- You are here:
-
Home

- k2 Feed
Case Study: Occupational Health Surveys in China
To understand the magnitude of occupational health problems in China, the Ministry of Public Health (MOPH) has organized a number of nationwide surveys, including the following:
- a survey on occupational exposures to benzene, lead, mercury, TNT and organophosphates (1979-81)
- a retrospective epidemiological investigation on occupational cancers in workers exposed to eight chemicals (1983-85)
- an epidemiological survey on pneumoconioses (1952-86)
- a survey on occupational health problems of small-scale industries and the relevant intervention strategies (1984-85, 1990-92).
The results of these surveys have served as a very important foundation for formulating national policies and regulations. At the same time, a national occupational health reporting system has been established by MOPH. The Annual Report of the National Occupational Health Situation has been published since 1983. The data are compiled and analysed by the National Center of Occupational Health Reporting (NCOHR) and then reported to the MOPH. There are local reporting offices in Occupational Health Institutes (OHIs) or Health Epidemic Prevention Stations (HEPS) at all levels from county to province. The reporting follows a “bottom-up” procedure annually, but, if an acute poisoning accident happened which involved three or more cases of poisoning or one death, it must be reported to the local OHI and also directly to the MOPH within 24 hours by the primary-contact medical institutions. The information required to be reported every year includes the following: registered new cases of compensable occupational diseases, the results of health examinations of workers and the monitoring of working environments (MOPH 1991). China is currently promoting the computerization of the reporting system and its computer network. It currently extends from the national centre to the provincial offices.
Measurement Strategies and Techniques for Occupational Exposure Assessment in Epidemiology
Other articles in this chapter present general principles of medical surveillance of occupational illnesses and exposure surveillance. This article outlines some principles of epidemiological methods that may be used to fulfil surveillance needs. Application of these methods must take into account basic principles of physical measurement as well as standard epidemiological data-gathering practice.
Epidemiology can quantify the association between occupational and non-occupational exposure to chemico-physical stressors or behaviour and disease outcomes, and can thus provide information to develop interventions and prevention programmes (Coenen 1981; Coenen and Engels 1993). Availability of data and access to workplace and personnel records usually dictate the design of such studies. Under the most favourable circumstances, exposures can be determined through industrial hygiene measurements that are carried out in an operating shop or factory, and direct medical examinations of workers are used to ascertain possible health effects. Such evaluations can be done prospectively for a period of months or years to estimate risks of diseases such as cancer. However, it is more often the case that past exposures must be reconstructed historically, projecting backwards from current levels or using measurements recorded in the past, which may not completely meet informational needs. This article presents some guidelines and limitations for measurement strategies and documentation that affect epidemiological assessment of workplace health hazards.
Measurements
Measurements should be quantitative wherever possible, rather than qualitative, because quantitative data are subject to more powerful statistical techniques. Observable data are commonly classified as nominal, ordinal, interval and ratio. Nominal level data are qualitative descriptors which differentiate only types, such as different departments within a factory or different industries. Ordinal variables may be arranged from “low” to “high” without conveying further quantitative relationships. An example is “exposed” vs. “unexposed”, or classifying smoking history as non-smoker (= 0), light smoker (= 1), medium smoker (= 2) and heavy smoker (= 3). The higher the numerical value, the stronger the smoking intensity. Most measurement values are expressed as ratio or interval scales, in which a concentration of 30 mg/m3 is double the concentration of 15 mg/m3. Ratio variables possess an absolute zero (like age) while interval variables (like IQ) do not.
Measurement strategy
Measurement strategy takes into account information about the measurement site, the surrounding conditions (e.g., humidity, air pressure) during the measurement, the duration of the measurement and the measurement technique (Hansen and Whitehead 1988; Ott 1993).
Legal requirements often dictate measurement of eight-hour time-weighted averages (TWAs) of levels of hazardous substances. However, not all individuals work eight-hour shifts all the time, and levels of exposures may fluctuate during the shift. A value measured for one person’s job might be considered representative of an eight-hour shift value if the exposure duration is longer than six hours during the shift. As a practical criterion, a sampling duration of at least two hours should be sought. With time intervals that are too short, the sampling in one time period can show higher or lower concentrations, thereby over- or underestimating the concentration during the shift (Rappaport 1991). Therefore, it can be useful to combine several measurements or measurements over several shifts into a single time-weighted average, or to use repeated measurements with shorter sampling durations.
Measurement validity
Surveillance data must satisfy well-established criteria. The measurement technique should not influence the results during the measurement process (reactivity). Furthermore, the measurement should be objective, reliable and valid. The results should not be influenced either by the measurement technique used (execution objectivity) or by the reading or documentation by the measurement technician (assessment objectivity). The same measurement values should be obtained under the same conditions (reliability); the intended thing should be measured (validity) and interactions with other substances or exposures should not unduly influence the results.
Quality of Exposure Data
Data sources. A basic principle of epidemiology is that measurements made at the individual level are preferable to those made at the group level. Thus, the quality of epidemiolological surveillance data decreases in the following order:
- direct measurements taken of persons; information on exposure levels and time progression
- direct measurements taken of groups; information on current exposure levels for specific groups of workers (sometimes expressed as job-exposure matrices) and their variation over time
- measurements abstracted or reconstructed for individuals; estimation of exposure from company records, purchasing lists, descriptions of product lines, interviews with employees
- measurements abstracted or reconstructed for groups; historical estimation of group-based exposure indexes.
In principle, the most precise determination of the exposure, using documented measurement values over time, should always be sought. Unfortunately, indirectly measured or historically reconstructed exposures are often the only data available for estimating exposure-outcome relationships, even though considerable deviations exist between measured exposures and exposure values reconstructed from company records and interviews (Ahrens et al. 1994; Burdorf 1995). The quality of the data declines in the order exposure measurement, activity-related exposure index, company information, employee interviews.
Exposure scales. The need for quantitative monitoring data in surveillance and epidemiology goes considerably beyond the narrow legal requirements of threshold values. The goal of an epidemiological investigation is to ascertain dose-effect relation-ships, taking into account potentially confounding variables. The most precise information possible, which in general can be expressed only with a high scale level (e.g., ratio scale level), should be used. Separation into larger or smaller threshold values, or coding in fractions of threshold values (e.g., 1/10, 1/4, 1/2 threshold value) as is sometimes done, essentially relies on data measured on a statistically weaker ordinal scale.
Documentation requirements. In addition to information on the concentrations and the material and time of measurement, external measurement conditions should be documented. This should include a description of the equipment used, measurement technique, reason for the measurement and other relevant technical details. The purpose of such documentation is to ensure uniformity of measurements over time and from one study to another, and to permit comparisons between studies.
Exposure and health outcome data gathered for individuals are usually subject to privacy laws that vary from one country to another. Documentation of exposure and health conditions must adhere to such laws.
Epidemiological Requirements
Epidemiological studies strive to establish a causal link between exposure and disease. Some aspects of surveillance measurements that affect this epidemiological assessment of risk are considered in this section.
Type of disease. A common starting point for epidemiological studies is the clinical observation of a surge in a particular disease in a company or area of activity. Hypotheses on potential biological, chemical or physical causal factors ensue. Depending on the availability of data, these factors (exposures) are studied using a retrospective or prospective design. The time between the beginning of the exposure and the onset of the disease (latency) also affects study design. The range of latency can be considerable. Infections from certain enteroviruses have latency/incubation times of 2 to 3 hours, whereas for cancers latencies of 20 to 30 years are typical. Therefore, exposure data for a cancer study must cover a considerably longer period of time than for an infectious disease outbreak. Exposures which began in the distant past can continue up to the onset of disease. Other diseases associated with age, such as cardiovascular disease and stroke, can appear in the exposed group after the study begins and must be treated as competing causes. It is also possible that people classified as “not sick” are merely people who have not yet manifested clinical illness. Thus, continued medical surveillance of exposed populations must be maintained.
Statistical power. As previously stated, measurements should be expressed on as high a data level (ratio scale level) as possible in order to optimize the statistical power to produce statistically significant results. Power in turn is affected by the size of the total study population, the prevalence of exposure in that population, the background rate of illness and the magnitude of risk of the disease that is caused by the exposure under study.
Mandated disease classification. Several systems are available for codifying medical diagnoses. The most common are ICD-9 (International Classification of Diseases) and SNOMED (Systematic Nomenclature of Medicine). ICD-O (oncology) is a particularization of the ICD for codifying cancers. ICD coding documentation is legally mandated in many health systems throughout the world, especially in Western countries. However, SNOMED codification can also codify possible causal factors and external conditions. Many countries have developed specialized coding systems to classify injuries and illnesses that also include the circumstances of the accident or exposure. (See the articles “Case study: Worker protection and statistics on accidents and occupational diseases—HVBG, Germany” and “Development and application of an occupational injury and illness classification system”, elsewhere in this chapter.)
Measurements that are made for scientific purposes are not bound by the legal requirements that apply to mandated surveillance activities, such as determination of whether threshold limits have been exceeded in a given workplace. It is useful to examine exposure measurements and records in such a way as to check for possible excursions. (See, for example, the article “Occupational hazard surveillance” in this chapter.)
Treatment of mixed exposures. Diseases often have several causes. Therefore it is necessary to record as completely as possible the suspected causal factors (exposures/confounding factors) in order to be able to distinguish the effects of suspected hazardous agents from one another and from the effects of other contributory or confounding factors, such as cigarette smoking. Occupational exposures are often mixed (e.g., solvent mixtures; welding fumes such as nickel and cadmium; and in mining, fine dust, quartz and radon). Additional risk factors for cancers include smoking, excess alcohol consumption, poor nutrition and age. Besides chemical exposures, exposures to physical stressors (vibration, noise, electromagnetic fields) are possible triggers for diseases and must be considered as potential causal factors in epidemiological studies.
Exposures to multiple agents or stressors may produce interaction effects, in which the effect of one exposure is magnified or reduced by another that occurs contemporaneously. A typical example is the link between asbestos and lung cancer, which is many times more pronounced among smokers. An example of the mixture of chemical and physical exposures is progressive systemic scleroderma (PSS), which is probably caused by a combined exposure to vibration, solvent mixtures and quartz dust.
Consideration of bias. Bias is a systematic error in classifying persons in the “exposed/not exposed” or “diseased/not diseased” groups. Two types of bias should be distinguished: observation (information) bias and selection bias. With observation (information) bias, different criteria may be used to classify subjects into the diseased/not diseased groups. It is sometimes created when the target of a study includes persons employed in occupations known to be hazardous, and who may already be under increased medical surveillance relative to a comparison population.
In selection bias two possibilities should be distinguished. Case-control studies begin by separating persons with the disease of interest from those without that disease, then examine differences in exposure between these two groups; cohort studies determine disease rates in groups with different exposures. In either type of study, selection bias exists when information on the exposure affects classification of subjects as sick or not sick, or when information on disease status affects classification of subjects as exposed or not exposed. A common example of selection bias in cohort studies is the “healthy worker effect”, which is encountered when disease rates in exposed workers are compared with those in the general population. This can result in underestimation of disease risk because working populations are often selected from the general population on the basis of continued good health, frequently based upon medical examination, whereas the general population contains the ill and infirm.
Confounders. Confounding is the phenomenon whereby a third variable (the confounder) alters the estimate of an association between a presumed antecedent factor and a disease. It can occur when the selection of subjects (cases and controls in a case-control study or exposed and unexposed in a cohort study) depends in some way upon the third variable, possibly in a manner unknown to the investigator. Variables associated only with exposure or disease are not confounders. To be a confounder a variable must meet three conditions:
- It must be a risk factor for the disease.
- It must be associated with the exposure in the study population.
- It must not be in the causal pathway from exposure to disease.
Before any data are collected for a study it is sometimes impossible to predict whether or not a variable is a likely confounder. A variable which has been treated as a confounder in a previous study might not be associated with exposure in a new study within a different population, and would therefore not be a confounder in the new study. For instance, if all subjects are alike with respect to a variable (e.g., sex), then that variable cannot be a confounder in that particular study. Confounding by a particular variable can be accounted for (“controlled”) only if the variable is measured along with exposure and illness outcomes. Statistical control of confounding may be done crudely using stratification by the con-founding variable, or more precisely using regression or other multivariate techniques.
Summary
The requirements of measuring strategy, measuring technology and documentation for industrial workplaces are sometimes statutorily defined in terms of threshold limit value surveillance. Data protection regulations also apply to the protection of company secrets and person-related data. These requirements call for the comparable measuring results and measurement conditions and for an objective, valid and reliable measuring technology. Additional requirements put forward by epidemiology refer to the representativeness of measurements and to the possibility of establishing links between exposures for individuals and subsequent health outcomes. Measurements may be representative for certain tasks, i.e. they may reflect typical exposure during certain activities or in specific branches or typical exposure of defined groups of persons. It would be desirable to have measurement data directly attributed to the study subjects. This would make it necessary to include with measurement documentation information about persons working at the concerned workplace during the measurement or to set up a registry allowing such direct attribution. Epidemiological data collected at the individual level are usually preferable to those obtained at the group level.
Case study: Wismut - A Uranium Exposure Revisited
Historical Development
The Erz mountains have been mined since the twelfth century, and beginning in 1470 silver mining brought the area to prominence. Around the year 1500 the first reports of a specific disease among miners appeared in Agricola’s writings. In 1879 this disease was recognized by Haerting and Hesse as lung cancer, but at that time what caused it was not clear. In 1925 “Schneeberg lung cancer” was added to the list of occupational diseases.
The material from which Marie Curie isolated the elements radium and polonium came from the slag heap of the Joachimstal (Jachymov) in Bohemia. In 1936 Rajewsky’s radon measurements near Schneeberg confirmed the already assumed connection between radon in the mining shafts and lung cancer.
In 1945 the Soviet Union intensified its atomic weapons research programme. The search for uranium was extended to the Erz Mountains, as the conditions for mining were better there than in the Soviet deposits. After initial inquiries, the whole area was placed under Soviet military administration and declared a restricted zone.
From 1946 to 1990 the Soviet Wismut Company (SAG), later the Soviet-German Wismut Company (SDAG), carried out uranium mining in Thuringia and Saxony (figure 1). At the time the Soviet Union was under pressure to obtain sufficient quantities of uranium to construct the first Soviet atomic bomb. Appropriate equipment was not available, so achieving the necessary level of uranium production was possible only by disregarding safety measures. Working conditions were especially bad in the years 1946 to 1954. According to an SAG Wismut health report, 1,281 miners had fatal accidents and 20,000 suffered injuries or other detrimental effects to their health just in the second half of 1949.
