- You are here:
-
Home

-
Part XVII. Services and Trade
-
Transport Industry and Warehousing
- Air Transport
Sculpture
In ancient times, the art of sculpture included engraving and carving of stone, wood, bone and other materials. Later, sculpture developed and refined modelling techniques in clay and plaster, and moulding and welding techniques in metals and glass. During the last century various additional materials and techniques have been used for the art of sculpture, including plastic foams, paper, found materials and several sources of energy such as light, kinetic energy and so on. The aim of many modern sculptors is to involve the viewer actively.
Sculpture often utilizes the natural colour of the material or treats its surface to achieve a certain colour or to emphasize the natural characteristics or to modify the light reflections. Such techniques belong to the finishing touches of the art piece. Health and safety risks for artists and their assistants arise from the characteristics of the materials; from the use of tools and equipment; from the various forms of energy (mainly electricity) used for the functioning of tools; and from heat for welding and fusing techniques.
Artists’ lack of information and their focusing on the work lead to underestimating the importance of safety; this can result in serious accidents and the development of occupational diseases.
The risks are sometimes linked to the design of the workplace or to the organization of the work (e.g., carrying out many working operations at the same time). Such risks are common to all workplaces, but in the arts and crafts environment they can have more serious outcomes.
General Precautions
These include: appropriate design of the studio, considering the type of power sources employed and the placement and movement of the artistic material; segregation of hazardous operations controlled with adequate warning displays; installation of exhaust systems for control and removal of powders, gases, fumes, vapours and aerosols; use of well-fitted and convenient personal protective equipment; efficient clean-up facilities, such as showers, sinks, eye-wash fountains and so on; knowledge of the risks associated with the use of chemical substances and of the regulations that govern their use, in order to avoid or at least reduce their potential harm; keeping informed on the possible risks of accidents and on hygiene regulations and being trained in first aid and. Local ventilation to remove airborne dust is necessary at its source, when it is produced in abundance. Daily vacuum cleaning, either wet or dry, or wet mopping of the floor and of work surfaces is highly recommended.
Main Sculpturing Techniques
Stone sculpture involves carving hard and soft stones, precious stones, plaster, cement and so on. Sculpture shaping involves work on more pliable materials—plaster and clay modelling and casting, wood sculpture, metalworking, glassblowing, plastic sculpture, sculpture in other materials and mixed techniques. See also the articles “Metalworking” and “Woodworking”. Glassblowing is discussed in the chapter Glass, ceramics and related materials.
Stone sculptures
Stones used for sculpture can be divided into soft stones and hard stones. The soft stones can be worked manually with tools such as saws, chisels, hammers and rasps, as well as with electric tools.
Hard stones such as granite, and other materials, such as cement blocks, can be used to create works of art and ornaments. This involves working with electric or pneumatic tools. The final stages of the work can be partially executed by hand.
Risks
Prolonged inhalation of high quantities of certain stone dusts containing free crystalline silica, which comes out of freshly cut surfaces, can lead to silicosis. Electric and pneumatic tools can cause a higher concentration in the air of dust which is finer than that produced by manual tools. Marble, travertine and limestone are inert materials and not pathogenic to the lungs; plaster (calcium sulphate) is irritating to the skin and to the mucous membranes.
Asbestos fibre inhalation, even in small quantities, can lead to a risk of lung cancer (laryngeal, tracheal, bronchial, lung and pleural malignancies) and probably also cancer of the digestive tract and of other organ systems. Such fibres can be found as impurities in serpentine and in talc. Asbestosis (fibrosis of the lung) can be contracted only through the inhalation of high doses of asbestos fibres, which is unlikely at this type of work. See table 1 for a list of the hazards of common stones.
Table 1. Hazards of common stones.
|
Hazardous ingredient |
Stones |
|
Free crystalline silica
|
Hard stones: Granites, basalt, jasper, porphyry, onyx, pietra serena |
|
Soft stones: steatite (soapstone), sandstone, slate, clays, some limestone |
|
|
Possible asbestos contamination |
Soft stones: soapstone, serpentine |
|
Free silica and asbestos
|
Hard stones: marble, travertine |
|
Soft stones: alabaster, tufa, marble, plaster |
High noise levels can be produced by the use of pneumatic hammers, electric saws and sanders, as well as manual tools. This can result in hearing loss and other effects on the autonomic nervous system (increase of heart rate, gastric disturbances and so on), psychological problems (irritability, attention deficits and so on), as well as general health problems, including headaches.
The use of electric and pneumatic tools can provoke damage to finger micro-circulation with the possibility of Raynaud’s phenomenon, and facilitate degenerative phenomena to the upper arm.
Work in difficult positions and lifting heavy objects can produce low-back pain, muscle strains, arthritis and joint bursitis (knee, elbow).
The risk of accidents is frequently connected with the use of sharp tools moved by powerful forces (manual, electric or pneumatic). Often stone splinters are violently shot into the working environment during the breaking of stones; falling or rolling of improperly fixed blocks or surfaces also occurs. The use of water can lead to slipping on wet floors, and to electric shocks.
Pigment and colourant substances (especially of spray type) used to cover the final layer (paints, lakes) expose the worker to the risk of inhalation of toxic compounds (lead, chromium, nickel) or of irritating or allergenic compounds (acrylic or resins). This can affect the mucous membranes as well as the respiratory tract.
Inhalation of evaporating paints solvents in high quantities over the course of the working day or in lower concentrations for longer periods, can provoke acute or chronic toxic effects on the central nervous system.
Precautions
Alabaster is a safer substitute for soapstone and other hazardous soft stones.
Pneumatic or electric tools with portable dust collectors should be used. The working environment should be cleaned frequently using vacuum cleaners or wet mopping; adequate general ventilation must be provided.
The respiratory system can be protected from the inhalation of dusts, solvents and aerosol vapours through use of proper respirators. Hearing can be protected with ear plugs and eyes can be protected with proper goggles. To reduce the risk of hand accidents leather gloves (when necessary) or lighter rubber gloves, lined with cotton, should be used to prevent contact with chemical substances. Anti-slipping and safety shoes should be used to prevent damage to the feet caused by the possible fall of heavy objects. During complicated and long operations, proper clothes should be worn; ties, jewellery and clothes which could easily get stuck in the machines should not be worn. Long hair should be put up or under a cap. A shower should be taken at the end of every work period; work clothes and shoes should never be taken home.
Pneumatic tool compressors should be placed out of the work area; noisy areas should be insulated; numerous breaks should be taken in warm areas during the working day. Pneumatic and electric tools equipped with comfortable handles (better if equipped with mechanical shock absorbers) which are able to direct the air away from the hands of the operator should be used; stretching and massage are suggested during the work period.
Sharp tools should be operated as far as possible from hands and body; broken tools should not be used.
Flammable substances (paints, solvents) must be kept far from flames, lit cigarettes and heat sources.
Sculpture shaping
The most common material used for sculpture shaping is clay (mixed with water or naturally soft clay); wax, plaster, concrete and plastic (sometimes reinforced with glass fibres) are also commonly used.
The facility with which a sculpture is shaped is directly proportional to the malleability of the material used. A tool (wood, metal, plastic) is often used.
Some materials, such as clays, can become hard after being heated in a furnace or kiln. Also, talc can be used as semi-liquid clay (slip), which can be poured into moulds and then fired in a kiln after drying.
These types of clays are similar to those used in the ceramic industry and may contain considerable amounts of free crystalline silica. See the article “Ceramics”.
Non-hardening clays, such as plasticine, contain fine particles of clays mixed with vegetable oils, preservatives and sometimes solvents. The hardening clays, also called polymer clays, are actually formed with polyvinyl chloride, with plasticizing materials such as various phthalates.
Wax is usually shaped by pouring it into a mould after it is heated, but it can also be formed with heated tools. Wax can be of natural or synthetic compounds (coloured waxes). Many types of waxes can be dissolved with solvents such as alcohol, acetone, mineral or white spirits, ligroin and carbon tetrachloride.
Plaster, concrete and papier mâché have different characteristics: it is not necessary to heat or to melt them; they are usually worked on a metal or fibreglass frame, or cast in moulds.
Plastic sculpture techniques can be divided into two main areas:
- work with already polymerized materials (casting, plate or sheet). They can be heated, softened, glued, cut, refined, refurbished and so on.
- work with non-polymerized plastic. The material is worked with monomers, obtaining a chemical reaction leading to polymerization.
Plastics can be formed by polyester, polyurethane, amino, phenolic, acrylic, epoxy and silicon resins. During polymerization, they can be poured into moulds, applied by hand layup, printed, laminated and skimmed by using catalyzers, accelerators, hardeners, loads and pigments.
See table 2 for a list of the hazards and precautions for common sculpture shaping materials.
Table 2. Main risks associated with material used for sculpture shaping.
|
Materials |
Hazards and precautions |
|
Clays
|
Hazards: Free crystalline silica; talc can be contaminated by asbestos; during heating operations, toxic gases can be released. |
|
Precautions: See “Ceramics”. |
|
|
Plasticine
|
Hazards: Solvents and preservatives can cause irritation to skin and mucous and allergic reactions in certain individuals. |
|
Precautions: Susceptible individuals should find other materials. |
|
|
Hard clays
|
Hazards: Some hardening or polymer clay plasticizers (phthalates) are possible reproductive or carcinogen toxins. During heating operations, hydrogen chloride can be released, especially if overheated. |
|
Precautions: Avoid overheating or using in an oven also used for cooking. |
|
|
Waxes
|
Hazards: Overheated vapours are flammable and explosive. Acrolein fumes, produced by decomposition from overheating wax, are strong respiratory irritants and sensitizers. Wax solvents can be toxic by contact and inhalation; carbon tetrachloride is carcinogenic and highly toxic to the liver and kidneys. |
|
Precautions: Avoid open flames. Do not use electric hot plates with exposed heating elements. Heat to minimum temperature necessary. Do not use carbon tetrachloride. |
|
|
Finished plastics
|
Hazards: Heating, machining, cutting plastics can result in decomposition to hazardous materials such as hydrogen chloride (from polyvinyl chloride), hydrogen cyanide (from polyurethanes and amino plastics), styrene (from polystyrene) and carbon monoxide from the combustion of plastics. Solvents used for gluing plastics are also fire and health hazards. |
|
Precautions: Have good ventilation when working with plastics and solvents. |
|
|
Plastics resins
|
Hazards: Most resin monomers (e.g., styrene, methyl methacrylate, formaldehyde) are hazardous by skin contact and inhalation. Methyl ethyl ketone peroxide hardener for polyester resins can cause blindness if splashed in the eyes. Epoxy hardeners are skin and respiratory irritants and sensitizers. Isocyanates used in polyurethane resins can cause severe asthma. |
|
Precautions: Use all resins with proper ventilation, personal protective equipment (gloves, respirators, goggles), fire precautions and so forth. Do not spray polyurethane resins. |
|
|
Glassblowing |
See Glass, ceramics and related materials. |
Drawing, Painting and Printmaking
Drawing involves making marks on a surface to express a feeling, experience or vision. The most commonly used surface is paper; drawing media include dry implements such as charcoal, coloured pencils, crayons, graphite, metalpoint and pastels, and liquids such as inks, markers and paints. Painting refers to processes that apply an aqueous or non-aqueous liquid medium (“paint”) to sized, primed or sealed surfaces such as canvas, paper or panel. Aqueous media include water-colours, tempera, acrylic polymers, latex and fresco; non-aqueous media include linseed or stand oils, dryers, varnish, alkyds, encaustic or molten wax, organic solvent-based acrylics, epoxy, enamels, stains and lacquers. Paints and inks typically consists of colouring agents (pigments and dyes), a liquid vehicle (organic solvent, oil or water), binders, bulking agents, antioxidants, preservatives and stabilizers.
Prints are works of art made by transferring a layer of ink from an image on a printing surface (such as woodblock, screen, metal plate or stone) onto paper, fabric or plastic. The printmaking process involves several steps: (1) preparation of the image; (2) printing; and (3) cleanup. Multiple copies of the image can be made by repeating the printing step. In monoprints, only one print is made.
Intaglio printing involves incising lines by mechanical means (e.g., engraving, drypoint) or etching the metal plate with acid to create depressed areas in the plate, which form the image. Various solvent-containing resists and other materials such as rosin or spray paint (aquatinting) can be used to protect the part of the plate not being etched. In printing, the ink (which is linseed oil based) is rolled onto the plate, and the excess wiped off, leaving ink in the depressed areas and lines. The print is made by placing the paper on the plate and applying pressure by a printing press to transfer the ink image to the paper.
Relief printing involves the cutting away of the parts of woodblocks or linoleum that are not to be printed, leaving a raised image. Water-or linseed oil–based inks are applied to the raised image and the ink image transferred to paper.
Stone lithography involves making an image with a greasy drawing crayon or other drawing materials that will make the image receptive to the linseed oil–based ink, and treating the plate with acids to make non-image areas water receptive and ink repellent. The image is washed out with mineral spirits or other solvents, inked with a roller and then printed. Metal plate lithography can involve a preliminary counteretch that often contains dichromate salts. Metal plates may be treated with vinyl lacquers containing ketone solvents for long print runs.
Screen printing is a stencil process where a negative image is made on the fabric screen by blocking out portions of the screen. For water-based inks, the blockout materials must be water insoluble; for solvent-based inks, the reverse. Cut plastic stencils are frequently used and adhered to the screen with solvents. The prints are made by scraping ink across the screen, forcing the ink through the unblocked parts of the screen onto paper located underneath the screen, thus creating the positive image. Large print runs using solvent-based inks involve the release of large amounts of solvent vapours into the air.
Collagraphs are made using either intaglio or relief printing techniques on a textured surface or collage, which can be made of many materials glued onto the plate.
Photoprintmaking processes can use either presensitized plates (often diazo) for lithography or intaglio, or the photoemulsion can be applied directly to the plate or stone. A mixture of gum arabic and dichromates have often been used on stones (gum printing). The photographic image is transferred to the plate, and then the plate exposed to ultraviolet light (e.g., carbon arcs, xenon lights, sunlight). When developed, the non-exposed portions of the photoemulsion are washed away, and the plate then printed. The coating and developing agents can often contain hazardous solvents and alkalis. In photo screen processes, the screen can be coated with dichromate or diazo photoemulsion directly, or an indirect process can be used, which involves adhering sensitized transfer films to the screen after exposure.
In printmaking techniques using oil-based inks, the ink is cleaned up with solvents or with vegetable oil and dishwashing liquid. Solvents also have to be used for cleaning lithography rollers. For water-based inks, water is used for cleanup. For solvent-based inks, large amounts of solvents are used for cleanup, making this one of the most hazardous processes in printmaking. Photoemulsions can be removed from screens using chlorine bleach or enzyme detergents.
Artists who draw, paint or make prints face significant health and safety hazards. The major sources of hazards for these artists include acids (in lithography and intaglio), alcohols (in paint, shellac, resin and varnish thinners and removers), alkalis (in paints, dye baths, photodevelopers and film cleaners), dusts (in chalks, charcoal and pastels), gases (in aerosols, etching, lithography and photoprocesses), metals (in pigments, photochemicals and emulsions), mists and sprays (in aerosols, air-brushing and aquatinting), pigments (in inks and paints), powders (in dry pigments and photochemicals, rosin, talc and whiting), preservatives (in paints, glues, hardeners and stabilizers) and solvents (such as aliphatic, aromatic and chlorinated hydrocarbons, glycol ethers and ketones). Common routes of exposure associated with these hazards include inhalation, ingestion and skin contact.
Among the well-documented health problems of painters, drawers and printmakers are: n-hexane-induced peripheral nerve damage in art students using rubber cement and spray adhesives; solvent-induced peripheral and central nervous system damage in silk-screen artists; bone marrow suppression related to solvents and glycol ethers in lithographers; onset or aggravation of asthma following exposure to sprays, mists, dusts, moulds and gases; abnormal heart rhythms following exposure to hydrocarbon solvents such as methylene chloride, freon, toluene and 1,1,1-trichloroethane found in glues or correction fluids; acid, alkali or phenol burns or irritation of the skin, eyes and mucous membranes; liver damage induced by organic solvents; and irritation, immune reaction, rashes and ulceration of the skin following exposure to nickel, dichromates and chromates, epoxy hardeners, turpentine or formaldehyde.
Although not well-documented, painting, drawing and printmaking may be associated with an increased risk of leukaemia, kidney tumours and bladder tumours. Suspected carcinogens to which painters, drawers and printmakers may be exposed include chromates and dichromates, polychlorinated biphenyls, trichloroethylene, tannic acid, methylene chloride, glycidol, formaldehyde, and cadmium and arsenic compounds.
The most important precautions in painting, drawing and printmaking include: substitution of water-based materials for materials based on organic solvents; proper use of general dilution ventilation and local exhaust ventilation (see figure 1); proper handling, labelling, storage and disposal of paints, flammable liquids and waste solvents; appropriate use of personal protective equipment such as aprons, gloves, goggles and respirators; and avoidance of products that contain toxic metals, especially lead, cadmium, mercury, arsenic, chromates and manganese. Solvents to be avoided include benzene, carbon tetrachloride, methyl n-butyl ketone, n-hexane and trichloroethylene.
Figure 1. Silk screen printing with slot exhaust hood.
Michael McCann
Additional efforts designed to reduce the risk of adverse health effects associated with painting, drawing and printmaking include early and continuous education of young artists concerning the hazards of art materials, and laws mandating labels on art materials that warn of both short-term and long-term health and safety hazards.
Entertainment and the Arts
Entertainment and the arts have been a part of human history ever since prehistoric people drew cave paintings of animals they hunted or acted out in song and dance the success of the hunt. Every culture from earliest times has had its own style of visual and performing arts, and decorated everyday objects like clothing, pottery and furniture. Modern technology and more leisure time has led to a major part of the world’s economy being devoted to satisfying the need for people to see or own beautiful objects and to be entertained.
The entertainment industry is a miscellaneous grouping of non-commercial institutions and commercial companies that provide these cultural, amusement and recreational activities for people. By contrast, artists and craftspeople are workers who create artwork or handicrafts for their own pleasure or for sale. They usually work alone or in groups of fewer than ten people, often organized around families.
The people who make this entertainment and art possible—artists and craftspeople, actors, musicians, circus performers, park attendants, museum conservators, professional sports players, technicians and others—often face occupational hazards that can result in injuries and illnesses. This chapter will discuss the nature of those occupational hazards. It will not discuss the hazards to people doing arts and crafts as hobbies or attending these entertainment events, although in many instances the hazards will be similar.
Entertainment and the arts can be thought of as a microcosm of all industry. The occupational hazards encountered are, in most instances, similar to those found in more conventional industries, and the same types of precautions can be used, although costs may be prohibitive factors for some engineering controls in the arts and crafts. In these instances, emphasis should be on substitution of safer materials and processes. Table 1 lists standard types of precautions associated with the various hazards found in the arts and entertainment industries.
Table 1. Precautions associated with hazards in the arts and entertainment industries.
|
Hazard |
Precautions |
|
Chemical hazards |
|
|
General |
Training in hazards and precautions Substitution of safer materials Engineering controls Adequate storage and handling No eating, drinking or smoking in work areas Personal protective equipment Spill and leak control procedures Safe disposal of hazardous materials |
|
Airborne contaminants (vapours, gases, spray mists, fogs, dusts, fumes, smoke) |
Enclosure Dilution or local exhaust ventilation Respiratory protection |
|
Liquids |
Cover containers Gloves and other personal protective clothing Splash goggles and face shields as needed Eyewash fountain and emergency showers when needed |
|
Powders |
Purchasing in liquid or paste form Glove boxes Local exhaust ventilation Wet mopping or vacuuming Respiratory protection |
|
Solids |
Gloves |
|
Physical hazards |
|
|
Noise |
Quieter machinery Proper maintenance Sound dampening Isolation and enclosure Hearing protectors |
|
Ultraviolet radiation |
Enclosure Skin protection and UV goggles |
|
Infrared radiation |
Skin protection and infrared goggles |
|
Lasers |
Using lowest-power laser possible Enclosure Beam restrictions and proper emergency cutoffs Laser goggles |
|
Heat |
Acclimatization Light, loose clothing Rest breaks in cool areas Adequate liquid intake |
|
Cold |
Warm clothing Rest breaks in heated areas |
|
Electrical hazards |
Adequate wiring Properly grounded equipment Ground fault circuit interrupters where needed Insulated tools, gloves, etc. |
|
Ergonomic hazards |
Ergonomic tools, instruments, etc., of proper size Properly designed work stations Proper posture Rest breaks |
|
Safety hazards |
|
|
Machinery |
Machine guards Accessible stop switch Good maintenance |
|
Flying particles (e.g., grinders) |
Enclosure Eye and face protection as needed |
|
Slips and falls |
Clean and dry walking and working surfaces Fall protection for elevated work Guardrails and toeboards on scaffolds, catwalks, etc. |
|
Falling objects |
Safety hats Safety shoes |
|
Fire hazards |
Proper exit routes Proper fire extinguishers, sprinklers, etc. Fire drills Removal of combustible debris Fireproofing of exposed materials Proper storage of flammable liquids and compressed gases Grounding and bonding when dispensing flammable liquids Removal of sources of ignition around flammables Proper disposal of solvent- and oil-soaked rags |
|
Biological hazards |
|
|
Moulds |
Humidity control Removal of standing water Cleanup after flooding |
|
Bacteria, viruses |
Vaccination where appropriate Universal precautions Disinfection of contaminated materials, surfaces |
Arts and Crafts
Artists and craftspeople are usually self-employed, and the work is done in homes, studios or backyards, using small amounts of capital and equipment. Skills are often handed down from generation to generation in an informal apprenticeship system, particularly in developing countries (McCann 1996). In industrialized countries, artists and craftspeople often learn their trade in schools.
Today, arts and crafts involve millions of people across the world. In many countries, craftwork is a major part of the economy. However, few statistics are available on the number of artists and craftspeople. In the United States, estimates gathered from a variety of sources indicate there are at least 500,000 professional artists, craftspeople and art teachers. In Mexico, it has been estimated that there are 5,000 families involved in the home-based pottery industry alone. The Pan American Health Organization found that 24% of the workforce in Latin America from 1980 to 1990 were self-employed (PAHO 1994). Other studies of the informal sector have found similar or higher percentages (WHO 1976; Henao 1994). What percentage of these are artists and craftspeople is unknown.
Arts and crafts evolve with the technology available and many artists and craftspeople adopt modern chemicals and processes for their work, including plastics, resins, lasers, photography and so on (McCann 1992a; Rossol 1994). Table 2 shows the range of physical and chemical hazards found in art processes.
Table 2. Hazards of art techniques
|
Technique |
Material/process |
Hazard |
|
Airbrush |
Pigments Solvents |
Lead, cadmium, manganese, cobalt, mercury, etc. Mineral spirits, turpentine |
|
Batik |
Wax Dyes |
Fire, wax, decomposition fumes See Dyeing |
|
Ceramics |
Clay dust Glazes Slip casting Kiln firing |
Silica Silica, lead, cadmium and other toxic metals Talc, asbestiform materials Sulphur dioxide, carbon monoxide, fluorides, infrared radiation, burns |
|
Commercial art |
Rubber cement Permanent markers Spray adhesives Airbrushing Typography Photostats, proofs |
N-hexane, heptane, fire Xylene, propyl alcohol N-hexane, heptane, 1,1,1-trichloroethane, fire See Airbrush See Photography Alkali, propyl alcohol |
|
Computer art |
Ergonomics Video display |
Carpal tunnel syndrome, tendinitis, poorly designed work stations Glare, Elf radiation |
|
Drawing |
Spray fixatives |
N-hexane, other solvents |
|
Dyeing |
Dyes Mordants Dyeing assistants |
Fibre-reactive dyes, benzidine dyes, naphthol dyes, basic dyes, disperse dyes, vat dyes Ammonium dichromate, copper sulphate, ferrous sulphate, oxalic acid, etc. Acids, alkalis, sodium hydrosulphite |
|
Electroplating |
Gold, silver Other metals |
Cyanide salts, hydrogen cyanide, electrical hazards Cyanide salts, acids, electrical hazards |
|
Enamelling |
Enamels Kiln firing |
Lead, cadmium, arsenic, cobalt, etc. Infrared radiation, burns |
|
Fibre arts |
See also Batik, Weaving Animal fibres Synthetic fibres Vegetable fibres |
Anthrax and other infectious agents Formaldehyde Moulds, allergens, dust |
|
Forging |
Hammering Hot forge |
Noise Carbon monoxide, polycyclic aromatic hydrocarbons, infrared radiation, burns |
|
Glassblowing |
Batch process Furnaces Colouring Etching Sandblasting |
Lead, silica, arsenic, etc. Heat, infrared radiation, burns Metal fumes Hydrofluoric acid, ammonium hydrogen fluoride Silica |
|
Holography (see also Photography) |
Lasers Developing |
Non-ionizing radiation, electrical hazards Bromine, pyrogallol |
|
Intaglio |
Acid etching Solvents Aquatint Photoetching |
Hydrochloric and nitric acids, nitrogen dioxide, chlorine gas, potassium chlorate Alcohol, mineral spirits, kerosene Rosin dust, dust explosion Glycol ethers, xylene |
|
Jewellery |
Silver soldering Pickling baths Gold reclaiming |
Cadmium fumes, fluoride fluxes Acids, sulphur oxides Mercury, lead, cyanide |
|
Lapidary |
Quartz gemstones Cutting, grinding |
Silica Noise, silica |
|
Lithography |
Solvents Acids Talc Photolithography |
Mineral spirits, isophorone, cyclohexanone, kerosene, gasoline, methylene chloride, etc. Nitric, phosphoric, hydrofluoric, hydrochloric, etc. Asbestiform materials Dichromates, solvents |
|
Lost wax casting |
Investment Wax burnout Crucible furnace Metal pouring Sandblasting |
Cristobalite Wax decomposition fumes, carbon monoxide Carbon monoxide, metal fumes Metal fumes, infrared radiation, molten metal, burns Silica |
|
Painting |
Pigments Oil, alkyd Acrylic |
Lead, cadmium, mercury, cobalt, manganese compounds, etc. Mineral spirits, turpentine Trace amounts ammonia, formaldehyde |
|
Papermaking |
Fibre separation Beaters Bleaching Additives |
Boiling alkali Noise, injuries, electrical Chlorine bleach Pigments, dyes, etc. |
|
Pastels |
Pigment dusts |
See Painting Pigments |
|
Photography |
Developing bath Stop bath Fixing bath Intensifier Toning Colour processes Platinum printing |
Hydroquinone, monomethyl-p-aminophenol sulphate, alkalis Acetic acid Sulphur dioxide, ammonia Dichromates, hydrochloric acid Selenium compounds, hydrogen sulphide, uranium nitrate, sulphur dioxide, gold salts Formaldehyde, solvents, colour developers, sulphur dioxide Platinum salts, lead, acids, oxalates |
|
Relief printing |
Solvents Pigments |
Mineral spirits See Painting Pigments |
|
Screen printing |
Pigments Solvents Photoemulsions |
Lead, cadmium, manganese and other pigments Mineral spirits, toluene, xylene Ammonium dichromate |
|
Sculpture, clay |
See Ceramics |
|
|
Sculpture, lasers |
Lasers |
Non-ionizing radiation, electrical hazards |
|
Sculpture, neon |
Neon tubes |
Mercury, cadmium phosphors, electrical hazards, ultraviolet radiation |
|
Sculpture, plastics |
Epoxy resin Polyester resin Polyurethane resins Acrylic resins Plastic fabrication |
Amines, diglycidyl ethers Styrene, methyl methacrylate, methyl ethyl ketone peroxide Isocyanates, organotin compounds, amines, mineral spirits Methyl methacrylate, benzoyl peroxide Heat decomposition products (e.g., carbon monoxide, hydrogen chloride, hydrogen cyanide, etc.) |
|
Sculpture, stone |
Marble Soapstone Granite, sandstone Pneumatic tools |
Nuisance dust Silica, talc, asbestiform materials Silica Vibration, noise |
|
Stained glass |
Lead came Colourants Soldering Etching |
Lead Lead-based compounds Lead, zinc chloride fumes Hydrofluoric acid, ammonium hydrogen fluoride |
|
Weaving |
Looms Dyes |
Ergonomic problems See Dyeing |
|
Welding |
General Oxyacetylene Arc Metal fumes |
Metal fumes, burns, sparks Carbon monoxide, nitrogen oxides, compressed gases Ozone, nitrogen dioxide, fluoride and other flux fumes, ultraviolet and infrared radiation, electrical hazards Oxides of copper, zinc, lead, nickel, etc. |
|
Woodworking |
Machining Glues Paint strippers Paints and finishes Preservatives |
Injuries, wood dust, noise, fire Formaldehyde, epoxy, solvents Methylene chloride, toluene, methyl alcohol, etc. Mineral spirits, toluene, turpentine, ethyl alcohol, etc. Chromated copper arsenate, pentachlorophenol, creosote |
Source: Adapted from McCann 1992a.
