibrating handle.
Activity interference
Acute exposure to hand-transmitted vibration can cause a temporary increase in vibrotactile thresholds due to a depression of the excitability of the skin mechanoreceptors. The magnitude of the temporary threshold shift as well as the time for recovery is influenced by several variables, such as the characteristics of the stimulus (frequency, amplitude, duration), temperature as well as the worker’s age and previous exposure to vibration. Exposure to cold aggravates the tactile depression induced by vibration, because low temperature has a vasoconstrictive effect on digital circulation and reduces finger skin temperature. In vibration-exposed workers who often operate in a cold environment, repeated episodes of acute impairment of tactile sensitivity can lead to permanent reduction in sensory perception and loss of manipulative dexterity, which, in turn, can interfere with work activity, increasing the risk for acute injuries due to accidents.
Non-Vascular Effects
Skeletal
Vibration-induced bone and joint injuries are a controversial matter. Various authors consider that disorders of bones and joints in workers using hand-held vibrating tools are not specific in character and similar to those due to the ageing process and to heavy manual work. On the other hand, some investigators have reported that characteristic skeletal changes in the hands, the wrists and the elbows can result from prolonged exposure to hand-transmitted vibration. Early x-ray investigations had revealed a high prevalence of bone vacuoles and cysts in the hands and wrists of vibration-exposed workers, but more recent studies have shown no significant increase with respect to control groups made up of manual workers. Excess prevalence of wrist osteoarthrosis and elbow arthrosis and osteophytosis has been reported in coal miners, road construction workers and metal-working operators exposed to shocks and low frequency vibration of high amplitude from pneumatic percussive tools. On the contrary, there is little evidence for an increased prevalence of degenerative bone and joint disorders in the upper limbs of workers exposed to mid- or high-frequency vibrations arising from chain saws or grinding machines. Heavy physical effort, forceful gripping and other biomechanical factors can account for the higher occurrence of skeletal injuries found in workers operating percussive tools. Local pain, swelling, and joint stiffness and deformities may be associated with radiological findings of bone and joint degeneration. In a few countries (including France, Germany, Italy), bone and joint disorders occurring in workers using hand-held vibrating tools are considered to be an occupational disease, and the affected workers are compensated.
Neurological
Workers handling vibrating tools may experience tingling and numbness in their fingers and hands. If vibration exposure continues, these symptoms tend to worsen and can interfere with work capacity and life activities. Vibration-exposed workers may exhibit increased vibratory, thermal and tactile thresholds in clinical examinations. It has been suggested that continuous vibration exposure can not only depress the excitability of skin receptors but also induce pathological changes in the digital nerves such as perineural oedema, followed by fibrosis and nerve fibre loss. Epidemiological surveys of vibration-exposed workers show that the prevalence of peripheral neurological disorders varies from a few per cent to more than 80 per cent, and that sensory loss affects users of a wide range of tool types. It seems that vibration neuropathy develops independently of other vibration-induced disorders. A scale of the neurological component of the HAV syndrome was proposed at the Stockholm Workshop 86 (1987), consisting of three stages according to the symptoms and the results of clinical examination and objective tests (table 2).
Table 2. Sensorineural stages of the Stockholm Workshop scale for the hand-arm vibration syndrome
|
Stage |
Signs and symptoms |
|
0SN |
Exposed to vibration but no symptoms |
|
1SN |
Intermittent numbness, with or without tingling |
|
2SN |
Intermittent or persistent numbness, reduced sensory perception |
|
3SN |
Intermittent or persistent numbness, reduced tactile discrimination and/or |
Source: Stockholm Workshop 86 1987.
Careful differential diagnosis is required to distinguish vibration neuropathy from entrapment neuropathies, such as carpal tunnel syndrome (CTS), a disorder due to compression of the median nerve as it passes through an anatomical tunnel in the wrist. CTS seems to be a common disorder in some occupational groups using vibrating tools, such as rock-drillers, platers and forestry workers. It is believed that ergonomic stressors acting on the hand and wrist (repetitive movements, forceful gripping, awkward postures), in addition to vibration, can cause CTS in workers handling vibrating tools. Electroneuromyography measuring sensory and motor nerve velocities has proven to be useful to differentiate CTS from other neurological disorders.
Muscular
Vibration-exposed workers may complain of muscle weakness and pain in the hands and arms. In some individuals muscle fatigue can cause disability. A decrease in hand-grip strength has been reported in follow-up studies of lumberjacks. Direct mechanical injury or peripheral nerve damage have been suggested as possible aetiological factors for muscle symptoms. Other work-related disorders have been reported in vibration-exposed workers, such as tendinitis and tenosynovitis in the upper limbs, and Dupuytren’s contracture, a disease of the fascial tissue of the palm of the hand. These disorders seem to be related to ergonomic stress factors arising from heavy manual work, and the association with hand-transmitted vibration is not conclusive.
Vascular Disorders
Raynaud’s phenomenon
Giovanni Loriga, an Italian physician, first reported in 1911 that stone cutters using pneumatic hammers on marble and stone blocks at some yards in Rome suffered from finger blanching attacks, resembling the digital vasospastic response to cold or emotional stress described by Maurice Raynaud in 1862. Similar observations were made by Alice Hamilton (1918) among stone cutters in the United States, and later by several other investigators. In the literature various synonyms have been used to describe vibration-induced vascular disorders: dead or white finger, Raynaud’s phenomenon of occupational origin, traumatic vasospastic disease, and, more recently, vibration-induced white finger (VWF). Clinically, VWF is characterized by episodes of white or pale fingers caused by spastic closure of the digital arteries. The attacks are usually triggered by cold and last from 5 to 30 to 40 minutes. A complete loss of tactile sensitivity may be experienced during an attack. In the recovery phase, commonly accelerated by warmth or local massage, redness may appear in the affected fingers as a result of a reactive increase of blood flow in the cutaneous vessels. In the rare advanced cases, repeated and severe digital vasospastic attacks can lead to trophic changes (ulceration or gangrene) in the skin of the fingertips. To explain cold-induced Raynaud’s phenomenon in vibration-exposed workers, some researchers invoke an exaggerated central sympathetic vasoconstrictor reflex caused by prolonged exposure to harmful vibration, while others tend to emphasize the role of vibration-induced local changes in the digital vessels (e.g., thickening of the muscular wall, endothelial damage, functional receptor changes). A grading scale for the classification of VWF has been proposed at the Stockholm Workshop 86 (1987), (table 3). A numerical system for VWF symptoms developed by Griffin and based on scores for the blanching of different phalanges is also available (Griffin 1990). Several laboratory tests are used to diagnose VWF objectively. Most of these tests are based on cold provocation and the measurement of finger skin temperature or digital blood flow and pressure before and after cooling of fingers and hands.
Table 3. The Stockholm Workshop scale for staging cold-induced Raynaud’s phenomenon in the hand-arm vibration syndrome
|
Stage |
Grade |
Symptoms |
|
0 |
— |
No attacks |
|
1 |
Mild |
Occasional attacks affecting only the tips of one or more fingers |
|
2 |
Moderate |
Occasional attacks affecting distal and middle (rarely also |
|
3 |
Severe |
Frequent attacks affecting all phalanges of most fingers |
|
4 |
Very severe |
As in stage 3, with trophic skin changes in the finger tips |
Source: Stockholm Workshop 86 1987.
Epidemiological studies have pointed out that the prevalence of VWF is very wide, from less than 1 to 100 per cent. VWF has been found to be associated with the use of percussive metal-working tools, grinders and other rotary tools, percussive hammers and drills used in excavation, vibrating machinery used in the forest, and other powered tools and processes. VWF is recognized as an occupational disease in many countries. Since 1975–80 a decrease in the incidence of new cases of VWF has been reported among forestry workers in both Europe and Japan after the introduction of anti-vibration chain saws and administrative measures curtailing saw usage time. Similar findings are not yet available for tools of other types.
Other Disorders
Some studies indicate that in workers affected with VWF hearing loss is greater than that expected on the basis of ageing and noise exposure from the use of vibrating tools. It has been suggested that VWF subjects may have an additional risk of hearing impairment due to vibration-induced reflex sympathetic vasoconstriction of the blood vessels supplying the inner ear. In addition to peripheral disorders, other adverse health effects involving the endocrine and central nervous system of vibration-exposed workers have been reported by some Russian and Japanese schools of occupational medicine (Griffin 1990). The clinical picture, called “vibration disease,” includes signs and symptoms related to dysfunction of the autonomic centres of the brain (e.g., persistent fatigue, headache, irritability, sleep disturbances, impotence, electroencephalographic abnormalities). These findings should be interpreted with caution and further carefully designed epidemiological and clinical research work is needed to confirm the hypothesis of an association between disorders of the central nervous system and exposure to hand-transmitted vibration.
Standards
Several countries have adopted standards or guidelines for hand-transmitted vibration exposure. Most of them are based on the International Standard 5349 (ISO 1986). To measure hand-transmitted vibration ISO 5349 recommends the use of a frequency-weighting curve which approximates the frequency-dependent sensitivity of the hand to vibration stimuli. The frequency-weighted acceleration of vibration (ah,w) is obtained with an appropriate weighting-filter or by summation of weighted acceleration values measured in octave or one-third octave bands along an orthogonal coordinate system (xh, yh, zh), (figure 1). In ISO 5349 the daily exposure to vibration is expressed in terms of energy-equivalent frequency-weighted acceleration for a period of four hours ((ah,w)eq(4) in m/s2 r.m.s), according to the following equation:
(ah,w)eq(4)=(T/4)½(ah,w)eq(T)
where T is the daily exposure time expressed in hours and (ah,w)eq(T) is the energy-equivalent frequency-weighted acceleration for the daily exposure time T. The standard provides guidance to calculate (ah,w)eq(T) if a typical work-day is characterized by several exposures of different magnitudes and durations. Annex A to ISO 5349 (which does not form part of the standard) proposes a dose-effect relationship between (ah,w)eq(4) and VWF, which can be approximated by the equation:
C=[(ah,w)eq(4) TF/95]2 x 100
where C is the percentile of exposed workers expected to show VWF (in the range 10 to 50%), and TF is the exposure time before finger blanching among the affected workers (in the range 1 to 25 years). The dominant, single-axis component of vibration directed into the hand is used to calculate (ah,w)eq(4), which should not be in excess of 50 m/s2. According to the ISO dose-effect relationship, VWF may be expected to occur in about 10% of workers with daily vibration exposure to 3 m/s2 for ten years.
Figure 1. Basicentric coordinate system for the measurement of hand-transmitted vibration
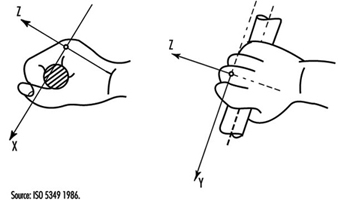
In order to minimize the risk of vibration-induced adverse health effects, action levels and threshold limit values (TLVs) for vibration exposure have been proposed by other committees or organizations. The American Conference of Government Industrial Hygienists (ACGIH) has published TLVs for hand-transmitted vibration measured according to the ISO frequency-weighting procedure (American Conference of Governmental Industrial Hygienists 1992), (table 4). According to ACGIH, the proposal TLVs concern vibration exposure to which “nearly all workers may be exposed repeatedly without progressing beyond Stage 1 of the Stockholm Workshop Classification System for VWF”. More recently, exposure levels for hand-transmitted vibration have been presented by the Commission of the European Communities within a proposal of a Directive for the protection of workers against the risks arising from physical agents (Council of the European Union 1994), (table 5). In the proposed Directive the quantity used for the assessment of vibration hazard is expressed in terms of an eight-hour energy-equivalent frequency-weighted acceleration, A(8)=(T/8)½ (ah,w)eq(T), by using the vector sum of weighted accelerations determined in orthogonal coordinates asum=(ax,h,w2+ay,h,w2+az,h,w2)½ on the vibrating tool handle or workpiece. The methods of measurement and assessment of vibration exposure reported in the Directive are basically derived from the British Standard (BS) 6842 (BSI 1987a). The BS standard, however, does not recommend exposure limits, but provides an informative appendix on the state of knowledge of the dose-effect relationship for hand-transmitted vibration. The estimated frequency-weighted acceleration magnitudes liable to cause VWF in 10% of workers exposed to vibration according to the BS standard are reported in table 6.
___________________________________________________________________________
Table 4. Threshold limit values for hand-transmitted vibration
|
Total daily exposure (hours) |
Frequency-weighted r.m.s. acceleration in the dominant direction that should not be exceeded |
|
|
|
|
g* |
|
4-8 |
4 |
0.40 |
|
2-4 |
6 |
0.61 |
|
1-2 |
8 |
0.81 |
|
1 |
12 |
1.22 |
* 1 g = 9.81 ![]() .
.
Source: According to the American Conference of Government Industrial Hygienists 1992.
___________________________________________________________________________
Table 5. Proposal of the Council of the European Union for a Council Directive on physical agents: Annex II A. Hand-transmitted vibration (1994)
|
Levels ( |
A(8)* |
Definitions |
|
Threshold |
1 |
The exposure value below which continuous and/or repetitive exposure has no adverse effect on health and safety of workers |
|
Action |
2.5 |
The value above which one or more of the measures** specified in the relevant Annexes must be undertaken |
|
Exposure limit value |
5 |
The exposure value above which an unprotected person is exposed to unacceptable risks. Exceeding this level is prohibited and must be prevented through the implementation of the provisions of the Directive*** |
* A(8) = 8 h energy-equivalent frequency-weighted acceleration.
** Information, training, technical measures, health surveillance.
*** Appropriate measures for the protection of health and safety.
___________________________________________________________________________
Table 6. Frequency-weighted vibration acceleration magnitudes (![]() r.m.s.) which may be expected to produce finger blanching in 10% of persons exposed*
r.m.s.) which may be expected to produce finger blanching in 10% of persons exposed*
|
Daily exposure (hours) |
Life-time exposure (years) |
|||||
|
|
0.5 |
1 |
2 |
4 |
8 |
16 |
|
0.25 |
256.0 |
128.0 |
64.0 |
32.0 |
16.0 |
8.0 |
|
0.5 |
179.2 |
89.6 |
44.8 |
22.4 |
11.2 |
5.6 |
|
1 |
128.0 |
64.0 |
32.0 |
16.0 |
8.0 |
4.0 |
|
2 |
89.6 |
44.8 |
22.4 |
11.2 |
5.6 |
2.8 |
|
4 |
64.0 |
32.0 |
16.0 |
8.0 |
4.0 |
2.0 |
|
8 |
44.8 |
22.4 |
11.2 |
5.6 |
2.8 |
1.4 |
* With short duration exposure the magnitudes are high and vascular disorders may not be the first adverse symptom to develop.
Source: According to British Standard 6842. 1987, BSI 1987a.
___________________________________________________________________________
Measurement and Evaluation of Exposure
Vibration measurements are made to provide assistance for the development of new tools, to check vibration of tools at purchase, to verify maintenance conditions, and to assess human exposure to vibration at the workplace. Vibration-measuring equipment generally consists of a transducer (usually an accelerometer), an amplifying device, filter (bandpass filter and/or frequency-weighting network), and amplitude or level indicator or recorder. Vibration measurements should be made on the tool handle or workpiece close to the surface of the hand(s) where the vibration enters the body. Careful selection of the accelerometers (e.g., type, mass, sensitivity) and appropriate methods of mounting the accelerometer on the vibrating surface are required to obtain accurate results. Vibration transmitted to the hand should be measured and reported in the appropriate directions of an orthogonal coordinate system (figure 1). The measurement should be made over a frequency range of at least 5 to 1,500 Hz, and the acceleration frequency content of vibration in one or more axes can be presented in octave bands with centre frequencies from 8 to 1,000 Hz or in one-third octave bands with centre frequencies from 6.3 to 1,250 Hz. Acceleration can also be expressed as frequency-weighted acceleration by using a weighting network which complies with the characteristics specified in ISO 5349 or BS 6842. Measurements at the workplace show that different vibration magnitudes and frequency spectra can occur on tools of the same type or when the same tool is operated in a different manner. Figure 2 reports the mean value and the range of distribution of weighted accelerations measured in the dominant axis of power-driven tools used in forestry and industry (ISSA International Section for Research 1989). In several standards hand-transmitted vibration exposure is assessed in terms of four-hour or eight-hour energy-equivalent frequency-weighted acceleration calculated by means of the equations above. The method for obtaining energy-equivalent acceleration assumes that the daily exposure time required to produce adverse health effects is inversely proportional to the square of frequency-weighted acceleration (e.g., if the vibration magnitude is halved then exposure time may be increased by a factor of four). This time dependency is considered to be reasonable for standardization purposes and is convenient for instrumentation, but it should be noted that it is not fully substantiated by epidemiological data (Griffin 1990).
