- You are here:
-
Home

- Part III. Management & Policy

Children categories

17. Disability and Work (10)

17. Disability and Work
Chapter Editors: Willi Momm and Robert Ransom
Table of Contents
Figures
Disability: Concepts and Definitions
Willi Momm and Otto Geiecker
Case Study: Legal Classification of Disabled People in France
Marie-Louise Cros-Courtial and Marc Vericel
Social Policy and Human Rights: Concepts of Disability
Carl Raskin
International Labour Standards and National Employment Legislation in Favour of Disabled Persons
Willi Momm and Masaaki Iuchi
Vocational Rehabilitation and Employment Support Services
Erwin Seyfried
Disability Management at the Workplace: Overview and Future Trends
Donald E. Shrey
Rehabilitation and Noise-induced Hearing Loss
Raymond Hétu
Rights and Duties: An Employer’s Perspective
Susan Scott-Parker
Case Study: Best Practices Examples
Rights and Duties: Workers’ Perspective
Angela Traiforos and Debra A. Perry
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.







18. Education and Training (9)
18. Education and Training
Chapter Editor: Steven Hecker
Table of Contents
Figures and Tables
Introduction and Overview
Steven Hecker
Principles of Training
Gordon Atherley and Dilys Robertson
Worker Education and Training
Robin Baker and Nina Wallerstein
Case Studies
Evaluating Health and Safety Training: A Case Study in Chemical Workers Hazardous Waste Worker Education
Thomas H. McQuiston, Paula Coleman, Nina Wallerstein, A.C. Marcus, J.S. Morawetz, David W. Ortlieb and Steven Hecker
Environmental Education and Training: The State of Hazardous Materials Worker Education in the United States
Glenn Paulson, Michelle Madelien, Susan Sink and Steven Hecker
Worker Education and Environmental Improvement
Edward Cohen-Rosenthal
Safety and Health Training of Managers
John Rudge
Training of Health and Safety Professionals
Wai-On Phoon
A New Approach to Learning and Training:A Case Study by the ILO-FINNIDA African Safety and Health Project
Antero Vahapassi and Merri Weinger
Tables
Click a link below to view table in article context.
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.












19. Ethical Issues (10)
19. Ethical Issues
Chapter Editor: Georges H. Coppée
Table of Contents
Codes and Guidelines
Colin L. Soskolne
Responsible Science: Ethical Standards and Moral Behaviour in Occupational Health
Richard A. Lemen and Phillip W. Strine
Ethical Issues in Occupational Health and Safety Research
Paul W. Brandt-Rauf and Sherry I. Brandt-Rauf
Ethics in the Workplace: A Framework for Moral Judgement
Sheldon W. Samuels
Surveillance of the Working Environment
Lawrence D. Kornreich
Canons of Ethical Conduct and Interpretive Guidelines
Ethical Issues: Information and Confidentiality
Peter J. M. Westerholm
Ethics in Health Protection and Health Promotion
D. Wayne Corneil and Annalee Yassi
Case Study: Drugs and Alcohol in the Workplace - Ethical Considerations
Behrouz Shahandeh and Robert Husbands
International Code of Ethics for Occupational Health Professionals
International Commission on Occupational Health
20. Development, Technology and Trade (10)
20. Development, Technology and Trade
Chapter Editor: Jerry Jeyaratnam
Table of Contents
Figures and Tables
Occupational Health Trends in Development
Jerry Jeyaratnam
Industrialized Countries and Occupational Health and Safety
Toshiteru Okubo
Case Studies in Technological Change
Michael J. Wright
Small Enterprises and Occupational Health and Safety
Bill Glass
Transfer of Technology and Technological Choice
Joseph LaDou
Free-Trade Agreements
Howard Frumkin
Case Study: World Trade Organization
Product Stewardship and the Migration of Industrial Hazards
Barry Castleman
Economic Aspects of Occupational Health and Safety
Alan Maynard
Case Study: Industrialization and Occupational Health Problems in China
Su Zhi
Tables
Click a link below to view table in the article context.
1. Small-scale enterprises
2. Information from foreign investors
3. Costs of work accidents & health (Britain)
4. Types of economic evaluation
5. Development of China’s township enterprises
6. Country HEPS & OHS coverages in China
7. Compliance rates of 6 hazards in worksites
8. Detectable rates of occupational diseases
9. Hazardous working & employers, China
10. OHS background in foreign-funded enterprises
11. Routine instruments for OHS, 1990, China
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|



21. Labour Relations and Human Resources Management (12)
21. Labour Relations and Human Resources Management
Chapter Editor: Anne Trebilcock
Table of Contents
Figures and Tables
Labour Relations and Human Resources Management: An Overview
Anne Trebilcock
Rights of Association and Representation
Breen Creighton
Collective Bargaining and Safety and Health
Michael J. Wright
National Level Tripartite and Bipartite Cooperation on Health and Safety
Robert Husbands
Forms of Workers’ Participation
Muneto Ozaki and Anne Trebilcock
Case Study: Denmark: Worker Participation in Health and Safety
Anne Trebilcock
Consultation and Information on Health and Safety
Marco Biagi
Labour Relations Aspects of Training
Mel Doyle
Labour Relations Aspects of Labour Inspection
María Luz Vega Ruiz
Collective Disputes over Health and Safety Issues
Shauna L. Olney
Individual Disputes over Health and Safety Issues
Anne Trebilcock
Tables
Click a link below to view table in article context.
1. Practical activities-health & safety training
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|



22. Resources: Information and OSH (5)
22. Resources: Information and OSH
Chapter Editor: Jukka Takala
Table of Contents
Figures and Tables
Information: A Precondition for Action
Jukka Takala
Finding and Using Information
P.K. Abeytunga, Emmert Clevenstine, Vivian Morgan and Sheila Pantry
Information Management
Gordon Atherley
Case study: Malaysian Information Service on Pesticide Toxicity
D.A. Razak, A.A. Latiff, M.I. A. Majid and R. Awang
Case Study: A Successful Information Experience in Thailand
Chaiyuth Chavalitnitikul
Tables
Click a link below to view table in article context.
1. Some core periodicals in occupational health & safety
2. Standard search form
3. Information required in occupational health & safety
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.




23. Resources, Institutional, Structural and Legal (20)
23. Resources, Institutional, Structural and Legal
Chapter Editors: Rachael F. Taylor and Simon Pickvance
Table of Contents
Figures and Tables
Institutional, Structural and Legal Resources: Introduction
Simon Pickvance
Labour Inspection
Wolfgang von Richthofen
Civil and Criminal Liability in Relation to Occupational Safety and Health
Felice Morgenstern (adapted)
Occupational Health as a Human Right
Ilise Levy Feitshans
Community Level
Community-Based Organizations
Simon Pickvance
Right to Know: The Role of Community-Based Organizations
Carolyn Needleman
The COSH Movement and Right to Know
Joel Shufro
Regional and National Examples
Occupational Health and Safety: The European Union
Frank B. Wright
Legislation Guaranteeing Benefits for Workers in China
Su Zhi
Case Study: Exposure Standards in Russia
Nikolai F. Izmerov
International Governmental and Non-Governmental Organizations
International Cooperation in Occupational Health: The Role of International Organizations
Georges H. Coppée
The United Nations and Specialized Agencies
Contact Information for the United Nations Organization
International Labour Organization
Georg R. Kliesch
Case Study: ILO Conventions--Enforcement Procedures
Anne Trebilcock
International Organization for Standardization (ISO)
Lawrence D. Eicher
International Social Security Association (ISSA)
Dick J. Meertens
Addresses of the ISSA International Sections
International Commission on Occupational Health (ICOH)
Jerry Jeyaratnam
International Association of Labour Inspection (IALI)
David Snowball
Tables
Click a link below to view table in article context.
1. Bases for Russian vs. American standards
2. ISO technical committees for OHS
3. Venues of triennial congresses since 1906
4. ICOH committees & working groups, 1996
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|




24. Work and Workers (6)
24. Work and Workers
Chapter Editors: Jeanne Mager Stellman and Leon J. Warshaw
Table of Contents
Figures
Work and Workers
Freda L. Paltiel
Shifting Paradigms and Policies
Freda L. Paltiel
Health, Safety and Equity in the Workplace
Joan Bertin
Precarious Employment and Child Labour
Leon J. Warshaw
Transformations in Markets and Labour
Pat Armstrong
Globalizing Technologies and the Decimation/Transformation of Work
Heather Menzies
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.

25. Worker's Compensation Systems (1)
25. Worker's Compensation Systems
Chapter Editor: Terence G. Ison
Table of Contents
Overview
Terence G. Ison
Part One: Workers' Compensation
Coverage
Organization, Administration and Adjudication
Eligibility for Benefits
Multiple Causes of Disability
Subsequent Consequential Disabilities
Compensable Losses
Multiple Disabilities
Objections to Claims
Employer Misconduct
Medical Aid
Money Payments
Rehabilitation and Care
Obligations to Continue the Employment
Finance
Vicarious Liability
Health and Safety
Claims against Third Parties
Social Insurance and Social Security
Part Two: Other Systems
Accident Compensation
Sick Pay
Disability Insurance
Employers’ Liability
26. Topics in Workers' Compensation Systems (6)
26. Topics in Workers' Compensation Systems
Chapter Editors: Paule Rey and Michel Lesage
Table of Contents
Tables
Work-Related Diseases and Occupational Diseases: The ILO International List
Michel Lesage
Workers’ Compensation: Trends and Perspectives
Paule Rey
Prevention, Rehabilitation and Compensation in the German Accident Insurance System
Dieter Greiner and Andreas Kranig
Employment Injuries Insurance and Compensation in Israel
Haim Chayon
Workers’ Accident Compensation in Japan
Kazutaka Kogi and Haruko Suzuki
Country Case Study: Sweden
Peter Westerholm
Tables
Click a link below to view table in article context.
1. Proposed ILO list of occupational diseases
2. Recipients of benefits in Israel
3. Premium rates in Japan
4. Enterprises, workers & costs in Japan
5. Payment of benefits by industry in Japan
A New Approach to Learning and Training: A Case Study by the ILO-FINNIDA African Safety and Health Project
Abuya: What’s the matter? You look worn out.
Mwangi: I am worn out—and disgusted. I was up half the night getting ready for this lecture I just gave and I don’t think it went very well. I couldn’t get anything out of them—no questions, no enthusiasm. For all I know, they didn’t understand a word I said.
Kariuki: I know what you mean. Last week I was having a terrible time trying to explain chemical safety in Swahili.
Abuya: I don’t think it’s the language. You were probably just talking over their heads. How much technical information do these workers really need to know anyway?
Kariuki: Enough to protect themselves. If we can’t get the point across, we’re just wasting our time. Mwangi, why didn’t you try asking them something or tell a story?
Mwangi: I couldn’t figure out what to do. I know there has to be a better way, but I was never trained in how to do these lectures right.
Abuya: Why all the fuss? Just forget about it! With all the inspections we have to do, who’s got time to worry about training?
The above discussion in an African factory inspectorate, which could take place anywhere, highlights a real problem: how to get the message through in a training session. Using a real problem as a discussion starter (or trigger) is an excellent training technique to identify potential obstacles to training, their causes and potential solutions. We have used this discussion as a role play in our Training of Trainers’ workshops in Kenya and Ethiopia.
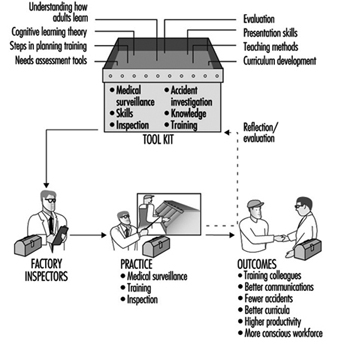
The ILO-FINNIDA African Safety and Health Project is part of the ILO’s technical cooperation activities aimed to improve occupational safety and health training and information services in 21 African countries where English is commonly spoken. It is sponsored by FINNIDA, the Finnish International Development Agency. The Project took place from 1991 to 1994 with a budget of US$5 million. One of the main concerns in the implementation of the Project was to determine the most appropriate training approach by which to facilitate high quality learning. In the following case study we will describe the practical implementation of the training approach, the Training the Trainers’ (TOT) course (Weinger 1993).
Development of a New Training Approach
In the past, the training approach in most African factory inspectorates, and also in many technical cooperation projects of the ILO, has been based on randomly selected, isolated topics of occupational safety and health (OSH) which were presented mainly by using lecturing methods. The African Safety and Health Project conducted the first pilot course in TOT in 1992 for 16 participating countries. This course was implemented in two parts, the first part dealing with basic principles of adult education (how people learn, how to establish learning objectives and select teaching contents, how to design the curriculum and select instructional methods and learning activities and how to improve personal teaching skills) and the second part with practical training in OSH based on individual assignments which each participant completed during a four month’s time period following the first part of the course.
The main characteristics of this new approach are participation and action orientation. Our training does not reflect the traditional model of classroom learning where participants are passive recipients of information and the lecture is the dominant instructional method. In addition to its action orientation and participatory training methods, this approach is based on the latest research in modern adult education and takes a cognitive and activity-theoretical view of learning and teaching (Engeström 1994).
On the basis of the experience gained during the pilot course, which was extremely successful, a set of detailed course material was prepared, call the Training of Trainers Package, which consists of two parts, a trainer’s manual and a supply of participants’ handout matter. This package was used as a guideline during planning sessions, attended by from 20 to 25 factory inspectors over a period of ten days, and concerned with establishing national TOT courses in Africa. By the spring of 1994, national TOT courses had been implemented in two African countries, Kenya and Ethiopia.
High Quality Learning
There are four key components of high quality learning.
Motivation for learning. Motivation occurs when participants see the “use-value” of what they are learning. It is stimulated when they can perceive the gap that separates what they know and what they need to know to solve a problem.
Organization of subject matter. The content of learning is too commonly thought of as separate facts stored in the brain like items in boxes on a shelf. In reality, people construct models, or mental pictures, of the world while learning. In promoting cognitive learning, teachers try to organize facts into models for better learning and include explanatory principles or concepts (the “but whys” behind a fact or skill).
Advancing through steps in the learning process. In the learning process, the participant is like an investigator looking for a model by which to understand the subject matter. With the help of the teacher, the participant forms this model, practices using it and evaluates its usefulness. This process can be divided into the following six steps:
- motivation
- orientation
- integrating new knowledge (internalization)
- application
- programme critique
- participant evaluation.
Social interaction. The social interaction between participants in a training session is an essential component of learning. In group activities, participants learn from one another.
Planning training for high quality learning
The kind of education aimed at particular skills and competencies is called training. The goal of training is to facilitate high quality learning and it is a process that takes place in a series of steps. It requires careful planning at each stage and each step is equally important. There are many ways of breaking the training into components but from the point of view of the cognitive conception of learning, the task of planning a training course can be analysed into six steps.
Step 1: Conduct a needs assessment (know your audience).
Step 2: Formulate learning objectives.
Step 3: Develop an orientation basis or “road map” for the course.
Step 4: Develop the curriculum, establishing its contents and associated training methods and using a chart to outline your curriculum.
Step 5: Teach the course.
Step 6: Evaluate the course and follow up on the evaluation.
Practical Implementation of National TOT Courses
Based on the above-mentioned training approach and experience from the first pilot course, two national TOT courses were implemented in Africa, the one in Kenya in 1993 and the other in Ethiopia in 1994.
Training needs were based on the work activity of factory inspectors and were determined by means of a pre-workshop questionnaire and a discussion with the course participants about their everyday work and about the kinds of skills and competencies necessary to carry it out (see figure 1). The course has thus been designed primarily for factory inspectors (in our national TOT courses, usually 20 to 25 inspectors participated), but it could be extended to other personnel who may need to carry out safety and health training, such as shop stewards, foremen, and safety and health officers.
Figure 1. Orientation basis for the factory inspector's work activity.

A compilation of course objectives for the national TOT course was assembled step by step in cooperation with the participants, and is given immediately below.
Objectives of the national TOT course
The aims of the training of trainers (TOT) course are as follows:
- Increase participants’ understanding of the changing role and tasks of factory inspectors from immediate enforcement to long-term advisory service, including training and consultation.
- Increase participants’ understanding of the basic principles of high quality learning and instruction.
- Increase participants’ understanding of the variety of skills involved in planning training programmes: identification of training needs, formulation of learning objectives, development of training curricula and materials, selection of appropriate teaching methods, effective presentation and programme evaluation.
- Enhance participants’ skills in effective communication for application during inspections and consultation, as well as in formal training sessions.
- Facilitate the development of short and long-term training plans in which new instructional practices will be implemented.
Course contents
The key subject areas or curriculum units that guided the implementation of the TOT course in Ethiopia are outlined in figure 2. This outline may also serve as an orientation basis for the whole TOT course.
Figure 2. The key subject areas of the TOT course.
Determining training methods
The external aspect of the teaching method is immediately observable when you step into a classroom. You might observe a lecture, a discussion, group or individual work. However, what you do not see is the most essential aspect of teaching: the kind of mental work being accomplished by the student at any given moment. This is called the internal aspect of the teaching method.
Teaching methods can be divided into three main groups:
- Instructional presentation: participant presentations, lectures, demonstrations, audio-visual presentations
- Independent assignment: tests or exams, small group activities, assigned reading, use of self-guided learning materials, role plays
- Cooperative instruction
Most of the above methods were used in our TOT courses. However, the method one selects depends on the learning objectives one wants to achieve. Each method or learning activity should have a function. These instructional functions, which are the activities of a teacher, correspond with the steps in the learning process described above and can help guide your selection of methods. There follows a list of the nine instructional functions:
- preparation
- motivation
- orientation
- transmitting new knowledge
- consolidating what has been taught
- practising (development of knowledge into skills)
- application (solving new problems with the help of new knowledge)
- programme critique
- participant evaluation.
Planning the curriculum: Charting your course
One of the functions of curriculum or course plan is to assist in guiding and monitoring the teaching and learning process. The curriculum can be divided into two parts, the general and the specific.
The general curriculum gives an overall picture of the course: its goals, objectives, contents, participants and guidelines for their selection, the teaching approach (how the course will be conducted) and the organizational arrangements, such as pre-course tasks. This general curriculum would usually be your course description and a draft programme or list of topics.
A specific curriculum provides detailed information on what one will teach and how one plans to teach it. A written curriculum prepared in chart form will serve as a good outline for designing a curriculum specific enough to serve as a guide in the implementation of the training. Such a chart includes the following categories:
Time: the estimated time needed for each learning activity
Curriculum Units: primary subject areas
Topics: themes within each curriculum unit
Instructional function: the function of each learning activity in helping to achieve your learning objectives
Activities: the steps for conducting each learning activity
Materials: the resources and materials needed for each activity
Instructor: the trainer responsible for each activity (when there are several trainers)
To design the curriculum with the aid of the chart format, follow the steps outlined below. Completed charts are illustrated in connection with a completed curriculum in Weinger 1993.
- Specify the primary subject areas of the course (curriculum units) which are based on your objectives and general orientation basis.
- List the topics you will cover in each of those areas.
- Plan to include as many instructional functions as possible in each subject area in order to advance through all the steps of the learning process.
- Choose methods which fulfil each function and estimate the amount of time required. Record the time, topic and function on the chart.
- In the activities column, provide guidelines for the instructor on how to conduct the activity. Entries can also include main points to be covered in this session. This column should offer a clear picture of exactly what will occur in the course during this time period.
- List the materials, such as worksheets, handouts or equipment required for each activity.
- Make sure to include appropriate breaks when designing a cycle of activities.
Evaluating the course and follow-up
The last step in the training process is evaluation and follow-up. Unfortunately, it is a step that is often forgotten, ignored and, sometimes, avoided. Evaluation, or the determination of the degree to which course objectives were met, is an essential component of training. This should include both programme critique (by the course administrators) and participant evaluation.
Participants should have an opportunity to evaluate the external factors of teaching: the instructor’s presentation skills, techniques used, facilities and course organization. The most common evaluation tools are post-course questionnaires and pre- and post-tests.
Follow-up is a necessary support activity in the training process. Follow-up activities should be designed to help the participants apply and transfer what they have learned to their jobs. Examples of follow-up activities for our TOT courses include:
- action plans and projects
- formal follow-up sessions or workshops
Selection of trainers
Trainers were selected who were familiar with the cognitive learning approach and had good communication skills. During the pilot course in 1992 we used international experts who had been involved in development of this learning approach during the 1980s in Finland. In the national courses we have had a mixture of experts: one international expert, one or two regional experts who had participated in the first pilot course and two to three national resource persons who either had responsibility for training in their own countries or who had participated earlier in this training approach. Whenever it was possible, project personnel also participated.
Discussion and Summary
Factory training needs assessment
The factory visit and subsequent practice teaching are a highlight of the workshop. This training activity was used for workplace training needs assessment (curriculum unit VI A, figure 1). The recommendation here would be to complete the background on theory and methods prior to the visit. In Ethiopia, we scheduled the visit prior to addressing ourselves to the question of teaching methods. While two factories were looked at, we could have extended the time for needs assessment by eliminating one of the factory visits. Thus, visiting groups will visit and focus on only that factory where they will be actually training.
The risk mapping component of the workshop (this is also part of curriculum unit VI A) was even more successful in Ethiopia than in Kenya. The risk maps were incorporated in the practice teaching in the factories and were highly motivating for the workers. In future workshops, we would stress that specific hazards be highlighted wherever they occur, rather than, for example, using a single green symbol to represent any of a variety of physical hazards. In this way, the extent of a particular type of hazard is more clearly reflected.
Training methods
The instructional methods focused on audio-visual techniques and the use of discussion starters. Both were quite successful. In a useful addition to the session on transparencies, the participants were asked to work in groups to develop a transparency of their own on the contents of an assigned article.
Flip charts and brainstorming were new teaching methods for participants. In fact, a flip chart was developed especially for the workshop. In addition to being an excellent training aid, the use of flip charts and “magic markers” is a very inexpensive and practical substitute for the overhead projector, which is unavailable to most inspectors in the developing countries.
Videotaped microteaching
“Microteaching”, or instruction in the classroom focusing on particular local problems, made use of videotape and subsequent critique by fellow participants and resource people, and was very successful. In addition to enhancing the working of external teaching methods, the taping was a good opportunity for comment on areas for improvement in content prior to the factory teaching.
A common error, however, was the failure to link discussion starters and brainstorm activities with the content or message of an activity. The method was perfunctorily executed, and its effect ignored. Other common errors were the use of excessively technical terminology and the failure to make the training relevant to the audience’s needs by using specific workplace examples. But the later presentations in the factory were designed to clearly reflect the criticisms that participants had received the day before.
Practice teaching in the factory
In their evaluation of the practice teaching sessions in the factory, participants were extremely impressed with the use of a variety of teaching methods, including audiovisuals, posters that they developed, flip charts, brainstorming, role plays, “buzz groups” and so on. Most groups also made use of an evaluation questionnaire, a new experience for them. Of particular note was their success in engaging their audiences, after having relied solely on the lecture method in the past. Common areas for improvement were time management and the use of overly technical terms and explanations. In the future, the resource persons should also try to ensure that all groups include the application and evaluation steps in the learning process.
Course planning as a training experience
During these two courses it was possible to observe significant changes in the participants’ understanding of the six steps in high quality learning.
In the last course a section on writing objectives, where each participant writes a series of instructional objectives, was added into the programme. Most participants had never written training objectives and this activity was extremely useful.
As for the use of the curriculum chart in planning, we have seen definite progress among all participants and mastery by some. This area could definitely benefit from more time. In future workshops, we would add an activity where participants use the chart to follow one topic through the learning process, using all of the instructional functions. There is still a tendency to pack the training with content material (topics) and to intersperse, without due consideration of their relevance, the various instructional functions throughout a series of topics. It is also necessary that trainers emphasize those activities that are chosen to accomplish the application step in the learning process, and that they acquire more practice in developing learners’ tasks. Application is a new concept for most and difficult to incorporate in the instructional process.
Finally the use of the term curriculum unit was difficult and sometimes confusing. The simple identification and ordering of relevant topic areas is an adequate beginning. It was also obvious that many other concepts of the cognitive learning approach were difficult, such as the concepts of orientation basis, external and internal factors in learning and teaching, instructional functions and some others.
In summary, we would add more time to the theory and curriculum development sections, as outlined above, and to the planning of future curriculum, which affords the opportunity of observing individual ability to apply the theory.
Conclusion
The ILO-FINNIDA African Safety and Health Project has undertaken a particularly challenging and demanding task: to change our ideas and old practices about learning and training. The problem with talking about learning is that learning has lost its central meaning in contemporary usage. Learning has come to be synonymous with taking in information. However, taking in information is only distantly related to real learning. Through real learning we re-create ourselves. Through real learning we become able to do something we were never able to do before (Senge 1990). This is the message in our Project’s new approach on learning and training.
Rehabilitation and Noise - Induced Hearing Loss
Raymond Hétu
* This article was written by Dr. Hétu shortly before his untimely death. His colleagues and friends consider it one memoriam to him.
Although this article deals with disability due to noise-exposure and hearing loss, it is included here because it also contains fundamental principles applicable to rehabilitation from disabilities arising from other hazardous exposures.
Psychosocial Aspects of Occupationally Induced Hearing Loss
Like all human experience, hearing loss caused by exposure to workplace noise is given meaning—it is qualitatively experienced and evaluated—by those whom it affects and by their social group. This meaning can, however, be a powerful obstacle to the rehabilitation of individuals suffering from occupationally induced hearing loss (Hétu and Getty 1991b). The chief reasons, as discussed below, are that the victims of hearing loss experience perceptual barriers related to the signs and effects of their deficiency and that the manifestation of overt signs of hearing loss is highly stigmatizing.
Communication problems due to the distorted perception of hearing
Difficulties in hearing and communication resulting from occupationally induced hearing loss are usually attributed to other causes, for example unfavourable conditions for hearing or communication or a lack of attention or interest. This erroneous attribution is observed in both the affected individual and among his or her associates and has multiple, although converging, causes.
- Internal ear injuries are invisible, and victims of this type of injury do not see themselves as physically injured by noise.
- Hearing loss per se progresses very insidiously. The virtually daily auditory fatigue due to workplace noise suffered by exposed workers makes the timely detection of irreversible alterations in hearing function a matter of the greatest difficulty. Individuals exposed to noise are never aware of tangible deteriorations of hearing capacity. In fact, in most workers exposed daily to harmful levels of noise, the increase in the auditory threshold is of the order of one decibel per year of exposure (Hétu, Tran Quoc and Duguay 1990). When hearing loss is symmetric and progressive, the victim has no internal reference against which to judge the induced hearing deficit. As a result of this insidious evolution of hearing loss, individuals undergo a very progressive change of habits, avoiding situations which place them at a disadvantage—without however explicitly associating this change with their hearing problems.
- The signs of hearing loss are very ambiguous and usually take the form of a loss of frequency discrimination, that is, a diminished ability to discriminate between two or more simultaneous acoustic signals, with the more intense signal masking the other(s). Concretely, this takes the form of varying degrees of difficulty in following conversations where reverberation is high or where background noise due to other conversations, televisions, fans, vehicle motors, and so forth, is present. In other words, the hearing capacity of individuals suffering from impaired frequency discrimination is a direct function of the ambient conditions at any given moment. Those with whom the victim comes into daily contact experience this variation in hearing capacity as inconsistent behaviour on the part of the affected individual and reproach him or her in terms like, “You can understand well enough when it suits your purpose”. The affected individual, on the other hand, considers his or her hearing and communication problems to be the result of background noise, inadequate articulation by those addressing him or her, or a lack of attention on their part. In this way, the most characteristic sign of noise-induced hearing loss fails to be recognized for what it is.
- The effects of hearing loss are usually experienced outside of the workplace, within the confines of family life. Consequently, problems are not associated with occupational exposure to noise and are not discussed with work colleagues suffering similar difficulties.
- Acknowledgement of hearing problems is usually triggered by reproaches from the victim’s family and social circles (Hétu, Jones and Getty 1993). Affected individuals violate certain implicit social norms, for example by speaking too loudly, frequently asking others to repeat themselves and turning the volume of televisions or radios up too high. These behaviours elicit the spontaneous—and usually derogatory—question, “Are you deaf?” from those around. The defensive behaviours that this triggers do not favour the acknowledgement of partial deafness.
As a result of the convergence of these five factors, individuals suffering from occupationally induced hearing loss do not recognize the effects of their affliction on their daily lives until the loss is well advanced. Typically, this occurs when they find themselves frequently asking people to repeat themselves (Hétu, Lalonde and Getty 1987). Even at this point, however, victims of occupationally induced hearing loss are very unwilling to acknowledge their hearing loss on account of the stigma associated with deafness.
Stigmatization of the signs of deafness
The reproaches elicited by the signs of hearing loss are a reflection of the extremely negative value construct typically associated with deafness. Workers exhibiting signs of deafness risk being perceived as abnormal, incapable, prematurely old, or handicapped—in short, they risk becoming socially marginalized in the workplace (Hétu, Getty and Waridel 1994). These workers’ negative self-image thus intensifies as their hearing loss progresses. They are obviously reluctant to embrace this image, and by extension, to acknowledge the signs of hearing loss. This leads them to attribute their hearing and communication problems to other factors and to become passive in the face of these factors.
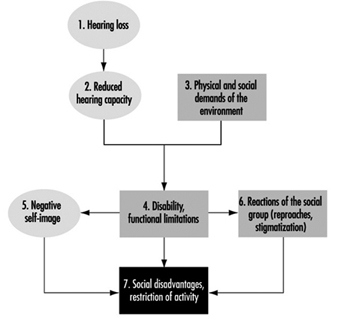
The combined effect of the stigma of deafness and the distorted perception of the signs and effects of hearing loss on rehabilitation is illustrated in figure 1.
Figure 1. Conceptual framework for incapacity from handicap