The arts and crafts industry, like much of the informal sector, is almost completely unregulated and is often exempted from workers’ compensation laws and other occupational safety and health regulations. In many countries, government agencies responsible for occupational safety and health are unaware of the risks facing artists and craftspeople, and occupational health services do not reach out to this group of workers. Special attention is needed to find ways to educate artists and craftspeople about the hazards and precautions needed with their materials and processes, and to make occupational health services available to them.
Health problems and disease patterns
Few epidemiological studies have been done on workers in the visual arts. This is mostly due to the decentralized and often unregistered nature of most of these industries. Much of the data that are available come from individual case reports in the literature.
The traditional arts and crafts can result in the same occupational diseases and injuries found in larger-scale industry, as evidenced by such old terms as potter’s rot, weaver’s back and painter’s colic. The hazards of such crafts as pottery, metalworking and weaving were first described by Bernardino Ramazzini almost three centuries ago (Ramazzini 1713). Modern materials and processes also are causing occupational illnesses and injuries.
Lead poisoning is still one of the most common occupational illnesses among artists and craftspeople, with examples of lead poisoning being found in:
- a stained-glass artist in the United States (Feldman and Sedman 1975)
- potters and their families in Mexico (Ballestros, Zuniga and Cardenas 1983; Cornell 1988) and Barbados (Koplan et al. 1977)
- families in Sri Lanka recovering gold and silver from jeweller’s waste using a molten lead procedure (Ramakrishna et al. 1982).
Other examples of occupational illnesses in the arts and crafts include:
- chromium sensitization in a fibre artist (MMWR 1982)
- neuropathy in a silk-screen artist (Prockup 1978)
- heart attacks from methylene chloride in a furniture refinisher (Stewart and Hake 1976)
- respiratory problems in photographers (Kipen and Lerman 1986)
- mesothelioma in jewellers (Driscoll et al. 1988)
- silicosis and other respiratory diseases in agate workers in India (Rastogi et al. 1991)
- asthma from carving ivory from elephant tusks in Africa (Armstrong, Neill and Mossop 1988)
- respiratory problems and ergonomic problems among carpet weavers in India (Das, Shukla and Ory 1992)
- as many as 93 cases of peripheral neuropathy from the use of hexane-based adhesives in sandal-making in Japan in the late 1960s (Sofue et al. 1968)
- paralysis in 44 apprentice shoemakers in Morocco due to glues containing tri-orthocresyl phosphate (Balafrej et al. 1984)
- leg, arm and back pain and other occupational health problems in home-based workers making ready-made garments in India (Chaterjee 1990).
A major problem in the arts and crafts is the prevalent lack of knowledge of hazards, materials and processes and how to work safely. Individuals who do develop occupational diseases often do not realize the connection between their illness and their exposures to hazardous materials, and are less likely to obtain proper medical assistance. In addition, whole families can be at risk—not only those adults and children actively working with the materials, but also younger children and infants who are present, since these arts and crafts are commonly done in the home (McCann et al. 1986; Knishkowy and Baker 1986).
A proportionate mortality ratio (PMR) study of 1,746 White professional artists by the United States National Cancer Institute found significant elevations in deaths of painters, and to a lesser degree for other artists, from arteriosclerotic heart disease and from cancers of all sites combined. For male painters, rates of leukaemia and cancers of the bladder, kidney and colorectum were significantly elevated. Proportionate cancer mortality rates were also elevated, but to a lesser degree. A case control study of bladder cancer patients found an overall relative risk estimate of 2.5 for artistic painters, confirming the results found in the PMR study (Miller, Silverman and Blair 1986). For other male artists, PMRs for colorectal and kidney cancer were significantly elevated.
Performing and Media Arts
Traditionally, the performing arts include theatre, dance, opera, music, storytelling and other cultural events that people would come to see. With music, the type of performance and their venue can vary widely: individuals performing music on the street, in taverns and bars, or in formalized concert halls; small musical groups playing in small bars and clubs; and large orchestras performing in large concert halls. Theatre and dance companies can be of several types, including: small informal groups associated with schools or universities; non-commercial theatres, which are usually subsidized by governments or private sponsors; and commercial theatres. Performing arts groups may also tour from one location to another.
Modern technology has seen the growth of the media arts, such as the print media, radio, television, motion pictures, videotapes and so on, which enable the performing arts, stories and other events to be recorded or broadcast. Today the media arts are a multi-billion-dollar industry.
Workers in the performing and media arts include the performers themselves—actors, musicians, dancers, reporters and others visible to the public. In addition, there are the technical crews and front office people—stage carpenters, scenic artists, electricians, special effects experts, motion picture or television camera crews, ticket sellers and others—who work backstage, behind the cameras and on other non-performing jobs.
Health effects and disease patterns
Actors, musicians, dancers, singers and other performers are also subject to occupational injuries and illnesses, which can include accidents, fire hazards, repetitive strain injuries, skin irritation and allergies, respiratory irritation, performance anxiety (stage fright) and stress. Many of these types of injuries are specific to particular groups of performers, and are discussed in separate articles. Even minor physical problems can often affect a performer’s peak performance capability, and subsequently end in lost time and even lost jobs. In recent years, the prevention, diagnosis and treatment of injuries to performers has led to the new field of arts medicine, originally an offshoot of sports medicine. (See “History of performing arts medicine” in this chapter.)
A PMR study of screen and stage actors found significant elevations for lung, oesophagus and bladder cancers in women, with the rate for stage actresses 3.8 times that of screen actresses (Depue and Kagey 1985). Male actors had significant PMR (but not proportionate cancer mortality ratio) increases for pancreatic and colon cancer; testicular cancer was twice the expected rate by both methods. PMRs for suicide and non–motor vehicle accidents were significantly elevated for both men and women, and the PMR for cirrhosis of the liver was elevated in men.
A recent survey of injuries among 313 performers in 23 Broadway shows in New York City found that 55.5% reported at least one injury, with a mean of 1.08 injuries per performer (Evans et al. 1996). For Broadway dancers, the most frequent sites of injury were the lower extremities (52%), back (22%) and neck (12%), with raked or slanted stages being a significant contributing factor. For actors, the most frequent sites of injuries were lower extremities (38%), the lower back (15%) and vocal cords (17%). The use of fogs and smoke on stage was listed as a major cause for the last.
In 1991, the United States National Institute for Occupational Safety and Health investigated the health effects of the use of smoke and fogs in four Broadway shows (Burr et al. 1994). All the shows used glycol-type fogs, although one also used mineral oil. A questionnaire survey of 134 actors in these shows with a control group of 90 actors in five shows not using fogs found significantly higher levels of symptoms in actors exposed to fogs, including upper-respiratory symptoms such as nasal symptoms and irritation of mucous membranes, and lower-respiratory symptoms such as coughing, wheezing, breathlessness and chest tightness. A follow-up study could not demonstrate a correlation between fog exposure and asthma, possibly due to the low number of responses.
The motion picture production industry has a high accident rate, and in California is classified as high risk, mostly as a result of stunts. During the 1980s, there were over 40 fatalities in American-produced motion pictures (McCann 1991). California statistics for 1980–1988 show an incidence of 1.5 fatalities per 1,000 injuries, compared to the California average of 0.5 for the same period.
A large number of studies have shown that dancers have high overuse and acute injury rates. Ballet dancers, for example, have high incidences of overuse syndrome (63%), stress fractures (26%) and major (51%) or minor (48%) problems during their professional careers (Hamilton and Hamilton 1991). One questionnaire study of 141 dancers (80 females), 18 to 37 years old, from seven professional ballet and modern dance companies in the United Kingdom, found that 118 (84%) of the dancers reported at least one dance-related injury that affected their dancing, 59 (42%) in the last six months (Bowling 1989). Seventy-four (53%) reported that they were suffering from at least one chronic injury that was giving them pain. The back, neck and ankles were the most common sites of injury.
As with dancers, musicians have a high incidence of overuse syndrome. A 1986 questionnaire survey by the International Conference of Symphony and Opera Musicians of 4,025 members from 48 American orchestras showed medical problems affecting performance in 76% of the 2,212 respondents, with severe medical problems in 36% (Fishbein 1988). The most common problem was overuse syndrome, reported by 78% of string players. A 1986 study of eight orchestras in Australia, the United States and England found a 64% occurrence of overuse syndrome, 42% of which involved a significant level of symptoms (Frye 1986).
Hearing loss among rock musicians has had significant press coverage. Hearing loss is also found, however, among classical musicians. In one study, sound level measurements at the Lyric Theatre and Concert Hall in Gothenberg, Sweden, averaged 83 to 89 dBA. Hearing tests of 139 male and female musicians from both theatres indicated that 59 musicians (43%) showed worse pure tone thresholds than would be expected for their age, with brass wind instrumentalists showing the greatest loss (Axelsson and Lindgren 1981).
A 1994-1996 study of sound level measurements in the orchestra pits of 9 Broadway shows in New York City showed average sound levels from 84 to 101 dBA, with a normal showtime of 2½ hours (Babin 1996).
The carpenters, scenic artists, electricians, camera crews and other technical support workers face, in addition to many safety hazards, a wide variety of chemical hazards from materials used in scene shops, prop shops and costume shops. Many of the same materials are used in the visual arts. However, there are no available injury or illness statistics on these workers.
Entertainment
The “Entertainment” section of the chapter covers a variety of entertainment industries that are not covered under “Arts and Crafts” and “Performing and Media Arts”, including: museums and art galleries; zoos and aquariums; parks and botanical gardens; circuses, amusement and theme parks; bullfighting and rodeos; professional sports; the sex industry; and nightlife entertainment.
Health effects and disease patterns
There are a wide variety of types of workers involved in the entertainment industry, including performers, technicians, museum conservators, animal handlers, park rangers, restaurant workers, cleaning and maintenance personnel and many more. Many of the hazards found in the arts and crafts and performing and media arts are also found among particular groups of entertainment workers. Additional hazards such as cleaning products, toxic plants, dangerous animals, AIDS, zoonoses, hazardous drugs, violence and so forth are also occupational hazards to particular groups of entertainment workers. Because of the disparateness of the various industries, there are no overall injury and illness statistics. The individual articles include relevant injury and illness statistics, where available.
Hours of Work
Shiftwork is work scheduled, either permanently or frequently, outside normal daytime working hours. Shiftwork can be e.g., permanent work at night, permanent work during the evening, or work hours can have changing assignment patterns. Each type of shift system has its advantages and disadvantages, and each is associated with differing effects on well-being, health, social life and work performance.
In the traditional slowly rotating shift systems, shifts change weekly; that is, a week of night shifts is followed by a week of evening shifts and then a week of morning shifts. In a quickly rotating shift system only one, two or a maximum of three consecutive days are spent on each shift. In some countries, like the United States, shifts longer than 8 hours, in particular 12 hours, are gaining in popularity (Rosa et al. 1990).
Human beings have evolved as essentially diurnal; that is, the body is mainly “programmed” towards daytime work performance and for night-time recreation and rest. Internal mechanisms (sometimes called the body or biological clock) control the physiology and biochemistry of the body to fit in with a 24-hour environment. These cycles are called circadian rhythms. The disruption of circadian variations in physiological function caused by having to be awake and at work at biologically unusual hours, as well as to sleep during the daytime, is one of the major stresses associated with shiftwork.
Despite the widespread assumption that disturbances of the circadian system may result, over the long run, in harmful effects, the actual cause-effect relation has been difficult to establish. Despite this lack of absolute proof, it is widely accepted that it is prudent to adopt shift systems at the workplace that minimize long-lasting disruption of circadian rhythms.
Combined Effects of Workplace Factors
Some shiftworkers are also exposed to other workplace hazards, such as toxic agents, or to jobs with high mental loads or physical demands. Only a few studies, however, have addressed the problems caused by the combination of shiftwork and unfavourable working, organizational and environmental conditions where the negative effects of shiftwork could be caused not only by the phase difference between circadian rhythms and living conditions, but also by the adverse negative working conditions that may be combined with shiftwork.
A variety of workplace hazards, such as noise, unfavourable climatic conditions, unfavourable lighting conditions, vibration and combinations of these, can sometimes occur more often in three-shift systems, irregular systems and night-shift systems than in two-shift systems or daywork.
Intervening Variables
People vary widely in their tolerance of shiftwork, according to Härmä (1993), which may be explained by the influence of many intervening variables. Some individual differences which may modify the strain of shiftworkers are: differences in the phase and amplitude of the circadian cycle, age, gender, pregnancy, physical fitness and flexibility in sleeping habits, and the ability to overcome drowsiness, as illustrated by figure 1.
Figure 1. Model of stress and strain of shiftworkers.
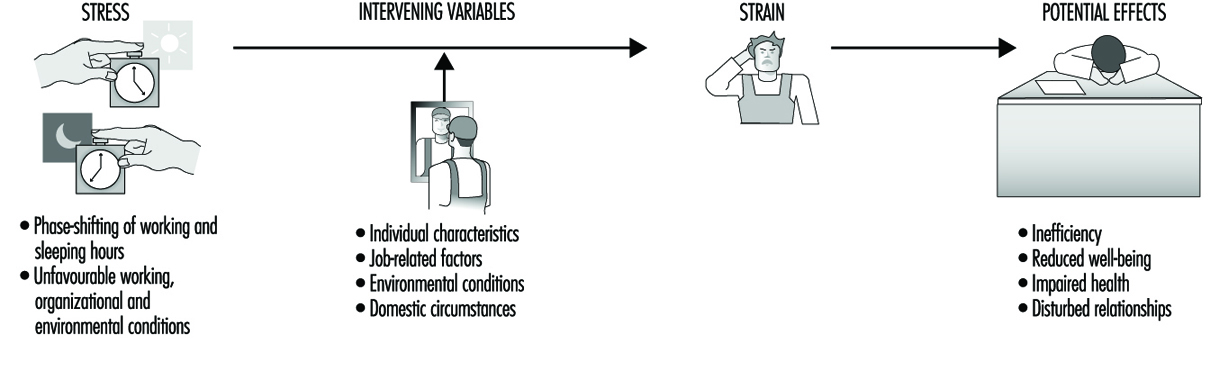
Although some authors found a correlation between a larger amplitude of circadian rhythms and fewer medical complaints (Andlauer et al. 1979; Reinberg et al. 1988; Costa et al. 1989; Knauth and Härmä 1992), others have found that it does not predict adjustment to shiftwork (Costa et al. 1989; Minors and Waterhouse 1981) even after three years of work (Vidacek et al. 1987).
There appear to be two main dimensions of personality related to the circadian phase: “morningness”/“eveningness” and intro-version/extroversion (Kerkhof 1985). Morningness/eveningness can be assessed by questionnaire (Horne and Östberg 1976; Folkard et al. 1979; Torsval and Åkerstedt 1980; Moog 1981) or by measuring body temperature (Breithaupt et al. 1978). Morning types, “larks”, having an advanced phase position of the circadian body temperature, go to bed earlier and rise earlier than the average population, whereas evening types, “owls,” have a delayed circadian phase position and go to bed and rise later. To be a “lark” would appear to be an advantage for morning shifts and an “owl” for night shifts. However, some authors report that a disproportionally large number of those who give up shiftwork were morning types (Åkerstedt and Fröberg 1976; Hauke et al. 1979; Torsvall and Åkerstedt 1979). A relation between morningness and decreased tolerance to shiftwork has been found by Bohle and Tilley (1989) and Vidacek et al. (1987). Other researchers, however, have found opposite results (Costa et al. 1989), and it should be noted that most studies have involved only extreme “larks” and “owls”, where each represents only 5% of the population.
In many questionnaire studies, more adverse health effects of shiftwork have been found with increasing age, the critical age being 40 to 50 years on average (Foret et al. 1981; Koller 1983; Åkerstedt and Torsvall 1981). With increasing age, sleep during the day becomes progressively more difficult (Åkerstedt and Torsvall 1981). There are also some indications of slower circadian adjustment to shiftwork in middle-aged shiftworkers compared to younger ones (Härmä et al. 1990; Matsumoto and Morita 1987).
Gender and pregnancy are two intervening variables which have often been discussed but not yet adequately investigated in longitudinal studies. Based on a review of the literature, Rutenfranz et al. (1987) conclude that the circadian rhythms of men and women react in the same way to the phase shifting of work and sleep in connection with night work. However, two aspects—the menstrual cycle and the additional load of child care and household duties—have to be taken into consideration.
Although some authors have found more frequent menstrual problems in groups of women shiftworkers compared to women in day work (Tasto et al. 1978; Uehata and Sasakawa 1982), the comparability of these shift and day-work groups was question-able. Pokorski et al. (1990) studied perception of discomfort among female triple-shift workers during three phases of the menstrual cycle (praemenstruum, menstruation and postmen-struum). Phase-related differences were more pronounced than differences between morning, evening and night shifts.
Child care at home reduced the duration of sleep and of leisure time in female shiftworking nurses. Estryn-Behar questioned 120 women on permanent night shift and found that the average duration of sleep after night shifts was 6 h 31 min for women without children, 5 h 30 min for women with older children, and 4 h 55 min for women with very young children (Estryn-Behar et al. 1978). Nevertheless, a study of policewomen found that those with children were more favourable towards shiftwork than were women without children (Beermann et al. 1990).
Physical fitness appeared to be a factor in increasing tolerance to shiftwork in a study by Härmä et al. (1988a, b). In a follow-up study with matched pair design, the group of participants who exercised regularly on a four-month programme reported a significant decrease in general fatigue, particularly when on the night shift, as well as a decrease in musculoskeletal symptoms and an increase in sleep length.
The “flexibility of sleeping habits” and “ability to overcome drowsiness”, as assessed by a questionnaire developed by Folkard et al. (1979; 1982) were related, in some studies, to a better tolerance to shiftwork (Wynne et al. 1986; Costa et al. 1989; Vidacek et al. 1987). In other studies, however, this relationship was not confirmed (e.g., Bohle and Tilley 1989).
Other intervening variables that may be important for shiftwork tolerance are the “commitment to night work” as the way in which people schedule their lives (Folkard et al. 1979; Minors and Waterhouse 1981) or the coping style of shiftworkers (Olsson et al. 1987; Olsson and Kandolin 1990).
Besides individual characteristics, situational factors seem to be of importance for explaining the extent of problems reported by shiftworkers. Küpper et al. (1980) and Knauth (1983) found that shiftworkers who tried to sleep during the day and were often or always disturbed by noise, complained more frequently about nervous and gastrointestinal symptoms than did shiftworkers with undisturbed or rarely disturbed sleep.
Health Effects of Shiftwork
Most of the health complaints of shiftworkers can be related to the quality of the day sleep after night shifts and, to a lesser extent, to the sleep before morning shifts. As circadian rhythms generally function such that the body is programmed for daytime performance and for night-time sleep, after the night shift the body is, in general, not completely adjusted for going to sleep. Other factors may also intervene. Daylight may disturb sleep. Noise during the day is in general louder than during the night. Most nightworkers complain about the noise of children and of traffic. Some nightworkers interrupt their day sleep in order to partake of a joint meal with the family, and some reduce their sleep because of their household duties and child care responsibilities. In one study of shiftworkers, the duration of night sleep was found to be reduced to 6 hours (Knauth 1983). Although there are large interindividual differences in sleep needs, 6 or less hours of sleep per day is inadequate for many human beings (Williams et al. 1974). In particular, after many consecutive night shifts an accumulation of sleep deficits has to be expected, with its accompanying effects in both social life and productivity (Naitoh et al. 1990) as well as the possibility of an increased accident rate. Several electroencephalographic studies have also shown that the quality of day sleep is also lower (Knauth 1983).
Sleep deficits may occur in both a week of night shifts and in a week of morning shifts. The prolonged sleep duration at the weekend after a week of morning shifts seems to indicate that there is an increased need for sleep.
Hak and Kampmann (1981) studied sleep and fatigue in train drivers. The earlier the morning shift started, the shorter was the preceding night-shift sleep and the more fatigued the train drivers during the morning shift. The reduction of sleep in connection with an earlier start of the morning shift has also been confirmed by studies of Moors (1990) as well as Folkard and Barton (1993). Such findings may be partially explained by the social pressure of the family not to go to bed too early, or by the body clock, which according to Lavie (1986) causes a “forbidden zone” for sleep, during which sleep propensity is greatly reduced. The latter explanation means that even if the shiftworkers go to bed earlier—because of the early start of the following morning shift—they might find it difficult to fall asleep.
Gastrointestinal disturbances. Night work leads to a change in the sequence and timing of meals. During the night, the stomach cannot cope with the composition and the quantity of a typical daytime meal. It is then understandable that nightworkers often suffer more from disturbances of appetite than do dayworkers or shiftworkers not on night shift, as Rutenfranz et al. (1981) have concluded from a review of the literature.
In the long run, irregular food intake can lead to gastrointestinal complaints or even to disorders. However, the reasons for the complex gastrointestinal symptoms are surely manifold. An analysis of existing studies, such as that of Costa (1996), is difficult, because of methodological differences. Most results are based on cross-sectional studies—that is, on workers currently engaged in shiftwork. Thus, if individuals have left shiftwork because of problems or diseases, we are left with a more or less self-selected population (the “healthy worker” effect). Therefore the health status of a group of shiftworkers may be better than a group of dayworkers, simply because shiftworkers with poorer health or social problems have changed to day work and those that remain may be better able to cope.
In longitudinal studies, which have been almost exclusively retrospective, the problems with self-selection and loss to follow-up are well known. For example, for the sample in the study of Leuliet (1963), the study population was almost halved in size during the study period of 12 years. As with cross-sectional studies, it is often former shiftworkers, who have transferred to day work out of shifts because of medical problems, who show the most serious effects. Thiis-Evensen (1958) found that peptic ulcers were twice as frequent among former shiftworkers as among dayworkers. Aanonsen (1964) and Angersbach et al. (1980) observed, respectively, two and three-and-a-half times as many cases of peptic ulcers among former regular shiftworkers, with a subsequent significant decrease in gastrointestinal disease after the transfer out of the shiftwork pattern.
Costa et al. (1981) computed the time interval between beginning shiftwork and when illnesses were diagnosed (table 1). Comparing groups with different working time arrangements, Costa et al. found the shortest mean intervals (4.7 years) for the appearance of gastroduodenitis in permanent nightworkers. In groups with night work (i.e., three-shift workers and permanent nightworkers), within an interval of about 5 years peptic ulcers developed. In his review Costa (1996) concludes that “there is sufficient evidence to consider shiftwork as a risk factor for gastrointestinal disorders and diseases—in particular peptic ulcer” (table 1).
Table 1. Time intervals from the beginning of shiftwork to the moment when the three illnesses were diagnosed (mean and standard deviation in years).
|
Work schedule |
Gastroduodenitis |
Peptic ulcer |
Neurotic disorders |
|
Day work |
12.6 ± 10.9 |
12.2 ± 9.9 |
9.7 ± 6.8 |
|
Two shifts |
7.8 ± 6.6 |
14.4 ± 8.2 |
9.0 ± 7.5 |
|
Three shifts |
7.4 ± 6.5 |
5.0 ± 3.9 |
6.8 ± 5.2 |
|
Night work |
4.7 ± 4.3 |
5.6 ± 2.8 |
3.6 ± 3.3 |
Source: Costa et al. 1981
Cardiovascular disorders. Kristensen (1989) has analysed the relevant studies on the incidence of cardiovascular disorders in shiftworkers for methodological and analytical factors, as shown in Table 2. Papers published after 1978 were more likely to report an increase in cardiovascular disorders, particularly among those who transferred away from shiftwork. Waterhouse et al. (1992) conclude that it is not possible simply to dismiss the relationship as had been generally accepted (Harrington 1978).
Table 2. Relationship between shiftwork and incidence of cardiovascular disorders
|
Reference |
Publication years |
Conclusion |
Methodological comments/ratings |
|
Thiis-Evenson (1949); Aanonsen (1964) |
1949-1964 |
0 |
2 |
|
Taylor and Pocock (1972) |
1972 |
0 |
? correct choice for controls |
|
Rutenfranz et el. (1977); Carpentier et al. (1977) |
1977 |
0, review articles |
|
|
Angersbach et al. (1980); |
1980-1983 |
+, particularly dropouts; |
2-3 |
|
Michel-Briand et al. (1981) |
1981 |
+, in retired workers |
1 |
|
Alfredsson et al. (1982; 1983; 1985); |
1982-1986 |
+, in men and women; |
3-4 |
|
Åkerstedt et al. (1984) |
1984-1986 |
+, review article |
|
|
Orth-Gomer (1985) |
1985 |
+, review article |
|
|
Andersen (1985) |
1985 |
+, occupations involving shiftwork |
|
|
Frese and Semmer (1986) |
1986 |
+, in dropouts |
Source: Waterhouse et al. 1992. Based on Kristensen 1989. Ratings on conclusions used by Kristensen: +, increased incidence; 0, no difference.
Methodological ratings, 1-4 from lowest to highest quality methodology.
Neurological disorders. Although there is a lack of standardization of the symptoms and disorders in studies of neurological disorders of shiftworkers (Waterhouse et al. 1992; Costa 1996), according to Waterhouse (1992), however, “there is now evidence for a greater tendency towards general malaise—including anxiety and depression elements—in shiftworkers than in day-working colleagues”. Costa (1996) comes to a similar but more cautious conclusion: “there is sufficient evidence to suggest that morbidity for psychoneurotic disorders can be influenced by shiftwork to a greater or lesser extent in relation to other individual and social factors.”
Mortality. There is only one very careful epidemiological study on the mortality of shiftworkers. Taylor and Pocock (1972) compared mortality rates in shiftworkers and dayworkers over a 13-year period in a sample of over 8,000 persons. There were no differences in rates between current shiftworkers and dayworkers. However, the standardized mortality ratio for former shiftworkers was 118.9, compared to 101.5 for current shiftworkers, which “might imply a selecting-out of less fit men” (Harrington 1978).
Social Problems of Shiftworkers
Shiftwork may have negative effects on family life, participation in institutional life and social contacts. The extent of problems which may exist is dependent on many factors, such as the type of shift system, gender, age, marital status, composition of family of the shiftworker, as well as how common shiftwork is in a particular region.
During a week of evening shifts, regular contacts between a shiftworker and his or her school-age children, or partner who may work in morning or day shifts, are dramatically reduced. This is an important problem for shiftworkers who work so-called permanent afternoon shifts (Mott et al. 1965). In the traditional discontinuous two-shift system, a week of morning shifts and evening shifts alternates such that every second week the contacts are disturbed. The traditional weekly rotating three-shift system has evening shifts every third week. In quickly rotating shift systems, contacts within the family are never impaired during a whole week. Researchers have obtained contradicting results. Mott et al. (1965) found that many consecutive evening or night shifts could impair the marital happiness of shiftworkers, while Maasen (1981) did not observe this. Shiftwork—in particular when both parents are shiftworkers—may have negative effects on the school performance of children (Maasen 1981; Diekmann et al. 1981).
Studies concerning the subjective value of free time during different hours of the week showed that weekends were rated higher than weekdays, and evenings higher than time off during the day (Wedderburn 1981; Hornberger and Knauth 1993). The contacts with friends, relatives, clubs, political parties, churches and so on are mainly impoverished by weekend work, evening shifts and night shifts (Mott et al. 1965), as has been reviewed by Bunnage (1981); Walker (1985); and Colligan and Rosa (1990).
Only with respect to hobbies and activities of a solitary or near-solitary nature are shiftworkers at an advantage compared to dayworkers, since gardening, walking, fishing or “do it yourself” projects are comparatively flexible activities which are possible any time, not only in the evening or on weekends.
Some studies have dealt with the burden of shiftworkers’ spouses (Banks 1956; Ulich 1957; Downie 1963; Sergean 1971), who have to alter their lifestyle (for example mealtimes) in order to fit in with the shift system of their mates. They may be forced to postpone noisy household duties and to keep children quiet when the shiftworker is asleep after the night shift. Furthermore, they are alone during evening, night and weekend shifts and have to cope with an irritable spouse. After a change from a weekly to a quickly rotating continuous shift system, 87% of shiftworkers’ spouses voted in favour of the new shift system. They argued that in the old shift system the spouse was very tired after the end of the period of night shifts, needed several days to recover and was not in the mood for joint leisure activities. However, in the new shift system with only two or three consecutive night shifts, the worker was less tired and they enjoyed more joint leisure activities.
Women on shiftwork may have more problems with domestic duties and sleep since household responsibility is not equally shared by the marriage partners. Nevertheless some permanent night nurses have specifically chosen to work at night for domestic reasons (Barton et al. 1993). However, as Walker (1985) concludes in his review, “to say that fixed night shifts for mothers is compatible with their child-rearing responsibilities ignores the ‘costs’”. Constant tiredness because of reduced sleep may be the cost.