Figure 2. Mean values and range of distribution of frequency-weighted r.m.s. acceleration in the dominant axis measured on the handle(s) of some power tools used in forestry and industry
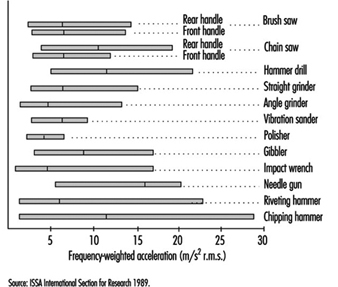
Prevention
The prevention of injuries or disorders caused by hand-transmitted vibration requires the implementation of administrative, technical and medical procedures (ISO 1986; BSI 1987a). Appropriate advice to the manufacturers and users of vibrating tools should also be given. Administrative measures should include adequate information and training to instruct the operators of vibrating machinery to adopt safe and correct work practices. Since continuous exposure to vibration is believed to increase vibration hazard, work schedules should be arranged to include rest periods. Technical measures should include the choice of tools with the lowest vibration and with appropriate ergonomic design. According to the EC Directive for the safety of machinery (Council of the European Communities 1989), the manufacturer shall make public whether the frequency-weighted acceleration of hand-transmitted vibration exceeds 2.5 m/s2, as determined by suitable test codes such as indicated in the International Standard ISO 8662/1 and its companion documents for specific tools (ISO 1988). Tool maintenance conditions should be carefully checked by periodic vibration measurements. Pre-employment medical screening and subsequent clinical examinations at regular intervals should be performed on vibration-exposed workers. The aims of medical surveillance are to inform the worker of the potential risk associated with vibration exposure, to assess health status and to diagnose vibration-induced disorders at the early stage. At the first screening examination particular attention should be paid to any condition which may be aggravated by exposure to vibration (e.g., constitutional tendency to white finger, some forms of secondary Raynaud’s phenomenon, past injuries to the upper limbs, neurological disorders). Avoidance or reduction of vibration exposure for the affected worker should be decided after considering both the severity of symptoms and the characteristics of the entire working process. The worker should be advised to wear adequate clothing to keep the entire body warm, and to avoid or minimize the smoking of tobacco and the use of some drugs which can affect peripheral circulation. Gloves may be useful to protect the fingers and hands from traumas and to keep them warm. So-called anti-vibration gloves may provide some isolation of the high frequency components of vibration arising from some tools.
Whole-Body Vibration
Occupational Exposure
Occupational exposures to whole-body vibration mainly occur in transport but also in association with some industrial processes. Land, sea and air transport can all produce vibration that can cause discomfort, interfere with activities or cause injury. Table 1 lists some environments which may be most likely to be associated with a health risk.
Table 1. Activities for which it may be appropriate to warn of the adverse effects of whole-body vibration
Tractor driving
Armoured fighting vehicles (e.g., tanks) and similar vehicles
Other off-road vehicles:
Earth-moving machinery—loaders, excavators, bulldozers, graders,
- scrapers, dumpers, rollers
- Forest machines
- Mine and quarry equipment
- Forklift trucks
Some truck driving (articulated and non-articulated)
Some bus and tram driving
Some helicopter and fixed-wing aircraft flying
Some workers with concrete production machinery
Some railway drivers
Some use of high-speed marine craft
Some motor bicycle riding
Some car and van driving
Some sports activities
Some other industrial equipment
Source: Adapted from Griffin 1990.
The most common exposure to severe vibration and shocks may occur on off-road vehicles, including earth moving machinery, industrial trucks and agricultural tractors.
Biodynamics
Like all mechanical structures, the human body has resonance frequencies where the body exhibits a maximum mechanical response. Human responses to vibration cannot be explained solely in terms of a single resonance frequency. There are many resonances in the body, and the resonance frequencies vary among people and with posture. Two mechanical responses of the body are often used to describe the manner in which vibration causes the body to move: transmissibility and impedance.
The transmissibility shows the fraction of the vibration which is transmitted from, say, the seat to the head. The transmissibility of the body is highly dependent on vibration frequency, vibration axis and body posture. Vertical vibration on a seat causes vibration in several axes at the head; for vertical head motion, the transmissibility tends to be greatest in the approximate range of 3 to 10 Hz.
The mechanical impedance of the body shows the force that is required to make the body move at each frequency. Although the impedance depends on body mass, the vertical impedance of the human body usually shows a resonance at about 5 Hz. The mechanical impedance of the body, including this resonance, has a large effect on the manner in which vibration is transmitted through seats.
Acute Effects
Discomfort
The discomfort caused by vibration acceleration depends on the vibration frequency, the vibration direction, the point of contact with the body, and the duration of vibration exposure. For vertical vibration of seated persons, the vibration discomfort caused by any frequency increases in proportion to the vibration magnitude: a halving of the vibration will tend to halve the vibration discomfort.
The discomfort produced by vibration may be predicted by the use of appropriate frequency weightings (see below) and described by a semantic scale of discomfort. There are no useful limits for vibration discomfort: the acceptable discomfort varies from one environment to another.
Acceptable magnitudes of vibration in buildings are close to vibration perception thresholds. The effects on humans of vibration in buildings are assumed to depend on the use of the building in addition to the vibration frequency, direction and duration. Guidance on the evaluation of building vibration is given in various standards such as British Standard 6472 (1992) which defines a procedure for the evaluation of both vibration and shock in buildings.
Activity interference
Vibration can impair the acquisition of information (e.g., by the eyes), the output of information (e.g., by hand or foot movements) or the complex central processes that relate input to output (e.g., learning, memory, decision-making). The greatest effects of whole-body vibration are on input processes (mainly vision) and output processes (mainly continuous hand control).
Effects of vibration on vision and manual control are primarily caused by the movement of the affected part of the body (i.e., eye or hand). The effects may be decreased by reducing the transmission of vibration to the eye or to the hand, or by making the task less susceptible to disturbance (e.g., increasing the size of a display or reducing the sensitivity of a control). Often, the effects of vibration on vision and manual control can be much reduced by redesign of the task.
Simple cognitive tasks (e.g., simple reaction time) appear to be unaffected by vibration, other than by changes in arousal or motivation or by direct effects on input and output processes. This may also be true for some complex cognitive tasks. However, the sparsity and diversity of experimental studies does not exclude the possibility of real and significant cognitive effects of vibration. Vibration may influence fatigue, but there is little relevant scientific evidence, and none which supports the complex form of the “fatigue-decreased proficiency limit” offered in International Standard 2631 (ISO 1974, 1985).
Changes in Physiological Functions
Changes in physiological functions occur when subjects are exposed to a novel whole-body vibration environment in laboratory conditions. Changes typical of a “startle response” (e.g., increased heart rate) normalize quickly with continuing exposure, whereas other reactions either proceed or develop gradually. The latter can depend on all characteristics of vibration including the axis, the magnitude of acceleration, and the kind of vibration (sinusoidal or random), as well as on further variables such as circadian rhythm and characteristics of the subjects (see Hasan 1970; Seidel 1975; Dupuis and Zerlett 1986). Changes of physiological functions under field conditions often cannot be related to vibration directly, since vibration is often acting together with other significant factors, such as high mental strain, noise and toxic substances. Physiological changes are frequently less sensitive than psychological reactions (e.g., discomfort). If all available data on persistent physiological changes are summarized with respect to their first significant appearance depending on the magnitude and frequency of whole-body vibration, there is a boundary with a lower border around 0.7 m/s2 r.m.s. between 1 and 10 Hz, and rising up to 30 m/s2 r.m.s. at 100 Hz. Many animal studies have been performed, but their relevance to humans is doubtful.
Neuromuscular changes
During active natural motion, motor control mechanisms act as a feed-forward control that is constantly adjusted by additional feedback from sensors in muscles, tendons and joints. Whole-body vibration causes a passive artificial motion of the human body, a condition that is fundamentally different from the self-induced vibration caused by locomotion. The missing feed-forward control during whole-body vibration is the most distinct change of the normal physiological function of the neuromuscular system. The broader frequency range associated with whole-body vibration (between 0.5 and 100 Hz) compared to that for natural motion (between 2 and 8 Hz for voluntary movements, and below 4 Hz for locomotion) is a further difference that helps to explain reactions of the neuromuscular control mechanisms at very low and at high frequencies.
Whole-body vibration and transient acceleration cause an acceleration-related alternating activity in the electromyogram (EMG) of superficial back muscles of seated persons that requires a tonic contraction to be maintained. This activity is supposed to be of a reflex-like nature. It usually disappears completely if the vibrated subjects sit relaxed in a bent position. The timing of muscle activity depends on the frequency and magnitude of acceleration. Electromyographic data suggest that an increased spinal load can occur due to reduced muscular stabilization of the spine at frequencies from 6.5 to 8 Hz and during the initial phase of a sudden upward displacement. In spite of weak EMG activity caused by whole-body vibration, back muscle fatigue during vibration exposure can exceed that observed in normal sitting postures without whole-body vibration.
Tendon reflexes may be diminished or disappear temporarily during exposure to sinusoidal whole-body vibration at frequencies above 10 Hz. Minor changes of postural control after exposure to whole-body vibration are quite variable, and their mechanisms and practical significance are not certain.
Cardiovascular, respiratory, endocrine and metabolic changes
The observed changes persisting during exposure to vibration have been compared to those during moderate physical work (i.e., increases of heart rate, blood pressure and oxygen consumption) even at a vibration magnitude near to the limit of voluntary tolerance. The increased ventilation is partially caused by oscillations of the air in the respiratory system. Respiratory and metabolic changes may not correspond, possibly suggesting a disturbance of the respiration control mechanisms. Various and partially contradictory findings have been reported for changes of the adrenocorticotropic hormones (ACTH) and catecholamines.
Sensory and central nervous changes
Changes of vestibular function due to whole-body vibration have been claimed on the basis of an affected regulation of posture, although posture is controlled by a very complex system in which a disturbed vestibular function can be largely compensated by other mechanisms. Changes of the vestibular function seem to gain significance for exposures with very low frequencies or those near the resonance of the whole body. A sensory mismatch between vestibular, visual and proprioceptive (stimuli received within the tissues) information is supposed to be an important mechanism underlying physiological responses to some artificial motion environments.
Experiments with short-term and prolonged combined exposures to noise and whole-body vibration, seem to suggest that vibration has a minor synergistic effect on hearing. As a tendency, high intensities of whole-body vibration at 4 or 5 Hz were associated with higher additional temporary threshold shifts (TTS). There was no obvious relation between the additional TTS and exposure time. The additional TTS seemed to increase with higher doses of whole-body vibration.
Impulsive vertical and horizontal vibrations evoke brain potentials. Changes of the function of the human central nervous system have also been detected using auditory evoked brain potentials (Seidel et al. 1992). The effects were influenced by other environmental factors (e.g., noise), the difficulty of the task, and by the internal state of the subject (e.g., arousal, degree of attention towards the stimulus).
Long-Term Effects
Spinal health risk
Epidemiological studies have frequently indicated an elevated health risk for the spine in workers exposed for many years to intense whole-body vibration (e.g., work on tractors or earth-moving machines). Critical surveys of the literature have been prepared by Seidel and Heide (1986), Dupuis and Zerlett (1986) and Bongers and Boshuizen (1990). These reviews concluded that intense long-term whole-body vibration can adversely affect the spine and can increase the risk of low-back pain. The latter may be a secondary consequence of a primary degenerative change of the vertebrae and disks. The lumbar part of the vertebral column was found to be the most frequently affected region, followed by the thoracic region. A high rate of impairments of the cervical part, reported by several authors, seems to be caused by a fixed unfavourable posture rather than by vibration, although there is no conclusive evidence for this hypothesis. Only a few studies have considered the function of back muscles and found a muscular insufficiency. Some reports have indicated a significantly higher risk of the dislocation of lumbar disks. In several cross-sectional studies Bongers and Boshuizen (1990) found more low-back pain in drivers and helicopter pilots than in comparable reference workers. They concluded that professional vehicle driving and helicopter flying are important risk factors for low-back pain and back disorder. An increase in disability pensioning and long-term sick leave due to intervertebral disc disorders was observed among crane operators and tractor drivers.
Due to incomplete or missing data on exposure conditions in epidemiological studies, exact exposure-effect relationships have not been obtained. The existing data do not permit the substantiation of a no-adverse-effect level (i.e., safe limit) so as to reliably prevent diseases of the spine. Many years of exposure below or near the exposure limit of the current International Standard 2631 (ISO 1985) are not without risk. Some findings have indicated an increasing health risk with increased duration of exposure, although selection processes have made it difficult to detect a relation in the majority of studies. Thus, a dose-effect relationship cannot currently be established by epidemiological investigations. Theoretical considerations suggest marked detrimental effects of high peak loads acting on the spine during exposures with high transients. The use of an “energy equivalent” method to calculate a vibration dose (as in International Standard 2631 (ISO 1985)) is therefore questionable for exposures to whole-body vibration containing high peak accelerations. Different long-term effects of whole-body vibration depending on the vibration frequency have not been derived from epidemiological studies. Whole-body vibration at 40 to 50 Hz applied to standing workers through the feet was followed by degenerative changes of the bones of the feet.
In general, differences between subjects have been largely neglected, although selection phenomena suggest they may be of major importance. There are no clear data showing whether the effects of whole-body vibration on the spine depend on gender.
The general acceptance of degenerative disorders of the spine as an occupational disease is debated. Specific diagnostic features are not known which would permit a reliable diagnosis of the disorder as an outcome of exposure to whole-body vibration. A high prevalence of degenerative spinal disorders in non-exposed populations hinders the assumption of a predominantly occupational aetiology in individuals exposed to whole-body vibration. Individual constitutional risk factors that might modify vibration-induced strain are unknown. The use of a minimal intensity and/or a minimal duration of whole-body vibration as a prerequisite for the recognition of an occupational disease would not take into account the expected considerable variability in individual susceptibility.
Other health risks
Epidemiological studies suggest that whole-body vibration is one factor within a causative set of factors which contribute to other health risks. Noise, high mental strain and shift work are examples of important concomitant factors which are known to be associated with health disorders. The results of investigations into disorders of other bodily systems have often been divergent or have indicated a paradoxical dependence of the prevalence of pathology on the magnitude of whole-body vibration (i.e., a higher prevalence of adverse effects with a lower intensity). A characteristic complex of symptoms and pathological changes of the central nervous system, the musculo-skeletal system and the circulatory system has been observed in workers standing on machines used for the vibro-compression of concrete and exposed to whole-body vibration beyond the exposure limit of ISO 2631 with frequencies above 40 Hz (Rumjancev 1966). This complex was designated as “vibration disease”. Although rejected by many specialists, the same term has sometimes been used to describe a vague clinical picture caused by long-term exposure to low-frequency whole-body vibration which, allegedly, is manifested initially as peripheral and cerebral vegeto-vascular disorders with a non-specific functional character. Based on the available data it can be concluded that different physiological systems react independently of one another and that there are no symptoms which might serve as an indicator of pathology induced by whole-body vibration.
Nervous system, vestibular organ and hearing. Intense whole-body vibration at frequencies higher than 40 Hz can cause damage and disturbances of the central nervous system. Conflicting data have been reported on effects of whole-body vibration at frequencies below 20 Hz. In some studies only, an increase of non-specific complaints such as headache and increased irritability has been found. Disturbances of the electroencephalogram (EEG) after long-term exposure to whole-body vibration have been claimed by one author and denied by others. Some published results are consistent with a decreased vestibular excitability and a higher incidence of other vestibular disturbances, including dizziness. However, it remains doubtful whether there are causal links between whole-body vibration and changes in the central nervous system or vestibular system because paradoxical intensity-effect relationships were detected.
In some studies, an additional increase of the permanent threshold shifts (PTS) of hearing has been observed after a combined long-term exposure to whole-body vibration and noise. Schmidt (1987) studied drivers and technicians in agriculture and compared the permanent threshold shifts after 3 and 25 years on the job. He concluded that whole-body vibration can induce an additional significant threshold shift at 3, 4, 6 and 8 kHz, if the weighted acceleration according to International Standard 2631 (ISO 1985) exceeds 1.2 m/s2 r.m.s. with a simultaneous exposure to noise at an equivalent level of more than 80 decibels (dBA).
Circulatory and digestive systems. Four main groups of circulatory disturbances have been detected with a higher incidence among workers exposed to whole-body vibration:
- peripheral disorders, such as the Raynaud-syndrome, near to the site of application of whole-body vibration (i.e., the feet of standing workers or, with a low degree only, the hands of drivers)
- varicose veins of the legs, haemorrhoids and varicocele
- ischaemic heart disease and hypertension
- neurovascular changes.
The morbidity of these circulatory disturbances did not always correlate with the magnitude or duration of vibration exposure. Although a high prevalence of various disorders of the digestive system has often been observed, almost all authors agree that whole-body vibration is but one cause and possibly not the most important.