When hearing problems progress to the point that it is no longer possible to deny or minimize them, individuals attempt to hide the problem. This invariably leads to social withdrawal on the part of the worker and exclusion on the part of the worker’s social group, which ascribes the withdrawal to a lack of interest in communicating rather than to hearing loss. The result of these two reactions is that the affected individual is not offered help or informed of coping strategies. Workers’ dissimulation of their problems may be so successful that family members and colleagues may not even realize the offensive nature of their jokes elicited by the signs of deafness. This situation only exacerbates the stigmatization and its resultant negative effects. As Figure 1 illustrates, the distorted perceptions of the signs and effects of hearing loss and the stigmatization which results from these perceptions are barriers to the resolution of hearing problems. Because affected individuals are already stigmatized, they initially refuse to use hearing aids, which unmistakably advertise deafness and so promote further stigmatization.
The model presented in Figure 1 accounts for the fact that most people suffering occupationally induced hearing loss do not consult audiology clinics, do not request modification of their workstations and do not negotiate enabling strategies with their families and social groups. In other words, they endure their problems passively and avoid situations which advertise their auditory deficit.
Conceptual Framework of Rehabilitation
For rehabilitation to be effective, it is necessary to overcome the obstacles outlined above. Rehabilitative interventions should therefore not be limited to attempts to restore hearing capacity, but should also address issues related to the way hearing problems are perceived by affected individuals and their associates. Because stigmatization of deafness is the greatest obstacle to rehabilitation (Hétu and Getty 1991b; Hétu, Getty and Waridel 1994), it should be the primary focus of any intervention. Effective interventions should therefore include both stigmatized workers and their circles of family, friends, colleagues and others with whom they come into contact, since it is they who stigmatize them and who, out of ignorance, impose impossible expectations on them. Concretely, it is necessary to create an environment which allows affected individuals to break out of their cycle of passivity and isolation and actively seek out solutions to their hearing problems. This must be accompanied by a sensitization of the entourage to the specific needs of affected individuals. This process is grounded in the ecological approach to incapacity and handicap illustrated in figure 2.
Figure 2. Model of restrictions due to hearing loss
In the ecological model, hearing loss is experienced as an incompatibility between an individual’s residual capacity and the physical and social demands of his or her environment. For example, workers suffering from a loss of frequency discrimination associated with noise-induced hearing loss will have difficulty detecting acoustic alarms in noisy workplaces. If the alarms required at workstations cannot be adjusted to levels significantly louder than those appropriate for people with normal hearing, the workers will be placed in a handicapped position (Hétu 1994b). As a result of this handicap, workers may be at the obvious disadvantage of being deprived of a means to protect themselves. Yet, simply acknowledging hearing loss puts the worker at risk of being considered “abnormal” by his or her colleagues, and when labelled disabled he or she will fear being seen as incompetent by colleagues or superiors. In either case, workers will attempt to hide their handicap or deny the existence of any problems, placing themselves at a functional disadvantage at work.
As figure 2 illustrates, disability is a complex state of affairs with several interrelated restrictions. In such a network of relationships, prevention or minimization of disadvantages or restrictions of activity require simultaneous interventions on many fronts. For example, hearing aids, while partially restoring hearing capacity (component 2), do not prevent either the development of a negative self-image or stigmatization by the worker’s entourage (components 5 and 6), both of which are responsible for isolation and avoidance of communication (component 7). Further, auditory supplementation is incapable of completely restoring hearing capacity; this is particularly true with regard to frequency discrimination. Amplification may improve the perception of acoustic alarms and of conversations but is incapable of improving the resolution of competing signals required for the detection of warning signals in the presence of significant background noise. The prevention of disability-related restrictions therefore necessitates the modification of the social and physical demands of the workplace (component 3). It should be superfluous to note that although interventions designed to modify perceptions (components 5 and 6) are essential and do prevent disability from arising, they do not palliate the immediate consequences of these situations.
Situation-specific Approaches to Rehabilitation
The application of the model presented in Figure 2 will vary depending on the specific circumstances encountered. According to surveys and qualitative studies (Hétu and Getty 1991b; Hétu, Jones and Getty 1993; Hétu, Lalonde and Getty 1987; Hétu, Getty and Waridel 1994; Hétu 1994b), the effects of disability suffered by victims of occupationally induced hearing loss are particularly felt: (1) at the workplace; (2) at the level of social activities; and (3) at the family level. Specific intervention approaches have been proposed for each of these situations.
The workplace
In industrial workplaces, it is possible to identify the following four restrictions or disadvantages requiring specific interventions:
- accident hazards related to the failure to detect warning signals
- efforts, stress and anxiety resulting from hearing and com-munication problems
- obstacles to social integration
- obstacles to professional advancement.
Accident hazards
Acoustic warning alarms are frequently used in industrial workplaces. Occupationally induced hearing loss may considerably diminish workers’ ability to detect, recognize or locate such alarms, particularly in noisy workplaces with high levels of reverberation. The loss of frequency discrimination which inevitably accompanies hearing loss may in fact be so pronounced as to require warning alarms to be 30 to 40db louder than background levels to be heard and recognized by affected individuals (Hétu 1994b); for individuals with normal hearing, the corresponding value is approximately 12 to 15db. Currently, it is rare that warning alarms are adjusted to compensate for background noise levels, workers’ hearing capacity or the use of hearing protection equipment. This puts affected workers at a serious disadvantage, especially as far as their safety is concerned.
Given these constraints, rehabilitation must be based on a rigorous analysis of the compatibility of auditory perception requirements with residual auditory capacities of affected workers. A clinical examination capable of characterizing an individual’s ability to detect acoustic signals in the presence of background noise, such as the DetectsoundTM software package (Tran Quoc, Hétu and Laroche 1992), has been developed, and is available to determine the characteristics of acoustic signals compatible with workers’ hearing capacity. These devices simulate normal or impaired auditory detection and take into account the characteristics of the noise at the workstation and the effect of hearing protection equipment. Of course, any intervention aimed at reducing the noise level will facilitate the detection of acoustic alarms. It is nevertheless necessary to adjust the alarms’ level as a function of the residual hearing capacity of affected workers.
In some cases of relatively severe hearing loss, it may be necessary to resort to other types of warning, or to supplement hearing capacity. For example, it is possible to transmit warning alarms over FM bandwidths and receive them with a portable unit connected directly to a hearing aid. This arrangement is very effective as long as: (1) the tip of the hearing aid fits perfectly (in order to attenuate background noise); and (2) the response curve of the hearing aid is adjusted to compensate for the masking effect of background noise attenuated by the hearing aid tip and the worker’s hearing capacity (Hétu, Tran Quoc and Tougas 1993). The hearing aid may be adjusted to integrate the effects of the full spectrum of background noise, the attenuation produced by the hearing aid’s tip, and the worker’s hearing threshold. Optimal results will be obtained if the frequency discrimination of the worker is also measured. The hearing aid-FM receptor may also be used to facilitate verbal communication with work colleagues when this is essential for worker safety.
In some cases, the workstation itself must be redesigned in order to ensure worker safety.
Hearing and communication problems
Acoustic warning alarms are usually used to inform workers of the state of a production process and as a means of inter operator communication. In workplaces where such alarms are used, individuals with hearing loss must rely upon other sources of information to perform their work. These may involve intense visual surveillance and discreet help offered by work colleagues. Verbal communication, whether over the telephone, in committee meetings or with superiors in noisy workshops, requires great effort on the part of affected individuals and is also highly problematic for affected individuals in industrial workplaces. Because these individuals feel the need to hide their hearing problems, they are also plagued by the fear of being unable to cope with a situation or of committing costly errors. Often, this may cause extremely high anxiety (Hétu and Getty 1993).
Under these circumstances, rehabilitation must first focus on eliciting explicit acknowledgement by the company and its representatives of the fact that some of their workers suffer from hearing difficulties caused by noise exposure. The legitimization of these difficulties helps affected individuals to communicate about them and to avail themselves of appropriate palliative means. However, these means must in fact be available. In this regard, it is astonishing to note that telephone receivers in the workplace are rarely equipped with amplifiers designed for individuals suffering from hearing loss and that conference rooms are not equipped with appropriate systems (FM or infrared transmitters and receptors, for example). Finally, a campaign to increase awareness of the needs of individuals suffering from hearing loss should be undertaken. By publicizing strategies which facilitate communication with affected individuals, communication-related stress will be greatly reduced. These strategies consist of the following phases:
- approaching the affected individual and facing him or her
- articulating without exaggeration
- repeating misunderstood phrases, using different words
- keeping as far away from sources of noise as possible
Clearly, any control measures that lead to lower noise and reverberation levels in the workplace also facilitate communication with individuals suffering from hearing loss.
Obstacles to social integration
Noise and reverberation in the workplace render communication so difficult that it is often limited to the strict minimum required by the tasks to be accomplished. Informal communication, a very important determinant of the quality of working life, is thus greatly impaired (Hétu 1994a). For individuals suffering from hearing loss, the situation is extremely difficult. Workers suffering from occupationally induced hearing loss are isolated from their work colleagues, not only at their workstation but even during breaks and meals. This is a clear example of the convergence of excessive work requirements and the fear of ridicule suffered by affected individuals.
The solutions to this problem lie in the implementation of the measures already described, such as the lowering of overall noise levels, particularly in rest areas, and the sensitization of work colleagues to the needs of affected individuals. Again, recognition by the employer of affected individuals’ specific needs itself constitutes a form of psychosocial support capable of limiting the stigma associated with hearing problems.
Obstacles to professional advancement
One of the reasons individuals suffering from occupationally induced hearing loss take such pains to hide their problem is the explicit fear of being disadvantaged professionally (Hétu and Getty 1993): some workers even fear losing their jobs should they reveal their hearing loss. The immediate consequence of this is a self-restriction with regard to professional advancement, for example, failure to apply for a promotion to shift supervisor, supervisor or foreman. This is also true of professional mobility outside the company, with experienced workers failing to take advantage of their accumulated skills since they feel that pre-employment audiometric examinations would block their access to better jobs. Self-restriction is not the only obstacle to professional advancement caused by hearing loss. Workers suffering from occupationally induced hearing loss have in fact reported instances of employer bias when positions requiring frequent verbal communication have become available.
As with the other aspects of disability already described, explicit acknowledgement of affected workers’ specific needs by employers greatly eliminates obstacles to professional advancement. From the standpoint of human rights (Hétu and Getty 1993), affected individuals have the same right to be considered for advancement as do other workers, and appropriate workplace modifications can facilitate their access to higher-level jobs.
In summary, the prevention of disability in the workplace requires sensitization of employers and work colleagues to the specific needs of individuals suffering from occupationally induced hearing loss. This can be accomplished by information campaigns on the signs and effects of noise-induced hearing loss aimed at dissipating the view of hearing loss as an improbable abnormality of little import. The use of technological aids is possible only if the need to use them has been legitimized in the workplace by colleagues, superiors and affected individuals themselves.
Social activities
Individuals suffering from occupationally induced hearing loss are at a disadvantage in any non-ideal hearing situation, for instance, in the presence of background noise, in situations requiring communication at a distance, in environments where reverberation is high and on the telephone. In practice, this greatly curtails their social life by limiting their access to cultural activities and public services, thus hindering their social integration (Hétu and Getty 1991b).
Access to cultural activities and public services
In accordance with the model in Figure 2, restrictions related to cultural activities involve four components (components 2, 3, 5 and 6) and their elimination relies on multiple interventions. Thus concert halls, auditoriums and places of worship can be made accessible to persons suffering from hearing loss by equipping them with appropriate listening systems, such as FM or infrared transmission systems (component 3) and by informing those responsible for these institutions of the needs of affected individuals (component 6). However, affected individuals will request hearing equipment only if they are aware of its availability, know how to use it (component 2) and have received the necessary psychosocial support to recognize and communicate their need for such equipment (component 5).
Effective communication, training and psychosocial support channels for hearing-impaired workers have been developed in an experimental rehabilitation programme (Getty and Hétu 1991, Hétu and Getty 1991a), discussed in “Family life”, below.
As regards the hearing-impaired, access to public services such as banks, stores, government services and health services is hindered primarily by a lack of knowledge on the part of the institutions. In banks, for example, glass screens may separate clients from tellers, who may be occupied in entering data or filling out forms while talking to clients. The resulting lack of face-to-face visual contact, coupled with unfavourable acoustic conditions and a context in which misunderstanding can have very serious consequences, render this an extremely difficult situation for affected individuals. In health service facilities, patients wait in relatively noisy rooms where their names are called by an employee located at a distance or via a public address system that may be difficult to comprehend. While individuals with hearing loss worry a great deal about being unable to react at the correct time, they generally neglect to inform staff of their hearing problems. There are numerous examples of this type of behaviour.
In most cases, it is possible to prevent these handicap situations by informing staff of the signs and effects of partial deafness and of ways to facilitate communication with affected individuals. A number of public services have already undertaken initiatives aimed at facilitating communication with individuals suffering from occupationally induced hearing loss (Hétu, Getty and Bédard 1994) with results as follows. The use of appropriate graphical or audio visual material allowed the necessary information to be communicated in less than 30 minutes and the effects of such initiatives were still apparent six months after the information sessions. These strategies greatly facilitated communication with the personnel of the services involved. Very tangible benefits were reported not only by clients with hearing loss but also by the staff, who saw their tasks simplified and difficult situations with this type of client prevented.
Social integration
Avoidance of group encounters is one of the most severe consequences of occupationally induced hearing loss (Hétu and Getty 1991b). Group discussions are extremely demanding situations for affected individuals, In this case, the burden of accommodation rests with the affected individual, as he or she can rarely expect the entire group to adopt a favourable rhythm of conversation and mode of expression. Affected individuals have three strategies available to them in these situations:
- reading facial expressions
- using specific communication strategies
- using a hearing aid.
The reading of facial expressions (and lip-reading) can certainly facilitate comprehension of conversations, but requires considerable attention and concentration and cannot be sustained over long periods. This strategy can, however, be usefully combined with requests for repetition, reformulation and summary. Nevertheless, group discussions occur at such a rapid rhythm that it is often difficult to rely upon these strategies. Finally, the use of a hearing aid may improve the ability to follow conversation. However, current amplification techniques do not allow the restoration of frequency discrimination. In other words, both signal and noise are amplified. This often worsens rather than improves the situation for individuals with serious frequency discrimination deficits.
The use of a hearing aid as well as the request for accommodation by the group presupposes that the affected individual feels comfortable revealing his or her condition. As discussed below, interventions aimed at strengthening self-esteem are therefore prerequisites for attempts to supplement auditory capacity.
Family life
The family is the prime locus of the expression of hearing problems caused by occupational hearing loss (Hétu, Jones and Getty 1993). A negative self-image is the essence of the experience of hearing loss, and affected individuals attempt to hide their hearing loss in social interactions by listening more intently or by avoiding overly demanding situations. These efforts, and the anxiety which accompanies them, create a need for release in the family setting, where the need to hide the condition is less strongly felt. Consequently, affected individuals tend to impose their problems on their families and coerce them to adapt to their hearing problems. This takes a toll on spouses and others and causes irritation at having to repeat oneself frequently, tolerate high television volumes and “always be the one to answer the telephone”. Spouses must also deal with serious restrictions in the couples’ social life and with other major changes in family life. Hearing loss limits companionship and intimacy, creates tension, misunderstandings and arguments and disturbs relations with children.
Not only does hearing and communication impairment affect intimacy, but its perception by affected individuals and their family (components 5 and 6 of figure 2) tends to feed frustration, anger and resentment (Hétu, Jones and Getty 1993). Affected individuals frequently do not recognize their impairment and do not attribute their communications problems to a hearing deficit. As a result, they may impose their problems on their families rather than negotiate mutually satisfactory adaptations. Spouses, on the other hand, tend to interpret the problems as a refusal to communicate and as a change in the affected individual’s temperament. This state of affairs may lead to mutual reproaches and accusations, and ultimately to isolation, loneliness and sadness, particularly on the part of the unaffected spouse.
The solution of this interpersonal dilemma requires the participation of both partners. In fact, both require:
- information on the auditory basis of their problems.
- psychosocial support
- training in the use of appropriate supplemental means of communication.
With this in mind, a rehabilitation programme for affected individuals and their spouses has been developed (Getty and Hétu 1991, Hétu and Getty 1991a). The goal of the programme is to stimulate research on the resolution of problems caused by hearing loss, taking into account the passivity and social withdrawal that characterize occupationally induced hearing loss.
Since the stigma associated with deafness is the principal source of these behaviours, it was essential to create a setting in which self-esteem could be restored so as to induce affected individuals to seek out actively solutions to their hearing-related problems. The effects of stigmatization can be overcome only when one is perceived by others as normal regardless of any hearing deficit. The most effective way to achieve this consists of meeting other people in the same situation, as was suggested by workers asked about the most appropriate aid to offer their hearing-impaired colleagues. However, it is essential that these meetings take place outside the workplace, precisely to avoid the risk of further stigmatization (Hétu, Getty and Waridel 1994).
The rehabilitation programme mentioned above was developed with this in mind, the group encounters taking place in a community health department (Getty and Hétu 1991). Recruitment of participants was an essential component of the programme, given the withdrawal and passivity of the target population. Accordingly, occupational health nurses first met with 48 workers suffering from hearing loss and their spouses at their homes. Following an interview on hearing problems and their effects, every couple was invited to a series of four weekly meetings lasting two hours each, held in the evening. These meetings followed a precise schedule aimed at meeting the objectives of information, support and training defined in the programme. Individual follow-up was provided to participants in order to facilitate their access to audio-logical and audioprosthetic services. Individuals suffering from tinnitus were referred to the appropriate services. A further group meeting was held three months after the last weekly meeting.
The results of the programme, collected at the end of the experimental phase, demonstrated that participants and their spouses were more aware of their hearing problems, and were also more confident of resolving them. Workers had undertaken various steps, including technical aids, revealing their impairment to their social group, and expressing their needs in an attempt to improve communication.
A follow-up study, performed with this same group five years after their participation in the programme, demonstrated that the programme was effective in stimulating participants to seek solutions. It also showed that rehabilitation is a complex process requiring several years of work before affected individuals are able to avail themselves of all the means at their disposal to regain their social integration. In most cases, this type of rehabilitation process requires periodic follow-up.
Conclusion
As figure 2 indicates, the meaning that individuals suffering from occupationally induced hearing loss and their associates give to their condition is a key factor in handicap situations. The approaches to rehabilitation proposed in this article explicitly take this factor into account. However, the manner in which these approaches are applied concretely will depend on the specific sociocultural context, since the perception of these phenomena may vary from one context to another. Even within the sociocultural context in which the intervention strategies described above were developed, significant modifications may be necessary. For example, the programme developed for individuals suffering from occupationally induced hearing loss and their spouses (Getty and Hétu 1991) was tested in a population of affected males. Different strategies would probably be necessary in a population of affected females, especially when one considers the different social roles men and women occupy in conjugal and parental relations (Hétu, Jones and Getty 1993). Modifications would be necessary a fortiori when dealing with cultures which differ from that of North America from which the approaches emerged. The conceptual framework proposed (figure 2) can nevertheless be used effectively to orient any intervention aimed at rehabilitating individuals suffering from occupationally induced hearing loss.
Furthermore, this type of intervention, if applied on a large scale, will have important preventive effects on hearing loss itself. The psychosocial aspects of occupationally induced hearing loss hinder both rehabilitation (figure 1) and prevention. The distorted perception of hearing problems delays their recognition, and their dissimulation by severely affected individuals fosters the general perception that these problem are rare and relatively innocuous, even in noisy workplaces. This being so, noise-induced hearing loss is not perceived by workers at risk or by their employers as an important health problem, and the need for prevention is thus not strongly felt in noisy workplaces. On the other hand, individuals already suffering from hearing loss who reveal their problems are eloquent examples of the severity of the problem. Rehabilitation can thus be seen as the first step of a prevention strategy.
Rights and Duties: An Employer's Perspective
The traditional approach to helping disabled people into work has had little success, and it is evident that something fundamental needs to be changed. For example, the official unemployment rates for disabled people are always at least twice that of their non-disabled peers—often higher. The numbers of disabled people not working often approach 70% (in the United States, United Kingdom, Canada). Disabled people are more likely than their non-disabled peers to live in poverty; for example, in the United Kingdom two-thirds of the 6.2 million disabled citizens have only state benefits as income.
These problems are compounded by the fact that rehabilitation services are often unable to meet employer demand for qualified applicants.
In many countries, disability is not generally defined as an equal opportunities or rights issue. It is thus difficult to encourage corporate best practice which positions disability firmly alongside race and gender as an equal opportunities or diversity priority. Proliferation of quotas or the complete absence of relevant legislation reinforces employer assumptions that disability is primarily a medical or charity issue.
Evidence of the frustrations created by inadequacies inherent in the present system can be seen in growing pressure from disabled people themselves for legislation based on civil rights and/or employment rights, such as exists in the United States, Australia, and, from 1996, in the United Kingdom. It was the failure of the rehabilitation system to meet the needs and expectations of enlightened employers which prompted the UK business community to establish the Employers Forum on Disability.
Employers’ attitudes unfortunately reflect those of the wider society—although this fact is often overlooked by rehabilitation practitioners. Employers share with many others widespread confusion regarding such issues as:
- What is a disability? Who is and who is not disabled?
- Where do I get advice and services to help me recruit and retain disabled people?
- How do I change my organization’s culture and working practices?
- What benefit will best practice on disability bring my business—and the economy in general?
The failure to meet the information and service needs of the employer community constitutes a major hurdle for disabled people wanting work, yet it is rarely addressed adequately by government policy makers or rehabilitation practitioners.
Deep-Rooted Myths that Disadvantage Disabled People in the Labour Market
Non-governmental organizations (NGOs), governments, indeed all those involved in the medical and employment rehabilitation of persons with disabilities, tend to share a set of deep-rooted, often unspoken assumptions which only further disadvantage the disabled individuals these organizations seek to help:
- “The employer is the problem—indeed, often the adversary.” It is employer attitudes which are often blamed for the failure of disabled people to find jobs, despite the evidence that numerous other factors may well have been highly significant.
- “The employer is not treated either as a client or a customer.” Rehabilitation services do not measure their success by the extent to which they make it easier for the employer to recruit and retain disabled employees. As a result, the unreasonable difficulties created by suppliers of rehabilitation services make it difficult for the well-intentioned and enlightened employer to justify the time, cost and effort required to effect change. The not-so-enlightened employer has his or her reluctance to effect change more than justified by the lack of cooperation from rehabilitation services..
- “Disabled people really cannot compete on merit.” Many service providers have low expectations of disabled people and their potential to work. They find it difficult to promote the “business case” to employers because they themselves doubt that employing people with disability brings genuine mutual benefit. Instead the tone and underlying ethos of their communication with employers stresses the moral and perhaps (occasional) legal obligation in a way which only further stigmatizes disabled people.
- “Disability is not a mainstream economic or business issue. It is best left in the hands of the experts, doctors, rehabilitation providers and charities.” The fact that disability is portrayed in the media and through fund-raising activities as a charity issue, and that disabled people are portrayed as the natural and passive recipients of charity, is a fundamental barrier to the employment of disabled people. It also creates tension in organizations that are trying to find jobs for people, while on the other hand using images which tug at the heartstrings.
The consequence of these assumptions is that:
- Employers and disabled people remain separated by a maze of well-meaning but often uncoordinated and fragmented services which only rarely define success in terms of employer satisfaction.
- Employers and disabled people alike remain excluded from real influence over policy development; only rarely is either party asked to evaluate services from its own perspective and to propose improvements.
We are beginning to see an international trend, typified by the development of “job coach” services, towards acknowledging that successful rehabilitation of disabled people depends upon the quality of service and support available to the employer.
The statement “Better services for employers equals better services for disabled people” must surely come to be much more widely accepted as economic pressures build on rehabilitation agencies everywhere in the light of governments’ retrenchment and restructuring. It is nonetheless very revealing that a recent report by Helios (1994), which summarizes the competencies required by vocational or rehabilitation specialists, fail to make any reference to the need for skills which relate to the employers as customer.
While there is a growing awareness of the need to work with employers as partners, our experience shows that it is difficult to develop and sustain a partnership until the rehabilitation practitioners first meet the needs of the employer as customer and begin to value that “employer as customer” relationship.
Employers’ Roles
At various times and in various situations the system and services position the employer in one or more of the following roles—though only rarely is it articulated. Thus we have the employer as:
- the Problem—“you require enlightenment”
- the Target—“you need education, information, or consciousness raising”
- the Customer—“the employer is encouraged to use us in order to recruit and retain disabled employees”
- the Partner—the employer is encouraged to “enter into a long term, mutually beneficial relationship”.
And at any time during the relationship the employer may be called upon—indeed is typically called upon—to be a funder or philanthropist.
The key to successful practice lies in approaching the employer as “The Customer”. Systems which regard the employer as only “The Problem”, or “The Target”, find themselves in a self-perpetuating dysfunctional cycle.
Factors outside the Employer’s Control
Reliance on perceived employer negative attitudes as the key insight into why disabled people experience high unemployment rates, consistently reinforces the failure to address other highly significant issues which must also be tackled before real change can be brought about.
For example:
- In the United Kingdom, in a recent survey 80% of employers were not aware they had ever had a disabled applicant.
- Benefits and social welfare systems often create financial disincentives for disabled people moving into work.
- Transport and housing systems are notoriously inaccessible; people can look for work successfully only when basic housing, transport and subsistence needs have been met.
- In a recent UK survey, 59% of disabled job seekers were unskilled compared to 23% of their peers. Disabled people, in general, are simply not able to compete in the labour market unless their skill levels are competitive.
- Medical professionals frequently underestimate the extent to which a disabled person can perform in work and are often unable to advise on adaptations and adjustments which might make that person employable.
- Disabled people often find it difficult to obtain high quality career guidance and throughout their lives are subject to the lower expectations of teachers and advisers.
- Quotas and other inappropriate legislation actively undermine the message that disability is an equal opportunities issue.
A legislative system that creates an adversarial or litigious environment can further undermine the job prospects of disabled people because bringing a disabled person into the company could expose the employer to risk.
Rehabilitation practitioners often find it difficult to access expert training and accreditation and are themselves rarely funded to deliver relevant services and products to employers.
Policy Implications
It is vital for service providers to understand that before the employer can effect organizational and cultural change, similar changes are required on the part of the rehabilitation provider. Providers approaching employers as customers need to recognize that actively listening to the employers will almost inevitably trigger the need to change the design and delivery of services.
For example, service providers will find themselves asked to make it easier for the employer to:
- find qualified applicants
- obtain high quality employer-oriented services and advice
- meet disabled people as applicants and colleagues
- understand not just the need for policy change but how to make such change come about
- promote attitude change across their organizations
- understand the business as well as the social case for employing disabled people
Attempts at significant social policy reforms related to disability are undermined by the failure to take into account the needs, expectations and legitimate requirements of the people who will largely determine success—that is, the employers. Thus, for example, the move to ensure that people currently in sheltered workshops obtain mainstream work frequently fails to acknowledge that it is only employers who are able to offer that employment. Success therefore is limited, not only because it is unnecessarily difficult for the employers to make opportunities available but also because of the missed added value resulting from active collaboration between employers and policy makers.
Potential for Employer Involvement
Employers can be encouraged to contribute in numerous ways to making a systematic shift from sheltered employment to supported or competitive employment. Employers can:
- advise on policy—that is, on what needs to be done which would make it easier for employers to offer work to disabled candidates.
- offer advice on the competencies required by disabled individ-uals if they are to be successful in obtaining work.
- advise on the competencies required by service providers if they are to meet employer expectations of quality provision.
- evaluate sheltered workshops and offer practical advice on how to manage a service that is most likely to enable people to move into mainstream work.
- offer work experience to rehabilitation practitioners, who thus gain an understanding of a particular industry or sector and are better able to prepare their disabled clients.
- offer on-the-job assessments and training to disabled individuals.
- offer mock interviews and be mentors to disabled job seekers.
- loan their own staff to work inside the system and/or its institutions.
- help to market rehabilitation agencies and promote policies, organizations and disabled job seekers to other employers.
- offer customized training whereby they become directly involved in helping disabled individuals to acquire specific job-related skills.
- participate on management boards of rehabilitation agencies or set themselves up in an informal advisory capacity to national policy makers or suppliers.
- lobby alongside rehabilitation providers and disabled people for better government policies and programmes.
- advise on the services and products they require in order to deliver best practice.
Employer as Customer
It is impossible for rehabilitation practitioners to build partnerships with employers without first acknowledging the need to deliver efficient services.
Services should emphasize the theme of mutual benefit. Those who do not passionately believe that their disabled clients have something of real benefit to contribute to the employer are unlikely to be able to influence the employer community.
Improving the quality of service to employers will quickly—and inevitably—improve services for disabled job-seekers. The following represents a useful audit for services wishing to improve the quality of service to the employer.
Does the service offer employers:
1. information and consultancy regarding:
- business benefits which result from employing disabled persons
- possible applicants
- access to the services and the nature of services offered
- models of policy and procedures proven successful by other employers
- legal obligations
2. recruitment services, including access to:
- suitable applicants
- job coaches
3. pre-screening of applicants as per employer expectations
4. professional job analysis and job modification services, able to advise on job restructuring and the use of technical aids and adaptations in the workplace, both for existing and potential employees
5. financial support programmes which are well marketed, appropriate to employer requirements, easy to access, efficiently delivered
6. information and practical help so that employers can make the worksite more physically accessible
7. training for employers and employees regarding the benefits of employing people with disabilities generally, and when specific individuals have been employed
8. work-experience services which provide the employer with relevant support
9. work habituation or employee-orientation services to include job coaches and job-sharing schemes
10. post–job offer support for employers to include advice on best practice in the management of absenteeism and presentation of work-related impairments
11. advice for employers on career development of disabled employees and on meeting the needs of underemployed disabled employees.
Practical Steps: Making it Easier for the Employer
Any system of services which aims to help disabled people into training and work will inevitably be more successful if the needs and expectations of the employer are adequately addressed. (Note: It is difficult to find a term which adequately encompasses all those agencies and organizations—governmental, NGOs, not for profit—which are involved in policy making and service delivery to disabled people seeking work. For the sake of brevity, the term service or service provider is used to encompass all those involved in this entire complex system.)
Close consultation over time with employers will in all likelihood produce recommendations similar to the following.
Codes of practice are needed which describe the high quality of service employers should receive from employment-related agencies. Such codes should, in consultation with employers, set standards which relate both to the efficiency of the existing services and to the nature of services offered—This code should be monitored via regular surveys of employer satisfaction.
Specific training and accreditation for rehabilitation practition-ers in how to meet the needs of employers is required and should be a high priority.
Services should recruit people who have direct experience of the world of industry and commerce and who are skilled in bridging the communication gap between the not-for-profit and profit-making sectors.
Services themselves should employ significantly more disabled people, thus minimizing the numbers of non-disabled intermediaries dealing with employers. They should ensure that disabled people in various capacities have a high profile in the employer community.
Services should minimize the fragmentation of education, marketing and campaigning activities. It is particularly counterproductive to create a milieu characterized by messages, posters and advertising which reinforces the medical model of disability and the stigma attached to particular impairments, rather than focusing on the employability of individuals and the need for employers to respond with appropriate policy and practice.
Services should collaborate to simplify access, to services and support, for both the employer and for the disabled person. Considerable attention should be given to analysing the client journey (with both employer and disabled person as client) in a way that minimizes assessments and moves the individual speedily, step by step, into employment. Services should build on mainstream business initiatives to ensure that disabled people are given priority.
Services should bring employers together routinely and ask their expert advice regarding what has to be done to make services and job candidates more successful.
Conclusion
In many countries, the services designed to help disabled people into work are complex, cumbersome and resistant to change, despite the evidence decade after decade that change is required.
A fresh approach to employers offers enormous potential to transform this situation significantly by radically altering the position of one key protagonist—the employer.
We see business and government engaged in a wide-ranging debate regarding the way in which relationships between stakeholders or social partners must inevitably change over the next 20 years. Thus employers launch the European Business against Social Exclusion Initiative in Europe, major companies join together to re-think their relationship with society in the UK in “Tomorrow’s Company”, and the Employers Forum on Disability becomes only one of various UK employer initiatives aimed at addressing issues of equality and diversity.
Employers have much to do if the issue of disability is to take its rightful place as a business and ethical imperative; the rehabilitation community in turn needs to take a fresh approach which redefines working relationships between all stakeholders in a way that makes it easier for employers to make equal opportunities a reality.
Rights and Duties: Workers' Perspective
Historically, people with disabilities have had tremendous barriers to entering the workforce, and those who became injured and disabled on the job have often faced job loss and its negative psychological, social and financial ramifications. Today, people with disabilities are still underrepresented in the workforce, even in countries with the most progressive civil rights and employment promotion legislation, and in spite of international efforts to address their situation.
Awareness has increased of the rights and needs of workers with disabilities and the concept of managing disability in the workplace. Workers’ compensation and social insurance programmes that protect income are common in industrialized countries. The increased costs related to operating such programmes have provided an economic basis for promoting the employment of people with disabilities and the rehabilitation of injured workers. At the same time, people with disabilities have become organized to demand their rights and integration into all aspects of community life, including the workforce.
Labour unions in many countries have been among those who have supported such efforts. Enlightened companies are recognizing the need to treat workers with disabilities equitably and are learning the importance of maintaining a healthy workplace. The concept of managing disability or dealing with disability issues in the workplace has emerged. Organized labour has been partly responsible for this emergence and continues to play an active role.
According to ILO Recommendation No. 168 concerning the vocational rehabilitation and employment of disabled persons, “workers’ organizations should adopt a policy for the promotion of training and suitable employment of disabled persons on an equal footing with other workers”. The recommendation further suggests that workers’ organizations become involved in formulating national policies, cooperate with rehabilitation specialists and organizations, and foster the integration and vocational rehabilitation of disabled workers.
The purpose of this article is to explore the issue of disability in the workplace from the perspective of the rights and duties of workers and to describe the specific role that labour unions play in facilitating the on-the-job integration of people with disabilities.
In a healthy work environment, both the employer and the worker care about the quality of work, health and safety, and the fair treatment of all workers. Workers are hired on the basis of their abilities. Both workers and employers contribute to maintaining health and safety and, when an injury or disability does occur, they have the rights and duties to minimize the impact of the disability on the individual and the workplace. Although workers and employers may have different perspectives, by working in partnership they can effectively achieve goals related to maintaining a healthy, safe and fair workplace.
The term rights is often associated with legal rights determined by legislation. Many European countries, Japan and others have enacted quota systems requiring that a certain percentage of employees be persons with disabilities. Fines may be levied on employers who fail to meet the prescribed quota. In the United States, the Americans with Disabilities Act (ADA) prohibits discrimination against people with disabilities in work and community life. Health and safety laws exist in most countries to protect workers from unsafe working conditions and practices. Workers’ compensation and social insurance programmes have been legislated to provide a variety of medical, social, and, in some instances, vocational rehabilitation services. Specific workers’ rights may also become part of negotiated labour agreements and therefore legally mandated.
A worker’s legal rights (and duties) related to disability and work will depend on the complexity of this legislative mix, which varies from country to country. For purposes of this article, workers’ rights are simply those legal or moral entitlements considered to be in the workers’ interest as they relate to productive activity in a safe and non-discriminating work environment. Duties refer to those obligations that workers have to themselves, other workers and their employers to contribute effectively to the productivity and safety of the workplace.
This article organizes worker rights and duties within the context of four key disability issues: (1) recruitment and hiring; (2) health, safety and the prevention of disability; (3) what happens when a worker becomes disabled, including rehabilitation and the return to work after injury; and (4) the total integration of the worker into the workplace and the community. Labour union activities related to these issues include: organizing and advocating for the rights of workers with disabilities through national legislation and other vehicles; ensuring and protecting rights by including them in negotiated labour agreements; educating union members and employers on disability issues and rights and responsibilities related to disability management; collaborating with management to further the rights and duties related to disability management; providing services to workers with disabilities to assist them in becoming integrated or more integrated into the workforce; and, when all else fails, engaging in resolving or litigating disputes, or fighting for legislative changes to protect rights.
Issue 1: Recruitment, Hiring and Employment Practices
While the legal obligations of labour unions may relate specifically to their members, unions traditionally helped to improve the working lives of all workers, including those with disabilities. This is a tradition that is as old as the labour movement itself. However, fair and equitable practices related to recruitment, hiring and employment practices take on special significance when the worker has a disability. Because of negative stereotypes as well as architectural, communication and other barriers related to disability, disabled job seekers and workers are often denied their rights or face discriminatory practices.
The following basic lists of rights (figure 1 to 4), although simply stated, have profound implications for equal access to employment opportunities by disabled workers. Disabled workers also have certain duties, as do all workers, to present themselves, including their interests, abilities, skills and workplace requirements, in an open and forthright manner.
Figure 1. Rights and duties: recruitment, hiring and employment practices