Figure 1. Mining areas of SDAG Wismut in East Germany
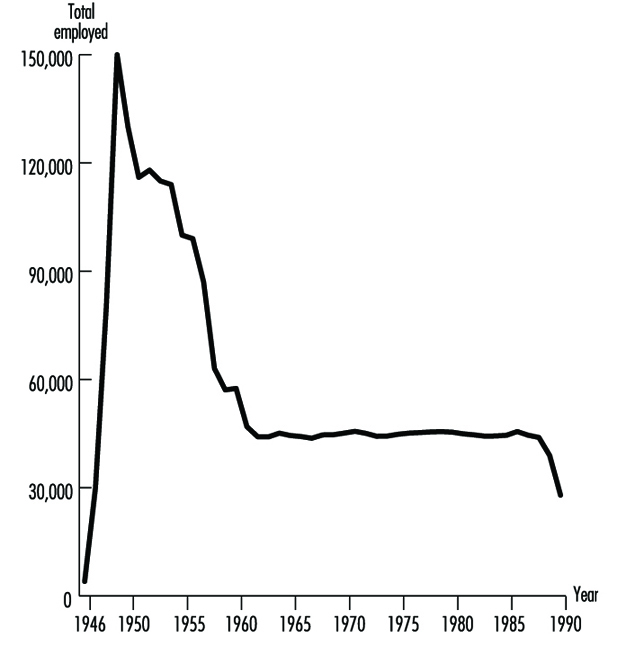
In post-war Germany, the Soviet Union considered uranium mining a form of reparations. Prisoners, conscripts and “volunteers” were mobilized, but at first there were hardly any skilled personnel. In all, Wismut employed between 400,000 and 500,000 people (figure 2).
Figure 2. Wismut employees 1946-90
Bad working conditions, the lack of suitable technology and intense work pressure led to extremely high numbers of accidents and illnesses. The working conditions gradually improved beginning in 1953, when German participation in the Soviet company began.
Dry-drilling, which produced high levels of dust, was employed from 1946 to 1955. No artificial ventilation was available, resulting in high radon concentrations. In addition, the workers’ health was adversely affected by the extremely heavy labour due to the lack of equipment, the lack of safety gear and long work shifts (200 hours per month).
Figure 3. Exposure records of former SDAG Wismut

The exposure level varied over time and from shaft to shaft. The systematic measurement of the exposure also ensued in different phases, as is shown in figure 3. The exposures to ionizing radiation (shown in Working Level Months (WLM)) can be given only very roughly (table 1). Today, comparisons with radiation-exposure situations in other countries, measurements made under experimental conditions and assessments of written records permit a more precise statement of the exposure level.
Table 1. Estimates of radiation exposure (Working Level Months/Year) in the Wismut mines
|
Year |
WLM/Year |
|
1946–1955 |
30–300 |
|
1956–1960 |
10–100 |
|
1961–1965 |
5–50 |
|
1966–1970 |
3–25 |
|
1971–1975 |
2–10 |
|
1976–1989 |
1–4 |
In addition to intensive exposure to rock dust, other factors relevant to illnesses were present, such as uranium dust, arsenic, asbestos and emissions from explosives. There were physical effects from noise, hand-arm vibrations and whole-body vibrations. Under these conditions, silicoses and radiation-related bronchial carcinomas dominate the record of occupational diseases from 1952 to 1990 (table 2).
Table 2. Comprehensive overview of known occupational diseases in Wismut uranium mines 1952-90
|
List No. BKVO 1 |
Absolute number |
% |
|
|
Diseases due to quartz |
40 |
14,733 |
47.8 |
|
Malignant tumours or pretumours from ionizing radiation |
92 |
5,276 |
17.1 |
|
Diseases due to partial body vibration |
54 |
— |
— |
|
Diseases of tendons and extremity joints |
71–72 |
4,950 |
16.0 |
|
Impaired hearing due to noise |
50 |
4,664 |
15.1 |
|
Skin diseases |
80 |
601 |
1.9 |
|
Other |
— |
628 |
2.1 |
|
Total |
30,852 |
100 |
1 Occupational disease classification of the former GDR.
Source: Wismut Health System Annual Reports.
Although over time the health services of SAG/SDAG Wismut provided increasing levels of comprehensive care for the miners, including annual medical examinations, the effects on health of extracting the ore were not systematically analysed. Production and working conditions were kept strictly secret; the Wismut companies were autonomous and organizationally were a “state within a state”.
The full magnitude of the events became known only in 1989-90 with the end of the German Democratic Republic (GDR). In December 1990 uranium mining was discontinued in Germany. Since 1991 the Berufsgenossenschaften (preventing, recording and compensating industrial and trade associations), as the statutory accident insurance carrier have been responsible for recording and compensating all accidents and occupational diseases related to the former Wismut operation. This means that the associations are responsible for providing affected individuals with the best possible medical care and for collecting all relevant occupational health and safety information.
In 1990, approximately 600 claims for bronchial carcinoma were still pending with the Wismut social insurance system; some 1,700 cases of lung cancer had been turned down in earlier years. Since 1991 these claims have been pursued or reopened by the responsible Berufsgenossenschaften. On the basis of scientific projections (Jacobi, Henrichs and Barclay 1992; Wichmann, Brüske-Hohlfeld and Mohner 1995), it is estimated that in the next ten years between 200 and 300 cases of bronchial carcinomas per year will be recognized as resulting from working at Wismut.
The Present: After the Change
The production and working conditions at SDAG Wismut left their mark on both the employees and the environment in Thuringia and Saxony. In accordance with the law of the Federal Republic of Germany, the federal government took over responsibility for cleaning up the environment in the affected region. The costs of these activities for the period 1991-2005 have been estimated at DM 13 billion.
After the GDR joined the Federal Republic of Germany in 1990, the Berufsgenossenschaften, as statutory accident insurance carriers, became responsible for managing occupational diseases in the former GDR. In light of the particular conditions at Wismut, the Berufsgenossenschaften decided to form a special unit to handle occupational safety and health for the Wismut complex. To the extent possible, while respecting legal regulations protecting the privacy of personal data, the Berufsgenossenschaften secured records on former working conditions. Thus when the company was dissolved for economic reasons all evidence that could possibly serve to substantiate the claims of employees in case of illness would not be lost. The “Wismut Central Care Office” (ZeBWis) was established by the Federation on 1 January 1992 and bears responsibility for occupational medical treatment, early detection and rehabilitation.
From ZeBWis’s goal of providing appropriate occupational medical care to former uranium mining employees, four essential health surveillance tasks emerged:
- organizing mass screening examinations for early diagnosis and treatment of diseases
- documenting the screening findings and linking them with data from the occupational disease detection procedures
- scientifically analysing the data
- support of research on early detection and treatment of disease.
Screening is provided to the exposed workers in order to assure early diagnosis whenever possible. Ethical, scientific and economic aspects of such screening procedures require a thorough discussion which is beyond the scope of this article.
A programme of occupational medicine was developed, based on the well-founded trade association principles for special occupational medical examinations. Integrated into this were examination methods known from mining and radiation protection. The component parts of the programme follow from the main agents of exposure: dust, radiation and other hazardous materials.
The ongoing medical surveillance of former Wismut employees is aimed primarily at early detection and treatment of bronchial carcinomas resulting from exposure to radiation or other carcinogenic materials. Whereas the connections between ionizing radiation and lung cancers are proven with adequate certainty, the effects on health of long-term, low-dosage radiation exposure have been less researched. Current knowledge is based on extrapolations of data from survivors of the atomic bombings of Hiroshima and Nagasaki, as well as data obtained from other international studies of uranium miners.
The situation in Thuringia and Saxony is exceptional in that significantly more people underwent a much broader range of exposures. Therefore, a wealth of scientific knowledge can be gained from this experience. To what degree radiation works synergistically with exposure to carcinogens like arsenic, asbestos or diesel motor emissions in causing lung cancer should be scientifically examined using newly obtained data. The early detection of bronchial carcinomas through the introduction of state-of-the-art examination techniques should be an important part of the prospective scientific research.
Available Data from the Wismut Health System
In response to the extreme accident and health problems it faced, Wismut established its own health service, which provided, among other things, annual medical screening examinations, including chest x rays. In later years additional occupational disease examination units were set up. Since the Wismut health service took over not only occupational medicine, but also full medical care for employees and their dependents, by 1990 SDAG Wismut had collected comprehensive health information on many former and current Wismut employees. In addition to complete information on the occupational medical examinations, and a complete archive of occupational diseases, a comprehensive x-ray archive exists with over 792,000 x rays.
In Stollberg the Wismut health system had a central pathology department in which comprehensive histological and pathological material was collected from the miners, as well as from the inhabitants of the area. In 1994 this material was given to the German Cancer Research Center (DKFZ) in Heidelberg for safekeeping and research purposes. A portion of the records of the former health system was first taken over by the statutory accident insurance system. For this purpose, ZeBWis established a temporary archive at Shaft 371 in Hartenstein (Saxony).
These records are used for processing insurance claims, for preparing and administering occupational medical care and for scientific study. In addition to being used by the Berufsgenossenschaften, the records are available to experts and to authorized physicians in the context of their clinical work with and management of each former employee.
The core of these archives consists of the complete files of occupational diseases (45,000) which were taken over, together with the corresponding occupational disease tracing files (28,000), the tracing files for monitoring dust-endangered persons (200,000), as well as targeted documentary records with the results of the occupational medical fitness and monitoring examinations. In addition, the autopsy records of Stollberg Pathology are kept in this ZeBWis archive.
These last-mentioned records, as well as the occupational disease tracing files, have in the meantime been prepared for data processing. Both these forms of documentation will be used for extracting data for a 60,000-person comprehensive epidemiological study by the federal ministry for the environment.
In addition to the data on exposure to radon and radon by-products, the records on the exposure of former employees to other agents are of special interest to the Berufsgenossenschaften. Thus the present-day Wismut GmbH has measurement results available for viewing, in list form, from the early 1970s to the present for silicogenic dusts, asbestos dusts, heavy metal dusts, wood dusts, explosives dusts, toxic vapours, welding fumes, diesel motor emissions, noise, partial- and whole-body vibrations and heavy physical labour. For the years 1987 to 1990 the individual measurements are archived in electronic media.
This is important information for retrospective analysis of the exposures in Wismut’s uranium mining operations. It also constitutes the basis for constructing a job-exposure matrix which assigns exposures to tasks for research purposes.
To round out the picture, further records are stored in the department that safeguards health data at Wismut GmbH, including: patient files of former out-patients, accident reports by the former company and by occupational safety inspections, clinical occupational medical records, biological exposure tests, occupational medical rehabilitation and neoplastic disease reports.
However, not all Wismut archives—primarily paper files—were designed for centralized evaluation. Thus, with the dissolution of SDAG Wismut on 31 December 1990, and the dissolution of the Wismut company health system, the question was posed of what to do with these unique records.
Digression: Incorporating the Holdings
The first task for ZeBWis was to define the people who worked underground or in the preparation plants and to determine their current location. The holdings comprise some 300,000 people. Few of the company’s records were in a form that could be used in data processing. Thus it was necessary to tread the wearisome path of viewing one card at a time. The card files from nearly 20 locations had to be collected.
The next step was to collect the vital statistics and addresses of these people. Information from old personnel and wage records was not useful for this. Old addresses were often no longer valid, in part because a blanket renaming of streets, squares and roads took place after the unification treaty was signed. The Central Inhabitant Registry of the former GDR was also not useful, as by this time the information was no longer complete.
Finding these people was eventually made possible with the assistance of the Association of German Pension Insurance Carriers, through which addresses for nearly 150,000 people were collected to communicate the offer of free occupational medical care.
To give the examining doctor an impression of the hazards and exposure that the patient was subject to from the so-called occupational or work case history a job-exposure matrix was constructed.
Occupational Medical Care
Approximately 125 specially trained occupational physicians with experience in diagnosing dust- and radiation-caused diseases were recruited for the examinations. They work under the direction of ZeBWis and are spread throughout the Federal Republic to ensure that the affected individuals can obtain the indicated examination near their current place of residence. Due to intensive training of the participating physicians, standard high-quality examinations are performed at all examination locations. By distributing uniform documentation forms ahead of time, it is ensured that all relevant information is collected according to set standards and is entered into ZeBWis’s data centres. By optimizing the number of files, every examining doctor carries out an adequate number of exams every year and thereby remains practised and experienced in the examination programme. Through regular exchange of information and continuing education, the physicians always have access to current information. All examining physicians are experienced in assessing chest x rays in accordance with the 1980 ILO guidelines (International Labour Organization 1980).
The data pool, which is growing as a result of the ongoing examinations, is geared to acquaint physicians and risk assessment experts in the occupational disease detection programme with relevant preliminary findings. It furthermore provides a basis for addressing specific symptoms or diseases that appear under defined risk situations.
The Future
Comparing the number of people who worked for Wismut underground and/or in preparation plants with the number who were employed in uranium mining in the Western world, it is evident that, even with big gaps, the data on hand present an extraordinary basis for gaining new scientific understanding. Whereas the 1994 overview by Lubin et al. (1994) on the risk of lung cancer covered approximately 60,000 affected individuals and about 2,700 cases of lung cancer in 11 studies, the data from some 300,000 former Wismut employees are now available. At least 6,500 have died to date from radiation-caused lung cancer. Furthermore, Wismut never collected the exposure information on a great number of persons exposed either to ionizing radiation or other agents.
As precise information as possible on exposure is necessary for optimal occupational disease diagnosis as well as for scientific research. This is taken into account in two research projects that are being sponsored or carried out by the Berufsgenossenschaften. A job-exposure matrix was prepared by consolidating available site measurements, analysing geological data, using information on production figures and, in some cases, reconstructing working conditions in the early years of Wismut. Data of this type are a prerequisite for developing a better understanding, through cohort studies or case-control studies, of the nature and extent of illnesses that result from uranium mining. Understanding the effect of long-term, low-level radiation doses and the cumulative effects of radiation, dust and other carcinogenic materials might also be improved in this manner. Studies of this are now beginning or are being planned. With the help of biological specimens that were collected in Wismut’s former pathology laboratories, scientific knowledge can also be obtained about the type of lung cancer and also about the interactive effects between silicogenic dusts and radiation, as well as other carcinogenic hazardous materials that are inhaled or ingested. Such plans are being pursued at this time by the DKFZ. Collaboration on this issue is now underway between the German research facilities and other research groups such as the US NIOSH and the National Cancer Institute (NCI). Corresponding work groups in countries like the Czech Republic, France and Canada are also cooperating in studying the exposure data.
