- You are here:
-
Home

- Part III. Management & Policy

Children categories

17. Disability and Work (10)

17. Disability and Work
Chapter Editors: Willi Momm and Robert Ransom
Table of Contents
Figures
Disability: Concepts and Definitions
Willi Momm and Otto Geiecker
Case Study: Legal Classification of Disabled People in France
Marie-Louise Cros-Courtial and Marc Vericel
Social Policy and Human Rights: Concepts of Disability
Carl Raskin
International Labour Standards and National Employment Legislation in Favour of Disabled Persons
Willi Momm and Masaaki Iuchi
Vocational Rehabilitation and Employment Support Services
Erwin Seyfried
Disability Management at the Workplace: Overview and Future Trends
Donald E. Shrey
Rehabilitation and Noise-induced Hearing Loss
Raymond Hétu
Rights and Duties: An Employer’s Perspective
Susan Scott-Parker
Case Study: Best Practices Examples
Rights and Duties: Workers’ Perspective
Angela Traiforos and Debra A. Perry
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.







18. Education and Training (9)
18. Education and Training
Chapter Editor: Steven Hecker
Table of Contents
Figures and Tables
Introduction and Overview
Steven Hecker
Principles of Training
Gordon Atherley and Dilys Robertson
Worker Education and Training
Robin Baker and Nina Wallerstein
Case Studies
Evaluating Health and Safety Training: A Case Study in Chemical Workers Hazardous Waste Worker Education
Thomas H. McQuiston, Paula Coleman, Nina Wallerstein, A.C. Marcus, J.S. Morawetz, David W. Ortlieb and Steven Hecker
Environmental Education and Training: The State of Hazardous Materials Worker Education in the United States
Glenn Paulson, Michelle Madelien, Susan Sink and Steven Hecker
Worker Education and Environmental Improvement
Edward Cohen-Rosenthal
Safety and Health Training of Managers
John Rudge
Training of Health and Safety Professionals
Wai-On Phoon
A New Approach to Learning and Training:A Case Study by the ILO-FINNIDA African Safety and Health Project
Antero Vahapassi and Merri Weinger
Tables
Click a link below to view table in article context.
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.












19. Ethical Issues (10)
19. Ethical Issues
Chapter Editor: Georges H. Coppée
Table of Contents
Codes and Guidelines
Colin L. Soskolne
Responsible Science: Ethical Standards and Moral Behaviour in Occupational Health
Richard A. Lemen and Phillip W. Strine
Ethical Issues in Occupational Health and Safety Research
Paul W. Brandt-Rauf and Sherry I. Brandt-Rauf
Ethics in the Workplace: A Framework for Moral Judgement
Sheldon W. Samuels
Surveillance of the Working Environment
Lawrence D. Kornreich
Canons of Ethical Conduct and Interpretive Guidelines
Ethical Issues: Information and Confidentiality
Peter J. M. Westerholm
Ethics in Health Protection and Health Promotion
D. Wayne Corneil and Annalee Yassi
Case Study: Drugs and Alcohol in the Workplace - Ethical Considerations
Behrouz Shahandeh and Robert Husbands
International Code of Ethics for Occupational Health Professionals
International Commission on Occupational Health
20. Development, Technology and Trade (10)
20. Development, Technology and Trade
Chapter Editor: Jerry Jeyaratnam
Table of Contents
Figures and Tables
Occupational Health Trends in Development
Jerry Jeyaratnam
Industrialized Countries and Occupational Health and Safety
Toshiteru Okubo
Case Studies in Technological Change
Michael J. Wright
Small Enterprises and Occupational Health and Safety
Bill Glass
Transfer of Technology and Technological Choice
Joseph LaDou
Free-Trade Agreements
Howard Frumkin
Case Study: World Trade Organization
Product Stewardship and the Migration of Industrial Hazards
Barry Castleman
Economic Aspects of Occupational Health and Safety
Alan Maynard
Case Study: Industrialization and Occupational Health Problems in China
Su Zhi
Tables
Click a link below to view table in the article context.
1. Small-scale enterprises
2. Information from foreign investors
3. Costs of work accidents & health (Britain)
4. Types of economic evaluation
5. Development of China’s township enterprises
6. Country HEPS & OHS coverages in China
7. Compliance rates of 6 hazards in worksites
8. Detectable rates of occupational diseases
9. Hazardous working & employers, China
10. OHS background in foreign-funded enterprises
11. Routine instruments for OHS, 1990, China
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|



21. Labour Relations and Human Resources Management (12)
21. Labour Relations and Human Resources Management
Chapter Editor: Anne Trebilcock
Table of Contents
Figures and Tables
Labour Relations and Human Resources Management: An Overview
Anne Trebilcock
Rights of Association and Representation
Breen Creighton
Collective Bargaining and Safety and Health
Michael J. Wright
National Level Tripartite and Bipartite Cooperation on Health and Safety
Robert Husbands
Forms of Workers’ Participation
Muneto Ozaki and Anne Trebilcock
Case Study: Denmark: Worker Participation in Health and Safety
Anne Trebilcock
Consultation and Information on Health and Safety
Marco Biagi
Labour Relations Aspects of Training
Mel Doyle
Labour Relations Aspects of Labour Inspection
María Luz Vega Ruiz
Collective Disputes over Health and Safety Issues
Shauna L. Olney
Individual Disputes over Health and Safety Issues
Anne Trebilcock
Tables
Click a link below to view table in article context.
1. Practical activities-health & safety training
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|



22. Resources: Information and OSH (5)
22. Resources: Information and OSH
Chapter Editor: Jukka Takala
Table of Contents
Figures and Tables
Information: A Precondition for Action
Jukka Takala
Finding and Using Information
P.K. Abeytunga, Emmert Clevenstine, Vivian Morgan and Sheila Pantry
Information Management
Gordon Atherley
Case study: Malaysian Information Service on Pesticide Toxicity
D.A. Razak, A.A. Latiff, M.I. A. Majid and R. Awang
Case Study: A Successful Information Experience in Thailand
Chaiyuth Chavalitnitikul
Tables
Click a link below to view table in article context.
1. Some core periodicals in occupational health & safety
2. Standard search form
3. Information required in occupational health & safety
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.




23. Resources, Institutional, Structural and Legal (20)
23. Resources, Institutional, Structural and Legal
Chapter Editors: Rachael F. Taylor and Simon Pickvance
Table of Contents
Figures and Tables
Institutional, Structural and Legal Resources: Introduction
Simon Pickvance
Labour Inspection
Wolfgang von Richthofen
Civil and Criminal Liability in Relation to Occupational Safety and Health
Felice Morgenstern (adapted)
Occupational Health as a Human Right
Ilise Levy Feitshans
Community Level
Community-Based Organizations
Simon Pickvance
Right to Know: The Role of Community-Based Organizations
Carolyn Needleman
The COSH Movement and Right to Know
Joel Shufro
Regional and National Examples
Occupational Health and Safety: The European Union
Frank B. Wright
Legislation Guaranteeing Benefits for Workers in China
Su Zhi
Case Study: Exposure Standards in Russia
Nikolai F. Izmerov
International Governmental and Non-Governmental Organizations
International Cooperation in Occupational Health: The Role of International Organizations
Georges H. Coppée
The United Nations and Specialized Agencies
Contact Information for the United Nations Organization
International Labour Organization
Georg R. Kliesch
Case Study: ILO Conventions--Enforcement Procedures
Anne Trebilcock
International Organization for Standardization (ISO)
Lawrence D. Eicher
International Social Security Association (ISSA)
Dick J. Meertens
Addresses of the ISSA International Sections
International Commission on Occupational Health (ICOH)
Jerry Jeyaratnam
International Association of Labour Inspection (IALI)
David Snowball
Tables
Click a link below to view table in article context.
1. Bases for Russian vs. American standards
2. ISO technical committees for OHS
3. Venues of triennial congresses since 1906
4. ICOH committees & working groups, 1996
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|




24. Work and Workers (6)
24. Work and Workers
Chapter Editors: Jeanne Mager Stellman and Leon J. Warshaw
Table of Contents
Figures
Work and Workers
Freda L. Paltiel
Shifting Paradigms and Policies
Freda L. Paltiel
Health, Safety and Equity in the Workplace
Joan Bertin
Precarious Employment and Child Labour
Leon J. Warshaw
Transformations in Markets and Labour
Pat Armstrong
Globalizing Technologies and the Decimation/Transformation of Work
Heather Menzies
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.

25. Worker's Compensation Systems (1)
25. Worker's Compensation Systems
Chapter Editor: Terence G. Ison
Table of Contents
Overview
Terence G. Ison
Part One: Workers' Compensation
Coverage
Organization, Administration and Adjudication
Eligibility for Benefits
Multiple Causes of Disability
Subsequent Consequential Disabilities
Compensable Losses
Multiple Disabilities
Objections to Claims
Employer Misconduct
Medical Aid
Money Payments
Rehabilitation and Care
Obligations to Continue the Employment
Finance
Vicarious Liability
Health and Safety
Claims against Third Parties
Social Insurance and Social Security
Part Two: Other Systems
Accident Compensation
Sick Pay
Disability Insurance
Employers’ Liability
26. Topics in Workers' Compensation Systems (6)
26. Topics in Workers' Compensation Systems
Chapter Editors: Paule Rey and Michel Lesage
Table of Contents
Tables
Work-Related Diseases and Occupational Diseases: The ILO International List
Michel Lesage
Workers’ Compensation: Trends and Perspectives
Paule Rey
Prevention, Rehabilitation and Compensation in the German Accident Insurance System
Dieter Greiner and Andreas Kranig
Employment Injuries Insurance and Compensation in Israel
Haim Chayon
Workers’ Accident Compensation in Japan
Kazutaka Kogi and Haruko Suzuki
Country Case Study: Sweden
Peter Westerholm
Tables
Click a link below to view table in article context.
1. Proposed ILO list of occupational diseases
2. Recipients of benefits in Israel
3. Premium rates in Japan
4. Enterprises, workers & costs in Japan
5. Payment of benefits by industry in Japan
The United Nations and Specialized Agencies
* This article is adapted from Basic Facts About the United Nations (United Nations 1992).
Origin of the United Nations
The United Nations was, in 1992, an organization of 179 nations legally committed to cooperate in supporting the principles and purposes set out in its Charter. These include commitments to eradicate war, promote human rights, maintain respect for justice and international law, promote social progress and friendly relations among nations, and use the Organization as a centre to harmonize their actions in order to attain these ends.
The United Nations Charter was written in the closing days of the Second World War by the representatives of 50 governments meeting at the United Nations Conference on International Organization in 1945. The Charter was drafted on the basis of proposals worked out by the representatives of China, France, the Soviet Union, the United Kingdom and the United States. It was adopted and signed on 26 June 1945.
To millions of refugees from war and persecution, the United Nations has provided shelter and relief. It has acted as a major catalyst in the evolution of 100 million people from colonial rule to independence and sovereignty. It has established peace-keeping operations many times to contain hostilities and to help resolve conflicts. It has expanded and codified international law. It has wiped smallpox from the face of the planet. In the five decades of its existence, the Organization has adopted some 70 legal instruments promoting or obligating respect for human rights, thus facilitating an historic change in the popular expectation of freedom throughout the world.
Membership
The Charter declares that membership of the UN is open to all peace-loving nations which accept its obligations and which, in the judgement of the Organization, are willing and able to carry out these obligations. States are admitted to membership by the General Assembly on the recommendation of the Security Council. The Charter also provides for the suspension or expulsion of Members for violation of the principles of the Charter, but no such action has ever been taken.
Official Languages
Under the Charter the official languages of the United Nations are Chinese, English, French, Russian and Spanish. Arabic has been added as an official language of the General Assembly, the Security Council and the Economic and Social Council.
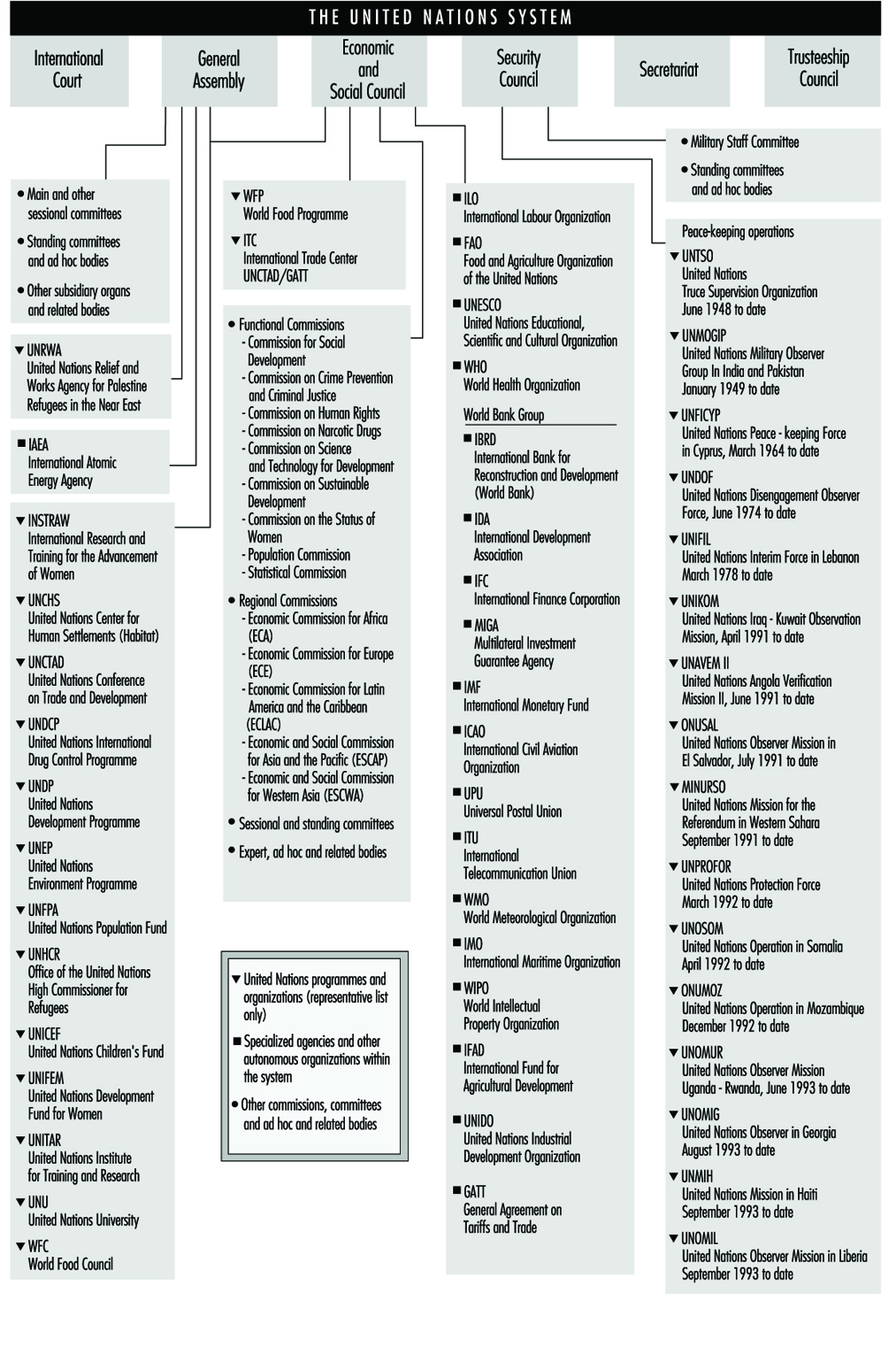
Structure
The United Nations is a complex network consisting of six main organs with a large number of related programmes, agencies, commissions and other bodies. These related bodies have different legal status (some are autonomous, some are under the direct authority of the UN and so on), objectives and areas of responsibility, but the system displays a very high level of cooperation and collaboration. Figure 1 provides a schematic illustration of the structure of the system and some of the links between the different bodies. For further information, reference should be made to: Basic Facts About the United Nations (1992).
Figure 1. The Charter established six principal organs of the United Nations
International Court of Justice
The International Court of Justice is the principal judicial organ of the UN. The Court is open to the parties to its Statute, which automatically includes all Members of the UN. Other States can refer cases to the Court under conditions laid down by the Security Council. In addition, the Security Council may recommend that a legal dispute be referred to the Court. Only States may be party to cases before the Court (i.e., the Court is not open to individuals). Both the General Assembly and the Security Council can ask the Court for an advisory opinion on any legal question; other organs of the UN and the specialized agencies, when authorized by the General Assembly, can ask for advisory opinions on legal questions within the scope of their activities (for example, the International Labour Organization could request an advisory opinion relating to an international labour standard).
The jurisdiction of the Court covers all matters provided for in the UN Charter or in treaties or conventions in force, and all other questions which States refer to it. In deciding cases, the Court is not restricted to principles of law contained in treaties or conventions, but may employ the entire sphere of international law (including customary law).
The General Assembly
The General Assembly is the main deliberative organ. It is composed of representatives of all Member States, each of which has one vote. Decisions on important questions, such as those on peace and security, admission of new Members and budgetary matters, require a two-thirds majority. Decisions on other questions are reached by a simple majority.
The functions and powers of the General Assembly include the consideration of and formulation of recommendations on the principles of cooperation in the maintenance of international peace and security, including disarmament and the regulation of armaments. The General Assembly also initiates studies and makes recommendations to promote international political cooperation, the development and codification of international law, the realization of human rights and fundamental freedoms for all, and international collaboration in the economic, social, cultural, educational and health fields. It receives and deliberates on reports from the Security Council and other UN organs; considers and approves the UN budget and apportions the contributions among Members; and elects the non-permanent members of the Security Council, the members of the Economic and Social Council and those members of the Trusteeship Council that are elected. The General Assembly also elects jointly with the Security Council the Judges of the International Court of Justice and, on the recommendation of the Security Council, appoints the Secretary-General.
At the beginning of each regular session, the General Assembly holds a general debate, in which Member States express their views on a wide range of matters of international concern. Because of the great number of questions which the General Assembly is called upon to consider (over 150 agenda items at the 1992 session, for example), the Assembly allocates most questions to its seven main committees:
- First Committee (disarmament and related international security matters)
- Special Political Committee
- Second Committee (economic and financial matters)
- Third Committee (social, humanitarian and cultural matters)
- Fourth Committee (decolonization matters)
- Fifth Committee (administrative and budgetary matters)
- Sixth Committee (legal matters).
Economic and Social Council (ECOSOC)
ECOSOC was established by the Charter as the principal organ to coordinate the economic and social work of the UN and the specialized agencies and institutions. The Economic and Social Council serves as the central forum for the discussion of international economic and social issues of a global or inter-disciplinary nature and the formulation of policy recommendations on those issues, and works to promote respect for, and observance of, human rights and fundamental freedoms for all. ECOSOC may make or initiate studies and reports and recommendations on international economic, social, cultural, educational, health and related matters, and call international conferences and prepare draft conventions for submission to the General Assembly. Other powers and functions include the negotiation of agreements with the specialized agencies defining their relationship with the UN and the coordination of their activities, and consultation with NGOs concerned with matters with which the Council deals.
Subsidiary bodies
The subsidiary machinery of the Council includes functional and regional commissions, six standing committees (for example, the Committee on Non-Governmental Organizations and on Transnational Corporations) and a number of standing expert bodies on such subjects as crime prevention and control, development planning, and the transport of dangerous goods.
Relations with non-governmental organizations
Over 900 NGOs have consultative status with the Council, with varying levels of involvement. These NGOs may send observers to public meetings of the Council and its subsidiary bodies and may submit written statements relevant to the Council’s work. They may also consult with the UN Secretariat on matters of mutual concern.
Security Council
The Security Council has primary responsibility, under the Charter, for the maintenance of international peace and security. While other organs of the UN make recommendations to governments, the Council alone has the power to take decisions which Member States are obligated under the Charter to carry out.
Secretariat
The Secretariat, an international staff working at UN Headquarters in New York and in the field, carries out the diverse day-to-day work of the Organization. It services the other organs of the UN and administers the programmes and policies laid down by them. At its head is the Secretary-General, who is appointed by the General Assembly on the recommendation of the Security Council for a term of five years.
Trusteeship Council
In setting up an International Trusteeship System, the Charter established the Trusteeship Council as one of the main organs of the UN and assigned to it the task of supervising the administration of Trust Territories placed under the Trusteeship System. Major goals of the System are to promote the advancement of the inhabitants of Trust Territories and their progressive development towards self-government or independence.
The Role of the United Nations System in Occupational Health and Safety
While the improvement of working conditions and environment will normally be part of national policy to further economic development and social progress in accordance with national objectives and priorities, a measure of international harmonization is necessary to ensure that the quality of the working environment everywhere is compatible with workers’ health and welfare, and to assist Member States to this effect. This is, essentially, the role of the UN system in this field.
Within the UN system, many organizations and bodies play a role in the improvement of the working conditions and the working environment. The International Labour Organization (ILO) has a constitutional mandate to improve working conditions and environment to humanize work; its tripartite structure can ensure that its international standards have a direct impact on national legislation, policies and practices and is discussed in a separate article in this chapter.
The World Health Organization (WHO) has a mandate in occupational health derived from its Constitution, which identified WHO as “the directing and coordinating authority on international health work”, and stated WHO’s functions which include the “promotion of ...economic and working conditions and other aspects of environmental hygiene”. Additional mandates are derived from various resolutions of the World Health Assembly and Executive Board. WHO’s occupational health programme aims to promote the knowledge and control of workers’ health problems, including occupational and work-related diseases, and to cooperate with countries in the development of health care programmes for workers, particularly those who are generally underserviced. The WHO, in collaboration with the ILO, UNEP and other organizations, undertakes technical cooperation with Member States, produces guidelines, and carries out field studies and occupational health training and personnel development. The WHO has set up the GEENET—the Global Environmental Epidemiology Network—which includes institutions and individuals from all over the world who are actively involved in research and training on environmental and occupational epidemiology. The International Agency for Research on Cancer (IARC) has been established as an independent research institute, but within the framework of the WHO. The statutes of the Agency set out its mission as “planning, promoting and developing research in all phases of the causation, treatment and prevention of cancer”. Since the start of its research activity, the Agency has devoted itself to studying the causes of cancer present in the human environment, in the belief that identification of a carcinogenic agent was the first and necessary step towards reducing or removing the causal agent from the environment, with the aim of preventing cancer that it might have caused. The Agency’s research activities fall into two main groups—epidemiological and laboratory-based experimental but there is considerable interaction between these groups in the actual research projects undertaken.
Besides these two organizations with a central focus on work and health, respectively, several UN bodies include health and safety matters within their specific sectoral or geographical functions:
The United Nations Environment Programme (UNEP) has the mandate to safeguard and enhance the environment for the benefit of present and future generations, including the working environment. It has a basic coordinating and catalytic function for environment in general within the UN system. It discharges this function through programme coordination and the support of activities by the Environment Fund. In addition to its general mandate, UNEP’s specific mandate with regard to the working environment stems from Recommendations 81 and 83 of the UN Conference on the Human Environment, and UNEP Governing Council Decisions requesting the Executive Director to integrate the principles and objectives related to the improvement of the working environment fully into the framework of the environment programme. UNEP is also required to collaborate with the appropriate organizations of workers and employers, in the development of a coordinated system-wide action programme on the working and living environment of workers, and with the UN bodies concerned (for example, UNEP cooperates with the WHO and the ILO in the International Programme on Chemical Safety).
UNEP maintains the International Register of Potentially Toxic Chemicals (IRPTC), which strives to bridge the gap between the world’s chemical knowledge and those who need to use it. UNEP’s network of environmental agreements is also having an ever-increasing international effect, and gathering momentum (for example, the historic Vienna Convention and the Montreal Protocol on the protection of the ozone layer).
The International Atomic Energy Agency (IAEA) is concerned with hazards resulting from ionizing radiation associated with the nuclear fuel cycle. The IAEA encourages and guides the development of peaceful uses of atomic energy, establishes standards for nuclear safety and environmental protection, aids member countries through technical cooperation, and fosters the exchange of scientific and technical information on nuclear energy. The activities of the Agency in the area of radiological protection of workers involve the development of these standards; preparation of safety guides, codes of practice and manuals; holding of scientific meetings for exchange of information or preparation of manuals or technical guidebooks; organizing training courses, visiting seminars and study tours; development of technical expertise in developing Member States through the awards of research contracts and fellowships; and helping the developing Member States in the organization of radiation protection programmes through the provision of technical assistance, experts’ services, advisory missions, and advisory services on nuclear law regulatory matters.
The United Nations Development Programme (UNDP) and the World Bank have included provisions on occupational safeguards in development assistance agreements. The UNDP is engaged in a large number of projects designed to assist developing countries to build up their nascent economies and raise their living standards. Several thousand internationally recruited experts are kept steadily at work in the field. Several amongst these projects are devoted to the improvement of occupational safety and health standards in industry and other walks of economic life, the implementation of which is entrusted to the ILO and WHO. Such field projects may range from the provision of short-term consultancy to more massive assistance over a period of several years for the establishment of fully fledged occupational safety and health institutes designed to provide training, applied field research and direct service to places of employment.
