- You are here:
-
Home

- Part I. The Body

Children categories

1. Blood (3)

1. Blood
Chapter Editor: Bernard D. Goldstein
Table of Contents
Tables
Haematopoietic and Lymphatic System
Bernard D. Goldstein
Leukaemia, Malignant Lymphomas and Multiple Myeloma
Timo Partanen, Paolo Boffetta, Elisabete Weiderpass
Agents or Work Conditions Affecting the Blood
Bernard D. Goldstein
Tables
Click a link below to view the table in the article context.
2. Cancer (4)
2. Cancer
Chapter Editor: Paolo Boffetta
Table of Contents
Tables
Introduction
Neil Pearce, Paolo Boffetta and Manolis Kogevinas
Occupational Carcinogens
Paolo Boffetta, Rodolfo Saracci, Manolis Kogevinas, Julian Wilbourn and Harri Vainio
Environmental Cancer
Bruce K. Armstrong and Paolo Boffetta
Prevention
Per Gustavsson
Tables
Click a link below to view table in article context.
- Occupational cancer: Key facts
- Estimated proportions of cancer (PAR) attributable to occupations
- Evaluation of evidence of carcinogenicity in the IARC Monographs
- IARC Monograph programme classification groups
- Group 1-Chemicals carcinogenic to humans
- Group 2A—Chemicals probably carcinogenic to humans
- Group 2B—Chemicals possibly carcinogenic to humans
- Pesticides evaluated in IARC Monographs, Volumes 1-63 (1972-1995)
- Drugs evaluated in IARC Monographs, Volumes 1-63 (1972-1995)
- Environmental agents/exposures known or suspected of human cancer
- Industries, occupations, exposures presenting a carcinogenic risk
- Industries, occs., exps. with cancer excess not definitive carcinogens
- Registered population variations of incidence of some common cancers
3. Cardiovascular System (7)
3. Cardiovascular System
Chapter Editors: Lothar Heinemann and Gerd Heuchert
Table of Contents
Tables and Figures
Introduction
Lothar Heinemann and Gerd Heuchert
Cardiovascular Morbidity and Mortality in the Workforce
Gottfried Enderlein and Lothar Heinemann
The Risk Factor Concept in Cardiovascular Disease
Lothar Heinemann, Gottfried Enderlein and Heide Stark
Rehabilitation and Prevention Programmes
Lothar Heinemann and Gottfried Enderlein
Physical, Chemical and Biological Hazards
Physical Factors
Heide Stark and Gerd Heuchert
Chemical Hazardous Materials
Ulrike Tittelbach and Wolfram Dietmar Schneider
Biological Hazards
Regina Jäckel, Ulrike Tittelbach and Wolfram Dietmar Schneider
Tables
Click a link below to view table in article context
- Mortality from cardiovascular diseases
- Mortality rates, special cardiovascular diagnosis groups
- Rate of disease and reduced work ability
- Work associated with cardiovascular hazards
- Occupation-related infection and disease
Figures
Point to a thumbnail to see figure caption, click to see the figure in the article context.



4. Digestive System (6)
4. Digestive System
Chapter Editor: Heikki Savolainen
Table of Contents
Figures
Digestive system
G. Frada
Mouth and teeth
F. Gobbato
Liver
George Kazantzis
Peptic ulcer
K. S. Cho
Liver cancer
Timo Partanen, Timo Kauppinen, Paolo Boffetta and Elisabete Weiderpass
Pancreatic cancer
Timo Partanen, Timo Kauppinen, Paolo Boffetta and Elisabete Weiderpass
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.

5. Mental Health (8)
5. Mental Health
Chapter Editors: Joseph J. Hurrell, Lawrence R. Murphy, Steven L. Sauter and Lennart Levi
Table of Contents
Tables and Figures
Work and Mental Health
Irene L.D. Houtman and Michiel A.J. Kompier
Work-related Psychosis
Craig Stenberg, Judith Holder and Krishna Tallur
Mood and Affect
Depression
Jay Lasser and Jeffrey P. Kahn
Work-related Anxiety
Randal D. Beaton
Post-traumatic Stress Disorder and its Relationship to Occupational Health and Injury Prevention
Mark Braverman
Stress and Burnout and their Implication in the Work Environment
Herbert J. Freudenberger
Cognitive Disorders
Catherine A. Heaney
Karoshi: Death from Overwork
Takashi Haratani
Tables
Click a link below to view table in article context.
1. Schematic overview of management strategies & examples
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.



6. Musculoskeletal System (14)
6. Musculoskeletal System
Chapter Editors: Hilkka Riihimäki and Eira Viikari-Juntura
Table of Contents
Tables and Figures
Overview
Hilkka Riihimäki
Muscles
Gisela Sjøgaard
Tendons
Thomas J. Armstrong
Bones and Joints
David Hamerman
Intervertebral Discs
Sally Roberts and Jill P.G. Urban
Low-back Region
Hilkka Riihimäki
Thoracic Spine Region
Jarl-Erik Michelsson
Neck
Åsa Kilbom
Shoulder
Mats Hagberg
Elbow
Eira Viikari-Juntura
Forearm, Wrist and Hand
Eira Viikari-Juntura
Hip and Knee
Eva Vingård
Leg, Ankle and Foot
Jarl-Erik Michelsson
Other Diseases
Marjatta Leirisalo-Repo
Tables
Click a link below to view table in article context.
- Structure-function of joint components
- Prevalence of back disorders, in Finns over 30 years
- Reducing the risks for low-back pain at work
- Classification-low-back disorders (Quebec Task Force)
- Permissible motions for head in prolonged driving
- Incidence of epicondylitis in various populations
- Incidence of tenosynovitis/peritendinitis
- Primary osteoarthrosis of the hip in Malmö, Sweden
- Guidelines for the treatment of rheumatoid arthritis
- Infections known to trigger reactive arthritis
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|
























7. Nervous System (9)
7. Nervous System
Chapter Editor: Donna Mergler
Table of Contents
Tables and Figures
Nervous System: Overview
Donna Mergler and José A. Valciukas
Anatomy and Physiology
José A. Valciukas
Chemical Neurotoxic Agents
Peter Arlien-Søborg and Leif Simonsen
Manifestations of Acute and Early Chronic Poisoning
Donna Mergler
Preventing Neurotoxicity at Work
Barry Johnson
Clinical Syndromes Associated with Neurotoxicity
Robert G. Feldman
Measuring Neurotoxic Deficits
Donna Mergler
Diagnosis
Anna Maria Seppäläinen
Occupational Neuroepidemiology
Olav Axelson
Tables
Click a link below to view table in article context.
- Names & main functions of each pair of cranial nerves
- Grouping neurotoxic effects as to neurotoxicity
- Gases associated with neurotoxic effects
- Neurotoxic metals & their inorganic compounds
- Neurotoxic monomers
- Organic solvents associated with neurotoxicity
- Classes of common neurotoxic pesticides
- Other chemicals associated with neurotoxicity
- Chronic symptoms checklist
- Neuro-functional effects of exposures to some neurotoxins
- Chemical exposures & associated neurotoxic syndromes
- Some “core” batteries for assessing early neurotoxic effects
- Decision tree for neurotoxic disease
- Consistent neuro-functional effects of worksite exposures to some leading neurotoxic substances
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|









8. Renal-Urinary System (2)
8. Renal-Urinary System
Chapter Editor: George P. Hemstreet
Table of Contents
Tables and Figures
Renal-Urinary Systems
George P. Hemstreet
Renal-Urinary Cancers
Timo Partanen, Harri Vainio, Paolo Boffetta and Elisabete Weiderpass
Tables
Click a link below to view table in article context.
- Drug-metabolism enzymes in kidney
- The most common causes of haematuria, by age & sex
- Criteria for biomarker selection
- Potential biomarkers linked to cell injury
- Acute renal insufficiency & occupation
- Segments of the nephron affected by selected toxicants
- Applications of urinary cytology
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.



9. Reproductive System (9)
9. Reproductive System
Chapter Editor: Grace Kawas Lemasters
Table of Contents
Tables and Figures
Reproductive System: Introduction
Lowell E. Sever
Introduction to Male and Female Reproductive Function
Donald R. Mattison
Male Reproductive System and Toxicology
Steven Schrader and Grace Kawas Lemasters
Structure of the Female Reproductive System and Target Organ Vulnerability
Donald R. Mattison
Maternal Occupational Exposures and Adverse Pregnancy Outcomes
Grace Kawas Lemasters
Preterm Delivery and Work
Nicole Mamelle
Occupational and Environmental Exposures to the Newborn
Mary S. Wolff and Patrisha M. Woolard
Maternity Protection in Legislation
Marie-Claire Séguret
Pregnancy and US Work Recommendations
Leon J. Warshaw
Tables
Click a link below to view table in article context.
1. Exposures with multiple adverse endpoints
2. Epidemiological studies of paternal effects on pregnancy outcome
3. Potential female reproductive toxicants
4. Definition of foetal loss & infant death
5. Factors for small for gestational age and foetal loss
6. Identified sources of occupational fatigue
7. Relative risks & fatigue indices for preterm delivery
8. Prematurity risk by number of occupational fatigue indices
9. Relative risks and changes in working conditions
10. Newborn exposure sources and levels
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|




10. Respiratory System (18)
10. Respiratory System
Chapters Editors: Alois David and Gregory R. Wagner
Table of Contents
Tables and Figures
Structure and Function
Morton Lippmann
Lung Function Examination
Ulf Ulfvarson and Monica Dahlqvist
Diseases Caused by Respiratory Irritants and Toxic Chemicals
David L.S. Ryon and William N. Rom
Occupational Asthma
George Friedman-Jimenez and Edward L. Petsonk
Diseases Caused by Organic Dusts
Ragnar Rylander and Richard S. F. Schilling
Beryllium Disease
Homayoun Kazemi
Pneumoconioses: Definition
Alois David
ILO International Classification of Radiographs of Pneumoconioses
Michel Lesage
Aetiopathogenesis of Pneumoconioses
Patrick Sébastien and Raymond Bégin
Silicosis
John E. Parker and Gregory R. Wagner
Coal Workers’ Lung Diseases
Michael D. Attfield, Edward L. Petsonk and Gregory R. Wagner
Asbestos-Related Diseases
Margaret R. Becklake
Hard Metal Disease
Gerolamo Chiappino
Respiratory System: The Variety of Pneumoconioses
Steven R. Short and Edward L. Petsonk
Chronic Obstructive Pulmonary Disease
Kazimierz Marek and Jan E. Zejda
Health Effects of Man-Made Fibres
James E. Lockey and Clara S. Ross
Respiratory Cancer
Paolo Boffetta and Elisabete Weiderpass
Occupationally Acquired Infections of the Lung
Anthony A. Marfin, Ann F. Hubbs, Karl J. Musgrave, and John E. Parker
Tables
Click a link below to view table in article context.
1. Respiratory tract regions & particle deposition models
2. Inhalable, thoracic & respirable dust criteria
3. Summary of respiratory irritants
4. Mechanisms of lung injury by inhaled substances
5. Compounds capable of lung toxicity
6. Medical case definition of occupational asthma
7. Steps in diagnostic evaluation of asthma in the workplace
8. Sensitizing agents that can cause occupational asthma
9. Examples of sources of hazards of exposure to organic dust
10. Agents in organic dusts with potential biological activity
11. Diseases induced by organic dusts & their ICD codes
12. Diagnostic criteria for byssinosis
13. Properties of beryllium & its compounds
14. Description of standard radiographs
15. ILO 1980 Classification: Radiographs of Pneumoconioses
16. Asbestos-related diseases & conditions
17. Main commercial sources, products & uses of asbestos
18. Prevalence of COPD
19. Risk factors implicated in COPD
20. Loss of ventilatory function
21. Diagnostic classification, chronic bronchitis & emphysema
22. Lung function testing in COPD
23. Synthetic fibres
24. Established human respiratory carcinogens (IARC)
25. Probable human respiratory carcinogens (IARC)
26. Occupationally acquired respiratory infectious diseases
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|




































11. Sensory Systems (8)
11. Sensory Systems
Chapter Editor: Heikki Savolainen
Table of Contents
Tables and Figures
The Ear
Marcel-André Boillat
Chemically-Induced Hearing Disorders
Peter Jacobsen
Physically-Induced Hearing Disorders
Peter L. Pelmear
Equilibrium
Lucy Yardley
Vision and Work
Paule Rey and Jean-Jacques Meyer
Taste
April E. Mott and Norman Mann
Smell
April E. Mott
Cutaneous Receptors
Robert Dykes and Daniel McBain
Tables
Click a link below to view table in article context.
1. Typical calculation of functional loss from an audiogram
2. Visual requirements for different activities
3. Recommended illuminance values for the lighting design
4. Visual requirements for a driving licence in France
5. Agents/processes reported to alter the taste system
6. Agents/processes associated with olfactory abnormalities
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|























12. Skin Diseases (7)
12. Skin Diseases
Chapter Editor: Louis-Philippe Durocher
Table of Contents
Tables and Figures
Overview: Occupational Skin Diseases
Donald J. Birmingham
Non-Melanocytic Skin Cancer
Elisabete Weiderpass, Timo Partanen, Paolo Boffetta
Malignant Melanoma
Timo Partanen, Paolo Boffetta, Elisabete Weiderpass
Occupational Contact Dermatitis
Denis Sasseville
Prevention of Occupational Dermatoses
Louis-Phillipe Durocher
Occupational Nail Dystrophy
C.D. Calnan
Stigmata
H. Mierzecki
Tables
Click a link below to view table in article context.
1. Occupations at risk
2. Types of contact dermatitis
3. Common irritants
4. Common skin allergens
5. Predisposing factors for occupational dermatitis
6. Examples of skin irritants & sensitizers with occupations
7. Occupational dermatoses in Quebec in 1989
8. Risk factors & their effects on the skin
9. Collective measures (group approach) to prevention
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.





13. Systemic Conditions (3)
13. Systemic Conditions
Chapter Editor: Howard M. Kipen
Table of Contents
Figures
Systemic Conditions: An Introduction
Howard M. Kipen
Sick Building Syndrome
Michael J. Hodgson
Multiple Chemical Sensitivities
Mark R. Cullen
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.