To what extent malignancies other than lung cancer may develop from radiation exposure during uranium ore mining is poorly understood. At the request of the trade associations, a model of this was developed (Jacobi and Roth 1995) to establish under what conditions cancers of the mouth and throat, liver, kidneys, skin or bones can be caused by working conditions such as those at Wismut.
Case Study: Worker Protection and Statistics on Accidents and Occupational Diseases - HVBG, Germany
The German Berufsgenossenschaften (BG)
Under the social insurance system in Germany, statutory accident insurance covers the results of accidents at work and accidents on the way to and from work, as well as occupational diseases. This statutory accident insurance is organized into three areas:
- industrial accident insurance (represented by the BGs)
- agricultural accident insurance
- public sector’s own accident insurance scheme.
The 35 Berufsgenossenschaften (BG) cover the various branches of the industrial economy in Germany. They are responsible for 39 million employees insured in 2.6 million enterprises. Every person in a work, service or training position is insured, regardless of age, sex or income level. Their umbrella organization is the Central Federation of the Berufsgenossenschaften (HVBG).
By law, the BG is responsible for using all appropriate means to prevent workplace accidents and occupational diseases, to provide effective first aid and optimal medical, occupational and social rehabilitation, and to pay benefits to the injured and sick, and to survivors. Thus prevention, rehabilitation and compensation are all under one roof.
The premiums to finance these benefits are paid exclusively by the employers. In 1993 all industrial employers paid on average DM 1.44 to the BG for every DM 100 wages, or 1.44%. In all, the premiums came to DM 16 billion (US billion used—one thousand million), of which about 80% was spent for rehabilitation and pensions. The remainder was used primarily for prevention programmes.
Occupational Safety and Health Protection
The employer is responsible for the health and safety of the employee at work. The legal scope of this responsibility is set by government in laws and ordinances, and in the protective labour regulations of the industrial BGs, which complete and concretize governmental protective labour law for each branch of industry. The system of prevention of the BGs is notable for its orientation to actual practice, its constant adaptation to the needs of the industry and to the state of technology, as well as for its effective support of the employer and the employee.
The BGs’ tasks of prevention, which are primarily carried out by the Technical Inspection Service (TAD) of the BG and the Occupational Medical Service (AMD), include:
- advising and motivating the employer
- supervising industrial occupational protective measures
- occupational medical care
- informing and training company staff
- safety checking on appliances and equipment
- initiating, carrying out and financing research.
Responsibility for implementing industrial occupational protection lies with the employer, who is legally obliged to hire appropriately qualified personnel to assist in occupational protection. These are specialists in work safety (safety officers, safety technicians and safety engineers) and company doctors. In companies with more than 20 employees, one or more safety representatives must be hired. The scope of the responsibility of the company for occupational safety specialists and company doctors is set by trade association regulations that are specific to the branch of industry and degree of hazard. In companies where an occupational safety specialist or a company doctor is employed, the employer must organize an occupational safety committee, made up of one company representative, two workers’ representatives, the company doctor, and occupational safety specialists and safety representatives. First-aid personnel, whose training is directed by the BG, also belong to the company occupational safety organization.
Occupational medical care has a special significance. Every employee who is at risk for a specific type of health threat at the workplace is examined in a uniform manner, and the results of the examination are assessed according to stated guidelines. In 1993 approximately four million occupational preventive medical examinations were carried out by specially authorized doctors. Lasting health concerns were ascertained in less than 1% of the examinations.
Employees who work with hazardous/carcinogenic materials also have a right to be medically examined even after the hazardous activity has been completed. The BGs have established services to be able to examine these employees. There are now three such services:
- Organizational Service for On-going Examinations (ODIN)
- Central Registration Service for Asbestos Dust-Endangered Employees (ZAs)
- Wismut Central Care Office (ZeBWis).
The three services cared for approximately 600,000 people in 1993. Collecting examination data assists in individual care and also helps improve scientific research for early detection of cancer cases.
Statistics on Workplace Accidents
Goal. The primary goal of collecting statistics on workplace accidents is to improve workplace safety by assessing and interpreting data on accident occurrences. These data are compiled from reports on workplace accidents; 5% to 10% of the accidents (approximately 100,000 accidents) are investigated each year by the Technical Inspection Services of the BGs.
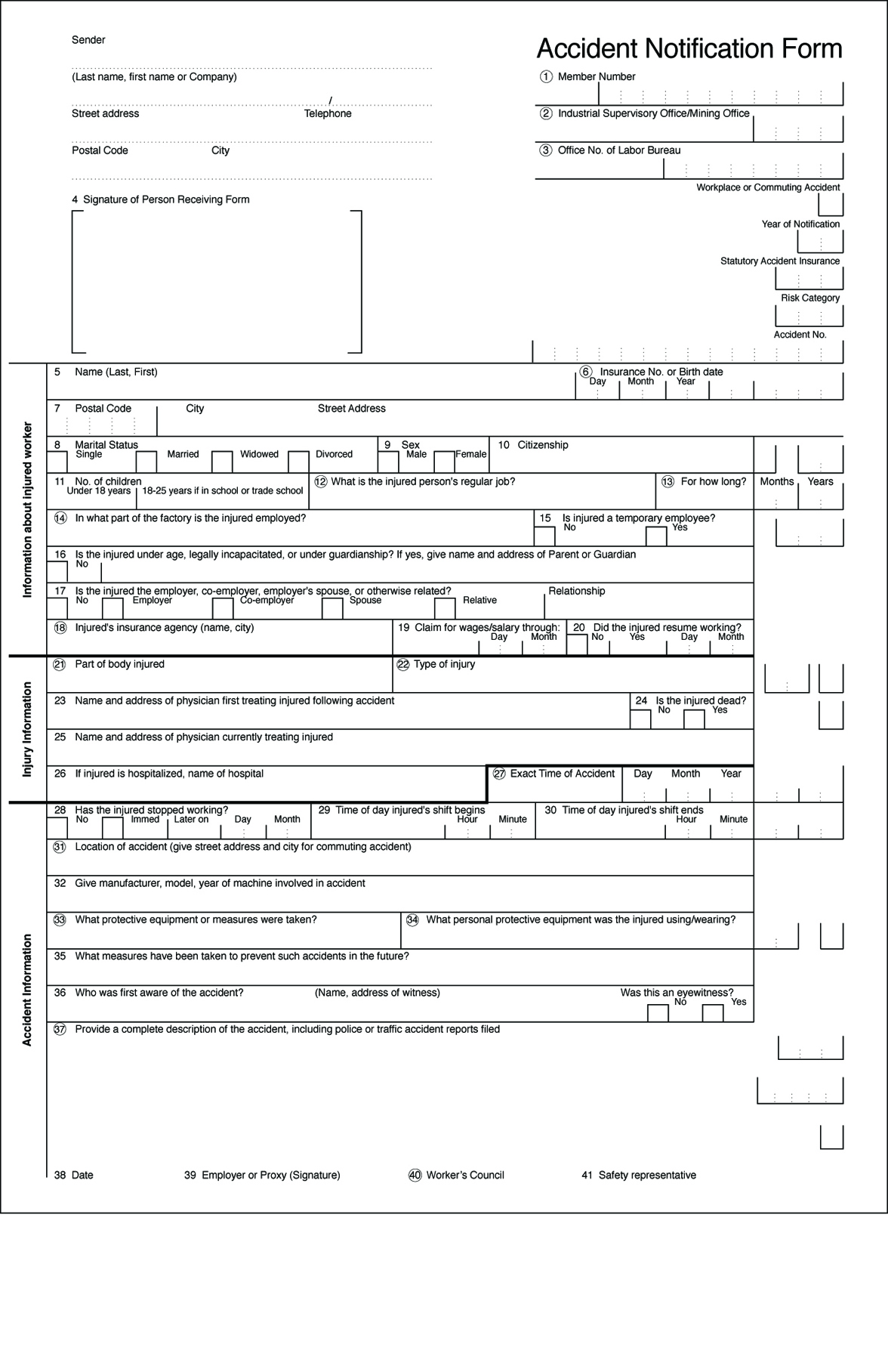
Employers’ reporting responsibility. Every employer is obliged to report a workplace accident to his responsible BG within three days if the accident results in an incapacity to work for three calendar days or causes the death of the insured (“legally reportable workplace accident”). This includes accidents going to or from work. Accidents that cause only property damage or prevent the injured person from working for less than three days do not have to be reported. For reportable workplace accidents, a form “Accident Notification” (figure 1) is submitted by the employer. The time away from work is the significant factor for reporting purposes, regardless of the seriousness of the injury. Accidents that appear harmless must be reported if the injured person cannot work for longer than three days. This three-day requirement facilitates pursuing later claims. Failure to file an accident report, or filing one late, constitutes a violation of regulations that can be punished by the BG with a monetary fine of up to DM 5,000.
Figure 1. An example of an accident notification form
Notification by the attending physician. To optimize medical rehabilitation and to determine how long the employee is unable to work, the injured person receives treatment from a medical specialist selected for this work. The doctor is paid by the responsible industrial BG. Thus, the BG also receives notification of reportable workplace injuries from the doctor if the employer has failed to (promptly) file an accident report. The BG can then request the employer to file a workplace accident notification. This dual reporting system (employer and doctor) assures the BG of receiving knowledge of practically all reportable workplace accidents.
Using the information on the accident notification report and the medical report, the BG checks whether the accident is, in the legal sense, a workplace accident within its jurisdictional competence. On the basis of the medical diagnosis, the BG can, if needed, proceed immediately to ensuring optimal treatment.
A correct and complete description of the circumstances of the accident is especially important for prevention. This enables the BG’s Technical Inspection Service to draw conclusions about defective machinery and equipment that require immediate action to avoid further similar accidents. In the case of serious or fatal workplace accidents, regulations require the employer to immediately notify the BG. These occurrences are immediately investigated by the BG’s occupational safety experts.
In calculating a company’s premium, the BG takes into account the number and cost of workplace accidents that have taken place at this company. A bonus/malus procedure set by law is used in the calculation, and a portion of the company’s premium is determined by the company’s accident trend. This can lead to a higher or lower premium, thus creating financial incentives for employers to maintain safe workplaces.
Collaboration of the employees’ representatives and the safety representatives. Any accident report must also be signed by the workers’ council (Betriebsrat) and by the safety representatives (if these exist). The purpose of this rule is to inform the workers’ council and the safety representatives of the company’s overall accident situation, so that they can effectively exercise their collaborative rights in questions of workplace safety.
Compiling workplace accident statistics. On the basis of the information that the BG receives on a workplace accident from the accident report and the doctor’s report, the accounts are translated into statistical code numbers. The coding covers three areas, among others:
- description of the injured (age, sex, job)
- description of the injury (location of injury, type of injury)
- description of the accident (location, object causing the accident and circumstances of the accident).
Coding is performed by highly trained data specialists who are familiar with the organization of BG industries, utilizing a list of accident and injury codes which contains over 10,000 entries. In order to achieve the highest quality statistics, the classifications are regularly reworked, in order, for example, to adapt them to new technological developments. Furthermore, coding personnel are periodically retrained, and the data are subject to formal-logical and content-sensitive tests.
Uses of workplace accident statistics
An important task of these statistics is to describe the circumstances of the accident at the workplace. Table 1 portrays trends in reportable workplace accidents, new accident pension cases and fatal workplace accidents between 1981 and 1993. Column 3 (“New pension cases”) shows cases for which, because of the seriousness of the accident, a pension payment was first made by the industrial BGs in the given year.
Table 1. Occurrences of workplace accidents, Germany, 1981-93
|
Year |
Workplace accidents |
||
|
Reportable accidents |
New pension cases |
Deaths |
|
|
1981 |
1,397,976 |
40,056 |
1,689 |
|
1982 |
1,228,317 |
39,478 |
1,492 |
|
1983 |
1,144,814 |
35,119 |
1,406 |
|
1984 |
1,153,321 |
34,749 |
1,319 |
|
1985 |
1,166,468 |
34,431 |
1,204 |
|
1986 |
1,212,064 |
33,737 |
1,069 |
|
1987 |
1,211,517 |
32,537 |
1,057 |
|
1988 |
1,234,634 |
32,256 |
1,130 |
|
1989 |
1,262,374 |
30,840 |
1,098 |
|
1990 |
1,331,395 |
30,142 |
1,086 |
|
1991 |
1,587,177 |
30,612 |
1,062 |
|
1992 |
1,622,732 |
32,932 |
1,310 |
|
1993 |
1,510,745 |
35,553 |
1,414 |
Source: Central Federation of Berufsgenossenschaften (HVBG), Germany.
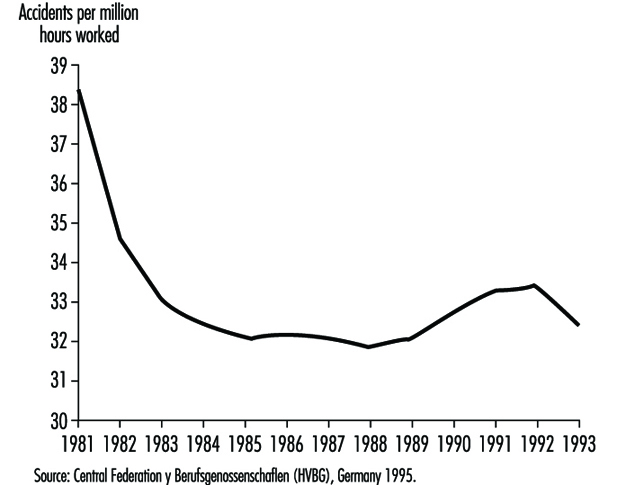
To judge the average accident risk of an insured, the number of workplace accidents is divided by the actual time worked, to produce an accident rate. The rate per one million hours worked is used for comparison internationally and across years. Figure 2 shows how this rate varied between 1981 and 1993.