The International Maritime Organization (IMO) deals with the safety of workers on board ships. IMO provides a forum for member governments and interested organizations to exchange information and endeavour to solve problems connected with technical, legal and other questions concerning shipping and the prevention of marine pollution by ships. IMO has drafted a number of conventions and recommendations which governments have adopted and which have entered into force. Among them are international conventions for the safety of life at sea, the prevention of marine pollution by ships, the training and certification of seafarers, the prevention of collisions at sea, several instruments dealing with liability and compensation, and many others. IMO has also adopted several hundred recommendations dealing with subjects such as the maritime transport of dangerous goods, maritime signals, safety for fishermen and fishing vessels, and the safety of nuclear merchant ships.
The Food and Agriculture Organization of the United Nations (FAO) has a role in protecting agricultural workers against hazards resulting from the use of pesticides, farm tools and machinery. A number of activities of FAO are directly or indirectly concerned with occupational safety and health and ergonomics in agricultural, forestry and fishery work. In fishery activities, FAO collaborates at the secretariat level with the ILO and the IMO on the IMO Sub-Committee on Safety of Fishing Vessels and participates actively in the work of the IMO Sub-Committee on Standards of Training and Watchkeeping. FAO collaborates with ILO in regard to conditions of work in the fishing industry. In forestry activities, the FAO/ECE/ILO Committee on Forest Working Techniques and Training of Forest Workers deals at the interagency level with health and safety matters. Field projects and publications in this area cover such aspects as safety in logging and industry and heat stress in forest work.
In the agricultural field some of the diseases of economic importance in livestock also present hazards to persons handling livestock and animal products (e.g., brucellosis, tuberculosis, leptospirosis, anthrax, rabies, Rift Valley fever). For these disease-related activities, close liaison is maintained with WHO through joint committees. FAO is also concerned with the harmonization of registration requirements for pesticides and the assessment of pesticide residues in food and in the environment. As regards atomic energy in food and agriculture, programmes are coordinated with the IAEA in order to assist scientists of developing countries to make safe and effective use of relevant isotope techniques (e.g., the use of radio-labelled enzyme substrates for detecting occupational exposure to insecticides).
The UN Industrial Development Organization (UNIDO) aims to accelerate the industrial development of developing countries. It is concerned with occupational safety and health hazards, environment and hazardous waste management in relation to the industrialization process.
Regional UN Economic Commissions play a role in promoting more effective and harmonized action within their regions.
The UN Conference on Trade and Development (UNCTAD) is concerned with the occupational aspects of the international transfer of goods, services and technology.
Ethical Issues in Occupational Health and Safety Research
In the last several decades, considerable effort has been devoted to defining and addressing the ethical issues that arise in the context of biomedical experimentation. Central ethical concerns that have been identified in such research include the relationship of risks to benefits and the ability of research subjects to give informed and voluntary prior consent. Assurance of adequate attention to these issues has normally been achieved by review of research protocols by an independent body, such as an Institutional Review Board (IRB). For example, in the United States, institutions engaging in biomedical research and receiving Public Health Service research funds are subject to strict federal governmental guidelines for such research, including review of protocols by an IRB, which considers the risks and benefits involved and the obtaining of informed consent of research subjects. To a large degree, this is a model which has come to be applied to scientific research on human subjects in democratic societies around the world (Brieger et al. 1978).
Although the shortcomings of such an approach have been debated—for example, in a recent Human Research Report, Maloney (1994) says some institutional review boards are not doing well on informed consent—it has many supporters when it is applied to formal research protocols involving human subjects. The deficiencies of the approach appear, however, in situations where formal protocols are lacking or where studies bear a superficial resemblance to human experimentation but do not clearly fall within the confines of academic research at all. The workplace provides one clear example of such a situation. Certainly, there have been formal research protocols involving workers that satisfy the requirements of risk-benefit review and informed consent. However, where the boundaries of formal research blur into less formal observances concerning workers’ health and into the day-to-day conduct of business, ethical concerns over risk-benefit analysis and the assurance of informed consent may be easily put aside.
As one example, consider the Dan River Company “study” of cotton dust exposure to its workers at its Danville, Virginia, plant. When the US Occupational Safety and Health Administration’s (OSHA) cotton dust standard went into effect following US Supreme Court review in 1981, the Dan River Company sought a variance from compliance with the standard from the state of Virginia so that it could conduct a study. The purpose of the study was to address the hypothesis that byssinosis is caused by micro-organisms contaminating the cotton rather than by the cotton dust itself. Thus, 200 workers at the Danville plant were to be exposed to varying levels of the micro-organism while being exposed to cotton dust at levels above the standard. The Dan River Company applied to OSHA for funding for the project (technically considered a variance from the standard, and not human research), but the project was never formally reviewed for ethical concerns because OSHA does not have an IRB. Technical review by an OSHA toxicologist cast serious doubt on the scientific merit of the project, which in and of itself should raise ethical questions, since incurring any risk in a flawed study might be unacceptable. However, even if the study had been technically sound, it is unlikely to have been approved by any IRB since it “violated all the major criteria for protection of subject welfare” (Levine 1984). Plainly, there were risks to the worker-subjects without any benefits for them individually; major financial benefits would have gone to the company, while benefits to society in general seemed vague and doubtful. Thus, the concept of balancing risks and benefits was violated. The workers’ local union was informed of the intended study and did not protest, which could be construed to represent tacit consent. However, even if there was consent, it might not have been entirely voluntary because of the unequal and essentially coercive relationship between the employer and the employees. Since Dan River Company was one of the most important employers in the area, the union’s representative admitted that the lack of protest was motivated by fear of a plant closing and job losses. Thus, the concept of voluntary informed consent was also violated.
Fortunately, in the Dan River case, the proposed study was dropped. However, the questions it raises remain and extend far beyond the bounds of formal research. How can we balance benefits and risks as we learn more about threats to workers’ health? How can we guarantee informed and voluntary consent in this context? To the extent that the ordinary workplace may represent an informal, uncontrolled human experiment, how do these ethical concerns apply? It has been suggested repeatedly that workers may be the “miner’s canary” for the rest of society. On an ordinary day in certain workplaces, they may be exposed to potentially toxic substances. Only when adverse reactions are noted does society initiate a formal investigation of the substance’s toxicity. In this way, workers serve as “experimental subjects” testing chemicals previously untried on humans.
Some commentators have suggested that the economic structure of employment already addresses risk/benefit and consent considerations. As to the balancing of risks and benefits, one could argue that society compensates hazardous work with “hazard pay”—directly increasing the benefits to those who assume the risk. Furthermore, to the extent that the risks are known, right-to-know mechanisms provide the worker with the information necessary for an informed consent. Finally, armed with the knowledge of the benefits to be expected and the risks assumed, the worker may “volunteer” to take the risk or not. However, “volunteer-ness” requires more than information and an ability to articulate the word no. It also requires freedom from coercion or undue influence. Indeed, an IRB would view a study in which the subjects received significant financial compensation—“hazard pay”, as it were—with a sceptical eye. The concern would be that powerful incentives minimize the possibility for truly free consent. As in the Dan River case, and as noted by the US Office of Technology Assessment,
(t)his may be especially problematic in an occupational setting where workers may perceive their job security or potential for promotion to be affected by their willingness to participate in research (Office of Technology Assessment 1983).
If so, cannot the worker simply choose a less hazardous occupation? Indeed, it has been suggested that the hallmark of a democratic society is the right of the individual to choose his or her work. As others have pointed out, however, such free choice may be a convenient fiction since all societies, democratic or otherwise,
have mechanisms of social engineering that accomplish the task of finding workers to take available jobs. Totalitarian societies accomplish this through force; democratic societies through a hegemonic process called freedom of choice (Graebner 1984).
Thus, it seems doubtful that many workplace situations would satisfy the close scrutiny required of an IRB. Since our society has apparently decided that those fostering our biomedical progress as human research subjects deserve a high level of ethical scrutiny and protection, serious consideration should be given before denying this level of protection to those who foster our economic progress: the workers.
It has also been argued that, given the status of the workplace as a potentially uncontrolled human experiment, all involved parties, and workers in particular, should be committed to the systematic study of the problems in the interest of amelioration. Is there a duty to produce new information concerning occupational hazards through formal and informal research? Certainly, without such research, the workers’ right to be informed is hollow. The assertion that workers have an active duty to allow themselves to be exposed is more problematic because of its apparent violation of the ethical tenet that people should not be used as a means in the pursuit of benefits to others. For example, except in very low risk cases, an IRB may not consider benefits to others when it evaluates risk to subjects. However, a moral obligation for workers’ participation in research has been derived from the demands of reciprocity, i.e., the benefits that may accrue to all affected workers. Thus, it has been suggested that “it will be necessary to create a research environment within which workers—out of a sense of the reciprocal obligations they have—will voluntarily act upon the moral obligation to collaborate in work, the goal of which is to reduce the toll of morbidity and mortality” (Murray and Bayer 1984).
Whether or not one accepts the notion that workers should want to participate, the creation of such an appropriate research environment in the occupational health setting requires careful attention to the other possible concerns of the worker-subjects. One major concern has been the potential misuse of data to the detriment of the workers individually, perhaps through discrimination in employability or insurability. Thus, due respect for the autonomy, equity and privacy considerations of worker-subjects mandates the utmost concern for the confidentiality of research data. A second concern involves the extent to which the worker-subjects are informed of research results. Under normal experimental situations, results would be available routinely to subjects. However, many occupational studies are epidemiological, e.g., retrospective cohort studies, which traditionally have required no informed consent or notification of results. Yet, if the potential for effective interventions exists, the notification of workers at high risk of disease from past occupational exposures could be important for prevention. If no such potential exists, should workers still be notified of findings? Should they be notified if there are no known clinical implications? The necessity for and logistics of notification and follow-up remain important, unresolved questions in occupational health research (Fayerweather, Higginson and Beauchamp 1991).
Given the complexity of all of these ethical considerations, the role of the occupational health professional in workplace research assumes great importance. The occupational physician enters the workplace with all of the obligations of any health care professional, as state by the International Commission on Occupational Health and reprinted in this chapter:
Occupational health professionals must serve the health and social well-being of the workers, individually and collectively. The obligations of occupational health professionals include protecting the life and the health of workers, respecting human dignity and promoting the highest ethical principles in occupational health policies and programmes.
In addition, the participation of the occupational physician in research has been viewed as a moral obligation. For example, the American College of Occupational and Environmental Medicine’s Code of Ethical Conduct specifically states that “(p)hysicians should participate in ethical research efforts as appropriate” (1994). However, as with other health professionals, the workplace physician functions as a “double agent”, with the potentially conflicting responsibilities that stem from caring for the workers while being employed by the corporation. This type of “double agent” problem is not unfamiliar to the occupational health professional, whose practice often involves divided loyalties, duties and responsibilities to workers, employers and other parties. However, the occupational health professional must be particularly sensitive to these potential conflicts because, as discussed above, there is no formal independent review mechanism or IRB to protect the subjects of workplace exposures. Thus, in large part it will fall to the occupational health professional to ensure that the ethical concerns of risk-benefit balancing and voluntary informed consent, among others, are given appropriate attention.
International Labour Organization
The ILO is one of 18 specialized agencies of the United Nations. It is the oldest international organization within the UN family, and was founded by the Versailles Peace Conference in 1919 after the First World War.
Foundation of the ILO
Historically, the ILO is the outgrowth of the social thought of the 19th century. Conditions of workers in the wake of the industrial revolution were increasingly seen to be intolerable by economists and sociologists. Social reformers believed that any country or industry introducing measures to improve working conditions would raise the cost of labour, putting it at an economic disadvantage compared to other countries or industries. That is why they laboured with such persistence to persuade the powers of Europe to make better working conditions and shorter hours of work the subject of international agreements. After 1890 three international conferences were held on the subject: the first was convened jointly by the German emperor and the Pope in Berlin in 1890; another conference held in 1897 in Brussels was stimulated by the Belgian authorities; and a third, held in 1906 in Bern, Switzerland, adopted for the first time two international agreements on the use of white phosphorus (manufacturing of matches) and on the ban of night work in industry by women. As the First World War had prevented any further activities on the internationalization of labour conditions, the Peace Conference of Versailles, in its intention to eradicate the causes of future war, took up the goals of the pre-war activities and established a Commission on International Labour Legislation. The elaborated proposal of the Commission on the establishment of an international body for the protection of workers became Part XIII of the Treaty of Versailles; to this day, it remains the charter under which the ILO operates.
The first International Labour Conference was held in Washington DC, in October 1919; the Permanent Secretariat of the Organization—the International Labour Office—was installed in Geneva, Switzerland.
The Constitution of the International Labour Organization
Permanent peace worldwide, justice and humanity were and are the motivations for the International Labour Organization, best expressed in the Preamble to the Constitution. It reads:
Whereas universal and lasting peace can be established only if it is based upon social justice;
And whereas conditions of labour exist involving such injustice, hardship and privation to large numbers of people as to produce unrest so great that the peace and harmony of the world are imperilled; and an improvement of those conditions is urgently required, as for example, by
- the regulation of the hours of work, including establishment of a maximum working day and week,
- the regulation of the labour supply,
- the prevention of unemployment,
- the provision of an adequate living wage,
- the protection of the worker against sickness, disease and injury arising out of his employment,
- the protection of children, young persons and women,
- the provision for old age and injury,
- the protection of the interests of workers when employed in countries other than their own,
- the recognition of the principle of equal remuneration for work of equal value,
- the recognition of the principle of freedom of association,
- the organization of vocational and technical education and other measures;
Whereas also the failure of any nation to adopt humane conditions of labour is an obstacle in the way of other nations which desire to improve the conditions in their own countries;
The High Contracting Parties, moved by sentiments of justice and humanity as well as by the desire to secure the permanent peace of the world, and with a view to attaining the objectives set forth in this Preamble, agree to the following Constitution of the International Labour Organisation. …”
The aims and purposes of the International Labour Organization in a modernized form are embodied in the Philadelphia Declaration, adopted in 1944 at the International Labour Conference in Philadelphia, USA. The Declaration is now an Annex to the Constitution of the ILO. It proclaims the right of all human beings “to pursue both their material well being and their spiritual development in conditions of freedom and dignity, of economic security and equal opportunity”. It further states that “poverty anywhere constitutes a danger to prosperity everywhere”.
The task of the ILO as determined in Article 1 of the Constitution is the promotion of the objects set forth in the Preamble and in the Philadelphia Declaration.
The International Labour Organization and its Structure
The International Labour Organization (ILO) is composed of 173 States. Any member of the United Nations may become a member of the ILO by communicating to the Director-General of the ILO its formal acceptance of the obligations of the Constitution. Non-Member States of the UN may be admitted by a vote of the International Labour Conference (Switzerland is a member of the ILO but not, however, of the UN) (Constitution, Article 1). Representation of Member States at the ILO has a structure which is unique within the UN family. In the UN and in all other specialized UN agencies, representation is only by government personnel: ministers, their deputies, or authorized representatives. However, at the ILO the concerned groups of society are part of the Member States’ representation. Representatives consist of government delegates, generally from the ministry of labour, and delegates representing the employers and the workers of each of the members (Constitution, Article 3). This is the ILO’s fundamental concept of tripartism.
The International Labour Organization consists of:
- the International Labour Conference, an annual Conference of representatives of all members
- the Governing Body, composed of 28 government representatives, 14 employers’ representatives, and 14 workers’ representatives
- the International Labour Office—the permanent secretariat of the organization—which is controlled by the Governing Body.
The International Labour Conference—also called the World Parliament of Labour—meets regularly in June each year with about 2,000 participants, delegates and advisers. The agenda of the Conference includes the discussion and adoption of international agreements (the ILO’s Conventions and Recommendations), the deliberation of special labour themes in order to frame future policies, the adoption of Resolutions directed towards action in Member States and instructions to the Director-General of the Organization on action by the Office, a general discussion and exchange of information and, every second year, the adoption of a biennial programme and budget for the International Labour Office.
The Governing Body is the link between the International Labour Conference of all Member States and the International Labour Office. In three meetings per year, the Governing Body executes its control over the Office by screening work progress, formulating instructions to the Director-General of the Office, adopting the output of Office activity such as Codes of Practice, monitoring and guiding financial affairs, and preparing the agendas for future International Labour Conferences. Membership of the Governing Body is subject to election for a three-year term by the three groups of Conference Representatives—governments, employers and workers. Ten government members of the Governing Body are permanent members as representatives of States of major industrial importance.
Tripartism
All the decision-making mechanisms of the ILO follow a unique structure. All decisions of Member representation are taken by the three groups of representatives, namely by the government representatives, the employers’ representatives and the workers’ representatives of each Member State. Decisions on the substance of work in the Conference Committees on International Conventions and Recommendations, in the Meeting of Experts on Codes of Practice, and in the Advisory Committees on conclusions regarding future labour conditions, are taken by members of the Committees, of which one-third represent governments, one-third represent employers and one-third represent workers. All political, financial and structural decisions are taken by the International Labour Conference (ILC) or the Governing Body, in which 50% of the voting power lies with government representatives (two per Member State in the Conference), 25% with employers’ representatives, and 25% with workers’ representatives (one for each group of a Member State in the Conference). Financial contributions to the Organization are paid solely by the governments, not by the two non-governmental groups; for this reason only governments comprise the Finance Committee.
The Conventions
The International Labour Conference has from 1919 to 1995 adopted 176 Conventions and 183 Recommendations.
Some 74 of the Conventions deal with working conditions, of which 47 are on general conditions of work and 27 are on safety and health in a narrow sense.
The subjects of the Conventions on general conditions of work are: hours of work; minimum age for admission to employment (child labour); night work; medical examination of workers; maternity protection; family responsibilities and work; and part time work. In addition, also relevant to health and safety are ILO Conventions aimed at eliminating discrimination against workers on various grounds (e.g., race, sex, disability), protecting them from unfair dismissal, and compensating them in case of occupational injury or disease.
Of the 27 Conventions on safety and health, 18 were adopted after 1960 (when decolonization led to a large increase in ILO membership) and only nine from 1919 to 1959. The most ratified Convention in this group is the Labour Inspection Convention, 1947 (No. 81), which has been ratified by more than 100 Member States of the ILO (its corollary for agriculture has been ratified by 33 countries).
High numbers of ratification can be one indicator of commitment to improving working conditions. For instance Finland, Norway and Sweden, which are famous for their safety and health record and which are the world’s showcase of safety and health practice, have ratified almost all Conventions in this field adopted after 1960.
The Labour Inspection Conventions are complemented by two further basic standards, the Occupational Safety and Health Convention, 1981 (No. 155) and the Occupational Health Services Convention, 1985 (No. 161).
The Occupational Safety and Health Convention establishes the framework for a national conception of safety and health constituting a model of what the safety and health law of a country should contain. The framework directive of the EU on safety and health follows the structure and contents of the ILO Convention. The EU directive has to be transposed into national legislation by all 15 members of the EU.
The Occupational Health Services Convention deals with the operational structure within enterprises for the implementation of safety and health legislation in companies.
Several Conventions have been adopted regarding branches of economic activity or hazardous substances. These include the Safety and Health in Mines Convention, 1995 (No. 176); the Safety and Health in Construction Convention, 1988 (No. 167); the Occupational Safety and Health (Dock Work) Convention, 1979 (No. 152); the White Lead (Painting) Convention, 1921 (No. 13); the Benzene Convention, 1971 (No. 136); the Asbestos Convention, 1986 (No. 162); the Chemicals Convention, 1990 (No. 170); and the Prevention of Major Industrial Accidents Convention, 1993 (No. 174).
Associated with these norms are: the Working Environment Convention, 1977 (No. 148) (Protection of Workers against occupational Hazards in the Working Environment due to Air Pollution, Noise and Vibration); the Occupational Cancer Convention, 1974 (No. 139); and the list of occupational diseases that is part of the Employment Injury Benefits Convention, 1964 (No. 121). The last revision of the list was adopted by the Conference in 1980 and is discussed in the Chapter Workers’ Compensation, Topics in.
Other safety and health Conventions are: the Marking of Weight Convention, 1929 (No. 27); the Maximum Weight Convention, 1967 (No. 127); the Radiation Protection Convention, 1960 (No. 115); the Guarding of Machinery Convention, 1963 (No. 119); and the Hygiene (Commerce and Offices) Convention, 1964 (No. 120).
During the early period of the ILO, Recommendations were adopted instead of Conventions, such as on anthrax prevention, white phosphorus and lead poisoning. However in recent times Recommendations have tended to complement a Convention by specifying details on implementing its provisions.
Contents of Conventions on Safety and Health
Structure and content of safety and health Conventions follow a general pattern:
- scope and definitions
- obligations of governments
- consultation with organizations of workers and employers
- obligations of employers
- duties of workers
- rights of workers
- inspections
- penalties
- final provisions (on conditions for entry into force, registrations of ratifications and denunciation).
A Convention prescribes the task of government or government authorities in regulating the subject matter, highlights obligations of owners of enterprises, specifies the role of workers and their organizations through duties and rights, and closes with provisions for inspection and action against violation of the law. The Convention must of course determine its scope of application, including possible exemptions and exclusions.
Design of Conventions concerning safetyand health at work
The Preamble
Each Convention is headed by a preamble referring to the dates and the item on the agenda of the International Labour Conference; other Conventions and documents related to the topic, concerns about the subject justifying the action; underlying causes; cooperation with other international organizations such as WHO and UNEP; the form of the international instrument as a Convention or Recommendation, and the date of the adoption and citation of the Convention.
Scope
Wording of the scope is governed by flexibility towards implementation of a Convention. The guiding principle is that the Convention applies to all workers and branches of economic activity. However, in order to facilitate ratification of the Convention by all Member States, the guiding principle is often supplemented by the possibility of partial or total non-application in various fields of activity. A Member State may exclude particular branches of economic activity or particular undertakings in respect of which special problems of a substantial nature arise from the application of certain provisions or of the Convention as a whole. The scope may also foresee step by step implementation of provisions to take into account existing conditions in a country. These exclusions reflect also the availability of national resources for the implementation of new national legislation on safety and health. General conditions of exclusion are that a safe and healthy working environment is otherwise attached by alternative means and that any decision on exclusion is subject to consultation with employers and workers. The scope also includes definitions of terms used in the wording of the international instrument such as branches of economic activity, workers, workplace, employer, regulation, workers’ representative, health, hazardous chemical, major hazard installation, safety report and so forth.
Obligations of governments
Conventions on safety and health establish as a first module the task for a government to elaborate, implement and review a national policy relating to the contents of the Convention. Organizations of employers and workers must be involved in the establishment of the policy and the specification of aims and objectives. The second module concerns the enactment of laws or regulations giving effect to the provisions of the Convention and the enforcement of the law, including the employment of qualified personnel and the provision of support for the staff for inspection and advisory services. Under Articles 19 and 22 of the ILO Constitution, governments are also obliged to report regularly or on request to the International Labour Office on the practice of implementation of the Convention and Recommendation. These obligations are the basis for ILO supervisory procedures.
Consultations with organizations of employers and workers
The importance of involvement of those who are directly associated with the implementation of regulations and the consequences of accidents is undoubted. Successful safety and health practice is based on collaboration and on incorporation of opinion and good will of the persons concerned. A Convention therefore provides that the government authorities must consult employers and workers when considering the exclusion of installations from legislation for step-by-step implementation of provisions and in the development of a national policy on the subject matter of the Convention.
Obligations of employers
The responsibility for the execution of legal requirements within an enterprise lies on the owner of an enterprise or his or her representative. Legal rights on workers’ participation in the decision-making process do not alter the primary responsibility of the employer. The obligations of employers as stated in Conventions include provision of safe and healthy working procedures; the purchase of safe machinery and equipment; the use of non-hazardous substances in work processes; the monitoring and assessment of airborne chemicals at the workplace; the provision of health surveillance of workers and of first aid; the reporting of accidents and diseases to the competent authority; the training of workers; the provision of information regarding hazards related to work and their prevention; cooperation in discharging their responsibilities with workers and their representatives.
Duties of workers
Since the 1980s, Conventions have stated that workers have a duty to cooperate with their employers in the application of safety and health measures and to comply with all procedures and practices relating to safety and health at work. The duty of workers may include the reporting to supervisors of any situation which could present a special risk, or the fact that a worker has removed himself/herself from the workplace in case of imminent and serious danger to his or her life or health.
Rights of workers
A variety of special rights of workers has been stated in ILO Conventions on safety and health. In general a worker is afforded the right to information on hazardous working conditions, on the identity of chemicals used at work and on chemical safety data sheets; the right to be trained in safe working practices; the right to consultation by the employer on all aspects of safety and health associated with the work; and the right to undergo medical surveillance free of charge and with no loss of earnings. Some of these Conventions also recognize the rights of workers’ representatives, particularly regarding consultation and information. These rights are reinforced by other ILO Conventions on freedom of association, collective bargaining, workers’ representatives and protection against dismissal.
Specific articles in Conventions adopted in 1981 and later deal with the worker’s right to remove himself/herself from danger at his or her workplace. A 1993 Convention (Prevention of Major Industrial Accidents, 1993 (No. 174)) recognized the worker’s right to notify the competent authority of potential hazards which may be capable of generating a major accident.