Environmental Cancer
Cancer is a common disease in all countries of the world. The probability that a person will develop cancer by the age of 70 years, given survival to that age, varies between about 10 and 40% in both sexes. On average, in developed countries, about one person in five will die from cancer. This proportion is about one in 15 in developing countries. In this article, environmental cancer is defined as cancer caused (or prevented) by non-genetic factors, including human behaviour, habits, lifestyle and external factors over which the individual has no control. A stricter definition of environmental cancer is sometimes used, comprising only the effect of factors such as air and water pollution, and industrial waste.
Geographical Variation
Variation between geographical areas in the rates of particular types of cancer can be much greater than that for cancer as a whole. Known variation in the incidence of the more common cancers is summarized in table 1. The incidence of nasopharyngeal carcinoma, for example, varies some 500-fold between South East Asia and Europe. This wide variation in frequency of the various cancers has led to the view that much of human cancer is caused by factors in the environment. In particular, it has been argued that the lowest rate of a cancer observed in any population is indicative of the minimum, possibly spontaneous, rate occurring in the absence of causative factors. Thus the difference between the rate of a cancer in a given population and the minimum rate observed in any population is an estimate of the rate of the cancer in the first population which is attributable to environmental factors. On this basis it has been estimated, very approximately, that some 80 to 90% of all human cancers are environmentally determined (International Agency for Research on Cancer 1990).
Table 1. Variation between populations covered by cancer registration in the incidence of common cancers.1
|
Cancer (ICD9 code) |
High-incidence area |
CR2 |
Low-incidence area |
CR2 |
Range of variation |
|
Mouth (143-5) |
France, Bas Rhin |
2 |
Singapore (Malay) |
0.02 |
80 |
|
Nasopharynx (147) |
Hong Kong |
3 |
Poland, Warsaw (rural) |
0.01 |
300 |
|
Oesophagus (150) |
France, Calvados |
3 |
Israel (Israeli-born Jews) |
0.02 |
160 |
|
Stomach (151) |
Japan, Yamagata |
11 |
USA, Los Angeles (Filipinos) |
0.3 |
30 |
|
Colon (153) |
USA, Hawaii (Japanese) |
5 |
India, Madras |
0.2 |
30 |
|
Rectum (154) |
USA, Los Angeles (Japanese) |
3 |
Kuwait (non-Kuwaiti) |
0.1 |
20 |
|
Liver (155) |
Thailand, Khon Khaen |
11 |
Paraguay, Asuncion |
0.1 |
110 |
|
Pancreas (157) |
USA, Alameda County (Calif.) (Blacks) |
2 |
India, Ahmedabad |
0.1 |
20 |
|
Lung (162) |
New Zealand (Maori) |
16 |
Mali, Bamako |
0.5 |
30 |
|
Melanoma of skin (172) |
Australia, Capital Terr. |
3 |
USA, Bay Area (Calif.)(Blacks) |
0.01 |
300 |
|
Other skin cancers (173) |
Australia, Tasmania |
25 |
Spain, Basque Country |
0.05 |
500 |
|
Breast (174) |
USA, Hawaii (Hawaiian) |
12 |
China, Qidong |
1.0 |
10 |
|
Cervix uteri (180) |
Peru, Trujillo |
6 |
USA, Hawaii (Chinese) |
0.3 |
20 |
|
Corpus uteri (182) |
USA, Alameda County (Calif.) (Whites) |
3 |
China, Qidong |
0.05 |
60 |
|
Ovary (183) |
Iceland |
2 |
Mali, Bamako |
0.09 |
20 |
|
Prostate (185) |
USA, Atlanta (Blacks) |
12 |
China, Qidong |
0.09 |
140 |
|
Bladder (188) |
Italy, Florence |
4 |
India, Madras |
0.2 |
20 |
|
Kidney (189) |
France, Bas Rhin |
2 |
China, Qidong |
0.08 |
20 |
1 Data from cancer registries included in IARC 1992. Only cancer sites with cumulative rate larger or equal to 2% in the high-incidence area are included. Rates refer to males except for breast, cervix uteri, corpus uteri and ovary cancers.
2 Cumulative rate % between 0 and 74 years of age.
Source: International Agency for Research on Cancer 1992.
There are, of course, other explanations for geographical variation in cancer rates. Under-registration of cancer in some populations may exaggerate the range of variation, but certainly cannot explain differences of the size shown in table 1. Genetic factors also may be important. It has been observed, however, that when populations migrate along a gradient of cancer incidence they often acquire a rate of cancer which is intermediate between that of their home country and that of the host country. This suggests that a change in environment, without genetic change, has changed the cancer incidence. For example, when Japanese migrate to the United States their rates of colon and breast cancer, which are low in Japan, rise, and their rate of stomach cancer, which is high in Japan, falls, both tending more closely towards United States’ rates. These changes may be delayed until the first post-migration generation but they still occur without genetic change. For some cancers, change with migration does not occur. For example, the Southern Chinese retain their high rate of cancer of the nasopharynx wherever they live, thus suggesting that genetic factors, or some cultural habit which changes little with migration, are responsible for this disease.
Time Trends
Further evidence of the role of environmental factors in cancer incidence has come from the observation of time trends. The most dramatic and well-known change has been the rise in lung cancer rates in males and females in parallel with but occurring some 20 to 30 years after the adoption of cigarette use, which has been seen in many regions of the world; more recently in a few countries, such as the United States, there has been the suggestion of a fall in rates among males following a reduction in tobacco smoking. Less well understood are the substantial falls in incidence of cancers including those of the stomach, oesophagus and cervix which have paralleled economic development in many countries. It would be difficult to explain these falls, however, except in terms of reduction in exposure to causal factors in the environment or, perhaps, increasing exposure to protective factors—again environmental.
Main Environmental Carcinogenic Agents
The importance of environmental factors as causes of human cancer has been further demonstrated by epidemiological studies relating particular agents to particular cancers. The main agents which have been identified are summarized in table 10. This table does not contain the drugs for which a causal link with human cancer has been established (such as diethylstilboestrol and several alkylating agents) or suspected (such as cyclophosphamide) (see also Table 9). In the case of these agents, the risk of cancer has to be balanced with the benefits of the treatment. Similarly, Table 10 does not contain agents that occur primarily in the occupational setting, such as chromium, nickel and aromatic amines. For a detailed discussion of these agents see the previous article “Occupational Carcinogens.” The relative importance of the agents listed in table 8 varies widely, depending on the potency of the agent and the number of people involved. The evidence of carcinogenicity of several environmental agents has been evaluated within the IARC Monographs programme (International Agency for Research on Cancer 1995) (see again “Occupational Carcinogens” for a discussion of the Monographs programme); table 10 is based mainly on the IARC Monograph evaluations. The most important agents among those listed in table 10 are those to which a substantial proportion of the population is exposed in relatively large amounts. They include particularly: ultraviolet (solar) radiation; tobacco smoking; alcohol drinking; betel quid chewing; hepatitis B; hepatitis C and human papilloma viruses; aflatoxins; possibly dietary fat, and dietary fiber and vitamin A and C deficiency; reproductive delay; and asbestos.
Attempts have been made to estimate numerically the relative contributions of these factors to the 80 or 90% of cancers which might be attributed to environmental factors. The pattern varies, of course, from population to population according to differences in exposures and possibly in the genetic susceptibility to various cancers. In many industrialized countries, however, tobacco smoking and dietary factors are likely to be responsible each for roughly one-third of environmentally determined cancers (Doll and Peto 1981); while in developing countries the role of biological agents is likely to be large and that of tobacco relatively small (but increasing, following the recent increase in the consumption of tobacco in these populations).
Interactions between Carcinogens
An additional aspect to consider is the presence of interactions between carcinogens. Thus for example, in the case of alcohol and tobacco, and cancer of the oesophagus, it has been shown that an increasing consumption of alcohol multiplies manyfold the rate of cancer produced by a given level of tobacco consumption. Alcohol by itself may facilitate transport of tobacco carcinogens, or others, into the cells of susceptible tissues. Multiplicative interaction may also be seen between initiating carcinogens, as between radon and its decay products and tobacco smoking in miners of uranium. Some environmental agents may act by promoting cancers which have been initiated by another agent—this is the most likely mechanism for an effect of dietary fat on the development of breast cancer (probably through increased production of the hormones which stimulate the breast). The reverse may also occur, as, for example, in the case of vitamin A, which probably has an anti-promoting effect on lung and possibly other cancers initiated by tobacco. Similar interactions may also occur between environmental and constitutional factors. In particular, genetic polymorphism to enzymes implicated in the metabolism of carcinogenic agents or DNA repair is probably an important requirement of individual susceptibility to the effect of environmental carcinogens.
The significance of interactions between carcinogens, from the point of view of cancer control, is that withdrawal of exposure to one of two (or more) interacting factors may give rise to a greater reduction in cancer incidence than would be predicted from consideration of the effect of the agent when acting alone. Thus, for example, withdrawal of cigarettes may eliminate almost entirely the excess rate of lung cancer in asbestos workers (although rates of mesothelioma would be unaffected).
Implications for Prevention
The realization that environmental factors are responsible for a large proportion of human cancers has laid the foundation for primary prevention of cancer by modification of exposure to the factors identified. Such modification may comprise: removal of a single major carcinogen; reduction, as discussed above, in exposure to one of several interacting carcinogens; increasing exposure to protective agents; or combinations of these approaches. While some of this may be achieved by community-wide regulation of the environment through, for example, environmental legislation, the apparent importance of lifestyle factors suggests that much of primary prevention will remain the responsibility of individuals. Governments, however, may still create a climate in which individuals find it easier to take the right decision.
Prevention
Occupational exposures account for only a minor proportion of the total number of cancers in the entire population. It has been estimated that 4% of all cancers can be attributed to occupational exposures, based on data from the United States, with a range of uncertainty from 2 to 8%. This implies that even total prevention of occupationally induced cancers would result in only a marginal reduction in national cancer rates.
However, for several reasons, this should not discourage efforts to prevent occupationally induced cancers. First, the estimate of 4% is an average figure for the entire population, including unexposed persons. Among people actually exposed to occupational carcinogens, the proportion of tumours attributable to occupation is much larger. Second, occupational exposures are avoidable hazards to which individuals are involuntarily exposed. An individual should not have to accept an increased risk of cancer in any occupation, especially if the cause is known. Third, occupationally induced cancers can be prevented by regulation, in contrast to cancers associated with lifestyle factors.
Prevention of occupationally induced cancer involves at least two stages: first, identification of a specific compound or occupational environment as carcinogenic; and second, imposing appropriate regulatory control. The principles and practice of regulatory control of known or suspected cancer hazards in the work environment vary considerably, not only among different parts of the developed and developing world, but also among countries of similar socio-economic development.
The International Agency for Research on Cancer (IARC) in Lyon, France, systematically compiles and evaluates epidemiological and experimental data on suspected or known carcinogens. The evaluations are presented in a series of monographs, which provide a basis for decisions on national regulations on the production and use of carcinogenic compounds (see “Occupational Carcinogens”, above.
Historical Background
The history of occupational cancer dates back to at least 1775, when Sir Percivall Pott published his classical report on scrotal cancer in chimney-sweeps, linking exposure to soot to the incidence of cancer. The finding had some immediate impact in that sweeps in some countries were granted the right to bathe at the end of the working day. Current studies of sweeps indicate that scrotal and skin cancer are now under control, although sweeps are still at increased risk for several other cancers.
In the 1890s, a cluster of bladder cancer was reported at a German dye factory by a surgeon at a nearby hospital. The causative compounds were later identified as aromatic amines, and these now appear in lists of carcinogenic substances in most countries. Later examples include skin cancer in radium-dial painters, nose and sinus cancer among woodworkers caused by inhalation of wood dust, and “mule-spinner’s disease”—that is, scrotal cancer among cotton industry workers caused by mineral oil mist. Leukaemia induced by exposure to benzene in the shoe repair and manufacturing industry also represents a hazard that has been reduced after the identification of carcinogens in the workplace.
In the case of linking asbestos exposure to cancer, this history illustrates a situation with a considerable time-lag between risk identification and regulatory action. Epidemiological results indicating that exposure to asbestos was associated with an increased risk of lung cancer were already starting to accumulate by the 1930s. More convincing evidence appeared around 1955, but it was not until the mid-1970s that effective steps for regulatory action began.
The identification of the hazards associated with vinyl chloride represents a different history, where prompt regulatory action followed identification of the carcinogen. In the 1960s, most countries had adopted an exposure limit value for vinyl chloride of 500 parts per million (ppm). In 1974, the first reports of an increased frequency of the rare tumour liver angiosarcoma among vinyl chloride workers were soon followed by positive animal experimental studies. After vinyl chloride was identified as carcinogenic, regulatory actions were taken for a prompt reduction of the exposure to the current limit of 1 to 5 ppm.
Methods Used for the Identificationof Occupational Carcinogens
The methods in the historical examples cited above range from observations of clusters of disease by astute clinicians to more formal epidemiological studies—that is, investigations of the disease rate (cancer rate) among human beings. Results from epidemiological studies are of high relevance for evaluations of the risk to humans. A major drawback of cancer epidemiological studies is that a long time period, usually at least 15 years, is necessary to demonstrate and evaluate the effects of an exposure to a potential carcinogen. This is unsatisfactory for surveillance purposes, and other methods must be applied for a quicker evaluation of recently introduced substances. Since the beginning of this century, animal carcinogenicity studies have been used for this purpose. However, the extrapolation from animals to humans introduces considerable uncertainty. The methods also have limitations in that a large number of animals must be followed for several years.
The need for methods with a more rapid response was partly met in 1971, when the short-term mutagenicity test (Ames test) was introduced. This test uses bacteria to measure the mutagenic activity of a substance (its ability to cause irreparable changes in the cellular genetic material, DNA). A problem in the interpretation of the results of bacterial tests is that not all substances causing human cancers are mutagenic, and not all bacterial mutagens are considered to be cancer hazards for human beings. However, the finding that a substance is mutagenic is usually taken as an indication that the substance might represent a cancer hazard for humans.
New genetic and molecular biology methods have been developed during the last 15 years, with the aim of detecting human cancer hazards. This discipline is termed “molecular epidemiology.” Genetic and molecular events are studied in order to clarify the process of cancer formation and thus develop methods for early detection of cancer, or indications of increased risk of the development of cancer. These methods include analysis of damage to the genetic material and the formation of chemical linkages (adducts) between pollutants and the genetic material. The presence of chromosomal aberrations clearly indicates effects on the genetic material which may be associated with cancer development. However, the role of molecular epidemiological findings in human cancer risk assessment remains to be settled, and research is under way to indicate more clearly exactly how results of these analyses should be interpreted.
Surveillance and Screening
The strategies for prevention of occupationally induced cancers differ from those applied for control of cancer associated with lifestyle or other environmental exposures. In the occupational field, the main strategy for cancer control has been reduction or total elimination of exposure to cancer-causing agents. Methods based on early detection by screening programmes, such as those applied for cervical cancer or breast cancer, have been of very limited importance in occupational health.
Surveillance
Information from population records on cancer rates and occupation may be used for surveillance of cancer frequencies in various occupations. Several methods to obtain such information have been applied, depending on the registries available. The limitations and possibilities depend largely on the quality of the information in the registries. Information on disease rate (cancer frequency) is typically obtained from local or national cancer registries (see below), or from death certificate data, while information on the age-composition and size of occupational groups is obtained from population registries.
The classical example of this type of information is the “Decennial supplements on occupational mortality,” published in the UK since the end of the nineteenth century. These publications use death certificate information on cause of death and on occupation, together with census data on frequencies of occupations in the entire population, to calculate cause-specific death rates in different occupations. This type of statistic is a useful tool to monitor the cancer frequency in occupations with known risks, but its ability to detect previously unknown risks is limited. This type of approach may also suffer from problems associated with systematic differences in the coding of occupations on the death certificates and in the census data.
The use of personal identification numbers in the Nordic countries has offered a special opportunity to link individual census data on occupations with cancer registration data, and to directly calculate cancer rates in different occupations. In Sweden, a permanent linkage of the censuses of 1960 and 1970 and the cancer incidence during subsequent years have been made available for researchers and have been used for a large number of studies. This Swedish Cancer-Environment Registry has been used for a general survey of certain cancers tabulated by occupation. The survey was initiated by a governmental committee investigating hazards in the work environment. Similar linkages have been performed in the other Nordic countries.
Generally, statistics based on routinely collected cancer incidence and census data have the advantage of ease in providing large amounts of information. The method gives information on the cancer frequencies regarding occupation only, not in relation to certain exposures. This introduces a considerable dilution of the associations, since exposure may differ considerably among individuals in the same occupation. Epidemiological studies of the cohort type (where the cancer experience among a group of exposed workers is compared with that in unexposed workers matched for age, sex and other factors) or the case-control type (where the exposure experience of a group of persons with cancer is compared to that in a sample of the general population) give better opportunities for detailed exposure description, and thus better opportunities for investigation of the consistency of any observed risk increase, for example by examining the data for any exposure-response trends.
The possibility of obtaining more refined exposure data together with routinely collected cancer notifications was investigated in a prospective Canadian case-control study. The study was set up in the Montreal metropolitan area in 1979. Occupational histories were obtained from males as they were added to the local cancer registry, and the histories were subsequently coded for exposure to a number of chemicals by occupational hygienists. Later, the cancer risks in relation to a number of substances were calculated and published (Siemiatycki 1991).
In conclusion, the continuous production of surveillance data based on recorded information provides an effective and comparatively easy way to monitor cancer frequency by occupation. While the main purpose achieved is surveillance of known risk factors, the possibilities for the identification of new risks are limited. Registry-based studies should not be used for conclusions regarding the absence of risk in an occupation unless the proportion of individuals significantly exposed is more precisely known. It is quite common that only a relatively small percentage of members of an occupation actually are exposed; for these individuals the substance may represent a substantial hazard, but this will not be observable (i.e., will be statistically diluted) when the entire occupational group is analysed as a single group.
Screening
Screening for occupational cancer in exposed populations for purposes of early diagnosis is rarely applied, but has been tested in some settings where exposure has been difficult to eliminate. For example, much interest has focused on methods for early detection of lung cancer among people exposed to asbestos. With asbestos exposures, an increased risk persists for a long time, even after cessation of exposure. Thus, continuous evaluation of the health status of exposed individuals is justified. Chest x rays and cytological investigation of sputum have been used. Unfortunately, when tested under comparable conditions neither of these methods reduces the mortality significantly, even if some cases may be detected earlier. One of the reasons for this negative result is that the prognosis of lung cancer is little affected by early diagnosis. Another problem is that the x rays themselves represent a cancer hazard which, while small for the individual, may be significant when applied to a large number of individuals (i.e., all those screened).
Screening also has been proposed for bladder cancer in certain occupations, such as the rubber industry. Investigations of cellular changes in, or mutagenicity of, workers’ urine have been reported. However, the value of following cytological changes for population screening has been questioned, and the value of the mutagenicity tests awaits further scientific evaluation, since the prognostic value of having increased mutagenic activity in the urine is not known.
Judgements on the value of screening also depend on the intensity of the exposure, and thus the size of the expected cancer risk. Screening might be more justified in small groups exposed to high levels of carcinogens than among large groups exposed to low levels.
To summarize, no routine screening methods for occupational cancers can be recommended on the basis of present knowledge. The development of new molecular epidemiological techniques may improve the prospects for early cancer detection, but more information is needed before conclusions can be drawn.
Cancer Registration
During this century, cancer registries have been set up at several locations throughout the world. The International Agency for Research on Cancer (IARC) (1992) has compiled data on cancer incidence in different parts of the world in a series of publications, “Cancer Incidence in Five Continents.” Volume 6 of this publication lists 131 cancer registries in 48 countries.
Two main features determine the potential usefulness of a cancer registry: a well-defined catchment area (defining the geographical area involved), and the quality and completeness of the recorded information. Many of those registries that were set up early do not cover a geographically well-defined area, but rather are confined to the catchment area of a hospital.
There are several potential uses of cancer registries in the prevention of occupational cancer. A complete registry with nationwide coverage and a high quality of recorded information can result in excellent opportunities for monitoring the cancer incidence in the population. This requires access to population data to calculate age-standardized cancer rates. Some registries also contain data on occupation, which therefore facilitates the monitoring of cancer risk in different occupations.
Registries also may serve as a source for the identification of cases for epidemiological studies of both the cohort and case-control types. In the cohort study, personal identification data of the cohort is matched to the registry to obtain information on the type of cancer (i.e., as in record linkage studies). This assumes that a reliable identifying system exists (for example, personal identification numbers in the Nordic countries) and that confidentiality laws do not prohibit use of the registry in this way. For case-control studies, the registry may be used as a source for cases, although some practical problems arise. First, the cancer registries cannot, for methodological reasons, be quite up to date regarding recently diagnosed cases. The reporting system, and necessary checks and corrections of the obtained information, results in some lag time. For concurrent or prospective case-control studies, where it is desirable to contact the individuals themselves soon after a cancer diagnosis, it usually is necessary to set up an alternative way of identifying cases, for example via hospital records. Second, in some countries, confidentiality laws prohibit the identification of potential study participants who are to be contacted personally.
Registries also provide an excellent source for calculating background cancer rates to use for comparison of the cancer frequency in cohort studies of certain occupations or industries.