Figure 2. Frequency of workplace accidents
Industry-specific accident statistics. In addition to describing general trends, workplace statistics can be broken down by industry. For example, one might ask, “How many workplace accidents with portable grinders in the metalworking trade were there in the last few years; how and where did they take place; and what injuries resulted?” Such analyses may be useful to many people and institutions, such as government ministries, supervisory officials, research institutes, universities, businesses and workplace safety experts (table 2).
Table 2. Workplace accidents with portable grinders in metalworking, Germany, 1984-93
|
Year |
Reportable accidents |
New accident pensions |
|
1984 |
9,709 |
79 |
|
1985 |
10,560 |
62 |
|
1986 |
11,505 |
76 |
|
1987 |
11,852 |
75 |
|
1988 |
12,436 |
79 |
|
1989 |
12,895 |
76 |
|
1990 |
12,971 |
78 |
|
1991 |
19,511 |
70 |
|
1992 |
17,180 |
54 |
|
1993 |
17,890 |
70 |
Source: Central Federation of Berufsgenossenschaften (HVBG), Germany.
For example, table 2 shows that reportable workplace accidents with portable grinders in metalworking rose continuously from the middle of the 1980s to 1990. From 1990 to 1991 a considerable increase in the accident figures is to be noted. This is an artefact resulting from the inclusion, beginning in 1991, of figures encompassing the new borders of reunited Germany. (The earlier figures cover only the Federal Republic of Germany.)
Other data compiled from accident reports reveal that not all accidents with metalworking portable grinders take place primarily in companies in the metalworking industry. Portable grinders, which of course are often used as angle grinders to cut pipes, iron bars and other objects, are frequently employed on construction sites. Accordingly, nearly one-third of the accidents are concentrated in companies in the construction industry. Working with portable grinders in metalworking results mainly in head and hand injuries. The most common head injuries affect the eyes and the area surrounding the eyes, which are injured by broken pieces, splinters and flying sparks. The tool has a fast-spinning grinding wheel, and hand injuries result when the person using the portable machine loses control of it. The high number of eye injuries proves that the importance and obligation of wearing safety glasses while grinding metal with this portable machine must be emphasized within companies.
Comparison of accident rates within and between industries. Although in 1993 there were nearly 18,000 workplace accidents with portable grinders in metalworking, compared to only 2,800 workplace accidents with hand-held power saws in woodworking, one cannot automatically conclude that this machinery poses a greater risk to metalworkers. To assess accident risk for specific industries, the number of accidents must first be related to a measure of exposure to danger, such as hours worked (see “Risk analysis of nonfatal workplace injuries and illnesses” [REC05AE]). However, this information is not always available. Therefore, a surrogate rate is derived as the proportion which serious accidents make of all reportable accidents. Comparing the serious-injury proportions for portable grinders in metalworking and portable circular saws in woodworking demonstrates that portable circular saws have an accident seriousness rate ten times higher than portable grinders. For prioritizing workplace safety measures, this is an important finding. This type of comparative risk analysis is an important component of an overall industrial accident prevention strategy.
Occupational Disease Statistics
Definition and reporting
In Germany an occupational disease is legally defined as a disease whose cause can be traced to the occupational activity of the affected person. An official list of occupational diseases exists. Therefore, assessing whether a sickness constitutes an occupational disease is both a medical and legal question and is referred by public law to the BG. If an occupational disease is suspected, it is not sufficient to prove that the employee suffers from, for example, an eczema. Additional knowledge is required about substances used at work and their potential for harming the skin.
Compiling occupational disease statistics. Because the BGs are responsible for compensating workers with occupational diseases as well as for providing rehabilitation and prevention, they have a considerable interest in application of statistics derived from occupational disease reports. These applications include targeting preventive measures on the basis of identified high-risk industries and occupations, and also providing their findings to the public, the scientific community and political authorities.
To support these activities, the BGs introduced in 1975 a set of occupational disease statistics, which contain data on every occupational disease report and its final determination—whether recognized or denied—including the reasons for the decision at the level of the individual case. This data base contains anonymous data on:
- the person, such as sex, year of birth, nationality
- diagnosis
- hazardous exposures
- the legal decision, including outcome of claim, determination of disability and any further actions taken by the BGs.
Results of the occupational disease statistics. An important function of the occupational disease statistics is to track the occurrence of occupational diseases over time. Table 3 charts the notifications of suspected occupational disease, the number of recognized occupational disease cases overall and the payment of pensions, as well as the number of fatal cases between 1980 and 1993. It should be cautioned that these data are not easy to interpret, since definitions and criteria differ widely. Furthermore, during this time period the number of officially designated occupational diseases rose from 55 to 64. Also, the figures from 1991 encompass the new borders of reunited Germany, whereas the earlier ones cover the Federal Republic of Germany alone.
Table 3. Occurrences of occupational disease, Germany, 1980-93
|
Year |
Notifications |
Recognized occupational disease cases |
Of those with |
Occupational disease fatalities |
|
1980 |
40,866 |
12,046 |
5,613 |
1,932 |
|
1981 |
38,303 |
12,187 |
5,460 |
1,788 |
|
1982 |
33,137 |
11,522 |
4,951 |
1,783 |
|
1983 |
30,716 |
9,934 |
4,229 |
1,557 |
|
1984 |
31,235 |
8,195 |
3,805 |
1,558 |
|
1985 |
32,844 |
6,869 |
3,439 |
1,299 |
|
1986 |
39,706 |
7,317 |
3,317 |
1,548 |
|
1987 |
42,625 |
7,275 |
3,321 |
1,455 |
|
1988 |
46,280 |
7,367 |
3,660 |
1,363 |
|
1989 |
48,975 |
9,051 |
3,941 |
1,281 |
|
1990 |
51,105 |
9,363 |
4,008 |
1,391 |
|
1991 |
61,156 |
10,479 |
4,570 |
1,317 |
|
1992 |
73,568 |
12,227 |
5,201 |
1,570 |
|
1993 |
92,058 |
17,833 |
5,668 |
2,040 |
Source: Central Federation of Berufsgenossenschaften (HVBG), Germany.
Example: infectious diseases. Table 4 shows the decline in the number of recognized cases of infectious diseases during the period 1980 to 1993. It specifically singles out viral hepatitis, for which one can clearly see that a strongly declining trend developed from approximately the mid-1980s in Germany, when employees at risk in the health service were given preventive inoculations. Thus occupational disease statistics can serve not only to find high rates of illnesses, but can also document the successes of protective measures. Declines in disease rates may of course have other explanations. In Germany, for example, the reduction in the number of cases of silicosis during the past two decades is chiefly a result of the decline in the number of jobs in mining.
Table 4. Infectious diseases recognized as occupational diseases, Germany, 1980-93
|
Year |
Total recognized cases |
Of those: hepatitis viral |
|
1980 |
1173 |
857 |
|
1981 |
883 |
736 |
|
1982 |
786 |
663 |
|
1983 |
891 |
717 |
|
1984 |
678 |
519 |
|
1985 |
417 |
320 |
|
1986 |
376 |
281 |
|
1987 |
224 |
152 |
|
1988 |
319 |
173 |
|
1989 |
303 |
185 |
|
1990 |
269 |
126 |
|
1991 |
224 |
121 |
|
1992 |
282 |
128 |
|
1993 |
319 |
149 |
Source: Central Federation of Berufsgenossenschaften (HVBG), Germany.
Sources of Information
The HVBG, as umbrella organization for the BGs, centralizes the common statistics and produces analyses and brochures. Furthermore, the HVBG sees statistical information as an aspect of the overall information that must be available to carry out the broad range of mandated responsibilities of the accident insurance system. For this reason, the Central Information System of the BGs (ZIGUV) was formed in 1978. It prepares relevant literature and makes it available to the BGs.
Workplace safety as an interdisciplinary, comprehensive approach requires optimum access to information. The BGs in Germany have resolutely taken this path and thereby made a considerable contribution to the efficient workplace safety system in Germany.
Risk Analysis of Nonfatal Workplace Injuries and Illnesses
The United States Bureau of Labor Statistics routinely classifies nonfatal workplace injuries and illnesses by worker and case characteristics, using data from the US Survey of Occupational Injuries and Illnesses. While these counts identify groups of workers who experience large numbers of workplace injuries, they do not measure risk. Thus a particular group may sustain many workplace injuries simply because of the large number of workers in that group, and not because the jobs performed are especially hazardous.
In order to quantify actual risk, data on workplace injuries must be related to a measure of exposure to risk, such as number of hours worked, a labour supply measure which may be available from other surveys. The rate of nonfatal workplace injuries for a group of workers may be calculated by dividing the number of injuries recorded for that group by the number of hours worked during the same time period. The rate obtained this way represents the risk of injury per hour of work:
![]()
A convenient way of comparing the risk of injury among various groups of workers is to compute the relative risk:
![]()
The reference group may be a special group of workers, such as all managerial and professional specialty workers. Alternatively, it might consist of all workers. In any case, the relative risk (RR) corresponds to the rate ratio commonly used in epidemiological studies (Rothman 1986). It is algebraically equivalent to the percentage of all injuries which occur to the special group divided by the percentage of hours accounted for by the special group. When the RR is greater than 1.0, it indicates that members of the selected group are more likely to sustain injuries than members of the reference group; when the RR is less than 1.0, it indicates that, on the average, members of this group experience fewer injuries per hour.
The following tables show how indexes of relative risk for different groups of workers can identify those at greatest risk of workplace injury. The injury data are from the 1993 Survey of Occupational Injuries and Illnesses (BLS 1993b) and measure the number of injuries and illnesses with days away from work. The calculation relies upon estimates of annual hours worked taken from the microdata files of the US Bureau of the Census Current Population Surveys for 1993, which is obtained from household surveys (Bureau of the Census 1993).
Table 1 presents data by occupation on the share of workplace injuries, the share of hours worked and their ratio, which is the RR for injuries and illnesses with days away from work. The reference group is taken to be “All nonfarm private industry occupations” with workers of age 15 and older, which comprises 100%. As an example, the group “Operators, fabricators and labourers” experienced 41.64% of all injuries and illnesses, but contributed only 18.37% of the total hours worked by the reference population. Therefore, the RR for “Operators, fabricators and labourers” is 41.64/18.37 = 2.3. In other words, workers in this group of occupations have on average 2.3 times the injury/illness rate of all nonfarm private industry workers combined. Furthermore, they are about 11 times as likely to sustain a serious injury as employees in a managerial or professional specialty.
Table 1. Risk of occupational injuries and illnesses
|
Occupation |
Percentage1 |
Index |
|
|
Injury and illness cases |
Hours worked |
||
|
All nonfarm private industry occupations |
100.00 |
100.00 |
1.0 |
|
Managerial and professional specialty |
5.59 |
24.27 |
0.2 |
|
Executive, administrative and managerial |
2.48 |
13.64 |
0.2 |
|
Professional specialty |
3.12 |
10.62 |
0.3 |
|
Technical, sales and administrative support |
15.58 |
32.19 |
0.5 |
|
Technicians and related support |
2.72 |
3.84 |
0.7 |
|
Sales occupations |
5.98 |
13.10 |
0.5 |
|
Administrative support, including clerical |
6.87 |
15.24 |
0.5 |
|
Service occupations2 |
18.73 |
11.22 |
1.7 |
|
Protective service3 |
0.76 |
0.76 |
1.0 |
|
Service occupations, except protective service |
17.97 |
10.46 |
1.7 |
|
Farming, forestry and fishing occupations4 |
1.90 |
0.92 |
2.1 |
|
Precision production, craft and repair |
16.55 |
13.03 |
1.3 |
|
Mechanics and repairers |
6.30 |
4.54 |
1.4 |
|
Construction trades |
6.00 |
4.05 |
1.5 |
|
Extractive occupations |
0.32 |
0.20 |
1.6 |
|
Precision production occupations |
3.93 |
4.24 |
0.9 |
|
Operators, fabricators and labourers |
41.64 |
18.37 |
2.3 |
|
Machine operators, assemblers and inspectors |
15.32 |
8.62 |
1.8 |
|
Transportation and material moving occupations |
9.90 |
5.16 |
1.9 |
|
Handlers, equipment cleaners, helpers and laborers |
16.42 |
4.59 |
3.6 |
1 Percentage of injuries and illnesses, hours worked and index of relative risk for occupational injuries and illnesses with days away from work, by occupation, US nonfarm private industry employees 15 years and over, 1993.
2 Excludes private household workers and protective service workers in the public sector
3 Excludes protective service workers in the public sector
4 Excludes workers in agricultural production industries
Sources: BLS Survey of Occupational Injuries and Illnesses, 1993; Current Population Survey, 1993.
The various occupational groups may be ranked according to degree of risk simply by comparing their RR indices. The highest RR in the table (3.6) is associated with “handlers, equipment cleaners, helpers and labourers”, while the group at lowest risk is managerial and professional specialty workers (RR = 0.2). More refined interpretations may be made. While the table suggests that workers with lower levels of skills are in jobs with higher risks of injury and illness, even among blue-collar occupations the injury and illness rate is higher for less-skilled operators, fabricators and labourers compared to precision production, craft and repair workers.
In the above discussion, the RRs have been based upon all injuries and illnesses with days away from work, since these data have long been readily available and understood. Using the extensive and newly developed coding structure of the Survey of Occupational Injuries and Illnesses, researchers may now examine specific injuries and illnesses in detail.
As an example, table 2 shows the RR for the same set of occupation groupings, but restricted to the single outcome “Repetitive Motion Conditions” (event code 23) with days away from work, by occupation and gender. Repetitive motion conditions include carpal tunnel syndrome, tendonitis and certain strains and sprains. The group most severely affected by this type of injury is quite clearly female machine operators, assemblers and inspectors (RR = 7.3), followed by female handlers, equipment cleaners, helpers and labourers (RR = 7.1).
