- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Healthcare Workers and Infectious Diseases
Codes and Guidelines
Range of Purposes Behind Codes
Codes of ethics in the professions serve numerous purposes. At the level of the profession itself, codes document the standards according to which the profession can be held accountable for the conduct of its members. Further, because society relegates control for many of the professions to the professional organizations themselves, the professions have developed codes to provide the basis of self-regulation (Soskolne 1989). At the level of the individual professional, codes can provide a practical guide to members of the profession who might be experiencing a moral or ethical dilemma concerning their professional conduct in a particular circumstance. Where a professional finds himself or herself in a state of moral or ethical tension, it is self-evident that codes can be helpful in providing counsel.
The existence of a code provides the basis of a profession’s ethics programme of activity designed to instil ethical standards among its membership (Gellermann, Frankel and Ladenson 1990; Hall 1993). Revisions to the code can be considered through grass-roots individual membership input at organizational meetings, workshops and conferences. This ongoing discussion of issues and concerns constitutes a review process ensuring that any code remains sensitive to changing social values. Professions depending for their sustenance on public support thereby improve their likelihood of remaining publicly accountable and relevant (Glick and Shamoo 1993).
Codes could assist professionals being charged with malpractice and perhaps even in litigation. Demonstrated adherence to one’s professional code would likely be deemed indicative of adherence to standards of practice consistent with professional norms. If such practice were to have resulted in harm, the code-abiding individual professional would be less likely to be found guilty of having committed a wrong. However, based on the principle of trust (Pellegrino, Veatch and Langan 1991), the public has the expectation that the best possible professional judgement will be exercised in the public interest. Where the physician-patient relationship is concerned, the patient has the right under the principle of trust to expect that his or her interests will be best served. However, an ethical tension arises when the public good is potentially harmed in circumstances where the individual patient’s best interests are being served. In such circumstances, it is the public good that will usually need to take precedence over that of the individual. Regardless, codes provide no substitute for legal liability dimensions of conduct for which government has enacted laws to protect the public interest (Cohen 1982).
Weight and Intent of Codes
Codes do have associated with them the notion of statutory force, implying the ability for their enforcement through the administering of some type of disciplinary action. Indeed, the notions of accountability and self-regulation referred to above have associated with them some sense of control (minimally, peer pressure; maximally, the removal of licence to practice) that can be exercised over the members of the profession by the professional organization itself. Because of this, some professional organizations have preferred to avoid these connotations associated with codes and opt rather for “guidelines”. The latter emphasize guidance with fewer implications for enforcement associated with them. Other groups have preferred to avoid all connotations associated with codes or guidelines; instead, they have preferred to develop “declarations on ethics” for their specific organizations (Jowell 1986). Throughout this chapter the term code will imply “guidelines”.
It should be apparent that codes (and also guidelines) do not carry the force of law. In essence, codes and guidelines are intended to provide guidance for professionals, collectively and individually, in their relationships with their clients (including patients and research subjects), with their colleagues and co-workers (including their students), and with the public (including stakeholder groups). In addition, codes require that the quality of professional work and hence the stature of the profession itself is advanced. In general, codes associated with the physician-patient relationship will require that the patient’s interests take precedence over any other interests; the physician is placed firmly in the position of “patient advocate”. One exception to this would arise in the context of infectious diseases, where the patient’s rights may have to be considered second to the public welfare. In contrast, however, it can generally be stated that codes associated with scientific research will require that the public interest take precedence over any individual or other interests. One exception would be where a researcher discovers child abuse in a research subject; here the researcher would have the obligation to report this to the child welfare authorities.
Code Development, Review and Revision
The process by which codes are developed has consequences for their application. By including members of the profession and students of the profession in code development, as well as in code review and revision, ownership of the resultant document by a greater number of individuals is believed more likely. With broad-based ownership, increased compliance by a greater number is believed more assured.
Content and Structure of Codes
The content of a code should be user friendly to maximize its utility. Codes can be of varying length. Some are brief, while some are substantial. The more substantial that a code is, the more specific it is possible for it to be. Codes can be made to be user friendly by virtue of their structure and content. For example, a summary set of the principles upon which the code is based could be presented first, followed by expanded aspirational or prescriptive statements, which constitute the code itself. These can be followed by a commentary that explicates each statement in turn, perhaps noting special circumstances in the form of case studies that might serve as useful examples. The principles and their interpretation(s), however, are highly dependent on the values recognized as inherent to the pursuits of a profession. While these values may be universal, interpretations as well as practices at the local and regional levels may differ. Thus, while a statement of the profession’s core values can provide an anchor for its statements on ethics and should appear as a preface to the guidelines (Gellermann, Frankel and Ladenson 1990), sensitivity to regional differences can be demonstrated through the more detailed commentary and case study materials.
The commentary should incorporate, or could be followed by or complemented with, case study materials that derive from real-life instances of ethical dilemmas or tensions. The case study materials could be ethically analysed in either sanitized (i.e., anonymous) form, or can be made to reflect the parties involved (of course, only with the approval of the parties for their names to be included) (for example, Soskolne 1991). The objective behind case studies is not to seek retribution, but rather to provide examples for teaching purposes. Learning is enhanced by real-life situations.
It is from an understanding of the code that it becomes possible for a profession to develop more detailed standards of practice. These address more specific areas of activity associated with professional conduct, including a broad range of activity from interpersonal behaviours to both how research is conducted and how the results of that research are communicated. Standards of practice for the profession could be included in an ethics package; they reflect on each profession’s skill set and therefore add particular considerations that go beyond the statement of its ethics principles.
Scope of Codes
The development of a code by any profession has almost invariably tended to be driven by issues having a direct bearing on that profession. Consequently, codes tend to have a focus narrowly defined by each profession’s own concerns. However, codes also need to take broader social issues into account (Fawcett 1993). In fact, in a recent analysis of several codes, Summers et al. (1995) found that guidelines on specific social issues, such as environmental effects or conflict resolution, are scarcely mentioned at all in existing codes. Because the professions manifest substantial influence, if their codes indeed were to take broader social issues into account, then a great confluence and concurrence of effort would be brought to bear on those areas of human endeavour that currently fall between the cracks in promoting the common social good. Such pressure could help reduce dangers to human welfare, such as militarism and ecological destruction.
Ethics Training
It should be recognized that there exist two schools of thought for ethics training: one is based in a principle-driven approach while the other is case based, also known as casuistry. It is this author’s view, which remains to be tested, that a balance between the two is essential for successful applied ethics training in the professions (Soskolne 1991/92). However, it is well known that ethically analyzed case study material has an invaluable role to play in the education process. Cases provide a context for applying principles.
Because graduate ethics training in the professions is becoming more recognized as an essential place for students to gain awareness of the values, ethical principles and standards of practice of the profession, a model curriculum might ideally be included as part of a code; this will facilitate the training of students intent on entering the profession. The need for this is demonstrated through a recent survey that identified inconsistencies and shortcomings regarding the ethics components in graduate training programmes across the United States (Swazey, Anderson and Seashore 1993).
Recent History of Codes in Selected Professions
In western cultures, the medical profession has had the advantage of discussions about ethics since the time of Socrates (470–399 B.C.), Plato (427–347 B.C.) and Aristotle (384–322 B.C.) (Johnson 1965). Since then, codes have been developed and periodically revised in response to newly recognized issues arising, for example, from human value shifts and, more recently, from technological advances (Declaration of Helsinki 1975; Ad hoc Committee on Medical Ethics 1984; Russel and Westrin 1992). Since the 1960s, other professions have become involved in code development for their own professional organizations. The area of professional codes in fact has become a cottage industry since the 1980s. The American Association for the Advancement of Science (AAAS) has been instrumental in this movement. Under the auspices of its Committee on Scientific Freedom and Responsibility, AAAS initiated a seminal professional ethics project designed to examine the features of and activities associated with codes in the science and engineering professions. The report arising from this effort subsequently generated renewed interest in discussing both code development and revision with many of the professions (Chalk, Frankel and Chafer 1980).
The health/caring professions have long been engaged in discussions of ethical tensions arising from the nature of their professional pursuits. The codes that have evolved have tended, however, to focus on the physician-patient relationship, with concerns about confidentiality being pre-eminent. More recently, perhaps motivated by the growth of applied health research, codes have expanded their attention to include issues pertaining to researcher-patient relationships. Because of population-based research, codes now are addressing concerns for researcher-population relationships. The latter has been aided by the experience of other professions such as sociology, anthropology and statistics.
Many of the caring professions related to the practice of occupational health have been engaged in the discussion of professional ethics. These include: industrial hygiene (Yoder 1982; LaDou 1986); epidemiology (Beauchamp et al. 1991; IEA Workshop on Ethics, Health Policy and Epidemiology 1990; Chemical Manufacturers Association’s Epidemiology Task Group 1991; Council for International Organizations of Medical Sciences 1991, 1993); medicine and numerous of its subspeciality areas, including occupational medicine (Coye 1982; American Occupational Medical Association 1986; International Commission on Occupational Health 1992; Standing Committee of Doctors of the EEC 1980); nursing; toxicology; statistics (International Statistical Institute 1986); psychology; engineering and risk analysis.
In the occupationally specific areas of health services (Guidotti et al. 1989), medicine (Samuels 1992) and health and safety (LaDou 1986), as well as in occupational and environmental health (Rest 1995), relevant portions of professional codes have been abstracted. These presentations serve well the need for furthering discussion in these areas with a view to revising extant codes.
The importance of integrating ethics into the day-to-day activities of professionals is exemplified by these recent texts, which contain appropriately detailed sections on ethics. The professional thereby is reminded that in all aspects of professional practice, all decisions and recommendations have consequences with associated ethical underpinnings.
More recent work on the subject of misconduct in science requires integration into newer texts (Dale 1993; Grandjean and Andersen 1993; Office of the Assistant Secretary for Health 1992; Price 1993; Reed 1989; Sharphorn 1993; Soskolne 1993a; Soskolne 1993b; Soskolne and Macfarlane, 1995; Teich and Frankel 1992). Because one of the fundamental goals of science is the pursuit of truth through objectivity, plagiarism and the fabrication or the falsification of data are counter to the scientific ethic. As the scientific enterprise expands to include more and more scientists, misconduct in science is coming to the attention of the public more frequently. However, it is believed that even in the face of increasing competition and the potential for conflicting interests, the vast majority of those engaged in science do adhere to the principles of truth and objectivity. The frequency of misconduct does, however, remain difficult to assess (Goldberg and Greenberg 1993; Greenberg and Martell 1992; Frankel 1992).
The potential harm to particular scientific efforts as a result of misconduct is one concern. Another concern is the loss of faith by the public in scientists, with consequent reductions in support for the scientific enterprise. The latter has such potentially dire consequences for both science and society that all scientists, and especially students of science, need to be trained in the scientific ethic and reminded of these principles from time to time.
Several case studies serve to demonstrate misconduct (Broad and Wade 1982; Office of Research Integrity 1993; Price 1993; Needleman, Geiger and Frank 1985; Soskolne and Macfarlane, 1995; Swazey, Anderson and Seashore 1993; Soskolne 1991). The determinants of ethical dilemmas are numerous, but one survey among risk analysts in New Jersey (Goldberg and Greenberg 1993) suggests that the two most important causes are “on the job pressure” and “pressure caused by economic implications of result”. The authors of this study noted that possible causes of misconduct include “conflicts of interest, competition with unregulated and unscrupulous competitors, and general lack of individual or societal ethics”. While some codes do address the need for honesty and objectivity in science, the seriousness of current pressures to perform in the presence of apparently declining awareness of societal ethics would dictate that training at all levels include the subject of ethics, values and philosophy. Indeed, the United States Public Health Service requires that universities seeking to obtain research grant support have procedures in place for dealing with and reporting misconduct in science (Reed 1989). Furthermore, university training programmes in public health disciplines must include ethics teaching to qualify for federal funding (Office of the Assistant Secretary for Health 1992).
Normative Nature of Codes
Codes of professional conduct tend to be a narrative description of an assemblage of normative practices. These practices pertain to the moral and ethical standards of a group, be it a professional organization, association or society, having a common skill set in the service of people.
The basis of respective codes has been the so-called Golden Rule, which prescribes that one should do to others what one would have others do to oneself, do one’s level best, and call to the attention of others any act of misconduct.
Approaches to Developing Codes
Most professional organizations have produced codes through the top-down approach, where the elected officials of the profession have undertaken the task. However, as noted earlier (see “Code development, review and revision”), the bottom-up approach is more likely to result in compliance with codes, because grass-roots participation in the process results in a feeling of ownership of the outcome and hence a greater likelihood of compliance. The view that the power brokers of the profession have major influence over the specification of what constitutes appropriate professional conduct could detract from the credibility associated with any resultant code. The more that the “final” code is reflective of community norms, the greater the likelihood that it will be adhered to.
Codes developed by international organizations do have the power of influencing regional groups of people to consider the concerns and statements included in international codes. In this way, regions that have not given attention to the development of codes might be stimulated to do so. Presumably, provided the intent of international codes is limited to a function of providing stimulus, ongoing interaction could serve to iteratively modify and update international codes so that ultimately the international code could well reflect transnational concerns. Care must be exercised to respect regional cultural norms that are not in conflict with, for example, accepted declarations on human rights. Hence, code makers should be sensitive to cultural differences, and not allow their work to homogenize human behaviour; cultural diversity must rather be encouraged.
Mechanisms for Enforcement
Noted earlier was the fact that codes do imply some degree of self-regulation if the expectation of accountability is to have meaning. This would suggest the existence of procedures for investigating allegations of misconduct (or malpractice) of any type, and for correcting conduct deemed professionally inappropriate (Price 1993; Dale 1993; Grandjean and Andersen 1993). In addition, some remedy might be provided for any harms that might have derived from professional misconduct.
The procedures to be invoked in investigations of allegations of misconduct or malpractice must be pre-specified. The maxim of “innocent until proven guilty” should be evident and be seen to be applied. However, because public confidence rests on professional self-regulation, investigations should be dealt with as efficiently as possible with respect for due process at all times (Sharphorn 1993; Soskolne 1993a, b).
The threat of revoking professional licence to practice is one way that the profession has leverage to maximize among its members adherence to any codes. Many professions have no such leverage; their membership is made up of dues-paying individuals with a wide range of qualifications for which regional legislatures have not required licensure as a requirement of membership in the profession. The loss of the right to practice one’s profession therefore is not applicable in many professions as a penalty for misconduct. The only recourse in such instances is that of peer pressure.
Current Issues of Concern to Occupational Health Professionals
It is not within the scope of this article to develop a comprehensive code, but rather to present the process by which codes are developed. It is the intent in so doing to provide motivation for the ongoing discussion of codes (as a component of a broader-based professional ethics programme) and to alert the reader to current issues about which further discussion is needed for the possible inclusion of such resolved matters into revised codes.
As noted by Guidotti et al. (1989), certain issues had been overlooked in codes that existed at that time. These included the virtue of full access to accurate information, and that the burden of risk should not be taken by the worker in the presence of unproved but sound evidence. The question of accurate information and implied truth has associated with it issues of scientific integrity (as referred to in North America) or of scientific dishonesty (as referred to in Denmark) (Andersen et al. 1992; Grandjean and Andersen 1993). Clearly, the pursuit of truth as the main target of scientific endeavour must be reinforced at every opportunity, including its full integration into codes, case study materials and ethics programmes generally (Hall 1993).
With technological advances, the ability grows to more precisely measure biological parameters. For example, biomarkers is one area that opens up a Pandora’s box of ethical issues and resulting tensions that have yet to be addressed in codes. Several such issues have been identified by Ashford (1986) and by Grandjean (1991). Since existing codes were developed prior to the availability on a commercial scale of this technology, codes would serve the occupational health community better if they were updated to provide some guidance on related concerns. To achieve this, explication of such thorny questions as the workers’ right to work in the face of high-risk susceptibility identified through biomarker assays, requires extensive discussion in workshops and conferences specially convened for the purpose. Case study materials would assist in this effort. So profound are the ramifications of biomarker studies that their implications, as well as those related to other potential high technology breakthroughs, could be best addressed through the profession’s continual review of the code.
Because issues such as biomarkers can be difficult to resolve, it may be appropriate for like professions dealing with similar issues to consolidate their efforts and establish mechanisms for exchanging information to assist in the resolution of difficult and challenging related ethical issues. In particular, the need to address the timing for introducing high technology procedures for which ethical considerations have not yet been established also needs to be recognized and addressed by standing committees on ethics for the respective occupational safety and health professions. Other stakeholder groups probably should be included in such deliberations, including the community representatives themselves on whom such studies would be conducted.
In a researcher’s enthusiasm to implement new technological measures into studies for which the ramifications are not fully understood (in the belief that benefit would result), it should be recognized that greater harm than benefit to the subjects of these studies could, in fact, arise (e.g., job loss today is potentially more harmful than the possibility of premature death at some future date). Hence, great caution must be exercised in advance of the implementation of such technologies. Only after due discussion has been exercised by the professional groups having an interest in the use of such technologies, together with a broad range of stakeholder interest groups, should their implementation be considered.
Another current issue involves the notion of data privacy, which is one that returns to the public arena periodically. In the age of computers, the potential exists for linking records created for one purpose with records created for another purpose. Advocates of data privacy have been concerned that records so created could be potentially damaging to individuals. While individual rights to privacy must take precedence over the research needs of the community, the fact that population-based research is uninterested in the data at the individual level must be brought to the attention of the data privacy advocates. In so doing, it should be easy to demonstrate that the public good is better served by allowing appropriately qualified researchers, trained in data processing and confidentiality, access to individual data for population-based research purposes.
Concern about the extension of principlism applied in the physician-patient setting to that of the community-research situation has been noted above (see “Recent history of codes in selected professions”). Vineis and Soskolne (1993) have found that the established principles of autonomy, beneficence, non-maleficence and distributive justice are not easily applicable at the societal level. For example, available information about the safety of exposures often is too scanty to allow decisional autonomy; beneficence is considered from the societal viewpoint rather than from that of the individual; and equity is frequently violated. Ethics require careful consideration when defining what is acceptable to society; the simple mathematical formulations used for risk-benefit evaluations cannot be applied directly to individuals. Further development and integration of these ideas are necessary.
In conclusion, codes have a fundamental role to play in the professions. They also could play an important role in safeguarding the common good if they took broader social issues into account. They need to be developed with grass-roots and stakeholder input as part of a broad-based programme of ethics supported by each profession. Codes—including the profession’s core values, the commentary associated with a code and case study materials—must be subjected to a process of periodic review and revision. Now, more than ever, codes are needed not only for professional accountability and self-regulation purposes, but also to help practitioners with the moral and ethical challenges faced by constantly advancing technologies that have implications, amongst others, for the rights and duties of all affected individuals and interest groups. A substantial and challenging task lies ahead.
Lung Function Examination
Lung function may be measured in a number of ways. However, the aim of the measurements has to be clear before the examination, in order to interpret the results correctly. In this article we will discuss lung function examination with special regard to the occupational field. It is important to remember the limitations in different lung function measurements. Acute temporary lung function effects may not be discernible in case of exposure to fibrogenic dust like quartz and asbestos, but chronic effects on lung function after long-term (>20 years) exposure may be. This is due to the fact that chronic effects occur years after the dust is inhaled and deposited in the lungs. On the other hand, acute temporary effects of organic and inorganic dust, as well as mould, welding fumes and motor exhaust, are well suited to study. This is due to the fact that the irritative effect of these dusts will occur after a few hours of exposure. Acute or chronic lung function effects also may be discernible in cases of exposure to concentrations of irritating gases (nitrogen dioxide, aldehydes, acids and acid chlorides) in the vicinity of well documented exposure limit values, especially if the effect is potentiated by particulate air contamination.
Lung function measurements have to be safe for the examined subjects, and the lung function equipment has to be safe for the examiner. A summary of the specific requirements for different kinds of lung function equipment are available (e.g., Quanjer et al. 1993). Of course, the equipment must be calibrated according to independent standards. This may be difficult to achieve, especially when computerized equipment is being used. The result of the lung function test is dependent on both the subject and the examiner. To provide satisfactory results from the examination, technicians have to be well trained, and able to instruct the subject carefully and also encourage the subject to carry out the test properly. The examiner should also have knowledge about the airways and lungs in order to interpret the results from the recordings correctly.
It is recommended that the methods used have a fairly high reproducibility both between and within subjects. Reproducibility may be measured as the coefficient of variation, that is, the standard deviation multiplied by 100 divided by the mean value. Values below 10% in repeated measurements on the same subject are deemed acceptable.
In order to determine if the measured values are pathological or not, they must be compared with prediction equations. Usually the prediction equations for spirometric variables are based on age and height, stratified for sex. Men have on the average higher lung function values than women, of the same age and height. Lung function decreases with age and increases with height. A tall subject will therefore have higher lung volume than a short subject of the same age. The outcome from prediction equations may differ considerably between different reference populations. The variation in age and height in the reference population will also influence the predicted values. This means, for example, that a prediction equation must not be used if age and/or height for the examined subject are outside the ranges for the population that is the basis for the prediction equation.
Smoking will also diminish lung function, and the effect may be potentiated in subjects who are occupationally exposed to irritating agents. Lung function used to be considered as not being pathological if the obtained values are within 80% of the predicted value, derived from a prediction equation.
Measurements
Lung function measurements are carried out to judge the condition of the lungs. Measurements may either concern single or multiple measured lung volumes, or the dynamic properties in the airways and lungs. The latter is usually determined through effort-dependent manoeuvres. The conditions in the lungs may also be examined with regard to their physiological function, that is, diffusion capacity, airway resistance and compliance (see below).
Measurements concerning ventilatory capacity are obtained by spirometry. The breathing manoeuvre is usually performed as a maximal inspiration followed by a maximal expiration, vital capacity (VC, measured in litres). At least three technically satisfactory recordings (i.e., full inspiration and expiration effort and no observed leaks) should be done, and the highest value reported. The volume may be directly measured by a water-sealed or a low-resistive bell, or indirectly measured by pneumotachography (i.e., integration of a flow signal over time). It is important here to note that all measured lung volumes should be expressed in BTPS, that is, body temperature and ambient pressure saturated with water vapour.
Forced expired vital capacity (FVC, in litres) is defined as a VC measurement performed with a maximally forced expiratory effort. Due to the simplicity of the test and the relatively inexpensive equipment, the forced expirogram has become a useful test in the monitoring of lung function. However, this has resulted in many poor recordings, of which the practical value is debatable. In order to carry out satisfactory recordings, the updated guideline for the collection and use of the forced expirogram, published by the American Thoracic Society in 1987, may be useful.
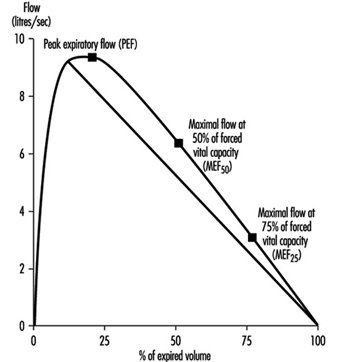
Instantaneous flows may be measured on flow-volume or flow-time curves, while time average flows or times are derived from the spirogram. Associated variables which can be calculated from the forced expirogram are forced expired volume in one second (FEV1, in litres per second), in percentage of FVC (FEV1%), peak flow (PEF, l/s), maximal flows at 50% and 75% of forced vital capacity (MEF50 and MEF25, respectively). An illustration of the derivation of FEV1 from the forced expirogram is outlined in figure 1. In healthy subjects, maximal flow rates at large lung volumes (i.e., at the beginning of expiration) reflect mainly the flow characteristics of the large airways while those at small lung volumes (i.e., the end of expiration) are usually held to reflect the characteristics of the small airways, figure 2. In the latter the flow is laminar, while in the large airways it may be turbulent.
Figure 1. Forced expiratory spirogram showing the derivation of FEV1 and FVC according to the extrapolation principle.
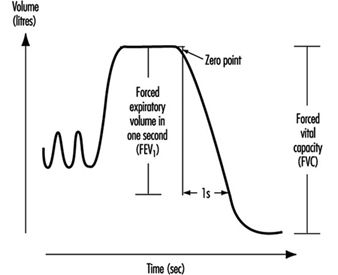
Figure 2. Flow-volume curve showing the derivation of peak expiratory flow (PEF), maximal flows at 50% and 75% of forced vital capacity (![]() and
and ![]() , respectively).
, respectively).
PEF may also be measured by a small portable device such as the one developed by Wright in 1959. An advantage with this equipment is that the subject may carry out serial measurements—for example, at the workplace. To get useful recordings, however, it is necessary to instruct the subjects well. Moreover, one should keep in mind that measurements of PEF with, for example, a Wright meter and those measured by conventional spirometry should not be compared due to the different blow techniques.
The spirometric variables VC, FVC and FEV1 show a reasonable variation between individuals where age, height and sex usually explain 60 to 70% of the variation. Restrictive lung function disorders will result in lower values for VC, FVC and FEV1. Measurements of flows during expiration show a great individual variation, since the measured flows are both effort and time dependent. This means, for example, that a subject will have extremely high flow in case of diminished lung volume. On the other hand, the flow may be extremely low in case of very high lung volume. However, the flow is usually decreased in case of a chronic obstructive disease (e.g., asthma, chronic bronchitis).
Figure 3. A principal outline of the equipment for determination of total lung capacity (TLC) according to the helium dilution technique.
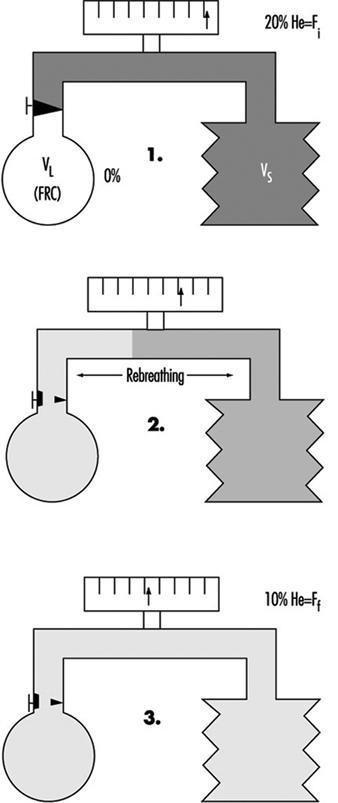
The proportion of residual volume (RV), that is, the volume of air which still is in the lungs after a maximal expiration, can be determined by gas dilution or by body plethysmography. The gas dilution technique requires less complicated equipment and is therefore more convenient to use in studies carried out at the workplace. In figure 3, the principle for the gas dilution technique has been outlined. The technique is based on dilution of an indicator gas in a rebreathing circuit. The indicator gas must be sparingly soluble in biological tissues so that it is not taken up by the tissues and blood in the lung. Hydrogen was initially used, but because of its ability to form explosive mixtures with air it was replaced by helium, which is easily detected by means of the thermal conductivity principle.