In the hiring process, applicants should be judged on their abilities and qualifications (figure 1). They need to have a full understanding of the job to evaluate their interest and ability to do the job. Further, once hired, all workers should be judged and evaluated according to their job performance, without bias based on factors not related to the job. They should have equal access to employment benefits and opportunities for advancement. When necessary, reasonable accommodations should be made so that an individual with a disability can perform the requisite job tasks. Job accommodations can be as simple as raising a workstation, making a chair available or adding a foot pedal.
In the United States, the Americans with Disabilities Act not only prohibits discrimination against qualified workers (a qualified worker is one who has the qualifications and abilities to perform the essential functions of the job) based on disability, but also requires that employers make reasonable accommodation—that is, the employer provides a piece of equipment, changes non-essential job functions or makes some other adjustment that does not cause the employer undue hardship, so that the person with a disability can perform the essential functions of the job. This approach is designed to protect workers’ rights and make it “safe” to request accommodations. According to the US experience, most accommodations are relatively low in cost (less than US$50).
Rights and duties go hand in hand. Workers have a responsibility to notify their employer of a condition that may affect their ability to do the job, or that may affect their safety or that of others. Workers have a duty to represent themselves and their abilities in an honest manner. They should request a reasonable accommodation, if necessary, and accept that which is most appropriate for the situation, cost-effective and least intrusive to the workplace while still meeting their needs.
ILO Convention No. 159 concerning the vocational rehabilitation and employment of disabled persons, and Recommendation No. 168 address these very rights and duties and their implications for workers’ organizations. Convention No.159 suggests that special positive measures may sometimes be necessary to ensure “effective equality of opportunity and treatment between disabled workers and other workers”. It adds that such measures “shall not be regarded as discriminating against other workers”. Recommendation No. 168 encourages the implementation of specific measures to create job opportunities, such as providing financial support to employers to make reasonable accommodations, and encourages labour organizations to promote such measures and provide advice about making such accommodations.
What labour unions can do
Union leaders typically have deep roots within the communities in which they operate and can be valuable allies in promoting the recruitment, hiring and continued employment of persons with disabilities. One of the first things they can do is to develop a policy statement on the employment rights of people with disabilities. Education of members and a plan of action to support the policy should follow. Labour unions can advocate rights for workers with disabilities on a broad scale by promoting, monitoring and supporting relevant legislative initiatives. In the workplace they should encourage management to develop policies and actions that remove barriers to employment for disabled workers. They can assist in developing appropriate job accommodations and, through negotiated labour agreements, protect and further the rights of disabled workers in all employment practices.
Organized labour can initiate programmes or cooperative efforts with employers, government ministries, non-governmental organizations, and companies to develop programmes that will result in increased recruitment and hiring of, and fair practices towards, people with disabilities. Representatives can sit on boards and lend their expertise to community-based organizations that work with people with disabilities. They can promote awareness among union members, and, in their role as employers, labour unions can set an example of fair and equitable hiring practices.
Examples of what labour unions are doing
In England, the Trades Union Congress (TUC) has taken an active role in promoting equal rights in employment for persons with disabilities, through published policy statements and active advocacy. It regards the employment of disabled people as an equal opportunities issue, and the experiences of disabled persons as not unlike those of other groups that have been discriminated against or excluded. The TUC supports existing quota legislation and advocates for levies (fines) on employers who fail to comply with the law.
It has published several related guides to support its activities and educate its members, including TUC Guidance: Trade Unions and Disabled Members, Employment of Disabled People, Disability Leave and Deaf People and Their Rights. Trade Unions and Disabled Members includes guidance about basic points that unions should consider when negotiating for disabled members. The Irish Congress of Trade Unions has produced a guide with similar intent, Disability and Discrimination in the Workplace: Guidelines for Negotiators. It provides practical steps to tackle workplace discrimination and to promote equality and access through negotiated labour agreements.
The Federation of German Trade Unions also has developed a comprehensive position paper stating its policy for integrative employment, its stance against discrimination and its commitment to use its influence to further its positions. It supports broad employment training and access to apprenticeships for disabled persons, addresses the double discrimination faced by disabled women, and advocates for union activities that support access to public transportation and integration into all aspects of society.
The Screen Actors Guild in the United States has approximately 500 members with disabilities. A statement on non-discrimination and affirmative action appears in its collective bargaining agreements. In a cooperative venture with the American Federation of Television and Radio Artists, the Guild has met with national advocacy groups to develop strategies to increase the representation of people with disabilities in their respective industries. The International Union of United Automobile, Aerospace and Agricultural Implement Workers of America is another labour union that includes language in its collective bargaining agreements prohibiting discrimination based on disability. It also fights for reasonable accommodations for its members and provides regular training on disability and work issues. The United Steel Workers of America has included for years non-discrimination clauses in its collective bargaining agreements, and resolves disability discrimination complaints through a grievance process and other procedures.
In the United States, the passage and implementation of the Americans with Disabilities Act (ADA) was, and continues to be, promoted by US-based labour unions. Even before passage of the ADA, many AFL-CIO member unions were actively involved in training their memberships on disability rights and awareness (AFL-CIO 1994). The AFL-CIO and other labour union representatives are carefully monitoring the implementation of the law, including litigation and alternative dispute resolution processes, to support the rights of workers with disabilities under the ADA and to ensure that their interests and the rights of all workers are fairly considered.
With passage of the ADA, labour unions have produced scores of publications and videos and organized training programmes and workshops to further educate their members. The Civil Rights Department of the AFL-CIO produced brochures and held workshops for their affiliated unions. The International Association of Machinists and Aerospace Workers Center for Administering Rehabilitation and Education Services (IAM CARES), with support from the federal government, produced two videos and ten booklets for employers, people with disabilities and union personnel to inform them of their rights and responsibilities under the ADA. The American Federation of State, County and Municipal Employees (AFSCME) has a long-standing history of protecting the rights of workers with disabilities. With passage of the ADA, AFSCME updated its publications and other efforts and trained thousands of members and AFSCME staff on the ADA and workers with disabilities.
Although Japan has a quota and levy system in place, one Japanese labour union recognized that individuals who are mentally disabled are the most likely to be underrepresented in the labour force, especially among larger employers. It has been taking action. The Kanagawa Regional Council of the Japanese Electrical, Electronic and Information Union is working with the city of Yokohama to develop an employment support center. Its purpose will include training individuals who are mentally disabled and providing services to facilitate their placement and that of other disabled persons. Further, the union plans to establish a training centre that will provide disability awareness and sign-language training to union members, personnel managers, production supervisors and others. It will capitalize on good labour-employer relationships and engage business people in the management and activities of the centre. Initiated by the labour union, the project promises to be a model of collaboration between business, labour and government.
In the United States and Canada, labour unions have been working cooperatively and creatively with government and employers to facilitate the employment of people with disabilities through a programme called Projects with Industry (PWI). By matching labour union resources with government funding, IAM CARES and the Human Resources Development Institute (HRDI) of the AFL-CIO have been operating training and job placement programmes for individuals with disabilities regardless of their union affiliation. In 1968, HRDI began to function as the AFL-CIO’s employment and training arm by providing assistance to diverse ethnic groups, women and people with disabilities. In 1972, it began a programme with a specific focus on people with disabilities, to place them with employers who had labour agreements with national and international labour unions. As of 1995, more than 5,000 people with disabilities have been employed as a result of this activity. Since 1981, the IAM CARES programme, which operates in the Canadian and US labour markets, has enabled more than 14,000 individuals, most of whom are severely disabled, to find jobs. Both programmes provide professional assessment, counselling and job placement assistance through linkages with businesses and with government and labour union support.
In addition to providing direct services to workers with disabilities, these PWI programmes engage in activities that enhance public awareness of people with disabilities, promote cooperative labour-management action to foster employment and job retention, and provide training and consulting services to local unions and employers.
These are only some examples from around the world of activities that labour unions have taken to facilitate fairness in employment for workers with disabilities. It is fully in line with their broad goal to facilitate worker solidarity and to end all forms of discrimination.
Issue 2: Disability Prevention, Health and Safety
While securing safe working conditions is a hallmark of labour union activity in many countries, maintaining health and safety in the workplace has traditionally been an employer function. Typically, management has control over job design, tool selection, and decisions about processes and the work environment that affect safety and prevention. Yet, only someone who performs the tasks and procedures on a regular basis, under specific work conditions and demands, can fully appreciate the implications of procedures, conditions and hazards on safety and productivity.
Fortunately, enlightened employers recognize the importance of worker feedback, and as the organizational structure of the workplace is changing to increase worker autonomy, such feedback is more readily invited. Safety and prevention research also supports the need to involve the worker in job design, policy formulation and the implementation of programmes on health, safety and disability prevention.
Another trend, the sharp increase in workers’ compensation and other costs of job-related injury and disability, has led employers to examine prevention as a key component of the disability management effort. Prevention programmes should focus on the full range of stressors, including those of a psychological, sensory, chemical or physical nature, as well as on trauma, accidents and exposure to obvious hazards. Disability can result from repeated exposure to mild stressors or agents, rather than from a single incident. For example, some agents can cause or activate asthma; repeated or loud noises can lead to hearing loss; production pressure, such as piece-rate demands, can cause symptoms of psychological stress; and repetitive motions can lead to cumulative stress disorders (e.g., carpal tunnel syndrome). Exposure to such stressors can exacerbate disabilities that already exist and make them more debilitating.
From a worker’s perspective, the benefits of prevention can never be overshadowed by compensation. Figure 2 lists some of the rights and responsibilities that workers have in relation to disability prevention in the workplace.
Figure 2. Rights and duties - health and safety
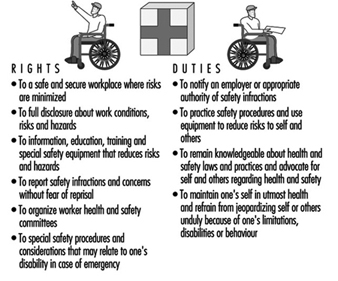
Workers have a right to the safest work environment possible and to the complete disclosure about risks and working conditions. Such knowledge is especially important to workers with disabilities who may need knowledge of certain conditions to determine whether they can perform the job functions without jeopardizing their health and safety or that of others.
Many jobs involve risks or dangers that cannot be fully removed. For example, construction jobs or those that deal with exposure to toxic substances have obvious, inherent risks. Other jobs, like data entry or sewing machine operation, seem relatively safe; however, repetitive motions or improper body mechanics can lead to disabilities. These risks can also be reduced.
All workers should be provided with necessary safety equipment and information on practices and procedures that reduce risk of injury or illness due to exposure to hazardous conditions, repetitive motions or other stressors. Workers must feel free to report/complain about safety practices, or to make suggestions to improve working conditions, without fear of losing their jobs. Workers should be encouraged to report an illness or disability, especially one that is caused or could be exacerbated by the work task or environment.
With regard to duties, workers have a responsibility to practice safety procedures that reduce risks to themselves and others. They must report unsafe conditions, advocate for health and safety issues, and be responsible regarding their health. For example, if a disability or illness places a worker or others at risk, the worker should remove him- or herself from the situation.
The field of ergonomics is emerging, with effective approaches to reducing disabilities incurred as a result of the manner in which the work is organized or performed. Ergonomics is basically the study of work. It involves fitting the job or task to the worker rather than vice versa (AFL-CIO 1992). Ergonomic applications have been used successfully to prevent disability in fields as diverse as agriculture and computers. Some ergonomic applications include flexible workstations that can be adapted to an individual’s height or other physical characteristics (e.g., adjustable office chairs), tools with handles to fit hand differences and simple changes in work routines to reduce repetitive motions or stress to certain parts of the body.
Increasingly, labour unions and employers recognize the need to extend health and safety programmes beyond the workplace. Even when disability or illness is not work-related, employers incur the costs of absenteeism, health insurance and perhaps rehiring and retraining. Further, some illnesses, such as alcoholism, drug addiction and psychological problems, can result in decreased worker productivity or increased vulnerability to on-the-job accidents and stress. For these and other reasons, many enlightened employers are engaging in education about health, safety and disability prevention on and off the job. Wellness programmes that address issues such as stress reduction, good nutrition, smoking cessation and AIDS prevention are being provided in the workplace by unions, management and through joint partnership efforts that may include the government as well.
Some employers provide wellness and employee assistance (counselling and referral) programmes to address these concerns. All of these prevention and health programmes are in the worker’s and employer’s best interests. For example, figures typically show savings-to-investment ratios between 3:1 and 15:1 for some health promotion and employee assistance programmes.
What can labour unions do?
Labour unions are in a unique position to use their leverage as representatives of workers to facilitate health, safety, disability prevention or ergonomics programmes in the workplace. Most prevention and ergonomics experts agree that worker participation and involvement in prevention policies and prescriptions increases the likelihood of their implementation and effectiveness (LaBar 1995; Westlander et al. 1995; AFL-CIO 1992). Labour unions can play a key role in establishing labour-management health and safety councils and ergonomics committees. They can lobby to promote legislation on workplace safety and work with management to establish joint safety committees, which can result in a substantial reduction in job-related accidents (Fletcher et al. 1992).
Labour unions need to educate their members about their rights, regulations and safe practices related to workplace safety and disability prevention on and off the job. Such programmes can become part of the negotiated labour agreement or union-based health and safety committees.
Further, in policy statements and labour agreements and through other mechanisms, labour unions can negotiate disability prevention measures and special conditions for those with disabilities. When a worker becomes disabled, especially if the disability is work-related, the union should support that worker’s right to accommodations, tools or reassignment to prevent exposure to stress or hazardous conditions that can increase the limitation. For example, those with occupationally induced hearing loss must be prevented from continued exposure to certain types of noise.
Examples of what labour unions are doing
The policy statement of the Federation of German Trade Unions concerning employees with disabilities specifically identifies the need to avoid health risks for workers with disabilities and to take measures to prevent them from incurring additional injury.
Under a negotiated labour agreement between the Boeing Aircraft Corporation and the International Association of Machinists and Aerospace Workers (IAMAW), the IAM/Boeing Health and Safety Institute authorizes funding, develops pilot programmes and makes recommendations for improvements related to worker health and safety issues, and manages the return to work of industrially impaired workers. The Institute was established in 1989 and funded by a four cent per hour health and safety trust fund. It is operated by a Board of Directors that is composed of 50% management and 50% union representation.
The Disabled Forestry Workers Foundation of Canada is another example of a joint labour-management project. It evolved from a group of 26 employers, unions and other organizations that collaborated to produce a video (Every Twelve Seconds) to draw attention to the high accident rate among forestry workers in Canada. Now the Foundation focuses on health, safety, accident prevention and workplace models for reintegrating injured workers.
IAM CARES is engaged in an active programme of educating its members on safety issues, particularly in high-risk and hazardous jobs in the chemical industries, the construction trades and the steel industry. It conducts training for shop stewards and line workers, and encourages the formation of safety and health committees that are union-operated and independent of management.
The George Meany Center of the AFL-CIO, with a grant from the US Department of Labor, is developing educational materials on substance abuse to help union members and their families deal with alcohol and drug addictions.
The Association of Flight Attendants (AFA) has done some remarkable work in the area of AIDS and AIDS prevention. Volunteer members have developed the AIDS, Critical and Terminal Illness Awareness Project, which is educating members on AIDS and other life-threatening illnesses. Thirty-three of its locals have educated a total of 10,000 members about AIDS. It has established a foundation to administer funds to members who are also coping with a life-threatening disease.
Issue 3: When a Worker Becomes Disabled—Support, Rehabilitation, Compensation
In many countries, labour unions have fought for workers’ compensation, disability and other benefits related to on-the-job injury. Since one purpose of disability management programmes is to decrease the costs related to these benefits, it may be assumed that labour unions are not in favour of such programmes. In fact, this is not the case. Labour unions support rights related to job protection, early intervention in the provision of rehabilitation services and aspects of sound disability management practice. Disability management programmes that focus on reducing the worker’s suffering, address concerns about work loss, including its financial implications, and try to prevent short- and long-term disability are welcomed. Such programmes should return the worker to his or her job, if feasible, and provide accommodations when necessary. When it is not feasible, alternatives such as reassignment and retraining should be provided. As a last resort, long-term compensation and wage replacement should be guaranteed.
Fortunately, data suggest that disability management programmes can be structured to meet the needs and rights of the workers and still be cost effective for employers. As workers’ compensation costs have skyrocketed in industrialized countries, effective models that incorporate rehabilitation services have been developed and are being evaluated. Unions have a definitive role to play in developing such programmes. They need to promote and protect the rights listed in Figure 3 and educate workers about their duties.
Figure 3. Rights and duties: support, rehabilitation and compensation.