Worker Performance
In addition to possible effects of shiftwork on worker health, worker performance can also be affected. Harrington’s (1978) generalized conclusions about performance were reached through consideration of productivity and accidents. They are still valid and have been reformulated by Waterhouse et al. (1992):
- Errors and general performance often showed rhythmic changes, with the night shift being worst.
- The nocturnal decrement in performance could be lessened or prevented if breaks in the work were feasible, if the work were interesting, or if motivation could be maintained.
- The performance worsened (generally with the night shift being more adversely affected than others) if boring, repetitive tasks were involved, if sleep loss had occurred, or if the amount of time spent on duty were increased.
Differences between individuals were often the largest variable in performance.
One problem in comparing productivity and accidents in morning, afternoon and night shifts is methodological. Working, environmental and organizational conditions at night and in the daytime in general are not completely comparable (Colquhoun 1976; Carter and Corlett 1982; Waterhouse et al. 1992). Therefore it is difficult to control all the variables. It is not astonishing that in a review of 24 studies there were almost as many studies with a higher frequency of accidents at night as studies with a higher frequency of accidents in the daytime (Knauth 1983). In some studies the workload in the daytime and during night-time were comparable and measures were available for all 24 hours. In most of these studies the authors found a degraded night-shift performance (e.g., Browne 1949; Bjerner et al. 1955; Hildebrandt et al. 1974; Harris 1977; Hamelin 1981). However, as Monk (1990) has concluded, it is possible that circadian effects can “show through” only when workers are under pressure. In the absence of pressure, workers may be able to equate day-shift and night-shift performance, because both are considerably suboptimal.
The Design of Shift Systems
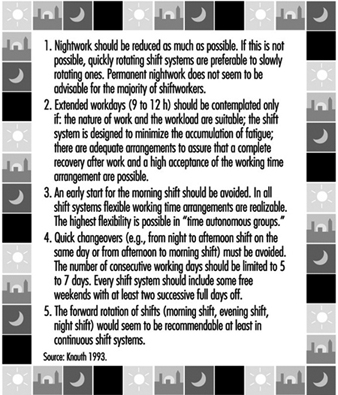
The most important recommendations for the design of shift systems are summarized in figure 2.
Figure 2. Recommendations for the design of shift systems.
Permanent night work
The night shift is the most disruptive of all shifts in terms of physiological adjustment, sleep and well-being. The circadian physiological rhythms of most shiftworkers may require more than one week for complete adjustment to night work. Any partial adjustment will be lost following days off from night shift. Thus, the body rhythms of permanent nightworkers are constantly in a state of disruption. In one study (Alfredsson et al. 1991) the permanent night security guards had a 2-to-3-times higher occurrence of sleep disturbances and fatigue than the national sample of the working population.
Some authors have suggested various ways in which to match employee tolerance for shiftwork and certain external stimuli for helping workers to adjust. According to Hildebrandt et al. (1987) persons with a late phase position (evening types) are able to adjust to night work. Moog (1988) posited that they should work in very long periods of night shifts—that is, much more than 10 nights in a row. To profit from an adjustment to night work, Folkard (1990) even suggested the creation of a “nocturnal subsociety”, which in addition to working permanently at night, would continue to be active at night and to sleep during the day, even when not at work. Although performance at night might in the long run be increased (Wilkinson 1992), such a proposal causes an accumulation of sleep deficits and social isolation, which seems to be unacceptable for most persons (Smith and Folkard 1993).
There are an increasing number of studies dealing with the influence of bright light on re-entrainment of circadian rhythms (some examples are Wever et al. 1983; special session at the IXth International Symposium on Night and Shift Work; Costa et al. 1990a; Rosa et al. 1990; Czeisler et al. 1990). However, “much work is necessary to determine the optimal light-work-sleep schedules for shift workers in terms of their ability to shift circadian rhythms, improve sleep, reduce fatigue, as well as in terms of their social feasibility”, according to Eastman (1990).
In comparison with other shift systems, fixed night shifts have more negative effects on families who must adapt their lifestyles to this schedule, on sexual relations and on workers’ ability to fulfil familial roles (Stein 1963; Mott et al. 1965; Tasto et al. 1978; Gadbois 1981). However, in some studies of permanent night shift, nurses reported fewer complaints than rotating nurses or dayshift nurses (Verhaegen et al. 1987; Barton et al. 1993). Barton et al. propose that one possible explanation for these results may be that the freedom to choose either day- or night-work may greatly influence the degree to which subsequent problems are experienced. The notion that this represents “freedom” is, however, questionable when many female nurses prefer permanent night work because this represents the only way of better arranging domestic responsibilities and employment outside the home (Gadbois 1981).
Permanent night work also has some advantages. Nightworkers report a greater feeling of independence and less supervision at night (Brown 1990; Hoff and Ebbing 1991). Furthermore, because it is less easy to obtain work relief for night-shift staff, apparently more “team spirit” (esprit de corps) develops. However, in most cases night work is chosen because of the increase in income due to the night-shift allowance (Hoff and Ebbing 1991).
Although we have insufficient knowledge about the long-term health effects of permanent night work and about optimal bright-light work-sleep schedules, it is known that the night shift is the most disruptive of all shifts in terms of physiological adjustment, sleep and well-being, and until results from further research are available, we will assume for the moment that permanent night work is not recommendable for the majority of shiftworkers.
Quickly rotating versus slowly rotating shift systems
More rapidly rotating schedules are more advantageous compared to weekly shift rotation. A fast rotation keeps the circadian rhythm in a daytime orientation and it is not in a constant state of disruption from partial adjustment to different day and night orientations. Consecutive night shifts may cause an accumulation of sleep deficits—that is, a chronic sleep deprivation (Tepas and Mahan 1989; Folkard et al. 1990). In the long run this could lead to long-term biological “costs” or even medical disorders. However, no well-controlled epidemiological study is available that compares the effects of permanent, slowly and quickly rotating shift systems. In most published studies the groups are not comparable with regard to the age structure, job content, degree of self-selection (e.g., Tasto et al. 1978; Costa et al. 1981) or because the employees working on fixed morning, afternoon and night shifts were combined to form a single category (Jamal and Jamal 1982). In several longitudinal field studies, the effects of a change from weekly to quicker rotating shift systems have been investigated (Williamson and Sanderson 1986; Knauth and Kiesswetter 1987; Knauth and Schönfelder 1990; Hornberger and Knauth 1995; Knauth 1996). In all 27 studied groups of shiftworkers, the majority of the shiftworkers voted in favour of the quicker rotating shifts after a trial period. Summing up, quickly rotating shift systems are preferable to slowly rotating ones. Åkerstedt (1988), however, does not agree, because the maximum sleepiness usually occurs on the first night shift because of extended prior waking. He recommends slow rotation.
Another argument for a quickly rotating shift system is that shiftworkers have free evenings in every week and thus more regular contact with friends and colleagues is possible than with weekly rotating shifts. Based on analyses of the periodic components of work and leisure time, Hedden et al. (1990) conclude that rotations that allow for a shorter but more frequent synchronization of work life with social life result in less impairment than rotations that lead to longer but infrequent synchronization.
Duration of shifts
There are many contradictory results of the effects of extended workdays, and thus a general recommendation for extended workdays cannot be made (Kelly and Schneider 1982; Tepas 1985). An extended workday of 9 to 12 hours should be contemplated only in the following cases (Knauth and Rutenfranz 1982; Wallace 1989; Tsaneva et al. 1990; Ong and Kogi 1990):
- The nature of work and the workload are suitable for extended working hours.
- The shift system is designed to minimize the accumulation of fatigue.
- There are adequate arrangements for cover of absentees.
- Overtime is not added.
- Toxic exposure is limited.
- It is likely that a complete recovery after work and a high acceptance of the working time arrangements are possible (e.g., housing, family problems, commuting, climate, no moonlighting).
Physiological requirements must be taken into account. According to Bonjer (1971), the acceptable oxygen rate consumption during an 8-hour shift should be about 30% or less of the maximum oxygen consumption. During a 12-hour shift it should be about 23% or less of the maximum oxygen consumption. Since the amount of oxygen consumption increases with the physical demands of the job, it would seem that 12-hour shifts are acceptable only for physically light work. However, even in this case, if the mental or emotional stress caused by the job is too high, extended working hours are not advisable. Before the introduction of extended working hours, the stress and strain at the specific workplace must be accurately evaluated by experts.
One of the potential disadvantages of 12-hour shifts, in particular 12-hour night shifts, is increased fatigue. Therefore the shift system should be designed to minimize the accumulation of fatigue—that is, there should not be many 12-hour shifts in a row and the day shift should not start too early. Koller et al. (1991) recommend single night shifts or a maximum of two night shifts. This recommendation is supported by favourable results of studies in shift systems with single 12-hour night shifts (Nachreiner et al. 1975; Nedeltcheva et al. 1990). In a Belgian study, the length of the shift was extended to 9 hours by starting one hour earlier in the morning (Moors 1990). The day shift started at 0630 instead of 0730 and the morning shift in a two-shift system started at 0500 instead of 0600. In a 5-day week these working time arrangements led to an accumulation of sleep deficits and complaints of tiredness. The author recommends that the shifts start as in the old working time arrangements and that the shift be extended by one hour in the evening.
Our knowledge is very limited concerning another problem: toxic exposure and toxic clearance during the time off work in connection with extended working hours (Bolt and Rutenfranz 1988). In general, exposure limits are based on 8 hours exposure, and one cannot simply extrapolate them to cover a 12-hour shift. Some authors have proposed mathematical procedures for adjusting these exposures for working times that deviate from the usual 8-hour shift, but no method has been uniformly adopted (e.g., Hickey and Reist 1977; OSHA 1978; Brief and Scala 1986; Koller et al. 1991).
Designers of shift systems must consider the workload, the working environment and the conditions outside the place of work. Ong and Kogi (1990) report that “the hot, tropical climate and noisy dwelling units of Singapore were not conducive to sound sleep for shiftworkers, who needed to sleep in the daytime”. Such circumstances increased fatigue and affected productivity on the 12-hour shift worked the next day. Another concern that relates to workers’ well-being is the way shiftworkers use their large blocks of leisure time. In some studies it appears that they may have second jobs (moonlighting), thus increasing their total workload (Angersbach et al. 1980; Wallace 1989; Ong and Kogi 1990). Many other social factors, like commuting, individual differences, social support or events in life must also be considered in the 12-hour shift systems (e.g., Tsaneva et al. 1990).
Timing of shifts
Although there is no optimal solution for the timing of shifts, there is much evidence in the literature that an early start for the morning shift should be avoided. An early start often reduces total sleep because the majority of shiftworkers go to bed at the usual time (Knauth et al. 1980; Åkerstedt et al. 1990; Costa et al. 1990b; Moors 1990; Folkard and Barton 1993). An increase in fatigue during the morning shift has also been observed (Reinberg et. al. 1975; Hak and Kampman 1981; Moors 1990), as well as an increase in the risk of errors and accidents in the morning shift (Wild and Theis 1967; Hildebrandt et al. 1974; Pokorny et al. 1981; Folkard and Totterdell 1991).
Assuming a constant shift length of 8 hours, a late start for the morning shift also means a late start for the night shift (e.g., shift change times at 0700/1500/2300 or 0800/1600/2400). A late start for the night shift means also a late end for the evening shift. In both cases there might be transport problems because buses, trams and trains run less frequently.
The decision in favour of a specific shift change time may also be dependent on the job content. In hospitals, in general, it is the night shift that wakes up, washes and prepares patients (Gadbois 1991).
Arguments in favour of an earlier start have also been made. Some studies have shown that the later the day sleep begins after a night shift, the shorter it will be (Foret and Lantin 1972; Åkerstedt and Gillberg 1981; Knauth and Rutenfranz 1981). Day sleep may be disturbed and a very early start of sleep after night shifts might avoid these problems. Debry et al. (1967) have proposed shift change times at 0400, 1200 and 2000 in order to facilitate workers having as many meals with the family as possible. According to Gadbois (1991) an early start for the night shift improves the contact between staff and patients in hospitals.
Flexible working time arrangements are also possible even in three-shift systems, where employees can choose their working hours (McEwan 1978; Knauth et al. 1981b; 1984; Knauth and Schönfelder 1988). However, in contrast to flexitime in dayworkers, shiftworkers must make pre-arrangements with co-workers.
Distribution of leisure time within the shift system
The distribution of leisure time between consecutive shifts has important implications for sleep, fatigue and well-being, as well as social and family life and the overall satisfaction of the shiftworker with the shift system. If there are only 8 hours between the end of one shift and the start of the next, there will be a reduction of sleep between the shifts and increased fatigue in the second shift (Knauth and Rutenfranz 1972; Saito and Kogi 1978; Knauth et al. 1983; Totterdell and Folkard 1990).
Too many working days in succession can lead to an accumulation of fatigue and sometimes overexposure to toxic substances (Bolt and Rutenfranz 1988). It is not easy to define a limit for the maximum number of consecutive working days, because the workload, the organization of breaks, and exposure to unfavourable environmental conditions vary. However, Koller et al. (1991) recommend limiting the number of consecutive working days to between 5 and 7.
Free weekends are of particular social importance. Pátkei and Dahlgren (1981) studied satisfaction with different types of rapidly rotating shift systems. The satisfaction with a 7-day shift system with 3 to 5 regular days free was significantly higher than in a system with only 2 free days. The authors concluded that “the length of the break might be an important factor in determining the attractivity of rapidly rotating shifts”. On the other hand, free days in the first shift system were counterbalanced by additional periods of holidays during the year.
Direction of rotation. The direction of rotation is another important consideration (Tsaneva et al. 1987; Totterdell and Folkard 1990). A shift system which first moves from morning shift to evening shift, and then to night shift, has a forward rotation (phase delay, clockwise rotation). An anticlockwise, or backward, rotation has a phase advance which moves from night to evening to morning shifts. The forward rotation appears to correspond more closely to the endogenous circadian rhythm, which has a period of more than 24 hours, but only two longitudinal field studies on the effects of different directions of rotation exist (Landen et al. 1981; Czeisler et al. 1982). The majority of the shiftworkers in these studies seem to prefer the forward rotation, but the studies are not definitive. Barton and Folkard (1993) found that an anticlockwise system led to higher levels of fatigue and more sleep disturbances between shifts. “Hybrid” systems were not better. Clockwise rotation was associated with the fewest problems. Turek (1986) proposes, however, that the sleep disturbance of both systems would be comparable.
Shiftworkers on a discontinuous shift system with backward rotation were found to like the long period off work between the end of the last morning shift and the start of the first night shift, in particular if this period includes a weekend.
Although the evidence is limited and further research is needed, forward rotation seems to be recommendable at least in continuous shift systems.
Optimizing shift systems
There is no “optimal” shift system. Each enterprise, its managers and shiftworkers should seek the best compromise between the demands of the enterprise and the needs of the workers. Furthermore, the decision should be founded on scientific recommendations for the design of shift systems. The implementation strategy is of particular importance for the acceptance of a new shift system. Many manuals and guidelines for the implementation of new working time arrangements have been published (ILO 1990). Too often shiftworkers are not sufficiently involved in the analysis, planning and design stage of the shifts.
A continuous shift system that has a rapid forward rotation pattern, with 8 hours of work per shift, some free weekends, at least two successive full days off and no quick changeovers, appears to be the system to be recommended. Such a basic shift system has an average of 33.6 hours per week, which may not be universally acceptable. If additional shifts are required, acceptance is higher when the additional shifts are planned on a long-term basis, such as at the beginning of the year so workers can plan holidays. Some employers do not require older shiftworkers to work additional shifts.
Figures 3 and 4 show schemes for continuous and discontinuous shift systems which accommodate these rules. Figure 5 shows a shift system for a less flexible workplace. It covers 128 operational hours per week, with an average individual workweek of 37 hours. This system has a maximum of three night shifts and two longer free weekends (third week: Thursday to Sunday; fifth/sixth week: Saturday to Monday). It is irregular and does not rotate in a forward direction, which is less optimizing. For shift systems with an operational time of 120 hours per week, gradually rotating shift systems cannot be used, such as from Monday 0600 to Saturday 0600, and an average working time of 40 hours per week.
Figure 3. Rotating continuous shift system.
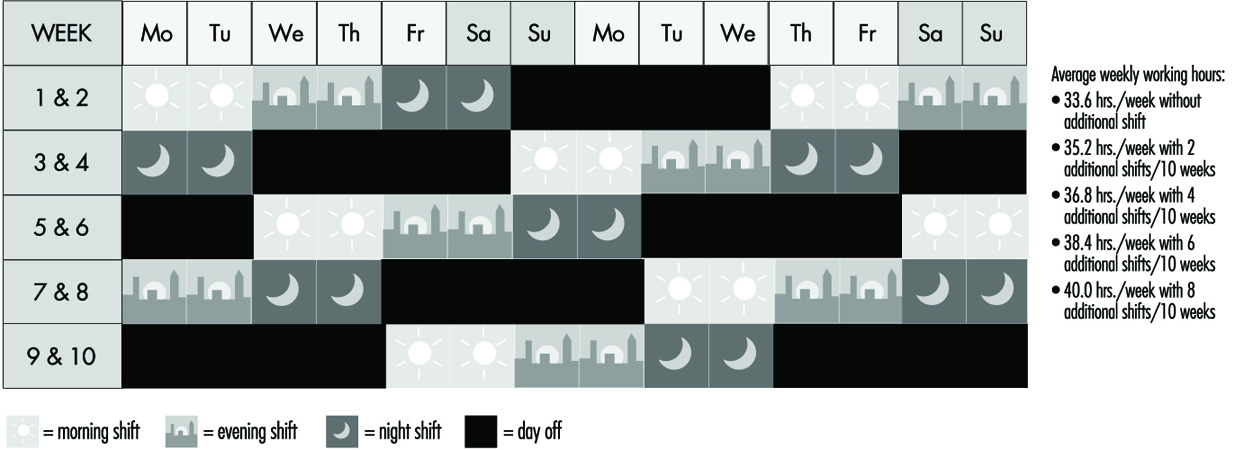
Figure 4. Rotating discontinuous shift system.
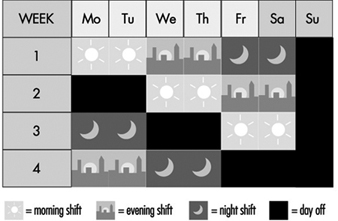
Figure 5. Rotating discontinuous shift system with seven teams.
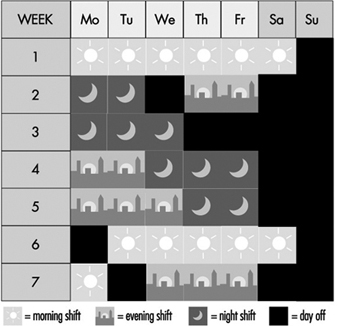
When the crew can be thinned out during the night, a shift system as shown in Figure 6 may be possible. From Monday to Friday, each day two subgroups work in morning shifts, two in evening shifts but only one subgroup works in night shifts. Therefore, the number of night shifts per person would be reduced, compared with the traditional three-shift system.
Figure 6. Discontinuous shift system with a 50% reduced staffing of night shifts.
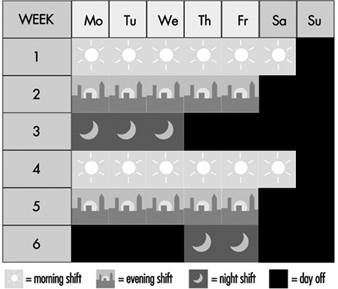
Rest Periods
In connection with the arrangement of hours of work, adequate periods of rest, such as breaks during working hours, breaks for meals, daily or nightly rest and weekly rest are also important for the workers’ well-being, health and safety.
There are various reasons for the introduction of rest periods.
Recuperation
When a worker performs heavy physical work, fatigue develops and it is necessary for the worker to stop and rest at intervals. During the breaks the symptoms of reversible functional changes of the organism disappear. When, for instance, heart rate is increased by physical work, it will return to the initial value before work during an adequate rest period. The efficiency of a rest period decreases exponentially with the increasing length of the break. As short breaks have a high efficiency, the rule has been deduced that many short breaks are better than a few long breaks.
Prevention of fatigue
During heavy physical work, many rest periods may not only reduce, but under certain circumstances, also prevent fatigue. This is illustrated by the classic studies of Karrasch and Müller (1951). In the laboratory, subjects had to exercise on bicycle ergonometers (Figure 7). This heavy physical work (10 mkp/s) was organized in the following way: after each period of work (100%) a longer rest period (150%) followed. The three experiments each had a different arrangement of work and rest periods. In the first experiment the subject worked 5 min, rested for 7.5 min, then worked again for 5 min and broke off the experiment when exhausted. The heart rate reached about 140 beats/minute in the first work period and more than 160 beats/minute in the second work period. Even one hour after the end of the experiment the heart rate had not returned to the initial value before the experiment. The second experiment shown in the figure involved shorter work and shorter rest periods (2 min and 3 min). Although the workload was identical to the first experiment, the subject in the second experiment was able to work longer before complete exhaustion set in. An extreme arrangement of 0.5 min work and 0.75 min rest period was set up in the third experiment. The heart rate remained at the steady-state level. The experiment was stopped, not because the subject was exhausted but for technical reasons. This extreme organization of work and of rest periods of course cannot be implemented in industry, but it illustrates that extreme fatigue may be prevented if rest periods are split up.
This phenomenon has also been demonstrated in other studies with other indicators such as blood lactic acid (Åstrand and Rodahl 1970).
Figure 7. Heart rate during and after heavy physical work with different lengths of work and rest periods but a constant work/rest ratio of 2:3.
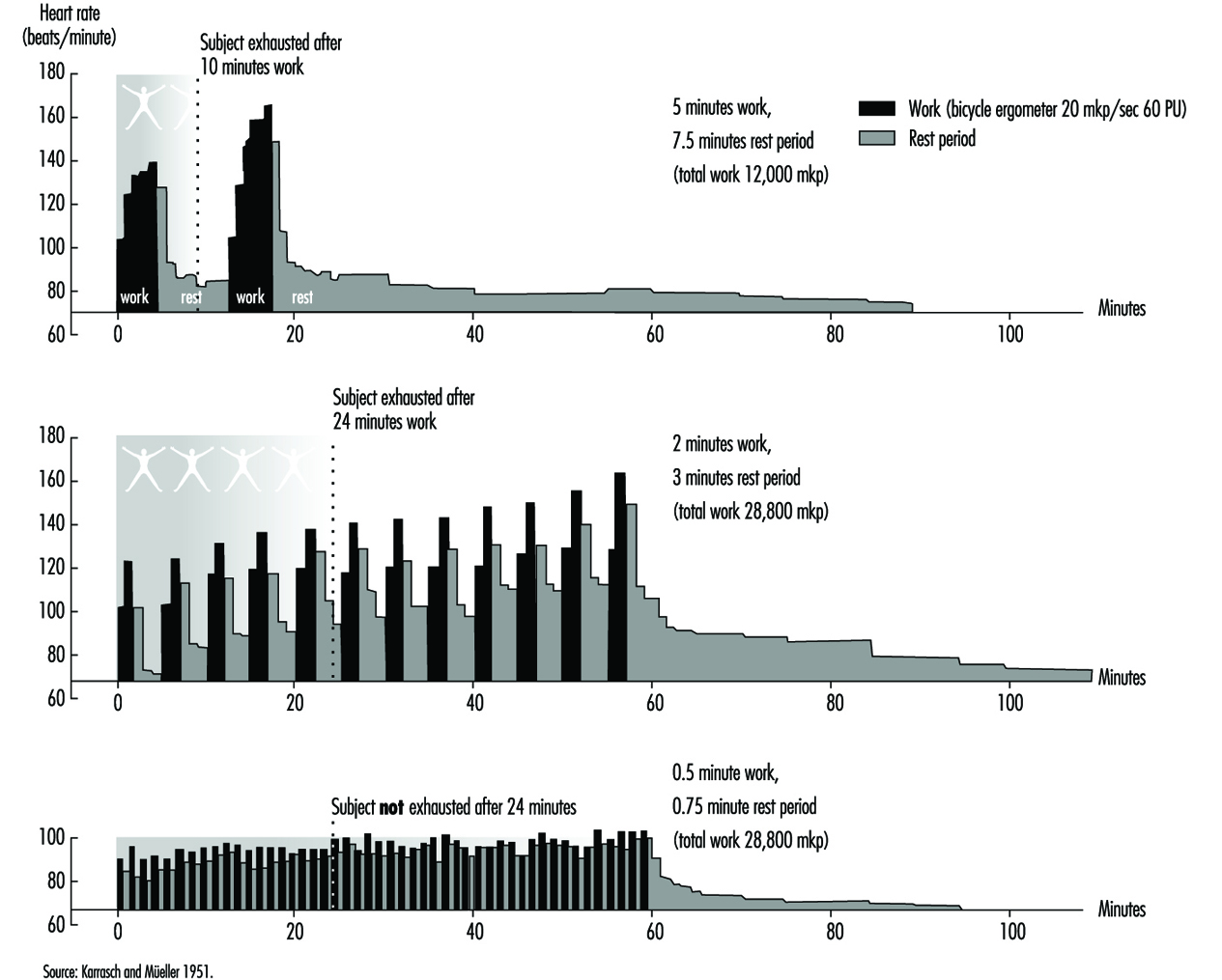
In a study on foundry workers, the comparison of an arrangement of 20 min of work followed always by a 10-min break with an arrangement of 10 min of work and a 5-min break showed the superiority of the second approach (Scholz 1963), because the average heart rate over 8 hours was lower in the second case.
The prevention of fatigue has also been demonstrated with help of heart rate measurements in experiments with learning of sensorimotoric performances (Rutenfranz et al. 1971). Moreover, the progress in learning was clearly greater in experiments with regular rest periods compared with experiments without rest periods, as shown in figure 8.
Figure 8. Effect of rest periods on the learning of simple sensumotoric performance.
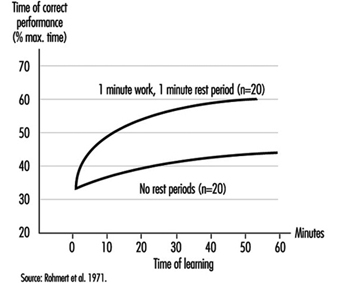
Increase in performance
In general, rest periods are considered simply as unproductive interruptions of working time. However, Graf (1922; 1927) showed that rest periods may be, so-to-speak, “rewarding”. We know from sports that athletes running 100 metres start at a high speed, whereas athletes running 5,000 metres start at a “throttled down” speed. Analogue findings on mental work have been published by Graf (figure 9). Three experimental groups were asked to perform calculations. Wages were dependent on the performance. Without being aware of this fact, group A (having the first rest period after 3 hours) started with a reduced speed compared to group B (expecting the first rest period after 45 minutes of work). The highest initial speed and subsequent performance was found in the group C (with rest periods after each 15 minutes of work).
Figure 9. Effects of short rest periods on mental performance.

Maintaining an adequate level of vigilance
In some monotonous monitoring or watchkeeping tasks and in highly simplified tasks with short cycle times, it is difficult to remain alert over longer periods. The reduction of alertness may be overcome by rest periods (or work-structuring measures).
Food intake
The recuperative value of meal breaks is often limited, in particular when the worker has to go a long distance to the canteen, line up for food, eat quickly and hurry back to the working place.
Compensatory physical exercise
If workers, such as visual display unit operators, have to work in constrained postures, it is recommended that they do some compensatory physical exercises during rest periods. Of course the better solution would be to improve the design of the workplace according to ergonomic principles. Physical exercises at the workplace seem to be more accepted in Asian countries than in many other places.
Communication
The social aspect of rest periods, referring to private communication between the workers, should not be neglected. There is a contradiction between the physiologically based recommendation of very short breaks in connection with heavy physical work and the wish of the workers to come together in rest areas and talk with colleagues. Therefore a compromise has to be found.
Hettinger (1993) has published the following rules for the optimal design of rest periods:
- The initial parts of a rest period have the highest recuperative value, which is what results in the effectiveness of short breaks (i.e., many short breaks are more favourable than a few longer breaks with regard to the recuperative value).
- Exceptions to this rule: The cooling-down rest period after work in a hot climate should last at least 10 min in a room with a neutral climate. The warming-up rest period after work in a cold climate (–15 to –30°C) should last for at least 30 min in a room with a neutral climate. The rest period after working in a very loud working environment should be relatively long in a room with less than 70 dB(A). These rest periods are problematic, if one bears in mind that, if the time of exposure is halved, merely a reduction of about 3 dB(A) is achieved in the noise dose.
- The frequency and duration of the rest period is dependent on the degree of difficulty of the physical or mental work. Concerning physical work, it may be specified that physical work with an energy consumption above the acceptable endurance limit but less than 40 KJ/min permits the rest period to be arranged within the shiftworking time. Physical work with an energy consumption of greater than 40 KJ/min demands a rest period immediately after stopping the heavy work, because of the exponential increase of fatigue.