The subject and the apparatus form a closed system, and the initial concentration of the gas is thus reduced when it is diluted into the gas volume in the lungs. After equilibration, the concentration of indicator gas is the same in the lungs as in the apparatus, and functional residual capacity (FRC) can be calculated by means of a simple dilution equation. The volume of the spirometer (including the addition of the gas mixture into the spirometer) is denoted by VS, VL is the volume of the lung, Fi is the initial gas concentration and Ff is the final concentration.
FRC = VL = [(VS · Fi) / Ff] – VS
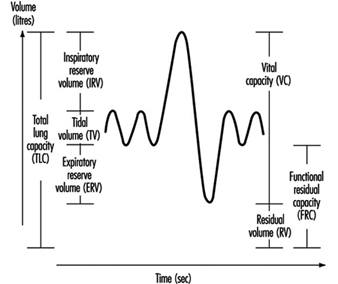
Two to three VC manoeuvres are carried out to provide a reliable base for the calculation of TLC (in litres). The subdivisions of the different lung volumes are outlined in figure 4.
Figure 4. Spirogram labelled to show the subdivisions of the total capacity.
Due to change in the elastic properties of the airways, RV and FRC increase with age. In chronic obstructive diseases, increased values of RV and FRC are usually observed, while VC is decreased. However, in subjects with badly ventilated lung areas—for example, subjects with emphysema—the gas dilution technique may underestimate RV, FRC and also TLC. This is due to the fact that the indicator gas will not communicate with closed-off airways, and therefore the decrease in the indicator gas concentration will give erroneously small values.
Figure 5. A principal outline of the recording of airway closure and the slope of the alveolar plateau (%![]() ).
).
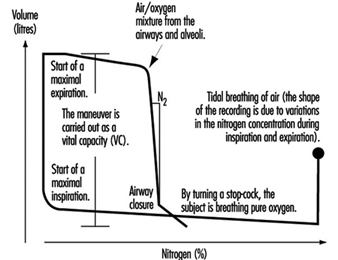
Measures of airway closure and gas distribution in the lungs can be obtained in one and the same manoeuvre by the single breath wash-out technique, figure 5. The equipment consists of a spirometer connected to a bag-in-box system and a recorder for continuous measurements of nitrogen concentration. The manoeuvre is carried out by means of a maximal inspiration of pure oxygen from the bag. In the beginning of the expiration, the nitrogen concentration increases as a result of emptying the subject’s deadspace, containing pure oxygen. The expiration continues with the air from the airways and alveoli. Finally, air from the alveoli, containing 20 to 40% nitrogen, is expired. When the expiration from the basal parts of the lungs increases, the nitrogen concentration will rise abruptly in case of airway closure in dependent lung regions, figure 5. This volume above RV, at which airways close during an expiration, is usually expressed as closing volume (CV) in percentage of VC (CV%). Distribution of the inspired air in the lungs is expressed as the slope of the alveolar plateau (%N2 or phase III, %N2/l). It is obtained by taking the difference in nitrogen concentration between the point when 30% of the air is exhaled and the point for airway closure, and dividing this by the corresponding volume.
Ageing as well as chronic obstructive disorders will result in increased values for both CV% and phase III. However, not even healthy subjects have a uniform gas distribution in the lungs, resulting in slightly elevated values for phase III, that is, 1 to 2% N2/l. The variables CV% and phase III are considered to reflect the conditions in the peripheral small airways with an internal diameter about 2 mm. Normally, the peripheral airways contribute to a small part (10 to 20%) of the total airway resistance. Quite extensive changes which are not detectable by conventional lung function tests like dynamic spirometry, may occur, for example, as a result of an exposure to irritating substances in the air in the peripheral airways. This suggests that airway obstruction begins in the small airways. Results from studies also have shown alterations in CV% and phase III before any changes from the dynamic and static spirometry have occurred. These early changes may go into remission when exposure to hazardous agents has ceased.
The transfer factor of the lung (mmol/min; kPa) is an expression of the diffusion capacity of oxygen transport into the pulmonary capillaries. The transfer factor can be determined using single or multiple breath techniques; the single breath technique is considered to be most suitable in studies at the workplace. Carbon monoxide (CO) is used since the back pressure of CO is very low in the peripheral blood, in contrast to that of oxygen. The uptake of CO is assumed to follow an exponential model, and this assumption can be used to determine the transfer factor for the lung.
Determination of TLCO (transfer factor measured with CO) is carried out by means of a breathing manoeuvre including a maximal expiration, followed by a maximal inspiration of a gas mixture containing carbon monoxide, helium, oxygen and nitrogen. After a breath-holding period, a maximal exhalation is done, reflecting the content in the alveolar air, Figure 10. Helium is used for the determination of the alveolar volume (VA). Assuming that the dilution of CO is the same as for helium, the initial concentration of CO, before the diffusion has started, can be calculated. TLCO is calculated according to the equation outlined below, where k depends on the dimensions of the component terms, t is the effective time for breath-holding and log is base 10 logarithm. Inspired volume is denoted Vi and the fractions F of CO and helium are denoted by i and a for inspired and alveolar, respectively.
TLCO = k Vi (Fa,He/Fi,He) log (Fi,CO Fa,He/Fa,CO Fi,He) (t)-1
Figure 6. A principal outline of the recording of transfer factor

The size of TLCO will depend on a variety of conditions—for example, the amount of available haemoglobin, the volume of ventilated alveoli and perfused lung capillaries and their relation to each other. Values for TLCO decrease with age and increase with physical activity and increased lung volumes. Decreased TLCO will be found in both restrictive and obstructive lung disorders.
Compliance (l/kPa) is a function, inter alia, of the elastic property of the lungs. The lungs have an intrinsic tendency to collaborate—that is, to collapse. The power to keep the lungs stretched will depend on the elastic lung tissue, the surface tension in the alveoli, and the bronchial musculature. On the other hand, the chest wall tends to expand at lung volumes 1 to 2 litres above the FRC level. At higher lung volumes, power has to be applied to further expand the chest wall. At the FRC level, the corresponding tendency in the lungs is balanced by the tendency to expand. The FRC level is therefore denoted by the resting level of the lung.
The compliance of the lung is defined as the change in volume divided by the change in transpulmonary pressure, that is, the difference between the pressures in the mouth (atmospheric) and in the lung, as the result of a breathing manoeuvre. Measurements of the pressure in the lung are not easily carried out and are therefore replaced by measurements of the pressure in the oesophagus. The pressure in the oesophagus is almost the same as the pressure in the lung, and it is measured with a thin polyethylene catheter with a balloon covering the distal 10 cm. During inspiratory and expiratory manoeuvres, the changes in volume and pressure are recorded by means of a spirometer and pressure transducer, respectively. When the measurements are performed during tidal breathing, dynamic compliance can be measured. Static compliance is obtained when a slow VC manoeuvre is carried out. In the latter case, the measurements are carried out in a body plethysmograph, and the expiration is intermittently interrupted by means of a shutter. However, measurements of compliance are cumbersome to perform when examining exposure effects on lung function at the worksite, and this technique is considered to be more appropriate in the laboratory.
A decreased compliance (increased elasticity) is observed in fibrosis. To cause a change in volume, large changes in pressure are required. On the other hand, a high compliance is observed, for example, in emphysema as the result of loss of elastic tissue and therefore also elasticity in the lung.
The resistance in the airways essentially depends on the radius and length of the airways but also on air viscosity. The airway resistance (RL in (kPa/l) /s), can be determined by use of a spirometer, pressure transducer and a pneumotachograph (to measure the flow). The measurements may also be carried out using a body plethysmograph to record the changes in flow and pressure during panting manoeuvres. By administration of a drug intended to cause broncho-constriction, sensitive subjects, as a result of their hyperreactive airways, may be identified. Subjects with asthma usually have increased values for RL.
Acute and Chronic Effects of Occupational Exposure on Pulmonary Function
Lung function measurement may be used to disclose an occupational exposure effect on the lungs. Pre-employment examination of lung function should not be used to exclude job-seeking subjects. This is because the lung function of healthy subjects varies within wide limits and it is difficult to draw a borderline below which it can safely be stated that the lung is pathological. Another reason is that the work environment should be good enough to allow even subjects with slight lung function impairment to work safely.
Chronic effects on the lungs in occupationally exposed subjects may be detected in a number of ways. The techniques are designed to determine historical effects, however, and are less suitable to serve as guidelines to prevent lung function impairment. A common study design is to compare the actual values in exposed subjects with the lung function values obtained in a reference population without occupational exposure. The reference subjects may be recruited from the same (or nearby) workplaces or from the same city.
Multivariate analysis has been used in some studies to assess differences between exposed subjects and matched unexposed referents. Lung function values in exposed subjects may also be standardized by means of a reference equation based on lung function values in the unexposed subjects.
Another approach is to study the difference between the lung function values in exposed and unexposed workers after adjustment for age and height with the use of external reference values, calculated by means of a prediction equation based on healthy subjects. The reference population may also be matched to the exposed subjects according to ethnic group, sex, age, height and smoking habits in order to further control for those influencing factors.
The problem is, however, to decide if a decrease is large enough to be classified as pathological, when external reference values are being used. Although the instruments in the studies have to be portable and simple, attention must be paid both to the sensitivity of the chosen method for detecting small anomalies in airways and lungs and the possibility of combining different methods. There are indications that subjects with respiratory symptoms, such as exertion dyspnoea, are at a higher risk of having an accelerated decline in lung function. This means that the presence of respiratory symptoms is important and so should not be neglected.
The subject may also be followed-up by spirometry, for example, once a year, for a number of years, in order to give a warning against the development of illness. There are limitations, however, since this will be very time-consuming and the lung function may have deteriorated permanently when the decrease can be observed. This approach therefore must not be an excuse for delay in carrying out measures in order to decrease harmful concentrations of air pollutants.
Finally, chronic effects on lung function may also be studied by examining the individual changes in lung function in exposed and unexposed subjects over a number of years. One advantage of the longitudinal study design is that the intersubject variability is eliminated; however, the design is considered to be time-consuming and expensive.
Susceptible subjects may also be identified by comparing their lung function with and without exposure during working shifts. In order to minimize possible effects of diurnal variations, lung function is measured at the same time of day on one unexposed and one exposed occasion. The unexposed condition can be obtained, for example, by occasionally moving the worker to an uncontaminated area or by use of a suitable respirator during a whole shift, or in some cases by performing lung function measurements in the afternoon of a worker’s day off.
One special concern is that repeated, temporary effects can result in chronic effects. An acute temporary lung function decrease may not only be a biological exposure indicator but also a predictor of a chronic lung function decrement. Exposure to air pollutants may result in discernible acute effects on lung function, although the mean values of the measured air pollutants are below the hygienic limit values. The question thus arises, whether these effects really are harmful in the long run. This question is hard to answer directly, especially since the air pollution in workplaces often has a complex composition and the exposure cannot be described in terms of mean concentrations of single compounds. The effect of an occupational exposure is also partly due to the sensitivity of the individual. This means that some subjects will react sooner or to a larger extent than others. The underlying pathophysiological ground for an acute, temporary decrease in lung function is not fully understood. The adverse reaction upon exposure to an irritating air contaminant is, however, an objective measurement, in contrast to subjective experiences like symptoms of different origin.
The advantage of detecting early changes in airways and lungs caused by hazardous air pollutants is obvious—the prevailing exposure may be reduced in order to prevent more severe illnesses. Therefore, an important aim in this respect is to use the measurements of acute temporary effects on lung function as a sensitive early warning system that can be used when studying groups of healthy working people.
Monitoring of Irritants
Irritation is one of the most frequent criteria for setting exposure limit values. It is, however, not certain that compliance with an exposure limit based on irritation will protect against irritation. It should be considered that an exposure limit for an air contaminant usually contains at least two parts—a time-weighted average limit (TWAL) and a short-term exposure limit (STEL), or at least rules for exceeding the time-weighted average limit, “excursion limits”. In the case of highly irritating substances, such as sulphur dioxide, acrolein and phosgene, it is important to limit the concentration even during very short periods, and it has therefore been common practice to fix occupational exposure limit values in the form of ceiling limits, with a sampling period that is kept as short as the measuring facilities will allow.
Time-weighted average limit values for an eight-hour day combined with rules for excursion above these values are given for most of the substances in the American Conference of Governmental Industrial Hygienists (ACGIH) threshold limit value (TLV) list. The TLV list of 1993-94 contains the following statement concerning excursion limits for exceeding limit values:
“For the vast majority of substances with a TLV-TWA, there is not enough toxicological data available to warrant a STEL = short-term exposure limit). Nevertheless, excursions above the TLV-TWA should be controlled even where the eight-hour TWA is within recommended limits.”
Exposure measurements of known air contaminants and comparison with well documented exposure limit values should be carried out on a routine basis. There are, however, many situations when the determination of compliance with exposure limit values is not enough. This is the case in the following circumstances (inter alia):
- when the limit value is too high to safeguard against irritation
- when the irritant is unknown
- when the irritant is a complex mixture and there is no suitable indicator known.
As advocated above, the measurement of acute, temporary effects on lung function can be used in these cases as a warning against over-exposure to irritants.
In cases (2) and (3), acute, temporary effects on lung function may be applicable also in testing the efficiency of control measures to decrease exposure to air contamination or in scientific investigations, for example, in attributing biological effects to components of air contaminants. A number of examples follow in which acute, temporary lung function effects have been successfully employed in occupational health investigations.
Studies of Acute, Temporary Lung Function Effects
Work-related, temporary decrease of lung function over a work shift was recorded in cotton workers at the end of 1950. Later, several authors reported work-related, acute, temporary changes of lung function in hemp and textile workers, coal miners, workers exposed to toluene di-isocyanate, fire-fighters, rubber processing workers, moulders and coremakers, welders, ski waxers, workers exposed to organic dust and irritants in water-based paints.
However, there are also several examples where measurements before and after exposure, usually during a shift, have failed to demonstrate any acute effects, despite a high exposure. This is probably due to the effect of normal circadian variation, mainly in lung function variables depending on the size of airway calibre. Thus the temporary decrease in these variables must exceed the normal circadian variation to be recognized. The problem may be circumvented, however, by measuring lung function at the same time of the day at each study occasion. By using the exposed employee as his or her own control, the interindividual variation is further decreased. Welders were studied in this way, and although the mean difference between unexposed and exposed FVC values was less than 3% in 15 examined welders, this difference was significant at the 95% confidence level with a power of more than 99%.
The reversible transient effects on the lungs can be used as an exposure indicator of complicated irritating components. In the study cited above, particles in the work environment were crucial for the irritating effects on the airways and lungs. The particles were removed by a respirator consisting of a filter combined with a welding helmet. The results indicated that the effects on the lungs were caused by the particles in welding fumes, and that the use of a particulate respirator might prevent this effect.
Exposure to diesel exhaust also gives measurable irritative effects on the lungs, shown as an acute, temporary lung function decrease. Mechanical filters mounted on the exhaust pipes of trucks used in loading operations by stevedores relieved subjective disorders and reduced the acute, temporary lung function decrease observed when no filtration was done. The results thus indicate that the presence of particles in the work environment does play a role in the irritative effect on airways and lungs, and that it is possible to assess the effect by measurements of acute changes in lung function.
A multiplicity of exposures and a continually changing work environment may present difficulties in discerning the causal relationship of the different agents existing in a work environment. The exposure scenario in sawmills is an illuminating example. It is not possible (e.g., for economical reasons) to carry out exposure measurements of all possible agents (terpenes, dust, mould, bacteria, endotoxin, mycotoxins, etc.) in this work environment. A feasible method may be to follow the development of lung function longitudinally. In a study of sawmill workers in the wood-trimming department, lung function was examined before and after a working week, and no statistically significant decrease was found. However, a follow-up study carried out a few years later disclosed that those workers who actually had a numerical decrease in lung function during a working week also had an accelerated long-term decline in lung function. This may indicate that vulnerable subjects can be detected by measuring changes in lung function during a working week.
Structure and Function
The respiratory system extends from the breathing zone just outside of the nose and mouth through the conductive airways in the head and thorax to the alveoli, where respiratory gas exchange takes place between the alveoli and the capillary blood flowing around them. Its prime function is to deliver oxygen (O2) to the gas-exchange region of the lung, where it can diffuse to and through the walls of the alveoli to oxygenate the blood passing through the alveolar capillaries as needed over a wide range of work or activity levels. In addition, the system must also: (1) remove an equal volume of carbon dioxide entering the lungs from the alveolar capillaries; (2) maintain body temperature and water vapour saturation within the lung airways (in order to maintain the viability and functional capacities of the surface fluids and cells); (3) maintain sterility (to prevent infections and their adverse consequences); and (4) eliminate excess surface fluids and debris, such as inhaled particles and senescent phagocytic and epithelial cells. It must accomplish all of these demanding tasks continuously over a lifetime, and do so with high efficiency in terms of performance and energy utilization. The system can be abused and overwhelmed by severe insults such as high concentrations of cigarette smoke and industrial dust, or by low concentrations of specific pathogens which attack or destroy its defence mechanisms, or cause them to malfunction. Its ability to overcome or compensate for such insults as competently as it usually does is a testament to its elegant combination of structure and function.
Mass Transfer
The complex structure and numerous functions of the human respiratory tract have been summarized concisely by a Task Group of the International Commission on Radiological Protection (ICRP 1994), as shown in figure 1. The conductive airways, also known as the respiratory dead space, occupy about 0.2 litres. They condition the inhaled air and distribute it, by convective (bulk) flow, to the approximately 65,000 respiratory acini leading off the terminal bronchioles. As tidal volumes increase, convective flow dominates gas exchange deeper into the respiratory bronchioles. In any case, within the respiratory acinus, the distance from the convective tidal front to alveolar surfaces is short enough so that efficient CO2-O2 exchange takes place by molecular diffusion. By contrast, airborne particles, with diffusion coefficients smaller by orders of magnitude than those for gases, tend to remain suspended in the tidal air, and can be exhaled without deposition.
Figure 1. Morphometry, cytology, histology, function and structure of the respiratory tract and regions used in the 1994 ICRP dosimetry model.

A significant fraction of the inhaled particles do deposit within the respiratory tract. The mechanisms accounting for particle deposition in the lung airways during the inspiratory phase of a tidal breath are summarized in figure 2. Particles larger than about 2 mm in aerodynamic diameter (diameter of a unit density sphere having the same terminal settling (Stokes) velocity) can have significant momentum and deposit by impaction at the relatively high velocities present in the larger airways. Particles larger than about 1 mm can deposit by sedimentation in the smaller conductive airways, where flow velocities are very low. Finally, particles with diameters between 0.1 and 1 mm, which have a very low probability of depositing during a single tidal breath, can be retained within the approximately 15% of the inspired tidal air that is exchanged with residual lung air during each tidal cycle. This volumetric exchange occurs because of the variable time-constants for airflow in the different segments of the lungs. Due to the much longer residence times of the residual air in the lungs, the low intrinsic particle displacements of 0.1 to 1 mm particles within such trapped volumes of inhaled tidal air become sufficient to cause their deposition by sedimentation and/or diffusion over the course of successive breaths.
Figure 2. Mechanisms for particle deposition in lung airways

The essentially particle-free residual lung air that accounts for about 15% of the expiratory tidal flow tends to act like a clean-air sheath around the axial core of distally moving tidal air, such that particle deposition in the respiratory acinus is concentrated on interior surfaces such as airway bifurcations, while interbranch airway walls have little deposition.
The number of particles deposited and their distribution along the respiratory tract surfaces are, along with the toxic properties of the material deposited, the critical determinants of pathogenic potential. The deposited particles can damage the epithelial and/or the mobile phagocytic cells at or near the deposition site, or can stimulate the secretion of fluids and cell-derived mediators that have secondary effects on the system. Soluble materials deposited as, on, or within particles can diffuse into and through surface fluids and cells and be rapidly transported by the bloodstream throughout the body.
Aqueous solubility of bulk materials is a poor guide to particle solubility in the respiratory tract. Solubility is generally greatly enhanced by the very large surface-to-volume ratio of particles small enough to enter the lungs. Furthermore, the ionic and lipid contents of surface fluids within the airways are complex and highly variable, and can lead to either enhanced solubility or to rapid precipitation of aqueous solutes. Furthermore, the clearance pathways and residence times for particles on airway surfaces are very different in the different functional parts of the respiratory tract.
The revised ICRP Task Group’s clearance model identifies the principal clearance pathways within the respiratory tract that are important in determining the retention of various radioactive materials, and thus the radiation doses received by respiratory tissues and other organs after translocation. The ICRP deposition model is used to estimate the amount of inhaled material that enters each clearance pathway. These discrete pathways are represented by the compartment model shown in figure 3. They correspond to the anatomic compartments illustrated in Figure 1, and are summarized in table 1, along with those of other groups providing guidance on the dosimetry of inhaled particles.
Figure 3. Compartment model to represent time-dependent particle transport from each region in 1994 ICRP model
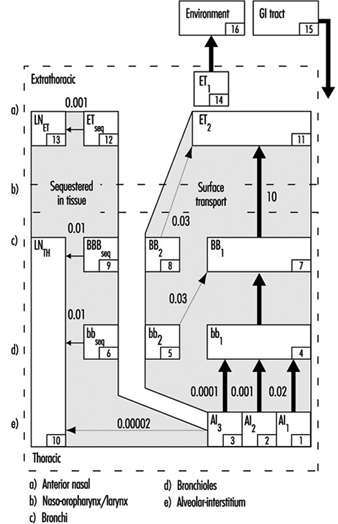
Table 1. Respiratory tract regions as defined in particle deposition models
| Anatomic structures included | ACGIH Region | ISO and CEN Regions | 1966 ICRP Task Group Region | 1994 ICRP Task Group Region |
| Nose, nasopharynx Mouth, oropharynx, laryngopharynx |
Head airways (HAR) | Extrathoracic (E) | Nasopharynx (NP) | Anterior nasal passages (ET1 ) All other extrathoracic (ET2 ) |
| Trachea, bronchi | Tracheobronchial (TBR) | Tracheobronchial (B) | Tracheobronchial (TB) | Trachea and large bronchi (BB) |
| Bronchioles (to terminal bronchioles) | Bronchioles (bb) | |||
| Respiratory bronchioles, alveolar ducts, alveolar sacs, alveoli |
Gas exchange (GER) | Alveolar (A) | Pulmonary (P) | Alveolar-interstitial (AI) |
Extrathoracic airways
As shown in figure 1, the extrathoracic airways were partitioned by ICRP (1994) into two distinct clearance and dosimetric regions: the anterior nasal passages (ET1) and all other extrathoracic airways (ET2)—that is, the posterior nasal passages, the naso- and oropharynx, and the larynx. Particles deposited on the surface of the skin lining the anterior nasal passages (ET1) are assumed to be subject only to removal by extrinsic means (nose blowing, wiping and so on). The bulk of material deposited in the naso-oropharynx or larynx (ET2) is subject to fast clearance in the layer of fluid that covers these airways. The new model recognizes that diffusional deposition of ultrafine particles in the extrathoracic airways can be substantial, while the earlier models did not.
Thoracic airways
Radioactive material deposited in the thorax is generally divided between the tracheobronchial (TB) region, where deposited particles are subject to relatively fast mucociliary clearance, and the alveolar-interstitial (AI) region, where the particle clearance is much slower.
For dosimetry purposes, the ICRP (1994) divided deposition of inhaled material in the TB region between the trachea and bronchi (BB), and the more distal, small airways, the bronchioles (bb). However, the subsequent efficiency with which cilia in either type of airways are able to clear deposited particles is controversial. In order to be certain that doses to bronchial and bronchiolar epithelia would not be underestimated, the Task Group assumed that as much as half the number of particles deposited in these airways is subject to relatively “slow” mucociliary clearance. The likelihood that a particle is cleared relatively slowly by the mucociliary system appears to depend on its physical size.
Material deposited in the AI region is subdivided among three compartments (AI1, AI2 and AI3) that are each cleared more slowly than TB deposition, with the subregions cleared at different characteristic rates.
Figure 4. Fractional deposition in each region of respiratory tract for reference light worker (normal nose breather) in 1994 ICRP model.

Figure 4 depicts the predictions of the ICRP (1994) model in terms of the fractional deposition in each region as a function of the size of the inhaled particles. It reflects the minimal lung deposition between 0.1 and 1 mm, where deposition is determined largely by the exchange, in the deep lung, between tidal and residual lung air. Deposition increases below 0.1 mm as diffusion becomes more efficient with decreasing particle size. Deposition increases with increasing particle size above 1 mm as sedimentation and impaction become increasingly effective.
Less complex models for size-selective deposition have been adopted by occupational health and community air pollution professionals and agencies, and these have been used to develop inhalation exposure limits within specific particle size ranges. Distinctions are made between:
- those particles that are not aspirated into the nose or mouth and therefore represent no inhalation hazard
- the inhalable (also known as inspirable) particulate mass (IPM)—those that are inhaled and are hazardous when deposited anywhere within the respiratory tract
- the thoracic particulate mass (TPM)—those that penetrate the larynx and are hazardous when deposited anywhere within the thorax and
- the respirable particulate mass (RPM)—those particles that penetrate through the terminal bronchioles and are hazardous when deposited within the gas-exchange region of the lungs.
In the early 1990s there has been an international harmonization of the quantitative definitions of IPM, TPM and RPM. The size-selective inlet specifications for air samplers meeting the criteria of the American Conference of Governmental Industrial Hygienists (ACGIH 1993), the International Organization for Standardization (ISO 1991) and the European Standardization Committee (CEN 1991) are enumerated in table 2. They differ from the deposition fractions of ICRP (1994), especially for larger particles, because they take the conservative position that protection should be provided for those engaged in oral inhalation, and thereby bypass the more efficient filtration efficiency of the nasal passages.