Most of the workers’ rights listed are part of standard return-to-work services for injured workers according to state-of-the-art rehabilitation techniques (Perlman and Hanson 1993). Workers have a right to prompt medical attention and to the assurance that their wages and jobs will be protected. Swift attention and early intervention are found to reduce the time away from work. Withholding benefits can result in refocusing efforts away from rehabilitation and returning to work, and into litigation and animosity towards the employer and the system. Workers need to understand what will happen if they become injured or disabled, and should have a clear understanding of company policy and legal protections. Unfortunately, some systems related to prevention, workers’ compensation and rehabilitation have been fragmented, open to abuse and confusing for those who depend on these systems at a vulnerable time.
Most trade unionists would agree that workers who become disabled gain little if they lose their jobs and their ability to work. Rehabilitation is a desired response to injury or disability and should include early intervention, comprehensive assessment and individualized planning with worker involvement and choice. Return-to-work plans may include returning to work gradually, with accommodation, at reduced hours or in reassigned positions until the worker is ready to return to optimal functioning.
Such accommodations, however, can interfere with the protected rights of workers in general, including those related to seniority. While trade unionists support and protect the rights of disabled workers to return to work, they seek solutions that do not interfere with negotiated seniority clauses or require restructuring of jobs in such a way that other workers are expected to assume new tasks or responsibilities for which they are not responsible or compensated. Collaboration and union involvement are necessary to resolve these issues when they arise, and such circumstances further illustrate the need for labour union involvement in the design and implementation of legislation, disability management and rehabilitation policies and programmes.
What labour unions can do
Labour unions need to be involved in national legislative planning committees related to disability, and in task forces which deal with such issues. Within corporate structures and the workplace, labour unions should help organize joint labour-management committees engaged in developing company-level disability management programmes, and should monitor individual outcomes. Unions can assist with return to work by suggesting accommodations, engaging the assistance of co-workers, and providing assurance to the injured worker.
Labour unions can work cooperatively with employers to develop model disability management programmes that assist workers and meet cost-containment goals. They can engage in research of worker needs, best practices and other activities to determine and protect worker interests. Worker education rights and responsibilities and needed actions are also critical to ensuring the best responses to injury and disability.
Examples of what labour unions have done
Some unions have been active in helping governments address the inadequacies of their systems related to on-the-job injuries and workers’ compensation. In 1988, responding to cost concerns related to injury compensation and to labour union concern over a lack of effective rehabilitation programmes, Australia passed the Commonwealth Employees Rehabilitation and Compensation Act, which provided a new coordination system for managing and preventing workplace illness and injuries of federal workers. The revised system is based on the premise that effective rehabilitation and return to work, if possible, is the most beneficial outcome for the worker and the employer. It incorporates prevention, rehabilitation and compensation into the system. Benefits and jobs are protected while the individual undergoes rehabilitation. Compensation includes wage replacement, medical and related expenses, and in certain instances limited lump sum payments. When individuals are unable to return to work they are adequately remunerated. Early results are demonstrating an 87% return-to-work rate. Success is attributed to many factors, including the collaborative involvement of all stakeholders, including labour unions, in the process.
The IAM/Boeing Health and Safety Institute, already mentioned, provides an example of a labour-management programme that was developed in one corporate setting. The model return-to-work programme was one of the first initiatives taken by the Institute because the needs of industrially injured workers were being neglected by fragmented service-delivery systems administered by federal, state, local and private rehabilitation agencies and programmes. After analysing data and conducting interviews, the union and the corporation set up a model programme that is felt to be in the best interests of both. The programme involves many of the rights already listed: early intervention; quick response with services and compensation requirements; intensive case management focused on return to work with accommodation, if needed; and regular evaluation of the programme’s outcomes and workers’ satisfaction.
Current satisfaction surveys indicate that management and injured workers have found the joint labour-management Return-to-Work Programme an improvement over existing services. The previous programme has been replicated at four additional Boeing plants and the joint programme is expected to become standard practice throughout the company. To date, more than 100,000 injured workers have received rehabilitation services through the programme.
The AFL-CIO’s HRDI programme also offers return-to-work rehabilitation services for workers injured on the job at companies with affiliated union representation. In partnership with Columbia University’s Workplace Center, it administered a demonstration programme called the Early Intervention Program, which sought to determine if early intervention can speed the process of getting workers, who are out of work because of short-term disability, back to the job. The programme returned 65% of participants to work and isolated several factors critical to success. Two findings are of particular significance to this discussion: (1)workers almost universally experience distress related to financial concerns; and (2) the programme’s union affiliation reduced suspicion and hostility.
The Disabled Forestry Workers Foundation of Canada developed a programme it calls the Case Management Model for Workplace Integration. Also using the joint union-management initiative, the programme rehabilitates and reintegrates disabled workers. It has published Industrial Disability Management: An Effective Economic and Human Resource Strategy to assist in the implementation of the model, built on partnership between employers, unions, government and consumers. Further, it has developed the National Institute of Occupational Disability and Research, involving labour, management, educators and rehabilitation professionals. The Institute is developing training programmes for human resource and union representatives that will lead to further implementation of its model.
Issue 4: Inclusion and Integration in the Community and the Workplace
In order for people with disabilities to become fully integrated in the workplace, they must first have equal access to all community resources that predispose and assist people to work (education and training opportunities, social services, etc.) and that give them access to the work environment (accessible housing, transportation, information, etc.). Many labour unions have recognized that people with disabilities are not able to participate in the workplace if they are excluded from full participation in community life. Further, once employed, people with disabilities may need special services and accommodations to be fully integrated or to maintain job performance. Equality in community life is a precursor to employment equity, and to fully address the issue of disability and work, the broader issue of human or civil rights must be considered.
Labour unions have also recognized that to ensure employment equity, sometimes special services or accommodations may be required for job maintenance, and in the spirit of solidarity, may provide such services to their members or promote the provision of such accommodations and services. Figure 4 lists the rights and duties that recognize the need for full access to community life.
Figure 4. Rights and duties: inclusion and integration in the community and the workplace.
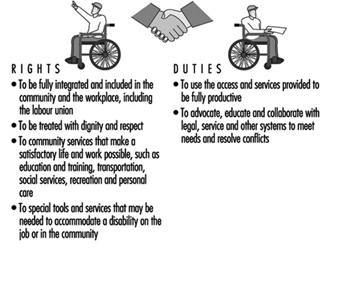
What unions can do
Labour unions can be direct agents of change in their communities by encouraging the total integration of people with disabilities in the workplace and community. Labour unions can reach out to workers with disabilities and the organizations that represent them, and collaborate to take positive action. The opportunities to exert political leverage and affect legislative change have been noted throughout this article, and they are fully in keeping with ILO Recommendation No. 168 and ILO Convention No. 159. Both stress the role of employers’ and workers’ organizations in the formulation of policies related to vocational rehabilitation, and their involvement in the implementation of policy and services.
Labour unions have a responsibility to represent the needs of all their workers. They should provide model services, programmes and representation within the labour union structure to include, accommodate and engage members with disabilities in all aspects of the organization. As some of the following examples will demonstrate, labour unions have used their members as a resource for raising funds, to serve as volunteers or to engage in direct services on the job and in the community to ensure that people with disabilities are fully included in community life and the workplace.
What unions have done
In Germany, a type of advocacy is legally mandated. According to the Severely Disabled Persons Act, any enterprise, including labour unions, that has five or more permanent employees, must have a person who is elected to the staff council as a representative of disabled employees. This representative ensures that the rights and concerns of disabled employees are addressed. Management is required to consult this representative in matters related to general recruitment as well as policy. As a result of this law, labour unions have become actively involved in disability issues.
The Irish Congress of Trade Unions (ICTU) has published and disseminated a Charter of Rights of People with Disabilities (1990), which is a list of 18 fundamental rights considered essential to the full equality of people with disabilities in the workplace and the community at large. It includes the rights to a barrier-free environment, housing, quality health care, education, training, employment and accessible transportation.
In 1946, the IAMAW began to help people with disabilities by establishing the International Guiding Eyes. This programme provides guide dogs and training in how to use them to blind and visually impaired individuals so that they can lead more independent and satisfying lives. Approximately 3,000 individuals from many countries have been helped. Part of the costs to operate the programme are borne by the contributions of union members.
The work of one Japanese labour union has been previously described. Its work was a natural evolution from the work of the Assembly of Trade Unions begun in the 1970s when a union member who had an autistic child requested labour union support to focus on the needs of children with disabilities. The Assembly established a foundation that was supported by the sale of matches and, later, boxes of tissues, by union members. The foundation started a counselling service and a telephone hotline to help parents cope with the challenges of raising a disabled child in a segregated society. As a result, parents became organized and lobbied the government to address accessibility (railways were pressured to improve accessibility, a process that continues today) and to provide educational training and upgrade other services. Summer activities and festivals were sponsored, as well as national and international tours, to foster understanding of disability issues.
After twenty years, when the children grew up, their needs for recreation and education became needs for vocational skills and employment. A vocational experience programme for youth with disabilities was developed and has been in effect for several years. The unions requested companies to provide work experiences for second-year high school students with disabilities. It was out of this programme that the need for the Employment Support Center, noted under Issue 1, became apparent.
Many unions provide extra support services to people with disabilities on the job to assist them in maintaining employment. The Japanese labour unions use on-the-job volunteers to support young people in work-experience programmes with companies that have union representation. IAM CARES in the United States and Canada uses a buddy system to match new employees who have disabilities with a union member who serves as a mentor. IAM CARES also has sponsored supported employment programmes with Boeing and other companies. Supported employment programmes provide job coaches to assist those with the most severe disabilities in learning their jobs and maintaining their performance at productive levels.
Some labour unions have established subcommittees or task forces composed of disabled workers, to ensure that the rights and needs of disabled members are fully represented within the union structure. The American Postal Workers Union is an excellent example of such a task force and the wide implications it can have. In the 1970s, the first deaf shop steward was appointed. Since 1985, several conferences have been held just for hearing-impaired members. These members also serve on negotiating teams to resolve job accommodation and disability management issues. In 1990, the task force worked with the postal service to develop an official stamp depicting the words “I love you” in a hand sign.
Conclusions
Unions, at their most basic level, are about people and their needs. Since the earliest days of labour union activity, unions have done more than fight for fair wages and optimal working conditions. They have sought to improve the quality of life and to maximize opportunities for all workers, including those with disabilities. Although the union perspective emanates from the workplace, the union influence is not limited to enterprises where negotiated labour agreements exist. As many examples in this article demonstrate, labour unions can also affect the larger social environment through a variety of activities and initiatives that are aimed at eliminating discrimination and inequities towards people with disabilities.
While unions, employers, government entities, vocational rehabilitation representatives and men and women with disabilities may have different perspectives, they should share the desire for a healthy and productive workplace. Unions are in a unique position to bring these groups together on common ground, and thereby play a key role in improving the lives of people with disabilities.
Case Study: Best Practices Examples
SABRE Employment (UK)
Mission Statement:To communicate overall objectives/business goals which not only embrace the provision of quality service to applicants, but clearly reflect the desire to provide an efficient recruitment service to employers and which assist employers to improve their capacity to employ people with disabilities. Emphasis should be placed on the primary aim to achieve customer satisfaction. “All of Sabre’s activities begin with our customers. Our goals are to provide recruitment solutions through effective job matching, reliable training and support and to offer expertise in the recruitment and employment of people with disabilities.”
A job fair was recently held to give people a chance to meet employers and learn about different jobs. McDonald’s Restaurants Ltd. ran a workshop on interview skills and also sponsored the job fair event along with Shell and Pizza Hut. There were employer displays which provided an opportunity for employers and prospective employees with learning difficulties to meet in an informal way.
The Coverdale Bursary Programme (UK)
For five years, Coverdale, a small (70 people) management consultancy has offered bursaries to the value of £10,000 per person to disabled individuals seeking high quality management training. These individuals then go into companies like Barclays Bank, the Post Office and Midland Bank for additional training, in a process which promotes long-term attitude change across participating companies. This programme is now being expanded. It has been adapted by The Canadian Council for Rehabilitation and Work.
Brook Street and FYD (UK)
A commercial recruitment agency, Brook Street, and a charity for young deaf people, Friends for the Young Deaf (FYD), have worked in partnership for some years. Brook Street offers work experience and assessment to the young deaf graduates completing the FYD leadership training programme; Brook Street then places appropriate candidates into jobs, charging the same commercial fee they would charge for any candidate.
Employers’ Forum on Disability (UK)
Companies involved in the Employers’ Forum on Disability, an employer-funded association that promotes the integration of disabled persons in the labour market and provides advisory services for interested enterprises, helped disabled entrepreneur Stephen Duckworth to establish his business, Disability Matters, which now offers high quality consultancy and awareness-raising on disability to companies across the UK. Its philosophy encompasses the following:
- to understand and define the business case for employing disabled people
- an authoritative employers’ voice on disability
- employment- and training-related services which are more market led
- to develop new ways to attract qualified disabled applicants and to retain disabled employees
- The key to influencing employers and mobilizing their involvement is to network in a way that:
- promotes the business case through business-to-business communication
- promotes personal contact between employers and disabled individuals
- promotes employer ownership of the issue and an awareness on the part of rehabilitation providers that the employer should be valued as stakeholder, customer and potential partner
- positions disability as part of the wider debate regarding economic and social regeneration, long-term unemployment, poverty and micro and macroeconomic policies
Other examples in the UK: The Employer Forum on Disabilities
Leading UK companies drafted a highly influential policy framework called the “Employers Agenda on Disability, a Ten Point Plan”. This was launched by the Prime Minister and is now publicly supported by more than 100 major firms. It has proven a powerful force for change because it was drafted by the employers themselves in consultation with disability experts. It is now a key tool in helping employers to comply with discrimination legislation.
Supporters of the Agenda are publicly committed to structuring their corporate policy on disability using a 10-point framework addressing the following issues: Equal Opportunities Policy and Procedures Statement; Staff Training and Disability Awareness; The Working Environment; Recruitment; Career Development; Retention, Retraining and Redeployment; Training and Work Experience; People with Disabilities in the Wider Community; Involvement of Disabled People; Monitoring Performance.
The Action File on Disability, a unique manual which provides practical information on how to implement the Agenda, has been produced by the Employers’ Forum on Disability.
Graduate Recruitment:
More than 20 companies are involved in a consortium working with “Workable”, which brokers work-experience opportunities to disabled students in a planned and structured manner.
Twenty-five companies jointly fund an initiative making annual Career Fairs for students accessible for disabled students. The Career Fairs are now wheelchair accessible, and interpreters for the deaf are available, as well as large-print brochures and other support. Employers had experienced such difficulty attracting disabled graduates to apply for jobs using traditional intermediaries that they are now pioneering recruitment methods which speak directly to the disabled students.
HIRED (US)
The project HIRED in San Francisco embodies this new employer orientation. The acronym stands for Helping Industry Recruit Employees with Disabilities. Their literature highlights the services they offer employers:
“Project HIRED is a private, not for profit organization serving the San Francisco Bay area. Our purpose is to assist individuals with disabilities to secure jobs appropriate to their qualifications and career goals. Our services to employers include:
- free referrals, pre-screened, qualified candidates matched to a company’s job openings
- quality temporary employment services at competitive rates
- customized, on site seminars on the technical, legal and interpersonal aspects of disability in the workplace, and
- consultation on all topics related to disabilities in the workplace.
In addition to less formal corporate partnerships, Project HIRED has a corporate membership programme involving approximately 50 Bay Area companies. As corporate members, these companies are entitled to free consulting and a discount on seminars. We are currently exploring additional services, such as library of video resources, to further assist corporate members successfully incorporate people with disabilities in their workforce.”
ASPHI (Italy)
The origins of ASPHI (Associazione per lo Sviluppo di Progetti Informatici per gli Handicappati) go back to the late 1970s when IBM Italy organized courses in computer programming for the visually impaired. A number of companies which had subsequently employed the trainees, together with specialist partner agencies from the non-profit sector, created ASPHI for the physically disabled and the hearing and mentally impaired. The Association involves more than 40 companies which provide financial support, staff and volunteer helpers, advice as well as employment opportunities for ASPHI’s graduates. ASPHI’s objective is to harness information technologies for the social and vocational integration of disadvantaged groups. Its activities include: job training, research and development of new products (mainly software) which facilitate alternative methods of communication, personal autonomy and rehabilitation, and community education, thus breaking down prejudices and discrimination against disabled people. Each year, some 60 young people are qualified by ASPHI. With about 85% of its graduates finding a permanent job, ASPHI’s success has brought it national and international recognition.
Swedish Employers’ Federation Initiative
The Swedish Employers’ Federation Initiative, “Persons with Disabilities in Companies”, positions disability firmly in the labour market debate in the country and conveys the message that disability is an issue of importance to the Swedish Employers Confederation and its members. The Federation states: “The path to employment for persons with disabilities must be made smoother. Requirements for this include:
- clear signals to employers concerning responsibility and costs
- financial compensation for extra costs, if any, incurred by employers who appoint persons with disabilities
- more knowledge of disabilities and the scope of persons with disabilities for changing attitudes and values
- improved cooperation between companies, authorities and individuals to create a dynamic and flexible labour market.”
Introduction and Overview
A 1981 study of worker safety and health training in the industrial nations begins by quoting the French writer Victor Hugo: “No cause can succeed without first making education its ally” (Heath 1981). This observation surely still applies to occupational safety and health in the late twentieth century, and is relevant to organization personnel at all levels.
As the workplace becomes increasingly complex, new demands have arisen for greater understanding of the causes and means of prevention of accidents, injuries and illnesses. Government officials, academics, management and labour all have important roles to play in conducting the research that furthers this understanding. The critical next step is the effective transmission of this information to workers, supervisors, managers, government inspectors and safety and health professionals. Although education for occupational physicians and hygienists differs in many respects from the training of workers on the shop floor, there are also common principles that apply to all.
National education and training policies and practices will of course vary according to the economic, political, social, cultural and technological background of the country. In general, industrially advanced nations have proportionally more specialized occupational safety and health practitioners at their disposal than do the developing nations, and more sophisticated education and training programmes are available to these trained workers. More rural and less industrialized nations tend to rely more on “primary health care workers”, who may be worker representatives in factories or fields or health personnel in district health centres. Clearly, training needs and available resources will vary greatly in these situations. However, they all have in common the need for trained practitioners.
This article provides an overview of the most significant issues concerning education and training, including target audiences and their needs, the format and content of effective training and important current trends in the field.
Target Audiences
In 1981, the Joint ILO/WHO Committee on Occupational Health identified the three levels of education required in occupational health, safety and ergonomics as (1) awareness, (2) training for specific needs and (3) specialization. These components are not separate, but rather are part of a continuum; any person may require information on all three levels. The main target groups for basic awareness are legislators, policy makers, managers and workers. Within these categories, many people require additional training in more specific tasks. For example, while all managers should have a basic understanding of the safety and health problems within their areas of responsibility and should know where to go for expert assistance, managers with specific responsibility for safety and health and compliance with regulations may need more intensive training. Similarly, workers who serve as safety delegates or members of safety and health committees need more than awareness training alone, as do government administrators involved in factory inspection and public health functions related to the workplace.
Those doctors, nurses and (especially in rural and developing areas) nonphysician primary health care workers whose primary training or practice does not include occupational medicine will need occupational health education in some depth in order to serve workers, for example by being able to recognize work-related illnesses. Finally, certain professions (for example, engineers, chemists, architects and designers) whose work has considerable impact on workers’ safety and health need much more specific education and training in these areas than they traditionally receive.
Specialists require the most intensive education and training, most often of the kind received in undergraduate and postgraduate programmes of study. Physicians, nurses, occupational hygienists, safety engineers and, more recently, ergonomists come under this category. With the rapid ongoing developments in all of these fields, continuing education and on-the-job experience are important components of the education of these professionals.
It is important to emphasize that increasing specialization in the fields of occupational hygiene and safety has taken place without a commensurate emphasis on the interdisciplinary aspects of these endeavours. A nurse or physician who suspects that a patient’s disease is work-related may well need the assistance of an occupational hygienist to identify the toxic exposure (for example) in the workplace that is causing the health problem. Given limited resources, many companies and governments often employ a safety specialist but not a hygienist, requiring that the safety specialist address health as well as safety concerns. The interdependence of safety and health issues should be addressed by offering interdisciplinary training and education to safety and health professionals.
Why Training and Education?
The primary tools needed to achieve the goals of reducing occupational injuries and illnesses and promoting occupational safety and health have been characterized as the “three E’s”—engineering, enforcement and education. The three are interdependent and receive varying levels of emphasis within different national systems. The overall rationale for training and education is to improve awareness of safety and health hazards, to expand knowledge of the causes of occupational illness and injury and to promote the implementation of effective preventive measures. The specific purpose and impetus for training will, however, vary for different target audiences.
Middle and upper level managers
The need for managers who are knowledgeable about the safety and health aspects of the operations for which they are responsible is more widely acknowledged today than heretofore. Employers increasingly recognize the considerable direct and indirect costs of serious accidents and the civil, and in some jurisdictions, criminal liability to which companies and individuals may be exposed. Although belief in the “careless worker” explanation for accidents and injuries remains prevalent, there is increasing recognition that “careless management” can be cited for conditions under its control that contribute to accidents and disease. Finally, firms also realize that poor safety performance is poor public relations; major disasters like the one in the Union Carbide plant in Bhopal (India) can offset years of effort to build a good name for a company.
Most managers are trained in economics, business or engineering and receive little or no instruction during their formal education in occupational health or safety matters. Yet daily management decisions have a critical impact on employee safety and health, both directly and indirectly. To remedy this state of affairs, safety and health concerns have begun to be introduced into management and engineering curricula and into continuing education programmes in many countries. Further efforts to make safety and health information more widespread is clearly necessary.
First-line supervisors
Research has demonstrated the central role played by first-line supervisors in the accident experience of construction employers (Samelson 1977). Supervisors who are knowledgeable about the safety and health hazards of their operations, who effectively train their crew members (especially new employees) and who are held accountable for their crew’s performance hold the key to improving conditions. They are the critical link between workers and the firm’s safety and health policies.
Employees
Law, custom and current workplace trends all contribute to the spread of employee education and training. Increasingly, employee safety and health training is being required by government regulations. Some apply to general practice, while in others the training requirements are related to specific industries, occupations or hazards. Although valid evaluation data on the effectiveness of such training as a countermeasure to work-related injuries and illnesses are surprisingly sparse (Vojtecky and Berkanovic 1984-85); nevertheless the acceptance of training and education for improving safety and health performance in many areas of work is becoming widespread in many countries and companies.
The growth of employee participation programmes, self-directed work teams and shop floor responsibility for decision-making has affected the way in which safety and health approaches are taken as well. Education and training are widely used to enhance knowledge and skills at the level of the line worker, who is now recognized as essential for the effectiveness of these new trends in work organization. A beneficial action employers can take is to involve employees early on (for example, in the planning and design stages when new technologies are introduced into a worksite) to minimize and to anticipate adverse effects on the work environment.
Trade unions have been a moving force both in advocating more and better training for employees and in developing and delivering curricula and materials to their members. In many countries, safety committee members, safety delegates and works council representatives have assumed a growing role in the resolution of hazard problems at the worksite and in inspection and advocacy as well. Persons holding these positions all require training that is more complete and sophisticated than that given to an employee performing a particular job.
Safety and health professionals
The duties of safety and health personnel comprise a broad range of activities that differ widely from one country to another and even within a single profession. Included in this group are physicians, nurses, hygienists and safety engineers either engaged in independent practice or employed by individual worksites, large corporations, government health or labour inspectorates and academic institutions. The demand for trained professionals in the area of occupational safety and health has grown rapidly since the 1970s with the proliferation of government laws and regulations paralleling the growth of corporate safety and health departments and academic research in this field.
Scope and Objectives of Training and Education
This ILO Encyclopaedia itself presents the multitude of issues and hazards that must be addressed and the range of personnel required in a comprehensive safety and health programme. Taking the large view, we can consider the objectives of training and education for safety and health in a number of ways. In 1981, the Joint ILO/WHO Committee on Occupational Health offered the following categories of educational objectives which apply in some degree to all of the groups discussed thus far: (1) cognitive (knowledge), (2) psychomotor (professional skills) and (3) affective (attitude and values). Another framework describes the “information–education–training” continuum, roughly corresponding to the “what”, the “why” and the “how” of hazards and their control. And the “empowerment education” model, to be discussed below, puts great emphasis on the distinction between training—the teaching of competency-based skills with predictable behavioural outcomes—and education—the development of independent critical thinking and decision-making skills leading to effective group action (Wallerstein and Weinger 1992).
Workers need to understand and apply the safety procedures, proper tools and protective equipment for performing specific tasks as part of their job skills training. They also require training in how to rectify hazards that they observe and to be familiar with internal company procedures, in accordance with the safety and health laws and regulations which apply to their area of work. Similarly, supervisors and managers must be aware of the physical, chemical and psychosocial hazards present in their workplaces as well as the social, organizational and industrial relations factors that may be involved in the creation of these hazards and in their correction. Thus, gaining knowledge and skills of a technical nature as well as organizational, communication and problem-solving skills are all necessary objectives in education and training.
In recent years, safety and health education has been influenced by developments in education theory, particularly theories of adult learning. There are different aspects of these developments, such as empowerment education, cooperative learning and participative learning. All share the principle that adults learn best when they are actively involved in problem-solving exercises. Beyond the transmission of specific bits of knowledge or skills, effective education requires the development of critical thinking and an understanding of the context of behaviours and ways of linking what is learned in the classroom to action in the workplace. These principles seem especially appropriate to workplace safety and health, where the causes of hazardous conditions and illnesses and injuries are often a combination of environmental and physical factors, human behaviour and the social context.
In translating these principles into an education programme four categories of objectives must be included:
Information objectives: the specific knowledge that trainees will acquire. For example, knowledge of the effects of organic solvents on the skin and on the central nervous system.
Behavioural objectives: the competencies and skills that workers will learn. For example, the ability to interpret chemical data sheets or to lift a heavy object safely.
Attitude objectives: the beliefs that interfere with safe performance or with response to training that must be addressed. The belief that accidents are not preventable or that “solvents can’t hurt me because I’ve worked with them for years and I’m fine” are examples.
Social action objectives: the ability to analyse a specific problem, identify its causes, propose solutions and plan and take action steps to resolve it. For example, the task of analysing a particular job where several people have sustained back injuries, and of proposing ergonomic modifications, requires the social action of changing the organization of work through labour-management cooperation.
Technological and Demographic Change
Training for awareness and management of specific safety and health hazards obviously depends on the nature of the workplace. While some hazards remain relatively constant, the changes that take place in the nature of jobs and technologies require continuous updating of training needs. Falls from heights, falling objects and noise, for example, have always been and will continue to be prominent hazards in the construction industry, but the introduction of many kinds of new synthetic building materials necessitates additional knowledge and awareness concerning their potential for adverse health effects. Similarly, unguarded belts, blades and other danger points on machinery remain common safety hazards but the introduction of industrial robots and other computer-controlled devices requires training in new types of machinery hazards.
With rapid global economic integration and the mobility of multinational corporations, old and new occupational hazards frequently exist side-by-side in both highly industrialized and developing countries. In an industrializing country sophisticated electronics manufacturing operations may be located next door to a metal foundry that still relies on low technology and the heavy use of manual labour. Meanwhile, in industrialized countries, garment sweatshops with miserable safety and health conditions, or lead battery recycling operations (with its threat of lead toxicity) continue to exist alongside highly automated state-of-the-art industries.
The need for continual updating of information applies as much to workers and managers as it does to occupational health professionals. Inadequacies in the training even of the latter is evidenced by the fact that most occupational hygienists educated in the 1970s received scant training in ergonomics; and even though they received extensive training in air monitoring, it was applied almost exclusively to industrial worksites. But the single largest technological innovation affecting millions of workers since that time is the widespread introduction of computer terminals with visual display units (VDUs). Ergonomic evaluation and intervention to prevent musculoskeletal and vision problems among VDU users was unheard of in the 1970s; by the mid-nineties, VDU hazards have become a major concern of occupational hygiene. Similarly, the application of occupational hygiene principles to indoor air quality problems (to remedy “tight/sick building syndrome”, for example) has required a great deal of continuing education for hygienists accustomed only to evaluating factories. Psychosocial factors, also largely unrecognized as occupational health hazards before the 1980s, play an important role in the treatment of VDU and indoor air hazards, and of many others as well. All parties investigating such health problems need education and training in order to understand the complex interactions among environment, the individual and social organization in these settings.
The changing demographics of the workforce must also be considered in safety and health training. Women make up an increasing proportion of the workforce in both developed and developing nations; their health needs in and out of the workplace must be addressed. The concerns of immigrant workers raise numerous new training questions, including those to do with language, although language and literacy issues are certainly not limited to immigrant workers: varying literacy levels among native-born workers must also be considered in the design and delivery of training. Older workers are another group whose needs must be studied and incorporated into education programmes as their numbers increase in the working population of many nations.