In studying cancer, cancer registries have several advantages over mortality registries commonly found in many countries. The accuracy of the cancer diagnoses is often better in cancer registries than in mortality registries, which are usually based on death certificate data. Another advantage is that the cancer registry often holds information on histological tumour type, and also permits the study of living persons with cancer, and is not limited to deceased persons. Above all, registries hold cancer morbidity data, permitting the study of cancers that are not rapidly fatal and/or not fatal at all.
Environmental Control
There are three main strategies for reducing workplace exposures to known or suspected carcinogens: elimination of the substance, reduced exposure by reduced emission or improved ventilation, and personal protection of the workers.
It has long been debated whether a true threshold for carcinogen exposure exists, below which no risk is present. It is often assumed that the risk should be extrapolated linearly down to zero risk at zero exposure. If this is the case, then no exposure limit, no matter how low, would be considered entirely risk-free. Despite this, many countries have defined exposure limits for some carcinogenic substances, while, for others, no exposure limit value has been assigned.
Elimination of a compound may give rise to problems when replacement substances are introduced and when the toxicity of the replacement substance must be lower than that of the substance replaced.
Reducing the exposure at the source may be relatively easily accomplished for process chemicals by encapsulation of the process and ventilation. For example, when the carcinogenic properties of vinyl chloride were discovered, the exposure limit value for vinyl chloride was lowered by a factor of one hundred or more in several countries. Although this standard was at first considered impossible to achieve by industry, later techniques allowed compliance with the new limit. Reduction of exposure at the source may be difficult to apply to substances that are used under less controlled conditions, or are formed during the work operation (e.g., motor exhausts). The compliance with exposure limits requires regular monitoring of workroom air levels.
When exposure cannot be controlled either by elimination or by reduced emissions, the use of personal protection devices is the only remaining way to minimize the exposure. These devices range from filter masks to air-supplied helmets and protective clothing. The main route of exposure must be considered in deciding appropriate protection. However, many personal protection devices cause discomfort to the user, and filter masks introduce an increased respiratory resistance which may be very significant in physically demanding jobs. The protective effect of respirators is generally unpredictable and depends on several factors, including how well the mask is fitted to the face and how often filters are changed. Personal protection must be considered as a last resort, to be attempted only when more effective ways of reducing exposure fail.
Research Approaches
It is striking how little research has been done to evaluate the impact of programmes or strategies to reduce the risk to workers of known occupational cancer hazards. With the possible exception of asbestos, few such evaluations have been conducted. Developing better methods for control of occupational cancer should include an evaluation of how present knowledge is actually put to use.
Improved control of occupational carcinogens in the workplace requires the development of a number of different areas of occupational safety and health. The process of identification of risks is a basic prerequisite for reducing exposure to carcinogens in the workplace. Risk identification in the future must solve certain methodological problems. More refined epidemiological methods are required if smaller risks are to be detected. More precise data on exposure for both the substance under study and possible confounding exposures will be necessary. More refined methods for description of the exact dose of the carcinogen delivered to the specific target organ also will increase the power of exposure-response calculations. Today, it is not uncommon that very crude substitutes are used for the actual measurement of target organ dose, such as the number of years employed in the industry. It is quite clear that such estimates of dose are considerably misclassified when used as a surrogate for dose. The presence of an exposure-response relationship is usually taken as strong evidence of an aetiological relationship. However, the reverse, lack of demonstration of an exposure-response relationship, is not necessarily evidence that no risk is involved, especially when crude measures of target organ dose are used. If target organ dose could be determined, then actual dose-response trends would carry even more weight as evidence for causation.
Molecular epidemiology is a rapidly growing area of research. Further insight into the mechanisms of cancer development can be expected, and the possibility of the early detection of carcinogenic effects will lead to earlier treatment. In addition, indicators of carcinogenic exposure will lead to improved identification of new risks.
Development of methods for supervision and regulatory control of the work environment are as necessary as methods for the identification of risks. Methods for regulatory control differ considerably even among western countries. The systems for regulation used in each country depend largely on socio-political factors and the status of labour rights. The regulation of toxic exposures is obviously a political decision. However, objective research into the effects of different types of regulatory systems could serve as a guide for politicians and decision-makers.
A number of specific research questions also need to be addressed. Methods to describe the expected effect of withdrawal of a carcinogenic substance or reduction of exposure to the substance need to be developed (i.e., the impact of interventions must be assessed). The calculation of the preventive effect of risk reduction raises certain problems when interacting substances are studied (e.g., asbestos and tobacco smoke). The preventive effect of removing one of two interacting substances is comparatively greater than when the two have only a simple additive effect.
The implications of the multistage theory of carcinogenesis for the expected effect of withdrawal of a carcinogen also adds a further complication. This theory states that the development of cancer is a process involving several cellular events (stages). Carcinogenic substances may act either in early or late stages, or both. For example, ionizing radiation is believed to affect mainly early stages in inducing certain cancer types, while arsenic acts mainly at late stages in lung cancer development. Tobacco smoke affects both early and late stages in the carcinogenic process. The effect of withdrawing a substance involved in an early stage would not be reflected in a reduced cancer rate in the population for a long time, while the removal of a “late-acting” carcinogen would be reflected in a reduced cancer rate within a few years. This is an important consideration when evaluating the effects of risk-reduction intervention programmes.
Finally, the effects of new preventive factors have recently attracted considerable interest. During the last five years, a large number of reports have been published on the preventive effect on lung cancer of consuming fruits and vegetables. The effect seems to be very consistent and strong. For example, the risk of lung cancer has been reported as double among those with a low consumption of fruits and vegetables versus those with high intake. Thus, future studies of occupational lung cancer would have greater precision and validity if individual data on fruit and vegetable consumption can be included in the analysis.
In conclusion, improved prevention of occupational cancer involves both improved methods for risk identification and more research on the effects of regulatory control. For risk identification, developments in epidemiology should mainly be directed toward better exposure information, while in the experimental field, validation of the results of molecular epidemiological methods regarding cancer risk are needed.
Introduction
Cardiovascular diseases (CVDs) are among the most common causes of illness and death in the working population, particularly in industrialized countries. They are also increasing in developing countries (Wielgosz 1993). In the industrialized countries, 15 to 20% of all working people will suffer from a cardiovascular dis- order sometime during their working lives and the frequency climbs sharply with age. Among those between 45 to 64 years of age, more than a third of the deaths among men and more than a quarter of deaths among women are caused by this group of diseases (see table 1). In recent years, CVDs have become the most frequent cause of death among post-menopausal women.
Table 1. Mortality from cardiovascular diseases in 1991 and 1990 in the age groups 45-54 and 55-64 for selected countries.
|
Country |
Men |
Women |
||||||
|
45-54 Years |
55-64 Years |
45-54 Years |
55-64 Years |
|||||
|
Rate |
% |
Rate |
% |
Rate |
% |
Rate |
% |
|
|
Russia** |
528 |
36 |
1,290 |
44 |
162 |
33 |
559 |
49 |
|
Poland** |
480 |
38 |
1,193 |
45 |
134 |
31 |
430 |
42 |
|
Argentina* |
317 |
40 |
847 |
44 |
131 |
33 |
339 |
39 |
|
Britain** |
198 |
42 |
665 |
47 |
59 |
20 |
267 |
32 |
|
USA* |
212 |
35 |
623 |
40 |
83 |
24 |
273 |
31 |
|
Germany** |
181 |
29 |
597 |
38 |
55 |
18 |
213 |
30 |
|
Italy* |
123 |
27 |
404 |
30 |
41 |
18 |
148 |
25 |
|
Mexico** |
128 |
17 |
346 |
23 |
82 |
19 |
230 |
24 |
|
France** |
102 |
17 |
311 |
22 |
30 |
12 |
94 |
18 |
|
Japan** |
111 |
27 |
281 |
26 |
48 |
22 |
119 |
26 |
*1990. **1991. Rate=Deaths per 100,000 inhabitants. % is from all causes of death in the age group.
Because of their complex aetiology, only a very small pro- portion of the cases of cardiovascular disease are recognized as occupational. Many countries, however, recognize that occu- pational exposures contribute to CVDs (sometimes referred to as work-related diseases). Working conditions and job demands play an important role in the multifactorial process that leads to these diseases, but ascertaining the role of the individual causal com- ponents is very difficult. The components interact in close, shifting relationships and often the disease is triggered by a combination or accumulation of different causal factors, including those that are work related.
The reader is referred to the standard cardiology texts for details of the epidemiology, pathophysiology, diagnosis and treatment of cardiovascular diseases. This chapter will focus on those aspects of cardiovascular disease that are particularly relevant in the workplace and are likely to be influenced by factors in the job and work environment.
Cardiovascular Morbidity and Mortality in the Workforce
In the following article, the term cardiovascular diseases (CVDs) refers to organic and functional disorders of the heart and circu- latory system, including the resultant damage to other organ systems, which are classified under numbers 390 to 459 in the 9th revision of the International Classification of Diseases (ICD) (World Health Organization (WHO) 1975). Based essentially on international statistics assembled by the WHO and data collected in Germany, the article discusses the prevalence of CVDs, new disease rates, and frequency of deaths, morbidity and disability.
Definition and Prevalence in the Working-Age Population
Coronary artery disease (ICD 410-414) resulting in ischaemia of the myocardium is probably the most significant CVD in the working population, particularly in industrialized countries. This condition results from a constriction in the vascular system that supplies the heart muscle, a problem caused primarily by arteriosclerosis. It affects 0.9 to 1.5% of working-age men and 0.5 to 1.0% of women.
Inflammatory diseases (ICD 420-423) may involve the endo- cardium, the heart valves, the pericardium and/or the heart muscle (myocardium) itself. They are less common in industrialized countries, where their frequency is well below 0.01% of the adult population, but are seen more frequently in developing countries, perhaps reflecting the greater prevalence of nutritional disorders and infectious diseases.
Heart rhythm disorders (ICD 427) are relatively rare, although much media attention has been given to recent instances of disability and sudden death among prominent professional athletes. Although they can have a significant impact on the ability to work, they are often asymptomatic and transitory.
The myocardiopathies (ICD 424) are conditions which involve enlargement or thickening of the heart musculation, effectively narrowing the vessels and weakening the heart. They have attracted more attention in recent years, largely because of improved methods of diagnosis, although their pathogenesis is often obscure. They have been attributed to infections, metabolic diseases, immunologic disorders, inflammatory diseases involving the capillaries and, of particular importance in this volume, to toxic exposures in the workplace. They are divided into three types:
- dilative—the most common form (5 to 15 cases per 100,000 people), which is associated with the functional weakening of the heart
- hypertrophic—thickening and enlargement of the myocardium resulting in relative insufficiency of the coronary arteries
- restrictive—a rare type in which myocardial contractions are limited.
Hypertension (ICD 401-405) (increased systolic and/or diastolic blood pressure) is the most common circulatory disease, being found among 15 to 20% of working people in industrialized countries. It is discussed in greater detail below.
Atherosclerotic changes in the major blood vessels (ICD 440), often associated with hypertension, cause disease in the organs they serve. Foremost among these is cerebrovascular disease (ICD 430-438), which may result in a stroke due to infarction and/or haemorrhage. This occurs in 0.3 to 1.0% of working people, most commonly among those aged 40 and older.
Atherosclerotic diseases, including coronary artery disease, stroke and hypertension, by far the most common cardiovascular diseases in the working population, are multifactorial in origin and have their onset early in life. They are of importance in the workplace because:
- so large a proportion of the workforce has an asymptomatic or unrecognized form of cardiovascular disease
- the development of that disease may be aggravated or acute symptomatic events precipitated by working conditions and job demands
- the acute onset of a symptomatic phase of the cardiovascular disease is often attributed to the job and/or the workplace environment
- most individuals with an established cardiovascular disease are capable of working productively, albeit, sometimes, only after effective rehabilitation and job retraining
- the workplace is a uniquely propitious arena for primary and secondary preventive programmes.
Functional circulatory disorders in the extremities (ICD 443) include Raynaud’s disease, short-term pallor of the fingers, and are relatively rare. Some occupational conditions, such as frostbite, long-term exposure to vinyl chloride and hand-arm exposure to vibration can induce these disorders.
Varicosities in the leg veins (ICD 454), often improperly dismissed as a cosmetic problem, are frequent among women, especially during pregnancy. While a hereditary tendency to weakness of the vein walls may be a factor, they are usually associated with long periods of standing in one position without movement, during which the static pressure within the veins is increased. The result- ant discomfort and leg oedema often dictate change or modifi- cation of the job.
Annual incidence rates
Among the CVDs, hypertension has the highest annual new case rate among working people aged 35 to 64. New cases develop in approximately 1% of that population every year. Next in frequency are coronary heart disease (8 to 92 new cases of acute heart attack per 10,000 men per year, and 3 to 16 new cases per 10,000 women per year) and stroke (12 to 30 cases per 10,000 men per year, and 6 to 30 cases per 10,000 women per year). As demonstrated by global data collected by the WHO-Monica project (WHO-MONICA 1994; WHO-MONICA 1988), the lowest new incidence rates for heart attack were found among men in China and women in Spain, while the highest rates were found among both men and women in Scotland. The significance of these data is that in the population of working age, 40 to 60% of heart attack victims and 30 to 40% of stroke victims do not survive their initial episodes.
Mortality
Within the primary working ages of 15 to 64, only 8 to 18% of deaths from CVDs occur prior to age 45. Most occur after age 45, with the annual rate increasing with age. The rates, which have been changing, vary considerably from country to country (WHO 1994b).
Table 1 shows the death rates for men and for women aged 45 to 54 and 55 to 64 for some countries. Note that the death rates for men are consistently higher than those for women of corresponding ages. Table 2 compares the death rates for various CVDs among people aged 55 to 64 in five countries.
Table 1. Mortality from cardiovascular diseases in 1991 and 1990 in the age groups 45-54 and 55-64 for selected countries.
|
Country |
Men |
Women |
||||||
|
45-54 Years |
55-64 Years |
45-54 Years |
55-64 Years |
|||||
|
Rate |
% |
Rate |
% |
Rate |
% |
Rate |
% |
|
|
Russia** |
528 |
36 |
1,290 |
44 |
162 |
33 |
559 |
49 |
|
Poland** |
480 |
38 |
1,193 |
45 |
134 |
31 |
430 |
42 |
|
Argentina* |
317 |
40 |
847 |
44 |
131 |
33 |
339 |
39 |
|
Britain** |
198 |
42 |
665 |
47 |
59 |
20 |
267 |
32 |
|
USA* |
212 |
35 |
623 |
40 |
83 |
24 |
273 |
31 |
|
Germany** |
181 |
29 |
597 |
38 |
55 |
18 |
213 |
30 |
|
Italy* |
123 |
27 |
404 |
30 |
41 |
18 |
148 |
25 |
|
Mexico** |
128 |
17 |
346 |
23 |
82 |
19 |
230 |
24 |
|
France** |
102 |
17 |
311 |
22 |
30 |
12 |
94 |
18 |
|
Japan** |
111 |
27 |
281 |
26 |
48 |
22 |
119 |
26 |
*1990. **1991. Rate=Deaths per 100,000 inhabitants. % is from all causes of death in the age group.
Table 2. Mortality rates from special cardiovascular diagnosis groups in the years 1991 and 1990 in the age group 55-64 for selected countries
|
Diagnosis group |
Russia (1991) |
USA (1990) |
Germany (1991) |
France (1991) |
Japan (1991) |
|||||
|
|
M |
F |
M |
F |
M |
F |
M |
F |
M |
F |
|
393–398 |
16.8 |
21.9 |
3.3 |
4.6 |
3.6 |
4.4 |
2.2 |
2.3 |
1.2 |
1.9 |
|
401–405 |
22.2 |
18.5 |
23.0 |
14.6 |
16.9 |
9.7 |
9.4 |
4.4 |
4.0 |
1.6 |
|
410 |
160.2 |
48.9 |
216.4 |
79.9 |
245.2 |
61.3 |
100.7 |
20.5 |
45.9 |
13.7 |
|
411–414 |
586.3 |
189.9 |
159.0 |
59.5 |
99.2 |
31.8 |
35.8 |
6.8 |
15.2 |
4.2 |
|
415–429 |
60.9 |
24.0 |
140.4 |
64.7 |
112.8 |
49.2 |
73.2 |
27.0 |
98.7 |
40.9 |
|
430–438 |
385.0 |
228.5 |
54.4 |
42.2 |
84.1 |
43.8 |
59.1 |
26.7 |
107.3 |
53.6 |
|
440 |
|
|
4.4 |
2.1 |
11.8 |
3.8 |
1.5 |
0.3 |
0.3 |
0.1 |
|
Total 390–459 |
1,290 |
559 |
623 |
273 |
597 |
213 |
311 |
94 |
281 |
119 |
Deaths per 100,000 inhabitants; M=male; F=female.
Work Disability and Early Retirement
Diagnosis-related statistics on time lost from work represent an important perspective on the impact of morbidity on the working population, even though the diagnostic designations are usually less precise than in cases of early retirement because of disability. The case rates, usually expressed in cases per 10,000 employees, provide an index of the frequency of the disease categories, while the average number of days lost per case indicates the relative seriousness of particular diseases. Thus, according to statistics on 10 million workers in western Germany compiled by the Allgemeinen Ortskrankenkasse, CVDs accounted for 7.7% of the total disability in 1991-92, although the number of cases for that period was only 4.6% of the total (Table 3). In some countries, where early retirement is provided when work ability is reduced due to illness, the pattern of disability mirrors the rates for different categories of CVD.
Table 3. Rate of cardiovascular disease among early pensioners* due to reduced ability to work (N = 576,079) and diagnosis-related work disability in the western part of Germany, 1990-92
|
Diagnosis group |
Main cause of illness |
Access to early retirement; number per 100,000 early retirees |
Average annual work disability 1990–92 |
||||
|
Cases per 100,000 employed |
Duration (days) per case |
||||||
|
Men |
Women |
Men |
Women |
Men |
Women |
||
|
390–392 |
Acute rheumatic fever |
16 |
24 |
49 |
60 |
28.1 |
32.8 |
|
393–398 |
Chronic rheumatic heart disease |
604 |
605 |
24 |
20 |
67.5 |
64.5 |
|
401–405 |
Hypertension, high blood pressure diseases |
4,158 |
4,709 |
982 |
1,166 |
24.5 |
21.6 |
|
410–414 |
Ischaemic heart diseases |
9,635 |
2,981 |
1,176 |
529 |
51.2 |
35.4 |
|
410, 412 |
Acute and existing myocardial infarction |
2,293 |
621 |
276 |
73 |
85.8 |
68.4 |
|
414 |
Coronary heart disease |
6,932 |
2,183 |
337 |
135 |
50.8 |
37.4 |
|
415–417 |
Pulmonary circulatory diseases |
248 |
124 |
23 |
26 |
58.5 |
44.8 |
|
420–429 |
Other non-rheumatic heart diseases |
3,434 |
1,947 |
645 |
544 |
36.3 |
25.7 |
|
420–423 |
Inflammatory heart diseases |
141 |
118 |
20 |
12 |
49.4 |
48.5 |
|
424 |
Heart valve disorders |
108 |
119 |
22 |
18 |
45.6 |
38.5 |
|
425 |
Myocardiopathy |
1,257 |
402 |
38 |
14 |
66.8 |
49.2 |
|
426 |
Stimulus performance disorder |
86 |
55 |
12 |
7 |
39.6 |
45.0 |
|
427 |
Cardiac rhythm disorder |
734 |
470 |
291 |
274 |
29.3 |
21.8 |
|
428 |
Cardiac insufficiency |
981 |
722 |
82 |
61 |
62.4 |
42.5 |
|
430–438 |
Cerebrovascular diseases |
4,415 |
2,592 |
172 |
120 |
75.6 |
58.9 |
|
440–448 |
Diseases of the arteries, arterioles and capillaries |
3,785 |
1,540 |
238 |
90 |
59.9 |
44.5 |
|
440 |
Arteriosclerosis |
2,453 |
1,090 |
27 |
10 |
71.7 |
47.6 |
|
443 |
Raynaud’s disease and other vascular diseases |
107 |
53 |
63 |
25 |
50.6 |
33.5 |
|
444 |
Arterial embolism and thrombosis |
219 |
72 |
113 |
34 |
63.3 |
49.5 |
|
451–456 |
Diseases of the veins |
464 |
679 |
1,020 |
1,427 |
22.9 |
20.3 |
|
457 |
Noninfectious diseases of the lymph nodes |
16 |
122 |
142 |
132 |
10.4 |
14.2 |
|
458 |
Hypotension |
29 |
62 |
616 |
1,501 |
9.4 |
9.5 |
|
459 |
Other circulatory diseases |
37 |
41 |
1,056 |
2,094 |
11.5 |
10.2 |
|
390–459 |
Total cardiovascular diseases |
26,843 |
15,426 |
6,143 |
7,761 |
29.6 |
18.9 |
*Early pensioned: Statutory pensions insurance for former Federal Republic of Germany, work disability AOK-West.
The Risk Factor Concept in Cardiovascular Disease
Risk factors are genetic, physiological, behavioural and socioeconomic characteristics of individuals that place them in a cohort of the population that is more likely to develop a particular health problem or disease than the rest of the population. Usually applied to multifactorial diseases for which there is no single precise cause, they have been particularly useful in identifying candidates for primary preventive measures and in assessing the effectiveness of the prevention programme in controlling the risk factors being targeted. They owe their development to large-scale prospective population studies, such as the Framingham study of coronary artery disease and stroke conducted in Framingham, Massachusetts, in the United States, other epidemiological studies, intervention studies and experimental research.
It should be emphasized that risk factors are merely expressions of probability—that is, they are not absolute nor are they diagnostic. Having one or more risk factors for a particular disease does not necessarily mean that an individual will develop the disease, nor does it mean that an individual without any risk factors will escape the disease. Risk factors are individual characteristics which affect that person’s chances of developing a particular disease or group of diseases within a defined future time period. Categories of risk factors include:
- somatic factors, such as high blood pressure, lipid metabolism disorders, overweight and diabetes mellitus
- behavioural factors, such as smoking, poor nutrition, lack of physical movement, type-A personality, high alcohol consumption and drug abuse
- strains, including exposures in the occupational, social and private spheres.
Naturally, genetic and dispositional factors also play a role in high blood pressure, diabetes mellitus and lipid metabolism disorders. Many of the risk factors promote the development of arteriosclerosis, which is a significant precondition for the onset of coronary heart disease.
Some risk factors may put the individual at risk for the development of more than one disease; for example, cigarette smoking is associated with coronary artery disease, stroke and lung cancer. At the same time, an individual may have multiple risk factors for a particular disease; these may be additive but, more often, the combinations of risk factors may be multiplicative. Somatic and lifestyle factors have been identified as the main risk factors for coronary heart disease and stroke.
Hypertension
Hypertension (increased blood pressure), a disease in its own right, is one of the major risk factors for coronary heart disease (CHD) and stroke. As defined by the WHO, blood pressure is normal when the diastolic is below 90 mm Hg and the systolic is below 140 mm Hg. In threshold or borderline hypertension, the diastolic ranges from 90 to 94 mm Hg and the systolic from 140 to 159 mm Hg. Individuals with diastolic pressures equal to or greater than 95 mm Hg and systolic pressures equal to or greater than 160 mm Hg are designated as being hypertensive. Studies have shown, however, that such sharp criteria are not entirely correct. Some individuals have a “labile” blood pressure—the pressure fluctuates between normal and hypertensive levels depending on the circumstances of the moment. Further, without regard to the specific categories, there is a linear progression of relative risk as the pressure rises above the normal level.
In the United States, for example, the incidence rate of CHD and stroke among men aged 55 to 61 was 1.61% per year for those whose blood pressure was normal compared to 4.6% per year for those with hypertension (National Heart, Lung and Blood Institute 1981).
Diastolic pressures over 94 mm Hg were found in 2 to 36% of the population aged 35 to 64 years, according to the WHO-MONICA study. In many countries of Central, Northern and Eastern Europe (e.g., Russia, the Czech Republic, Finland, Scotland, Romania, France and parts of Germany, as well as Malta), hypertension was found in over 30% of the population aged 35 to 54, while in countries including Spain, Denmark, Belgium, Luxembourg, Canada and the United States, the corresponding figure was less than 20% (WHO-MONICA 1988). The rates tend to increase with age, and there are racial differences. (In the United States, at least, hypertension is more frequent among African-Americans than in the White population.)
Risks for developing hypertension
The important risk factors for developing hypertension are excess body weight, high salt intake, a series of other nutritional factors, high alcohol consumption, physical inactivity, and psychosocial factors, including stress (Levi 1983). Furthermore, there is a certain genetic component whose relative significance is not yet fully understood (WHO 1985). Frequent familial high blood pressure should be considered a danger and special attention paid to controlling lifestyle factors.
