- You are here:
-
Home

-
Part XVI. Construction
-
Construction
- Major Sectors and Their Hazards
Radiation Accidents
Description, Sources, Mechanisms
Apart from the transportation of radioactive materials, there are three settings in which radiation accidents can occur:
- use of nuclear reactions to produce energy or arms, or for research purposes
- industrial applications of radiation (gamma radiography, irradiation)
- research and nuclear medicine (diagnosis or therapy).
Radiation accidents may be classified into two groups on the basis of whether or not there is environmental emission or dispersion of radionuclides; each of these types of accident affects different populations.
The magnitude and duration of the exposure risk for the general population depends on the quantity and the characteristics (half-life, physical and chemical properties) of the radionuclides emitted into the environment (table 1). This type of contamination occurs when there is rupture of the containment barriers at nuclear power plants or industrial or medical sites which separate radioactive materials from the environment. In the absence of environmental emissions, only workers present onsite or handling radioactive equipment or materials are exposed.
Table 1. Typical radionuclides, with their radioactive half-lives
|
Radionuclide |
Symbol |
Radiation emitted |
Physical half-life* |
Biological half-life |
|
Barium-133 |
Ba-133 |
γ |
10.7 y |
65 d |
|
Cerium-144 |
Ce-144 |
β,γ |
284 d |
263 d |
|
Caesium-137 |
Cs-137 |
β,γ |
30 y |
109 d |
|
Cobalt-60 |
Co-60 |
β,γ |
5.3 y |
1.6 y |
|
Iodine-131 |
I-131 |
β,γ |
8 d |
7.5 d |
|
Plutonium-239 |
Pu-239 |
α,γ |
24,065 y |
50 y |
|
Polonium-210 |
Po-210 |
α |
138 d |
27 d |
|
Strontium-90 |
Sr-90 |
β |
29.1 y |
18 y |
|
Tritium |
H-3 |
β |
12.3 y |
10 d |
* y = years; d = days.
Exposure to ionizing radiation may occur through three routes, regardless of whether the target population is composed of workers or the general public: external irradiation, internal irradiation, and contamination of skin and wounds.
External irradiation occurs when individuals are exposed to an extracorporeal radiation source, either point (radiotherapy, irradiators) or diffuse (radioactive clouds and fallout from accidents, figure 1). Irradiation may be local, involving only a portion of the body, or whole body.
Figure 1. Exposure pathways to ionizing radiation after an accidental release of radioactivity in the environment
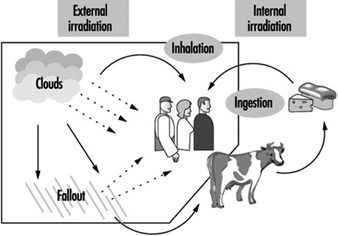
Internal radiation occurs following incorporation of radioactive substances into the body (figure 1) through either inhalation of airborne radioactive particles (e.g., caesium-137 and iodine-131, present in the Chernobyl cloud) or ingestion of radioactive materials in the food chain (e.g., iodine-131 in milk). Internal irradiation may affect the whole body or only certain organs, depending on the characteristics of the radionuclides: caesium-137 distributes itself homogeneously throughout the body, while iodine-131 and strontium-90 concentrate in the thyroid and the bones, respectively.
Finally, exposure may also occur through direct contact of radioactive materials with skin and wounds.
Accidents involving nuclear power plants
Sites included in this category include power-generating stations, experimental reactors, facilities for the production and processing or reprocessing of nuclear fuel and research laboratories. Military sites include plutonium breeder reactors and reactors located aboard ships and submarines.
Nuclear power plants
The capture of heat energy emitted by atomic fission is the basis for the production of electricity from nuclear energy. Schematically, nuclear power plants can be thought of as comprising: (1) a core, containing the fissile material (for pressurized-water reactors, 80 to 120 tonnes of uranium oxide); (2) heat-transfer equipment incorporating heat-transfer fluids; (3) equipment capable of transforming heat energy into electricity, similar to that found in power plants that are not nuclear.
Strong, sudden power surges capable of causing core meltdown with emission of radioactive products are the primary hazards at these installations. Three accidents involving reactor-core meltdown have occurred: at Three Mile Island (1979, Pennsylvania, United States), Chernobyl (1986, Ukraine), and Fukushima (2011, Japan) [Edited, 2011].
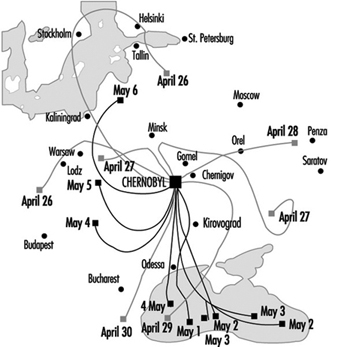
The Chernobyl accident was what is known as a criticality accident—that is, a sudden (within the space of a few seconds) increase in fission leading to a loss of process control. In this case, the reactor core was completely destroyed and massive amounts of radioactive materials were emitted (table 2). The emissions reached a height of 2 km, favouring their dispersion over long distances (for all intents and purposes, the entire Northern hemisphere). The behaviour of the radioactive cloud has proven difficult to analyse, due to meteorological changes during the emission period (figure 2) (IAEA 1991).
Table 2. Comparison of different nuclear accidents
|
Accident |
Type of facility |
Accident |
Total emitted |
Duration |
Main emitted |
Collective |
|
Khyshtym 1957 |
Storage of high- |
Chemical explosion |
740x106 |
Almost |
Strontium-90 |
2,500 |
|
Windscale 1957 |
Plutonium- |
Fire |
7.4x106 |
Approximately |
Iodine-131, polonium-210, |
2,000 |
|
Three Mile Island |
PWR industrial |
Coolant failure |
555 |
? |
Iodine-131 |
16–50 |
|
Chernobyl 1986 |
RBMK industrial |
Critically |
3,700x106 |
More than 10 days |
Iodine-131, iodine-132, |
600,000 |
|
Fukushima 2011
|
The final report of the Fukushima Assessment Task Force will be submitted in 2013. |
|
|
|
|
|
Source: UNSCEAR 1993.
Figure 2. Trajectory of emissions from the Chernobyl accident, 26 April-6 May 1986
Contamination maps were drawn up on the basis of environmental measurements of caesium-137, one of the main radioactive emission products (table 1 and table 2). Areas of Ukraine, Byelorussia (Belarus) and Russia were heavily contaminated, while fallout in the rest of Europe was less significant (figure 3 and figure 4 (UNSCEAR 1988). Table 3 presents data on the area of the contaminated zones, characteristics of the exposed populations and routes of exposure.
FIgure 3. Caesium-137 deposition in Byelorussia, Russia and Ukraine following the Chernobyl accident.

Figure 4. Caesium-137 fallout (kBq/km2) in Europe following the Chernobyl accident
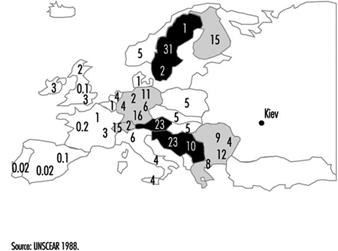
Table 3. Area of contaminated zones, types of populations exposed and modes of exposure in Ukraine, Byelorussia and Russia following the Chernobyl accident
|
Type of population |
Surface area ( km2 ) |
Population size (000) |
Main modes of exposure |
|
Occupationally exposed populations: |
|||
|
Employees onsite at |
≈0.44 |
External irradiation, |
|
|
General public: |
|||
|
Evacuated from the |
|
115 |
External irradiation by |
* Individuals participating in clean-up within 30 km of the site. These include fire-fighters, military personnel, technicians and engineers who intervened during the first weeks, as well as physicians and researchers active at a later date.
** Caesium-137 contamination.
Source: UNSCEAR 1988; IAEA 1991.
The Three Mile Island accident is classified as a thermal accident with no reactor runaway, and was the result of a reactor-core coolant failure lasting several hours. The containment shell ensured that only a limited quantity of radioactive material was emitted into the environment, despite the partial destruction of the reactor core (table 2). Although no evacuation order was issued, 200,000 residents voluntarily evacuated the area.
Finally, an accident involving a plutonium production reactor occurred on the west coast of England in 1957 (Windscale, table 2). This accident was caused by a fire in the reactor core and resulted in environmental emissions from a chimney 120 metres high.
Fuel-processing facilities
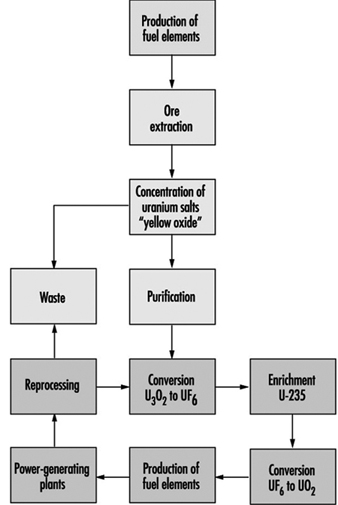
Fuel production facilities are located “upstream” from nuclear reactors and are the site of ore extraction and the physical and chemical transformation of uranium into fissile material suitable for use in reactors (figure 5). The primary accident hazards present in these facilities are chemical in nature and related to the presence of uranium hexafluoride (UF6), a gaseous uranium compound which may decompose upon contact with air to produce hydrofluoric acid (HF), a very corrosive gas.
Figure 5. Nuclear fuel processing cycle.
“Downstream” facilities include fuel storage and reprocessing plants. Four criticality accidents have occurred during chemical reprocessing of enriched uranium or plutonium (Rodrigues 1987). In contrast to accidents occurring at nuclear power plants, these accidents involved small quantities of radioactive materials—tens of kilograms at most—and resulted in negligible mechanical effects and no environmental emission of radioactivity. Exposure was limited to very high dose, very short term (of the order of minutes) external gamma ray and neutron irradiation of workers.
In 1957, a tank containing highly radioactive waste exploded at Russia’s first military-grade plutonium production facility, located in Khyshtym, in the south Ural Mountains. Over 16,000 km2 were contaminated and 740 PBq (20 MCi) were emitted into the atmosphere (table 2 and table 4).
Table 4. Surface area of the contaminated zones and size of population exposed after the Khyshtym accident (Urals 1957), by strontium-90 contamination
|
Contamination ( kBq/m2 ) |
( Ci/km2 ) |
Area ( km2 ) |
Population |
|
≥ 37,000 |
≥ 1,000 |
20 |
1,240 |
|
≥ 3,700 |
≥100 |
120 |
1,500 |
|
≥ 74 |
≥ 2 |
1,000 |
10,000 |
|
≥ 3.7 |
≥ 0.1 |
15,000 |
270,000 |
Research reactors
Hazards at these facilities are similar to those present at nuclear power plants, but are less serious, given the lower power generation. Several criticality accidents involving significant irradiation of personnel have occurred (Rodrigues 1987).
Accidents related to the use of radioactive sources in industry and medicine (excluding nuclear plants) (Zerbib 1993)
The most common accident of this type is the loss of radioactive sources from industrial gamma radiography, used, for example, for the radiographic inspection of joints and welds. However, radioactive sources may also be lost from medical sources (table 5). In either case, two scenarios are possible: the source may be picked up and kept by a person for several hours (e.g., in a pocket), then reported and restored, or it may be collected and carried home. While the first scenario causes local burns, the second may result in long-term irradiation of several members of the general public.
Table 5. Accidents involving the loss of radioactive sources and which resulted in exposure of the general public
|
Country (year) |
Number of |
Number of |
Number of deaths** |
Radioactive material involved |
|
Mexico (1962) |
? |
5 |
4 |
Cobalt-60 |
|
China (1963) |
? |
6 |
2 |
Cobalt 60 |
|
Algeria (1978) |
22 |
5 |
1 |
Iridium-192 |
|
Morocco (1984) |
? |
11 |
8 |
Iridium-192 |
|
Mexico |
≈4,000 |
5 |
0 |
Cobalt-60 |
|
Brazil |
249 |
50 |
4 |
Caesium-137 |
|
China |
≈90 |
12 |
3 |
Cobalt-60 |
|
United States |
≈90 |
1 |
1 |
Iridium-192 |
* Individuals exposed to doses capable of causing acute or long-term effects or death.
** Among individuals receiving high doses.
Source: Nénot 1993.
The recovery of radioactive sources from radiotherapy equipment has resulted in several accidents involving the exposure of scrap workers. In two cases—the Juarez and Goiânia accidents—the general public was also exposed (see table 5 and box below).
The Goiвnia Accident, 1987
Between 21 September and 28 September 1987, several people suffering from vomiting, diarrhoea, vertigo and skin lesions at various parts of the body were admitted to the hospital specializing in tropical diseases in Goiânia, a city of one million inhabitants in the Brazilian state of Goias. These problems were attributed to a parasitic disease common in Brazil. On 28 September, the physician responsible for health surveillance in the city saw a woman who presented him with a bag containing debris from a device collected from an abandoned clinic, and a powder which emitted, according to the woman “a blue light”. Thinking that the device was probably x-ray equipment, the physician contacted his colleagues at the hospital for tropical diseases. The Goias Department of the Environment was notified, and the next day a physicist took measurements in the hygiene department’s yard, where the bag was stored overnight. Very high radioactivity levels were found. In subsequent investigations the source of radioactivity was identified as a caesium-137 source (total activity: approximately 50 TBq (1,375 Ci)) which had been contained within radiotherapy equipment used in a clinic abandoned since 1985. The protective housing surrounding the caesium had been disassembled on 10 September 1987 by two scrapyard workers and the caesium source, in powder form, removed. Both the caesium and the fragments of the contaminated housing were gradually dispersed throughout the city. Several people who had transported or handled the material, or who had simply come to see it (including parents, friends and neighbours) were contaminated. In all, over 100,000 people were examined, of whom 129 were very seriously contaminated; 50 were hospitalized (14 for medullary failure), and 4, including a 6-year-old girl, died. The accident had dramatic economic and social consequences for the entire city of Goiânia and the state of Goias: 1/1000 of the city’s surface area was contaminated, and the price of agricultural produce, rents, real estate, and land all fell. The inhabitants of the entire state suffered real discrimination.
Source: IAEA 1989a
The Juarez accident was discovered serendipitously (IAEA 1989b). On 16 January 1984, a truck entering the Los Alamos (New Mexico, United States) scientific laboratory loaded with steel bars triggered a radiation detector. Investigation revealed the presence of cobalt-60 in the bars and traced the cobalt-60 to a Mexican foundry. On January 21, a heavily contaminated scrapyard in Juarez was identified as the source of the radioactive material. Systematic monitoring of roads and highways by detectors resulted in the identification of a heavily contaminated truck. The ultimate radiation source was determined to be a radiotherapy device stored in a medical centre until December 1983, at which time it was disassembled and transported to the scrapyard. At the scrapyard, the protective housing surrounding the cobalt-60 was broken, freeing the cobalt pellets. Some of the pellets fell into the truck used to transport scrap, and others were dispersed throughout the scrapyard during subsequent operations, mixing with the other scrap.
Accidents involving the entry of workers into active industrial irradiators (e.g., those used to preserve food, sterilize medical products, or polymerize chemicals) have occurred. In all cases, these have been due to failure to follow safety procedures or to disconnected or defective safety systems and alarms. The dose levels of external irradiation to which workers in these accidents were exposed were high enough to cause death. Doses were received within a few seconds or minutes (table 6).
Table 6. Main accidents involving industrial irradiators
|
Site, date |
Equipment* |
Number of |
Exposure level |
Affected organs |
Dose received (Gy), |
Medical effects |
|
Forbach, August 1991 |
EA |
2 |
several deciGy/ |
Hands, head, trunk |
40, skin |
Burns affecting 25–60% of |
|
Maryland, December 1991 |
EA |
1 |
? |
Hands |
55, hands |
Bilateral finger amputation |
|
Viet nam, November 1992 |
EA |
1 |
1,000 Gy/minute |
Hands |
1.5, whole body |
Amputation of the right hand and a finger of the left hand |
|
Italy, May 1975 |
CI |
1 |
Several minutes |
Head, whole body |
8, bone marrow |
Death |
|
San Salvador, February 1989 |
CI |
3 |
? |
Whole body, legs, |
3–8, whole body |
2 leg amputations, 1 death |
|
Israel, June 1990 |
CI |
1 |
1 minute |
Head, whole body |
10–20 |
Death |
|
Belarus, October 1991 |
CI |
1 |
Several minutes |
Whole body |
10 |
Death |
* EA: electron accelerator CI: cobalt-60 irradiator.
Source: Zerbib 1993; Nénot 1993.
Finally, medical and scientific personnel preparing or handling radioactive sources may be exposed through skin and wound contamination or inhalation or ingestion of radioactive materials. It should be noted that this type of accident is also possible in nuclear power plants.
Public Health Aspects of the Problem
Temporal patterns
The United States Radiation Accident Registry (Oak Ridge, United States) is a worldwide registry of radiation accidents involving humans since 1944. To be included in the registry, an accident must have been the subject of a published report and have resulted in whole-body exposure exceeding 0.25 Sievert (Sv), or skin exposure exceeding 6 Sv or exposure of other tissues and organs exceeding 0.75 Sv (see "Case Study: What does dose mean?" for a definition of dose). Accidents that are of interest from the point of view of public health but which resulted in lower exposures are thus excluded (see below for a discussion of the consequences of exposure).
Analysis of the registry data from 1944 to 1988 reveals a clear increase in both the frequency of radiation accidents and the number of exposed individuals starting in 1980 (table 7). The increase in the number of exposed individuals is probably accounted for by the Chernobyl accident, particularly the approximately 135,000 individuals initially residing in the prohibited area within 30 km of the accident site. The Goiânia (Brazil) and Juarez (Mexico) accidents also occurred during this period and involved significant exposure of many people (table 5).
Table 7. Radiation accidents listed in the Oak Ridge (United States) accident registry (worldwide, 1944-88)
|
1944–79 |
1980–88 |
1944–88 |
|
|
Total number of accidents |
98 |
198 |
296 |
|
Number of individuals involved |
562 |
136,053 |
136,615 |
|
Number of individuals exposed to doses exceeding |
306 |
24,547 |
24,853 |
|
Number of deaths (acute effects) |
16 |
53 |
69 |
* 0.25 Sv for whole-body exposure, 6 Sv for skin exposure, 0.75 Sv for other tissues and organs.
Potentially exposed populations
From the point of view of exposure to ionizing radiation, there are two populations of interest: occupationally exposed populations and the general public. United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR 1993) estimates that 4 million workers worldwide were occupationally exposed to ionizing radiation in the period 1985-1989; of these, approximately 20% were employed in the production, use and processing of nuclear fuel (table 8). IAEA member countries were estimated to possess 760 irradiators in 1992, of which 600 were electron accelerators and 160 gamma irradiators.
Table 8. Temporal pattern of occupational exposure to ionizing radiation worldwide (in thousands)
|
Activity |
1975–79 |
1980–84 |
1985–89 |
|
Nuclear fuel processing* |
560 |
800 |
880 |
|
Military applications** |
310 |
350 |
380 |
|
Industrial applications |
530 |
690 |
560 |
|
Medical applications |
1,280 |
1,890 |
2,220 |
|
Total |
2,680 |
3,730 |
4,040 |
* Production and reprocessing of fuel: 40,000; reactor operation: 430,000.
** including 190,000 shipboard personnel.
Source: UNSCEAR 1993.
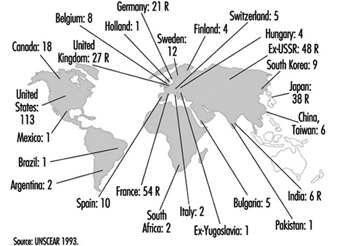
The number of nuclear sites per country is a good indicator of the potential for exposure of the general public (figure 6).
Figure 6. Distribution of power-generating reactors and fuel reprocessing plants in the world, 1989-90
Health Effects
Direct health effects of ionizing radiation
In general, the health effects of ionizing radiation are well known and depend on the dose level received and the dose rate (received dose per unit of time (see "Case Study: What does dose mean?").
Deterministic effects
These occur when the dose exceeds a given threshold and the dose rate is high. The severity of the effects is proportional to the dose, although the dose threshold is organ specific (table 9).
Table 9. Deterministic effects: thresholds for selected organs
|
Tissue or effect |
Equivalent single dose |
|
Testicles: |
|
|
Temporary sterility |
0.15 |
|
Permanent sterility |
3.5–6.0 |
|
Ovaries: |
|
|
Sterility |
2.5–6.0 |
|
Crystalline lens: |
|
|
Detectable opacities |
0.5–2.0 |
|
Impaired vision (cataracts) |
5.0 |
|
Bone marrow: |
|
|
Depression of haemopoiesis |
0.5 |
Source: ICRP 1991.
In the accidents such as those discussed above, deterministic effects may be caused by local intense irradiation, such as that caused by external irradiation, direct contact with a source (e.g., a misplaced source picked up and pocketed) or skin contamination. All these result in radiological burns. If the local dose is of the order of 20 to 25 Gy (table 6, "Case Study: What does dose mean?") tissue necrosis may ensue. A syndrome known as acute irradiation syndrome, characterized by digestive disorders (nausea, vomiting, diarrhoea) and bone marrow aplasia of variable severity, may be induced when the average whole-body irradiation dose exceeds 0.5 Gy. It should be recalled that whole-body and local irradiation may occur simultaneously.
Nine of 60 workers exposed during criticality accidents at nuclear fuel processing plants or research reactors died (Rodrigues 1987). Decedents received 3 to 45 Gy, while survivors received 0.1 to 7 Gy. The following effects were observed in survivors: acute irradiation syndrome (gastro-intestinal and haematological effects), bilateral cataracts and necrosis of limbs, requiring amputation.
At Chernobyl, power plant personnel, as well as emergency response personnel not using special protective equipment, suffered high beta and gamma radiation exposure in the initial hours or days following the accident. Five hundred people required hospitalization; 237 individuals who received whole-body irradiation exhibited acute irradiation syndrome, and 28 individuals died despite treatment (table 10) (UNSCEAR 1988). Others received local irradiation of the limbs, in some cases affecting over 50% of the body surface and continue to suffer, many years later, multiple skin disorders (Peter, Braun-Falco and Birioukov 1994).
Table 10. Distribution of patients exhibiting acute irradiation syndrome (AIS) after the Chernobyl accident, by severity of condition
|
Severity of AIS |
Equivalent dose |
Number of |
Number of |
Average survival |
|
I |
1–2 |
140 |
– |
– |
|
II |
2–4 |
55 |
1 (1.8) |
96 |
|
III |
4–6 |
21 |
7 (33.3) |
29.7 |
|
IV |
>6 |
21 |
20 (95.2) |
26.6 |
Source: UNSCEAR 1988.
Stochastic effects
These are probabilistic in nature (i.e., their frequency increases with received dose), but their severity is independent of dose. The main stochastic effects are:
- Mutation. This has been observed in animal experiments but has been difficult to document in humans.
- Cancer. The effect of irradiation on the risk of developing cancer has been studied in patients receiving radiation therapy and in survivors of the Hiroshima and Nagasaki bombings. UNSCEAR (1988, 1994) regularly summarizes the results of these epidemiological studies. The duration of the latency period is typically 5 to 15 years from the date of exposure depending on organ and tissue. Table 11 lists the cancers for which an association with ionizing radiation has been established. Significant cancer excesses have been demonstrated among survivors of the Hiroshima and Nagasaki bombings with exposures above 0.2 Sv.
- Selected benign tumours. Benign thyroid adenomas.