- The efficiency of a rest period should not be reduced by “pseudo-activities” (disguised breaks). Workers and superiors should be informed accordingly.
Rest periods for food intake should last at least 15 minutes.
For further information concerning rest periods after muscular work, see Laurig (1981); and for rest periods after mental work, see Luczak (1982).
Reduction of Sleep Problems
There are no magic formulae to help shiftworkers fall asleep quickly or sleep well. What works for one person may not work for another.
Some useful proposals, mainly for day sleep following night shifts, include:
- Use individual headphones for TV and radio for the other members of the family, and a silent telephone answering machine. Switch off the door-bell.
- Let one’s family know about the work schedule and avoid household noise during sleep times.
- Reduce outside light and noise by using heavy, dark curtains, soundproofed doors and windows, and an air conditioner.
- Ear plugs, a sleeping mask and not drinking any caffeinated drinks within 5 hours of your expected bedtime can also help.
- If the living quarters are noisy, workers should consider moving to quieter living quarters.
Workers should avoid using alcohol to assist in going to sleep and should give themselves time to slow down after work (Community Health Network 1984; Monk 1988; Wedderburn 1991).
For cases where safety is at stake, some authors recommend “maintenance naps” during the night shift as a bridge over the night-time low point in circadian alertness (Andlauer et al. 1982). Many Japanese 24-hour industries allow napping practices on night shifts (Kogi 1981).
Diet
Although there is no evidence that diet assists in coping with night work (Rosa et al. 1990), the following prudent recommendations have been made:
- During night shift, the main meal should be eaten at or before 0100 and should be rich in protein rather than carbohydrates, and have a low fat content.
- Have a snack of fresh fruit or milk products at about 0400–0415.
- Eating meals at the same time each day is recommended.
- A heavy meal just before bedtime should be avoided. Workers should learn to listen to their bodies, to judge stomach comfort and energy levels (Community Health Network 1984; Wedderburn 1991; Knauth et al. 1991).
Occupational Health Measures
Some authors recommend pre-employment screening and medical surveillance of shiftworkers (e.g., Rutenfranz et al. 1985; Scott and LaDou 1990). Workers should be counselled against night work if they have or are:
- a history of digestive tract disorders (e.g., recurrent peptic ulcer disease, irritable bowel syndrome, if symptoms are severe)
- insulin-dependent diabetes mellitus
- thyrotoxicosis
- coronary artery disease, especially if there is unstable angina or a history of myocardial infarction
- narcoleptics and others suffering from chronic sleep disturbances
- epileptics
- severe psychiatric disorders, in particular chronic depression
- asthma requiring medication, especially if the patient is steroid dependent
- active and extensive tuberculosis
- alcoholics and drug addicts
- marked visual impairment or hemeralopia (day blindness) that is too severe for effective correction.
In addition, Scott and LaDou (1990) also mention some “relative contra-indications” most appropriately used for counselling prospective employees, such as extreme “morningness”, sleep rigidity. They may wish to consider their age and the extent of their family responsibilities.
Hermann (1982) has proposed the following intervals for regular health checks: there should be a second health check not later than 12 months after starting night work, and regular health checks at least every 2 years for those under 25, every 5 years for those between 25 and 50, every 2 to 3 years for those between 50 and 60, and every 1 to 2 years for those above 60.
Individual Behavioural Techniques
There are only a few studies analysing shiftworkers’ ability to cope with stress (Olsson et al. 1987; Olsson and Kandolin 1990; Kandolin 1993, Spelten et al. 1993). An active coping strategy—for example, discussing the problems with others—appears to reduce stress better than passive strategies, such as the use of alcohol (Kandolin 1993). However, longitudinal studies are necessary to study the relationship between coping style or behavioural techniques and stress.
Money Payments
Although many compensation plans exist whereby a worker is compensated more for shiftwork (shift bonus), money payments are not an appropriate trade-off for possible negative health effects and disruption of social life.
The best way, of course, to solve problems is to eliminate or reduce the causes. However, since complete elimination of shiftwork is not possible, an alternative strategy worth considering is such as the following: a reduction of unusual working hours for the individual; reduction of night shifts; reduce the unnecessary part of the night work (sometimes activities may be shifted to the morning or evening shift by reorganization of work); implement mixed shift systems with, for example, at least one month per year without shiftwork; insertion of additional shift crews, such as by changing from a 3-shift system to a 4-shift system or from a 4-shift system to a 5-shift system, or by reduction of overtime. Reduction of working time for shiftworkers is another possibility, with shorter weekly working hours for shiftworkers than for dayworkers, with paid breaks and longer holiday periods. Extra days off and stepwise or early retirement are other possible remedies.
All these proposals have already been implemented in some companies in industry or the services sector (e.g., Knauth et al. 1990).
Other Measures
Many other measures such as physical exercise (Härmä et al. 1988a, b), pharmacological aids (Rosa et al. 1990), family counselling (Rosa et al. 1990), improvement of environmental conditions at work (Knauth et al. 1989), better communication between shiftworkers and unions or shiftworkers and their congressperson (Monk 1988; Knauth et al. 1989), or a “Shift Work Awareness Programme” within the company (Monk 1988) have been proposed to reduce the problems of shiftworkers. As there is not one best way to reduce the problems of shiftworkers many creative solutions should be tried (Colquhoun et al. 1996).
Cold Indices and Standards
Cold stress is defined as a thermal load on the body under which greater than normal heat losses are anticipated and compensatory thermoregulatory actions are required to maintain the body thermally neutral. Normal heat losses, hence, refer to what people normally experience during indoor living conditions (air temperature 20 to 25ºC).
In contrast to conditions in the heat, clothing and activity are positive factors in the sense that more clothing reduces heat loss and more activity means higher internal heat production and a greater potential for balancing heat loss. Accordingly, assessment methods focus on the determination of required protection (clothing) at given activity levels, required activity levels for given protection or “temperature” values for given combinations of the two (Burton and Edholm 1955; Holmér 1988; Parsons 1993).
It is important to recognize, however, that there are limits as to how much clothing can be worn and how high a level of activity can be sustained for extended time periods. Cold-protective clothing tends to be bulky and hobbling. More space is required for motion and movements. Activity level may be determined by paced work but should, preferably, be controlled by the individual. For each individual there is a certain highest energy production rate, depending on physical work capacity, that can be sustained for prolonged time periods. Thus, high physical work capacity may be advantageous for prolonged, extreme exposures.
This article deals with methods for assessment and control of cold stress. Problems related to organizational, psychological, medical and ergonomic aspects are dealt with elsewhere.
Cold Work
Cold work encompasses a variety of conditions under natural as well as artificial conditions. The most extreme cold exposure is associated with missions in outer space. However, cold working conditions on the surface of the earth cover a temperature range of more than 100ºC (table 1). Naturally, the magnitude and severity of cold stress will be expected to increase with lowered ambient temperature.
Table 1. Air temperatures of various cold occupational environments
|
–120 ºC |
Climatic chamber for human cryotherapy |
|
–90 ºC |
Lowest temperature at south polar base Vostock |
|
–55 ºC |
Cold store for fish meat and production of frozen, dried products |
|
–40 ºC |
“Normal” temperature at polar base |
|
–28 ºC |
Cold store for deep-frozen products |
|
+2 to +12 ºC |
Storage, preparation and transportation of fresh, alimentary products |
|
–50 to –20 ºC |
Average January temperature of northern Canada and Siberia |
|
–20 to –10 ºC |
Average January temperature of southern Canada, northern Scandinavia, central Russia |
|
–10 to 0 ºC |
Average January temperature of northern USA, southern Scandinavia, central Europe, parts of middle and far East, central and northern Japan |
Source: Modified from Holmér 1993.
It is clear from 1 table that large populations of outdoor workers in many countries experience more or less severe cold stress. In addition cold store work occurs in all parts of the world. Surveys in Scandinavian countries reveal that approximately 10% of the total worker population regard cold as a major annoyance factor in the workplace.
Types of Cold Stress
The following types of cold stress can be defined:
- whole-body cooling
- local cooling, including extremity cooling, convective skin cooling (wind chill), conductive skin cooling (contact cooling) and cooling of respiratory tract.
Most likely, several if not all of these may be present at the same time.
The assessment of cold stress involves the ascertainment of a risk of one or more of the mentioned effects. Typically, table 2 may be used as a first rough classification. In general cold stress increases, the lower the level of physical activity and the less protection available.
Table 2. Schematic classification of cold work
|
Temperature |
Type of work |
Type of cold stress |
|
10 to 20 ºC |
Sedentary, light work, fine manual work |
Whole-body cooling, extremity cooling |
|
0 to 10 ºC |
Sedentary and stationary, light work |
Whole-body cooling, extremity cooling |
|
–10 to 0 ºC |
Light physical work, handling tools and materials |
Whole-body cooling, extremity cooling, contact cooling |
|
–20 to –10 ºC |
Moderate activity, handling metals and fluids (petrol etc.), windy conditions |
Whole-body cooling, extremity cooling, contact cooling, convective cooling |
|
Below –20 ºC |
All types of work |
All types of cold stress |
Information given in the table should be interpreted as a signal to action. In other words, the particular type of cold stress should be evaluated and controlled, if required. At moderate temperatures problems associated with discomfort and losses of function due to local cooling prevail. At lower temperatures the imminent risk of a cold injury as a sequel to the other effects is the important factor. For many of the effects discrete relationships between stress level and effect do not yet exist. It cannot be excluded that a particular cold problem may persist also outside the range of temperatures denoted by the table.
Assessment Methods
Methods for assessment of cold stress are presented in ISO Technical Report 11079 (ISO TR 11079, 1993). Other standards concerning determination of metabolic heat production (ISO 8996, 1988), estimation of clothing thermal characteristics (ISO 9920, 1993), and physiological measurements (ISO DIS 9886, 1989c) provide complementary information useful for the evaluation of cold stress.
Figure 1 outlines the relationships between climate factors, anticipated cooling effect and recommended method for assessment. Further details about methods and data collection are given below.
Figure 1. Assessment of cold stress in relation to climatic factors and cooling effects.
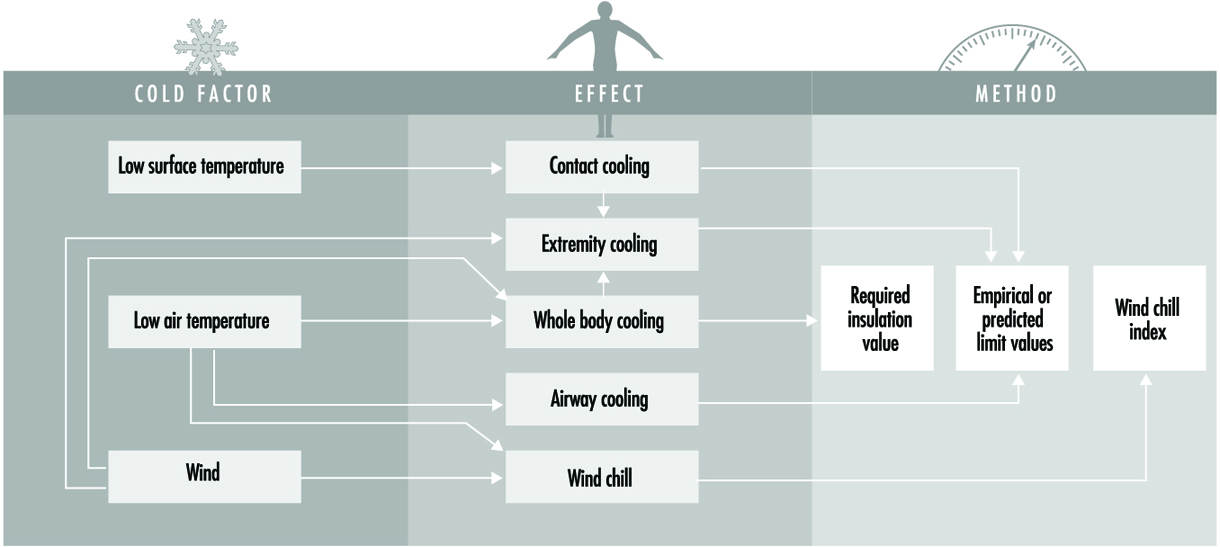
Whole-Body Cooling
The risk of whole-body cooling is determined by analysing the conditions for body heat balance. The clothing insulation level required for heat balance at defined levels of physiological strain, is calculated with a mathematical heat balance equation. The calculated required insulation value, IREQ, can be regarded as a cold stress index. The value indicates a protection level (expressed in clo). The higher the value, the greater the risk of body heat imbalance. The two levels of strain correspond to a low level (neutral or “comfort” sensation) and a high level (slightly cold to cold sensation).
Using IREQ comprises three evaluation steps:
- determination of IREQ for given exposure conditions
- comparison of IREQ with protection level provided by clothing
- determination of exposure time if protection level is of lesser value than IREQ
Figure 2 shows IREQ values for low physiological strain (neutral thermal sensation). Values are given for different activity levels.
Figure 2. IREQ values needed to maintain low-level physiological strain (neutral thermal sensation) at varying temperature.
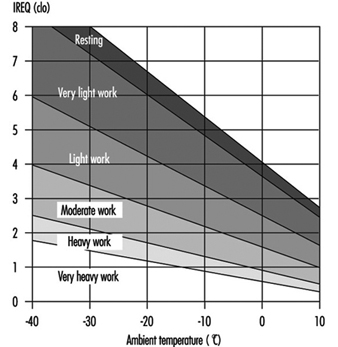
Methods to estimate activity levels are described in ISO 7243 (table 3).
Table 3. Classification of levels of metabolic rate
|
Class |
Metabolic rate range, M |
Value to be used for calculation of mean metabolic rate |
Examples |
||
|
Related to |
For a mean skin surface area |
|
|
||
|
0 |
M≤65 |
M≥117 |
65 |
117 |
Resting |
|
1 |
65M≤130 |
117M≤234 |
100 |
180 |
Sitting at ease: light manual work (writing, typing, drawing, sewing, book-keeping); hand and arm work (small bench tools, inspection, assembly or sorting of light material); arm and leg work (driving vehicle in normal conditions, operating foot switch or pedals). Standing: drill (small parts); milling machine (small parts); coil winding; small armature winding; machining with low power tools; casual walking (speed up to 3.5 km/h). |
|
2 |
130M≤200 |
234M≤360 |
165 |
297 |
Sustained hand and arm work (hammering in nails, filling); arm and leg work (off-road operation of lorries, tractors or construction equipment); arm and trunk work (work with pneumatic hammer, tractor assembly, plastering, intermittent handling of moderately heavy material, weeding, hoeing, picking fruit or vegetables); pushing or pulling light weight carts or wheelbarrows; walking at a speed of 3.5 km/h; forging. |
|
3 |
200M≤260 |
360M≤468 |
230 |
414 |
Intense arm and trunk work: carrying heavy material; shoveling; sledge hammer work; sawing, planning or chiselling hard wood; hand mowing; digging; walking at a speed of 5.5 km/h to 7 km/h. Pushing or pulling heavily loaded handcarts or wheelbarrows; chipping castings; concrete block laying. |
|
4 |
M>260 |
M>468 |
290 |
522 |
Very intensive activity at fast to maximum pace; working with an axe; intense shovelling or digging; climbing stairs, ramp or ladder; walking quickly with small steps, running, walking at a speed greater than 7 km/h. |
Source: ISO 7243 1989a
Once IREQ is determined for given conditions, the value is compared with the protection level offered by clothing. Protection level of a clothing ensemble is determined by its resultant insulation value (“clo-value”). This property is measured according to the draft European standard prEN-342 (1992). It can also be derived from basic insulation values provided in tables (ISO 9920).
Table 4. provides examples of basic insulation values for typical ensembles. Values must be corrected for presumed reduction caused by body motion and ventilation. Typically, no correction is made for resting level. Values are reduced by 10% for light work and by 20% for higher activity levels.
Table 4. Examples of basic insulation values (Icl) of clothing*
|
Clothing ensemble |
Icl (m2 ºC/W) |
Icl (clo) |
|
Briefs, short-sleeve shirt, fitted trousers, calf-length socks, shoes |
0.08 |
0.5 |
|
Underpants, shirt, fitted, trousers, socks, shoes |
0.10 |
0.6 |
|
Underpants, coverall, socks, shoes |
0.11 |
0.7 |
|
Underpants, shirt, coverall, socks, shoes |
0.13 |
0.8 |
|
Underpants, shirt, trousers, smock, socks, shoes |
0.14 |
0.9 |
|
Briefs, undershirt, underpants, shirt, overalls, calf-length socks, shoes |
0.16 |
1.0 |
|
Underpants, undershirt, shirt, trousers, jacket, vest, socks, shoes |
0.17 |
1.1 |
|
Underpants, shirt, trousers, jacket, coverall, socks, shoes |
0.19 |
1.3 |
|
Undershirt, underpants, insulated trousers, insulated jacket, socks, shoes |
0.22 |
1.4 |
|
Briefs, T-shirt, shirt, fitted trousers, insulated coveralls, calf-length socks, shoes |
0.23 |
1.5 |
|
Underpants, undershirt, shirt, trousers, jacket, overjacket, hat, gloves, socks, shoes |
0.25 |
1.6 |
|
Underpants, undershirt, shirt, trousers, jacket, overjacket, overtrousers, socks, shoes |
0.29 |
1.9 |
|
Underpants, undershirt, shirt, trousers, jacket, overjacket, overtrousers, socks, shoes, hat, gloves |
0.31 |
2.0 |
|
Undershirt, underpants, insulated trousers, insulated jacket, overtrousers, overjacket, socks, shoes |
0.34 |
2.2 |
|
Undershirt, underpants, insulated trousers, insulated jacket, overtrousers, socks, shoes, hat, gloves |
0.40 |
2.6 |
|
Undershirt, underpants, insulated trousers, insulated jacket, overtrousers and parka with lining, socks, shoes, hat, mittens |
0.40–0.52 |
2.6–3.4 |
|
Arctic clothing systems |
0.46–0.70 |
3–4.5 |
|
Sleeping bags |
0.46–1.1 |
3–8 |
*Nominal protection level applies only to static, windstill conditions (resting). Values must be reduced with increased activity level.
Source: Modified from ISO/TR-11079 1993.
The protection level offered by the best available clothing systems corresponds to 3 to 4 clo. When the available clothing system does not provide sufficient insulation, a time limit is calculated for the actual conditions. This time limit depends on the difference between required clothing insulation and that of the available clothing. Since, full protection against cooling is no longer achieved, the time limit is calculated on the basis of an anticipated reduction of body heat content. Similarly, a recovery time can be calculated to restore the same amount of heat.
Figure 3 shows examples of time limits for light and moderate work with two insulation levels of clothing. Time limits for other combinations may be estimated by interpolation. Figure 4 can be used as a guideline for assessment of exposure time, when the best cold protective clothing is available.
Figure 3. Time limits for light and moderate work with two insulation levels of clothing.
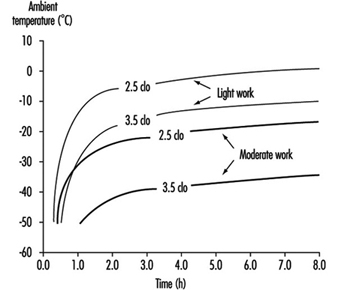
Figure 4. Time-weighted IREQ values for intermittent and continuous exposure to cold.
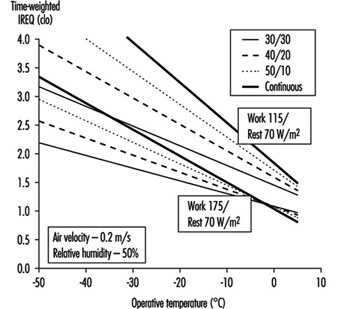
Intermittent exposures typically comprise work periods interrupted by warm-up breaks or by work periods in a warmer environment. In most conditions, little or no replacement of clothing takes place (mostly for practical reasons). IREQ may then be determined for the combined exposure as a time-weighted average. Averaging period must not be longer than one to two hours. Time-weighted IREQ values for some types of intermittent exposure are given in figure 4.
IREQ values and time limits should be indicative rather than normative. They refer to the average person. The individual variation in terms of characteristics, requirements and preferences is large. Much of this variation must be handled by selecting clothing ensembles with great flexibility in terms of, for example, adjustment of the protection level.
Extremity Cooling
The extremities—in particular, fingers and toes—are susceptible to cooling. Unless sufficient heat input by warm blood can be maintained, tissue temperature progressively falls. Extremity blood flow is determined by energetic (required for muscles activity) as well as thermoregulatory needs. When whole-body thermal balance is challenged, peripheral vasoconstriction helps to reduce core heat losses at the expense of peripheral tissues. With high activity more heat is available and extremity blood flow can more easily be maintained.
The protection offered by handwear and footwear in terms of reducing heat losses is limited. When heat input to the extremity is low (e.g., with resting or low activity), the insulation required to keep hands and feet warm is very large (van Dilla, Day and Siple 1949). The protection offered by gloves and mittens only provides retardation of cooling rate and, correspondingly, longer times to reach a critical temperature. With higher activity levels, improved protection allows warm hands and feet at lower ambient temperatures.
No standard method is available for assessment of extremity cooling. However, ISO TR 11079 recommends 24ºC and 15ºC as critical hand temperatures for levels of low and high stress, respectively. Fingertip temperature may easily be 5 to 10 °C lower than the average hand skin temperature or simply the temperature of the back of the hand.
The information given in figure 5 is useful when determining acceptable exposure times and required protection. The two curves refer to conditions with and without vasoconstriction (high and low activity level). Furthermore, it is assumed that finger insulation is high (two clo) and adequate clothing is used.
Figure 5. Finger protection.
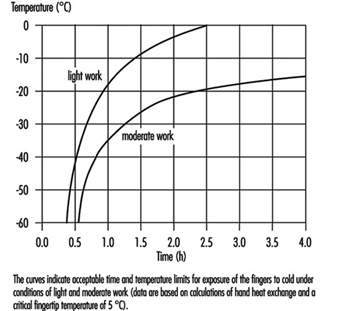
A similar set of curves should apply to toes. However, more clo may be available for protection of feet, resulting in longer exposure times. Nevertheless, it follows from figures 3 and 5 that extremity cooling most likely is more critical for exposure time than whole-body-cooling.
Protection provided by handwear is evaluated by using methods described in the European standard EN-511 (1993). Thermal insulation of the whole handwear is measured with an electrically heated hand model. A wind speed of 4 m/s is used to simulate realistic wear conditions. Performance is given in four classes (table 5).
Table 5. Classification of thermal resistance (I) to convective cooling of handwear
|
Class |
I (m2 ºC/W) |
|
1 |
0.10 ≤ I 0.15 |
|
2 |
0.15 ≤ I 0.22 |
|
3 |
0.22 ≤ I 0.30 |
|
4 |
I ≤ 0.30 |
Source: Based on EN 511 (1993).
Contact Cold
Contact between bare hand and cold surfaces may quickly reduce skin temperature and cause freezing injury. Problems may arise with surface temperatures as high as 15ºC. In particular, metal surfaces provide excellent conductive properties and may quickly cool contacting skin areas.
At present no standard method exists for general assessment of contact cooling. The following recommendations can be given (ACGIH 1990; Chen, Nilsson and Holmér 1994; Enander 1987):
- Prolonged contact with metal surfaces below 15ºC may impair dexterity.
- Prolonged contact with metal surfaces below 7ºC may induce numbness.
- Prolonged contact with metal surfaces below 0ºC may induce frostnip or frostbite.
- Brief contact with metal surfaces below –7ºC may induce frostnip or frostbite.
- Any contact with liquids at subzero temperature must be avoided.
Other materials present a similar sequence of hazards, but temperatures are lower with less conducting material (plastics, wood, foam).
Protection against contact cooling provided by handwear can be determined using the European standard EN 511. Four performance classes are given (table 6).
Table 6. Classification of contact thermal resistance of handwear (I)
|
Class |
I (m2 ºC/W) |
|
1 |
0.025 ≤ I 0.05 |
|
2 |
0.05 ≤ I 0.10 |
|
3 |
0.10 ≤ I 0.15 |
|
4 |
I ≤ 0.15 |
Source: Based on EN 511 (1993).
Convective Skin Cooling
The Wind Chill Index (WCI) represents a simple, empirical method for assessment of cooling of unprotected skin (face) (ISO TR 11079). The method predicts tissue heat loss on the basis of air temperature and wind speed.
Responses associated with different values of WCI are denoted in table 7.
Table 7. Wind Chill Index (WCI), equivalent cooling temperature (Teq ) and freezing time of exposed flesh
|
WCI (W/m2) |
Teq (ºC) |
Effect |
|
1,200 |
–14 |
Very cold |
|
1,400 |
–22 |
Bitterly cold |
|
1,600 |
–30 |
Exposed flesh freezes |
|
1,800 |
–38 |
within 1 hour |
|
2,000 |
–45 |
Exposed flesh freezes |
|
2,200 |
–53 |
within 1 minute |
|
2,400 |
–61 |
Exposed flesh freezes |
|
2,600 |
–69 |
within 30 seconds |
A frequently used interpretation of WCI is the equivalent cooling temperature. This temperature under calm conditions (1.8 m/s) represents the same WCI value as the actual combination of temperature and wind. Table 8 provides equivalent cooling temperatures for combinations of air temperature and wind speed. The table applies to active, well-dressed persons. A risk is present when equivalent temperature drops below –30ºC, and skin may freeze within 1 to 2 min below –60ºC.
Table 8. Cooling power of wind on exposed flesh expressed as an equivalent cooling temperature under almost calm conditions (wind speed 1.8 m/s)
|
Wind speed (m/s) |
Actual thermometer reading (ºC) |
||||||||||
|
0 |
–5 |
–10 |
–15 |
–20 |
–25 |
–30 |
–35 |
–40 |
–45 |
–50 |
|
|
Equivalent cooling temperature (ºC) |
|||||||||||
|
1.8 |
0 |
–5 |
–10 |
–15 |
–20 |
–25 |
–30 |
–35 |
–40 |
–45 |
–50 |
|
2 |
–1 |
–6 |
–11 |
–16 |
–21 |
–27 |
–32 |
–37 |
–42 |
–47 |
–52 |
|
3 |
–4 |
–10 |
–15 |
–21 |
–27 |
–32 |
–38 |
–44 |
–49 |
–55 |
–60 |
|
5 |
–9 |
–15 |
–21 |
–28 |
–34 |
–40 |
–47 |
–53 |
–59 |
–66 |
–72 |
|
8 |
–13 |
–20 |
–27 |
–34 |
–41 |
–48 |
–55 |
–62 |
–69 |
–76 |
–83 |
|
11 |
–16 |
–23 |
–31 |
–38 |
–46 |
–53 |
–60 |
–68 |
–75 |
–83 |
–90 |
|
15 |
–18 |
–26 |
–34 |
–42 |
–49 |
–57 |
–65 |
–73 |
–80 |
–88 |
–96 |
|
20 |
–20 |
–28 |
–36 |
–44 |
–52 |
–60 |
–68 |
–76 |
–84 |
–92 |
–100 |
Underlined values represent a risk for frostnip or frostbite.
Cooling of Respiratory Tract
Inhaling cold, dry air may cause problems for sensitive persons at +10 to 15ºC. Healthy persons performing light to moderate work require no particular protection of the respiratory tract down to –30ºC. Very heavy work during prolonged exposures (e.g., athletic endurance events) should not take place at temperatures below –20ºC.
Similar recommendations apply to cooling of the eye. In practice, the great discomfort and visual impairment associated with eye cooling normally require the use of goggles or other protection long before the exposure becomes hazardous.
Measurements
Depending on type of expected risk, different sets of measurements are required (figure 6). Procedures for data collection and accuracy of measurements depend on the purpose of the measurements. Pertinent information must be obtained regarding variation in time of the climatic parameters, as well as of activity level and/or clothing. Simple time-weighting procedures should be adopted (ISO 7726).
Figure 6. The relationship of expected cold stress risk to required measurement procedures.
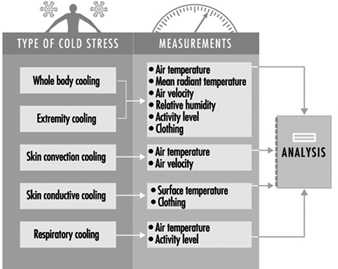
Preventive Measures for Alleviation of Cold Stress
Actions and measures for the control and reduction of cold stress imply a number of considerations during the planning and preparatory phases of work shifts, as well as during work, which are dealt with elsewhere in this chapter and this Encyclopaedia.
Prevention of Cold Stress in Extreme Outdoor Conditions
The prevention of the physiopathological effects of exposure to cold must be considered from two points of view: the first concerns the physiopathological effects observed during general exposure to cold (that is, the entire body), and the second concerns those observed during local exposure to cold, mainly affecting the extremities (hands and feet). Preventive measures in this connection aim to reduce the incidence of the two main types of cold stress—accidental hypothermia and frostbite of the extremities. A twofold approach is required: physiological methods (e.g., adequate feeding and hydration, development of adaptational mechanisms) and pharmacological and technological measures (e.g., shelter, clothing). Ultimately all these methods aim to increase tolerance to cold at both the general and local levels. Moreover, it is essential that workers exposed to cold have the information and the understanding of such injury needed to ensure effective prevention.