Table 2. Index of relative risk for repetitive motion conditions with days away from work, by occupation and gender, US nonfarm private industry employees 15 years and over, 1993
|
Occupation |
All |
Men |
Women |
|
All nonfarm private industry occupations |
1.0 |
0.6 |
1.5 |
|
Managerial and professional specialty |
0.2 |
0.1 |
0.3 |
|
Executive, administrative and managerial |
0.2 |
0.0 |
0.3 |
|
Professional specialty |
0.2 |
0.1 |
0.3 |
|
Technical, sales and administrative support |
0.8 |
0.3 |
1.1 |
|
Technicians and related support |
0.6 |
0.3 |
0.8 |
|
Sales occupations |
0.3 |
0.1 |
0.6 |
|
Administrative support, including clerical |
1.2 |
0.7 |
1.4 |
|
Service occupations1 |
0.7 |
0.3 |
0.9 |
|
Protective service2 |
0.1 |
0.1 |
0.4 |
|
Service occupations, except protective service |
0.7 |
0.4 |
0.9 |
|
Farming, forestry and fishing occupations3 |
0.8 |
0.6 |
1.8 |
|
Precision production, craft and repair |
1.0 |
0.7 |
4.2 |
|
Mechanics and repairers |
0.7 |
0.6 |
2.4 |
|
Construction trades |
0.6 |
0.6 |
— |
|
Extractive occupations |
0.1 |
0.1 |
— |
|
Precision production occupations |
1.8 |
1.0 |
4.6 |
|
Operators, fabricators and laborers |
2.7 |
1.4 |
6.9 |
|
Machine operators, assemblers and inspectors |
4.1 |
2.3 |
7.3 |
|
Transportation and material moving occupations |
0.5 |
0.5 |
1.6 |
|
Handlers, equipment cleaners, helpers and laborers |
2.4 |
1.4 |
7.1 |
1 Excludes private household workers and protective service workers in the public sector
2 Excludes protective service workers in the public sector
3 Excludes workers in agricultural production industries
Note: Long dashes — indicate that data do not meet publication guidelines.
Source: Calculated from the BLS Survey of Occupational Injuries and Illnesses, 1993, and Current Population Survey, 1993.
The table shows striking differences in the risk of repetitive motion conditions that depend on the gender of the worker. Overall, a woman is 2.5 times as likely as a man to lose work due to repetitive motion illness (2.5 = 1.5/0.6). However, this difference does not simply reflect a difference in the occupations of men and women. Women are at higher risk in all of the major occupational groups, as well as the less aggregated occupational groupings reported in the table. Their risk relative to men is especially high in sales and blue-collar occupations. Women are six times as likely as men to lose work time from repetitive motion injuries in sales and in precision production, craft and repair occupations.
Musicians
The musician relies on the skilled use of the muscles, nerves and bones (neuromusculoskeletal system). Playing an instrument requires finely controlled repetitive motions and often entails working in unnatural postures for extended periods of practice and performance (figure 1). These demands on the body can result in specific types of health problems. In addition, adverse working conditions, such as excessive sound exposure levels, prolonged periods of performance without rest, and inadequate preparation for new and difficult repertoire or instruments may affect the health of musicians in all age groups and at all levels of performing ability. Recognition of these hazards, accurate diagnosis and early treatment will prevent occupational disabilities that may interfere with, interrupt or end careers.
Figure 1. Orchestra.

Neuromusculoskeletal Problems
Studies from the United States, Australia and Canada suggest that around 60% of musicians will face career-threatening injuries during their working lifetime. Clinical cross-sectional studies have examined the prevalence of muscle-tendon disorders, of peripheral nerve entrapment syndromes and motor control problems. These studies have revealed several common diagnoses, which include various overuse syndromes, including strain of the muscles and connective tissue which control the bending and extending motions in the wrist and fingers. These syndromes result from the repetitive forceful movement of the muscle-tendon units. Other common diagnoses relate to pain in body parts which are involved in prolonged strain from awkward and imbalanced postures while playing musical instruments. Playing the instruments in the groups described below involves putting pressure on the branches of the nerves in the wrist and forearm, the shoulders, arm and neck. Occupational cramp or muscle spasms (focal dystonia) are also common problems which often can affect performers at the pinnacle of their careers.
String instruments: Violin, viola, cello, bass, harp, classical guitar and electric guitar
Health problems in musicians who play string instruments often are caused by the manner in which the musician supports the instrument and the posture assumed while sitting or standing and playing. For example, most violinists and violists support their instruments between the left shoulder and chin. Often the musician’s left shoulder will be elevated and the left chin and jaw will bear down in order to allow the left hand to move over the fingerboard. Elevating a joint and bearing down at the same time leads to a state of static contraction which promotes neck and shoulder pain, temporomandibular joint disorders involving the nerves and muscles of the jaw, and thoracic outlet syndrome, which can include pain or numbness in the neck, shoulder and upper chest area. Prolonged static sitting postures, particularly while assuming a bent posture, promote pain in the large muscle groups which support posture. Static twisting rotation of the spine is often required to play the string bass, harp and classical guitar. Heavy electric guitars are usually supported by a strap over the left neck and shoulder, contributing to pressure on the nerves of the shoulder and upper arm (the brachial plexus) and thus to pain. These problems of posture and support contribute to the development of strain and pressure of the nerves and muscles of the wrist and fingers by promoting their faulty alignment. For example, the left wrist may be used for excessive repetitive bending motions which result in strain of the extensor muscles of the wrist and fingers and the development of carpal tunnel syndrome. Pressure on the nerves of the shoulder and arm (lower trunks of the brachial plexus) may contribute to problems with the elbow, such as a double crush syndrome and ulnar neuropathy.
Keyboard instruments: Piano, harpsichord, organ, synthesizers and electronic keyboards
Playing a keyboard instrument requires assuming a similar posture to that of typing. Often the forward and downward orientation of the head to look at the keys and hands and repetitive upward movement to look at the music causes pain in the nerves and muscles of the neck and back. The shoulders will often be rounded, combined with a forward head poking posture and a shallow breathing pattern. A condition known as thoracic outlet syndrome can develop from chronic compression of the nerves and blood vessels that pass between the muscles in the neck, shoulder and rib cage. In addition, a musician’s tendency to bend the wrists and curl the fingers while keeping the hand/finger joints flat places excessive strain on the wrist and finger muscles in the forearm. Additionally, the repeated use of the thumb kept in a position under the hand strains the thumb muscles which extend and binds the finger extensor muscles across the back of the hand. The high repetitive force needed to play large chords or octaves may strain the capsule of the wrist joint and result in ganglion formation. Prolonged co-contraction of the muscles that turn and move the arms up and down can lead to nerve entrapment syndromes. Muscle spasms and cramps (focal dystonia) are common among this group of instrumentalists, sometimes requiring long periods of neuromuscular retraining to correct movement patterns which can lead to these difficulties.
Wind and brass instruments: Flute, clarinet, oboe, saxophone, bassoon, trumpet, french horn, trombone, tuba and bagpipes
A musician who plays one of these instruments will vary his or her posture according to the need to control airflow since posture will control the area from which diaphragmatic and intercostal breath is drawn. Playing these instruments depends on the way the mouthpiece is held (the embouchure) which is controlled by the facial and pharyngeal muscles. The embouchure controls sound production of vibrating reeds or the mouthpiece. Posture also affects how the musician supports the instrument while sitting or standing and in operating the keys or valves of the instrument that govern the pitch of the note played by the fingers. For example, the traditional French open-holed flute requires sustained adduction and flexion (bending forward) of the left shoulder, sustained abduction (drawing away) of the right shoulder and rotation of the head and neck to the left in slight movement. The left wrist is often held in an extremely bent position while the hand is also extended in order to support the instrument by the curled left index finger and both thumbs, counter balanced by the right little finger. This promotes strain of the forearm muscles and the muscles which permit extension of the fingers and thumbs. The tendency to project the head and neck forward and use shallow breathing increases the chances of developing thoracic outlet syndrome.
Percussion instruments: Drums, timpani, cymbals, xylophone, marimba, tabla and taiko
The use of sticks, mallets and bare hands to strike various percussion instruments results in rapid pulling back of the wrists and fingers at impact. The impulse vibration caused by striking the instrument is transmitted up the hand and arm and contributes to repetitive strain injuries of the muscle-tendon units and the peripheral nerves. Biomechanical factors, such as the amount of force used, the repetitive nature of the playing and static load placed on the muscles can add to the injuries. Carpal tunnel syndrome and nodule formation in tendon sheaths are common in this group of musicians.
Hearing Loss
The risk of hearing loss from music exposure depends on the intensity and duration of exposure. It is not uncommon to have exposure levels of 100 dB during a quiet passage of orchestral music, with peak values of 126 dB measured at the shoulder of an instrumentalist in the middle of the orchestra. At the position of the conductor or teacher, levels of 110 dB in an orchestra or band are common. Exposure levels for pop/rock and jazz musicians may be significantly higher, depending on the physical acoustics of the stage or pit, amplification system and placement of speakers or other instruments. The average duration of exposure may be approximately 40 hours per week, but many professional musicians will perform 60 to 80 hours per week on occasion. Hearing loss among musicians is far more common than expected, with approximately 89% of professional musicians who were found to have suffered musculoskeletal injuries also showing an abnormal hearing test result, with a hearing loss in the 3 to 6 KHz region.
Personal ear protection can be used but it must be adapted for each instrument type (Chasin and Chong 1992). By inserting an acoustic attenuator or filter into custom-moulded earplugs, the intensity of higher frequency sounds transmitted by ordinary earplugs is reduced to a flat attenuation as measured at the eardrum, which should be less damaging to the ear. The use of a tuned or adjustable vent in a custom earplug will allow the lower frequencies and some harmonic energy to pass through the earplug unattenuated. Earplugs can be designed to provide a slight amplification to alter perception of the singer’s voice, thus allowing the artist to reduce the risk of vocal strain. Depending on the psycho-acoustical nature of the instrument and surrounding music exposures, substantial reduction in risk for the development of hearing loss can be obtained. Improvement in the perception of the relative intensity of the musician’s own performance may reduce the risk of repetitive strain injuries by a relative reduction of the force of repetitive movements.
There are practical strategies for reducing the exposure of musicians that do not interfere with music production (Chasin and Chong 1995). Loudspeaker enclosures can be elevated above floor level, which results in minimal loss of low-frequency sound energy, while preserving sufficient loudness for the musician to perform at a lower intensity level. Musicians who play high-intensity, highly directional instruments such as trumpets and trombones should be on risers so that the sound passes above the other musicians, thereby lowering its impact. There should be 2 m of unobstructed floor space in front of the orchestra. Small stringed instruments should always have at least 2 m of unobstructed space above them.
History of Performing Arts Medicine
While interest in the physiology of music making dates back to antiquity, the first real summary of the occupational diseases of performing artists is Bernardino Ramazzini’s 1713 treatise Diseases of Workers. Sporadic interest in arts medicine continued through the eighteenth and nineteenth centuries. In 1932 the English translation of Kurt Singer’s Diseases of the Music Profession: A Systematic Presentation of Their Causes, Symptoms and Methods of Treatment appeared. This was the first textbook to bring together all the current knowledge on performing arts medicine. After World War II, the medical literature began to feature case reports of injured artists. The musical literature also began to carry short items and letters. There was a parallel growth of awareness among dancers.
One of the catalysts for the development of performing arts medicine as a cross-disciplinary field was the Danube Symposium on Neurology, held in Vienna in 1972. The conference focused on music and led to the publication of Music and the Brain: Studies in the Neurology of Music, by MacDonald Critchley and R.A. Henson. Also in 1972 the first Care of the Professional Voice Symposium was organized by the Voice Foundation. This has become an annual conference, with proceedings appearing in the Journal of Voice.
While injured performers and the health professionals serving them began to cooperate more closely, the general public was unaware of these developments. In 1981 a New York Times article described the hand problems suffered by pianists Gary Graffman and Leon Fleisher, and their treatment at Massachusetts General Hospital. These were virtually the first well-known musicians to admit to physical problems, so the publicity generated by their cases brought forth a large, previously unknown group of injured artists.
Since then, the field of performing arts medicine has advanced rapidly, with conferences, publications, clinics and associations. In 1983 the first Medical Problems of Musicians and Dancers symposium was held, in conjunction with the Aspen Music Festival, in Aspen, Colorado. This has become an annual conference and is perhaps the most important in the field. Meetings such as these usually include lectures by health professionals as well as demonstrations and master classes by artists.
In 1986 the journal Medical Problems of Performing Artists was launched. This is the only journal completely dedicated to arts medicine, and it publishes many of the Aspen symposium presentations. Related journals include the Journal of Voice, Kinesiology and Medicine for Dance, and the International Journal of Arts-Medicine. In 1991 the Textbook of Performing Arts Medicine, edited by Robert Sataloff, Alice Brandfonbrener and Richard Lederman, became the first modern, comprehensive text on the subject.
As publishing grew and conferences continued, clinics serving the performing arts community were organized. Generally these clinics are in large cities that support an orchestra or dance company, such as New York, San Francisco and Chicago. There are now more than twenty such centres in the United States and several in various other countries.
Those active in the field of performing arts medicine have also founded associations to further research and education. The Performing Arts Medicine Association, set up in 1989, now co-sponsors the Aspen symposiums. Other organizations include the International Association for Dance Medicine and Science, the International Arts-Medicine Association and the Association of Medical Advisors to British Orchestras.
Research in performing arts medicine has grown from case reports and prevalence studies to sophisticated projects using advanced technology. New treatments, more responsive to the artists’ specific needs, are being developed and the emphasis is beginning to shift to prevention and education.
Dancers
Dance involves patterned and rhythmic body movements, usually performed to music, that serve as a form of expression or communication. There are many different types of dances, including ceremonial, folk, ballroom, classical ballet, modern dance, jazz, flamenco, tap and so forth. Each of these has its unique movements and physical demands. Audiences associate dance with grace and enjoyment, yet very few people regard dance as one of the most demanding and strenuous athletic activities. Sixty-five to 80% of dance-related injuries are in the lower limbs, out of which about 50% are in the foot and ankle (Arheim 1986). Most of the injuries are due to over-use (about 70%) and the rest are of the acute type (ankle sprain, fractures and so on).
Dance medicine is a multidisciplinary profession because causes of injuries are multifactorial and hence treatment should be comprehensive and take into consideration the specific needs of dancers as artists. The goal of the treatment should be to prevent potentially dangerous specific stresses, allowing the dancer to keep active, acquiring and perfecting physical creativity and psychological well-being.
Training should preferably start at an early age in order to develop strength and flexibility. However, incorrect training results in injury to young dancers. Proper technique is the main concern, as incorrect posture and other bad dancing habits and methods will cause permanent deformities and over-use injuries (Hardaker 1987). One of the most basic movements is the turn-out—opening of the lower limbs outwards. This should take place in the hip joints; if it is forced more than the anatomic external rotation these joints will allow, compensations occur. The most common compensations are rolling-in of the feet, internal flexing of the knees and hyperlordosis of the lower back. These positions contribute to deformities such as hallux valgus (displacement of the great toe towards the other toes). Inflammations of tendons such as the flexor hallucis longus (the tendon for the great toe) and others may also result (Hamilton 1988; Sammarco 1982).