Training Venues and Providers
The location of training and education programmes is determined by the audience, the purpose, the content, the duration of the programme and, to be realistic, the resources available in the country or region. The audience for safety and health education starts with schoolchildren, trainees and apprentices, and extends to workers, supervisors, managers and safety and health professionals.
Training in schools
Incorporation of safety and health education into elementary and secondary education, and especially in vocational and technical training schools, is a growing and very positive trend. The teaching of hazard recognition and control as a regular part of skills training for particular occupations or trades is far more effective than trying to impart such knowledge later, when the worker has been in the trade for a period of years, and has already developed set practices and behaviours. Such programmes, of course, necessitate that the teachers in these schools also be trained to recognize hazards and apply preventive measures.
On-the-job training
On-the-job training at the worksite is appropriate for workers and supervisors facing specific hazards found onsite. If the training is of significant length, a comfortable classroom facility within the worksite is strongly recommended. In cases where locating the training at the workplace may intimidate workers or otherwise discourage their full participation in the class, an offsite venue is preferable. Workers may feel more comfortable in a union setting where the union plays a major role in designing and delivering the programme. However, field visits to actual work locations which illustrate the hazards in question are always a positive addition to the course.
Training of safety delegates and committee members
The longer and more sophisticated training recommended for safety delegates and committee representatives is often delivered at specialized training centres, universities or commercial facilities. More and more efforts are being made to implement regulatory requirements for training and certification of workers who are to perform in certain hazardous fields such as asbestos abatement and hazardous waste handling. These courses usually include both classroom and hands-on sessions, where actual performance is simulated and specialized equipment and facilities are required.
Providers of onsite and offsite programmes for workers and safety representatives include government agencies, tripartite organizations like the ILO or analogous national or sub-national bodies, business associations and labour unions, universities, professional associations and private training consultants. Many governments provide funds for the development of safety and health training and education programmes targeted at specific industries or hazards.
Academic and professional training
The training of safety and health professionals varies widely among countries, depending on the needs of the working population and the country’s resources and structures. Professional training is centred in undergraduate and postgraduate university programmes, but these vary in availability in different parts of the world. Degree programmes may be offered for specialists in occupational medicine and nursing and occupational health may be incorporated into the training of general practitioners and of primary care and public health nurses. The number of degree-granting programmes for occupational hygienists has increased dramatically. However, there remains a strong demand for short courses and less comprehensive training for hygiene technicians, many of whom have received their basic training on the job in particular industries.
There is an acute need for more trained safety and health personnel in the developing world. While more university-trained and credentialed physicians, nurses and hygienists will undoubtedly be welcomed in these countries, it is nonetheless realistic to expect that many health services will continue to be delivered by primary health care workers. These people need training in the relationship between work and health, in the recognition of the major safety and health risks associated with the type of work carried on in their region, in basic survey and sampling techniques, in the use of the referral network available in their region for suspected cases of occupational illness and in health education and risk communication techniques (WHO1988).
Alternatives to university-based degree programmes are critically important to professional training in both developing and industrialized nations, and would include continuing education, distance education, on-the-job training and self-training, among others.
Conclusion
Education and training cannot solve all occupational safety and health problems, and care must be taken that the techniques learned in such programmes are in fact applied appropriately to the identified needs. They are, however, critical components of an effective safety and health programme when employed in conjunction with engineering and technical solutions. Cumulative, interactive and continuous learning is essential to prepare our rapidly changing work environments to meet the needs of workers, especially as regards the prevention of debilitating injuries and illnesses. Those who labour in the workplace as well as those who provide support from the outside need the most up-to-date information available and the skills to put this information to use in order to protect and promote worker health and safety.
Occupational Health and Safety: The European Union
The European Union (EU) today exercises a major influence on worldwide health and safety law and policy. In 1995, the Union comprised the following Member States: Austria, Belgium, Denmark, Finland, France, Germany, Greece, Ireland, Italy, Luxembourg, Netherlands, Portugal, Spain, Sweden and the United Kingdom. It will probably expand in years to come.
The forerunner of the Union, the European Community, was created in the 1950s by three treaties: The European Coal and Steel Community Treaty (ECSC) signed in Paris in 1951, and the European Economic Community (EEC) and European Atomic Energy Community (EAEC) Treaties signed in Rome in 1957. The European Union was formed with the entry into force of the Maastricht Treaty (concluded in 1989) on 1 January 1992.
The Community has four institutions, namely, the Commission, the Council, the Parliament and the European Court of Justice. They derive their powers from the treaties.
The Structures
The Commission
The Commission is the Community’s executive body. It is responsible for initiating, proposing and implementing Community policy, and if a Member State fails to fulfil its obligations under the treaties, the Commission can take proceedings against that Member State in the European Court of Justice.
It is composed of seventeen members appointed by the governments of Member States for a renewable four-year period. Each Commissioner is responsible for a portfolio and has authority over one or more Directorates General. One such Directorate General, DG V, is concerned with Employment, Industrial Relations and Social Affairs, and it is from within this Directorate General (DG V/F) that health and safety and public health policies are both initiated and proposed. The Commission is assisted in its health and safety law and policy-making role by the Advisory Committee on Safety, Hygiene and Health Protection at Work and the European Foundation for the Improvement of Living and Working Conditions.
Advisory Committee on Safety, Hygiene and Health Protection at Work
The Advisory Committee was established in 1974 and is chaired by the Commissioner responsible for the Directorate-General for Employment, Industrial Relations and Social Affairs. It consists of 96 full members: two representatives each of government, trade unions, and employers’ organizations from each Member State.
The role of the Advisory Committee is to “assist the Commission in the preparation and implementation of activities in the fields of safety, hygiene and health protection at work”. Because of its constitution and membership, the Advisory Committee is much more important and pro-active than its title suggests, so that, over the years, it has had a significant influence on strategic policy development, acting alongside the European Parliament and the Economic and Social Committee. More specifically, the Committee is responsible for the following matters within its general frame of reference:
- conducting exchanges of views and experience regarding existing or planned regulations
- contributing towards the development of a common approach to problems existing in the fields of safety, hygiene and health protection at work and towards the choice of Community priorities as well as measures necessary for implementing them
- drawing the Commission’s attention to areas in which there is an apparent need for the acquisition of new knowledge and for the implementation of appropriate educational and research projects
- defining, within the framework of Community action programmes, and in cooperation with the Mines Safety and Health Commission, (i) the criteria and aims of the campaign against the risk of accidents at work and health hazards within the undertaking; and (ii) methods enabling undertakings and their employees to evaluate and to improve the level of protection
- contributing towards keeping national administrations, trade unions and employers’ organizations informed of Community measures in order to facilitate their cooperation and to encourage initiatives promoted by them aiming at exchanges of experience and at laying down codes of practice
- submitting opinions on proposals for directives and on all measures proposed by the Commission which are of relevance to health and safety at work.
In addition to these functions, the Committee prepares an annual report, which the Commission then forwards to the Council, the Parliament and the Economic and Social Committee.
The Dublin Foundation
The European Foundation for the Improvement of Living and Working Conditions, located in Dublin, was established in 1975 as a specialized, autonomous Community body. The Foundation is primarily engaged in applied research in the areas of social policy, the application of new technologies, and the improvement and protection of the environment, in an effort to identify, cope with and forestall problems in the working environment.
European Agency for Health and Safety at the Workplace
The European Council has recently established the European Agency for Health and Safety at the Workplace in Bilbao, Spain, which is responsible for collating and disseminating information in its sector of activities. It will also organize training courses, supply technical and scientific support to the Commission and forge close links with specialized national bodies. The agency will also organize a network system with a view to exchanging information and experiences between Member States.
The European Parliament
The European Parliament exercises an increasingly important consultative role during the Community’s legislative process, controls a part of the Community’s budget jointly with the Council, approves Community Association agreements with non-member countries and treaties for the accession of new Member States, and is the Community’s supervisory body.
The Economic and Social Committee
The Economic and Social Committee is an advisory and consultative body which is required to give its opinion on a range of social and vocational issues, including health and safety at work. The Committee draws its membership from three main groups: employers, workers and an independant group comprising members with a wide spectrum of interests including professional, business, farming, the cooperative movement and consumer affairs.
Legal Instruments
There are four main instruments available to the Community legislator. Article 189 of the EEC Treaty as amended provides that “In order to carry out their task and in accordance with the provisions of this Treaty, the European Parliament acting jointly with the Council and the Commission shall make regulations and issue directives, take decisions, make recommendations or deliver opinions.”
Regulations
It is stated that “A regulation shall have general application. It shall be binding in its entirety and directly applicable in all Member States.” Regulations are directly enforceable in Member States. There is no need for further implementation. Indeed, it is not permissible for legislatures to consider them with a view to that end. In the field of health and safety at work, regulations are rare and those that have been made are administrative in nature.
Directives and decisions
It is stated that “A directive shall be binding, as to the result to be achieved, upon each Member State to which it is addressed, but shall leave to the national authorities the choice of form and methods.” Directives are instructions to Member States to enact laws to achieve an end result. In practice, directives are used mainly to bring about the harmonization or approximation of national laws in accordance with Article 100. They are therefore the most appropriate and commonly used instruments for occupational health and safety matters. In relation to decisions, it is stated that “A decision shall be binding in its entirety upon those to whom it is addressed.”
Recommendations and opinions
Recommendations and opinions have no binding force but are indicative of policy stances.
Policy
The European Communities made a decision in the mid-1980s to press ahead strongly with harmonization measures in the field of health and safety. Various reasons have been put forward to explain the developing importance of this area, of which four may be considered to be significant.
First, it is said that common health and safety standards assist economic integration, since products cannot circulate freely within the Community if prices for similar items differ in various Member States because of variable health and safety costs imposed on business. Second, 10 million people a year are the victims of, and 8,000 people a year die from, workplace accidents (out of a workforce which numbered 138 million people in 1994). These grim statistics give rise to an estimated bill of ECU 26,000 million paid in compensation for occupational accidents and diseases annually, whilst in Britain alone the National Audit Office in their Report Enforcing Health and Safety in the Workplace estimated that the cost of accidents to industry and the taxpayer is £10 billion per year. It is argued that a reduction of the human, social and economic costs of accidents and ill-health borne by this workforce will not only bring about a huge financial saving but will also bring about a significant increase in the quality of life for the whole Community. Third, the introduction of more efficient work practices is said to bring with it increased productivity, lower operational costs and better industrial relations.
Finally, it is argued that the regulation of certain risks, such as those arising from massive explosions, should be harmonized at a supranational level because of the scale of resource costs and (an echo of the first reason canvassed above) because any disparity in the substance and application of such provisions produces distortions of competition and affects product prices.
Much impetus was given to this programme by the campaign organized by the Commission in collaboration with the twelve Member States in the European Year of Health and Safety, which took place during the 12-month period commencing 1 March 1992. This campaign sought to reach the whole of the Community’s working population, particularly targeting high-risk industries and small and medium-sized enterprises.
Each of the founding treaties laid the basis for new health and safety laws. The EEC Treaty, for example, contains two provisions which are, in part at least, devoted to the promotion of health and safety, namely articles 117 and 118.
Community Charter of the Fundamental Social Rights of Workers
To meet the challenge, a comprehensive programme of measures was proposed by the Commission in 1987 and adopted by the Council in the following year. This programme contained a series of health and safety measures grouped under the headings of safety and ergonomics, health and hygiene, information and training, initiatives concerning small and medium enterprises, and social dialogue. Added impetus to these policies was provided by the Community Charter of the Fundamental Social Rights of Workers, adopted in Strasbourg in December 1989 by 11 of the 12 Member States (the United Kingdom abstained).
The Social Charter, as agreed in December 1989, covers 12 categories of “fundamental social rights” among them are several of practical relevance here:
- Improvement of living and working conditions. There should be improvement in working conditions, particularly in terms of limits on working time. particular mention is made of the need for improved conditions for workers on part-time or seasonal contracts and so on.
- Social protection. Workers, including the unemployed, should receive adequate social protection and social security benefits.
- Information, consultation and participation for workers. This should apply especially in multinational companies and in particular at times of restructuring, redundancies or the introduction of new technology.
- Health protection and safety at the workplace.
- Protection of children and adolescents. The minimum employment age should be no lower than the minimum school-leaving age, and in any case not lower than 15 years. The hours which those aged under 18 can work should be limited, and they should not generally work at night.
- Elderly persons. Workers should be assured of resources providing a decent standard of living upon retirement. Others should have sufficient resources and appropriate medical and social assistance.
- Disabled people. All disabled people should have additional help towards social and professional integration.
Member States are given responsibility in accordance with national practices for guaranteeing the rights in the Charter and implementing the necessary measures, and the Commission is asked to submit proposals on areas within its competence.
Since 1989, it has become clear that within the Community as a whole there is much support for the Social Charter. Undoubtedly, Member States are anxious to show that workers, children and older workers should benefit from the Community as well as shareholders and managers.
The 1989 Framework Directive
The principles in the Commission’s health and safety programme were set out in another “Framework Directive” (89/391/EEC) on the introduction of measures to encourage improvements in the safety and health of workers at work. This makes a significant step forward from the approach witnessed in the earlier “Framework Directive” of 1980. In particular, the 1989 Directive, while endorsing and adopting the approach of “self-assessment”, also sought to establish a variety of basic duties, especially for the employer. Furthermore, the promotion of “social dialogue” in the field of health and safety at work was explicitly incorporated into detailed provisions in the 1989 Directive, introducing significant requirements for information, consultation and participation for workers and their representatives at the workplace. This 1989 Directive required compliance by 31 December 1992.
The Directive contains re-stated general principles concerning, in particular, the prevention of occupational risks, the protection of safety and health and the informing, consultation and training of workers and their representatives, as well as principles concerning the implementation of such measures. This measure constituted a first attempt to provide an overall complement to the technical harmonization directives designed to complete the internal market. The 1989 Directive also brought within its scope the provisions of the 1980 Framework Directive on risks arising from use at work of chemical, physical and biological agents. It parallels the ILO Convention concerning Occupational Safety and Health, 1981 (No. 155) and its accompanying Recommendation (No. 161).
The overall objectives of the 1989 Directive may be summarized as being:
- humanization of the working environment
- accident prevention and health protection at the workplace
- to encourage information, dialogue and balanced participation on safety and health by means of procedures and instruments
- to promote throughout the Community, the harmonious development of economic activities, a continuous and balanced expansion and an accelerated rise in the standard of living
- to encourage the increasing participation of management and labour in decisions and initiatives
- to establish the same level of health protection for workers in all undertakings, including small and medium-sized enterprises, and to fulfil the single market requirements of the Single European Act 1986; and
- the gradual replacement of national legislation by Community legislation.
General duties placed upon the employer include duties of awareness, duties to take direct action to ensure safety and health, duties of strategic planning to avoid risks to safety and health, duties to train and direct the workforce, duties to inform, consult and involve the workforce, and duties of recording and notification.
The Directive provided similar safeguards for small and medium-sized enterprises. It is stated, for example, that the size of the undertaking and/or establishment is a relevant matter in relation to determining the sufficiency of resources for dealing with the organization of protective and preventive measures. It is also a factor to be considered in relation to obligations concerning first aid, fire fighting and evacuation of workers. Furthermore, the Directive included a power for differential requirements to be imposed upon varying sizes of undertakings as regards documentation to be provided. Finally, in relation to the provision of information, it is stated that national measures “may take account, inter alia, of the size of the undertaking and/or establishment”.
Under the umbrella of the 1989 Directive, a number of individual directives have also been adopted. In particular, “daughter” directives have been adopted on minimum safety and health requirements for the workplace, for the use of work equipment, for the use of personal protective equipment, for the manual handling of loads, and for work with display screen equipment.
The following Directives have also been adopted:
- Council Directive of 20 December 1993 concerning the minimum safety and health requirements for work on board fishing vessels (93/103/EEC)
- Council Directive of 12 October 1993 amending Directive 90/679/EEC on the protection of workers from risks related to exposure to biological agents at work (93/88/EEC)
- Council Directive of 3 December 1992 on the minimum requirements for improving the safety and health protection of workers in surface and underground mineral-extracting industries (92/104/EEC)
- Council Directive of 3 November 1992 on the minimum requirements for improving the safety and health protection of workers in mineral-extracting industries that involve drilling (92/91/EEC)
- Council Directive of 19 October 1992 on the introduction of measures to encourage improvements in the safety and health at work of pregnant workers and workers who have recently given birth or who are breast-feeding (92/85/EEC)
- Council Directive of 24 June 1992 on the minimum requirements for the provision of safety and/or health signs at work (92/58/EEC)
- Council Directive of 24 June 1992 on the implementation of minimum safety and health requirements at temporary or mobile construction sites (92/57/EEC)
- Council Directive of 31 March 1992 on the minimum safety and health requirements for improved medical treatment on board vessels (92/29/EEC)
- Council Directive of 23 April 1990 on the contained use of genetically modified micro-organisms. (90/219/ EEC)
Since the passage of the Maastricht Treaty, further measures have been passed, namely: a Recommendation on a European schedule of industrial diseases; a directive on asbestos; a directive on safety and health signs at the workplace; a directive on medical assistance on board vessels; directives on health and safety protection in the extractive industries; and a directive introducing measures to promote improvements in the travel conditions of workers with motor disabilities.
The Single Market
The original Article 100 has been replaced by a new provision in the Treaty of European Union. The new Article 100 ensures that the European Parliament and the Economic and Social Committee must be consulted in all cases and not simply when the implementation of a directive would involve the amendment of legislation in one or more Member States.
Principles of Training
Training can and will produce positive results if it is based on clearly defined needs specific to the workplace and if it is delivered with a view to those needs and the ways in which adults learn. This is, of course, true for safety and health training as well. The principles of safety and health training are no different from those which apply to any form of industrial training. Indeed, a good case can be made for the integration of skill training along with safety training wherever possible. Safety and health training which fails to produce positive results because it is not based on sound analysis is, at best, a waste of time and money. At worst, such training may result in false confidence, thus increasing the risk of accidents.
Needs Assessment
The first step in safety and health training design is to identify the problems which need to be addressed. This may be done for the entire organization, for a particular location or for a particular job. Alternatively, the analysis of training needs may have a specific focus, for example, compliance with safety and health legislation or the performance of the joint safety and health committee. However, not all problems can be solved by training; in some cases, other action is needed to supplement it. A simple example of this is the case where the problem identified is a low level of compliance with the rule obliging workers to wear personal protective equipment. While part of the problem may be due to the fact that employees do not understand why the equipment is needed or how to use it correctly, it is equally possible that some or all of the problem may be caused by the fact that there is consistent failure to replace broken or missing equipment.
The existence of problems may surface in the form of a high rate of accidents, refusal-to-work situations or government inspectors' orders or citations. However, it is the problems which underlie such outward signs of trouble that need to be clearly identified. A training needs assessment may be defined as the process of identifying problems that are signalled by deficiencies in compliance with standards or external requirements and that can be resolved wholly or partly by training. A systems approach to training needs analysis involves a number of logical steps: problem identification, analysis, identification of training needs, the ranking of needs in order of urgency and the setting of training goals or objectives.
Problem identification
The sorts of problems that lend themselves to solution by means of training include the following:
Those that are identified after accidents have already happened. In this case, problems may be identified through review of accident statistics, accident investigation reports or, more broadly, through the failure to meet organizational goals for safety and health.
Problems that can be anticipated. Dangers can be identified before actual harm is done—for example, hazards can be foreseen when new machinery, substances or processes are introduced into the workplace, where there exist processes that have never been thoroughly analysed or where existing practice conflicts with known safe procedures .
The existence of external requirements. New legal requirements which either impose specific safety and health training duties or other requirements suggesting the need for training are examples of external requirements. The development of new industry codes of practice or national or international standards affecting safety and health are other examples.
Problem analysis
The next step is to analyse the problems so that necessary training may be identified. Problem analysis involves collecting information about the problem so that its causes can be determined. It also requires determining an appropriate standard which should be met. If, for example, the problem identified relates to a lack of effectiveness of the joint safety and health committee, analysis seeks to answer several questions. First, what is the committee supposed to be doing? Second, how well is the committee performing each of its required tasks? (This question requires the analyst to determine appropriate performance standards which should apply.) Third, why is the committee not performing particular tasks effectively?
Determining solutions
Once the problem has been analysed, the next step is to determine suitable solutions. If training is the solution or part of the solution, the particular training needs must be identified. What combination of skills and knowledge is required and by whom?
A critical part of the investigation of training needs is the assessment of the people involved. The purpose of this is threefold: first, people are likely to be more committed to training (and thus more likely to learn) if they have played a part in identifying the needs themselves; second, it is often necessary to assess the current level of required skill and knowledge among the target group of employees (for example, one might investigate whether joint safety and health committee members actually know what it is they are supposed to be doing); third, basic educational levels and literacy and language skills must be known so that appropriate instructional methods are applied. Surveys can be used to assess a number of these variables. If they are used, however, care should be taken to ensure individual confidentiality.
Setting priorities and goals
Once training needs have been clearly identified, the next step is to set priorities and objectives. Consideration must be given to the relative urgency of various training needs, taking into account factors such as the relative severity of consequences should accidents occur, the frequency with which problems are likely to occur, the number of people affected and legal compliance.
Training objectives must be specific because, if they are not, evaluating whether the training has been successful will prove difficult. Specifically defined objectives also help determine appropriate training content and delivery method. Training objectives or goals establish the results that training should achieve. Examples of specific training objectives might include (a) to ensure that every manager and supervisor knows and understands legal safety and health duties and rights applying to themselves and to all workers, (b) to ensure that all welders know and understand the hazards of welding and the required control procedures or (c) to provide fork-lift truck operators with the skill to operate their vehicles safely according to required procedures
Needs Assessment Methods
Methods for analysing training needs depend on the scope of the assessment and on available resources. All or some of the following methods may be used:
- Documentation review. For example, written statements of safe working practices, legal requirements, company policies and procedures, accident statistics and workplace inspection reports can be examined to determine their bearing on training needs.
- Specific analysis. Accident statistics, joint committee minutes, accident investigation reports and job and task hazard analyses may be examined for their specific relevance to the problem in question.
- Interviews and observation. Interviews with representative samples of supervisors, workers and others may be used to assess attitudes and perceived problem areas; observations can be made of representative jobs to assess compliance with safe working practices.
- Surveys. A survey can be used for relatively large groups to gain information about current skills and knowledge levels and about perceived training needs and problem areas as well.
Choosing Appropriate Instructional Methods
Instructional methods include a number of techniques such as lectures, problem-solving exercises, small group discussion and role-playing.The methods chosen must be appropriate to what is being learned (whether knowledge, skills or concepts) and the training objectives. If, for example, the training objective is to impart knowledge about basic safety rules in the workplace, then a short lecture may be appropriate. However, there are different levels of learning in adults. The lowest level of learning is listening to information; the next level is acquiring knowledge; then, developing understanding; and finally, at the highest level, the ability to apply what is learned to different situations. In most training situations, participants will need to learn at more than one level and so a variety of instructional techniques will be required. Instructional methods must also be based upon sound principles of how adults learn best.
Principles of Adult Learning
The way in which adults learn differs from the way children learn in several important respects. Adults approach the task of learning in possession of life experiences and a developed concept of self. The process of learning is an individual experience which takes place within the learner and depends on the learner's willingness to learn, the ability to relate his or her own experiences to what is being learned and the perceived value of what is being learned to the learner. In many cases, adults make a free choice to learn and so, unlike school children, they are voluntary participants. However, when safety and health training is provided in the workplace, workers and managers may be required to attend training sessions, with little room for individual choice. Where this is so, particular attention needs to be paid to involving learners both in the process of identifying training needs and in the design of the programme itself. Addressing the perceived training needs of workers may be as important as the identification of needs in other areas. Above all, adult training involves change. As with any change, acceptance is dependent on the learners’ belief that they have some control over the change and that the change is not perceived as threatening.
Research has identified a number of factors which facilitate learning in adults:
- Motivation. Since learning is an individual experience, adults must want to learn and must perceive the relevance of what they learn to their personal interest.
- Seeing and hearing. Adults tend to learn best when they can see as well as hear what is being taught. This means that lectures should include accompanying visual material such as overhead transparencies or slides.
- Practice. The opportunity to practise what is being taught facilitates learning. When a skill is being taught (for example, the correct fitting of self-contained breathing apparatus) learners should be allowed to exercise it for themselves. Where the objective is applied knowledge, problem-solving exercises can be used. “Experiential” exercises whereby learners actually experience the application of abstract concepts such as teamwork are valuable instructional tools.
- Relationship to practical experience. Learning is facilitated when the training material can easily be related to the practical experience of the learners. This suggests that examples used should, as far as possible, relate to the industry processes familiar to the learners.
- Participation in the learning process. Adults should know from the start what the learning objectives are and be given the opportunity to test the lesson content against these objectives.
- Feedback. Adults need feedback on their own results (how well they are doing) and positive reinforcement.
- Trying out ideas. The opportunity to try out and develop ideas is part of the individual process of internalizing new information and its application. This can be achieved through small peer group discussions.
- Physical environment. The training facility and equipment should be sympathetic to the learners, allowing them, for example, to see visual material and to work effectively in small groups.
Training Implementation
Careful consideration should be given to the selection of trainers, the scheduling of training and pilot testing. In selecting trainers, two equally important abilities must be sought: knowledge of the subject and teaching ability. Not everyone who has the required safety and health knowledge will necessarily have teaching ability. On the whole, it is easier for people to acquire knowledge than it is to acquire teaching ability. In most workplaces, including the shop floor, there will be a number of people who have a natural teaching ability, and they will have the advantage of knowing the workplace and being able to understand practical examples. In small group learning, a “group learning facilitator” may be used in place of a trainer. In this case, the facilitator is learning along with the group but has responsibilities for the process of learning.
The scheduling of training involves several important considerations. For example, it should be arranged at a time convenient for the learners and when interruptions can be minimized. Training can also be packaged in self-contained modules so that it can be spread out over time—perhaps a three hour module once a week could be scheduled. Not only does this approach sometimes cause less interference with production, it also allows time between sessions for learners to try to apply what has been learned.
Every training programme should be pilot tested before initial use. This allows the programme to be tested against training objectives. Pilot testing should involve not only the trainers but a representative sample of the prospective learners as well.
Training Evaluation
The purpose of evaluating training is quite simply to establish whether the training objectives have been met and, if so, whether this has resulted in solving the problem addressed by those objectives. Preparation for training evaluation should begin at the training design stage. In other words, the problem to be addressed by training must be clear, the training objectives must be specific and the status quo prior to training must be known. For example, if the problem to be addressed is poor observance of safe working practices in material handling operations, and training has been designed to address part of this problem by providing information and skills to, say, fork-lift operators, then a successful outcome in this case would be high observance of correct safe working practices.
Evaluation of training can be done at various levels. At the first level, the aim is simply to assess student reactions to the training programme. Did they like the programme, the instructor and the course material, were they bored, did they feel that they had learned something? This approach may be useful in assessing whether or not the programme was perceived to be of value by the students. Such evaluations are most usefully conducted through an attitude survey and should not generally be administered by the course instructor. Participants are unlikely to provide candid answers at this point even if the questionnaires are anonymous. As an aid to this type of evaluation, students can be allowed to test themselves on the training content.
The next level of evaluation is the assessment of whether or not the learning objectives have been met. Learning objectives are related to the content of the training and they define what the student should be able to do or know when training is completed. Learning objectives are usually developed for each part of the course content and are shared with students so that they know what they should expect to learn. Evaluation at this level is designed to assess whether or not students have learned what is defined in the learning objectives. This can be done by testing participants at the end of the course. Knowledge, concepts and abstract skills can be assessed in written tests whereas practical skills can be assessed by direct observation of students demonstrating the skill. Where this level of evaluation is used, it is absolutely necessary to have prior knowledge of the knowledge or skill baseline of the students before training begins.
The third level of evaluation is the assessment of whether or not the knowledge and skills learned in the training are actually being applied on the job. Such assessment can be made through direct observation at specified intervals of time following training. Evaluation of application on the day following training may produce a result quite different from that based on an evaluation some three months later. It is important to note, however, that if the evaluation shows a lack of application after three months, it may not be the training itself which is defective; it may be due to a lack of reinforcement in the workplace itself.