Table 2. Inhalable, thoracic and respirable dust criteria of ACGIH, ISO and CEN, and PM10 criteria of US EPA
| Inhalable | Thoracic | Respirable | PM10 | ||||
| Particle aero- dynamic diameter (mm) |
Inhalable Particulate Mass (IPM) (%) |
Particle aero- dynamic diameter (mm) |
Thoracic Particulate Mass (TPM) (%) |
Particle aero- dynamic diameter (mm) |
Respirable Particulate Mass (RPM) (%) |
Particle aero- dynamic diameter (mm) |
Thoracic Particulate Mass (TPM) (%) |
| 0 | 100 | 0 | 100 | 0 | 100 | 0 | 100 |
| 1 | 97 | 2 | 94 | 1 | 97 | 2 | 94 |
| 2 | 94 | 4 | 89 | 2 | 91 | 4 | 89 |
| 5 | 87 | 6 | 80.5 | 3 | 74 | 6 | 81.2 |
| 10 | 77 | 8 | 67 | 4 | 50 | 8 | 69.7 |
| 20 | 65 | 10 | 50 | 5 | 30 | 10 | 55.1 |
| 30 | 58 | 12 | 35 | 6 | 17 | 12 | 37.1 |
| 40 | 54.5 | 14 | 23 | 7 | 9 | 14 | 15.9 |
| 50 | 52.5 | 16 | 15 | 8 | 5 | 16 | 0 |
| 100 | 50 | 18 | 9.5 | 10 | 1 | ||
| 20 | 6 | ||||||
| 25 | 2 | ||||||
The US Environmental Protection Agency (EPA 1987) standard for ambient air particle concentration is known as PM10, that is, particulate matter less than 10 mm in aerodynamic diameter. It has a sampler inlet criterion that is similar (functionally equivalent) to TPM but, as shown in Table 2, somewhat different numerical specifications.
Air Pollutants
Pollutants can be dispersed in air at normal ambient temperatures and pressures in gaseous, liquid and solid forms. The latter two represent suspensions of particles in air and were given the generic term aerosols by Gibbs (1924) on the basis of analogy to the term hydrosol, used to describe dispersed systems in water. Gases and vapours, which are present as discrete molecules, form true solutions in air. Particles consisting of moderate to high vapour pressure materials tend to evaporate rapidly, because those small enough to remain suspended in air for more than a few minutes (i.e., those smaller than about 10 mm) have large surface-to-volume ratios. Some materials with relatively low vapour pressures can have appreciable fractions in both vapour and aerosol forms simultaneously.
Gases and vapours
Once dispersed in air, contaminant gases and vapours generally form mixtures so dilute that their physical properties (such as density, viscosity, enthalpy and so on) are indistinguishable from those of clean air. Such mixtures may be considered to follow ideal gas law relationships. There is no practical difference between a gas and a vapour except that the latter is generally considered to be the gaseous phase of a substance that can exist as a solid or liquid at room temperature. While dispersed in air, all molecules of a given compound are essentially equivalent in their size and probabilities of capture by ambient surfaces, respiratory tract surfaces and contaminant collectors or samplers.
Aerosols
Aerosols, being dispersions of solid or liquid particles in air, have the very significant additional variable of particle size. Size affects particle motion and, hence, the probabilities of physical phenomena such as coagulation, dispersion, sedimentation, impaction onto surfaces, interfacial phenomena and light-scattering properties. It is not possible to characterize a given particle by a single size parameter. For example, a particle’s aerodynamic properties depend on density and shape as well as linear dimensions, and the effective size for light scattering is dependent on refractive index and shape.
In some special cases, all of the particles are essentially the same in size. Such aerosols are considered to be monodisperse. Examples are natural pollens and some laboratory-generated aerosols. More typically, aerosols are composed of particles of many different sizes and hence are called heterodisperse or polydisperse. Different aerosols have different degrees of size dispersion. It is, therefore, necessary to specify at least two parameters in characterizing aerosol size: a measure of central tendency, such as a mean or median, and a measure of dispersion, such as an arithmetic or geometric standard deviation.
Particles generated by a single source or process generally have diameters following a log-normal distribution; that is, the logarithms of their individual diameters have a Gaussian distribution. In this case, the measure of dispersion is the geometric standard deviation, which is the ratio of the 84.1 percentile size to the 50 percentile size. When more than one source of particles is significant, the resulting mixed aerosol will usually not follow a single log-normal distribution, and it may be necessary to describe it by the sum of several distributions.
Particle characteristics
There are many properties of particles other than their linear size that can greatly influence their airborne behaviour and their effects on the environment and health. These include:
Surface. For spherical particles, the surface varies as the square of the diameter. However, for an aerosol of given mass concentration, the total aerosol surface increases with decreasing particle size. For non-spherical or aggregate particles, and for particles with internal cracks or pores, the ratio of surface to volume can be much greater than for spheres.
Volume. Particle volume varies as the cube of the diameter; therefore, the few largest particles in an aerosol tend to dominate its volume (or mass) concentration.
Shape. A particle’s shape affects its aerodynamic drag as well as its surface area and therefore its motion and deposition probabilities.
Density. A particle’s velocity in response to gravitational or inertial forces increases as the square root of its density.
Aerodynamic diameter. The diameter of a unit-density sphere having the same terminal settling velocity as the particle under consideration is equal to its aerodynamic diameter. Terminal settling velocity is the equilibrium velocity of a particle that is falling under the influence of gravity and fluid resistance. Aerodynamic diameter is determined by the actual particle size, the particle density and an aerodynamic shape factor.
Types of aerosols
Aerosols are generally classified in terms of their processes of formation. Although the following classification is neither precise nor comprehensive, it is commonly used and accepted in the industrial hygiene and air pollution fields.
Dust. An aerosol formed by mechanical subdivision of bulk material into airborne fines having the same chemical composition. Dust particles are generally solid and irregular in shape and have diameters greater than 1 mm.
Fume. An aerosol of solid particles formed by condensation of vapours formed by combustion or sublimation at elevated temperatures. The primary particles are generally very small (less than 0.1 mm) and have spherical or characteristic crystalline shapes. They may be chemically identical to the parent material, or may be composed of an oxidation product such as metal oxide. Since they may be formed in high number concentrations, they often rapidly coagulate, forming aggregate clusters of low overall density.
Smoke. An aerosol formed by condensation of combustion products, generally of organic materials. The particles are generally liquid droplets with diameters less than 0.5 mm.
Mist. A droplet aerosol formed by mechanical shearing of a bulk liquid, for example, by atomization, nebulization, bubbling or spraying. The droplet size can cover a very large range, usually from about 2 mm to greater than 50 mm.
Fog. An aqueous aerosol formed by condensation of water vapour on atmospheric nuclei at high relative humidities. The droplet sizes are generally greater than 1 mm.
Smog. A popular term for a pollution aerosol derived from a combination of smoke and fog. It is now commonly used for any atmospheric pollution mixture.
Haze. A submicrometer-sized aerosol of hygroscopic particles that take up water vapour at relatively low relative humidities.
Aitken or condensation nuclei (CN). Very small atmospheric particles (mostly smaller than 0.1 mm) formed by combustion processes and by chemical conversion from gaseous precursors.
Accumulation mode. A term given to the particles in the ambient atmosphere ranging from 0.1 to about 1.0 mm in diameter. These particles generally are spherical (having liquid surfaces), and form by coagulation and condensation of smaller particles that derive from gaseous precursors. Being too large for rapid coagulation and too small for effective sedimentation, they tend to accumulate in the ambient air.
Coarse particle mode. Ambient air particles larger than about 2.5 mm in aerodynamic diameter and generally formed by mechanical processes and surface dust resuspension.
Biological Responses of the Respiratory System to Air Pollutants
Responses to air pollutants range from nuisance to tissue necrosis and death, from generalized systemic effects to highly specific attacks on single tissues. Host and environmental factors serve to modify the effects of inhaled chemicals, and the ultimate response is the result of their interaction. The main host factors are:
- age—for example, older people, especially those with chronically reduced cardiovascular and respiratory function, who may not be able to cope with additional pulmonary stresses
- state of health—for example, concurrent disease or dysfunction
- nutritional status
- immunological status
- sex and other genetic factors—for example, enzyme-related differences in biotransformation mechanisms, such as deficient metabolic pathways, and inability to synthesize certain detoxification enzymes
- psychological state—for example, stress, anxiety and
- cultural factors—for example, cigarette smoking, which may affect normal defences, or may potentiate the effect of other chemicals.
The environmental factors include the concentration, stability and physicochemical properties of the agent in the exposure environment and the duration, frequency and route of exposure. Acute and chronic exposures to a chemical may result in different pathological manifestations.
Any organ can respond in only a limited number of ways, and there are numerous diagnostic labels for the resultant diseases. The following sections discuss the broad types of responses of the respiratory system which may occur following exposure to environmental pollutants.
Irritant response
Irritants produce a pattern of generalized, non-specific tissue inflammation, and destruction may result at the area of contaminant contact. Some irritants produce no systemic effect because the irritant response is much greater than any systemic effect, while some also have significant systemic effects following absorption—for example, hydrogen sulphide absorbed via the lungs.
At high concentrations, irritants may cause a burning sensation in the nose and throat (and usually also in the eyes), pain in the chest and coughing producing inflammation of the mucosa (tracheitis, bronchitis). Examples of irritants are gases such as chlorine, fluorine, sulphur dioxide, phosgene and oxides of nitrogen; mists of acids or alkali; fumes of cadmium; dusts of zinc chloride and vanadium pentoxide. High concentrations of chemical irritants may also penetrate deep into the lungs and cause lung oedema (the alveoli are filled with liquid) or inflammation (chemical pneumonitis).
Highly elevated concentrations of dusts which have no chemical irritative properties can also mechanically irritate bronchi and, after entering the gastrointestinal tract, may also contribute to stomach and colon cancer.
Exposure to irritants may result in death if critical organs are severely damaged. On the other hand, the damage may be reversible, or it may result in permanent loss of some degree of function, such as impaired gas-exchange capacity.
Fibrotic response
A number of dusts lead to the development of a group of chronic lung disorders termed pneumoconioses. This general term encompasses many fibrotic conditions of the lung, that is, diseases characterized by scar formation in the interstitial connective tissue. Pneumoconioses are due to the inhalation and subsequent selective retention of certain dusts in the alveoli, from which they are subject to interstitial sequestration.
Pneumoconioses are characterized by specific fibrotic lesions, which differ in type and pattern according to the dust involved. For example, silicosis, due to the deposition of crystalline-free silica, is characterized by a nodular type of fibrosis, while a diffuse fibrosis is found in asbestosis, due to asbestos-fibre exposure. Certain dusts, such as iron oxide, produce only altered radiology (siderosis) with no functional impairment, while the effects of others range from a minimal disability to death.
Allergic response
Allergic responses involve the phenomenon known as sensitization. Initial exposure to an allergen results in the induction of antibody formation; subsequent exposure of the now “sensitized” individual results in an immune response—that is, an antibody-antigen reaction (the antigen is the allergen in combination with an endogenous protein). This immune reaction may occur immediately following exposure to the allergen, or it may be a delayed response.
The primary respiratory allergic reactions are bronchial asthma, reactions in the upper respiratory tract which involve the release of histamine or histamine-like mediators following immune reactions in the mucosa, and a type of pneumonitis (lung inflammation) known as extrinsic allergic alveolitis. In addition to these local reactions, a systemic allergic reaction (anaphylactic shock) may follow exposure to some chemical allergens.
Infectious response
Infectious agents can cause tuberculosis, anthrax, ornithosis, brucellosis, histoplasmosis, Legionnaires’ disease and so on.
Carcinogenic response
Cancer is a general term for a group of related diseases characterized by the uncontrolled growth of tissues. Its development is due to a complex process of interacting multiple factors in the host and the environment.
One of the great difficulties in attempting to relate exposure to a specific agent to cancer development in humans is the long latent period, typically from 15 to 40 years, between onset of exposure and disease manifestation.
Examples of air pollutants that can produce cancer of the lungs are arsenic and its compounds, chromates, silica, particles containing polycyclic aromatic hydrocarbons and certain nickel-bearing dusts. Asbestos fibres can cause bronchial cancer and mesothelioma of the pleura and peritoneum. Deposited radioactive particles may expose lung tissue to high local doses of ionizing radiation and be the cause of cancer.
Systemic response
Many environmental chemicals produce a generalized systemic disease due to their effects upon a number of target sites. Lungs are not only the target for many harmful agents but the site of entry of toxic substances which pass through the lungs into the bloodstream without any damage to the lungs. However, when distributed by the blood circulation to various organs, they can damage them or cause general poisoning and have systemic effects. This role of the lungs in occupational pathology is not the subject of this article. However, the effect of finely dispersed particulates (fumes) of several metal oxides which are often associated with an acute systemic syndrome known as metal fume fever should be mentioned.
The WHO Guidelines to Classification of Pesticides by Hazard (Present Acute Hazard continued)
Table 5. List of of technical products unlikely to present acute hazard in normal use (continued)
| Name | Status | Main use | Chemical type | Physical state | Route | LD50 (mg/kg) | Remarks |
|
Hexaconazole |
N(B) |
F |
S |
O |
2,180 |
||
|
Hexaflumuron |
ISO |
I |
S |
O |
+5,000 |
||
|
Hexythiazox |
N(B) |
AC |
S |
O |
+5,000 |
||
|
Hydroprene |
N(A) |
IGR |
L |
O |
+10,000 |
||
|
2-Hydroxyethyl octyl sulphide |
C |
RP (insect) |
L |
O |
8,530 |
||
|
Hydroxyisoxazole |
N(J) |
See hymexazol |
|||||
|
Hymexazol |
N(B) |
FST |
S |
O |
3,900 |
||
|
Imazamethabenz-methyl |
(ISO) |
H |
S |
O |
+5,000 |
||
|
Imazapyr |
ISO |
H |
S |
O |
+5,000 |
Irritant to eyes |
|
|
Imazaquin |
ISO |
H |
S |
O |
+5,000 |
||
|
Imazethapyr |
N(B) |
H |
S |
O |
+5,000 |
||
|
Imibenconazole |
ISO |
F |
S |
O |
+5,000 |
||
|
Inabenfide |
ISO |
PGR |
S |
O |
+10,000 |
||
|
Iodofenphos |
N(A,B) |
See jodfenphos |
|||||
|
Iprodione |
ISO |
F |
S |
O |
3,500 |
||
|
Isopropalin |
ISO |
H |
L |
O |
+5,000 |
||
|
Isoxaben |
N(B) |
H |
S |
O |
+10,000 |
||
|
Jodfenphos |
ISO |
I |
OP |
S |
O |
2,100 |
DS 43 |
|
Karbutilate |
ISO |
H |
S |
O |
3,000 |
||
|
Kasugamycin |
N(J) |
F |
S |
O |
+10,000 |
||
|
Kinoprene |
ISO |
IGR |
S |
O |
4,900 |
||
|
Lenacil |
ISO |
H |
S |
O |
+10,000 |
||
|
Linuron |
ISO |
H |
S |
O |
4,000 |
||
|
Maleic hydrazide |
ISO |
PGR |
S |
O |
6,950 |
||
|
Mancozeb |
ISO |
F |
TC |
S |
O |
+8,000 |
Irritant to skin on multiple exposure; DS 94 |
|
Maneb |
ISO |
F |
TC |
S |
O |
6,750 |
Irritant to skin on multiple exposure; DS 94 |
|
Mefenacet |
ISO |
H |
S |
O |
+5,000 |
||
|
Mepanipyrim |
ISO |
F |
S |
O |
+5,000 |
||
|
Mepronil |
N(J) |
F |
S |
O |
+10,000 |
||
|
Metamitron |
ISO |
H |
S |
O |
3,343 |
||
|
Metazachlor |
ISO |
H |
S |
O |
2,150 |
||
|
Methabenzthiazuron |
ISO |
H |
S |
O |
+2,500 |
||
|
Methoprene |
ISO |
IGR |
L |
O |
+10,000 |
DS 47 |
|
|
Methoprotryne |
ISO |
H |
S |
O |
+5,000 |
||
|
Methoxychlor |
ISO |
I |
OC |
S |
O |
6,000 |
DS 28 |
|
Methoxyphenone |
N(J) |
H |
S |
O |
+4,000 |
||
|
Methyldymron |
N(J) |
H |
S |
O |
3,948 |
||
|
Metiram |
N(J) |
F |
S |
O |
+10,000 |
||
|
Metobromuron |
ISO |
H |
S |
O |
2,500 |
||
|
Metosulam |
ISO |
H |
S |
O |
+5,000 |
||
|
Metoxuron |
ISO |
H |
S |
O |
+3,200 |
||
|
Metribuzin |
ISO |
H |
T |
S |
O |
2,200 |
|
|
Metsulfovax |
ISO |
F |
S |
O |
3,929 |
||
|
Metsulfuron |
N(A,B) |
H |
S |
O |
+5,000 |
||
|
Monalide |
ISO |
H |
S |
O |
+4,000 |
||
|
Monolinuron |
ISO |
H |
S |
O |
2,250 |
||
|
Monuron |
ISO |
H |
S |
O |
3,600 |
||
|
Monuron-TCA |
N(A) |
H |
S |
O |
3,700 |
||
|
Naphthalene |
C |
F |
S |
O |
2,200 |
||
|
Naphthalic anhydride |
C |
PGR |
S |
O |
+10,000 |
||
|
2-(1-naphthyl) acetamide |
ISO |
PGR |
S |
O |
6,400 |
||
|
1-naphthylacetic acid |
ISO |
PGR |
S |
O |
c3,000 |
||
|
Napropamide |
ISO |
H |
S |
O |
5,000 |
||
|
Naptalam |
ISO |
PGR |
S |
O |
8,200 |
||
|
Neburon |
ISO |
H |
S |
O |
+10,000 |
||
|
Niclosamide |
ISO |
M |
S |
O |
5,000 |
DS 63 |
|
|
Nicosulfuron |
ISO |
H |
S |
O |
+5,000 |
Irritant to eyes |
|
|
Nitralin |
ISO |
H |
S |
O |
+2,000 |
||
|
Nitrothal-isopropyl |
ISO |
F |
S |
O |
6,400 |
||
|
Norflurazon |
ISO |
H |
S |
O |
+8,000 |
||
|
(octylthio)ethanol |
C |
See 2-hydroxyethyl octyl sulphide |
|||||
|
Ofurace |
ISO |
F |
S |
O |
2,600 |
||
|
Oryzalin |
ISO |
H |
S |
O |
+10,000 |
||
|
Oxabetrinil |
ISO |
H |
S |
O |
+5,000 |
||
|
Oxadiazon |
ISO |
H |
S |
O |
+8,000 |
||
|
Oxine copper |
ISO |
F |
S |
O |
10,000 |
||
|
Oxycarboxin |
ISO |
F |
S |
O |
2,000 |
||
|
Oxyfluorfen |
ISO |
H |
S |
O |
+5,000 |
||
|
Penconazole |
N(B) |
F |
S |
O |
2,120 |
||
|
Pencycuron |
ISO |
F |
S |
O |
+5,000 |
||
|
Pentanochlor |
ISO |
H |
S |
O |
+10,000 |
||
|
Phenisobromolate |
N(J) |
See bromopropylate |
|||||
|
Phenisopham |
ISO |
H |
S |
O |
+4,000 |
||
|
Phenmedipham |
ISO |
H |
S |
O |
+8,000 |
||
|
Phenothrin |
ISO |
I |
PY |
L |
O |
+5,000 |
DS 85; EHC 96; HSG 32 |
|
2-Phenylphenol |
ISO |
F |
S |
O |
2,480 |
||
|
Phosdiphen |
N(J) |
F |
L |
O |
6,200 |
||
|
Phthalide |
N(J) |
F |
S |
O |
+10,000 |
||
|
Picloram |
ISO |
H |
S |
O |
8,200 |
||
|
Piperonyl butoxide |
N(A) |
SY |
oil |
O |
+7,500 |
||
|
Pretilachlor |
ISO |
H |
L |
O |
6,100 |
||
|
Primisulfuron |
ISO |
H |
S |
O |
+5,050 |
||
|
Probenazole |
N(J) |
F |
S |
O |
2,030 |
||
|
Procymidone |
ISO |
F |
S |
O |
6,800 |
||
|
Prodiamine |
ISO |
H |
S |
O |
+5,000 |
||
|
Profluralin |
ISO |
H |
S |
O |
c10,000 |
||
|
Proglinazine |
ISO |
H |
S |
O |
+8,000 |
||
|
Prometon |
ISO |
H |
T |
S |
O |
2,980 |
|
|
Prometryn |
ISO |
H |
T |
S |
O |
3,150 |
|
|
Pronamide |
N(A) |
See propyzamide |
|||||
|
Propamocarb |
ISO |
F |
S |
O |
8,600 |
||
|
Propaquizafop |
ISO |
H |
S |
O |
+5,000 |
||
|
Propazine |
ISO |
H |
T |
S |
O |
+5,000 |
|
|
Propham |
ISO |
H |
S |
O |
5,000 |
||
|
Propineb |
ISO |
H |
TC |
S |
O |
8,500 |
|
|
Propyzamide |
ISO |
H |
S |
O |
5,620 |
||
|
Pyracarbolid |
ISO |
F |
S |
O |
+10,000 |
||
|
Pyrazolynate |
ISO |
H |
S |
O |
9,550 |
||
|
Pyrazon |
N(A) |
See chloridazon |
|||||
|
Pyrazosulfuron |
ISO |
H |
S |
O |
+5,000 |
||
|
Pyrimethanil |
ISO |
F |
S |
O |
4,150 |
||
|
Pyriminobac |
ISO |
H |
S |
O |
+5,000 |
||
|
Pyriproxyfen |
N(B) |
I |
S |
O |
+5,000 |
||
|
Quinclorac |
ISO |
H |
S |
O |
2,680 |
||
|
Quinmerac |
ISO |
H |
S |
O |
+5,000 |
||
|
Quinomethinoate |
N(B) |
See chinomethionat |
|||||
|
Quinonamid |
ISO |
F |
S |
O |
+10,000 |
||
|
Quintozene |
ISO |
F |
S |
O |
+10,000 |
EHC 41 |
|
|
Rimsulfuron |
C |
H |
S |
O |
+5,000 |
||
|
Secbumeton |
ISO |
H |
T |
S |
O |
2,680 |
|
|
Siduron |
ISO |
H |
S |
O |
+7,500 |
||
|
Simazine |
ISO |
H |
T |
S |
O |
+5,000 |
|
|
Sodium metaborate |
C |
See borax |
|||||
|
Sodium trichloracetate |
The data shown refer to sodium trichloroacetic acid. In many countries, the term TCA refers to the free acid (now accepted by ISO): this is a solid with an oral LD50 of 400 mg/kg and if used as a pesticide is placed in Class II. It is highly corrosive to skin |
||||||
|
Solan |
N(A) |
See pentanochlor |
|||||
|
Stirofos |
N(A) |
See tetrachlorvinphos |
|||||
|
Sulfometuron |
N(B) |
H |
S |
O |
+5,000 |
||
|
Sulfur |
N(A,J) |
See sulphur |
|||||
|
Sulphur |
ISO |
F,I |
S |
O |
+3,000 |
Irritant to skin and mucous membranes. Sulphur dust can spontaneously ignite unless diluted about 50% with inert material |
|
|
TCA |
ISO |
H |
S |
O |
3,200 |
Irritant to skin and eyes; see sodium trichloracetate |
|
|
Tebuconazole |
ISO |
F |
S |
O |
4,000 |
||
|
Tebutam |
ISO |
H |
oil |
O |
6,210 |
||
|
Tecnazene |
ISO |
F |
S |
O |
+10,000 |
EHC 42; HSG 12 |
|
|
Tedion |
N(U) |
See tetradifon |
|||||
|
Teflubenzuron |
N(B) |
I |
S |
O |
+5,000 |
||
|
Temephos |
ISO |
I |
OP |
L |
O |
8,600 |
DS 8 |
|
Terbacil |
ISO |
H |
S |
O |
+5,000 |
||
|
Terbuthylazine |
ISO |
H |
T |
S |
O |
2,160 |
|
|
Terbutryn |
ISO |
H |
T |
S |
O |
2,400 |
|
|
Tetrachlorvinphos |
ISO |
I |
OP |
S |
O |
4,000 |
|
|
Tetradifon |
ISO |
AC |
S |
O |
+10,000 |
EHC 67; HSG 11 |
|
|
Tetramethrin |
ISO |
O |
PY |
S |
O |
+5,000 |
EHC 98; HSG 31 |
|
Tetrasul |
ISO |
AC |
S |
O |
6,810 |
||
|
Thiabendazole |
ISO |
F |
S |
O |
3,330 |
||
|
Thidiazuron |
ISO |
PGR |
S |
O |
+4,000 |
||
|
Thifensulfuron |
N(B) |
H |
S |
O |
+5,000 |
||
|
Thiophanate |
ISO |
F |
S |
O |
+10,000 |
||
|
Thiophanate-methyl |
ISO |
F |
S |
O |
+6,000 |
||
|
Tiocarbazil |
ISO |
H |
TC |
L |
O |
10,000 |
|
|
Tolclofos-methyl |
ISO |
F-S |
S |
O |
c5,000 |
||
|
Tolyfluanid |
ISO |
F |
S |
O |
+5,000 |
||
|
Transfluthrin |
ISO |
I |
PY |
S |
O |
+5,000 |
|
|
Triasulfuron |
ISO |
H |
S |
O |
+5,000 |
||
|
Tribenuron |
N(B) |
H |
S |
O |
+5,000 |
||
|
Trichlamide |
ISO |
F |
S |
O |
+5,000 |
||
|
Trietazine |
ISO |
H |
T |
S |
O |
2,830 |
|
|
Trifluralin |
ISO |
H |
S |
O |
+10,000 |
||
|
Triflumuron |
ISO |
PGR |
S |
O |
+5,000 |
||
|
Triforine |
ISO |
F |
S |
O |
+6,000 |
||
|
Triticonazole |
N(B) |
F |
triazole |
S |
O |
+2,000 |
|
|
Validamycin |
N(J) |
F |
S |
O |
+10,000 |
||
|
Vinclozolin |
ISO |
F |
S |
O |
10,000 |
||
|
Zineb |
ISO |
F |
S |
O |
+5,000 |
DS 94 |
Source: WHO 1996.