Female reproductive organs, pregnancy and male urogenital system. Increased risks of abortions, menstrual disturbances and anomalies of positions (e.g., uterine descent) have been assumed to be associated with long-term exposure to whole-body vibration (see Seidel and Heide 1986). A safe exposure limit in order to avoid a higher risk for these health risks cannot be derived from the literature. The individual susceptibility and its temporal changes probably co-determine these biological effects. In the available literature, a harmful direct effect of whole-body vibration on the human foetus has not been reported, although some animal studies suggest that whole-body vibration can affect the foetus. The unknown threshold value for adverse effects on pregnancy suggests a limitation on an occupational exposure to the lowest reasonable extent.
Divergent results have been published for the occurrence of diseases of the male urogenital system. In some studies, a higher incidence of prostatitis was observed. Other studies could not confirm these findings.
Standards
No precise limit can be offered to prevent disorders caused by whole-body vibration, but standards define useful methods of quantifying vibration severity. International Standard 2631 (ISO 1974, 1985) defined exposure limits (see figure 1) which were “set at approximately half the level considered to be the threshold of pain (or limit of voluntary tolerance) for healthy human subjects ”. Also shown in figure 1 is a vibration dose value action level for vertical vibration derived from British Standard 6841 (BSI 1987b); this standard is, in part, similar to a draft revision of the International Standard.
Figure 1. Frequency dependencies for human response to whole-body vibration
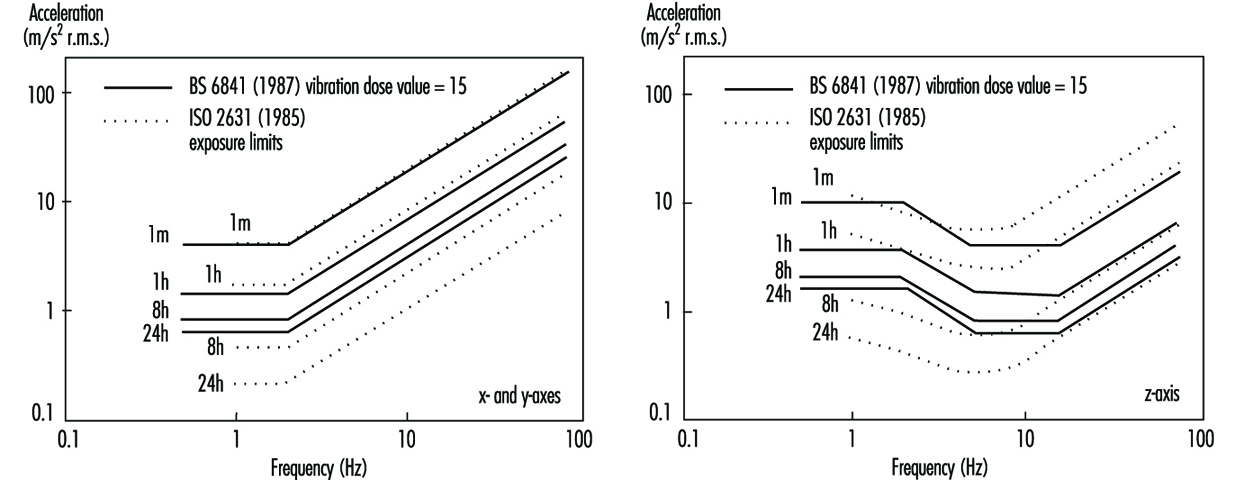
The vibration dose value can be considered to be the magnitude of a one-second duration of vibration which will be equally severe to the measured vibration. The vibration dose value uses a fourth-power time dependency to accumulate vibration severity over the exposure period from the shortest possible shock to a full day of vibration (e.g., BSI 6841):
Vibration dose value = 
The vibration dose value procedure can be used to evaluate the severity of both vibration and repetitive shocks. This fourth-power time dependency is simpler to use than the time dependency in ISO 2631 (see figure 2).
Figure 2. Time dependencies for human response to a whole-body vibration
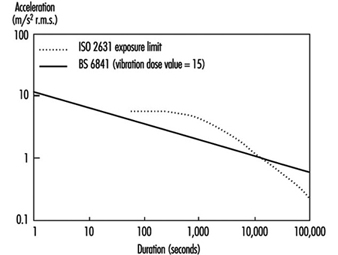
British Standard 6841 offers the following guidance.
High vibration dose values will cause severe discomfort, pain and injury. Vibration dose values also indicate, in a general way, the severity of the vibration exposures which caused them. However there is currently no consensus of opinion on the precise relation between vibration dose values and the risk of injury. It is known that vibration magnitudes and durations which produce vibration dose values in the region of 15 m/s1.75 will usually cause severe discomfort. It is reasonable to assume that increased exposure to vibration will be accompanied by increased risk of injury (BSI 1987b).
At high vibration dose values, prior consideration of the fitness of the exposed persons and the design of adequate safety precautions may be required. The need for regular checks on the health of routinely exposed persons may also be considered.
The vibration dose value provides a measure by which highly variable and complex exposures can be compared. Organizations may specify limits or action levels using the vibration dose value. For example, in some countries, a vibration dose value of 15 m/s1.75 has been used as a tentative action level, but it may be appropriate to limit vibration or repeated shock exposures to higher or lower values depending on the situation. With current understanding, an action level merely serves to indicate the approximate values that might be excessive. Figure 2 illustrates the root-mean-square accelerations corresponding to a vibration dose value of 15 m/s1.75 for exposures between one second and 24 hours. Any exposure to continuous vibration, intermittent vibration, or repeated shock may be compared with the action level by calculating the vibration dose value. It would be unwise to exceed an appropriate action level (or the exposure limit in ISO 2631) without consideration of the possible health effects of an exposure to vibration or shock.
The Machinery Safety Directive of the European Economic Community states that machinery must be designed and constructed so that hazards resulting from vibration produced by the machinery are reduced to the lowest practicable level, taking into account technical progress and the availability of means of reducing vibration. The Machinery Safety Directive (Council of the European Communities 1989) encourages the reduction of vibration by means additional to reduction at source (e.g., good seating).
Measurement and Evaluation of Exposure
Whole-body vibration should be measured at the interfaces between the body and the source of vibration. For seated persons this involves the placement of accelerometers on the seat surface beneath the ischial tuberosities of subjects. Vibration is also sometimes measured at the seat back (between the backrest and the back) and also at the feet and hands (see figure 3).
Figure 3. Axes for measuring vibration exposures of seated persons
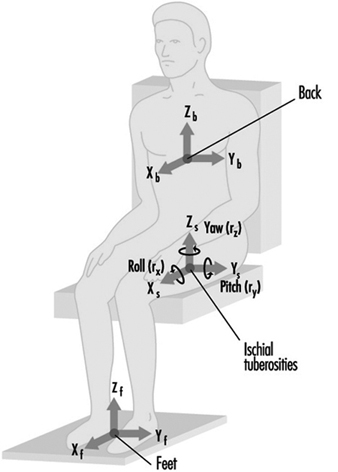
Epidemiological data alone are not sufficient to define how to evaluate whole-body vibration so as to predict the relative risks to health from the different types of vibration exposure. A consideration of epidemiological data in combination with an understanding of biodynamic responses and subjective responses is used to provide current guidance. The manner in which the health effects of oscillatory motions depend upon the frequency, direction and duration of motion is currently assumed to be the same as, or similar to, that for vibration discomfort. However, it is assumed that the total exposure, rather than the average exposure, is important, and so a dose measure is appropriate.
In addition to evaluating the measured vibration according to current standards, it is advisable to report the frequency spectra, magnitudes in different axes and other characteristics of the exposure, including the daily and lifetime exposure durations. The presence of other adverse environmental factors, especially sitting posture, should also be considered.
Prevention
Wherever possible, reduction of vibration at the source is to be preferred. This may involve reducing the undulations of the terrain or reducing the speed of travel of vehicles. Other methods of reducing the transmission of vibration to operators require an understanding of the characteristics of the vibration environment and the route for the transmission of vibration to the body. For example, the magnitude of vibration often varies with location: lower magnitudes will be experienced in some areas. Table 2 lists some preventive measures that may be considered.
Table 2. Summary of preventive measures to consider when persons are exposed to whole-body vibration
|
Group |
Action |
|
Management |
Seek technical advice |
|
|
Seek medical advice |
|
|
Warn exposed persons |
|
|
Train exposed persons |
|
|
Review exposure times |
|
|
Have policy on removal from exposure |
|
Machine manufacturers |
Measure vibration |
|
|
Design to minimize whole-body vibration |
|
|
Optimize suspension design |
|
|
Optimize seating dynamics |
|
|
Use ergonomic design to provide good posture etc. |
|
|
Provide guidance on machine maintenance |
|
|
Provide guidance on seat maintenance |
|
|
Provide warning of dangerous vibration |
|
Technical-at workplace |
Measure vibration exposure |
|
|
Provide appropriate machines |
|
|
Select seats with good attenuation |
|
|
Maintain machines |
|
|
Inform management |
|
Medical |
Pre-employment screening |
|
|
Routine medical checks |
|
|
Record all signs and reported symptoms |
|
|
Warn workers with apparent predisposition |
|
|
Advise on consequences of exposure |
|
|
Inform management |
|
Exposed persons |
Use machine properly |
|
|
Avoid unnecessary vibration exposure |
|
|
Check seat is properly adjusted |
|
|
Adopt good sitting posture |
|
|
Check condition of machine |
|
|
Inform supervisor of vibration problems |
|
|
Seek medical advice if symptoms appear |
|
|
Inform employer of relevant disorders |
Source: Adapted from Griffin 1990.
Seats can be designed to attenuate vibration. Most seats exhibit a resonance at low frequencies, which results in higher magnitudes of vertical vibration occurring on the seat than on the floor! At high frequencies there is usually attenuation of vibration. In use, the resonance frequencies of common seats are in the region of 4 Hz. The amplification at resonance is partially determined by the damping in the seat. An increase in the damping of the seat cushioning tends to reduce the amplification at resonance but increase the transmissibility at high frequencies. There are large variations in transmissibility between seats, and these result in significant differences in the vibration experienced by people.
A simple numerical indication of the isolation efficiency of a seat for a specific application is provided by the seat effective amplitude transmissibility (SEAT) (see Griffin 1990). A SEAT value greater than 100% indicates that, overall, the vibration on the seat is worse than the vibration on the floor. Values below 100% indicate that the seat has provided some useful attenuation. Seats should be designed to have the lowest SEAT value compatible with other constraints.
A separate suspension mechanism is provided beneath the seat pan in suspension seats. These seats, used in some off-road vehicles, trucks and coaches, have low resonance frequencies (around 2 Hz) and so can attenuate vibration at frequencies above about 3 Hz. The transmissibilities of these seats are usually determined by the seat manufacturer, but their isolation efficiencies vary with operating conditions.
Vibration
Vibration is oscillatory motion. This chapter summarizes human responses to whole-body vibration, hand-transmitted vibration and the causes of motion sickness.
Whole-body vibration occurs when the body is supported on a surface which is vibrating (e.g., when sitting on a seat which vibrates, standing on a vibrating floor or recumbent on a vibrating surface). Whole-body vibration occurs in all forms of transport and when working near some industrial machinery.
Hand-transmitted vibration is the vibration that enters the body through the hands. It is caused by various processes in industry, agriculture, mining and construction where vibrating tools or workpieces are grasped or pushed by the hands or fingers. Exposure to hand-transmitted vibration can lead to the development of several disorders.
Motion sickness can be caused by low frequency oscillation of the body, some types of rotation of the body and movement of displays relative to the body.
Magnitude
Oscillatory displacements of an object involve alternately a velocity in one direction and then a velocity in the opposite direction. This change of velocity means that the object is constantly accelerating, first in one direction and then in the opposite direction. The magnitude of a vibration can be quantified by its displacement, its velocity or its acceleration. For practical convenience, the acceleration is usually measured with accelerometers. The units of acceleration are metres per second per second (m/s2). The acceleration due to the Earth’s gravity is approximately 9.81 m/s2.
The magnitude of an oscillation can be expressed as the distance between the extremities reached by the motion (the peak-to-peak value) or the distance from some central point to the maximum deviation (the peak value). Often, the magnitude of vibration is expressed in terms of an average measure of the acceleration of the oscillatory motion, usually the root-mean-square value (m/s2 r.m.s.). For a single frequency (sinusoidal) motion, the r.m.s. value is the peak value divided by √2.
For a sinusoidal motion the acceleration, a (in m/s2), can be calculated from the frequency, f (in cycles per second), and the displacement, d (in metres):
a=(2πf)2d
This expression may be used to convert acceleration measurements to displacements, but it is only accurate when the motion occurs at a single frequency.
Logarithmic scales for quantifying vibration magnitudes in decibels are sometimes used. When using the reference level in International Standard 1683, the acceleration level, La, is expressed by La = 20 log10(a/a0), where a is the measured acceleration (in m/s2 r.m.s.) and a0 is the reference level of 10-6 m/s2. Other reference levels are used in some countries.
Frequency
The frequency of vibration, which is expressed in cycles per second (hertz, Hz), affects the extent to which vibration is transmitted to the body (e.g., to the surface of a seat or the handle of a vibratory tool), the extent to which it is transmitted through the body (e.g., from the seat to the head), and the effect of vibration in the body. The relation between the displacement and the acceleration of a motion are also dependent on the frequency of oscillation: a displacement of one millimetre corresponds to a very low acceleration at low frequencies but a very high acceleration at high frequencies; the vibration displacement visible to the human eye does not provide a good indication of vibration acceleration.
The effects of whole-body vibration are usually greatest at the lower end of the range, from 0.5 to 100 Hz. For hand-transmitted vibration, frequencies as high as 1,000 Hz or more may have detrimental effects. Frequencies below about 0.5 Hz can cause motion sickness.
The frequency content of vibration can be shown in spectra. For many types of whole-body and hand-transmitted vibration the spectra are complex, with some motion occurring at all frequencies. Nevertheless, there are often peaks, which show the frequencies at which most of the vibration occurs.
Since human responses to vibration vary according to the vibration frequency, it is necessary to weight the measured vibration according to how much vibration occurs at each frequency. Frequency weightings reflect the extent to which vibration causes the undesired effect at each frequency. Weightings are required for each axis of vibration. Different frequency weightings are required for whole-body vibration, hand-transmitted vibration and motion sickness.
Direction
Vibration may take place in three translational directions and three rotational directions. For seated persons, the translational axes are designated x-axis (fore-and-aft), y-axis (lateral) and
z-axis (vertical). Rotations about the x-, y- and z-axes are designated rx (roll), ry (pitch) and rz (yaw), respectively. Vibration is usually measured at the interfaces between the body and the vibration. The principal coordinate systems for measuring vibration with respect to whole-body and hand-transmitted vibration are illustrated in the next two articles in the chapter.
Duration
Human responses to vibration depend on the total duration of vibration exposure. If the characteristics of vibration do not change with time, the root-mean-square vibration provides a convenient measure of the average vibration magnitude. A stopwatch may then be sufficient to assess the exposure duration. The severity of the average magnitude and total duration can be assessed by reference to the standards in the following articles.
If the vibration characteristics vary, the measured average vibration will depend on the period over which it is measured. Furthermore, root-mean-square acceleration is believed to underestimate the severity of motions which contain shocks, or are otherwise highly intermittent.
Many occupational exposures are intermittent, vary in magnitude from moment to moment or contain occasional shocks. The severity of such complex motions can be accumulated in a manner which gives appropriate weight to, for example, short periods of high magnitude vibration and long periods of low magnitude vibration. Different methods of calculating doses are used (see “Whole-body vibration”; “Hand-transmitted vibration”; and “Motion sickness” in this chapter).
More...
Violence in the Workplace
Violence is pervasive in modern society and appears to be escalating. Entirely apart from repression, wars and terrorist activities, the media daily report in banner headlines on the mayhem inflicted by humans upon each other in “civilized” as well as more primitive communities. Whether there has been a real increase or this simply represents more thorough reporting is arguable. After all, violence has been a feature of human interaction since prehistoric ages. Nevertheless, violence has become one of the leading causes of death in modern industrial societies—in some segments of the community it is the leading cause of death—and it is increasingly being recognized as a public health problem.
Inescapably, it finds its way into the workplace. From 1980 to 1989, homicide was the third leading cause of death from injury in North American workplaces, according to data compiled by the National Traumatic Occupational Facilities Surveillance System (NIOSH 1993a). During this period, occupational homicides accounted for 12% of deaths from injury in the workplace; only motor vehicles and machines accounted for more. By 1993, that figure had risen to 17%, a rate of 0.9 per 100,000 workers, now second only to motor vehicle deaths (Toscano and Windau 1994). For women workers, it remained the leading cause of work-related death, although the rate (0.4 deaths per 100,000) was lower than that for men (1.2 deaths per 100,000) (Jenkins 1995).