Table 11. Results of epidemiological studies of the effect of high dose rate of external irradiation on cancer
|
Cancer site |
Hiroshima/Nagasaki |
Other studies |
|
|
Mortality |
Incidence |
||
|
Haematopoietic system |
|||
|
Leukaemia |
+* |
+* |
6/11 |
|
Lymphoma (not specified) |
+ |
0/3 |
|
|
Non-Hodgkin lymphoma |
+* |
1/1 |
|
|
Myeloma |
+ |
+ |
1/4 |
|
Oral cavity |
+ |
+ |
0/1 |
|
Salivary glands |
+* |
1/3 |
|
|
Digestive system |
|||
|
Oesophagus |
+* |
+ |
2/3 |
|
Stomach |
+* |
+* |
2/4 |
|
Small intestine |
1/2 |
||
|
Colon |
+* |
+* |
0/4 |
|
Rectum |
+ |
+ |
3/4 |
|
Liver |
+* |
+* |
0/3 |
|
Gall bladder |
0/2 |
||
|
Pancreas |
3/4 |
||
|
Respiratory system |
|||
|
Larynx |
0/1 |
||
|
Trachea, bronchi, lungs |
+* |
+* |
1/3 |
|
Skin |
|||
|
Not specified |
1/3 |
||
|
Melanoma |
0/1 |
||
|
Other cancers |
+* |
0/1 |
|
|
Breast (women) |
+* |
+* |
9/14 |
|
Reproductive system |
|||
|
Uterus (non-specific) |
+ |
+ |
2/3 |
|
Uterine body |
1/1 |
||
|
Ovaries |
+* |
+* |
2/3 |
|
Other (women) |
2/3 |
||
|
Prostate |
+ |
+ |
2/2 |
|
Urinary system |
|||
|
Bladder |
+* |
+* |
3/4 |
|
Kidneys |
0/3 |
||
|
Other |
0/1 |
||
|
Central nervous system |
+ |
+ |
2/4 |
|
Thyroid |
+* |
4/7 |
|
|
Bone |
2/6 |
||
|
Connective tissue |
0/4 |
||
|
All cancers, excluding leukaemias |
1/2 |
||
+ Cancer sites studied in the Hiroshima and Nagasaki survivors.
* Positive association with ionizing radiation.
1 Cohort (incidence or mortality) or case-control studies.
Source: UNSCEAR 1994.
Two important points concerning the effects of ionizing radiation remain controversial.
Firstly, what are the effects of low-dose irradiation (below 0.2 Sv) and low dose rates? Most epidemiological studies have examined survivors of the Hiroshima and Nagasaki bombings or patients receiving radiation therapy—populations exposed over very short periods to relatively high doses—and estimates of the risk of developing cancer as a result of exposure to low doses and dose rates depends essentially on extrapolations from these populations. Several studies of nuclear power plant workers, exposed to low doses over several years, have reported cancer risks for leukaemia and other cancers that are compatible with extrapolations from high-exposure groups, but these results remain unconfirmed (UNSCEAR 1994; Cardis, Gilbert and Carpenter 1995).
Secondly, is there a threshold dose (i.e., a dose below which there is no effect)? This is currently unknown. Experimental studies have demonstrated that damage to genetic material (DNA) caused by spontaneous errors or environmental factors are constantly repaired. However, this repair is not always effective, and may result in malignant transformation of cells (UNSCEAR 1994).
Other effects
Finally, the possibility of teratogenic effects due to irradiation during pregnancy should be noted. Microcephaly and mental retardation have been observed in children born to female survivors of the Hiroshima and Nagasaki bombings who received irradiation of at least 0.1 Gy during the first trimester (Otake, Schull and Yoshimura 1989; Otake and Schull 1992). It is unknown whether these effects are deterministic or stochastic, although the data do suggest the existence of a threshold.
Effects observed following the Chernobyl accident
The Chernobyl accident is the most serious nuclear accident to have occurred to date. However, even now, ten years after the fact, not all the health effects on the most highly exposed populations have been accurately evaluated. There are several reasons for this:
- Some effects appear only many years after the date of exposure: for example, solid-tissue cancers typically take 10 to 15 years to appear.
- As some time elapsed between the accident and the commencement of epidemiological studies, some effects occurring in the initial period following the accident may not have been detected.
- Useful data for the quantification of the cancer risk were not always gathered in a timely fashion. This is particularly true for data necessary to estimate the exposure of the thyroid gland to radioactive iodides emitted during the incident (tellurium-132, iodine-133) (Williams et al. 1993).
- Finally, many initially exposed individuals subsequently left the contaminated zones and were probably lost for follow-up.
Workers. Currently, comprehensive information is unavailable for all the workers who were strongly irradiated in the first few days following the accident. Studies on the risk to clean-up and relief workers of developing leukaemia and solid-tissue cancers are in progress (see table 3). These studies face many obstacles. Regular follow-up of the health status of clean-up and relief workers is greatly hindered by the fact that many of them came from different parts of the ex-USSR and were redispatched after working on the Chernobyl site. Further, received dose must be estimated retrospectively, as there are no reliable data for this period.
General population. The only effect plausibly associated with ionizing radiation in this population to date is an increase, starting in 1989, of the incidence of thyroid cancer in children younger than 15 years. This was detected in Byelorussia (Belarus) in 1989, only three years after the incident, and has been confirmed by several expert groups (Williams et al. 1993). The increase was particularly noteworthy in the most heavily contaminated areas of Belarus, especially the Gomel region. While thyroid cancer was normally rare in children younger than 15 years, (annual incidence rate of 1 to 3 per million), its incidence increased tenfold on a national basis and twentyfold in the Gomel area (table 12, figure 7), (Stsjazhko et al. 1995). A tenfold increase of the incidence of thyroid cancer was subsequently reported in the five most heavily contaminated areas of Ukraine, and an increase in thyroid cancer was also reported in the Bryansk (Russia) region (table 12). An increase among adults is suspected but has not been confirmed. Systematic screening programmes undertaken in the contaminated regions allowed latent cancers present prior to the accident to be detected; ultrasonographic programmes capable of detecting thyroid cancers as small as a few millimetres were particularly helpful in this regard. The magnitude of the increase in incidence in children, taken together with the aggressiveness of the tumours and their rapid development, suggests that the observed increases in thyroid gland cancer are partially due to the accident.
Table 12. Temporal pattern of the incidence and total number of thyroid cancers in children in Belarus, Ukraine & Russia, 1981-94
|
Incidence* (/100,000) |
Number of cases |
|||
|
1981–85 |
1991–94 |
1981–85 |
1991–94 |
|
|
Belarus |
||||
|
Entire country |
0.3 |
3.06 |
3 |
333 |
|
Gomel area |
0.5 |
9.64 |
1 |
164 |
|
Ukraine |
||||
|
Entire country |
0.05 |
0.34 |
25 |
209 |
|
Five most heavily |
0.01 |
1.15 |
1 |
118 |
|
Russia |
||||
|
Entire country |
? |
? |
? |
? |
|
Bryansk and |
0 |
1.00 |
0 |
20 |
* Incidence: the ratio of the number of new cases of a disease during a given period to the size of the population studied in the same period.
Source: Stsjazhko et al. 1995.
Figure 7. Incidence of cancer of the thyroid in children younger than 15 years in Belarus

In the most heavily contaminated zones (e.g., the Gomel region), the thyroid doses were high, particularly among children (Williams et al. 1993). This is consistent with the significant iodine emissions associated with the accident and the fact that radioactive iodine will, in the absence of preventive measures, concentrate preferentially in the thyroid gland.
Exposure to radiation is a well-documented risk factor for thyroid cancer. Clear increases in the incidence of thyroid cancer have been observed in a dozen studies of children receiving radiation therapy to the head and neck. In most cases, the increase was clear ten to 15 years after exposure, but was detectable in some cases within three to seven years. On the other hand, the effects in children of internal irradiation by iodine-131 and by short half-life iodine isotopes are not well established (Shore 1992).
The precise magnitude and pattern of the increase in the coming years of the incidence of thyroid cancer in the most highly exposed populations should be studied. Epidemiological studies currently under way should help to quantify the association between the dose received by the thyroid gland and the risk of developing thyroid cancer, and to identify the role of other genetic and environmental risk factors. It should be noted that iodine deficiency is widespread in the affected regions.
An increase in the incidence of leukaemia, particularly juvenile leukaemia (since children are more sensitive to the effects of ionizing radiation), is to be expected among the most highly exposed members of the population within five to ten years of the accident. Although no such increase has yet been observed, the methodological weaknesses of the studies conducted to date prevent any definitive conclusions from being drawn.
Psychosocial effects
The occurrence of more or less severe chronic psychological problems following psychological trauma is well established and has been studied primarily in populations faced with environmental disasters such as floods, volcanic eruptions and earthquakes. Post-traumatic stress is a severe, long-lasting and crippling condition (APA 1994).
Most of our knowledge on the effect of radiation accidents on psychological problems and stress is drawn from studies conducted in the wake of the Three Mile Island accident. In the year following the accident, immediate psychological effects were observed in the exposed population, and mothers of young children in particular exhibited increased sensitivity, anxiety and depression (Bromet et al. 1982). Further, an increase in depression and anxiety-related problems was observed in power-plant workers, compared to workers in another power plant (Bromet et al. 1982). In the following years (i.e., after the reopening of the power plant), approximately one-quarter of the surveyed population exhibited relatively significant psychological problems. There was no difference in the frequency of psychological problems in the rest of the survey population, compared to control populations (Dew and Bromet 1993). Psychological problems were more frequent among individuals living close to the power plant who were without a social support network, had a history of psychiatric problems, or who had evacuated their home at the time of the accident (Baum, Cohen and Hall 1993).
Studies are also under way among populations exposed during the Chernobyl accident and for whom stress appears to be an important public health issue (e.g., clean-up and relief workers and individuals living in a contaminated zone). For the moment, however, there are no reliable data on the nature, severity, frequency and distribution of psychological problems in the target populations. The factors that must be taken into account when evaluating the psychological and social consequences of the accident on residents of the contaminated zones include the harsh social and economic situation, the diversity of the available compensation systems, the effects of evacuation and resettlement (approximately 100,000 additional people were resettled in the years following the accident), and the effects of lifestyle limitations (e.g., modification of nutrition).
Principles of Prevention and Guidelines
Safety principles and guidelines
Industrial and medical use of radioactive sources
While it is true that the major radiation accidents reported have all occurred at nuclear power plants, the use of radioactive sources in other settings has nevertheless resulted in accidents with serious consequences for workers or the general public. The prevention of accidents such as these is essential, especially in light of the disappointing prognosis in cases of high-dose exposure. Prevention depends on proper worker training and on the maintenance of a comprehensive life-cycle inventory of radioactive sources which includes information on both the sources’ nature and location. The IAEA has established a series of safety guidelines and recommendations for the use of radioactive sources in industry, medicine and research (Safety Series No. 102). The principles in question are similar to those presented below for nuclear power plants.
Safety in nuclear power plants (IAEA Safety Series No. 75, INSAG-3)
The goal here is to protect both humans and the environment from the emission of radioactive materials under any circumstance. To this end, it is necessary to apply a variety of measures throughout the design, construction, operation and decommissioning of nuclear power plants.
The safety of nuclear power plants is fundamentally dependent on the “defence in depth” principle—that is, the redundancy of systems and devices designed to compensate for technical or human errors and deficiencies. Concretely, radioactive materials are separated from the environment by a series of successive barriers. In nuclear power production reactors, the last of these barriers is the containment structure (absent on the Chernobyl site but present at Three Mile Island). To avoid the breakdown of these barriers and to limit the consequences of breakdowns, the following three safety measures should be practised throughout the power plant’s operational life: control of the nuclear reaction, cooling of fuel, and containment of radioactive material.
Another essential safety principle is “operating experience analysis”—that is, using information gleaned from events, even minor ones, occurring at other sites to increase the safety of an existing site. Thus, analysis of the Three Mile Island and Chernobyl accidents has resulted in the implementation of modifications designed to ensure that similar accidents do not occur elsewhere.
Finally, it should be noted that significant efforts have been expended to promote a culture of safety, that is, a culture that is continually responsive to safety concerns related to the plant’s organization, activities and practices, as well as to individual behaviour. To increase the visibility of incidents and accidents involving nuclear power plants, an international scale of nuclear events (INES), identical in principle to scales used to measure the severity of natural phenomena such as earthquakes and wind, has been developed (table 12). This scale is not however suitable for the evaluation of a site’s safety or for performing international comparisons.
Table 13. International scale of nuclear incidents
|
Level |
Offsite |
Onsite |
Protective structure |
|
7—Major accident |
Major emission, |
||
|
6—Serious accident |
Significant emission, |
||
|
5—Accident |
Limited emission, |
Serious damage to |
|
|
4—Accident |
Low emission, public |
Damage to reactors |
|
|
3—Serious incident |
Very low emission, |
Serious |
Accident barely avoided |
|
2—Incident |
Serious contamination |
Serious failures of safety measures |
|
|
1—Abnormality |
Abnormality beyond |
||
|
0—Disparity |
No significance from |
Principles of the protection of the general public from exposure to radiation
In cases involving the potential exposure of the general public, it may be necessary to apply protective measures designed to prevent or limit exposure to ionizing radiation; this is particularly important if deterministic effects are to be avoided. The first measures which should be applied in emergency are evacuation, sheltering and administration of stable iodine. Stable iodine should be distributed to exposed populations, since this will saturate the thyroid and inhibit its uptake of radioactive iodine. To be effective, however, thyroid saturation must occur before or soon after the start of exposure. Finally, temporary or permanent resettlement, decontamination, and control of agriculture and food may eventually be necessary.
Each of these countermeasures has its own “action level” (table 14), not to be confused with the ICRP dose limits for workers and the general public, developed to ensure adequate protection in cases of non-accidental exposure (ICRP 1991).
Table 14. Examples of generic intervention levels for protective measures for general population
|
Protective measure |
Intervention level (averted dose) |
|
Emergency |
|
|
Containment |
10 mSv |
|
Evacuation |
50 mSv |
|
Distribution of stable iodine |
100 mGy |
|
Delayed |
|
|
Temporary resettlement |
30 mSv in 30 days; 10 mSv in the next 30 days |
|
Permanent resettlement |
1 Sv lifetime |
Source: IAEA 1994.
Research Needs and Future Trends
Current safety research concentrates on improving the design of nuclear power-generating reactors—more specifically, on the reduction of the risk and effects of core meltdown.
The experience gained from previous accidents should lead to improvements in the therapeutic management of seriously irradiated individuals. Currently, the use of bone marrow cell growth factors (haematopoietic growth factors) in the treatment of radiation-induced medullary aplasia (developmental failure) is being investigated (Thierry et al. 1995).
The effects of low doses and dose rates of ionizing radiation remains unclear and needs to be clarified, both from a purely scientific point of view and for the purposes of establishing dose limits for the general public and for workers. Biological research is necessary to elucidate the carcinogenic mechanisms involved. The results of large-scale epidemiological studies, especially those currently under way on workers at nuclear power plants, should prove useful in improving the accuracy of cancer risk estimates for populations exposed to low doses or dose rates. Studies on populations which are or have been exposed to ionizing radiation due to accidents should help further our understanding of the effects of higher doses, often delivered at low dose rates.
The infrastructure (organization, equipment and tools) necessary for the timely collection of data essential for the evaluation of the health effects of radiation accidents must be in place well in advance of the accident.
Finally, extensive research is necessary to clarify the psychological and social effects of radiation accidents (e.g., the nature and frequency of, and risk factors for, pathological and non-pathological post-traumatic psychological reactions). This research is essential if the management of both occupationally and non-occupationally exposed populations is to be improved.
Transportation of Hazardous Material: Chemical and Radioactive
The industries and economies of nations depend, in part, on the large numbers of hazardous materials transported from the supplier to the user and, ultimately, to the waste disposer. Hazardous materials are transported by road, rail, water, air and pipeline. The vast majority reach their destination safely and without incident. The size and scope of the problem is illustrated by the petroleum industry. In the United Kingdom it distributes around 100 million tons of product every year by pipeline, rail, road and water. Approximately 10% of those employed by the UK chemical industry are involved in distribution (i.e., transport and warehousing).
A hazardous material can be defined as “a substance or material determined to be capable of posing an unreasonable risk to health, safety or property when transported”. “Unreasonable risk” covers a broad spectrum of health, fire and environmental considerations. These substances include explosives, flammable gases, toxic gases, highly flammable liquids, flammable liquids, flammable solids, substances which become dangerous when wet, oxidizing substances and toxic liquids.
The risks arise directly from a release, ignition, and so on, of the dangerous substance(s) being transported. Road and rail threats are those which could give rise to major accidents “which could affect both employees and members of the public”. These dangers can occur when materials are being loaded or unloaded or are en route. The population at risk is people living near the road or railway and the people in other road vehicles or trains who might become involved in a major accident. Areas of risk include temporary stopover points such as railway marshalling yards and lorry parking areas at motorway service points. Marine risks are those linked to ships entering or leaving ports and loading or discharging cargoes there; risks also arise from coastal and straits traffic and inland waterways.
The range of incidents which can occur in association with transport both while in transit and at fixed installations include chemical overheating, spillage, leakage, escape of vapour or gas, fire and explosion. Two of the principal events causing incidents are collision and fire. For road tankers other causes of release may be leaks from valves and from overfilling. Generally, for both road and rail vehicles, non-crash fires are much more frequent than crash fires. These transport-associated incidents can occur in rural, urban industrial and urban residential areas, and can involve both attended and unattended vehicles or trains. Only in the minority of cases is an accident the primary cause of the incident.
Emergency personnel should be aware of the possibility of human exposure and contamination by a hazardous substance in accidents involving railways and rail yards, roads and freight terminals, vessels (both ocean and inland based) and associated waterfront warehouses. Pipelines (both long distance and local utility distribution systems) can be a hazard if damage or leakage occurs, either in isolation or in association with other incidents. Transportation incidents are often more dangerous than those at fixed facilities. The materials involved may be unknown, warning signs may be obscured by rollover, smoke or debris, and knowledgeable operatives may be absent or casualties of the event. The number of people exposed depends on population density, both by day and night, on the proportions indoors and outdoors, and on the proportion who may be considered particularly vulnerable. In addition to the population who are normally in the area, personnel of the emergency services who attend the accident are also at risk. It is not uncommon in an incident involving transport of hazardous materials that a significant proportion of the casualties include such personnel.
In the 20-year period 1971 through 1990, about 15 people were killed on the roads of the United Kingdom because of dangerous chemicals, compared with the annual average of 5,000 persons every year in motor accidents. However, small quantities of dangerous goods can cause significant damage. International examples include:
- A plane crashed near Boston, USA, because of leaking nitric acid.
- Over 200 people were killed when a road tanker of propylene exploded over a campsite in Spain.
- In a rail accident involving 22 rail cars of chemicals in Mississauga, Canada, a tanker containing 90 tonnes of chlorine was ruptured and there was an explosion and a large fire. There were no fatalities, but 250,000 persons were evacuated.
- A rail collision alongside the motorway in Eccles, United Kingdom, resulted in three deaths and 68 injuries from the collision, but none from the resulting serious fire of the petroleum products being transported.
- A petrol tanker went out of control in Herrborn, Germany, burning down a large part of the town.
- In Peterborough, United Kingdom, a vehicle carrying explosives killed one person and almost destroyed an industrial centre.
- A petrol tanker exploded in Bangkok, Thailand, killing a large number of people.
The largest number of serious incidents have arisen with flammable gas or liquids (partially related to the volumes moved), with some incidents from toxic gases and toxic fumes (including products of combustion).
Studies in the UK have shown the following for road transport:
- frequency of accident while conveying hazardous materials: 0.12 x 10–6/km
- frequency of release while conveying hazardous materials: 0.027 x 10–6/km
- probability of a release given a traffic accident: 3.3%.
These events are not synonymous with hazardous material incidents involving vehicles, and may constitute only a small proportion of the latter. There is also the individuality of accidents involving the road transport of hazardous materials.
International agreements covering the transport of potentially hazardous materials include:
Regulations for the Safe Transport of Radioactive Material 1985 (as amended 1990): International Atomic Energy Agency, Vienna, 1990 (STI/PUB/866). Their purpose is to establish standards of safety which provide an acceptable level of control of the radiation hazards to persons, property and the environment that are associated with the transport of radioactive material.
The International Convention for the Safety of Life at Sea 1974 (SOLAS 74). This sets basic safety standards for all passenger and cargo ships, including ships carrying hazardous bulk cargoes.
The International Convention for the Prevention of Pollution from Ships 1973, as modified by the Protocol of 1978 (MARPOL 73/78). This provides regulations for the prevention of pollution by oil, noxious liquid substances in bulk, pollutants in packaged form or in freight containers, portable tanks or road and rail wagons, sewage and garbage. Regulation requirements are amplified in the International Maritime Dangerous Goods Code.
There is a substantial body of international regulation of the transportation of harmful substances by air, rail, road and sea (converted into national legislation in many countries). Most are based on standards sponsored by the United Nations, and cover the principles of identification, labelling, prevention and mitigation. The United Nations Committee of Experts on the Transport of Dangerous Goods has produced Recommendations on the Transport of Dangerous Goods. They are addressed to governments and international organizations concerned with the regulation of the transport of dangerous goods. Among other aspects, the recommendations cover principles of classification and definitions of classes, listing of the content of dangerous goods, general packing requirements, testing procedures, making, labelling or placarding, and transport documents. These recommendations—the “Orange Book”—do not have the force of law, but form the basis of all the international regulations. These regulations are generated by various organizations:
- the International Civil Aviation Organization: Technical Instructions for Safe Transport of Dangerous Goods by Air (Tis)
- the International Maritime Organization: International Maritime Dangerous Goods Code (IMDG Code)
- the European Economic Community: The European Agreement Concerning the International Carriage of Dangerous Goods by Road (ADR)
- the Office of International Rail Transport: Regulations Concerning the International Carriage of Dangerous Goods by Rail (RID).
The preparation of major emergency plans to deal with and mitigate the effects of a major accident involving dangerous substances is as much needed in the transportation field as for fixed installations. The planning task is made more difficult in that the location of an incident will not be known in advance, thus requiring flexible planning. The substances involved in a transport accident cannot be foreseen. Because of the nature of the incident a number of products may be mixed together at the scene, causing considerable problems to the emergency services. The incident may occur in an area which is highly urbanized, remote and rural, heavily industrialized, or commercialized. An added factor is the transient population who may be unknowingly involved in an event because the accident has caused a backlog of vehicles either on the public highway or where passenger trains are stopped in response to a rail incident.
There is therefore a necessity for the development of local and national plans to respond to such events. These must be simple, flexible and easily understood. As major transport accidents can occur in a multiplicity of locations the plan must be appropriate to all potential scenes. For the plan to work effectively at all times, and in both remote rural and heavily populated urban locales, all organizations contributing to the response must have the ability to maintain flexibility while conforming to the basic principles of the overall strategy.
The initial responders should obtain as much information as possible to try to identify the hazard involved. Whether the incident is a spillage, a fire, a toxic release, or a combination of these will determine responses. The national and international marking systems used to identify vehicles transporting hazardous substances and carrying hazardous packaged goods should be known to the emergency services, who should have access to one of the several national and international databases which can help to identify the hazard and the problems associated with it.
Rapid control of the incident is vital. The chain of command must be identified clearly. This may change during the course of the event from the emergency services through the police to the civil government of the affected area. The plan must be able to recognize the effect on the population, both those working in or resident in the potentially affected area and those who may be transients. Sources of expertise on public health matters should be mobilized to advise on both the immediate management of the incident and on the potential for longer-term direct health effects and indirect ones through the food chain. Contact points for obtaining advice on environmental pollution to water courses and so on, and the effect of weather conditions on the movement of gas clouds must be identified. Plans must identify the possibility of evacuation as one of the response measures.
However, the proposals must be flexible, as there may be a range of costs and benefits, both in incident management and in public health terms, which will have to be considered. The arrangements must outline clearly the policy with respect to keeping the media fully informed and the action being taken to mitigate the effects. The information must be accurate and timely, with the spokesperson being knowledgeable as to the overall response and having access to experts to respond to specialized queries. Poor media relations can disrupt the management of the event and lead to unfavourable and sometimes unjustified comments on the overall handling of the episode. Any plan must include adequate mock disaster drills. These enable the responders to and managers of an incident to learn each other’s personal and organizational strengths and weaknesses. Both table-top and physical exercises are required.
Although the literature dealing with chemical spills is extensive, only a minor part describes the ecological consequences. Most concern case studies. The descriptions of actual spills have focused on human health and safety problems, with ecological consequences described only in general terms. The chemicals enter the environment predominantly through the liquid phase. In only a few cases did accidents having ecological consequences also affect humans immediately, and the effects on the environment were not caused by identical chemicals or by identical release routes.
Controls to prevent risk to human health and life from the transport of hazardous materials include quantities carried, direction and control of means of transport, routing, as well as authority over interchange and concentration points and developments near such areas. Further research is required into risk criteria, quantification of risk, and risk equivalence. The United Kingdom Health and Safety Executive has developed a Major Incident Data Service (MHIDAS) as a database of major chemical incidents worldwide. It currently holds information on over 6,000 incidents.