Inspection
Conventions on safety and health express the needs for the government to provide appropriate inspection services to supervise the application of the measures taken to implement the Convention. The inspection requirement is supplemented by the obligation to provide the inspection services with the resources necessary for the accomplishment of their task.
Penalties
Conventions on safety and health often call for national regulation regarding the imposition of penalties in case of non-compliance with legal obligations. Article 9 (2) of the framework Occupational Safety and Health Convention, 1981 (No 155) states: “The enforcement system shall provide for adequate penalties for violations of the laws and regulations.” These penalties may be administrative, civil or criminal in nature.
The Labour Inspection Convention, 1947 (No. 81)
The Labour Inspection Convention of 1947 (No. 81) calls on States to maintain a system of labour inspection in industrial workplaces. It fixes government obligations in regard to inspection and sets out rights, duties and powers of inspectors. This instrument is complemented by two Recommendations (Nos. 81 and 82) and by the Protocol of 1995, which extends its scope of application to the non-commercial services sector (such as the public service and state-run enterprises). The Labour Inspection (Agriculture) Convention, 1969 (No. 129), contains provisions very similar to Convention No. 81 for the agricultural sector. ILO Maritime Conventions and Recommendations also address inspection of seafarers’ working and living conditions.
The government has to establish an independent qualified corps of inspectors in sufficient number. The inspectorate must be fully equipped to provide good services. Legal provision of penalties for violation of safety and health regulations are an obligation of the government. Inspectors have the duty to enforce legal requirements, and to provide technical information and advice to employers and workers regarding effective means of complying with legal provisions.
Inspectors are to report gaps in regulations to authorities and submit annual reports on their work. Governments are called on to compile annual reports giving statistics on inspections done.
Rights and powers of inspectors are laid down, such as the right to enter workplaces and premises, to carry out examinations and tests, to initiate remedial measures, to issue orders on alteration of the installation and immediate execution. They have also the right to issue citations and institute legal proceedings in case of a violation of an employer’s duties.
The Convention contains provisions on the conduct of inspectors, such as having no financial interest in undertakings under supervision, no disclosure of trade secrets and, of particular importance, confidentiality in case of complaints by workers, which means giving no hint to the employer about the identity of complainant.
Promotion of progressive development by Conventions
Work on Conventions tries to mirror law and practice in Member States of the Organization. However, there are cases where new elements are introduced which have so far not been the subject of widespread national regulation. The initiative may come from delegates, during the discussion of a norm in a Conference Committee; where justified, it may be proposed by the Office in the first draft of a new instrument. Here are two examples:
(1)The right of a worker to remove himself or herself from work that poses an imminent and serious danger to his or her life or health.
Normally people consider that it is a natural right to leave a workplace in case of danger to life. However this action may cause damage to materials, machinery or products—and can sometimes be very costly. As installations get more sophisticated and expensive, the worker might be blamed for having unnecessarily removed himself or herself, with attempts to make him or her liable for the damage. During discussion in a Conference Committee on the Safety and Health Convention a proposal was made to protect the worker against recourse in such cases. The Conference Committee considered the proposal for hours and finally found wording to protect the worker which was acceptable to the majority of the Committee.
Article 13 of Convention No. 155 thus reads: “A worker who has removed himself from a work situation which he has reasonable justification to believe presents an imminent and serious danger to his life or health shall be protected from undue consequences in accordance with national conditions and practice”. The “undue consequences” include, of course, dismissal and disciplinary action as well as liability. Several years later, the situation was reconsidered in a new context. During the discussions at the Conference of the Construction Convention in 1987-88, the workers’ group tabled an amendment to introduce the right of a worker to remove himself or herself in case of imminent and serious danger. The proposal was finally accepted by the majority of Committee members under the condition that it was combined with a worker’s duty to immediately inform his or her supervisor about the action.
The same provision has been introduced in the Chemicals Convention, 1990 (No. 170); a similar text is included in the Safety and Health in Mines Convention, 1995 (No. 176). This means that countries which have ratified the Safety and Health Convention or the Convention on Construction, Chemical Safety or Safety and Health in Mines must provide in national law for the right of a worker to remove himself or herself and to be protected against “undue consequences”. This will probably sooner or later lead to application of this right for workers in all sectors of economic activity. This newly recognized right for workers has in the meantime been incorporated in the basic EU Directive on Safety and Health Organization of 1989; all Member States of the EU were to have incorporated the right in their legislation by the end of 1992.
(2)The right for a worker to have a medical examination instead of mandatory medical examinations.
For many years national legislation had required medical examinations for workers in special occupations as a prerequisite for assignment to or continuation of work. Over time, a long list of mandatory medical examinations before assignment and at periodic intervals had been prescribed. This well-meaning intention is increasingly turning into a burden, however, as there may be too many medical examinations administered to one person. Should the examinations be recorded in a health passport of a worker for lifelong testimony to ill-health, as practised in some countries, the medical examination in the end could become a tool for selection into unemployment. A young worker having recorded a long list of medical examinations in his or her life due to exposure to hazardous substances may not find an employer ready to give him or her a job. The doubt may be too strong that this worker may sooner or later be absent too often because of illness.
A second consideration has been that any medical examination is an intrusion into a person’s private life and therefore a worker should be the one to decide on medical procedures.
The International Labour Office proposed, therefore, to introduce in the Night Work Convention, 1990 (No. 171) the right of a worker to have a medical examination instead of calling for mandatory surveillance. This idea won broad support and was finally reflected in Article 4 of the Night Work Convention by the International Labour Conference in 1990, which reads:
1.At their request, workers shall have the right to undergo a health assessment without charge and to receive advice on how to reduce or avoid health problems associated with their work: (a) before taking up an assignment as a night worker; (b) at regular intervals during such an assignment; (c) if they experience health problems during such an assignment which are not caused by factors other than the performance of the night work.
2.With the exception of a finding of unfitness for night work, the findings of such assessments shall not be transmitted to others without the worker’s consent and shall not be used to their detriment.
It is difficult for many health professionals to follow this new conception. However, they should realize that a person’s right to determine whether to undergo a medical examination is an expression of contemporary notions of human rights. The provision has been already taken up by national legislation, for example in the 1994 Act on Working Time in Germany, which makes reference to the Convention. And more importantly, the EU Framework Directive on Safety and Health follows this model in its provisions on health surveillance.
Functions of the International Labour Office
The functions of the International Labour Office as laid down in Article 10 of the Constitution include the collection and distribution of information on all subjects related to the international adjustment of conditions of industrial life and labour with special emphasis on future international labour standards, the preparation of documents on the various items of the agenda for the meeting of the ILC (especially the preparatory work on contents and wording of Conventions and Recommendations), the provision of advisory services to governments, employers’ organizations and workers’ organizations of member states related to labour legislation and administrative practice, including systems of inspection, and the edition and dissemination of publications of international interest dealing with problems of industry and employment.
Like any ministry of labour, the International Labour Office is made up of bureaus, departments and branches concerned with the various fields of labour policy. Two special institutes were established to support the Office and Member States: the International Institute for Labour Studies at ILO headquarters, and the International Training Centre of the ILO in Turin, Italy.
A Director-General, elected by the Governing Body for a five-year term, and three Deputy Director-Generals, appointed by the Director-General, govern (as of 1996) 13 departments; 11 bureaus at headquarters in Geneva, Switzerland; two liaison offices with international organizations; five regional departments, in Africa, the Americas, Asia and the Pacific, the Arab States, and Europe, with 35 area and branch offices and 13 multi-disciplinary teams (a group of professionals of various disciplines who provide advisory services in Member States of a subregion).
The Working Conditions and Environment Department is the Department in which the bulk of safety and health work is carried out. It comprises a staff of about 70 professionals and general service personnel of 25 nationalities, including professional experts in the multi-disciplinary teams. As of 1996, it has two branches: the Conditions of Work and Welfare Facilities Branch (CONDI/T) and the Occupational Safety and Health Branch (SEC/HYG).
The Safety and Health Information Services Section of SEC/HYG maintains the International Occupational Safety and Health Information Centre (CIS) and the Occupational Safety and Health Information Support Systems Section. The work on this edition of the Encyclopaedia is housed in the Support Systems Section.
A special unit of the Department was established in 1991: the International Programme on the Elimination of Child Labour (IPEC). The new programme executes, jointly with Member States in all regions of the world, national programmes of activity against child labour. The programme is financed by special contributions of several Member States, such as Germany, Spain, Australia, Belgium, the United States, France and Norway.
In addition, in the course of the review of the ILO’s major safety and health programme established in the 1970s, the International Programme for the Improvement of Working Conditions and the Environment—known under its French acronym PIACT—the International Labour Conference adopted in 1984 the PIACT Resolution. In principle, the Resolution constitutes a framework of operation for all action by the ILO and by Member States of the Organization in the field of safety and health:
- Work should take place in a safe and healthy working environment.
- Conditions of work should be consistent with workers’ well-being and human dignity.
- Work should offer real possibilities for personal achievement, self-fulfilment, and service to society.
Publications concerning workers’ health are published in the Occupational Safety and Health Series, such as Occupational Exposure Limits for Airborne Toxic Substances, a listing of national exposure limits of 15 Member States; or the International Directory of Occupational Safety and Health Services and Institutions, which compiles information on the safety and health administrations of Member States; or Protection of Workers from Power Frequency Electric and Magnetic Fields, a practical guide to provide information on the possible effects of electric and magnetic fields on human health and on procedures for higher standards of safety.
Typical products of the safety and health work of the ILO are the codes of practice, which constitute a kind of model set of regulations on safety and health in many fields of industrial work. These codes are often elaborated in order to facilitate the ratification and application of ILO Conventions. For example, the Code of Practice on Prevention of Major Industrial Accidents, whose objective is to provide guidance in the setting up of an administrative, legal and technical system for the control of major hazard installations in order to avoid major disasters. The Code of Practice on Recording and Notification of Occupational Accidents and Diseases aims at a harmonized practice in the collection of data and the establishment of statistics on accidents and diseases and associated events and circumstances in order to stimulate preventive action and to facilitate comparative work between Member States (these are just two examples from a long list). Within the field of information exchange two major events are organized by the Safety and Health Branch of the ILO: the World Congress on Occupational Safety and Health, and the ILO International Pneumoconiosis Conference (which is now called The International Conference on Occupational Respiratory Diseases).
The World Congress is organized every three or four years jointly with the International Social Security Association (ISSA) and a national safety and health organization in one of the ILO Member States. World Congresses have been held since the 1950s. Some 2,000 to 3,000 experts from more than 100 countries meet at these congresses in order to exchange information on good practices in safety and health and on modern trend setting, and to establish relations with colleagues from other countries and other parts of the world.
The Pneumoconiosis Conference has been organized by the ILO since the 1930s; the next is planned for 1997 in Kyoto, Japan. One of the outstanding outputs of these conferences is the ILO International Classification of Radiographs of Pneumoconiosis.
The ILO’s technical cooperation in the field of safety and health has many facets. Several projects assisted Member States in preparing new legislation on safety and health and in strengthening their inspection services. In other countries, support has been provided for the creation of safety and health institutes in order to promote research work and develop training programmes and activities. Special projects were designed and executed on mine safety and chemical safety, including the establishment of major hazard control systems. These projects may be targeted towards one Member State, or to a regional group of countries. The tasks at ILO headquarters include the assessment of needs, project development and design, identification of financial support from international funds and national aid programmes, selection and provision of technical expertise, procurement of equipment and planning, and the organization and implementation of study tours and fellowship programmes.
Standard setting, research, collection and dissemination of information and technical cooperation reflect the operational arms of the ILO. In active partnership with the Organization’s tripartite membership these activities reinforce the struggle for the goal of social justice and peace in the world.
This is why in 1969, at the 50th anniversary of the Organization, the work and achievements of the International Labour Organization were awarded the Nobel Peace Prize.
Ethics in the Workplace: A Framework for Moral Judgement
The Framework
There is no ethical possibility of serious dialogue on moral issues without disclosing the framework of critical decision-making tools—the assumptions—of the participants. Different tools result in different decisions.
The most important critical assumptions made in labour-management relations are those which become the basis of assigning obligations or duties in the face of multiple and often conflicting paths to the protection of “rights” of workers and their employers.
How do we decide to meet different and often conflicting needs found both in natural sets of humans (such as individual, family, peer group, community) and in synthetic sets of humans (such as political party, union, corporation, nation) which may include many diverse natural sets?
How do we decide who is responsible to provide family health care and “safe” tools to design a work station? How do we choose a level of risk in setting a permissible exposure limit?
How do we allocate moral responsibility and distribute the burden of risk?
The “Ladder of Social Justice”
To allocate responsibility, we can posit a “ladder of social justice”. On this ladder, those most able to act are rationally obligated to rise to the highest rung of responsibility so that they may act first in pursuit of a moral objective. They are obligated to act before others, because they are best or uniquely able to do so. This does not mean that only they should act. When those with special obligations fail to act, or need assistance, the obligation falls on the shoulders of those on the next rung.
By rational we mean not only an action that logically follows another. We also mean actions taken to avoid pain, disability, death and loss of pleasure (Gert 1993).
An application of the ladder is found in the US Occupational Safety and Health Act of 1970. The Act provides that “employers and employees have separate but dependent responsibilities and rights with respect to achieving safe and healthful working conditions”.
An employee has a duty to comply with rules uniquely “applicable to his own actions and conduct”. The employer has duties based on a unique ability to ensure compliance with rules applicable to an entire workplace. Government has a separate duty based on its unique abilities, for example, to mandate rules if persuasion fails.
There are other assumptions in the framework common to any system of ethical values in any culture. Here, we need to highlight those having to do with the nature of our community, the meaning of “rights”, the method of moral axioms, truth or the good, risk allocation, ideals and reality, and the ethical need for worker participation.
We exist, ecologically, as a global community. In our niche, natural sets of humans (such as families or peer groups) are more meaningful than synthetic sets (such as a corporation or politically defined entity). In this community, we share necessary obligations to protect and to help everyone to act rationally in accordance with their rights, just as we should protect our own rights, regardless of differences in mores and cultural values. These obligations, when they result in actions that protect workers across an international border, are not the imposition of the synthetic values of one nation upon another synthetic set of people. They are acts of reverent recognition of natural, timeless, universal moral values.
Basic human rights, the generic rights to freedom and life (or well being) derive from needs which, if met, enable us to be human (Gewirth 1986). They are not given us by any government or enterprise. We always have had them, logically and phylogenetically. Laws governing the work environment, and rules consistent with rights they implement, are not gifts of charity or benevolence. They are expressions of morality.
The specifications of basic rights, such as personal privacy and the “rights” to know and act in the avoidance of the risks of work, while expressed differently in different cultures, fundamentally are the same among all people in every nation.
Acting on the specifications of our rights may result in conflicts between those rights which protect the individual, such as protecting the privacy of personal medical records, and those concerned with the duties of the employer, such as deriving information from medical records to protect other lives through the avoidance of health hazards thus made known.
These conflicts may be resolved, not by depending upon the ability of a lone physician or even a professional society to withstand court or company challenges, but by choosing axioms of moral behaviour that are rational for everyone collectively in the workplace. Thus, taking encompassing action through stewardship of personal medical records by agencies such as a government-supervised labour-management “neutral” entity (like Germany’s Berufgenossenschaften) may resolve this conflict.
A critical assumption at the very base of this framework of moral judgement is the belief that there is only one real world and that the generic rights apply to everyone in that world, not as ideals that need not be achieved, but as generic conditions of actual existence. If they cannot be applied, it is because we haven’t learned to cope with the fact that knowledge of that world and of the most rational way of conducting ourselves in it is never complete. What we should learn is how to use postulates or axioms not only in ethics, but to describe the world and to guide conduct in the absence of perfect knowledge.
The nature of moral axioms is illuminated by Bertrand Russell’s observation that “all rational conduct of life is based upon the method of the frivolous historical game in which we discuss what the world would be like if Cleopatra’s nose had been half an inch longer” (Russell 1903).
The game of “as if” allows us to act in the face of ever-present moral and scientific uncertainty. But axioms must not be confused with ultimate “truth” (Woodger 1937). They are kept and used if fruitful in the application of basic ethical principles. When they are found to be no longer useful, they can be discarded and replaced with another set of conventions.
Moral axioms bring the framework of judgement to the level of practice, to the “shop floor”. An example is the common practice of developing professional codes of ethics for corporate physicians and other professionals. They are drafted to protect generic rights and their specifications by bridging gaps in knowledge, to organize experience and to permit us to act in advance of morally or scientifically certain knowledge.
These sets of axioms, like all systems of axioms, are neither right nor wrong, true nor false. We act as if they are right or true (in fact they may be) and retain them only as long as they continue to be fruitful in permitting us to act rationally. The test of fruitfulness will yield different results in different cultures at different points in time because, unlike generic ethical principles, cultural norms reflect relative values.
In cultures of the East, powerful social and legal sanctions enforced professional behaviours consistent with the Buddhist belief in the eightfold path to righteous living, the fifth fold of which was righteous livelihood, or with Confucian traditions of professional responsibility. In such settings, professional codes of ethics can be powerful tools in the protection of the patient or research subject, as well as the physician or scientist.
In cultures of the West, at least at this time despite the strong Hippocratic tradition in medicine, the codes are less effective, albeit retaining a limited value. This is not only because the social and legal sanctions are less powerful, but also because of some assumptions that simply do not fit the realities of current western cultures.
It is clear, for example, that the incorporation in codes of ethics of the widespread doctrine, an axiom, requiring “voluntary”, “informed” consent prior to privacy-invasive procedures (such as genetic testing) is irrational. The consent is seldom really voluntary or informed. The information conveyed is seldom certain or complete (even in the mind of the scientist or physician). Consent is usually obtained under socially (or economically) coercive conditions. The promises of the researcher to protect privacy and confidentiality cannot always be kept. The professional may be socially and legally protected by codes that incorporate this doctrine, but the worker easily becomes the victim of a cruel hoax resulting in social stigma and economic duress due to job and insurance discrimination.
Thus, continued use of the consent doctrine in codes of professional behaviour, as in protecting the worker from the dangers of genetic testing, is unethical because a facade is created that doesn’t fit the modern context of a culture westernized and made global by international data banks served by linked telephones and computers. The practice should be discarded and replaced with codes made effective by assumptions that fit the real world coupled with socially and legally enforceable protections.
Risk Allocation
It is irrational (and therefore immoral) to distribute or allocate the burden of risk by caste, that is, to assign different levels of risk for different sets of humans, as marked by genome, age, socioeconomic status, geographic location within the global community, ethnicity or occupation. Risk allocation by caste assumes that there are humans whose generic rights are different from others. Basic human needs are the same. Therefore, basic human rights are the same.
The concept of “acceptable risk”, widely if not universally used in the setting of standards, is a form of risk allocation by caste. It depends upon the assignment of a risk differential based on calculating the risks of past work practice or prevalent exposure to a toxic substance or hazard in the workplace. This common practice accepts and promotes unnecessary risks by arbitrarily assigning, for example, an “acceptable” risk ratio of one death per thousand in setting a permissible exposure level for workers, compared to one death per million for other members of the same community.
Other examples of irrational (immoral) risk allocation are the acceptance of risk differentials within a caste, as between adults and more vulnerable children (setting one standard for both when stronger protection is needed for children), between the work and community environments, between “guest” (or other less empowered) and indigenous workers, and risks (greater than we have set for ourselves) imposed upon the less protected workers in underdeveloped countries by market demands for their products in more developed countries.
Unnecessary risks are never morally acceptable. A risk is ethically “acceptable” only if it is necessary to protect life (or well-being) and freedom or (1) is culturally impacted and very difficult to eliminate or control in a short time and (2) has a lower priority for control within a rational abatement scheme than another biologically adverse hazard.
Worker Participation
The generic rights to life and freedom necessitate empowering workers to rationally make and act upon choices made in pursuit of these rights. Empowerment occurs through access to information, educational opportunities to understand (and not simply react to information), and unfettered or uncoerced ability to act on this understanding in avoiding or taking risks.
Education that yields understanding may not happen in a typical safety training session, since training is meant to induce a conditioned response to a set of foreseeable signals or events, and not to provide in-depth understanding. Yet not all the causal factors, including events under the control of workers or management, that result in so-called accidents can be foreseen.
True accidents themselves are defined as “occurrences by chance” (Webster’s Third International Dictionary 1986). Thus they do not exist in nature. Every event has a cause (Planck 1933; Einstein 1949). The concept of chance is an axiom fruitfully used when a cause is not known or understood. It should not be confused with invariable reality. Even when injury or disease is clearly associated with work, all the causal factors of the events—in or out of the workplace—resulting in harm are never known or understood when they occur (Susser 1973). Thus, even if time, financing and training resources were infinitely available, it is impossible to condition a worker to every possible set of signals for every possible event.
To effectively reduce the risk of “accidents”, understanding a chemical process or a materials handling practice enables the worker to deal with unforeseen events. Education of the worker and his natural set, such as the family and peer group to which the worker belongs, enhances both understanding and the ability to act in preventing or reducing risk. Therefore, it is a specification of generic rights.
There is another ethical role for a worker’s natural set. Choosing an appropriate location where the worker decides or consents to a risk is a critical factor in assuring an ethical outcome. Many decisions (such as the acceptance of hazard pay) should be made, if they are to even approach being truly voluntary, only in a milieu other than a synthetic setting such as the place of work or a union hall. Family, peer group and other natural sets may provide less coercive alternatives.
Providing an economic incentive to accept an unnecessary risk known to a worker, employer or government—even as the result of a fairly negotiated contract—is always immoral. It is just compensation, if adequate, to a worker’s family when the risk can be justified and when a worker has equal alternative employment available without stigma. Making this choice ethically requires the most neutral or non-coercive setting possible.
If these settings are not available, the decision should be made in the most relatively neutral place associated with the most relatively neutral synthetic set or agency that can protect the empowerment of the worker and his or her natural set. The importance to the well-being of a worker of cultural and ethical values found in his or her family, peer group and community underline the importance of protecting their involvement and understanding as ethically based elements in the empowerment process.
Confusing Axioms and Reality in Communication
Most of us, even physicians, scientists and engineers, have been educated in primary school to understand axiomatic methods. It is not otherwise possible to understand arithmetic and geometry. Yet many consciously confuse assumptions and facts (which can be, but are not always, the same) in an effort to impose personal social values on a specific course of action or inaction. This is most obvious in how information is presented, selected, organized and interpreted.
Use of words like accidents and safe are good examples. We have discussed accidents as events that do not occur in nature. Safe is a similar concept. Most people believe that this word means “free from harm, injury or risk” (Webster’s Third International Dictionary 1986). A riskless void cannot be found, but it is standard practice for “experts” to use this word in describing a condition or chemical, leaving the impression that there is an absence of risk, while assuming or having in mind another meaning—such as their belief that the risk is relatively low or “acceptable”—without informing the audience. If this is done unknowingly, it is a simple mistake called a semi-logical fallacy. If it is done consciously, as is too often the case, it is a simple lie.
The confusion with invariable reality of sets of axioms, models of scientific explanation or assessments of data, seems to be concentrated in the setting of standards. Axiomatic concepts and methods in regulation, the validity of which are assumed and commonly confused with incontrovertible truth, include:
- thresholds of toxic effects in populations (never found)
- levels of observed effects (depend on methods)
- statistical confidence factors (arbitrary by definition)
- exact risk extrapolations (seldom fit data)
- zero risk tolerances (exist only with zero exposure)
- margins of “safety” (always speculative)
- control feasibility (depends on values)
- measurement methods (choice of instruments)
- physiological norms (abstractions from averages)
- biological end-points (valuing an effect)
- lifestyle and genetic homogeneity (never found).
These axioms usually are discussed as if they are the truth. They are no more than discardable assumptions about individuals, risks and their control, based (at best) on limited information.
Social and economic values implicit in the selection and use of these axioms guide the policy judgements of those who govern, manage and control. These values, not scientific data alone, determine environmental and biological norms and standards in the community and workplace. Thus, these values, judgements based on them, and the axioms selected also must be judged by their reasonableness, i.e., their success in avoiding the risk of pain, death and disability.
Law and Contracts: Systems of Moral Axioms
Even the most encompassing system of moral axioms should be understood as an experiment in applying moral principles in the work environment, especially the systems of laws and contracts that govern the workplace.
The laws of the state, the rules of its ministerial bodies and even informally adopted procedures (such as models of risk assessment) can be treated—and changed—just like any system of axioms. Consistent with our framework of moral principles, treated as moral axioms, occupational safety and health laws and rules can be fully integrated with other axiomatic systems that meet other community health needs. They can be a differentiated (but not degraded) part of the total community system.
Health care, education, wage replacement and rehabilitation, social security, protection of the disabled, and other public health and environmental protection programmes are often coordinated by legislatures with occupational safety and health programmes. In doing this, care must be taken not to impose or inadvertently create or perpetuate a caste system.