Physiological Methods for Preventing Cold Injury
Exposure to cold in the human being at rest is accompanied by peripheral vasoconstriction, which limits cutaneous heat loss, and by metabolic heat production (essentially by means of the activity of shivering), which implies the necessity of food intake. The expenditure of energy required by all physical activity in the cold is increased on account of the difficulty of walking in snow or on ice and the frequent need to deal with heavy equipment. Moreover, water loss may be considerable on account of the sweating associated with this physical activity. If this water loss is not compensated for, dehydration may occur, increasing susceptibility to frostbite. The dehydration is often aggravated not only by voluntary restriction of water intake because of the difficulty of taking in adequate fluid (available water may be frozen, or one may have to melt snow) but also by the tendency to avoid adequately frequent micturition (urination), which requires leaving the shelter. The need for water in the cold is difficult to estimate because it depends on the individual’s workload and on the insulation of the clothing. But in any case, fluid intake must be abundant and in the form of hot drinks (5 to 6 l per day in the case of physical activity). Observation of the colour of the urine, which must remain clear, gives a good indication of the course of fluid intake.
As regards caloric intake, it may be assumed that an increase of 25 to 50% in a cold climate, as compared with temperate or hot climates, is necessary. A formula allows the calculation of the caloric intake (in kcal) essential for energy equilibrium in the cold per person and per day: kcal/person per day = 4,151–28.62Ta, where Ta is the ambient temperature in °C (1 kcal = 4.18 joule). Thus, for a Ta of –20ºC, a need for about 4,723 kcal (2.0 x 104 J) must be anticipated. Food intake does not seem to have to be modified qualitatively in order to avoid digestive troubles of the diarrhoea type. For example, the cold weather ration (RCW) of the United States Army consists of 4,568 kcal (1.9 x 104 J), in dehydrated form, per day and per person, and is divided qualitatively as follows: 58% carbohydrate, 11% protein and 31% fat (Edwards, Roberts and Mutter 1992). Dehydrated foods have the advantage of being light and easy to prepare, but they have to be rehydrated before consumption.
As far as possible, meals must be taken hot and divided into breakfast and lunch in normal amounts. A supplement is provided by hot soups, dry biscuits and cereal bars nibbled throughout the day, and by increasing the caloric intake at dinner. This lattermost expedient augments diet-induced thermogenesis and helps the subject to fall asleep. The consumption of alcohol is extremely inadvisable in a cold climate because alcohol induces cutaneous vasodilatation (a source of heat loss) and increases diuresis (a source of water loss), while modifying the sensitivity of the skin and impairing the judgement (which are basic factors involved in recognizing the first signs of cold injury). Excessive consumption of drinks containing caffeine is also harmful because this substance has a peripheral vasoconstrictor effect (increased risk of frostbite) and a diuretic effect.
In addition to adequate food, the development of both general and local adaptational mechanisms can reduce the incidence of cold injury and improve psychological and physical performance by reducing the stress caused by a cold environment. However, it is necessary to define the concepts of adaptation, acclimatization and habituation to cold, the three terms varying in their implications according to the usage of different theorists.
In Eagan’s view (1963), the term adaptation to cold is a generic term. He groups under the concept of adaptation the concepts of genetic adaptation, acclimatization and habituation. Genetic adaptation refers to physiological changes transmitted genetically that favour survival in a hostile environment. Bligh and Johnson (1973) differentiate between genetic adaptation and phenotypic adaptation, defining the concept of adaptation as “changes which reduce the physiological strain produced by a stressful component of the total environment”.
Acclimatization may be defined as functional compensation that is established over a period of several days to several weeks in response either to complex factors of the surroundings such as climatic variations in a natural environment, or to a unique factor in the surroundings, such as in the laboratory (the “artificial acclimatization” or “acclimation” of those writers) (Eagan 1963).
Habituation is the result of a change in physiological responses resulting from a diminution in the responses of the central nervous system to certain stimuli (Eagan 1963). This habituation can be specific or general. Specific habituation is the process involved when a certain part of the body becomes accustomed to a repeated stimulus, while general habituation is that by which the whole body becomes accustomed to a repeated stimulus. Local or general adaptation to cold is generally acquired through habituation.
Both in the laboratory and in natural surroundings, different types of general adaptation to cold have been observed. Hammel (1963) established a classification of these different adaptational types. The metabolic type of adaptation is shown by maintenance of the internal temperature combined with a greater production of metabolic heat, as in the Alacalufs of Tierra del Fuego or the Indians of the Arctic. Adaptation of the insulational type is also shown by maintenance of the internal temperature but with a diminution in the mean cutaneous temperature (aborigines of the tropical coast of Australia). Adaptation of the hypothermal type is shown by a more or less considerable fall in the internal temperature (tribe of the Kalahari Desert, Quechua Indians of Peru). Finally, there is adaptation of mixed isolational and hypothermal type (aborigines of central Australia, Lapps, Amas Korean divers).
In reality, this classification is merely qualitative in character and does not take into account all the components of thermal balance. We have therefore recently proposed a classification that is not only qualitative but also quantitative (see Table 1). Modification in body temperature alone does not necessarily indicate the existence of general adaptation to cold. Indeed, a change in the delay in starting to shiver is a good indication of the sensitivity of the thermoregulatory system. Bittel (1987) has also proposed reduction in the thermal debt as an indicator of adaptation to cold. In addition, this author demonstrated the importance of the caloric intake in the development of adaptational mechanisms. We have confirmed this observation in our laboratory: subjects acclimatized to cold in the laboratory at 1 °C for 1 month in a discontinuous manner developed an adaptation of the hypothermal type (Savourey et al. 1994, 1996). The hypothermia is directly related to the reduction in the percentage of the body’s fat mass. The level of aerobic physical aptitude (VO2max) does not seem to be involved in the development of this type of adaptation to cold (Bittel et al. 1988; Savourey, Vallerand and Bittel 1992). Adaptation of the hypothermal type appears to be the most advantageous because it maintains the energy reserves by delaying the onset of shivering but without the hypothermia’s being dangerous (Bittel et al. 1989). Recent work in the laboratory has shown that it is possible to induce this type of adaptation by subjecting people to intermittent localized immersion of the lower limbs in iced water. Moreover, this type of acclimatization has developed a “polar tri-iodothyronine syndrome” described by Reed and co-workers in 1990 in subjects who had spent long periods in the polar region. This complex syndrome remains imperfectly understood and is evidenced mainly by a diminution in the pool of total tri-iodothyronine both when the environment is thermally neutral and during acute exposure to cold. The relationship between this syndrome and adaptation of the hypo-thermal type has yet to be defined, however (Savourey et al. 1996).
Table 1. General adaptational mechanisms to cold studied during a standard cold test carried out before and after a period of acclimatization.
|
Measure |
Use of measure as indicator |
Change in |
Type of adaptation |
|
Rectal |
Difference between tre at the end of the cold test and tre at thermal neutrality after acclimatization |
+ or = |
normothermal |
|
|
|
|
|
|
|
|
|
|
Local adaptation of the extremities is well documented (LeBlanc 1975). It has been studied both in native tribes or professional groups naturally exposed to cold in the extremities (Eskimos, Lapps, fishermen on the island of Gaspé, English fish carvers, letter carriers in Quebec) and in subjects artificially adapted in the laboratory. All these studies have shown that this adaptation is evidenced by higher skin temperatures, less pain and earlier paradoxical vasodilatation that occurs at higher skin temperatures, thus permitting the prevention of frostbite. These changes are basically connected with an increase in peripheral skin blood flow and not with local production of heat at the muscular level, as we have recently shown (Savourey, Vallerand and Bittel 1992). Immersion of the extremities several times a day in cold water (5ºC) over several weeks is sufficient to induce the establishment of these local adaptational mechanisms. On the other hand, there are few scientific data on the persistence of these different types of adaptation.
Pharmacological Methods for Preventing Cold Injury
The use of drugs to enhance tolerance to cold has been the subject of a number of studies. General tolerance to cold can be enhanced by favouring thermogenesis with drugs. Indeed, it has been shown in human subjects that the activity of shivering is accompanied notably by an increase in the oxidation of carbohydrates, combined with an increased consumption of muscular glycogen (Martineau and Jacob 1988). Methylxanthinic compounds exert their effects by stimulating the sympathetic system, exactly like cold, thereby increasing the oxidation of carbohydrates. However, Wang, Man and Bel Castro (1987) have shown that theophylline was ineffective in preventing the fall in body temperature in resting human subjects in the cold. On the other hand, the combination of caffeine with ephedrine permits a better maintenance of body temperature under the same conditions (Vallerand, Jacob and Kavanagh 1989), while the ingestion of caffeine alone modifies neither the body temperature nor the metabolic response (Kenneth et al. 1990). The pharmacological prevention of the effects of cold at the general level is still a matter for research. At the local level, few studies have been carried out on the pharmacological prevention of frostbite. Using an animal model for frostbite, a certain number of drugs were tested. Platelet anti-aggregants, corticoids and also various other substances had a protective effect provided that they were administered before the rewarming period. To our knowledge, no study has been carried out in humans on this subject.
Technical Methods for PreventingCold Injury
These methods are a basic element in the prevention of cold injury, and without their use human beings would be incapable of living in cold climatic zones. The construction of shelters, the use of a source of heat and also the use of clothing permit people to live in very cold regions by creating a favourable ambient microclimate. However, the advantages provided by civilization are sometimes not available (in the case of civil and military expeditions, shipwrecked persons, injured persons, vagrants, victims of avalanches, etc.). These groups are therefore particularly liable to cold injury.
Precautions for Work in the Cold
The problem of conditioning for work in the cold relates mainly to people who are not accustomed to work in the cold and/or who come from temperate climatic zones. Information on injury that can be caused by cold is of basic importance, but it is also necessary to acquire information about a certain number of types of behaviour too. Every worker in a cold zone must be familiar with the first signs of injury, especially local injury (skin colour, pain). Behaviour as regards clothing is vital: several layers of clothing permit the wearer to adjust the insulation given by clothing to current levels of energy expenditure and external stress. Wet garments (rain, sweat) must be dried. Every attention must be given to the protection of the hands and feet (no tight bandages, attention to adequate covering, timely changing of socks—say twice or three times a day—because of sweating). Direct contact with all cold metallic objects must be avoided (risk of immediate frostbite). The clothing must be guaranteed against cold and tested before any exposure to cold. Feeding rules should be remembered (with attention to caloric intake and hydration needs). Abuse of alcohol, caffeine and nicotine must be forbidden. Accessory equipment (shelter, tents, sleeping bags) must be checked. Condensation in tents and sleeping bags must be removed in order to avoid ice formation. Workers must not blow into their gloves to warm them or this will also cause the formation of ice. Finally, recommendations should be made for improving physical fitness. Indeed, a good level of aerobic physical fitness allows greater thermogenesis in severe cold (Bittel et al. 1988) but also ensures better physical endurance, a favourable factor because of the extra energy loss from physical activity in the cold.
Middle-aged persons must be kept under careful surveillance because they are more susceptible to cold injury than younger people on account of their more limited vascular response. Excessive fatigue and a sedentary occupation increase the risk of injury. Persons with certain medical conditions (cold urticaria, Raynaud’s syndrome, angina pectoris, prior frostbite) must avoid exposure to intense cold. Certain additional advice may be useful: protect exposed skin against solar radiation, protect the lips with special creams and protect the eyes with sunglasses against ultraviolet radiation.
When a problem does occur, workers in a cold zone must keep calm, must not separate themselves from the group, and must maintain their body heat by digging holes and huddling together. Careful attention must be paid to the provision of food and means of calling for help (radio, distress rockets, signal mirrors, etc.). Where there is a risk of immersion in cold water, lifeboats must be provided as well as equipment that is watertight and gives good thermal insulation. In case of shipwreck without a lifeboat, the individual must try to limit heat loss to the maximum by hanging on to floating materials, curling up and swimming in moderation with the chest out of the water if possible, because the convection created by swimming considerably increases heat loss. Drinking sea-water is harmful because of its high salt level.
Modification of Tasks in the Cold
In a cold zone, work tasks are considerably modified. The weight of the clothing, the carrying of loads (tents, food, etc.) and the need to traverse difficult terrain increase the energy expended by physical activity. Moreover, movement, coordination and manual dexterity are hindered by clothing. The field of vision is often reduced by the wearing of sunglasses. Further, perception of the background is altered and reduced to 6 m when the temperature of dry air is below –18ºC or when there is a wind. Visibility may be nil in a snowfall or in fog. The presence of gloves makes difficult certain tasks requiring fine work. Because of condensation, tools are often coated with ice, and grasping them with bare hands carries a certain risk of frostbite. The physical structure of clothing is altered in extreme cold, and the ice that may form as a result of freezing combined with condensation often blocks zip-fasteners. Finally, fuels must be protected against freezing by the use of antifreeze.
Thus, for the optimal performance of tasks in a cold climate there must be several layers of clothing; adequate protection of the extremities; measures against condensation in clothing, on tools and in tents; and regular warming in a heated shelter. Work tasks must be undertaken as a sequence of simple tasks, if possible carried out by two work teams, one working while the other is warming itself. Inactivity in the cold must be avoided, as must solitary work, away from used paths. A competent person may be designated to be responsible for protection and accident prevention.
In conclusion, it appears that a good knowledge of cold injury, a knowledge of the surroundings, good preparation (physical fitness, feeding, induction of adaptational mechanisms), appropriate clothing and suitable distribution of tasks can prevent cold injury. Where injury does occur, the worst can be avoided by means of rapid assistance and immediate treatment.
Protective Clothing: Waterproof Garments
Wearing waterproof garments has the object of protecting against the consequences of accidental immersion and therefore concerns not only all workers likely to suffer such accidents (sailors, air pilots) but also those working in cold water (professional divers). Table 2, extracted from the Oceanographic Atlas of the North American Ocean, shows that even in the western Mediterranean the water temperature rarely exceeds 15ºC. Under conditions of immersion, the survival time for a clothed individual with a lifebelt but without anti-immersion equipment has been estimated at 1.5 hours in the Baltic and 6 hours in the Mediterranean in January, whereas in August it is 12 hours in the Baltic and is limited only by exhaustion in the Mediterranean. Wearing protective equipment is therefore a necessity for workers at sea, particularly those liable to be immersed without immediate assistance.
Table 2. Monthly and annual mean of the number of days when water temperature is below 15 °C.
|
Month |
Western Baltic |
German Gulf |
Atlantic Ocean |
Western Mediterranean |
|
January |
31 |
31 |
31 |
31 |
|
February |
28 |
28 |
28 |
28 |
|
March |
31 |
31 |
31 |
31 |
|
April |
30 |
30 |
30 |
26 to 30 |
|
May |
31 |
31 |
31 |
8 |
|
June |
25 |
25 |
25 |
sometimes |
|
July |
4 |
6 |
sometimes |
sometimes |
|
August |
4 |
sometimes |
sometimes |
0 |
|
September |
19 |
3 |
sometimes |
sometimes |
|
October |
31 |
22 |
20 |
2 |
|
November |
30 |
30 |
30 |
30 |
|
December |
31 |
31 |
31 |
31 |
|
Total |
295 |
268 |
257 |
187 |
The difficulties of producing such equipment are complex, because account has to be taken of multiple, often conflicting, requirements. These constraints include: (1) the fact that the thermal protection must be effective in both air and water without impeding evaporation of sweat (2) the need to keep the subject at the surface of the water and (3) the tasks to be carried out. The equipment must furthermore be designed in accordance with the risk involved. This requires exact definition of the anticipated needs: thermal environment (temperature of water, air, wind), time before help arrives, and presence or absence of a lifeboat, for example. The insulation characteristics of the clothing depend on the materials used, the contours of the body, the compressibility of the protective fabric (which determines the thickness of the layer of air imprisoned in the clothing on account of the pressure exerted by the water), and the humidity that may be present in the clothing. The presence of humidity in this type of clothing depends mainly on how watertight it is. Evaluation of such equipment must take into account the effectiveness of the thermal protection provided not only in the water but also in cold air, and involve estimates of both probable survival time in terms of the water and air temperatures, and the anticipated thermal stress and the possible mechanical hindrance of the clothing (Boutelier 1979). Finally, tests of watertightness carried out on a moving subject will allow possible deficiencies in this respect to be detected. Ultimately, anti-immersion equipment must meet three requirements:
- It must provide effective thermal protection in both water and air.
- It must be comfortable.
- It must be neither too restrictive nor too heavy.
To meet these requirements, two principles have been adopted: either to use a material that is not watertight but maintains its insulating properties in the water (as is the case of so-called “wet” suiting) or to ensure total watertightness with materials that are in addition insulating (“dry” suiting). At present, the principle of the wet garment is being applied less and less, especially in aviation. During the last decade, the International Maritime Organization has recommended the use of an anti-immersion or survival suit meeting the criteria of the International Convention for the safety of human life at sea (SOLAS) adopted in 1974. These criteria concern in particular insulation, minimum infiltration of water into the suit, the size of the suit, ergonomics, compatibility with aids for floating, and testing procedures. However, the application of these criteria poses a certain number of problems (notably, those to do with the definition of the tests to be applied).
Although they have been known for a very long time, since the Eskimos used sealskin or seal intestines sewn together, anti- immersion suits are difficult to perfect and the criteria for standardization will probably be reviewed in future years.
Cold Environment and Cold Work
A cold environment is defined by conditions that cause greater than normal body heat losses. In this context “normal” refers to what people experience in everyday life under comfortable, often indoor conditions, but this may vary due to social, economic or natural climatic conditions. For the purpose of this article environments with an air temperature below 18 to 20ºC would be considered cold.
Cold work comprises a variety of industrial and occupational activities under different climatic conditions (see table 1). In most countries the food industry requires work under cold conditions—normally 2 to 8ºC for fresh food and below –25ºC for frozen food. In such artificial cold environments, conditions are relatively well defined and the exposure is about the same from day to day.
Table 1. Air temperatures of various cold occupational environments
|
–120 ºC |
Climatic chamber for human cryotherapy |
|
–90 ºC |
Lowest temperature at south polar base Vostock |
|
–55 ºC |
Cold store for fish meat and production of frozen, dried products |
|
–40 ºC |
“Normal” temperature at polar base |
|
–28 ºC |
Cold store for deep-frozen products |
|
+2 to +12 ºC |
Storage, preparation and transportation of fresh, alimentary products |
|
–50 to –20 ºC |
Average January temperature of northern Canada and Siberia |
|
–20 to –10 ºC |
Average January temperature of southern Canada, northern Scandinavia, central Russia |
|
–10 to 0 ºC |
Average January temperature of northern USA, southern Scandinavia, central Europe, parts of middle and far East, central and northern Japan |
Source: Modified from Holmér 1993.
In many countries the seasonal climatic changes imply that outdoor work and work in unheated buildings for shorter or longer periods has to be carried out under cold conditions. The cold exposure may vary considerably between different locations on the earth and type of work (see table 1). Cold water presents another hazard, encountered by people engaged in, for example, offshore work. This article deals with responses to cold stress, and preventive measures. Methods for assessment of cold stress and acceptable temperature limits according to recently adopted international standards are dealt with elsewhere in this chapter.
Cold Stress and Work in the Cold
Cold stress may be present in many different forms, affecting the whole-body heat balance as well as the local heat balance of extremities, skin and lungs. The type and nature of cold stress is extensively described elsewhere in this chapter. The natural means of dealing with cold stress is by behavioural action—in particular, change and adjustment of clothing. Sufficient protection prevents cooling. However, protection itself may cause unwanted, adverse effects. The problem is illustrated in figure 1.
Figure 1. Examples of cold effects.
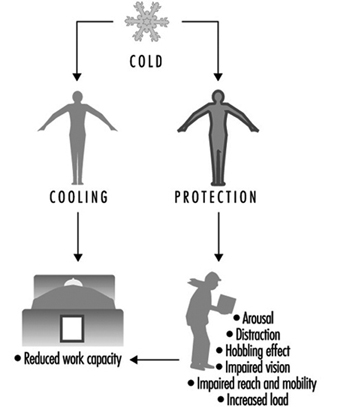
Cooling of the whole body or parts of the body results in discomfort, impaired sensory and neuro-muscular function and, ultimately, cold injury. Cold discomfort tends to be a strong stimulus to behavioural action, reducing or eliminating the effect. Prevention of cooling by means of donning cold-protective clothing, footwear, gloves and headgear interferes with the mobility and dexterity of the worker. There is a “cost of protection” in the sense that movements and motions become restricted and more exhausting. The continuous need for adjustment of the equipment to maintain a high level of protection requires attention and judgement, and may compromise factors such as vigilance and reaction time. One of the most important objectives of ergonomics research is the improvement of the functionality of clothing while maintaining cold protection.
Accordingly, effects of work in the cold must be divided into:
- effects of tissue cooling
- effects of protective measures (“cost of protection”).
On exposure to cold, behavioural measures reduce the cooling effect and, eventually, allow the maintenance of normal thermal balance and comfort. Insufficient measures evoke thermoregulatory, physiologically compensatory reactions (vasoconstriction and shivering). The combined action of behavioural and physiological adjustments determines the resulting effect of a given cold stress.
In the following sections these effects will be described. They are divided into acute effects (occurring within minutes or hours), long-term effects (days or even years) and other effects (not directly related to cooling reactions per se). Table 2 presents examples of reactions associated with the duration of cold exposure. Naturally, types of responses and their magnitude depend largely upon the stress level. However, long exposures (days and longer) hardly involve the extreme levels that can be attained for a short time.
Table 2. Duration of uncompensated cold stress and associated reactions
|
Time |
Physiological effects |
Psychological effect |
|
Seconds |
Inspiratory gasp |
Skin sensation, discomfort |
|
Minutes |
Tissue cooling |
Performance decrement |
|
Hours |
Impaired physical work capacity |
Impaired mental function |
|
Days/months |
Non-freezing cold injury |
Habituation |
|
Years |
Chronic tissue effects (?) |
Acute effects of cooling
The most obvious and direct effect of cold stress is the immediate cooling of the skin and the upper airways. Thermal receptors respond and a sequence of thermoregulatory reactions is initiated. The type and magnitude of reaction is determined primarily by the type and severity of cooling. As previously mentioned, peripheral vasoconstriction and shivering are the main defence mechanisms. Both contribute to preserving body heat and core temperature, but compromise cardiovascular and neuro-muscular functions.
However, the psychological effects of cold exposure also modify the physiological reactions in a complex and partly unknown way. The cold environment causes distraction in the sense that it requires increased mental effort to handle the new stress factors (avoid cooling, take protective measures, etc.). On the other hand, the cold also causes arousal, in the sense that the increased stress level increases sympathetic nervous activity and, thereby, preparedness for action. In normal conditions people use only minor portions of their capacity, thereby preserving a large buffer capacity for unexpected or demanding conditions.
Cold perception and thermal comfort
Most humans experience a sensation of thermal neutrality at an operative temperature between 20 and 26ºC when engaged in very light, sedentary work (office work at 70 W/m2) in appropriate clothing (insulation values between 0.6 and 1.0 clo). In this state and in the absence of any local thermal imbalances, like draught, people are in thermal comfort. These conditions are well documented and specified in standards such as ISO 7730 (see the chapter Controlling the indoor environment in this Encyclopaedia).
Human perception of cooling is closely related to whole-body heat balance as well as local tissue heat balance. Cold thermal discomfort arises when body heat balance cannot be maintained due to inappropriate matching of activity (metabolic heat production) and clothing. For temperatures between +10 and +30ºC, the magnitude of “cold discomfort” in a population can be predicted by Fanger’s comfort equation, described in ISO 7730.
A simplified and reasonably accurate formula for computation of the thermoneutral temperature (t) for the average person is:
t = 33.5 – 3·Icl – (0.08 + 0.05·Icl)·M
where M is the metabolic heat measured in W/m2 and Icl the insulation value of clothing measured in clo.
The required clothing insulation (clo value) is higher at +10ºC than that calculated with the IREQ method (calculated required insulation value) (ISO TR 11079, 1993). The reason for this discrepancy is the application of different “comfort” criteria in the two methods. ISO 7730 focuses heavily on thermal comfort and allows for considerable sweating, whereas ISO TR 11079 allows only “control” sweating at minimal levels—a necessity in the cold. Figure 2 depicts the relationship between clothing insulation, activity level (heat production) and air temperature according to the equation above and the IREQ method. The filled areas should represent the expected variation in required clothing insulation due to different levels of “comfort”.
Figure 2. Optimal temperature for thermal "comfort" as function of clothing and activity level (![]() ).
).

The information in figure 2 is only a guide for establishing optimal indoor thermal conditions. There is considerable individual variation in perception of thermal comfort and discomfort from cold. This variation originates from differences in clothing and activity patterns, but subjective preferences and habituation also contribute.
In particular, people engaged in very light, sedentary activity become increasingly susceptible to local cooling when air temperature drops below 20 to 22ºC. In such conditions air velocity must be kept low (below 0.2 m/s), and additional insulative clothing must be selected to cover sensitive body parts (e.g., head, neck, back and ankles). Seated work at temperatures below 20ºC requires insulated seat and backrest to reduce local cooling due to compression of clothing.
When ambient temperature falls below 10ºC, the comfort concept becomes more difficult to apply. Thermal asymmetries become “normal” (e.g., cold face and cold air inhalation). Despite an optimal body heat balance, such asymmetries may be felt to be uncomfortable and require extra heat to eliminate. Thermal comfort in the cold, unlike under normal indoor conditions, is likely to coincide with a slight feeling of warmth. This should be remembered when cold stress is assessed using the IREQ index.
Performance
Cold exposure and the associated behavioural and physiological reactions have an impact on human performance at various levels of complexity. Table 3 presents a schematic overview of different types of performance effects that may be anticipated with mild and extreme cold exposure.
Table 3. Indication of anticipated effects of mild and severe cold exposure
|
Performance |
Mild cold exposure |
Severe cold exposure |
|
Manual performance |
0 – |
– – |
|
Muscular performance |
0 |
– |
|
Aerobic performance |
0 |
– |
|
Simple reaction time |
0 |
– |
|
Choice reaction time |
– |
– – |
|
Tracking, vigilance |
0 – |
– |
|
Cognitive, mental tasks |
0 – |
– – |
0 indicates no effect; – indicates impairment; – – indicates strong impairment; 0 – indicates contradictory finding.
Mild exposure in this context implies no or negligible body core cooling and moderate cooling of the skin and extremities. Severe exposure results in negative heat balance, a drop in core temperature and concomitant pronounced lowering of temperature of the extremities.
The physical characteristics of mild and severe cold exposure are very much dependent on the balance between internal body heat production (as a result of physical work) and heat losses. Protective clothing and ambient climatic conditions determine the amount of heat loss.
As previously mentioned, cold exposure causes distraction and cooling (figure 1). Both have an impact on performance, although the magnitude of impact varies with the type of task.
Behaviour and mental function are more susceptible to the distraction effect, whereas physical performance is more affected by cooling. The complex interaction of physiological and psychological responses (distraction, arousal) to cold exposure is not fully understood and requires further research work.
Table 4 indicates reported relationships between physical performance and temperatures of the body. It is assumed that physical performance is highly dependent on tissue temperature and deteriorates when temperature of vital tissue and organ parts drops. Typically, manual dexterity is critically dependent upon finger and hand temperature, as well as muscle temperature of the forehand. Gross muscular activity is little affected by local surface temperature, but very sensitive to muscle temperature. Since some of these temperatures are related to each other (e.g., core and muscle temperature) it is difficult to determine direct relationships.
Table 4. Importance of body tissue temperature for human physical performance
|
Performance |
Hand/finger skin temperature |
Mean skin temperature |
Muscle temperature |
Core temperature |
|
Simple manual |
– |
0 |
– |
0 |
|
Complex manual |
– – |
(–) |
– – |
– |
|
Muscular |
0 |
0 – |
– – |
0 – |
|
Aerobic |
0 |
0 |
– |
– – |
0 indicates no effect; – indicates impairment with lowered temperature; – – indicates strong impairment; 0 – indicates contradictory findings; (–) indicates possible minor effect.
The overview of performance effects in table 3 and 4 is by necessity very schematic. The information should serve as a signal for action, where action means a detailed assessment of conditions or undertaking of preventive measures.
An important factor contributing to performance decrements is exposure time. The longer the cold exposure, the greater the effect upon the deeper tissues and neuro-muscular function. On the other hand, factors such as habituation and experience modify the detrimental effects and restore some of the performance capacity.
Manual performance
Hand function is very susceptible to cold exposure. Due to their small mass and large surface area, hands and fingers lose much heat while maintaining high tissue temperatures (30 to 35ºC). Accordingly, such high temperatures can be maintained only with a high level of internal heat production, allowing for sustained high blood flow to the extremities.