Finally, the highest level of evaluation is the determination of whether or not the problem addressed by the training has been resolved. If the problem identified was a high rate of musculoskeletal injuries in the shipping and receiving area, is there evidence of the desired drop in the injury rate? Here again, timing is important. In this case, it may take time for the training to become effective. The rate may not drop for a number of months because such injuries are often cumulative; and so the rate for some time may reflect conditions prior to training. Furthermore, the training may result in greater awareness of the problem leading to increased reporting soon after training.
Ideally, all four levels of training evaluation should be built into the training design and implementation. However, if only one level is used, its limitations should be clearly understood by all concerned.
Where training is designed and provided by an external agency, the organization can and should nevertheless evaluate its potential usefulness by applying criteria based on the principles outlined in this article.
Training Reinforcement
No matter how successful training is in meeting objectives, its effect will decline with time if reinforcement is not provided in the workplace on a regular and consistent basis. Such reinforcement should be the routine responsibility of supervisors, managers and joint safety and health committees. It can be provided through regular monitoring of performance on the job, recognition of proper performance and routine reminders through the use of short meetings, notices and posters.
Legislation Guaranteeing Benefits for Workers in China
The occupational safety and health of workers has been an important aspect of legislation laid down in the form of the Labour Law promulgated in July 1994. To urge enterprises into the market system, and in the meantime to protect the rights of labourers, in-depth reforms in the system of labour contracts and wage distribution and in social security have been major priorities in the government agenda. Establishing a uniform welfare umbrella for all workers regardless of the ownership of the enterprises is one of the goals, which also include unemployment coverage, retirement pension systems, and occupational disease and injuries compensation insurance. The Labour Law requires that all employers pay a social security contribution for their workers. Part of the legislation, the draft of the Occupational Disease Prevention and Control Law, will be an area of the Labour Law to which major attention has been devoted in order to regulate the behaviour and define the responsibilities of employers in controlling occupational hazards, while at the same time giving more rights to workers in protecting their own health.
Cooperation Between Governmental Agencies and the All-China Federation of Trade Unions in Policy Making and Legislation Enforcement
The Ministry of Public Health (MOPH), the Ministry of Labour (MOL), and the All-China Federation of Trade Unions (ACFTU) have a long history of cooperation. Many important policies and activities have resulted from their joint efforts.
The current division of responsibility between the MOPH and the MOL in occupational safety and health is as follows:
- From the preventive medical point of view, the MOPH oversees industrial hygiene and occupational health, enforcing national health inspection.
- The focus of the MOL is on engineering the control of occupational hazards and on the organization of labour, as well as overseeing occupational safety and health and enforcing national labour inspection (figure 1) (MOPH and MOL 1986).
Figure 1. Governmental organization and division of responsibility for occupational health and safety
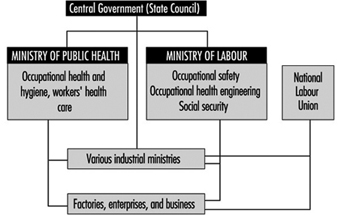
It is difficult to draw a line between the responsibilities of the MOPH and the MOL. It is expected that further cooperation will focus on enhancing enforcement of occupational safety and health regulations.
The ACFTU has been increasingly involved in safeguarding workers’ rights. One of the important tasks of the ACFTU is to promote the establishment of trade unions in foreign-funded enterprises. Only 12% of overseas-funded enterprises have established unions.
Worker Education and Training
Worker training in occupational safety and health may serve many different purposes. Too often, worker training is viewed only as a way to comply with governmental regulations or to reduce insurance costs by encouraging individual workers to follow narrowly defined safe work behaviours. Worker education serves a far broader purpose when it seeks to empower workers to take an active part in making the workplace safe, rather than simply to encourage worker compliance with management safety rules.
Over the past two decades, there has been a move in many countries toward the concept of broad worker involvement in safety and health. New regulatory approaches rely less on government inspectors alone to enforce safety and health on the job. Labour unions and management are increasingly encouraged to collaborate in promoting safety and health, through joint committees or other mechanisms. This approach requires a skilled and well-informed workforce that can interact directly with management on issues of safety and health.
Fortunately, there are many international models for training workers in the full range of skills necessary to participate broadly in workplace health and safety efforts. These models have been developed by a combination of labour unions, university-based labour education programmes and community-based non-governmental organizations. Many innovative worker training programmes were developed originally with financing from special government grant programmes, union funds or employer contributions to collectively bargained safety and health funds.
These participatory worker training programmes, designed in a variety of national settings for diverse worker populations, share a general approach to training. The educational philosophy is based on sound adult education principles and draws upon the empowerment philosophy of “popular education”. This article describes the educational approach and its implications for designing effective worker training.
Educational Approach
Two disciplines have influenced the development of labour-oriented safety and health education programmes: the field of labour education and, more recently, the field of “popular” or empowerment education.
Labour education began simultaneously with the trade union movement in the 1800s. Its early goals were directed towards social change, that is, to promote union strength and the integration of working people into political and union organizing. Labour education has been defined as a “specialized branch of adult education that attempts to meet the educational needs and interests arising out of workers’ participation in the union movement”. Labour education has proceeded according to well-recognized principles of adult learning theory, including the following:
- Adults are self-motivated, especially with information that has immediate application to their lives and work. They expect, for example, practical tools to help them solve problems in the workplace.
- Adults learn best by building on what they already know so that they can incorporate new ideas into their existing, vast reservoir of learning. Adults wish to be respected for their experience in life. Therefore, effective methods draw on participants' own knowledge and encourage reflection on their knowledge base.
- Adults learn in different ways. Each person has a particular learning style. An educational session will work best if participants have the opportunity to engage in multiple learning modalities: to listen, look at visuals, ask questions, simulate situations, read, write, practice with equipment and discuss critical issues. Variety not only ensures that each cognitive style is addressed but also provides repetition to reinforce learning and, of course, combats boredom.
- Adults learn best when they are actively engaged, when they “learn by doing”. They are more responsive to active, participatory methods than to passive measures. Lectures and written materials have their place in a full repertoire of methods. But case studies, role plays, hands-on simulations and other small-group activities that allow each individual to be involved are more likely to result in the retention and application of new learning. Ideally, each session involves interaction between participants and includes occasions for learning new information, for applying new skills and for discussing causes of problems and barriers to solving them. Participatory methods require more time, smaller groups and perhaps different instructional skills than those that many trainers currently possess. But to increase the impact of education, active participation is essential.
Since the beginning of the 1980s, worker safety and health training has also been influenced by the perspective of “popular” or “empowerment” education. Popular education since the 1960s has developed largely from the philosophy of Brazilian educator Paulo Freire. It is an approach to learning that is participatory and is based on the reality of student/worker experiences in their worksites. It fosters dialogue between educators and workers; critically analyses the barriers to change, such as organizational or structural causes of problems; and has worker action and empowerment as its goals. These tenets of popular education incorporate the basic principles of adult education, yet stress the role of worker action in the educational process, both as a goal to improve worksite conditions and as a mechanism for learning.
Participatory education in an empowerment context is more than small group activities that involve students/workers in active learning within the classroom. Participatory popular education means students/workers have the opportunity to acquire analytic and critical thinking skills, practice social action skills and develop the confidence to develop strategies for the improvement of the work environment long after the education sessions end.
Design of Education Programmes
It is important to realize that education is a continuing process, not a one-time event. It is a process that requires careful and skilful planning though each major stage. To implement a participatory education process that is based on sound adult education principles and that empowers workers, certain steps must be taken for planning and implementing participatory worker education which are similar to those used in other training programmes (see “Principles of Training”), but require special attention to meeting the goal of worker empowerment:
Step one: Assess needs
Needs assessment forms the foundation for the entire planning process. A thorough needs assessment for worker training includes three components: a hazards assessment, a profile of the target population and background on the social context of training. The hazards assessment is aimed at identifying high-priority problems to be addressed. The target population profile attempts to answer a broad set of questions about the workforce: Who can most benefit from training? What training has the target population already received? What knowledge and experience will the trainees bring to the process? What is the ethnic and gender makeup of the workforce? What is the literacy level of the workers and what languages do they speak? Whom do they respect and whom do they mistrust? Finally, gathering information on the social context of training allows the trainer to maximize the impact of training by looking at the forces that may support improved safety and health conditions (such as strong union protection that allow workers to speak out freely about hazards) and those that may pose barriers (such as productivity pressures or lack of job security).
Needs assessment can be based on questionnaires, review of documents, observations made in the workplace and interviews with workers, their union representatives and others. The popular education approach utilizes an ongoing “listening” process to gather information about the social context of training, including people's concerns and the obstacles that might inhibit change.
Step two: Gain support
Successful worker education programmes rely on identifying and involving key actors. The target population must be involved in the planning process; it is difficult to gain their trust without having sought their input. In a popular education model, the educator attempts to develop a participatory planning team from the union or shop floor who can provide ongoing advice, support, networking and a check on the validity of the needs assessment findings.
Labour unions, management and community-based groups are all potential providers of worker safety and health education. Even if not sponsoring the training directly, each of these groups may have a key role to play in supporting the educational effort. The union can provide access to the workforce and back up the efforts for change that hopefully will emerge from the training. Union activists who are respected for their knowledge or commitment can assist in outreach and help ensure a successful training outcome. Management is able to provide paid released time for training and may more readily support efforts to improve safety and health that grow out of a training process they have “bought into”. Some employers understand the importance and cost-effectiveness of comprehensive worker training in safety and health, while others will not participate without government-mandated training requirements or a collectively bargained right to paid educational leave for safety and health training.
Community-based non-governmental organizations can provide training resources, support or follow-up activities. For non-union workers, who may be especially vulnerable to retaliation for safety and health advocacy on the job, it is particularly important to identify community support resources (such as religious groups, environmentalist organizations, disabled worker support groups or minority workers’ rights projects). Whoever has a significant role to play must be involved in the process through co-sponsorship, participation on an advisory committee, personal contact or other means.
Step three: Establish education objectives and content
Using information from the needs assessment, the planning team can identify specific learning objectives. A common mistake is to assume that the objective of workshops is simply to present information. What is presented matters less than what the target population receives. Objectives should be stated in terms of what workers will know, believe, be able to do or accomplish as a result of the training. The majority of traditional training programmes focus on objectives to change the individuals' knowledge or behaviours. The goal of popular worker education is to create an activist workforce that will advocate effectively for a healthier work environment. Popular education objectives may include learning new information and skills, changing attitudes and adopting safe behaviours. However, the ultimate goal is not individual change, but collective empowerment and workplace change. The objectives leading to this goal include the following:
- Information objectives are geared towards the specific knowledge the learner will receive, for example, information about the health hazards of solvents.
- Skill objectives are intended to ensure that participants can do specific tasks that they will need to be able to perform back on the job. These can range from individual, technical skills (such as how to lift properly) to group action skills (such as how to advocate for ergonomic redesign of the workplace). Empowerment-oriented education emphasizes social action skills over mastery of individual tasks.
- Attitude objectives aim to have an impact on what the worker believes. They are important for ensuring that people move beyond their own barriers to change so that they are able to actually put their new-found knowledge and skills to use. Examples of attitudes that may be addressed include beliefs that accidents are caused by the careless worker, that workers are apathetic and do not care about safety and health or that things never change and nothing one can do will make a difference.
- Individual behavioural objectives aim to affect not just what a worker can do, but what a worker actually does back on the job as a result of training. For example, a training programme with behavioural objectives would aim to have a positive impact on respirator use on the job, not just to convey information in the classroom as to how to use a respirator properly. The problem with individual behaviour change as an objective is that workplace safety and health improvements rarely take place on an individual level. One can use a respirator properly only if the right respirator is provided and if there is time allowed for taking all necessary precautions, regardless of production pressures.
- Social action objectives also aim to have an effect on what the worker will do back on the job but address the goal of collective action for change in the work environment, rather than individual behaviour change. Actions that result from such training can range from small steps, such as investigating one specific hazard, to large undertakings, such as starting an active safety and health committee or campaigning to redesign a dangerous work process.
There is a hierarchy of these objectives (figure 1). Compared with the other training objectives, knowledge objectives are the easiest to achieve (but they are by no means easy to attain in an absolute sense); skill objectives require more hands-on training to ensure mastery; attitude objectives are more difficult because they may involve challenging deeply held beliefs; individual behaviour objectives are achievable only if attitude barriers are addressed and if performance, practice and on-the-job follow-up are built into the training; and social action objectives are most challenging of all, because training must also prepare participants for collective action in order to achieve more than they can on an individual basis.
Figure 1. Hierarchy of training objectives.
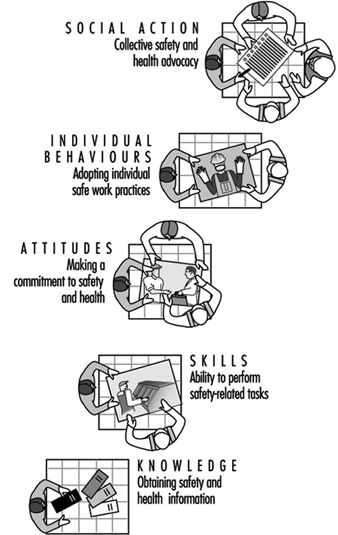
For example, it is a reasonably straightforward task to communicate the risks that asbestos poses to workers. The next step is to ensure that they have the technical skills to follow all safety procedures on the job. It is more difficult still to change what workers believe (e.g., to convince them that they and their fellow workers are at risk and that something can and should be done about it). Even armed with the right skills and attitudes, it may be difficult for workers to actually follow safe work practices on the job, especially since they may lack the proper equipment or management support. The ultimate challenge is to promote social action, so that workers may gain the skills, confidence and willingness to insist on using less hazardous substitute materials or to demand that all necessary environmental controls be used when they are working with asbestos.
Empowerment-oriented labour education always aims to have an impact on the highest level—social action. This requires that workers develop critical thinking and strategic planning skills that will allow them to set achievable goals, constantly respond to barriers and reshape their plans as they go. These are complex skills that require the most intensive, hands-on approach to training, as well as strong on-going support that the workers will need in order to sustain their efforts.
The specific content of educational programmes will depend on the needs assessment, regulatory mandates and time considerations. Subject areas that are commonly addressed in worker training include the following:
- health hazards of relevant exposures (such as noise, chemicals, vibration, heat, stress, infectious diseases and safety hazards)
- hazard identification methods, including means of obtaining and interpreting data regarding workplace conditions
- control technologies, including engineering and work organization changes, as well as safe work practices and personal protective equipment
- legal rights, including those relating to regulatory structures, the worker’s right to know about job hazards, the right to file a complaint and the right to compensation for injured workers
- union safety and health provisions, including collectively bargained agreements giving members the right to a safe environment, the right to information and the right to refuse to perform under hazardous conditions
- union, management, government and community resources
- the roles and responsibilities of safety and health committee members
- prioritizing hazards and developing strategies to improve the worksite, including analysis of possible structural or organizational barriers and design of action plans
Step four: Select education methods
It is important to select the right methods for the chosen objectives and content areas. In general, the more ambitious the objectives, the more intensive the methods must be. Whatever methods are selected, the profile of the workforce must be considered. For example, educators need to respond to workers’ language and literacy levels. If literacy is low, the trainer should use oral methods and highly graphic visuals. If a variety of languages is in use among the target population the trainer should use a multilingual approach.
Because of time limitations, it may not be possible to present all of the relevant information. It is more important to provide a good mix of methods to enable workers to acquire research skills and to develop social action strategies so that they can pursue their own knowledge, rather than attempt to condense too much information into a short period of time.
The teaching methods chart (see table 1) provides a summary of different methods and the objectives which each might fulfil. Some methods, such as lectures or informational films, primarily fulfil knowledge objectives. Worksheets or brainstorming exercises can fulfil information or attitude objectives. Other more comprehensive methods, such as case studies, role-plays or short videotapes that trigger discussion may be aimed at social action objectives, but may also contain new information and may present opportunities to explore attitudes.
Table 1. Teaching methods chart
| Teaching methods | Strengths | Limitations | Objectives achieved |
| Lecture | Presents factual material in direct and logical manner. Contains experiences which inspire. Stimulates thinking to open a discussion. For large audiences. |
Experts may not always be good teachers. Audience is passive. Learning difficult to gauge. Needs clear introduction and summary. |
Knowledge |
| Worksheets and questionnaires | Allow people to think for themselves without being influenced by others in discussion. Individual thoughts can then be shared in small or large groups. |
Can be used only for short period of time. Handout requires preparation time. Requires literacy. | Knowledge Attitudes/emotions |
| Brainstorming | Listening exercise that allows creative thinking for new ideas. Encourages full participation because all ideas equally recorded. | Can become unfocused. Needs to be limited to 10 to 15 minutes. |
Knowledge Attitudes/emotions |
| Planning deck | Can be used to quickly catalogue information. Allows students to learn a procedure by ordering its component parts. Group planning experience. |
Requires planning and creation of multiple planning decks. | Knowledge |
| Risk mapping | Group can create visual map of hazards, controls, and plans for action. Useful as follow-up tool. |
Requires workers from same or similar workplace. May require outside research. |
Knowledge Skills/social action |
| Audiovisual materials (films, slide shows, etc.) | Entertaining way of teaching content and raising issues. Keeps audience’s attention. Effective for large groups. |
Too many issues often presented at one time. Too passive if not combined with discussion. |
Knowledge/skills |
| Audiovisuals as triggers | Develops analytic skills. Allows for exploration of solutions. |
Discussion may not have full participation. | Social action Attitudes/emotions |
| Case studies as triggers | Develops analytic and problem-solving skills. Allows for exploration of solutions. Allows students to apply new knowledge and skills. |
People may not see relevance to own situation. Cases and tasks for small groups must be clearlydefined to be effective. |
Social action Attitudes/emotions Skills |
| Role playing session (trigger) | Introduces problem-situation dramatically. Develops analytic skills. Provides opportunity for people to assume roles of others. Allows for exploration of solutions. |
People may be too self-conscious. Not appropriate for large groups. |
Social action Attitudes/emotions Skills |
| Report back session | Allows for large group discussion of role plays, case studies, and small group exercise. Gives people a chance to reflect on experience. | Can be repetitive if each small group says the same thing. Instructors need to prepare focused questions to avoid repetitiveness. | Social action skills Information |
| Prioritizing and planning activity | Ensures participation by students. Provides experience in analysing and prioritizing problems. Allows for active discussion and debate. | Requires a large wall or blackboard for posting. Posting activity should proceed at a lively pace to be effective. | Social action Skills |
| Hands-on practice | Provides classroom practise of learned behaviour. | Requires sufficient time, appropriate physical space, and equipment. | Behaviours Skills |
Adapted from: Wallerstein and Rubenstein 1993. By permission.
Step five: Implementing an education session
Actually conducting a well-designed education session becomes the easiest part of the process; the educator simply carries out the plan. The educator is a facilitator who takes the learners through a series of activities designed to (a) learn and explore new ideas or skills, (b) share their own thoughts and abilities and (c) combine the two.
For popular education programmes, based on active participation and sharing of worker’s own experiences, it is critical that workshops establish a tone of trust, safety in discussion and ease of communication. Both physical and social environments need to be well planned to allow for maximum interaction, small group movement and confidence that there is a shared group norm of listening and willingness to participate. For some educators, this role of learning facilitator may require some “retooling”. It is a role that relies less on a talent for effective public speaking, the traditional centrepiece of training skills, and more on an ability to foster cooperative learning.
The use of peer trainers is gaining in popularity. Training workers to train their peers has two major advantages: (1) worker trainers have the practical knowledge of the workplace to make training relevant and (2) peer trainers remain in the workplace to provide on-going safety and health consultation. The success of peer trainer programmes is dependent on providing a solid foundation for worker trainers through comprehensive “training of trainer” programmes and access to technical experts when needed.
Step six: Evaluate and follow up
Though often overlooked in worker education, evaluation is essential and serves several purposes. It allows the learner to judge his or her progress toward new knowledge, skills, attitudes or actions; it allows the educator to judge the effectiveness of the training and to decide what has been accomplished; and it can document the success of training to justify future expenditures of resources. Evaluation protocols should be set up in concert with the education objectives. An evaluation effort should tell you whether or not you have achieved your training objectives.
The majority of evaluations to date have assessed immediate impact, such as knowledge learned or degree of satisfaction with the workshop. Behaviour-specific evaluations have used observations at the worksite to assess performance.
Evaluations that look at workplace outcomes, particularly injury and illness incidence rates, can be deceptive. For example, management safety promotion efforts often include incentives for keeping accident rates low (e.g., by offering a prize to the crew with the least accidents in a year). These promotional efforts result in under-reporting of accidents and often do not represent actual safety and health conditions on the job. Conversely, empowerment-oriented training encourages workers to recognize and report safety and health problems and may result, at first, in an increase in reported injuries and illnesses, even when safety and health conditions are actually improving.
Recently, as safety and health training programmes have begun to adopt empowerment and popular education goals and methods, evaluation protocols have been broadened to include assessment of worker actions back at the worksite as well as actual worksite changes. Social action objectives require long-term evaluation that assesses changes on both the individual level and on the environmental and organization level, and the interaction between individual and environmental change. Follow-up is critical for this long-term evaluation. Follow-up phone calls, surveys or even new sessions may be used not only to assess change, but also to support the students/workers in applying their new knowledge, skills, inspiration or social action resulting from training.
Several programmatic components have been identified as important for promoting actual behavioural and worksite changes: union support structures; equal union participation with management; full access to training, information and expert resources for workers and their unions; conducting training within the context of a structure for comprehensive changes; programme development based on worker and workplace needs assessments; use of worker-produced materials; and integration of small group interactive methods with worker empowerment and social action goals.
Conclusion
In this article, the growing need for preparing workers for broad participation in workplace injury and illness prevention efforts has been depicted as well as the critical role of workers as advocates for safety and health. The distinct role of labour empowerment training in responding to these needs and the educational principles and traditions that contribute to a labour empowerment approach to education were addressed. Finally, a step-by-step educational process that is required to achieve the goals of worker involvement and empowerment was described.
This learner-centred approach to education implies a new relationship between occupational safety and health professionals and workers. Learning can no longer be a one-way street with an “expert” imparting knowledge to the “students”. The educational process, instead, is a partnership. It is a dynamic process of communication that taps the skills and knowledge of workers. Learning occurs in all directions: workers learn from the instructors; instructors learn from workers; and workers learn from one another (see figure 2).
Figure 2. Learning is a three-way process.
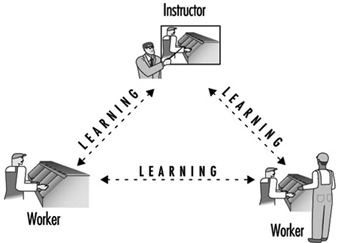
For a successful partnership, workers must be involved in every stage of the educational process, not just in the classroom. Workers must participate in the who, what, where, when and how of training: Who will design and deliver the training? What will be taught? Who will pay for it? Who will have access to it? Where and when will training take place? Whose needs will be met and how will success be measured?
More...
Case Study: Exposure Standards in Russia
Comparison of the Philosophical Bases of Maximum Allowable Concentrations (MACs) and Threshold Limit Values (TLVs)
Rapid development of chemistry and wide usage of chemical products require specific toxicological studies and hazards evaluation with regard to long-term and combined effects of chemical substances. The setting of standards for chemicals in the working environment is being conducted by occupational hygienists in many countries of the world. Experience on the matter has been accumulated in international and multilateral organizations such as the International Labour Organization, the World Health Organization, the United Nations Environment Programme, the Food and Agriculture Organization and the European Union.
Much has been done in this field by Russian and American scientists. In 1922 studies were launched in Russia to set up standards for chemicals in the air of indoor work areas, and the first maximum allowable concentration (MAC) value for sulphur-containing gas was adopted. By 1930 only 12 MAC values were established, whereas by 1960 their number reached 181.
The American Conference of Governmental Industrial Hygienists (ACGIH) started its work in 1938, and the first threshold limit values (TLVs) list was published in 1946 for 144 substances. The TLVs are to be interpreted and used only by the specialists in this field. If a TLV has been included in the safety standards (the so-called standards of national consensus) and the federal standards, it becomes legal.
At present more than 1,500 MAC values have been adopted for workplace air in Russia. More than 550 TLVs for chemical substances have been recommended in the United States.
Analysis of hygienic standards made in 1980–81 showed that 220 chemicals of the MAC list (Russia) and the TLV list (United States) had the following differences: from two- to fivefold differences were found in 48 substances (22%), 42 substances had five- to ten-fold differences, and 69% substances (31%) had more than ten-fold differences. Ten per cent of the recommended TLVs were 50 times higher than the MAC values for the same substances. The MAC values, in turn, were higher than the TLVs for 16 substances.
The largest divergence of standards occurs in the class of chlorinated hydrocarbons. Analysis of the TLV list adopted in 1989–90 showed a trend toward a reduction of the earlier recommended TLVs compared with the MAC values for chlorinated hydrocarbons and some solvents. Differences among the TLVs and the MACs for the majority of metal aerosols, metalloids, and their compounds were insignificant. The divergences for irritant gases were also slight. The TLVs for lead, manganese and tellurium compared with their MAC analogues disagreed 15, 16 and 10 times, respectively. The differences for acetic aldehyde and formaldehyde were the most extreme—36 and 6 times, respectively. In general, the MAC values adopted in Russia are lower than the TLVs recommended in the United States.
These divergences are explained by the principles used in the development of hygienic standards in the two countries and by the way of these standards are applied to protect workers’ health.
A MAC is a hygienic standard used in Russia to denote a concentration of a harmful substance in the air of the workplace which will not cause, in the course of work for eight hours daily or for any other period of time (but not more than 41 hours per week throughout the working life of an individual), any disease or deviation in the health status as detectable by the available methods of investigation, during the working life or during the subsequent life of the present and next generations. Thus, the concept used in defining the MAC does not allow for any adverse effect on a worker or his or her progeny. The MAC is a safe concentration.
A TLV is the concentration (in air) of a material to which most workers can be exposed daily without adverse effect. These values are established (and revised annually) by the ACGIH and are time-weighted concentrations for a seven- or eight-hour workday and 40-hour workweek. For most materials the value may be exceeded, to a certain extent, provided there are compensatory periods of exposure below the value during the workday (or in some cases the week). For a few materials (mainly those that produce a rapid response) the limit is given as ceiling concentration (i.e., a maximum allowable concentration) that should never be exceeded. The ACGIH states that TLVs should be used as guides in the control of health hazards, and are not fine lines between safe and dangerous concentrations, nor are they a relative index of toxicity.
The TLV definition also contains the principle of inadmissibility of harmful impact. However, it does not cover all of the working population, and it is admitted that a small percentage of workers may manifest health changes or even occupational pathologies. Thus TLVs are not safe for all workers.
According to ILO and WHO experts, these divergences are the result of different scientific approaches to a number of interrelated factors including the definition of an adverse health effect. Therefore, different initial approaches for the control of chemical hazards lead to different methodological principles, essential points of which are presented below.
The main principles of setting hygienic standards for dangerous substances in the air of workplaces in Russia compared with those in the United States are summarized in table 1. Of special importance is the theoretical concept of the threshold, the basic difference between the Russian and the American specialists that underlies their approaches to setting standards. Russia accepts the concept of a threshold for all types of dangerous effects of chemical substances.
Table 1. A comparison of some ideological bases for Russian and American standards
|
Russia (MACs) |
United States (TLVs) |
|
Threshold nature of all kinds of adverse effects. Changes of specific and non-specific factors regarding the criteria of harmful impact are evaluated. |
No recognition of threshold for mutagens and some carcinogens. Changes of specific and non-specific factors depending on “dose-effect ”and “dose-response” relationship are evaluated. |
|
Priority of medical and biological factors over technological and economic criteria. |
Technological and economic criteria prevail. |
|
Prospective toxicological assessment and interpretation of standards before the commercialization of chemical products. |
Retrospective setting of standards. |
However, the recognition of a threshold for some types of effects requires the distinction between injurious and non-injurious effects produced by chemical substances. Consequently, the threshold of unhealthy effects established in Russia is the minimal concentration (dose) of a chemical that causes changes beyond the limits of physiological adaptive responses or produces latent (temporarily compensated) pathologies. In addition, various statistical, metabolic, and toxico-kinetic criteria of adverse effects of chemicals are used to differentiate between the processes of physiological adaptation and pathological compensation. Pathomorphological changes and narcotic symptoms of earliest impairment have been suggested in the United States for the identification of injurious and non-injurious effects. It means that more sensitive methods have been chosen for the toxicity evaluation in Russia than those in the United States. This, therefore, explains the generally lower levels of MACs compared to TLVs. When the detection criteria for injurious and non-injurious effects of chemicals are close or practically coincide, as in the case of irritant gases, the differences in standards are not so significant.
The evolution of toxicology has put into practice new methods for the identification of minor changes in tissues. These are enzyme induction in the smooth endoplastic reticular hepatic tissue and reversible hypertrophy of the liver. These changes may appear after exposure to low concentrations of many chemical substances. Some researchers consider these to be adaptive reactions, while others interpret them as early impairments. Today, one of the most difficult tasks of toxicology is obtaining data that show whether enzyme disturbances, nervous system disorders and changes in behavioural responses are the result of deteriorated physiological functions. This would make it possible to predict more serious and/or irreversible impairments in case of long-term exposure to dangerous substances.
Special emphasis is placed on the differences in the sensitivity of methods used for the establishment of MACs and TLVs. Very sensitive methods of conditioned reflexes applied to studies of the nervous system in Russia have been found to be the main cause of divergences between the MACs and the TLVs. However, the use of this method in the process of hygienic standardization is not obligatory. Numerous methods of different sensitivities are normally used for the developing of a hygienic standard.
A great number of studies conducted in the United States in connection with the setting-up of exposure limits are aimed at examining the transformation of industrial compounds in the human body (routes of exposure, circulation, metabolism, removal, etc.). Methods of chemical analysis used to establish the values of TLVs and MACs also cause divergences due to their different selectivities, accuracies and sensitivities. An important element usually taken into consideration by OSHA in the standardization process in the United States is the “technical attainability” of a standard by industry. As a result, some standards are recommended on a basis of the lowest presently existing concentrations.