How is this care to be taken? Participation by workers and representatives from their freely organized unions in contracted workplace and governmental bodies is a safeguard that should be part of the experiment. Participation is another specification of human rights. Tested barriers to caste systems in the workplace include workers’ councils (guaranteed in the constitutions of some countries), labour-management committees, ministerial committees on policies and practices, those dealing with standard-setting and enforcement, and education (both professional and rank-and-file) and other participative structures.
The exercise of participatory “rights” by workers in the determination of their own risks is an ethically mandated means of defence against the rise of castes of humans designated by the colour of their collars. It is the first step to the ethical allocation of responsibility and the distribution of the burden of risk in the workplace. The exercise of these rights, however, may conflict with the rights of management and of society as a whole.
Resolution of the conflict is found in understanding that these rights are specifications of generic rights, the imperative of which is absolute and which must ultimately prevail through recognition of the participatory rights of workers, management and the public at large in decisions that affect life and freedom in the community they each share.
ILO Conventions-Enforcement Procedures
A country ratifying an ILO Convention pledges to “take such action as may be necessary to make effective” its provisions (ILO Constitution, article 19(5)). There are several ways that other countries and workers’ and employers’ organizations (but not individuals) can take action to encourage a government to respect the obligations it has undertaken. An organization need only send a letter containing sufficient information to the Director-General, International Labour Office, 4 route des Morillons, 1211 Geneva 22, Switzerland (fax number 41-22-798-8685). The procedures described here are complemented by the ILO’s work to promote international labor standards, such as seminars and workshops carried out by regional advisers.
Article 22 procedures. A government must submit reports on the application of Conventions it has ratified to the International Labour Office (Article 22). The government is also bound to provide copies of those reports to the most representative organizations of employers and workers in the country (Article 23). These organizations can make comments on the reports and provide additional information on the application of an instrument. An independent Committee of Experts on the Application of Conventions and Recommendations (CEARC) examines the reports and any comments made, and it may then address comments to governments to recommend changes in law or practice or to note cases of progress. The CEARC in turn submits its report each year to the tripartite International Labour Conference. The Conference sets up an Applications Committee, which addresses selected cases before reporting to the plenary. The Conference report appeals to governments to respect the obligations they have undertaken by ratifying ILO Conventions and sometimes urges them to accept “direct contacts” missions, during which solutions can be sought in consultation with the government and workers’ and employers’ organizations in the country.
Article 24 procedures. Under this article of the ILO Constitution, any “industrial association of employers or of workers” may make a representation alleging that an ILO Member State has failed to observe any ILO Convention to which it is a party. To be receivable, a representation must come from such an organization, be in writing, refer to Article 24 of the ILO Constitution and indicate in which respect the Member State concerned has failed to secure the effective observance within its jurisdiction of a Convention (identified by name and/or number) it has ratified. The ILO Governing Body may then set up a committee to examine the representation, communicate it to the government for comment and prepare a report, which the Governing Body can order to be published. It may also lead to a direct contacts mission. Where a government has not acted on the report of an Article 24 representation, the Governing Body may initiate the complaint procedure provided by Article 26 of the ILO Constitution.
Article 26 procedures. This article of the ILO Constitution permits complaints to be filed with the International Labour Office against a Member State which has allegedly failed to secure the observance of a Convention it has ratified. A complaint may be lodged by another Member State having also ratified the same Convention, by a delegate (government, employer or worker) to the International Labour Conference or by the Governing Body of the ILO. The Governing Body may appoint a Commission of Inquiry to consider the complaint and report back to it. The Commission of Inquiry’s findings of fact and recommendations are then published. The recommendations may include a direct contacts mission. In case of disagreement as regards the recommendations of the Commission of Inquiry, a complaint may be referred to the International Court of Justice, whose decision is final.
Freedom of association procedures. With freedom of association and the right to engage in collective bargaining at the heart of membership of the ILO, it has established special procedures to deal with complaints alleging infringements of these rights. A Governing Body Committee on Freedom of Association examines complaints made by national or international organizations of employers or workers against any ILO Member State, even when it has not ratified the two main ILO Conventions on freedom of association and collective bargaining. This Committee can also recommend that a government accept a direct contacts mission to assist it in ensuring respect for these basic principles.
Effect. While the ILO has no police force or labor inspectorate empowered to order a workplace to be made safer, governments are sensitive to pleas that they fulfill the obligations they have undertaken in ratifying ILO Conventions. The public pressure brought to bear by use of the ILO procedures has in a number of cases led to changes in law and practice, and thus through them to an improvement of working conditions.
Surveillance of the Working Environment
Since Ramazzini published the seminal text on occupational medicine (Ramazzini 1713), we have come to realize that working at certain jobs can cause specific illnesses. At first, only observational tools were available to survey the work environment. As technology developed, we began to be able to measure the environments in which workers plied their trades. Measuring the workers’ environment has helped identify the sources of workplace stresses. However, this improved knowledge brought with it a need to set exposure limits to protect workers’ health. Indeed, we have found ways to detect the presence of toxic substances at low levels, before they can create health problems. Now we often can predict the results of exposures without waiting for the effects to appear, and thus prevent disease and permanent injury. Good health in the workplace is no accident; it requires surveillance of workers and their environments.
Workplace Exposure Limits
Early workplace exposure limits were set to prevent acute illness and death. Today, with much better information, we try to meet much lower limits in order to prevent chronic illness and subclinical health effects. The most successful systematic attempt to develop occupational exposure limits was the effort of the Committee on Threshold Limits established by the American Conference of Governmental Industrial Hygienists (ACGIH) in 1943. (The ACGIH is a US organization with no formal ties to any government regulatory agency.) The success of this effort is shown by the fact that many countries around the world have adopted the threshold limit values (TLVs) published by ACGIH, which now number more than 600, as workplace exposure standards. Their wide use as enforceable standards has invited critical examination of TLVs and the process by which they were set. Despite their usefulness, TLVs have been criticized from three sectors of the decision-making process: scientific, political and ethical. A brief review of several criticisms follows:
Scientists criticized the fact that the TLVs set on the basis of substantial data are not distinguished from those based on considerably less data.
TLVs were never intended to be “safe” exposure levels for all workers. The TLV Committee recognized that the biological variations among workers, and other factors that could not be calculated, made it impossible to set limits that would guarantee safety for all workers in all environments. Adopting TLVs as enforceable standards creates a political problem, because part of the worker population is not protected. Only zero exposure can provide this guarantee, but zero exposure and zero risk are not practical alternatives.
The data that the TLV Committee worked with were often produced and paid for by industry, and were unavailable to the public. Those protected by this limit-setting process argue that they should have access to the data upon which the limits are based. Industry’s attempts to restrict access to their data, no matter what the reason, are seen by many as unethical and self-serving.
TLVs are still widely respected as guidelines for workers’ exposures to environmental stresses, to be used by professionals who can interpret them properly.
Community Exposure Standards
There is a link between occupational and community exposures. Any adverse health effects seen in workers are a result of their total exposure to environmental contaminants. Total dose is important in selecting appropriate exposure limits. This need is already recognized for poisons that accumulate in the body, such as lead and radioactive substances.
Present exposure limits differ for workers and for the community, in part, because workers’ exposures are intermittent, not continuous. TLVs were set for a five-day work week of eight-hour days, the norm in the United States. TLVs reflect the action of human repair mechanisms. However, many argue that community and occupational exposure limits should not be different.
Without specific information about synergistic or antagonistic effects, exposure limits for both workers and the public reflect only additive interactions between multiple environmental contaminants. When setting limits for a single substance, the complexities of the environments in which we live and work make it impossible to evaluate all potential interactions among environmental contaminants. Instead, we make the following simplifying assumptions: (1) the basic mix of chemicals in our environment has not changed materially; and (2) the epidemiological information and the environmental criteria used to set standards reflect our exposure to this mix of chemicals. By making these assumptions when setting community exposure limits for individual substances, interactions can be ignored. Although it would be useful to apply the same reasoning to setting workplace exposure limits, the logic is questionable because the mix of substances in the various work environments is not uniform when compared with that in our communities.
A part of the political debate is whether to adopt enforceable international exposure standards. Should an individual country set its own priorities, as reflected in its exposure limits, or should international standards be adopted, based on the best data available? Many governments of developing countries take the position that the developed countries should have stricter community exposure standards, because the latter’s industrial and agricultural pollution has created a less healthy environment.
Health Criteria Based on the Type of Risk
Currently, we rely heavily on toxicity testing of animals to set human exposure limits. Today’s sophisticated technology makes it possible to determine both the degree and kind of toxicity that a body will suffer after exposure to a substance. We measure a substance’s ability to cause cancer, to damage a foetus, to cause even benign tumours. We also measure the degree to which that substance can affect somatic systems. Many scientists assume that there is a safe level of exposure, and this has been validated by observations of mankind’s early diseases. However, such an assumption may not be justified today, especially for cancer. Experts still argue both for the existence and absence of a no-effect or “safe” level of exposure.
We co-exist with natural carcinogens in our environment. To deal with them, we must calculate the risk associated with exposure to these substances, and then use the best available technology to reduce that risk to an acceptable level. To think we can achieve zero risk is a misleading idea, and possibly the wrong path to take. Because of the cost and complexity of animal testing, we use mathematical models to predict the risks of exposures to substances at low doses. The best we can do is compute statistically reliable predictions of what are likely to be safe levels of exposure to environmental stresses, assuming a level of risk that the community accepts.
Monitoring the Working Environment
Monitoring of the working environment is the speciality of occupational hygienists. (In North America, they are called industrial hygienists.) These professionals practice the art and science of identification, evaluation and control of occupational stresses. They are schooled in the techniques of measuring the environment in which people work. Because of their obligation to protect the health and well-being of employees and the community, occupational hygienists have a deep concern for ethical issues. As a result, the principal industrial hygiene societies in the United States recently completed a revision to their Code of Ethics, which was originally drafted in 1978 (see also “Canons of Ethical Conduct and Interpretive Guidelines”).
Problems of Secrecy
Data developed from monitoring the work environment are critical to improving exposure limits both for workers and for the community. In order to come up with the best limits, which balance risk, cost and technical feasibility, all data from industry, labour and government must be available to those who set the limits. This consensus approach seems to be growing in popularity in a number of countries, and may become the procedure of choice for setting international standards.
Regarding trade secrets and other proprietary information, the new Code of Ethics provides guidelines for industrial hygienists. As professionals, they are obliged to make sure that all parties who need to know information regarding health risks and exposures are given that information. However, hygienists must keep key business information confidential, except when overriding health and safety considerations require them to reveal it.
International Organization for Standardization (ISO)
The International Organization for Standardization (ISO) is a worldwide federation of national standards bodies at present comprising the national standards bodies of 120 countries as of 1996. The object of ISO is to promote the development of standards in the world with a view to facilitating international exchange of goods and services and to developing mutual cooperation in the sphere of intellectual, scientific, technological and economic activity. The results of ISO technical work are published as International Standards.
The scope of ISO is not limited to any particular branch; it covers all standardization fields except standards for electrical and electronic engineering, which are the responsibility of the International Electrotechnical Commission (IEC).
ISO brings together the interests of producers, users (including consumers), governments and the scientific community in the preparation of International Standards.
ISO work is carried out through some 2,800 technical bodies. More than 100,000 experts from all parts of the world are engaged in this work which, to date, has resulted in the publication of over 10,000 International Standards, representing some 188,000 pages of concise reference data in English and French.
Origin and Membership
International standardization started in the electrotechnical field some 90 years ago. While some attempts were made in the 1930s to develop International Standards in other technical fields, it was not until ISO was created that an international organization devoted to standardization as a whole came into existence.
Following a meeting in London in 1946, delegates from 25 countries decided to create a new international organization “whose object shall be to facilitate the international coordination and unification of industrial standards”. The new organization, ISO, began to function officially on 23 February 1947.
A member body of ISO is the national body “most representative of standardization in its country”. It follows that only one such body for each country is accepted for membership in ISO. Member bodies are entitled to participate and exercise full voting rights on any technical committee of ISO, are eligible for membership in the Council and have a seat in the General Assembly. By September 1995 the number of member bodies was 83. More than 70% of ISO member bodies are governmental institutions or organizations incorporated by public law. The remainder have close links with the public administration in their respective countries.
A correspondent member is normally an organization in a developing country which does not yet have its own national standards body. Correspondent members do not take an active part in the technical work, but are kept fully informed of it. Normally, a correspondent member becomes a member body after a few years. Nearly all the present correspondent members are governmental institutions. By September 1995 the number of correspondent members was 24.
A third category, subscriber membership, has been established for countries with smaller-scale economies. These subscriber members pay reduced membership fees that nevertheless allow them to maintain contact with international standardization. By September 1995, the number of subscriber members was eight.
Basic data on each ISO member body are given in the publication ISO Membership.
Technical Work
The technical work of ISO is carried out through technical committees (TC). The decision to set up a technical committee is taken by the Technical Management Board, which also approves the scope of the committee. Within this scope, the committee determines its own programme of work.
The technical committees may, in turn, create subcommittees (SC) and working groups (WG) to cover different aspects of the work. Each technical committee or subcommittee has a secretariat assigned to an ISO member body. At the end of 1995 there were in existence 185 technical committees, 611 subcommittees and 2,022 working groups.
A proposal to introduce a new field of technical activity into the ISO working programme normally comes from a member body, but it may also originate from some other international organization. Since resources are limited, priorities must be established. Therefore, all new proposals are submitted for consideration by the ISO member bodies. If accepted, either the new work will be referred to the appropriate existing technical committee or a new committee will be created.
Each member body interested in a subject for which a technical committee has been authorized has the right to be represented on that committee. Detailed rules of procedure are given in the ISO/IEC Directives.
International Standards
An International Standard is the result of an agreement between the member bodies of ISO. It may be used as such or implemented through incorporation into national standards of different countries.
An important first step towards an International Standard takes the form of a committee draft (CD), a document circulated for study within the technical committee. This document must pass through a number of stages before it can be accepted as an International Standard. This procedure is designed to ensure that the final result is acceptable to as many countries as possible. When agreement is finally reached within the technical committee, the draft proposal is sent to the central secretariat for registration as a draft International Standard (DIS); the DIS is then circulated to all member bodies for voting. In many countries, the DIS is made available for public enquiry, thereby ensuring the widest possible consultations. If 75% of the votes cast are in favour of the DIS, it is accepted for further processing as a Final Draft International Standard (FDIS) which is circulated to all member bodies for formal adoption by ISO. Again, 75% of the votes cast must be in favour of the FDIS in order for the International Standard to be published. Normally the fundamental technical issues are resolved at the technical committee level. However, the member body voting procedure provides assurance that no important objections have been overlooked.
The greater part of the work is done by correspondence, and meetings are convened only when thoroughly justified. Each year some 10,000 working documents are circulated. Most standards require periodic revision. Several factors combine to render a standard out of date: technological evolution, new methods and materials, and new quality and safety requirements. To take account of these factors, ISO has established the general rule that all ISO standards should be reviewed every five years. On occasion it is necessary to revise a standard earlier.
A full list of all published ISO standards is given in the ISO Catalogue.
ISO Work in the Field of Occupational Safety
Every ISO International Standard is prepared with concern for safety; the safety factor is an integral part of the work of ISO.
The more than 10,000 International Standards already published by ISO cover a wide spectrum, from aerospace, aircraft and agriculture to building, fire tests, containers, medical equipment, mining equipment, computer languages, the environment, personal safety, ergonomics, pesticides, nuclear energy and so on.
Many International Standards are easily recognized as important in preventing occupational risks: examples are the basic symbol for signifying ionizing radiation or radioactive materials (ISO 361), safety colours and signs (ISO 3864) and the industrial safety helmet (ISO 3873) specified for medium protection in mining, quarrying, shipbuilding, structural engineering and forestry, and so on. Other International Standards are not so easily identified as being directly relevant, but have an equal impact on the prevention of occupational accidents and diseases; one example is ISO 2631, Evaluation of human exposure to whole body vibration, published in three parts, which grades the “reduced comfort boundary”, the “fatigue-decreased proficiency boundary” and the “exposure limit” according to varying levels of vibration frequency, acceleration magnitude and exposure time, and according to the direction of vibration relative to recognized axes of the human body. This Standard, like all others, is continuously updated in the light of research and experience, and relates to such forms of transport as dumpers, tractors, excavators and many other vehicles and worksites.
The ISO technical committees listed in table 1 are among the most prominent in the work for safety and accidents and disease prevention.
Table 1. ISO technical committees most concerned with prevention of occupational accidents and diseases
|
No. |
Title |
Typical example of ISO standard |
|
|
10 |
Technical drawings, product definition and related documentation |
ISO/DIS 11604 |
Technical product documentation—Data sheets for drawing materials and equipment and related documentation |
|
21 |
Equipment for fire protection and fire-fighting |
ISO 3941 |
Classification of fires |
|
23 |
Tractors and machinery for agriculture and forestry |
ISO 3776 |
Tractors for agriculture—Seat belt anchorages |
|
35 |
Paints and varnishes |
ISO 3679 |
Paints, varnishes, petroleum and related products—Determination of flashpoint—Rapid equilibrium method |
|
43 |
Acoustics |
ISO 4872 |
Acoustics—Measurement of airborne noise emitted by construction equipment intended for outdoor use—Method for determining compliance with noise limits |
|
44 |
Welding and allied processes |
ISO/DIS 10882-2 |
Health and safety in welding and allied processes—Sampling of airborne particles and gases in the operator’s breathing zone—Part 2: Sampling of gases |
|
59 |
Building construction |
ISO/TR 9527 |
Building construction —Needs of disabled people in buildings —Design guidelines |
|
67 |
Materials, equipment and offshore structures for petroleum and natural gas industries |
ISO 10418 |
Petroleum and natural gas industries—Offshore production platforms—Analysis, design, installation and testing of basic surface safety systems |
|
82 |
Mining |
ISO 3155 |
Stranded wire ropes for mine hoisting—Fibre components—Characteristics and tests |
|
85 |
Nuclear energy |
ISO 1709 |
Nuclear energy—Fissile materials—Principles of criticality, safety in storing, handling and processing |
|
86 |
Refrigeration |
ISO 5149 |
Mechanical refrigerating systems used for cooling and heating—Safety requirements |
|
92 |
Fire safety |
ISO 1716 |
Building materials—Determination of calorific potential |
|
94 |
Personal safety—Protective clothing and equipment |
ISO 2801 |
Clothing for protection against heat and fire—General recommendations for users and for those in charge of such users |
|
96 |
Cranes |
ISO 10245-1 |
Cranes—Limiting and indicating devices—Part 1: General |
|
98 |
Bases for design of structures |
ISO 2394 |
General principles on reliability for structures |
|
101 |
Continuous mechanical handling equipment |
ISO 1819 |
Continuous mechanical handling equipment—Safety code—General rules |
|
108 |
Mechanical vibration and shock |
ISO 2631-1 |
Evaluation of human exposure to whole-body vibration—Part 1: General requirements |
|
110 |
Industrial trucks |
ISO 1074 |
Counterbalanced fork-lift trucks—Stability tests |
|
118 |
Compressors, pneumatic tools and pneumatic machines |
ISO 5388 |
Stationary air compressors—Safety rules and code of practice |
|
146 |
Air quality |
ISO 8518 |
Workplace air—Determination of particulate lead and lead compounds—Flame atomic absorption spectrometric method |
|
159 |
Ergonomics |
ISO 7243 |
Hot environments—Estimation of the heat stress on worker, based on the WBGT index (wet bulb globe temperature) |
|
199 |
Safety of machinery |
ISO/TR 12100-1 |
Safety of machinery—Basic concepts, general principles for design—Part 1: Basic terminology, methodology |
These technical committees and others have prepared or are preparing International Standards concerned with occupational risks in such areas as building construction sites, factories, docks, agriculture and forestry, nuclear installations, handling of materials and personal protective clothing and equipment.
The field of building provides a very clear example of the intensive concern for accident and disease prevention in the work of ISO. Of the more than 50 ISO technical committees dealing with some aspect of building or building materials, ten deal with the problems of the working environment. The physical factors in the building field cover aspects such as personal safety, vibration and shock, noise, plant and equipment, earth-moving machinery, cranes and lifting devices, and ergonomics. The chemical factors cover air quality, paints and varnishes, protection of welding workers, and protective clothing and equipment.
ISO TC 127 (Earth-moving machinery) has set up a subcommittee to deal specifically with safety requirements and human factors in respect of all the current basic types of earth-moving machinery such as tractors, loaders, dumpers, tractor scrapers, excavators and graders. Standards are already in existence for safe access to driving cabs via steps, ladders, walkways and platforms, and the dimensions of cabs have been established for both large and small operators, sitting or standing and in arctic clothing or not, as appropriate.
Sitting positions and the sizes and shapes of seats for different operators are also the subject of International Standards. Sitting positions are now being related to areas of comfort and to reach for both hand and foot controls, and Standards have been prepared to determine the field of view available to operators of earth-moving machines, based upon determination of the shape, size and position of areas of invisibility caused by obstructing parts of the machines.
To prevent machines from crushing their operators in the event of accidental overturning, roll-over protective structures (ROPS) have been developed and standardized. Falling rocks, trees and parts of buildings in the process of demolition can prove hazardous, so falling-object protective structures (FOPS) have been standardized so as to minimize the possibility of injury to the operator.
ISO 7000, Graphical symbols for use on equipment—Index and synopsis, provides a synopsis of several hundred internationally agreed graphic symbols to be placed on equipment or parts of equipment of any kind in order to instruct the persons handling the equipment as to its use and operation.
ISO work in the building field is both intensive and extensive, just as it is in other fields covered by ISO. (The scope of ISO includes most industrial, agricultural and maritime activities except the electrotechnical field, which is handled by the International Electrotechnical Commission, and pharmaceutical products, handled by the World Health Organization.)
On the factory floor, International Standards take on a special meaning as persons seeking work migrate from one country to another and often to jobs where they cannot speak or read the local language. Easily recognized graphic symbols for controls on machinery that conform to International Standards are vital here as in the building industry; so are standardized locations for foot and hand controls and International Standards for guards to moving parts.
An ISO safety code for compressors covers a wide range of safety and environmental factors, such as the prevention of oil inhalation and the control of toxic oil inhibitors, the prevention of oil coke ignition and of crankcase explosion, and the use of relief and safety valves.
The safety of continuous mechanical handling equipment is the subject of nearly 40 International Standards. They cover such aspects as safety and safety codes for the different kinds of equipment, such as belt conveyors, vibrating feeders, overhead chain conveyors, hydraulic conveyors, pneumatic handling equipment, and roller and screw conveyors.
In the field of agriculture and forestry, ISO has developed important International Standards that protect the worker. Anchorages for seat belts for farm tractors are the subject of a well known standard that is making the import-export trade easier for manufacturers as it is implemented, replacing a plethora of national standards and regulations on the subject. ISO standards even provide rules for presenting operators’ manuals and technical publications for agricultural tractors and machines, making them easy to read and understand.
On the docks the worker is protected by International Standards that determine the stability of cranes and mobile cranes in action and determine the effect of wind loads on crane structures. Other Standards cover indicators and safety devices that will operate in the event of an operator’s misjudgement. Still others cover indicators such as wind gauges, overvoltage annunciators and mass, slope and slew indicators and “automatic cut-off”, such as derricking limiters, load-lifting capacity limiters and slack rope stops. The Standards produced and in preparation should not only assist operators in their work, but enhance the working environment by inspiring confidence in all works personnel moving under and around cranage. A related International Standard provides discard criteria in relation to wear, corrosion, deformation and wire strand breaks, and is intended to guide competent persons involved in the maintenance and examination of cranes and lifting appliances. New Standards under development include out-of-service anchoring devices, maintenance, condition monitoring, safe use and safety signs.
Safety for the worker and others at or near nuclear installations is covered by a number of International Standards, and the work continues in this area. Subjects covered are methods for testing exposure meters and dosimeters, a test for contents leakage and radiation leakage, and the general principles for sampling airborne radioactive materials.
International Standards for protective clothing and equipment are the responsibility of ISO TC 94. In addition to the Standard for industrial safety helmets, it has developed a standardized vocabulary for personal eye-protectors, established utilization and transmittance requirements for infrared filters for eye protectors, and general recommendations for users and those in charge of users of clothing for protection against heat and fire.
The production and use of ISO International Standards such as these, produced through worldwide cooperation, have unquestionably improved the quality of the workplace.
Ethical Issues: Information and Confidentiality
This article deals with the ethical issues that arise in the practice of occupational health activities, including occupational health research, with respect to the handling of information on individual employees, not in terms of practicality or efficiency but by referring to what may be regarded as right or wrong. It does not provide a universal formula for decisions on whether or not practices in handling information or in dealing with issues of confidentiality are ethically justified or defensible. It describes the cornerstone ethical principles of autonomy, beneficence, non-maleficence and equity and their implications for these human rights issues.
The basic principles used in ethical analyses can be used in examining the ethical implications in the generation, communication and utilization of other types of information as well as, for example, the conduct of occupational health research. Since this article is an overview, specific applications will not be discussed in great detail.
Scenario
On the labour market, in an enterprise, or at a workplace, health issues involve, first and foremost, free-living and economically active people. They may be healthy or experience health disturbances which are, in their causation, manifestation and consequences, more or less related to work and workplace conditions. Furthermore, a broad range of professionals and persons with various roles and responsibilities may become involved in the health issues concerning individuals or groups at the workplace, such as:
- employers and their representatives
- trade unions and their representatives
- health professionals
- social security and insurance administrators
- researchers
- media representatives.