Hand heat loss can be reduced in the cold by wearing appropriate handwear. However, good handwear for cold weather means thickness and volume, and, consequently, impaired dexterity and manual function. Hence, manual performance in the cold cannot be preserved by passive measures. At best, the reduction in performance may be limited as the result of a balanced compromise between the choice of functional handwear, work behaviour and exposure scheme.
Hand and finger function is much dependent on local tissue temperatures (figure 3). Fine, delicate and fast finger movements deteriorate when tissue temperature drops by a few degrees. With more profound cooling and temperature drop, gross hand functions are also impaired. Significant impairment in hand function is found at hand skin temperatures around 15ºC, and severe impairments occur at skin temperatures about 6 to 8ºC due to blocking of function of sensory and thermal skin receptors. Depending on task requirements, it may be necessary to measure skin temperature at several sites on the hand and fingers. Temperature of the fingertip may be more than ten degrees lower than on the back of the hand under certain exposure conditions.
Figure 3. Relation between finger dexterity and finger skin temperature.
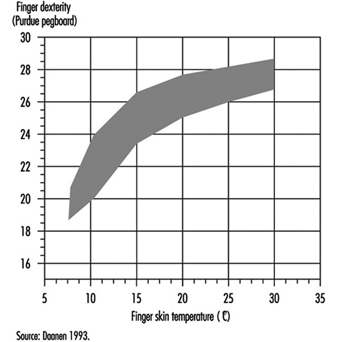
Figure 4 indicates critical temperatures for different types of effects on manual function.
Figure 4. Estimated gross effects on manual performance at different levels of hand/finger temperature.
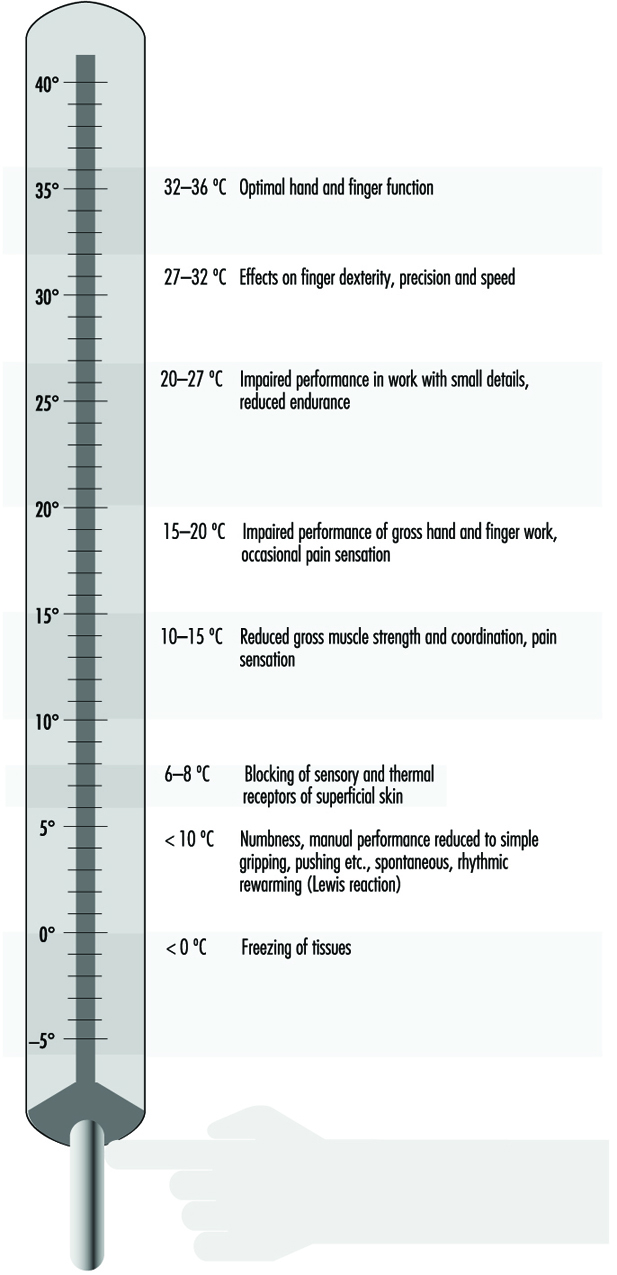
Neuro-muscular performance
It is evident from figures 3 and 4 that there is a pronounced effect of cold on muscular function and performance. Cooling of muscle tissue reduces blood flow and slows down neural processes like transmission of nerve signals and synaptic function. In addition, viscosity of tissues increases, resulting in higher internal friction during motion.
Isometric force output is reduced by 2% per ºC of lowered muscle temperature. Dynamic force output is reduced by 2 to 4% per ºC of lowered muscle temperature. In other words, cooling reduces the force output of muscles and has an even greater effect on dynamic contractions.
Physical work capacity
As previously mentioned, muscular performance deteriorates in the cold. With impaired muscle function there is a general impairment of physical work capacity. A contributing factor to the reduction in aerobic work capacity is the increased peripheral resistance of the systemic circulation. Pronounced vasoconstriction increases central circulation, eventually leading to cold diuresis and elevated blood pressure. Cooling of the core may also have a direct effect on the contractility of the heart muscle.
Work capacity, as measured by maximal aerobic capacity, decreases by 5 to 6% per ºC lowered core temperature. Thus endurance may deteriorate rapidly as the practical consequence of the lowered maximal capacity and with an increased energy requirement of muscular work.
Other cold effects
Body temperatures
As the temperature drops, the surface of the body is most affected (and also most tolerant). Skin temperature may fall below 0ºC in a few seconds when the skin is in contact with very cold metal surfaces. Likewise hand and finger temperatures may decrease by several degrees per minute under conditions of vasoconstriction and poor protection. At normal skin temperature the arms and hands are superperfused due to peripheral arterio-venous shunts. This creates warmth and enhances dexterity. Cooling of the skin shuts these shunts and decreases perfusion in hands and feet to one tenth. The extremities constitute 50% of the body surface and 30% of its volume. The return of blood passes via deep veins concomitant to the arteries, thereby reducing heat loss according to the counter-current principle.
Adrenergic vasoconstriction does not occur in the head-neck region, which must be borne in mind in emergency situations to prevent hypothermia. A bareheaded individual may lose 50% or more of his or her resting heat production at subzero temperatures.
A high and sustained rate of whole-body heat loss is required for the development of hypothermia (drop in core temperature) (Maclean and Emslie-Smith 1977). The balance between heat production and heat loss determines the resultant cooling rate, be it a whole-body cooling or a local cooling of a part of the body. The conditions for heat balance can be analysed and assessed on the basis of the IREQ index. A remarkable response to local cooling of protruding parts of the human body (e.g., fingers, toes and ears) is the hunting phenomenon (Lewis reaction). After an initial drop to a low value, finger temperature increases by several degrees (figure 5). This reaction is repeated in a cyclic manner. The response is very local—more pronounced at the tip of the finger than at the base. It is absent in the hand. The response on the palm of the hand most likely reflects the variation in temperature of the blood flow supplying the fingers. The response can be modified by repeated exposures (amplified), but is more or less abolished in association with whole-body cooling.
Figure 5. Cold-induced vasodilatation of finger vessels causing cyclic rises in tissue temperature.
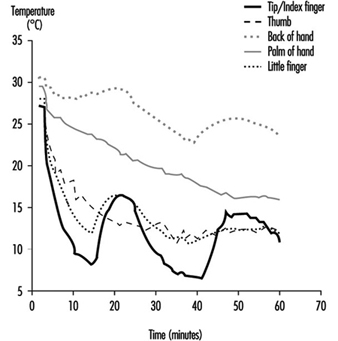
Progressive cooling of the body results in a number of physio-logical and mental effects. Table 16 indicates some typical responses associated with different levels of core temperature.
Table 5. Human responses to cooling: Indicative reactions to different levels of hypothermia
|
Phase |
Core |
Physiological |
Psychological |
|
Normal |
37 36 |
Normal body temperature Vasoconstriction, cold hands and feet |
Thermoneutral sensation Discomfort |
|
Mild hypothermia |
35 34 33 |
Intense shivering, reduced work capacity Fatigue Fumbling and stumbling |
Impaired judgment, disorientation, apathy Conscious and |
|
Moderate |
32 31 30 29 |
Muscle rigidity Faint breathing No nerve reflexes, heart rate slow and almost unnoticeable |
Progressive Consciousness clouds Stuporous |
|
Severe |
28 27 25 |
Heart dysrhythmias (atrial Pupils non reactive to Death due to ventricular fibrillation or asystole |
Heart and circulation
Cooling of the forehead and head elicit acute elevation of systolic blood pressure and, eventually, elevated heart rate. A similar reaction may be seen when putting bare hands in very cold water. The reaction is of short duration, and normal or slightly elevated values are attained after seconds or minutes.
Excessive body heat loss causes peripheral vasoconstriction. In particular, during the transient phase the increased peripheral resistance results in an elevation of systolic blood pressure and increased heart rate. Cardiac work is greater than it would be for similar activities at normal temperatures, a phenomenon painfully experienced by persons with angina pectoris.
As previously mentioned, deeper tissue cooling generally slows down the physiological processes of cells and organs. Cooling weakens the innervation process and suppresses heart contractions. Contraction power is reduced and, in addition to the increase in peripheral resistance of the blood vessels, cardiac output is reduced. However, with moderate and severe hypothermia, cardiovascular function declines in relation to the general reduction in metabolism.
Lungs and airways
Inhalation of moderate volumes of cold, dry air presents limited problems in healthy persons. Very cold air may cause discomfort, in particular, with nasal breathing. High ventilation volumes of very cold air may also cause micro-inflammation of the mucosal membrane of the upper airways.
With progression of hypothermia, lung function is depressed contemporaneously with the general reduction in body meta-bolism.
Functional aspects (work capacity)
A fundamental requirement for function in cold environments is the provision of sufficient protection against cooling. However, protection itself may seriously interfere with conditions for performance. The hobbling effect of clothing is well-known. Headgear and helmets interfere with speech and vision, and handwear impairs manual function. Whereas protection is necessary for preservation of healthy and comfortable working conditions, the consequences in terms of impaired performance must be fully recognized. Tasks take longer to complete and require greater effort.
Protective clothing against cold may easily weigh 3 to 6 kg including boots and headwear. This weight adds to workload, in particular during ambulatory work. Also, friction between layers in multi-layer clothing yields resistance to motion. The weight of boots should be kept low, since added weight on the legs contributes relatively more to workload.
Work organization, workplace and equipment should be adapted to the specific requirements of a cold work task. More time must be allowed for tasks, and frequent breaks for recovery and warming are needed. The workplace must allow for easy movements, despite bulky clothing. Similarly, equipment must be designed so that it can be operated by a gloved hand or insulated in the case of bare hands.
Cold Injuries
Serious injuries by cold air are in most cases preventable and occur only sporadically in civilian life. On the other hand, these injuries are often of major significance in war and in cataclysms. However, many workers run the risk of getting cold injuries in their routine activities. Outdoor work in harsh climate (as in arctic and subarctic areas—for example, fishing, agriculture, construction, gas and oil exploration and reindeer herding) as well as indoor work carried out in cold environments (as in food or warehousing industries) can all involve danger of cold injury.
Cold injuries may be either systemic or localized. The local injuries, which most often precede systemic hypothermia, constitute two clinically different entities: freezing cold injuries (FCI) and non-freezing cold injuries (NFCI).
Freezing cold injuries
Pathophysiology
This type of local injury occurs when heat loss is sufficient to allow a true freezing of the tissue. Besides a direct cryogenic insult to the cells, vascular damage with decreased perfusion and tissue hypoxia are contributing pathogenic mechanisms.
The vasoconstriction of cutaneous vessels is of great importance in the origin of a frostbite. Due to wide arteriovenous shunts, peripheral structures such as hands, feet, nose and ears are superperfused in a warm environment. Only about one-tenth of the blood flow in the hands, for example, is needed for tissue oxygenation. The rest creates warmth, thereby facilitating dexterity. Even in the absence of any decrease in core temperature, local cooling of the skin occludes these shunts.
In order to protect the viability of the peripheral parts of the extremities during cold exposure, an intermittent cold-induced vasodilatation (CIVD) takes place. This vasodilatation is a result of opening of the arteriovenous anastomoses and occurs every 5 to 10 minutes. The phenomenon is a compromise in the human physiological plan to conserve heat and yet intermittently preserve function of hands and feet. The vasodilatation is perceived by the person as periods of prickling heat. CIVD becomes less pronounced as body temperature decreases. Individual variations in the degree of CIVD might explain different susceptibility to local cold injury. People indigenous to a cold climate present a more pronounced CIVD.
In contrast to cryopreservation of living tissue, where ice crystallization occurs both intra- and extracellularly, the clinical FCI, with a much slower rate of freezing, produces only extra- cellular ice crystals. The process is an exothermic one, liberating heat, and therefore tissue temperature remains at the freezing point until freezing is complete.
As the extracellular ice crystals grow, extracellular solutions are condensed, causing this space to become a hyperosmolar milieu, which leads to passive diffusion of water from the intracellular compartment; that water in turn freezes. This process progresses until all “available” water (not otherwise bound to protein, sugar and other molecules) has been crystallized. Cell dehydration alters protein structures, membrane lipids and cellular pH, leading to destruction incompatible with cell survival. Resistance to FCI varies in different tissues. Skin is more resistant than muscles and nerves, for example, which might be the result of a smaller water content both intra- and intercellularly in the epidermis.
The role of indirect haemorheological factors was earlier interpreted as similar to that found in non-freezing cold injuries. Recent studies in animals have, however, shown that freezing causes lesions in the intima of arterioles, venules and capillaries prior to any evidence of damage to other skin elements. Thus, it is obvious that the rheological part of the pathogenesis of FCI is also a cryobiological effect.
When a frostbite is rewarmed, water begins to rediffuse to the dehydrated cells, leading to intracellular swelling. Thawing induces maximal vascular dilation, creating oedema and blister formation due to the endothelial (internal layer of the skin) cell injury. Disruption of the endothelial cells exposes the basement membrane, which initiates platelet adhesions and starts the coagulation cascade. The following blood stagnation and thrombosis induce anoxia.
As it is the heat loss from the exposed area that determines the risk of getting a frostbite, wind-chill is an important factor in this respect, and this means not only the wind which is blowing but also any movement of air past the body. Running, skiing, skijoring and riding in open vehicles must be considered in this context. However, the exposed flesh will not freeze as long as the ambient temperature is above the freezing point, even at high wind velocities.
Use of alcohol and tobacco products as well as under-nourishment and fatigue are predisposing factors to FCI. A previous cold injury increases the risk of subsequent FCI, due to an abnormal post-traumatic sympathetic response.
Cold metal can rapidly cause a frostbite when grasped with the bare hand. Most people are aware of this, but often don’t realize the risk of handling super-cooled liquids. Petrol cooled down to –30ºC will freeze exposed flesh almost instantly as evaporative heat loss is combined with conductive loss. Such rapid freezing causes extra- as well as intracellular crystallization with destruction of cell membranes primarily on a mechanical basis. A similar type of FCI occurs when liquid propane is spilled directly onto the skin.
Clinical picture
Freezing cold injuries are subdivided into superficial and deep frostbites. The superficial injury is limited to the skin and the immediate underlying subcutaneous tissues. In most cases the injury is localized to nose, earlobes, fingers and toes. Stinging, pricking pain is often the first sign. The affected part of the skin turns pale or wax-white. It is numb, and will indent upon pressure, as the underlying tissues are viable and pliable. When the FCI extends into a deep injury, the skin becomes white and marble-like, feels hard, and adheres when touched.
Treatment
A frostbite should be taken care of immediately in order to prevent a superficial injury from turning into a deep one. Try to take the victim indoors; otherwise protect him or her from the wind by shelter of comrades, a wind sack or other similar means. The frost-bitten area should be thawed by passive transmission of heat from a warmer part of the body. Put the warm hand against the face and the cold hand into the armpit or into the groin. As the frostbitten individual is under cold stress with peripheral vaso-constriction, a warm companion is a much better therapist. Massage and rubbing the frostbitten part with snow or woollen muffler is contraindicated. Such mechanical treatment would only aggravate the injury, as the tissue is filled with ice crystals. Nor should thawing in front of a campfire or a camp stove be considered. Such heat does not penetrate to any depth, and as the area is partly anaesthetized the treatment may even result in a burn injury.
The signals of pain in a frostbitten foot disappear before actual freezing takes place, as nerve conductivity is abolished at around +8ºC. The paradox is that the last sensation one feels is that one does not feel anything at all! Under extreme conditions when evacuation requires travel on foot, thawing should be avoided. Walking on frostbitten feet does not seem to increase the risk of tissue loss, whereas refreezing of a frostbite does so in the highest degree.
The best treatment for a frostbite is thawing in warm water at 40 to 42ºC. The thawing procedure should continue at that water temperature until sensation, colour and tissue softness return. This form of thawing often ends up in not a pink, but rather a burgundy hue due to venous stasis.
Under field conditions one must be aware that treatment requires more than local thawing. The whole individual has to be taken care of, as a frostbite is often the first sign of a creeping hypothermia. Put on more clothes and give warm, nourishing beverages. The victim is most often apathetic and has to be forced to cooperate. Urge the victim to do muscular activity such as buffeting arms against sides. Such manoeuvres open peripheral arteriovenous shunts in the extremities.
A deep frostbite is present when thawing with passive warmth transfer for 20 to 30 minutes is without success. If so, the victim should be sent to the nearest hospital. However, if such transportation can take hours, it is preferable to get the person into the nearest housing and thaw his or her injuries in warm water. After complete thawing, the patient should be put to bed with the injured area elevated, and prompt transportation to the nearest hospital should be arranged.
Rapid rewarming gives moderate to severe pain, and the patient will often need an analgesic. The capillary damage causes leakage of serum with local swelling and blister formation during the first 6 to 18 hours. Blisters should be kept intact in order to prevent infection.
Non-freezing cold injuries
Pathophysiology
Prolonged exposure to cold and wet conditions above the freezing point combined with immobilization causing venous stagnation are the prerequisites for NFCI. Dehydration, inadequate food, stress, inter-current illness or injury, and fatigue are contributory factors. NFCI almost exclusively affects legs and feet. Severe injuries of this type occur with great rarity in civilian life, but in wartime and catastrophes it has been and will always be a serious problem, most often caused by an unawareness of the condition due to the slow and indistinct first appearance of symptoms.
NFCI can occur under any conditions where the environmental temperature is lower than body temperature. As in FCI, sympathetic constrictor fibres, together with the cold itself, induce prolonged vasoconstriction. The initial event is rheological in nature and resembles that observed in ischaemic reperfusion injury. In addition to the duration of the low temperature, the susceptibility of the victim seems to be of importance.
The pathological change due to the ischaemic injury affects many tissues. Muscles degenerate, undergoing necrosis, fibrosis and atrophy; bones show early osteoporosis. Of special interest are the effects on the nerves, as nerve damage accounts for the pain, prolonged dysaesthesia and hyperhidrosis often found as a sequel in these injuries.
Clinical picture
In a non-freezing cold injury the victim realizes too late the threatening danger because the initial symptoms are so vague. The feet become cold and swollen. They feel heavy, woody and numb. The feet are presented as cool, painful, tender, often with wrinkled soles. The first ischaemic phase last for hours up to a few days. It is followed by a hyperaemic phase of 2 to 6 weeks, during which the feet are warm, with bounding pulses and increased oedema. Blistering and ulcerations are not uncommon, and in severe cases gangrene can arise.
Treatment
The treatment is above all supportive. On the worksite, the feet should be dried carefully but kept cool. On the other hand, the whole body should be warmed. Plenty of warm beverages should be given. Contrary to the freezing cold injuries, NFCI should never be actively warmed. Warm water treatment in local cold injuries is only allowed when ice-crystals are present in the tissue. The further treatment should as a rule be conservative. However, fever, signs of disseminated intravascular coagulation, and liquefaction of affected tissues requires surgical intervention, occasionally ending in an amputation.
Non-freezing cold injuries can be prevented. Exposure time should be minimized. Adequate foot care with time to dry the feet is of importance, as well as facilities to change into dry socks. Rest with feet elevated as well as administering hot beverages whenever possible may seem ridiculous but often is of crucial importance.
Hypothermia
Hypothermia means subnormal body temperature. However, from a thermal point of view the body consists of two zones—the shell and the core. The former is superficial and its temperature varies considerably according to the external environment. The core consists of deeper tissues (e.g., brain, heart and lungs, and upper abdomen), and the body strives to maintain a core temperature of 37 ± 2ºC. When thermoregulation is impaired and core temperature starts to decline, the individual suffers cold stress, but not until the central temperature reaches 35ºC is the victim considered to be in a hypothermic state. Between 35 and 32ºC, the hypothermia is classified as mild; between 32 and 28ºC it is moderate and below 28ºC, severe (Table 16).
Physiological effects of lowered core temperature
When core temperature starts to decline, an intense vasoconstriction redirects blood from the shell to the core, thereby preventing heat conduction from the core to the skin. In order to maintain temperature, shivering is induced, often preceded by increased muscular tone. Maximal shivering can increase the metabolic rate four- to sixfold, but as the involuntary contractions oscillate, the net result is often not more than doubled. Heart rate, blood pressure, cardiac output and respiratory rate increase. The centralization of blood volume causes an osmolal diuresis with sodium and chloride as the main constituents.
Atrial irritability in early hypothermia often induces atrial fibrillation. At lower temperatures, ventricular extra systoles are common. Death occurs at or below 28ºC, most often resulting from ventricular fibrillation; asystole may also supervene.
Hypothermia depresses the central nervous system. Lassitude and apathy are early signs of decreasing core temperature. Such effects impair judgement, cause bizarre behaviour and ataxia, and end in lethargy and coma between 30 and 28ºC.
Nerve conduction velocity decreases with lowered temperature. Dysarthria, fumbling and stumbling are clinical manifestations of this phenomena. Cold also affects muscles and joints, impairing manual performance. It slows reaction time and coordination, and increases frequency of mistakes. Muscle rigidity is observed in even mild hypothermia. At a core temperature lower than 30ºC, physical activity is impossible.
Exposure to an abnormally cold environment is the basic prerequisite for hypothermia to occur. Extremes of age are risk factors. Elderly persons with impaired thermoregulatory function, or persons whose muscle mass and insulating fat layer are reduced, run a greater risk of suffering hypothermia.
Classification
From a practical point of view the following subdivision of hypo-thermia is useful (see also Table 16):
- accidental hypothermia
- acute immersion hypothermia
- sub-acute exhaustion hypothermia
- hypothermia in trauma
- sub-clinical chronic hypothermia.
Acute immersion hypothermia occurs when a person falls into cold water. Water has a thermal conductivity approximately 25 times that of air. The cold stress becomes so great that the core temperature is forced down despite a maximal heat production of the body. Hypothermia sets in before the victim becomes exhausted.
Sub-acute exhaustion hypothermia may happen to any worker in a cold environment as well as to skiers, climbers and walkers in the mountains. In this form of hypothermia, muscular activity maintains the body temperature as long as energy sources are available. However, then hypoglycaemia ensures the victim is at risk. Even a relatively mild degree of cold exposure may be sufficient to continue cooling and cause a hazardous situation.
Hypothermia with major trauma is an ominous sign. The injured person is often unable to maintain body temperature, and heat loss may be exacerbated by infusion of cold fluids and by removal of clothing. Patients in shock who become hypothermic have a much higher mortality than normothermic victims.
Sub-clinical chronic hypothermia is often encountered in elderly persons, often in association with malnutrition, inadequate clothing and restricted mobility. Alcoholism, drug abuse and chronic metabolic diseases as well as psychiatric disorders are contributory causes in this type of hypothermia.
Pre-hospital management
The main principle of primary care of a worker suffering from hypothermia is to prevent further heat loss. A conscious victim should be moved indoors, or at least into a shelter. Remove wet clothing and try to insulate the person as much as possible. Keeping the victim in a lying position with the head covered is mandatory.
Patients with acute immersion hypothermia require quite different treatment from that required by those with sub-acute exhaustion hypothermia. The immersion victim is often in a more favourable situation. The decreased core temperature occurs long before the body becomes exhausted, and heat-generating capacity remains unimpaired. Water and electrolyte balance is not deranged. Therefore such an individual may be treated with rapid immersion in a bath. If a tub is not available, put the patient’s feet and hands into warm water. The local heat opens the arterio- venous shunts, rapidly increases the blood circulation in the extremities and enhances the warming process.
In exhaustion hypothermia, on the other hand, the victim is in a much more serious situation. The caloric reserves are consumed, the electrolyte balance is deranged and, above all, the person is dehydrated. The cold diuresis starts immediately after cold exposure; the fight against the cold and wind exaggerates sweating, but this is not perceived in the cold and dry environment; and lastly, the victim does not feel thirsty. A patient suffering from exhaustion hypothermia should never be rapidly rewarmed out in the field due to the risk of inducing hypovolemic shock. As a rule it is better not to actively rewarm the patient out in the field or during transportation to hospital. A prolonged state of not progressing hypothermia is far better than enthusiastic efforts to warm the patient under circumstances where supervening complications cannot be managed. It is mandatory to handle the patient gently to minimize the risk of possible ventricular fibrillation.
Even for trained medical personnel it is often difficult to determine whether a hypothermic individual is alive or not. Apparent cardiovascular collapse may actually be only depressed cardiac output. Palpation or auscultation for at least a minute to detect spontaneous pulses is often necessary.
The decision as to whether or not to administer cardiopulmonary resuscitation (CPR) is difficult out in the field. If there is any sign of life at all, CPR is contra-indicated. Prematurely performed chest compressions may induce ventricular fibrillation. CPR should, however, immediately be initiated following a witnessed cardiac arrest and when the situation allows the procedures to be performed reasonably and continuously.
Health and cold
A healthy person with appropriate clothing and equipment and working in an organization suitable for the task is not in a health risk situation, even if it is very cold. Whether or not long-term cold exposure while living in cold climate areas means health risks is controversial. For individuals with health problems the situation is quite different, and cold exposure could be a problem. In a certain situation cold exposure or exposure to cold-related factors or combinations of cold with other risks can produce health risks, especially in an emergency or accident situation. In remote areas, when communication with a supervisor is difficult or does not exist, the employees themselves must be allowed to decide whether a health risk situation is at hand or not. In these situations they must take necessary precautions to make the situation safe or stop work.
In arctic regions, climate and other factors can be so harsh that other considerations must be taken.
Infectious diseases. Infectious diseases are not related to cold. Endemic diseases occur in arctic and subarctic regions. Acute or chronic infectious disease in an individual dictates cessation of exposure to cold and hard work.
The common cold, without fever or general symptoms, does not make work in the cold harmful. However, for individuals with complicating diseases like asthma, bronchitis or cardiovascular problems, the situation is different and indoor work in warm conditions during the cold season is recommended. This is also valid with a cold with fever, deep cough, muscle pain and impaired general condition.
Asthma and bronchitis are more common in cold regions. Exposure to cold air often worsens the symptoms. Change of medication sometimes reduces the symptoms during the cold season. Some individuals can also be helped by using medicinal inhalers.
People with asthmatic or cardiovascular diseases may respond to cold air inhalation with bronchoconstriction and vasospasm. Athletes training several hours at high intensities in cold climates have been shown to develop asthmatic symptoms. Whether or not extensive cooling of the pulmonary tract is the primary explanation is not yet clear. Special, light masks are now on the market that do provide some kind of heat exchanger function, thereby conserving energy and moisture.
An endemic type of chronic disease is “Eskimo lung”, typical for Eskimo hunters and trappers exposed to extreme cold and hard work for long periods. A progressive pulmonary hyper- tension often ends in a right-sided heart failure.
Cardiovascular disorders. Exposure to cold affects the cardio- vascular system to a higher degree. The noradrenalin released from the sympathetic nerve terminals raises the cardiac output and heart rate. Chest pain due to angina pectoris often worsens in a cold environment. The risk of getting an infarct increases during cold exposure, especially in combination with hard work. Cold raises blood pressure with an increased risk of cerebral haemorrhage. Individuals at risk should therefore be warned and reduce their exposure to hard work in the cold.
Increased mortality during winter season is a frequent observation. One reason could be the previously mentioned increase in heart work, promoting arrhythmia in sensitive persons. Another observation is that the haematocrit is increased during the cold season, causing increased viscosity of blood and increased resistance to flow. A plausible explanation is that cold weather may expose people to sudden, very heavy work loads, such as snow cleaning, walking in deep snow, slipping and so on.
Metabolic disorders. Diabetes mellitus is also found with a higher frequency in the colder areas of the world. Even an uncomplicated diabetes, especially when treated with insulin, can make cold outdoor work impossible in more remote areas. Early peripheral arteriosclerosis makes these individuals more sensitive to cold and increases the risk of local frostbite.