Case Study: Transport of Hazardous Materials
An articulated road tanker carrying about 22,000 litres of toluene was travelling on a main arterial road which runs through Cleveland, UK. A car pulled into the path of the vehicle, and, as the truckdriver took evasive action, the tanker overturned. The manlids of all five compartments sprang open and toluene spilled on the roadway and ignited, resulting in a pool fire. Five cars travelling on the opposite carriageway were involved in the fire but all occupants escaped.
The fire brigade arrived within five minutes of being called. Burning liquid had entered the drains, and drain fires were evident approximately 400m from the main incident. The County Emergency Plan was put into action, with social services and public transport put on alert in case evacuation was needed. Initial action by the fire brigade concentrated on extinguishing car fires and searching for occupants. The next task was identifying an adequate water supply. A member of the chemical company’s safety team arrived to coordinate with the police and fire commanders. Also in attendance were staff from the ambulance service and the environmental health and water boards. Following consultation it was decided to permit the leaking toluene to burn rather than extinguish the fire and have the chemical emitting vapours. Police put out warnings over a four-hour period utilizing national and local radio, advising people to stay indoors and close their windows. The road was closed for eight hours. When the toluene fell below the level of the manlids, the fire was extinguished and the remaining toluene removed from the tanker. The incident was concluded approximately 13 hours after the accident.
Potential harm to humans existed from thermal radiation; to the environment, from air, soil and water pollution; and to the economy, from traffic disruption. The company plan which existed for such a transportation incident was activated within 15 minutes, with five persons in attendance. A county offsite plan existed and was instigated with a control centre coming into being involving police and the fire brigade. Concentration measurement but not dispersion prediction was performed. The fire brigade response involved over 50 persons and ten appliances, whose major actions were fire-fighting, washing down and spillage retention. Over 40 police officers were committed in traffic direction, warning the public, security and press control. The health service response encompassed two ambulances and two onsite medical staff. Local government reaction involved environmental health, transport and social services. The public were informed of the incident by loudspeakers, radio and word of mouth. The information focused on what to do, especially on sheltering indoors.
The outcome to humans was two admissions to a single hospital, a member of the public and a company employee, both injured in the crash. There was noticeable air pollution but only slight soil and water contamination. From an economic perspective there was major damage to the road and extensive traffic delays, but no loss of crops, livestock or production. Lessons learned included the value of rapid retrieval of information from the Chemdata system and the presence of a company technical expert enabling correct immediate action to be taken. The importance of joint press statements from responders was highlighted. Consideration needs to be given to the environmental impact of fire-fighting. If the fire had been fought in the initial stages, a considerable amount of contaminated liquid (firewater and toluene) potentially could have entered the drains, water supplies and soil.
Avalanches: Hazards and Protective Measures
Ever since people began to settle in mountainous regions, they have been exposed to the specific hazards associated with mountain living. Among the most treacherous hazards are avalanches and landslides, which have taken their toll of victims even up to the present day.
When the mountains are covered with several feet of snow in winter, under certain conditions, a mass of snow lying like a thick blanket on the steep slopes or mountain tops can become detached from the ground underneath and slide downhill under its own weight. This can result in huge quantities of snow hurtling down the most direct route and settling into the valleys below. The kinetic energy thus released produces dangerous avalanches, which sweep away, crush or bury everything in their path.
Avalanches can be divided into two categories according to the type and condition of the snow involved: dry snow or “dust” avalanches, and wet snow or “ground” avalanches. The former are dangerous because of the shock waves they set off, and the latter because of their sheer volume, due to the added moisture in the wet snow, flattening everything as the avalanche rolls downhill, often at high speeds, and sometimes carrying away sections of the subsoil.
Particularly dangerous situations can arise when the snow on large, exposed slopes on the windward side of the mountain is compacted by the wind. Then it often forms a cover, held together only on the surface, like a curtain suspended from above, and resting on a base that can produce the effect of ball-bearings. If a “cut” is made in such a cover (e.g., if a skier leaves a track across the slope), or if for any reason, this very thin cover is torn apart (e.g., by its own weight), then the whole expanse of snow can slide downhill like a board, usually developing into an avalanche as it progresses.
In the interior of the avalanche, enormous pressure can build up, which can carry off, smash or crush locomotives or entire buildings as though they were toys. That human beings have very little chance of surviving in such an inferno is obvious, bearing in mind that anyone who is not crushed to death is likely to die from suffocation or exposure. It is not surprising, therefore, in cases where people have been buried in avalanches, that, even if they are found immediately, about 20% of them are already dead.
The topography and vegetation of the area will cause the masses of snow to follow set routes as they come down to the valley. People living in the region know this from observation and tradition, and therefore keep away from these danger zones in the winter.
In earlier times, the only way to escape such dangers was to avoid exposing oneself to them. Farmhouses and settlements were built in places where topographical conditions were such that avalanches could not occur, or which years of experience had shown to be far removed from any known avalanche paths. People even avoided the mountain areas altogether during the danger period.
Forests on the upper slopes also afford considerable protection against such natural disasters, as they support the masses of snow in the threatened areas and can curb, halt or divert avalanches that have already started, provided they have not built up too much momentum.
Nevertheless, the history of mountainous countries is punctuated by repeated disasters caused by avalanches, which have taken, and still take, a heavy toll of life and property. On the one hand, the speed and momentum of the avalanche is often underestimated. On the other hand, avalanches will sometimes follow paths which, on the basis of centuries of experience, have not previously been considered to be avalanche paths. Certain unfavourable weather conditions, in conjunction with a particular quality of snow and the state of the ground underneath (e.g., damaged vegetation or erosion or loosening of the soil as a result of heavy rains) produce circumstances that can lead to one of those “disasters of the century”.
Whether an area is particularly exposed to the threat of an avalanche depends not only on prevailing weather conditions, but to an even greater extent on the stability of the snow cover, and on whether the area in question is situated in one of the usual avalanche paths or outlets. There are special maps showing areas where avalanches are known to have occurred or are likely to occur as a result of topographical features, especially the paths and outlets of frequently occurring avalanches. Building is prohibited in high-risk areas.
However, these precautionary measures are no longer sufficient today, as, despite the prohibition of building in particular areas, and all the information available on the dangers, increasing numbers of people are still attracted to picturesque mountain regions, causing more and more building even in areas known to be dangerous. In addition to this disregard or circumvention of building bans, one of the manifestations of the modern leisure society is that thousands of tourists go to the mountains for sport and recreation in winter, and to the very areas where avalanches are virtually pre-programmed. The ideal ski slope is steep, free of obstacles and should have a sufficiently thick carpet of snow—ideal conditions for the skier, but also for the snow to sweep down into the valley.
If, however, risks cannot be avoided or are to a certain extent consciously accepted as an unwelcome “side-effect” of the enjoyment gained from the sport, then it becomes necessary to develop ways and means of coping with these dangers in another manner.
To improve the chances of survival for people buried in avalanches, it is essential to provide well-organized rescue services, emergency telephones near the localities at risk and up-to-date information for the authorities and for tourists on the prevailing situation in dangerous areas. Early warning systems and excellent organization of rescue services with the best possible equipment can considerably increase chances of survival for people buried in avalanches, as well as reducing the extent of the damage.
Protective Measures
Various methods of protection against avalanches have been developed and tested all over the world, such as cross-frontier warning services, barriers and even the artificial triggering-off of avalanches by blasting or firing guns over the snow fields.
The stability of the snow cover is basically determined by the ratio of mechanical stress to density. This stability can vary considerably according to the type of stress (e.g., pressure, tension, shearing strain) within a geographical region (e.g., that part of the snow field where an avalanche might start). Contours, sunshine, winds, temperature and local disturbances in the structure of the snow cover—resulting from rocks, skiers, snowploughs or other vehicles—can also affect stability. Stability can therefore be reduced by deliberate local intervention such as blasting, or increased by the installation of additional supports or barriers. These measures, which can be of a permanent or temporary nature, are the two main methods used for protection against avalanches.
Permanent measures include effective and durable structures, support barriers in the areas where the avalanche might start, diversionary or braking barriers on the avalanche path, and blocking barriers in the avalanche outlet area. The object of temporary protective measures is to secure and stabilize the areas where an avalanche might start by deliberately triggering off smaller, limited avalanches to remove the dangerous quantities of snow in sections.
Support barriers artificially increase the stability of the snow cover in potential avalanche areas. Drift barriers, which prevent additional snow from being carried by the wind to the avalanche area, can reinforce the effect of support barriers. Diversionary and braking barriers on the avalanche path and blocking barriers in the avalanche outlet area can divert or slow down the descending mass of snow and shorten the outflow distance in front of the area to be protected. Support barriers are structures fixed in the ground, more or less perpendicular to the slope, which put up sufficient resistance to the descending mass of snow. They must form supports reaching up to the surface of the snow. Support barriers are usually arranged in several rows and must cover all parts of the terrain from which avalanches could, under various possible weather conditions, threaten the locality to be protected. Years of observation and snow measurement in the area are required in order to establish correct positioning, structure and dimensions.
The barriers must have a certain permeability to let minor avalanches and surface landslides flow through a number of barrier rows without getting larger or causing damage. If permeability is not sufficient, there is the danger that the snow will pile up behind the barriers, and subsequent avalanches will slide over them unimpeded, carrying further masses of snow with them.
Temporary measures, unlike the barriers, can also make it possible to reduce the danger for a certain length of time. These measures are based on the idea of setting off avalanches by artificial means. The threatening masses of snow are removed from the potential avalanche area by a number of small avalanches deliberately triggered off under supervision at selected, predetermined times. This considerably increases the stability of the snow cover remaining on the avalanche site, by at least reducing the risk of further and more dangerous avalanches for a limited period of time when the threat of avalanches is acute.
However, the size of these artificially produced avalanches cannot be determined in advance with any great degree of accuracy. Therefore, in order to keep the risk of accidents as low as possible, while these temporary measures are being carried out, the entire area to be affected by the artificial avalanche, from its starting point to where it finally comes to a halt, must be evacuated, closed off and checked beforehand.
The possible applications of the two methods of reducing hazards are fundamentally different. In general, it is better to use permanent methods to protect areas that are impossible or difficult to evacuate or close off, or where settlements or forests could be endangered even by controlled avalanches. On the other hand, roads, ski runs and ski slopes, which are easy to close off for short periods, are typical examples of areas in which temporary protective measures can be applied.
The various methods of artificially setting off avalanches involve a number of operations which also entail certain risks and, above all, require additional protective measures for persons assigned to carry out this work. The essential thing is to cause initial breaks by setting off artificial tremors (blasts). These will sufficiently reduce the stability of the snow cover to produce a snow-slip.
Blasting is especially suitable for releasing avalanches on steep slopes. It is usually possible to detach small sections of snow at intervals and thus avoid major avalanches, which take a long distance to run their course and can be extremely destructive. However, it is essential that the blasting operations be carried out at any time of day and in all types of weather, and this is not always possible. Methods of artificially producing avalanches by blasting differ considerably according to the means used to reach the area where the blasting is to take place.
Areas where avalanches are likely to start can be bombarded with grenades or rockets from safe positions, but this is successful (i.e., produces the avalanche) in only 20 to 30% of cases, as it is virtually impossible to determine and to hit the most effective target point with any accuracy from a distance, and also because the snow cover absorbs the shock of the explosion. Besides, shells may fail to go off.
Blasting with commercial explosives directly into the area where avalanches are likely to start is generally more successful. The most successful methods are those whereby the explosive is carried on stakes or cables over the part of the snow field where the avalanche is to start, and detonated at a height of 1.5 to 3 m above the snow cover.
Apart from the shelling of the slopes, three different methods have been developed for getting the explosive for the artificial production of avalanches to the actual location where the avalanche is to start:
- dynamite cableways
- blasting by hand
- throwing or lowering the explosive charge from helicopters.
The cableway is the surest and at the same time the safest method. With the help of a special small cableway, the dynamite cableway, the explosive charge is carried on a winding rope over the blasting location in the area of snow cover in which the avalanche is to start. With proper rope control and with the help of signals and markings, it is possible to steer accurately towards what are known from experience to be the most effective locations, and to get the charge to explode directly above them. The best results with respect to triggering off avalanches are achieved when the charge is detonated at the correct height above the snow cover. Since the cableway runs at a greater height above the ground, this requires the use of lowering devices. The explosive charge hangs from a string wound around the lowering device. The charge is lowered to the correct height above the site selected for the explosion with the help of a motor which unwinds the string. The use of dynamite cableways makes it possible to carry out the blasting from a safe position, even with poor visibility, by day or night.
Because of the good results obtained and the relatively low production costs, this method of setting off avalanches is used extensively in the entire Alpine region, a licence being required to operate dynamite cableways in most Alpine countries. In 1988, an intensive exchange of experience in this field took place between manufacturers, users and government representatives from the Austrian, Bavarian and Swiss Alpine areas. The information gained from this exchange of experience has been summarized in leaflets and legally binding regulations. These documents basically contain the technical safety standards for equipment and installations, and instructions on carrying out these operations safely. When preparing the explosive charge and operating the equipment, the blasting crew must be able to move as freely as possible around the various cableway controls and appliances. There must be safe and easily accessible footpaths to enable the crew to leave the site quickly in case of emergency. There must be safe access routes up to cableway supports and stations. In order to avoid failure to explode, two fuses and two detonators must be used for every charge.
In the case of blasting by hand, a second method for artificially producing avalanches, which was frequently done in earlier times, the dynamiter has to climb to the part of the snow cover where the avalanche is to be set off. The explosive charge can be placed on stakes planted in the snow, but more generally thrown down the slope towards a target point known from experience to be particularly effective. It is usually imperative for helpers to secure the dynamiter with a rope throughout the entire operation. Nonetheless, however carefully the blasting team proceeds, the danger of falling or of encountering avalanches on the way to the blasting site cannot be eliminated, as these activities often involve long ascents, sometimes under unfavourable weather conditions. Because of these hazards, this method, which is also subject to safety regulations, is rarely used today.
Using helicopters, a third method, has been practised for many years in the Alpine and other regions for operations to set off avalanches. In view of the dangerous risks for persons on board, this procedure is used in most Alpine and other mountainous countries only when it is urgently needed to avert an acute danger, when other procedures cannot be used or would involve even greater risk. In view of the special legal situation arising from the use of aircraft for such purposes and the risks involved, specific guidelines on setting off avalanches from helicopters have been drawn up in the Alpine countries, with the collaboration of the aviation authorities, the institutions and authorities responsible for occupational health and safety, and experts in the field. These guidelines deal not only with matters concerning the laws and regulations on explosives and safety provisions, but also are concerned with the physical and technical qualifications required of persons entrusted with such operations.
Avalanches are set off from helicopters either by lowering the charge on a rope and detonating it above the snow cover or by dropping a charge with its fuse already lit. The helicopters used must be specially adapted and licensed for such operations. With regard to safely carrying out the operations on board, there must be a strict division of responsibilities between the pilot and the blasting technician. The charge must be correctly prepared and the length of fuse selected according to whether it is to be lowered or dropped. In the interests of safety, two detonators and two fuses must be used, as in the case of the other methods. As a rule, the individual charges contain between 5 and 10 kg of explosive. Several charges can be lowered or dropped one after the other during one operational flight. The detonations must be visually observed in order to check that none has failed to go off.
All these blasting processes require the use of special explosives, effective in cold conditions and not sensitive to mechanical influences. Persons assigned to carry out these operations must be specially qualified and have the relevant experience.
Temporary and permanent protective measures against avalanches were originally designed for distinctly different areas of application. The costly permanent barriers were mainly constructed to protect villages and buildings especially against major avalanches. The temporary protective measures were originally limited almost exclusively to protecting roads, ski resorts and amenities which could be easily closed off. Nowadays, the tendency is to apply a combination of the two methods. To work out the most effective safety programme for a given area, it is necessary to analyse the prevailing situation in detail in order to determine the method that will provide the best possible protection.
Weather-Related Problems
It was long accepted that weather-related problems were a natural phenomenon and death and injury from such events were inevitable (see table 1). It is only in the past two decades that we have begun to look at factors contributing to weather-related death and injury as a means of prevention. Because of the short duration of study in this area, the data are limited, particularly as they pertain to the number and circumstances of weather-related deaths and injuries among workers. The following is an overview of the findings thus far.
Table 1. Weather-related occupational risks
|
Weather event |
Type of worker |
Biochemical agents |
Traumatic injuries |
Drowning |
Burns/heatstroke |
Vehicle accidents |
Mental stress |
|
Floods |
Police, Transport Underground Linemen Clean-up |
*
*** |
*
*
*
|
*
** *
|
*
|
|
* * * * |
|
Tornadoes |
Police, Transportation Cleanup |
*
** |
*
*** * |
|
|
* |
*
* |
|
Light forest fires |
Fire-fighters |
** |
** |
|
** |
*** |
* |
*degree of risk.
Floods, Tidal Waves
Definitions, sources and occurrences
Flooding results from a variety of causes. Within a given climatic region, tremendous variations of flooding occur because of fluctuations within the hydrological cycle and other natural and synthetic conditions (Chagnon, Schict and Semorin 1983). The US National Weather Service has defined flash floods as those that follow within a few hours of heavy or excessive rain, a dam or levee failure or a sudden release of water impounded by an ice or log jam. Although most flash floods are the result of intense local thunderstorm activity, some occur in conjunction with tropical cyclones. Forerunners to flash floods usually involve atmospheric conditions that influence the continuation and intensity of rainfall. Other factors that contribute to flash floods include steepness of slopes (mountain terrain), absence of vegetation, lack of infiltration capability of the soil, floating debris and ice jams, rapid snow melt, dam and levee failures, rupture of a glacial lake, and volcanic disturbances (Marrero 1979). River flooding can be influenced by factors which cause flash flooding, but more insidious flooding may be caused by stream channel characteristics, character of soil and subsoil, and degree of synthetic modification along its path (Chagnon, Schict and Semorin 1983; Marrero 1979). Coastal flooding can result from storm surge, which is the result of a tropical storm or cyclone, or ocean waters driven inland by wind-generated storms. The most devastating type of coastal flooding is the tsunami, or tidal wave, which is generated by submarine earthquakes or certain volcanic eruptions. Most recorded tsunamis have occurred in the Pacific and Pacific coast regions. The islands of Hawaii are particularly prone to tsunami damage because of their location in the mid-Pacific (Chagnon, Schict and Semorin 1983; Whitlow 1979).
Factors influencing morbidity and mortality
It has been estimated that floods account for 40% of all the world’s disasters, and they do the greatest amount of damage. The most lethal flood in recorded history struck the Yellow River in 1887, when the river overflowed 70-foot-high levees, destroying 11 cities and 300 villages. An estimated 900,000 people were killed. Several hundred thousand may have died in China’s Shantung Province in 1969 when storm surges pushed flood tides up the Yellow River Valley. A sudden flood in January 1967 in Rio de Janeiro killed 1,500 people. In 1974 heavy rains flooded Bangladesh and caused 2,500 deaths. In 1963 heavy rains caused an enormous landslide that fell into the lake behind the Vaiont Dam in Northern Italy, sending 100 million tons of water over the dam and causing 2,075 deaths (Frazier 1979). In 1985 an estimated 7 to 15 inches of rain fell in a ten-hour period in Puerto Rico, killing 180 people (French and Holt 1989).
River flooding has been curtailed by engineering controls and increased forestation of watersheds (Frazier 1979). However, flash floods have increased in recent years, and are the number one weather-related killer in the United States. The increased toll from flash floods is attributed to increased and more urbanized populations on sites that are ready targets for flash floods (Mogil, Monro and Groper 1978). Fast-flowing water accompanied by such debris as boulders and fallen trees account for the primary flood-related morbidity and mortality. In the United States studies have shown a high proportion of car-related drownings in floods, due to people driving into low-lying areas or across a flooded bridge. Their cars may stall in high water or be blocked by debris, trapping them in their cars while high levels of fast-flowing water descend upon them (French et al. 1983). Follow-up studies of flood victims show a consistent pattern of psychological problems up to five years after the flood (Melick 1976; Logue 1972). Other studies have shown a significant increase in the incidence of hypertension, cardiovascular disease, lymphoma and leukaemia in flood victims, which some investigators feel are stress related (Logue and Hansen 1980; Janerich et al. 1981; Greene 1954). There is a potential for increased exposure to biological and chemical agents when floods cause disruption of water purification and sewage-disposal systems, rupture of underground storage tanks, overflowing of toxic waste sites, enhancement of vector-breeding conditions and dislodgement of chemicals stored above ground (French and Holt 1989).
Although, in general, workers are exposed to the same flood-related risks as the general population, some occupational groups are at higher risk. Clean-up workers are at high risk of exposure to biological and chemical agents following floods. Underground workers, particularly those in confined places, may be trapped during flash floods. Truck drivers and other transportation workers are at high risk from vehicle-related flood mortality. As in other weather-related disasters, fire-fighters, police and emergency medical personnel are also at high risk.
Prevention and control measures and research needs
Prevention of death and injury from floods can be accomplished by identifying flood-prone areas, making the public aware of these areas and advising them on appropriate prevention actions, conducting dam inspections and issuing dam safety certification, identifying meteorological conditions that will contribute to heavy precipitation and runoff, and issuing early warnings of floods for a specific geographic area within a specific time frame. Morbidity and mortality from secondary exposures can be prevented by assuring that water and food supplies are safe to consume and are not contaminated with biological and chemical agents, and by instituting safe human waste disposal practices. Soil surrounding toxic waste sites and storage lagoons should be inspected to determine if there has been contamination from overflowing storage areas (French and Holt 1989). Although mass vaccination programmes are counterproductive, clean-up and sanitation workers should be properly immunized and instructed in appropriate hygienic practices.
There is a need to improve technology so that early warnings for flash floods can be more specific in terms of time and place. Conditions should be assessed to determine whether evacuation should be by car or on foot. Following a flood a cohort of workers engaged in flood-related activities should be studied to assess the risk of adverse physical and mental health effects.
Hurricanes, Cyclones, Tropical Storms
Definitions, sources and occurrences
A hurricane is defined as a rotating wind system that whirls counterclockwise in the northern hemisphere, forms over tropical water, and has sustained wind speeds of at least 74 miles per hour (118.4 km/h). This whirling accumulation of energy is formed when circumstances involving heat and pressure nourish and nudge the winds over a large area of ocean to wrap themselves around an atmospheric low-pressure zone. A typhoon is comparable to a hurricane except that it forms over Pacific waters. Tropical cyclone is the term for all wind circulations rotating around an atmospheric low over tropical waters. A tropical storm is defined as a cyclone with winds from 39 to 73 mph (62.4 to 117.8 km/h), and a tropical depression is a cyclone with winds less than 39 mph (62.4 km/h).
It is presently thought that many tropical cyclones originate over Africa, in the region just south of the Sahara. They start as an instability in a narrow east to west jet stream that forms in that area between June and December, as a result of the great temperature contrast between the hot desert and the cooler, more humid region to the south. Studies show that the disturbances generated over Africa have long lifetimes, and many of them cross the Atlantic (Herbert and Taylor 1979). In the 20th century an average of ten tropical cyclones each year whirl out across the Atlantic; six of these become hurricanes. As the hurricane (or typhoon) reaches its peak intensity, air currents formed by the Bermuda or Pacific high-pressure areas shift its course northward. Here the ocean waters are cooler. There is less evaporation, less water vapour and energy to feed the storm. If the storm hits land, the supply of water vapour is cut off entirely. As the hurricane or typhoon continues to move north, its winds begin to diminish. Topographical features such as mountains may also contribute to the breakup of the storm. The geographic areas at greatest risk for hurricanes are the Caribbean, Mexico, and the eastern seaboard and Gulf Coast states of the United States. A typical Pacific typhoon forms in the warm tropical waters east of the Philippines. It may move westward and strike the Chinese mainland or veer to the north and approach Japan. The storm’s path is determined as it moves around the western edge of the Pacific high-pressure system (Understanding Science and Nature: Weather and Climate 1992).
The destructive power of a hurricane (typhoon) is determined by the way storm surge, wind and other factors are combined. Forecasters have developed a five-category disaster potential scale to make the predicted hazards of approaching hurricanes clearer. Category 1 is a minimum hurricane, category 5 a maximum hurricane. In the period 1900-1982, 136 hurricanes struck the United States directly; 55 of these were of at least category 3 intensity. Florida felt the effects of both the highest number and the most intense of these storms, with Texas, Louisiana and North Carolina following in descending order (Herbert and Taylor 1979).