The WHO Guidelines to Classification of Pesticides by Hazard (Unlikely to Present Acute Hazard)
Table 5. List of technical products unlikely to present acute hazard in normal use
|
Name |
Status |
Main use |
Chemical type |
Physical state |
Route |
LD50 (mg/kg) |
Remarks |
|
Aclonifen |
N(B) |
H |
S |
O |
+5,000 |
||
|
Acrinathrin |
ISO |
MT |
S |
O |
+5,000 |
||
|
Alloxydim |
ISO |
H |
S |
O |
2,260 |
||
|
Aminotriazole |
N(F) |
See amitrole |
|||||
|
Amitrole |
ISO |
H |
T |
S |
O |
5,000 |
EHC 158, DS 79; HSG 85 |
|
Ammonium sulfamate |
ISO |
H |
S |
O |
3,900 |
||
|
Ancymidol |
ISO |
PGR |
S |
O |
4,500 |
||
|
Anilazine |
ISO |
F |
T |
S |
O |
2,710 |
Irritant to eyes and skin |
|
Anthraquinone |
ISO |
RP (birds) |
S |
O |
+5,000 |
||
|
Asulam |
ISO |
H |
TC |
S |
O |
+4,000 |
|
|
Atrazine |
ISO |
H |
T |
S |
O |
c2,000 |
DS 82; HSG 47 |
|
Aziprotryne |
ISO |
H |
T |
S |
O |
3,600 |
|
|
Benalaxyl |
ISO |
F |
S |
O |
c4,200 |
||
|
Benazolin |
ISO |
H |
S |
O |
3,200 |
Irritant to skin and eyes |
|
|
Benefin |
N(A) |
See benfluralin |
|||||
|
Benfluralin |
ISO |
H |
S |
O |
+10,000 |
||
|
Benfuresate |
ISO |
H |
S |
O |
2,031 |
||
|
Benomyl |
ISO |
F |
TC |
S |
O |
+10,000 |
EHC 148, DS 87; HSG 81 |
|
Benoxacor |
ISO |
H |
S |
O |
+5,000 |
||
|
Bensulfuron |
N(B) |
H |
S |
O |
+5,000 |
||
|
Benthrodine |
N(J) |
See benfluralin |
|||||
|
Benzamizole |
See isoxaben |
||||||
|
Benzoximate |
ISO |
AC |
S |
O |
+10,000 |
||
|
Bifenox |
ISO |
H |
S |
O |
+6,400 |
||
|
Bioresmethrin |
ISO |
I |
PY |
L |
O |
+7,000 |
DS 34 |
|
Biphenyl |
ISO |
F |
S |
O |
3,280 |
||
|
Bispyribac |
ISO |
H |
S |
O |
2,635 |
||
|
Bitertanol |
ISO |
F |
S |
O |
+5,000 |
||
|
Borax |
ISO |
F |
S |
O |
4,500 |
||
|
Bromacil |
ISO |
H |
S |
O |
5,200 |
||
|
Bromobutide |
ISO |
H |
S |
O |
+5,000 |
||
|
Bromocyclen |
ISO |
I,AC |
S |
O |
+10,000 |
||
|
Bromopropylate |
ISO |
AC |
S |
O |
+5,000 |
||
|
Bupirimate |
ISO |
F |
S |
O |
c4,000 |
||
|
Buprofezin |
ISO |
I |
S |
O |
2,200 |
||
|
Butachlor |
ISO |
H |
L |
O |
3,300 |
||
|
Buthiobate |
ISO |
F |
L |
O |
3,200 |
||
|
Butopyronoxyl |
N(A) |
RP (insects) |
L |
O |
7,840 |
||
|
Butralin |
ISO |
H |
S |
O |
+10,000 |
||
|
Buturon |
ISO |
H |
S |
O |
3,000 |
||
|
Butylate |
ISO |
F |
TC |
L |
O |
+4,000 |
|
|
Captan |
ISO |
F |
S |
O |
9,000 |
Irritant to skin; DS 9; HSG 50 |
|
|
Carbendazim |
ISO |
F |
S |
O |
+10,000 |
DS 89; EHC 149; HSG 82 |
|
|
Carbetamide |
ISO |
H |
S |
O |
+10,000 |
||
|
Carboxin |
ISO |
FST |
S |
O |
3,820 |
||
|
Chinomethionat |
ISO |
AC,F |
S |
O |
2,500 |
||
|
Chlomethoxyfen |
N(B) |
H |
S |
O |
+10,000 |
||
|
Chloramben |
ISO |
H |
S |
O |
5,620 |
||
|
Chlorbromuron |
ISO |
H |
S |
O |
+5,000 |
||
|
Chlorbufam |
ISO |
H |
S |
O |
2,500 |
||
|
Chlorfenidim |
N(U) |
See monuron |
|||||
|
Chlorfluazuron |
ISO |
IGR |
S |
O |
8,500 |
||
|
Chlorflurecol |
N(B) |
See chlorflurenol |
|||||
|
Chlorflurenol |
ISO |
PGR |
OC |
S |
O |
+10,000 |
|
|
Chloridazon |
ISO |
H |
S |
O |
2,420 |
||
|
Chlorimuron |
N(B) |
H |
S |
O |
4,102 |
||
|
Chlornitrofen |
ISO |
H |
S |
O |
+10,000 |
||
|
Chloromethiuron |
ISO |
Ix |
S |
O |
2,500 |
||
|
Chloroneb |
ISO |
H |
OC |
S |
O |
+10,000 |
|
|
Chloropropylate |
ISO |
AC |
OC |
S |
O |
+5,000 |
|
|
Chlorothalonil |
ISO |
F |
S |
O |
+10,000 |
||
|
Chlorotoluron |
ISO |
H |
S |
O |
+10,000 |
||
|
Chloroxifenidim |
N(U) |
See chloroxuron |
|||||
|
Chloroxuron |
ISO |
H |
S |
O |
+3,000 |
||
|
Chlorphoxim |
ISO |
I |
OP |
S |
O |
+2,500 |
DS 32 |
|
Chlorpropham |
ISO |
H |
S |
O |
+5,000 |
||
|
Chlorpyrifos methyl |
ISO |
I |
OP |
L |
O |
+3,000 |
DS 33 |
|
Chlorsulfuron |
ISO |
H |
S |
O |
5,545 |
||
|
Chlorthal-dimethyl |
ISO |
H |
S |
O |
+3,000 |
||
|
Chlozolinate |
N(B) |
F |
S |
O |
+4,000 |
||
|
Cinmethylin |
ISO |
H |
L |
O |
3,960 |
||
|
Cinosulfuron |
ISO |
H |
S |
O |
+5,000 |
||
|
Clofentezine |
N(B) |
AC |
S |
O |
+5,200 |
||
|
Clomeprop |
ISO |
H |
S |
O |
+5,000 |
||
|
Clonitralide |
N(A) |
See niclosamide |
|||||
|
Clopyralid |
N(B) |
H |
S |
O |
4,300 |
Severe irritant to eyes |
|
|
Cloxyfonac |
ISO |
PGR |
S |
O |
+5,000 |
||
|
CNA |
N(J) |
See dicloran |
|||||
|
COMU |
N(J) |
See cycluron |
|||||
|
Credazine |
N(J) |
H |
S |
O |
3,090 |
||
|
Cryolite |
C |
I |
S |
O |
+10,000 |
||
|
Cycloprothrin |
ISO |
I |
PY |
L |
O |
+5,000 |
|
|
Cycloxydim |
N(B) |
H |
S |
O |
3,900 |
||
|
Cycluron |
ISO |
H |
S |
O |
2,600 |
||
|
Cyometrinil |
N(B) |
H |
S |
O |
2,277 |
||
|
Cyromazine |
ISO |
L |
S |
O |
3,300 |
||
|
Caimuron |
ISO |
H |
S |
O |
+5,000 |
||
|
Dalapon |
N(A,B,F) |
H |
S |
O |
9,330 |
||
|
Daminozide |
ISO |
H |
S |
O |
8,400 |
||
|
Desmedipham |
ISO |
H |
S |
O |
+9,600 |
||
|
Diafenthiuron |
ISO |
AC |
S |
O |
2,068 |
||
|
Dichlobenil |
ISO |
H |
S |
O |
3,160 |
||
|
Dichlorfenidim |
N(U) |
See diuron |
|||||
|
Dichlofluanid |
ISO |
F |
S |
O |
+5,000 |
||
|
Dichloropicolinic acid |
See clopyralid |
||||||
|
Diclobutrazol |
ISO |
F |
T |
S |
O |
+4,000 |
|
|
Diclomezine |
ISO |
F |
S |
O |
+10,000 |
||
|
Dicloran |
N(B) |
F |
S |
O |
4,000 |
||
|
Diethatyl |
ISO |
H |
S |
O |
2,300 |
||
|
Diethofencarb |
ISO |
F |
S |
O |
+5,000 |
||
|
Difenoxuron |
ISO |
H |
S |
O |
+7,750 |
||
|
Diflubenzuron |
ISO |
L |
S |
O |
+4,640 |
DS 77 |
|
|
Diflufenican |
N(B) |
H |
S |
O |
+2,000 |
||
|
Dikegulac |
ISO |
PGR |
S |
O |
+10,000 |
||
|
Dimefuron |
ISO |
H |
S |
O |
+2,000 |
||
|
Dimethirimol |
ISO |
F |
S |
O |
2,350 |
||
|
Dimethomorph |
ISO |
F |
S |
O |
+5,000 |
||
|
Dimethyl phthalate |
C |
RP (insect) |
L |
O |
8,200 |
||
|
Dinitramine |
ISO |
H |
S |
O |
3,000 |
||
|
Diphenyl |
See biphenyl |
||||||
|
Dipropetryn |
ISO |
H |
T |
S |
O |
4,050 |
|
|
Dipropyl isocinchomerate |
C |
RP (fly) |
L |
O |
5,230 |
||
|
Disodium octaborate |
See borax |
||||||
|
Ditalmifos |
ISO |
F |
OP |
S |
O |
5,660 |
Irritant to skin; allergenic |
|
Dithiopyr |
ISO |
H |
O |
+5,000 |
|||
|
Diuron |
ISO |
H |
S |
O |
3,400 |
||
|
Dodemorph |
ISO |
H |
L |
O |
4,500 |
||
|
Eglinazine |
ISO |
H |
S |
O |
+10,000 |
||
|
Ethalfluralin |
ISO |
H |
S |
O |
+10,000 |
||
|
Ethephon |
N(A) |
PGR |
S |
O |
+4,000 |
||
|
Ethidimuron |
ISO |
H |
S |
O |
+5,000 |
||
|
Ethirimol |
ISO |
FST |
S |
O |
6,340 |
||
|
Ethofumesate |
ISO |
H |
S |
O |
+6,400 |
||
|
Etofenprox |
N(B) |
I |
S |
O |
+10,000 |
||
|
Fenarimol |
ISO |
F |
S |
O |
2,500 |
||
|
Fenbutatin oxide |
ISO |
MT |
OT |
S |
O |
2,630 |
EHC 15 |
|
Fenchlorazole |
ISO |
H |
S |
O |
+5,000 |
||
|
Fenclorim |
ISO |
H |
S |
O |
+5,000 |
||
|
Fenfuram |
ISO |
FST |
S |
O |
+10,000 |
||
|
Fenidim |
N(U) |
See fenuron |
|||||
|
Fenitropan |
ISO |
F |
S |
O |
3,230 |
||
|
Fenoxaprop-ethyl |
N(B) |
H |
S |
O |
2,350 |
||
|
Fenoxycarb |
ISO |
I |
C |
S |
O |
+10,000 |
|
|
Fenpiclonil |
ISO |
FST |
S |
O |
+5,000 |
||
|
Fenpropimorph |
ISO |
F |
oil |
O |
3,515 |
||
|
Fenuron |
ISO |
H |
S |
O |
6,400 |
||
|
Fenuron-TCA |
(ISO) |
H |
S |
O |
4,000 |
||
|
Ferbam |
ISO |
F |
TC |
S |
O |
+10,000 |
|
|
Flamprop-M |
ISO |
H |
S |
O |
+3,000 |
||
|
Fluazifop |
ISO |
H |
P |
L |
O |
3,330 |
|
|
Flubenzimine |
ISO |
AC |
S |
O |
3,000 |
||
|
Flucycloxuron |
ISO |
AC |
S |
O |
+5,000 |
||
|
Flufenoxuron |
ISO |
I |
S |
O |
+3,000 |
||
|
Flumetralin |
N(B) |
PGR |
S |
O |
+5,000 |
||
|
Flumetsulam |
ISO |
H |
S |
O |
+5,000 |
||
|
Fluometuron |
ISO |
H |
S |
O |
+8,000 |
||
|
Fluorodifen |
ISO |
H |
S |
O |
9,000 |
||
|
Fluoromide |
N(J) |
F |
S |
O |
+10,000 |
||
|
Flupropanate |
ISO |
H |
S |
O |
+10,000 |
||
|
Flurecol butyl |
See flurenol |
||||||
|
Flurenol |
ISO |
PGR |
S |
O |
+5,000 |
||
|
Fluridone |
ISO |
H |
S |
O |
+10,000 |
||
|
Flurochloridone |
ISO |
H |
S |
O |
4,000 |
||
|
Fluthiacet |
ISO |
H |
S |
O |
+5,000 |
||
|
Fluroxypyr |
N(B) |
H |
S |
O |
+5,000 |
||
|
Fluthiacet |
ISO |
H |
S |
O |
+5,000 |
||
|
Flutolanil |
ISO |
F |
S |
O |
+10,000 |
||
|
Tau-fluvalinate |
ISO |
I |
PY |
oil |
O |
+3,000 |
Skin and eye irritant |
|
Folpet |
ISO |
F |
S |
O |
+10,000 |
HSG 72 |
|
|
Fosamine |
ISO |
H |
S |
O |
2,400 |
||
|
Fosetyl |
N(B) |
F |
S |
O |
5,800 |
||
|
Furmecyclox |
N(B) |
FST |
S |
O |
3,780 |
||
|
Gibberellic acid |
N(B) |
PGR |
S |
O |
+10,000 |
||
|
Glyphosate |
ISO |
H |
S |
O |
4,230 |
EHC 159, DS 91 |
|
|
Glyphosine |
ISO |
H |
S |
O |
3,920 |
Continues on next page.
The WHO Guidelines to Classification of Pesticides by Hazard (Obsolete or Discontinued)
Table 6. Technical products not included in the WHO Classification and believed to be obsolete or discontinued for use as pesticides
|
Allyxycarb |
Dinex |
Methacarbate |
Table 7. List of gaseous or volatile fumigants not classified under the WHO Recommended Classification of Pesticides by Hazard
|
Acrylonitrile (EHC 28; HSG 1) |
Ethylene dichloride (EHC 176) |
Note: The WHO Classification does not set out any criteria for air concentrations on which classification could be based. Most of these compounds are of high hazard and recommended exposure limits for occupational exposure have been adopted by national authorities in many countries.
Source: WHO 1996.
The entries and abbrevations used in the tables’ various columns are explained here under the corresponding heading.
Name
The first column in the tables list the approved name of active ingredients. Trade names are not listed since there are many of these.
Status
The following abbreviations are used:
- ISO: Indicates the common name approved by the International Organization for Standardization (ISO). Such names are, when available, preferred by the WHO to all other common names. However, some of these names may not be acceptable for national use in some countries. If the letters ISO appear within parentheses (e.g., with fentin acetate), this indicates that ISO has standardized (or is in the process of standardizing) the name of the base, but not the name of the derivative listed in the “Name” column. (Fentin is an ISO name, but fentin acetate is not.)
- N( ): Indicates approval by a national ministry or other body, which is shown in parentheses as follows: A: United States Environmental Protection Agency (EPA), American National Standards Institute (ANSI), the Weed Science Society of America or the Entomological Society of America; B: British Standards Institution or the British Pharmacopoeia Commission; F: Association française de normalisation; J: Japanese Ministry of Agriculture and Forestry; U: Gosudarstvennyi Komitet Standartov, former USSR.
- C: Chemical, trivial or other common name.
Main use
In most cases only a single use is given. This is only for identification purposes and does not exclude other uses. The following abbreviations are used:
- AC: acaricide
- AP: aphicide
- B: bacteriostat (soil)
- FM: fumigant
- F: fungicide, other than for seed treatment
- FST: fungicide, for seed treatment
- H: herbicide
- I: insecticide
- IGR: insect growth regulator
- Ix: ixodicide (for tick control)
- L: larvicide
- M: molluscicide
- N: nematocide
- O: other use for plant pathogens
- PGR: plant growth regulator
- R: rodenticide
- RP( ): repellent (species)
- -S: applied to soil; not used with herbicides or PGRs
- SY: synergist.
Chemical type
A limited number of chemical types are shown in this column. Most have some significance in the sense that they may have a common antidote or may be confused in the nomenclature with other chemical types. For example, thiocarbamates are not cholinesterase inhibitors and do not have the same effects as carbamates. The following abbreviations are used:
- C: carbamate
- CNP: chloronitrophenol derivative
- OC: organochlorine compound
- OM: organomercury compound
- OP: organophosphorus compound
- OT: organotin compound
- P: pyridyl derivative
- PA: phenoxyacetic acid derivative
- PY: pyrethroid
- T: triazine derivative
- TC: thiocarbamate.
These chemical classification are included only for convenience and do not represent a recommendation on the part of the WHO as to the way in which pesticides should be classified. It should, furthermore, be understood that some pesticides may fall into more than one type.
Chemical type is not shown where it is apparent from the name.
Physical state
This refers only to the technical compound. The following are used:
- L: liquid, including solids with a melting point below 50C
- oil: oily liquid; refers to physical state only
- S: solid, includes waxes.
It may happen in a few cases that where the technical product is a solid, highly concentrated liquid formulations may need to be classified in a more hazardous class. In most cases, oils have been classified as liquids unless very viscous at ordinary temperatures.
Route
Oral route values are used unless the dermal route values place the compound in a hazardous class or the dermal values are significantly lower than the oral values, although in the same class. The following abbreviations are used:
- D: dermal
- O: oral.
LD50 (mg/kg)
The LD50 value is a statistical estimate of the number of mg of toxicant per kg of body weight required to kill 50% of a large population of test animals; the rat is used unless otherwise states. A single value is given: “c” preceding the value indicates that it is a value within a wider than usual range, adopted for classification purposes; “+” preceding the value indicates that the kill at the stated dose was less than 50% of the test animals.
The toxicity data for pyrethroids are highly variable according to isomer ratios, the vehicle for oral administration and the husbandry of the test animals. The variability is reflected in the prefix “c”. The single LD50 value now chosen for classification purposes is based on administration in corn oil and is much lower than that in aqueous solutions. This has resulted in considerable changes in the classification of some products and also underlines the need for classification by formulation if labelling is to reflect true hazard.
The figures in this column are not median values; rather, a safety margin is incorporated by choosing the lower confidence limit in most cases. Where a sex difference occurs in LD50 values, the value for the more sensitive sex is used. A number of classification adjustments have been made in respect of some pesticides and these are explained. A borderline case has been classified in the more or less hazardous class after consideration of its toxicology and use experience.
In table 5, a number of pesticides are listed as unlikely to present any acute hazard in normal use. The WHO Classification is open-ended but it is clear that there must be a point at which the acute hazard posed by the use of these compounds is so low as to be negligible provided that the necessary precautions are taken. For the purposes of this table, it has been assumed that this point is an oral LD50 of 2,000 mg/kg for solids and 3,000 mg/kg for liquids. However, it should not be overlooked that in formulations of these technical products, solvents or vehicles may present a greater hazard than the actual pesticide and therefore classification of a formulation in one of the higher hazard classes may be necessary.
Biological pesticides are not included in the WHO Classification because the methods of the safety testing of live biological agents are not appropriate to classification procedures applied to chemical compounds.
Remarks
Where the classification of a technical product has been adjusted, the basis for this is indicated in this column. Major irritant properties are noted; these do not affect classification. Where the name of a technical product is cross-referenced, the referenced product will be found in the same table. Abbreviations are used to indicate that a WHO/FAO Data Sheet (DS) or an issue of International Programme on Chemical Safety (IPCS) Environmental Health Criteria (EHC) Series or Health and Safety Guide contains further information on the product; the relevant issue numbers follow the abbreviations.