There is evidence that psychosocial and psychophysical factors, in conjunction with the job, can have an influence on developing hypertension, especially for short-term blood pressure increases. Increases have been found in the concentration of certain hormones (adrenalin and noradrenalin) as well as cortisol (Levi 1972), which, alone and in combination with high salt consumption, can lead to increased blood pressure. Work stress also appears to be related to hypertension. A dose-effect relationship with intensity of air traffic was shown (Levi 1972; WHO 1985) in comparing groups of air traffic controllers with different high psychic strain.
Treatment of hypertension
Hypertension can and should be treated, even in the absence of any symptoms. Lifestyle changes such as weight control, reduction of sodium intake and regular physical exercise, coupled when necessary with anti-hypertensive medications, regularly evoke re- ductions in blood pressure, often to normal levels. Unfortunately, many individuals found to be hypertensive are not receiving adequate treatment. According to the WHO-MONICA study (1988), less than 20% of hypertensive women in Russia, Malta, eastern Germany, Scotland, Finland and Italy were receiving adequate treatment during the mid-1980s, while the comparable figure for men in Ireland, Germany, China, Russia, Malta, Finland, Poland, France and Italy was under 15%.
Prevention of hypertension
The essence of preventing hypertension is identifying individuals with blood pressure elevation through periodic screening or medical examination programmes, repeated checks to verify the extent and duration of the elevation, and the institution of an appropriate treatment regimen that will be maintained indefinitely. Those with a family history of hypertension should have their pressures checked more frequently and should be guided to elimination or control of any risk factors they may present. Control of alcohol abuse, physical training and physical fitness, normal weight maintenance and efforts to reduce psychological stress are all important elements of prevention programmes. Improvement in workplace conditions, such as reducing noise and excess heat, are other preventive measures.
The workplace is a uniquely advantageous arena for programmes aimed at the detection, monitoring and control of hypertension in the workforce. Convenience and low or no cost make them attractive to the participants and the positive effects of peer pressure from co-workers tend to enhance their compliance and the success of the programme.
Hyperlipidemia
Many long-term international studies have demonstrated a convincing relationship between abnormalities in lipid metabolism and an increased risk of CHD and stroke. This is particularly true for elevated total cholesterol and LDL (low density lipoproteins) and/or low levels of HDL (high density lipoproteins). Recent research provides further evidence linking the excess risk with different lipoprotein fractions (WHO 1994a).
The frequency of elevated total cholesterol levels >>6.5 mmol/l) was shown to vary considerably in population groups by the worldwide WHO-MONICA studies in the mid-1980s (WHO- MONICA 1988). The rate of hypercholesterolemia for popu- lations of working age (35 to 64 years of age) ranged from 1.3 to 46.5% for men and 1.7 to 48.7% for women. Although the ranges were generally similar, the mean cholesterol levels for the study groups in different countries varied significantly: in Finland, Scot- land, East Germany, the Benelux countries and Malta, a mean of over 6 mmol/l was found, while the means were lower in east Asian countries like China (4.1 mmol/l) and Japan (5.0 mmol/l). In both regions, the means were below 6.5 mmol/l (250 mg/dl), the level designated as the threshold of normal; however, as noted above for blood pressure, there is a progressive increase of risk as the level rises, rather than a sharp demarcation between normal and abnormal. Indeed, some authorities have pegged a total chol- esterol level of 180 mg/dl as the optimal level that should not be exceeded.
It should be noted that gender is a factor, with women averaging lower levels of HDL. This may be one reason why women of working age have a lower mortality rate from CHD.
Except for the relatively few individuals with hereditary hyper- cholesterolemia, cholesterol levels generally reflect the dietary intake of foods rich in cholesterol and saturated fats. Diets based on fruit, plant products and fish, with reduced total fat intake and substitution of poly-unsaturated fats, are generally associated with low cholesterol levels. Although their role is not yet entirely clear, intake of anti-oxidants (vitamin E, carotene, selenium and so on) is also thought to influence cholesterol levels.
Factors associated with higher levels of HDL cholesterol, the “protective” form of lipoprotein, include race (Black), gender (female), normal weight, physical exercise and moderate alcohol intake.
Socio-economic level also appears to play a role, at least in industrialized countries, as in West Germany, where higher cholesterol levels were found in population groups of both men and women with lower education levels (under ten years of schooling) compared to those completing 12 years of education (Heinemann 1993).
Cigarette Smoking
Cigarette smoking is among the most important risk factors for CVD. The risk from cigarette smoking is directly related to the number of cigarettes one smokes, the length of time one has been smoking, the age at which one began to smoke, the amount one inhales and the tar, nicotine and carbon monoxide content of the inspired smoke. Figure 1 illustrates the striking increase in CHD mortality among cigarette smokers compared to non-smokers. This increased risk is demonstrated among both men and women and in all socio-economic classes.
The relative risk of cigarette smoking declines after tobacco use is discontinued. This is progressive; after about ten years of non-smoking, the risk is down almost to the level of those who never smoked.
Recent evidence has demonstrated that those inhaling “second-hand smoke” (i.e., passive inhalation of smoke from cigarettes smoked by others) are also at significant risk (Wells 1994; Glantz and Parmley 1995).
Rates of cigarette smoking vary among countries, as demonstrated by the international WHO-MONICA study (1988). The highest rates for men aged 35 to 64 were found in Russia, Poland, Scotland, Hungary, Italy, Malta, Japan and China. More women smokers were found in Scotland, Denmark, Ireland, the United States, Hungary and Poland (the recent Polish data are limited to large cities).
Social status and occupational level are factors in the level of smoking among workers. Figure 1, for example, demonstrates that the proportions of smokers among men in East Germany increased in the lower social classes. The reverse is found in countries with relatively low numbers of smokers, where there is more smoking among those at higher social levels. In East Germany, smoking is also more frequent among shift-workers when compared with those on a “normal” work schedule.
Figure 1. Relative mortality risk from cardiovascular diseases for smokers (including ex-smokers) and social classes compared to non-smoking, normal weight, skilled workers (male) based on occupational medical care examinations in East Germany, mortality 1985-89, N= 2.7 million person years.
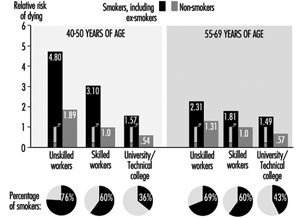
Unbalanced Nutrition, Salt Consumption
In most industrialized countries traditional low-fat nutrition has been replaced by high-calorie, high-fat, low carbohydrate, too sweet or too salty eating habits. This contributes to the development of overweight, high blood pressure, and high cholesterol level as elements of high cardiovascular risk. The heavy consumption of animal fats, with their high proportion of saturated fatty acids, leads to an increase in LDL cholesterol and increased risk. Fats derived from vegetables are much lower in these substances (WHO 1994a). Eating habits are also strongly associated with both socio-economic level and occupation.
Overweight
Overweight (excess fat or obesity rather than increased muscle mass) is a cardiovascular risk factor of lesser direct significance. There is evidence that the male pattern of excess fat distribution (abdominal obesity) is associated with a greater risk of cardiovascular and metabolic problems than the female (pelvic) type of fat distribution.
Overweight is associated with hypertension, hypercholesterolemia and diabetes mellitus, and, to a much greater extent in women than men, tends to increase with age (Heuchert and Enderlein 1994) (Figure 2). It is also a risk factor for musculoskeletal problems and osteoarthritis, and makes physical exercise more difficult. The frequency of significant overweight varies considerably among countries. Random population surveys conducted by the WHO-MONICA project found it in more than 20% of females aged 35 to 64 in the Czech Republic, East Germany, Finland, France, Hungary, Poland, Russia, Spain and Yugoslavia, and in both sexes in Lithuania, Malta and Romania. In China, Japan, New Zealand and Sweden, fewer than 10% of both men and women in this age group were significantly overweight.
Common causes of overweight include familial factors (these may in part be genetic but more often reflect common dietary habits), overeating, high-fat and high-carbohydrate diets and lack of physical exercise. Overweight tends to be more common among the lower socio-economic strata, particularly among women, where, among other factors, financial constraints limit the availability of a more balanced diet. Population studies in Germany demonstrated that the proportion of significant overweight among those with lower education levels is 3 to 5 times greater than that among people with more education, and that some occupations, notably food preparation, agriculture and to some extent shift work, have a high percentage of overweight people (Figure 3) (Heinemann 1993).
Figure 2. Prevalence of hypertension by age, sex and six levels of relative body weight according tot he body-mass index (BMI) in occupational medical care examinations in East Germany (normal BMI values are underlined).
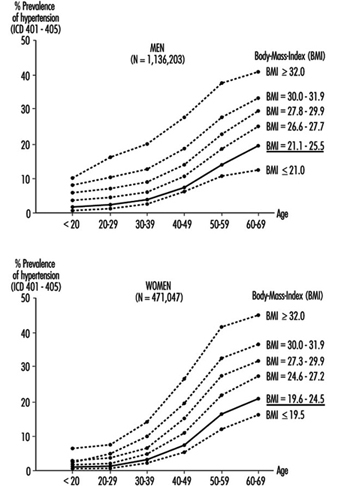
Figure 3. Relative risk from overweight by length of education(years of schooling) in Germay (population 25-64 years).
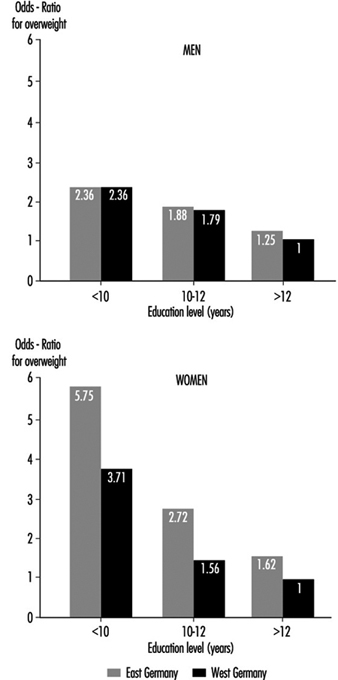
Physical Inactivity
The close association of hypertension, overweight and diabetes mellitus with lack of exercise at work and/or off the job has made physical inactivity a significant risk factor for CHD and stroke (Briazgounov 1988; WHO 1994a). A number of studies have demonstrated that, holding all other risk factors constant, there was a lower mortality rate among persons engaging regularly in high-intensity exercises than among those with a sedentary lifestyle.
The amount of exercise is readily measured by noting its duration and either the amount of physical work accomplished or the extent of the exercise-induced increase in heart rate and the time required for that rate to return to its resting level. The latter is also useful as an indicator of the level of cardiovascular fitness: with regular physical training, there will be less of an increase in heart rate and a more rapid return to the resting rate for a given intensity of exercise.
Workplace physical fitness programmes have been shown to be effective in enhancing cardiovascular fitness. Participants in these tend also to give up cigarette smoking and to pay greater attention to proper diets, thus significantly reducing their risk of CHD and stroke.
Alcohol
High alcohol consumption, especially the drinking of high-proof spirits, has been associated with a greater risk of hypertension, stroke and myocardiopathy, while moderate alcohol use, particularly of wine, has been found to reduce the risk of CHD (WHO 1994a). This has been associated with the lower CHD mortality among the upper social strata in industrialized countries, who generally prefer wine to “hard” liquors. It should also be noted that while their alcohol intake may be similar to that of wine drinkers, beer drinkers tend to accumulate excess weight, which, as noted above, may increase their risk.
Socio-economic Factors
A strong correlation between socio-economic status and the risk of CVD has been demonstrated by analyses of the death register mortality studies in Britain, Scandinavia, Western Europe, the United States and Japan. For example, in eastern Germany, the cardiovascular death rate is considerably lower for the upper social classes than for the lower classes (see Figure 1) (Marmot and Theorell 1991). In England and Wales, where general mortality rates are declining, the relative gap between the upper and lower classes is widening.
Socio-economic status is typically defined by such indicators as occupation, occupational qualifications and position, level of education and, in some instances, income level. These are readily translated into standard of living, nutritional patterns, free-time activities, family size and access to medical care. As noted above, behavioural risk factors (such as smoking and diet) and the somatic risk factors (such as overweight, hypertension and hyperlipidemia) vary considerably among social classes and occupational groups (Mielck 1994; Helmert, Shea and Maschewsky Schneider 1995).
Occupational Psychosocial Factors and Stress
Occupational stress
Psychosocial factors at the workplace primarily refer to the combined effect of working environment, work content, work demands and technological-organizational conditions, and also to personal factors like capability, psychological sensitivity, and finally also to health indicators (Karasek and Theorell 1990; Siegrist 1995).
The role of acute stress on people who already suffer from cardiovascular disease is uncontested. Stress leads to episodes of angina pectoris, rhythm disorders and heart failure; it can also precipitate a stroke and/or a heart attack. In this context stress is generally understood to mean acute physical stress. But evidence has been mounting that acute psychosocial stress can also have these effects. Studies from the 1950s showed that people who work two jobs at a time, or who work overtime for long periods, have a relatively higher risk of heart attack, even at a young age. Other studies showed that in the same job, the person with the greater work and time pressure and frequent problems on the job is at significantly greater risk (Mielck 1994).
In the last 15 years, job stress research suggests a causal relationship between work stress and the incidence of cardiovascular disease. This is true for cardiovascular mortality as well as frequency of coronary disease and hypertension (Schnall, Landsbergis and Baker 1994). Karasek’s job strain model defined two factors that could lead to an increased incidence of cardiovascular disease:
- extent of job demands
- extent of decision-making latitude.
Later Johnson added as a third factor the extent of social support (Kristensen 1995) which is discussed more fully elsewhere in this Encyclopaedia. The chapter Psychosocial and Organizational Factors includes discussions on individual factors, such as Type A personality, as well as social support and other mechan- isms for overcoming the effects of stress.
The effects of factors, whether individual or situational, that lead to increased risk of cardiovascular disease can be reduced by “coping mechanisms”, that is, by recognizing the problem and overcoming it by attempting to make the best of the situation.
Until now, measures aimed at the individual have predominated in the prevention of the negative health effects of work stress. Increasingly, improvements in organizing the work and expanding employee decision-making latitude have been used (e.g., action research and collective bargaining; in Germany, occupational quality and health circles) to achieve an improvement in productivity as well as to humanize the work by decreasing the stress load (Landsbergis et al. 1993).
Night and Shift Work
Numerous publications in the international literature cover the health risks posed by night and shift work. It is generally accepted that shift work is one risk factor which, together with other relev- ant (including indirect) work-related demands and expectation factors, leads to adverse effects.
In the last decade research on shift work has increasingly dealt with the long-term effects of night and shift work on the frequency of cardiovascular disease, especially ischaemic heart disease and myocardial infarction, as well as cardiovascular risk factors. The results of epidemiological studies, especially from Scandinavia, permit a higher risk of ischemic heart disease and myocardial infarction to be presumed for shift workers (Alfredsson, Karasek and Theorell 1982; Alfredsson, Spetz and Theorell 1985; Knutsson et al. 1986; Tüchsen 1993). In Denmark it was even estimated that 7% of cardiovascular disease in men as well as women can be traced to shift work (Olsen and Kristensen 1991).
The hypothesis that night and shift workers have a higher risk (estimated relative risk approximately 1.4) for cardiovascular disease is supported by other studies that consider cardiovascular risk factors like hypertension or fatty acid levels for shift workers as compared to day workers. Various studies have shown that night and shift work may induce increased blood pressure and hypertension as well as increased triglyceride and/or serum cholesterol (as well as normal range fluctuations for HDL-cholesterol in increased total cholesterol). These changes, together with other risk factors (like heavy cigarette smoking and overweight among shift workers), can cause increased morbidity and mortality due to atherosclerotic disease (DeBacker et al. 1984; DeBacker et al. 1987; Härenstam et al. 1987; Knutsson 1989; Lavie et al. 1989; Lennernäs, Åkerstedt and Hambraeus 1994; Orth-Gomer 1983; Romon et al. 1992).
In all, the question of possible causal links between shift work and atherosclerosis cannot be definitively answered at present, as the pathomechanism is not sufficiently clear. Possible mechanisms discussed in the literature include changes in nutrition and smoking habits, poor sleep quality, increases in lipid level, chronic stress from social and psychological demands and disrupted circadian rhythms. Knutsson (1989) has proposed an interesting pathogenesis for the long-term effects of shift work on chronic morbidity.
The effects of various associated attributes on risk estimation have hardly been studied, since in the occupational field other stress-inducing working conditions (noise, chemical hazardous materials, psychosocial stress, monotony and so on) are connected with shift work. From the observation that unhealthy nutritional and smoking habits are often connected with shift work, it is often concluded that an increased risk of cardiovascular disease among shift workers is more the indirect result of unhealthy behaviour (smoking, poor nutrition and so on) than directly the result of night or shift work (Rutenfranz, Knauth and Angersbach 1981). Furthermore, the obvious hypothesis of whether shift work promotes this conduct or whether the difference comes primarily from the choice of workplace and occupation must be tested. But regardless of the unanswered questions, special attention must be paid in cardiovascular prevention programmes to night and shift workers as a risk group.
Summary
In summary, risk factors represent a broad variety of genetic, somatic, physiological, behavioural and psychosocial characteristics which can be assessed individually for individuals and for groups of individuals. In the aggregate, they reflect the probability that CVD, or more precisely in the context of this article, CHD or stroke will develop. In addition to elucidating the causes and pathogenesis of multifactorial diseases, their chief importance is that they delineate individuals who should be targets for risk factor elimination or control, an exercise admirably suited to the workplace, while repeated risk assessments over time demonstrate the success of that preventive effort.
Rehabilitation and Prevention Programmes
Most individuals with recognized CVD are able to work effectively and productively in most of the jobs found in the modern workplace. Just a few decades ago, individuals surviving an acute myocardial infarction were cosseted and pampered for weeks and months with close supervision and enforced inactivity. Laboratory confirmation of the diagnosis was enough to justify labelling the individual as “permanently and totally disabled”. New diagnostic technology that provides more accurate evaluation of cardiac status and the favourable experiences of those who could not or would not accept such a label, soon demonstrated that an early return to work and an optimal level of activity was not only possible but desirable (Edwards, McCallum and Taylor 1988; Theorell et al. 1991; Theorell 1993). Today, patients commence supervised physical activity as soon as the acute effects of the infarction subside, are often out of the hospital in a few days instead of the mandatory 6 to 8 weeks of yore, and are often back on the job within a few weeks. When desirable and feasible, surgical procedures such as angioplasty, by-pass operations and even cardiac transplantation can improve the coronary blood flow, while a regimen featuring diet, exercise and control of the risk factors for CHD can minimize (or even reverse) the progression of coronary atherosclerosis.
Once the acute, often life-threatening phases of the CVD have been overcome, passive movement followed by active exercise should be initiated early during the stay in the hospital or clinic. With heart attacks, this phase is completed when the individual can climb stairs without great difficulty. At the same time, the individual is schooled in a risk-prevention regimen that includes proper diet, cardiovascular conditioning exercises, adequate rest and relaxation, and stress management. During these phases of rehabilitation, support from family members, friends and co-workers can be particularly helpful (Brusis and Weber-Falkensammer 1986). The programme can be carried out in rehabilitation facilities or in ambulatory “heart groups” under the supervision of a trained physician (Halhubar and Traencker 1986). The focus on controlling lifestyle and behavioural risk factors and controlling stress has been shown to result in a measurable reduction in the risk of re-infarction and other cardiovascular problems.
Throughout the programme the attending physician should maintain contact with the employer (and particularly with the company doctor, if there is one) to discuss the prospects for recovery and the probable duration of the period of disability, and to explore the feasibility of any special arrangements that may be needed to permit an early return to the job. The worker’s knowledge that the job is waiting and that he or she is expected to be able to return to it is a potent motivating factor for the enhancement of recovery. Experience has amply demonstrated that the success of the rehabilitation effort diminishes as the absence from work lengthens.
In instances where desirable adjustments in the job and/or the workplace are not possible or feasible, retraining and appropriate job placement can obviate unnecessary invalidism. Specially protected workshops are often helpful in reintegrating into the workplace people who have been absent from the job for long periods while receiving treatment for the serious effects of stroke, congestive heart failure or disabling angina pectoris.
Following the return to work, continued surveillance by both the attending physician and the occupational physician is eminently desirable. Periodic medical evaluations, at intervals that are frequent initially but lengthen as recovery is assured, are helpful in assessing the worker’s cardiovascular status, adjusting medications and other elements in the maintenance regimen and monitoring the adherence to the lifestyle and behavioural recommendations. Satisfactory findings in these examinations may allow the gradual easing of any work limitations or restrictions until the worker is fully integrated into the workplace.
Workplace Health Promotion and Prevention Programmes
The prevention of occupational diseases and injuries is a prime responsibility of the organization’s occupational health and safety programme. This includes primary prevention (i.e., the identifica- tion and elimination or control of potential hazards and strains by changing the work environment or the job). It is supplemented by secondary prevention measures which protect the workers from the effects of existing hazards and strains that cannot be elim- inated (i.e., personal protective equipment and periodic medical surveillance examinations). Workplace health promotion and pre- vention (HPP) programmes go beyond these goals. They place their emphasis on health-conscious behaviour as it relates to life- style, behavioural risk factors, eliminating or coping with stress and so on. They are of great significance, particularly in pre- venting CVD. The goals of HPP, as formulated by the WHO Committee on Environmental and Health Monitoring in Occupational Health, extend beyond the mere absence of disease and injury to include well-being and functional capacity (WHO 1973).
The design and operation of HPP programmes are discussed in more detail elsewhere in the chapter. In most countries, they have a particular focus on the prevention of CVDs. For example, in Germany, the “Have a heart for your heart” programme supplements the heart health circles organized by the health insurance companies (Murza and Laaser 1990, 1992), while the “Take Heart” movement in Britain and Australia has similar goals (Glasgow et al. 1995).
That such programmes are effective was verified in the 1980s by the WHO Collaborative Trial in Prevention of Heart Disease, which was carried out in 40 pairs of factories in four European countries and involved approximately 61,000 men aged 40 to 59. The preventive measures largely comprised health education activities, carried out primarily by the organization’s employee health service, focused on cholesterol-lowering diets, giving up cigarette smoking, weight control, increased physical activity and controlling hypertension. A randomized screening of 10% of the eligible workers in the factories designated as controls demonstrated that during the 4 to 7 years of the study, overall risk of CVDs could be reduced by 11.1% (19.4% among those initially at high risk). In the study factories, mortality from CHDs fell by 7.4%, while overall mortality fell by 2.7%. The best results were achieved in Belgium, where the intervention was carried out continuously during the entire study period, while the poorest results were seen in Britain, where the prevention activities were sharply curtailed prior to the last follow-up examination. This disparity emphasizes the relationship of success to the duration of the health education effort; it takes time to inculcate the desired lifestyle changes. The intensity of the educational effort was also a factor: in Italy, where six full-time health educators were involved, a 28% reduction in overall risk-factor profile was achieved, whereas in Britain, where only two full-time educators served three times the number of workers, a risk factor reduction of only 4% was achieved.