Factors influencing morbidity and mortality
Although winds do much damage to property, the wind is not the biggest killer in a hurricane. Most victims die from drowning. The flooding that accompanies a hurricane may come from the intense rain or from the storm surges. The US National Weather Service estimates that storm surges cause nine of every ten hurricane-associated fatalities (Herbert and Taylor 1979). The occupational groups most heavily impacted by hurricanes (typhoons) are those related to boating and shipping (which would be affected by the unusually rough seas and high winds); utility line workers who are called into service to repair damaged lines, often while the storm is still raging; fire-fighters and police officers, who are involved in evacuations and protecting the property of evacuees; and emergency medical personnel. Other occupational groups are discussed in the section on floods.
Prevention and control, research needs
The incidence of deaths and injuries associated with hurricanes (typhoons) has dropped dramatically in the past twenty years in those areas where sophisticated advanced warning systems have been put into effect. The principal steps to follow for preventing death and injury are: to identify meteorological precursors of these storms and track their course and potential development into hurricanes, to issue early warnings to provide for timely evacuation when indicated, to enforce stringent land use management practices and building codes in high-risk areas, and to develop emergency contingency plans in high-risk areas to provide for an orderly evacuation and adequate shelter capacity for evacuees.
Because the meteorological factors contributing to hurricanes have been well studied, a good deal of information is available. More information is needed on the variable pattern of incidence and intensity of hurricanes over time. The effectiveness of existing contingency plans should be assessed following each hurricane, and it should be determined if buildings protected from wind speed are also protected from storm surges.
Tornadoes
Formation and patterns of occurrence
Tornadoes are formed when layers of air of different temperature, density and windflow combine to produce powerful updrafts forming huge cumulonimbus clouds which are transformed into rotating tight spirals when strong cross winds blow through the cumulonimbus cloud. This vortex draws even more warm air into the cloud, which makes the air spin faster until a funnel cloud packing explosive force drops out of the cloud (Understanding Science and Nature: Weather and Climate 1992). The average tornado has a track approximately 2 miles long and 50 yards wide, affecting about 0.06 square miles and with wind speeds as high as 300 mph. Tornadoes occur in those areas where warm and cold fronts are apt to collide, causing unstable conditions. Although the probability that a tornado will strike any specific location is extremely small (probability 0.0363), some areas, such as the Midwest states in the United States, are particularly vulnerable.
Factors influencing morbidity and mortality
Studies have shown that people in mobile homes and in lightweight cars when tornadoes strike are at particularly high risk. In the Wichita Falls, Texas, Tornado Study, occupants of mobile homes were 40 times more likely to sustain a serious or fatal injury than those in permanent dwellings, and occupants of automobiles were at approximately five times greater risk (Glass, Craven and Bregman 1980). The leading cause of death are craniocerebral trauma, followed by crushing wounds of the head and trunk. Fractures are the most frequent form of non-fatal injury (Mandlebaum, Nahrwold and Boyer 1966; High et al. 1956). Those workers who spend a major part of their working time in lightweight automobiles, or whose offices are in mobile homes, would be at high risk. Other factors relating to clean-up operators discussed in the flood section would apply here.
Prevention and control
The issuing of appropriate warnings, and the need for the population to take appropriate action on the basis of those warnings, are the most important factors in preventing tornado-related death and injury. In the United States, the National Weather Service has acquired sophisticated instrumentation, such as Doppler radar, which permits them to identify conditions conducive to the formation of a tornado and to issue warnings. A tornado watch means that conditions are conducive to tornado formation in a given area, and a tornado warning means that a tornado has been sighted in a given area and those residing in that area should take appropriate shelter, which entails going to the basement if one exists, going to an inside room or closet, or if outside, going to a ditch or gully.
Research is needed to assess whether warnings are effectively disseminated and the extent to which people heed those warnings. It should also be determined whether the prescribed shelter areas really provide adequate protection from death and injury. Information should be gathered on the number of deaths and injuries to tornado workers.
Lightning and Forest Fires
Definitions, sources and occurrences
When a cumulonimbus cloud grows into a thunderstorm, different sections of the cloud accumulate positive and negative electric charges. When the charges have built up, the negative charges flow toward the positive charges in a lightning flash that travels within the cloud or between the cloud and the ground. Most lightning travels from cloud to cloud, but 20% travels from cloud to ground.
A lightning flash between a cloud and the ground can be either positive or negative. Positive lightning is more powerful and is more likely to start forest fires. A lightning strike will not start a fire unless it meets easily ignitable fuel like pine needles, grass and pitch. If the fire hits decaying wood, it can burn unnoticed for a long period of time. Lightning ignites fires more often when it touches the ground and the rain within the thunder cloud evaporates before it reaches the ground. This is called dry lightning (Fuller 1991). It is estimated that in dry, rural areas such as Australia and the western United States, 60% of forest fires are caused by lightning.
Factors causing morbidity and mortality
Most of the fire-fighters who die in a fire die in truck or helicopter accidents or from being hit by falling snags, rather than from the fire itself. However, fighting fire can cause heat stroke, heat exhaustion and dehydration. Heat stroke, caused by the body temperature rising to over 39.4°C, can cause death or brain damage. Carbon monoxide is also a threat, particularly in smouldering fires. In one test, researchers found that the blood of 62 of 293 fire-fighters had carboxyhaemoglobin levels above the maximum allowable level of 5% after eight hours on the fire line (Fuller 1991).
Prevention, control and research needs
Because of the danger and the mental and physical stress associated with fire-fighting, crews should not work for more than 21 days, and must have one day off for every 7 days worked within that time. In addition to wearing appropriate protective gear, fire-fighters must learn safety factors such as planning safety routes, keeping in communication, watching for hazards, keeping track of the weather, making sure of directions and acting before a situation becomes critical. The standard fire-fighting orders emphasize knowing what the fire is doing, posting lookouts and giving clear, understandable instructions (Fuller 1991).
Factors relating to prevention of lightning forest fires include limiting fuels such as dry underbrush or fire-susceptible trees like eucalyptus, preventing building in fire-prone areas and early detection of forest fires. Early detection has been enhanced by the development of new technology such as an infrared system which is mounted on helicopters to check whether lightning strikes reported from aerial lookout and detection systems have actually started fires and to map hot spots for ground crews and helicopter drops (Fuller 1991).
More information is needed on the number and circumstances of deaths and injuries associated with lightning-related forest fires.
Post-Disaster Activities
Industrial accidents may affect groups of workers exposed in the workplace as well as the population living around the plant where the accident takes place. When pollution caused by accident occurs, the size of the affected population is likely to be orders of magnitude greater than the workforce, posing complex logistic problems. The present article focuses on these problems, and applies to agricultural accidents as well.
Reasons for quantifying health effects of an accident include:
- the need to ensure that all exposed persons have received medical attention (regardless of whether or not treatment was actually needed by each of them). Medical attention may consist of the search for and alleviation of clinically recognizable adverse consequences (if any) as well as implementation of means for preventing possible delayed effects and complications. This is obligatory when an accident occurs within a plant; then all the people working there will be known and full follow-up is feasible
- the need to identify persons deserving of compensation as victims of the accident. This implies that individuals must be characterized as to the severity of disease and the credibility of a causal association between their condition and the disaster.
- the acquisition of new knowledge on disease pathogenesis in humans
- the scientific interest of unravelling mechanisms of toxicity in humans, including those aspects which may help in reassessing, for a given exposure, doses considered to be “safe” in humans.
Characterization of Accidents in Relation to Health Consequences
Environmental accidents include a broad range of events occurring under the most diverse of circumstances. They may be first noticed or suspected because of environmental changes or because of the occurrence of disease. In both situations, the evidence (or suggestion) that “something may have gone wrong” may appear suddenly (e.g., the fire in the Sandoz storehouse in Schweizerhalle, Switzerland, in 1986; the epidemic of the condition later labelled as “toxic oil syndrome” (TOS) in Spain in 1981) or insidiously (e.g., excesses of mesothelioma following environmental—non-occupational—exposure to asbestos in Wittenoom, Australia). In all circumstances, at any given moment, uncertainty and ignorance surround both key questions: “Which health consequences have occurred so far?” and “What can be predicted to occur?”
In assessing the impact of an accident on human health, three types of determinants may interact:
- the agent(s) being released, its hazardous properties and the risk created by its release
- the individual disaster experience
- the response measures (Bertazzi 1991).
The nature and quantity of the release might be difficult to determine, as well as the ability of the material to enter into the different compartments of the human environment, such as the food chain and water supply. Twenty years after the accident, the amount of 2,3,7,8-TCDD released in Seveso on July 10, 1976, remains a matter of dispute. In addition, with the limited knowledge about the toxicity of this compound, in the early days after the accident, any prediction of risk was necessarily questionable.
Individual disaster experience consists of fear, anxiety and distress (Ursano, McCaughey and Fullerton 1994) consequent to the accident, irrespective of the nature of the hazard and of the actual risk. This aspect covers both conscious—not necessarily justified—behavioural changes (e.g., the marked decrease in birth rates in many Western European Countries in 1987, following the Chernobyl accident) and psychogenic conditions (e.g., symptoms of distress in school children and Israeli soldiers following the escape of hydrogen sulphide from a faulty latrine in a school on the West Bank of Jordan in 1981). Attitudes towards the accident are also influenced by subjective factors: in Love Canal, for instance, young parents with little experience of contact with chemicals in the workplace were more prone to evacuate the area than were older people with grown-up children.
Finally, an accident may have an indirect impact on the health of those exposed, either creating additional hazards (e.g., distress associated with evacuation) or, paradoxically, leading to circumstances with some potential for benefit (such as people who stop smoking tobacco as a consequence of contact with the milieu of health workers).
Measuring the Impact of an Accident
There is no doubt that each accident requires an assessment of its measurable or potential consequences on the exposed human population (and animals, domestic and/or wild), and periodic updates of such assessment may be required. In fact, many factors influence the detail, extent and nature of the data which can be collected for such an assessment. The amount of available resources is critical. Accidents of the same severity may be granted different levels of attention in different countries, in relation to the ability to divert resources from other health and social issues. International cooperation may partly mitigate this discrepancy: in fact, it is limited to episodes which are particularly dramatic and/or present unusual scientific interest.
The overall impact of an accident upon health ranges from negligible to severe. Severity depends on the nature of the conditions which are produced by the accident (which may include death), on the size of the exposed population, and on the proportion that develop disease. Negligible effects are more difficult to demonstrate epidemiologically.
Sources of data to be used for evaluating health consequences of an accident include in the first place current statistics which exist already (attention to their potential use should always precede any suggestion of creating new population databases). Additional information can be derived from analytical, hypothesis-centred epidemiological studies for the purpose of which current statistics may or may not be useful. If in an occupational setting no health surveillance of the workers is present, the accident can provide the opportunity to establish a surveillance system which will eventually help to protect workers from other potential health hazards.
For the purposes of clinical surveillance (short or long term) and/or provision of compensation, the exhaustive enumeration of the exposed persons is a sine qua non. This is relatively simple in the case of intra-factory accidents. When the affected population can be defined by the place where they live, the list of residents in administrative municipalities (or smaller units, when available) provides a reasonable approach. The construction of a roster may be more problematic under other circumstances, particularly when the need is for a list of people showing symptoms possibly attributable to the accident. In the TOS episode in Spain, the roster of persons to be included in the long-term clinical follow-up was derived from the list of the 20,000 persons applying for financial compensation, subsequently corrected through a revision of the clinical records. Given the publicity of the episode, it is believed that this roster is reasonably complete.
A second requirement is that activities aiming at the measure of the impact of an accident be rational, clear-cut and easy to explain to the affected population. Latency may range between days and years. If some conditions are met, the nature of disease and probability of occurrence can be hypothesized a priori with a precision sufficient for the adequate design of a clinical surveillance programme and ad hoc studies aiming at one or more of the goals mentioned at the beginning of this article. These conditions include the rapid identification of the agent released by the accident, availability of adequate knowledge on its short- and long-term hazardous properties, a quantification of the release, and some information on inter-individual variation in susceptibility to the agent’s effects. In fact, these conditions are rarely met; a consequence of the underlying uncertainty and ignorance is that the pressure of public opinion and the media for prevention or definite medical intervention of doubtful usefulness is more difficult to resist.
Finally, as soon as possible after the occurrence of an accident has been established, a multidisciplinary team (including clinicians, chemists, industrial hygienists, epidemiologists, human and experimental toxicologists) needs to be established, which will be responsible to the political authority and the public. In the selection of experts, it must be borne in mind that the range of chemicals and technology which may underlie an accident is very large, so that different types of toxicity involving a variety of biochemical and physiological systems may result.
Measuring the Impact of Accidents through Current Statistics
Current health status indicators (such as mortality, natality, hospital admissions, sickness absence from work and physician visits) have the potential to provide early insight on the consequences of an accident, provided they are stratifiable for the affected region, which often will not be possible because affected areas can be small and not necessarily overlapping with administrative units. Statistical associations between the accident and an excess of early events (occurring within days or weeks) detected through existing health status indicators are likely to be causal, but do not necessarily reflect toxicity (e.g., an excess of physician visits may be caused by fear rather than by actual occurrence of disease). As always, care must be exercised when interpreting any change in health status indicators.
Although not all accidents produce death, mortality is an easily quantifiable endpoint, either by direct count (e.g., Bhopal) or through comparisons between observed and expected number of events (e.g., acute episodes of air pollution in urban areas). Ascertaining that an accident has not been associated with an early excess of mortality may help in assessing the severity of its impact and in addressing attention to non-lethal consequences. Further, the statistics needed in order to calculate expected numbers of deaths are available in most countries and allow for estimates in areas as small as those which are usually affected by an accident. Assessing mortality from specific conditions is more problematic, because of possible bias in certifying causes of death by health officers who are aware of the diseases expected to increase after the accident (diagnostic suspicion bias).
From the foregoing, the interpretation of health status indicators based on existing data sources requires a careful design of ad hoc analyses, including a detailed consideration of possible confounding factors.
On occasions, early after an accident, the question is posed whether the creation of a conventional population-based cancer registry or a registry of malformations is warranted. For these specific conditions, such registries may provide more reliable information than other current statistics (such as mortality or hospital admissions), particularly if newly created registries are run according to internationally acceptable standards. Nevertheless, their implementation requires the diversion of resources. In addition, if a population-based registry of malformations is established de novo after an accident, probably within nine months it will hardly be capable of producing data comparable to those produced by other registries and a series of inferential problems (particularly statistical error of the second type) will ensue. In the end, the decision largely relies on the evidence of carcinogenicity, embryotoxicity or teratogenicity of the hazard(s) which have been released, and on possible alternative uses of the available resources.
Ad Hoc Epidemiological Studies
Even in areas covered by the most accurate systems for monitoring the reasons for patients’ contacts with physicians and/or hospital admissions, indicators from these areas will not provide all the information needed in order to assess the health impact of an accident and the adequacy of the medical response to it. There are specific conditions or markers of individual response which either do not require contact with the medical establishment or do not correspond to the disease classifications conventionally used in current statistics (so that their occurrence would hardly be identifiable). There may be the need for counting as “victims” of the accident, subjects whose conditions are borderline between occurrence and non-occurrence of disease. It is often necessary to investigate (and evaluate the efficacy of) the range of therapeutical protocols which are used. The problems noted here are but a sampling and do not cover all those which might create the need for an ad hoc investigation. In any case, procedures should be established in order to receive additional complaints.
Investigations differ from the provision of care in that they are not directly related to the individual’s interest as a victim of the accident. An ad hoc investigation should be shaped in order to fulfil its purposes—to provide reliable information and/or demonstrate or disprove a hypothesis. Sampling may be reasonable for research purposes (if accepted by the affected population), but not in the provision of medical care. For instance, in the case of a spill of an agent suspected of damaging bone marrow, there are two totally different scenarios in order to respond to each of the two questions: (1) whether the chemical actually induces leukopenia, and (2) whether all exposed persons have been exhaustively screened for leukopenia. In an occupational setting both questions can be pursued. In a population, the decision also will depend on the possibilities for constructive intervention to treat those affected.
In principle, there is a need to have sufficient epidemiological skill locally to contribute to the decision on whether ad hoc studies ought to be carried out, to design them and to supervise their conduct. However, health authorities, media and/or the population may not consider the epidemiologists of the affected area to be neutral; thus, help from outside may be needed, even at a very early stage. The same epidemiologists should contribute to the interpretation of descriptive data based on the currently available statistics, and to the development of causal hypotheses when needed. If epidemiologists are not available locally, collaboration with other institutions (usually, National Institutes of Health, or WHO) is necessary. Episodes which are unravelled because of the lack of epidemiological skill are regrettable.
If an epidemiological study is believed to be necessary, however, attention should be addressed to some preliminary questions: To what use will predictable results be put? Might the desire for a more refined inference resulting from the planned study unduly delay clean-up procedures or other preventive measures? Must the proposed research programme first be fully documented and evaluated by the multidisciplinary scientific team (and perhaps by other epidemiologists)? Will there be adequate provision of details to the persons to be studied to ensure their fully informed, prior and voluntary consent? If a health effect is found, what treatment is available and how will it be delivered?
Finally, conventional prospective cohort mortality studies ought to be implemented when the accident has been severe and there are reasons to fear later consequences. Feasibility of these studies differs between countries. In Europe, they range between the possibility of nominal “flagging” of persons (e.g., rural populations in Shetland, UK, following the Braer Oil Spill) and the need for systematic contacts with the victims’ families in order to identify dying persons (e.g., TOS in Spain).
Screening for Prevalent Conditions
Offering affected people medical attention is a natural reaction to an accident which may have caused them harm. The attempt to identify all those in the exposed population who exhibit conditions related to the accident (and give them medical care if needed) corresponds to the conventional concept of screening. Basic principles, potentialities and limitations common to any screening programme (regardless of the population to which it is addressed, the condition to be identified and the tool used as a diagnostic test) are as valid after an environmental accident as in any other circumstance (Morrison 1985).
Estimating participation and understanding reasons for non-response are just as crucial as measuring sensitivity, specificity and predictive value of the diagnostic test(s), designing a protocol for subsequent diagnostic procedures (when needed) and the administration of therapy (if required). If these principles are neglected, short- and/or long-term screening programmes may produce more harm than benefit. Unnecessary medical examinations or laboratory analyses are a waste of resources and a diversion from providing necessary care to the population as a whole. Procedures for ensuring a high level of compliance have to be carefully planned and evaluated.
Emotional reactions and uncertainties surrounding environmental accidents may further complicate things: physicians tend to loose specificity when diagnosing borderline conditions, and some “victims” may consider themselves entitled to receive medical treatment regardless of whether or not it is actually needed or even useful. In spite of the chaos which often follows an environmental accident, some sine qua non for any screening programme should be borne in mind:
- Procedures should be laid down in a written protocol (including second level diagnostic tests and therapy to be provided to those who are found to be affected or sick).
- One person should be identified as responsible for the programme.
- There should be a preliminary estimate of specificity and sensitivity of the diagnostic test.
- There should be coordination between clinicians participating in the programme.
- Participation rates should be quantified and reviewed at regular intervals.
Some a priori estimates of efficacy of the whole programme would also help in deciding whether or not the programme is worth implementing (e.g., no programme for anticipating the diagnosis of a lung cancer should be encouraged). Also, a procedure should be established in order to recognize additional complaints.
At any stage, screening procedures may have a value of a different type—to estimate the prevalence of conditions, as a basis for an assessment of the consequences of the accident. A major source of bias in these estimates (which becomes more severe with time) is the representativeness of the exposed persons submitting themselves to the diagnostic procedures. Another problem is the identification of adequate control groups for comparing the prevalence estimates which are obtained. Controls drawn from the population may suffer from as much selection bias as the exposed person’s sample. Nevertheless, under some circumstances, prevalence studies are of the utmost importance (particularly when the natural history of the disease is not known, such as in TOS), and control groups external to the study, including those assembled elsewhere for other purposes, may be used when the problem is important and/or serious.
Use of Biological Materials for Epidemiological Purposes
For descriptive purposes, the collection of biological materials (urine, blood, tissues) from members of the exposed population can provide markers of internal dose, which by definition are more precise than (but do not replace totally) those obtainable through estimates of the concentration of the pollutant in the relevant compartments of the environment and/or through individual questionnaires. Any evaluation ought to take into account possible bias ensuing from the lack of representativeness of those members of the community from whom the biological samples were obtained.
Storing biological samples may prove useful, at a later stage, for the purpose of ad hoc epidemiological studies requiring estimates of internal dose (or early effects) at the individual level. Collecting (and properly preserving) the biological samples early after the accident is crucial, and this practice should be encouraged even in the absence of precise hypotheses for their use. The informed consent process must ensure that the patient understands that his or her biological material is to be stored for use in tests hitherto undefined. Here it is helpful to exclude the use of such specimens from certain tests (e.g., identification of personality disorders) to better protect the patient.
Conclusions
The rationale for medical intervention and epidemiological studies in the population affected by an accident ranges between two extremes—assessing the impact of agents which are proved to be potential hazards and to which the affected population is (or has been) definitely exposed, and exploring the possible effects of agents hypothesized to be potentially hazardous and suspected to be present in the area. Differences between experts (and between people in general) in their perception of the relevance of a problem are inherent to humanity. What matters is that any decision has a recorded rationale and a transparent plan of action, and is supported by the affected community.
Disaster Preparedness
Over the last two decades the emphasis in disaster reduction has switched from mainly improvised relief measures in the post-impact phase to forward planning, or disaster preparedness. For natural disasters this approach has been embraced in the philosophy of the United Nations International Decade for Natural Disaster Reduction (IDNDR) programme. The following four phases are the components of a comprehensive hazard management plan which can be applied to all types of natural and technological disasters:
- pre-disaster planning
- emergency preparedness
- emergency response
- post-impact recovery and reconstruction.
The aim of disaster preparedness is to develop disaster prevention or risk reduction measures in parallel with emergency preparedness and response capabilities. In this process hazard and vulnerability analyses are the scientific activities which provide the basis for the applied tasks of risk reduction and emergency preparedness to be undertaken in collaboration with planners and the emergency services.
Most health professionals would see their role in disaster preparedness as one of planning for the emergency treatment of large numbers of casualties. However, if the impact of disasters is to be drastically reduced in the future, the health sector needs to be involved in the development of preventive measures and in all phases of disaster planning, with scientists, engineers, emergency planners and decision makers. This multidisciplinary approach poses a major challenge to the health sector at the end of the 20th century as natural and human-made calamities become increasingly destructive and costly in terms of lives and property with the expansion of human populations across the globe.
Natural sudden or rapid-onset disasters include extreme weather conditions (floods and high winds), earthquakes, landslides, volcanic eruptions, tsunamis and wild fires, and their impacts have much in common. Famines, drought and desertification, on the other hand, are subject to more long-term processes which at present are only very poorly understood, and their consequences are not so amenable to reduction measures. Presently the most common cause of famine is war or so-called complex disasters (e.g., in Sudan, Somalia or former Yugoslavia).
Large numbers of displaced persons are a common feature of natural and complex disasters, and their nutritional and other health needs require specialized management.
Modern civilization is also becoming accustomed to technological or human-made disasters such as acute air pollution episodes, fires and chemical and nuclear reactor accidents, the last two being the most important today. This article will focus on disaster planning for chemical disasters, as nuclear power accidents are dealt with elsewhere in the Encyclopaedia.
Natural Sudden-Onset Disasters
The most important of these in terms of destructiveness are floods, hurricanes, earthquakes and volcanic eruptions. There have already been some well-publicized successes in disaster reduction through early warning systems, hazard mapping and structural engineering measures in seismic zones.
Thus satellite monitoring using global weather forecasting, together with a regional system for timely delivery of warnings and effective evacuation planning, was responsible for the comparatively small loss of life (just 14 deaths) when Hurricane Hugo, the strongest hurricane so far recorded in the Caribbean, struck Jamaica and the Cayman Islands in 1988. In 1991 adequate warnings provided by Philippine scientists closely monitoring Mount Pinatubo saved many thousands of lives through timely evacuation in one of the largest eruptions of the century. But the “technological fix” is only one aspect of disaster mitigation. The large human and economic losses wrought by disasters in developing countries highlight the major importance of socio-economic factors, above all poverty, in increasing vulnerability, and the need for disaster preparedness measures to take these into account.