Being cognizant of individual anatomic differences in addition to the unusual biomechanical loads, such as in point position (standing on the tip of the toes), allows one to take actions to prevent some of these undesired outcomes (Teitz, Harrington and Wiley 1985).
The environment of dancers has great influence on their well-being. A proper floor should be resilient and absorb shock to prevent cumulative trauma to the feet, legs and spine (Seals 1987). Temperature and humidity also influence performance. Diet is a major issue as dancers are always under pressure to keep slim and look light and pleasing (Calabrese, Kirkendal and Floyd 1983). Psychological maladjustment may lead to anorexia or bulimia.
Psychological stress may contribute to some hormonal disturbances, which may present as amenorrhoea. The incidence of stress fractures and osteoporosis may increase in hormonally imbalanced dancers (Warren, Brooks-Gunn and Hamilton 1986). Emotional stress due to competition between peers, and direct pressure from choreographers, teachers and directors may enhance psychological problems (Schnitt and Schnitt 1987).
A good screening method for both students and professional dancers should detect psychological and physical risk factors and avoid problems.
Any change in activity levels (whether return from a holiday, sickness or pregnancy), intensity of work (rehearsals before a premiere tour), choreographer, style or technique, or environment (such as floors, stages or even type of dance shoes) makes the dancer more vulnerable.
Graphic Arts
The term graphic arts (also called graphic design, commercial art, visual design or visual communication) refers to the organization of ideas and concepts in a visual form that conveys a particular message to a target audience. Graphic designers work in a wide array of venues, including magazines, books, posters, packaging, film, video, exhibition design and, most recently, in digital forms such as computer screen design, multimedia presentations and pages on the World Wide Web. There are two types of visual communicators: graphic designers, who work with typography and page layout as well as photography and illustration; and illustrators, who work exclusively with visual images. Frequently the two roles overlap, but most commonly graphic designers hire illustrators to create visualizations of the ideas that will be used within a typographic context.
Graphic Design
The hazards of graphic design were very different in the late 1990s compared to only a few years earlier when some designers were still producing traditional mechanicals for offset printing (figure 1). Now, virtually all page layout and graphic design is produced in a digital format before it is printed on paper. Much graphic design is even created exclusively for a final digital form: a floppy disk, CD-ROM or a page on the Internet. Graphic designers use computers to create and store both text and images. These digitally created artworks are stored on floppy disks, removable storage cartridges or CD-ROMs, and then given to the client for the final presentation (package design, magazine, film titles, poster, business stationery or many other applications).
Figure 1. Hand lettering for graphic arts.

Graphic designers must now be concerned with the potential hazards of prolonged work at a computer. Unfortunately, this technology is too new to know all the associated hazards. At present the hazards identified from working for extended periods at a visual display unit (VDU) (also called a video display terminal, or VDT) include eyestrain, headaches, backaches, stiff necks, sore hands and wrists, dizziness, nausea, irritability and stress. There have also been reports of skin rashes and dermatitis associated with VDU use. While the health effects of VDU use have been studied for a couple of decades, there are no proven links between long-term use of VDUs and long-term health problems. VDUs do emit comparatively low-level radiation, but there are no hard data to support any permanent adverse health effects from VDU use.
Ergonomic computer workstations, elimination of glare and frequent work breaks enable graphic designers to work more safely than most other artistic professions. Generally the digital revolution has greatly reduced the health hazards previously associated with the graphic design profession.
Illustration
Illustrators create images in a wide variety of media and techniques for use in various commercial venues. For example, an illustrator may create work for magazines, book jackets, packaging, movie posters, advertising and many other forms of promotion and publicity. Generally illustrators are freelancers who are hired by art directors for a particular project, though some illustrators work for publishing houses and greeting card companies. Since illustrators generally create their own workspaces, the burden for creating a safe working environment usually falls upon the individual.
The materials used by professional illustrators are as varied as the techniques and styles exhibited in contemporary illustration. Therefore, it is imperative that each individual artist be aware of any hazards associated with his or her particular medium. Among the materials commonly used by illustrators are drawing and painting materials such as markers, water colours, oil paints, coloured inks, coloured pencils, dry pastels, oil pastels, dyes, acrylic paints and gouache.
Many commonly used colours contain hazardous ingredients such as xylene and petroleum distillates; pigments may contain such dangerous ingredients as mercury, cadmium, cobalt and lead. Precautions include working in a well-ventilated studio, wearing gloves and a respirator when using oil-based materials (particularly from aerosols) and substituting safer materials (water- and alcohol-based colours) when possible. Materials such as pastels can be hazardous when they become airborne dust; good ventilation is particularly important when using any material that can be breathed into the lungs. A final general precaution is to avoid eating, drinking or smoking while working with any toxic artists’ materials.
The wide assortment of materials used by illustrators requires an individual approach to safe working conditions, since each artist has a personal technique and selection of materials. Manufacturers in some countries are required by law to provide information about product ingredients and hazards. Each individual artist should carefully scrutinize every material used, working in the safest possible manner with the available media.
Adhesives
Adhesives used include rubber cement, spray mount, contact cement, electric waxers, dry-mount tissues, glue sticks, hot-melt glue guns, adhesive transfer materials, double-coated tape and water-soluble glues. Associated hazards include: dangerous chemicals such as n-hexane (a neurotoxin) in some rubber cements and contact cement; cyanoacrylate instant-action glues; airborne toxic chemicals and fire hazards associated with spray adhesives; and possible burns from hot-melt glue gun use. Many of the commonly used adhesives (rubber cement in particular) can also cause skin irritation.
Proper ventilation and use of gloves can prevent many of the hazards associated with common adhesives. Substitution of non-toxic adhesives whenever possible, such as electric waxers, adhesive transfer materials, dry-mount tissues, double-coated tapes, and water-soluble glues is recommended. Heptane-containing rubber cements and spray adhesives are less toxic than hexane types, although they are still flammable.
Solvents
Solvents include rubber cement thinner, turpentine, acetone, correction fluid and mineral spirits.
Hazards include skin irritation, headaches, damage to respiratory and nervous systems, kidney and liver damage, and flammability. Primary precautions include substituting safer solvents whenever possible (for example, mineral spirits are less toxic than turpentine) or switching to water-based pigments that do not require solvents for cleanup. Excellent ventilation or respiratory protection, careful storage, use of gloves and chemical splash goggles are also important when using any solvents.
Aerosol sprays
Aerosol sprays include fixative spray, spray markers, varnish, texture sprays and airbrush colours.
Hazards include respiratory problems, skin irritation, headaches, dizziness and nausea from toxic chemicals such as toluene and xylene; long-term adverse effects include damage to kidneys, liver and central nervous system. Sprays are also frequently flammable; care must be exercised to use them away from heat or flames. Precautions include using a respirator or adequate studio ventilation (such as a spray booth), and working with non-toxic pigments when using an airbrush.
Cutting tools
The various types of cutting tools can include paper cutters, razor knives and mat cutters. The hazards can range from cuts and, in the case of large paper cutters, the severing of fingers. Precautions include careful use of knives and cutters, keeping hands away from blades, and maintaining blades in sharp condition.
Jewellery
Jewellery manufacturing can include working with a variety of materials, such as precious and semi-precious stones, synthetic stones, shells, coral, pearls, precious metals, metal enamels and newer materials such as epoxy resins and vinyl polymers. These can be used to make rings, earrings, necklaces, pendants and a variety of other personal decorative items. Jewellery manufacturing shops vary in size, and different manufacturing processes may be adopted. Thus, health hazards may vary from one workshop to another.
Processes, Hazards and Precautions
Precious stones and settings
Much jewellery manufacturing involves the setting of precious stones into bases of precious metals or alloys of precious metals. Stones are initially cut into desired sizes, then polished. Base metals are cast, then ground and polished. Traditionally, the metal settings were made using “injection” mouldings. Alloys of low melting point, including alloys of cadmium and mercury, have also been used for metal casting. Recently, “lost wax” methods have been used to achieve a better quality of casting. Stones are held on metal bases using adhesives, soldering or mechanical clamping by parts of the metal frame. Metal bases are usually plated with precious metals.
Health hazards may result from exposure to metal fumes, wax fumes or dust of stones and metals, and visual impairment from poor lighting. Working with fine parts of jewellery items generally requires proper ventilation, adequate illumination and the use of magnifying lenses. In addition, proper ergonomic design in the workplace is recommended.
Stone cutting and polishing
Precious, semi-precious and synthetic stones (including diamond, jade, ruby, garnet, jasper, agate, travertine, opal, turquoise and amethyst) are usually cut to the desired size with small saws before setting. Injury hazards include abrasions and lacerations of the skin or eyes; other health hazards include dust inhalation (e.g., silicosis from quartz stones).
Precautions include proper ventilation, dust collectors, using magnifying lenses, local illumination, eye protection and ergonomic design of tools and working environments.
Lost wax metal casting
Rubber or silicon moulds are made from original moulds that are custom-made or designed by artists. Wax is subsequently injected into these moulds. Moulds (called investments) of plaster of Paris and/or silica are made to enclose these wax moulds. The whole investment is then heated in the kiln or oven to drain the wax out of the block, then filled with molten metal with the aid of centrifugation. The mould is shattered to recover the metal piece. This is polished, and also may be electroplated with a thin layer of precious metal.
Precious metals and their alloys, including gold, silver, platinum and copper as well as zinc and tin, are commonly used in constructing metal pieces. Injury hazards include fire or explosion from flammable gas used for melting metals, and burns from heated plaster casts or blocks, molten metal spillage, oxyacetylene torches or ovens; other health hazards include inhalation of metal fumes or dusts of silver, gold, zinc, lead, tin and so on.
Precautions include using alternative casting methods to lower the level of exposures and toxicity, proper local exhaust ventilation for metal dust and fumes, dust collectors, personal protective equipment including goggles, insulating gloves and working gowns, and proper storage of flammable gas.
Enamelling
Enamelling involves the fusion of pre-ground, powdered lead or borosilicate glass particles mixed with various coloured oxides onto a base metal to form an enamelled surface. Base metals can include silver, gold or copper. Common colourants include antimony, cadmium, cobalt, chromium, manganese, nickel and uranium.
Cleaning
The metal surface must first be cleaned with a torch or in a kiln to burn off oils and grease; it is then pickled with dilute nitric or sulphuric acid, or the safer sodium bisulphate, to remove firescale. Hazards include thermal and acid burns. Precautions include protective gloves, goggles and apron.
Application
Some enamellists grind and sift their enamels to obtain desired particle sizes. Application techniques include brushing, spraying, stencilling and sifting or wet packing of the enamel onto the metal surface. Inhalation of enamel powder or spray mist is the greatest hazard, particularly with lead-based enamels. Precautions include use of lead-free enamels and respiratory protection. In cloisonné, different enamel colours are separated by metal wires that have been soldered onto the metal. (See the discussion on silver soldering below). In champleve, designs are etched with ferric chloride or nitric acid, and depressed areas filled with enamels. Another technique involves applying enamels mixed with resin in turpentine. Ventilation and precautions to prevent skin contact are required.
Firing
The enamelled metal is then fired in a small kiln. Ventilation is required to remove toxic metal fumes, fluorides and decomposition products (from gums and other organic materials in the enamel). Other hazards include thermal burns and infrared radiation. Infrared goggles and heat-protective gloves are recommended.
The enamel piece can then be finished by such methods as filing the edges and grinding and sanding the enamelled surface. Standard precautions against dust inhalation and eye contact are needed.
Metal jewellery
Metal jewellery can be made by cutting, bending and otherwise fabricating metals, electroplating, anodizing, soldering, gluing, finishing and so on. Many of these processes are discussed in “Metalworking”. Some specific applications are discussed below.
Electroplating
Gold, silver, copper and strong acid as well as cyanide are used in the electroplating process. Injury hazards include electrical shock and burns from acid or alkali spillage; other health hazards include the inhalation of metal, acid and cyanide mist, organic solvents, as well as hydrogen cyanide gas.
Precautions include substitution of non-cyanide plating solutions, avoidance of mixing cyanide solution with acids, local exhaust ventilation, using a tank cover to reduce mist production, proper storage of chemicals, electrical precautions and adequate personal protective equipment.
Soldering or gluing
Soldering involves metals such as tin, lead, antimony, silver, cadmium, zinc and bismuth. Safety hazards include burns; other health hazards include the inhalation of metal fumes, including lead and cadmium (Baker et al. 1979), and fluoride and acid fluxes.
Using epoxy resin and quick-drying agents with solvents to bind stones and metal pieces is a common practice. Injury hazards from gluing include fire and explosion; other health hazards include the inhalation of solvents and skin contact with epoxy resin, other adhesives and solvents.
Precautions include avoidance of lead and cadmium solders, adequate local exhaust ventilation, proper storage of chemicals, adequate illumination and personal protective equipment.
Metal grinding and polishing
Rotating wheels and linear actuators of varied sizes are used for grinding, polishing and cutting. Injury hazards include skin abrasions; other health hazards include the inhalation of metal dusts, as well as repetitive motion, vibration, awkward position and forces.
Precautions include adequate local exhaust ventilation, dust collectors, goggles for eye protection and ergonomic designs for workplaces and tools.
Shells
Mother-of-pearl (from oyster shells) and coral, as well as abalone and other shells, can be made into jewellery by cutting, drilling, sawing, shaving, grinding, polishing, finishing and so on. Hazards include hand and eye injuries from flying particles and sharp edges, respiratory irritation and allergic reactions from inhalation of fine shell dust, and, in the case of mother-of-pearl, possible hypersensitivity pneumonia and ossification with inflammation of tissues covering the bones, especially in young people.
Precautions include cleaning shells thoroughly to remove organic matter, wet grinding and polishing techniques, and local exhaust ventilation or respiratory protection. Goggles should be worn to prevent eye injury.
Beads
Beads can be made from a variety of materials, including glass, plastic, seed, bone, shells, pearls, gemstones and so on. A newer material used for beads and other jewellery is heat-cured polyvinyl chloride (polymer clays). Hazards include inhalation of dust from drilling the holes for the string or wire used to hold the beads, and possible eye injuries. Precautions include wet drilling, ventilation or respiratory protection and goggles. The polymer clays can release hydrogen chloride, a respiratory irritant, if heated above recommended temperatures. Using cooking ovens for heat curing is not recommended. There has also been concern about plasticizers such as diethylhexyl phthalate, a possible carcinogen and reproductive toxin, present in these polymer clays.