Information arising in the practice or science of occupational health and the issues of need-to-know involve all these groups and their interaction. This means that the question of openness or confidentiality of information with regard to human rights, individual workers’ rights and the needs of employers or the needs of society at large is of broad scope. It may also be of high complexity. It is, in reality, an area of core importance in occupational health ethics.
Basic Considerations
The underlying assumption of this article is that people have a need and also a prima facie right to privacy. This means a need, and a right, to conceal and to reveal, to know as well as to be left in ignorance on various aspects of life in society and one’s own relations with the outer world. Likewise a collective, or a society, needs to know some things about individual citizens. With regard to other things there may be no such need. At the workplace or on the enterprise level, the issues of productivity and health involve the employer and those employed, both as a collective and as individuals. There are also situations where public interests are involved, represented by government agencies or other institutions claiming a legitimate need to know.
The question which immediately arises is how these needs are to be reconciled and what conditions should be satisfied before the needs to know of the enterprise or society can legitimately override the individual’s right to privacy. There are ethical conflicts needing to be resolved in this reconciliation process. If the needs to know of the enterprise or employer are not compatible with the needs to protect the privacy of the employees, a decision has to be made as to which need, or right to information, is paramount. The ethical conflict arises from the fact that the employer is usually responsible for taking preventive action against occupational health hazards. To exercise this responsibility the employer needs information on both working conditions and the health of the employees. The employees may wish some types of information about themselves to be kept confidential or secret, even while accepting the need for preventive measures.
Moral Perspectives
The ethical issues and conflicts in the occupational health sphere may be approached using the two classical ethical paradigms—consequentialist ethics or deontological ethics. Consequentialist ethics focuses on what is good or bad, harmful or useful in its consequences. As an example, the social ambition expressed as the principle of maximizing benefits for the greatest number in a community is a reflection of consequentialist ethics. The distinctive feature of deontological ethics is to regard certain actions or human behaviour as obligatory, such as for example the principle of always telling the truth—the principle of veracity—regardless of its consequences. The deontologist holds moral principles to be absolute, and that they impose an absolute duty on us to obey them. Both these paradigms of basic moral philosophy, separately or in combination, may be used in ethical assessments of activities or behaviours of humans.
Human Rights
When discussing ethics in occupational health, the impact of ethical principles on human relationships and the questions of needs to know at the workplace, it is necessary to clarify the main underlying principles. These can be found in international human rights documents and in recommendations and guidelines stemming from decisions adopted by international organizations. They are also reflected in professional codes of ethics and conduct.
Both individual and social human rights play a role in health care. The right to life, the right to physical integrity, and the right to privacy are of particular relevance. These rights are included in:
- the 1948 Universal Declaration of Human Rights adopted by the United Nations
- the European Convention for the Protection of Human Rights and Fundamental Freedoms (Council of Europe 1950)
- the 1966 United Nations International Covenant on Civil and Political Rights
Of particular relevance for occupational health service personnel are the codes of conduct formulated and adopted by the World Medical Association. These are:
- International Code of Medical Ethics (1949–1968) and Declaration of Geneva (1948–1968)
- Declaration of Helsinki: Recommendation Guiding Medical Doctors in Biomedical Research Involving Human Subjects (1964–1975–1983)
Individual human rights are in principle unrelated to economic conditions. Their foundation lies in the right of self determination, which involves human autonomy as well as human liberty.
Ethical Principles
The principle of autonomy focuses on the individual’s right to self-determination. According to this principle all human beings have a moral obligation to respect the human right to self- determination so long as it does not infringe on the rights of others to determine their own actions on matters concerning themselves. One important consequence of this principle for the practice of occupational health is the moral duty to regard some types of information on individuals as confidential.
The second principle, the principle of care, is a combination of two ethical principles—the non-maleficence principle and the beneficence principle. The first prescribes a moral obligation for all humans not to cause human suffering. The beneficence principle is the duty to do good. It dictates that all humans are under a moral obligation to prevent and to eliminate suffering or harm and also to some extent to promote well-being. One practical consequence of this in the practice of occupational health is the obligation to seek in a systematic way to identify health risks at the workplace, or instances where health or life quality are disturbed as a result of workplace conditions, and to take preventive or remedial action wherever such risks or risk factors are found. The beneficence principle may also be evoked as a basis for occupational health research.
The principle of equity implies the moral obligation of all human beings to respect each other’s rights in an impartial way and to contribute to a distribution of burdens and benefits in such a way that the least privileged members of the community or the collective are given particular attention. The important practical consequences of this principle lie in the obligation to respect the right to self-determination of everyone concerned, with the implication that priority should be given to groups or individuals at the workplace or in the labour market who are most vulnerable or most exposed to health risks at the workplace.
In considering these three principles it is proper to re-emphasize that in the health services the autonomy principle has in the course of time largely superseded beneficence as the first principle of medical ethics. This in fact constitutes one of the most radical re-orientations in the long history of the Hippocratic tradition. The emergence of autonomy as a sociopolitical, legal and moral concept has profoundly influenced medical ethics. It has shifted the centre of decision-making from the physician to the patient and thereby re-oriented the whole physician-patient relationship in a revolutionary way. This trend has obvious implications for the whole field of occupational health. Within the health services and biomedical research it is related to a range of factors which have an impact on the labour market and industrial relations. Among these should be mentioned the attention given to participatory approaches involving workers in decision processes in many countries, the expansion and advance of public education, the emergence of civil rights movements of many types and the rapidly accelerating technological changes in production techniques and work organization.
These trends have supported the emergence of the concept of integrity as an important value, intimately related to autonomy. Integrity in its ethical meaning signifies the moral value of wholeness, constituting all human beings as persons and ends in themselves, independent in all functions and demanding respect for their dignity and moral value.
The concepts of autonomy and integrity are related in the sense that the integrity is expressing a fundamental value equivalent to the dignity of the human person. The concept of autonomy rather expresses the principle of freedom of action directed towards safeguarding and promoting this integrity. There is an important difference between these concepts in that the value of integrity admits no degrees. It may be either intact or violated or even lost. Autonomy has degrees and is variable. In that sense autonomy can be more or less restricted, or, conversely, expanded.
Privacy and Confidentiality
Respect for the privacy and confidentiality of persons follows from the principle of autonomy. Privacy may be invaded and confidentiality violated by revealing or releasing information that can be used to identify or expose a person to unwanted or even hostile reactions or responses from others. This means that there is a need to protect such information from being disseminated. On the other hand, in the event the information is essential to discover or prevent health risks at the workplace, there is a need to protect the health of individual employees and indeed sometimes the health of a larger collective of employees who are exposed to the same workplace risks.
It is important to examine whether the need to protect information on individuals and the need to protect the health of the employee collective and to improve working conditions are compatible. It is a question of weighing the needs of the individual versus the benefits of the collective. Conflicts may therefore arise between the principles of autonomy and beneficence, respectively. In such situations it is necessary to examine the questions of who should be authorized to know what and for what purposes.
It is important to explore both these aspects. If information derived from the individual employees could be used to improve working conditions for the benefit of the whole collective, there are good ethical reasons to examine the case in depth.
Procedures have to be found to deny unauthorized access to information and to use of the information for purposes other than those stated and agreed on in advance.
Ethical Analysis
In an ethical analysis it is essential to proceed step by step in identifying, clarifying and solving ethical conflicts. As has been mentioned earlier, vested interests of various kinds, and of various actors at the workplace or in the labour market, can present themselves as ethical interests or stakeholders. The first elementary step is therefore to identify the main parties involved and to describe their rational interests and to locate potential and manifest conflicts of interests. It is an essential prerequisite that such conflicts of interests between the different stakeholders are made visible and are explained instead of being denied. It is also important to accept that such conflicts are quite common. In every ethical conflict there are one or several agents and one or several subjects concerned by the action undertaken by the agent or agents.
The second step is to identify the relevant ethical principles of autonomy, beneficence, non-maleficence and equity. The third step consists in identifying ethical advantages or benefits and costs or disadvantages for those persons or bodies who are involved in or affected by the problem or the occupational health issue. The expressions ethical gains or ethical costs are here given a rather broad meaning. Anything which may reasonably be judged to be beneficial or to have a positive impact from an ethical point of view is a gain. Anything which may affect the group in a negative way is in an analogous way an ethical cost.
These basic principles of ethics (autonomy, beneficence and equity) and associated steps of analysis apply both for handling of information in the day-to-day practice of professional occupational health work and for handling and communication of scientific information. Seen in this perspective, the confidentiality of medical records or results of occupational health research projects may be analysed on the principal grounds outlined above.
Such information may for instance concern suspected or potential health hazards at work, and it may be of varying quality and practical value. Obviously the use of such information involves ethical issues.
It is to be emphasized that this model for ethical analyses is intended primarily for structuring of a complex pattern of relationships involving the individual employee, the employees at the enterprise as a collective and vested interests at the workplace and in the community at large. Basically, in the present context, it is a pedagogic exercise. It is fundamentally based on the assumption, from some quarters regarded as controversial in moral philosophy, that the objective and correct solution in an ethical conflict simply does not exist. To cite Bertrand Russell:
(We) are ourselves the ultimate and irrefutable arbiters of values and in the world of value nature is only a part. Thus, in this world we are greater than Nature. In the world of values, nature itself is neutral, neither good nor bad, deser- ving neither admiration nor censure. It is we who create values and our desires which confer value. In this realm we are kings, and we debase kingship if we bow down to Na- ture. It is for us to determine the good life, not for Nature—not even nature personified as God (Russell 1979).
This is another way of saying that the authority of ethical principles, as referred to earlier in this text, is determined by the individual person or group of persons, who may or may not agree as to what is intellectually or emotionally acceptable.
This means that in solving ethical conflicts and problems the dialogue between the different interests involved assumes significant importance. It is essential to create a possibility for everyone concerned to exchange views with the others involved in mutual respect. If it is accepted as a fact of life that there are no objectively correct solutions for ethical conflicts, it does not follow that the definition of ethical positioning is entirely based on subjective and unprincipled thinking. It is important to keep in mind that issues related to confidentiality and integrity may be approached by various groups or individuals with points of departure based on widely differing norms and values. One of the important steps in an ethical analysis is therefore to design the procedure for contacts with and between the persons and collective interests concerned, and the steps to be taken to initiate the process ending in agreement or disagreement with respect to the handling or transfer of sensitive information.
Lastly, it is emphasized that ethical analysis is a tool for examination of practices and optional strategies of action. It does not provide blueprint answers to what is right or wrong, or to what is thought to be acceptable or not acceptable from an ethical point of view. It provides a framework for decisions in situations involving the basic ethical principles of autonomy, beneficence, maleficence and equity.
Ethics and Information in Occupational Health
The ethical questions and dilemmas arising in the practice and science of occupational health derive from the collection, storage, analyses and use of information about individual persons. Such processes may be carried out on a routine or ad hoc basis with the objective of improving the health and life quality of employees or the working conditions at the workplace. These are, in themselves, motives which are of fundamental importance in all occupational health work. The information may, however, also be used for selective practices, even of a discriminatory nature, if used for instance in hiring or making work assignments. Information collected from health records or personnel files has, therefore, in principle a potential to be used against the individual in a way which may be unacceptable or regarded as a violation of basic ethical principles.
The information may consist of data and recorded observations from pre-employment medical examinations or periodic screening or health monitoring programmes. Such programmes or routines are often initiated by the employer. They may also be motivated by legal requirements. It may also include information collected at medical consultations initiated by the person concerned. One data source of particular relevance in the occupational health field is the biological monitoring of workplace exposures.
In occupational health practice and in occupational health research many different types of data and observations are collected, documented and, to varying extents, eventually used. The information may concern past health conditions and health-related behaviours, such as absence due to sickness. It may also include observations of symptoms and findings at clinical examinations or results of laboratory examinations of many kinds. The latter type of information may concern functional capacity, muscle strength, physical stamina, cognitive or intellectual abilities, or it may include judgements of performance in various regards. The information may also contain, at the opposite end of the health spectrum, information on health deficiencies; handicaps; extremes of lifestyle; use of alcohol, drugs and other toxicants; and so on. Even if many single items of information of this kind are in themselves relatively trivial or innocuous, combinations of them and the continuous collection of them over time may provide a very detailed and comprehensive description of the characteristics of a person.
The information may be recorded and stored in various forms. Manual records are most common in files containing information on individual persons. Computer databases may also be used with information carriers such as magnetic tapes and floppy discs. Since the memory capacity of such computerized personnel files commonly is of huge dimensions, the databases constitute in themselves potential threats to personal integrity. The information in such data banks and registers and files may, in the hands of less scrupulous persons, constitute a tool of power, which may be used contrary to the interests of the person concerned.
It is beyond the scope of this article to define what type of information is sensitive and what is not. Nor is it the intention in this context to give an operational definition of the concept of personal integrity or to provide a blueprint for judgements on what information is to be regarded as more or less sensitive with respect to basic ethical principles. This is simply not possible. The sensitivity of information in this regard is contextually determined and dependent on many factors. The important consideration lies in applying basic ethical principles in dealing with questions of how, by whom and under what circumstances such data and information are handled.
Risk Analysis and Research Information
In explaining the principles of an ethical analysis the focus has been set on health information and health-related information in individual records such as health records and personnel files. There are, however, both in the practice and in the science of occupational health, other types of information which may, in their generation, processing and use, involve ethical considerations and even conflicts of ethical principles. Such information can, however, usually be analysed using the ethical principles of autonomy, beneficence and equity as points of departure. This applies, for example, in hazard assessments and risk analysis. In a situation where, for instance, relevant information on a health hazard at work is deliberately withheld from the employees, it is to be expected that ethical analysis will demonstrate clearly that all three basic ethical principles are violated. This applies regardless of whether or not the information is judged to be confidential by one of the stakeholding partners involved. The difficulty arises when the information involved is uncertain, insufficient or even inaccurate. Widely differing judgements may also be at hand concerning the strength of the evidence. This, however, does not alter the fundamental structure of the ethical issues involved.
In occupational health research it is quite common to have situations where information on past, present or future research projects is to be communicated to employees. If research is undertaken involving employees as research subjects without explaining the motives and full implications of the project and without seeking proper informed consent by everyone concerned, ethical analysis will demonstrate that the basic tenets of autonomy, beneficence and equity have been violated.
Obviously, the technical and complex nature of the subject matter may cause practical difficulties in the communication between researchers and others concerned. This, in itself, does not change the structuring of the analysis and the ethical issues involved.
Safeguards
There are various administrative safeguards which may be applied to protect sensitive information. Common methods are:
1. Secrecy and confidentiality. Contents of medical records and other items labelled as health information may be regarded as confidential or secret, in legal terms. It is to be observed though that not all contents of such documents are necessarily of a sensitive nature. They also contain items of information which could be communicated freely without causing harm to anyone.
Another aspect is the obligation imposed on members of selected professional groups to keep secret the information given them in confidence. This may be the case in consultations in the types of relationship which may be referred to as fiduciary. This may for instance apply to health information or other information dealt with in a physician-patient relationship. Such information may be protected in legislation, in collective-bargaining agreements or in professional codes.
It should, however, be observed that the concept of health information has—just as the concept of health—no practical operational definition. This means that the term may be given different interpretations.
2. Authorization for access to information. This requirement may for instance apply to researchers seeking information in health records or in social security files of individual citizens.
3. Informed consent as a condition for data collection and access to records containing information on individual persons. The principle of informed consent, implying right to co-decision by the person concerned, is a legally established practice in many countries in all questions regarding collection and access to personal information.
The principle of informed consent is being increasingly recognized as important in handling of personal information. It implies that the concerned subject has a prima facie right to decide what information is acceptable or permissible to be collected, for what purposes, by whom, by using what methods, on what conditions and with which administrative or technical safeguards against unauthorized or unwanted access.
4. Technical safeguards to protect computerized information. This may for instance concern introduction of coding and ciphering routines for prevention of unauthorized access to records containing information on persons or—if access is legitimate—prevention of identification of persons in the data base (protection of anonymity). It should however be observed that anonymity, meaning coding or concealment of name and other identity particulars, such as social security numbers, may not provide reliable protection against identification. The other information contained in the personal file may often be sufficient to allow individual persons to be identified.
5. Legal regulation, including prohibition, authorization and control for establishing and operating computerized data sources containing personnel files or records.
6. Professional ethical code. Principles of ethical standards in professional performance may be adopted by professional bodies and organizations in the form of codes of professional ethics. Such documents exist both on the national level in many countries and also on the international level. For further reference the following international documents are recommended:
- International Code of Ethics for Occupational Health Professionals, adopted by the International Commission on Occupational Health in 1992
- Ethical Guidelines, adopted by the International Epidemiological Association
- International Guidelines for Ethical Review of Epidemiological Studies, adopted by the Council for International Organizations of Medical Sciences (CIOMS)
In concluding this section it is appropriate to emphasize that an elementary principle in planning or establishing practices for data collection is to avoid collection of data without a carefully considered motive and occupational health relevance. The ethical hazards inherent in collecting information which is not utilized for the benefit, including health benefit, of the employee or person concerned, are obvious. In principle, the options and strategies at hand in planning for collection and processing of information on employees are amenable to ethical analyses in terms of autonomy, beneficence and equity.
Computerized Personnel Files
The development of computer technology has created possibilities for employers to collect, store and process information about employees on many diverse aspects relevant to their behaviour and functioning at the workplace. The use of such advanced computer systems has increased significantly during recent years and has led to concerns for the risks of intrusion into individual integrity. It is reasonable to predict that such risks will be still more common in the future. There will be a growing need to use data protection and various measures to guard against violations of integrity.
At the same time it is obvious that new technology brings significant benefits for production in an enterprise or in the public sector, as well as providing means to improve work organization or eliminate such problems as monotonous and short-cycled work tasks. The fundamental question is how to achieve reasonable balance between the benefits in the use of computer techniques and the legitimate rights and needs of the employees to be protected against intrusions into their personal integrity.
The Council of Europe has in 1981 adopted a recommendation (No. R 81–1) on medical databases and a convention on Protection of Individuals with Regard to Automatic Processing of Personal Data. The Council of the European Union has in a directive (95/46/EC)—On the Protection of Individuals with Regard to the Processing of Personal Data and on the Free Movement of such Data dealt with these issues. It should be observed that the implementation of such regulations on computerized personal data is in many countries regarded as issues of industrial relations.
Conclusion
Practical situations involving handling of information in occupational health involve judgements by occupational health professionals and many others. Questions regarding what is right or wrong, or more or less acceptable, arise in the practice of occupational health in many contextually and culturally differing circumstances. Ethical analysis is a tool providing the basis of judgements and decisions, by using ethical principles and sets of values to help evaluate and choose between different courses of action.
International Social Security Association (ISSA)
Raison d’être and Historical Perspective
The aim of the ISSA is to cooperate, at the international level, in the defence, promotion and development of social security throughout the world, basically through its technical and administrative improvement. The prevention of social risks is today considered to form an integral part of social security.
The ISSA had an early forerunner, the Permanent International Committee on Social Insurance (CPIAS), which at first was concerned with the risk of accidents and in 1891 extended its scope to social insurance in general. In 1927, the Tenth Session of the International Labour Conference adopted Convention No. 24, known as the Sickness Insurance (Industry) Convention, and Convention No. 25, known as the Sickness Insurance (Agriculture) Convention. The ISSA was founded at this time, upon the initiative of the International Labour Office, with the aim of gaining support from experts in a number of European countries for the ratification of these instruments. Until 1947 the organization was known as the International Conference of Sickness Insurance Funds and Mutual Benefit Societies (CIMAS).
The concept of prevention already existed in the minds of the CIMAS pioneers when they included this notion in the fundamental policy principles adopted by their Constituent Assembly. It was not until 1954, however, that the Association became actively involved in occupational safety and health activities, through the establishment of its Permanent Committee on Prevention of Occupational Risks. It should be noted that, in this respect, the role of the ISSA is complementary to that of the ILO. The ISSA’s experts may not only be instrumental in bringing about ILO Conventions and Recommendations, but are also called upon to implement them.
Although prevention programmes are obviously most prevalent in the field of occupational safety and health, over the last two decades prevention has gained increasing importance in other branches of social security as well, particularly as regards sickness insurance and, more recently, unemployment insurance, as may be seen from the activities of ISSA Permanent Committees. Over the last decade, activities aimed at preventing employment accidents and occupational diseases have undergone considerable changes in modern industrialized societies, as elaborated below concerning the “Prevention Concept” of the Association.
Structure and Membership
The ISSA is an international organization of services, institutions or bodies administering one or more branches of social security or mutual benefit societies. It has its offices at the headquarters of the ILO in Geneva.
The Association has two categories of membership—affiliate membership, for government departments, central institutions and national federations of institutions administering social security or one of its branches at the national level, and associate membership, open to national non-profit institutions, such as research and safety and health institutions, the aims of which are compatible with those of the Association, but which are not qualified to become affiliate members.
In 1995 the ISSA had over 240 affiliate member organizations in 117 countries, and 95 associate member institutions in 35 countries, for a total membership of some 338 organizations in 127 countries around the world. More than 200 member institutions are directly involved in insurance against employment accidents and occupational diseases and/or in the prevention of accidents and the promotion of safety and health.
Figure 1. Structure of the International Social Security Association (ISSA)

As can be seen from the organigramme (figure 1), all ISSA activities are directed by the General Assembly, which is comprised of delegates appointed by member institutions and is sometimes described as the world parliament of social security. The Council, which consists of one delegate from each country having affiliate member institutions, meets regularly on the occasion of the Association’s triennial General Assemblies. The Bureau, which together with the Council gives effect to the decisions taken by the General Assembly, meets twice a year and is composed of 30 elected members and the Chairpersons of the Permanent Committees.
Activities
The Association has three main programmes:
- Regional activities. These are aimed at serving the special needs of member institutions in the various parts of the world. For this purpose the ISSA has regional offices for Africa, the Americas, Asia and the Pacific and Europe situated in Abidjan, Buenos Aires, Manila and Paris respectively.
- Research and documentation. Worldwide developments and trends in social security are monitored and analysed from the perspective of national and cross-national research through a network of correspondents. The Association maintains the largest social security library in the world and collaborates with the ILO’s Social Security Department in providing timely social security information.
- Technical activities. Ten Permanent Committees and a Study Group each deal with a specific branch or aspect of social security. They investigate sector-specific problems such as those relating to health insurance, pension insurance, unemployment insurance, family protection, rehabilitation, organization and methods, actuarial and statistical issues.
The Permanent Committee on Insurance against Employment Accidents and Occupational Diseases and the Permanent Committee on Prevention of Occupational Risks with its 11 International Sections on Accident Prevention are of particular importance in fostering safety and health.
The Permanent Committee on Prevention of Occupational Risks
Two different and complementary aspects (i.e., promotional activities related to prevention, and technical activities) fall within the scope of competence of this Committee, which together with its Advisory Council monitors worldwide developments and undertakes surveys and studies on overall problem areas.
The Committee is charged with undertaking at the international level the following types of activities for the prevention of occupational risks:
- exchange of information and experience
- organization of international meetings and World Congresses
- implementation of surveys and promotion of research in the field of prevention of occupational risks
- coordination of the activities of the ISSA International Sections for the Prevention of Occupational Risks
- cooperation with the ILO and other agencies active in the prevention of occupational risks
- other measures appropriate to the purposes of the Committee.
World Congresses
Since 1955 the ILO and the ISSA have organized triennial World Congresses on Occupational Safety and Health in cooperation with the ISSA member institutions and ILO constituents concerned in the host country. It is not easy to quantify the extent to which the World Congresses have kept pace with the different stages of development in the prevention of occupational risks coinciding with the social, economic and industrial progress of the past 25 years, or the extent to which they have given a lead to or encouraged this development. There is no doubt however that the resultant exchange of ideas and information relating to recent research and to its practical application in different countries, both at the national level and within industry, has enabled a large number of participants in these Congresses to be cognizant of the many changes being introduced. This, in turn, has enabled them to make a greater contribution to their particular field of activity.
The last four World Congresses took place in Ottawa-Hull (1983), Stockholm (1987), Hamburg (1990), New Delhi (1993) and Madrid (1996). In 1999, the site is Brazil.
ISSA International Sections for Prevention
Since the end of the 1960s, on the advice of the Permanent Committee on Prevention of Occupational Risks and its Advisory Council, the Bureau of the ISSA has set up 11 International Sections for the Prevention of Occupational Risks. Eight of them deal with accident prevention in various sectors of industry and agriculture and three deal respectively with information techniques, research in the area of occupational safety and health, and education and training for prevention of accidents.
Each ISSA International Section is represented by its Chairman and Secretary General on the Advisory Council of the Permanent Committee, which advises the Bureau of the Committee on fundamental questions relating to the activities of the Committee and its International Sections. A concrete example is the prevention concept (discussed separately below).