MAC values in Russia are established on a basis of the prevalence of medico-biological characteristics, whereas the technological attainability of a standard is practically ignored. This partly explains lower MAC values for some chemical substances.
In Russia MAC values are assessed in toxicological studies before a substance is authorized for industrial use. A tentative safe exposure level is established during the laboratory synthesis of a chemical. The MAC value is established after animal experiments, at the design stage of the industrial process. The correction of the MAC value is carried out after evaluation of working conditions and workers’ health when the substance is used in industry. Most of the safe levels of exposure in Russia have been recommended after experiments on animals.
In the United States a final standard is established after a chemical substance has been introduced in industry, because the values of permissible levels of exposure are based on the assessment of health. As long as the differences of principle between the MACs and the TLVs remain, it is unlikely to expect the convergence of these standards in the near future. However, there is a trend towards the reduction of some TLVs that makes this not so impossible as it may seem.
Codes and Guidelines
Range of Purposes Behind Codes
Codes of ethics in the professions serve numerous purposes. At the level of the profession itself, codes document the standards according to which the profession can be held accountable for the conduct of its members. Further, because society relegates control for many of the professions to the professional organizations themselves, the professions have developed codes to provide the basis of self-regulation (Soskolne 1989). At the level of the individual professional, codes can provide a practical guide to members of the profession who might be experiencing a moral or ethical dilemma concerning their professional conduct in a particular circumstance. Where a professional finds himself or herself in a state of moral or ethical tension, it is self-evident that codes can be helpful in providing counsel.
The existence of a code provides the basis of a profession’s ethics programme of activity designed to instil ethical standards among its membership (Gellermann, Frankel and Ladenson 1990; Hall 1993). Revisions to the code can be considered through grass-roots individual membership input at organizational meetings, workshops and conferences. This ongoing discussion of issues and concerns constitutes a review process ensuring that any code remains sensitive to changing social values. Professions depending for their sustenance on public support thereby improve their likelihood of remaining publicly accountable and relevant (Glick and Shamoo 1993).
Codes could assist professionals being charged with malpractice and perhaps even in litigation. Demonstrated adherence to one’s professional code would likely be deemed indicative of adherence to standards of practice consistent with professional norms. If such practice were to have resulted in harm, the code-abiding individual professional would be less likely to be found guilty of having committed a wrong. However, based on the principle of trust (Pellegrino, Veatch and Langan 1991), the public has the expectation that the best possible professional judgement will be exercised in the public interest. Where the physician-patient relationship is concerned, the patient has the right under the principle of trust to expect that his or her interests will be best served. However, an ethical tension arises when the public good is potentially harmed in circumstances where the individual patient’s best interests are being served. In such circumstances, it is the public good that will usually need to take precedence over that of the individual. Regardless, codes provide no substitute for legal liability dimensions of conduct for which government has enacted laws to protect the public interest (Cohen 1982).
Weight and Intent of Codes
Codes do have associated with them the notion of statutory force, implying the ability for their enforcement through the administering of some type of disciplinary action. Indeed, the notions of accountability and self-regulation referred to above have associated with them some sense of control (minimally, peer pressure; maximally, the removal of licence to practice) that can be exercised over the members of the profession by the professional organization itself. Because of this, some professional organizations have preferred to avoid these connotations associated with codes and opt rather for “guidelines”. The latter emphasize guidance with fewer implications for enforcement associated with them. Other groups have preferred to avoid all connotations associated with codes or guidelines; instead, they have preferred to develop “declarations on ethics” for their specific organizations (Jowell 1986). Throughout this chapter the term code will imply “guidelines”.
It should be apparent that codes (and also guidelines) do not carry the force of law. In essence, codes and guidelines are intended to provide guidance for professionals, collectively and individually, in their relationships with their clients (including patients and research subjects), with their colleagues and co-workers (including their students), and with the public (including stakeholder groups). In addition, codes require that the quality of professional work and hence the stature of the profession itself is advanced. In general, codes associated with the physician-patient relationship will require that the patient’s interests take precedence over any other interests; the physician is placed firmly in the position of “patient advocate”. One exception to this would arise in the context of infectious diseases, where the patient’s rights may have to be considered second to the public welfare. In contrast, however, it can generally be stated that codes associated with scientific research will require that the public interest take precedence over any individual or other interests. One exception would be where a researcher discovers child abuse in a research subject; here the researcher would have the obligation to report this to the child welfare authorities.
Code Development, Review and Revision
The process by which codes are developed has consequences for their application. By including members of the profession and students of the profession in code development, as well as in code review and revision, ownership of the resultant document by a greater number of individuals is believed more likely. With broad-based ownership, increased compliance by a greater number is believed more assured.
Content and Structure of Codes
The content of a code should be user friendly to maximize its utility. Codes can be of varying length. Some are brief, while some are substantial. The more substantial that a code is, the more specific it is possible for it to be. Codes can be made to be user friendly by virtue of their structure and content. For example, a summary set of the principles upon which the code is based could be presented first, followed by expanded aspirational or prescriptive statements, which constitute the code itself. These can be followed by a commentary that explicates each statement in turn, perhaps noting special circumstances in the form of case studies that might serve as useful examples. The principles and their interpretation(s), however, are highly dependent on the values recognized as inherent to the pursuits of a profession. While these values may be universal, interpretations as well as practices at the local and regional levels may differ. Thus, while a statement of the profession’s core values can provide an anchor for its statements on ethics and should appear as a preface to the guidelines (Gellermann, Frankel and Ladenson 1990), sensitivity to regional differences can be demonstrated through the more detailed commentary and case study materials.
The commentary should incorporate, or could be followed by or complemented with, case study materials that derive from real-life instances of ethical dilemmas or tensions. The case study materials could be ethically analysed in either sanitized (i.e., anonymous) form, or can be made to reflect the parties involved (of course, only with the approval of the parties for their names to be included) (for example, Soskolne 1991). The objective behind case studies is not to seek retribution, but rather to provide examples for teaching purposes. Learning is enhanced by real-life situations.
It is from an understanding of the code that it becomes possible for a profession to develop more detailed standards of practice. These address more specific areas of activity associated with professional conduct, including a broad range of activity from interpersonal behaviours to both how research is conducted and how the results of that research are communicated. Standards of practice for the profession could be included in an ethics package; they reflect on each profession’s skill set and therefore add particular considerations that go beyond the statement of its ethics principles.
Scope of Codes
The development of a code by any profession has almost invariably tended to be driven by issues having a direct bearing on that profession. Consequently, codes tend to have a focus narrowly defined by each profession’s own concerns. However, codes also need to take broader social issues into account (Fawcett 1993). In fact, in a recent analysis of several codes, Summers et al. (1995) found that guidelines on specific social issues, such as environmental effects or conflict resolution, are scarcely mentioned at all in existing codes. Because the professions manifest substantial influence, if their codes indeed were to take broader social issues into account, then a great confluence and concurrence of effort would be brought to bear on those areas of human endeavour that currently fall between the cracks in promoting the common social good. Such pressure could help reduce dangers to human welfare, such as militarism and ecological destruction.
Ethics Training
It should be recognized that there exist two schools of thought for ethics training: one is based in a principle-driven approach while the other is case based, also known as casuistry. It is this author’s view, which remains to be tested, that a balance between the two is essential for successful applied ethics training in the professions (Soskolne 1991/92). However, it is well known that ethically analyzed case study material has an invaluable role to play in the education process. Cases provide a context for applying principles.
Because graduate ethics training in the professions is becoming more recognized as an essential place for students to gain awareness of the values, ethical principles and standards of practice of the profession, a model curriculum might ideally be included as part of a code; this will facilitate the training of students intent on entering the profession. The need for this is demonstrated through a recent survey that identified inconsistencies and shortcomings regarding the ethics components in graduate training programmes across the United States (Swazey, Anderson and Seashore 1993).
Recent History of Codes in Selected Professions
In western cultures, the medical profession has had the advantage of discussions about ethics since the time of Socrates (470–399 B.C.), Plato (427–347 B.C.) and Aristotle (384–322 B.C.) (Johnson 1965). Since then, codes have been developed and periodically revised in response to newly recognized issues arising, for example, from human value shifts and, more recently, from technological advances (Declaration of Helsinki 1975; Ad hoc Committee on Medical Ethics 1984; Russel and Westrin 1992). Since the 1960s, other professions have become involved in code development for their own professional organizations. The area of professional codes in fact has become a cottage industry since the 1980s. The American Association for the Advancement of Science (AAAS) has been instrumental in this movement. Under the auspices of its Committee on Scientific Freedom and Responsibility, AAAS initiated a seminal professional ethics project designed to examine the features of and activities associated with codes in the science and engineering professions. The report arising from this effort subsequently generated renewed interest in discussing both code development and revision with many of the professions (Chalk, Frankel and Chafer 1980).
The health/caring professions have long been engaged in discussions of ethical tensions arising from the nature of their professional pursuits. The codes that have evolved have tended, however, to focus on the physician-patient relationship, with concerns about confidentiality being pre-eminent. More recently, perhaps motivated by the growth of applied health research, codes have expanded their attention to include issues pertaining to researcher-patient relationships. Because of population-based research, codes now are addressing concerns for researcher-population relationships. The latter has been aided by the experience of other professions such as sociology, anthropology and statistics.
Many of the caring professions related to the practice of occupational health have been engaged in the discussion of professional ethics. These include: industrial hygiene (Yoder 1982; LaDou 1986); epidemiology (Beauchamp et al. 1991; IEA Workshop on Ethics, Health Policy and Epidemiology 1990; Chemical Manufacturers Association’s Epidemiology Task Group 1991; Council for International Organizations of Medical Sciences 1991, 1993); medicine and numerous of its subspeciality areas, including occupational medicine (Coye 1982; American Occupational Medical Association 1986; International Commission on Occupational Health 1992; Standing Committee of Doctors of the EEC 1980); nursing; toxicology; statistics (International Statistical Institute 1986); psychology; engineering and risk analysis.
In the occupationally specific areas of health services (Guidotti et al. 1989), medicine (Samuels 1992) and health and safety (LaDou 1986), as well as in occupational and environmental health (Rest 1995), relevant portions of professional codes have been abstracted. These presentations serve well the need for furthering discussion in these areas with a view to revising extant codes.
The importance of integrating ethics into the day-to-day activities of professionals is exemplified by these recent texts, which contain appropriately detailed sections on ethics. The professional thereby is reminded that in all aspects of professional practice, all decisions and recommendations have consequences with associated ethical underpinnings.
More recent work on the subject of misconduct in science requires integration into newer texts (Dale 1993; Grandjean and Andersen 1993; Office of the Assistant Secretary for Health 1992; Price 1993; Reed 1989; Sharphorn 1993; Soskolne 1993a; Soskolne 1993b; Soskolne and Macfarlane, 1995; Teich and Frankel 1992). Because one of the fundamental goals of science is the pursuit of truth through objectivity, plagiarism and the fabrication or the falsification of data are counter to the scientific ethic. As the scientific enterprise expands to include more and more scientists, misconduct in science is coming to the attention of the public more frequently. However, it is believed that even in the face of increasing competition and the potential for conflicting interests, the vast majority of those engaged in science do adhere to the principles of truth and objectivity. The frequency of misconduct does, however, remain difficult to assess (Goldberg and Greenberg 1993; Greenberg and Martell 1992; Frankel 1992).
The potential harm to particular scientific efforts as a result of misconduct is one concern. Another concern is the loss of faith by the public in scientists, with consequent reductions in support for the scientific enterprise. The latter has such potentially dire consequences for both science and society that all scientists, and especially students of science, need to be trained in the scientific ethic and reminded of these principles from time to time.
Several case studies serve to demonstrate misconduct (Broad and Wade 1982; Office of Research Integrity 1993; Price 1993; Needleman, Geiger and Frank 1985; Soskolne and Macfarlane, 1995; Swazey, Anderson and Seashore 1993; Soskolne 1991). The determinants of ethical dilemmas are numerous, but one survey among risk analysts in New Jersey (Goldberg and Greenberg 1993) suggests that the two most important causes are “on the job pressure” and “pressure caused by economic implications of result”. The authors of this study noted that possible causes of misconduct include “conflicts of interest, competition with unregulated and unscrupulous competitors, and general lack of individual or societal ethics”. While some codes do address the need for honesty and objectivity in science, the seriousness of current pressures to perform in the presence of apparently declining awareness of societal ethics would dictate that training at all levels include the subject of ethics, values and philosophy. Indeed, the United States Public Health Service requires that universities seeking to obtain research grant support have procedures in place for dealing with and reporting misconduct in science (Reed 1989). Furthermore, university training programmes in public health disciplines must include ethics teaching to qualify for federal funding (Office of the Assistant Secretary for Health 1992).
Normative Nature of Codes
Codes of professional conduct tend to be a narrative description of an assemblage of normative practices. These practices pertain to the moral and ethical standards of a group, be it a professional organization, association or society, having a common skill set in the service of people.
The basis of respective codes has been the so-called Golden Rule, which prescribes that one should do to others what one would have others do to oneself, do one’s level best, and call to the attention of others any act of misconduct.
Approaches to Developing Codes
Most professional organizations have produced codes through the top-down approach, where the elected officials of the profession have undertaken the task. However, as noted earlier (see “Code development, review and revision”), the bottom-up approach is more likely to result in compliance with codes, because grass-roots participation in the process results in a feeling of ownership of the outcome and hence a greater likelihood of compliance. The view that the power brokers of the profession have major influence over the specification of what constitutes appropriate professional conduct could detract from the credibility associated with any resultant code. The more that the “final” code is reflective of community norms, the greater the likelihood that it will be adhered to.
Codes developed by international organizations do have the power of influencing regional groups of people to consider the concerns and statements included in international codes. In this way, regions that have not given attention to the development of codes might be stimulated to do so. Presumably, provided the intent of international codes is limited to a function of providing stimulus, ongoing interaction could serve to iteratively modify and update international codes so that ultimately the international code could well reflect transnational concerns. Care must be exercised to respect regional cultural norms that are not in conflict with, for example, accepted declarations on human rights. Hence, code makers should be sensitive to cultural differences, and not allow their work to homogenize human behaviour; cultural diversity must rather be encouraged.
Mechanisms for Enforcement
Noted earlier was the fact that codes do imply some degree of self-regulation if the expectation of accountability is to have meaning. This would suggest the existence of procedures for investigating allegations of misconduct (or malpractice) of any type, and for correcting conduct deemed professionally inappropriate (Price 1993; Dale 1993; Grandjean and Andersen 1993). In addition, some remedy might be provided for any harms that might have derived from professional misconduct.
The procedures to be invoked in investigations of allegations of misconduct or malpractice must be pre-specified. The maxim of “innocent until proven guilty” should be evident and be seen to be applied. However, because public confidence rests on professional self-regulation, investigations should be dealt with as efficiently as possible with respect for due process at all times (Sharphorn 1993; Soskolne 1993a, b).
The threat of revoking professional licence to practice is one way that the profession has leverage to maximize among its members adherence to any codes. Many professions have no such leverage; their membership is made up of dues-paying individuals with a wide range of qualifications for which regional legislatures have not required licensure as a requirement of membership in the profession. The loss of the right to practice one’s profession therefore is not applicable in many professions as a penalty for misconduct. The only recourse in such instances is that of peer pressure.
Current Issues of Concern to Occupational Health Professionals
It is not within the scope of this article to develop a comprehensive code, but rather to present the process by which codes are developed. It is the intent in so doing to provide motivation for the ongoing discussion of codes (as a component of a broader-based professional ethics programme) and to alert the reader to current issues about which further discussion is needed for the possible inclusion of such resolved matters into revised codes.
As noted by Guidotti et al. (1989), certain issues had been overlooked in codes that existed at that time. These included the virtue of full access to accurate information, and that the burden of risk should not be taken by the worker in the presence of unproved but sound evidence. The question of accurate information and implied truth has associated with it issues of scientific integrity (as referred to in North America) or of scientific dishonesty (as referred to in Denmark) (Andersen et al. 1992; Grandjean and Andersen 1993). Clearly, the pursuit of truth as the main target of scientific endeavour must be reinforced at every opportunity, including its full integration into codes, case study materials and ethics programmes generally (Hall 1993).
With technological advances, the ability grows to more precisely measure biological parameters. For example, biomarkers is one area that opens up a Pandora’s box of ethical issues and resulting tensions that have yet to be addressed in codes. Several such issues have been identified by Ashford (1986) and by Grandjean (1991). Since existing codes were developed prior to the availability on a commercial scale of this technology, codes would serve the occupational health community better if they were updated to provide some guidance on related concerns. To achieve this, explication of such thorny questions as the workers’ right to work in the face of high-risk susceptibility identified through biomarker assays, requires extensive discussion in workshops and conferences specially convened for the purpose. Case study materials would assist in this effort. So profound are the ramifications of biomarker studies that their implications, as well as those related to other potential high technology breakthroughs, could be best addressed through the profession’s continual review of the code.
Because issues such as biomarkers can be difficult to resolve, it may be appropriate for like professions dealing with similar issues to consolidate their efforts and establish mechanisms for exchanging information to assist in the resolution of difficult and challenging related ethical issues. In particular, the need to address the timing for introducing high technology procedures for which ethical considerations have not yet been established also needs to be recognized and addressed by standing committees on ethics for the respective occupational safety and health professions. Other stakeholder groups probably should be included in such deliberations, including the community representatives themselves on whom such studies would be conducted.
In a researcher’s enthusiasm to implement new technological measures into studies for which the ramifications are not fully understood (in the belief that benefit would result), it should be recognized that greater harm than benefit to the subjects of these studies could, in fact, arise (e.g., job loss today is potentially more harmful than the possibility of premature death at some future date). Hence, great caution must be exercised in advance of the implementation of such technologies. Only after due discussion has been exercised by the professional groups having an interest in the use of such technologies, together with a broad range of stakeholder interest groups, should their implementation be considered.
Another current issue involves the notion of data privacy, which is one that returns to the public arena periodically. In the age of computers, the potential exists for linking records created for one purpose with records created for another purpose. Advocates of data privacy have been concerned that records so created could be potentially damaging to individuals. While individual rights to privacy must take precedence over the research needs of the community, the fact that population-based research is uninterested in the data at the individual level must be brought to the attention of the data privacy advocates. In so doing, it should be easy to demonstrate that the public good is better served by allowing appropriately qualified researchers, trained in data processing and confidentiality, access to individual data for population-based research purposes.
Concern about the extension of principlism applied in the physician-patient setting to that of the community-research situation has been noted above (see “Recent history of codes in selected professions”). Vineis and Soskolne (1993) have found that the established principles of autonomy, beneficence, non-maleficence and distributive justice are not easily applicable at the societal level. For example, available information about the safety of exposures often is too scanty to allow decisional autonomy; beneficence is considered from the societal viewpoint rather than from that of the individual; and equity is frequently violated. Ethics require careful consideration when defining what is acceptable to society; the simple mathematical formulations used for risk-benefit evaluations cannot be applied directly to individuals. Further development and integration of these ideas are necessary.
In conclusion, codes have a fundamental role to play in the professions. They also could play an important role in safeguarding the common good if they took broader social issues into account. They need to be developed with grass-roots and stakeholder input as part of a broad-based programme of ethics supported by each profession. Codes—including the profession’s core values, the commentary associated with a code and case study materials—must be subjected to a process of periodic review and revision. Now, more than ever, codes are needed not only for professional accountability and self-regulation purposes, but also to help practitioners with the moral and ethical challenges faced by constantly advancing technologies that have implications, amongst others, for the rights and duties of all affected individuals and interest groups. A substantial and challenging task lies ahead.
International Cooperation in Occupational Health: The Role of International Organizations
The role of international organizations is essentially to offer an organized framework for international cooperation. Over the centuries people have exchanged information and experiences in many ways. Cooperation between countries, scientists and professional groups developed progressively over time, but by the beginning of the 20th century it had become obvious that some issues could be faced only collectively.
In general, a distinction is made between “intergovernmental” and “non-governmental” international organizations. Intergovernmental organizations (IGOs) include the United Nations and its specialized agencies. There are also many other intergovernmental organizations, such as the Organization for Economic Cooperation and Development (OECD), the Organization of African Unity (OAU), the Organization of American States (OAS), and regional or subregional entities, such as the European Union (formerly the European Communities), MERCOSUR (Southern Market—Mercado Comun del Sur), the Caribbean Community (CARICOM), the European Free Trade Association (EFTA) and the North American Free Trade Agreement (NAFTA) between Canada, the United States and Mexico.
Some international non-governmental organizations, such as the International Commission on Occupational Health (ICOH) and the International Social Security Association (ISSA), cover all aspects of occupational health and safety. Many international non-governmental organizations are interested in occupational health and safety within the frameworks of their broader activities, such as the employers’ and workers’ organizations and the international associations of various professional groups. Some non-governmental organizations, such as the International Organization for Standardization (ISO), deal with standardization, and many other non-governmental organizations deal with specific subject areas or with specific sectors of economic activities.
Many intergovernmental and non-governmental organizations have interests in occupational health and safety, which involves technical, medical, social and legal aspects as well as a variety of disciplines, professions and social groups. There is a comprehensive network of organizations whose knowledge and capabilities can be used to promote exchange of information and experience among countries.
Aims and Purposes of Intergovernmental Organizations
One of the important roles of international organizations is to translate agreed-upon values into rights and obligations. The Charter of the United Nations (United Nations 1994) provides a good example of what the role of an international organization in the UN system should be—that is, “to achieve international cooperation in solving international problems of an economic, social, cultural, or humanitarian character, and in improving and encouraging respect for human rights and for fundamental freedom for all without distinction as to race, sex, language or religion.” The International Covenant on Economic, Social and Cultural Rights refers to the principles proclaimed in the Charter of the United Nations and recognizes the right of everyone to safe and healthy working conditions.
The aims and purposes of international organizations are set out in their Charters, Constitutions, Statutes or Basic Texts. For example, the Constitution of the World Health Organization (WHO) (1978) states that its aim is “the attainment by all people of the highest possible level of health”. Protection of the worker against sickness, disease and injury arising from employment is one of the tasks assigned to the International Labour Organization (ILO) in the words of the Preamble of its Constitution (see below and ILO 1992). The Declaration on the Aims and Purposes of the International Labour Organization, adopted by the International Labour Conference at its 26th Session in Philadelphia in 1944, recognizes the obligation of the ILO to further, among the nations of the world, the implementation of programmes that will achieve “adequate protection for the life and health of workers in all occupations”.
The international community recognizes that there are issues where countries are interdependent. One of the main roles of the intergovernmental organizations is to address such issues. The Preamble of the ILO Constitution adopted in 1919 recognizes that “the failure of any nation to adopt humane conditions of labour is an obstacle in the way of other nations which desire to improve the conditions in their own countries” and considers that “a universal and lasting peace can only be established if it is based on social justice”. The ILO Declaration of Philadelphia states that “poverty anywhere constitutes a danger to prosperity everywhere”. The WHO Constitution states that an “unequal development in different countries in the promotion of health and control of diseases, especially communicable diseases, is a common danger” and that “the achievement of any State in the promotion and protection of health is valuable to all”. The role of international organizations is to ensure a continuity and create a stability over time towards such long-term policy objectives, while short- and medium-term planning often prevails at the national level because of local social and economic conditions and political circumstances.
Each international organization has a mandate assigned by its constituents. It is within their mandates that international organizations address specific issues such as occupational health and safety. Common features of intergovernmental organizations are that they provide guidance, formulate recommendations and develop standards. International instruments created within the United Nations system that can be applicable at the national level may be divided into two categories. Nonbinding instruments usually take the form of recommendations or resolutions and can serve as a basis for national legislation. Binding instruments entail the obligation that national laws and practices will be brought into line with the decisions agreed upon at the international level. Most binding instruments take the form of international Conventions that require an additional international act of ratification, approval or accession whereby a State establishes its consent to be bound by the obligations of the Convention.
International organizations represent a forum where their constituents elaborate and establish their common policies and strategies in a great variety of fields, including occupational safety and health. This is where countries confront their values and their opinions; exchange information and experience; discuss and propose solutions; and determine the ways to work together towards objectives in order to achieve consensus, agreement, or international conventions that define a common understanding of what is right to do and what should not be done.
One of the advantages of an international organization is to provide for international debates a controlled environment that is governed by rules and procedures agreed upon by its constituents, allowing, at the same time, for a multitude of informal and diplomatic contacts much wider than those that can be made at the level of a single country. Various groups and countries having similar problems in common may compare their approaches and improve their strategies. From an international perspective, it is easier to achieve objectivity about difficult but specific problems linked to national institutional arrangements or to particular historical conditions. Social partners who can hardly meet at the national level sit at the same table. The dialogue is renewed, and hope for a consensus may come to light where it might have been impossible at the national level. Pressure groups can play a catalytic role in the process of consensus building without a need for aggressive strategies. Not only can exchanges of information and experience take place at international conferences, but various groups can measure the worldwide acceptability of their ideas, values and policies at these conferences.
In practice, intergovernmental organizations are involved in a wide variety of activities covering exchange of information, transfer of knowledge, harmonization of terminology and concepts, consensus building, codes of conduct and of good practice, and promotion and coordination of research. Most international organizations also have numerous programmes and activities aimed at assisting their member States to achieve objectives relevant to their mandate, including technical cooperation. International organizations have at their disposal a variety of means of action, such as reports and studies, meetings of experts, seminars, workshops, symposia, conferences, technical advisory services, information exchanges, and a clearinghouse role. In the course of time, basic mandates of international organizations have been enlarged and made more specific by resolutions and programmes that have been approved by their constituents on the occasion of their general assemblies, such as the International Labour Conference of the ILO or the World Health Assembly of the WHO.
The United Nations and Its Specialized Agencies
In the United Nations system, two specialized agencies are directly concerned with occupational health and safety taken as a whole: the International Labour Organization (ILO) and the World Health Organization (WHO). Among the specialized agencies of the United Nations, the International Labour Organization has a unique character since it is tripartite (i.e., its constituents are governments, employers and workers). Another characteristic of the ILO is its standard-setting activities (i.e., the International Labour Conference adopts international Conventions and Recommendations). Since the working environment is considered an integral part of the human environment (International Labour Organization/United Nations Environment Programme/World Health Organization 1978) the United Nations Environment Programme (UNEP) also deals with the matter, in particular as regards chemicals. Its International Register of Potentially Toxic Chemicals (IRPTC) cooperates closely with the ILO and the WHO within the framework of the International Program on Chemical Safety (IPCS).
Apart from their headquarters, international organizations have field structures and specialized institutions or bodies, such as the WHO’s International Agency for Research on Cancer (IARC), and the Pan-American Centre for Human Ecology and Health (ECO), which contributes to the implementation of the Regional Workers’ Health Program of the Pan-American Health Organization (PAHO). The ILO International Training Centre in Turin (Italy) carries out training activities in occupational health and safety and develops training materials for various professional groups, and the International Institute for Labour Studies (IILS) addresses from time to time occupational safety and health issues. The WHO and the ILO have regional offices, area offices and national correspondents. Regional ILO and WHO conferences are convened periodically. The PAHO was founded in 1902 and is also the WHO Regional Office for the Americas. In 1990, the Pan-American Sanitary Conference adopted a resolution on workers’ health (PAHO 1990) which established guidelines for PAHO’s programme and designated 1992 the “Year of Workers’ Health in the Americas”.
The ILO headquarters and field structures support the commitment and the activities of its member States in occupational health and safety within the framework of its International Programme for the Improvement of Working Conditions and Environment (PIACT) (ILO 1984). This programme includes a large variety of advisory services and technical cooperation activities all over the world. The ILO has recently adopted an active partnership policy (APP) that brings the organization closer to its tripartite constituents in member States by strengthening its field structures, most notably through the establishment of multidisciplinary teams (MDTs).
Several other UN specialized agencies have an important role concerning specific aspects of occupational health and safety, such as the International Atomic Energy Agency (IAEA), which is concerned with nuclear safety, the protection of workers from radiation, and the safety of radiation sources. The United Nations Industrial Development Organization (UNIDO) is concerned with occupational safety and health in specific sectors of industry, and is engaged together with the UNEP and the World Bank in preparing guidelines for industrial pollution prevention and control that cover occupational health and safety issues as well. The Food and Agriculture Organization of the United Nations (FAO) promotes safety in the use of pesticides (FAO 1985) and occupational health and safety in forestry, including cooperative arrangements with the ILO and the United Nations Economic Commission for Europe.
The Committee of Experts on Transport of Dangerous Goods of the Economic and Social Council of the United Nations prepared the Recommendations on the Transport of Dangerous Goods, which provide guidance in drafting national legislation and achieving some uniformity throughout the world for various modes of transport. The International Civil Aviation Organization (ICAO) has established international standards for the operation of aircraft and has published a manual of civil aviation medicine that covers aspects relating to occupational health for flying personnel. The International Maritime Organization (IMO) has adopted an International Convention on Safety of Life at Sea (SOLAS). The WHO, the ILO, and the IMO have prepared an International Medical Guide for ships that includes distinct parts containing a schedule for the contents of a ship’s medicine chest and a medical section of the International Code of Signals. A medical first aid guide for use in accidents involving dangerous substances was jointly prepared by the IMO, the WHO and the ILO.