Natural disaster reduction has to compete in all countries with other priorities. Disaster reduction can also be promoted through legislation, education, building practices and so on, as part of a society’s general risk reduction programme or safety culture—as an integral part of sustainable development policies and as a quality assurance measure for investment strategies (e.g., in the planning of buildings and infrastructure in new land developments).
Technological Disasters
Clearly, with natural hazards it is impossible to prevent the actual geological or meteorological process from occurring.
However, with technological hazards, major inroads into disaster prevention can be made using risk reduction measures in the design of plants and governments can legislate to establish high standards of industrial safety. The Seveso Directive in EC countries is an example which also includes requirements for the development of onsite and offsite planning for emergency response.
Major chemical accidents comprise large vapour or flammable gas explosions, fires, and toxic releases from fixed hazardous installations or during the transport and distribution of chemicals. Special attention has been given to the storage in large quantities of toxic gases, the most common being chlorine (which, if suddenly released due to the disruption of a storage tank or from a leak in a pipe, can form large denser-than-air clouds which can be blown in toxic concentrations for large distances downwind). Computer models of dispersion of dense gases in sudden releases have been produced for chlorine and other common gases and these are used by planners to devise emergency response measures. These models can also be used to determine the numbers of casualties in a reasonably foreseeable accidental release, just as models are being pioneered for predicting the numbers and types of casualties in major earthquakes.
Disaster Prevention
A disaster is any disruption of the human ecology that exceeds the capacity of the community to function normally. It is a state which is not merely a quantitative difference in the functioning of the health or emergency services—for example, as caused by a large influx of casualties. It is a qualitative difference in that the demands cannot be adequately met by a society without help from unaffected areas of the same or another country. The word disaster is too often used loosely to describe major incidents of a highly publicized or political nature, but when a disaster has actually occurred there may be a total breakdown in normal functioning of a locality. The aim of disaster preparedness is to enable a community and its key services to function in such disorganized circumstances in order to reduce human morbidity and mortality as well as economic losses. Large numbers of acute casualties are not a prerequisite for a disaster, as was shown in the chemical disaster at Seveso in 1976 (when a massive evacuation was mounted because of fears of long-term health risks arising from ground contamination by dioxin).
“Near disasters” may be a better description of certain events, and outbreaks of psychological or stress reactions may also be the only manifestation in some events (e.g., at the reactor accident at Three Mile Island, USA, in 1979). Until the terminology becomes established we should recognize Lechat’s description of the health objectives of disaster management, which include:
- prevention or reduction of mortality due to the impact, to a delay in rescue and to lack of appropriate care
- provision of care for casualties such as immediate post-impact trauma, burns and psychological problems
- management of adverse climatic and environmental conditions (exposure, lack of food and drinking water)
- prevention of short-term and long-term disaster-related morbidity (e.g., outbreaks of communicable diseases due to disruption of sanitation, living in temporary shelters, overcrowding and communal feeding; epidemics such as malaria due to interruption of control measures; rise of morbidity and mortality due to disruption of the health care system; mental and emotional problems)
- ensuring restoration of normal health by preventing long-term malnutrition due to disruption of food supplies and agriculture.
Disaster prevention cannot take place in a vacuum, and it is essential that a structure exists at the national governmental level of every country (the actual organization of which will vary from country to country), as well as at the regional and community level. In countries with high natural risks, there may be few ministries which can avoid being involved. The responsibility for planning is given to existing bodies such as armed forces or civil defence services in some countries.
Where a national system exists for natural hazards it would be appropriate to build on to it a response system for technological disasters, rather than devise a whole new separate system. The Industry and Environment Programme Activity Centre of the United Nations Environment Programme has developed the Awareness and Preparedness for Emergencies at Local Level (APELL) Programme. Launched in cooperation with industry and government, the programme aims to prevent technological accidents and reduce their impacts in developing countries by raising community awareness of hazardous installations and providing assistance in developing emergency response plans.
Hazard Assessment
The different types of natural disaster and their impacts need to be assessed in terms of their likelihood in all countries. Some countries such as the UK are at low risk, with wind storms and floods being the main hazards, while in other countries (e.g., the Philippines) there is a wide range of natural phenomena which strike with relentless regularity and can have serious effects on the economy and even the political stability of the country. Each hazard requires a scientific evaluation which will include at least the following aspects:
- its cause or causes
- its geographical distribution, magnitude or severity and probable frequency of occurrence
- the physical mechanisms of destruction
- the elements and activities most vulnerable to destruction
- possible social and economic consequences of a disaster.
Areas at high risk of earthquakes, volcanoes and floods need to have hazard zone maps prepared by experts to predict the locations and nature of the impacts when a major event occurs. Such hazard assessments can then be used by land-use planners for long-term risk reduction, and by emergency planners who have to deal with the pre-disaster response. However, seismic zoning for earthquakes and hazard mapping for volcanoes are still in their infancy in most developing countries, and extending such risk mapping is seen as a crucial need in the IDNDR.
Hazard assessment for natural hazards requires a detailed study of the records of previous disasters in the preceding centuries and exacting geological field work to ascertain major events such as earthquakes and volcanic eruptions in historic or prehistoric times. Learning about the behaviour of major natural phenomena in the past is a good, but far from infallible, guide for hazard assessment for future events. There are standard hydrological methods for flood estimation, and many flood-prone areas can be easily recognized because they coincide with a well-defined natural flood plain. For tropical cyclones, records of impacts around coastlines can be used to determine the probability of a hurricane striking any one part of the coastline in a year, but each hurricane has to be urgently monitored as soon as it has formed in order to actually forecast its path and speed at least 72 hours ahead, before it makes landfall. Associated with earthquakes, volcanoes and heavy rains are landslides which may be triggered by these phenomena. In the last decade it has been increasingly appreciated that many large volcanoes are at risk from slope failure because of the instability of their mass, which has been built up during periods of activity, and devastating landslides may result.
With technological disasters, local communities need to make inventories of the hazardous industrial activities in their midst. There are now ample examples from past major accidents of what these hazards can lead to, should a failure in a process or containment occur. Quite detailed plans now exist for chemical accidents around hazardous installations in many developed countries.
Risk Assessment
After evaluating a hazard and its likely impacts, the next step is to undertake a risk assessment. Hazard may be defined as the possibility of harm, and risk is the probability of lives being lost, persons injured or property damaged due to a given type and magnitude of natural hazard. Risk can be quantitatively defined as:
Risk = value x vulnerability x hazard
where value can represent a potential number of lives or capital value (of buildings, for example) which may be lost in the event. Ascertaining vulnerability is a key part of risk assessment: for buildings it is the measure of the intrinsic susceptibility of structures exposed to potentially damaging natural phenomena. For example, the likelihood of a building collapsing in an earthquake can be determined from its location relative to a fault line and the seismic resistance of its structure. In the above equation the degree of loss resulting from the occurrence of a natural phenomenon of a given magnitude can be expressed on a scale from 0 (no damage) to 1 (total loss), while hazard is the specific risk expressed as a probability of preventable loss per unit time. Vulnerability is therefore the fraction of value that is likely to be lost as a result of an event. The information needed for making a vulnerability analysis can come, for example, from surveys of homes in hazard areas by architects and engineers. Figure 1 provides some typical risk curves.
Figure 1. Risk is a product of hazard and vulnerability: typical curve shapes
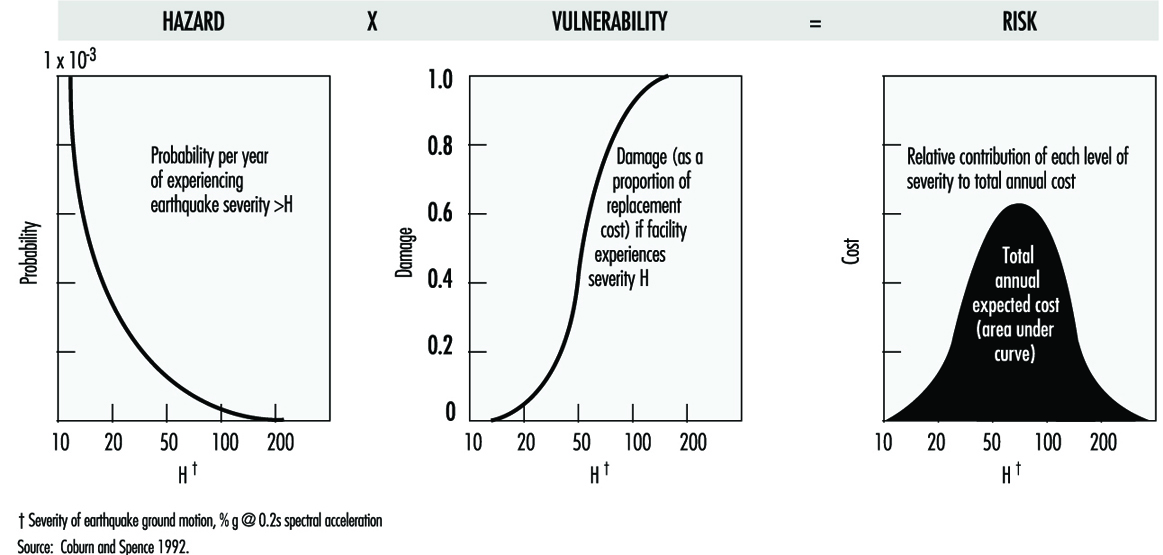
Vulnerability assessments utilizing information on different causes of death and injury according to the different types of impact are much more difficult to undertake at the present time, as the data on which to base them are crude, even for earthquakes, since standardization of injury classifications and even the accurate recording of the number, let alone the causes of deaths, are not yet possible. These serious limitations show the need for much more effort to be put into epidemiological data-gathering in disasters if preventive measures are to develop on a scientific basis.
At present mathematical computation of risk of building collapse in earthquakes and from ash falls in volcanic eruptions can be digitalized onto maps in the form of risk scales, to graphically demonstrate those areas of high risk in a foreseeable event and predict where, therefore, civil defence preparedness measures should be concentrated. Thus risk assessment combined with economic analysis and cost effectiveness will be invaluable in deciding between different options for risk reduction.
In addition to building structures, the other important aspect of vulnerability is infrastructure (lifelines) such as:
- transport
- telecommunications
- water supplies
- sewer systems
- electricity supplies
- health care facilities.
In any natural disaster all of these are at risk of being destroyed or heavily damaged, but as the type of destructive force may differ according to the natural or technological hazard, appropriate protective measures need to be devised in conjunction with the risk assessment. Geographical information systems are modern computer techniques for mapping different data sets to assist in such tasks.
In planning for chemical disasters, quantified risk assessment (QRA) is used as a tool to determine the probability of plant failure and as a guide for decision makers, by providing numerical estimates of risk. Engineering techniques for making this type of analysis are well advanced, as are the means of developing hazard zone maps around hazardous installations. Methods exist for predicting pressure waves and concentrations of radiant heat at different distances from the sites of vapour or flammable gas explosions. Computer models exist for predicting the concentration of denser-than-air gases for kilometres downwind from an accidental release in specified amounts from a vessel or plant under different weather conditions. In these incidents vulnerability mainly has to do with the proximity of housing, schools, hospitals and other key installations. Individual and societal risks need to be computed for the different types of disaster and their significance should be communicated to the local population as part of overall disaster planning.
Risk Reduction
Once vulnerability has been assessed, the feasible measures to reduce vulnerability and overall risk need to be devised.
Thus new buildings should be made seismic resistant if built in a seismic zone, or old buildings can be retrofitted so that they are less likely to collapse. Hospitals may need resiting or “hardening” against hazards such as windstorms, for example. The need for good roads as evacuation routes must never be forgotten in land developments in areas at risk of windstorms or volcanic eruptions and a host of other civil engineering measures can be enacted depending upon the situation. In the longer term the most important measure is the regulation of land use to prevent the development of settlements in hazardous areas, such as flood plains, the slopes of active volcanoes or around major chemical plants. Over-reliance on engineering solutions can bring false reassurance in at-risk areas, or be counterproductive, increasing the risk of rare catastrophic events (e.g., building levees along major rivers prone to severe flooding).
Emergency Preparedness
The planning and organization of emergency preparedness should be a task for a multidisciplinary planning team involved at the community level, and one which should be integrated into hazard assessment, risk reduction and emergency response. In the management of casualties it is now well recognized that medical teams from outside may take at least three days to arrive at the scene in a developing country. As most preventable deaths occur within the first 24 to 48 hours, such assistance will arrive too late. Thus it is at the local level that emergency preparedness should be focused, so that the community itself has the means to begin rescue and relief actions immediately after an event.
Providing adequate information to the public in the planning phase should therefore be a key aspect of emergency preparation.
Information and communication needs
On the basis of the hazard and risk analyses, the means of providing early warning will be essential, together with a system for evacuating people from areas of high risk should an emergency arise. Pre-planning of communications systems between the different emergency services at the local and national levels is necessary and for the effective provision and dissemination of information in a disaster a formal chain of communication will have to be established. Other measures such as stockpiling emergency food and water supplies in households may be included.
A community near a hazardous installation needs to be aware of the warning it may receive in an emergency (e.g., a siren if there is a gas release) and the protective measures people should adopt (e.g., immediately go inside houses and close windows until advised to come out). An essential feature of a chemical disaster is the need to be able to rapidly define the health hazard posed by a toxic release, which means identifying the chemical or chemicals involved, having access to knowledge of their acute or long-term effects and determining who, if anyone, in the general population has been exposed. Establishing lines of communication with poison information and chemical emergency centres is an essential planning measure. Unfortunately it may be difficult or impossible to know the chemicals involved in the event of runaway reactions or chemical fires, and even if it is easy to identify a chemical, knowledge of its toxicology in humans, particularly chronic effects, may be sparse or non-existent, as was found after the release of methyl isocyanate at Bhopal. Yet without information on the hazard, the medical management of casualties and the exposed population, including decisions on the need for evacuation from the contaminated area, will be severely hampered.
A multidisciplinary team to gather information and to undertake rapid health risk assessments and environmental surveys to exclude contamination of ground, water and crops should be pre-planned, recognizing that all available toxicological databases may be inadequate for decision making in a major disaster, or even in small incidents in which a community believes it has suffered serious exposure. The team should have the expertise to confirm the nature of the chemical release and to investigate its likely health and environmental impacts.
In natural disasters, epidemiology is also important for making an assessment of the health needs in the post-impact phase and for infectious diseases surveillance. Information gathering on the effects of the disaster is a scientific exercise which should also be part of a response plan; a designated team should undertake this work to provide important information for the disaster coordinating team as well as for assisting in the modification and improvement of the disaster plan.
Command and control and emergency communications
The designation of the emergency service in charge, and the constitution of a disaster coordinating team, will vary from country to country and with the type of disaster, but it needs to be pre-planned. At the scene a specific vehicle may be designated as the command and control, or onsite coordinating centre. For example, emergency services cannot rely on telephone communications, as these may become overloaded, and so radio links will be needed.
The hospital major incident plan
The capability of hospitals in terms of staff, physical reserves (theatres, beds and so on) and treatment (medicines and equipment) for dealing with any major incident will need to be assessed. Hospitals should have specific plans for dealing with a sudden large influx of casualties, and there should be provision for a hospital flying squad to go to the scene to work with search and rescue teams in extricating trapped victims or to undertake field triage of large numbers of casualties. Major hospitals may be unable to function because of disaster damage, as happened in the earthquake in Mexico City in 1985. Restoring or supporting devastated health services may therefore be necessary. For chemical incidents, hospitals should have established links with poison information centres. As well as being able to draw on a large fund of health care professionals from inside or outside a disaster area to cope with the injured, planning should also include the means for the rapid sending of emergency medical equipment and drugs.
Emergency equipment
The types of search and rescue equipment needed for a specific disaster should be identified at the planning stage along with where it will be stored, as it will need to be rapidly deployed in the first 24 hours, when the most lives can be saved. Key medicines and medical equipment need to be available for rapid deployment, along with personal protective equipment for emergency crews, including health workers at the disaster scene. Engineers skilled in urgently restoring water, electricity, communications and roads can have a major role in alleviating the worst effects of disasters.
Emergency response plan
The separate emergency services and the health care sector, including public health, occupational health and environmental health practitioners, should each have plans for dealing with disasters, which can be incorporated together as one major disaster plan. In addition to the hospital plans, health planning should include detailed response plans for different types of disaster, and these need to be devised in the light of the hazard and risk assessments produced as part of disaster preparedness. Treatment protocols should be drawn up for the specific types of injury that each disaster may produce. Thus a range of traumas, including crush syndrome, should be anticipated from the collapse of buildings in earthquakes, whereas body burns and inhalational injuries are a feature of volcanic eruptions. In chemical disasters, triage, decontamination procedures, the administration of antidotes where applicable and emergency treatment of acute pulmonary injury from irritant toxic gases should all be planned for. Forward planning should be flexible enough to cope with transport emergencies involving toxic substances, especially in areas without fixed installations which would normally require the authorities to make intensive local emergency plans. The emergency management of physical and chemical trauma in disasters is a vital area of health care planning and one which requires training of hospital staff in disaster medicine.
The management of evacuees, the location of evacuation centres and the appropriate preventive health measures should be included. The need for emergency stress management to prevent stress disorders in victims and emergency workers should also be considered. Sometimes psychological disorders may be the predominant or even the only health impact, particularly if the response to an incident has been inadequate and engendered undue anxiety in the community. This is also a special problem of chemical and radiation incidents which can be minimized with adequate emergency planning.
Training and education
Medical staff and other health care professionals at the hospital and primary care level are likely to be unfamiliar with working in disasters. Training exercises involving the health sector and the emergency services are a necessary part of emergency preparedness. Table-top exercises are invaluable and should be made as realistic as possible, since large-scale physical exercises are likely to be held very infrequently because of their high cost.
Post-impact recovery
This phase is the returning of the affected area to its pre-disaster state. Pre-planning should include post-emergency social, economic and psychological care and rehabilitation of the environment. For chemical incidents the latter also includes environmental assessments for contaminants of water and crops, and remedial actions, if needed, such as decontamination of soils and buildings and restoration of potable water supplies.
Conclusion
Relatively little international effort has been put into disaster preparedness compared to relief measures in the past; however, although investment in disaster protection is costly, there is now a large body of scientific and technical knowledge available which if applied correctly would make a substantial difference to the health and economic impacts of disasters in all countries.
Disasters and Major Accidents
Type and Frequency of Disasters
In 1990, the 44th General Assembly of the United Nations launched the decade for the reduction of frequency and impact of natural disasters (Lancet 1990). A committee of experts endorsed a definition of disasters as “a disruption of the human ecology that exceeds the capacity of the community to function normally”.
Over the past few decades, disaster data on a global level reveal a distinct pattern with two main features—an increase over time of the number of people affected, and a geographical correlation (International Federation of Red Cross and Red Crescent Societies (IFRCRCS) 1993). In figure 1, despite the great variation from year to year, a definite rising trend is quite visible. Figure 2 shows the countries most severely affected by major disasters in 1991. Disasters affect every country of the world, but it is the poorest countries where people most frequently lose their lives.
Figure 1. Number of persons affected worldwide by disasters per year during 1967-91
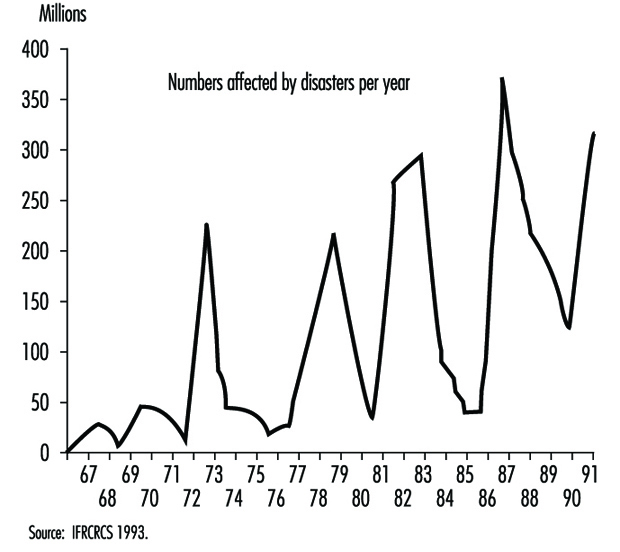
Figure 2. Number of people dead from major disasters in 1991: Top 20 countries
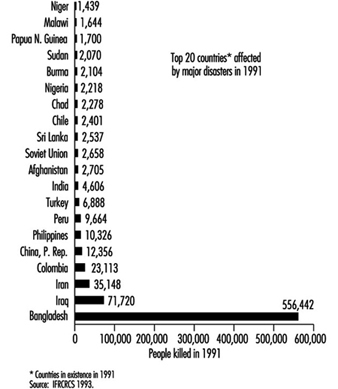
Numerous and different definitions and classifications of disasters are available and have been reviewed (Grisham 1986; Lechat 1990; Logue, Melick and Hansen 1981; Weiss and Clarkson 1986). Three of them are mentioned here as examples: The US Centers for Disease Control (CDC 1989) identified three major categories of disasters: geographical events such as earthquakes and volcanic eruptions; weather-related problems, including hurricanes, tornadoes, heat waves, cold environments and floods; and, finally, human-generated problems, which encompass famines, air pollutions, industrial disasters, fires and nuclear reactor incidents. Another classification by cause (Parrish, Falk and Melius 1987) included weather and geological events among natural disasters, whereas human-made causes were defined as non-natural, technological, purposeful events perpetuated by people (e.g., transportation, war, fire/explosion, chemical and radioactive release). A third classification (table1), compiled at the Centre for Research on the Epidemiology of Disaster in Louvain, Belgium, was based on a workshop convened by the UN Disaster Relief Organization in 1991 and was published in the World Disaster Report 1993 (IFRCRCS 1993).
Table 1. Definitions of disaster types
|
Sudden natural |
Long-term natural |
Sudden human-made |
Long-term human-made |
|
Avalanche Cold wave Earthquake Aftershock Floods Flash flood Dam collapse Volcanic eruption Glowing Heat wave High wind Storm Hail Sand storm Storm surges Thunder storm Tropical storm Tornado Insect infestation Landslide Earth flow Power shortage Tsunami and tidal |
Epidemics Drought Desertification Famine Food shortage or |
Structural collapse Building collapse Mine collapse or cave-in Air disaster Land disaster Sea disaster Industrial/technological Explosions Chemical explosions Nuclear explosion Mine explosions Pollution Acid rain Chemical pollution Atmosphere pollution Chlorofluoro-carbons Oil pollution Fires Forest/grassland fire |
National (civil strife, International Displaced population Displaced persons Refugees |
Source: IFRCRCS 1993.
Figure 3 reports the number of events for individual disaster types. The item “Accidents” includes all sudden human-made events, and is second only to “Flood” in frequency. “Storm” is in third place, followed by “Earthquake” and “Fire”.
Figure 3. 1967-91: Total number of events for each type of disaster
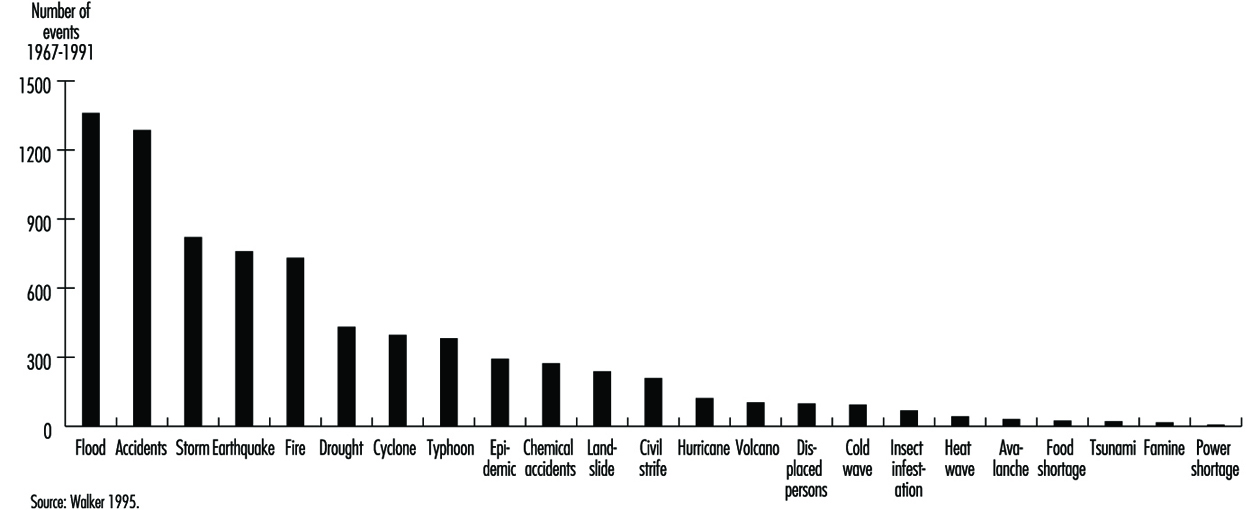
Additional information on type, frequency and consequences of natural and non-natural disasters between 1969 and 1993 has been drawn from data of the IFRCRCS 1993.