The International Sections are financially autonomous, having a decentralized structure and their own membership consisting of full members, associate members and corresponding members. Full membership is open to ISSA member institutions and other non-profit organizations; profit-making entities with activities compatible with the area of competence of a Section may be admitted as associate members, and individual experts may apply for corresponding membership. The Secretariats of the Sections are provided in various countries by member institutions of the ISSA specialized in the respective fields.
Each Section is a clearing house for information in its own area of competence. All Sections organize international symposia, round tables and expert meetings, the proceedings and reports of which are published in the ISSA Prevention Series 1000. The Sections currently have some 45 internationally composed working groups working on specific topical subjects, which range, for example, from safety advice for migrant workers in the construction industry or a checklist for the classification of machines on the basis of ergonomic principles, to safe working with biological agents. The findings of these working groups are published as technical brochures in the ISSA Prevention Series 2000. Most titles exist in English, French and German, some also in Spanish and other languages. Such publications may be ordered directly from the Secretariat of the Section concerned.
Of special interest are the International Film and Video Festivals, which are held during World Congresses and for which a Working Group of the Electricity Section forms a clearing house. All productions submitted to these festivals are listed in a catalogue in four languages which is available free from this Section.
A brief description of each of the ISSA International Sections follows.
ISSA International Section for Research.
The Section offers the latest information on both current and planned research projects worldwide. Two data banks allow quick and efficient access to this information. The Working Group “Research Concepts” promotes the necessary theoretical bases to effectively ensure that more than in the past research further serves both the field and the more practical implementation of research results.
ISSA International Section on Information.
The Information Section provides information on efficient information techniques. The Working Group “Safety and Health Periodicals” informs safety experts on the most effective way to reach their audience. The Section offers expert advice on “advertising for safety”.
ISSA International Section for the Mining Industry.
The Section deals with the classical risks of underground work in coal mines (darkness, dust, heat, gases, explosions, cave-ins) and concerns itself with the training of mine rescue teams.
ISSA International Section for the Chemical Industry.
Although new substances result in new risks, the chemical industry has developed high safety standards that have proven to be exemplary. The Chemical Section strives to ensure that these safety standards transcend borders just as much as—if not even more than—risks do.
ISSA International Section for the Iron and Metal Industry.
The high accident rate in this important branch of activity must be reduced. Safety strategies are developed against the most frequent hazards and causes of accident. The Section’s Working Groups are primarily concerned with new technologies and substitutes for dangerous working substances.
ISSA International Section for Electricity.
“Invisible” energy generates many invisible risks. The Section evolves recommendations for practical accident prevention, principles for a regulatory control of electrical appliances and systems, backed up by effective first aid measures in the event of electrical accidents. The Section maintains a clearinghouse for films and videos in the field of safety, health and the environment.
ISSA International Section for the Construction Industry.
The extremely high accident risks in the construction industry call for a safety strategy that can deal with the continuous changes of the working environment on construction sites. The Section’s aim is not only to solve individual problems, but to increase safety and accident prevention in construction industry operations overall, especially by intensified cooperation between the various trades working on the same site.
ISSA International Section for Agriculture.
The mechanization of agriculture and the use of chemical substances in agriculture are worldwide problems. The Section advocates a rapid socio-technical evolution in the light of the technical revolution, while endeavouring to ensure that the production of food does not put life at risk.
ISSA International Section for Machine Safety.
The Section deals with system safety and accident prevention relating to machines, appliances, apparatus and systems. Standardization of safety appliances, ergonomic questions, noise reduction, safety switches and the prevention of dust explosions are focal points of the Section’s Working Groups.
ISSA International Section for Education and Training.
Technical progress is expanding in all areas of life; but at the same time it brings along new risks. The major factor in accidents is the lack of education and training in the field of safety. Safety must be an integrated part of human behaviour in all areas of life. The Section deals with pedagogical aspects of education and training for prevention and aims at a global approach of prevention, making use of the experiences gained in prevention at the workplace for safety in all areas of life.
ISSA International Section for Health Services.
The Section endeavours through international cooperation to overcome the safety deficits in the health sector. The health sector has typical professional risks which in part differ greatly from those in other fields of activity—for instance, direct exposure to diseases, risks from medications, particularly gas anaesthetics, disinfectants and infectious waste.
The ISSA Prevention Concept “Safety Worldwide”
The ISSA Bureau adopted this concept in October 1994 under the title “ISSA Prevention Concept ‘Safety Worldwide’—The Golden Path to Social Policy”.
Because only seven out of every 100 fatal accidents are work accidents, with all others occurring in traffic, in the home, during sports or at school, the concept seeks to make meaningful use, in other areas, of the experience gained in prevention in the world of work.
Starting from the viewpoint that the preservation of health is a fundamental mission of humanity and thus a central aim of social security, the concept calls for the interlinking of prevention, rehabilitation and compensation and for the preservation of an intact environment. Emphasis will be laid on the human factor at the planning, organization and implementation stages and the need to begin education in prevention during early childhood. Efforts will be made to address all those who, through their own activities, can provide better protection against hazards for individuals. These include legislators and standard-setters, social partners, persons responsible for developing, planning, designing and manufacturing products and services, and school curriculum planners and teachers, as well as information specialists in public information work, occupational health physicians, supervisory and consultative bodies, responsible officials in social and private insurance, decision-makers and programme managers in international organizations, professional and other organizations and so on—and, last but not least, parents and children.
The thorough promotion of safety and health at work and elsewhere requires measures of three types—technical measures, behavioural change measures and organizational measures. To this end, the ISSA’s prevention concept defines three levels of intervention:
- informing the general public and developing awareness relating to safety and health matters through the mass media, newspapers, brochures, posters and so on
- achieving both broad and in-depth impact by seeking to change attitudes and behaviour through agents with a multiplier effect and using target-group-specific media and techniques such as educational films and other educational materials
- aiming at an in-depth impact on groups directly at risk through specific measures such as counselling or subject-specific brochures.
The first step in the implementation of the concept will be a stock-taking of prevention activities to determine regional needs and deficiencies. An inventory of existing support facilities and materials will also be drawn up. In addition, the ISSA will step up its information and research activities and its programme of meetings, strengthen cooperation with international organizations active in the prevention field, and take their projects into account in its own activities.
In summary, the only sure way to success lies in cooperation between prevention, rehabilitation and compensation services; the positive experiences of prevention within enterprises must be carried over into non-occupational fields; and greater account must be taken of the human factor.
Publications
The ISSA issues a whole range of periodical and non-periodical publications, studies, surveys, newsletters and bulletins; further information concerning them is contained in the ISSA Catalogue of Publications, which may be ordered free of charge at the following address: ISSA, Case postale 1, CH-1211 Geneva 22, Switzerland.
In addition to the proceedings of World Congresses on Occupational Safety and Health, which are published by the National Organizing Committee of the host country, the publications issued by the International Sections are listed in the ISSA Prevention Series 1000 and 2000, and are also available at the above address.
Ethics in Health Protection and Health Promotion
While occupational health services are becoming more prevalent throughout the world, resources to develop and sustain these activities often do not keep pace with growing demands. Meanwhile, the boundaries of private and work life have been shifting, raising the issue of what can be, or should be, legitimately encompassed by occupational health. Workplace programmes that screen for drugs or HIV seropositivity, or provide counselling for personal problems, are obvious manifestations of the blurring of the boundary between private and work life.
From a public health viewpoint there are good arguments as to why health behaviours should not be compartmentalized into lifestyle factors, workplace factors and broader environmental factors. While the goals of eliminating drug abuse and other deleterious activities are laudable, there are ethical dangers in how these issues are addressed at the workplace. It will also be necessary to ensure that measures against such activities do not displace other health protection measures. The purpose of this article is specifically to examine the ethical issues in health protection and health promotion in the workplace.
Health Protection
Individual and collective protection of workers
While ethical behaviour is essential to all aspects of health care, the definition and promotion of ethical behaviour is often more complex in occupational health settings. The primary care clinician must prioritize the needs of the individual patient, and the community health professional must prioritize the health needs of the collective. The occupational health professional, on the other hand, has a duty to both the individual patient and the collective—the worker, the workforce and the public at large. Sometimes this multiple obligation presents conflicting responsibilities.
In most countries workers have an undeniable legal right to be protected from workplace hazards, and the focus of occupational health programmes should be precisely to address this right. Ethical issues associated with the protection of workers from unsafe conditions are generally those related to the fact that often the employer’s financial interests, or at least perceived financial interests, militate against undertaking the activities needed to protect workers’ health. The ethical stance that the occupational health professional must adopt, however, is clear-cut. As noted in the International Code of Ethics for Occupational Health Professionals (reprinted in this chapter): “Occupational health professionals must always act, as a matter of priority, in the interests of the health and safety of the workers.”
The occupational health professional, whether an employee or a consultant, often experiences pressures to compromise on ethical practice in worker health protection. The professional may even be asked by an employee to serve as an advocate against the organization when legal issues arise or when the employee, or the professional him- or herself, feels that health protection measures are not being provided.
To minimize such real-life conflicts it is necessary to establish societal expectations, market incentives and infrastructural mechanisms to counteract the employer’s real or perceived financial disadvantages in providing worker health protection measures. These may consist of clear regulations that require safe practices, with steep fines for violation of these standards; this, in turn, requires adequate compliance and enforcement infrastructure. It may also comprise a system of workers’ compensation premiums designed to promote prevention practices. Only when societal factors, norms, expectations and legislation reflect the importance of workplace health protection will ethical practice be truly allowed to flourish.
The right to be protected from unsafe conditions and acts of others
Occasionally, another ethical issue arises with respect to health protection: that is the situation in which an individual worker may him- or herself pose a workplace hazard. In keeping with the multiple responsibilities of the occupational health professional, the right of members of the collective (the workforce and the public) to be protected from the acts of others must always be considered. In many jurisdictions “fitness to work” is defined not only in terms of the worker’s ability to do the job, but also to do the job without posing an undue risk to co-workers or the public. It is unethical to deny someone a job (i.e., declare the worker unfit to work) on the basis of a health condition when no scientific evidence exists to substantiate the claim that this condition impairs the worker’s ability to work safely. However, sometimes clinical judgement suggests that a worker may pose a hazard to others, even when the scientific documentation to support a declaration of unfit is weak or even completely lacking. The repercussions, for example, of allowing a worker with undiagnosed dizzy spells to drive a crane, can be extremely serious. Indeed it may be unethical to allow an individual to assume special responsibilities in these cases.
The need to balance individual rights with collective rights is not unique to occupational health. In most jurisdictions it is legally required that a health practitioner report to the public health authorities conditions such as sexually transmitted diseases, tuberculosis or child abuse, even if this requires the breaching of confidentiality of the individuals involved. While there are often no concrete guidelines to assist the occupational health practitioner when formulating such opinions, ethical principles require that the practitioner utilize the scientific literature as thoroughly as possible in combination with his or her best professional judgement. Thus public health and safety considerations must be combined with concerns for the individual worker when performing medical and other exams for jobs with special responsibilities. Indeed screening for drugs and alcohol, if it is to be justified at all as a legitimate occupational health activity, could be justified only on this basis. The International Code of Ethics for Occupational Health Professionals states:
Where the health condition of the worker and the nature of the tasks performed are such as to be likely to endanger the safety of others, the worker must be clearly informed of the situation. In the case of a particularly hazardous situation, the management and, if so required by national regulations, the competent authority, must also be informed of the measures necessary to safeguard other persons.
The emphasis on the individual tends to overlook and indeed ignore the professional’s obligations to the overall good of society or even specific collective groups. For example, when the behaviour of the individual becomes a danger either to self or others, at what point should the professional act on behalf of the collective and override individual rights? Such decisions can have important ramifications for providers of employee assistance programmes (EAPs) who work with impaired workers. The duty to warn co-workers or clients who may use the impaired person’s services, as opposed to the obligation to protect the confidentiality of the person, has to be clearly understood. The professional cannot hide behind confidentiality or the protection of individual rights, as was discussed above.
Health Promotion Programmes
The assumptions and the debate
The assumptions generally underlying lifestyle change promotion activities in the workplace are that:
(l) employees’ daily lifestyle decisions regarding exercise, eating, smoking and stress management have a direct impact on their present and future health, the quality of their lives, and their job performance and (2) a company-sponsored positive lifestyle change programme, administered by full-time personnel but voluntary and open to all employees, will motivate employees to make positive lifestyle changes sufficient to affect both health and quality of life (Nathan 1985).
How far can the employer go in attempting to modify a behaviour such as off-hours drug use, or a condition such as overweight, which does not directly affect others or employee job performance. In health promotion activities, enterprises commit themselves to a role of reformer of those aspects of employees’ lifestyles that are, or are perceived to be, harmful to their health. In other words, the employer may wish to become an agent of social change. The employer may even strive to become the health inspector with regard to those conditions which are deemed to be favourable or unfavourable to health, and implement disciplinary action to keep employees in good health. Some have specific restrictions which prohibit employees from exceeding set body weights. Incentive measures are in place which reduce insurance or other benefits to employees who care for their bodies, especially through exercise. Policies may be used to encourage certain sub-groups, i.e., smokers, to give up practices that are harmful to their health.
Many organizations contend that they do not intend to direct the personal lives of employees, but rather are seeking to influence the workers to act sensibly. However, some question whether employers should intervene in an area that is recognized as private behaviour. Opponents argue that such activities are an abuse of employers’ power. What is rejected is less the legitimacy of the health proposals than the motivation behind them, which appears to be paternalistic and elitist. The health promotion programme may also be perceived to be hypocritical where the employer does not make changes to organizational factors that contribute to ill health, and where the principal motive appears to be cost containment.
Cost containment as the primary motivator
A central feature of the context of worksite-based health services is that the “main” business of the organization is not to provide health care, though services to employees may be seen as an important contribution to the achievement of the organization’s goals, such as efficient operation and cost containment. In most cases, health promotion EAPs and rehabilitation services are provided by employers seeking to meet organizational goals—i.e., a more productive work force, or the reduction of costs of insurance and workers’ compensation. While corporate rhetoric has emphasized the humanitarian motives underlying EAPs, the major rationale and impetus usually involves the organization’s concerns about the costs, absenteeism and loss of productivity associated with mental health problems and abuse of alcohol and drugs. These goals are substantially different from the traditional goals of health practitioners, since they take into consideration the goals of the organization as well as the needs of the patient.
When employers pay directly for the services, and services are provided at the worksite, professionals delivering services must, by necessity, take into account the organizational goals of the employer and the specific culture of the workplace involved. Programmes may be framed in terms of “bottom line impact”; and compromises on goals for health services may need to be made in the face of cost containment realities. The choice of action recommended by the professional may be influenced by these considerations, sometimes presenting an ethical dilemma as to how to balance what would be best for the individual worker with what would be most cost-effective for the organization. Where the professional’s primary responsibility is managed care with a stated goal of cost containment, conflicts may be exacerbated. Considerable caution must therefore be exercised in managed care approaches to ensure that health care objectives are not compromised by efforts to limit or reduce costs.
Which employees are entitled to EAP services, which types of problem should be considered and should the programme be extended to family members or retirees? It would appear that many decisions are based not on the stated intent of improved health but rather the limit of benefit coverage. Part-time staff who have no benefit coverage tend not to have access to EAP services so that the organization does not have to pay additional costs. However, part-time staff may also have problems which affect performance and productivity.
In the trade-off between quality care and lowered costs, who should decide how much quality is required and at what price—the patient, who uses the services but is not accountable for the payment or price, or the EAP gatekeeper, who does not pay the bill but whose job may depend upon the success of the treatment? Should the provider or the insurer, the ultimate payer, take the decision?
Similarly, who should decide when an employee is expendable? And, if insurance and treatment costs dictate such a decision, when is it more cost-efficient to fire an employee—for example, because of mental illness—and then recruit and train a new employee? More discussion of the role of occupational health professionals in addressing such decisions is certainly warranted.
Voluntarism or coercion?
The ethical problems created by unclear client allegiance are immediately evident in EAPs. Most EAP professionals would argue from their clinical training that their legitimate focus is the individual for whom they are the advocates. This concept depends on the notion of voluntarism. That is, the client seeks out assistance voluntarily and consents to the relationship, which is maintained only with his or her active participation. Even where the referral is made by a supervisor or management, the argument is made that participation is still fundamentally voluntary. Similar arguments are made for health promotion activities.
This contention of EAP practitioners that clients are operating on their own free will often falls apart in practice. The notion that participation is entirely voluntary is largely an illusion. Client perceptions of choice are sometimes much less than proclaimed, and supervisory referrals can well be based on confrontation and coercion. So are the majority of so-called self-referrals, which occur after a strong suggestion has been given by a powerful other. While the language is one of choice, it is clear that choices are indeed limited and there is only one right way to proceed.
When health care costs are paid by the employer or through the employer’s insurance, the boundaries between public and private life become less distinct, further increasing the potential for coercion. The current ideology of programmes is one of voluntarism; but can any activity be completely voluntary in the work setting?
Bureaucracies are not democracies and any so-called voluntary behaviour in organizational setting is likely to be open to challenge. Unlike the community setting, the employer has a fairly long term contractual relationship with most employees, which in many cases is dynamic with the possibility of raises, promotions, as well as overt and covert demotions. This may result in deliberate or inadvertent impressions that participation in a particular active preventive programme is normative and expected (Roman 1981).
Health education too must be cautious about claims of voluntarism as this fails to recognize the subtle forces which have great potency in the workplace on shaping behaviour. The fact that health promotion activities receive considerable positive publicity and are also provided free of cost, can lead to the perception that participation is not only supported but highly desired by management. There may be expectations of rewards for participation beyond those related to health. Participation may be seen as necessary to advancement or at least to maintaining one’s profile in the organization.
There may also be a subtle deception on the part of management, which promotes health activities as part of its sincere interest in the well-being of staff, while burying its real concerns related to cost containment expectations. Overt incentives such as higher insurance premiums for smokers or overweight employees may increase participation but at the same time be coercive.
Individual and collective risk factors
The overwhelming focus of work-based health promotion on individual lifestyle as the unit of intervention distorts the complexities underlying social behaviours. Social factors, such as racism, sexism and class bias, are generally overlooked by programmes which focus solely on changing personal habits. This approach takes behaviour out of context and assumes “that personal habits are discrete and independently modifiable, and that individuals can voluntarily choose to alter such behaviour” (Coriel, Levin and Jaco 1986).
Given the influence of social factors, what is the true extent to which people have control over modifying health risks? Certainly behavioural risk factors do exist, but the effects of social structure, the environment, heredity or simple chance must also be taken into account. The individual is not solely responsible for the development of disease, yet this is precisely what many work-site health promotion efforts assume.
A health promotion programme in which individual responsibility can be overstated, leads to moralizing.
Although personal responsibility is undeniably a factor in smoking for example, social influences such as class, stress, education and advertising are also involved. Deeming that only individual factors are causally responsible facilitates blaming the victim. Employees who smoke, are overweight, have high blood pressure, and so on, are blamed, albeit sometimes implicitly, for their condition. This absolves the organization and society from any responsibility for the problem. Employees may be blamed both for the condition and for not doing something about it.
The tendency to assign responsibility solely to the individual ignores a large body of scientific data. Evidence suggests that the physiological sequelae of work may have an impact on health which continues after the workday is done. It has been widely demonstrated that linkages between organizational factors (such as participation in decision making, social interaction and support, pace of work, work overload, etc.), and health outcomes, particularly cardiovascular disease, exist. Implications for organizational interventions, rather than or in addition to individual behaviour change, are quite clear. Nonetheless, most health promotion programmes aim to change individual behaviour but rarely consider such organizational factors.
The focus on individuals is less surprising when it is recognized that most professionals in health promotion, wellness and EAP programmes are clinicians who do not have a background in occupational health. Even when clinicians do identify workplace factors of concern, they are seldom equipped to recommend or carry out organizationally oriented interventions.
Diverting attention from health protection
Rarely have wellness programmes proposed interventions in the corporate culture or included alterations in work organization such as stressful management styles, the content of boring work or noise levels. By ignoring the contribution of the work environment to the health outcomes, popular programmes such as stress management may have a negative impact on health. For example, by focusing on individual stress reduction rather than altering stressful working conditions, workplace health promotion may be helping workers to adapt to unhealthy environments and in the long term increasing disease. Moreover, the research conducted has not provided much support for the clinical approaches. For example, in one study, individual stress management programmes had smaller effects on catecholamine production than did the manipulation of pay systems (Ganster et al. 1982).
In addition, Pearlin and Schooler (1978) found that while various problem-solving, coping responses were effective in one’s personal and family life, this type of coping is not effective in dealing with work-related stressors. Other studies further suggested that some personal coping behaviours actually increase distress if applied in the workplace (Parasuramen and Cleek 1984).
The advocates of wellness programmes are generally uninterested in the traditional concerns of occupational health and, consciously or otherwise, turn attention away from workplace hazards. As wellness programmes generally ignore the risk of occupational disease or hazardous working conditions, health protection advocates fear that individualizing the problem of employee health is an expedient way for some companies to deflect attention from costly but risk-reducing changes in the structure and content of workplace or jobs.
Confidentiality
Employers sometimes feel they have the right to have access to clinical information about workers who receive services from the professional. Yet the professional is bound by the ethics of the profession and by the practical need to maintain the trust of the worker. This problem becomes particularly troublesome if legal proceedings are at issue or if the problem at hand is surrounded by emotionally charged issues, such as disability from AIDS.
Professionals may also become involved in confidential issues related to the employer’s business practices and operations. If the industry in question is highly competitive, the employer may wish to keep secret such information as organizational plans, reorganizations and downsizing. Where business practices may have an impact on the health of employees, how does the professional prevent the occurrence of such adverse effects without jeopardizing the proprietary or competitive secrets of the organization?
Roman and Blum (1987) argue that confidentiality serves to protect the practitioner from extensive scrutiny. Citing client confidentiality, many oppose quality review or peer case review, which might reveal that the practitioner has exceeded the bounds of professional training or expertise. This is an important ethical consideration given the power of the counsellor to influence the health and well-being of clients. The issue is the need to clearly identify for the client the nature of the intervention in terms of what it can or cannot do.
The confidentiality of information collected by programmes which focus on individuals rather than systems of work may be prejudicial to the worker’s job security. Health promotion information can be misused to influence the employee’s status with health insurance or personnel issues. When aggregate data are available, it may be difficult to ensure that such data will not be used to identify individual employees, especially in small work groups.
Where the clinical utilization patterns of the EAP draw attention to a particular work unit or site, practitioners have been loath to bring this to management’s attention. Sometimes the citation of confidentiality issues in reality masks an inability to make reasonable recommendations for intervention due to fears that management will not be receptive to negative feedback about their behaviour or organizational practices. Unfortunately, clinicians sometimes lack the research and epidemiological skills which allow them to present solid data in support of their observations.
Other concerns relate to the misuse of information by a variety of different interest groups. Insurance companies, employers, trade unions, client groups and health professionals may misuse both collective and individual information gathered in the course of a health promotion activity.
Some may use data to deny services or coverage to employees or their survivors in legal or administrative proceedings dealing with compensation or insurance claims. Participants in programmes may believe that the “guarantee of confidentiality” provided by such programmes is inviolate. Programmes need to clearly advise employees that under certain circumstances (i.e., legal or administrative inquiries) personal information gathered by the programme may be made available to other parties.
Aggregate data may be misused so as to shift the burden from one party to another. Access to such information may not be equitable, in that collective information may be available only to organizational representatives and not those individuals seeking benefits. While releasing data on workers focusing on the individual lifestyle contributions to a condition, organizations may be able to restrict information about corporate practices which also created the problem.
Epidemiological data about patterns of conditions or work-related factors should not be gathered in such a manner as to facilitate exploitation by the employer, the insurer, the compensation system or by the clients.
Conflict with other professional or service standards
Professional standards and values may be in conflict with practices already in place in a given organization. Confrontational methods used by occupational alcoholism programmes may be unproductive or in conflict with professional values when dealing with other disorders or disabilities, yet the professional working in this context may be pressured to participate in the use of such methods.
Ethical relationships with outside providers must also be considered. While EAPs have clearly articulated the need for practitioners to avoid referrals to treatment services with which they are closely affiliated, health promotion providers have not been as resolute in defining their relationships with external providers of services that may be attractive to employees for personal lifestyle counselling. Arrangements between EAPs and particular providers which lead to referrals to treatment based on economic advantages to the providers rather than clinical needs of clients present an obvious conflict of interest.
There is also the temptation to engage unqualified individuals in health promotion. EAP practitioners do not normally have the training in health education techniques, physiology or fitness instruction to qualify them to provide such activities. When programmes are provided and administered by management and cost is of primary concern, there is less motivation to scrutinize skills and expertise and to invest in the best qualified professionals, as this will change the cost-benefit outcomes.
The use of peers to provide services raises other concerns. It has been shown that social support from one’s co-workers could buffer the health effects of certain job stressors. Many programmes have capitalized on the positive influence of social support by the use of peer counsellors or self-help support groups. However, while peers can be used as a supplement to some extent, they do not eliminate the need for qualified health professionals. Peers need to have a strong orientation programme, which includes content on ethical practices and not exceeding one’s personal limits or qualifications whether overtly or through misrepresentation.