These deaths, however, represent only the “tip of the iceberg”. For example, in 1992, about 22,400 American workers were injured seriously enough in non-fatal assaults in the workplace to require days away from work to recuperate (Toscano and Windau 1994). Reliable and complete data are lacking, but it is estimated that for every death there have been many thousands—perhaps, even hundreds of thousands—of instances of violence in the workplace.
In its newsletter, Unison, the large British union of health care and governmental service workers, has labelled violence as “the most threatening risk faced by members at work. It is the risk which is most likely to lead to injury. It can bring unmanageable levels of occupational stress which damages personal esteem and threatens people’s ability to continue on the job” (Unison 1992).
This article will summarize the characteristics of violence in the workplace, the kinds of people involved, its effects on them and their employers, and the steps that may be taken to prevent or control such effects.
Definition of Violence
There is no consensus on the definition of violence. For example, Rosenberg and Mercy (1991) include in the definition both fatal and nonfatal interpersonal violence where physical force or other means is used by one person with the intent of causing harm, injury or death to another. The Panel on the Understanding and Control of Violent Behavior convened by the US National Academy of Sciences adopted the definition of violence as: behaviours by individuals that intentionally threaten, attempt or inflict physical harm on others (Reiss and Roth 1993).
These definitions focus on threatening or causing physical harm. However, they exclude instances in which verbal abuse, harassment or humiliation and other forms of psychological trauma may be the sole harm to the victim and which may be no less devastating. They also exclude sexual harassment, which may be physical but which is usually entirely non-physical. In the national survey of American workers conducted by the Northwestern National Life Insurance Company, the researchers separated violent acts into: harassment (the act of creating a hostile environment through unwelcome words, actions or physical contacts not resulting in physical harm), threats (expressions of an intent to cause physical harm), and physical attacks (aggression resulting in a physical assault with or without the use of a weapon) (Lawless, 1993).
In the UK, the Health and Safety Executive’s working definition of workplace violence is: any incident in which an employee is abused, threatened or assaulted by a member of the public in circumstances arising out of the course of his or her employment. Assailants may be patients, clients or co-workers (MSF 1993).
In this article, the term violence will be used in its broadest sense to include all forms of aggressive or abusive behaviour that may cause physical or psychological harm or discomfort to its victims, whether they be intentional targets or innocent bystanders involved only impersonally or incidentally. While workplaces may be targets of terrorist attacks or may become involved in riots and mob violence, such instances will not be discussed.
Prevalence of Violence in the Workplace
Accurate information on the prevalence of violence in the workplace is lacking. Most of the literature focuses on cases that are formally reported: homicides which get tallied in the obligatory death registries, cases that get enmeshed in the criminal justice system, or cases involving time off the job that generate workers’ compensation claims. Yet, for every one of these, there is an untold number of instances in which workers are victims of aggressive, abusive behaviour. For example, according to a survey conducted by the Bureau of Justice Statistics in the US Department of Justice, over half the victimizations sustained at work were not reported to the police. About 40% of the respondents said they did not report the incident because they considered it to be a minor or a personal matter, while another 27% said they did report it to a manager or a company security officer but, apparently, the report was not relayed to the police (Bachman 1994). In addition to the lack of a consensus on a taxonomy of violence, other reasons for under-reporting include:
- Cultural acceptance of violence. There is in many communities a widespread tolerance for violence among or against certain groups (Rosenberg and Mercy 1991). Although frowned upon by many, violence is often rationalized and tolerated as a “normal” response to competition. Violence among minority and ethnic groups is often condoned as a righteous response to discrimination, poverty and lack of access to social or economic equity resulting in low self-esteem and low valuations of human life. As a result, the assault is seen as a consequence of living in a violent society rather than working in an unsafe workplace. Finally, there is the “on-the-job syndrome”, in which workers in certain jobs are expected to put up with verbal abuse, threats and, even, physical attacks (SEIU 1995; Unison 1992).
- Lack of a reporting system. Only a small proportion of organizations have articulated an explicit policy on violence or have designed procedures for reporting and investigating instances of alleged violence in the workplace. Even where such a system has been installed, the trouble of obtaining, completing and filing the required report form is a deterrent to reporting all but the most outrageous incidents.
- Fear of blame or reprisal. Workers may fear being held responsible when they have been attacked by a client or a patient. Fear of reprisal by the assailant is also a potent deterrent to reporting, especially when that person is the worker’s superior and in a position to affect his or her job status.
- Lack of interest on the part of the employer. The employer’s lack of interest in investigating and reacting to prior incidents will certainly discourage reporting. Also, supervisors, concerned that workplace violence might reflect unfavourably on their managerial capabilities may actually discourage or even block the filing of reports by workers in their units.
To determine the prevalence of violence in the workplace in the absence of reliable data, attempts have been made to extrapolate both from available statistics (e.g., death certificates, crime reports and workers’ compensation systems) and from specially designed surveys. Thus, the US National Crime Victimization Survey estimated that about 1 million American workers (out of a workforce of 110 million) are assaulted at work each year (Bachman 1994). And, a 1993 telephone survey of a national sample of 600 American full-time workers (excluding self-employed and military personnel) found that one in four said that he or she had been a victim of workplace violence during the study year: 19%ere harassed, 7% were threatened, and 3% were attacked physically. The researchers reported further that 68%of the harassment victims, 43% of the threat victims and 24% of the attack victims had not reported the incident (Lawless 1993).
A similar survey of workers in the UK employed by the National Health Service revealed that, during the previous year, 0.5% had required medical treatment following an on-the-job physical assault; 11% had suffered a minor injury requiring only first aid, 4 to 6% had been threatened by persons wielding a deadly weapon, and 17% had received verbal threats. Violence was a special problem for emergency staff in ambulances and accident departments, nurses, and workers involved in the care of psychologically disturbed patients (Health Services Advisory Committee 1987). The risk of health workers being confronted by violence has been labelled a feature of everyday work in primary care and in accident/emergency departments (Shepherd 1994).
Homicide in the Workplace
Although workplace homicides are only a small proportion of all homicides, their substantial contribution to work-related deaths, at least in the United States, their unique features, and the possibility of preventive interventions by employers earn them special attention. For example, while most homicides in the community involve people who know each other, many of them close relatives, and only 13% were reported to have been associated with another felony, these proportions were reversed in the workplace, where more than three-fourths of the homicides were committed in the course of a robbery (NIOSH 1992). Further, while persons aged 65 and older in the general population have the lowest rates of being victims of homicide, this age group has the highest rates of such involvement in workplace homicides (Castillo and Jenkins 1994).
American workplaces with the highest rates of homicide are listed in table 1. Over 50% are accounted for by only two industries: retail trade and services. The latter includes taxi driving, which has nearly 40 times the average workplace homicide rate, followed by liquor/convenience stores and gas stations, prime targets for robberies, and by detective/protective services (Castillo and Jenkins 1994).
Table 1. US workplaces with the highest rates of occupational homicide, 1980-1989
|
Workplaces |
No. of homicides |
Rate1 |
|
Taxicab establishments |
287 |
26.9 |
|
Liquor stores |
115 |
8.0 |
|
Gas stations |
304 |
5.6 |
|
Detective/protective services |
152 |
5.0 |
|
Justice/public order establishments |
640 |
3.4 |
|
Grocery stores |
806 |
3.2 |
|
Jewellery stores |
56 |
3.2 |
|
Hotels/motels |
153 |
3.2 |
|
Eating/drinking places |
754 |
1.5 |
1 Number per 100,000 workers per year.
Source: NIOSH 1993b.
Table 2 lists the occupations with the highest rates of workplace homicides. Again, reflecting the likelihood of involvement in attempted felonies, taxi drivers head the list, followed by law-enforcement personnel, hotel clerks and workers in various types of retail establishments. Commenting on similar data from the UK, Drever (1995) noted that most of the occupations with the highest mortality from homicides had high rates of drug dependence (scaffolders, literary and artistic occupations, painters and decorators) or alcohol abuse (cooks and kitchen porters, publicans, bartenders and caterers).
Table 2. US occupations with the highest rates of occupational homicide, 1980-1989
|
Occupations |
No. of homicides |
Rate1 |
|
Taxicab drivers/chauffeurs |
289 |
15.1 |
|
Law enforcement officers |
520 |
9.3 |
|
Hotel clerks |
40 |
5.1 |
|
Gas station workers |
164 |
4.5 |
|
Security guards |
253 |
3.6 |
|
Stock handlers/baggers |
260 |
3.1 |
|
Store owners/managers |
1,065 |
2.8 |
|
Bartenders |
84 |
2.1 |
1 Number per 100,000 workers per year.
Source: NIOSH 1993b.
As noted above, the vast majority of work-related homicides occur during the course of a robbery or other crime committed by a person or persons usually not known to the victim. Risk factors associated with such incidents are listed in table 3.
Table 3. Risk factors for workplace homicides
Working alone or in small numbers
Exchange of money with the public
Working late night or early morning hours
Working in high crime areas
Guarding valuable property or possessions
Working in community settings (e.g. taxi drivers and police)
Source: NIOSH 1993b.
About 4% of workplace homicides occur during confrontations with family members or acquaintances who have followed the victim into the workplace. About 21% arise out of a confrontation related to the workplace: about two-thirds of these are perpetrated by workers or former employees with a grudge against a manager or a co-worker, while angry customers or clients account for the rest (Toscano and Windau 1994). In these cases, the target may be the particular manager or worker whose actions provoked the assault or, where there is a grudge against the organization, the target may be the workplace itself, and any employees and visitors who just happen to be in it at the critical moment. Sometimes, the assailant may be emotionally disturbed, as in the case of Joseph T. Weisbecker, an employee on long-term disability leave from his employer in Louisville, Kentucky, because of mental illness, who killed eight co-workers and injured 12 others before taking his own life (Kuzmits 1990).
Causes of Violence
Current understanding of the causes and risk factors for assaultive violence is very rudimentary (Rosenberg and Mercy 1991). Clearly, it is a multifactorial problem in which each incident is shaped by the characteristics of the assailant, the characteristics of the victim(s) and the nature of the interplay between them. Reflecting such complexity, a number of theories of causation have been developed. Biological theories, for example, focus on such factors as gender (most of the assailants are male), age (involvement in violence in the community diminishes with age but, as noted above, this is not so in the workplace), and the influence of hormones such as testosterone, neurotransmitters such as serotonin, and other such biological agents. The psychological approach focuses on personality, holding that violence is engendered by deprivation of love during childhood, and childhood abuse, and is learned from role models, reinforced by rewards and punishments in early life. Sociological theories emphasize as breeders of violence such cultural and subcultural factors as poverty, discrimination and lack of economic and social equity. Finally, interactional theories converge on a sequence of actions and reactions that ultimately escalate into violence (Rosenberg and Mercy 1991).
A number of risk factors have been associated with violence. They include:
Mental illness
The vast majority of people who are violent are not mentally ill, and the vast proportion of individuals with mental illness are not violent (American Psychiatric Association 1994). However, mentally disordered individuals are sometimes frightened, irritable, suspicious, excitable, or angry, or a combination of these (Bullard 1994). The resultant behaviour poses a particular risk of violence to the physicians, nurses and staff members involved in their care in ambulances, emergency departments and both inpatient and outpatient psychiatric facilities.
Certain types of mental illness are associated with a greater propensity for violence. Persons with psychopathic personalities tend to have a low threshold for anger and frustration, which often generate violent behaviour (Marks 1992), while individuals with paranoia are suspicious and prone to attack individuals or entire organizations whom they blame when things do not go as they would wish. However, violence may be exhibited by persons with other forms of mental illness. Furthermore, some mentally ill individuals are prone to episodes of acute dementia in which they may inflict violence on themselves as well as on those trying to restrain them.
Alcohol and drug abuse
Alcohol abuse has a strong association with aggressive and violent behaviour. While drunkenness on the part of either assailants or victims, or both, often results in violence, there is disagreement as to whether alcohol is the cause of the violence or merely one of a number of factors involved in its causation (Pernanen 1993). Fagan (1993) emphasized that while alcohol affects neurobiological functions, perception and cognition, it is the immediate setting in which the drinking takes place that channels the disinhibiting responses to alcohol. This was confirmed by a study in Los Angeles County which found that violent incidents were much more frequent in some bars and relatively uncommon in others where just as much drinking was taking place, and concluded that violent behaviour was not related to the amount of alcohol being consumed but, rather, to the kinds of individuals attracted to a particular drinking establishment and the kinds of unwritten rules in effect there (Scribner, MacKinnon and Dwyer 1995).
Much the same may be said for abuse of illicit drugs. Except perhaps for crack cocaine and the amphetamines, drug use is more likely to be associated with sedation and withdrawal rather than aggressive, violent behaviour. Most of the violence associated with illegal drugs seems to be associated not with the drugs, but with the effort to obtain them or the wherewithal to purchase them, and from involvement in the illegal drug traffic.
Violence in the community
Violence in the community not only spills over into workplaces but is a particular risk factor for workers such as police and firefighters, and for postal workers and other government employees, repair and service personnel, social workers and others whose jobs take them into neighbourhoods in which violence and crime are indigenous. Important factors in the frequency of violence, particularly in the United States, is the prevalence of firearms in the hands of the general public and, especially for young people, the amount of violence depicted in films and on television.
Work-Related Factors Associated with Violence
Instances of violence may occur in any and all workplaces. There are, however, certain jobs and work-related circumstances that are particularly associated with a risk of generating or being subjected to violence. They include:
Criminal activities
Perhaps the least complex of episodes of work-related violence are those associated with criminal violence, the major cause of worksite homicides. These fall into two categories: those involved with attempts at robbery or other felonies, and those related to traffic in illicit drugs. Police, security guards and other personnel with law-enforcement responsibilities face a constant risk of attack by felons attempting to enter the workplace and those resisting detection and arrest. Those working alone and field workers whose duties take them into high-crime neighbourhoods are frequent targets of robbery attempts. Health professionals making home visits to such areas are particularly at risk because they often carry drugs and drug paraphernalia such as hypodermic syringes and needles.
Dealing with the public
Workers in government and private community service agencies, banks and other institutions serving the public are frequently confronted by attacks from individuals who have been kept waiting unduly, have been greeted with disinterest and indifference (whether real or perceived), or were thwarted in obtaining the information or services they desired because of complicated bureaucratic procedures or technicalities that made them ineligible. Clerks in retail establishments receiving items being returned, workers staffing airport ticket counters when flights are overbooked, delayed or cancelled, urban bus or trolley drivers and conductors, and others who must deal with customers or clients whose wants cannot immediately be satisfied are often targets for verbal and sometimes even physical abuse. Then, there are also those who must contend with impatient and unruly crowds, such as police officers, security guards, ticket takers and ushers at popular sporting and entertainment events.
Violent attacks on government workers, particularly those in uniform, and on government buildings and offices in which workers and visitors may be indiscriminately injured or killed, may result from resentment and anger at laws and official policies which the perpetrators will not accept.
Work stress
High levels of work stress may precipitate violent behaviour, while violence in the workplace can, in turn, be a potent stressor. The elements of work stress are well known (see chapter Psychosocial and Organizational Factors). Their common denominator is a devaluation of the individual and/or the work he or she performs, resulting in fatigue, frustration and anger directed at managers and co-workers perceived to be inconsiderate, unfair and abusive. Several recent population studies have demonstrated an association between violence and job loss, one of the most potent job-related stressors (Catalano et al. 1993; Yancey et al. 1994).
Interpersonal environment in the workplace
The interpersonal environment in the workplace may be a breeding ground for violence. Discrimination and harassment, forms of violence in themselves as defined in this article, may provoke violent retaliation. For example, MSF, the British union of workers in management, science and finance, calls attention to workplace bullying (defined as persistent offensive, abusive, intimidating, malicious or insulting behaviour, abuse of power or unfair penal sanctions), as a characteristic of the management style in some organizations (MSF 1995).
Sexual harassment has been branded a form of assault on the job (SEIU 1995). It may involve unwelcome touching or patting, physical assault, suggestive remarks or other verbal abuse, staring or leering, requests for sexual favours, compromising invitations, or a work environment made offensive by pornography. It is illegal in the United States, having been declared a form of sexual discrimination under Title VII of the Civil Rights Act of 1964 when the worker feels that his or her job status depends on tolerating the advances or if the harassment creates an intimidating, hostile or offensive workplace environment.
Although women are the usual targets, men have also been sexually harassed, albeit much less frequently. In a 1980 survey of US federal employees, 42% of female respondents and 15% of males said that they had been sexually harassed on the job, and a follow-up survey in 1987 yielded similar results (SEIU 1995). In the United States, extensive media coverage of the harassment of women who had “intruded” into jobs and workplaces traditionally filled by males, and the notoriety given to the involvement of prominent political and public figures in alleged harassment, have resulted in an increase in the number of complaints received by state and federal anti-discrimination agencies and the number of civil law suits filed.