While the time required to detect reductions in CHD mortality and morbidity is a formidable limiting factor in epidemiological studies aimed at evaluating the results of company health programmes (Mannebach 1989), reductions in risk factors have been demonstrated (Janssen 1991; Gomel et al. 1993; Glasgow et al. 1995). Temporary decreases in the number of lost workdays and a decline in hospitalization rates have been reported (Harris 1994). There seems to be general agreement that HPP activities in the community and particularly in the workplace have significantly contributed to the reduction in cardiovascular mortality in the United States and other western industrialized countries.
Conclusion
CVDs loom large in the workplace, not so much because the cardiovascular system is particularly vulnerable to environmental and job hazards, but because they are so common in the popu- lation of working age. The workplace offers a singularly advant- ageous arena for the detection of unrecognized, asymptomatic CVDs, for the circumvention of workplace factors that might accelerate or aggravate them and for the identification of factors that increase the risk of CVDs and the mounting of programmes to eliminate or control them. When CVDs do occur, prompt attention to control of job-related circumstances that may prolong or increase their severity can minimize the extent and duration of disability, while early, professionally supervised rehabilitation efforts will facilitate the restoration of working capacity and reduce the risk of recurrences.
Physical, Chemcial and Biological Hazards
The intact cardiovascular system is remarkably resistant to the harmful effects of physical, chemical and biological hazards encountered on the job or in the workplace. With a very few exceptions, such hazards are rarely a direct cause of CVDs. On the other hand, once the integrity of the cardiovascular system is compromised—and this may be entirely silent and unrecognized—exposure to these hazards may contribute to the ongoing development of a disease process or precipitate symptoms reflecting functional impairment. This dictates early identification of workers with incipient CVD and modification of their jobs and/or the work environment to reduce the risk of harmful effects. The following segments will include brief discussions of some of the more commonly encountered occupational hazards that may affect the cardiovascular system. Each of the hazards presented below is discussed more fully elsewhere in the Encyclopaedia.
Digestive System
The digestive system exerts a considerable influence on the efficiency and work capacity of the body, and acute and chronic illnesses of the digestive system are among the commonest causes of absenteeism and disablement. In this context, the occupational physician may be called upon in either of the following ways to offer suggestions concerning hygiene and nutritional requirements in relation to the particular needs of a given occupation: to assess the influence that factors inherent in the occupation may have either in producing morbid conditions of the digestive system, or in aggravating others that may pre-exist or be otherwise independent of the occupation; or to express an opinion concerning general or specific fitness for the occupation.
Many of the factors that are harmful to the digestive system may be of occupational origin; frequently a number of factors act in concert and their action may be facilitated by individual predisposition. The following are among the most important occupational factors: industrial poisons; physical agents; and occupational stress such as tension, fatigue, abnormal postures, frequent changes in work tempo, shift work, night work and unsuitable eating habits (quantity, quality and timing of meals).
Chemical Hazards
The digestive system may act as a portal for the entry of toxic substances into the body, although its role here is normally much less important than that of the respiratory system which has an absorption surface area of 80-100 m2 whereas the corresponding figure for the digestive system does not exceed 20 m2. In addition, vapours and gases entering the body by inhalation reach the bloodstream and hence the brain without meeting any intermediate defence; however, a poison that is ingested is filtered and, to some degree, metabolized by the liver before reaching the vascular bed. Nevertheless, the organic and functional damage may occur both during entry into and elimination from the body or as a result of accumulation in certain organs. This damage suffered by the body may be the result of the action of the toxic substance itself, its metabolites or the fact that the body is depleted of certain essential substances. Idiosyncrasy and allergic mechanisms may also play a part. The ingestion of caustic substances is still a fairly common accidental occurrence. In a retrospective study in Denmark, the annual incidence was of 1/100,000 with an incidence of hospitalization of 0.8/100,000 adult person-years for oesophageal burns. Many household chemicals are caustic.
Toxic mechanisms are highly complex and may vary considerably from substance to substance. Some elements and compounds used in industry cause local damage in the digestive system affecting, for example, the mouth and neighbouring area, stomach, intestine, liver or pancreas.
Solvents have particular affinity for lipid-rich tissues. The toxic action is generally complex and different mechanisms are involved. In the case of carbon tetrachloride, liver damage is thought to be mainly due to toxic metabolites. In the case of carbon disulphide, gastrointestinal involvement is attributed to the specific neurotropic action of this substance on the intramural plexus whilst liver damage seems to be more due to the solvent’s cytotoxic action, which produces changes in lipoprotein metabolism.
Liver damage constitutes an important part of the pathology of exogenic poisons since the liver is the prime organ in metabolizing toxic agents and acts with the kidneys in detoxication processes. The bile receives from the liver, either directly or after conjugation, various substances that can be reabsorbed in the enterohepatic cycle (for instance, cadmium, cobalt, manganese). Liver cells participate in oxidation (e.g., alcohols, phenols, toluene), reduction, (e.g., nitrocompounds), methylation (e.g., selenic acid), conjugation with sulphuric or glucuronic acid (e.g., benzene), acetylation (e.g., aromatic amines). Kupffer cells may also intervene by phagocytosing the heavy metals, for example.
Severe gastro-intestinal syndromes, such as those due to phosphorus, mercury or arsenic are manifested by vomiting, colic, and bloody mucus and stools and may be accompanied by liver damage (hepatomegalia, jaundice). Such conditions are relatively rare nowadays and have been superseded by occupational intoxications which develop slowly and even insidiously; consequently liver damage, in particular, may often be insidious too.
Infectious hepatitis deserves particular mention; it may be related to a number of occupational factors (hepatotoxic agents, heat or hot work, cold or cold work, intense physical activity, etc.), may have an unfavourable course (protracted or persistent chronic hepatitis) and may easily result in cirrhosis. It frequently occurs with jaundice and thus creates diagnostic difficulties; moreover, it presents difficulties of prognosis and estimation of the degree of recovery and hence of fitness for resumption of work.
Although the gastro-intestinal tract is colonized by abundant microflora which have important physiological functions in human health, an occupational exposure may give rise to occupational infections. For example, abattoir workers may be at risk to contract a helicobacter infection. This infection may often be symptomless. Other important infections include the Salmonella and Shigella species, which must be also controlled in order to maintain product safety, such as in the food industry and in catering services.
Smoking and alcohol consumption are the major risks for oesophageal cancer in industrialized countries, and occupational aetiology is of lesser importance. However, butchers and their spouses seem to be at elevated risk of colorectal cancer.
Physical Factors
Various physical agents may cause digestive system syndromes; these include direct or indirect disabling traumata, ionizing radiations, vibration, rapid acceleration, noise, very high and low temperatures or violent and repeated climatic changes. Burns, especially if extensive, may cause gastric ulceration and liver damage, perhaps with jaundice. Abnormal postures or movements may cause digestive disorders especially if there are predisposing conditions such as para-oesophageal hernia, visceroptosis or relaxatio diaphragmatica; in addition, extra-digestive reflexes such as heartburn may occur where digestive disorders are accompanied by autonomic nervous system or neuro-psychological troubles. Troubles of this type are common in modern work situations and may themselves be the cause of gastro-intestinal dysfunction.
Occupational Stress
Physical fatigue may also disturb digestive functions, and heavy work may cause secretomotor disorders and dystrophic changes, especially in the stomach. Persons with gastric disorders, especially those who have undergone surgery are limited in the amount of heavy work they can do, if only because heavy work requires higher levels of nutrition.
Shift work may cause important changes in eating habits with resultant functional gastro-intestinal problems. Shift work may be associated with elevated blood cholesterol and triglyceride levels, as well as increased gamma-glutamyltransferase activity in serum.
Nervous gastric dyspepsia (or gastric neurosis) seems to have no gastric or extragastric cause at all, nor does it result from any humoral or metabolic disorder; consequently, it is considered to be due to a primitive disorder of the autonomic nervous system, sometimes associated with excessive mental exertion or emotional or psychological stress. The gastric disorder is often manifested by neurotic hypersecretion or by hyperkinetic or atonic neurosis (the latter frequently associated with gastroptosis). Epigastric pain, regurgitation and aerophagia may also come under the heading of neurogastric dyspepsia. Elimination of the deleterious psychological factors in the work environment may lead to remission of symptoms.
Several observations point to an increased frequency of peptic ulcers among people carrying responsibilities, such as supervisors and executives, workers engaged in very heavy work, newcomers to industry, migrant workers, seafarers and workers subject to serious socio-economic stress. However, many people suffering the same disorders lead a normal professional life, and statistical evidence is lacking. In addition to working conditions drinking, smoking and eating habits, and home and social life all play a part in the development and prolongation of dyspepsia, and it is difficult to determine what part each one plays in the aetiology of the condition.
Digestive disorders have also been attributed to shift work as a consequence of frequent changes of eating hours and poor eating at workplaces. These factors can aggravate pre-existing digestive troubles and release a neurotic dyspepsia. Therefore, workers should be assigned to shift work only after medical examination.
Medical Supervision
It can be seen that the occupational health practitioner is faced with many difficulties in the diagnosis and estimation of digestive system complaints (due inter alia to the part played by deleterious non-occupational factors) and that his or her responsibility in prevention of disorders of occupational origin is considerable.
Early diagnosis is extremely important and implies periodical medical examinations and supervision of the working environment, especially when the level of risk is high.
Health education of the general public, and of workers in particular, is a valuable preventive measure and may yield substantial results. Attention should be paid to nutritional requirements, choice and preparation of foodstuffs, the timing and size of meals, proper chewing and moderation in the consumption of rich foods, alcohol and cold drinks, or complete elimination of these substances from the diet.
Mouth and Teeth
The mouth is the portal of entry to the digestive system and its functions are, primarily, the chewing and swallowing of food and the partial digestion of starches by means of salivary enzymes. The mouth also participates in vocalizing and may replace or complement the nose in respiration. Due to its exposed position and the functions it fulfils, the mouth is not only a portal of entry but also an area of absorption, retention and excretion for toxic substances to which the body is exposed. Factors which lead to respiration via the mouth (nasal stenoses, emotional situations) and increased pulmonary ventilation during effort, promote either the penetration of foreign substances via this route, or their direct action on the tissues in the buccal cavity.
Respiration through the mouth promotes:
- greater penetration of dust into the respiratory tree since the buccal cavity has a retention quotient (impingement) of solid particles much lower than that of the nasal cavities
- dental abrasion in workers exposed to large dust particles, dental erosion in workers exposed to strong acids, caries in workers exposed to flour or sugar dust, etc.
The mouth may constitute the route of entry of toxic substances into the body either by accidental ingestion or by slow absorption. The surface area of the buccal mucous membranes is relatively small (in comparison with that of the respiratory system and gastro-intestinal system) and foreign substances will remain in contact with these membranes for only a short period. These factors considerably limit the degree of absorption even of substances which are highly soluble; nevertheless, the possibility of absorption does exist and is even exploited for therapeutic purposes (perlingual absorption of drugs).
The tissues of the buccal cavity may often be the site of accumulation of toxic substances, not only by direct and local absorption, but also by transport via the bloodstream. Research using radioactive isotopes has shown that even the tissues which seem metabolically the most inert (such as dental enamel and dentine) have a certain accumulative capacity and a relatively active turnover for certain substances. Classical examples of storage are various discolorations of the mucous membranes (gingival lines) which often provide valuable diagnostic information (e.g. lead).
Salivary excretion is of no value in the elimination of toxic substances from the body since the saliva is swallowed and the substances in it are once more absorbed into the system, thus forming a vicious circle. Salivary excretion has, on the other hand, a certain diagnostic value (determination of toxic substances in the saliva); it may also be of importance in the pathogenesis of certain lesions since the saliva renews and prolongs the action of toxic substances on the buccal mucous membrane. The following substances are excreted in the saliva: various heavy metals, the halogens (the concentration of iodine in the saliva may be 7-700 times greater than that in plasma), the thiocyanates (smokers, workers exposed to hydrocyanic acid and cyanogen compounds), and a wide range of organic compounds (alcohols, alkaloids, etc.).
Aetiopathogenesis and Clinical Classification
Lesions of the mouth and teeth (also called stomatological lesions) of occupational origin may be caused by:
- physical agents (acute traumata and chronic microtraumata, heat, electricity, radiations, etc.)
- chemical agents which affect the tissues of the buccal cavity directly or by means of systemic changes
- biological agents (viruses, bacteria, mycetes).
However, when dealing with mouth and teeth lesions of occupational origin, a classification based on topographical or anatomical location is preferred to one employing aetiopathogenic principles.
Lips and cheeks. Examination of the lips and cheeks may reveal: pallor due to anaemia (benzene, lead poisoning, etc.), cyanosis due to acute respiratory insufficiency (asphyxia) or chronic respiratory insufficiency (occupational diseases of the lungs), cyanosis due to methaemoglobinaemia (nitrites and organic nitro-compounds, aromatic amines), cherry-red colouring due to acute carbon monoxide poisoning, yellow colouring in cases of acute poisoning with picric acid, dinitrocresol, or in a case of hepatotoxic jaundice (phosphorus, chlorinated hydrocarbon pesticides, etc.). In argyrosis, there is brown or grey-bluish coloration caused by the precipitation of silver or its insoluble compounds, especially in areas exposed to light.
Occupational disorders of the lips include: dyskeratoses, fissures and ulcerations due to the direct action of caustic and corrosive substances; allergic contact dermatitis (nickel, chrome) which may also include the dermatitis found in tobacco industry workers; microbial eczemas resulting from the use of respiratory protective equipment where the elementary rules of hygiene have not been observed; lesions caused by anthrax and glanders (malignant pustules and cancroid ulcer) of workers in contact with animals; inflammation due to solar radiation and found among agricultural workers and fishermen; neoplastic lesions in persons handling carcinogenic substances; traumatic lesions; and chancre of the lip in glassblowers.
Teeth. Discoloration caused by the deposition of inert substances or due to the impregnation of the dental enamel by soluble compounds is of almost exclusively diagnostic interest. The important colourings are as follows: brown, due to the deposition of iron, nickel and manganese compounds; greenish-brown due to vanadium; yellowish-brown due to iodine and bromine; golden-yellow, often limited to gingival lines, due to cadmium.
Of greater importance is dental erosion of mechanical or chemical origin. Even nowadays it is possible to find dental erosions of mechanical origin in certain craftsmen (caused by holding nails or string, etc., in the teeth) which are so characteristic that they can be considered occupational stigmata. Lesions caused by abrasive dusts have been described in grinders, sandblasters, stone industry workers and precious stone workers. Prolonged exposure to organic and inorganic acids will often cause dental lesions occurring mainly on the labial surface of the incisors (rarely on the canines); these lesions are initially superficial and limited to the enamel but later become deeper and more extensive, reaching the dentine and resulting in solubilization and mobilization of calcium salts. The localization of these erosions to the anterior surface of the teeth is due to the fact that when the lips are open it is this surface which is the most exposed and which is deprived of the natural protection offered by the buffer effect of saliva.
Dental caries is such a frequent and widespread disease that a detailed epidemiological study is required to determine whether the condition is really of occupational origin. The most typical example is that of the caries found in workers exposed to flour and sugar dust (flourmillers, bakers, confectioners, sugar industry workers). This is a soft caries which develops rapidly; it starts at the base of the tooth (rampant caries) and immediately progresses to the crown; the affected sides blacken, the tissue is softened and there is considerable loss of substance and finally the pulp is affected. These lesions begin after a few years of exposure and their severity and extent increases with the duration of this exposure. X rays may also cause rapidly developing dental caries which usually commences at the base of the tooth.
In addition to pulpites due to dental caries and erosion, an interesting aspect of pulp pathology is barotraumatic odontalgia, i.e., pressure-induced toothache. This is caused by the rapid development of gas dissolved in the pulp tissue following sudden atmospheric decompression: this is a common symptom in the clinical manifestations observed during rapid climbing in aircrafts. In the case of persons suffering from septic-gangrenous pulpites, where gaseous material is already present, this toothache may commence at an altitude of 2,000-3,000 m.
Occupational fluorosis does not lead to dental pathology as is the case with endemic fluorosis: fluorine causes dystrophic changes (mottled enamel) only when the period of exposure precedes the eruption of permanent teeth.
Mucous membrane changes and stomatitis. Of definite diagnostic value are the various discolorations of the mucous membranes due to the impregnation or precipitation of metals and their insoluble compounds (lead, antimony, bismuth, copper, silver, arsenic). A typical example is Burton’s line in lead poisoning, caused by the precipitation of lead sulphide following the development in the oral cavity of hydrogen sulphide produced by the putrefaction of food residues. It has not been possible to reproduce Burton’s line experimentally in herbivorous animals.
There is a very curious discoloration in the lingual mucous membrane of workers exposed to vanadium. This is due to impregnation by vanadium pentoxide which is subsequently reduced to trioxide; the discoloration cannot be cleaned away but disappears spontaneously a few days after termination of exposure.
The oral mucous membrane can be the site of severe corrosive damage caused by acids, alkalis and other caustic substances. Alkalis cause maceration, suppuration and tissue necrosis with the formation of lesions which slough off easily. Ingestion of caustic or corrosive substances produces severe ulcerative and very painful lesions of the mouth, oesophagus and stomach, which may develop into perforations and frequently leave scars. Chronic exposure favours the formation of inflammation, fissures, ulcers and epithelial desquamation of the tongue, palate and other parts of the oral mucous membranes. Inorganic and organic acids have a coagulating effect on proteins and cause ulcerous, necrotic lesions which heal with contractive scarring. Mercury chloride and zinc chloride, certain copper salts, alkaline chromates, phenol and other caustic substances produce similar lesions.
A prime example of chronic stomatitis is that caused by mercury. It commences gradually, with discreet symptoms and a prolonged course; the symptoms include excessive saliva, metallic taste in the mouth, bad breath, slight gingival reddening and swelling, and these constitute the first phase of periodontitis leading towards loss of teeth. A similar clinical picture is found in stomatitis due to bismuth, gold, arsenic, etc.
Salivary glands. Increased salivary secretion has been observed in the following cases:
- in a variety of acute and chronic stomatites which is due mainly to the irritant action of the toxic substances and may, in certain cases, be extremely intense. For example, in cases of chronic mercurial poisoning, this symptom is so prominent and occurs at such an early stage that English workers have called this the “salivation disease”.
- in cases of poisoning in which there is central nervous system involvement—as is the case in manganese poisoning. However, even in the case of chronic mercurial poisoning, salivary gland hyperactivity is thought to be, at least in part, nervous in origin.
- in cases of acute poisoning with organophosphorus pesticides which inhibit cholinesterases.
There is reduction in salivary secretion in severe thermoregulation disorders (heatstroke, acute dinitrocresol poisoning), and in serious disorders of water and electrolyte balance during toxic hepatorenal insufficiency.
In cases of acute or chronic stomatitis, the inflammatory process may, sometimes, affect the salivary glands. In the past there have been reports of “lead parotitis”, but this condition has become so rare nowadays that doubts about its actual existence seem justified.
Maxillary bones. Degenerative, inflammatory and productive changes in the skeleton of the mouth may be caused by chemical, physical and biological agents. Probably the most important of the chemical agents is white or yellow phosphorus which causes phosphorus necrosis of the jaw or “phossy jaw”, at one time a distressing disease of match industry workers. The absorption of phosphorus is facilitated by the presence of gingival and dental lesions, and produces, initially, productive periosteal reaction followed by destructive and necrotic phenomena which are activated by bacterial infection. Arsenic also causes ulceronecrotic stomatitis which may have further bone complications. The lesions are limited to the roots in the jaw, and lead to the development of small sheets of dead bones. Once the teeth have fallen out and the dead bone eliminated, the lesions have a favourable course and nearly always heal.
Radium was the cause of maxillary osteonecrotic processes observed during the First World War in workers handling luminous compounds. In addition, damage to the bone may also be caused by infection.
Preventive Measures
A programme for the prevention of mouth and teeth diseases should be based on the following four main principles:
- application of measures of industrial hygiene and preventive medicine including monitoring of workplace environment, analysis of production processes, elimination of hazards in the environment, and, where necessary, the use of personal protective equipment
- education of workers in the need for scrupulous oral hygiene—in many cases it has been found that lack of oral hygiene may reduce resistance to general and localized occupational diseases
- a careful check on the mouth and teeth when workers undergo pre-employment or periodical medical examinations
- early detection and treatment of any mouth or teeth disease, whether of an occupational nature or not.
Liver
The liver acts as a vast chemical factory with diverse vital functions. It plays an essential role in the metabolism of protein, carbohydrate and fat, and is concerned with the absorption and storage of vitamins and with the synthesis of prothrombin and other factors concerned with blood clotting. The liver is responsible for the inactivation of hormones and the detoxification of many drugs and exogenous toxic chemical substances. It also excretes the breakdown products of haemoglobin, which are the principal constituents of the bile. These widely varying functions are performed by parenchymal cells of uniform structure which contain many complex enzyme systems.
Pathophysiology
An important feature of liver disease is a rise in the level of bilirubin in the blood; if of sufficient magnitude, this stains the tissues to give rise to jaundice. The mechanism of this process is shown in figure 1. Haemoglobin released from worn out red blood cells is broken down to haem and then, by removal of iron, to bilirubin before it reaches the liver (prehepatic bilirubin). In its passage through the liver cell, bilirubin is conjugated by enzymatic activity into water-soluble glucuronides (posthepatic bilirubin) and then secreted as bile into the intestine. The bulk of this pigment is eventually excreted in the stool, but some is reabsorbed through the intestinal mucosa and secreted a second time by the liver cell into the bile (enterohepatic circulation). However, a small proportion of this reabsorbed pigment is finally excreted in the urine as urobilinogen. With normal liver function there is no bilirubin in the urine, as prehepatic bilirubin is protein bound, but a small amount of urobilinogen is present.
Figure 1. The excretion of bilirubinthrough thte liver, showing the enterohepatic circulation.