Drug screening and testing
Drug testing has become a quagmire of regulations and legal interpretation and has not proven to be an effective avenue to either treatment or prevention. The recent report from the National Research Institute (O’Brien 1993) has concluded that drug testing is not a strong deterrent to alcohol and drug abuse. Further evidence suggests that it does not have a significant impact on work performance.
A positive drug test may reveal much about an employee’s lifestyle but nothing about his or her level of impairment or ability to perform work.
Drug testing has been seen as the thin edge of the wedge with which employers drive out all but the most invulnerable employee—the super-resilient person. The trouble is how far does the organization go? Can one test for compulsive behaviours such as gambling or for mental disorders, such as depression?
There is also a concern that organizations may use screening to identify undesirable traits (e.g., predisposition to heart disease or back injury) and to make personnel decisions based on this information. At present this practice appears to be limited to health insurance coverage, but how long can it be resisted by management attempting to reduce cost?
The government-stimulated practice of screening for drugs, and the future possibility of screening for defective genes and excluding whole classes of high-cost employees from health insurance coverage, advances the old presumption that characteristics of workers, not work, explain disabilities and dysfunctions; and this becomes a justification for making workers bear the social and economic costs. This leads again to a perspective in which factors based on the individual, not work, become the focus of health promotion activities.
Exploitation by the client
On occasion it may be clear to the professional that workers are attempting to take improper advantage of the system of services provided by an employer or by its insurance carrier or by workers’ compensation. Problems may include clearly unrealistic rehabilitation demands or outright malingering for financial gain. Appropriate methods of confronting such behaviour, and for taking action as needed, have to be balanced against other clinical realities, such as psychological reactions to disability.
Promotion of activities with questionable effectiveness
Despite the broad claims for worksite health promotion, the scientific data available to evaluate them are limited. The profession as a whole has not addressed the ethical issues of promoting activities which do not have a strong scientific support, or of choosing to engage in services which produce more revenue rather than focusing on ones which have a demonstrated impact.
Ironically, what is being sold is based upon little conclusive evidence of cost reduction, decreased absenteeism, reduced health care expenditures, reductions in employee turnover or increased productivity. Studies are poorly designed, seldom having comparison groups or long-term follow-up. The few that meet the standards of scientific rigour have provided little evidence of a positive return on investment.
There is also some evidence that the participants in worksite health promotion activities tend to be relatively healthy individuals:
Overall it appears participants are likely to be nonsmokers, more concerned with health matters, perceive themselves in better health, and be more interested in physical activities, especially aerobic exercise, than nonparticipants. There is also some evidence that participants may use less health services and be somewhat younger than nonparticipants (Conrad 1987).
Individuals at risk may not be using the health services.
Even where there is evidence to support particular activities and all of the professionals agree on the necessity for such services as follow-up, in practice services are not always provided. Generally EAPs concentrate on finding new cases while devoting little time to workplace prevention. Follow-up services are either non-existent or limited to one or two visits after return to work. With the chronic relapse potential of alcohol and drug cases, it would appear that EAPs are not devoting energies to continuing care, which is very costly to provide, but rather emphasize activities which generate new revenues.
Health examinations for insurance purposes and determination of benefits
Just as the boundary between private life and work factors affecting health has become increasingly blurred, so too has the distinction between fit and unfit or healthy and sick. Thus instead of examinations for insurance or benefits focusing on whether or not a worker is ill or disabled, and therefore “deserving” of benefits, there is an increasing realization that with workplace changes and health promotion activities, the worker, even with his or her illness or disability, can be accommodated. Indeed “adaptation of work to the capabilities of workers in the light of their state of physical and mental health” has been enshrined in the ILO Occupational Health Services Convention, 1985 (No. 161).
The linking of health protection measures and health promotion activities is nowhere as important as it is in addressing workers with special health needs. Just as an indexed patient may reflect pathology in a group, a worker with special health needs may reflect needs in the workforce as a whole. Alteration of the workplace to accommodate such workers very often results in improvements in the workplace that benefit all workers. Providing treatment and health promotion to workers with special health needs may decrease costs to the organization, by containing insurance or workers’ compensation benefits; more importantly, it is the ethical way to proceed.
In recognition that prompt rehabilitation and accommodation of injured workers is “good business,” many employers have introduced early intervention, rehabilitation and return to modified work programmes. Sometimes these programmes are offered through workers’ compensation boards, which have come to realize that both the employer and the individual worker suffer if the benefit system provides an incentive to maintain “the sick role,” rather than an incentive towards physical, mental and vocational rehabilitation.
Conclusion
The International Code of Ethics for Occupational Health Professionals (reprinted in this chapter) provides guidelines to ensure that health promotion activities do not divert attention from health protection measures, and to promote ethical practice in such activities. The Code states:
Occupational health professionals may contribute to public health in different ways, in particular by their activities in health education, health promotion and health screening. When engaging in these programmes, occupational health professionals must seek the participation ... of both employers and workers in their design and in their implementation. They must also protect the confidentiality of personal health data of the workers.
Finally, it is necessary to reiterate that the ethical practice of occupational health could best be promoted by addressing the workplace and societal infrastructure that must be designed to promote the interests of both the individual and the collective. Thus stress management, health promotion and EAPs, which until now have focused almost exclusively on individuals, must address institutional factors in the workplace. It will also be necessary to ensure that such activities do not displace health protection measures.
More...
The International Commission on Occupational Health (ICOH)
Historical Perspective and Raison d’être
The International Commission on Occupational Health (ICOH) is an international non-governmental professional society whose aims are to foster the scientific progress, knowledge and development of occupational health and safety in all its aspects. It was founded in 1906 in Milan as the Permanent Commission on Occupational Health. Today, ICOH is the world’s leading international scientific society in the field of occupational health, with a membership of 2,000 professionals from 91 countries. The ICOH is recognized by the United Nations and has close working relationships with ILO, WHO, UNEP, CEC and ISSA. Its official languages are English and French.
At its founding the Commission had 18 members representing 12 countries. One of its primary tasks was to organize international congresses every three years to exchange ideas and experience among leading scientists in occupational health, a tradition which has continued to this day, with the 25th Congress held in 1996 in Stockholm.
After the London Congress in 1948 the international interest was evident and the Commission was internationalized with changes in its constitution, and the name was changed to Permanent Commission and International Association on Occupation Health, a change finalized in 1957. The internationalization and democratization of the commission grew with time and in 1984 the present name was established.
ICOH provides a forum for scientific and professional communication. To achieve this purpose, the ICOH:
- sponsors international congresses and meetings on occupational health
- establishes scientific committees in various fields of occupational health and related subjects
- disseminates information on occupational health activities
- issues guidelines and reports on occupational health and related subjects
- collaborates with appropriate international and national bodies on matters concerning occupational and environmental health
- takes any other appropriate action related to the field of occupational health
- solicits and administers such funds as may be required in furtherance of its objectives.
Structure and Membership
The ICOH is governed by its officers and board on behalf of its membership. The officers of the ICOH are the President, two Vice-Presidents and the Secretary-General, while the board comprises the past president and 16 members elected from among the general membership. Further, if necessary the President may co-opt two members to the board to represent underrepresented geographical areas or disciplines.
ICOH has both individual and collective members. An organization, society, industry or enterprise may become a sustaining member of the ICOH. A professional organization or a scientific society may become an affiliate member.
Sustaining members may nominate a representative who fulfils the criteria for full membership and enjoys all the benefits of an individual member. An affiliate member may nominate one representative who fulfils the criteria for full membership and enjoys the same rights as a full member. ICOH’s individual members have a wide professional distribution and include medical doctors, occupational hygienists, occupational health nurses, safety engineers, psychologists, chemists, physicists, ergonomics, statisticians, epidemiologists, social scientists and physiotherapists. These professionals work either for universities, institutes of occupational health, governments or industries. At the end of 1993, the largest national groups were those of France, the United States, Finland, Japan, United Kingdom and Sweden, each with more than 100 members. Sustaining and affiliate members can be represented in the General Assembly, and can participate in the activities of scientific committees; they can also submit materials for publication in the newsletter, which also keeps them informed of ongoing and planned activities.
Activities
The most visible activities of ICOH are the triennial World Congresses on Occupational Health, which are usually attended by some 3,000 participants. The 1990 Congress was held in Montreal, Canada, and in 1993 in Nice and the 1996 Congress in Stockholm. The Congress in the year 2000 is scheduled to be held in Singapore. The venues of the triennial congresses since 1906 are listed in table 1.
Table 1. Venues of triennial congresses since 1906
|
Venue |
Year |
Venue |
Year |
|
Milan |
1906 |
Madrid |
1963 |
|
Brussels |
1910 |
Vienna |
1966 |
|
Vienna (cancelled) |
1924 |
Tokyo |
1969 |
|
Amsterdam |
1925 |
Buenos Aires |
1972 |
|
Budapest |
1928 |
Brighton |
1975 |
|
Geneva |
1931 |
Dubrovnik |
1978 |
|
Brussels |
1935 |
Cairo |
1981 |
|
Frankfurt |
1938 |
Dublin |
1984 |
|
London |
1948 |
Sydney |
1987 |
|
Lisbon |
1951 |
Montreal |
1990 |
|
Naples |
1954 |
Nice |
1993 |
|
Helsinki |
1957 |
Stockholm |
1996 |
|
New York |
1960 |
Singapore |
2000 |
At present the ICOH has 26 scientific committees and four working groups, listed in table 2. Most of the committees have regular symposia, publish monographs and preview the abstracts submitted to the international congresses. ICOH issues a quarterly newsletter, which is circulated to all members free of charge. The bilingual newsletter contains congress reports, reviews of publications, a list of coming events and information on research and education, and other announcements relevant to members. Several of the scientific committees also publish monographs and proceedings from their meetings. ICOH keeps a computerized membership file, which is printed at regular intervals and circulated to the membership. The ICOH sponsors its scientific journal, the International Journal of Occupational and Environmental Health (IJOEH). The journal is available for members at a very affordable subscription rate.
Table 2. List of ICOH scientific committees and working groups, 1996
Scientific committees
1. Accident prevention
2. Ageing and work
3. Agriculture
4. Cardiology
5. Chemical industry (Medichem)
6. Computing in occupational and environmental health
7. Construction industry
8. Developing countries
9. Education and training
10. Epidemiology in occupational health
11. Fibres
12. Health-care workers
13. Health services research and evaluation
14. Industrial hygiene
15. Musculoskeletal disorders
16. Neurotoxicology and psychophysiology
17. Occupational health nursing
18. Occupational toxicology
19. Organic dusts
20. Pesticides
21. Radiation and work
22. Occupational health services in small industries
23. Shiftwork
24. Toxicology of metals
25. Work-related respiratory disorders
26. Vibration and noise
Scientific working groups
1. Occupational and environmental dermatoses
2. Handicap and work
3. Reproductive hazards in the workplace
4. Thermal factors
Case Study: Drugs and Alcohol in the Workplace - Ethical Considerations
Introduction
The management of alcohol and drug problems in the workplace can pose ethical dilemmas for an employer. What course of conduct an employer takes involves a balancing of considerations with respect to individuals who have alcohol and drug abuse problems with the obligation to correctly manage the shareholder’s financial resources and safeguard the safety of other workers.
Although in a number of cases both preventive and remedial measures can be of mutual interest to the workers and the employer, in other situations what may be advanced by the employer as good for the worker’s health and well-being may be viewed by workers as a significant restriction on individual freedom. Also, employer actions taken because of concerns about safety and productivity may be viewed as unnecessary, ineffective and an unwarranted invasion of privacy.
Right to Privacy at Work
Workers consider privacy to be a fundamental right. It is a legal right in some countries, but one which, however, is interpreted flexibly according to the needs of the employer to ensure, inter alia, a safe, healthy and productive workforce, and to ensure that a company’s products or services are not dangerous to consumers and the public at large.
The use of alcohol or drugs is normally done in a worker’s free time and off-premises. In the case of alcohol, it can also occur on-premises if this is allowed by local law. Any intrusion by the employer with respect to the worker’s use of alcohol or drugs should be justified by a compelling reason, and should take place by the least intrusive method if costs are roughly comparable.
Two types of employer practices designed to identify alcohol and drug users among job applicants and workers have aroused strong controversy: testing of bodily substances (breath, blood, urine) for alcohol or drugs, and oral or written inquiries into present and past alcohol or drug use. Other methods of identification such as observation and monitoring, and computer-based performance testing, have also raised issues of concern.
Testing of Bodily Substances
The testing of bodily substances is perhaps the most controversial of all methods of identification. For alcohol, this normally involves using a breathalyser device or taking a blood sample. For drugs, the most widespread practice is urinalysis.
Employers argue that testing is useful to promote safety and prevent liability for accidents; to determine medical fitness for work; to enhance productivity; to reduce absenteeism and tardiness; to control health costs; to promote confidence among the public that a company’s products or services are being produced or delivered safely and properly, to prevent embarrassment to the employer’s image, to identify and rehabilitate workers, to prevent theft and to discourage illegal or socially unbecoming conduct by workers.
Workers argue that testing is objectionable because taking samples of bodily substances is very invasive of privacy; that the procedures of taking samples of bodily substances can be humiliating and degrading, particularly if one must produce a urine sample under the watchful eye of a controller to prevent cheating; that such testing is an inefficient way to promote safety or health; and that better prevention efforts, more attentive supervision and the introduction of employee assistance programmes are more efficient ways to promote safety and health.
Other arguments against screening include that testing for drugs (as opposed to alcohol) does not give an indication of current impairment, but only prior use, and therefore is not indicative of an individual’s present ability to perform the job; that testing, particularly drug testing, requires sophisticated procedures; that in case such procedures are not observed, misidentification having dramatic and unfair job consequences may occur; and that such testing can create morale problems between management and labour and an atmosphere of distrust.
Others argue that testing is designed to identify behaviour that is morally unacceptable to the employer, and that there is no persuasive empirical basis that many workplaces have alcohol or drug problems that require pre-employment, random or periodic screening, which constitute severe intrusions into a worker’s privacy because these forms of testing are done in the absence of reasonable suspicion. It has also been asserted that testing for illegal drugs is tantamount to the employer assuming a law enforcement role which is not the vocation or role of an employer.
Some European countries, including Sweden, Norway, the Netherlands and the United Kingdom, allow alcohol and drug testing, although usually in narrowly defined circumstances. For example, in many European countries statutes exist which allow the police to test workers engaged in road, aviation, rail and sea transport, normally based on reasonable suspicion of intoxication on the job. In the private sector, testing has also been reported to occur, but it is usually on the basis of reasonable suspicion of intoxication on the job, in post-accident or post-incident circumstances. Some pre-employment testing and, in very limited cases, periodic or random testing, has been reported in the context of safety-sensitive positions. However, random testing is relatively rare in European countries.
In the United States, different standards apply depending on whether alcohol and drug testing is carried out by the public- or private-sector establishments. Testing conducted by the government or by companies pursuant to legal regulation must satisfy constitutional requirements against unreasonable state action. This has led the courts to allow testing only for safety- and security-sensitive jobs, but to allow virtually all types of testing including pre-employment, reasonable cause, periodic, post-incident or post-accident, and random testing. There is no requirement that the employer demonstrate a reasonable suspicion of drug abuse in a given enterprise or administrative unit, or on the basis of individual use, before engaging in testing. This has led some observers to claim such an approach is unethical because there is no requirement for the demonstration of even a reasonable suspicion of a problem at the enterprise or individual level before any type of testing, including random screening, occurs.
In the private sector, there are no federal constitutional restrictions on testing, although a small number of American states have some procedural and substantive legal restrictions on drug testing. In most American states, however, there are few if any legal restrictions on alcohol and drug testing by private employers and it is performed on an unprecedented scale compared to European private employers, who test principally for reasons of safety.
Inquiries or Questionnaires
Although less intrusive than testing of bodily substances, employer inquiries or questionnaires designed to elicit prior and current use of alcohol and drugs are invasive of workers’ privacy and irrelevant to the requirements of most jobs. Australia, Canada, a number of European countries, and the United States have privacy laws applicable to the public and/or private sectors which require that inquiries or questionnaires be directly relevant to the job in question. In most cases, these laws do not explicitly restrict inquiries about substance abuse, although in Denmark, for example, it is prohibited to collect and store information about excessive use of intoxicants. Similarly, in Norway and Sweden, alcohol and drug abuse are characterized as sensitive data which in principle cannot be collected unless deemed necessary for specific reasons and approved by the data inspectorate authority.
In Germany, the employer can ask questions only to judge the abilities and competence of the candidate with regard to the job in question. A job applicant may answer untruthfully to inquiries of a personal character that are irrelevant. For example, it has been held by court decision that a woman can legally answer that she is not pregnant when in fact she is. Such privacy issues are judicially decided on a case-by-case basis, and whether one could answer untruthfully about one’s present or prior alcohol or drug consumption would probably depend on whether such inquiries were reasonably relevant to performance of the job in question.
Observation and Monitoring
Observation and monitoring are the traditional methods of detection of alcohol and drug problems in the workplace. Simply put, if a worker shows clear signs of intoxication or its after-effects, then he or she can be identified on the basis of such behaviour by the person’s supervisor. This reliance on management supervision to detect alcohol and drug problems is the most widespread, the least controversial and the most favoured by workers’ representatives. The doctrine that holds that treatment of alcohol and drug problems has a higher chance of success if it is based on early intervention, however, raises an ethical issue. In applying such an approach to observation and monitoring, supervisors might be tempted to note signs of ambiguous behaviour or decreased work performance, and speculate about a worker’s private alcohol or drug use. Such minute observation combined with a certain degree of speculation could be characterized as unethical, and supervisors should confine themselves to instances where a worker is clearly under the influence, and hence cannot function in the job at an acceptable level of performance.
The other question that arises is what a supervisor should do when a worker shows clear signs of intoxication. A number of commentators previously felt that the worker should be confronted by the supervisor, who should play a direct role in assisting the worker. However, most observers currently are of the view that such confrontation can be counterproductive and possibly aggravate a worker’s alcohol or drug problems, and that the worker should be referred to an appropriate health service for assessment and, if required, counselling, treatment and rehabilitation.
Computer-Based Performance Tests
Some commentators have suggested computer-based performance tests as an alternative method of detecting workers under the influence of alcohol or drugs at work. It has been argued that such tests are superior to other identification alternatives because they measure current impairment rather than previous use, they are more dignified and less intrusive of personal privacy, and persons can be identified as impaired for any reason, for example, lack of sleep, illness, or alcohol or drug intoxication. The main objection is that technically these tests may not accurately measure the job skills that they purport to measure, that they may not detect low amounts of alcohol and drugs which could potentially affect performance, and that the most sensitive and accurate tests are also those which are the most costly and difficult to set up and administer.
Ethical Issues in Choosing between Discipline and Treatment
One of the most difficult issues for an employer is when discipline should be imposed as a response to an incident of alcohol or drug use at work; when counselling, treatment and rehabilitation should be the appropriate response; and under what circumstances both alternatives—discipline and treatment—should be undertaken concurrently. Bound up in this is the question as to whether alcohol and drug use is essentially behavioural in nature, or an illness. The view that is advanced here is that alcohol and drug use is essentially behavioural in nature, but that consumption of inappropriate quantities over a period of time can lead to a condition of dependence which can be characterized as an illness.
From the employer’s point of view, it is conduct—the worker’s job performance—that is of primary interest. An employer has the right and, in certain circumstances where the worker’s misconduct has implications for the safety, health or economic well-being of others, the duty to impose disciplinary sanctions. Being under the influence of alcohol or drugs at work can be correctly characterized as misconduct, and such a situation can be characterized as serious misconduct if the person occupies a safety-sensitive position. However, a person experiencing problems at work connected to alcohol or drugs may also have a health problem.
For ordinary misconduct involving alcohol or drugs, an employer should offer the worker assistance to determine if the person has a health problem. The decision to refuse an offer of assistance may be a legitimate choice for workers who may choose not to expose their health problems to the employer, or who may not have a health problem at all. Depending on the circumstances, the employer may wish to impose a disciplinary sanction as well.
The response of an employer to a situation involving serious misconduct connected with alcohol or drugs, such as being under the influence of alcohol or drugs in a safety-sensitive position, should probably be different. Here the employer is confronted with both the ethical duty to maintain safety for other workers and the public at large, and the ethical obligation to be fair to the worker concerned. In such a situation, the employer’s principal ethical concern should be to safeguard public safety and immediately remove the worker from the job. Even in the case of such serious misconduct, the employer should assist the worker to obtain health care as appropriate.
Ethical Issues in Counselling, Treatment and Rehabilitation
Ethical issues can also arise with regard to assistance extended to workers. The initial problem that can arise is one of assessment and referral. Such services may be undertaken by the occupational health service in an establishment, by a health care provider associated with an employee assistance programme, or by the worker’s personal physician. If none of the above possibilities exists, an employer may need to identify professionals who specialize in alcohol and drug counselling, treatment and rehabilitation, and suggest that the worker contact one of them for assessment and referral, if necessary.
An employer should also make attempts to reasonably accommodate a worker during absence for treatment. Paid sick leave and other types of appropriate leave should be put at the disposition of the worker to the extent possible for in-patient treatment. If out-patient treatment requires adjustments to the person’s work schedule or transfer to part-time status, then an employer should make reasonable accommodation to such requests, particularly as the individual’s continued presence in the workforce may be a stabilizing factor in recovery. The employer should also be supportive and monitor the worker’s performance. To the extent that the working environment may have contributed initially to the alcohol or drug problem, the employer should make appropriate changes in the working environment. If this is not possible or practical, the employer should consider transferring the worker to another position with reasonable retraining if necessary.
One difficult ethical question which arises is to what extent an employer should continue to support a worker who is absent from work for health reasons due to alcohol and drug problems, and at what stage an employer should dismiss such a worker for reasons of illness. As a guiding principle, an employer should treat absence from work associated with alcohol and drug problems as any absence from work for health reasons, and the same considerations that apply to any dismissal for reasons of health should also be applicable to dismissal for absence due to alcohol and drug problems. Moreover, employers should keep in mind that relapse can occur and is, in fact, part of a process towards complete recovery.
Ethical Issues in Dealing with Illegal Drug Users
An employer is faced with difficult ethical choices when dealing with a worker who uses, or who in the past has used, illegal drugs. The question, for example, has been raised as to whether an employer should dismiss a worker who is arrested or convicted for illegal drug offences. If the offence is of such a serious nature that the person must serve time in prison, evidently the person will not be available for work. However, in many cases consumers or small-time pushers who sell just enough to support their own habit may be given only suspended sentences or fines. In such a case, an employer should ordinarily not consider disciplinary sanctions or dismissal for such off-duty and off-premises conduct. In some countries, if the person has a spent conviction, i.e., a fine that has been paid or a suspended or actual prison sentence that has been completed in full, there may be an actual legal bar against employment discrimination towards the person in question.
Another question that is sometimes posed is whether a previous or current user of illegal drugs should be subject to job discrimination by employers. It is argued here that the ethical response should be that no discrimination should take place against either previous or current users of illegal drugs if it occurs during off-duty time and off the establishment’s premises, as long as the person is otherwise fit to perform the job. In this respect, the employer should be prepared to make a reasonable accommodation in the arrangement of work to a current user of illegal drugs who is absent for purposes of counselling, treatment and rehabilitation. Such a view is recognized in Canadian federal human rights law, which prohibits job discrimination on the basis of disability and qualifies alcohol and drug dependence as a disability. Similarly, French labour law prohibits job discrimination on the basis of health or handicap unless the occupational physician determines the person is unfit for work. American federal law, on the other hand, protects previous illegal drug users from discrimination, but not current users.
As a general principle, if it comes to the attention of an employer that a job applicant or worker uses or is suspected of using illegal drugs off-duty or off-premises, and such use does not materially affect the functioning of the establishment, then there should be no duty to report this information to the law enforcement authorities. Provisions of American law which require testing by government agencies mandate that job applicants and workers who test positive for illegal drugs are not to be reported to law enforcement authorities for criminal prosecution.
If, on the other hand, a worker engages in activity involving illegal drugs on-duty or on-premises, an employer may have an ethical obligation to act either in terms of imposing disciplinary sanction or reporting the matter to law enforcement authorities or both.
An important consideration that employers should keep in mind is that of confidentiality. It may come to the employer’s attention that a job applicant or worker uses illegal drugs because the person may voluntarily disclose such information for health reasons—for example, to facilitate a rearrangement of work during counselling, treatment and rehabilitation. An employer has a strict ethical obligation, and frequently a legal obligation as well, to keep any information of a health character strictly confidential. Such information should not be disclosed to law enforcement authorities or to anyone else without the concerned person’s express consent.
In many cases, the employer may not be aware of whether a worker uses illegal drugs, but the occupational health service will know as a result of examinations to determine fitness for work. The health professional is bound by an ethical duty to maintain the confidentiality of health data, and may also be bound by medical confidentiality. In such circumstances, the occupational health service may report to the employer only whether the person is medically fit or not for work (or fit with reservations), and may not disclose the nature of any health problem or the prognosis to the employer, or to any third-parties such as law enforcement authorities.