The WHO Guidelines to Classification of Pesticides by Hazard (Slightly Hazardous)
Table 4. List of technical products classified in Class III: "Slightly hazardous"
|
Name |
Status |
Main use |
Chemical type |
Physical state |
Route |
LD50 (mg/kg) |
Remarks |
|
Acephate |
ISO |
I |
OP |
S |
O |
945 |
|
|
Acetochlor |
ISO |
H |
L |
O |
2,950 |
||
|
Acifluorfen |
ISO |
H |
S |
O |
1,370 |
Strong irritant to eyes |
|
|
Allethrin |
ISO |
I |
PY |
oil |
O |
c685 |
EHC 87; HSG 24 |
|
Ametryn |
ISO |
H |
T |
S |
O |
1,110 |
|
|
Amitraz |
ISO |
AC |
S |
O |
800 |
||
|
Azamethiphos |
ISO |
I |
OP |
S |
O |
1,010 |
|
|
Azidithion |
N(F) |
See menazon |
|||||
|
Barban |
ISO |
H |
S |
O |
1,300 |
||
|
Bensultap |
ISO |
I |
S |
O |
1,100 |
||
|
Bentazone |
ISO |
H |
S |
O |
1,100 |
||
|
Benzoylprop-ethyl |
(ISO) |
H |
S |
O |
1,555 |
||
|
Benzthiazuron |
ISO |
H |
S |
O |
1,280 |
||
|
Bromofenoxim |
ISO |
H |
S |
O |
1,217 |
||
|
Bromophos |
ISO |
I |
OP |
S |
O |
c1,600 |
DS 76 |
|
Buthidazole |
ISO |
H |
S |
O |
1,480 |
||
|
Cacodylic acid |
See dimethylarsinic acid |
||||||
|
Carbofos |
N(U) |
See malathion |
|||||
|
Chlorfenac |
ISO |
H |
OC |
S |
O |
575 |
|
|
Chlorfenethol |
ISO |
AC |
OC |
S |
O |
930 |
|
|
Chlorfenson |
ISO |
AC |
OC |
S |
O |
c2,000 |
Irritant to skin |
|
Chlorinat |
N(U) |
See barban |
|||||
|
Chlormequat (chloride) |
ISO |
PGR |
S |
O |
670 |
||
|
Chloroacetic acid |
C |
H |
S |
O |
650 |
Irritant to skin and eyes; data refer to sodium salt |
|
|
Chlorobenzilate |
ISO |
AC |
OC |
S |
O |
700 |
|
|
Chlorocholine chloride |
C |
See chlormequat |
|||||
|
Chlorthiamid |
ISO |
H |
S |
O |
757 |
||
|
Cismethrin |
ISO |
Resmethrin is a mixture of isomers, the trans isomer (70-80%) being also known as bioresmethrin and the cis isomer (20-30%) as cismethrin. Bioresmethrin (see table 62.5) alone is of much lower toxicity (oral LD50 9,000 mg/kg) (DS 34) |
|||||
|
Citrex |
N(U) |
See dodine |
|||||
|
Clofop |
ISO |
H |
L |
O |
1,208 |
||
|
Copper hydroxide |
C |
F |
S |
O |
1,000 |
||
|
Copper oxychloride |
C |
F |
S |
O |
1,440 |
||
|
4-CPA |
ISO |
PGR |
S |
O |
850 |
||
|
Crufomate |
ISO |
I |
OP |
S |
O |
770 |
|
|
Cycloate |
ISO |
H |
TC |
L |
O |
+2,000 |
|
|
Cyhexatin |
ISO |
AC |
OT |
S |
O |
540 |
|
|
Cymoxanil |
ISO |
F |
S |
O |
1,196 |
||
|
Cyproconazole |
N(B) |
F |
S |
O |
1,020 |
||
|
Dazomet |
ISO |
F-S |
S |
O |
640 |
Irritant to skin and eyes |
|
|
2,4-DB |
N(B) |
H |
S |
O |
700 |
||
|
DCBN |
N(J) |
See chlorthiamid |
|||||
|
Deet |
See diethyltoluamide |
||||||
|
Dehydroacetic acid |
C |
F |
S |
O |
1,000 |
||
|
2,4-DES |
N(B,U) |
See disul |
|||||
|
Desmetryn |
ISO |
H |
T |
S |
O |
1,390 |
|
|
Diallyl dichloroacetamide |
See dichlormid |
||||||
|
Dicamba |
ISO |
H |
S |
O |
1,707 |
||
|
Dichlone |
ISO |
FST |
S |
O |
1,300 |
||
|
Dichlormid |
N(A) |
H |
L |
O |
2,080 |
||
|
Dichlorobenzene |
C |
FM |
S |
O |
500-5,000 |
Mixture of isomers |
|
|
Dichlorophen |
ISO |
F |
OC |
S |
O |
1,250 |
|
|
Dichlorprop |
ISO |
H |
S |
O |
800 |
||
|
Diclofop |
ISO |
H |
S |
O |
565 |
||
|
Dicofol |
ISO |
AC |
S |
O |
c690 |
DS 81 |
|
|
Dienochlor |
ISO |
AC |
S |
O |
3,160 |
Acutely toxic by inhalation; skin sensitizer |
|
|
Diethyltoluamide |
ISO |
RP (insect) |
L |
O |
c2,000 |
DS 80 |
|
|
Difenoconazole |
ISO |
F |
T |
S |
O |
1,453 |
|
|
Dimepiperate |
ISO |
H |
TC |
S |
O |
946 |
|
|
Dimethachlor |
ISO |
H |
S |
O |
1,600 |
||
|
Dimethametryn |
ISO |
H |
T |
L |
O |
3,000 |
|
|
Dimethipin |
ISO |
H |
S |
O |
1,180 |
||
|
Dimethylarsinic acid |
C |
H |
S |
O |
1,350 |
||
|
Diniconazole |
ISO |
F |
S |
O |
639 |
||
|
Dinocap |
ISO |
AC,F |
CNP |
S |
O |
980 |
|
|
Diphenamid |
ISO |
H |
S |
O |
970 |
||
|
Disul |
ISO |
H |
S |
O |
730 |
||
|
Dithianon |
ISO |
F |
S |
O |
640 |
||
|
2,4-DP |
N(U) |
See dichlorprop |
|||||
|
Dodine |
ISO |
F |
S |
O |
1,000 |
||
|
Doguadine |
N(F) |
See dodine |
|||||
|
DSMA |
See methylarsonic acid |
||||||
|
Empenthrin ((1R) isomers) |
ISO |
I |
PY |
oil |
O |
+2,280 |
|
|
Ephirsulphonate |
N(U) |
See chlorfenson |
|||||
|
Esprocarb |
ISO |
H |
TC |
L |
O |
+2,000 |
Skin and eye irritant |
|
Etacelasil |
ISO |
PGR |
L |
O |
2,065 |
||
|
Etaconazole |
ISO |
F |
S |
O |
1,340 |
||
|
Ethohexadiol |
N(A) |
RP (insect) |
L |
O |
2,400 |
||
|
Etridiazole |
ISO |
F |
L |
O |
2,000 |
||
|
Fenoprop |
ISO |
H |
S |
O |
650 |
||
|
Fenson |
ISO |
AC |
S |
O |
1,550 |
||
|
Fenothiocarb |
ISO |
L |
C |
S |
O |
1,150 |
|
|
Fenpropidin |
ISO |
F |
S |
O |
1,440 |
||
|
Fenthiaprop |
N(B) |
H |
S |
O |
915 |
||
|
Ferimzone |
ISO |
F |
S |
O |
725 |
||
|
Flamprop |
ISO |
H |
S |
O |
1,210 |
||
|
Fluchloralin |
ISO |
H |
S |
O |
1,550 |
||
|
Fluoroglycofen |
N(B) |
H |
S |
O |
1,500 |
||
|
Flurprimidol |
ISO |
PGR |
S |
O |
709 |
||
|
Flusilazole |
N(B) |
F |
S |
O |
1,110 |
||
|
Flutriafol |
ISO |
F,FST |
T |
S |
O |
1,140 |
|
|
Fomesafen |
ISO |
H |
OC |
S |
O |
1,250 |
|
|
Fuberidazole |
ISO |
F |
S |
O |
1,100 |
||
|
Furalaxyl |
ISO |
F |
S |
O |
940 |
||
|
Glufosinate |
ISO |
H |
S |
O |
1,625 |
||
|
Heptopargil |
ISO |
PGR |
L |
O |
2,100 |
||
|
Hexazinone |
ISO |
H |
S |
O |
1,690 |
||
|
Hydramethylnon |
N(A,B) |
I |
S |
O |
1,200 |
||
|
IBP |
See iprobenphos |
||||||
|
Iprobenphos |
N(B) |
F |
S |
O |
600 |
||
|
Isoprothiolane |
ISO |
F |
S |
O |
1,190 |
||
|
Isoproturon |
ISO |
H |
S |
O |
1,800 |
||
|
Isouron |
ISO |
H |
S |
O |
630 |
||
|
Isoxapyrifop |
ISO |
H |
S |
O |
500 |
||
|
Kelthane |
N(J) |
See dicofol |
|||||
|
Malathion |
ISO |
I |
OP |
L |
O |
c2,100 |
LD50 value can vary according to impurities. This value has been adopted for classification purposes and is that of a technical product conforming to WHO specifications; DS 29 |
|
Maldison |
N(Aus,NZ) |
See malathion |
|||||
|
MCPA |
ISO |
H |
S |
O |
700 |
||
|
MCPA-thioethyl |
ISO |
H |
S |
O |
790 |
||
|
MCPB |
ISO |
H |
S |
O |
680 |
||
|
Mecoprop |
ISO |
H |
S |
O |
930 |
||
|
Mecoprop-P |
ISO |
H |
S |
O |
1,050 |
||
|
Mefluidide |
ISO |
H |
S |
O |
1,920 |
||
|
Menazon |
ISO |
AP |
OP |
S |
O |
1,950 |
|
|
Mepiquat |
ISO |
PGR |
S |
O |
1,490 |
||
|
Metalaxyl |
ISO |
F |
S |
O |
670 |
||
|
Metaxon |
N(U) |
See MCPA |
|||||
|
Metconazole |
ISO |
F |
S |
O |
660 |
||
|
Methazole |
N(A,B) |
H |
S |
O |
4,543 |
Slightly irritant to eyes |
|
|
2-Methoxyethlymercury silicate |
C |
FST |
OM |
S |
O |
1,140 |
|
|
Methylarsonic acid |
ISO |
H |
S |
O |
1,800 |
||
|
Metolachlor |
ISO |
H |
L |
O |
2,780 |
||
|
MSMA |
See methylarsonic acid |
||||||
|
Myclobutanil |
N(B) |
F |
S |
O |
1,600 |
||
|
2-Napthyloxy acetic acid |
ISO |
PGR |
S |
O |
600 |
||
|
Nitrapyrin |
ISO |
B-S |
S |
O |
1,072 |
||
|
Nuarimol |
ISO |
F |
S |
O |
1,250 |
||
|
Octhilinone |
ISO |
F |
S |
O |
1,470 |
||
|
N-octyl bicycloheptene dicarboximide |
C |
SY |
L |
O |
2,800 |
||
|
Oxadixyl |
N(B) |
F |
S |
O |
1,860 |
||
|
Paclobutrazol |
ISO |
PGR |
S |
O |
1,300 |
||
|
Pallethrine |
N(F) |
See allethrin |
|||||
|
Para-dichlorobenzene |
See dichlorobenzene |
||||||
|
Pendimethalin |
ISO |
H |
S |
O |
1,050 |
||
|
Perfluidone |
ISO |
H |
S |
O |
920 |
||
|
Pimaricin |
N(B) |
F |
S |
O |
2,730 |
Antibiotic, identical with tennecetin and natamycin |
|
|
Piproctanyl |
ISO |
PGR |
S |
O |
820 |
||
|
Pirimiphos-methyl |
ISO |
I |
OP |
L |
O |
2,018 |
DS 49 |
|
Prochloraz |
ISO |
F |
S |
O |
1,600 |
||
|
Propachlor |
ISO |
H |
S |
O |
1,500 |
DS 78 |
|
|
Propanil |
ISO |
H |
S |
O |
c1,400 |
||
|
Propargite |
ISO |
AC |
L |
O |
2,200 |
||
|
Pyrazoxyfen |
ISO |
H |
S |
O |
1,644 |
||
|
Pyridaben |
ISO |
AC |
S |
O |
820 |
||
|
Pyridaphenthion |
N(J) |
I |
OP |
S |
O |
769 |
|
|
Pyridate |
ISO |
H |
S |
O |
c2,000 |
||
|
Pyrifenox |
ISO |
F |
L |
O |
2,900 |
||
|
Quinoclamine |
ISO |
H |
S |
O |
1,360 |
||
|
Quizalofop |
N(B) |
H |
S |
O |
1,670 |
||
|
Resmethrin |
ISO |
I |
PY |
S |
O |
2,000 |
See cismethrin; EHC 92, DS 83, HSG 25 |
|
Ryania |
C |
I |
S |
O |
c750 |
LD50 varies: vegetable product |
|
|
Sesamex |
N(A) |
SY |
L |
O |
2,000 |
||
|
Sethoxydim |
ISO |
H |
L |
O |
3,200 |
||
|
Silvex |
N(A) |
See fenoprop |
|||||
|
Simetryn |
ISO |
H |
T |
S |
O |
1,830 |
|
|
Sodium chlorate |
ISO |
H |
S |
O |
1,200 |
||
|
Sulfluramid |
ISO |
I |
S |
O |
543 |
||
|
Sulfoxide |
N(A) |
SY |
L |
O |
2,000 |
||
|
2,3,6-TBA |
ISO |
H |
S |
O |
1,500 |
||
|
Tebuthiuron |
ISO |
H |
S |
O |
644 |
||
|
Thiram |
ISO |
F |
S |
O |
560 |
DS 71 |
|
|
TMTD |
N(U) |
See thiram |
|||||
|
2,4,5-TP |
N(F,J,U) |
See fenoprop |
|||||
|
Tralkoxydim |
ISO |
H |
S |
O |
934 |
||
|
Triadimefon |
ISO |
F |
S |
O |
602 |
||
|
Triadimenol |
ISO |
FST |
S |
O |
900 |
||
|
Tri-allate |
ISO |
H |
TC |
L |
O |
2,165 |
HSG 89 |
|
Trichlorfon |
ISO |
H |
OP |
S |
O |
560 |
DS 27; EHC 132; HSG 66 |
|
Triclopyr |
ISO |
H |
S |
O |
710 |
||
|
Tridiphane |
N(B) |
H |
S |
O |
1,740 |
||
|
Trifenmorph |
ISO |
M |
S |
O |
1,400 |
DS 64 |
|
|
Triflumizole |
N(B) |
F |
S |
O |
695 |
||
|
Undecan-2-one |
C |
RP (dogs,cats) |
oil |
O |
2,500 |
||
|
Uniconazole |
ISO |
PGR |
S |
O |
1,790 |
||
|
XMC |
N(J) |
I |
C |
S |
O |
542 |
|
|
Ziram |
ISO |
F |
S |
O |
1,400 |
Irritant to skin; DS 73 |
Source: WHO 1996.
The WHO Guidelines to Classification of Pesticides by Hazard (Extremely Hazardous to Moderately Hazardous)
Adapted from WHO 1996.
Individual products are classified in a series of tables according to the products’ oral and dermal toxicity and physical states. Technical products classified as Class IA (extremely hazardous, Class IB (highly hazardous), Class II (moderately hazardous) and Class III (slightly hazardous) are listed in table 1, table 2, table 3 and table 4, respectively. Technical products unlikely to present any acute hazard in normal use are listed in table 5. The classification given in tables 1 to 5 is of technical compounds and only forms the starting point for the final classification of an actual formulation: the final classification of any product depends on its formulation. Classification of mixtures of pesticides is not included; many of these mixtures are marketed with varying concentrations of active constituents. (For information on how to find the hazard class of formulations and mixtures, see WHO 1996.) Technical products believed to be absolete or discontinued (see table 6) are not inclued in the Classification. Table 7 lists gaseous fumigants not included in the WHO Recommanded Classification of Pesticides by Hazard.C
On this page are the following tables. Please return to the Minerals and Agricultural Chemicals chapter page for the remaining tables.
Table 1. List of technical products classified in Class IA: "Extremely hazardous"
Table 2. List of technical products classified in Class IB: "Highly hazardous"
Table 3. List of technical products classified in Class II: "Moderately hazardous"
Table 1. List of technical products classified in Class IA: "Extremely hazardous"
|
Name |
Status |
Main use |
Chemical type |
Physical state |
Route |
LD50 (mg/kg) |
Remarks |
|
Acrolein |
C |
H |
L |
O |
29 |
EHC 127; HSG 67 |
|
|
Alachlor |
ISO |
H |
S |
O |
930 |
Adjusted classification; carcinogenic in rats and mice; DS 84 |
|
|
Aldicarb |
ISO |
I-S |
C |
S |
O |
0.93 |
DS 53; EHC 121; HSG 64 |
|
Arsenous oxide |
C |
R |
S |
O |
180 |
Adjusted classification; minimum lethal dose for humans of 2 mg/kg; evidence of carcinogenicity for humans is sufficient; EHC 18; HSG 70 |
|
|
Brodifacoum |
ISO |
R |
S |
O |
0.3 |
DS 57; EHC 175; HSG 93 |
|
|
Bromadialone |
ISO |
R |
S |
O |
1.12 |
DS 88; EHC 175; HSG 94 |
|
|
Bromethalin |
ISO |
R |
S |
O |
2 |
||
|
Calcium cyanide |
C |
FM |
S |
O |
39 |
Adjusted classification; calcium cyanide is in Class IA as it reacts with moisture to produce hydrogen cyanide gas; the gas is not classified under the WHO system (see table 7) |
|
|
Captafol |
ISO |
F |
S |
O |
5,000 |
Adjusted classification; carcinogenic in rats and mice; HSG 49 |
|
|
Chlorfenvinphos |
ISO |
I |
OP |
L |
O |
10 |
|
|
Chlormephos |
ISO |
I |
OP |
L |
O |
7 |
|
|
Chlorophacinone |
ISO |
R |
S |
O |
3.1 |
DS 62; EHC 175 |
|
|
Chlorthiophos |
ISO |
I |
OP |
L |
O |
9.1 |
|
|
Coumaphos |
ISO |
AC, MT |
OP |
L |
O |
7.1 |
|
|
CVP |
N(J) |
See chlorfenvinphos |
|||||
|
Cycloheximide |
ISO |
F |
S |
O |
2 |
||
|
DBCP |
N(J) |
See dibromochloropropane |
|||||
|
Demephion-O and -S |
ISO |
I |
OP |
L |
O |
15 |
|
|
Demeton-O and -S |
ISO |
I |
OP |
L |
O |
2.5 |
DS 60 |
|
Dibromochloropropane |
C |
F-S |
L |
O |
170 |
Adjusted classification; has been found to cause sterility in humans and is mutagenic and carcinogenic in animals |
|
|
Difenacoum |
ISO |
R |
S |
O |
1.8 |
EHC 175; HSG 95 |
|
|
Difethialone |
ISO |
R |
S |
O |
0.56 |
EHC 175 |
|
|
Difolatan |
N(J) |
See captafol |
|||||
|
Dimefox |
ISO |
I |
OP |
L |
O |
1 |
Volatile |
|
Diphacinone |
ISO |
R |
S |
O |
2.3 |
EHC 175 |
|
|
Disulfoton |
ISO |
I |
OP |
L |
O |
2.6 |
DS 68 |
|
EPN |
N(A,J) |
I |
OP |
S |
O |
14 |
Has been reported as causing delayed neurotoxicity in hens |
|
Ethoprop |
N(A) |
See ethoprophos |
|||||
|
Ethoprophos |
ISO |
I-S |
OP |
L |
D |
26 |
DS 70 |
|
Ethylthiometon |
N(J) |
See disulfoton |
|||||
|
Fenamiphos |
ISO |
N |
OP |
L |
O |
15 |
DS 92 |
|
Fensulfothion |
ISO |
I |
OP |
L |
O |
3.5 |
DS 44 |
|
Flocoumafen |
N(B) |
R |
S |
O |
0.25 |
EHC 175 |
|
|
Fonofos |
ISO |
I-S |
OP |
L |
O |
c8 |
|
|
Hexachlorobenzene |
ISO |
FST |
S |
D |
10,000 |
Adjusted classification; has caused a serious outbreak of porphyria in humans; DS 26 |
|
|
Leptophos |
ISO |
I |
OP |
S |
O |
50 |
Adjusted classification; has been shown to cause delayed neurotoxicity; DS 38 |
|
M74 |
N(J) |
See disulfoton |
|||||
|
MBCP |
N(J) |
See leptophos |
|||||
|
Mephosfolan |
ISO |
I |
OP |
L |
O |
9 |
|
|
Mercuric chloride |
ISO |
F-S |
S |
O |
1 |
||
|
Merkaptophos |
N(U) |
When mixed with merkaptophosteolovy, see demeton -O and -S |
|||||
|
Metaphos |
N(U) |
See parathion-methyl |
|||||
|
Mevinphos |
ISO |
I |
OP |
L |
D |
4 |
DS 14 |
|
Nitrofen |
ISO |
H |
S |
O |
c3,000 |
Adjusted classification; carcinogenic in rats and mice; teratogenic in several species tested; DS 84 |
|
|
Parathion |
ISO |
I |
OP |
L |
O |
13 |
DS 6; HSG 74 |
|
Parathion-methyl |
ISO |
I |
OP |
L |
O |
14 |
DS 7; EHC 145; HSG 75 |
|
Phenylmercury acetate |
ISO |
FST |
S |
O |
24 |
Adjusted classification; highly toxic to mammals and very small doses have produced renal lesions; teratogenic in the rat |
|
|
Phorate |
ISO |
I |
OP |
L |
O |
2 |
DS 75 |
|
Phosfolan |
ISO |
I |
OP |
L |
O |
9 |
|
|
Phosphamidon |
ISO |
I |
OP |
L |
O |
7 |
DS 74 |
|
Prothoate |
ISO |
AC,I |
OP |
L |
O |
8 |
|
|
Red squill |
See scilliroside |
||||||
|
Schradan |
ISO |
I |
OP |
L |
O |
9 |
|
|
Scilliroside |
C |
R |
S |
O |
c0.5 |
Induces vomiting in mammals |
|
|
Sodium fluoroacetate |
C |
R |
S |
O |
0.2 |
DS 16 |
|
|
Sulfotep |
ISO |
I |
OP |
L |
O |
5 |
|
|
TEPP |
ISO |
AC |
OP |
L |
O |
1.1 |
|
|
Terbufos |
ISO |
I-S |
OP |
L |
O |
c2 |
|
|
Thiofos |
N(U) |
See parathion |
|||||
|
Thionazin |
ISO |
N |
OP |
L |
O |
11 |
|
|
Timet |
N(U) |
See phorate |
Table 2. List of technical products classified in Class IB: "Highly hazardous"
|
Name |
Status |
Main use |
Chemical type |
Physical state |
Route |
LD50 (mg/kg) |
Remarks |
|
Aldoxycarb |
ISO |
I,N |
C |
S |
O |
27 |
|
|
Aldrin |
ISO |
I |
OC |
S |
D |
98 |
DS41; EHC 91; HSG 21 |
|
Allyl alcohol |
C |
H |
L |
O |
64 |
Highly irritant to skin and eyes |
|
|
Aminocarb |
ISO |
I |
C |
S |
O |
50 |
|
|
Antu |
ISO |
R |
S |
O |
8 |
Induces vomiting in dogs. Some impurities are carcinogenic |
|
|
Azinphos-ethyl |
ISO |
I |
OP |
S |
O |
12 |
DS 72 |
|
Azinphos-methyl |
ISO |
I |
OP |
S |
O |
16 |
DS 59 |
|
Benfuracarb |
N(B) |
I |
C |
L |
O |
138 |
|
|
Bis(tributyltin) oxide |
C |
F,M |
L |
O |
194 |
Irritant to skin. DS 65; EHC 15 |
|
|
Blasticidin-S |
N(J) |
F |
S |
O |
16 |
||
|
Bromophos-ethyl |
ISO |
I |
OP |
L |
O |
71 |
|
|
Butocarboxim |
ISO |
I |
C |
L |
O |
158 |
|
|
Butoxycarboxim |
ISO |
I |
C |
L |
D |
288 |
|
|
Cadusafos |
ISO |
N,I |
OP |
L |
O |
37 |
|
|
Calcium arsenate |
C |
I |
S |
O |
20 |
||
|
Carbofuran |
ISO |
I |
C |
S |
O |
8 |
DS 56 |
|
Carbophenothion |
ISO |
I |
OP |
L |
O |
32 |
|
|
3-chloro-1,2-propanediol |
C |
R |
L |
O |
112 |
In non-lethal dosage is a sterilant for male rats |
|
|
Coumachlor |
ISO |
R |
S |
D |
33 |
||
|
Coumatetralyl |
ISO |
R |
S |
O |
16 |
||
|
Crotoxyphos |
ISO |
I |
OP |
L |
O |
74 |
|
|
zeta-Cypermethrin |
ISO |
I |
PY |
L |
O |
c86 |
|
|
DDVF |
N(U) |
See dichlorvos |
|||||
|
DDVP |
N(J) |
See dichlorvos |
|||||
|
Delnav |
N(U) |
See dioxathion |
|||||
|
Demeton-S-methyl |
ISO |
I |
OP |
L |
O |
40 |
DS 61 |
|
Demeton-S-methylsulphon |
ISO |
I |
OP |
S |
O |
37 |
|
|
Dichlorvos |
ISO |
I |
OP |
L |
O |
56 |
Volatile, DS 2; EHC 79; HSG 18 |
|
Dicrotophos |
ISO |
I |
OP |
L |
O |
22 |
|
|
Dieldrin |
ISO |
I |
OC |
S |
O |
37 |
DS 17: EHC 91 |
|
Dimetilan |
N(A,B) |
I |
C |
S |
O |
47 |
|
|
Dinoseb |
ISO |
H |
CNP |
L |
O |
58 |
|
|
Dinoseb acetate |
ISO |
H |
CNP |
L |
O |
60 |
|
|
Dinoterb |
ISO |
H |
CNP |
S |
O |
25 |
|
|
Dioxathion |
ISO |
I |
OP |
L |
O |
23 |
|
|
DMTP |
N(J) |
See methidathion |
|||||
|
DNBP |
N(J) |
See dinoseb |
|||||
|
DNBPA |
N(J) |
See dinoseb acetate |
|||||
|
DNOC |
ISO |
I-S,H |
CNP |
S |
O |
25 |
|
|
EDDP |
N(J) |
See edifenfos |
|||||
|
Edifenphos |
ISO |
F |
OP |
L |
O |
150 |
|
|
Endrin |
ISO |
I |
OC |
S |
O |
7 |
DS 1; EHC 130; HSG 60 |
|
ESP |
N(J) |
I |
OP |
L |
O |
105 |
|
|
Famphur |
N(A) |
I |
OP |
S |
O |
48 |
|
|
Flucythrinate |
ISO |
I |
PY |
L |
O |
c67 |
Irritant to skin and eyes |
|
Fluoroacetamide |
C |
R |
S |
O |
13 |
||
|
Formetanate |
ISO |
AC |
C |
S |
O |
21 |
|
|
Fosmethilan |
ISO |
I |
OP |
S |
O |
49 |
Irritant to skin and eyes. |
|
Furathiocarb |
N(B) |
I-S |
C |
L |
O |
42 |
|
|
Heptenophos |
ISO |
I |
OP |
L |
O |
96 |
|
|
Isazofos |
ISO |
I-S |
OP |
L |
O |
60 |
|
|
Isofenphos |
ISO |
I |
OP |
oil |
O |
28 |
|
|
Isothioate |
ISO |
I |
OP |
L |
O |
150 |
|
|
Isoxathion |
ISO |
I |
OP |
L |
O |
112 |
|
|
Lead arsenate |
C |
L |
S |
O |
c10 |
||
|
Mecarbam |
ISO |
I |
C |
oil |
O |
36 |
|
|
Mercuric oxide |
ISO |
O |
S |
O |
18 |
||
|
Methamidophos |
ISO |
I |
OP |
L |
O |
30 |
HSG 79 |
|
Methidathion |
ISO |
I |
OP |
L |
O |
25 |
|
|
Methomyl |
ISO |
I |
C |
S |
O |
17 |
DS 55, EHC 178; HSG 97 |
|
Methyl-merkapto-phosteolovy |
N(U) |
See demeton-S-methyl |
|||||
|
Metilmerkapto-phosoksid |
N(U) |
See oxydemeton-methyl |
|||||
|
Metriltriazotion |
N(U) |
See azinphos-methyl |
|||||
|
Monocrotophos |
ISO |
I |
OP |
S |
O |
14 |
HSG 80 |
|
MPP |
N(J) |
See fenthion |
|||||
|
Nicotine |
ISO |
L |
D |
50 |
|||
|
Omethoate |
ISO |
I |
OP |
L |
O |
50 |
|
|
Oxamyl |
ISO |
I |
C |
S |
O |
6 |
DS 54 |
|
Oxydemeton-methyl |
ISO |
I |
OP |
L |
O |
65 |
|
|
Oxydeprofos |
N(B) |
See ESP |
|||||
|
Paris green |
C |
L |
S |
O |
22 |
Copper-arsenic complex |
|
|
Pentachlorophenol |
ISO |
I,F,H |
CNP |
S |
D |
80 |
Irritant to skin; EHC 71; HSG 19 |
|
Phenylmercury nitrate |
C |
FST |
OM |
S |
Oral LD50 not available, rat i.v. LD50 is 27 mg/kg |
||
|
Pirimiphos-ethyl |
ISO |
I |
OP |
L |
O |
140 |
|
|
Propaphos |
N(J) |
I |
OP |
L |
O |
70 |
|
|
Propetamphos |
ISO |
I |
OP |
L |
O |
106 |
|
|
Sodium arsenite |
C |
R |
S |
O |
10 |
||
|
Sodium cyanide |
C |
R |
S |
O |
6 |
||
|
Strychnine |
C |
R |
S |
O |
16 |
||
|
TBTO |
See bis-(tributyltin) oxide |
||||||
|
Tefluthrin |
N(B) |
I-S |
PY |
S |
O |
c22 |
|
|
Thallium sulfate |
C |
R |
S |
O |
11 |
DS 10 |
|
|
Thiofanox |
ISO |
I-S |
C |
S |
O |
8 |
|
|
Thiometon |
ISO |
I |
OP |
oil |
O |
120 |
DS 67 |
|
Thioxamyl |
See oxyamyl |
||||||
|
Triamiphos |
ISO |
F |
S |
O |
20 |
||
|
Triazophos |
ISO |
I |
OP |
L |
O |
82 |
|
|
Triazotion |
N(U) |
See azinphos-ethyl |
|||||
|
Vamidothion |
ISO |
I |
OP |
L |
O |
103 |
|
|
Warfarin |
ISO |
R |
S |
O |
10 |
DS 35, EHC 175; HSG 96 |
|
|
Zinc phosphide |
C |
R |
S |
O |
45 |
DS 24, EHC 73 |
Table 3. List of technical products classified in Class II: "Moderately hazardous"
|
Name |
Status |
Main Use |
Chemical type |
Physical state |
Route |
LD50 (mg/kg) |
Remarks |
|
Alanycarb |
ISO |
I |
C |
S |
O |
330 |
|
|
Allidochlor |
ISO |
H |
L |
O |
700 |
Irritant to skin and eyes |
|
|
Anilofos |
ISO |
H |
S |
O |
472 |
||
|
Azaconazole |
N(B) |
F |
S |
O |
308 |
||
|
Azocyclotin |
ISO |
AC |
OT |
S |
O |
80 |
|
|
Bendiocarb |
ISO |
I |
C |
S |
O |
55 |
DS 52 |
|
Bensulide |
ISO |
H |
L |
O |
270 |
||
|
Benzofos |
N(U) |
See phosalone |
|||||
|
BHC |
ISO |
See HCH |
|||||
|
gamma-BHC |
See gamma-HCH |
||||||
|
Bifenthrin |
N(B) |
I |
PY |
S |
O |
c55 |
|
|
Bilanafos |
ISO |
H |
S |
O |
268 |
||
|
Binapacryl |
ISO |
AC |
S |
O |
421 |
||
|
Bioallethrin |
C |
I |
PY |
L |
O |
c700 |
Bioallethrin, esbiothrin, esbiol and esdepalléthrine are members of the allethrin series; their toxicity varies considerably within this series according to concentrations of isomers. |
|
Bisthiosemi |
N(J) |
R |
S |
O |
c150 |
Induces vomiting in non-rodents |
|
|
BPMC |
See fenobucarb |
||||||
|
Bromoxynil |
ISO |
H |
S |
O |
190 |
||
|
Bronopol |
N(B) |
B |
S |
O |
254 |
||
|
Bufencarb |
ISO |
I |
C |
S |
O |
87 |
|
|
Butamifos |
ISO |
H |
L |
O |
630 |
||
|
Butenachlor |
ISO |
H |
L |
O |
1,630 |
||
|
Butylamine |
ISO |
F |
L |
O |
380 |
Irritant to skin |
|
|
Camphechlor |
ISO |
I |
OC |
S |
O |
80 |
DS 20; EHC 45 |
|
Carbaryl |
ISO |
I |
C |
S |
O |
c300 |
DS 3; EHC 153; HSG 78 |
|
Carbosulfan |
ISO |
I |
L |
O |
250 |
||
|
Cartap |
ISO |
I |
S |
O |
325 |
||
|
Chloralose |
C |
R |
S |
O |
400 |
||
|
Chlordane |
ISO |
I |
OC |
L |
O |
460 |
DS 36; EHC 34; HSG 13 |
|
Chlordimeform |
ISO |
AC |
OC |
S |
O |
340 |
|
|
Chlorphenamidine |
N(J) |
See chlordimeform |
|||||
|
Chlorphonium |
ISO |
PGR |
S |
O |
178 |
Irritant to skin and eyes |