More...
Woodworking
Woodworking is practised as an art form and utilitarian craft all over the world. It includes wood sculpture, furniture and cabinet making (figure 1), musical instrument making and so on. Techniques include carving (figure 2), laminating, joining, sawing, sanding, paint removing, painting and finishing. Woodworking uses a large number of different types of hard and soft woods, including many exotic tropical woods, plywood and composition boards, and sometimes woods treated with pesticides and wood preservatives.
Figure 1. Furniture making.

Figure 2. Carving wood with hand tools.
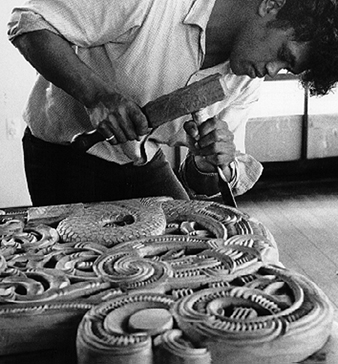
Hazards and Precautions
Woods
Many woods are hazardous, especially tropical hardwoods. Types of reactions can include skin allergies and irritation from the sap, wood dust or sometimes the wood, as well as conjunctivitis, respiratory allergies, hypersensitivity pneumonia and toxic reactions. Inhalation of hardwood dust is associated with a particular type of nasal and nasal sinus cancer (adenocarcinoma). See the chapter Woodworking industry.
Precautions include avoiding use of sensitizing woods for people who have a history of allergies, or for objects where people would be in frequent contact with the wood, and controlling dust levels by using local exhaust ventilation or wearing a toxic-dust respirator. When handling woods that can cause skin irritation or allergies, the artist should wear gloves or apply a barrier cream. Hands should be washed carefully after work.
Plywoods and composition board
Plywood and composition board (e.g., particle board) are made by gluing thin sheets of wood, or wood dust and chips, together with either urea-formaldehyde glues or phenol-formaldehyde glues. These materials can emit unreacted formaldehyde for some years after manufacture, with composition board emitting more formaldehyde. Heating these materials or machining them can cause decomposition of the glue to release formaldehyde. Formaldehyde is a skin, eye and respiratory irritant and strong sensitizer, and a probable human carcinogen.
Precautions include using low-formaldehyde products whenever possible, not storing large amounts of plywood or composition board in the shop, and using dust collectors connected to woodworking machines that are exhausted to the outside.
Wood preservatives and other treatments
Pesticides and preservatives are often applied to wood when it is being timbered, processed or shipped. Pentachlorophenol and its salts, creosote and chromated copper arsenate (CCA) have been banned for sale in the United States as wood preservatives because of possible carcinogenicity and reproductive hazards. They can, however, still be found in older woods, and chromated copper arsenate is still allowed as a commercial treatment (e.g., “green” lumber, playground equipment and other outdoor uses). A variety of other chemicals can be used in treating wood, including fire retardants and bleaches.
Precautions include not handling woods that have been treated with pentachlorophenol or creosote, using local exhaust ventilation when machining CCA-treated wood or wearing a respirator with high-efficiency filters. Wood that has been treated with creosote, pentachlorophenol or chromated copper arsenate should not be burned.
Carving and machining wood
Woods can be hand carved with chisels, rasps, hand saws, sandpaper and the like, or they can be machined with electric saws, sanders and other woodworking machines. Hazards include exposure to wood dusts, excessive noise levels from woodworking machines, accidents from using tools and machines, electrical shock or fire from faulty wiring, and wood fires. Vibrating tools—for example, chain saws—can cause “white fingers” (Raynaud’s phenomenon), involving numbness of the fingers and hands.
Precautions include equipping woodworking machines with dust collectors (figure 3) and machine guards, cleaning up sawdust to avoid fire hazards, wearing goggles (and sometimes face shields) and reducing noise. Using the appropriate machine for the desired operation, and repairing defective machines immediately; keeping hand tools sharpened, and using them safely; keeping all electrical equipment and wiring in good repair, and avoiding extension cords which can be tripped over; not wearing ties, long loose hair, loose sleeves or other items that could catch in machinery are some other precautions.
Figure 3. Woodworking machines with dust collector.

Michael McCann
Gluing wood
A variety of glues are used for laminating and joining wood, including contact adhesives, casein glue, epoxy glues, formaldehyde-resin glues, hide glues, white glue (polyvinyl acetate emulsion) and the cyanoacrylate “instant” glues. Many of these contain toxic solvents or other chemicals, and can be skin, eye and respiratory hazards.
Precautions include avoiding formaldehyde resin glues; using water-based glues rather then solvent-type glues; wearing gloves or barrier creams when using epoxy glues, solvent-based adhesives or formaldehyde-resin glues; and having good ventilation when using epoxy glues, cyanoacrylate glues and solvent-based glues. Sources of ignition should be avoided when using flammable solvents.
Painting and finishing
Wood can be painted with most types of paint; can be stained, lacquered or varnished; and can be treated with linseed or other types of oil. Other materials that are used in finishing wood include shellacs, polyurethane coatings and waxes. Many materials are sprayed. Some woodworkers mix their own paints from dry pigments. Hazards include inhalation of toxic pigment powder (especially lead chromate pigments), skin and inhalation hazards from solvents, fire hazards from flammable solvents, and spontaneous combustion from rags soaked with oil or turpentine.
Precautions include using ready-made paints rather than mixing your own; avoiding eating, drinking or smoking in the work area; using water-based paints rather than solvent-based ones; and placing oil- and solvent-soaked rags in self-closing oily-waste cans, or even a pail of water.
Precautions with solvents include wearing gloves and goggles, as well as having adequate ventilation; doing the operation outside; or wearing a respirator with organic vapour cartridges. Materials should be brushed on whenever possible, to avoid the hazards of spraying. Spraying finishes inside an explosion-proof spray booth, or wearing a respirator with organic vapour cartridges and spray filters; avoiding open flames, lit cigarettes and other sources of ignition (e.g., lit pilot lights) in the area when applying flammable finishes, or when spraying, are other precautions to be taken.
Paint stripping
Stripping old paint and varnish from wood and furniture is done with paint and varnish removers containing a wide variety of toxic and often flammable solvents. “Non-flammable” paint strippers contain methylene chloride. Caustic soda (sodium hydroxide), acids, blowtorches and heat guns are also used to remove old paint. Old stains on wood are often removed with bleaches, which can contain corrosive alkalis and oxalic acid, hydrogen peroxide or hypochlorite. Heat guns and torches can vaporize the paint, possibly causing lead poisoning with lead-based paint, and are a fire hazard.
See the previous section for precautions with solvent-based paint strippers. Gloves and goggles should be worn when handling caustic soda, oxalic acid bleaches or chlorine-type bleaches. An eyewash fountain and emergency shower should be available. Avoid using torches or heat guns to remove lead-containing paint.
Ceramics
Foodware, sculpture, decorative tiles, dolls and other ceramic or clay items are made in both large and small professional studios and shops, classrooms in public schools, universities and trade schools, and in homes as a hobby or cottage industry. The methods can be divided into ceramics and pottery, although terminology can vary in different countries. In ceramics, objects are made by slip casting—pouring a slurry of water, clay and other ingredients into a mould. The clay objects are removed from the mould, trimmed and fired in a kiln. Some ware (bisque ware) is sold after this stage. Other types are decorated with glazes that are mixtures of silica and other substances which form a glass surface. In pottery, objects are formed from plastic clay, usually by hand-forming or wheel-throwing, after which they are dried and fired in a kiln. Objects may then be glazed. Slip cast ceramics usually are glazed with china paints, which are commercially produced in dry or liquid pre-packaged form (figure 1). Potters may glaze their ware with these commercial glazes or with glazes they compound themselves. All types of ware are produced, from terra cotta and earthenware, which are fired at low temperatures, to stoneware and porcelain, which are fired at high temperatures.
Figure 1. Decorating a pot with China paints.

Clay and Glaze Materials
All clays and glazes are mixtures of silica, aluminium and metallic minerals. These ingredients usually contain significant amounts of respirable-sized particles such as those in silica flour and ball clays. Clay bodies and glazes are composed of essentially the same types of minerals (see table 1, but glazes are formulated to melt at lower temperatures (have more flux) than the bodies on which they are applied. Lead is a common flux. Raw lead minerals such as galena and lead oxides derived from burning car battery plates and other scrap are used as fluxes, and have poisoned potters and their families in some developing countries. Commercially sold glazes for industrial and hobby use are more likely to contain lead and other chemicals which have been mixed and pre-fired into powdered frits. Glazes are formulated to mature in either oxidation or reduction firing (see below) and may contain metal compounds as colourants. Lead, cadmium, barium and other metals may leach into food when glazed ceramic wares are used.
Table 1. Ingredients of ceramic bodies and glazes.
|
Basic constituents |
|
|
|
Clays (hydroaluminium silicates) |
Alumina |
Silica |
|
Kaolins and other white clays Red iron-rich clays Fire clays Ball clays Bentonite |
Aluminium oxide, corundum, usual source in glazes is from clays and feldspars |
Quartz from flint, sand, diatomaceous earth; cristobalite from calcined silica or fired silica minerals |
|
Other ingredients and some mineral sources |
||
|
Fluxes |
Opacifiers |
Colourants |
|
Sodium, potassium, lead, magnesium, lithium, barium, boron, calcium, strontium, bismuth |
Tin, zinc, antimony, zirconium, titanium, fluorine, cerium, arsenic |
Cobalt, copper, chrome, iron, manganese, cadmium, vanadium, nickel, uranium |
|
Sources include oxides and carbonates of metals above, feldspars, talc, nepheline syenite, borax, colemanite, whiting, lead frits, lead silicates |
Sources include oxides and carbonates of metals above, cryolite fluorspar, rutile, zirconium silicate |
Sources include oxides, carbonates and sulphates of metals above, chromates, spinels and other metal complexes |
Other special surface treatments include metallic lustre glazes containing tack oils and solvents such as chloroform, iridescent effects obtained by fuming metallic salts (usually chlorides of tin, iron, titanium or vanadium) onto surfaces during firing, and new paints containing plastic resins and solvents, which look like fired ceramic glazes when dry. Specially textured clay bodies may include fillers such as vermiculite, perlite and grog (ground fire brick).
Exposure to clay and glaze ingredients occurs during mixing, sanding and spray-applying glazes, and when grinding or chipping fired glaze imperfections from the bottoms of pottery or from kiln shelves (figure 2). Cleaning kiln shelves exposes workers to flint, kaolin and other kiln wash ingredients. Silica dust from fired kiln wash or bisque is more hazardous because it is in the cristobalite form. Hazards include: silicosis and other pneumoconioses from inhalation of minerals such as silica, kaolin, talc and fibrous amphibole asbestos in some talcs; toxicity from exposure to metals such as lead, barium and lithium; dermatitis from sensitizing metals such as chrome, nickel and cobalt; cumulative trauma disorders such as carpal tunnel syndrome (“potter’s thumb”) from wheel throwing; back injuries from digging clay, lifting 100-pound sacks of bulk minerals or from wedging (hand working clay to remove air bubbles); slips and falls on wet floors; shocks from electric pottery wheels and other equipment used in wet areas; allergies to moulds in clay; fungal and bacterial infections of nail beds and skin; and accidents with clay mixers, pug mills, blungers, slab rollers and the like.
Figure 2. Exposure to clay and glaze dusts while hand sanding a pot.
Henry Dunsmore
Precautions: outlaw open lead burning; use substitutes for raw lead, lead frits, cadmium and asbestos-containing materials; isolate work from family areas and children; practice housekeeping and hygiene; control dust; use local exhaust ventilation for glaze spraying and dusty processes (figure 3); use respiratory protection; work with adequate rest periods; lift safely; guard machines; and use ground fault interrupters on wheels and all other electrical equipment.
Figure 3. Local exhaust ventilation for clay mixing.

Michael McCann
Kiln Firing
Kilns vary from railroad-car size to a few cubic inches for firing test tiles and miniatures. They are heated with electricity or fuels such as gas, oil or wood. Electric kilns produce ware fired in primarily oxidizing atmospheres. Reduction firing is achieved by adjusting fuel/air ratios in fuel-fired kilns to create chemically reducing atmospheres. Firing methods include salt firing, raku (putting red-hot pots into organic matter such as damp hay to produce a smoky reduced clay body), climbing kilns (many-chambered wood or coal fired kilns built on hillsides), sawdust firing (kilns packed tight with pots and sawdust) and open-pit firing with many fuels including grass, wood and dung.
Primitive fuel-fired kilns are poorly insulated because they are usually made of fired clay, brick or mud. Such kilns can burn large amounts of wood and can contribute to fuel shortages in developing countries. Commercial kilns are insulated with refractory brick, castable refractory or ceramic fibre. Asbestos insulation is still found in older kilns. Refractory ceramic fibre is in very wide use in industry and hobby kilns. There are even small fibre kilns which are heated by putting them in home kitchen microwave ovens.
Kiln emissions include combustion products from fuels and from organic matter that contaminates clay and glaze minerals, sulphur oxides, fluorine and chlorine from minerals such as cryolite and sodalite, and metal fumes. Salt firing emits hydrochloric acid. Emissions are especially hazardous when fuels such as painted or treated wood and waste oils are burned. Hazards include: respiratory irritation or sensitization from aldehydes, sulphur oxides, halogens and other emissions; asphyxiation from carbon monoxide; cancer from inhalation of asbestos or ceramic fibre; eye damage from infrared radiation from glowing hot kilns; and thermal injury and burns.
Precautions: use clean-burning fuels; design fuel-efficient, well-insulated kilns; substitute refractory brick for asbestos or ceramic fibre; encapsulate or remove existing fibre insulation; locally vent indoor kilns; locate kilns in areas free of combustible materials; equip electric kilns with two automatic shut-offs; wear infrared-blocking goggles and gloves when handling hot objects.
Fibre and Textile Crafts
Contemporary fibre or textile artists use a wide range of processes, such as weaving, needlework, papermaking, leatherworking and so forth. These can be done by hand or aided by machines (see table 1). They may also use many processes for preparing fibres or finished textile, such as carding, spinning, dyeing, finishing and bleaching (see table 2). Finally the fibreworks or textiles may be painted, silk-screened, treated with photographic chemicals, scorched or otherwise modified. See separate articles in this chapter describing these techniques.