Other Ethical Issues
Sensitivity to the working environment
Employers normally have a legal duty to provide a safe and healthy working environment. How this is applied in the context of alcohol and drugs, however, is frequently left to the discretion of employers. Workers’ representatives have argued that many alcohol and drug problems are principally the result of work-related factors such as long hours of work, isolated work, night work, boring or dead-end work, situations involving strained interpersonal relations, job insecurity, poor pay, job functions with high pressure and low influence, and other circumstances resulting in stress. Other factors such as easy access to alcohol or drugs, and corporate practices which encourage drinking on- or off-premises, may also result in substance abuse problems. Employers should be sensitive to such factors and take appropriate remedial actions.
Restrictions on the consumption of alcohol and drugs in the workplace
There is little debate that alcohol and drugs should not be consumed during actual working time in virtually all occupations. However, the more subtle question is whether an establishment should prohibit or restrict the availability of alcohol, for example, in an establishment’s canteen, cafeteria or dining room. Purists would argue that an absolute ban is the appropriate course to take, that the availability of alcohol on an establishment’s premises might actually encourage workers who would not otherwise drink to consume, and that any amount of alcohol consumption can have adverse health effects. Libertarians would argue that such restrictions on a legal activity are unwarranted, and that in one’s free time during meal breaks one should be free to relax and to consume alcohol in moderation if one so desires.
An adequate ethical response, however, lies somewhere between these two extremes and depends heavily on social and cultural factors, as well as the occupational setting. In some cultures, drinking is such a part of the fabric of social and business life that employers have found that making available certain types of alcohol during meal breaks is better than prohibiting it altogether. A prohibition may drive workers off the establishment’s premises to bars or pubs, where actual drinking behaviour may be more extreme. Consumption of greater quantities of alcohol, or of distilled alcohol as opposed to beer or wine, may be the result. In other cultures where drinking is not such an integrated feature of social and business life, a ban on any kind of alcohol being served on company premises may be readily accepted, and not lead to counterproductive results in terms of off-premises consumption.
Prevention through information, education and training programmes
Prevention is perhaps the most important component of any workplace alcohol and drug policy. Although problem drinkers and drug abusers certainly merit special attention and treatment, the majority of workers are moderate drinkers or consume legal drugs such as tranquillizers as a means of coping. Because they constitute the majority of workers, even a small impact on their conduct can have a substantial impact on the potential number of accidents at work, productivity, absenteeism and tardiness.
One can question whether the workplace is an appropriate place to conduct prevention activities through information, education and training programmes. Such prevention efforts have an essentially public health focus on the health risks associated with alcohol and drug consumption generally, and they are aimed at a captive audience of workers who are economically dependent on their employer. The response to these concerns is that such programmes also contain valuable and useful information concerning the risks and consequences of alcohol and drug consumption that are particular to the workplace, that the workplace is perhaps the most structured part of a person’s daily environment and may be a suitable forum for public health information, and that workers tend not to be offended by public health campaigns as a general proposition if they are persuasive but not coercive in terms of recommending a change in behaviour or lifestyle.
Although employers should be sensitive to concerns that public health programmes have a persuasive rather than a coercive orientation, the appropriate ethical choice mitigates in favour of initiating and supporting such programmes not only for the potential good of the establishment in terms of economic benefits associated with fewer alcohol and drug problems, but also for the general well-being of workers.
It should also be remarked that workers have ethical responsibilities with respect to alcohol and drugs in the workplace. Among these ethical responsibilities one could include a duty to be fit for work and to abstain from use of intoxicants immediately before or during work, and a duty to be vigilant with respect to substance use when one exercises safety-sensitive functions. Other ethical precepts could include an obligation to assist colleagues who appear to be having alcohol or drug problems as well as to provide a supportive and friendly work environment for those trying to overcome these problems. Also, workers should cooperate with the employer with respect to reasonable measures taken to promote safety and health in the workplace with respect to alcohol and drugs. However, workers should not be obligated to accept an invasion of their privacy when there is no compelling work-related justification or when the measures requested by the employer are disproportionate to the end to be attained.
In 1995, an ILO international meeting of experts, composed of 21 experts drawn equally from governments, employers’ groups and workers’ organizations, adopted a Code of Practice on the Management of Alcohol- and Drug-related Issues in the Workplace (ILO 1996). This Code of Practice addresses many of the ethical considerations that should be examined when dealing with workplace-related issues concerning alcohol and drugs. The Code of Practice is particularly useful as a reference because it also makes practical recommendations concerning how to manage potential alcohol- and drug-related problems that may arise in the employment context.
International Association of Labour Inspection (IALI)
Historical Perspective and Raison d’être
The International Association of Labour Inspection (IALI) was founded in 1972 in order to provide a professional forum for the exchange of information and experience between inspectors about their work. It promotes closer cooperation and greater understanding between inspectorates, authorities and other institutions of the role, the realities and challenges of labour inspection. The statutes exclude any political, trade union or religious activity and any judgement in respect of the labour law or inspection systems of individual states. The Association is a non-governmental organization (NGO) recognized by the ILO.
Structure and Membership
In 1996, the General Assembly (which meets every three years at the same time as the Triennial Congress) elected a seven-person Executive Committee (EC). The EC elected the President (Germany) and appointed the Honorary Secretary (United Kingdom) as well as the Honorary Treasurer (Switzerland). The four Vice-Presidents came from Spain, Denmark, Tunisia and Hungary. The EC meets as necessary to manage the affairs of the Association, whose registered office is at 23 rue Ferdinand-Hodler, CP3974/1211, Geneva 3, Switzerland. The Secretariat is located at: Hessisches Ministerium fur Frauen, Arbeit und Sozialordnung, Dostojewskistrasse 4, 65187 Wiesbaden, Germany. Tel: +49-611-8173316; Fax: +49-611-86837.
Membership of IALI is open to:
- national and regional labour departments (directorates of labour inspection, safety and hygiene directorates and so on)
- national groups of labour inspectors (associations, unions and so on).
There is an annual membership fee which is dependent upon the size of the organization making the application. This covers the expenses of organizing the programme of activities. In September 1995 the Association comprised 65 member organizations from 50 countries. The majority of members are now labour departments or labour inspectorates.
Activities
By gathering and summarizing information and documentation on particular aspects of labour inspectorate work and by undertaking comparative studies among its members, the Association promotes professional understanding of all aspects of labour inspection and provides opportunities for the exchange of views between practitioners. The technical symposia (organized jointly with member countries) and the triennial congress let inspectors get to know their colleagues personally, to exchange information on problems, solutions and new developments, and to develop their own thinking. These meetings also serve to focus attention in a practical way on a wide range of specific, but carefully chosen, aspects of labour inspection, thus promoting greater consistency of practice between inspectorates in different countries. The proceedings are published and a regular newsletter is also sent to members.
The programmes of IALI are devoted exclusively to the distribution of information collected through international enquiries based on questionnaires and reports from international or regional symposia. There is an international congress every three years in Geneva, undertaken with the generous technical assistance of the ILO at the time of its annual international conference. The ILO also collaborates in the organization of many of the symposia. Since 1974 programmes have been devoted to the study of a wide range of practices in the field of safety, health and the working environment. Topics have included recording systems for premises and accidents, methods of inspecting smaller enterprises, the problems of large construction sites and the use of computers by inspectors. The Association has considered causes of accidents and other problems in relation to the use of robots and other programmable electronic systems. More recently its symposia and congresses have included topics as diverse as human factors, training of inspectors, inspection of public services, child labour, agriculture, risk assessment and occupational health.
The Changing World of Work
The need for a more effective exchange of information and experience has been stimulated by a number of significant developments in the field of labour inspection, including:
- the increasing complexity and breadth of coverage of labour law
- the introduction of new concepts of oversight such as risk assessment and risk management
- the scale and breadth of technological innovation (seen, for instance, in the introduction of new chemicals and compounds, the increasing reliance on programmable electronic systems, genetic manipulation, new applications for ionizing radiation or generally the growth in the use of information technology)
- the changing structure of industry in established market economies, in countries in transition to a market economy and in developing countries
- the growth, in part as a result of the previous development, in the number of small and medium-sized enterprises
- the decline in membership and influence of trade unions, particularly in many industrial market economies
- the pressure on labour inspectorates themselves through budgetary constraints and demands by government that they justify their existence and demonstrate (and where possible improve) their efficiency and effectiveness.
Challenges to Inspection
Affecting all these issues is the increased emphasis on the human factor. Labour inspectors need to analyse, understand and constructively use their skills to help employers and employees to take this central element into account in developing preventive strategies for health and safety. In many countries too there is increasing public awareness of and concern about the consequences of work and work processes. In much forward-looking legislation this is expressed as the aim that no one should be harmed in any way by the need to work. But it is also evident in concerns about the impact of industry and commerce on the environment and the quality of life.
Labour inspectors cannot simply ignore these trends; they have to take the initiative and explain through the media their role, the advice they give and the effect of their compliance work, in order to promote confidence in the constructive work they do. Inspectorates throughout the world have had to review how they work, set their priorities and carry out their inspections so they can devote more time and more of their limited resources to productive activities.
The exchange of information and experience about all these matters is of enormous interest to inspectors. For whilst inspectorates operate in very different political, economic, legal and social climates, experience shows that they have many practical concerns in common and can benefit in a very instructive way from the experience, the different viewpoints, the ideas and the successes and failures of their colleagues in other countries.
International Code of Ethics for Occupational Health Professionals
International Commission on Occupational Health
Introduction
Codes of ethics for occupational health professionals, as distinct from Codes of ethics for medical practitioners, have been adopted during the past ten years by a number of countries. There are several reasons for the development of interest in ethics in occupational health at the national and international levels.
One is the increased recognition of the complex and sometimes competing responsibilities of occupational health and safety professionals towards the workers, the employers, the public, the competent authority and other bodies (public health and labour authorities, social security and judicial authorities). Another reason is the increasing number of occupational health and safety professionals as a result of the compulsory or voluntary establishment of occupational health services. Yet another factor is the development of a multi-disciplinary and intersectoral approach in occupational health which implies an increasing involvement in occupational health services of specialists who belong to various professions.
For the purpose of this Code, the expression “occupational health professionals” is meant to include all those who by profession carry out occupational safety and health activities, provide occupational health services or who are involved in occupational health practice, even if this happens only occasionally. A wide range of disciplines is concerned with occupational health since it is at an interface between technology and health involving technical, medical, social and legal aspects. Occupational health professionals include occupational health physicians and nurses, factory inspectors, occupational hygienists and occupational psychologists, specialists involved in ergonomics, in accident prevention and in the improvement of the working environment as well as in occupational health and safety research. The trend is to mobilise the competence of these occupational health professionals within the framework of a multi-disciplinary approach which may sometimes take the form of a multi-disciplinary team.
Many other professionals from a variety of disciplines such as chemistry, toxicology, engineering, radiation health, epidemiology, environmental health, applied sociology and health education may also be involved, to some extent, in occupational health practice. Furthermore, officials of the competent authorities, employers, workers and their representatives and first aid workers have an essential role and even a direct responsibility in the implementation of occupational health policies and programmes, although they are not occupational health specialists by profession. Finally, many other professions such as lawyers, architects, manufacturers, designers, work analysts, work organisation specialists, teachers in technical schools, universities and other institutions as well as the media personnel have an important role to play in the improvement of the working environment and of working conditions.
The aim of occupational health practice is to protect workers’ health and to promote the establishment and maintenance of a safe and healthy working environment as well as to promote the adaptation of work to the capabilities of workers, taking into account their state of health. A clear priority should be given to vulnerable groups and to underserved working populations. Occupational health is essentially preventive and should help the workers, individually and collectively, in safeguarding their health in their employment. It should thereby help the enterprise in ensuring healthy and safe working conditions and environment, which are criteria of efficient management and are to be found in well-run enterprises.
The field of occupational health is comprehensive and covers the prevention of all impairments arising out of employment, work injuries and work-related diseases, including occupational diseases as well as all aspects relating to the interactions between work and health. Occupational health professionals should be involved, whenever possible, in the design of health and safety equipment, methods and procedures and they should encourage workers’ participation in this field. Occupational health professionals have a role to play in the promotion of workers’ health and should assist workers in obtaining and maintaining employment notwithstanding their health deficiencies or their handicap. The word “workers” is used here in a broad sense and covers all employees, including management staff and the self-employed.
The approach in occupational health is multi-disciplinary and inter-sectoral. There is a wide range of obligations and complex relationships among those concerned. It is therefore important to define the role of occupational health professionals and their relationships with other professionals, with other health professionals and with social partners in the purview of economic, social and health policies and development. This calls for a clear view about the ethics of occupational health professionals and standards in their professional conduct.
In general, duties and obligations are defined by statutory regulations. Each employer has the responsibility for the health and safety of the workers in his or her employment. Each profession has its responsibilities which are related to the nature of its duties. When specialists of several professions are working together within a multi-disciplinary approach, it is important that they base their action on some common principles of ethics and that they have an understanding of each others’ obligations, responsibilities and professional standards. Special care should be taken with respect to ethical aspects, in particular when there are conflicting rights such as the right to the protection of employment and the right to the protection of health, the right to information and the right to confidentiality, as well as individual rights and collective rights.
Some of the conditions of execution of the functions of occupational health professionals and the conditions of operation of occupational health services are often defined in statutory regulations. One of the basic requirements for a sound occupational health practice is a full professional independence, i.e. that occupational health professionals must enjoy an independence in the exercise of their functions which should enable them to make judgements and give advice for the protection of the workers’ health and for their safety within the undertaking in accordance with their knowledge and conscience.
There are basic requirements for acceptable occupational health practice; these conditions of operation are sometimes specified by national regulations and include in particular free access to the work place, the possibility of taking samples and assessing the working environment, making job analyses and participating in enquiries after an accident as well as the possibility to consult the competent authority on the implementation of occupational safety and health standards in the undertaking. Occupational health professionals should be allocated a budget enabling them to carry out their functions according to good practice and to the highest professional standards. This should include adequate staffing, training and re-training, support and access to relevant information and to an appropriate level of senior management.
This code lays down general principles of ethics in occupational health practice. More detailed guidance on a number of particular aspects can be found in national codes of ethics or guidelines for specific professions. Reference to a number of documents on ethics in occupational health are given at the end of this document. The provisions of this code aim to serve as a guide for all those who carry out occupational health activities and cooperate in the improvement of the working environment and working conditions. Its purpose is to contribute, as regards ethics and professional conduct, to the development of common rules for team work and a multi-disciplinary approach in occupational health.
The preparation of this code of ethics was discussed by the Board of ICOH in Sydney in 1987. A draft was distributed to the Board members in Montreal and was subject to a process of consultations at the end of 1990 and at the beginning of 1991. The ICOH Code of Ethics for Occupational Health Professionals was approved by the Board on 29 November 1991. This document will be periodically reviewed. Comments to improve its content may be addressed to the Secretary-General of the International Commission on Occupational Health.
Basic Principles
The three following paragraphs summarize the principles of ethics on which is based the International Code of Ethics for Occupational Health Professionals prepared by the International Commission on Occupational Health (ICOH).
Occupational health practice must be performed according to the highest professional standards and ethical principles. Occupational health professionals must serve the health and social wellbeing of the workers, individually and collectively. They also contribute to environmental and community health.
The obligations of occupational health professionals include protecting the life and the health of the worker, respecting human dignity and promoting the highest ethical principles in occupational health policies and programmes. Integrity in professional conduct, impartiality and the protection of the confidentiality of health data and of the privacy of workers are part of these obligations.
Occupational health professionals are experts who must enjoy full professional independence in the execution of their functions. They must acquire and maintain the competence necessary for their duties and require conditions which allow them to carry out their tasks according to good practice and professional ethics.
Duties and Obligations of Occupational Health Professionals
- The primary aim of occupational health practice is to safeguard the health of workers and to promote a safe and healthy working environment. In pursuing this aim, occupational health professionals must use validated methods of risk evaluation, propose efficient preventive measures and follow-up their implementation. The occupational health professionals must provide competent advice to the employer on fulfilling his or her responsibility in the field of occupational safety and health and they must honestly advise the workers on the protection and promotion of their health in relation to work. The occupational health professionals should maintain direct contact with safety and health committees, where they exist.
- Occupational health professionals must continuously strive to be familiar with the work and the working environment as well as to improve their competence and to remain well informed in scientific and technical knowledge, occupational hazards and the most efficient means to eliminate or to reduce the relevant risks. Occupational health professionals must regularly and routinely, whenever possible, visit the workplaces and consult the workers, the technicians and the management on the work that is performed.
- The occupational health professionals must advise the management and the workers on factors within the undertaking which may affect workers’ health. The risk assessment of occupational hazards must lead to the establishment of an occupational safety and health policy and of a programme of prevention adapted to the needs of the undertaking. The occupational health professionals must propose such a policy on the basis of scientific and technical knowledge currently available as well as of their knowledge of the working environment. Occupational health professionals must also provide advice on a programme of prevention which should be adapted to the risks in the undertaking and which should include, as appropriate, measures for controlling occupational safety and health hazards, for monitoring them and for mitigating their consequences in the case of an accident.
- Special consideration should be given to the rapid application of simple preventive measures which are cost-effective, technically sound and easily implemented. Further investigations must check whether these measures are efficient and a more complete solution must be recommended, where necessary. When doubts exist about the severity of an occupational hazard, prudent precautionary action should be taken immediately.
- In the case of refusal or of unwillingness to take adequate steps to remove an undue risk or to remedy a situation which presents evidence of danger to health or safety, the occupational health professionals must make, as rapidly as possible, their concern clear, in writing, to the appropriate senior management executive, stressing the need for taking into account scientific knowledge and for applying relevant health protection standards, including exposure limits, and recalling the obligation of the employer to apply laws and regulations and to protect the health of workers in his or her employment. Whenever necessary, the workers concerned and their representatives in the enterprise should be informed and the competent authority should be contacted.
- Occupational health professionals must contribute to the information of workers on occupational hazards to which they may be exposed in an objective and prudent manner which does not conceal any fact and emphasises the preventive measures. The occupational health personnel must cooperate with the employer and assist him or her in fulfilling his or her responsibility of providing adequate information and training on health and safety to the management personnel and workers, about the known level of certainty concerning the suspected occupational hazards.
- Occupational health professionals must not reveal industrial or commercial secrets of which they may become aware in the exercise of their activities. However, they cannot conceal information which is necessary to protect the safety and health of workers or of the community. When necessary, the occupational health professionals must consult the competent authority in charge of supervising the implementation of the relevant legislation.
- The objectives and the details of the health surveillance must be clearly defined and the workers must be informed about them. The validity of such surveillance must be assessed and it must be carried out with the informed consent of the workers by an occupational health professional approved by the competent authority. The potentially positive and negative consequences of participation in screening and health surveillance programmes should be discussed with the workers concerned.
- The results of examinations, carried out within the framework of health surveillance must be explained to the worker concerned. The determination of fitness for a given job should be based on the assessment of the health of the worker and on a good knowledge of the job demands and of the worksite. The workers must be informed of the opportunity to challenge the conclusions concerning their fitness for their work that they feel contrary to their interest. A procedure of appeal must be established in this respect.
- The results of the examinations prescribed by national laws or regulations must only be conveyed to management in terms of fitness for the envisaged work or of limitations necessary from a medical point of view in the assignment of tasks or in the exposure to occupational hazards. General information on work fitness or in relation to health or the potential or probable health effects of work hazards, may be provided with the informed consent of the worker concerned.
- Where the health condition of the worker and the nature of the tasks performed are such as to be likely to endanger the safety of others, the worker must be clearly informed of the situation. In the case of a particularly hazardous situation, the management and, if so required by national regulations, the competent authority must also be informed of the measures necessary to safeguard other persons.
- Biological tests and other investigations must be chosen from the point of view of their validity for protection of the health of the worker concerned, with due regard to their sensitivity, their specificity and their predictive value. Occupational health professionals must not use screening tests or investigations which are not reliable or which do not have a sufficient predictive value in relation to the requirements of the work assignment. Where a choice is possible and appropriate, preference must always be given to non-invasive methods and to examinations, which do not involve any danger to the health of the worker concerned. An invasive investigation or an examination which involves a risk to the health of the worker concerned may only be advised after an evaluation of the benefits and the risks involved and cannot be justified in relation to insurance claims. Such an investigation is subject to the worker’s informed consent and must be performed according to the highest professional standards.
- Occupational health professionals may contribute to public health in different ways, in particular by their activities in health education, health promotion and health screening. When engaging in these programmes, occupational health professionals must seek the participation of both employers and workers in their design and in their implementation. They must also protect the confidentiality of personal health data of the workers.
- Occupational health professionals must be aware of their role in relation to the protection of the community and of the environment. They must initiate and participate, as appropriate, in identifying, assessing and advising on the prevention of environmental hazards arising or which may result from operations or processes in the enterprise.
- Occupational health professionals must report objectively to the scientific community on new or suspected occupational hazards and relevant preventive methods. Occupational health professionals involved in research must design and carry out their activities on a sound scientific basis with full professional independence and follow the ethical principles attached to research work and to medical research, including an evaluation by an independent committee on ethics, as appropriate.
Conditions of Execution of the Functions of Occupational Health Professionals
- Occupational health professionals must always act, as a matter of priority, in the interest of the health and safety of the workers. Occupational health professionals must base their judgements on scientific knowledge and technical competence and call upon specialized expert advice as necessary. Occupational health professionals must refrain from any judgement, advice or activity which may endanger the trust in their integrity and impartiality.
- Occupational health professionals must maintain full professional independence and observe the rules of confidentiality in the execution of their functions. Occupational health professionals must under no circumstances allow their judgement and statements to be influenced by any conflict of interest, in particular when advising the employer, the workers or their representatives in the undertaking on occupational hazards and situations which present evidence of danger to health or safety.
- The occupational health professionals must build a relationship of trust, confidence and equity with the people to whom they provide occupational health services. All workers should be treated in an equitable manner without any form of discrimination with regards to age, sex, social status, ethnic background, political, ideological or religious opinions, nature of the illness or the reason which led to the consultation of the occupational health professionals. A clear channel of communication must be established and maintained between occupational health professionals and the senior management executive responsible for decisions at the highest level about the conditions and the organisation of work and the working environment in the undertaking, or with the board of directors.
- Whenever appropriate, occupational health professionals must request that a clause on ethics be incorporated in their contract of employment. This clause on ethics should include, in particular, the right of occupational health specialists to apply professional standards and principles of ethics. Occupational health professionals must not accept conditions of occupational health practice which do not allow for performance of their functions according to the desired professional standards and principles of ethics. Contracts of employment should contain guidance on the legal contractual and ethical position on matters of conflict, access to records and confidentiality in particular. Occupational health professionals must ensure that their contract of employment or service does not contain provisions which could limit their professional independence. In case of doubt, the terms of the contract must be checked with the assistance of the competent authority.
- Occupational health professionals must keep good records with the appropriate degree of confidentiality for the purpose of identifying occupational health problems in the enterprise. Such records include data relating to the surveillance of the working environment, personal data such as the employment history and health-related data such as the history of occupational exposure, results of personal monitoring of exposure to occupational hazards and fitness certificates. Workers must be given access to their own records.
- Individual medical data and the results of medical investigations must be recorded in confidential medical files which must be kept secured under the responsibility of the occupational health physician or the occupational health nurse. Access to medical files, their transmission, as well as their release, and the use of information contained in these files is governed by national laws or regulations and national codes of ethics for medical practitioners.
- When there is no possibility of individual identification, information on group health data of workers may be disclosed to management and workers’ representatives in the undertaking or to safety and health committees, where they exist, in order to help them in their duties to protect the health and safety of exposed groups of workers. Occupational injuries and occupational diseases must be reported to the competent authority according to national laws and regulations.
- Occupational health professionals must not seek personal information which is not relevant to the protection of workers’ health in relation to work. However, occupational physicians may seek further medical information or data from the worker’s personal physician or hospital medical staff, with the worker’s informed consent, for the purpose of protecting the health of this worker. In so doing, the occupational health physician must inform the worker’s personal physician or hospital medical staff of his or her role and of the purpose for which the medical information or data is required. With the agreement of the worker, the occupational physician or the occupational health nurse may, if necessary, inform the worker’s personal physician of relevant health data as well as of hazards, occupational exposures and constraints at work which represent a particular risk in view of the worker’s state of health.
- Occupational health professionals must cooperate with other health professionals in the protection of the confidentiality of the health and medical data concerning workers. When there are problems of particular importance, occupational health professionals must inform the competent authority of procedures or practices currently used which are, in their opinion, contrary to the principles of ethics. This concerns in particular the medical confidentiality, including verbal comments, record keeping and the protection of confidentiality in the recording and in the use of information placed on computer.
- Occupational health professionals must increase the awareness of employers, workers and their representatives of the need for full professional independence and avoid any interference with medical confidentiality in order to respect human dignity and to enhance the acceptability and effectiveness of occupational health practice.
- Occupational health professionals must seek the support of employers, workers and their organisations, as well as of the competent authorities, for implementing the highest standards of ethics in occupational health practice. They should institute a programme of professional audit of their own activities in order to ensure that appropriate standards have been set, that they are being met and that deficiencies, if any, are detected and corrected.
(This article is a reprint of the ICOH published Code.)
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."