Although agencies measure the severity of disasters by the number of people killed, it is becoming increasingly important also to look at the number affected. Across the world, almost a thousand times more people are affected by disaster than are killed and, for many of these people, survival after the disaster is becoming increasingly difficult, leaving them more vulnerable to future shocks. This point is relevant not only for natural disasters (table 2) but also human-made disasters (table 3), especially in the case of chemical accidents whose effects on exposed people may become apparent after years or even decades (Bertazzi 1989). Addressing human vulnerability to disaster is at the heart of disaster preparedness and prevention strategies.
Table 2. Number of victims of disasters with a natural trigger from 1969 to 1993: 25-year average by region
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Killed |
76,883 |
9,027 |
56,072 |
2,220 |
99 |
144,302 |
|
Injured |
1,013 |
14,944 |
27,023 |
3,521 |
100 |
46,601 |
|
Otherwise affected |
10,556,984 |
4,400,232 |
105,044,476 |
563,542 |
95,128 |
120,660,363 |
|
Homeless |
172,812 |
360,964 |
3,980,608 |
67,278 |
31,562 |
4,613,224 |
Source: Walker 1995.
Table 3. Number of victims of disasters with a non-natural trigger from 1969 to 1993: 25-year average by region
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Killed |
16,172 |
3,765 |
2,204 |
739 |
18 |
22,898 |
|
Injured |
236 |
1,030 |
5,601 |
483 |
476 |
7,826 |
|
Affected |
3,694 |
48,825 |
41,630 |
7,870 |
610 |
102,629 |
|
Homeless |
2,384 |
1,722 |
6,275 |
7,664 |
24 |
18,069 |
Source: Walker 1995.
Drought, famine and floods continue to affect far more people than any other type of disaster. High winds (cyclones, hurricanes and typhoons) cause proportionally more deaths than famines and floods, in relation to the affected population as a whole; and earthquakes, the most sudden-onset disaster of all, continue to have the greatest ratio of deaths to affected population (table 4). Technological accidents affected more people than fires (table 5).
Table 4. Number of victims of disasters with a natural trigger from 1969 to 1993: 25-year average by type
|
Earthquake |
Drought |
Flood |
High wind |
Landslide |
Volcano |
Total |
|
|
Killed |
21,668 |
73,606 |
12,097 |
28,555 |
1,550 |
1,009 |
138,486 |
|
Injured |
30,452 |
0 |
7,704 |
7,891 |
245 |
279 |
46,571 |
|
Affected |
1,764,724 |
57,905,676 |
47,849,065 |
9,417,442 |
131,807 |
94,665 |
117,163,379 |
|
Homeless |
224,186 |
22,720 |
3,178,267 |
1,065,928 |
106,889 |
12,513 |
4,610,504 |
Source: Walker 1995.
Table 5. Disasters and Major Accidents
|
Accident |
Technological accident |
Fire |
Total |
|
|
Killed |
3,419 |
603 |
3,300 |
7,321 |
|
Injured |
1,596 |
5,564 |
699 |
7,859 |
|
Affected |
17,153 |
52,704 |
32,771 |
102,629 |
|
Homeless |
868 |
8,372 |
8,829 |
18,069 |
Source: Walker 1995.
Table 6 and table 7 show the number of grouped disaster types over 25 years, by continent. High winds, accidents (mostly transport accidents) and floods account for the largest number of disaster events, with the largest proportion of events being in Asia. Africa accounts for the vast majority of the world’s drought events. While few people are killed by disasters in Europe, the region suffers from disaster events on a scale comparable to that in Asia or Africa, the lower mortality figures reflecting a much lower human vulnerability to crisis. A clear example is the comparison of the human death tolls after the chemical accidents in Seveso (Italy) and in Bhopal (India) (Bertazzi 1989).
Table 6. Disasters with a natural trigger from 1969 to 1993: Number of events over 25 years
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Earthquake |
40 |
125 |
225 |
167 |
83 |
640 |
|
Drought and famine |
277 |
49 |
83 |
15 |
14 |
438 |
|
Flood |
149 |
357 |
599 |
123 |
138 |
1,366 |
|
Landslide |
11 |
85 |
93 |
19 |
10 |
218 |
|
High wind |
75 |
426 |
637 |
210 |
203 |
1,551 |
|
Volcano |
8 |
27 |
43 |
16 |
4 |
98 |
|
Other* |
219 |
93 |
186 |
91 |
4 |
593 |
* Other includes: avalanche, cold wave, heat wave, insect infestation, tsunami.
Source: Walker 1995.
Table 7. Disasters with a non-natural trigger from 1969 to 1993: Number of events over 25 years
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Accident |
213 |
321 |
676 |
274 |
18 |
1,502 |
|
Technological accident |
24 |
97 |
97 |
88 |
4 |
310 |
|
Fire |
37 |
115 |
236 |
166 |
29 |
583 |
Source: Walker 1995.
Figures for 1994 (table 8 and table 9) show that Asia continues to be the most disaster-prone region, with major accidents, floods and high wind disasters being the most common event types. Earthquakes, while causing high death rates per event, are in fact no more common than major technological disasters. The one-year average number of non-natural events, apart from fire, is slightly diminished in comparison with the preceding 25-year period. The average numbers of natural disasters, instead, were higher, with the exception of floods and volcanoes. In 1994, Europe had more human-made disasters than Asia (39 versus 37).
Table 8. Disasters with a natural trigger: Number by global region and type in 1994
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Earthquake |
3 |
3 |
12 |
1 |
1 |
20 |
|
Drought and famine |
0 |
2 |
1 |
0 |
1 |
4 |
|
Flood |
15 |
13 |
27 |
13 |
0 |
68 |
|
Landslide |
0 |
1 |
3 |
1 |
0 |
5 |
|
High wind |
6 |
14 |
24 |
5 |
2 |
51 |
|
Volcano |
0 |
2 |
5 |
0 |
1 |
8 |
|
Other* |
2 |
3 |
1 |
2 |
0 |
8 |
* Other includes: avalanche, cold wave, heat wave, insect infestation, tsunami.
Source: Walker 1995.
Table 9. Disasters with a non-natural trigger: Number by global region and type in 1994
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Accident |
8 |
12 |
25 |
23 |
2 |
70 |
|
Technological accident |
1 |
5 |
7 |
7 |
0 |
20 |
|
Fire |
0 |
5 |
5 |
9 |
2 |
21 |
Source: Walker 1995.
Major Chemical Accidents
In this century, the worst non-natural disasters resulting in human suffering and death have been caused by wars, transport and industrial activities. At first, industrial disasters mainly affected people engaged in specific occupations, but later, particularly after the Second World War with the rapid growth and expansion of the chemical industry and the use of nuclear power, these occurrences led to serious danger even to people outside work areas, and to the general environment. We focus here on major accidents involving chemicals.
The first documented chemical disaster with industrial origins goes back to the 1600s. It was described by Bernardino Ramazzini (Bertazzi 1989). Today’s chemical disasters differ in the way they happen and in the type of chemicals involved (ILO 1988). Their potential hazard is a function both of the inherent nature of the chemical and the quantity that is present on site. A common feature is that they usually are uncontrolled events involving fires, explosions or releases of toxic substances that result either in the death and injury of a large number of people inside or outside the plant, extensive property and environmental damage, or both.
Table 10 gives some examples of typical major chemical accidents due to explosions. Table 11 lists some major fire disasters. Fires occur in industry more frequently than explosions and toxic releases, although the consequences in terms of loss of life are generally less. Better prevention and preparedness might be the explanation. Table 12 lists some major industrial accidents involving toxic releases of different chemicals. Chlorine and ammonia are the toxic chemicals most commonly used in major hazard quantities, and both have a history of major accidents. The release of flammable or toxic materials in the atmosphere may also lead to fires.
Table 10. Examples of industrial explosions
|
Chemical involved |
Consequences |
Place and date |
|
|
Death |
Injuries |
||
|
Dimethyl ether |
245 |
3,800 |
Ludwigshafen, Federal Republic of Germany, 1948 |
|
Kerosene |
32 |
16 |
Bitburg, Federal Republic of Germany, 1948 |
|
Isobutane |
7 |
13 |
Lake Charles, Louisiana, United States, 1967 |
|
Oil slops |
2 |
85 |
Pernis, Netherlands, 1968 |
|
Propylene |
– |
230 |
East Saint Louis, Illinois, United States, 1972 |
|
Propane |
7 |
152 |
Decatur, Illinois, United States, 1974 |
|
Cyclohexane |
28 |
89 |
Flixborough, United Kingdom, 1974 |
|
Propylene |
14 |
107 |
Beek, Netherlands, 1975 |
Adapted from ILO 1988.
Table 11. Examples of major fires
|
Chemical involved |
Consequences |
Place and date |
|
|
Death |
Injuries |
||
|
Methane |
136 |
77 |
Cleveland, Ohio, United States, 1944 |
|
Liquefied petroleum gas |
18 |
90 |
Ferzyn, France, 1966 |
|
Liquefied natural gas |
40 |
– |
Staten Island, New York, United States, 1973 |
|
Methane |
52 |
– |
Santa Cruz, Mexico, 1978 |
|
Liquefied petroleum gas |
650 |
2,500 |
Mexico City, Mexico, 1985 |
Adapted from ILO 1988.
Table 12. Examples of major toxic releases
|
Chemical involved |
Consequences |
Place and date |
|
|
Death |
Injuries |
||
|
Phosgene |
10 |
– |
Poza Rica, Mexico, 1950 |
|
Chlorine |
7 |
– |
Wilsum, Federal Republic of Germany, 1952 |
|
Dioxin/TCDD |
– |
193 |
Seveso, Italy, 1976 |
|
Ammonia |
30 |
25 |
Cartagena, Colombia, 1977 |
|
Sulphur dioxide |
– |
100 |
Baltimore, Maryland, United States, 1978 |
|
Hydrogen sulphide |
8 |
29 |
Chicago, Illinois, United States, 1978 |
|
Methyl isocyanate |
2,500 |
200,000 |
Bhopal, India, 1984 |
Adapted from ILO 1988.
A review of the literature concerning major chemical disasters enables us to identify several other common characteristics of today’s industrial disasters. We will review them briefly, to provide not only a classification of general value, but also an appreciation of the nature of the problem and the challenges that face us.
Overt Disasters
Overt disasters are environmental releases which leave no ambiguity about their sources and their potential harm. Examples are Seveso, Bhopal and Chernobyl.
Seveso plays the role of prototype for chemical industrial disasters (Homberger et al. 1979; Pocchiari et al. 1983, 1986). The accident took place on 10 July 1976 in the Seveso area, close to Milan, Italy, in a plant where trichlorophenol was produced, and it caused the contamination of several square kilometres of populated countryside by the powerfully toxic 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD). More than 700 people were evacuated, and restrictions were applied to another 30,000 inhabitants. The most clearly established health effect was chloracne, but the picture of health consequences possibly linked to this incident has not yet been completed (Bruzzi 1983; Pesatori 1995).
Bhopal represents, probably, the worst chemical industrial disaster ever (Das 1985a, 1985b; Friedrich Naumann Foundation 1987; Tachakra 1987). On the night of 2 December 1984, a gas leak caused a deadly cloud to spread over the city of Bhopal, in central India, leaving thousands dead and hundreds of thousands injured in the space of a few hours. The accident occurred because of a runaway reaction in one of the tanks in which methyl isocyanate (MIC) was stored. The concrete storage tank, containing some 42 tons of this compound, which was used to manufacture pesticides, burst open and vented MIC and other breakdown chemicals into the air. Above and beyond the obvious catastrophic impact of the accident, questions still exist as to the possible long-term consequences for the health of those affected and/or exposed (Andersson et al. 1986; Sainani et al. 1985).
Slow-Onset Disasters
Slow-onset disasters may become apparent only because human targets happen to be on the release path, or because, as time passes, some environmental evidence of a threat from noxious materials crops up.
One of the most impressive and instructive examples of the first type is “Minamata disease”. In 1953 unusual neurological disorders began to strike people living in fishing villages along Minamata Bay, Japan. The disease was named kibyo, the “mystery illness”. After numerous investigations, poisoned fish emerged as the probable culprit, and in 1957 the disease was produced experimentally by feeding cats with fish caught in the bay. The following year, the suggestion was put forward that the clinical picture of kibyo, which included polyneuritis, cerebellar ataxia and cortical blindness, was similar to that due to poisoning by alkyl mercury compounds. A source of organic mercury had to be sought, and it was eventually found in a factory discharging its effluent into Minamata Bay. By July 1961, the disease had occurred in 88 persons, of whom 35 (40%) had died (Hunter 1978).
An example of the second type is Love Canal, an excavation site near Niagara Falls in the United States. The area had been used as a chemical and municipal disposal site over a period of about 30 years, until 1953. Homes were later built next to the landfill. In the late 1960s, there were complaints of chemical odours in home basements, and chemical leaching in areas surrounding the site began to be reported with increasing frequency over time. In the 1970s, residents began to fear that a serious threat to their health could arise, and this shared perception prompted environmental and health investigations to be carried out. None of the published studies could conclusively support a causal link between exposure to chemicals at the disposal site and adverse health effects among the residents. Yet, there is no doubt that serious social and psychological consequences have resulted among the population in the area, particularly those who were evacuated (Holden 1980).
Mass Food Poisonings
Outbreaks of food poisoning can be caused by toxic chemicals released into the environment through the use of chemicals in the handling and processing of food. One of the most serious episodes of this type occurred in Spain (Spurzem and Lockey 1984; WHO 1984; Lancet 1983). In May 1981, an outbreak of a previously unknown syndrome began to appear in the working-class suburbs of Madrid. Over 20,000 persons were ultimately involved.
By June 1982, 315 patients had died (around 16 deaths per 1,000 cases). Initially, the clinical features included interstitial pneumonitis, diverse skin rashes, lymphadenopathies, intense eosinophilia, and gastro-intestinal symptoms. Nearly one-fourth of those who survived the acute phase required later hospitalization for neuromuscular alterations. Schleroderma-like changes of the skin also were observed in this late stage along with pulmonary hypertension and Raynaud’s phenomenon.
One month after the occurrence of the first cases, the illness was found to be associated with the consumption of inexpensive denatured rapeseed oil, sold in unlabelled plastic containers and usually acquired from itinerant salesmen. The warning issued by the Spanish government against the consumption of the suspected oil caused a dramatic fall in the number of hospitalizations from toxic pneumonitis (Gilsanz et al. 1984; Kilbourne et al. 1983).
Polychlorinated biphenyls (PCBs) were involved in other widely reported accidental mass food poisonings in Japan (Masuda and Yoshimura 1984) and in Taiwan (Chen et al. 1984).
Transnational Disasters
Today’s human-made disasters do not necessarily respect national political boundaries. An obvious example is Chernobyl, whose contamination reached from the Atlantic Ocean to the Ural Mountains (Nuclear Energy Agency, 1987). Another example comes from Switzerland (Friedrich Naumann Foundation 1987; Salzman 1987). On 1 November 1986, shortly after midnight, a fire developed in a warehouse operated by the multinational pharmaceutical company Sandoz in Schweizerhalle, 10 km southeast of Basel, and some 30 tons of the chemicals stored in the warehouse were drained along with water from the fire-fighting into the nearby River Rhine. Severe ecological damage occurred over a length of about 250 km. Apart from symptoms of irritation reported in the parts of the Basel area reached by gases and vapours produced by the fire, no cases of serious illness were reported. Nonetheless, this accident triggered serious concern in at least four European countries (Switzerland, France, Germany, The Netherlands).
Transnationality applies not only to consequences and harm caused by disasters, but also to their remote causes. Bhopal might serve as an example. In analysing the causes of that disaster, some persons reached the conclusion that “The Bhopal disaster occurred because of specific acts and decisions which were taken in Danbury, Connecticut or elsewhere in the corporate superstructure, but not in Bhopal.” (Friedrich Naumann Foundation 1987.)
“Developing” Disasters
The emerging pattern of industrialization as well as modernization of agriculture in developing countries involves the application and use of imported or adopted technology and products, within contexts which are quite different from those in which they were intended to be used. Businesses facing the tightening of regulations in industrial countries may export hazardous industries to world regions where less stringent measures for protection of the environment and public health exist. Industrial activities become concentrated in existing urban settlements and add significantly to the pressure caused by overcrowding and shortages of community services. Such activities are distributed between a small highly organized sector and a large unorganized sector; governmental controls in regard to labour and environmental safety in the latter sector are less stringent (Krishna Murti 1987). An example comes from Pakistan, where among 7,500 field workers in a malaria control programme in 1976, as many as 2,800 experienced some form of toxicity (Baker et al. 1978). It was also estimated that about 500,000 acute pesticide poisonings occur annually, resulting in about 9,000 deaths, and that only about 1% of the deadly cases occur in industrialized countries, although those countries consume about 80% of the total world agrochemical production (Jeyaratnam 1985).
It has also been argued that developing societies might actually find themselves carrying a double burden instead of being cleared from the one of underdevelopment. It could be, in fact, that the consequences of improper industrialization are simply being added to those of the countries’ underdeveloped states (Krishna Murti 1987). It is clear, thus, that international cooperation ought to be urgently strengthened in three domains: scientific work, public health and industrial siting and safety policies.
Lessons for the Future
Despite the variety of the reviewed industrial disasters, some common lessons have been learned on how to prevent their occurrence, and also on how to mitigate the impact of major chemical disasters on the population. In particular:
- Different experts should be on the scene working in close coordination; they should usually cover the fields related to the environmental fate of the agent, its toxic properties to humans and biota, analytical methods, clinical medicine and pathology, biostatistics and epidemiology.
- Based on pre-existing and/or early available evidence, a comprehensive study plan should be developed as early as possible to identify goals, problems and resource requirements.
- Early phase activities affect the course of any subsequent action. Since long-term effects should be expected after virtually every type of industrial disaster, great care should be devoted to insure availability of requisite information for later studies (e.g., proper identifiers of the exposed for follow-up).
- In planning long-term investigations, feasibility should be given high consideration to facilitate scientific and public health achievements and clarity of communication.
- Overall, for reasons of validity and cost effectiveness, it is advisable to rely on “hard” information, whenever available, either in identifying and enumerating the study population (e.g., residence) or in estimating exposure (e.g., environmental and biological measurements) and choosing the endpoints (e.g., mortality).
Control of Major Hazard Installations for the Prevention of Major Accidents
The objective of this article is to provide guidance for establishing a system to control major hazard installations. Two ILO documents and the more recent ILO Convention (see "ILO Convention") form the basis of the first part of this article. The European Directive forms the basis for the second part of this article.
The ILO Perspective
Much of what follows has been extracted from two documents Prevention of Major Industrial Accidents (ILO 1991) and Major Hazard Control: A Practical Manual (ILO 1988). The document “Convention concerning the Prevention of Major Industrial Accidents” (ILO 1993) (see "ILO Convention") serves to complement and update material from the earlier two documents. Each of these documents proposes ways to protect workers, the public and the environment against the risk of major accidents by (1) preventing major accidents from occurring at these installations and (2) minimizing the consequences of a major accident onsite and offsite, for example by (a) arranging appropriate separation between major hazard installations and housing and other centres of population nearby, such as hospitals, schools and shops, and (b) appropriate emergency planning.
The 1993 ILO Convention should be referred to for specifics; what follows is more of a narrative overview of the document.
Major hazard installations possess the potential, by virtue of the nature and quantity of hazardous substances present, to cause a major accident in one of the following general categories:
- the release of toxic substances in tonnage quantities which are lethal or harmful even at considerable distances from the point of release through contamination of air, water and/or soil
- the release of extremely toxic substances in kilogram quantities, which are lethal or harmful even at considerable distance from the point of release
- the release of flammable liquids or gases in tonnage quantities, which may either burn to produce high levels of thermal radiation or form an explosive vapour cloud
- the explosion of unstable or reactive materials.
Member country obligations
The 1993 Convention expects member countries who are not immediately able to implement all of the preventive and protective measures provided for in the Convention:
- to draw up plans, in consultation with the most representative organizations of employers and workers, and with other interested parties who may be affected, for the progressive implementation of said measures within a fixed time-frame
- to implement and periodically review a coherent national policy concerning the protection of workers, the public and the environment against the risk of major accidents
- to implement the policy through preventive and protective measures for major hazard installations and, where, practicable, promote the use of the best available safety technologies and
- to apply the Convention in accordance with national law and practice.
Components of a major hazard control system
The variety of major accidents leads to the concept of major hazard as an industrial activity requiring controls over and above those applied in normal factory operations, in order to protect both workers and people living and working outside. These controls aim not only at preventing accidents but also at mitigating the consequences of any accidents which could occur.
Controls need to be based on a systematic approach. Basic components of this system are:
- identification of major hazard installations together with their respective threshold quantities and inventory. Governmental authorities and employers should require the identification of major hazard installations on a priority basis; these should be regularly reviewed and updated.
- information about the installation. Once the major hazard installations have been identified, additional information needs to be collected about their design and operation. The information should be gathered and arranged systematically, and should be accessible to all parties concerned within the industry and outside the industry. In order to achieve a complete description of the hazards, it may be necessary to carry out safety studies and hazard assessments to discover possible process failures and to set priorities during the process of hazard assessment.
- special provision to protect confidential information
- action inside the industrial activity. Employers have the primary responsibility for operating and maintaining a safe facility. A sound safety policy is required. Technical inspection, maintenance, facility modification, training and selecting of suitable personnel must be carried out according to standard quality control procedures for major hazard installations. In addition to the preparation of the safety report, accidents of any type should be investigated and copies of reports submitted to the competent authority.
- actions by the government or other competent authorities. Assessment of the hazards for the purposes of licensing (where appropriate), inspection and enforcement of legislation. Land-use planning can appreciably reduce the potential for a disaster. The training of factory inspectors also is an important role of the government or other competent authority.
- emergency planning. This aims at the reduction of the consequences of major accidents. In setting up emergency planning, a distinction is made between onsite and offsite planning.
The responsibilities of employers
Major hazard installations have to be operated at a very high standard of safety. In addition, employers play a key role in the organization and implementation of a major hazard control system. In particular, as outlined in table 13, employers have the responsibility to:
- Provide the information required to identify major hazard installations within a fixed time-frame.
- Carry out the hazard assessment.
- Report to the competent authority on the results of the hazard assessment.
- Introduce technical measures, including design, safety systems construction, choice of chemicals, operation, maintenance and systematic inspection of the installation.
- Introduce organizational measures, including, among others, training and instruction of personnel and staffing levels.
- Set up an emergency plan.
- Take measures to improve plant safety and limit the consequences of an accident.
- Consult with workers and their representatives.
- Improve the system by learning from near misses and related information.
- Ensure that quality control procedures are in effect and audit these periodically.
- Notify the competent authority before any permanent closure of a major hazard installation.
Table 13. The role of major hazard installations management in hazard control
|
Actions (depending on local legislation) |
Action in the event of a major |
|||
|
Provide notification to authorities |
Provide information on |
Prepare an onsite emergency plan |
Inform the public about the major hazard |
Notify authority about major accident |
|
Prepare and submit safety report |
Provide further information on request |
Provide information to local authority to enable it to draw |
Provide information on major accident |
|
First and foremost, employers of installations which can cause a major accident have a duty to control this major hazard. To do this, they must be aware of the nature of the hazard, of the events that cause accidents, and of the potential consequences of such accidents. This means that, in order to control a major hazard successfully, employers must have answers to the following questions:
- Do toxic, explosive or flammable substances in the facility constitute a major hazard?