Working in health care and social services
In addition to the attempted robberies as noted above, health care staff are often targets of violence from anxious and disturbed patients, especially in emergency and outpatient departments, where long waits and impersonal procedures are not uncommon and where anxiety and anger may boil over into verbal or physical assaults. They may also be victims of assault by family members or friends of patients who had unfavourable outcomes which they rightly or wrongfully attribute to denials, delays or errors in treatment. In such instances they may attack the particular health worker(s) whom they hold responsible, or the violence may be aimed randomly at any staff member(s) of the medical facility.
Effects of Violence on the Victim
The trauma caused by physical assault varies with the nature of the attack and the weapons employed. Bruises and cuts on the hands and forearms are common when the victim has tried to defend himself or herself. Since the face and head are frequent targets, bruises and fractures of the facial bones are common; these can be traumatic psychologically because the swelling and ecchymoses are so visible and may take weeks to disappear (Mezey and Shepherd 1994).
The psychological effects may be more troublesome than the physical trauma, especially when a health worker has been assaulted by a patient. The victims may experience a loss of composure and self-confidence in their professional competence accompanied by a sense of guilt at having provoked the attack or having failed to detect that it was coming. Unfocused or directed anger may persist at the apparent rejection of their well-intended professional efforts, and there may be a persistent loss of confidence in themselves as well as a lack of trust in their co-workers and supervisors that can interfere with work performance. All this may be accompanied by insomnia, nightmares, diminished or increased appetite, increased consumption of tobacco, alcohol and/or drugs, social withdrawal and absenteeism from the job (Mezey and Shepherd 1994).
Post-traumatic stress disorder is a specific psychological syndrome (PTSD) that may develop after major disasters and instances of violent assault, not only in those directly involved in the incident but also in those who have witnessed it. While usually associated with life-threatening or fatal incidents, PTSD may occur after relatively trivial attacks that are perceived as life-threatening (Foa and Rothbaum 1992). The symptoms include: re-experiencing the incident through recurrent and intrusive recollections (“flashbacks”) and nightmares, persistent feelings of arousal and anxiety including muscular tension, autonomic hyperactivity, loss of concentration, and exaggerated reactivity. There is often conscious or unconscious avoidance of circumstances that recall the incident. There may be a long period of disability but the symptoms usually respond to supportive psychotherapy. They can often be prevented by a post-incident debriefing conducted as soon as possible after the incident, followed, when needed, by short-term counselling (Foa and Rothbaum 1992).
After the Incident
Interventive measures to be taken immediately after the incident include:
Care of the victim
Appropriate first-aid and medical care should be provided as quickly as possible to all injured individuals. For possible medico-legal purposes (e.g., criminal or civil actions against the assailant) the injuries should be described in detail and, if possible, photographed.
Clean-up of the workplace
Any damage or debris in the workplace should be cleaned up, and any equipment that was involved should be checked to make sure that the safety and cleanliness of the workplace have been fully restored (SEIU 1995).
Post-incident debriefing
As soon as possible, all those involved in or witnessing the incident should participate in a post-incident debriefing or a “trauma-crisis counselling” session conducted by an appropriately qualified staff member or an outside consultant. This will not only provide emotional support and identify those for whom referral for one-on-one counselling may be advisable, but also enable the collection of details of exactly what has happened. Where necessary, the counselling may be supplemented by the formation of a peer support group (CAL/OSHA 1995).
Reporting
A standardized report form should be completed and submitted to the proper individual in the organization and, when appropriate, to the police in the community. A number of sample forms that may be adapted to the needs of a particular organization have been designed and published (Unison 1991, MSF 1993, SEIU 1995). Aggregating and analysing incident report forms will provide epidemiological information that may identify risk factors for violence in the particular workplace and point the way to suitable preventive interventions.
Investigating the incident
Each reported incident of alleged violence, however trivial it may seem, should be investigated by a designated properly trained individual. (Assignment for such investigations may be made by the joint labour/management safety and health committee, where one exists.) The investigation should be aimed at identifying the cause(s) of the incident, the person(s) involved, what, if any, disciplinary measures should be invoked, and what may be done to prevent recurrences. Failure to conduct an impartial and effective investigation is a signal of management’s disinterest and a lack of concern for employees’ health and welfare.
Employer support
Victims and observers of the incident should be assured that they will not be subject to discrimination or any other form of reprisal for reporting it. This is especially important when the alleged assailant is the worker’s superior.
Depending on the regulations extant in the particular jurisdiction, the nature and extent of any injuries, and the duration of any absence from work, the employee may be eligible for workers’ compensation benefits. In such cases, the appropriate claim forms should be filed promptly.
When appropriate, a report should be filed with the local law enforcement agency. When needed, the victim may be provided with legal advice on pressing charges against the assailant, and assistance in dealing with the media.
Union Involvement
A number of unions have been playing a prominent role in dealing with workplace violence, most notably those representing workers in the health care and service industries, such as the Service Employees International Union (SEIU) in the United States, and Management, Science and Finance (MSF) and Unison in the UK. Through the development of guidelines and the publication of fact sheets, bulletins and pamphlets, they have focused on the education of workers, their representatives and their employers about the importance of violence in the workplace, how to deal with it, and how to prevent it. They have acted as advocates for members who have been victims to ensure that their complaints and allegations of violence are given appropriate consideration without threats of reprisal, and that they receive all of the benefits to which they may be entitled. Unions also advocate with employers’ and trade associations and government agencies on behalf of policies, rules and regulations intended to reduce the prevalence of violence in the workplace.
Threats of Violence
All threats of violence should be taken seriously, whether aimed at particular individuals or at the organization as a whole. First, steps must be taken to protect the targeted individual(s). Then, where possible, the assailant should be identified. If that person is not in the workforce, the local law enforcement agencies should be notified. If he or she is in the organization, it may be desirable to consult a qualified mental health professional to guide the handling of the situation and/or deal directly with the assailant.
Preventive Strategies
Preventing violence in the workplace is fundamentally the employer’s responsibility. Ideally, a formal policy and programme will have been developed and implemented before victimization occurs. This is a process that should involve not only the appropriate individuals in human resources/personnel, security, legal affairs, and employee health and safety departments, but also line managers and shop stewards or other employee representatives. A number of guides for such an exercise have been published (see table 4). They are generic and are intended to be tailored to the circumstances of a particular workplace or industry. Their common denominators include:
Table 4. Guides for programmes to prevent workplace violence
|
Date |
Title |
Source |
|
1991 |
Violence in the Workplace: |
Unison Health Care |
|
1993 |
CAL/OSHA Guidelines for Security |
Division of Occupational Safety and Health |
|
1993 |
Prevention of Violence at Work: |
MSF Health and Safety Office |
|
1995 |
Assault on the Job: We Can Do |
Service Employees International Union |
|
1995 |
CAL/OSHA: Model Injury and |
Division of Occupational Safety and Health |
|
1996 |
Guidelines for Preventing Work- |
OSHA Publications Office |
Establishing a policy
A policy explicitly outlawing discriminatory and abusive behaviour and the use of violence for dispute resolution, accompanied by specified disciplinary measures for infractions (up to and including dismissal), should be formulated and published.
Risk assessment
An inspection of the workplace, supplemented by analysis of prior incidents and/or information from employee surveys, will enable an expert to assess risk factors for violence and suggest preventive interventions. Examination of the prevailing style of management and supervision and the organization of work may disclose high levels of work stress that may precipitate violence. Study of interactions with clients, customers or patients may reveal features that may generate needless anxiety, frustration and anger, and precipitate violent reactions.
Workplace modifications to reduce crime
Guidance from police or private security experts may suggest changes in work procedures and in the layout and furnishing of the workplace that will make it a less attractive target for robbery attempts. In the United States, the Virginia Department of Criminal Justice has been using Crime Prevention Through Environmental Design (CPTED), a model approach developed by a consortium of the schools of architecture in the state that includes: changes in interior and exterior lighting and landscaping with particular attention to parking areas, stairwells and restrooms; making sales and waiting areas visible from the street; use of drop safes or time-release safes to hold cash; alarm systems, television monitors and other security equipment (Malcan 1993). CPTED has been successfully applied in convenience stores, banks (particularly in relation to automatic teller machines which may be accessed around the clock), schools and universities, and in the Washington, DC, Metro subway system.
In New York City, where robbery and killing of taxi drivers is relatively frequent compared to other large cities, the Taxi and Limousine Commission issued regulations that mandated the insertion of a transparent, bullet-resistant partition between the driver and passengers in the rear seat, a bullet-proof plate in the back of the driver’s seat, and an external distress signal light that could be turned on by the driver while remaining invisible to those inside the cab (NYC/TLC 1994). (There has been a spate of head and facial injuries among rear seat passengers who were not wearing seat belts and were thrown forward against the partition when the cab stopped suddenly.)
Where work involves interaction with customers or patients, employee safety may be enhanced by interposing barriers such as counters, desks or tables, transparent, shatter-proof partitions, and locked doors with shatter-proof windows (CAL/OSHA 1993). Furniture and equipment can be arranged to avoid entrapment of the employee and, where privacy is important, it should not be maintained at the expense of isolating the employee with a potentially aggressive or violent individual in a closed or secluded area.
Security systems
Every workplace should have a well-designed security system. Intrusion of strangers may be reduced by limiting entry to a designated reception area where visitors may have an identity check and receive ID badges indicating the areas to be visited. In some situations, it may be advisable to use metal detectors to identify visitors carrying concealed weapons.
Electronic alarm systems triggered by strategically located “panic buttons” can provide audible and/or visual signals that can alert co-workers to danger and summon help from a nearby security station. Such alarm systems may also be rigged to summon local police. However, they are of little use if guards and co-workers have not been trained to respond promptly and properly. Television monitors can not only provide protective surveillance but also record any incidents as they occur, and may help identify the perpetrator. Needless to say, such electronic systems are of little use unless they are maintained properly and tested at frequent intervals to ensure that they are in working order.
Two-way radios and cellular telephones can provide a measure of security for field personnel and those who are working alone. They also provide a means of reporting their location and, when necessary, summoning medical and other forms of assistance.
Work practice controls
Work practices should be reviewed periodically and modified to minimize the build-up of work stress. This involves attention to work schedules, work load, job content, and monitoring of work performance. Adequate staffing levels should be maintained in high-risk work areas both to discourage violent behaviour and to deal with it when it occurs. Adjustment of staffing levels to cope with peak flows of clients or patients will help to minimize irritating delays and crowding of work areas.
Staff training
Workers and supervisors should be trained to recognize rising tension and anger and in non-violent methods of defusing them. Training involving role-playing exercises will help employees to cope with overly aggressive or abusive individuals without being confrontational. In some situations, training employees in self-defence may be indicated, but there is the danger that this will breed a level of self-confidence that will lead them to delay or entirely neglect calling for available help.
Security guards, staff in psychiatric or penal institutions, and others likely to be involved with physically violent individuals should be trained to subdue and restrain them with minimal risk of injury to others or to themselves (SEIU 1995). However, according to Unison (1991), training can never be a substitute for good work organization and the provision of adequate security.
Employee assistance programmes
Employee assistance programmes (EAPs—also known as member assistance programmes, or MAPs, when provided by a union) can be particularly helpful in crisis situations by providing counselling and support to victims and witnesses of violent incidents, referring them to outside mental health professionals when needed, monitoring their progress and overseeing any protective arrangements intended to facilitate their return to work.
EAPs can also counsel employees whose frustration and anger might culminate in violent behaviour because they are overburdened by work-related problems or those arising from life in the family and/or in the community, whose frustration and anger might culminate in violent behaviour. When they have several such clients from a particular area of the workplace, they can (without breaching the confidentiality of personal information essential to their operation) guide managers to making desirable work modifications that will defuse the potential “powder keg” before violence erupts.
Research
Because of the seriousness and complexity of the problem and the paucity of reliable information, research is needed in the epidemiology, causation, prevention and control of violence in society in general and in the workplace. This requires a multidisciplinary effort involving (in addition to experts in occupational safety and health), mental health professionals, social workers, architects and engineers, experts in management science, lawyers, judges and experts in the criminal justice system, authorities on public policy, and others. Urgently needed are expanded and improved systems for the collection and analysis of the relevant data and the development of a consensus on a taxonomy of violence so that information and ideas can be more easily transposed from one discipline to others.
Conclusion
Violence is endemic in the workplace. Homicides are a major cause of work-related deaths, but their impact and cost are considerably outweighed by the prevalence of near misses, non-fatal physical assaults, threats, harassment, aggressive behaviour and abuse, much of which remains undocumented and unreported. Although most of the homicides and many of the assaults occur in conjunction with criminal activities, workplace violence is not just a criminal justice problem. Nor is it solely a problem for mental health professionals and specialists in addictions, although much of it is associated with mental illness, alcoholism and drug abuse. It requires a coordinated effort by experts in a broad variety of disciplines, led by occupational health and safety professionals, and aimed at developing, validating and implementing a coherent set of strategies for intervention and prevention, keeping in mind that the diversity in workers, jobs and industries dictates an ability to tailor them to the unique characteristics of a particular workforce and the organization that employs it.
Ergonomics Standards
Introduction
Ergonomics standards can take many forms, such as regulations which are promulgated on a national level, or guidelines and standards instituted by international organizations. They play an important role in improving the usability of systems. Design and performance standards give managers confidence that the systems they buy will be capable of being used productively, efficiently, safely and comfortably. They also provide users with a benchmark by which to judge their own working conditions. In this article we focus on the International Organization for Standardization (ISO) ergonomics standard 9241 (ISO 1992) because it provides important, internationally recognized, criteria for selecting or designing VDU equipment and systems. ISO carries out its work through a series of technical committees, one of which is ISO TC 159 SC4 Ergonomics of Human System Interaction Committee, which is responsible for ergonomics standards for situations in which human beings and technological systems interact. Its members are representatives of the national standards bodies of member countries and meetings involve national delegations in discussing and voting on resolutions and technical documents. The primary technical work of the committee takes place in eight Working Groups (WGs), each of which has responsibility for different work items listed in figure 1. This sub-committee has developed ISO 9241.
Figure 1. Technical Working Groups of the Ergonomics of Human System Interaction Technical Committee (ISO TC 159 SC4). ISO 9241: Five working groups broke down the “parts” of the standard to those listed below. This illustration shows the correspondence between the parts of the standard and the various aspects of the workstation with which they are concerned
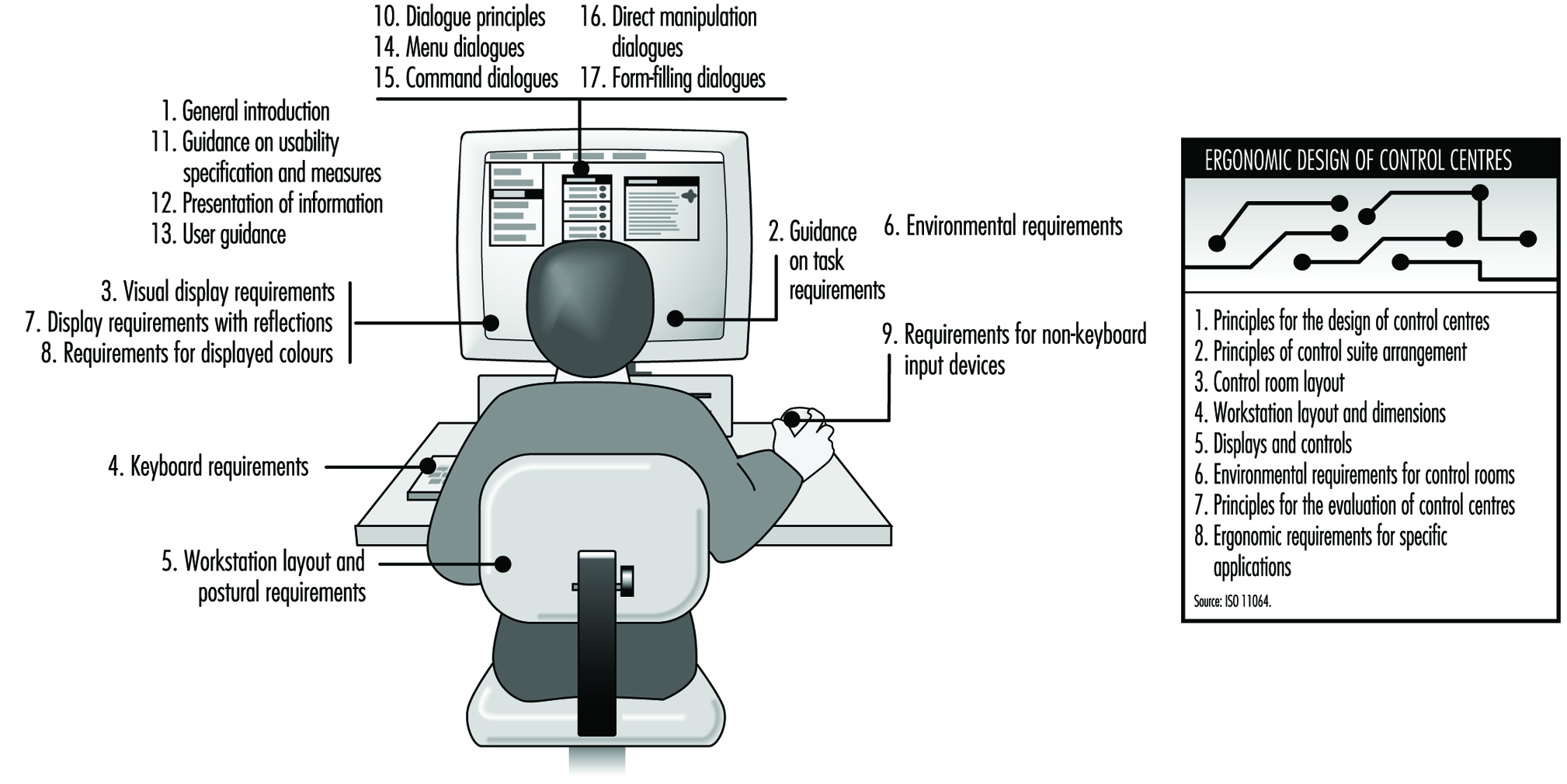 The work of the ISO has major international importance. Leading manufacturers pay great heed to ISO specifications. Most producers of VDUs are international corporations. It is obvious that the best and most effective solutions to workplace design problems from the international manufacturers’ point of view should be agreed upon internationally. Many regional authorities, such as the European Standardization Organization (CEN) have adopted ISO standards wherever appropriate. The Vienna Agreement, signed by the ISO and CEN, is the official instrument which ensures effective collaboration between the two organizations. As different parts of ISO 9241 are approved and published as international standards, they are adopted as European standards and become part of EN 29241. Since CEN standards replace national standards in the European Union (EU) and the European Free Trade Agreement (EFTA) Member States, the significance of ISO standards in Europe has grown, and, in turn, has also increased pressure on the ISO to efficiently produce standards and guidelines for VDUs.