|
|
Chlorpyrifos |
ISO |
I |
OP |
S |
O |
135 |
DS 18 |
|
Clomazone |
ISO |
H |
L |
O |
1,369 |
||
|
Copper sulfate |
C |
F |
S |
O |
300 |
||
|
Cuprous oxide |
C |
F |
S |
O |
470 |
||
|
Cyanazine |
ISO |
H |
T |
S |
O |
288 |
|
|
Cyanofenphos |
ISO |
I |
OP |
S |
O |
89 |
Has been reported as causing delayed neurotoxicity in hens; no longer manufactured |
|
Cyanophos |
ISO |
I |
OP |
L |
O |
610 |
|
|
CYAP |
N(J) |
See cyanophos |
|||||
|
Cyfluthrin |
ISO |
I |
PY |
S |
O |
c250 |
|
|
beta-Cyfluthrin |
ISO |
I |
PY |
S |
O |
450 |
|
|
Cyhalothrin |
ISO |
Ix |
PY |
oil |
O |
c144 |
EHC 99 |
|
lambda-Cyhalothrin |
N(B) |
I |
PY |
S |
O |
c56 |
EHC 142; HSG 38 |
|
CYP |
N(J) |
See cyanofenphos |
|||||
|
Cypermethrin |
ISO |
I |
PY |
S |
O |
c250 |
DS 58; EHC 82; HSG 22 |
|
alpha-Cypermethrin |
ISO |
I |
PY |
S |
O |
c79 |
EHC 142 |
|
beta-Cypermethrin |
ISO |
I |
PY |
S |
O |
166 |
|
|
Cyphenothrin ((1R)-isomers) |
ISO |
I |
PY |
L |
O |
318 |
|
|
Cyprofuram |
ISO |
F |
S |
O |
174 |
||
|
2,4-D |
ISO |
H |
PA |
S |
O |
375 |
DS 37; EHC 29; EHC 84 |
|
DAPA |
N(J) |
See fenaminosulf |
|||||
|
DDT |
ISO |
I |
OC |
S |
O |
113 |
DS 21; EHC 9; EHC 83 |
|
Deltamethrin |
ISO |
I |
PY |
S |
O |
c135 |
DS 50; EHC 97; HSG 30 |
|
Dialifor |
N(A,J) |
See dialifos |
|||||
|
Dialifos |
ISO |
I |
OP |
S |
D |
145 |
|
|
Di-allate |
ISO |
H |
TC |
L |
O |
395 |
|
|
Diazinon |
ISO |
I |
OP |
L |
O |
300 |
DS 45 |
|
Dibrom |
N (Denmark) |
See naled |
|||||
|
Dichlofenthion |
ISO |
I-S |
OP |
L |
O |
270 |
|
|
Difenzoquat |
ISO |
H |
S |
O |
470 |
||
|
Dimethoate |
ISO |
I |
OP |
S |
O |
c150 |
DS 42; EHC 90; HSG 20 |
|
Dinobuton |
ISO |
AC,F |
S |
O |
140 |
||
|
Dioxabenzophos |
N(B) |
I |
OP |
S |
O |
125 |
|
|
Dioxacarb |
ISO |
I |
C |
S |
O |
90 |
|
|
Diquat |
ISO |
H |
P |
S |
O |
231 |
Irritant to skin, and eyes, and damages nails; DS 40; EHC 39; HSG 52 |
|
Drazoxolon |
(ISO) |
FST |
S |
O |
126 |
||
|
ECP |
N(J) |
See dichlofenthion |
|||||
|
Endosulfan |
ISO |
I |
OC |
S |
O |
80 |
DS 15; EHC 40; HSG 17 |
|
Endothal-sodium |
(ISO) |
H |
S |
O |
51 |
||
|
EPBP |
N(J) |
I-S |
OP |
oil |
O |
275 |
|
|
EPTC |
ISO |
H |
TC |
L |
O |
1,652 |
|
|
Esbiol |
See bioallethrin |
||||||
|
Esbiothrin |
See bioallethrin |
||||||
|
Esdepalléthrine |
See bioallethrin |
||||||
|
Esfenvalerate |
ISO |
I |
PY |
S |
O |
87 |
|
|
Ethiofencarb |
ISO |
I |
C |
L |
O |
411 |
|
|
Ethion |
ISO |
I |
OP |
L |
O |
208 |
|
|
Etrimfos |
ISO |
I |
OP |
L |
O |
1,800 |
|
|
Fenaminosulf |
ISO |
F-S |
S |
O |
60 |
||
|
Fenazaquin |
ISO |
AC |
S |
O |
134 |
||
|
Fenchlorphos |
ISO |
I |
OP |
L |
O |
1,740 |
DS 69 |
|
Fenitrothion |
ISO |
I |
OP |
L |
O |
503 |
DS 30; EHC 133; HSG 65 |
|
Fenobucarb |
N(B) |
I |
C |
S |
O |
620 |
|
|
Fenpropathrin |
ISO |
I |
PY |
S |
O |
c66 |
|
|
Fenthion |
ISO |
I,L |
OP |
L |
D |
586 |
DS 23 |
|
Fentin acetate |
(ISO) |
F |
OT |
S |
O |
125 |
DS 22 |
|
Fentin hydroxide |
(ISO) |
F |
OT |
S |
O |
108 |
DS 22 |
|
Fenvalerate |
ISO |
I |
PY |
L |
O |
c450 |
EHC 95, DS 90; HSG 34 |
|
Fipronil |
N(B) |
I |
Pyrazole |
S |
O |
92 |
|
|
Fluvalinate |
N(B) |
I |
oil |
O |
282 |
Irritant to skin |
|
|
Fluxofenim |
ISO |
H |
oil |
O |
670 |
||
|
Formothion |
ISO |
I |
OP |
L |
O |
365 |
|
|
Fosfamid |
N(U) |
See dimethoate |
|||||
|
Furconazole-cis |
ISO |
F |
S |
O |
450 |
||
|
Guazatine |
N(B) |
FST |
S |
O |
230 |
LD50 value refers to triacetate |
|
|
Haloxyfop |
N(A,B) |
H |
S |
O |
393 |
||
|
HCH |
ISO |
I |
OC |
S |
O |
100 |
The LD50 varies according to the mixture of isomers. The value shown has been chosen, and the technical product placed in Class II, as a result of the cumulative properties of the beta isomer |
|
Gamma-HCH |
ISO |
I |
OC |
S |
O |
88 |
DS 12; EHC 124; HSG 54 |
|
Heptachlor |
ISO |
I |
OC |
S |
O |
100 |
DS 19; EHC 38; HSG 14 |
|
Imazalil |
ISO |
F |
S |
0 |
320 |
||
|
Imidacloprid |
N(B) |
I |
Nitro- guanidine |
S |
O |
450 |
|
|
Iminoctadine |
ISO |
F |
S |
O |
300 |
Eye irritant |
|
|
Ioxynil |
ISO |
H |
S |
O |
110 |
||
|
Ioxynil octanoate |
(ISO) |
H |
S |
O |
390 |
||
|
Isoprocarb |
ISO |
I |
C |
S |
O |
403 |
|
|
Karbation |
N(U) |
See metam-sodium |
|||||
|
Lindane |
ISO |
See gamma-HCH |
|||||
|
MEP |
N(J) |
See fenitrothion |
|||||
|
Mercaptodimethur |
See methiocarb |
||||||
|
Mercurous chloride |
C |
F |
S |
O |
210 |
||
|
Metaldehide |
ISO |
M |
S |
O |
227 |
||
|
Metam-sodium |
(ISO) |
F-S |
S |
O |
285 |
||
|
Methacrifos |
ISO |
I |
OP |
L |
O |
678 |
|
|
Methasulfocarb |
ISO |
F |
S |
O |
112 |
||
|
Methiocarb |
ISO |
I |
C |
S |
O |
100 |
|
|
Methyl isothiocyanate |
ISO |
F-S |
S |
O |
72 |
Skin and eye irritant |
|
|
Metolcarb |
ISO |
I |
C |
S |
O |
268 |
|
|
MICP |
N(J) |
See isoprocarb |
|||||
|
Molinate |
ISO |
H |
TC |
L |
O |
720 |
|
|
MPMC |
See xylylcarb |
||||||
|
Nabam |
ISO |
F |
TC |
S |
O |
395 |
Goitrogenic in rats |
|
NAC |
N(J) |
See carbaryl |
|||||
|
Naled |
ISO |
I |
OP |
L |
O |
430 |
DS 39 |
|
Norbormide |
ISO |
R |
S |
O |
52 |
||
|
2,4-PA |
N(J) |
See 2,4-D |
|||||
|
PAP |
N(J) |
See phenthoate |
|||||
|
Paraquat |
ISO |
H |
P |
S |
O |
150 |
Has serious delayed effects if absorbed; is relatively low hazard in actual use but is dangerous if accidentally taken orally; DS 4; EHC 39; HSG 51 |
|
Pebulate |
ISO |
H |
TC |
L |
O |
1,120 |
|
|
Permethrin |
ISO |
I |
PY |
L |
O |
c500 |
DS 51; EHC 94; HSG 33 |
|
PHC |
N(J) |
See propoxur |
|||||
|
Phenthoate |
ISO |
I |
OP |
L |
O |
c400 |
DS 48 |
|
Phosalone |
ISO |
I |
OP |
L |
O |
120 |
|
|
Phosmet |
ISO |
I,AC |
OP |
S |
O |
230 |
|
|
Phoxim |
ISO |
I |
OP |
L |
D |
1,975 |
DS 31 |
|
Phthalofos |
N(U) |
See phosmet |
|||||
|
Pindone |
ISO |
R |
S |
O |
50 |
||
|
Piperophos |
ISO |
H |
oil |
O |
324 |
||
|
Pirimicarb |
ISO |
AP |
C |
S |
O |
147 |
|
|
Polychlorcamphene |
N(U) |
See camphechlor |
|||||
|
Prallethrin |
ISO |
I |
PY |
oil |
O |
460 |
|
|
Profenofos |
ISO |
I |
OP |
L |
O |
358 |
|
|
Promacyl |
N(Aust) |
Ix |
C |
L |
O |
1,220 |
|
|
Promecarb |
ISO |
I |
C |
S |
O |
74 |
|
|
Propiconazole |
ISO |
F |
L |
O |
1,520 |
||
|
Propoxur |
ISO |
I |
C |
S |
O |
95 |
DS 25 |
|
Prosulfocarb |
ISO |
H |
L |
O |
1,820 |
||
|
Prothiofos |
ISO |
I |
OP |
L |
O |
925 |
|
|
Prothiophos |
See prothiofos |
||||||
|
Pyraclofos |
N(B) |
I |
OP |
L |
O |
237 |
|
|
Pyrazophos |
ISO |
F |
S |
O |
435 |
||
|
Pyrethrins |
C |
I |
L |
O |
500-1,000 |
Mixture of compounds present in Pyrethrum, Cineraefolium and other flowers; DS 11 |
|
|
Pyroquilon |
ISO |
F |
S |
O |
320 |
||
|
Quinalphos |
ISO |
I |
OP |
S |
O |
62 |
|
|
Quizalofop-p-tefuryl |
ISO |
H |
L |
O |
1,012 |
||
|
Reglon |
N(U) |
See diquat |
|||||
|
Ronnel |
N(A) |
See fenchlorphos |
|||||
|
Rotenone |
C |
I |
S |
O |
132-1,500 |
Compounds from roots of Derris and Lonchocarpus spp.; HSG 73 |
|
|
Salithion |
See dioxabenzofos |
||||||
|
SAP |
N(J) |
See bensulide |
|||||
|
Sec-butylamine |
See butylamine |
||||||
|
Sevin |
N(U) |
See carbaryl |
|||||
|
Sodium fluoride |
ISO |
I |
S |
O |
180 |
||
|
Sodium hexafluorosilicate |
ISO |
L-S |
S |
O |
125 |
||
|
Sulfallate |
ISO |
H |
oil |
0 |
850 |
Irritant to skin and eyes |
|
|
Sulprofos |
ISO |
I |
OP |
oil |
O |
130 |
|
|
2,4,5-T |
ISO |
H |
S |
O |
500 |
May contain a contaminant TCDD which affects toxicity: it should not exceed 0.01 mg/kg technical material; DS 13 |
|
|
TCA |
ISO |
The data shown refer to sodium trichloroacetic acid. In many countries, the term TCA refers to the free acid (now accepted by ISO); this is a solid with an oral LD50 of 400 mg/kg and if used as a pesticide is placed in Class II. It is highly corrosive to skin. |
|||||
|
Terbumeton |
ISO |
H |
T |
S |
O |
483 |
|
|
Tetraconazole |
ISO |
F |
oil |
O |
1,031 |
||
|
Thiazafluron |
ISO |
H |
S |
O |
278 |
||
|
Thiazfluron |
N(B) |
See thiazafluron |
|||||
|
Thicyofen |
ISO |
F |
S |
O |
368 |
||
|
Thiobencarb |
ISO |
H |
TC |
L |
O |
1,300 |
|
|
Thiocyclam |
ISO |
I |
S |
O |
310 |
||
|
Thiodan |
N(U) |
See endosulfan |
|||||
|
Thiodicarb |
ISO |
I |
S |
O |
66 |
||
|
Tolyl-methyl-carbamate |
See metolcarb |
||||||
|
Toxaphene |
N(A) |
See camphechlor |
|||||
|
Tralomethrin |
N(B) |
I |
PY |
S |
O |
c85 |
|
|
Trichloroacetic acid |
|||||||
|
Tricyclazole |
ISO |
F |
S |
O |
305 |
||
|
Tridemorph |
ISO |
F |
oil |
O |
650 |
||
|
Vernolate |
ISO |
H |
TC |
L |
O |
1,780 |
|
|
Xylylcarb |
N(B) |
I |
C |
S |
O |
380 |
Source: WHO 1996.
Renal-Urinary Cancers
Kidney Cancer
Epidemiology
Historically, kidney cancer has been used to mean either all malignancies of the renal system (renal cell carcinoma (RCC), ICD-9 189.0; renal pelvis, ICD-9 189.1; and ureter, ICD-9 189.2) or RCC only. This categorization has led to some confusion in epidemiological studies, resulting in a need to scrutinize previously reported data. RCC comprises 75 to 80% of the total, with the remainder being primarily transitional cell carcinomas of the renal pelvis and ureter. Separation of these two cancer types is appropriate since the pathogenesis of RCC and of transitional cell carcinoma is quite different, and epidemiological risk factors are distinct as are the signs and symptoms of the two diseases. This section focuses on RCC.
The major identified risk factor for kidney cancer is tobacco smoking, followed by suspected but poorly defined occupational and environmental risk factors. It is estimated that the elimination of tobacco smoking would decrease the incidence of kidney cancer by 30 to 40% in industrialized countries, but occupational determinants of RCC are not well established. The population attributable risk due to occupational exposures has been estimated to be between zero, based on recognized carcinogenesis, and 21%, based on a multicentric multisite case-control study in the Montreal area of Canada. Early biomarkers of effect in association with biomarkers of exposure should assist in clarifying important risk factors. Several occupations and industries have been found in epidemiological studies to entail an increased risk of renal cancer. However, with the possible exception of agents used in dry cleaning and exposures in petroleum refining, the available evidence is not consistent. Statistical analysis of epidemiological exposure data in relation to biomarkers of susceptibility and effect will clarify additional aetiological causes.
Several epidemiological studies have associated specific industries, occupations and occupational exposures with increased risks of renal cell carcinoma. The pattern that emerges from these studies is not fully consistent. Oil refining, printing, dry cleaning and truck driving are examples of jobs associated with excess risk of kidney cancer. Farmers usually display decreased risk of RCC, but a Danish study linked long-term exposure to insecticides and herbicides with an almost fourfold excess of RCC risk. This finding requires confirmation in independent data, including specification of the possible causal nature of the association. Other products suspected of being associated with RCC include: various hydrocarbon derivatives and solvents; products of oil refining; petroleum, tar and pitch products; gasoline exhaust; jet fuel; jet and diesel engine emissions; arsenic compounds; cadmium; chromium (VI) compounds; inorganic lead compounds; and asbestos. Epidemiological studies have associated occupational gasoline vapour exposure with kidney cancer risk, some in a dose-response fashion, a phenomenon observed in the male rat for unleaded gasoline vapour exposure. These findings gain some potential weight, given the widespread human exposure to gasoline vapours in retail service stations and the recent increase in kidney cancer incidence. Gasoline is a complex mixture of hydrocarbons and additives, including benzene, which is a known human carcinogen.
The risk of kidney cancer is not consistently linked with social class, although increased risk has occasionally been associated with higher socio-economic status. However, in some populations a reverse gradient was observed, and in yet others, no clear pattern emerged. Possibly these variations may be related to lifestyle. Studies with migrant people show modification in RCC risk towards the level of the host country population, suggesting that environmental factors are important in the development of this malignancy.
Except for nephroblastoma (Wilms’ tumour), which is a childhood cancer, kidney cancer usually occurs after 40 years of age. An estimated 127,000 new cases of kidney cancer (including RCC and transitional cell carcinoma (TCC) of the renal pelvis and ureter), corresponding to 1.7% of the world total cancer incidence, occurred globally in 1985. The incidence of kidney cancer varies among populations. High rates have been reported for both men and women in North America, Europe, Australia and New Zealand; low rates in Melanesia, middle and eastern Africa and southeastern and eastern Asia. The incidence of kidney cancer has been increasing in most western countries, but stagnated in a few. Age-standardized incidence of kidney cancer in 1985 was highest in North America and western, northern and eastern Europe, and lowest in Africa, Asia (except in Japanese men) and the Pacific. Kidney cancer is more frequent in men than in women and ranks among the ten most frequent cancers in a number of countries.
Transitional cell carcinoma (TCC) of the renal pelvis is associated with similar aetiological agents as bladder cancer, including chronic infection, stones and phenacetin-containing analgesics. Balkan nephropathy, a slowly progressive, chronic and fatal nephropathy prevalent in the Balkan countries, is associated with high rates of tumours of the renal pelvis and ureter. The causes of Balkan nephropathy are unknown. Excessive exposure to ochratoxin A, which is considered possibly carcinogenic to humans, has been associated with the development of Balkan nephropathy, but the role of other nephrotoxic agents cannot be excluded. Ochratoxin A is a toxin produced by fungi which can be found in many food stuffs, particularly cereals and pork products.
Screening and diagnosis of kidney cancer
The sign and symptom pattern of RCC varies among patients, even up to the stage when metastasis appears. Because of the location of the kidneys and the mobility of contiguous organs to the expanding mass, these tumours are frequently very large at the time of clinical detection. Although haematuria is the primary symptom of RCC, bleeding occurs late compared to transitional cell tumours because of the intra-renal location of RCC. RCC has been considered the “medical doctor’s dream” but the “surgeon’s curse” because of the interesting constellation of symptoms related to paraneoplastic syndromes. Substances that increase the red blood cell count, calcium and factors which mimic abnormal adrenal gland function have been reported, and abdominal mass, weight loss, fatigue, pain, anaemia, abnormal liver function and hypertension have all been observed. Computerized axial tomography (CAT scan) of the abdomen and ultrasound are being ordered by physicians with increased frequency so, consequently, it is estimated that 20% of RCCs are diagnosed serendipitously as a result of evaluation for other medical problems.
Clinical evaluation of an RCC case consists of a physical examination to identify a flank mass, which occurs in 10% of patients. A kidney x ray with contrast may delineate a renal mass and the solid or cystic nature is usually clarified by ultrasound or CAT scan. The tumours are highly vascular and have a characteristic appearance when the artery is injected with radio-opaque contrast material. Arteriography is performed to embolize the tumour if it is very large or to define the arterial blood supply if a partial nephrectomy is anticipated. Fine-needle aspiration may be used to sample suspect RCC.
Localized RCC tumours are surgically removed with regional lymph nodes and, operatively, early ligation of the artery and vein is important. Symptomatically, the patient may be improved by removing large or bleeding tumours that have metastasized, but this does not improve survival. For metastatic tumours, localized pain control may be achieved with radiation therapy but the treatment of choice for metastatic disease is biological response modifiers (Interleukin-2 or α-interferon), although chemotherapy is occasionally used alone or in combination with other therapies.
Markers such as the cancer gene on chromosome 3 observed in cancer families and in von Hippel-Lindau disease may serve as biomarkers of susceptibility. Although tumour marker antigens have been reported for RCC, there is currently no way to detect these reliably in the urine or blood with adequate sensitivity and specificity. The low prevalence of this disease in the general population requires a high specificity and sensitivity test for early disease detection. Occupational cohorts at risk could potentially be screened with ultrasound. Evaluation of this tumour remains a challenge to the basic scientist, molecular epidemiologist and clinician alike.
Bladder Cancer
Epidemiology
More than 90% of bladder cancers in Europe and North America are transitional cell carcinomas (TCC). Squamous cell carcinoma and adenocarcinoma account for 5 and 1%, respectively, of bladder cancer in these regions. The distribution of histopathological types in bladder cancer is strikingly different in regions such as the Middle East and Africa where bladder cancer is associated with schistosomal infection. For instance, in Egypt, where schistosomiasis is endemic and bladder cancer is the major oncogenic problem, the most common type is squamous cell carcinoma, but the incidence of TCC is increasing with the rising prevalence of cigarette smoking. The discussion which follows focuses on TCC.
Bladder cancer continues to be a disease of significant importance. It accounted for about 3.5% of all malignancies in the world in 1980. In 1985, bladder cancer was estimated to be 11th in frequency on a global scale, being the eighth most frequent cancer among men, with an expected total of 243,000 new cases. There is a peak incidence in the seventh decade of life, and worldwide the male to female ratio is around three to one. Incidence has been increasing in almost all populations in Europe, particularly in men. In Denmark, where annual incidence rates are among the highest in the world, at 45 per 100,000 in men and 12 per 100,000 in women, the recent trend has been a further rise of 8 to 9% every 5 years. In Asia, the very high rates among the Chinese in Hong Kong have declined steadily, but in both sexes bladder cancer incidence is still much higher than elsewhere in Asia and more than twice as high as that among the Chinese in Shanghai or Singapore. Bladder cancer rates among the Chinese in Hawaii are also high.
Cigarette smoking is the single most important aetiological factor in bladder cancer, and occupational exposures rank second. It has been estimated that tobacco is responsible for one-third of all bladder cancer cases outside of regions where schistosomal infection is prevalent. The number of bladder cancer cases attributed in 1985 to tobacco smoking has been estimated at more than 75,000 worldwide, and may account for 50% of bladder cancer in western populations. The fact that all individuals who smoke similar amounts do not develop bladder cancer at the same rate suggests genetic factors are important in controlling the susceptibility. Two aromatic amines, 4-aminobiphenyl and 2-naphthylamine, are carcinogens associated with cigarette smoking; these are found in higher concentrations in “black tobacco” (air-cured) than in “blend tobacco” (flue-cured). Passive smoke increases the adducts in the blood and a dose-response of adduct formation has been correlated with increased risk of bladder cancer. Higher levels of adduct formation have been observed in cigarette smokers who are slow acetylators compared to fast acetylators, which suggests that genetically inherited acetylation status may be an important biomarker of susceptibility. The lower incidence of bladder cancer in Black compared to White races may be attributed to conjugation of carcinogenic metabolic intermediates by sulphotransferases that produce electrophiles. Detoxified phenolic sulphates may protect the urothelium. Liver sulphotransferase activity for N-hydroxyarylamines has been reported to be higher in Blacks than Whites. This may result in a decrease in the amount of free N-hydroxymetabolites to function as carcinogens.
Occupational bladder cancer is one of the earliest known and best documented occupational cancers. The first identified case of occupational bladder cancer appeared some 20 years after the inception of the synthetic dye industry in Germany. Numerous other occupations have been identified in the last 25 years as occupational bladder cancer risks. Occupational exposures may contribute to up to 20% of bladder cancers. Workers occupationally exposed include those working with coal-tar pitches, coal gasification and production of rubber, aluminium, auramine and magenta, as well as those working as hairdressers and barbers. Aromatic amines have been shown to cause bladder cancer in workers in many countries. Notable among this class of chemicals are 2-naphthylamine, benzidine, 4-nitrobiphenyl and 3,3r´-dichlorobenzidine. Two other aromatic amines, 4,4´-methylene dianiline (MDA) and 4,4´-methylene-bis-2-chloroaniline (MOCA) are among the most widely used of the suspected bladder carcinogens. Other carcinogens associated with industrial exposures are largely undetermined; however, aromatic amines are frequently present in the workplace.