Obstruction to the biliary system can occur in the bile ducts, or at cellular level by swelling of the hepatic cells due to injury, with resulting obstruction to the fine bile canaliculi. Posthepatic bilirubin then accumulates in the bloodstream to produce jaundice, and overflows into the urine. The secretion of bile pigment into the intestine is hindered, and urobilinogen is no longer excreted in the urine. The stools are therefore pale due to lack of pigment, the urine dark with bile, and the serum conjugated bilirubin raised above its normal value to give rise to obstructive jaundice.
Damage to the liver cell, which may follow injection of or exposure to toxic agents, also gives rise to an accumulation of posthepatic, conjugated bilirubin (hepatocellular jaundice). This may be sufficiently severe and prolonged to give rise to a transient obstructive picture, with bilirubin but no urobilinogen in the urine. However, in the early stages of hepatocellular damage, without obstruction present, the liver is unable to re-excrete reabsorbed bilirubin, and an excessive amount of urobilinogen is excreted in the urine.
When blood cells are broken down at an excessive rate, as in the haemolytic anaemias, the liver becomes overloaded and the unconjugated prehepatic bilirubin is raised. This again gives rise to jaundice. However, prehepatic bilirubin cannot be excreted in the urine. Excessive amounts of bilirubin are secreted into the intestine, rendering the faeces dark. More is reabsorbed via the enterohepatic circulation and an increased amount of urobilinogen excreted in the urine (haemolytic jaundice).
Diagnosis
Liver function tests are used to confirm suspected liver disease, to estimate progress and to assist in the differential diagnosis of jaundice. A series of tests is usually applied to screen the various functions of the liver, those of established value being:
- Examination of the urine for the presence of bilirubin and urobilinogen: The former is indicative of hepatocellular damage or of biliary obstruction. The presence of excessive urobilinogen can precede the onset of jaundice and forms a simple and sensitive test of minimal hepatocellular damage or of the presence of haemolysis.
- Estimation of total serum bilirubin: Normal value 5-17 mmol/l.
- Estimation of serum enzyme concentration: Hepatocellular damage is accompanied by a raised level of a number of enzymes, in particular of g-glutamyl transpeptidase, alanine amino-transferase (glutamic pyruvic transaminase) and aspartate amino-transferase (glutamic oxalo-acetic transaminase), and by a moderately raised level of alkaline phosphatase. An increasing level of alkaline phosphatase is indicative of an obstructive lesion.
- Determination of plasma protein concentration and electrophoretic pattern: Hepatocellular damage is accompanied by a fall in plasma albumin and a differential rise in the globulin fractions, in particular in g-globulin. These changes form the basis for the flocculation tests of liver function.
- Bromsulphthalein excretion test: This is a sensitive test of early cellular damage, and is of value in detecting its presence in the absence of jaundice.
- Immunological tests: Estimation of the levels of immunoglobulins and detection of autoantibodies is of value in the diagnosis of certain forms of chronic liver disease. The presence of hepatitis B surface antigen is indicative of serum hepatitis and the presence of alpha-fetoprotein suggests a hepatoma.
- Haemoglobin estimation, red cell indices and report on blood film.
Other tests used in the diagnosis of liver disease include scanning by means of ultrasound or radio-isotope uptake, needle biopsy for histological examination and peritoneoscopy. Ultrasound examination provides a simple, safe, non-invasive diagnostic technique but which requires skill in application.
Occupational disorders
Infections. Schistosomiasis is a widespread and serious parasitic infection which may give rise to chronic hepatic disease. The ova produce inflammation in the portal zones of the liver, followed by fibrosis. The infection is occupational where workers have to be in contact with water infested with the free-swimming cercariae.
Hydatid disease of the liver is common in sheep-raising communities with poor hygienic standards where people are in close contact with the dog, the definitive host, and sheep, the intermediate host for the parasite, Echinococcus granulosus. When a person becomes the intermediate host, a hydatid cyst may form in the liver giving rise to pain and swelling, which may be followed by infection or rupture of the cyst.
Weil’s disease may follow contact with water or damp earth contaminated by rats harbouring the causative organism, Leptospira icterohaemorrhagiae. It is an occupational disease of sewer workers, miners, workers in rice-fields, fishmongers and butchers. The development of jaundice some days after the onset of fever forms only one stage of a disease which also involves the kidney.
A number of viruses give rise to hepatitis, the most common being virus type A (HAV) causing acute infective hepatitis and virus type B (HBV) or serum hepatitis. The former, which is responsible for world-wide epidemics, is spread by the faecal-oral route, is characterized by febrile jaundice with liver cell injury and is usually followed by recovery. Type B hepatitis is a disease with a more serious prognosis. The virus is readily transmitted following skin or venipuncture, or transfusion with infected blood products and has been transmitted by drug addicts using the parenteral route, by sexual, especially homosexual contact or by any close personal contact, and also by blood-sucking arthropods. Epidemics have occurred in dialysis and organ transplant units, laboratories and hospital wards. Patients on haemodialysis and those in oncology units are particularly liable to become chronic carriers and hence provide a reservoir of infection. The diagnosis can be confirmed by the identification of an antigen in the serum originally called Australia antigen but now termed hepatitis B surface antigen HBsAg. Serum containing the antigen is highly infectious. Type B hepatitis is an important occupational hazard for health care personnel, especially for those working in clinical laboratories and on dialysis units. High levels of serum positivity have been found in pathologists and surgeons, but low in doctors without patient contact. There is also a hepatitis virus non-A, non-B, identified as hepatitis virus C (HCV). Other hepatitis virus types are likely to be still unidentified. The delta virus cannot cause hepatitis independently but it acts in conjunction with the hepatitis B virus. Chronic virus hepatitis is an important aetiology of liver cirrhosis and cancer (malignant hepatoma).
Yellow fever is an acute febrile illness resulting from infection with a Group B arbovirus transmitted by culicine mosquitoes, in particular Aedes aegypti. It is endemic in many parts of West and Central Africa, in tropical South America and some parts of the West Indies. When jaundice is prominent, the clinical picture resembles infective hepatitis. Falciparum malaria and relapsing fever may also give rise to high fever and jaundice and require careful differentiation.
Toxic conditions. Excessive red blood cell destruction giving rise to haemolytic jaundice may result from exposure to arsine gas, or the ingestion of haemolytic agents such as phenylhydrazine. In industry, arsine may be formed whenever nascent hydrogen is formed in the presence of arsenic, which may be an unsuspected contaminant in many metallurgical processes.
Many exogenous poisons interfere with liver-cell metabolism by inhibiting enzyme systems, or may damage or even destroy the parenchymal cells, interfering with the excretion of conjugated bilirubin and giving rise to jaundice. The injury caused by carbon tetrachloride may be taken as a model for direct hepatotoxicity. In mild cases of poisoning, dyspeptic symptoms may be present without jaundice, but liver damage is indicated by the presence of excess urobilinogen in the urine, raised serum amino-transferase (transaminase) levels and impaired bromsulphthalein excretion. In more severe cases the clinical features resemble those of acute infective hepatitis. Loss of appetite, nausea, vomiting and abdominal pain are followed by a tender, enlarged liver and jaundice, with pale stools and dark urine. An important biochemical feature is the high level of serum amino-transferase (transaminase) found in these cases. Carbon tetrachloride has been widely used in dry cleaning, as a constituent of fire extinguishers and as an industrial solvent.
Many other halogenated hydrocarbons have similar hepatotoxic properties. Those of the aliphatic series which damage the liver are methyl chloride, tetrachloroethane, and chloroform. In the aromatic series the nitrobenzenes, dinitrophenol, trinitrotoluene and rarely toluene, the chlorinated naphthalenes and chlorinated diphenyl may be hepatotoxic. These compounds are used variously as solvents, degreasers and refrigerants, and in polishes, dyes and explosives. While exposure may produce parenchymal cell damage with an illness not dissimilar to infectious hepatitis, in some cases (e.g., following exposure to trinitrotoluene or tetrachlorethane) the symptoms may become severe with high fever, rapidly increasing jaundice, mental confusion and coma with a fatal termination from massive necrosis of the liver.
Yellow phosphorus is a highly poisonous metalloid whose ingestion gives rise to jaundice which may have a fatal termination. Arsenic, antimony and ferrous iron compounds may also give rise to liver damage.
Exposure to vinyl chloride in the polymerization process for the production of polyvinyl chloride has been associated with the development of hepatic fibrosis of a non-cirrhotic type together with splenomegaly and portal hypertension. Angiosarcoma of the liver, a rare and highly malignant tumour developed in a small number of exposed workers. Exposure to vinyl chloride monomer, in the 40-odd years preceding the recognition of angiosarcoma in 1974, had been high, especially in men engaged in the cleaning of the reaction vessels, in whom most of the cases occurred. During that period the TLV for vinyl chloride was 500 ppm, subsequently reduced to 5 ppm (10 mg/m3). While liver damage was first reported in Russian workers in 1949, attention was not paid to the harmful effects of vinyl chloride exposure until the discovery of Raynaud’s syndrome with sclerodermatous changes and acro-osteolysis in the 1960s.
Hepatic fibrosis in vinyl chloride workers can be occult, for as parenchymal liver function can be preserved, conventional liver function tests may show no abnormality. Cases have come to light following haematemesis from the associated portal hypertension, the discovery of thrombocytopoenia associated with splenomegaly or the development of angiosarcoma. In surveys of vinyl chloride workers, a full occupational history including information on alcohol and drug consumption should be taken, and the presence of hepatitis B surface antigen and antibody determined. Hepatosplenomegaly may be detected clinically, by radiography or more precisely by grey scale ultrasonography. The fibrosis in these cases is of a periportal type, with a mainly presinusoidal obstruction to portal flow, attributed to an abnormality of the portal vein radicles or the hepatic sinusoids and giving rise to portal hypertension. The favourable progress of workers who have undergone portocaval shunt operations following haematemesis is likely to be attributed to the sparing of the liver parenchymal cells in this condition.
Fewer than 200 cases of angiosarcoma of the liver which fulfil current diagnostic criteria have been reported. Less than half of these have occurred in vinyl chloride workers, with an average duration of exposure of 18 years, range 4-32 years. In Britain, a register set up in 1974 has collected 34 cases with acceptable diagnostic criteria. Two of these occurred in vinyl chloride workers, with possible exposure in four others, eight were attributable to past exposure to thorotrast and one to arsenical medication. Thorium dioxide, used in the past as a diagnostic aid, is now responsible for new cases of angiosarcoma and hepatoma. Chronic arsenic intoxication, following medication or as an occupational disease among vintners in the Moselle has also been followed by angiosarcoma. Non-cirrhotic perisinusoidal fibrosis has been observed in chronic arsenic intoxication, as in vinyl chloride workers.
Aflatoxin, derived from a group of moulds, in particular Aspergillus flavus, gives rise to liver cell damage, cirrhosis and liver cancer in experimental animals. The frequent contamination of cereal crops, particularly on storage in warm, humid conditions, with A. flavus, may explain the high incidence of hepatoma in certain parts of the world, especially in tropical Africa. In industrialized countries hepatoma is uncommon, more often developing in cirrhotic livers. In a proportion of cases HBsAg antigen has been present in the serum and some cases have followed treatment with androgens. Hepatic adenoma has been observed in women taking certain oral contraceptive formulations.
Alcohol and cirrhosis. Chronic parenchymal liver disease may take the form of chronic hepatitis or of cirrhosis. The latter condition is characterized by cellular damage, fibrosis and nodular regeneration. While in many cases the aetiology is unknown, cirrhosis may follow viral hepatitis, or acute massive necrosis of the liver, which itself may result from drug ingestion or industrial chemical exposure. Portal cirrhosis is frequently associated with excessive alcohol consumption in industrialized countries such as France, Britain and the United States, although multiple risk factors may be involved to explain variation in susceptibility. While its mode of action is unknown, liver damage is primarily dependent on the amount and duration of drinking. Workers who have easy access to alcohol are at greatest risk of developing cirrhosis. Among the occupations with the highest mortality from cirrhosis are bartenders and publicans, restaurateurs, seafarers, company directors and medical practitioners.
Fungi. Mushrooms of the amanita species (e.g., Amanita phalloides) are highly toxic. Ingestion is followed by gastro-intestinal symptoms with watery diarrhoea and after an interval by acute liver failure due to centrizonal necrosis of the parenchyma.
Drugs. A careful drug history should always be taken before attributing liver damage to an industrial exposure, for a variety of drugs are not only hepatotoxic, but are capable of enzyme induction which may alter the liver’s response to other exogenous agents. Barbiturates are potent inducers of liver microsomal enzymes, as are some food additives and DDT.
The popular analgesic acetaminophen (paracetamol) gives rise to hepatic necrosis when taken in overdose. Other drugs with a predictable dose-related direct toxic action on the liver cell are hycanthone, cytotoxic agents and tetracyclines (though much less potent). Several antituberculous drugs, in particular isoniazid and para-aminosalicylic acid, certain monoamine oxidase inhibitors and the anaesthetic gas halothane may also be hepatotoxic in some hypersensitive individuals.
Phenacetin, sulphonamides and quinine are examples of drugs which may give rise to a mild haemolytic jaundice, but again in hypersensitive subjects. Some drugs may give rise to jaundice, not by damaging the liver cell, but by damaging the fine biliary ducts between the cells to give rise to biliary obstruction (cholestatic jaundice). The steroid hormones methyltestosterone and other C-17 alkyl-substituted compounds of testosterone are hepatotoxic in this way. It is important to determine, therefore, whether a female worker is taking an oral contraceptive in the evaluation of a case of jaundice. The epoxy resin hardener 4,4´-diamino-diphenylmethane led to an epidemic of cholestatic jaundice in England following ingestion of contaminated bread.
Several drugs have given rise to what appears to be a hypersensitive type of intrahepatic cholestasis, as it is not dose related. The phenothiazine group, and in particular chlorpromazine are associated with this reaction.
Preventive Measures
Workers who have any disorder of the liver or gall bladder, or a past history of jaundice, should not handle or be exposed to potentially hepatotoxic agents. Similarly, those who are receiving any drug which is potentially injurious to the liver should not be exposed to other hepatic poisons, and those who have received chloroform or trichlorethylene as an anaesthetic should avoid exposure for a subsequent interval. The liver is particularly sensitive to injury during pregnancy, and exposure to potentially hepatotoxic agents should be avoided at this time. Workers who are exposed to potentially hepatotoxic chemicals should avoid alcohol. The general principle to be observed is the avoidance of a second potentially hepatotoxic agent where there has to be exposure to one. A balanced diet with an adequate intake of first class protein and essential food factors affords protection against the high incidence of cirrhosis seen in some tropical countries. Health education should stress the importance of moderation in the consumption of alcohol in protecting the liver from fatty infiltration and cirrhosis. The maintenance of good general hygiene is invaluable in protecting against infections of the liver like hepatitis, hydatid disease and schistosomiasis.
Control measures for type B hepatitis in hospitals include precautions in the handling of blood samples in the ward; adequate labelling and safe transmission to the laboratory; precautions in the laboratory, with the prohibition of mouth pipetting; the wearing of protective clothing and disposable gloves; prohibition of eating, drinking or smoking in areas where infectious patients or blood samples might be handled; extreme care in the servicing of non-disposable dialysis equipment; surveillance of patients and staff for hepatitis and mandatory screening at intervals for the presence of HBsAg antigen. Vaccination against hepatitis A and B viruses is an efficient method to prevent infection in high risk occupations.
Peptic Ulcer
Gastric and duodenal ulcers—collectively called “peptic ulcers”—are a sharply circumscribed loss of tissue, involving the mucosa, submucosa and muscular layer, occurring in areas of the stomach or duodenum exposed to acid-pepsin gastric juice. Peptic ulcer is a common cause of recurring or persistent upper abdominal distress, especially in young men. Duodenal ulcer comprises about 80% of all peptic ulcers, and is commoner in men than in women; in gastric ulcer the gender ratio is about one. It is important to distinguish between gastric ulcer and duodenal ulcer because of differences in diagnosis, treatment and prognosis. The causes of peptic ulcer have not been completely determined; many factors are believed to be involved, and in particular nervous tension, the ingestion of certain drugs (such as salicylates and corticoids) and hormonal factors may play roles.
Persons at Risk
Although peptic ulcer cannot be regarded as a specific occupational disease, it has a higher-than-average incidence among professional people and those working under stress. Stress, either physical or emotional, is believed to be an important factor in the aetiology of peptic ulcer; prolonged emotional stress in various occupations may increase the secretion of hydrochloric acid and the susceptibility of the gastroduodenal mucosa to injury.
The results of many investigations of the relationship between peptic ulcer and occupation clearly reveal substantial variations in the incidence of ulcers in different occupations. Numerous studies point to the likelihood of transport workers, such as drivers, motor mechanics, tramcar conductors and railway employees, contracting ulcers. Thus, in one survey covering over 3,000 railway workers, peptic ulcers were found to be more frequent in train crew, signal operators and inspectors than in maintenance and administrative staff; shift work, hazards and responsibility being noted as contributing factors. In another large-scale survey, however, transport workers evidenced “normal” ulcer rates, the incidence being highest in doctors and a group of unskilled workers. Fishers and sea pilots also tend to suffer from peptic ulcer, predominantly of the gastric type. In a study of coal miners, the incidence of peptic ulcers was found to be proportional to the arduousness of the work, being highest in miners employed at the coal face. Reports of cases of peptic ulcer in welders and in workers in a magnesium refining plant suggest that metal fumes are capable of inducing this condition (although here the cause would appear to be not stress, but a toxic mechanism). Elevated incidences have also been found among overseers and business executives, i.e., generally in persons holding responsible posts in industry or trade; it is noteworthy that duodenal ulcers account almost exclusively for the high incidence in these groups, the incidence of gastric ulcer being average.
On the other hand, low incidences of peptic ulcer have been found among agricultural workers, and apparently prevail among sedentary workers, students and draftsmen.
Thus, while the evidence regarding the occupational incidence of peptic ulcer appears to be contradictory to a degree, there is agreement at least on one point, namely that the higher the stresses of the occupation, the higher the ulcer rate. This general relationship can also be observed in the developing countries, where, during the process of industrialization and modernization, many workers are coming increasingly under the influence of stress and strain, caused by such factors as congested traffic and difficult commuting conditions, introduction of complex machinery, systems and technologies, heavier workloads and longer working hours, all of which are found to be conducive to the development of peptic ulcer.
Diagnosis
The diagnosis of peptic ulcer depends upon obtaining a history of characteristic ulcer distress, with relief of distress on ingestion of food or alkali, or other manifestations such as gastro-intestinal bleeding; the most useful diagnostic technique is a thorough x-ray study of the upper gastro-intestinal tract.
Attempts to gather data on the prevalence of this condition have been seriously hampered by the fact that peptic ulcer is not a reportable disease, that workers with peptic ulcer frequently put off consulting a physician about their symptoms, and that when they do so, the criteria for diagnosis are not uniform. The detection of peptic ulcer in workers is, therefore, not simple. Some excellent researchers, indeed, have had to rely on attempts to gather data from necropsy records, questionnaires to physicians, and insurance company statistics.
Preventive Measures
From the viewpoint of occupational medicine, the prevention of peptic ulcer—seen as a psychosomatic ailment with occupational connotations—must be based primarily on the alleviation, wherever possible, of overstress and nervous tension due to directly or indirectly work-related factors. Within the broad framework of this general principle, there is room for a wide variety of measures, including, for example, action on the collective plane towards a reduction of working hours, the introduction or improvement of facilities for rest and relaxation, improvements in financial conditions and social security, and (hand in hand with local authorities) steps to improve commuting conditions and make suitable housing available within a reasonable distance of workplaces—not to mention direct action to pinpoint and eliminate particular stress-generating situations in the working environment.
At the personal level, successful prevention depends equally on proper medical guidance and on intelligent cooperation by the worker, who should have an opportunity of seeking advice on work-connected and other personal problems.
The liability of individuals to contract peptic ulcers is heightened by various occupational factors and personal attributes. If these factors can be recognized and understood, and above all, if the reasons for the apparent correlation between certain occupations and high ulcer rates can be clearly demonstrated, the chances of successful prevention, and treatment of relapses, will be greatly enhanced. A possible Helicobacter infection should also be eradicated. In the meantime, as a general precaution, the implications of a past history of peptic ulcer should be borne in mind by persons conducting pre-employment or periodic examinations, and efforts should be made not to place—or to leave—the workers concerned in jobs or situations where they will be exposed to severe stresses, particularly of a nervous or psychological nature.
More...
Liver Cancer
The predominant type of malignant tumour of the liver (ICD-9 155) is hepatocellular carcinoma (hepatoma; HCC), i.e., a malignant tumour of the liver cells. Cholangiocarcinomas are tumours of the intrahepatic bile ducts. They represent some 10% of liver cancers in the US but may account for up to 60% elsewhere, such as in north-eastern Thai populations (IARC 1990). Angiosarcomas of the liver are very rare and very aggressive tumours, occurring mostly in men. Hepatoblastomas, a rare embryonal cancer, occur in early life, and have little geographic or ethnic variation.
The prognosis for HCC depends on the size of the tumour and on the extent of cirrhosis, metastases, lymph node involvement, vascular invasion and presence/absence of a capsule. They tend to relapse after resection. Small HCCs are resectable, with a five-year survival of 40-70%. Liver transplantation results in about 20% survival after two years for patients with advanced HCC. For patients with less advanced HCC, the prognosis after transplantation is better. For hepatoblastomas, complete resection is possible in 50-70% of the children. Cure rates after resection range from 30-70%. Chemotherapy can be used both pre- and postoperatively. Liver transplantation may be indicated for unresectable hepatoblastomas.
Cholangiocarcinomas are multifocal in more than 40% of the patients at the time of diagnosis. Lymph node metastases occur in 30-50% of these cases. The response rates to chemotherapy vary widely, but usually are less than 20% successful. Surgical resection is possible in only a few patients. Radiation therapy has been used as the primary treatment or adjuvant therapy, and may improve survival in patients who have not undergone a complete resection. Five-year survival rates are less than 20%. Angiosarcoma patients usually present distant metastases. Resection, radiation therapy, chemotherapy and liver transplantation are, in most cases, unsuccessful. Most patients die within six months of diagnosis (Lotze, Flickinger and Carr 1993).
An estimated 315,000 new cases of liver cancer occurred globally in 1985, with a clear absolute and relative preponderance in populations of developing countries, except in Latin America (IARC 1994a; Parkin, Pisani and Ferlay 1993). The average annual incidence of liver cancer shows considerable variation across cancer registries worldwide. During the 1980s, average annual incidence ranged from 0.8 in men and 0.2 in women in Maastricht, The Netherlands, to 90.0 in men and 38.3 in women in Khon Kaen, Thailand, per 100,000 of population, standardized to the standard world population. China, Japan, East Asia, and Africa represented high rates, while Latin and North American, European, and Oceanian rates were lower, except for New Zealand Maoris (IARC 1992). The geographic distribution of liver cancer is correlated with the distribution of the prevalence of chronic carriers of hepatitis B surface antigen and also with the distribution of local levels of aflatoxin contamination of foodstuffs (IARC 1990). Male-to-female ratios in incidence are usually between 1 and 3, but may be higher in high-risk populations.
Statistics on the mortality and incidence of liver cancer by social class indicate a tendency of excess risk to concentrate in the lower socio-economic strata, but this gradient is not observed in all populations.
The established risk factors for primary liver cancer in humans include aflatoxin-contaminated food, chronic infection with hepatitis B virus (IARC 1994b), chronic infection with hepatitis C virus (IARC 1994b), and heavy consumption of alcoholic beverages (IARC 1988). HBV is responsible for an estimated 50-90% of hepatocellular carcinoma incidence in high-risk populations, and for 1-10% in low-risk populations. Oral contraceptives are a further suspected factor. The evidence implicating tobacco smoking in the aetiology of liver cancer is insufficient (Higginson, Muir and Munoz 1992).