- Do chemicals or agents exist which, if combined, could become a toxic hazard?
- Which failures or errors can cause abnormal conditions leading to a major accident?
- If a major accident occurs, what are the consequences of a fire, an explosion or a toxic release for the employees, people living outside the facility, the plant or the environment?
- What can management do to prevent these accidents from happening?
- What can be done to mitigate the consequences of an accident?
Hazard assessment
The most appropriate way to answer the above questions is to carry out a hazard assessment, the purpose of which is to understand why accidents occur and how they can be avoided or at least mitigated. Methods which can be used for an assessment are summarized in table 14.
Table 14. Working methods for hazard assessment
|
Method |
Purpose |
Aim |
Working principle |
|
1. Preliminary hazard analysis |
1. Identification of hazards |
1. Completeness of safety concept |
1. Use of “thinking aids” |
|
2. Matrix diagrams of |
|||
|
3. Use of check-lists |
|||
|
4. Failure effect |
2. Use of “searching |
||
|
5. Hazard and |
|||
|
6. Accident sequence |
2. Assessment of hazard according to |
2. Optimization of |
3. Graphic description |
|
7. Fault tree analysis |
|||
|
8. Accident consequence analysis |
3. Assessment of accident consequences |
3. Mitigation of |
4. Mathematical |
Source: ILO 1988.
Safe operation
A general outline of how the hazards should be controlled will be given.
Plant component design
A component has to withstand the following: static loads, dynamic loads, internal and external pressure, corrosion, loads arising from large differences in temperature, loads arising from external impacts (wind, snow, earthquakes, settling). Design standards are therefore a minimum requirement as far as major hazard installations are concerned.
Operation and control
When an installation is designed to withstand all loads that can occur during normal or foreseen abnormal operating conditions, it is the task of a process control system to keep the plant safely within these limits.
In order to operate such control systems, it is necessary to monitor the process variables and active parts of the plant. Operating personnel should be well trained to be aware of the mode of operation and the importance of the control system. To ensure that the operating personnel do not have to rely solely on the functioning of automatic systems, these systems should be combined with acoustic or optical alarms.
It is most important to realize that any control system will have problems in rare operating conditions such as start-up and shut-down phases. Special attention must be paid to these phases of operation. Quality control procedures will be audited by management periodically.
Safety systems
Any major hazard installation will require some form of safety system. The form and design of the system depend on the hazards present in the plant. The following gives a survey of available safety systems:
- systems preventing deviation from permissible operating conditions
- systems preventing failure of safety-related components
- safety-related utility supplies
- alarm systems
- technical protective measures
- prevention of human and organizational errors.
Maintenance and monitoring
The safety of a plant and the function of a safety-related system can only be as good as the maintenance and monitoring of these systems.
Inspection and repair
It is necessary to establish a plan for onsite inspections, for the operating personnel to follow, which should include a schedule and the operating conditions to be adhered to during inspection work. Strict procedures must be specified for carrying out repair work.
Training
As people can have a negative as well as a positive influence on plant safety, it is important to reduce the negative influences and support the positive ones. Both goals can be achieved by proper selection, training and periodic evaluation/assessment of the personnel.
Mitigation of consequences
Even if a hazard assessment has been carried out and the hazards have been detected and appropriate measures to prevent accidents have been taken, the possibility of an accident cannot be completely ruled out. For this reason, it must be part of the safety concept to plan and provide measures which can mitigate the consequences of an accident.
These measures have to be consistent with the hazards identified in the assessment. Furthermore, they must be accompanied by proper training of plant personnel, the emergency forces and responsible representatives from public services. Only training and rehearsals of accident situations can make emergency plans realistic enough to work in a real emergency.
Safety reporting to the competent authority
Depending on local arrangements in different countries, employers of a major hazard installation shall report to the appropriate competent authority. Reporting may be carried out in three steps. These are:
- identification/notification of major hazard installation (including any future changes that are to be made to the installation)
- the preparation of periodic safety reports (which shall be revised in the light of any modifications made to a facility)
- immediate reporting of any type of accident, followed by a detailed report.
Rights and duties of workers and their representatives
Workers and their representatives shall be consulted through appropriate cooperative mechanisms in order to ensure a safe system of work. They shall be consulted in the preparation of, and have access to, safety reports, emergency plans and procedures, and accident reports. They shall receive training for preventing major accidents and in emergency procedures to be followed in the event of a major accident. Finally, workers and their representatives should be able to take corrective action where needed within the scope of their duties, if they believe that there is any imminent danger of a major accident. They also have the right to notify the competent authority of any hazard.
Workers shall comply with all practices and procedures for preventing major accidents and for the control of developments likely to lead to a major accident. They shall comply with all emergency procedures should a major accident occur.
Implementation of a major hazard control system
Although the storage and use of large quantities of hazardous materials is widespread across most countries of the world, the present systems for their control will differ substantially from one country to another. This means that the speed of implementation of a major hazard control system will depend on the facilities already existing in each country, particularly with regard to trained and experienced facility inspectors, together with the resources available locally and nationally for the different components of the control system. For all countries, however, implementation will require the setting of priorities for a stage-by-stage programme.
Identification of major hazards
This is the essential starting point for any major hazard control system—the definition of what actually constitutes a major hazard. Although definitions exist in some countries and particularly in the EU, a particular country’s definition of a major hazard should reflect local priorities and practices and, in particular, the industrial pattern in that country.
Any definition for identifying major hazards is likely to involve a list of hazardous materials, together with an inventory for each, such that any major hazard installation storing or using any of these in excess quantities is by definition a major hazard installation. The next stage is to identify where the major hazard installation exists for any particular region or country. Where a country wishes to identify major hazard installations before the necessary legislation is in place, considerable progress can be achieved informally, particularly where the cooperation of industry is available. Existing sources such as factory inspectorate records, information from industrial bodies and so on, may enable a provisional list to be obtained which, apart from allowing early inspection priorities to be allocated, will enable an assessment to be made of the resources required for different parts of the control system.
Establishment of a group of experts
For countries considering establishing a major hazard control system for the first time, an important first stage is likely to be setting up a group of experts as a special unit at government level. The group will have to set priorities in deciding on its initial programme of activity. The group may be required to train factory inspectors in the techniques of major hazard inspection, including operational standards for such major hazard installations. They should also be able to provide advice about the siting of new major hazards and the use of land nearby. They will need to establish contacts in other countries in order to keep up to date with major hazard developments.
Onsite emergency preparedness
Emergency plans require that the major hazard installation be assessed for the range of accidents that could take place, together with how they would be tackled in practice. The handling of these potential accidents will require both staff and equipment, and a check should be made to ensure that both are available in sufficient numbers. The plans should include the following elements:
- assessment of the size and nature of the events foreseen and the probability of their occurrence
- formulation of the plan and liaison with outside authorities, including emergency services
- procedures: (a) raising the alarm; (b) communications within the plant and outside the plant
- appointment of key personnel and their duties and responsibilities
- emergency control centre
- action onsite and offsite.
Offsite emergency preparedness
This is an area which has received less attention than onsite emergency planning, and many countries will be faced with considering this for the first time. The offsite emergency plan will have to link the possible accidents identified by the major hazard installation, their expected likelihood of occurrence and the proximity of people living and working nearby. It must have addressed the need for the expeditious warning and evacuation of the public, and how these might be achieved. It should be remembered that conventional housing of solid construction offers substantial protection from toxic gas clouds, whereas a shanty-type house is vulnerable to such accidents.
The emergency plan must identify organizations whose help will be required in the event of an emergency and must ensure that they know what role is expected of them: hospitals and medical staff should, for example, have decided how they would handle large numbers of casualties and in particular what treatment they would provide. The offsite emergency plan will need to be rehearsed with public involvement from time to time.
Where a major accident could have transboundary effects, full information is to be provided to the jurisdictions concerned, as well as assistance in cooperation and coordination arrangements.
Siting
The basis for needing a siting policy for major hazard installations is straightforward: since absolute safety cannot be guaranteed, major hazard installations should be separated from people living and working outside the facility. As a first priority, it may be appropriate to concentrate efforts on proposed new major hazards and to try to prevent the encroachment of housing, particularly shanty houses, which are a common feature in many countries.
Training and facility inspectors
The role of the facility inspectors is likely to be central in many countries in implementing a major hazard control system. Facility inspectors will have the knowledge that will enable early identification of major hazards to take place. Where they have specialist inspectors to call upon, factory inspectors will be assisted in the often highly technical aspects of major hazard inspection.
Inspectors will need appropriate training and qualifications to aid them in this work. Industry itself is likely to be the largest source of technical expertise within many countries, and may be able to provide assistance in facility inspectorate training.
The competent authority shall have the right to suspend any operation which poses an imminent threat of a major accident.
Evaluation of major hazards
This should be carried out by specialists, if possible according to guidelines drawn up, for example, by the group of experts or by specialist inspectors, possibly with assistance from the major hazard installation employer management group. Evaluation involves a systematic study for major accident hazard potential. It will be a similar exercise, although in much less detail, to that carried out by the major hazard installation management in producing its safety report for the facility inspectorate and in establishing an onsite emergency plan.
Evaluation will include a study of all handling operations of hazardous materials, including transport.
An examination of the consequences of process instability or major changes in the process variables will be included.
The evaluation also should consider the positioning of one hazardous material in relation to another.
The consequences of common mode failure will also need to be assessed.
The evaluation will consider the consequences of the identified major accidents in relation to offsite populations; this may determine whether the process or plant can be put into operation.
Information to the public
Experience of major accidents, particularly those involving toxic gas releases, has shown the importance of the public nearby having prior warning of: (a) how to recognize that an emergency is occurring; (b) what action they should take; and (c) what remedial medical treatment would be appropriate for anyone being affected by the gas.
For inhabitants of conventional housing of solid construction, the advice in the event of an emergency usually is to go indoors, close all doors and windows, switch off all ventilation or air conditioning, and switch on the local radio for further instructions.
Where large numbers of shanty-dwellers live close to a major hazard installation, this advice would be inappropriate, and large-scale evacuation might be necessary.
Prerequisites for a major hazard control system
Personnel
A fully developed major hazard control system requires a wide variety of specialized personnel. Apart from industrial staff concerned either directly or indirectly with the safe operation of the major hazard installation, required resources include general factory inspectors, specialist inspectors, risk assessors, emergency planners, quality control officers, local authority land planners, police, medical facilities, river authorities and so on, plus legislators to promulgate new legislation and regulations for major hazard control.
In most countries, human resources for these tasks are likely to be limited, and the setting of realistic priorities is essential.
Equipment
A feature of establishing a major hazard control system is that much can be achieved with very little equipment. Factory inspectors will not need much in addition to their existing safety equipment. What will be required is the acquisition of technical experience and knowledge and the means to relay this from the group of experts to, say, the regional labour institute, the facility inspectorate and the industry. Additional training aids and facilities may be necessary.
Information
A key element in establishing a major hazard control system is obtaining state-of-the-art information and quickly passing this information on to all those who will need it for their safety work.
The volume of literature covering the various aspects of major hazards work is now considerable, and, used selectively, this could provide an important source of information to a group of experts.
Responsibility of exporting countries
When, in an exporting member country, the use of hazardous substances, technologies or processes is prohibited as a potential source of a major accident, the information on this prohibition and the reasons for it shall be made available by the exporting member country to any importing country.
Certain non-binding recommendations flowed from the Convention. In particular, one had a transnational focus. It recommends that a national or a multinational enterprise with more than one establishment or facility should provide safety measures relating to the prevention of major accidents and the control of developments likely to lead to a major accident, without discrimination, to the workers in all its establishments, regardless of the place or country in which they are situated. (The reader should also refer to the section “Transnational disasters” in this article.)
The European Directive on Major Accident Hazards of Certain Industrial Activities
Following serious incidents in the chemical industry in Europe in the last two decades, specific legislation covering major hazard activities was developed in various countries in Western Europe. A key feature in the legislation was the obligation of the employer of a major hazard industrial activity to submit information about the activity and its hazards based on the results of systematic safety studies. After the accident in Seveso (Italy) in 1976, the major hazard regulations in the various countries were put together and integrated in an EC Directive. This Directive, on the major accident hazards of certain industrial activities, has been in force since 1984 and is often referred to as the Seveso Directive (Council of the European Communities 1982, 1987).
For the purpose of identifying major hazard installations, the EC Directive uses criteria based on the toxic, flammable and explosive properties of the chemicals (see table 15).
Table 15. EC Directive criteria for major hazard installations
|
Toxic substances (very toxic and toxic): |
|||
|
Substances showing the following values of acute toxicity and having physical and chemical properties capable of entailing major accident hazards: |
|||
|
LD50 oral. rat mg/kg |
LD50 cut. rat/rab mg/kg |
LC50 ihl. 4hr. rat mg/1 |
|
|
1. |
LD50 <5 |
LD <1 |
LD50 <0.10 |
|
2. |
5<LD50 <25 |
10 <LD50 <50 |
0.1<LC50 <0.5 |
|
3. |
25 <LD50 <200 |
50 <LD50 <400 |
0.5 <LC50 <2 |
|
Flammable substances: |
|||
|
1. |
Flammable gases: substances which in the gaseous state at normal pressure and mixed with air become flammable and the boiling-point of which at normal pressure is 20 ºC or below. |
||
|
2. |
Highly flammable liquids: substances which have a flashpoint lower than 21 °C and the boiling point of which at normal pressure is above 20 °C. |
||
|
3. |
Flammable liquids: substances which have a flashpoint lower than 55 °C and which remain liquid under pressure, where particular processing conditions, such as high pressure and high temperature, may create major accident hazards. |
||
|
Explosive substances: |
|||
|
Substances which may explode under the effect of flame or which are more sensitive to shocks or friction than dinitrobenzene. |
|||
For the selection of specific major hazard industrial activities, a list of substances and threshold limits is provided in annexes to the Directive. An industrial activity is defined by the Directive as the aggregate of all installations within a distance of 500 metres of each other and belonging to the same factory or plant. When the quantity of the substances present exceeds the given threshold limit appearing in the list, the activity is referred to as a major hazard installation. The list of substances consists of 180 chemicals, whereas the threshold limits vary between 1 kg for extremely toxic substances to 50,000 tonnes for highly flammable liquids. For isolated storage of substances, a separate list of a few substances is given.
In addition to flammable gases, liquids and explosives, the list contains chemicals such as ammonia, chlorine, sulphur dioxide and acrylonitrile.
In order to facilitate the application of a major hazard control system and to encourage the authorities and management to apply it, it must be priority oriented, with attention being focused on the more hazardous installations. A suggested list of priorities is given in table 16.
Table 16. Priority chemicals used in identifying major hazard installations
|
Names of substances |
Quantity (>) |
EC list serial number |
|
General flammable substances: |
||
|
Flammable gases |
200 t |
124 |
|
Highly flammable liquids |
50,000 t |
125 |
|
Specific flammable substances: |
||
|
Hydrogen |
50 t |
24 |
|
Ethylene oxide |
50 t |
25 |
|
Specific explosives: |
||
|
Ammonium nitrate |
2,500 t |
146 b |
|
Nitroglycerine |
10 t |
132 |
|
Trinitrotoluene |
50 t |
145 |
|
Specific toxic substances: |
||
|
Acrylonitrile |
200 t |
18 |
|
Ammonia |
500 t |
22 |
|
Chlorine |
25 t |
16 |
|
Sulphur dioxide |
250 t |
148 |
|
Hydrogen sulphide |
50 t |
17 |
|
Hydrogen cyanide |
20 t |
19 |
|
Carbon disulphide |
200 t |
20 |
|
Hydrogen fluoride |
50 t |
94 |
|
Hydrogen chloride |
250 t |
149 |
|
Sulphur trioxide |
75 t |
180 |
|
Specific very toxic substances: |
||
|
Methyl isocyanate |
150 kg |
36 |
|
Phosgene |
750 kg |
15 |
With the chemicals shown in the table acting as a guide, a list of installations can be identified. If the list is still too big to be coped with by the authorities, new priorities can be set by means of setting new quantity thresholds. Priority setting also can be used inside the factory to identify the more hazardous parts. In view of the diversity and complexity of industry in general, it is not possible to restrict major hazard installations to certain sectors of industrial activity. Experience, however, indicates that major hazard installations are most commonly associated with the following activities:
- petrochemical works and refineries
- chemical works and chemical production plants
- LPG storage and terminals
- stores and distribution centres for chemicals
- large fertilizer stores
- explosives factories
- works in which chlorine is used in bulk quantities.
Country Case Study: Sweden
Objectives
The Swedish official system for compensating workers with occupational injuries is regulated by law—the official act on occupational injury insurance (Official Act on Occupational Injury Insurance 1993). The system is organized to function as an integral part of the framework of Swedish national social security, receiving monetary contributions from levies on employers and a basic funding through government revenue sources.
The objective of occupational injury compensation, according to the law, is to compensate for loss of income and for assessed loss of earning capacity. In addition, a large part of the labour market has a supplementary system, based on collective agreements between the social partners on the labour market (employers organizations in the public and private sectors and corresponding trade unions) for compensation to the insured population for pain and suffering, disability and handicap and other types of incapacity. This collective insurance programme is referred to as the Labour Market No-Fault Liability Insurance (TFA). It operates on a no-fault basis, meaning that, for recognition of a claim, there is no requirement on the claimant to prove negligence on the part of the employer or anyone else involved in the claim at issue. This supplementary insurance system is not required or regulated by law, and is operated jointly on a partnership basis by the employers’ organizations and the trade unions.
The following discussion will focus on the official legislated system in Sweden.
Organization
The official system operates on the basis of notifications submitted by those insured when the injury occurs. The insured population consists of everyone employed on the labour market at the point in time when the disease or health problem manifests itself. The notification—which in practice means that the injured person fills out a form—is handed to the employer, who is obliged to forward it to a local or regional social insurance bureau. After due examination of the documentation and evidence appended to the notification, a decision is taken by a regional Social Insurance Board, approving or rejecting the claim.
If the claimant or somebody else involved is not satisfied with the decision taken by the Social Insurance Board, the case may be referred to an administrative court of appeal. This court is part of the Swedish judiciary.
The Swedish system in force as of 1 January 1993 is designed to operate on the basis of three fundamental principles:
- the concept of occupational injury
- the concept of hazardous agent at work
- the concept of causality of hazardous agent with regard to the disease at issue.
Occupational Injury
The occupational injury concept has two main components, namely occupational accidents and occupational diseases. The operative part of the concept lies in the term injury. This may be caused by either an accident at work or a hazardous factor causing a disease and operating at the present workplace or in some previously held work. The injury concept thus encompasses both consequences of bodily harm caused by accidents and diseases or impairments viewed as caused by other agents, such as physical, chemical, psychological or other types of environmental factors operating at work. The disease concept as implemented has a broad scope. It covers both diseases, as classified by, for instance, the WHO classification of diseases, and, in addition, functional disturbances, ailments or impairments perceived by the individual as health aberrations. This means that there is no officially defined list of occupational diseases or work-related diseases in Sweden. Any disease or impairment, as referred to above, may be regarded and recognized as occupationally induced, depending on the evidence presented to support a claim for economic compensation. This means that, in addition to a disease or health problem directly caused by work or workplace factors, the following factors may be included in the concept of occupational injury:
- early manifestation of disease that is work-related but which also occurs in the general population without any association to working conditions
- disease or functional disturbances causally unrelated to working conditions but where workplace factors may contribute to accelerating or worsening the disease.
This broad occupational injury concept has been applied since 1977, and it was not changed in the amended law in force since 1 January 1993. This means that there is no closed list of occupational diseases. Nor is any distinction made between diseases that are occupationally caused and those that are work-related. Recognition of a disease or functional disturbance reported by an injured person (who is covered by the social security system) as an occupational injury depends on the evidence presented by the claimant.
The use of this broad concept aims at making the system capable of identifying any health problem that may have been contributed to or caused by conditions at work.
The Hazardous Agent at the Workplace
The recognition of an occupational injury is dependent on identifying a hazardous agent at the workplace. If such an agent cannot be identified and assessed to be sufficiently relevant to the type of injury at issue, the disease or functional impairment cannot be approved as a case of occupational injury.
Hazardous agent implies any physical, chemical or other agent which may adversely affect the health status of the employees. There are some limitations with regard to scope. The law does not consider to be hazardous agents factors related to closing down enterprises, industrial disputes, lack of social support, or non-adaptation to prevailing workplace culture and other similar conditions.
The requirements in the law in force as of 1 January 1993 have been defined as: “A hazardous agent is a factor which in high probability may cause disease or impairment.”
This phrasing represents—in comparison with the law in force until 31 December 1992— an enhanced level of requirement on the evidence to be considered by the social insurance boards. It is also made explicit in the explanatory texts attached to the legislation that the assessments of hazardous properties of the agent under consideration should conform to a mainstream of opinion—or ideally a consensus—among qualified medical experts. If there are diverse and dissenting expert opinions on the assessment of hazardous properties the criterion of high probability will not be satisfied.
The assessment of the hazardous agent also implies an assessment of quantity. The exposure to the agent at issue is to be considered with regard to duration, intensity and other criteria judged to determine hazardous properties.
Causal Relationship
Once the existence or previous occurrence of a hazardous agent has been established as highly probable—which in this context also includes an assessment of quantity—the next step is to arrive at a conclusive judgement on the plausibility of a causal relationship in the individual case at issue. The general rule to follow is that the weight of evidence should be in favour of causality for recognition of the disease or health problem as an occupational injury. According to the earlier legislation, in force until 31 December 1992, the causality concept was significantly more flexible. Causality was presumed once the presence of a hazardous agent had been accepted as a probability and no evidence to the contrary could be presented. The burden of evidence has now been reversed. The requirement is now a positive weight of evidence in favour of a causal relationship. In practice it means that a need arises to also consider alternative causal explanations. This may include, for instance, aspects of the claimant’s lifestyle and leisure time activities or personal situation in general.
Assessment of Individual Vulnerability
The basic principle in implementing the legislation is that all insured are to be accepted, with their constitutional weaknesses and vulnerabilities. This principle may give rise to considerable difficulties, for instance in assessing health problems related to hypersensitivity reactions and allergic diseases. It may be very difficult to make informed judgements of the relative contributions from the person’s constitution and environmental/occupational factors, respectively. The difficulty in such instances arises in defining and assessing the properties of the hazardous agent. The agent (for instance, exposure to a workplace chemical or an air pollutant) may be harmless to most exposed persons but not to those who are particularly susceptible.
Occupational Injury Compensation and Preventive Action
The Swedish legal system for paying compensation to injured persons and the legal systems for enforcing occupational health preventive measures are separate and not directly related. The rate of workplace accidents or occupational injuries does not affect the level of financial contributions by employers or enterprises. This is sometimes referred to as a flat rate of payment.
The compensation system functions only for payments to persons with recognized occupational injury and has no bearing on enforcement of preventive action.
The same rules applies for occupational rehabilitation, regardless of whether the disease or injury has been recognized as an occupational injury or not. The employer has an obligation in principle to take steps to initiate a rehabilitation process when workers have been absent from work for 4 weeks or more.
The Role of Social Partners
The social insurance legislation accords the social partners (i.e., employers’ organizations and the trade unions) no role in rejecting or approving compensation claims for occupational injury. On the company level the employer is obliged by law to pass on to the social insurance system any claim for occupational injury submitted by an employee. The trade union organizations commonly provide advice and support to claimants among their members. Such assistance includes drafting claims, examining workplace conditions and giving advice.
The Present Situation
Since the present legislation has been officially in force, the supervising authorities have to a large extent been busy dealing with the considerable accumulation of injuries reported under the previous legislation. This means that there is only limited experience from the present law and the official public statistics are incomplete.
At the present time there is a need to elaborate practical guidelines for implementing the legislation. The Swedish Labour Market Insurance (TFA) trust—jointly with the National Institute for Working Life—recently published a report describing the extent of knowledge regarding disease and occupational factors for selected disease categories. At the present time such descriptions are available for tumour disease, diseases of the nervous system, diseases of the lung and pleura, malignant disease, cardiovascular disease, skin disease and work-related loss of hearing (National Institute for Working Life and Labour Market No-Fault Liability Insurance Trust 1995). A further volume on psychological disturbances and stress-related mental disorders is in preparation.