Funding organizations such as the United Nations Development Programme (UNDP) have been financially supporting over the last 25 years a large number of occupational health and safety projects in many countries, including the establishment of national occupational safety and health institutes. The executing agencies for these projects have been the ILO, the WHO, and both organizations jointly. In its economic development projects, the World Bank takes into account environmental, health and human ecological considerations (World Bank 1974), including occupational health and safety. In 1987, the World Bank embarked on a major effort to incorporate environmental concerns into all aspects of its activities. This includes a stronger focus on the development of institutional capacity for environmental management at the country level, a greater recognition of the need to embed environmental concerns into sectoral work, and increased emphasis on the social aspects of environmentally sustainable development (World Bank 1993a). Furthermore, the Report Investing in Health, examines the interplay between human health, health policy and economic development (World Bank 1993b).
Other Intergovernmental Organizations
The activities of the Organization for Economic Cooperation and Development (OECD) are particularly important as regards environmental health issues, safety in the use of chemicals, methods for the evaluation of chemical risks, and protection from radiation. The Council of Europe has adopted a number of resolutions relating to occupational safety and health concerning, for example, safety services within enterprises. The European Social Charter, adopted by the Council of Europe in 1961, recognizes the right of workers to safe and healthy working conditions. The Nordic Council is concerned with occupational safety and health and environmental problems and makes recommendations regarding toxic and dangerous substances, nuclear safety, and protection from radiation, as well as programmes of action on the occupational environment. The Arab Labour Organization, chartered in 1965, is a specialized agency within the framework of the Arab League; it undertakes studies and conducts research in industrial safety and occupational health. The countries from MERCOSUR have a special commission for the harmonization of legislation in occupational health and safety.
The European Union adopts directives that are compulsory for its member States and should be translated into national laws. The European directives cover the whole field of occupational health and safety with the aim of harmonizing national legislation, taking into account the principle of subsidiarity. Three levels of directives can be identified (TUTB 1991): the framework directives, such as the Directive on the Introduction of Measures to Encourage Improvement in Safety and Health of Workers at Work (89/391); those that cover the risks to which workers are exposed (lead, asbestos, noise, ionizing radiation and so on); and those that establish the rules governing the design of work equipment. Technical standards are developed by European Commissions for Standardization (CEN, CENELEC). The Commission of the European Union (formerly the Commission of the European Communities) prepares the directives and has an important occupational safety and health programme (Commission of the European Communities 1990). The European Foundation for the Improvement of Living and Working Conditions, in Dublin, has activities in occupational safety and health, including a working group on occupational health strategies in Europe. The year 1992 was designated the “European Year of Safety, Hygiene and Health Protection at Work”, and a large number of occupational safety and health activities have been supported in countries of the European Union. A European Agency for Safety and Health at Work was established in Bilbao (Spain) as a specialized body of the European Union.
International Non-governmental Organizations
Scientific, professional and other groups also felt the need to develop international cooperation and join in international non-governmental organizations. They may be formed of individual specialists, national associations of specialists, or institutions. The International Commission on Occupational Health (ICOH) was founded in 1906 as the Permanent Commission on Occupational Diseases. It is discussed in a separate article in this chapter.
The International Social Security Association (ISSA) is an international organization of official agencies responsible for the administration of social security and has had a programme concerning the prevention of occupational risks since 1954 and is also discussed separately in this chapter.
While the ICOH and the ISSA are concerned with the whole field of occupational health and safety, there are a number of non-governmental organizations that deal with specific sectors of economic activity, such as agriculture, or with specific subject areas as varied as technology, toxicology, psychology, work organization, process safety, human engineering, epidemiology, social medicine, lifting appliances, cargo handling, pressured vessels, transport of containers and of dangerous materials, safety signals, road safety and nuclear safety. Numerous international non-governmental organizations are concerned with the environment and the protection of consumers, including the International Union for Conservation of Nature and Natural Resources—World Conservation Union (IUCN) and the International Organization of Consumers Unions (IOCU). They are interested in environmental health and, to some extent, in occupational health, particularly in chemical safety and pesticides.
In the field of the protection of workers, patients and the public from adverse effects of ionizing radiation, the work of the International Commission on Radiological Protection (ICRP) is authoritative worldwide and serves as a basis for international recommendations by intergovernmental organizations. The International Radiation Protection Association (IRPA) has established an International Commission on Non-Ionizing Radiation Protection (ICNIRP), which issues guidelines on exposure limits and contributes to the ILO and WHO publications on non-ionizing radiation. Many other international non-governmental organizations or associations could be mentioned since they deal with occupational health and safety or are interested in specific aspects of occupational health and safety, including the International Ergonomic Association (IEA), the Ergonomics Society of French-Speaking Countries (SELF), the International Council of Nurses (ICN), the Inter-American Safety Council (IASC), the International Association of Labour Inspection (IALA), the International Occupational Hygiene Association (IOHA), the International Association on Agricultural Medicine and Rural Health (IAAMRH), the International Association of Public and Rural Health, the Latino-American Association of Occupational Safety and Hygiene (ALASEHT), the International Federation of Associations of Specialists in Occupational Safety and Industrial Hygiene, the European Association of Schools of Occupational Medicine, the World Federation of Associations of Clinical Toxicology and Poison Control Centres, and the International Safety Council, a global subsidiary of the US National Safety Council.
Another group of non-governmental organizations consists of those having standardization as their objective, such as the International Organization for Standardization (ISO) and the International Electrotechnical Commission (IEC). ISO is discussed in a separate article in this chapter.
International employers’ and workers’ organizations play a significant role in defining occupational health and safety policies and priorities at the international level. Their involvement is important because national labour laws and regulations make employers responsible for protection against occupational hazards, and the most concerned are the workers themselves, since it is their health and safety that are at risk. A number of employers’ and workers’ international organizations are concerned with occupational safety and health taken as a whole, including the International Employers Organization (IOE), the Union of Industrial and Employers Confederations of Europe (UNICE), the International Confederation of Free Trade Unions (ICFTU), the World Confederation of Labour (WCL), and the World Federation of Trade Unions (WFTU). There are many sectoral international trade union organizations that deal with specific aspects, such as the International Confederation of Chemical, Energy, Mine and General Workers’ Union (ICEM), the International Metal Workers Federation (IMF), the International Federation of Building and Wood Workers (IFBWW), the International Federation of Plantation, Agricultural and Allied Workers, and the International Federation of Commercial, Clerical and Technical Employees (FIET). There also exist regional organizations, such as the Organization of African Trade Union Unity (OATUU) and the European Confederation of Trade Unions (ECTU), which has established a European Trade Union Technical Bureau for Occupational Safety and Health (TUTB). These organizations have a wide variety of activities, in particular concerning the dissemination of information, technical advice, and training in occupational health and safety.
Producers, manufacturers, and operators are also active in the field of occupational safety and health, either through their associations or through institutes and bodies that they have established, such as the International Council of Chemical Associations (ICCA), the European Council of Chemical Manufacturers Federations (CEFIC), the International Group of National Associations of Agrochemical Manufacturers (GIFAP), the International Air Transport Association (IATA), the World Association of Nuclear Power Plant Operators (WANO), the Illuminating Engineering Society (IES), the Asbestos International Association (AIA), the International Fiber Safety Group (IFSG), and the Viral Hepatitis Prevention Board (action on hepatitis B as an occupational hazard). In addition, a number of institutions and international bodies established by producers, manufacturers and their organizations develop activities relating to the protection of the environment and environmental health, which may include occupational health to some extent, such as the International Centre for Industry and the Environment (ICIE), the International Council on Metals and the Environment (ICME), the International Primary Aluminum Institute (IPAI), and the Oil Companies International Study Group for Conservation of Clean Air and Water (CONCAWE).
Finally, there are many international non-governmental organizations established by scientists, professional associations or groups having similar scientific, humanitarian or economic interests that do not have direct interests in occupational health but are dealing with scientific, technical, medical or social issues that are relevant to occupational health and safety, such as the World Medical Association (WMA), the Council for International Organizations of Medical Sciences (CIOMS), the International Union of Pure and Applied Chemistry (IUPAC), the International Council for Building Research Studies and Documentation, the International Epidemiological Association, the International Society for Labour Law and Social Security, and the International Bureau for Epilepsy (IBE), which prepared a Code of Principles of Good Practice for Employing People with Epilepsy.
Joint Programmes in International Cooperation
It is interesting to examine how international organizations complement each other and mobilize their various means of action to combat specific occupational hazards. As regards noise and vibration, for example, the IEC provides standards for measuring equipment, the ISO defines methods of measurement, the WHO provides health criteria, the ILO recommends exposure limits in its Code of Practice on Noise and Vibration and defines a general approach and strategy in its Working Environment (Air Pollution, Noise and Vibration) Convention, 1977 (No. 148) and Recommendation (No. 156).
The role of international organizations is increasingly characterized by cooperation within the framework of international programmes or joint ventures on specific subjects involving the countries themselves and inter-governmental and non-governmental organizations. International cooperation in protection against ionizing radiation and in promotion of chemical safety are two examples of such activities.
In the field of protection against ionizing radiation, the International Commission on Radiological Protection (ICRP) and the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) provide the scientific input. The ILO adopted in 1960 the Radiation Protection Convention (No. 115) and Recommendation (No. 114), which make specific reference to the guidance issued by the ICRP. More guidance is given in a number of codes of practice prepared by the IAEA, cosponsored by the ILO and the WHO, where appropriate, and in the ILO Code of Practice on Radiation Protection (ionizing radiation), 1987. These are supplemented by guides, manuals, training materials and technical documents published essentially by the IAEA and by the Nuclear Energy Agency of the OECD. Technical cooperation activities in this field are mainly carried out by the IAEA; other organizations are involved when needed.
In 1990, an important step towards international harmonization of radiation safety took place: the Inter-Agency Committee on Radiation Safety (IACRS) was established as a forum for consultation on and collaboration in radiation safety matters between international organizations. A joint secretariat was set up to revise the 1982 edition of the IAEA/ILO/WHO/NEA-OECD Basic Safety Standards for Radiation Protection. Six international organizations—the FAO, the IAEA, the ILO, the Nuclear Energy Agency of the OECD, the PAHO, and the WHO—joined to prepare international standards with the aim of helping their member States in drafting their own laws. Under the leadership of the IAEA, a major process of consultations with countries and among intergovernmental and non-governmental organizations, including employers’ and workers’ organizations, led to the elaboration of the International Standards for Protection against Ionizing Radiation and the Safety of Radiation Sources (IAEA 1994). These international standards can be regarded as unified standards for the UN system.
International cooperation in promoting chemical safety illustrates how international organizations interact in order to respond to concerns of people in the world expressed by the international community, and how general declarations of principles adopted by intergovernmental conferences are translated into programmes of action and practical activities based on scientific knowledge. There is a consensus that the evaluation of chemicals should address concerns about occupational exposures, public exposures, and the environment. To carry out risk assessments in an international framework is an asset for mobilizing limited expertise and resources. This led to the establishment in 1980 of the International Programme on Chemical Safety (IPCS) by the WHO, the United Nations Environment Programme (UNEP) and the ILO. The commitment of the three cooperating organizations to collaborate in the IPCS was expressed through a memorandum of understanding in 1988 that establishes the objectives of the IPCS. The technical work of the IPCS relies on a network of national and international institutions that participate in its activities and are responsible for particular tasks. The programme maintains close and efficient working relations with several other intergovernmental and non-governmental organizations, associations, and professional bodies that have important activities in the field of chemical safety.
The United Nations Conference on Environment and Development (UNCED), held in Rio de Janeiro in 1992, recognized the need to ensure the environmentally sound management of toxic chemicals and identified six programme areas for international cooperation:
- expanding and accelerating the international assessment of chemical risks
- harmonization of classification and labelling of chemicals
- information exchange on toxic chemicals and chemical risks
- establishment of risk reduction programmes
- strengthening of national capabilities and capacities for management of chemicals
- prevention of illegal international traffic of toxic and dangerous products.
This was followed in 1994 by an International Conference on Chemical Safety (Stockholm Conference 1994), which established the Intergovernmental Forum on Chemical Safety, identified a number of priorities for action, and invited intergovernmental organizations to participate in an expanded collaborative programme on chemical safety. An Inter-Organization Programme for the Sound Management of Chemicals (IOMC) was established in which the WHO, ILO, UNEP, FAO, UNIDO and OECD participate. It includes an Inter-Organization Coordinating Committee (IOCC), which ensures the coordination of activities on chemical safety carried out by the participating organizations, individually or jointly, and follows up the implementation of the recommendations of UNCED.
There are signs of an increasing trend to mobilize expertise and resources within the framework of joint activities. Such is the case, for example, in the field of training and information exchange in occupational health and safety. As regards biological safety, cooperation was developed between the UNIDO, the UNEP, the WHO and the FAO, and some activities were carried out within the framework of the IPCS. The UNIDO has been designated to follow up Chapter 16 of Agenda 21 (environmentally sound management of biotechnology) of the Rio Conference, to catalyze joint activities and programmes, and to develop common UN system strategies on biotechnology. The OECD has a programme on environmental aspects of biotechnology. The European Directive concerning the protection of workers against biological agents at work (90/679 and 93/88) was adopted in 1990 and modified in 1993. In 1993, the International Labour Conference of the International Labour Organization adopted a resolution concerning exposure to and safety in the use of biological agents at work that indicates that the issue should be studied, including the need for new international instruments (convention, recommendation, or both) to minimize the risks to workers, the public and the environment.
Two additional examples concern the protection of workers against non-ionizing radiation and the harmonization of chemical classification and labelling systems. Environmental health criteria documents on non-ionizing radiation were prepared by the WHO, the UNEP and the International Commission on Non-Ionizing Radiation Protection (ICNIRP). A broader cooperation on protection against non-ionizing radiation, including occupational exposure, is now developing, which includes the ILO, the Commission of the European Union, the International Electrotechnical Commission (IEC), the International Agency for Research on Cancer (IARC) and the Scientific Committee on Radiation and Work of the ICOH. The harmonization of chemical classification and labelling systems is a field where extensive cooperation is promoted, under the leadership of the ILO, among countries, intergovernmental organizations (e.g., OECD; the European Union), non-governmental organizations (employers’ and workers’ organizations; international consumer and environmental protection associations), the UN Committee of Experts on Transport of Dangerous Goods, the FAO, the UNEP, the WHO, the IMO and the ICAO.
There are many other fields where new, flexible forms of international cooperation among countries and international organizations are emerging or could be developed, such as occupational stress and combating occupational lung diseases, in particular silicosis. International networking for occupational health and safety is developing increasingly with objectives such as coordinating research. It would be an advantage if an international network for occupational health and safety could be developed on the basis of existing structures in international organizations that could be interconnected, such as the Collaborating Centres of WHO, the Scientific Committees of ICOH, the International Sections of ISSA, the National Correspondents of IRPTC, the contact points of the OECD Complementary Information Procedure, the Participating Institutions of IPCS, the National and Collaborating Centres of the ILO International Occupational Safety and Health Information Centre (CIS), and the designated bodies of the ILO International Occupational Safety and Health Hazard Alert System.
Common Goals and Complementary Approaches in Occupational Health
In the field of occupational health, the ultimate goals of the WHO and the ILO are the same: to protect and promote the health of the workers in all occupations. Policy guidance is given by the ILO on the basis of its international Conventions and Recommendations on occupational health and safety and by the WHO through the resolutions adopted by the World Health Assembly concerning workers’ health and the primary health care approach that it advocates.
Since the Primary Health Care Conference in Alma-Ata in 1978, the WHO workers’ health programme has attempted to extend its health protection and health promotion activities to cover all people at work, paying special attention to the underserved and the vulnerable working populations. The 40th World Health Assembly requested the Director-General of the WHO:
- to promote the implementation of the workers’ health programme, as part of the national health system based on primary health care, in close cooperation with other relevant programmes, non-governmental organizations, and all United Nations agencies
- to elaborate guidelines on primary health care in the workplace, addressed particularly to the underserved working populations and including the educational materials needed at various levels
- to develop guidelines on health promotion in the workplace in cooperation with the WHO collaborating centres
- to promote regional activities in workers’ health where appropriate.
In October 1994, the Second Meeting of the Network of Collaborating Centres in Occupational Health (52 research and expert institutions from 35 countries) adopted a “Global Strategy on Occupational Health for All” and recommended that this document be submitted for consideration by the WHO to be converted into the WHO “Global Strategy on Occupational Health for All”. This was done in May 1996, with the support of the ILO.
The ILO Conventions and Recommendations on occupational safety and health define the rights of the workers and allocate duties and responsibilities to the competent authority, the employers and the workers in the field of occupational safety and health. The ILO Conventions and Recommendations adopted by the International Labour Conference, taken as a whole, constitute the International Labour Code, which defines minimum standards in the labour field. The ILO policy on occupational health and safety is essentially contained in two international Conventions and their accompanying Recommendations. The ILO Occupational Safety and Health Convention 1981 (No. 155) and Recommendation (No. 164), provide for the adoption of a national occupational safety and health policy and describe the actions needed at the national level and at the enterprise level to promote occupational safety and health and to improve the working environment. The ILO Occupational Health Services Convention 1985 (No. 161) and Recommendation (No. 171), provide for the establishment of occupational health services which will contribute to the implementation of the occupational safety and health policy and will perform their functions at the enterprise level.
In 1984, the International Labour Conference adopted a Resolution concerning the improvement of working conditions and environment, which recalled that the improvement of the working conditions and environment was an essential element in the promotion of social justice. It stressed that improved working conditions and improved environment are a positive contribution to national development and represent a measure of success of any economic and social policy. It spelled out the three fundamental principles that:
- Work should take place in a safe and healthy working environment.
- Conditions of work should be consistent with workers’ well-being and human dignity.
- Work should offer real possibilities for personal achievement, self-fulfilment, and service to society.
There are many similar features between the ILO strategy for the improvement of the working conditions and environment and the WHO primary health care approach. They rest on similar basic principles and they both:
- aim at all concerned, workers or the public
- define policies, strategies and means of action
- insist on the responsibility of each employer for the health and safety of the workers in his or her employment
- emphasize primary prevention, control of risk at the source, and health education
- give special importance to information and training
- indicate the need to develop an occupational health practice that is easily accessible to all and available at the workplace
- recognize the central place of participation—community participation in health programmes and workers’ participation in the improvement of the working conditions and the working environment.
- highlight the interactions between health environment and development, as well as between occupational safety and health and productive employment.
The current trend of globalization for the world economy, and regional integration, has increased interdependence and the need for cooperation between countries. This overview shows that there are common goals, approaches and policies in occupational health and safety. There is also a structure on which a global cooperation can be built. This is the objective of the Global Programme on Safety, Health and the Environment, to be launched by the ILO in 1998.
Responsible Science: Ethical Standards and Moral Behaviour in Occupational Health
From the onset, we wish to make it clear that we are not experts in ethics, nor do we represent ourselves as experts. Just like the rest of you, we are scientists, doing scientific things, searching for truth. In that arena, we are faced with the same issues as you—the difference between right and wrong, good and bad, and objectivity and subjectivity. As researchers, we grapple with difficult questions concerning methods and outcome. And those of us who become administrators agonize over the same questions, especially in regard to policy decisions in developing adequate occupational standards to protect workers.
In preparing this paper, we reviewed a number of books and documents in search of simple answers to complex problems. We looked not only at papers written by occupational safety and health professionals, but also reviewed some of the classic textbooks on ethics.
On the professional side, we read a number of articles and codes of ethics from various research groups. They all have components relevant to occupational health research. Yet the focus of each is quite different, reflecting the kind of research done by each author. Some include numerous pages of what to do and what not to do. Others are more general in content.
On the textbook side, ethical theories abound, from before Socrates up until today. There is no shortage of articles about ethics, codes of conduct, and written discussions of ethical standards. In the United States at least, most of the medical colleges have medical ethicists on staff, and almost every university with a sizeable department of philosophy has an ethicist on the faculty. It is a discipline to which people devote their lifetimes, which confirms the complexity of the issue.
Before we begin this discussion, it is important that we attempt to make it clear what we are talking about. What is meant by the term ethics? In the English language, the terms ethics and morals are used interchangeably. Since we are preparing this paper for a diverse group, we did what we think to be an interesting poll of some Centers for Disease Control and Prevention (CDC) professionals for whom English is their second language. A woman whose first languages are Slavic, German and Russian replied that there are similar words in all of her first languages. She said that in the Slavic language, neither ethics nor morals stands alone as they do in English. For example, she said that you wouldn’t say that someone is without morals, you would say that they exhibit behaviour that is not moral. She said that in the Slavic language you wouldn’t say that someone is without ethics, you would say instead that the person is without ethical principles. A Chinese national said that there are separate Chinese words for both morals and ethics, but they are used interchangeably. Spanish-, French- and German-speaking people said there are words for both in their respective languages and that the words are used interchangeably.
In the textbooks on ethical theory that we reviewed, however, the ethicists made a distinction between ethics and morals which we choose to accept for the sake of clarity. Melden (1955) and Mothershead (1955) both suggest that the word ethics is used when referring to a set of principles or standards for conduct, and that the word morals is used when referring to the conduct of a person or group, i.e., their behaviour. This usage is consistent with the replies of the CDC professionals.
Professor Melden says in his book, “We are all familiar with such rules of conduct. Each society, religion, professional group, or distinguishable community has its principles, its standards of conduct. As persons who are concerned with being responsible in our conduct, we rely ordinarily upon a body of principles for guidance in conduct.” Examples of these principles are all around us. In the Judeo-Christian community, there are at minimum the Ten Commandments. In every society, we have laws at the local, national and international levels which describe and dictate both unacceptable and acceptable behaviour. There are also the scientific method, the International Code of Ethics for Occupational Health Professionals and Guidance on Ethics for Occupational Physicians, to name a few examples. The list could go on and on. The point here is that we are exposed to a number of standards of conduct, or ethics, as we use the term. It is quite fitting that we begin the work of setting some standards for ourselves.
Why do health professionals need standards for our work? As Professor Melden states, we are persons who are concerned with being responsible. To make good science demands the highest responsibility on our part, which leads to the promotion of safety and health. On the other hand, no matter how good the intentions of the researcher may be, compromised science can lead to death, disease, disability and dismemberment, rather than the protection of workers. The bottom line is that workers suffer when science is compromised.
Why does compromised science happen? From our perspective, there are a number of reasons.
Sometimes science is compromised because we don’t know any better. Take for example three workplace tragedies: asbestos, benzene and silica. In the early days, the dangers of these substances were unknown. As technology improved, as the science of epidemiology developed and as medicine became more sophisticated, the obvious became evident. In each of these histories, the problems existed, but scientists did not possess or in some cases apply the tools available to uncover them.
Sometimes science is compromised because it is bad science. We are certain that all of you have seen bad science or have read about it in scientific journals. It is bad because it isn’t science at all. It is opinion expressed in such a way that it appears scientific and therefore factual. This situation is one that can easily be addressed through a rigorous peer review process.
Sometimes science is compromised because the researcher is rushed, due to unrealistic time constraints, lack of funds or influences other than purely scientific analysis. An obvious example of this is a toxicological cancer study in which the test animals’ lives were terminated after less than a third of their normal life span, thus eliminating a sufficient latency period for them to develop cancer as a result of their exposures. Thoroughness was compromised and conclusions reached with only part of the picture considered.
And perhaps worst of all, sometimes science is compromised in pursuit of profit or academic advancement. Likewise, we have all seen evidence of this in the newspapers and professional journals. In some of these instances, the gain to the researcher was academic standing and not financial at all. In others, financial gain, either immediate or future, influenced the outcome. In the first case referred to above, researchers with financial interests in asbestos did not report their own positive findings until many years later, when many thousands of workers had already suffered and died of diseases associated with uncontrolled asbestos exposure (Lemen and Bingham 1994). In some instances, we have seen that those who pay for the research may ultimately influence the outcome.
These are but a few of the cases where a code of ethics could come into play, although any code, no matter how wonderful, will not stop the unscrupulous.
Occupational health is a complex and difficult discipline in which to prevent unethical conduct. Even when we discover methods for prevention of occupational diseases and injuries, the solution to the problem is often viewed as cutting into profits, or the problem is hidden to avoid the expense of the remedy. The profit motive and the complexity of the issues we address can lead to both abuse and shortcuts in the system. What are some of the major difficulties?
Often, occupationally caused maladies have incredibly long incubation periods, giving rise to confounding variables. By comparison, in many infectious diseases results seem quick and simple. An example is a well-managed vaccine campaign for measles in an outbreak situation. In this case, there is a short incubation period, an almost 100% infection rate of those susceptible, a vaccine that is 95 to 98% effective and a total eradication of an epidemic, all accomplished in a few days. That situation is quite different from asbestosis or carpal tunnel syndrome, where some people are affected, but others are not, and most often months or years elapse before disability occurs.
Occupational health concerns are multidisciplinary. When a chemist works with other chemists, they all speak the same language, each has but one interest and the work can be shared. Occupational health, on the other hand, is multidisciplinary, often involving chemists, physicists, industrial hygienists, epidemiologists, engineers, microbiologists, physicians, behaviourists, statisticians and others. In the epidemiological-triad (host, agent, environment), the host is unpredictable, the agents are numerous and the environment is complex. The cooperation of several disciplines is mandatory. A variety of professionals, with totally different backgrounds and skills, is brought together to address a problem. The only commonality between them is the protection of the worker. This aspect makes peer review even more difficult because each speciality brings its own nomenclature, equipment and methods to apply to the problem.
Because of long incubation periods in many occupational diseases and conditions, coupled with the mobility of the workforce, occupational health professionals are often forced to fill in some blanks since many of those workers exposed or at risk cannot be located. This condition leads to a reliance on modelling, statistical calculations, and sometimes compromise in the conclusions. The opportunity for error is great, because we are not able to fill in all of the cells.
Sometimes it is difficult to relate a malady to the work environment or, even worse, to identify the cause. In infectious diseases, the epidemiological triad is often less complex. In the 1990s, CDC staff investigated an outbreak of illness on a cruise ship. The host was well defined and easily located, the agent was easily identified, the mode of transmission was obvious, and the remedial action was evident. In occupationally related disease and injury, the host is defined, but often difficult to find. There are a number of agents in the work environment, often causing synergism, plus other workplace factors which are not directly involved in the health problem but which play an important role in the solution. These other workplace factors include such things as the interests and concerns of the labour force, the management and involved government agencies.
So now to the business at hand—coming up with a code of ethics, a set of principles or standards of conduct, used to guide our conduct, our behaviour, in this complex environment.
As Professor Melden (1955) so clearly writes, “Further, we cannot depend wholly upon such principles for guidance, simply because it is impossible to lay down a set of rules complete enough to anticipate all possible occasions for moral decision.” He goes on to say that “A set of moral principles covering all possible moral eventualities is just as impossible as a set of laws so complete that no further legislation is necessary”. Similarly, Kenneth W. Goodman (1994b), states that “While it is important to realize that science and ethics are closely, even inextricably, linked, there is no reason to suppose that a formal code of ethics will provide closure for all or most disagreements about the nature of data, selection of data, data management, and so forth.” To quote Professor Melden once again, “To be useful, moral principles must be general; but being general, their utility is inescapably limited”.
With the above caveats in mind, we propose to you that the following statements be part of a code of ethics for occupational health.
- That, at a minimum, peer review be required and include tripartite review with worker, industry and government representation, as well as review by academia. This process is difficult because it takes time—time to identify learned reviewers from all three areas, time to bring them together for discussion, and often considerable time to address each of their concerns. For the US National Institute for Occupational Safety and Health, at least, this process is required for all publications. We do not pretend to have all the answers, nor do we alone have all the facts. Much can be learned from labour and industry about workplace situations and problem resolution. Tripartite review is the only way we know of to minimize the effects of special interest groups.
- That even perceived compromises are avoided. Sometimes good science has no credibility because of perceived compromise. Examples of compromises include the funding source for the study, the interest groups selected to review the study, and known bias of reviewers. There are judgement calls on the part of the researcher, and even though the judgement and subsequent decision may be sound, there can be a perceived compromise in the study.
- That study protocols receive review by peers before the study is undertaken. The best-intentioned researcher can build a bias into a protocol. This will become obvious only upon careful protocol review.
- That the scientific method is followed from the start: (a) form a hypothesis, (b) do a literature search, (c) collect data, (d) collate data, (e) test the hypothesis and (f) disseminate results.
- That when using science to develop an occupational health or safety standard, all parties involved in the decision declare their affiliations, their financial interests, their potential conflicts with the industry or substance being regulated, and that all of these facts are clearly delineated in the final documentation of the standard. For any standard or recommended standard, perception is of utmost importance. If it is viewed that the standard was based on a biased interpretation, then the standard will lack credibility. Standards based solely on the interpretation of the science by individuals associated with the industry under consideration would suffer from such an interpretation or, worse yet, could fall short of adequately protecting the workers at risk. Building in check factors such as those described above during the development of the new standard will assure that this will not occur.
We have attempted to discuss a complex and sensitive issue. There are no easy solutions. What we are attempting is right and just, however, because its goal, to protect the worker in the workplace, is right and just. We cannot do this alone, we cannot do it in a vacuum, because the problems we address are not in a vacuum. We need each other, and others, to ferret out our natural instincts for personal gain and glory and to uncover our built-in biases. Such an effort will enable us to contribute to the knowledge and enhance the well-being of humanity.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."