Screening and diagnosis of bladder cancer
Screening for bladder cancer continues to receive attention in the quest to diagnose bladder cancer before it becomes symptomatic and, presumably, less amenable to curative treatment. Voided urine cytology and urinalysis for haematuria have been considered candidate screening tests. A pivotal question for screening is how to identify high-risk groups and then individuals within these groups. Epidemiological studies identify groups at risk while biomarkers potentially identify individuals within groups. In general, occupational screening for bladder cancer with haematuria testing and Papanicolaou cytology has been ineffective.
Improved detection of bladder cancer may be possible using the 14-day hemastick testing described by Messing and co-workers. A positive test was observed at least once in 84% of 31 patients with bladder cancer at least 2 months prior to the cystoscopic diagnosis of disease. This test suffers from a false-positive rate of 16 to 20% with half of these patients having no urological disease. The low cost may make this a useful test in a two-tier screen in combination with biomarkers and cytology (Waples and Messing 1992).
In a recent study, the DD23 monoclonal antibody using quantitative fluorescence image analysis detected bladder cancer in exfoliated uroepithelial cells. A sensitivity of 85% and specificity of 95% were achieved in a mixture of low- and high-grade transitional cell carcinomas including TaT1 tumours. The M344 tumour-associated antigen in conjunction with DNA ploidy had a sensitivity approaching 90%.
Recent studies indicate combining biomarkers with haematuria testing may be the best approach. A list of the applications of quantitative fluorescence urinary cytology in combination with biomarkers is summarized in Table 1. Genetic, biochemical and morphological early cell changes associated with premalignant conditions support the concept that individuals at risk can be identified years in advance of the development of overt malignancy. Biomarkers of susceptibility in combination with biomarkers of effect promise to detect individuals at risk with an even higher precision. These advances are made possible by new technologies capable of quantitating phenotypic and genotypic molecular changes at the single cell level thus identifying individuals at risk. Individual risk assessment facilitates stratified, cost-effective monitoring of selected groups for targeted chemoprevention.
Table 1. Applications of urinary cytology
Detection of CIS1 and bladder cancer
Monitoring surgical therapy:
Monitoring bladder following TURBT2
Monitoring upper urinary tract
Monitoring urethral remnant
Monitoring urinary diversion
Monitoring intravesical therapy
Selecting intravesical therapy
Monitoring effect of laser therapy
Evaluation of patients with haematuria
Establishing need for cystoscopy
Screening high-risk populations:
Occupational exposure groups
Drug abuse groups at risk for bladder cancer
Decision criteria for:
Cystectomy
Segmental ureteral resection versus nephroureterectomy
Other indications:
Detecting vesicoenteric fistula
Extraurological tumours invading the urinary tract
Defining effective chemopreventive agents
Monitoring effective chemotherapy
1 CIS, carcinoma in situ.
2 TURBT, transurethral resection for bladder tumour.
Source: Hemstreet et al. 1996.
Signs and symptoms of bladder cancer are similar to those of urinary tract infection and may include pain on urination, frequent voiding and blood and pus cells in the urine. Because symptoms of a urinary tract infection may herald a bladder tumour particularly when associated with gross haematuria in older patients, confirmation of the presence of bacteria and a keen awareness by the examining physician is needed. Any patient treated for a urinary tract infection which does not resolve immediately should be referred to a urology specialist for further evaluation.
Diagnostic evaluation of bladder cancer first requires an intravenous pyelogram (IVP) to exclude upper tract disease in the renal pelvis or ureters. Confirmation of bladder cancer requires looking in the bladder with a light (cystoscope) with multiple biopsies performed with a lighted instrument through the urethra to determine if the tumour is non-invasive (i.e., papillary or CIS) or invasive. Random biopsies of the bladder and prostatic urethra help to define field cancerization and field effect changes. Patients with non-invasive disease require close monitoring, as they are at risk of subsequent recurrences, although stage and grade progression are uncommon. Patients who present with bladder cancer that is already high-grade or invasive into the lamina propria are at equally high risk of recurrence but stage progression is much more likely. Thus, they usually receive intravesical instillation of immuno- or chemotherapeutic agents following transurethral resection. Patients with tumours invading the muscularis propria or beyond are much more likely to have metastasis already and can rarely be managed by conservative means. However, even when treated by total cystectomy (the standard therapy for muscle-invading bladder cancer), 20 to 60% eventually succumb to their disease, almost always due to metastasis. When regional or distal metastasis is present at diagnosis, the 5-year survival rates drop to 35 and 9%, respectively, despite aggressive treatment. Systemic chemotherapy for metastatic bladder cancer is improving with complete response rates reported at 30%. Recent studies suggest chemotherapy prior to cystectomy may improve survival in selected patients.
Bladder cancer staging is predictive of the biological potential for progression, metastasis, or recurrence in 70% of the cases. Staging of bladder cancer usually requires CAT scan to rule out liver metastasis, radioisotope bone scan to exclude spread to the bone, and chest x ray or CAT scan to exclude lung metastasis. A search continues for biomarkers in the tumour and the bladder cancer field that will predict which tumours will metastasize or recur. The accessibility of exfoliated bladder cells in voided specimens shows promise for using biomarkers for monitoring recurrence and for cancer prevention.
Renal-Urinary Systems
The renal and urinary systems are comprised of a complex series of organs which together function to filter wastes from the blood, and manufacture, store and discharge urine. These organ systems are vital to homeostasis through maintaining fluid balance, acid-base balance and blood pressure. The primary organs of the renal-urinary systems are the two kidneys and the urinary bladder. In the process of filtering waste products from the blood the kidneys are potentially exposed to high concentrations of endogenous and exogenous toxic substances. Thus, some kidney cells are exposed to concentrations a thousand times higher than in blood.
Problems that result in damage to the kidney may be pre-renal (affect blood supply to the kidney), renal (affect the kidney itself) or post-renal (affect any point along the path which the urine travels from the kidney to the end of the urethra or penis). Post-renal problems are usually obstructive in nature; a common site of obstruction is the prostate, juxtapositioned between the bladder and the urethra. Pre-existing disease of the prostate, bladder or ureters, particularly infection, obstruction or foreign bodies such as stones, can compromise kidney function and increase susceptibility to either acquired or genetic defects.
Understanding the microanatomy and molecular mechanisms of the kidneys and bladder is important to assessing susceptibility to, and monitoring and prevention of, occupational exposures. Toxicants seem to target specific parts of the kidney or bladder and result in the expression of specific biomarkers directly related to the damaged segment. Historically, predisposition to disease has been viewed from the epidemiological perspective of identifying a group of workers at risk. Today, with better understanding of the fundamental mechanisms of disease, individual risk assessment through the use of biomarkers of susceptibility, exposure, effect and disease is on the horizon. New ethical issues arise because of the pressure to develop cost-effective strategies to protect workers from occupational hazards. The pressure arises, in part, because genetic testing is gaining acceptance for evaluating disease predisposition and biomarkers of exposure and effect can serve as intermediate end-points at which intervention may be beneficial. The purpose of this chapter is to provide a medical review of the renal and urinary systems on the basis of which guidelines for assessing and reducing individual risk in the workplace could be set forth with due account taken of the ethical aspects involved.
Anatomy and Pathophysiology of the Kidney
The human kidney is a complex organ which functions to filter wastes from the blood through the production of urine. The two kidneys also perform a variety of other vital functions including maintaining homeostasis, regulating blood pressure, osmotic pressure and acid-base balance. The kidneys receive 25% of the total cardiac output of blood, potentially exposing them to endogenous and exogenous toxins.
The kidneys are located on each side of the spine in the lower portion of the back. Each weighs about 150 grams and is about the size of an orange. The kidney consists of three layers: the cortex (outer layer), the medulla and the renal pelvis. Blood flows into the cortex and medulla through the renal artery and branches into increasingly smaller arteries. Each of the arteries ends in a blood filtration unit called a nephron. A healthy kidney contains approximately 1.2 million nephrons, strategically positioned within the cortex and medulla.
A nephron consists of the glomerulus (a group of tiny blood vessels) surrounded by Bowman’s capsule (a two-layer membrane) that opens into a convoluted tubule. The fluid portion of blood, plasma, is forced through the glomerulus into Bowman’s capsule and then, as filtered plasma, passes into the convoluted tubule. About 99% of the water and essential nutrients that have been filtered are reabsorbed by the tubule cells and passed into the capillaries which surround the convoluted tubule. The unfiltered blood which remains in the glomerulus also flows into capillaries and returns through the renal vein to the heart.
The nephrons appear as long, looped ducts comprised of multiple segments each of which performs a variety of different functions designed to maintain the body’s homeostatic mechanisms. Figure 1 depicts a nephron and its orientation within the renal cortex and the medulla. Each nephron segment has a differential blood supply regulating the ionic gradient. Certain chemicals may directly affect specific segments of the nephron acutely or chronically depending on the type and dose of xenobiotic exposure. Depending on the segment of the microanatomy targeted, various aspects of kidney function may be affected.
Figure 1. Relationships of the vascular supply, the glomerulus and the tubular components of the nephron to each other and the orientation of these components within the renal cortex and medulla

Blood vessels to the kidney supply only the glomerular and tubular elements, delivering wastes to be filtered and absorbing nutrients, proteins and electrolytes in addition to supplying oxygen for organ viability. Ninety per cent of the blood flow is to the cortex, with a gradient decrease to the medulla. Such differential blood flow, and the positioning of the nephron units, are vital to the countercurrent mechanism which further concentrates the urine and potential nephrotoxins.
The glomerulus is positioned between the afferent and efferent arterioles. The efferent arterioles form a web of capillaries around each nephron unit with the exception of the distal tubule juxtaposition adjacent to the afferent blood supply of the glomerulus. Afferent and efferent tubules enervated by the sympathetic nerves respond to autonomic stimulation and hormonal mediators such as vasopression and antidiuretic hormone (ADH). An area called the macula densa, part of the juxtaglomerular apparatus, produces renin, a mediator of blood pressure, in response to osmotic changes and blood pressure. Renin is converted by liver enzymes to an octapeptide, angiotensin II, that regulates blood flow to the kidneys preferentially targeting the afferent arterioles and the mesangial cells of the glomerulus.
The glomerulus allows only certain size proteins with defined charge to pass through during filtration. Plasma filtration is controlled by a balance of osmotic and hydrostatic pressure. Specialized sugar molecules, glycosaminoglycans, provide negative anionic charge which inhibit, by electrostatic forces, the filtration of negatively charged materials. The three-cell layer of the glomerular basement membrane consists of multiple foot processes that increase the absorption area and create the pores through which the filtrate passes. Damage to the specialized basement membrane or the capillary endothelium may permit albumin, a type of protein, to be spilled in increased amounts into the urine. The presence of an excess amount of albumin or other micro-proteins in the urine serves as a marker of glomerular or tubular damage.
The renal interstitium is the space between the nephron units and is more prominent in the central medullary portion than in the outer cortex. Within the interstitium are interstitial cells that are in close proximity to the medullary blood vessels and tubule cells. With ageing there may be an increased prominence of interstitial cells in the cortex with associated fibrosis and scarring. The interstitial cells contain lipid droplets and may be involved in the control of blood pressure with the release of vascular relaxing or constricting factors. Chronic disease of the interstitium may affect the glomerulus and tubules, or conversely, disease of the glomerulus and tubules may affect the interstitium. Thus, in end-stage kidney disease it is sometimes difficult to precisely define the pathological mechanisms of renal failure.
The proximal collecting tubules absorb 80% of the sodium, water and chloride, and 100% of the urea. Each proximal tubule has three segments, with the last segment (P-3) the most vulnerable to xenobiotic (toxic foreign substance) exposures. When the proximal cells are damaged by heavy metals such as chromium, the concentrating ability of the kidney is impaired and urine may be more dilute. Toxicity to the P-3 segment results in the release into the urine of enzymes, such as intestinal alkaline phosphatase, N-acetyl-beta-D-glucosaminidase (NAG), or Tamm-Horsfall protein, which is associated with the brush-like border of the proximal tubule cells increasing the effective absorbing area.
Diagnosis and Testing for Nephrotoxicity
Serum creatinine is another substance filtered by the glomerulus but minimally absorbed by the proximal tubules. Damage to the glomerulus results in its inability to remove toxins produced by the body and there is an accumulation of serum creatinine. Because serum creatinine is a product of muscle metabolism and dependent on the patient’s body mass, it has low sensitivity and specificity for measuring renal function, but it is used frequently because it is convenient. A more sensitive and specific test is to quantitate the filtrate by measuring the creatinine (Cr) clearance; serum urinary creatinine clearance is calculated by the general formula CCr=UCr V/PCr, where UCrV is the amount of Cr excreted per unit time and PCr is the plasma concentration of the Cr. However, creatinine clearance is more complex, in terms of sampling for the test, and is thus impractical for occupational testing. Isotope clearance tests performed by radioactive labelling of compounds such as ortho-iodohippurate which are also cleared by the kidney are also effective, but not practical or cost-effective in the workplace setting. Differential function of individual kidneys may be determined using differential renal nuclear scans or selective catheterization of both kidneys by passage of a catheter from the bladder up through the ureter into the kidney. However these methods also are not readily employed for large-scale workplace testing. Because kidney function may be reduced by 70 to 80% prior to a detectable elevation in serum creatinine, and because other existing tests are either impractical or costly, non-invasive biomarkers are needed to detect low-dose acute intermittent exposures to the kidney. A number of biomarkers for detecting low-dose kidney damage or early changes associated with carcinogenesis are discussed in the section on biomarkers.
Although the proximal tubule cells absorb 80% of the fluids, the countercurrent mechanism and the distal collecting ducts fine-tune the amount of fluids absorbed by regulating ADH. ADH is released from the pituitary gland deep within the brain and responds to osmotic pressures and fluid volume. Exogenous compounds such as lithium may damage the distal collecting ducts and result in renal diabetes insipidus (passage of dilute urine). Inherited genetic disorders may also cause this defect. Xenobiotics normally affect both kidneys but complexities of interpretation arise when exposures are difficult to document or when there is pre-existing renal disease. Consequently, high-dose accidental exposures have served as markers for identifying nephrotoxic compounds in many instances. The majority of occupational exposures occur at low doses, and are masked by the reserve filtration and repair compensatory capability (hypertrophy) of the kidney. The challenge which remains is to detect low-dose exposures clinically undetected by current methods.
Anatomy and Pathophysiology of the Bladder
The urinary bladder is a hollow pouch in which urine is stored; normally, it contracts on demand for controlled emptying through the urethra. The bladder is located in the front, lower part of the pelvic cavity. The bladder is joined on either side to the two kidneys by muscular, peristaltic tubes, the ureters, which carry the urine from the kidneys to the bladder. The renal pelvis, ureters and bladder are lined with transitional epithelium. The outer layer of the urothelium consists of umbrella cells coated with a carbohydrate, glycosaminoglycan (GAG), layer. The transitional cells extend to the basement membrane of the bladder. The deep basal cells are thus protected by the umbrella cells but if the protective GAG layer is damaged the basal cells are susceptible to injury from urinary components. The microanatomy of the transitional epithelium allows it to expand and contract, and even with normal shedding of the umbrella cells the protective integrity of the basal cells is maintained.
The balanced neurological system that regulates storage and emptying may be damaged during electroshock or other trauma, such as spinal cord injury, occurring in the workplace. A major cause of death among quadraplegics is loss of bladder function resulting in chronic renal damage secondary to infection and stone formation. Chronic infection from incomplete emptying due to neurogenic or obstructive causes such as pelvic fracture or other trauma to the urethra and subsequent stricture formation is common. Persistent bacterial infection or stone formation that results in chronic inflammatory and malignant conditions of the bladder may be caused by reduced resistance (i.e., susceptibility) to exogenous exposures in the workplace.
Molecules associated with damage and repair within the bladder serve as potential intermediate end-point markers for both toxic and malignant conditions because many biochemical alterations occur during the changes related to cancer development. Like the kidney, bladder cells have active enzyme systems such as the cytochrome P-450 which may activate or inactivate xenobiotics. The functional activity of the enzymes is determined by genetic inheritance and exhibits genetic polymorphism. Voided urine contains cells exfoliated from the kidney, ureters, bladder, prostate and urethra. These cells provide targets, through the use of biomarkers, for evaluating changes in bladder and renal pathology. Remembering Virchow’s comment that all diseases start in the cells focuses our attention on the importance of cells, which are the molecular mirror of exposure episodes.
Environmental and Occupational Toxicology
A considerable volume of epidemiological data supports the causal relationship of occupational exposures in bladder cancer, but the precise contributions of workplace exposures to kidney failure and kidney cancer are difficult to estimate. In a recent report, it was estimated that up to 10% of end-stage renal disease could be attributed to workplace exposures, but results are difficult to validate because of changing environmental and chemical hazards, variations in diagnostic criteria and the often long latency period between exposure and disease. It is estimated that function of two-thirds of the nephrons of both kidneys may be lost before renal damage is clinically evident. However, evidence is mounting that what were previously thought to be socioeconomic or ethnic causes of nephrotoxicity may in fact be environmental, adding validity to the role of toxicants in disease development.
Nephrotoxicity may be directly related to the xenobiotic, or the xenobiotic may go through a single-step or multi-step activation or inactivation in the kidney or the liver. Activation of xenobiotics is regulated by complex sets of enzymes identified as Phase I, II and Ancillary. One Phase I enzyme is the P-450 oxidative system which acts through reduction or hydrolysis pathways. Phase II enzymes catalyse conjugation while ancillary enzymes regulate drug metabolism (Table 1 lists these enzymes). Various animal models have provided insight into metabolic mechanisms, and studies of kidney slices and microdissection of the kidney nephron units in tissue culture add insight into the pathological mechanisms. However, species and individual variables are considerable and, although mechanisms may be similar, caution is mandated in extrapolating results to humans in the workplace. The primary issues now are to determine which xenobiotics are nephrotoxic and/or carcinogenic, and to what target sites, and to develop methods to identify more accurately subclinical toxicity in the renal-urinary system.
Table 1. Drug-metabolism enzymes in kidney1
| ENZYMES | ||
| Phase I | Phase II | Ancillary |
| Cytochrome P-450 | Esterase | GSH peroxides |
| Microsomal FAD-containing mono-oxygenase | N-Acetyltransferase | GSSG reductase |
| Alcohol and aldehyde dehydrogenases | GSH S-transferase | Superoxide dismutase |
| Epoxide hydrolase | Thiol S-methyl-transferase | Catalase |
| Prostaglandin synthase | UDP glucuronosyltransferase | DT-diaphorase |
| Monoamine oxidase | Sulphotransferase | NADPH-generating pathways |
1 Phase I enzymes catalyse oxidation, reduction or hydrolysis.
Phase II enzymes generally catalyse conjugation.
Ancillary enzymes function in a secondary or supporting manner to facilitate drug metabolism.
Source: National Research Council 1995.
Non-malignant Renal-Urinary Disorders
Glomerulonephritis is an inflammatory reactive condition of the glomerular basement membrane or capillary endothelium. Acute and chronic forms of the disease are caused by a variety of infectious, autoimmune or inflammatory conditions or by exposure to toxic agents. Glomerulonephritis is associated with vasculitis, either systemic or limited to the kidney. Secondary chronic damage to the glomerulus also occurs during an intense cycle of assault from nephrotoxicity to the interstitium of the tubule cells. Epithelial glomerular crescents or proliferative forms are a hallmark of glomerulonephritis in kidney biopsy specimens. Blood, red blood cell (RBC) casts, or protein in the urine, and hypertension are symptoms of glomerulonephritis. A change in blood proteins may occur with lowering of certain fractions of the serum complement, a complex set of interacting proteins involved in the immune system, host defenses and clotting functions. Direct and indirect evidence supports the significance of xenobiotics as a causal factor of glomerulonephritis.
The glomerulus protects the oxygen-carrying red blood cells from passing through its filter. After centrifugation, normal urine contains only one RBC in 10 ml when viewed with high-power light microscopy. When RBCs leak through the glomerular filter and perhaps become individually dysmorphic, RBC casts that assume the cylindrical shape of the collecting nephrons form.
In support of the importance of toxins as an aetiological factor in glomerulonephritis, epidemiological studies reveal increased evidence of toxic exposures in patients who have undergone dialysis or who have been diagnosed with glomerulonephritis. Evidence of glomerular injury from acute hydrocarbon exposure is rare, but has been observed in epidemiological studies, with odds ratios ranging from 2.0 to 15.5. One example of acute toxicity is Goodpasture’s disease which results from hydrocarbon stimulation of antibody production to liver and lung proteins that cross-react with the basement membrane. Exacerbation of nephrotic syndrome, large amounts of protein in the urine, has also been observed in individuals re-exposed to organic solvents, while other studies reveal an historic relationship with a spectrum of renal disorders. Other solvents such as degreasing agents, paints and glues are implicated in more chronic forms of the disease. Awareness of the mechanisms of solvent excretion and reabsorption assists in identifying biomarkers because even minimal damage to the glomerulus results in increased leakage of RBCs into the urine. Although RBCs in the urine are a cardinal sign of glomerular injury, it is important to rule out other causes of haematuria.
Interstitial and tubular nephritis. As mentioned previously, the aetiology of chronic end-stage renal disease is frequently difficult to ascertain. It may be primarily glomerular, tubular or interstitial in origin and occur because of multiple acute episodes or chronic, low-dose processes. Chronic interstitial nephritis involves fibrosis and tubular atrophy. In its acute form, the disease is expressed by marked inflammatory infiltrate with accompanying fluid collection in the interstitial spaces. Interstitial nephritis may involve primarily the interstitium, or be manifest as a secondary event from chronic tubular injury, or it may result from post-renal causes such as obstruction. Prostaglandin-A synthase, an enzyme, is found primarily in the interstitium and is associated with the endoplasmic reticulum, a part of the protein machinery of the cell. Certain xenobiotics, such as benzidine and nitrofuranes, are reducing co-substrates for prostaglandin synthase and are toxic to the tubular interstitium.
Tubular and interstitial injury may occur from exposure to cadmium, lead or a variety of organic solvents. Most of the exposures are chronic, low-dose and toxicity is masked by the renal function reserve and the ability of the kidney to recover some functions. Interstitial nephritis may also result from vascular injury as caused, for example, by chronic carbon monoxide exposure. Proximal tubule cells are the most vulnerable to toxic substances in the blood because of intense exposure to toxins which filter through the glomerulus, internal enzyme systems that activate toxicants and the selective transport of toxicants. The epithelium in the various segments of the proximal tubule has slightly different qualities of lysosomal peroxidase enzymes and other compounds of genetic machinery. Thus, chromium exposure may result in both interstitial and tubular injury. Damage to the collecting tubules may occur when specific enzymes activate various xenobiotics such as chloroform, acetaminophen and p-aminophenol, and antibiotics such as Loradine. A secondary result of damage to the collecting ducts is the inability of the kidney to acidify the urine and the subsequent development of a metabolic acid state.
Nephrogenic diabetes insipidus, the condition in which urine becomes dilute, may be genetic or acquired. The genetic form involves mutations of the ADH receptors which are located on the basal lateral membrane of the collecting ducts, in the descending loop of Henle. ADH fine-tunes the reabsorption of water and certain ions such as potassium. Acquired diabetes insipidus may involve the tubule cells or the associated interstitium, both of which may be diseased because of a variety of conditions. Nephrogenic diabetes insipidus may accompany end-stage renal disease because of diffuse involvement of the interstitium. Consequently, the interstitium is unable to maintain a hypertonic environment for passive water movement from the tubular collecting ducts. Conditions which may cause diffuse interstitial changes are pyelonephritis, sickle cell anaemia and obstructive uropathy. The possible association of these conditions in relation to occupational exposure is an increased susceptibility of the kidney to xenobiotics. A limited number of nephrotoxic compounds have been identified that especially target the collecting tubule cells. Frequency, nocturia (more frequent voiding at night) and polydipsia (chronic thirst) are symptoms of nephrogenic diabetes insipidus. Movement of fluids through the collecting duct cells results in channels that form in response to ADH, affecting the microtubular function of the cells; consequently, drugs such as colchicine may affect the ADH. Two drugs which appear to act by slightly different mechanisms to correct ADH are hydrochlorothiazide and indomethacin, a prostaglandin synthase inhibitor.
Lithium-induced diabetes insipidus correlates with the duration of lithium therapy, average serum lithium level and total lithium carbonate dose. Interestingly, lithium concentrates in the collecting ducts and affects cyclic AMP, part of the energy metabolic pump pathway. Exposure to other compounds such as methoxyflurane and demeclocycline, the latter of which is used for the treatment of acne, also results in nephrogenic diabetes insipidus through an alternative pathway rendering the epithelial cells unresponsive to ADH.
Hypertension, or elevated blood pressure, the second most common cause of end-stage renal disease, is associated with multiple aetiological pathways. Hypertension can be caused by diabetic nephropathy, obstructive nephropathy, glomerulonephritis, polycystic kidney disease, pyelonephritis and vasculitis, and many of those diseases are associated with exposure to toxic compounds. A limited number of occupational exposures are directly associated with hypertension. One is lead, which causes renal vascular ischaemia and injury. The mechanism for lead-induced hypertension is probably regulated through the juxtaglomerular apparatus, the release of renin and the cleavage of renin by liver enzymes to angiotensin II. Drugs implicated in hypertension include amphetamines, oestrogens and oral contraceptives, steroids, cis-platinum, alcohol and tricyclic antidepressants. Hypertension may be gradual in onset or acute and malignant in nature. Malignant hypertension in which diastolic pressure is greater than 110 mm Hg is associated with nausea, vomiting and severe headache, and constitutes a medical emergency. Numerous drugs are available for the treatment of hypertension but over-treatment may result in decreased renal perfusion and a further loss of renal function. Whenever possible, withdrawal of the nephrotoxicant is the treatment of choice.