Before the change of the law on compensation for occupational injury, the level of occupational diseases in the early 1990s was around 50,000 to 55,000 claims recognized annually. The number of reported and recognized occupational accidents during this time was 20,000 to 22,000. Musculoskeletal disorders constituted a major part (80%) of the reported occupational diseases.
One important factor affecting levels of reported occupational injuries is the automatic coordination of payments received from the occupational injury system and the general sickness benefit system, respectively. In 1993 the coordination time was increased from 90 days to 180 days. This implies that an injury or disease, although causally related to work, is not compensated unless it leads to long-term absence from work (more than 180 days) or to permanent disability. The compensation during the first 180-day period is covered by the general sickness benefit scheme.
It is expected that the number of reported occupational injuries and, consequently, of recognized cases will decline significantly, starting in the near future. The official statistic routines have not yet been adapted to the changes in legislation. This means that the number of notifications and recognized occupational injuries recorded at the present time consist of a combination of claims under the previous legislation and claims that are settled on the basis of the legislation in force as of 1 January 1993. As a consequence, the official statistics cannot at the present time describe the impact of the amendments in the legislation referred to above.
Workers' Accident Compensation in Japan
Summary of Coverage and Goal
Coverage
Hazards covered
The workers’ accident compensation insurance system in Japan is under the control of the government, based on the Workmen’s Accident Compensation Law (1947). It gives workers insurance benefits in order to protect them promptly and fairly against injuries, diseases, disabilities or deaths incurred “because of duty”. The definition of “because of duty” is not stipulated by the provisions in related laws. The criteria used by the government administration make it clear, however, that the system is applied to injuries, disabilities or deaths that result from employment, namely “during the duty situation in which workers are under the control of an employer according to work contracts” and “due to an accident or a circumstance caused by this duty situation”. Thus the system is applied to all the injuries, disabilities and deaths incurred while workers are working or commuting to work. It is also applied to “diseases or disorders to workers engaged in work with hazards that can harm health from sudden or chronic action of such hazards”. These because-of-duty diseases include those caused by injury resulting from employment and occupational diseases caused by physical, chemical and biological agents or specific forms of work performance, and those apparently caused by work.
Industries and workers covered
The workmen’s accident compensation insurance system is applied compulsorily to all workers who are employed in enterprises to which the Labour Standards Law is applied and receive wages. They include those regularly or temporarily employed, daily-wage workers, and both full-time and part-time workers, irrespective of the size of enterprises.
All industries are covered by the system, except part of the agriculture, forestry and fishery industries. The exceptions are agricultural undertakings individually owned and employing less than five workers, forestry undertakings not employing regular workers, and fishery undertakings employing less than five workers and operating in sea areas without significant accident. Government employees, local government employees and sailors are covered by separate workmen’s compensation systems.
Types of payment
The following types of insurance benefits are available for on-the-job injuries and diseases:
- medical benefit: in principle, medical treatment (in exceptional cases cash reimbursement for treatment expenses)
- temporary disability benefit: when unable to work and earn wages because of treatment
- injury and disease compensation pension: when not recovered one-and-a-half years after starting to receive treatment and the extent of disabilities remains at a certain level
- physical handicaps compensation benefit: according to the degree of physical handicap the workers are left with
- bereaved family compensation benefit: to the spouse, children, parents, grandchildren, grandparents or brothers and sisters who had been supported by the income of the workers concerned
- expenses for funeral rites
- nursing compensation benefit: for full-time or occasional nursing in the case of a grade 1 or grade 2 physical handicaps compensation pension or an injury and disease compensation pension.
For injury, disease, disability or death incurred during commuting, the following benefits are paid: (a) medical benefit; (b) temporary disability benefit; (c) injury and disease pension; (d) physical handicaps benefit; (e) bereaved family benefit; (f) funeral rites benefit; and (g) nursing benefit. The details of these benefits are the same as in the case of on-the-job accidents or occupational diseases.
The income benefits are calculated on the basis of the average daily wage of the workers concerned. The temporary disability benefit amounts to 60 of the average daily wage and is given starting from the fourth day of absence from work, together with the temporary disability special supplement equivalent to 20% of the average daily wage (the employer must pay compensation equivalent to 60% of the average wage for the first three days). The amount of injury and disease compensation pension, given when workers do not recover within one-and-a-half years, ranges from 245 to 313 days of the average daily wage. The physical handicaps benefit ranges from 131 to 313 days of the average daily wage. The amount of the bereaved family compensation lump sum ranges from 153 to 245 days of the average daily wage.
The temporary disability benefit, the pension and the lump sum benefit are subject to the sliding scale system which reflects the movement of wages. In cases where the average pay of all the workers for a quarter of the year surpasses 110% or falls short of 90% of the average pay for the quarter to which the day belongs when the worker concerned was injured or taken ill, the average daily wage used for the calculation of temporary disability benefit is automatically revised according to the fluctuating average pay rate. Similar calculations are done for pension and lump sum benefits when the average pay of all the workers for a year surpasses or falls short of the average pay for the year in which the worker concerned died or became ill.
Other aspects
Welfare services
The purpose of the Workmen’s Accident Compensation Insurance is to advance the welfare of workers by promoting return to work or social life of the victims, to give support to them and their bereaved families and to secure proper working conditions. Therefore the system has separate provisions for various welfare services and some preventive measures. Some of these services are managed by the Labour Welfare Services Association, to which the insurance system supplies the funds. Welfare services include the establishment and management of employment injury hospitals, spinal cord impediment centres, rehabilitation workshops, housing loans, relief funds for education and long-term family nursing, installation and operation of special care facilities for workers suffering from employment injuries, home help services and nursing device leasing.
Extension of coverage
Employers of small and medium-sized enterprises and self-employed persons to whom it is appropriate to give the same protection as workers considering the nature of their business may be covered by the workers’ compensation insurance. Entry into the insurance system is allowed to employers of small and medium-sized enterprises which entrust insurance procedures to a labour insurance business association, as well as to the self-employed who join an organization capable of executing insurance procedures.
Workers who are dispatched overseas by employers in Japan or dispatched as representatives for overseas small and medium-sized enterprises are covered.
Description of the System
History
The need for compensating workers for on-the-job injury was first noted by the Factory Law (1911) and the Mine Law (1905). These laws stipulated that employers were responsible for providing sufferers of industrial injuries with assistance. The Health Insurance Law (1922) covered short-term injuries incurred on or outside the job by workers engaged in enterprises to which these laws were applicable. The coverage was later extended to long-term injuries and to civil engineering, construction and transportation workers. A new stage began when the two principal laws described below were enacted in 1947, following the termination of the Second World War. The Labour Standards Law introduced for the first time the idea of employers’ liability and compensation in place of “assistance” in the case of employment injury. The Workmen’s Accident Compensation Insurance Law set up insurance within the jurisdiction of the newly established Ministry of Labour. The insurance system has been improved by repeated revisions of the law. It operates as a system independent from the social security programmes of the country.
Types of insurance coverage
Workmen’s Accident Compensation Insurance is a state insurance system administered by the government. The scope of the insurance extends to all on-the-job accidents and diseases and commuting accidents. It covers both medical and cash income benefits. The medical and rehabilitation costs for workers suffering from injuries or diseases covered by this system are paid by the insurance, a separate treatment not covered by health insurance schemes.
Employers covered by Workmen’s Accident Compensation Insurance are no longer liable for compensation stipulated by the Labour Standards Law for cases compensated by this insurance. However, there are collective agreements that provide for supplementary compensation beyond the levels provided by the state insurance. Furthermore, there are a number of private enterprises that join the compensation insurance schemes managed by private insurance companies.
Disputes about the amount of supplementary compensation for victims of occupational injuries and disease and their families are often brought before the court.
All types of employment and commuting injuries are covered. As for diseases, there is a list of occupational diseases attached to Article 35 of the Enforcement Ordinance of the Labour Standards Law (revised in 1978). The list is comprehensive and covers in effect all types of work-related diseases. The following nine categories are mentioned:
- diseases caused by injury resulting from employment
- diseases caused by physical agents (13 items)
- diseases caused by specific forms of work performance in which an extreme physiological tension is involved (5 items)
- diseases caused by chemical substances and others (8 items)
- pneumoconiosis caused by work in places where dust is dispersed, and diseases complicated by pneumoconiosis stipulated by the Enforcement Ordinance of the Pneumoconiosis Law (1960)
- diseases caused by bacteria, viruses and other pathogenic organisms (5 items)
- diseases caused by carcinogenic substances or agents, or work performed in a carcinogenic manufacturing process (18 items)
- other diseases designated by the Minister of Labour
- other diseases apparently caused by work.
Role of social partners
Development of compensation principles
Workmen’s Accident Compensation Insurance started as an insurance system financed wholly by employers. Partial payment by the government began in 1960, when long-term injury and disease compensation was adopted and lump sum payment was replaced with annuity payment for the physically handicapped. In 1965, government subsidies were introduced for the expenses of administering the workers’ compensation insurance and for insurance payments. This was accomplished by serial amendments of the Workmen’s Accident Compensation Law, which in the beginning was applicable only to enterprises regularly employing five or more workers, except part of the agriculture, forestry and fishery industries. Any such enterprise is obliged to automatically join the insurance system as soon as its business starts. Administration of the insurance system is supervised by the Bureau of Labour Standards of the Ministry of Labour. Penalties are applied in the case of violations. Thus the roles of employers and workers are basically what they were at the beginning of the system.
The benefits received by the injured workers and the bereaved families have been improved by several modifications of the law. These modifications improved long-term benefits and bereaved family compensation pensions, introduced the sliding scale of payments as determined by wage level changes, extended benefits to all commuting accidents, and established the special supplement system and the labour welfare services in 1976. In 1981, the adjustment rules between the workers’ compensation insurance benefit and the civil damage compensation were established. Nursing compensation benefits are being introduced.
Deciding whether an injury or disease is because of work duty is based on administrative interpretations. Those who are not satisfied with the decisions may demand an examination or arbitration by a Workmen’s Accident Compensation Insurance examiner appointed by the Minister of Labour. If they are not satisfied with the examiner’s decision, they may demand a re-examination of their case by the Labour Insurance Council. Those who are dissatisfied with the council’s decision can file a suit in court.
Mechanism for updating
The terms of operation of the insurance system are approved by the Council of Workmen’s Accident Compensation Insurance, in which employers, workers and academia are represented. The development of the system and modifications of insurance benefits are examined by the council. As a result, the Workmen’s Accident Compensation Insurance Law was revised several times as mentioned above.
Decisions of the appeal and the civil court systems concerning compensation cases contribute to updating of benefit levels and criteria.
Finances
The government collects the insurance premium from employers. The premium is calculated by multiplying the total wages payable to all the workers in the enterprise in the insurance year by the premium rate. This premium rate is determined for each category of enterprise, taking into account the past accident rates and other factors. A merit system is applied in determining the premium rate for different industries. The premium rates as of April 1992 for different industries are given in table 1.
Table 1. Premium rates of workmen’s accident compensation insurance in Japan (April 1992)
|
Industry |
Types of undertaking |
Premium rate |
|
Forestry |
Felling and transport of wood |
0.142 |
|
Others |
0.041 |
|
|
Fishery |
Sea fishery (except below) |
0.067 |
|
Fishery by stationary nets or by culture |
0.042 |
|
|
Mining |
Coal mining |
0.111 |
|
Metal and non-metal mining |
0.099 |
|
|
Others other than below |
0.040-0.072 |
|
|
Petroleum or natural gas mining |
0.010 |
|
|
Construction |
New construction or power plants and tunnels |
0.149 |
|
New construction of railroads |
0.068 |
|
|
New construction of roads |
0.049 |
|
|
Others |
0.025-0.038 |
|
|
Manufacturing |
Ceramics |
0.020-0.027 |
|
Wood products |
0.026 |
|
|
Ship building and repair |
0.023 |
|
|
Metal products |
0.022 |
|
|
Foundry |
0.021 |
|
|
Others |
0.006-0.018 |
|
|
Transport |
Ship loading/unloading |
0.053 |
|
Other kinds of cargo handling in ports |
0.029 |
|
|
Freight handling other than above |
0.019 |
|
|
Traffic and transportation |
0.007 |
|
|
Supply of electicity, gas, water or heat |
0.006 |
|
|
Others |
Cleaning,, cremation or meat-processing |
0.014 |
|
Others |
0.006-0.012 |
Special exceptional measures to increase or decrease the premium rate determined throughout the merit system are to be applicable starting in 1997 to small and medium-sized enterprises that have taken special measures to secure the safety and health of workers.
The injured workers or bereaved families are expected to provide the information necessary for demanding the insurance payment. The workers who receive the medical benefit for commuting injuries must have contributed to the expenses up to the limit of two hundred yen for the first medical treatment.
Prevention
Some preventive measures are undertaken as part of the labour welfare services within the Workmen’s Accident Compensation Insurance. These include:
- establishing and managing occupational health centres; and
- supporting industrial safety and health associations.
As a result, a variety of preventive activities are supported by means of the insurance funds.
Summary of Cost Experience
The changes in the numbers of enterprises and workers covered by the workers’ compensation system and the total annual amount of insurance payments are indicated in table 2. It should be noted that sliding scales of pension rates were first applied in 1983 and that the lowest and highest limits of average daily wage of temporary disability benefit for those who need prolonged care were established in 1990. The table shows that the number of workers covered by the insurance system has been steadily increasing, but that the number of cases receiving insurance payments has decreased since 1988.
Table 2. Enterprises and workers where the workmen’s accident compensation insurance was applicable and amount of benefits in Japan
|
Fiscal year (April-March) |
Number of applicable |
Number of applicable workers (thousand) |
Amount of insurance benefits |
Number of |
|
1960 |
808 |
16,186 |
27,172 |
874 |
|
1965 |
856 |
20,141 |
58,372 |
1,341 |
|
1970 |
1,202 |
26,530 |
122,019 |
1,650 |
|
1975 |
1,535 |
29,075 |
287,640 |
1,099 |
|
1980 |
1,840 |
31,840 |
567,288 |
1,099 |
|
1985 |
2,067 |
36,215 |
705,936 |
902 |
|
1986 |
2,110 |
36,697 |
724,260 |
859 |
|
1987 |
2,177 |
38,800 |
725,922 |
847 |
|
1988 |
2,270 |
39,725 |
733,380 |
832 |
|
1989 |
2,342 |
41,249 |
741,378 |
818 |
|
1990 |
2,421 |
43,222 |
753,128 |
798 |
|
1991 |
2,492 |
44,469 |
770,682 |
765 |
|
1992 |
2,542 |
45,832 |
791,626 |
726 |
|
1993 |
2,577 |
46,633 |
799,975 |
696 |
|
1994 |
2,604 |
47,008 |
806,932 |
675 |
In 1994, 25% of the total insurance benefits were for medical benefits, 14% for temporary disability benefits, 6% for physical handicaps compensation lump sum, 39% for pension and 14% for special grants. The distribution of the insurance benefits by industry is given in table 3.
Table 3. Payment of insurance benefits by industry in Japan
|
Industry |
Applicable plants1 |
Applicable workers1 |
Amount of insurance benefits2 |
|||
|
Number |
(%) |
Number |
(%) |
(Thousand yen) |
(%) |
|
|
Forestry |
26,960 |
(1.0) |
126,166 |
(0.3) |
33,422,545 |
(4.2) |
|
Fishery |
6,261 |
(0.3) |
56,459 |
(0.1) |
3,547,307 |
(0.4) |
|
Mining |
6,061 |
(0.2) |
55,026 |
(0.1) |
58,847,081 |
(7.3) |
|
Construction |
666,500 |
(25.6) |
5,886,845 |
(12.5) |
268,977,320 |
(33.6) |
|
Manufacturing |
544,275 |
(20.9) |
11,620,223 |
(24.7) |
217,642,629 |
(27.2) |
|
Transportation |
70,334 |
(2.7) |
2,350,323 |
(5.0) |
64,536,818 |
(8.1) |
|
Supply of electricity, gas, water or heat |
1,962 |
(0.1) |
188,255 |
(0.4) |
1,344,440 |
(0.2) |
|
Others |
1,281,741 |
(49.2) |
26,724,978 |
(56.9) |
151,657,177 |
(19.0) |
|
Total |
2,604,094 |
(100%) |
47,008,275 |
(100%) |
799,975,317 |
(100%) |
1 As of end of the 1994 fiscal year.
2 As of end of the 1993 fiscal year.
Fall Protection for Transport Category Aircraft Manufacture and Maintenance
Transport category aircraft are used for transporting passengers and freight in the commercial airline/airfreight industry. Both the manufacturing and maintenance process involve operations that remove, fabricate, alter and/or install components all over the aircraft itself. These aircraft vary in size but some (e.g., Boeing 747, Airbus A340) are among the largest aircraft in the world. Due to the size of the aircraft, certain operations require personnel to work while elevated above the floor or ground surface.
There are many potential fall situations within both aircraft manufacturing and maintenance operations throughout the air transport industry. While each situation is unique and may require a different solution for protection, the preferred method of fall protection is by preventing falls through an aggressive plan for hazard identification and control.
Effective fall protection involves an institutional commitment addressing every aspect of hazard identification and control. Each operator must continually evaluate its operation for specific fall exposures and develop a protection plan comprehensive enough to address each exposure throughout their operation.
Fall Hazards
Any time an individual is elevated they have the potential to fall to a lower level. Falls from elevations often result in serious injuries or fatalities. For this reason, regulations, standards and policies have been developed to assist companies in addressing the fall hazards throughout their operations.
A fall hazard exposure consists of any situation in which an individual is working from an elevated surface where that surface is several feet above the next level down. Assessing the operation for these exposures involves identifying all areas or tasks where it is possible that individuals are exposed to elevated work surfaces. A good source of information is injury and illness records (labour statistics, insurance logs, safety records, medical records and so on); however, it is important to look further than historical events. Each work area or process must be evaluated to determine whether there are any instances where the process or task requires the individual to work from a surface or area that is elevated several feet above the next lower surface.
Fall Situation Categorization
Virtually any manufacturing or maintenance task performed on one of these aircraft has the potential to expose personnel to fall hazards because of the size of the aircraft. These aircraft are so large that virtually every area of the entire aircraft is several feet above ground level. Although this provides many specific situations where personnel could be exposed to fall hazards, all the situations may be categorized as either work from platforms or work from aircraft surfaces. The division between these two categories originates with the factors involved in addressing the exposures themselves.
The work-from-platforms category involves personnel using a platform or stand to access the aircraft. It includes any work performed from a non-aircraft surface that is specifically used to access the aircraft. Tasks performed from aircraft docking systems, wing platforms, engine stands, lift trucks and so on would all be in this category. Potential fall exposures from surfaces in this category may be addressed with traditional fall-protection systems or a variety of guidelines that are currently in existence.
The work from aircraft surfaces category involves personnel using the aircraft surface itself as the platform for access. It includes any work performed from an actual aircraft surface such as wings, horizontal stabilizers, fuselages, engines and engine pylons. Potential fall exposures from surfaces in this category are very diverse depending on the specific maintenance task and sometimes require non-conventional approaches for protection.
The reason for the distinction between these two categories becomes clear when attempting to implement protective measures. Protective measures are those steps that are taken to eliminate or control each fall exposure. The methods for controlling fall hazards may be engineering controls, personal protective equipment (PPE) or procedural controls.
Engineering Controls
Engineering controls are those measures which consist of altering the facility in such a way that the individual’s exposure is minimized. Some examples of engineering controls are railings, walls or similar area reconstruction. Engineering controls are the preferred method for protecting personnel from fall exposures.
Engineering controls are the most common measure employed for platforms in both manufacturing and maintenance. They usually consist of standard railings; however, any barrier on all open sides of a platform effectively protects personnel from the fall exposure. If the platform were positioned right next to the aircraft, as is common, the side next to the aircraft would not need rails, as protection is provided by the aircraft itself. The exposures to be managed are then limited to gaps between the platform and the aircraft.
Engineering controls are usually not found in maintenance from aircraft surfaces, because any engineering controls designed into the aircraft add weight and decrease the aircraft’s efficiency during flight. The controls themselves prove inefficient when designed to protect the perimeter of an aircraft surface, as they have to be specific to the aircraft type, area and location and must be positioned without causing damage to the aircraft.
Figure 1 shows a portable rail system for an aircraft wing. Engineering controls are used extensively during manufacturing processes from aircraft surfaces. They are effective during manufacturing because the processes occur in the same location with the aircraft surface in the same position every time, so the controls may be customized to that location and position.
An alternative to railings for engineering controls involves netting positioned around the platform or aircraft surface to catch individuals when they fall. These are effective in stopping someone’s fall but are not preferred, as individuals may be injured during the impact with the net itself. These systems also require a formal procedure for rescue/retrieval of personnel once they have fallen into the nets.
Figure 1. Boeing 747 portable rail system; a two-sided guardrail system attaches to side of aircraft body, providing fallprotection during work on over-wing door and wing roof area.
Courtesy of The Boeing Company
Personal Protective Equipment
PPE for falls consists of a full body harness with a lanyard attached to either a lifeline or other suitable anchorage. These systems are typically used for fall arrest; however, they may also be used in a fall restraint system.
Used in a personal fall arrest system (PFAS), PPE may be an effective means for preventing an individual from impacting the next lower level during a fall. To be effective, the anticipated fall distance must not exceed the distance to the lower level. It is important to note that with such a system the individual may still experience injuries as a result of the fall arrest itself. These systems also require a formal procedure for rescue/retrieval of personnel once they have fallen and been arrested.
PFASs are used with work from platforms most often when engineering controls are not functional—usually due to restriction of the work process. They are also used with work from aircraft surfaces because of the logistical difficulties associated with engineering controls. The most challenging aspects of PFASs and aircraft surface work are the fall distance with respect to personnel mobility and the added weight to the aircraft structure to support the system. The weight issue may be eliminated by designing the system to attach to the facility around the aircraft surface, rather than the aircraft structure; however, this also limits fall protection capability to that one facility location. Figure 2 shows a portable gantry used for providing a PFAS. PFASs are used more extensively in maintenance operations than manufacturing, but are used during certain manufacturing situations.
Figure 2. Engine gantry providing fall protection for aircraft engine worker.

Courtesy of The Boeing Company
A fall restraint system (FRS) is a system designed so that the individual is prevented from falling over the edge. FRSs are very similar to PFASs in that all the components are the same; however, the FRSs restrict the individual’s range of movement such that the individual cannot reach close enough to the edge of the surface to fall over. FRSs are the preferred evolution of PPE systems for both manufacturing and maintenance operations, because they prevent any fall-related injury and they eliminate the need for a rescue process. They are not extensively used in either work from platforms or aircraft surfaces, because of the challenges of designing the system so that personnel have the mobility needed to perform the work process, but are restricted from reaching the edge of the surface. These systems decrease the weight/efficiency issue with work from aircraft surfaces, because FRSs do not require the strength that a PFAS requires. At the time of printing, only one aircraft type (the Boeing 747) had an airframe-based FRS available. See figure 3 and figure 4.
Figure 3. Boeing 747 wing lanyard system.

Courtesy of The Boeing Company
Figure 4. Boeing 747 wing lanyard system fall protection zones.
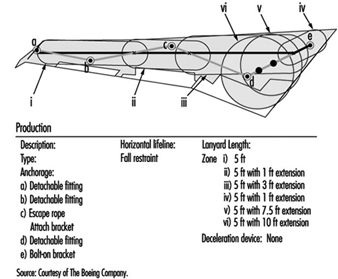
Courtesy of The Boeing Company
A horizontal lifeline attaches to permanent fittings on the wing surface, creating six fall protection zones. Employees connect a 1.5 m lanyard to D-rings or strap extensions that slide along the horizontal lifeline in zones i through iv, and are fixed in zones v and vi. The system allows access only to the edge of the wing, preventing the possibility of falling from the wing surface.
Procedural Controls
Procedural controls are used when both engineering controls and PPE are either ineffective or impractical. This is the least preferred method of protection, but is effective if managed properly. Procedural controls consist of designating the work surface as a restricted area for only those individuals that are required to enter during that specific maintenance process. Fall protection is achieved through very aggressive written procedures covering hazard exposure identification, communication and individual actions. These procedures mitigate the exposure as best as possible under the circumstances of the situation. They must be site specific and must address the specific hazards of that situation. These are very seldom used for work from platforms in either manufacturing or maintenance, but they are used for maintenance work from aircraft surfaces.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."