The work of the ISO has major international importance. Leading manufacturers pay great heed to ISO specifications. Most producers of VDUs are international corporations. It is obvious that the best and most effective solutions to workplace design problems from the international manufacturers’ point of view should be agreed upon internationally. Many regional authorities, such as the European Standardization Organization (CEN) have adopted ISO standards wherever appropriate. The Vienna Agreement, signed by the ISO and CEN, is the official instrument which ensures effective collaboration between the two organizations. As different parts of ISO 9241 are approved and published as international standards, they are adopted as European standards and become part of EN 29241. Since CEN standards replace national standards in the European Union (EU) and the European Free Trade Agreement (EFTA) Member States, the significance of ISO standards in Europe has grown, and, in turn, has also increased pressure on the ISO to efficiently produce standards and guidelines for VDUs.
User performance standards
An alternative to product standards is to develop user performance standards. Thus, rather than specify a product feature such as character height which it is believed will result in a legible display, standards makers develop procedures for testing directly such characteristics as legibility. The standard is then stated in terms of the user performance required from the equipment and not in terms of how that is achieved. The performance measure is a composite including speed and accuracy and the avoidance of discomfort.
User performance standards have a number of advantages; they are
- relevant to the real problems experienced by users
- tolerant of developments in the technology
- flexible enough to cope with interactions between factors.
However, user performance standards can also suffer a number of disadvantages. They cannot be totally complete and scientifically valid in all cases, but do represent reasonable compromises, which require significant time to obtain the agreement of all the parties involved in standards-setting.
Coverage and Use of ISO 9241
The VDU ergonomics requirements standard, ISO 9241, provides detail on ergonomic aspects of products, and on assessing the ergonomic properties of a system. All references to ISO 9241 also apply to EN 29241. Some parts provide general guidance to be considered in the design of equipment, software and tasks. Other parts include more specific design guidance and requirements relevant to current technology, since such guidance is useful to designers. In addition to product specifications, ISO 9241 emphasizes the need to specify factors affecting user performance, including how to assess user performance in order to judge whether or not a system is appropriate to the context in which it will be used.
ISO 9241 has been developed with office-based tasks and environments in mind. This means that in other specialized environments some acceptable deviation from the standard may be needed. In many cases, this adaptation of the office standard will achieve a more satisfactory result than the “blind” specification or testing of an isolated standard specific to a given situation. Indeed, one of the problems with VDU ergonomics standards is that the technology is developing faster than standards makers can work. Thus it is quite possible that a new device may fail to meet the strict requirements in an existing standard because it approaches the need in question in a way radically different from any that were foreseen when the original standard was written. For example, early standards for character quality on a display assumed a simple dot matrix construction. Newer more legible fonts would have failed to meet the original requirement because they would not have the specified number of dots separating them, a notion inconsistent with their design.
Unless standards are specified in terms of the performance to be achieved, the users of ergonomics standards must allow suppliers to meet the requirement by demonstrating that their solution provides equivalent or superior performance to achieve the same objective.
The use of the ISO 9241 standard in the specification and procurement process places display screen ergonomics issues firmly on management’s agenda and helps to ensure proper consideration of these issues by both procurer and supplier. The standard is therefore a useful part of the responsible employer’s strategy for protecting the health, safety and productivity of display screen users.
General issues
ISO 9241 Part 1 General introduction explains the principles underlying the multipart standard. It describes the user performance approach and provides guidance on how to use the standard and on how conformance to parts of ISO 9241 should be reported.
ISO 9241 Part 2 Guidance on task requirements provides guidance on job and task design for those responsible for planning VDU work in order to enhance the efficiency and the well-being of individual users by applying practical ergonomic knowledge to the design of office VDU tasks. Objectives and characteristics of task design are also discussed (see figure 2) and the standard describes how task requirements may be identified and specified within individual organizations and can be incorporated into the organization’s system design and implementation process.
Figure 2. Guidance and task requirements
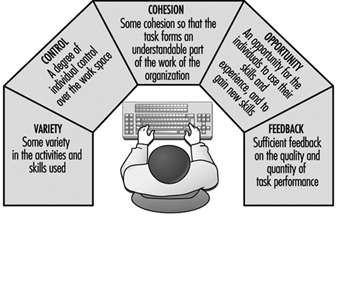
Case Study: Display Screen Equipment Directive (90/270/EEC)
The Display Screen Directive is one in a series of “daughter”directives dealing with specific aspects of health and safety. The directives form part of the European Union’s programme for promoting health and safety in the single market. The “parent” or “Framework” Directive (89/391/EEC) sets out the general principles of the Community’s approach to Health and Safety. These common principles include the avoidance of risk, where possible, by eliminating the source of the risk and the encouragement of collective protective measures instead of individual protective measures.
Where risk is unavoidable, it must be properly evaluated by people with the relevant skills and measures must be taken which are appropriate to the extent of the risk. Thus if the assessment shows that the level of risk is slight, informal measures may be entirely adequate. However, where significant risk is identified, then stringent measures must be taken. The Directive itself only placed obligations on Member States of the EU, not on individual employers or manufacturers. The Directive required Member States to transpose the obligations into appropriate national laws, regulations and administrative provisions. These in turn place obligations on employers to ensure a minimum level of health and safety for display screen users. The main obligations are for employers to: The intention behind the Display Screen Directive is to specify how workstations should be used rather than how products should be designed. The obligations therefore fall on employers, not on manufacturers of workstations. However, many employers will ask their suppliers to reassure them that their products “conform”. In practice, this means little since there are only a few, relatively simple design requirements in the Directive. These are contained in the Annex (not given here) and concern the size and reflectance of the work surface,the adjustability of the chair, the separation of the keyboard and the clarity of the displayed image.
Hardware and environmental ergonomics issues
Display screen
ISO 9241 (EN 29241) Part 3 Visual display requirements specifies the ergonomic requirements for display screens which ensure that they can be read comfortably, safely and efficiently to perform office tasks. Although it deals specifically with displays used in offices, the guidance is appropriate to specify for most applications which require general purpose displays. A user performance test which, once approved, can serve as the basis for performance testing and will become an alternate route to compliance for VDUs.
ISO 9241 Part 7 Display requirements with reflections. The purpose of this part is to specify methods of measurement of glare and reflections from the surface of display screens, including those with surface treatments. It is aimed at display manufacturers who wish to ensure that anti-reflection treatments do not detract from image quality.
ISO 9241 Part 8 Requirements for displayed colours. The purpose of this part is to deal with the requirements for multicolour displays which are largely in addition to the monochrome requirements in Part 3, requirements for visual display in general.
Keyboard and other input devices
ISO 9241 Part 4 Keyboard requirements requires that the keyboard should be tiltable, separate from the display and easy to use without causing fatigue in the arms or hands. This standard also specifies the ergonomic design characteristics of an alphanumeric keyboard which may be used comfortably, safely and efficiently to perform office tasks. Again, although Part 4 is a standard to be used for office tasks, it is appropriate to most applications which require general purpose alphanumeric keyboards. Design specifications and an alternative performance test method of compliance are included.
ISO 9241 Part 9 Requirements for non-keyboard input devices specifies the ergonomic requirements from such devices as the mouse and other pointing devices which may be used in conjunction with a visual display unit. It also includes a performance test.
Workstations
ISO 9241 Part 5 Workstation layout and postural requirements facilitates efficient operation of the VDU and encourages the user to adopt a comfortable and healthy working posture. The requirements for a healthy, comfortable posture are discussed. These include:
- the location of frequently used equipment controls, displays and work surfaces within easy reach
- the opportunity to change position frequently
- the avoidance of excessive, frequent and repetitive movements with extreme extension or rotation of the limbs or trunk
- support for the back allowing an angle of 90 degrees to 110 degrees between back and thighs.
The characteristics of the workplace which promote a healthy and comfortable posture are identified and design guidelines given.
Working environments
ISO 9241 Part 6 Environmental requirements specifies the ergonomic requirements for the visual display unit working environment which will provide the user with comfortable, safe and productive working conditions. It covers the visual, acoustic and thermal environments. The objective is to provide a working environment which should facilitate efficient operation of the VDU and provide the user with comfortable working conditions.
The characteristics of the working environment which influence efficient operation and user comfort are identified, and design guidelines presented. Even when it is possible to control the working environment within strict limits, individuals will differ in their judgements of its acceptability, partly because individuals vary in their preferences and partly because different tasks may require quite different environments. For example, users who sit at VDUs for prolonged periods are far more sensitive to draughts than users whose work involves moving about an office and only working at the VDU intermittently.
VDU work often restricts the opportunities that individuals have for moving about in an office and so some individual control over the environment is highly desirable. Care must be taken in common work areas to protect the majority of users from extreme environments which may be preferred by some individuals.
Software ergonomics and dialogue design
ISO 9241 Part 10 Dialogue principles presents ergonomic principles which apply to the design of dialogues between humans and information systems, as follows:
- suitability for the task
- self-descriptiveness
- controllability
- conformity with user expectations
- error tolerance
- suitability for individualization
- suitability for learning.
The principles are supported by a number of scenarios which indicate the relative priorities and importance of the different principles in practical applications. The starting point for this work was the German DIN 66234 Part 8 Principles of Ergonomic Dialogue Design for Workplaces with Visual Display Units.
ISO 9241 Part 11 Guidance on usability specification and measures helps those involved in specifying or measuring usability by providing a consistent and agreed framework of the key issues and parameters involved. This framework can be used as part of an ergonomic requirements specification and it includes descriptions of the context of use, the evaluation procedures to be carried out and the criterion measures to be satisfied when the usability of the system is to be evaluated.
ISO 9241 Part 12 Presentation of information provides guidance on the specific ergonomics issues involved in representing and presenting information in a visual form. It includes guidance on ways of representing complex information, screen layout and design and the use of windows. It is a useful summary of the relevant materials available among the substantial body of guidelines and recommendations which already exist. The information is presented as guidelines without any need for formal conformance testing.
ISO 9241 Part 13 User guidance provides manufacturers with, in effect, guidelines on how to provide guidelines to users. These include documentation, help screens, error handling systems and other aids that are found in many software systems. In assessing the usability of a product in practice, real users should take into account the documentation and guidance provided by the supplier in the form of manuals, training and so on, as well as the specific characteristics of the product itself.
ISO 9241 Part 14 Menu dialogues provides guidance on the design of menu-based systems. It applies to text-based menus as well as to pull-down or pop-up menus in graphical systems. The standard contains a large number of guidelines developed from the published literature and from other relevant research. In order to deal with the extreme variety and complexity of menu-based systems, the standard employs a form of “conditional compliance”. For each guideline, there are criteria to help establish whether or not it is applicable to the system in question. If it is determined that the guidelines are applicable, criteria to establish whether or not the system meets those requirements are provided.
ISO 9241 Part 15 Command dialogues provides guidance for the design of text-based command dialogues. Dialogues are the familiar boxes which come onto the screen and query the VDU user, such as in a search command. The software creates a “dialogue” in which the user must supply the term to be found, and any other relevant specifications about the term, such as its case or format.
ISO 9241 Part 16 Direct manipulation dialogues deals with the design of direct manipulation dialogues and WYSIWYG (What You See Is What You Get) dialogue techniques, whether provided as the sole means of dialogue or combined with some other dialogue technique. It is envisaged that the conditional compliance developed for Part 14 may be appropriate for this mode of interaction also.
ISO 9241 Part 17 Form-filling dialogues is in the very early stages of development.
Ergonomic Aspects of Human-Computer Interaction
Introduction
The development of effective interfaces to computer systems is the fundamental objective of research on human-computer interactions.
An interface can be defined as the sum of the hardware and software components through which a system is operated and users informed of its status. The hardware components include data entry and pointing devices (e.g., keyboards, mice), information-presentation devices (e.g., screens, loudspeakers), and user manuals and documentation. The software components include menu commands, icons, windows, information feedback, navigation systems and messages and so on. An interface’s hardware and software components may be so closely linked as to be inseparable (e.g., function keys on keyboards). The interface includes everything the user perceives, understands and manipulates while interacting with the computer (Moran 1981). It is therefore a crucial determinant of the human-machine relation.
Research on interfaces aims at improving interface utility, accessibility, performance and safety, and usability. For these purposes, utility is defined with reference to the task to be performed. A useful system contains the necessary functions for the completion of tasks users are asked to perform (e.g., writing, drawing, calculations, programming). Accessibility is a measure of an interface’s ability to allow several categories of users—particularly individuals with handicaps, and those working in geographically isolated areas, in constant movement or having both hands occupied—to use the system to perform their activities. Performance, considered here from a human rather than a technical viewpoint, is a measure of the degree to which a system improves the efficiency with which users perform their work. This includes the effect of macros, menu short-cuts and intelligent software agents. The safety of a system is defined by the extent to which an interface allows users to perform their work free from the risk of human, equipment, data, or environmental accidents or losses. Finally, usability is defined as the ease with which a system is learned and used. By extension, it also includes system utility and performance, defined above.
Elements of Interface Design
Since the invention of shared-time operating systems in 1963, and especially since the arrival of the microcomputer in 1978, the development of human-computer interfaces has been explosive (see Gaines and Shaw 1986 for a history). The stimulus for this development has been essentially driven by three factors acting simultaneously:
First, the very rapid evolution of computer technology, a result of advances in electrical engineering, physics and computer science, has been a major determinant of user interface development. It has resulted in the appearance of computers of ever-increasing power and speed, with high memory capacities, high-resolution graphics screens, and more natural pointing devices allowing direct manipulation (e.g., mice, trackballs). These technologies were also responsible for the emergence of microcomputing. They were the basis for the character-based interfaces of the 1960s and 1970s, graphical interfaces of the late 1970s, and multi- and hyper-media interfaces appearing since the mid-1980s based on virtual environments or using a variety of alternate-input recognition technologies (e.g., voice-, handwriting-, and movement-detection). Considerable research and development has been conducted in recent years in these areas (Waterworth and Chignel 1989; Rheingold 1991). Concomitant with these advances was the development of more advanced software tools for interface design (e.g., windowing systems, graphical object libraries, prototyping systems) that greatly reduce the time required to develop interfaces.
Second, users of computer systems play a large role in the development of effective interfaces. There are three reasons for this. First, current users are not engineers or scientists, in contrast to users of the first computers. They therefore demand systems that can be easily learned and used. Second, the age, sex, language, culture, training, experience, skill, motivation and interest of individual users is quite varied. Interfaces must therefore be more flexible and better able to adapt to a range of needs and expectations. Finally, users are employed in a variety of economic sectors and perform a quite diverse spectrum of tasks. Interface developers must therefore constantly reassess the quality of their interfaces.