Table 1. Description of fibre and textile crafts.
|
Process |
Description |
|
Basketry |
Basketry is the making of baskets, bags, mats, etc., by hand weaving, plaiting and coiling techniques using materials such as reeds, cane and sisal fibre. Knives and scissors are often used, and coiled baskets are often sewed together. |
|
Batik |
Batik involves the creating of dye patterns on fabric by applying molten wax to the fabric with a djanting to form a resist, dyeing the fabric and removing the wax with solvents or by ironing between newsprint. |
|
Crocheting |
Crocheting is similar to knitting except that a hook is used to loop threads into the fabric. |
|
Embroidery |
The embellishment of a fabric, leather, paper or other materials by sewing of designs worked in thread with a needle. Quilting comes under this category. |
|
Knitting |
Knitting is the craft of forming a fabric by interlocking of yarn in a series of connected loops using long hand or mechanized needles. |
|
Lacemaking |
Lacemaking involves the production of ornamental openwork of threads that have been twisted, looped and intertwined to form patterns. This can involve very fine and intricate hand stitching. |
|
Leatherworking |
Leather crafts involve two basic steps: cutting, carving, sewing and other physical processes; and cementing, dyeing and finishing the leather. The first can involve a variety of tools. The latter can involve the use of solvents, dyes, lacquers and such. For tanning, see the chapter Leather, fur and footwear. |
|
Macrame |
Macrame is the ornamental knotting of yarn into bags, wall hangings or similar materials. |
|
Papermaking |
Papermaking involves preparing the pulp and then making the paper. A variety of plants, wood, vegetables, used paper rags and so forth can be used. The fibres must be separated out, often by boiling in alkali. The fibres are washed and placed in a beater to complete preparation of the pulp. Then paper is made by trapping the pulp on a wire or fabric screen, and allowed to dry in the air or by being pressed between layers of felt. The paper can be treated with sizings, dyes, pigments and other materials. |
|
Silk screen printing |
See “Drawing, Painting and Printmaking”. |
|
Weaving |
Weaving uses a machine called a loom to combine two sets of yarn, the warp and the weft, to produce fabric. The warp is wound on large reels, called beams, which run the length of the loom. The warp yarns are threaded through the loom to form vertical parallel threads. The weft is fed from the side of the loom by bobbins. The loom shuttle carries the weft yarns across the loom horizontally under and above alternate warp threads. A starch sizing is used to protect warp threads from breaking during weaving. There are many types of looms, both hand-operated and mechanical. |
Table 2. Description of fibre and textile processes.
|
Process |
Description |
|
Carding |
Process of cleaning and straightening fibres into parallel lines by combing it (by hand or by special machinery) and twisting the fibres into a rope-like form. This process can create large amounts of dust. |
|
Spinning |
A foot-pedal-operated spinning wheel is used to turn the spindle, which combines several fibres into twisted, elongated yarn. |
|
Finishing |
The woven fabric can be singed to remove projecting hairs, desized with enzymes, and scoured by boiling in alkali to remove fats and waxes. |
|
Dyeing |
Yarn or fabric can be dyed using a variety of types of dyes (natural, direct, acid, basic, disperse, fibre-reactive and more) depending upon the type of fabric. Many dyeing processes involve heating the dyebath to near boiling. Many dyeing assistants can be used, including acids, alkalis, salt, sodium hydrosulphite and, in the case of natural dyes, mordants such as urea, ammonium dichromate, ammonia, copper sulphate, and ferrous sulphate. Dyes are usually purchased in powder form. Some dyes may contain solvents. |
|
Bleaching |
Fabrics can be bleached with chlorine bleaches to remove colour. |
No material is off limits for artists, who may use any of thousands of animal, vegetable or synthetic materials in their work. They gather materials such as weeds, vines or animal hair from the outdoors, or purchase products from suppliers who may have altered them by treating them with oils, fragrances, dyes, paints or pesticides (e.g., rat poison in twine or rope intended for agricultural use). Imported animal or vegetable materials that have been processed to eliminate disease carrying insects, spores or fungi are also used. Old rags, bones, feathers, wood, plastics or glass are among many other materials incorporated in fibre crafts.
Potential Sources of Health Hazards in the Fibre Arts
Chemicals
Health hazards in fibre or textile arts, as in any workplace, include air pollutants such as dusts, gases, fumes and vapours that are inherent in the materials or are produced in the work process, and can be inhaled or affect the skin. In addition to chemical hazards of dyes, paints, acids, alkalis, mothproofing agents and so on, fibre or textile materials may be contaminated with biological materials that can cause disease.
Vegetable dusts
Workers heavily exposed to dusts of raw cotton, sisal, jute and other vegetable fibres in industrial workplaces have developed various chronic lung problems such as “brown lung” (byssinosis), which begins with chest tightness and shortness of breath, and can be disabling after many years. Exposure to vegetable dusts in general may cause lung irritation or other effects such as asthma, hay fever, bronchitis and emphysema. Other materials associated with vegetable fibres, such as moulds, mildew, sizing materials and dyes, may also cause allergic or other reactions.
Animal dusts
Animal products used by fibre artists such as wool, hair, hides and feathers may be contaminated with bacteria, moulds, lice or mites that are capable of causing “Q” fever, mange, respiratory symptoms, skin rashes, anthrax, allergies and so on, if they are not treated or fumigated before use. Fatal cases of inhalation anthrax have occurred in craft weavers, including the 1976 death of a California weaver.
Synthetic materials
The effects of dusts of polyesters, nylon, acrylic, rayon and acetates are not well known. Some plastic fibres may release gas or components or residues which are left in the fabric after processing, as in the case of formaldehyde released by polyesters or permanent-press fabrics. Sensitive individuals have reported allergic responses in rooms or stores where these materials were present, and some have developed skin rashes after wearing clothing of these fabrics, even after repeated washings.
Heating, scorching or otherwise altering synthetic materials chemically may release potentially hazardous gases or fumes.
Physical Effects of Working with Fibres and Textiles
The physical characteristics of materials may affect the user. Rough, thorny or abrasive materials can cut or abrade skin. Glass fibres or stiff grasses or rattan can penetrate the skin and cause infections or rashes.
Much of fibre or fabric work is done while the worker is seated for prolonged periods, and involves repetitious motion of arms, wrists, hands and fingers, and often the entire body. This may produce pain and eventual repetitive strain injuries. Weavers, for example, can develop back problems, carpal tunnel syndrome, skeletal deformation from weaving in a squatting position on older types of looms (particularly in young children), hand and finger disorders (e.g., swollen joints, arthritis, neuralgia) from threading and tying knots, and eyestrain from poor lighting (figure 1). Many of the same problems can occur in other fibre crafts involving sewing, tying knots, knitting and so forth. Needlework crafts can also involve hazards of needle pricks.
Figure 1. Weaving with a hand loom.

Lifting of large papermaking screens containing water-saturated pulp can cause possible back injuries due to the weight of the water and pulp.
Precautions
As with all work, the adverse effects depend upon the amount of time spent working on a project each day, the number of workdays, weeks or years, the quantity of work and the nature of the workplace, and the type of work itself. Other factors such as ventilation and lighting also affect the health of the artist or craftsperson. One or two hours a week spent at a loom in a dusty environment may not affect a person seriously, unless that person is highly allergic to dusts, but a prolonged period of work in the same environment over months or years may result in some health effects. However, even one episode of untrained lifting of a heavy object can cause injury to the spine.
Generally, for prolonged or regular work in fibre art or textiles:
- Obtain and use only treated or fumigated animal or vegetable materials. Other materials should be cleaned or washed, and stored in closed containers to minimize dusts.
- Damp mop or wipe work area surfaces frequently.
- In many countries, manufacturers are required to provide information that describes the hazardous aspects of chemicals such as dyes, adhesives, paints or solvents in any product purchased, such as a manufacturer’s Material Safety Data Sheet (MSDS). Request such information.
- Avoid eating, drinking or smoking in the work area.
- Take frequent rest and exercise periods when work involves repetitive motion.
- Modify work processes to reduce the need for excessive lifting or straining. For example, in papermaking use smaller screens or have another person assist in lifting the screen with the pulp.
- Use exhaust ventilation for regular or prolonged use of dusty materials, spray painting, heating of wax or work with solvent-containing materials such as oil-based paints or permanent ink markers.
- Avoid boiling acids and alkalis if possible. Wear gloves, goggles, face shield and protective apron.
- Remember that dusts, gases and vapours travel throughout buildings and may affect others present, particularly infants, children, the aged and the chronically ill.
- Consult an industrial hygienist or safety and health professional when planning a production workshop.
New Technology in Art
This article describes the basic health and safety concerns associated with the use of lasers, neon sculpture and computers in the arts. Creative artists often work very intimately with the technology, and in experimental ways. This scenario too often increases the risk of injury. The primary concerns are for eye and skin protection, for reducing the possibilities of electrical shock and for preventing exposure to toxic chemicals.
Lasers
Laser radiation may be hazardous to the eyes and skin of artists and audiences by both direct viewing and reflection. The degree of laser injury is a function of power. Higher-power lasers are more likely to cause serious injury and more hazardous reflections. Lasers are classified and labelled by their manufacturer in classes I to IV. Class I lasers exhibit no laser radiation hazard and Class IV are very dangerous.
Artists have used all laser classes in their work, and most use visible wavelengths. Besides the safety controls required of any laser system, artistic applications require special considerations.
In laser exhibits, it is important to isolate the audience from direct beam contact and scattered radiation, using plastic or glass enclosures and opaque beam stops. For planetariums and other indoor light shows, it is critical to maintain direct beam or reflected laser radiation at Class I levels where the audience is exposed. Class III or IV laser radiation levels must be kept at safe distances from performers and the audience. Typical distances are 3 m away when an operator controls the laser and 6 m away without continuous operator control. Written procedures are needed for set-up, alignment and testing of Class III and IV lasers. Required safety controls include warning in advance of energizing these lasers, key controls, fail-safe safety interlocks and manual reset buttons for Class IV lasers. For Class IV lasers, appropriate laser goggles should be worn.
Scanning laser art displays often used in the performing arts use rapidly moving beams that are generally safer since the duration of inadvertent eye or skin contact with the beam is short. Still, operators must employ safeguards to ensure exposure limits will not be exceeded if the scanning equipment fails. Outdoor displays cannot allow aircraft to fly through hazardous beam levels, or the illumination with greater than Class I levels of radiation of tall buildings or personnel in high-reach equipment.
Holography is the process of producing a three-dimensional photograph of an object using lasers. Most images are displayed off-axis from the laser beam, and intrabeam viewing is typically not a hazard. A transparent display case around the hologram can help reduce the possibilities of injury. Some artists create permanent images from their holograms, and many chemicals used in the development process are toxic and must be managed for accident prevention. These include pyrogallic acid, alkalis, sulphuric and hydrobromic acids, bromine, parabenzoquinone and dichromate salts. Safer substitutes are available for most of these chemicals.
Lasers also have serious non-radiological hazards. Most performance-level lasers use high voltages and amperage, creating significant risks of electrocution, particularly during design stages and maintenance. Dye lasers use toxic chemicals for the active lasing medium, and high-powered lasers may generate toxic aerosols, especially when the beam strikes a target.
Neon Art
Neon art uses neon tubes to produce lighted sculptures. Neon signage for advertising is one application. Producing a neon sculpture involves bending leaded glass to the desired shape, bombarding the evacuated glass tube at a high voltage to remove impurities from the glass tube, and adding small amounts of neon gas or mercury. A high voltage is applied across electrodes sealed into each end of the tube to give the luminous effect by exciting the gases trapped in the tube. To obtain a wider range of colours, the glass tube can be coated with fluorescent phosphors, which convert the ultraviolet radiation from the mercury or neon into visible light. The high voltages are achieved by using step-up transformers.
Electrical shock is a threat mostly when the sculpture is connected to its bombarding transformer to remove impurities from the glass tube, or to its electrical power source for testing or display (figure 1). The electrical current passing through the glass tube also causes the emission of ultraviolet light that in turn interacts with the phosphor-covered glass to form colours. Some near-ultraviolet radiation (UVA) may pass through the glass and present an eye hazard to those nearby; therefore, eyewear that blocks UVA should be worn.
Figure 1. Neon sculpture manufacture showing an artist behind a protective barrier.

Fred Tschida
Some phosphors that coat the neon tube are potentially toxic (e.g., cadmium compounds). Sometimes mercury is added to the neon gas to create a particularly vivid blue colour. Mercury is highly toxic by inhalation and is volatile at room temperature.
Mercury should be added to the neon tube with great care and stored in unbreakable sealed containers. The artist should use trays to contain spillage, and mercury spill kits should be available. Mercury should not be vacuumed up, as this may disperse a mist of mercury through the vacuum cleaner’s exhaust.
Computer Art
Computers are used in art for a variety of purposes, including painting, displaying scanned photographic images, producing graphics for printing and television (e.g., on-screen credits), and for a variety of animated and other special effects for motion pictures and television. The latter is a rapidly expanding use of computer art. This can bring about ergonomic problems, typically due to repetitive tasks and uncomfortably arranged components. The predominant complaints are discomfort in the wrists, arms, shoulders and neck, and vision problems. Most complaints are of a minor nature, but disabling injuries such as chronic tendinitis or carpal tunnel syndrome are possible.
Creating with computers often involves long periods manipulating the keyboard or mouse, designing or fine tuning the product. It is important that computer users take a break away from the screen periodically. Short, frequent breaks are more effective than long breaks every couple of hours.
Regarding the proper arrangement of components and the user, design solutions for correct posture and visual comfort are the key. Computer work station components should be easy to adjust for the variety of tasks and people involved.
Eye strain may be prevented by taking periodic visual breaks, preventing glare and reflection and by placing the top of the monitor so that it is at eye level. Vision problems may also be avoided if the monitor has a refresh rate of 70 Hz, so that image flicker is reduced.
Many kinds of radiation effects are possible. Ultraviolet, visible, infrared, radio frequency and microwave radiation emissions from computer hardware are generally at or below normal background levels. The possible health effects of lower-frequency waves from the electrical circuitry and electronic components are not well understood. To date, however, no solid evidence identifies a health risk from exposure to the electromagnetic fields associated with computer monitors. Computer monitors do not emit hazardous levels of x rays.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."