Individuals with impaired thyroid function can easily develop hypothermia due to lack of the thermogenic hormone, while hyperthyroid persons tolerate cold even when lightly dressed.
Patients with these diagnoses should be given extra attention from health professionals and be informed of their problem.
Musculoskeletal problems. Cold itself is not supposed to cause diseases in the musculoskeletal system, not even rheumatism. On the other hand, work in cold conditions is often very demanding for muscles, tendons, joints and spine because of the high load often involved in these kinds of work. The temperature in the joints decreases faster than the temperature of the muscles. Cold joints are stiff joints, because of increasing resistance to movement due to augmented viscosity of the synovial fluid. Cold decreases the power and duration of muscle contraction. In combination with heavy work or local overload, the risk of injury increases. Furthermore, protective clothing may impair the ability to control movement of body parts, hence contributing to the risk.
Arthritis in the hand is a special problem. It is suspected that frequent cold exposure may cause arthritis, but so far the scientific evidence is poor. An existing arthritis of the hand reduces hand function in the cold and causes pain and discomfort.
Cryopathies. Cryopathies are disorders where the individual is hypersensitive to cold. The symptoms vary, including those involving the vascular system, blood, connective tissue, “allergy” and others.
Some individuals suffer from white fingers. White spots on the skin, a sensation of cold, reduced function and pain are symptoms when fingers are exposed to cold. The problems are more common among women, but above all are found in smokers and workers using vibrating tools or driving snowmobiles. Symptoms can be so troublesome that work during even slight cold exposure is impossible. Certain types of medication can also worsen the symptoms.
Cold urticaria, due to sensitized mast cells, appears as an itching erythema of cold-exposed parts of the skin. If exposure is stopped, the symptoms usually disappear within one hour. Rarely the disease is complicated with general and more threatening symptoms. If so, or if the urticaria itself is very troublesome, the individual should avoid exposure to any kind of cold.
Acrocyanosis is manifested by changes in skin colour towards cyanosis after exposure to cold. Other symptoms could be dysfunction of hand and fingers in the acrocyanotic area. The symptoms are very common, and can often be acceptably reduced by reduced cold exposure (e.g., proper clothing) or reduced nicotine use.
Psychological stress. Cold exposure, especially in combination with cold-related factors and remoteness, stresses the individual, not only physiologically but also psychologically. During work in cold climate conditions, in bad weather, over long distances and perhaps in potentially dangerous situations, the psychological stress can disturb or even deteriorate the individual’s psychological function so much that work cannot be safely done.
Smoking and snuffing. The unhealthy long-term effects of smoking and, to some extent, snuffing are well known. Nicotine increases peripheral vasoconstriction, reduces dexterity and raises the risk of cold injury.
Alcohol. Drinking alcohol gives a pleasant feeling of warmth, and it is generally thought that the alcohol inhibits cold-induced vasoconstriction. However, experimental studies on humans during relatively short exposures to cold have shown that alcohol does not interfere with heat balance to any greater extent. However, shivering becomes impaired and, combined with strenuous exercise, the heat loss will become obvious. Alcohol is known to be a dominant cause of death in urban hypothermia. It gives a feeling of bravado and influences judgement, leading to ignoring prophylactic measures.
Pregnancy. During pregnancy women are not more sensitive to cold. To the contrary, they can be less sensitive, due to raised metabolism. Risk factors during pregnancy are combined with the cold-related factors such as accident risks, clumsiness due to clothing, heavy lifting, slipping and extreme working positions. The health care system, the society and the employer should therefore pay extra attention to the pregnant woman in cold work.
Pharmacology and cold
Negative side effects of drugs during cold exposure could be thermoregulatory (general or local), or the effect of the drug can be altered. As long as the worker retains normal body temperature, most prescribed drugs don’t interfere with performance. However, tranquilizers (e.g., barbiturates, benzodiazepines, phentothiazides as well as cyclic antidepressants) may disturb vigilance. In a threatening situation the defence mechanisms against hypothermia may be impaired and the awareness of the hazardous situation is reduced.
Beta-blockers induce peripheral vasoconstriction and decrease the tolerance to cold. If an individual needs medication and has cold exposure in his or her working situation, attention should be paid to negative side effects of these drugs.
On the other hand, no drug or anything else drunk, eaten or otherwise administered to the body has been shown to be able to raise normal heat production, for example in an emergency situation when hypothermia or a cold injury threatens.
Health control programme
Health risks connected to cold stress, cold-related factors and accidents or trauma are known only to a limited extent. There is a large individual variation in capacities and health status, and this requires careful consideration. As previously mentioned, special diseases, medication and some other factors may render a person more susceptible to the effects of cold exposure. A health control programme should be part of the employment procedure, as well as a repeated activity for the staff. Table 6 specifies factors to control for in different types of cold work.
Table 6. Recommended components of health control programs for personnel exposed to cold stress and cold-related factors
|
Factor |
Outdoor work |
Cold store work |
Arctic and subarctic work |
|
Infectious diseases |
** |
** |
*** |
|
Cardio-vascular diseases |
*** |
** |
*** |
|
Metabolic diseases |
** |
* |
*** |
|
Musculoskeletal problems |
*** |
* |
*** |
|
Cryopathies |
** |
** |
** |
|
Psychological stress |
*** |
** |
*** |
|
Smoking and snuffing |
** |
** |
** |
|
Alcohol |
*** |
** |
*** |
|
Pregnancy |
** |
** |
*** |
|
Medication |
** |
* |
*** |
*= routine control, **= important factor to consider, ***= very important factor to consider.
Prevention of Cold Stress
Human adaptation
With repeated exposures to cold conditions, people perceive less discomfort and learn to adjust to and cope with conditions in an individual and more efficient way, than at the onset of exposure. This habituation reduces some of the arousal and distraction effect, and improves judgement and precaution.
Behaviour
The most apparent and natural strategy for prevention and control of cold stress is that of precaution and intentional behaviour. Physiological responses are not very powerful in preventing heat losses. Humans are, therefore, extremely dependent on external measures such as clothing, shelter and external heat supply. The continuous improvement and refinement of clothing and equipment provides one basis for successful and safe exposures to cold. However, it is essential that products be adequately tested in accordance with international standards.
Measures for prevention and control of cold exposure are often the responsibility of the employer or the supervisor. However, the efficiency of protective measures relies to a significant degree upon knowledge, experience, motivation and ability of the individual worker to make the necessary adjustments to his or her requirements, needs and preferences. Hence, education, information and training are important elements in health control programmes.
Acclimatization
There is evidence for different types of acclimatization to long-term cold exposure. Improved hand and finger circulation allows for the maintenance of a higher tissue temperature and produces a stronger cold-induced vasodilatation (see Figure 18). Manual performance is better maintained after repeated cold exposures of the hand.
Repeated whole-body cooling appears to enhance peripheral vasoconstriction, thereby increasing surface tissue insulation. Korean pearl-diving women showed marked increases in skin insulation during the winter season. Recent investigations have revealed that the introduction and use of wet suits reduces the cold stress so much that tissue insulation does not change.
Three types of possible adaptations have been proposed:
- increased tissue insulation (as previously mentioned)
- hypothermic reaction (“controlled” drop in core temperature)
- metabolic reaction (increased metabolism).
The most pronounced adaptations should be found with native people in cold regions. However, modern technology and living habits have reduced most extreme types of cold exposure. Clothing, heated shelters and conscious behaviour allow most people to maintain an almost tropical climate at the skin surface (micro- climate), thereby reducing cold stress. The stimuli to physiological adaptation become weaker.
Probably the most cold-exposed groups today belong to polar expeditions and industrial operations in arctic and subarctic regions. There are several indications that any eventual adaptation found with severe cold exposure (air or cold water) is of the insulative type. In other words, higher core temperatures can be kept with a reduced or unchanged heat loss.
Diet and water balance
In many cases cold work is associated with energy-demanding activities. In addition, protection against cold requires clothing and equipment weighing several kilograms. The hobbling effect of clothing increases muscular effort. Hence, given work tasks require more energy (and more time) under cold conditions. The caloric intake through food must compensate for this. An increase of the percentage of calories provided by fat should be recommended to outdoor workers.
Meals provided during cold operations must provide sufficient energy. Enough carbohydrates must be included to ensure stable and safe blood sugar levels for workers engaged in hard work. Recently, food products have been launched on the market with claims that they stimulate and increase body heat production in the cold. Normally, such products consist merely of carbohydrates, and they have so far failed in tests to perform better than similar products (chocolate), or better than expected from their energy content.
Water loss may be significant during cold exposure. First, tissue cooling causes a redistribution of blood volume, inducing “cold diuresis”. Tasks and clothing must allow for this, since it may develop rapidly and requires urgent execution. The almost dry air at subzero conditions allows a continuous evaporation from skin and respiratory tract that is not readily perceived. Sweating contributes to water loss, and should be carefully controlled and preferably avoided, due to its detrimental effect on insulation when absorbed by clothing. Water is not always readily available at subzero conditions. Outdoors it must be supplied or produced by melting snow or ice. As there is a depression of thirst it is mandatory that workers in the cold drink water frequently to eliminate the gradual development of dehydration. Water deficit may lead to reduced working capacity and increased risk of getting cold injuries.
Conditioning workers for work in the cold
By far the most effective and appropriate measures for adapting humans to cold work, are by conditioning—education, training and practice. As previously mentioned, much of the success of adjustments to cold exposure depends on behavioural action. Experience and knowledge are important elements of this behavioural process.
Persons engaged in cold work should be given a basic introduction to the specific problems of cold. They must receive information about physiological and subjective reactions, health aspects, risk of accidents, and protective measures, including clothing and first aid. They should be gradually trained for the required tasks. Only after a given time (days to weeks) should they work full hours under the extreme conditions. Table 7 provides recommendations as to the contents of conditioning programmes for various types of cold work.
Table 7. Components of conditioning programs for workers exposed to cold
|
Element |
Outdoor work |
Cold store work |
Arctic and subarctic work |
|
Health control |
*** |
** |
*** |
|
Basic introduction |
*** |
** |
*** |
|
Accident prevention |
*** |
** |
*** |
|
Basic first aid |
*** |
*** |
*** |
|
Extended first aid |
** |
* |
*** |
|
Protective measures |
*** |
** |
*** |
|
Survival training |
see text |
* |
*** |
*= routine level, **= important factor to consider, ***= very important factor to consider.
Basic introduction means education and information about the specific cold problems. Registration and analysis of accidents/injuries is the best base for preventive measures. Training in first aid should be given as a basic course for all personnel, and specific groups should get an extended course. Protective measures are natural components of a conditioning programme and are dealt with in the following section. Survival training is important for arctic and subarctic areas, and also for outdoor work in other remote areas.
Technical control
General principles
Due to the many complex factors that influence human heat balance, and the considerable individual variations, it is difficult to define critical temperatures for sustained work. The temperatures given in Figure 6 must be regarded as action levels for improvement of conditions by various measures. At temperatures below those given in figure 6, exposures should be controlled and evaluated. Techniques for assessment of cold stress and recommendations for time-limited exposures are dealt with elsewhere in this chapter. It is assumed that best protection of hands, feet and body (clothing) is available. With inappropriate protection, cooling will be expected at considerably higher temperatures.
Figure 6. Estimated temperatures at which certain thermal imbalances of the body may develop.*
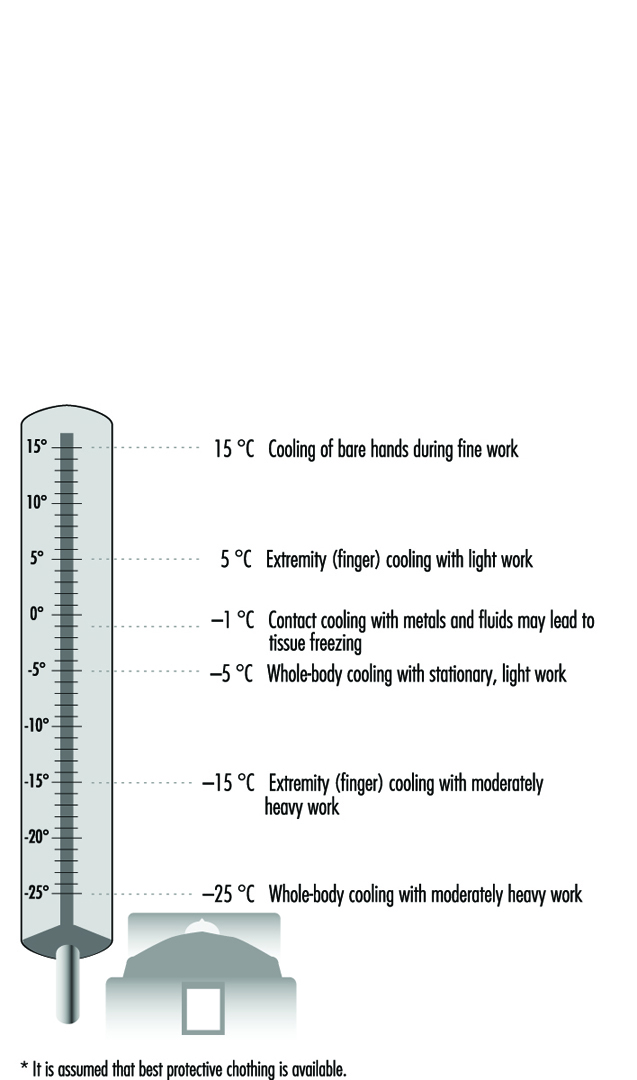
Tables 8 and 9 list different preventive and protective measures that can be applied to most types of cold work. Much effort is saved with careful planning and foresight. Examples given are recommendations. It must be emphasized that the final adjustment of clothing, equipment and work behaviour must be left to the individual. Only with a cautious and intelligent integration of behaviour with the requirements of the real environmental conditions can a safe and efficient exposure be created.
Table 8. Strategies and measures during various phases of work for prevention and alleviation of cold stress
|
Phase/factor |
What to do |
|
Planning phase |
Schedule work for a warmer season (for outdoor work). Check if work can be done indoors (for outdoor work). Allow more time per task with cold work and protective clothing. Analyse suitability of tools and equipment for work. Organize work in suitable work-rest regimens, considering task, load and protection level. Provide heated space or heated shelter for recovery. Provide training for complex work tasks under normal conditions. Check medical records of staff. Ascertain appropriate knowledge and competence of staff. Provide information about risks, problems, symptoms and preventive actions. Separate goods and worker line and keep different temperature zones. Care for low velocity, low humidity and low noise level of the air- Provide extra personnel to shorten exposure. Select adequate protective clothing and other protective equipment. |
|
Before work shift |
Check climatic conditions at onset of work. Schedule adequate work-rest regimens. Allow for individual control of work intensity and clothing. Select adequate clothing and other personal equipment. Check weather and forecast (outdoors). Prepare schedule and control stations (outdoors). Organize communication system (outdoors). |
|
During work shift |
Provide for break and rest periods in heated shelter. Provide for frequent breaks for hot drinks and food. Care for flexibility in terms of intensity and duration of work. Provide for replacement of clothing items (socks, gloves, etc.). Protect from heat loss to cold surfaces. Minimize air velocity in work zones. Keep workplace clear from water, ice and snow. Insulate ground for stationary standing work places. Provide access to extra clothing for warmth. Monitor subjective reactions (buddy system) (outdoors). Report regularly to foreman or base (outdoors). Provide for sufficient recovery time after severe exposures (outdoors). Protect against wind effects and precipitation (outdoors). Monitor climatic conditions and anticipate weather change (outdoors). |
Source: Modified from Holmér 1994.
Table 9. Strategies and measures related to specific factors and equipment
|
Behaviour |
Allow for time to adjust clothing. Prevent sweating and chilling effects by making adjustments of clothing in due time before change in work rate and/or exposure. Adjust work rate (keep sweating minimal). Avoid rapid shifts in work intensity. Allow for adequate intake of hot fluid and hot meals. Allow for time to return to protected areas (shelter, warm room) (outdoors). Prevent wetting of clothing from water or snow. Allow for sufficient recovery in protected area (outdoors). Report on progress of work to foreman or base (outdoors). Report major deviations from plan and schedule (outdoors). |
|
Clothing |
Select clothing you have previous experience with. With new clothing, select tested garments. Select insulation level on the basis of anticipated climate and activity. Care for flexibility in clothing system to allow for great adjustment of insulation. Clothing must be easy to put on and take off. Reduce internal friction between layers by proper selection of fabrics. Select size of outer layers to make room for inner layers. Use multi-layer system: —inner layer for micro climate control —middle layer for insulation control —outer layer for environmental protection. Inner layer should be non-absorbent to water, if sweating cannot be sufficiently controlled. Inner layer may be absorbent, if sweating is anticipated to be none or low. Inner layer may consist of dual-function fabrics, in the sense that fibre in contact with skin is non absorbing and fibres next to the middle layer is absorbing water or moisture. Middle layer should provide loft to allow stagnant air layers. Middle layer should be form-stable and resilient. Middle layer may be protected by vapour barrier layers. Garments should provide sufficient overlap in the waist and back region. Outer layer must be selected according to additional protection requirements, such as wind, water, oil, fire, tear or abrasion. Design of outer garment must allow easy and extensive control of openings at neck, sleeves, wrists etc., to regulate ventilation of interior space. Zippers and other fasteners must function also with snow and windy conditions. Buttons should be avoided. Clothing shall allow operation even with cold, clumsy fingers. Design must allow for bent postures without compression of layers and loss of insulation. Avoid unnecessary constrictions. Carry extra wind proof blankets (NOTE! The aluminized “astronaut blanket” does not protect more than expected from being wind proof. A large polyethylene garbage bag has the same effect). |
|
Education Training |
Provide education and information on the special problems of cold. Provide information and training in first-aid and treatment of cold injuries. Test machinery, tools and equipment in controlled cold conditions. Select tested goods, if available. Train complex operations under controlled cold conditions. Inform about accidents and accident prevention. |
|
Handwear |
Mittens provide the best overall insulation. Mittens should allow fine gloves to be worn underneath. Prolonged exposures requiring fine hand work, must be intercepted by frequent warm-up breaks. Pocket heaters or other external heat sources may prevent or delay hand cooling. Sleeve of clothing must easily accommodate parts of gloves or mittens —underneath or on top. Outer garment must provide easy storage or fixing of handwear when taken off. |
|
Footwear |
Boots shall provide high insulation to the ground (sole). Sole shall be made of a flexible material and have an anti-slippery pattern. Select size of boot so it can accommodate several layers of socks and an insole. Ventilation of most footwear is poor, so moisture should be controlled by frequent replacement of socks and insole. Control moisture by vapour barrier between inner and outer layer. Allow boots to dry completely between shifts. Legs of clothing must easily accommodate parts of boots —underneath or on top. |
|
Headgear |
Flexible headgear comprises an important instrument for control of heat and whole-body heat losses. Headgear should be windproof. Design should allow sufficient protection of ears and neck. Design must accommodate other types of protective equipment (e.g., ear muffs, safety goggles). |
|
Face |
Face mask should be windproof and insulative. No metallic details should contact skin. Significant heating and humidification of inspired air can be achieved by special breathing masks or mouth pieces. Use safety goggles outdoors, especially in sleet and snow. Use eye protection against ultra-violet radiation and glare. |
|
Equipment Tools |
Select tools and equipment intended and tested for cold conditions. Choose design that allows operation by gloved hands. Prewarm tools and equipment. Store tools and equipment in heated space. Insulate handles of tools and equipment. |
|
Machinery |
Select machinery intended for operation in cold environments. Store machinery in protected space. Prewarm machinery before use. Insulate handles and controls. Design handles and controls for operation by gloved hands. Prepare for easy repair and maintenance under adverse conditions. |
|
Workplace |
Keep air velocity as low as possible. Use wind-breaking shields or windproof clothing. Provide insulation to ground with prolonged standing, kneeling or lying work. Provide auxiliary heating with light, stationary work. |
Source: Modified from Holmér 1994.
Some recommendations as to the climatic conditions under which certain measures should be taken have been given by the American Conference of Governmental Industrial Hygienists (ACGIH 1992). The fundamental requirements are that:
- workers be provided with sufficient and appropriate protective clothing
- special precautions should be taken for older workers or workers with circulatory problems.
Further recommendations related to the provision of hand protection, to workplace design and to work practices are presented below.
Hand protection
Fine barehanded operations below 16ºC require provision for heating the hands. Metal handles of tools and bars should be covered by insulating materials at temperatures below –1ºC. Anticontact gloves should be worn when surfaces at –7ºC or lower are within reach. At –17ºC insulative mittens must be used. Evaporative liquids at temperatures below 4 °C should be handled so as to avoid splashes to bare or poorly protected skin areas.
Work practices
Below –12ºC Equivalent Chill Temperature, workers should be under constant supervision (buddy system). Many of the measures given in Table 18 apply. With lowered temperatures it is increasingly important that workers are instructed in safety and health procedures.
Workplace design
Workplaces must be shielded from wind, and air velocities kept below 1 m/s. Wind-protective clothing should be used when appropriate. Eye protection must be supplied for special outdoor conditions with sunshine and snow-covered ground. Medical screening is recommended for persons working routinely in cold below –18ºC. Recommendations as to workplace monitoring include the following:
- Suitable thermometry should be arranged when the temperature is below 16ºC.
- Indoor wind speeds should be monitored at least every 4 hours.
- Outdoor work requires measurement of wind speed and air temperatures below –1ºC.
- The Equivalent Chill Temperature should be determined for combinations of wind and air temperature.
Most of the recommendations in Tables 8 and 9 are pragmatic and straightforward.
Clothing is the most important measure for individual control. The multi-layer approach allows for more flexible solutions than single garments incorporating the function of several layers. In the end, however, the specific needs of the worker should be the ultimate determinant of what would be the most functional system. Clothing protects against cooling. On the other hand overdressing in the cold is a common problem, also reported from the extreme exposures of arctic expeditions. Overdressing may rapidly result in large amounts of sweat, which accumulates in clothing layers. During periods of low activity, the drying of moist clothing increases body heat loss. The obvious preventive measure is to control and reduce sweating by appropriate selection of clothing and early adjustments to changes in work rate and climate conditions. There is no clothing fabric that can absorb large amounts of sweat and also preserve good comfort and insulative properties. Wool remains lofty and apparently dry despite absorption of some water (moisture regain), but large amounts of sweat will condense and cause problems similar to those of other fabrics. The moisture yields some heat liberation and may contribute to the preservation of warmth. However, when the wool garment dries on the body, the process reverses as discussed above, and the person is inevitably cooled.
Modern fibre technology has produced many new materials and fabrics for clothing manufacturing. Garments are now available that combine waterproofness with good water vapour permeability, or high insulation with reduced weight and thickness. It is essential, however, to select garments with guaranteed tested properties and functions. Many products are available that try to mimic the more expensive original products. Some of them represent such poor quality that they may even be hazardous to use.
Protection against cold is determined primarily by the thermal insulation value of the complete clothing ensemble (clo value). However, properties such as air permeability, vapour permeability and waterproofness of the outer layer in particular are essential for cold protection. International standards and test methods are available for measuring and classifying these properties. Similarly, handgear and footwear may be tested for their cold-protective properties using international standards such as European standards EN 511 and EN 344 (CEN 1992, 1993).
Outdoor cold work
Specific problems of outdoor cold work are the aggregate of climatic factors that may result in cold stress. The combination of wind and low air temperature significantly increases the cooling power of the environment, which has to be considered in terms of work organization, workplace shielding and clothing. Precipitation, either in the air as snow or rain, or on the ground, requires adjustments. The variation in weather conditions requires workers to plan for, bring and use additional clothing and equipment.
Much of the problem in outdoor work relates to the sometimes great variations in activity and climate during a work shift. No clothing system is available that can accommodate such large variations. Consequently, clothing must be frequently changed and adjusted. Failure to do so may result in cooling due to insufficient protection, or sweating and overheating caused by too much clothing. In the latter case, most of the sweat condenses or is absorbed by clothing. During periods of rest and low activity, wet clothing represents a potential hazard, since its drying drains the body of heat.
Protective measures for outdoor work include appropriate work-rest regimens with rest pauses taken in heated shelters or cabins. Stationary work tasks can be protected from wind and precipitation by tents with or without additional heating. Spot heating by infrared or gas heaters may be used for certain work tasks. Prefabrication of parts or components may be carried out indoors. Under subzero conditions, workplace conditions including weather should be regularly monitored. Clear rules must exist regarding what procedures to apply when conditions get worse. Temperature levels, eventually corrected for wind (wind chill index), should be agreed upon and linked to an action programme.
Cold storage work
Frozen food requires storage and transportation at low ambient temperatures (–20ºC). Work in cold stores can be found in most parts of the world. This kind of artificial cold exposure is characterized by a constant, controlled climate. Workers may perform continuous work or, most common, intermittent work, shifting between cold and temperate or warm climates outside the storehouse.
As long as work requires some physical effort, heat balance can be achieved by selecting appropriate protective clothing. The special problems of hand and feet often require regular breaks every 1.5 to 2 hours. The break must be long enough to allow rewarming (20 minutes).
Manual handling of frozen goods requires protective gloves with sufficient insulation (in particular, of the palm of the hand). Requirements and test methods for cold-protective gloves are given in the European standard EN 511, which is described in more detail in the article “Cold indices and standards” in this chapter. Local heaters (e.g., infrared radiator), placed in workplaces with stationary work, improve heat balance.
Much work in cold stores is carried out with fork-lifts. Most of these vehicles are open. Driving creates a relative wind speed, which in combination with the low temperature increases body cooling. In addition, the work itself is rather light and the associated metabolic heat production low. Accordingly, the required clothing insulation is quite high (around 4 clo) and cannot be met with most types of overalls in use. The driver gets cold, starting with feet and hands, and exposure has to be time limited. Depending on available protective clothing, appropriate work schedules should be organized in terms of work in cold and work or rest in normal environments. A simple measure to improve heat balance is to install a heated seat in the truck. This may prolong work time in the cold and prevent local cooling of the seat and back. More sophisticated and expensive solutions include the use of heated cabs.
Special problems arise in hot countries, where the cold store worker, usually the truck driver, is intermittently exposed to cold (–30ºC) and heat (30ºC). Brief exposures (1 to 5 min) to each condition make it difficult to adopt suitable clothing—it may be too warm for the outdoor period and too cold for the cold store work. Truck cabs may be one solution, once the problem of condensation upon windows is solved. Appropriate work-rest regimens must be elaborated and based on work tasks and available protection.
Cool workplaces, found for example in the fresh food industry, comprise climatic conditions with air temperatures of +2 to +16ºC, depending on type. Conditions are sometimes characterized by high relative humidities, inducing condensation of water at cold spots and moist or water-covered floors. The risk of slipping is increased in such workplaces. Problems can be solved by good workplace hygiene and cleaning routines, which contribute to reducing the relative humidity.
The local air velocity of work stations is often too high, resulting in complaints of draught. The problems can often be solved by changing or adjusting the inlets for cold air or by rearranging work stations. Buffers of frozen or cold goods close to work stations may contribute to draught sensation due to the increased radiation heat exchange. Clothing must be selected on the basis of an assessment of the requirements. The IREQ method should be used. In addition clothing should be designed to protect from local draught, moisture and water. Special hygienic requirements for food handling put some restrictions on design and type of clothing (i.e., the outer layer). An appropriate clothing system must integrate underwear, insulating middle layers and the outer layer to form a functional and sufficient protective system. Headgear is often required due to hygienic demands. However, existing headgear for this purpose is often a paper cap, which does not offer any protection against cold. Similarly, footwear often comprises clogs or light shoes, with poor insulation properties. Selection of more suitable headgear and footwear should better preserve warmth of these body parts and contribute to an improved general heat balance.
A special problem in many cool workplaces is the preservation of manual dexterity. Hands and fingers cool rapidly when muscular activity is low or moderate. Gloves improve protection but impair dexterity. A delicate balance between the two demands has to be found. Cutting meat often requires a metal glove. A thin textile glove worn underneath may reduce the cooling effect and improve comfort. Thin gloves may be sufficient for many purposes. Additional measures to prevent hand cooling include the provision of insulated handles of tools and equipment or spot heating using, for example, infrared radiators. Electrically heated gloves are on the market, but often suffer from poor ergonomics and insufficient heating or battery capacity.
Cold-water exposure
During immersion of the body in water the potential for large losses of heat in a short time is great and presents an apparent hazard. The heat conductivity of water is more than 25 times higher than that of air, and in many exposure situations the capacity of surrounding water to absorb heat is effectively infinite.
Thermoneutral water temperature is around 32 to 33ºC, and at lower temperatures the body responds by cold vasoconstriction and shivering. Long exposures in water at temperatures between 25 and 30ºC provoke body cooling and progressive development of hypothermia. Naturally, this response becomes stronger and more serious with the lowering of the water temperature.