Lastly, intense market competition and increased safety expectations favour the development of better interfaces. These preoccupations are driven by two sets of partners: on the one hand, software producers who strive to reduce their costs while maintaining product distinctiveness that furthers their marketing goals, and on the other, users for whom the software is a means of offering competitive products and services to clients. For both groups, effective interfaces offer a number of advantages:
For software producers:
- better product image
- increased demand for products
- shorter training times
- lower after-sales service requirements
- solid base upon which to develop a product line
- reduction of the risk of errors and accidents
- reduction of documentation.
For users:
- shorter learning phase
- increased general applicability of skills
- improved use of the system
- increased autonomy using the system
- reduction of the time needed to execute a task
- reduction in the number of errors
- increased satisfaction.
Effective interfaces can significantly improve the health and productivity of users at the same time as they improve the quality and reduce the cost of their training. This, however, requires basing interface design and evaluation on ergonomic principles and practice standards, be they guidelines, corporate standards of major system manufacturers or international standards. Over the years, an impressive body of ergonomic principles and guidelines related to interface design has accumulated (Scapin 1986; Smith and Mosier 1986; Marshall, Nelson and Gardiner 1987; Brown 1988). This multidisciplinary corpus covers all aspects of character-mode and graphical interfaces, as well as interface evaluation criteria. Although its concrete application occasionally poses some problems—for example, imprecise terminology, inadequate information on usage conditions, inappropriate presentation—it remains a valuable resource for interface design and evaluation.
In addition, the major software manufacturers have developed their own guidelines and internal standards for interface design. These guidelines are available in the following documents:
- Apple Human Interface Guidelines (1987)
- Open Look (Sun 1990)
- OSF/Motif Style Guide (1990)
- IBM Common User Access guide to user interface design (1991)
- IBM Advanced Interface Design Reference (1991)
- The Windows interface: An application design guide (Microsoft 1992)
These guidelines attempt to simplify interface development by mandating a minimal level of uniformity and consistency between interfaces used on the same computer platform. They are precise, detailed, and quite comprehensive in several respects, and offer the additional advantages of being well-known, accessible and widely used. They are the de facto design standards used by developers, and are, for this reason, indispensable.
Furthermore, the International Organization for Standardization (ISO) standards are also very valuable sources of information about interface design and evaluation. These standards are primarily concerned with ensuring uniformity across interfaces, regardless of platforms and applications. They have been developed in collaboration with national standardization agencies, and after extensive discussion with researchers, developers and manufacturers. The main ISO interface design standard is ISO 9241, which describes ergonomic requirements for visual display units. It is comprised of 17 parts. For example, parts 14, 15, 16 and 17 discuss four types of human-computer dialogue—menus, command languages, direct manipulation, and forms. ISO standards should take priority over other design principles and guidelines. The following sections discuss the principles which should condition interface design.
A Design Philosophy Focused on the User
Gould and Lewis (1983) have proposed a design philosophy focused on the video display unit user. Its four principles are:
- Immediate and continuous attention to users. Direct contact with users is maintained, in order to better understand their characteristics and tasks.
- Integrated design. All aspects of usability (e.g., interface, manuals, help systems) are developed in parallel and placed under centralized control.
- Immediate and continuous evaluation by users. Users test the interfaces or prototypes early on in the design phase, under simulated work conditions. Performance and reactions are measured quantitatively and qualitatively.
- Iterative design. The system is modified on the basis of the results of the evaluation, and the evaluation cycle started again.
These principles are explained in further detail in Gould (1988). Very relevant when they were first published in 1985, fifteen years later they remain so, due to the inability to predict the effectiveness of interfaces in the absence of user testing. These principles constitute the heart of user-based development cycles proposed by several authors in recent years (Gould 1988; Mantei and Teorey 1989; Mayhew 1992; Nielsen 1992; Robert and Fiset 1992).
The rest of this article will analyse five stages in the development cycle that appear to determine the effectiveness of the final interface.
Task Analysis
Ergonomic task analysis is one of the pillars of interface design. Essentially, it is the process by which user responsibilities and activities are elucidated. This in turn allows interfaces compatible with the characteristics of users’ tasks to be designed. There are two facets to any given task:
- The nominal task, corresponding to the organization’s formal definition of the task. This includes objectives, procedures, quality control, standards and tools.
- The real task, corresponding to the users’ decisions and behaviours necessary for the execution of the nominal task.
The gap between nominal and real tasks is inevitable and results from the failure of nominal tasks to take into account variations and unforeseen circumstances in the work flow, and differences in users’ mental representations of their work. Analysis of the nominal task is insufficient for a full understanding of users’ activities.
Activity analysis examines elements such as work objectives, the type of operations performed, their temporal organization (sequential, parallel) and frequency, the operational modes relied upon, decisions, sources of difficulty, errors and recovery modes. This analysis reveals the different operations performed to accomplish the task (detection, searching, reading, comparing, evaluating, deciding, estimating, anticipating), the entities manipulated (e.g., in process control, temperature, pressure, flow-rate, volume) and the relation between operators and entities. The context in which the task is executed conditions these relations. These data are essential for the definition and organization of the future system’s features.
At its most basic, task analysis is composed of data collection, compilation and analysis. It may be performed before, during or after computerization of the task. In all cases, it provides essential guidelines for interface design and evaluation. Task analysis is always concerned with the real task, although it may also study future tasks through simulation or prototype testing. When performed prior to computerization, it studies “external tasks” (i.e., tasks external to the computer) performed with the existing work tools (Moran 1983). This type of analysis is useful even when computerization is expected to result in major modification of the task, since it elucidates the nature and logic of the task, work procedures, terminology, operators and tasks, work tools and sources of difficulty. In so doing, it provides the data necessary for task optimization and computerization.
Task analysis performed during task computerization focuses on “internal tasks”, as performed and represented by the computer system. System prototypes are used to collect data at this stage. The focus is on the same points examined in the previous stage, but from the point of view of the computerization process.
Following task computerization, task analysis also studies internal tasks, but analysis now focuses on the final computer system. This type of analysis is often performed to evaluate existing interfaces or as part of the design of new ones.
Hierarchical task analysis is a common method in cognitive ergonomics that has proven very useful in a wide variety of fields, including interface design (Shepherd 1989). It consists of the division of tasks (or main objectives) into sub-tasks, each of which can be further subdivided, until the required level of detail is attained. If data is collected directly from users (e.g., through interviews, vocalization), hierarchical division can provide a portrait of users’ mental mapping of a task. The results of the analysis can be represented by a tree diagram or table, each format having its advantages and disadvantages.
User Analysis
The other pillar of interface design is the analysis of user characteristics. The characteristics of interest may relate to user age, sex, language, culture, training, technical or computer-related knowledge, skills or motivation. Variations in these individual factors are responsible for differences within and between groups of users. One of the key tenets of interface design is therefore that there is no such thing as the average user. Instead, different groups of users should be identified and their characteristics understood. Representatives of each group should be encouraged to participate in the interface design and evaluation processes.
On the other hand, techniques from psychology, ergonomics and cognitive engineering can be used to reveal information on user characteristics related to perception, memory, cognitive mapping, decision-making and learning (Wickens 1992). It is clear that the only way to develop interfaces that are truly compatible with users is to take into account the effect of differences in these factors on user capacities, limits and ways of operating.
Ergonomic studies of interfaces have focused almost exclusively on users’ perceptual, cognitive and motor skills, rather than on affective, social or attitudinal factors, although work in the latter fields has become more popular in recent years. (For an integrated view of humans as information-processing systems see Rasmussen 1986; for a review of user-related factors to consider when designing interfaces see Thimbleby 1990 and Mayhew 1992). The following paragraphs review the four main user-related characteristics that should be taken into account during interface design.
Mental representation
The mental models users construct of the systems they use reflect the manner in which they receive and understand these systems. These models therefore vary as a function of users’ knowledge and experience (Hutchins 1989). In order to minimize the learning curve and facilitate system use, the conceptual model upon which a system is based should be similar to users’ mental representation of it. It should be recognized however that these two models are never identical. The mental model is characterized by the very fact that it is personal (Rich 1983), incomplete, variable from one part of the system to another, possibly in error on some points and in constant evolution. It plays a minor role in routine tasks but a major one in non-routine ones and during diagnosis of problems (Young 1981). In the latter cases, users will perform poorly in the absence of an adequate mental model. The challenge for interface designers is to design systems whose interaction with users will induce the latter to form mental models similar to the system’s conceptual model.
Learning
Analogy plays a large role in user learning (Rumelhart and Norman 1983). For this reason, the use of appropriate analogies or metaphors in the interface facilitates learning, by maximizing the transfer of knowledge from known situations or systems. Analogies and metaphors play a role in many parts of the interface, including the names of commands and menus, symbols, icons, codes (e.g., shape, colour) and messages. When pertinent, they greatly contribute to rendering interfaces natural and more transparent to users. On the other hand, when they are irrelevant, they can hinder users (Halasz and Moran 1982). To date, the two metaphors used in graphical interfaces are the desktop and, to a lesser extent, the room.
Users generally prefer to learn new software by using it immediately rather than by reading or taking a course—they prefer action-based learning in which they are cognitively active. This type of learning does, however, present a few problems for users (Carroll and Rosson 1988; Robert 1989). It demands an interface structure which is compatible, transparent, consistent, flexible, natural-appearing and fault tolerant, and a feature set which ensures usability, feedback, help systems, navigational aides and error handling (in this context, “errors” refer to actions that users wish to undo). Effective interfaces give users some autonomy during exploration.
Developing knowledge
User knowledge develops with increasing experience, but tends to plateau rapidly. This means that interfaces must be flexible and capable of responding simultaneously to the needs of users with different levels of knowledge. Ideally, they should also be context sensitive and provide personalized help. The EdCoach system, developed by Desmarais, Giroux and Larochelle (1993) is such an interface. Classification of users into beginner, intermediate and expert categories is inadequate for the purpose of interface design, since these definitions are too static and do not account for individual variations. Information technology capable of responding to the needs of different types of users is now available, albeit at the research, rather than commercial, level (Egan 1988). The current rage for performance-support systems suggests intense development of these systems in coming years.
Unavoidable errors
Finally, it should be recognized that users make mistakes when using systems, regardless of their skill level or the quality of the system. A recent German study by Broadbeck et al. (1993) revealed that at least 10% of the time spent by white-collar workers working on computers is related to error management. One of the causes of errors is users’ reliance on correction rather than prevention strategies (Reed 1982). Users prefer acting rapidly and incurring errors that they must subsequently correct, to working more slowly and avoiding errors. It is essential that these considerations be taken into account when designing human-computer interfaces. In addition, systems should be fault tolerant and should incorporate effective error management (Lewis and Norman 1986).
Needs Analysis
Needs analysis is an explicit part of Robert and Fiset’s development cycle (1992), it corresponds to Nielsen’s functional analysis and is integrated into other stages (task, user or needs analysis) described by other authors. It consists of the identification, analysis and organization of all the needs that the computer system can satisfy. Identification of features to be added to the system occurs during this process. Task and user analysis, presented above, should help define many of the needs, but may prove inadequate for the definition of new needs resulting from the introduction of new technologies or new regulations (e.g., safety). Needs analysis fills this void.
Needs analysis is performed in the same way as functional analysis of products. It requires the participation of a group of people interested by the product and possessing complementary training, occupations or work experience. This can include future users of the system, supervisors, domain experts and, as required, specialists in training, work organization and safety. Review of the scientific and technical literature in the relevant field of application may also be performed, in order to establish the current state of the art. Competitive systems used in similar or related fields can also be studied. The different needs identified by this analysis are then classified, weighted and presented in a format appropriate for use throughout the development cycle.
Prototyping
Prototyping is part of the development cycle of most interfaces and consists of the production of a preliminary paper or electronic model (or prototype) of the interface. Several books on the role of prototyping in human-computer interaction are available (Wilson and Rosenberg 1988; Hartson and Smith 1991; Preece et al. 1994).
Prototyping is almost indispensable because:
- Users have difficulty evaluating interfaces on the basis of functional specifications—the description of the interface is too distant from the real interface, and evaluation too abstract. Prototypes are useful because they allow users to see and use the interface and directly evaluate its usefulness and usability.
- It is practically impossible to construct an adequate interface on the first try. Interfaces must be tested by users and modified, often repeatedly. To overcome this problem, paper or interactive prototypes that can be tested, modified or rejected are produced and refined until a satisfactory version is obtained. This process is considerably less expensive than working on real interfaces.
From the point of view of the development team, prototyping has several advantages. Prototypes allow the integration and visualization of interface elements early on in the design cycle, rapid identification of detailed problems, production of a concrete and common object of discussion in the development team and during discussions with clients, and simple illustration of alternative solutions for the purposes of comparison and internal evaluation of the interface. The most important advantage is, however, the possibility of having users evaluate prototypes.
Inexpensive and very powerful software tools for the production of prototypes are commercially available for a variety of platforms, including microcomputers (e.g., Visual Basic and Visual C++ (™Microsoft Corp.), UIM/X (™Visual Edge Software), HyperCard (™Apple Computer), SVT (™SVT Soft Inc.)). Readily available and relatively easy to learn, they are becoming widespread among system developers and evaluators.
The integration of prototyping completely changed the interface development process. Given the rapidity and flexibility with which prototypes can be produced, developers now tend to reduce their initial analyses of task, users and needs, and compensate for these analytical deficiencies by adopting longer evaluation cycles. This assumes that usability testing will identify problems and that it is more economical to prolong evaluation than to spend time on preliminary analysis.
Evaluation of Interfaces
User evaluation of interfaces is an indispensable and effective way to improve interfaces’ usefulness and usability (Nielsen 1993). The interface is almost always evaluated in electronic form, although paper prototypes may also be tested. Evaluation is an iterative process and is part of the prototype evaluation-modification cycle which continues until the interface is judged acceptable. Several cycles of evaluation may be necessary. Evaluation may be performed in the workplace or in usability laboratories (see the special edition of Behaviour and Information Technology (1994) for a description of several usability laboratories).
Some interface evaluation methods do not involve users; they may be used as a complement to user evaluation (Karat 1988; Nielsen 1993; Nielsen and Mack 1994). A relatively common example of such methods consists of the use of criteria such as compatibility, consistency, visual clarity, explicit control, flexibility, mental workload, quality of feedback, quality of help and error handling systems. For a detailed definition of these criteria, see Bastien and Scapin (1993); they also form the basis of an ergonomic questionnaire on interfaces (Shneiderman 1987; Ravden and Johnson 1989).
Following evaluation, solutions must be found to problems that have been identified, modifications discussed and implemented, and decisions made concerning whether a new prototype is necessary.
Conclusion
This discussion of interface development has highlighted the major stakes and broad trends in the field of human-computer interaction. In summary, (a) task, user, and needs analysis play an essential role in understanding system requirements and, by extension, necessary interface features; and (b) prototyping and user evaluation are indispensable for the determination of interface usability. An impressive body of knowledge, composed of principles, guidelines and design standards, exists on human-computer interactions. Nevertheless, it is currently impossible to produce an adequate interface on the first try. This constitutes a major challenge for the coming years. More explicit, direct and formal links must be established between analysis (task, users, needs, context) and interface design. Means must also be developed to apply current ergonomic knowledge more directly and more simply to the design of interfaces.
Psychosocial Aspects of VDU Work
Introduction
Computers provide efficiency, competitive advantages and the ability to carry out work processes that would not be possible without their use. Areas such as manufacturing process control, inventory management, records management, complex systems control and office automation have all benefited from automation. Computerization requires substantial infrastructure support in order to function properly. In addition to architectural and electrical changes needed to accommodate the machines themselves, the introduction of computerization requires changes in employee knowledge and skills, and application of new methods of managing work. The demands placed on jobs which use computers can be very different from those of traditional jobs. Often computerized jobs are more sedentary and may require more thinking and mental attention to tasks, while at the same time require less physical energy expenditure. Production demands can be high, with constant work pressure and little room for decision-making.
The economic advantages of computers at work have overshadowed associated potential health, safety and social problems for workers, such as job loss, cumulative trauma disorders and increased mental stress. The transition from more traditional forms of work to computerization has been difficult in many workplaces, and has resulted in significant psychosocial and sociotechnical problems for the workforce.
Psychosocial Problems Specific to VDUs
Research studies (for example, Bradley 1983 and 1989; Bikson 1987; Westlander 1989; Westlander and Aberg 1992; Johansson and Aronsson 1984; Stellman et al. 1987b; Smith et al. 1981 and 1992a) have documented how the introduction of computers into the workplace has brought substantial changes in the process of work, in social relationships, in management style and in the nature and content of job tasks. In the 1980s, the implementation of the technological changeover to computerization was most often a “top-down” process in which employees had no input into the decisions regarding the new technology or the new work structures. As a result, many industrial relations, physical and mental health problems arose.
Experts disagree on the success of changes that are occurring in offices, with some arguing that computer technology improves the quality of work and enhances productivity (Strassmann 1985), while others compare computers to earlier forms of technology, such as assembly-line production that also make working conditions worse and increase job stress (Moshowitz 1986; Zuboff 1988). We believe that visual display unit (VDU) technology does affect work in various ways, but technology is only one element of a larger work system that includes the individual, tasks, environment and organizational factors.