Differential diagnosis of haematuria and proteinuria
Haematuria (RBCs in the urine) and pyuria (white blood cells in the urine) are primary symptoms of many diseases of the renal-urinary system, and for categorical purposes may be considered non-specific cellular biomarkers. Because of their importance they are discussed separately here. A challenge to the occupational practitioner is to determine if haematuria signifies a permanent underlying medical condition that may be potentially life threatening or if it is attributable to occupational exposures. Clinical assessment of haematuria requires standardization and determination of whether it is pre-renal, renal or post-renal in origin.
Haematuria may be derived from lesions in the kidney per se or anywhere along the pathway of voided urine. Sites of origin include the kidney, collecting renal pelvis, ureters, bladder, prostate and urethra. Because of the serious diseases associated with haematuria, a single episode warrants a medical or urological evaluation. Greater than one RBC per high-power field can be a signal of disease, but significant haematuria may be missed on microscopic analysis in the presence of hypotonic (dilute) urine which may lyse RBCs. Pseudo-haematuria may be caused by beets, berries, vegetable dyes and concentrated urates. Initial haematuria suggests a urethral origin, terminal haematuria is usually prostatic in origin, and blood throughout voiding is from the bladder, kidney or ureter. Gross haematuria is associated with bladder tumours in 21% of the cases, but microscopic haematuria is much less frequently associated (2.2 to 12.5%).
Finding dysmorphic cells when haematuria is quantitatively assessed suggests an upper tract origin, particularly when associated with red blood cell casts. Understanding haematuria in relation to proteinuria provides additional information. The glomerular filtration device almost completely excludes proteins of a molecular weight greater than 250,000 Daltons, while low molecular weight proteins are freely filtered and absorbed normally by the tubule cells. The presence of high molecular weight proteins in the urine suggests lower tract bleeding while low molecular weight proteins are associated with tubular injury. Evaluation of the ratio of α-microglobulin to albumin and α-macroglobulin to albumin helps delineate glomerular from tubular interstitial nephropathy and lower tract bleeding potentially associated with urothelial neoplasia and other post-renal causes such as urinary tract infections.
A special diagnostic problem arises when two or more disease processes that cause the same symptoms are present concurrently. For example, haematuria is seen in both urothelial neoplasia and urinary tract infections. In a patient with both diseases, if the infection is treated and resolved, the cancer would remain. Therefore, it is important to identify the true cause of the symptoms. Haematuria is present in 13% of screened populations; approximately 20% of individuals have significant renal or bladder disorders and 10% of those will go on to develop genitourinary malignancy. Consequently, haematuria is an important biomarker of disease that must be appropriately evaluated.
Clinical interpretation of haematuria is enhanced by a knowledge of the patient’s age and sex, as indicated in Table 2 which shows causes of haematuria relative to the age and sex of the patient. Other causes of haematuria include renal vein thrombosis, hypercalcuria and vasculitis, as well as trauma such as jogging or other sports, and occupational events or exposures. Clinical evaluation of haematuria requires an x ray of the kidney, intravenous pyelogram (IVP), to rule out upper tract diseases including kidney stones and tumours, and a cystoscopy (looking into the bladder through a lighted instrument) to exclude bladder, prostate or urothelial cancers. Subtle vaginal causes must be excluded in women. Regardless of a patient’s age, a clinical evaluation is indicated if haematuria occurs and, depending on the identified aetiology, sequential follow-up evaluations may be indicated.
Table 2. The most common causes of haematuria, by age and sex
| 0–20 Years | 40–60 Years (females) |
| Acute glomerulonephritis Acute urinary tract infection Congenital urinary tract anomalies with obstruction |
Acute urinary tract infection Stones Bladder tumour |
| 20–40 Years | 60+Years (males) |
| Acute urinary tract infection Stones Bladder tumour |
Benign prostatic hyperplasia Bladder tumour Acute urinary tract infection |
| 40–60 Years (males) | 60+Years (females) |
| Bladder tumour Stones Acute urinary tract infection |
Bladder tumours Acute urinary tract infection |
Source: Wyker 1991.
The use of recently identified biomarkers in conjunction with conventional cytology for evaluation of haematuria helps to assure that no occult or incipient malignancy is missed (see next section on biomarkers). For the occupational specialist, determining whether haematuria is a result of toxic exposure or occult malignancy is important. Knowledge of exposure and the patient’s age are critical parameters for making an informed clinical management decision. A recent study has demonstrated that together haematuria and biomarker analysis on exfoliated urinary cells from the bladder were the two best markers for detecting premalignant bladder lesions. Haematuria is observed in all cases of glomerular injury, in only 60% of patients with bladder cancer and in only 15% of patients with malignancies of the kidney itself. Thus, haematuria remains a cardinal symptom of renal and post-renal disease, but the final diagnosis may be complex.
Tests for nephrotoxicity: biomarkers
Historically, monitoring of toxins in the work environment has been the primary method of identifying risk. However, not all toxicants are known and, therefore, cannot be monitored. Also, susceptibility is a factor in whether xenobiotics will affect individuals.
Figure 2. Categories of biomarkers.
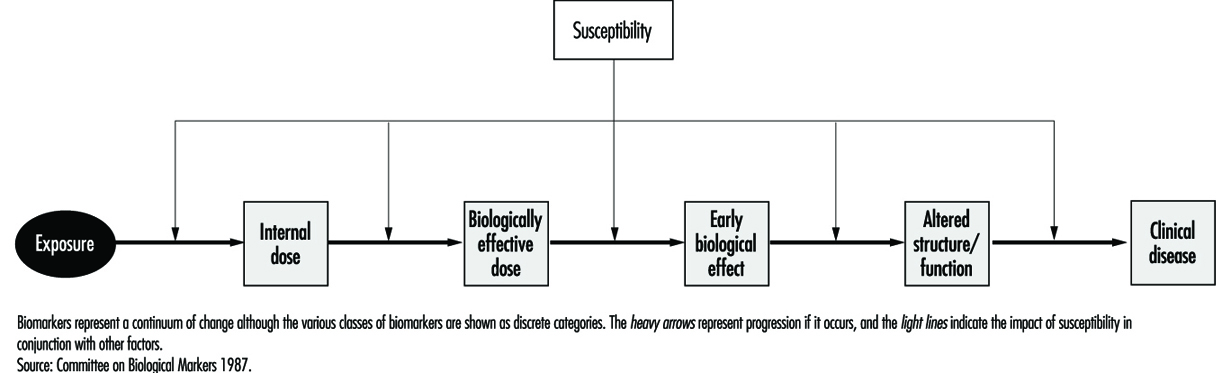
Biomarkers provide new opportunities for defining individual risk. For descriptive purposes and to provide a framework for interpretation, biomarkers have been classified according to the schema depicted in Figure 2. As in other diseases, biomarkers of nephrotoxicity and genitourinary toxicity may be related to susceptibility, exposure, effect or disease. Biomarkers may be genotypic or phenotypic, and may be functional, cellular or soluble in urine, blood or other body fluids. Examples of soluble markers are proteins, enzymes, cytokines and growth factors. Biomarkers may be assayed as the gene, message or protein product. These variable systems add to the complexity of biomarker evaluation and selection. One advantage of assaying the protein is that it is the functional molecule. The gene may not be transcribed and the quantity of message may not correspond to the protein product. A list of criteria for biomarker selection is shown in Table 3.
Table 3. Criteria for biomarker selection
| Clinical utility | Assay considerations |
| Strong biomarker | Stability of reagent |
| Sensitivity | Cost of reagent |
| Specificity | Fixation requirements |
| Negative predictive value | Reproducibility of the assay |
| Positive predictive value | Machine sensible parameters |
| Functional role | Contribution to biomarker profile |
| Sequence in oncogenesis | Adaptability to automation |
Source: Hemstreet et al. 1996.
The international scientific commitment to map the human genome made possible by advances in molecular biology established the basis for identifying biomarkers of susceptibility. Most instances of human disease, especially those resulting from environmental exposure to toxicants, involve a constellation of genes reflecting marked genetic diversity (genetic polymorphism). An example of such a gene product, as mentioned previously, is the P-450 oxidative enzyme system which may metabolize xenobiotics in the liver, kidney or bladder. Susceptibility factors may also control the basic mechanism for DNA repair, influence the susceptibility of various signalling pathways important to tumourigenesis (i.e., growth factors) or be related to inherited conditions that predispose to disease. An important example of an inherited susceptibility factor is the slow or fast acetylation phenotype that regulates the acetylation and inactivation of certain aromatic amines known to cause bladder cancer. Biomarkers of susceptibility may include not only genes that regulate the activation of xenobiotics but also proto-oncogenes and suppressor-oncogenes. The control of tumour cell growth involves a number of complex, interacting systems. These include a balance of positive (proto) oncogenes and negative (suppressor) oncogenes. Proto-oncogenes control normal cell growth and development, while suppressor-oncogenes control normal cellular division and differentiation. Other genes may contribute to pre-existing conditions such as a propensity to renal failure triggered by underlying conditions such as polycystic kidney disease.
A biomarker of exposure may be the xenobiotic itself, the metabolic metabolite or markers such as DNA adducts. In some instances the biomarker may be bound to a protein. Biomarkers of exposure may also be biomarkers of effect, if the effect is transient. If a biomarker of effect persists, it may become a biomarker of disease. Useful biomarkers of effect have a high association with a toxicant and are indicative of exposure. For disease detection, expression of the biomarker in close sequence to the onset of disease will have the highest specificity. The expected sensitivity and specificity of a biomarker depends on the risk versus benefit of the intervention. For instance, a biomarker such as F-actin, a cytoskeletal protein differentiation marker, that appears altered in early carcinogenesis may have a poor specificity for detection of pre-cancerous states because not all individuals with an abnormal marker will progress to disease. It may, however, be useful for selecting individuals and monitoring them while undergoing chemoprevention, provided the therapy is non-toxic. Understanding the time-frame and functional linkage between individual biomarkers is extremely important to individual risk assessment and to comprehending the mechanisms of carcinogenesis and nephrotoxicity.
Biomarkers of nephrotoxicity
Biomarkers of nephrotoxicity may be related to the aetiology of kidney failure (i.e., pre-renal, renal or post-renal) and the mechanisms involved in the pathogenesis of the process. This process includes cellular damage and repair. Toxic injury can affect the cells, glomerulus, interstitium or tubules with release of corresponding biomarkers. Xenobiotics may affect more than one compartment or may cause biomarker changes because of the interdependence of cells within the compartment. Inflammatory changes, autoimmune processes and immunological processes further promote the release of biomarkers. Xenobiotics may target one compartment in some circumstances and another under different conditions. One example is mercury which is, acutely, nephrotoxic to the proximal tubule while chronically it affects the arterioles. Response to injury can be divided into several major categories including hypertrophy, proliferation, degeneration (necrosis and apoptosis, or programmed cell death) and membrane alterations.
The majority of susceptibility factors are related to non-xenobiotic-associated renal disease. However, 10% of renal failure cases are attributed to environmental exposures to toxic compounds or iatrogenic induction by various compounds, such as antibiotics, or procedures such as administration of kidney x-ray contrast to a diabetic. In the workplace, identifying subclinical renal failure prior to potential additional nephrotoxic stress has potential practical utility. If a compound is suspected to be xenobiotic and it results in an effect specifically in the causal pathway of disease, intervention to reverse the effect is a possibility. Thus, biomarkers of effect eliminate many of the problems of calculating exposure and defining individual susceptibility. Statistical analysis of biomarkers of effect in relation to biomarkers of susceptibility and exposure should improve marker specificity. The more specific the biomarker of effect the less the requirement for a large sample size required for scientifically identifying potential toxins.
Biomarkers of effect are the most important class of markers and link exposure to susceptibility and disease. We have previously addressed the combining of cellular and soluble biomarkers to differentiate between haematuria originating in the upper tract or the lower tract. A list of soluble biomarkers potentially related to cellular nephrotoxicity is shown in Table 4. To date, none of these alone or as multiple biomarker panels detects subclinical toxicity with adequate sensitivity. Some problems with using soluble biomarkers are lack of specificity, enzyme instability, the dilutional effect of urine, variations in renal function, and non-specific protein interactions that may cloud the specificity of analysis.
Table 4. Potential biomarkers linked to cell injury
|
Immunological factors: -Humoral-antibodies and antibody fragments; components of complement cascade, and coagulation factors -Cellular-lymphocytes, mononuclear phagocytes, and other marrow- derived effectors (oesinophils, basophils, neutrophils and platelets) Lymphokines Major histocompatibility antigens Growth factors and cytokines: platelet- derived growth factor, epidermal growth factor, transforming growth factor (TGF), tumour-necrosis factor, interleukin-1, etc. Lipid mediators: prostaglandins Endothelin |
Extracellular-matrix components: -Collagens -Procollagen -Laminin -Fibronectin Reactive oxygen and nitrogen species Transcription factors and proto-oncogenes: c-myc, c-fos, c-jun, c-Haras, c-Ki-ras, and Egr-1 Heat shock proteins |
Source: Finn, Hemstreet et al. in National Research Council 1995.
One soluble growth factor with potential clinical application is urinary epidermal growth factor (EGF) which may be excreted by the kidney and is also altered in patients with transitional cell carcinoma of the bladder. Quantitation of urinary enzymes has been investigated but the usefulness of this has been limited by the inability to determine the origin of the enzyme and lack of assay reproducibility. The use of urinary enzymes and their widespread acceptance has been slow because of the restrictive criteria mentioned previously. Enzymes evaluated include alaminopeptidase, NAG and intestinal alkaline phosphatase. NAG is perhaps the most widely accepted marker for monitoring proximal tubule cell injury because of its localization in the S3 segment of the tubule. Because the precise cell of origin and pathological cause of urinary enzyme activity are unknown, interpretation of results is difficult. Furthermore, drugs, diagnostic procedures and co-existing diseases such as myocardial infarction may cloud the interpretation.
An alternative approach is to use monoclonal antibody biomarkers to identify and quantitate tubular cells in urine from various areas of the nephron segment. The utility of this approach will depend on maintaining the integrity of the cell for quantification. This requires appropriate fixation and sample handling. Monoclonal antibodies are now available which target specific tubule cells and distinguish, for example, proximal tubule cells from distal tubule cells or convoluted tubule cells. Transmission microscopy cannot effectively resolve differences between leukocytes and various types of tubule cells in contrast to electron microscopy which has been effective in detecting transplant rejection. Techniques such as high-speed quantitative fluorescence image analysis of tubular cells stained with monoclonal antibodies should solve this problem. In the near future, it should be possible to detect subclinical nephrotoxicity with a high degree of certainty as exposure occurs.
Biomarkers of malignant disease
Solid cancers arise in many cases from a field of biochemically altered cells which may or may not be histologically or cytologically altered. Technologies such as quantitative fluorescence image analysis capable of detecting biomarkers associated with premalignant conditions with certainty provide the horizon for targeted chemoprevention. Biochemical alterations may occur in a varied or ordered process. Phenotypically, these changes are expressed by a gradual morphological progression from atypia to dysplasia and finally to overt malignancy. Knowledge of the “functional role” of a biomarker and “when in the sequence of tumorigenesis it is expressed” assists in defining its utility for identifying premalignant disease, for making an early diagnosis and for developing a panel of biomarkers to predict tumour recurrence and progression. A paradigm for biomarker evaluation is evolving and requires the identification of single and multiple biomarker profiles.
Bladder cancer appears to develop along two separate pathways: a low-grade pathway seemingly associated with alterations on chromosome 9 and a second pathway associated with P-53 suppressor gene genetically altered on chromosome 17. Clearly, multiple genetic factors are related to cancer development, and defining the genetic factors in each individual is a difficult task, particularly when the genetic pathway must be linked to a complexity of perhaps multiple exposures. In epidemiological studies, exposures over prolonged intervals have been difficult to reconstruct. Batteries of phenotypic and genotypic markers are being identified to define individuals at risk in occupational cohorts. One profile of phenotypic biomarkers and their relationship to bladder cancer is shown in Figure 3, which illustrates that G-actin, a precursor protein to the cytoskeletal protein F-actin, is an early differentiation marker and may be followed by sequential alterations of other intermediate end-point markers such as M344, DD23 and DNA ploidy. The strongest biomarker panels for detecting premalignant disease and overt cancer, and for prognostication, remain to be determined. As machine-sensible biochemical criteria are defined it may be possible to detect disease risk at prescribed points in the disease continuum.
Figure 3. Four biomarkers, G-actin, P-300, DD23 and DNA, in relation to tumour progression and response to surgical treatment and chemoprevention.
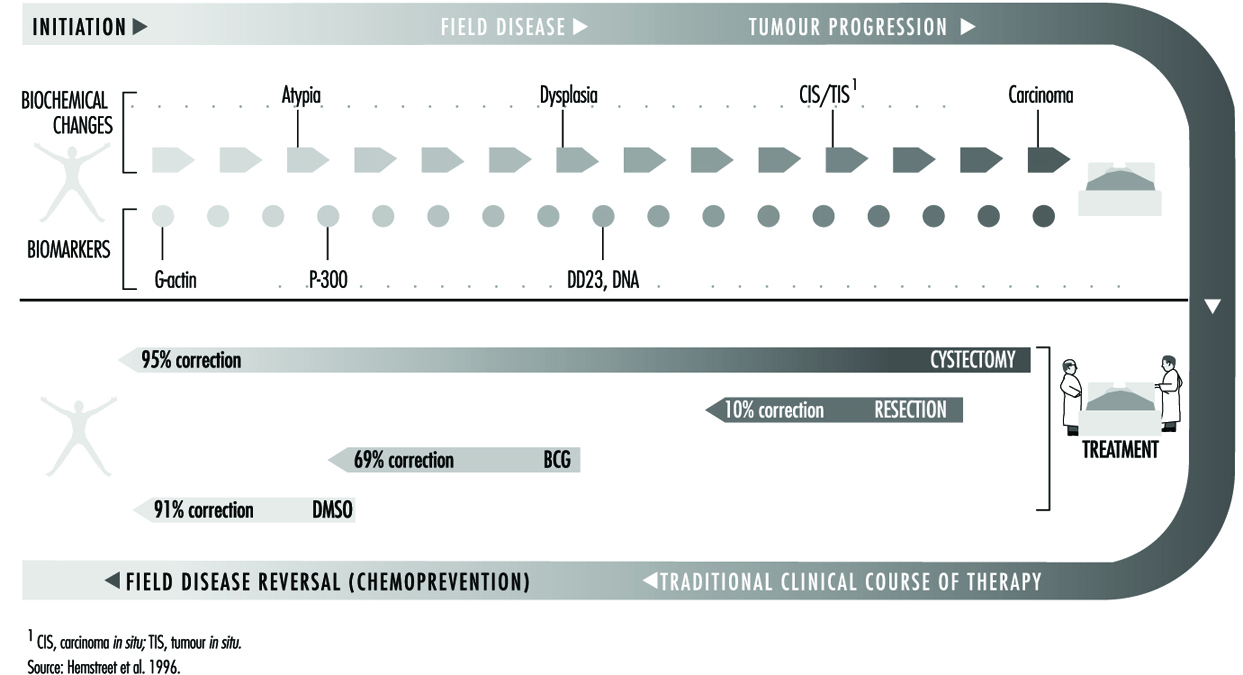
Diagnosis and management of work-relatedrenal-urinary disease
Pre-existing renal disease
Changes in health care delivery systems worldwide bring into focus issues of insurability and protection of workers from additional exposure. Significant pre-existing renal disease is manifest by increased serum creatinine, glucosuria (sugar in the urine), proteinuria, haematuria and dilute urine. Immediately ruling out systemic underlying causes such as diabetes and hypertension is required, and depending on the age of the patient other congenital aetiologies such as multiple cysts in the kidney should be investigated. Thus, the urinalysis, both dipstick and microscopic evaluations, for detection of biochemical and cellular alterations, is useful to the occupational physician. Tests of serum creatinine and creatinine clearance are indicated if significant haematuria, pyuria or proteinuria suggests underlying pathology.
Multiple factors are important to assess risk for progression of chronic disease or acute kidney failure. The first is inherent or acquired limitation of the kidney to resist xenobiotic exposure. The kidney’s response to the nephrotoxicant, such as an increase in the amount of toxicant absorbed or alterations in kidney metabolism, may be influenced by a pre-existing condition. Of particular importance is a decrease in detoxifying function in the very young or the very old. In one study susceptibility to occupational exposure was correlated highly with family history of renal disease, signifying the importance of hereditary predisposition. Underlying conditions, such as diabetes and hypertension, increase susceptibility. Rare conditions, such as lupus erythematosis and vasculitis, may be additional susceptibility factors. In the majority of cases, increased susceptibility is multifactorial and frequently involves a battery of insults which occur either alone or simultaneously. Thus, the occupational physician should be cognizant of the patient’s family history of renal disease and pre-existing conditions affecting renal function, as well as any vascular or cardiac disease, particularly in older workers.
Acute renal failure
Acute renal failure may arise from pre-renal, renal, or post-renal causes. The condition is usually caused by an acute insult resulting in rapid, progressive loss of kidney function. When the nephrotoxicant or precipitating causal factor is removed there is a progressive return of renal function with a gradual decline of serum creatinine and improved renal concentrating ability. A listing of occupational causes of acute renal failure is shown in Table 5. Acute renal failure from high-dose xenobiotic exposure has been useful to signal potential aetiological causes that may also contribute to more chronic forms of progressive renal disease. Acute renal failure from obstruction of the outflow tract caused by benign disease or malignancy is relatively rare, but surgical causes may contribute more frequently. Ultrasound of the upper tract delineates the problem of obstruction, whatever the contributing factor. Renal failure associated with drug or occupational toxicants results in a mortality rate of approximately 37%; the remainder of affected individuals improve to various degrees.
Table 5. Principal causes of acute renal insufficiency of occupational origin
| Renal ischaemia | Tubular necrosis | Haemoglobinuria, myoglobinuria |
| Traumatic shock Anaphylactic shock Acute carbon monoxide poisoning Heat stroke |
Mercury Chromium Arsenic Oxalic acid Tartrates Ethylene glycol Carbon tetrachloride Tetrachlorethane |
Arsine Crush syndrome Struck by lightning |
Source: Crepet 1983.
Acute renal failure may be attributed to a variety of pre-renal causes which have as an underlying theme renal ischaemia resulting from a prolonged decreased renal perfusion. Cardiac failure and renal artery obstruction are two examples. Tubular necrosis may be caused by an ever-growing number of nephrotoxicants present in the workplace. Herbicides and pesticides have all been implicated in a number of studies. In a recent report, hemlock poisoning resulted in the deposition of the myosin and actin from the breakdown of muscle cells in the tubules and an acute decrease in renal function. Endosulfan, an insecticide, and triphenyltin acetate (TPTA), an organotin, both were initially classified as neurotoxins but have recently been reported to be associated with tubular necrosis. Anecdotal reports of additional cases bring into perspective the need for finding biomarkers to identify more subtle subclinical toxicants that may not yet have resulted in high-dose toxic exposures.
Signs and symptoms of acute renal failure are: no urine output (anuria); oliguria (decreased urine output); decreased renal concentrating capacity; and/or a rising serum potassium that may stop the heart in a relaxed state (diastolic arrest). Treatment involves clinical support and, whenever possible, removal from exposure to the toxicant. Rising serum potassium or excessive fluid retention are the two primary indicators for either haemodialysis or peritoneal dialysis, with the choice dependent on the patient’s cardiovascular stability and vascular access for haemodialysis. The nephrologist, a medical kidney specialist, is key in the management strategy for these patients who may also require the care of a urological surgical specialist.
Long-term management of patients following renal failure is largely dependent on the degree of recovery and rehabilitation and the patient’s overall health status. A return to limited work and avoiding conditions that will stress the underlying condition are desirable. Patients with persistent haematuria or pyuria require careful monitoring, possibly with biomarkers, for 2 years following recovery.
Chronic renal disease
Chronic or end-stage renal disease is most frequently the result of a chronic, ongoing subclinical process that involves a multiplicity of factors most of which are poorly understood. Glomerulonephritis, cardiovascular causes and hypertension are major contributing factors. Other factors include diabetes and nephrotoxicants. Patients present with progressive elevations in serum blood urea nitrogen, creatinine, serum potassium and oliguria (decreased urine output). Improved biomarkers or biomarker panels are needed to identify more precisely subclinical nephrotoxicity. For the occupational practitioner, the methods of assessment need to be non-invasive, highly specific and reproducible. No single biomarker has as yet met these criteria to become practical on a large clinical scale.
Chronic renal disease may result from a variety of nephrotoxicants, the pathogenesis of which is better understood for some than others. A list of nephrotoxicants and sites of toxicity is shown in Table 6. As mentioned, toxins may target the glomerulus, segments of the tubules or the interstitial cells. Symptoms of xenobiotic exposure may include haematuria, pyuria, glucosuria, amino acids in the urine, frequent urination and decreased urine output. The precise mechanisms of renal damage for many nephrotoxicants have not been defined but the identification of specific biomarkers of nephrotoxicity should assist in addressing this problem. Although some protection of the kidney is afforded by the prevention of vasoconstriction, tubular injury persists in most cases. As an example, lead toxicity is primarily vascular in origin, while chromium at low doses affects the proximal tubule cells. These compounds appear to affect the metabolic machinery of the cell. Multiple forms of mercury have been implicated in acute elemental nephrotoxicity. Cadmium, in contrast to mercury and like many other occupational nephrotoxicants, first targets the proximal tubule cells.
Table 6. Segments of the nephron affected by selected toxicants
|
Proximal tubule Antibiotics -Cephalosporins Aminoglycosides Antineoplastics -Nitrosoureas -Cisplatin and analogs Radiographic contrast agents Halogenated hydrocarbons -Chlorotrifluoroethylene -Hexafluropropene -Hexachlorobutadiene -Trichloroethylene -Chloroform -Carbon tetrachloride Maleic acid Citrinin Metals -Mercury -Uranyl nitrate -Cadmium -Chromium |
Glomerulus Immune complexes Aminoglycoside antibiotics Puromycin aminonucleoside Adriamycin Penicillamine Distal tubule/collecting duct -Lithium -Tetracyclines -Amphotericin -Fluoride -Methoxyflurane
Papilla -Aspirin -Phenacetin -Acetaminophen -Non-steroidal anti-inflammatory agents -2-Bromoethylamine |
Source: Tarloff and Goldstein 1994.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."