The substantial geographical variation in the incidence of liver cancer suggests that a high proportion of liver cancers might be preventable. The preventive measures include HBV vaccination (estimated potential theoretical reduction in incidence is roughly 70% in endemic areas), reduction of contamination of food by mycotoxins (40% reduction in endemic areas), improved methods of harvesting, dry storing of crops, and reduction of consumption of alcoholic beverages (15% reduction in Western countries; IARC 1990).
Liver cancer excesses have been reported in a number of occupational and industrial groups in different countries. Some of the positive associations are readily explained by workplace exposures such as the increased risk of liver angiosarcoma in vinyl chloride workers (see below). For other high-risk jobs, such as metal work, construction painting, and animal feed processing, the connection with workplace exposures is not firmly established and is not found in all studies, but could well exist. For others, such as service workers, police officers, guards, and governmental workers, direct workplace carcinogens may not explain the excess. Cancer data for farmers do not provide many clues for occupational aetiologies in liver cancer. In a review of 13 studies involving 510 cases or deaths of liver cancer among farmers (Blair et al. 1992), a slight deficit (aggregated risk ratio 0.89; 95% confidence interval 0.81-0.97) was observed.
Some of the clues provided by industry- or job-specific epidemiological studies do suggest that occupational exposures may have a role in the induction of liver cancer. Minimization of certain occupational exposures therefore would be instrumental in the prevention of liver cancer in occupationally exposed populations. As a classical example, occupational exposure to vinyl chloride has been shown to cause angiosarcoma of the liver, a rare form of liver cancer (IARC 1987). As a result, vinyl chloride exposure has been regulated in a large number of countries. There is increasing evidence that chlorinated hydrocarbon solvents may cause liver cancer. Aflatoxins, chlorophenols, ethylene glycol, tin compounds, insecticides and some other agents have been associated with the risk of liver cancer in epidemiological studies. Numerous chemical agents occurring in occupational settings have caused liver cancer in animals and may therefore be suspected of being liver carcinogens in humans. Such agents include aflatoxins, aromatic amines, azo dyes, benzidine-based dyes, 1,2-dibromoethane, butadiene, carbon tetrachloride, chlorobenzenes, chloroform, chlorophenols, diethylhexyl phthalate, 1,2-dichloroethane, hydrazine, methylene chloride, N-nitrosoamines, a number of organochlorine pesticides, perchloroethylene, polychlorinated biphenyls and toxaphene.
Pancreatic Cancer
Pancreatic cancer (ICD-9 157; ICD-10 C25), a highly fatal malignancy, ranks amongst the 15 most common cancers globally but belongs to the ten most common cancers in the populations of developed countries, accounting for 2 to 3% of all new cases of cancer (IARC 1993). An estimated 185,000 new cases of pancreatic cancer occurred globally in 1985 (Parkin, Pisani and Ferlay 1993). The incidence rates of pancreatic cancer have been increasing in developed countries. In Europe, the increase has levelled off, except in the UK and some Nordic countries (Fernandez et al. 1994). The incidence and mortality rates rise steeply with advancing age between 30 and 70 years. The age-adjusted male/female ratio of new cases of pancreatic cancer is 1.6/1 in developed countries but only 1.1/1 in developing countries.
High annual incidence rates of pancreatic cancer (up to 30/100,000 for men; 20/100,000 for women) in the period 1960-85, have been recorded for New Zealand Maoris, Hawaiians, and in Black populations in the US. Regionally, the highest age-adjusted rates in 1985 (over 7/100,000 for men and 4/100,000 in women) were reported for both genders in Japan, North America, Australia, New Zealand, and Northern, Western and Eastern Europe. The lowest rates (up to 2/100,000 for both men and women) were reported in the regions of West and Middle Africa, South-eastern Asia, Melanesia, and in temperate South America (IARC 1992; Parkin, Pisani and Ferlay 1993).
Comparisons between populations in time and space are subject to several cautions and interpretation difficulties because of variations in diagnostic conventions and technologies (Mack 1982).
The vast majority of pancreatic cancers occur in the exocrine pancreas. The major symptoms are abdominal and back pain and weight loss. Further symptoms include anorexia, diabetes and obstructive jaundice. Symptomatic patients are subjected to procedures such as a series of blood and urine tests, ultrasound, computerized tomography, cytological examination and pancreatoscopy. Most patients have metastases at diagnosis, which makes their prognosis bleak.
Only 15% of patients with pancreatic cancer are operable. Local recurrence and distant metastases occur frequently after surgery. Irradiation therapy or chemotherapy do not bring about significant improvements in survival except when combined with surgery on localized carcinomas. Palliative procedures provide little benefit. Despite some diagnostic improvements, survival remains poor. During the period 1983-85, the five-year average survival in 11 European populations was 3% for men and 4% for women (IARC 1995). Very early detection and diagnosis or identification of high-risk individuals may improve the success of surgery. The efficacy of screening for pancreatic cancer has not been determined.
Mortality and incidence of pancreatic cancer do not reveal a consistent global pattern across socio-economic categories.
The dismal picture offered by diagnostic problems and treatment inefficacy is completed by the fact that the causes of pancreatic cancer are largely unknown, which effectively hampers the prevention of this fatal disease. The unique established cause of pancreatic cancer is tobacco smoking, which explains about 20-50% of the cases, depending on the smoking patterns of the population. It has been estimated that elimination of tobacco smoking would decrease the incidence of pancreatic cancer by about 30% worldwide (IARC 1990). Alcohol consumption and coffee drinking have been suspected as increasing the risk of pancreatic cancer. On closer scrutiny of the epidemiological data, however, coffee consumption appears unlikely to be causally connected to pancreatic cancer. For alcoholic beverages, the only causal link with pancreatic cancer is probably pancreatitis, a condition associated with heavy alcohol consumption. Pancreatitis is a rare but potent risk factor of pancreatic cancer. It is possible that some as yet unidentified dietary factors might account for a part of the aetiology of pancreatic cancer.
Workplace exposures may be causally associated with pancreatic cancer. Results of several epidemiological studies that have linked industries and jobs with an excess of pancreatic cancer are heterogeneous and inconsistent, and exposures shared by alleged high-risk jobs are hard to identify. The population aetiologic fraction for pancreatic cancer from occupational exposures in Montreal, Canada, has been estimated to lie between 0% (based on recognized carcinogens) and 26% (based on a multi-site case-control study in the Montreal area, Canada) (Siemiatycki et al. 1991).
No single occupational exposure has been confirmed to increase the risk of pancreatic cancer. Most of the occupational chemical agents that have been associated with an excess risk in epidemiological studies emerged in one study only, suggesting that many of the associations may be artefacts from confounding or chance. If no additional information, e.g., from animal bio-assays, is available, the distinction between spurious and causal associations presents formidable difficulties, given the general uncertainty about the causative agents involved in the development of pancreatic cancer. Agents associated with increased risk include aluminium, aromatic amines, asbestos, ashes and soot, brass dust, chromates, combustion products of coal, natural gas and wood, copper fumes, cotton dust, cleaning agents, grain dust, hydrogen fluoride, inorganic insulation dust, ionizing radiation, lead fumes, nickel compounds, nitrogen oxides, organic solvents and paint thinners, paints, pesticides, phenol-formaldehyde, plastic dust, polycyclic aromatic hydrocarbons, rayon fibres, stainless steel dust, sulphuric acid, synthetic adhesives, tin compounds and fumes, waxes and polishes, and zinc fumes (Kauppinen et al. 1995). Among these agents, only aluminium, ionizing radiation and unspecified pesticides have been associated with excess risk in more than one study.
Work and Mental Health
This chapter provides an overview of major types of mental health disorder that can be associated with work—mood and affective disorders (e.g., dissatisfaction), burnout, post-traumatic stress disorder (PTSD), psychoses, cognitive disorders and substance abuse. The clinical picture, available assessment techniques, aetiological agents and factors, and specific prevention and management measures will be provided. The relationship with work, occupation or branch of industry will be illustrated and discussed where possible.
This introductory article first will provide a general perspective on occupational mental health itself. The concept of mental health will be elaborated upon, and a model will be presented. Next, we will discuss why attention should be paid to mental (ill) health and which occupational groups are at greatest risk. Finally, we will present a general intervention framework for successfully managing work-related mental health problems.
What Is Mental Health: A Conceptual Model
There are many different views about the components and processes of mental health. The concept is heavily value laden, and one definition is unlikely to be agreed upon. Like the strongly associated concept of “stress”, mental health is conceptualized as:
- a state—for example, a state of total psychological and social well-being of an individual in a given sociocultural environment, indicative of positive moods and affects (e.g., pleasure, satisfaction and comfort) or negative ones (e.g., anxiety, depressive mood and dissatisfaction).
- a process indicative of coping behaviour—for example, striving for independence, being autonomous (which are key aspects of mental health).
- the outcome of a process—a chronic condition resulting either from an acute, intense confrontation with a stressor, such as is the case in a post-traumatic stress disorder, or from the continuing presence of a stressor which may not necessarily be intense. This is the case in burnout, as well as in psychoses, major depressive disorders, cognitive disorders and substance abuse. Cognitive disorders and substance abuse are, however, often considered as neurological problems, since pathophysiological processes (e.g., degeneration of the myelin sheath) resulting from ineffective coping or from the stressor itself (alcohol use or occupational exposition to solvents, respectively) can underlie these chronic conditions.
Mental health may also be associated with:
- Person characteristics like “coping styles”—competence (including effective coping, environmental mastery and self-efficacy) and aspiration are characteristic of a mentally healthy person, who shows interest in the environment, engages in motivational activity and seeks to extend him- or herself in ways that are personally significant.
Thus, mental health is conceptualized not only as a process or outcome variable, but also as an independent variable—that is, as a personal characteristic that influences our behaviour.
In figure 1 a mental health model is presented. Mental health is determined by environmental characteristics, both in and outside the work situation, and by characteristics of the individual. Major environmental job characteristics are elaborated upon in the chapter “Psychosocial and organizational factors”, but some points on these environmental precursors of mental (ill) health have to be made here as well.
Figure 1. A model for mental health.
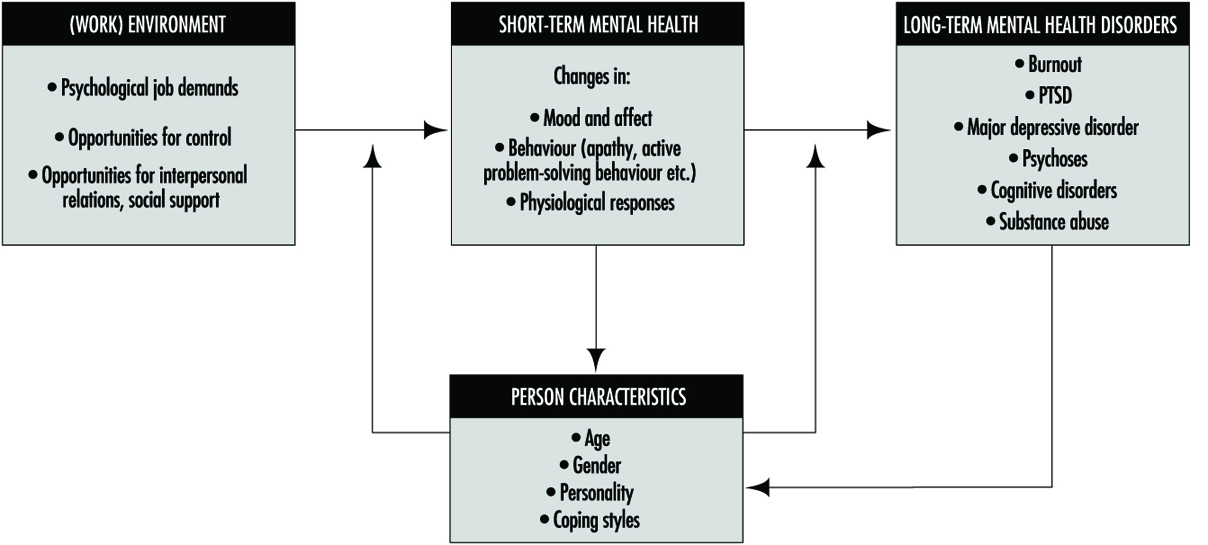
There are many models, most of them stemming from the field of work and organizational psychology, that identify precursors of mental ill health. These precursors are often labelled “stressors”. Those models differ in their scope and, related to this, in the number of stressor dimensions identified. An example of a relatively simple model is that of Karasek (Karasek and Theorell 1990), describing only three dimensions: psychological demands, decision latitude (incorporating skill discretion and decision authority) and social support. A more elaborate model is that of Warr (1994), with nine dimensions: opportunity for control (decision authority), opportunity for skill use (skill discretion), externally generated goals (quantitative and qualitative demands), variety, environmental clarity (information about consequences of behaviour, availability of feedback, information about the future, information about required behaviour), availability of money, physical security (low physical risk, absence of danger), opportunity for interpersonal contact (prerequisite for social support), and valued social position (cultural and company evaluations of status, personal evaluations of significance). From the above it is clear that the precursors of mental (ill) health are generally psychosocial in nature, and are related to work content, as well as working conditions, conditions of employment and (formal and informal) relationships at work.
Environmental risk factors for mental (ill) health generally result in short-term effects such as changes in mood and affect, like feelings of pleasure, enthusiasm or a depressed mood. These changes are often accompanied by changes in behaviour. We may think of restless behaviour, palliative coping (e.g., drinking) or avoiding, as well as active problem-solving behaviour. These affects and behaviours are generally accompanied by physiological changes as well, indicative of arousal and sometimes also of a disturbed homeostasis. When one or more of these stressors remains active, the short-term, reversible responses may result in more stable, less reversible mental health outcomes like burnout, psychoses or major depressive disorder. Situations that are extremely threatening may even immediately result in chronic mental health disorders (e.g., PTSD) which are difficult to reverse.
Person characteristics may interact with psychosocial risk factors at work and exacerbate or buffer their effects. The (perceived) coping ability may not only moderate or mediate the effects of environmental risk factors, but may also determine the appraisal of the risk factors in the environment. Part of the effect of the environmental risk factors on mental health results from this appraisal process.
Person characteristics (e.g., physical fitness) may not only act as precursors in the development of mental health, but may also change as a result of the effects. Coping ability may, for example, increase as the coping process progresses successfully (“learning”). Long-term mental health problems will, on the other hand, often reduce coping ability and capacity in the long run.
In occupational mental health research, attention has been particularly directed to affective well-being—factors such as job satisfaction, depressive moods and anxiety. The more chronic mental health disorders, resulting from long-term exposure to stressors and to a greater or lesser extent also related to personality disorders, have a much lower prevalence in the working population. These chronic mental health problems have a multitude of causal factors. Occupational stressors will consequently be only partly responsible for the chronic condition. Also, people suffering from these kinds of chronic problem will have great difficulty in maintaining their position at work, and many are on sick leave or have dropped out of work for quite a long period of time (1 year), or even permanently. These chronic problems, therefore, are often studied from a clinical perspective.
Since, in particular, affective moods and affects are so frequently studied in the occupational field, we will elaborate on them a little bit more. Affective well-being has been treated both in a rather undifferentiated way (ranging from feeling good to feeling bad), as well as by considering two dimensions: “pleasure” and “arousal” (figure 2). When variations in arousal are uncorrelated with pleasure, these variations alone are generally not considered to be an indicator of well-being.
Figure 2. Three principal axes for the measurement of affective well-being.
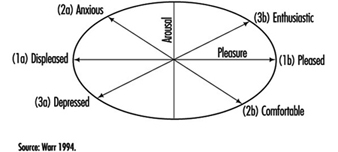
When, however, arousal and pleasure are correlated, four quadrants can be distinguished:
- Highly aroused and pleased indicates enthusiasm.
- Low aroused and pleased indicates comfort.
- Highly aroused and displeased indicates anxiety.
- Low aroused and displeased indicates depressed mood (Warr 1994).
Well-being can be studied at two levels: a general, context-free level and a context-specific level. The work environment is such a specific context. Data analyses support the general notion that the relation between job characteristics and context-free, non-work mental health is mediated by an effect on work-related mental health. Work-related affective well-being has commonly been studied along the horizontal axis (Figure 2) in terms of job satisfaction. Affects related to comfort in particular have, however, largely been ignored. This is regrettable, since this affect might indicate resigned job satisfaction: people may not complain about their jobs, but may still be apathetic and uninvolved (Warr 1994).
Why Pay Attention to Mental Health Issues?
There are several reasons that illustrate the need for attention to mental health issues. First of all, national statistics of several countries indicate that a lot of people drop out of work because of mental health problems. In the Netherlands, for example, for one-third of those employees who are diagnosed as disabled for work each year, the problem is related to mental health. The majority of this category, 58%, is reported to be work related (Gründemann, Nijboer and Schellart 1991). Together with musculoskeletal problems, mental health problems account for about two-thirds of those who drop out for medical reasons each year.
Mental ill health is an extensive problem in other countries as well. According to the Health and Safety Executive Booklet, it has been estimated that 30 to 40% of all sickness absence from work in the UK is attributable to some form of mental illness (Ross 1989; O’Leary 1993). In the UK, it has been estimated that one in five of the working population suffers each year from some form of mental illness. It is difficult to be precise about the number of working days lost each year because of mental ill health. For the UK, a figure of 90 million certified days—or 30 times that lost as a result of industrial disputes—is widely quoted (O’Leary 1993). This compares with 8 million days lost as a result of alcoholism and drink-related diseases and 35 million days as a result of coronary heart disease and strokes.
Apart from the fact that mental ill health is costly, both in human and financial terms, there is a legal framework provided by the European Union (EU) in its framework directive on health and safety at work (89/391/EEC), enacted in 1993. Although mental health is not as such an element which is central to this directive, a certain amount of attention is given to this aspect of health in Article 6. The framework directive states, among other things, that the employer has:
“a duty to ensure the safety and health of workers in every aspect related to work, following general principles of prevention: avoiding risks, evaluating the risks which cannot be avoided, combating the risks at source, adapting the work to the individual, especially as regards the design of workplaces, the choice of work equipment and the choice of work and production methods, with a view, in particular, to alleviating monotonous work and work at a predetermined work rate and to reduce their effects on health.”
Despite this directive, not all European countries have adopted framework legislation on health and safety. In a study comparing regulations, policies and practices concerning mental health and stress at work in five European countries, those countries with such framework legislation (Sweden, the Netherlands and the UK) recognize mental health issues at work as important health and safety topics, whereas those countries which do not have such a framework (France, Germany) do not recognize mental health issues as important (Kompier et al. 1994).
Last but not least, prevention of mental ill health (at its source) pays. There are strong indications that important benefits result from preventive programmes. For example, of the employers in a national representative sample of companies from three major branches of industry, 69% state that motivation increased; 60%, that absence due to sickness decreased ; 49%, that the atmosphere improved; and 40%, that productivity increased as a result of a prevention programme (Houtman et al. 1995).
Occupational Risk Groups of Mental Health
Are specific groups of the working population at risk of mental health problems? This question cannot be answered in a straightforward manner, since hardly any national or international monitoring systems exist which identify risk factors, mental health consequences or risk groups. Only a “scattergram” can be given. In some countries national data exist for the distribution of occupational groups with respect to major risk factors (e.g., for the Netherlands, Houtman and Kompier 1995; for the United States, Karasek and Theorell 1990). The distribution of the occupational groups in the Netherlands on the dimensions of job demands and skill discretion (figure 3) agree fairly well with the US distribution shown by Karasek and Theorell, for those groups that are in both samples. In those occupations with high work pace and/or low skill discretion, the risk of mental health disorders is highest.
Figure 3. Risk for stress and mental ill health for different occupational groups, as determined by the combined effects of work pace and skill discretion.
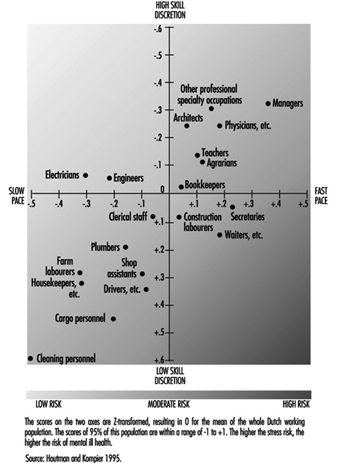
Also, in some countries there are data for mental health outcomes as related to occupational groups. Occupational groups that are especially prone to drop out for reasons of mental ill health in the Netherlands are those in the service sector, such as health care personnel and teachers, as well as cleaning personnel, housekeepers and occupations in the transport branch (Gründemann, Nijboer and Schellart1991).
In the United States, occupations which were highly prone to major depressive disorder, as diagnosed with standardized coding systems (i.e., the third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM III)) (American Psychiatric Association 1980), are juridicial employees, secretaries and teachers (Eaton et al. 1990).
Management of Mental Health Problems
The conceptual model (figure 1) suggests at least two targets of intervention in mental health issues:
- The (work) environment.
- The person—either his or her characteristics or the mental health consequences.
Primary prevention, the type of prevention that should prevent mental ill health from occurring, should be directed at the precursors by alleviating or managing the risks in the environment and increasing the coping ability and capacity of the individual. Secondary prevention is directed at the maintenance of people at work who already have some form of (mental) health problem. This type of prevention should embrace the primary prevention strategy, accompanied by strategies to make both employees and their supervisors sensitive to signals of early mental ill health in order to reduce the consequences or prevent them from getting worse. Tertiary prevention is directed at the rehabilitation of people who have dropped out of work due to mental health problems. This type of prevention should be directed at adapting the workplace to the possibilities of the individual (which is often found to be quite effective), along with individual counselling and treatment. Table 1 provides a schematic framework for the management of mental health disorders at the workplace. Effective preventive policy plans of organizations should, in principle, take into account all three types of strategy (primary, secondary and tertiary prevention), as well as be directed at risks, consequences and person characteristics.
Table 1. A schematic overview of management strategies on mental health problems, and some examples.
|
Type of |
Intervention level |
|
|
Work environment |
Person characteristics and/or health outcomes |
|
|
Primary |
Redesign of task content Redesign of communication structure |
Training groups of employees on signalling and handling specific work- related problems (e.g., how to manage time pressure, robberies etc.) |
|
Secondary |
Introduction of a policy on how to act in case of absenteeism (e.g., training supervisors to discuss absence and return with employees concerned) Provide facilities within the organization, especially for risk groups (e.g., counsellor for sexual harassment) |
Training in relaxation techniques |
|
Tertiary |
Adaptation of an individual workplace |
Individual counselling Individual treatment or therapy (may also be with medication) |
The schedule as presented provides a method for systematic analysis of all possible types of measure. One can discuss whether a certain measure belongs somewhere else in the schedule; such a discussion is, however, not very fruitful, since it is often the case that primary preventive measures can work out positively for secondary prevention as well. The proposed systematic analysis may well result in a large number of potential measures, several of which may be adopted, either as a general aspect of the (health and safety) policy or in a specific case.
In conclusion: Although mental health is not a clearly defined state, process or outcome, it covers a generally agreed upon area of (ill) health. Part of this area can be covered by generally accepted diagnostic criteria (e.g., psychosis, major depressive disorder); the diagnostic nature of other parts is neither as clear nor as generally accepted. Examples of the latter are moods and affects, and also burnout. Despite this, there are many indications that mental (ill) health, including the more vague diagnostic criteria, is a major problem. Its costs are high, both in human and financial terms. In the following articles of this chapter, several mental health disorders—moods and affects (e.g., dissatisfaction), burnout, post-traumatic stress disorder, psychoses, cognitive disorders and substance abuse—will be discussed in much more depth with respect to the clinical picture, available assessment techniques, aetiological agents and factors, and specific prevention and management measures.
Work-Related Psychosis
Psychosis is a general term often used to describe a severe impairment in mental functioning. Usually, this impairment is so substantial that the individual is unable to carry on normal activities of daily living, including most work activities. More formally, Yodofsky, Hales and Fergusen (1991) define psychosis as:
“A major mental disorder of organic or emotional origin in which a person’s ability to think, respond emotionally, remember, communicate, interpret reality and behave appropriately is sufficiently impaired so as to interfere grossly with the capacity to meet the ordinary demands of life. [Symptoms are] often characterized by regressive behaviour, inappropriate mood, diminished impulse control and such abnormal mental context as delusions and hallucinations [p. 618].”
Psychotic disorders are comparatively rare in the general population. Their incidence in the workplace is even lower, probably due to the fact that many individuals who frequently become psychotic often have problems maintaining stable employment (Jorgensen 1987). Precisely how rare it is, is difficult to estimate. However, there are some suggestions that the prevalence within the general population of psychoses (e.g., schizophrenia) is less than 1% (Bentall 1990; Eysenck 1982). While psychosis is rare, individuals who are actively experiencing a psychotic state usually exhibit profound difficulties in functioning at work and in other aspects of their lives. Sometimes acutely psychotic individuals exhibit behaviours which are engaging, inspiring or even humorous. For example, some individuals who suffer from bipolar illness and are entering a manic phase exhibit high energy and grand ideas or plans. For the most part, however, psychosis is associated with behaviours which evoke reactions such as discomfort, anxiety, anger or fear in co-workers, supervisors and others.