Conceptualizing Computerized Job Design
Many working conditions jointly influence the VDU user. The authors have proposed a comprehensive job design model which illustrates the various facets of working conditions which can interact and accumulate to produce stress (Smith and Carayon-Sainfort 1989). Figure 1 illustrates this conceptual model for the various elements of a work system that can exert loads on workers and may result in stress. At the centre of this model is the individual with his/her unique physical characteristics, perceptions, personality and behaviour. The individual uses technologies to perform specific job tasks. The nature of the technologies, to a large extent, determines performance and the skills and knowledge needed by the worker to use the technology effectively. The requirements of the task also affect the required skill and knowledge levels needed. Both the tasks and technologies affect the job content and the mental and physical demands. The model also shows that the tasks and technologies are placed within the context of a work setting that comprises the physical and the social environment. The overall environment itself can affect comfort, psychological moods and attitudes. Finally, the organizational structure of work defines the nature and level of individual involvement, worker interactions, and levels of control. Supervision and standards of performance are all affected by the nature of the organization.
Figure 1. Model of working conditions and their impact on the individual
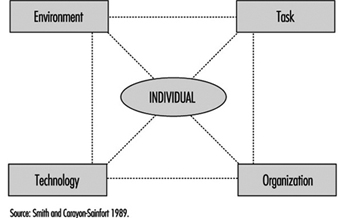
This model helps to explain relationships between job requirements, psychological and physical loads and resulting health strains. It represents a systems concept in which any one element can influence any other element, and in which all elements interact to determine the way in which work is accomplished and the effectiveness of the work in achieving individual and organizational needs and goals. The application of the model to the VDU workplace is described below.
Environment
Physical environmental factors have been implicated as job stressors in the office and elsewhere. General air quality and housekeeping contribute, for example, to sick building syndrome and other stress responses (Stellman et al. 1985; Hedge, Erickson and Rubin 1992.) Noise is a well-known environmental stressor which can cause increases in arousal, blood pressure, and negative psychological mood (Cohen and Weinstein 1981). Environmental conditions that produce sensory disruption and make it more difficult to carry out tasks increase the level of worker stress and emotional irritation are other examples (Smith et al. 1981; Sauter et al. 1983b).
Task
With the introduction of computer technology, expectations regarding performance increase. Additional pressure on workers is created because they are expected to perform at a higher level all the time. Excessive workload and work pressure are significant stressors for computer users (Smith et al. 1981; Piotrkowski, Cohen and Coray 1992; Sainfort 1990). New types of work demands are appearing with the increasing use of computers. For instance, cognitive demands are likely to be sources of increased stress for VDU users (Frese 1987). These are all facets of job demands.
Electronic Monitoring of Employee Performance
The use of electronic methods to monitor employee work performance has increased substantially with the widespread use of personal computers which make such monitoring quick and easy. Monitoring provides information which can be used by employers to better manage technological and human resources. With electronic monitoring it is possible to pinpoint bottlenecks, production delays and below average (or below standard) performance of employees in real time. New electronic communication technologies have the capability of tracking the performance of individual elements of a communication system and of pinpointing individual worker inputs. Such work elements as data entry into computer terminals, telephone conversations, and electronic mail messages can all be examined through the use of electronic surveillance.
Electronic monitoring increases management control over the workforce, and may lead to organisational management approaches that are stressful. This raises important issues about the accuracy of the monitoring system and how well it represents worker contributions to the employer’s success, the invasion of worker privacy, worker versus technology control over job tasks, and the implications of management styles that use monitored information to direct worker behaviour on the job (Smith and Amick 1989; Amick and Smith 1992; Carayon 1993b). Monitoring can bring about increased production, but it may also produce job stress, absences from work, turnover in the workforce and sabotage. When electronic monitoring is combined with incentive systems for increased production, work-related stress can also be increased (OTA 1987; Smith et al. 1992a). In addition, such electronic performance monitoring raises issues of worker privacy (ILO 1991) and several countries have banned the use of individual performance monitoring.
A basic requirement of electronic monitoring is that work tasks be broken up into activities that can easily be quantified and measured, which usually results in a job design approach that reduces the content of the tasks by removing complexity and thinking, which are replaced by repetitive action. The underlying philosophy is similar to a basic principle of “Scientific Management” (Taylor 1911) that calls for work “simplification.”
In one company, for example, a telephone monitoring capability was included with a new telephone system for customer service operators. The monitoring system distributed incoming telephone calls from customers, timed the calls and allowed for supervisor eavesdropping on employee telephone conversations. This system was instituted under the guise of a work flow scheduling tool for determining the peak periods for telephone calls to determine when extra operators would be needed. Instead of using the monitoring system solely for that purpose, management also used the data to establish work performance standards, (seconds per transaction) and to bring disciplinary action against employees with “below average performance.” This electronic monitoring system introduced a pressure to perform above average because of fear of reprimand. Research has shown that such work pressure is not conducive to good performance but rather can bring about adverse health consequences (Cooper and Marshall 1976; Smith 1987). In fact, the monitoring system described was found to have increased employee stress and lowered the quality of production (Smith et al. 1992a).
Electronic monitoring can influence worker self-image and feelings of self-worth. In some cases, monitoring could enhance feelings of self-worth if the worker gets positive feedback. The fact that management has taken an interest in the worker as a valuable resource is another possible positive outcome. However, both effects may be perceived differently by workers, particularly if poor performance leads to punishment or reprimand. Fear of negative evaluation can produce anxiety and may damage self-esteem and self-image. Indeed electronic monitoring can create known adverse working conditions, such as paced work, lack of worker involvement, reduced task variety and task clarity, reduced peer social support, reduced supervisory support, fear of job loss, or routine work activities, and lack of control over tasks (Amick and Smith 1992; Carayon 1993).
Michael J. Smith
Positive aspects also exist since computers are able to do many of the simple, repetitive tasks that were previously done manually, which can reduce the repetitiveness of the job, increase the content of the job and make it more meaningful. This is not universally true, however, since many new computer jobs, such as data entry, are still repetitive and boring. Computers can also provide performance feedback that is not available with other technologies (Kalimo and Leppanen 1985), which can reduce ambiguity.
Some aspects of computerized work have been linked to decreased control, which has been identified as a major source of stress for clerical computer users. Uncertainty regarding the duration of computer-related problems, such as breakdown and slowdown, can be a source of stress (Johansson and Aronsson 1984; Carayon-Sainfort 1992). Computer-related problems can be particularly stressful if workers, such as airline reservation clerks, are highly dependent on the technology to perform their job.
Technology
The technology being used by the worker often defines his or her ability to accomplish tasks and the extent of physiological and psychological load. If the technology produces either too much or too little workload, increased stress and adverse physical health outcomes can occur (Smith et al. 1981; Johansson and Aronsson 1984; Ostberg and Nilsson 1985). Technology is changing at a rapid pace, forcing workers to adjust their skills and knowledge continuously to keep up. In addition, today’s skills can quickly become obsolete. Technological obsolescence may be due to job de-skilling and impoverished job content or to inadequate skills and training. Workers who do not have the time or resources to keep up with the technology may feel threatened by the technology and may worry about losing their job. Thus, workers’ fears of having inadequate skills to use the new technology are one of the main adverse influences of technology, which training, of course, can help to offset. Another effect of the introduction of technology is the fear of job loss due to increased efficiency of technology (Ostberg and Nilsson 1985; Smith, Carayon and Miezio 1987).
Intensive, repetitive, long sessions at the VDU can also contribute to increased ergonomic stress and strain (Stammerjohn, Smith and Cohen 1981; Sauter et al. 1983b; Smith et al. 1992b) and can create visual or musculoskeletal discomfort and disorders, as described elsewhere in the chapter.
Organizational factors
The organizational context of work can influence worker stress and health. When technology requires new skills, the way in which workers are introduced to the new technology and the organizational support they receive, such as appropriate training and time to acclimatize, has been related to the levels of stress and emotional disturbances experienced (Smith, Carayon and Miezio 1987). The opportunity for growth and promotion in a job (career development) is also related to stress (Smith et al. 1981). Job future uncertainty is a major source of stress for computer users (Sauter et al. 1983b; Carayon 1993a) and the possibility of job loss also creates stress (Smith et al. 1981; Kasl 1978).
Work scheduling, such as shift work and overtime, have been shown to have negative mental and physical health consequences (Monk and Tepas 1985; Breslow and Buell 1960). Shift work is increasingly used by companies that want or need to keep computers running continuously. Overtime is often needed to ensure that workers keep up with the workload, especially when work remains incomplete as a result of delays due to computer breakdown or misfunction.
Computers provide management with the capability to continuously monitor employee performance electronically, which has the potential to create stressful working conditions, such as by increasing work pressure (see the box “Electronic Monitoring”). Negative employee-supervisor relationships and feelings of lack of control can increase in electronically supervised workplaces.
The introduction of VDU technology has affected social relationships at work. Social isolation has been identified as a major source of stress for computer users (Lindström 1991; Yang and Carayon 1993) since the increased time spent working on computers reduces the time that workers have to socialize and receive or give social support. The need for supportive supervisors and co-workers has been well documented (House 1981). Social support can moderate the impact of other stressors on worker stress. Thus, support from colleagues, supervisor or computer staff becomes important for the worker who is experiencing computer-related problems but the computer work environment may, ironically, reduce the level of such social support available.
The individual
A number of personal factors such as personality, physical health status, skills and abilities, physical conditioning, prior experiences and learning, motives, goals and needs determine the physical and psychological effects just described (Levi 1972).
Improving the Psychosocial Characteristics of VDU Work
The first step in making VDU work less stressful is to identify work organization and job design features that can promote psychosocial problems so that they can be modified, always bearing in mind that VDU problems which can lead to job stress are seldom the result of single aspects of the organization or of job design, but rather, are a combination of many aspects of improper work design. Thus, solutions for reducing or eliminating job stress must be comprehensive and deal with many improper work design factors simultaneously. Solutions that focus on only one or two factors will not succeed. (See figure 2.)
Figure 2. Keys to reducing isolation and stress

Improvements in job design should start with the work organization providing a supportive environment for employees. Such an environment enhances employee motivation to work and feelings of security, and it reduces feelings of stress (House 1981). A policy statement that defines the importance of employees within an organization and is explicit on how the organization will provide a supportive environment is a good first step. One very effective means for providing support to employees is to provide supervisors and managers with specific training in methods for being supportive. Supportive supervisors can serve as buffers that “protect” employees from unnecessary organizational or technological stresses.
The content of job tasks has long been recognized as important for employee motivation and productivity (Herzberg 1974; Hackman and Oldham 1976). More recently the relationship between job content and job stress reactions has been elucidated (Cooper and Marshall 1976; Smith 1987). Three main aspects of job content that are of specific relevance to VDU work are task complexity, employee skills and career opportunities. In some respects, these are all related to the concept of developing the motivational climate for employee job satisfaction and psychological growth, which deals with the improvement of employees’ intellectual capabilities and skills, increased ego enhancement or self-image and increased social group recognition of individual achievement.
The primary means for enhancing job content is to increase the skill level for performing job tasks, which typically means enlarging the scope of job tasks, as well as enriching the elements of each specific task (Herzberg 1974). Enlarging the number of tasks increases the repertoire of skills needed for successful task performance, and also increases the number of employee decisions made while defining task sequences and activities. An increase in the skill level of the job content promotes employee self-image of personal worth and of value to the organization. It also enhances the positive image of the individual in his or her social work group within the organization.
Increasing the complexity of the tasks, which means increasing the amount of thinking and decision-making involved, is a logical next step that can be achieved by combining simple tasks into sets of related activities that have to be coordinated, or by adding mental tasks that require additional knowledge and computational skills. Specifically, when computerized technology is introduced, new tasks in general will have requirements that exceed the current knowledge and skills of the employees who are to perform them. Thus there is a need to train employees in the new aspects of the tasks so that they will have the skills to perform the tasks adequately. Such training has more than one benefit, since it not only may improve employee knowledge and skills, and thus enhance performance, but may also enhance employee self-esteem and confidence. Providing training also shows the employee that the employer is willing to invest in his or her skill enhancement, and thus promotes confidence in employment stability and job future.
The amount of control that an employee has over the job has a powerful psychosocial influence (Karasek et al. 1981; Sauter, Cooper and Hurrell 1989). Important aspects of control can be defined by the answers to the questions, “What, how and when?” The nature of the tasks to be undertaken, the need for coordination among employees, the methods to be used to carry out the tasks and the scheduling of the tasks can all be defined by answers to these questions. Control can be designed into jobs at the levels of the task, the work unit and the organization (Sainfort 1991; Gardell 1971). At the task level, the employee can be given autonomy in the methods and procedures used in completing the task.
At the work-unit level, groups of employees can self-manage several interrelated tasks and the group itself can decide on who will perform particular tasks, the scheduling of tasks, coordination of tasks and production standards to meet organizational goals. At the organization level, employees can participate in structured activities that provide input to management about employee opinions or quality improvement suggestions. When the levels of control available are limited, it is better to introduce autonomy at the task level and then work up the organizational structure, insofar as possible (Gardell 1971).
One natural result of computer automation appears to be an increased workload, since the purpose of the automation is to enhance the quantity and quality of work output. Many organizations believe that such an increase is necessary in order to pay for the investment in the automation. However, establishing the appropriate workload is problematic. Scientific methods have been developed by industrial engineers for determining appropriate work methods and workloads (the performance requirements of jobs). Such methods have been used successfully in manufacturing industries for decades, but have had little application in office settings, even after office computerization. The use of scientific means, such as those described by Kanawaty (1979) and Salvendy (1992), to establish workloads for VDU operators, should be a high priority for every organization, since such methods set reasonable production standards or work output requirements, help to protect employees from excessive workloads, as well as help to ensure the quality of products.
The demand that is associated with the high levels of concentration required for computerized tasks can diminish the amount of social interaction during work, leading to social isolation of employees. To counter this effect, opportunities for socialization for employees not engaged in computerized tasks, and for employees who are on rest breaks, should be provided. Non-computerized tasks which do not require extensive concentration could be organized in such a way that employees can work in close proximity to one another and thus have the opportunity to talk among themselves. Such socialization provides social support, which is known to be an essential modifying factor in reducing adverse mental health effects and physical disorders such as cardiovascular diseases (House 1981). Socialization naturally also reduces social isolation and thus promotes improved mental health.
Since poor ergonomic conditions can also lead to psychosocial problems for VDU users, proper ergonomic conditions are an essential element of complete job design. This is covered in some detail in other articles in this chapter and elsewhere in the Encyclopaedia.
Finding Balance
Since there are no “perfect” jobs or “perfect” workplaces free from all psychosocial and ergonomic stressors, we must often compromise when making improvements at the workplace. Redesigning processes generally involves “trade-offs” between excellent working conditions and the need to have acceptable productivity. This requires us to think about how to achieve the best “balance” between positive benefits for employee health and productivity. Unfortunately, since so many factors can produce adverse psychosocial conditions that lead to stress, and since these factors are interrelated, modifications in one factor may not be beneficial if concomitant changes are not made in other related factors. In general, two aspects of balance should be addressed: the balance of the total system and compensatory balance.
System balance is based on the idea that a workplace or process or job is more than the sum of the individual components of the system. The interplay among the various components produces results that are greater (or less) than the sum of the individual parts and determines the potential for the system to produce positive results. Thus, job improvements must take account of and accommodate the entire work system. If an organization concentrates solely on the technological component of the system, there will be an imbalance because personal and psychosocial factors will have been neglected. The model given in figure 1 of the work system can be used to identify and understand the relationships between job demands, job design factors, and stress which must be balanced.
Since it is seldom possible to eliminate all psychosocial factors that cause stress, either because of financial considerations, or because it is impossible to change inherent aspects of job tasks, compensatory balance techniques are employed. Compensatory balance seeks to reduce psychological stress by changing aspects of work that can be altered in a positive direction to compensate for those aspects that cannot be changed. Five elements of the work system—physical loads, work cycles, job content, control, and socialization—function in concert to provide the resources for achieving individual and organizational goals through compensatory balance. While we have described some of the potential negative attributes of these elements in terms of job stress, each also has positive aspects that can counteract the negative influences. For instance, inadequate skill to use new technology can be offset by employee training. Low job content that creates repetition and boredom can be balanced by an organizational supervisory structure that promotes employee involvement and control over tasks, and job enlargement that introduces task variety. The social conditions of VDU work could be improved by balancing the loads that are potentially stressful and by considering all of the work elements and their potential for promoting or reducing stress. The organizational structure itself could be adapted to accommodate enriched jobs in order to provide support to the individual. Increased staffing levels, increasing the levels of shared responsibilities or increasing the financial resources put toward worker well-being are other possible solutions.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."