Exposure to cold water is common in accidents at sea and in conjunction with water sports of various kinds. However, even in occupational activities, workers run the risk of immersion hypo-thermia (e.g., diving, fishing, shipping and other offshore operations).
Victims of shipwrecks may have to enter cold water. Their protection varies from pieces of thin clothing to immersion suits. Lifejackets are mandatory equipment aboard ships. They should be equipped with a collar to reduce heat loss from the head of unconscious victims. The equipment of the ship, the efficiency of the emergency procedures and the behaviour of crew and passengers are important determinants for the success of the operation and the subsequent exposure conditions.
Divers regularly enter cold waters. The temperature of most waters with commercial diving, in particular at some depth, is low—often lower than 10ºC. Any prolonged exposure in such cold water requires thermally insulated diving suits.
Heat loss. Heat exchange in the water may be seen as simply a flow of heat down two temperature gradients—one internal, from core to skin, and one external, from the skin surface to the surrounding water. Body surface heat loss can be simply described by:
Cw = hc·(Tsk–Tw)·AD
where Cw is the rate of convective heat loss (W), hc is the convective heat transfer coefficient (W/°Cm2), Tsk is the average skin temperature (°C), Tw is the water temperature (°C) and AD is the body surface area. The small components of heat loss from respiration and from non-immersed parts (e.g., head) can be neglected (see the section on diving below).
The value of hc is in the range of 100 to 600 W/°Cm2. The lowest value applies to still water. Turbulence, be it caused by swimming movements or flowing water, doubles or triples the convection coefficient. It is easily understood that the unprotected body may suffer a considerable heat loss to the cold water—eventually exceeding what can be produced even with heavy exercise. In fact, a person (dressed or undressed) who falls into cold water in most cases saves more heat by lying still in the water than by swimming.
Heat loss to the water can be significantly reduced by wearing special protective suits.
Diving. Diving operations several hundreds of metres below sea level must protect the diver from the effects of pressure (one ATA or 0.1 MPa/10 m) and cold. Breathing cold air (or a cold gas mixture of helium and oxygen) drains the lung tissues of body heat. This direct heat loss from the body core is large at high pressures and can easily achieve values higher than the resting metabolic heat production of the body. It is poorly sensed by the human organism. Dangerously low internal temperatures may develop without a shivering response if the body surface is warm. Modern offshore work requires the diver to be supplied with extra heat to the suit as well as to the breathing apparatus, to compensate for large convective heat losses. In deep-sea diving, the comfort zone is narrow and warmer than at sea level: 30 to 32ºC at 20 to 30 ATA (2 to 3 MPa) and increasing to 32 to 34ºC up to 50 ATA (5 MPa).
Physiological factors: Cold immersion elicits a strong, acute respiratory drive. The initial responses include an “inspiratory gasp”, hyperventilation, tachycardia, peripheral vasoconstriction and hypertension. An inspiratory apnoea for several seconds is followed by an increased ventilation. The response is almost impossible to control voluntarily. Hence, a person may easily inhale water if the sea is rough and the body becomes submersed. The first seconds of exposure to very cold water, accordingly, are dangerous, and sudden drowning may occur. Slow immersion and proper protection of the body reduce the reaction and allow for better control of respiration. The reaction gradually fades and normal breathing is usually achieved within a few minutes.
The rapid rate of heat loss at the skin surface emphasizes the importance of internal (physiological or constitutional) mechanisms for reducing the core-to-skin heat flow. Vasoconstriction reduces extremity blood flow and preserves central heat. Exercise increases extremity blood flow, and, in conjunction with the increased external convection, it may in fact accelerate heat loss despite the elevated heat production.
After 5 to 10 min in very cold water, extremity temperature drops quickly. Neuromuscular function deteriorates and the ability to coordinate and control muscular performance degrades. Swimming performance may be severely reduced and quickly put the person at risk in open waters.
Body size is another important factor. A tall person has a larger body surface area and loses more heat than a small person at given ambient conditions. However, the relatively larger body mass compensates for this in two ways. Metabolic heat production rate increases in relation to the larger surface area, and the heat content at a given body temperature is greater. The latter factor comprises a larger buffer to heat losses and a slower rate of core temperature decrease. Children are at a greater risk than adults.
By far the most important factor is body fat content—in parti-cular, subcutaneous fat thickness. Adipose tissue is more insulating than other tissues and is bypassed by much of the peripheral circulation. Once vasoconstriction has occurred, the layer of subcutaneous fat acts as an extra layer. The insulative effect is almost linearly related to the layer thickness. Accordingly, women in general have more cutaneous fat than men and lose less heat under the same conditions. In the same way, fat persons are better off than lean persons.
Personal protection. As previously mentioned, prolonged stay in cold and temperate waters requires additional external insulation in the form of diving suits, immersion suits or similar equipment. The wet suit of foamed neoprene provides insulation by the thickness of the material (closed foam cells) and by the relatively controlled “leakage” of water to the skin microclimate. The latter phenomenon results in the warming of this water and the establishment of a higher skin temperature. Suits are available in various thickness, providing more or less insulation. A wet suit compresses at depth and loses thereby much of its insulation.
The dry suit has become standard at temperatures below 10ºC. It allows the maintenance of a higher skin temperature, depending on the amount of extra insulation worn under the suit. It is a fundamental requirement that the suit not leak, as small amounts of water (0.5 to 1 l) seriously reduce the insulative power. Although the dry suit also compresses at depth, dry air is automatically or manually added from the scuba tank to compensate for the reduced volume. Hence, a microclimate air layer of some thickness can be maintained, providing good insulation.
As previously mentioned, deep-sea diving requires auxiliary heating. Breathing gas is prewarmed and the suit is heated by the flushing of warm water from the surface or the diving bell. More recent warming techniques rely upon electrically heated underwear or closed-circuit tubules filled with warm fluid.
Hands are particularly susceptible to cooling and may require extra protection in the form of insulative or heated gloves.
Safe exposures. The rapid development of hypothermia and the imminent danger of death from cold-water exposure necessitates some sort of prediction of safe and unsafe exposure conditions.
Figure 7 depicts predicted survival times for typical North Sea offshore conditions. The applied criterion is a drop in core temperature to 34ºC for the tenth percentile of the population. This level is assumed to be associated with a conscious and manageable person. The proper wearing, use and functioning of a dry suit doubles the predicted survival time. The lower curve refers to the unprotected person immersed in normal clothing. As clothing gets completely soaked with water the effective insulation is very small, resulting in short survival times (modified from Wissler 1988).
Figure 7. Predicted survival times for typical North Sea offshore scenarios.

Work in arctic and subarctic regions
Arctic and subarctic regions of the world comprise additional problems to those of normal cold work. The cold season coincides with darkness. Days with sunlight are short. These regions cover vast, unpopulated or sparsely populated areas, such as Northern Canada, Siberia and Northern Scandinavia. In addition nature is harsh. Transportation takes place over large distances and takes a long time. The combination of cold, darkness and remoteness require special consideration in terms of work organization, preparation and equipment. In particular, training in survival and first aid must be provided and the appropriate equipment supplied and made easily available at work.
For the working population in the arctic regions there are many health-threatening hazards, as mentioned elsewhere. The risks of accident and injury are high, drug abuse is common, cultural patterns produce problems, as does the confrontation between local/native culture and modern western industrial demands. Snowmobile driving is an example of multiple-risk exposure in typical arctic conditions (see below). Cold stress is thought to be one of the risk factors that produces higher frequencies of certain diseases. Geographical isolation is another factor producing different types of genetic defects in some native areas. Endemic diseases—for example, certain infectious diseases—are also of local or regional importance. Settlers and guest workers also run a higher risk for different kinds of psychological stress reactions secondary to new environment, remoteness, harsh climate conditions, isolation and awareness.
Specific measures for this kind of work must be considered. Work must be carried out in groups of three, so that in case of emergency, one person may go for help while one is left taking care of the victim of, for example, an accident. The seasonal variation in daylight and climate must be considered and work tasks planned accordingly. Workers must be checked for health problems. If required, extra equipment for emergency or survival situations must be available. Vehicles such as cars, trucks or snowmobiles must carry special equipment for repair and emergency situations.
A specific work problem in these regions is the snowmobile. Since the sixties the snowmobile has developed from a primitive, low-technology vehicle to one that is fast and technically highly developed. It is most frequently used for leisure activities, but also for work (10 to 20%). Typical professions using the snowmobile are police, military personnel, reindeer herders, lumberjacks, farmers, tourist industry, trappers and search and rescue teams.
The vibration exposure from a snowmobile means a highly increased risk for vibration-induced injuries to the driver. The driver and the passengers are exposed to unpurified exhaust gas. The noise produced by the engine may induce hearing loss. Due to high speed, terrain irregularities and poor protection for the driver and the passengers, the risk of accidents is high.
The musculoskeletal system is exposed to vibrations and extreme working positions and loads, especially when driving in harsh terrain areas or slopes. If you get stuck, handling the heavy engine induces perspiration and often musculoskeletal problems (e.g., lumbago).
Cold injuries are common among snowmobile workers. The speed of the vehicle aggravates the cold exposure. Typical injured parts of the body are especially the face (could in extreme cases include cornea), ears, hands and feet.
Snowmobiles are usually used in remote areas where climate, terrain and other conditions contribute to the risks.
The snowmobile helmet must be developed for the working situation on the snowmobile with attention to the specific exposure risks produced by the vehicle itself, terrain conditions and climate. Clothing must be warm, windproof and flexible. The activity transients experienced during snowmobile riding are difficult to accommodate in one clothing system and require special consideration.
Snowmobile traffic in remote areas also presents a communication problem. Work organization and equipment should ensure safe communication with the home base. Extra equipment must be carried to handle emergency situations and allow protection for a time long enough for the rescue team to function. Such equipment includes, for example, wind sack, extra clothing, first-aid equipment, snow shovel, repair kit and cooking gear.
Hazardous-Response Personnel
Employees in occupations that respond to hazardous-substance emergencies or incidents can be broadly classified as hazardous-response personnel. A hazardous-substance emergency or incident can be defined as an uncontrolled or illegal release or threatened release of a hazardous material or its hazardous by-products. A hazardous-substance emergency can arise from a transportation-related incident or at a fixed-site facility. Transportation-related incidents can occur as a result of accidents on land, water or in the air. Fixed-site facilities include industrial facilities, commercial office buildings, schools, farms or any other fixed site that contains hazardous materials.
Employees whose primary responsibility is response to hazardous-materials incidents are generally considered members of hazardous materials (HAZMAT) response teams. HAZMAT team professionals include public-sector employees such as fire-fighters, police and transportation officials who have received specialized training in managing hazardous-substance emergencies. Fixed-site facilities such as manufacturing plants, oil refineries or research laboratories often have internal HAZMAT teams who are trained to manage hazardous-materials incidents inside their facilities. Environmental regulations may necessitate that such facilities report incidents to public agencies when the surrounding community is at risk, or if a threshold quantity of a regulated hazardous material has been released. Public health professionals with training in exposure assessment and hazardous materials management, such as industrial (occupational) hygienists, are often members of public- or private-sector HAZMAT teams.
Police and fire personnel are frequently the first professionals to respond to hazardous-substance emergencies, since they may encounter a leak or release of a hazardous substance associated with a transportation accident or structural fire. These employees are typically considered to be first responders, and their primary responsibility is to isolate the public from the release by denying public access to the site of the incident. This is generally achieved through physical control measures such as physical barriers and crowd- and traffic-control measures. First responders typically do not take actions to contain or control the release. First responders may be at greater risk of exposure to hazardous materials than other HAZMAT teams since they may encounter a hazardous-material release without the benefit of full personal protective equipment, or encounter an unexpected exposure. First responders typically notify HAZMAT team members to manage the incident. The specific health concerns of police and fire personnel are described elsewhere in this chapter.
The primary responsibility of the HAZMAT team is to contain and control the release. This activity can be very hazardous when the incident involves explosive or highly toxic materials such as chlorine gas. The incident commander is responsible for deciding what actions should be taken to resolve the emergency. It may take a considerable amount of time to develop a plan of control for complex accidents such as a multiple railroad car derailment or a chemical plant explosion and fire. In some circumstances where mitigation measures involve a significant risk of major injury to HAZMAT personnel, a decision may be reached not to take specific containment measures, and the hazardous material may be released into the environment.
The final phase of a hazardous-substance emergency often involves the clean-up of residual hazardous substances. This is frequently done by labourers. In some jurisdictions, health and safety regulations mandate that such workers receive specialized training in hazardous-material response and participate in a programme of medical surveillance. These employees may be at a greater risk of exposure since clean-up operations can involve close contact with the hazardous materials. Other occupations at risk of chemical exposure from hazardous-substance emergencies are emergency heath-care providers including emergency medical technicians, paramedics, emergency room medical staff and other hospital personnel.
Potential Hazards
The potential hazards associated with a hazardous-substance emergency are incident specific and can include chemical, radiological and biological hazards. These agents can be gases or vapours, aerosols including mists, fumes, dusts or particulates, solids and/or liquids. The potential hazards faced by hazardous-substance response personnel depend on the exposure potential of the agent, reactivity (flammability, explosivity and so on) and toxicity potential.
Information regarding the type of agents involved in hazardous-substance emergencies is available in the United States from the Agency for Toxic Substances and Disease Registry (ATSDR) Hazardous Substances Emergency Events Surveillance (HSEES) system. The HSEES system is an active surveillance system which tracks incidents that have a public-health impact (Hall et al. 1994). The HSEES system was developed because of reported deficiencies in other national US systems that track releases of hazardous substances (Binder 1989). HSEES does not identify all releases since limited spills at fixed-site facilities are not recorded. The registry was established in 1990 and initially involved five states, but has grown to include eleven states. In 1993 HSEES recorded 3,945 hazardous-substances emergencies. Other countries and states also have systems that record hazardous-material events (Winder et al. 1992).
HSEES data summarizing the types of chemical substances released during hazardous substance emergencies including those associated with personnel injuries, during the two-year period 1990–1992 showed that the most common chemical classes of substances released were volatile organic compounds, herbicides, acids and ammonia. The greatest risk of developing an injury occurred during incidents involving cyanides, insecticides, chlorine, acids and bases. During 1990–1992, 93% of the incidents involved the release of only one chemical, and 84% of the releases occurred at fixed-site facilities.
Health Outcomes
Hazardous-substance personnel face several distinct types of acute health threats. The first category of health threat relates to the toxicity potential of the agent as well as potential contact with blood and other body fluids of incident victims. The second threat is the risk of sustaining major physical trauma including burns associated with an explosion and/or fire from an unexpected chemical reaction, or with structural collapse of a building or container. The third type of acute health effect is risk of heat stress or exhaustion associated with performing heavy work, often in chemical protective clothing, which impairs the body’s efficiency of evaporative cooling. Employees with pre-existing health problems such as cardiovascular disease, respiratory disease, diabetes, disorders of consciousness, or those who take medications that may impair heat exchange or cardiorespiratory response to exercise, are at additional risk when performing such arduous work.
There is limited information concerning the health outcomes of hazardous-substance personnel responding to hazardous-substance emergencies. The HSEES registry indicated that for 1990 to 1992, 467, or 15%, of 4,034 emergency response events resulted in 446 injuries. Two hundred of the injured persons were classified as first responders, including fire-fighters, law-enforcement personnel, emergency medical response personnel and HAZMAT team members. Nearly one-quarter of first responders (22%) did not utilize any type of personal protective equipment.
The principle reported health effects among all persons sustaining injuries included respiratory irritation (37.3%), eye irritation (22.8%) and nausea (8.9%). Chemical burns were reported in 6.1% of those injured. Heat stress was reported in 2%. Eleven deaths were recorded, including one in a first responder. The causes of death among the entire group were reported as trauma, chemical burns, asphyxiation, thermal burns, heat stress and cardiac arrest. Other reports have suggested that first responders are at risk of being injured in acute responses.
The health risks associated with chronic exposures to a wide array of hazardous-materials incidents have not been characterized. Epidemiological studies have not been completed of HAZMAT team members. Epidemiological studies of fire-fighters who perform first response activities at fire scenes have revealed that they may be at greater risk of developing several types of malignancies (see the article “Firefighting hazards” in this chapter).
Preventive Measures
Several measures can reduce the incident of hazardous-substance emergencies. These are described in figure 1. First, prevention through the adoption and enforcement of regulations involving production, storage, transportation and use of hazardous substances can lessen the potential for unsafe work practices. Training of employees in proper workplace practices and hazard management is critical in preventing accidents.
Figure 1. Preventive guidelines.

Second, proper management and supervision of the incident can lessen the impact of an incident. The management of the activities of the first responders and clean-up workers by the incident commander is critical. There must be supervision and evaluation of the progress of the emergency response to ensure that the response objectives are being met safely, effectively and efficiently.
The third measure includes health-related actions that are taken during and after an incident. These actions include the provision of appropriate first aid at the scene and proper decontamination procedures. Failure to properly decontaminate a victim may result in ongoing absorption of the hazardous agent and place the HAZMAT or medical staff at risk of exposure from direct patient contact (Cox 1994). Medical personnel should also be trained regarding specific treatment and personal protective measures for unusual chemical events.
Participation in a medical surveillance programme by workers is a measure that can be utilized to prevent health problems among hazardous-response personnel. Medical surveillance can potentially detect conditions at an early stage before significant adverse health effects have occurred in workers. In addition, medical conditions which may place employees at significantly greater risk from performing the work, such as cardiovascular disease, can be identified and monitored. Sensory impairments that can interfere with field communications, including hearing and vision defects, can also be identified to determine whether they would pose a significant threat during hazardous emergency response.
Most of the identified preventive measures are based upon community awareness of local hazards. Implementation of hazardous-substance emergency plans by adequately trained staff and the wise allocation of resources are imperative. Community awareness of hazards includes informing communities of hazardous materials which are at fixed facilities or materials that are being transported through a community (e.g., by road, rail, airport or water). This information should enable fire departments and other agencies to plan for emergency incidents. Fixed facilities and transporters of hazardous materials should also have individual response plans developed that include specific provisions for notification of public agencies in a timely manner. Emergency medical personnel should have the necessary knowledge of the potential hazards in their local community. Trained medical staff should be available to provide appropriate treatment and diagnosis for the symptoms, signs and specific treatment recommendations for hazardous substances in their communities. Fixed site facilities should establish liaisons with local emergency departments and inform them of potential hazards in the workplace and the need for special supplies or mediations needed to manage potential incidents at these facilities. Planning and training should help enhance the provision of appropriate medical care and decrease the number of injuries and deaths from incidents.
The potential also exists for hazardous-substance emergencies to occur as a result of a natural disaster such as floods, earthquakes, lightning, hurricanes, winds or severe storms. Although the number of such events appears to be increasing, planning and preparation for these potential emergencies is very limited (Showalter and Myers 1994). Planning efforts need to include natural causes of emergency incidents.
Paramedical Personnel and Ambulance Attendants
Paramedical personnel, including emergency medical technicians (EMTs) and ambulance attendants, provide the initial medical response at the scene of an accident, disaster or acute illness, and transport patients to the point where more definitive treatment can be rendered. Advances in medical equipment and communications have increased the capabilities of these workers to resuscitate and stabilize victims en route to an emergency centre. The increased capabilities of EMTs is matched by the increase in hazards which they now face in performance of their duties. The emergency medical responder works as a member of a small unit, usually two to three persons. Job tasks must often be performed rapidly in poorly equipped locations with limited access. The work environment may present unanticipated or uncontrolled biological, physical and chemical hazards. Dynamic, rapidly changing situations and hostile patients and surroundings magnify the dangers of the work. A consideration of the health risks to paramedical personnel is important in the design of strategies to reduce and prevent injury at work.
Risks to paramedical personnel fall broadly into four main categories: physical hazards, inhalation risks, infectious exposures and stress. Physical hazards involve both musculoskeletal injuries related to job tasks, and effects of the environment in which the work takes place. Heavy and awkward lifting is the predominant physical hazard for these workers, accounting for over one-third of injuries. Back strains constitute the most common type of injury; one retrospective survey found 36% of all reported injuries were due to lower-back strain (Hogya and Ellis 1990). Patient and equipment lifting appear to be the main factors in lower-back injury; nearly two-thirds of back injuries occur at the scene of response. Recurrent back injuries are common and may lead to prolonged or permanent disability and early retirement of experienced workers. Other frequent injuries include contusions of the head, neck, trunk, legs and arms, ankle sprains, wrist and hand sprains and finger wounds. Falls, assaults (both by patients and by bystanders) and motor vehicle accidents are additional major sources of injury. Collisions account for the majority of motor vehicle accidents; associated factors may be heavy work schedules, time pressures, poor weather conditions and inadequate training.
Thermal injury from both cold and hot environments has been reported. Local climate and weather conditions, along with improper clothing and equipment, may contribute to heat stress and cold injury. Accelerated hearing loss from exposure to sirens, which produce ambient noise levels exceeding mandated thresholds, has also been observed in ambulance personnel.
Smoke inhalation and poisoning by gases, including carbon monoxide, represent significant respiratory hazards for paramedics. Though occurring infrequently, these exposures can have dire consequences. Responders arriving on the scene may initially be inadequately prepared for rescue work, and can be overcome by smoke or toxic gases before additional help and equipment are available.
In common with other health-care workers, paramedical personnel are at increased risk of infection with blood-borne pathogenic viruses, especially hepatitis B virus (HBV) and presumably hepatitis C. Serologic markers for HBV infection were found in 13 to 22% of emergency medical technicians, a prevalence level three to four times that of the general population (Pepe et al. 1986). In one survey, evidence of infection was found to correlate with years worked as an EMT. Measures for protection against HBV and HIV transmission established for health-care workers apply to paramedical technicians, and are outlined elsewhere in this Encyclopaedia. As a sidelight, use of latex gloves for protection against blood-borne pathogens may lead to an increased risk for contact urticaria and other manifestations of allergy to rubber products similar to those noted in health-care workers in hospital settings.
Paramedical and ambulance work, which involves work in uncontrolled and hazardous environments as well as responsibility for important decisions with limited equipment and time pressures, leads to high levels of occupational stress. Impaired professional performance, work dissatisfaction and loss of concern for patients, all of which may arise from the effects of stress, endanger both providers and the public. Intervention by mental health workers after major disasters and other traumatic incidents, along with other strategies to reduce burnout among emergency workers, have been proposed to mitigate the destructive effects of stress in this field (Neale 1991).
Few specific recommendations exist for screening and preventive measures in paramedical workers. Blood-borne pathogen training and immunization to HBV should be undertaken in all employees with exposure to infectious fluids and materials. In the United States, health-care facilities are required to inform an emergency response employee who sustains an unprotected exposure to a blood-borne disease or to an airborne, uncommon or rare infectious disease, including tuberculosis (NIOSH 1989). Similar guidelines and statutes exist for other countries (Laboratory Center for Disease Control 1995). Compliance with standard immunization practices for infectious agents (e.g., measles-mumps-rubella vaccine) and tetanus is essential. Periodic screening for tuberculosis is recommended if the potential for high-risk exposure is present. Properly designed equipment, instruction in body mechanics and scene hazard education have been proposed to reduce lifting injuries, although the setting in which much ambulance work is performed may render the most well-designed controls ineffective. The environment in which paramedical work occurs should be considered carefully, and appropriate clothing and protective equipment provided when necessary. Respirator training is appropriate for personnel who may be exposed to toxic gases and smoke. Finally, the erosive effects of stress on paramedical workers and emergency technicians must be borne in mind, and strategies for counselling and intervention should be developed to lessen its impact.
Health and Safety Hazards of Maritime Rescues
Oceans, lakes, rivers and other large bodies of water present extremes of environmental conditions demanding the maximum in human performance. The defining attribute that characterizes health and safety hazards of maritime rescues is the pervasive presence of the water itself.
Maritime rescues share many of the health and safety hazards experienced in land-based rescues. The risk of communicable disease transmission, exposure to toxic substances, threat of interpersonal violence and exposure to various physical agents (e.g., noise, vibration, radiation) are examples of commonly shared hazards of water and land rescues. The maritime environment, however, presents several unique or exaggerated hazards compared to the land-based environment. This article will focus on those health and safety hazards most identified with at-sea rescues.
Modes of Response
Before discussing specific health and safety hazards it is important to understand that maritime rescues can take place by either surface vessel or aircraft, or a combination of both. The importance of understanding the mode of response is that characteristics of hazard exposure are determined, in part, by the mode.
Surface vessels typically used in maritime rescues travel at speeds under 40 knots (74.1 km/h), have a relatively limited operational range (under 200 miles (320 km)), are heavily influenced by water surface and weather conditions, are subject to damage by floating debris and generally are not sensitive to weight consideration. Helicopters, the most commonly used aircraft in maritime rescue, can travel in excess of 150 knots (278 km/h), may have an effective operational range of 300 miles (480 km) (more with in-flight refuelling), are more influenced by weather than water conditions and are very sensitive to weight concerns.
Factors that determine the mode of response include distance, urgency, geographic location, resource availability, environmental conditions and character of the responding rescue organization. Factors that tend to favour surface vessel response are closer proximity, lower urgency, proximity to metropolitan or developed regions, milder water surface conditions and a less well developed aviation system and infrastructure. Rescue by air tends to be favoured by longer distances, higher urgency, remoteness from metropolitan or developed regions, harsher water surface conditions, and regions with better-developed aviation systems and infrastructure. Figure 1 and figure 2 show both types of rescue.
Figure 1. Maritime rescue by ship.
US Army
Figure 2. Maritime rescue by helicopter.

US Army
Maritime Hazards
The dominant hazards of maritime rescues are those intrinsic to the watery environment. Rescue personnel are directly exposed to maritime elements and must be prepared for survival themselves.
Drowning is the most common cause of occupation-related death in the maritime environment. People require specialized flotation equipment to survive in water for any length of time. Even the best swimmers require flotation assistance to survive in rough weather. Prolonged (more that several hours) survival in stormy weather is usually impossible without specialized survival suits or rafts. Injuries, reduced level of consciousness, confusion and panic or uncontrolled fear will reduce the likelihood of water survival.
Water is more efficient than air at conducting away body heat. The risk of death due to hypothermia or hypothermia-induced drowning increases rapidly as water temperature decreases below 24 °C. As water temperatures approach freezing, effective survival time is measured in minutes. Prolonged survival in cold water, even when the surface is calm, is possible only with the assistance of specialized survival suits or rafts.
The maritime environment exhibits the extremes of weather conditions. Wind, rain, fog, snow and icing can be severe. Visibility and the ability to communicate can be seriously restricted. Rescuers are constantly at risk for getting wet through wave and splash action, wind-driven rain or spray, and vessel- or aircraft-generated spray. Water, especially salt water, can damage mechanical and electrical equipment essential for vessel or flight operations.
Exposure to salt water can result in skin, mucosal and eye irritation. Ingestion of water-borne infectious micro-organisms (e.g., Vibrio spp.) increases the likelihood of gastro-intestinal disease. The water around rescue sites can be contaminated with pollutants (e.g., sewage) or substances hazardous to human health (e.g., petroleum products). Potential envenomation by water snakes and by various coelenterates (e.g., jellyfish) can occur in areas supporting these organisms. Water and thermal protective clothing is often cumbersome, restrictive and prone to promote heat stress. During sunny conditions, rescuers can experience skin and eye damage due to reflected ultraviolet light.
The surface of large bodies of water, such as the oceans, typically has undulant wave motion with coexistent surface chop. Rescue personnel, therefore, conduct work on a moving platform, which complicates any movement or procedures. Motion sickness is a constant threat. Surface vessels travelling through rough conditions can experience severe pounding and instability which promotes fatigue, an increased likelihood of falls or being struck by falling objects and equipment failure. Aircraft operating in stormy weather experience turbulence that can induce motion sickness, accelerate fatigue and compound the risks of surface-to-air evacuation.
Planning and Prevention
The maritime environment can be extremely hostile. However, the health and safety hazards associated with maritime rescues can be controlled or minimized through careful planning and prevention efforts. Safe and effective rescues can take place.
Rescue organizations must be acutely aware of the nature of the maritime environment, understand the operational characteristics and limitations of response equipment and personnel, practice system safety and provide suitable equipment, training and leadership. Rescue personnel must be in good physical and mental condition, know their equipment and procedures, stay alert, be prepared, remain proficient and understand the specifics of the situation they are dealing with.
Rescue personnel can be involved in vessel or aviation mishaps. The difference between being a rescuer and needing to be rescued can be only a matter of moments. Ultimate mishap survival is dependent on:
- survival of the impact itself
- successful egress
- enduring post-mishap until rescued.
Each stage of mishap survival has its own set of necessary training, equipment, ergonomics and procedures to maximize survival. Maritime rescue personnel usually act in isolation, without immediate backup, and often at long distances from shore. A rule of thumb is for rescuers to have the necessary resources to survive the time it takes to be rescued themselves in the event of their own mishap. Rescuers need to be trained, equipped and prepared to survive in the worst of conditions.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."