This article will first provide an overview of the various neurological conditions and mental states in which psychosis can occur. Then, it will review workplace factors potentially associated with the occurrence of psychosis. Finally, it will summarize treatment approaches for managing both the psychotic worker and the work environment (i.e., medical management, return-to-work clearance procedures, workplace accommodations and workplace consultations with supervisors and co-workers).
Neurological Conditions and Mental Stateswithin which Psychosis Occurs
Psychosis can occur within a number of diagnostic categories identified in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM IV) (American Psychiatric Association 1994). At this point, there is no commonly agreed upon definitive diagnostic set. The following are widely accepted as medical conditions within which psychoses arise.
Neurological and general medical conditions
Delusional symtomatology can be caused by a range of neurological disorders affecting the limbic system or basal ganglia, where cerebral cortical functioning remains intact. Partial complex seizure episodes are often preceded by olfactory hallucinations of peculiar smells. To an external observer, this seizure activity may appear to be simple staring or day-dreaming. Cerebral neoplasms, especially in temporal and occipital areas, can cause hallucinations. Also, delirium-causing diseases, such as Parkinson’s, Huntington’s, Alzheimer’s, and Pick’s, can result in altered states of consciousness. Several sexually transmitted diseases such as tertiary syphilis and AIDS can also produce psychosis. Lastly, deficiencies of certain nutrients, such as B-12, niacin, folic acid and thiamine, have the potential of causing neurological problems which can result in psychosis.
Psychotic symptoms such as hallucinations and delusions also occur among patients with various general medical conditions. These include several systemic diseases, such as hepatic encephalopathy, hypercalcaemia, diabetic ketoacidosis, and malfunction of endocrine glands (i.e., adrenal, thyroid, parathyroid and pituitary). Sensory and sleep deprivation have also been shown to cause psychosis.
Mental states
Schizophrenia is probably the most widely known of the psychotic disorders. It is a progressively deteriorating condition which usually has an insidious onset. A number of specific subcategories have been identified including paranoid, disorganized, catatonic, undifferentiated and residual types. People who suffer from this disorder often have limited work histories and often do not remain in the workforce. Occupational impairment among schizophrenics is very common, and many schizophrenics lose their interest or will to work as the disease progresses. Unless a job is of very low complexity, it is usually very difficult for them to stay employed.
Schizophreniform disorder is similar to schizophrenia, but an episode of this disorder is of short duration, usually lasting less than six months. Generally, persons with this disorder have good premorbid social and occupational functioning. As the symptoms resolve, the person returns to baseline functioning. Consequently, the occupational impact of this disorder may be significantly less than in cases of schizophrenia.
Schizoaffective disorder also has a better prognosis than schizophrenia but a worse prognosis than affective disorders. Occupational impairment is quite common in this group. Psychosis is also sometimes observed in major affective disorders. With appropriate treatment, occupational functioning among workers suffering from major affective disorders is generally substantially better than for those with schizophrenia or schizoaffective disorders.
Severe stressors such as losing a loved one or losing one’s job can result in a brief reactive psychosis. This psychotic disorder is probably observed more frequently in the workplace than other types of psychotic disorder, especially with schizoid, schizotypal and borderline features.
Delusional disorders are probably relatively common in the workplace. There are several types. The erotomanic type typically believes that another person, usually of a higher social status, is in love with them. Sometimes, they harass the person who they believe is in love with them by attempting contact via telephone calls, letters or even stalking. Often, individuals with these disorders are employed in modest occupations, living isolated and withdrawn lives with limited social and sexual contact. The grandiose type usually exhibits delusions of inflated worth, power, knowledge or a special relationship with a deity or a famous person. The jealous type believes inaccurately that their sexual partner has been unfaithful. The persecutory type believes inaccurately that they (or someone to whom they are close) are being cheated, maligned, harassed or in other ways malevolently treated. These persons are often resentful and angry and may resort to violence against those they believe to be hurting them. They rarely want to seek help, as they do not think there is anything wrong with them. Somatic types develop delusions, contrary to all evidence, that they are afflicted with infections. They can also believe that a part of their body is disfigured, or worry about having a bad body odour. These workers with delusional beliefs can often create work-related difficulties.
Work-related chemical factors
Chemical factors such as mercury, carbon disulphide, toluene, arsenic and lead have been known to cause psychosis in blue-collar workers. For example, mercury has been found to be responsible for causing psychosis in workers in the hat industry, appropriately named the “Mad Hatter’s psychosis” (Kaplan and Sadock 1995). Stopford (personal communication, 6 November 1995) suggests that carbon disulphide was found to cause psychosis among workers in France in 1856. In the United States, in 1989, two brothers in Nevada purchased a carbon disulphide compound to kill gophers. Their physical contact with this chemical resulted in severe psychosis—one brother shooting a person and the other shooting himself due to severe confusion and psychotic depression. The incidence of suicide and homicide increases thirteenfold with exposure to carbon disulphide. Further, Stopford reports that exposure to toluene (used in making explosives and dyestuffs) is known to cause acute encephalopathy and psychosis. Symptoms can manifest also as memory loss, mood changes (e.g., dysphoria), deterioration in eye-hand coordination and speech impediments. Hence, some organic solvents, especially those found in the chemical industry, have a direct influence on the human central nervous system (CNS), causing biochemical changes and unpredictable behaviour (Levi, Frandenhaeuser and Gardell 1986). Special precautions, procedures and protocols have been established by the US Occupational Safety and Health Administration (OSHA), National Institute for Occupational Safety and Health (NIOSH) and the chemical industry to ensure minimum risk to employees working with toxic chemicals in their work environments.
Other factors
A number of medications can cause delirium which in turn can result in psychosis. These include antihypertensives, anticholinergics (including a number of medications used to treat the common cold), antidepressants, anti-tuberculosis medicines, anti-Parkinson’s disease medicines, and ulcer medicines (such as cimetidine). Further, substance-induced psychosis can be caused by a number of licit and illicit drugs which are sometimes abused, such as alcohol, amphetamines, cocaine, PCP, anabolic steroids and marijuana. The delusions and hallucinations which result are usually temporary. Although the content may vary, persecutory delusions are quite common. In alcohol-related hallucinations a person may believe that he or she is hearing voices which are threatening, insulting, critical or condemning. Sometimes, these insulting voices speak in the third person. As with individuals exhibiting paranoid or persecutory delusions, these individuals should be carefully evaluated for dangerousness to self or others.
Post-partum psychosis is comparatively uncommon in the workplace, but is worth noting as some women are returning to work more quickly. It tends to occur in new mothers (or more rarely fathers), usually within two to four weeks after delivery.
In a number of cultures, psychosis may result from various commonly held beliefs. A number of culturally based psychotic reactions have been described, including episodes such as “koro” in South and East Asia, “qi-gong psychotic reaction” within Chinese populations, “piblokto” in Eskimo communities and “whitigo” among several American Indian groups (Kaplan and Sadock 1995). The relationship of these psychotic phenomena to various occupational variables does not appear to have been studied.
Workplace Factors Associated with the Occurrence of Psychosis
Although information and empirical research on work-related psychosis are extremely scarce, due in part to the low prevalence in the work setting, researchers have noted a relationship between psychosocial factors in the work environment and psychological distress (Neff 1968; Lazarus 1991; Sauter, Murphy and Hurrell 1992; Quick et al. 1992). Significant psychosocial stressors on the job, such as role ambiguity, role conflicts, discrimination, supervisor-supervisee conflicts, work overload and work setting have been found to be associated with greater susceptibility to stress-related illness, tardiness, absenteeism, poor performance, depression, anxiety and other psychological distress (Levi, Frandenhaeuser and Gardell 1986; Sutherland and Cooper 1988).
Stress appears to have a prominent role in the complex manifestations of various types of physiological and psychological disorders. In the workplace, Margolis and Kroes (1974) believe that occupational stress occurs when some factor or combination of factors at work interact with the worker to disrupt his or her psychological or physiological homeostasis. These factors can be external or internal. External factors are the various pressures or demands from the external environment which stem from a person’s occupation, as well as from marriage, family or friends, whereas internal factors are the pressures and demands a worker places upon him- or herself—for example, by being “ambitious, materialistic, competitive and aggressive” (Yates 1989). It is these internal and external factors, separately or in combination, which can result in occupational distress whereby the worker experiences significant psychological and physical health problems.
Researchers have speculated on whether severe or cumulative stress, known as “stress-induced arousal”, originating from the work environment, could induce work-related psychotic disorders (Bentall, Dohrenwend and Skodol 1990; Link, Dohrenwend and Skodol 1986). For example, there is evidence linking hallucinatory and delusional experiences to specific stressful events. Hallucinations have been associated with stress-induced arousal occurring as a result of mining accidents, hostage situations, chemical-factory explosions, wartime exposure, sustained military operations and loss of a spouse (Comer, Madow and Dixon 1967; Hobfoll 1988; Wells 1983).
DeWolf (1986) believes that either the exposure to or interaction of multiple stressful conditions over an extended period of time is a complex process whereby some workers experience psychological health-related problems. Brodsky (1984) found in her examination of 2,000 workers who were her patients over 18 years that: (1) the timing, frequency, intensity and duration of unpleasant work conditions were potentially harmful, and she believed that 8 to 10% of the workforce experienced disabling psychological, emotional and physical health-related problems; and (2) workers react to work-related stress in part as “a function of perceptions, personality, age, status, life stage, unrealized expectations, prior experiences, social support systems and their capacity to respond adequately or adapt.” In addition, psychological distress can potentially be exacerbated by the worker feeling a sense of uncontrollability (e.g., inability to make decisions) and unpredictability in the work environment (e.g., corporate downsizing and reorganizing) (Labig 1995; Link and Stueve 1994).
Specific examination of the work-related “antecedents” of workers experiencing psychosis has received limited attention. The few researchers who have empirically examined the relationship between psychosocial factors in the work environment and severe psychopathology have found a relationship between “noisome” work conditions (i.e., noise, hazardous conditions, heat, humidity, fumes and cold) and psychosis (Link, Dohrenwend and Skodol 1986; Muntaner et al. 1991). Link, Dohrenwend and Skodol (1986) were interested in understanding the types of jobs schizophrenics had when they experienced their first schizophrenic episode. First full-time occupations were examined for workers who experienced: (a) schizophrenic or schizophrenic-like episodes; (b) depression; and (c) no psychopathology. These researchers found that noisome work conditions existed among more blue-collar than white-collar professions. These researchers concluded that noisome work conditions were potentially significant risk factors in the manifestation of psychotic episodes (i.e., schizophrenia).
Muntaner et al. (1991) replicated the findings of Link, Dohrenwend and Skodol (1986) and examined in greater detail whether various occupational stressors contributed to increased risk of developing or experiencing psychoses. Three types of psychotic condition were examined using the criteria of DSM III—schizophrenia; schizophrenia criterion A (hallucinations and delusions); and schizophrenia criterion A with affective episode (psychotic-affective disorder). Participants in their retrospective study were from a larger Epidemiologic Catchment Area (ECA) study examining the incidence of psychiatric disorders across five sites (Connecticut, Maryland, North Carolina, Missouri and California). These researchers found that psychosocial work characteristics (i.e., high physical demands, lack of control over work and working conditions—noisome factors) placed participants at increased risk of psychotic occurrences.
As illustrations, in the Muntaner et al. (1991) study, people in construction trade occupations (i.e., carpenters, painters, roofers, electricians, plumbers) were 2.58 times more likely to experience delusions or hallucinations than people in managerial occupations. Workers in housekeeping, laundry, cleaning and servant-type occupations were 4.13 times more likely to become schizophrenic than workers in managerial occupations. Workers who identified themselves as writers, artists, entertainers and athletes were 3.32 times more likely to experience delusions or hallucinations in comparison to workers in executive, administrative and managerial occupations. Lastly, workers in occupations such as sales, mail and message delivery, teaching, library science and counselling were more at risk of psychotic, affective disorders. It is important to note that the associations between psychotic conditions and occupational variables were examined after alcohol and drug use was controlled for in their study.
A significant difference between blue-collar and white-collar professions is the types of psychological demand and psychosocial stress placed on the worker. This is illustrated in the findings of Muntaner et al. (1993). They found an association between a work environment’s cognitive complexity and psychotic forms of mental illness. The most frequent occupations held by schizophrenic patients during their last full-time job were characterized by their low level of complexity in dealing with people, information and objects (e.g., janitors, cleaners, gardeners, guards). A few researchers have examined some of the consequences of first episodic psychosis relative to employment, job performance and capacity to work (Jorgensen 1987; Massel et al. 1990; Beiser et al. 1994). For example, Beiser and co-workers examined occupational functioning after the first episode of psychosis. These researchers found 18 months after the first episode that the “psychosis compromise[d] occupational functioning”. In other words, there was a higher post-morbid decline among schizophrenic workers than among those suffering from affective disorders. Similarly, Massel et al. (1990) found that the work capacity of psychotics (e.g., people with schizophrenia, affective disorders with psychotic features or atypical psychotic disorders) was impaired in comparison to non-psychotics (e.g., people with affective disorders without psychotic features, anxiety disorders, personality disorders and substance abuse disorders). Psychotics in their study showed marked thought disturbance, hostility and suspiciousness which correlated with poor work performance.
In summary, our knowledge about the relationship between work-related factors and psychosis is in the embryonic stage. As Brodsky (1984) states, “the physical and chemical hazards of the workplace have received considerable attention, but the psychological stresses associated with work have not been as widely discussed, other than in relation to managerial responsibilities or to the coronary-prone behaviour pattern”. This means that research on the topic of work-related psychosis is vitally needed, especially since workers spend an average of 42 to 44% of their lives working (Hines, Durham and Geoghegan 1991; Lemen 1995) and work has been associated with psychological well-being (Warr 1978). We need to have a better understanding of what types of occupational stressor under what types of condition influence which types of psychological disorder. For example, research is needed to determine whether there are stages which workers move through based upon intensity, duration and frequency of psychosocial stress in the work environment, in conjunction with personal, social, cultural and political factors occurring in their daily lives. We are dealing with complex issues which will require in-depth inquiries and ingenious solutions.
Acute Management of the Psychotic Worker
Typically, the primary role of persons in the workplace is to respond to an acutely psychotic worker in a manner which facilitates the person being transported safely to an emergency room or psychiatric treatment facility. The process may be greatly facilitated if the organization has an active employee assistance programme and a critical incident response plan. Ideally, the organization will train key employees in advance for emergency crisis responses and will have a plan in place for coordinating as needed with local emergency response resources.
Treatment approaches for the psychotic worker will vary depending upon the specific type of underlying problem. In general, all psychotic disorders should be evaluated by a professional. Often, immediate hospitalization is warranted for the safety of the worker and the workplace. Thereafter, a thorough evaluation can be completed to establish a diagnosis and develop a treatment plan. The primary goal is to treat the underlying cause(s). However, even prior to conducting a comprehensive evaluation or initiating a comprehensive treatment plan, the physician responding to the emergency may need to focus initially on providing symptomatic relief. Providing a structured, low-stress environment is desirable. Neuroloptics may be used to help the patient calm down. Benzodiazepines may help reduce acute anxiety.
After managing the acute crisis, a comprehensive evaluation may include collecting a detailed history, psychological testing, a risk assessment to establish dangerousness to self or others and careful monitoring of response to treatment (including not only response to medications, but also to psychotherapeutic interventions). One of the more difficult problems with many patients who exhibit psychotic symptomatology is treatment compliance. Often these individuals tend not to believe that they have serious difficulties, or, even if they recognize the problem, they are sometimes inclined to decide unilaterally to discontinue treatment prematurely. In these instances, family members, co-workers, treating clinicians, occupational health personnel and employers are sometimes placed in awkward or difficult situations. Sometimes, for the safety of the employee and the workplace, it becomes necessary to mandate compliance with treatment as a condition for returning to the job.
Managing the Psychotic Worker and the Work Environment
Case example
A skilled worker on the third shift at a chemical plant began to exhibit unusual behaviour as the company began to modify its production schedule. For several weeks, instead of leaving work after his shift ended, he began to stay for several hours discussing his concerns about increased job demands, quality control and changes in production procedures with his counterparts on the morning shift. He appeared quite distressed and behaved in a manner which was atypical for him. He had formerly been somewhat shy and distant, with an excellent job performance history. During this period of time, he became more verbal. He also approached individuals and stood close to them in a manner which several co-workers reported made them feel uncomfortable. While these co-workers later reported that they felt his behaviour was unusual, no one notified the employee assistance programme (EAP) or management of their concerns. Then, suddenly one evening, this employee was observed by his co-workers as he began to shout incoherently, walked over to a storage area for volatile chemicals, laid down on the ground and began to flick a cigarette lighter on and off. His co-workers and supervisor interfered and, after consultation with the EAP, he was taken by ambulance to a nearby hospital. The treating physician determined that he was acutely psychotic. After a brief treatment period he was successfully stabilized on medications.After several weeks, his treating physician felt he was able to return to his job. He underwent a formal return-to-work evaluation with an independent clinician and was judged ready to return to work. While his company doctor and the treating physician determined that it was safe for him to return, his co-workers and supervisors expressed substantial concerns. Some employees noted that they might be harmed if this episode were repeated and the chemical storage areas ignited. The company took steps to increase security in safety sensitive areas. Another concern also surfaced. A number of workers stated that they believed this individual might bring a weapon to work and start shooting. None of the professionals involved in treating this worker or in evaluating him for return to work believed that there was a risk of violent behaviour. The company then elected to bring in mental health professionals (with the worker’s consent) to assure co-workers that the risk of violent behaviour was exceedingly low, to provide education on mental illnesses, and to identify proactive steps that co-workers could take to facilitate the return to work of a colleague who had undergone treatment. However, in this situation, even after this educational intervention, co-workers were unwilling to interact with this worker, further compounding the return-to-work process. While the legal rights of individuals suffering from mental disorders, including those associated with psychotic states, have been addressed by the Americans with Disabilities Act, practically speaking the organizational challenges to effectively managing occurrences of psychosis at work are often as great or greater than the medical treatment of psychotic workers.
Return to Work
The primary question to be addressed after a psychotic episode is whether the employee can safely return to his or her current job. Sometimes organizations permit this decision to be made by the treating clinicians. However, ideally, the organization should require their occupational medical system to conduct an independent fitness-for-duty evaluation (Himmerstein and Pransky 1988). In the fitness-for-duty evaluation process a number of key pieces of information should be reviewed, including the treating clinician’s evaluation, treatment and recommendations, as well as the worker’s prior job performance and the specific features of the job, including the required job tasks and the organizational environment.
If the occupational medical physician is not trained in psychiatric or psychological fitness-for-duty evaluation, then the evaluation should be performed by an independent mental health professional who is not the treating clinician. If some aspects of the job pose safety risks, then specific work restrictions should be developed. These restrictions may range from minor alterations in work activities or work schedule to more significant modifications such as alternate job placement (e.g., a light-duty assignment or a job transfer to an alternate position). In principle, these work restrictions are not different in kind from other restrictions commonly provided by occupational health physicians, such as specifying the amount of weight which a worker may be cleared to lift following a musculoskeletal injury.
As is evident in the case example above, the return to work often raises challenges not only for the affected worker, but also for co-workers, supervisors and the broader organization. While professionals are obligated to protect the confidentiality of the affected worker to the fullest extent permitted by law, if the worker is willing and competent to sign an appropriate release of information, then the occupational medical system can provide or coordinate consultation and educational interventions to facilitate the return-to-work process. Often, coordination between the occupational medical system, the employee assistance programme, supervisors, union representatives and co-workers is critical to a successful outcome.
The occupational health system should also periodically monitor the worker’s readjustment to the workplace in collaboration with the supervisor. In some instances, it may be necessary to monitor the worker’s compliance with a medication regimen recommended by the treating physician—for example, as a precondition for being permitted to engage in certain safety-sensitive job tasks. More importantly, the occupational medical system must consider not only what is best for the worker, but also what is safe for the workplace. The occupational medical system may also play a critical role in assisting the organization in complying with legal requirements such as the Americans with Disabilities Act as well as in interfacing with treatments provided under the organization’s health care plan and/or the workers’ compensation system.
Prevention Programming
At present, there is no literature on specific prevention or early intervention programmes for reducing the incidence of psychosis in the workforce. Employee assistance programmes may play a crucial role in the early identification and treatment of psychotic workers. Since stress may contribute to the incidence of psychotic episodes within working populations, various organizational interventions which identify and modify organizationally created stress may also be helpful. These general programmatic efforts may include job redesign, flexible scheduling, self-paced work, self-directed work teams and microbreaks, as well as specific programming to reduce the stressful impact of reorganization or downsizing.
Conclusion
While psychosis is a comparatively rare and multiply determined phenomenon, its occurrence within working populations raises substantial practical challenges for co-workers, union representatives, supervisors and occupational health professionals. Psychosis may occur as a direct consequence of a work-related toxic exposure. Work-related stress may also increase the incidence of psychosis among workers who suffer from (or are at risk of developing) mental disorders which place them at risk of psychosis. Additional research is needed to: (1) better understand the relationship between workplace factors and psychosis; and (2) develop more effective approaches for managing psychosis in the workplace and reduce its incidence.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."